Are effective nonsurgical treatments available for women with pelvic organ prolapse?
|
|
|
- Christiana Barker
- 5 years ago
- Views:
Transcription
1
2 Are effective nonsurgical treatments available for women with pelvic organ prolapse? For women with asymptomatic prolapse, education and reassurance are appropriate. Women may not realize that symptoms of voiding or defecatory dysfunction are related to prolapse, so education about how prolapse symptoms manifest can be helpful. ACOG PB 176
3 Are effective nonsurgical treatments available for women with pelvic organ prolapse? Some symptoms related to pelvic organ prolapse may be managed with lifestyle modifications. For example, defecatory dysfunction may improve with fiber supplementation and use of an osmotic laxative Sitting with feet elevated may decrease bulge symptoms. Pelvic muscle exercises, performed either independently or under professional supervision (PT) may improve symptoms or slow the progression of POP ACOG PB 176





4 Vaginal estrogen There is limited evidence for the treatment or prevention of POP with local or systemic estrogen However, some clinicians believe that local estrogen may help with the vaginal irritation associated with POP. ACOG PB 176

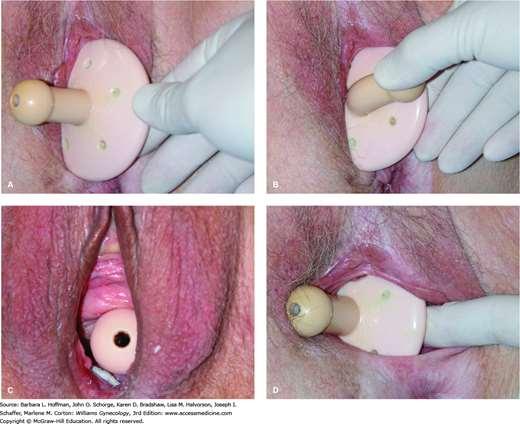
5 Pessary Women considering treatment of POP should be offered a vaginal pessary as an alternative to surgery. A pessary should be considered for a woman with symptomatic POP who wishes to become pregnant in the future. A vaginal pessary is an effective nonsurgical treatment for women with POP, and up to 92% of women can be fitted successfully with a pessary. ACOG PB 176
 and stage III (71%) prolapse, and stage IV prolapse more frequently required Gellhorn")
6 Pessary In one study protocol, a ring pessary was inserted first, followed by a Gellhorn pessary if the ring did not stay in place. Ring pessaries were used more successfully with stage II (100%) and stage III (71%) prolapse, and stage IV prolapse more frequently required Gellhorn pessaries (64%) ACOG PB 176

7
 is necessary.")
8 Pessary If possible, women should be taught to change their pessary independently. If a woman is unable to remove and replace her pessary, regular follow-up (such as every 3 4 months) is necessary. Annual follow-up is recommended for patients who are able to maintain pessary hygiene on their own. ACOG PB 176
9 Pessary management Pressure on the vaginal wall from the pessary may result in local devascularization or erosion in 2 9% of patients. Therapy should consist of removing the pessary for 2 4 weeks and local estrogen therapy. Resolution may occur without local estrogen therapy. ACOG PB 176
10 Pessary management If the problems persist, more frequent pessary changes or a different pessary may be required. Caregivers to patients with dementia should be made aware of the regular pessary changes needed to avoid complications. Although rare complications such as fistula can occur, pessary use is a low-risk intervention that can be offered to all women who are considering treatment of POP. ACOG PB 176
11 When is surgery indicated for the management of pelvic organ prolapse, and what are the primary approaches? Surgery is indicated for the treatment of POP in women who are bothered by their POP and have failed or declined nonsurgical treatments. Important considerations for deciding the type and route of surgery include: location and severity of prolapse nature of the symptoms (eg, presence of urinary, bowel, or sexual dysfunction) patient s general health patient preference, and the surgeon s expertise ACGO PB 176

12 ACOG PB 176
13 Are vaginal surgical approaches effective for the management of pelvic organ prolapse? Vaginal hysterectomy and vaginal apex suspension with vaginal repair of anterior and posterior vaginal wall prolapse as needed are effective treatments for most women with uterovaginal and anterior and posterior vaginal wall prolapse. Vaginal native tissue repairs are performed without the use of synthetic mesh or graft materials. These are relatively low-risk surgeries that may be considered as surgical options for most women with primary POP. ACOG PB 176
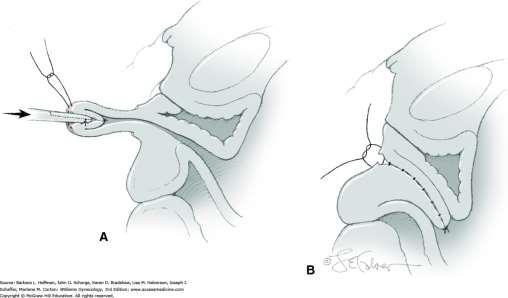
14 If a patient has uterine prolapse, vaginal hysterectomy alone is not adequate treatment. Vaginal apex suspension should be performed at the time of hysterectomy for uterine prolapse to reduce the risk of recurrent POP Vaginal apex suspension involves attachment of the vaginal apex to the uterosacral ligaments or sacrospinous ligaments. Uterosacral and sacrospinous ligament suspension for apical POP with native tissue are equally effective surgical treatments of POP, with comparable anatomic, functional, and adverse outcomes. ACOG PB 176
15


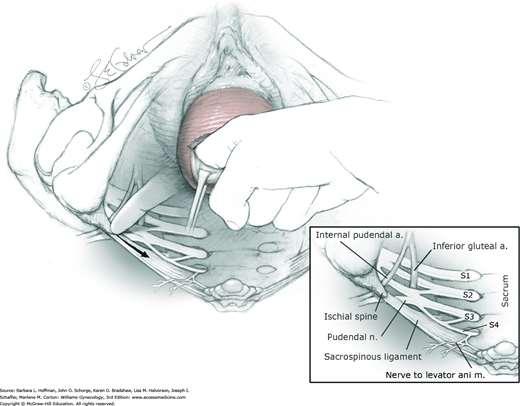
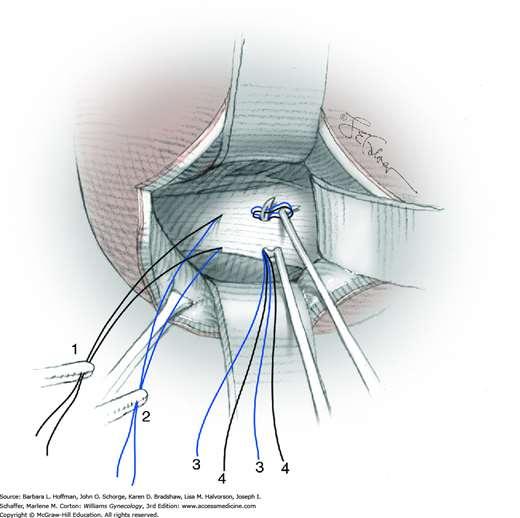
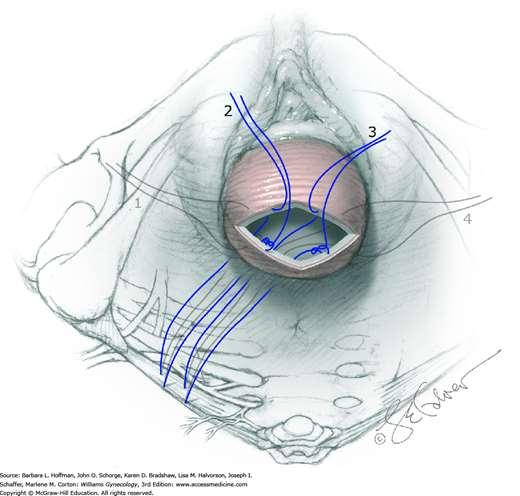
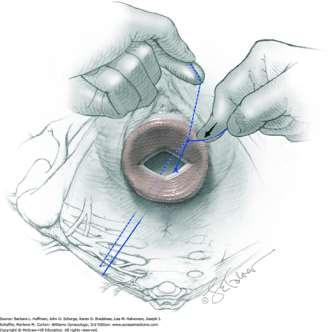
16 SSLF Williams Gyn 3 rd ed
17
18

19
20

21 Surgical Techniques of USLS 1927: Miller - lifting sutures passed through the peritoneum and underlying fascial and muscular structures at the base of the sacro-uterine ligament. 2000: Shull modification composite of those of the master surgeons
22 Anatomy of the Uterosacral Ligament First described in the early 1900 s in the English literture Originating from the posterolateral aspect of the cervix at the level of the internal cervical os and from the lateral vaginal fornix (Campbell) Insertion: Fibers which attached to the fascia covering the levator ani, coccygeus, and obturator muscles, as well as the presacral fascia (Blaisdell) Study of plastinated cross sections could not find a direct attachment to the sacrum (Fritsch et al.) 72
:1483-94.")

23 Anatomy and histology of apical support: a literature review concerning cardinal and uterosacral ligaments Rajeev Ramanah & Mitchell B. Berger & Bernard M. Parratte & John O. L. DeLancey Int Urogynecol J Nov;23(11): USL extends from S2 to S4 vertebra region to the dorsal margin of the uterine cervix and/or to the upper third of the posterior vaginal wall It has a superficial and deep component. Autonomous nerve fibers are a major constituent of the deep USL. Both the deep USL and the caudal CL are closely related to the inferior hypogastric plexus. USL and CL are visceral ligaments, with mesentery-like structures containing vessels, nerves, connective tissue, and adipose tissue.
 (a) showing mainly nerve fibers (n), adipose tissue (ad), and a few vessels (v), and of the cardinal")
24 Histology of USL: Attenuated, poorly organized connective tissue Sparse collagen fibers Muscle fibers Scattered elastin beneath peritoneum Few fibroblasts Adipose tissue Cole et al Fig. 3 Histology after trichrome staining of biopsy specimen of the deep uterosacral ligament (USL) (a) showing mainly nerve fibers (n), adipose tissue (ad), and a few vessels (v), and of the cardinal ligament (CL) (b) showing mainly vessels (v) Ramanah et al. 2012

25 Ramanah et al. 2012

26 Attached broadly to 1 st, 2 nd, and 3 rd sacral vertebrae, variably to 4 th vertebrae Distance from ureter: 0.9 cm at cervical portion 2.3 cm at intermediate portion 4.1 cm at sacral portion Cervical and intermediate portions supported 17 kg before failure
27 MRI of uterosacral ligament origin and insertion Origin Cervix - 33% Cervix and Vagina 63% Vagina- 4% DeLancey. Umek. Uterosacral Ligament Anatomy on MRI. Obstet Gynecol Insertion Sacrospinous ligament/coccygeus muscle complex 82% Sacrum 7% Piriformis muscle, sciatic foramen or ischial spine 11%
 and their insertions (black arrowheads) on the pelvic sidewall are seen.")
28 MRI of uterosacral ligament origin and insertion Figure 1. Axial scan at the level of the cervix. This image demonstrates the uterosacral ligament origins and insertions, and the measuring strategy. The origin of the uterosacral ligaments from the cervix (white arrowheads) and their insertions (black arrowheads) on the pelvic sidewall are seen. The location of the insertion point (b) on a line (ac) between the body midline and the ischium (I) was measured as described in Materials and Methods. The location of the bladder (B), cervix (C), rectum (R), coccyx (X), and coccygeus muscle (CM) are shown. In healthy women, the uterosacral ligament origin and insertion points exhibited greater anatomic variation than their name would imply DeLancey. Umek. Uterosacral Ligament Anatomy on MRI. Obstet Gynecol 2004.


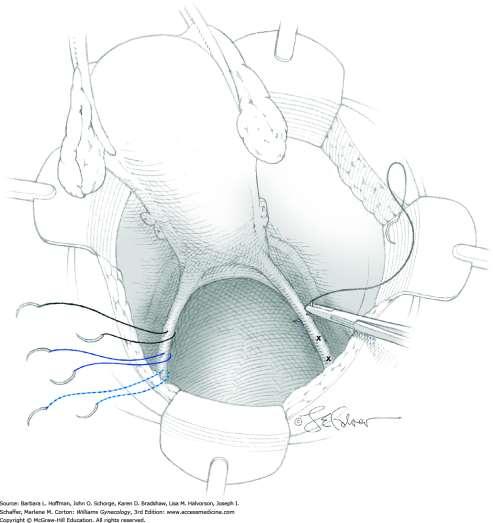
29 Uterosacral Ligament Suspension restores Level 1 vaginal support The USLS suspends the vaginal apex to the proximal remnants of the uterosacral ligaments usually using an intraperitoneal surgical approach Restores the vagina to its normal axis, avoiding the retroflexion associated with SSLS DeLancey
 for the anterior segment 98.3 % (95 % CI 95.7 100 %) for the apical segment 87.4 % (95 % CI, 67.")

30 USLS Meta-analysis of 11 studies anatomical success (POPQ stage 0 1) 81.2 % (95%CI %) for the anterior segment 98.3 % (95 % CI %) for the apical segment 87.4 % (95 % CI, %) for the posterior segment Postoperative prolapse symptoms reported in 5 of the 11 studies in this review and were relieved in % of patients Marguilies et al. Am J Obstet Gynecol 202(2):
31 Williams Gynecology Siddiqui et al.
32 A Transvaginal Approach to Repair of Apical and Other Associated Sites of Pelvic Organ Prolapse with Uterosacral Ligaments Shull BL, BachofenCG, Coates KW, KuehlTJ. Am J ObstetGynecol, 2000: 183; Results: All patients (n= 289) had preoperative or intraoperative evidence of grade 1 or greater apical loss of support of and at least one other site of pelvic organ prolapse. 87% had optimal anatomic outcomes, with no persistent or recurrent support defects at any site 5% had grade 2 or greater persistent or recurrent support defects The anterior segment (bladder) was the site with the most persistent or recurrent support defects, which means that it was the site of the least durable repair. The urethra and cuff had the most durable repairs Morbidity included a 1% transfusion rate, a 1% ureteral injury or ureteral kinking rate, and a 0.3% postoperative death rate.
33 Uterosacral ligament vault suspension: fiveyear outcomes N=72 Mean follow-up period was 5.1 years (range years) Concurrent procedures Vaginal hysterectomy (37.5%) anterior colporrhaphy (58.3%), posterior colporrhaphy (87.5%) suburethral slings (31.9%) Surgical failure (symptomatic recurrent prolapse of stage 2 or greater in any compartment) 15.3% Two patients (2.8%) had recurrence of apical prolapse of stage 2 or greater Silva WA, Pauls RN, Segal JL, Rooney CM, Kleeman SD,Karram MM. Uterosacral ligament Vault suspension: Fiveyear outcomes.obstet Gynecol2006;108:

34 Uterosacral Ligament Suspension (57283)
35
36
37
38 Abdominal USLS Retrospective review of 107 women 75 completed 1 year follow up 12% reported recurrent or persistent prolapse symptoms 7% had anatomic failure of Stage 2 or greater prolapse 9% erosion rate of apical Gortex sutures average time to erosion 56 mo (3-75 mos) Lowenstein et al, 2009
39 Laparoscopic USLS Retrospective comparison 96 vaginal USLS vs 22 laparoscopic USLS No significant differences in perioperative morbidity or anatomical or subjective outcomes Failure at the Apex Vaginal - 6.3% Laparoscopic 0% Ureteral compromise in 4.2% of vaginal group None in laparoscopic group Rardin et al 2009

40 Abdominal approach USLS
41 Complications of Uterosacral Ligament Suspension Ureteral kinking/injury rate of 1 11 % Ureteral reimplantation rate in this series was only 0.6 % Blood transfusions were reported in 1.3 % Cystotomy in 0.1 % Bowel injury in 0.2 % A review of 700 consecutive vaginal prolapse surgeries found intraopertive uretreral kinking/injury of 5.9% directly attributable to the USLS 87% were identified at cystoscopy before the completion of the index surgery and were relieved by removing suspension sutures intraoperatively with no long-term consequences for the patient. Marguiles et al 2010, Guistilo-Ashby et al. 2006

42 Ureter 1.4 cm from uterosacral ligament at cervix al. Elkins et Distance from ureter: 0.9 cm at cervical portion 2.3 cm at intermediate portion 4.1 cm at sacral portion Buller,
43 Recognition and management of nerve entrapment pain after uterosacral ligament suspension Chung CP, Kuehl TJ, Larsen WI, Yandell PM, Shull BL. Results: Eight (1.6%) of 515 patients had neuropathic pain requiring suture removal from the affected side Operative pain was recognized after discontinuation of intravenous narcotics on postoperative day 1 Patients reported their pain improved after removal of all sutures on the affected side Patients with neuropathic pain did not differ from those without regard to age, BMI, and preoperative prolapse stage, or in the number of sutures placed None of the eight had recurrent pelvic organ prolapse (POP), with a median follow-up of 5 months Chung CP, KuehlTJ, Larsen WI, Yandell PM, Shull BL. Recognition and Management of Nerve Entrapment Pain After Uterosacral Ligament Suspension. Obstet& Gynecol Vol120; No 2, Part 1, August 2012 pp
 traverses the peritoneum only, whereas the green (deep UR-6) and white (deep CT-1) sutures are visualized encircling S2 and S3 nerves. SP, sacral promontory. Siddiqui.")
44 Suture entrapment of S2/S3 sacral nerves. Image of right hemipelvis with peritoneum reflected off of underlying structures (*). The S2, S3, and S4 sacral nerve roots are marked. The blue suture (Allis) traverses the peritoneum only, whereas the green (deep UR-6) and white (deep CT-1) sutures are visualized encircling S2 and S3 nerves. SP, sacral promontory. Siddiqui. Nerve Entrapment in Uterosacral Ligament Suspension. Obstet Gynecol 2010.

45 Schematic of pelvis with sacral nerves. The circular zone denotes locations where nerve entrapment was identified in cadaveric specimens. IS, ischial spine; LS, lumbosacral trunk; S2-S5, sacral nerve roots; R, rectum; V, vagina; U, urethra. Illustration by Stan Coffman. Siddiqui. Nerve Entrapment in Uterosacral Ligament Suspension. Obstet Gynecol 2010.

46 Neural Entrapment During Uterosacral Ligament Suspension Bilateral Uterosacral ligament suspension was performed in 10 unembalmed female cadavers using different techniques described in literature Median location of sutures relative to the ischial spine did not differ significantly by suture technique Portions of sacral nerve roots were encircled by uterosacral ligament suspension sutures in 7 cadavers There were no instances of nerve entrapment when sutures were placed while tenting the ligament with an Allis clamp, although these sutures contained a less substantial purchase of connective tissue. In six cadavers, sacral nerves were encircled by sutures placed using a dorsal and posterior arc, regardless of the needle size. Entrapment was more likely with sutures placed into the right hemipelvis compared with the left (43% compared with 13%; P.001). CONCLUSION: Sacral nerve roots are the most vulnerable neural structures during uterosacral ligament suspension. Suture placement directly into the uterosacral ligament with a dorsal and posterior needle arc results in a higher risk of nerve entrapment compared with ventral tenting of the ligament. Siddiqui. Nerve Entrapment in Uterosacral Ligament Suspension. Obstet Gynecol 2010.
47 In the Operations and Pelvic Muscle Training in the Management of Apical Support Loss (OPTIMAL) trial (2014) 2-year follow-up surgical success rate 64.5% (n=186) for uterosacral ligament suspension compared with 63.1% (n=188) for sacrospinous ligament fixation (adjusted odds ratio [OR], 1.1; 95% confidence interval [CI], ) The serious adverse event rate at 2-year follow-up was 16.5% for uterosacral ligament suspension compared with 16.7% for sacrospinous ligament fixation (adjusted OR, 0.9; 95% CI, ) Barber JAMA 2014 ACOG PB 176
48 Vaginal surgery has been the defining characteristic of the gynecologic surgeon since the successful repair of urinary fistulas >100 years ago. The majority of cases of prolapse of the vagina can be successfully operated upon via the vagina. The cure is not infrequently difficult, and a great deal of surgical ingenuity is required. Richard W. TeLinde, 1966

49
50 Cochrane Database Syst Rev Apr 30 Surgical management of pelvic organ prolapse in women. Maher C1, Feiner B, Baessler K, Schmid C. Conclusions: -Sacral colpopexy has superior outcomes to a variety of vaginal procedures including sacrospinous colpopexy, uterosacral colpopexy and transvaginal mesh. These benefits must be balanced against a longer operating time, longer time to return to activities of daily living, and increased cost of the abdominal approach.
51 Anterior vaginal wall repair Anterior colporrhaphy is an effective treatment for most anterior vaginal wall prolapse Many women with anterior vaginal wall prolapse also have an apical prolapse In these women, surgery should correct the apical prolapse and the anterior vaginal wall prolapse Resupport of the vaginal apex concurrently with repair of the anterior vaginal wall defect reduces the risk of recurrent POP surgery ACOG PB 176
52 Anterior vaginal wall repair Paravaginal defects are lateral detachments of the vaginal wall from the fascial condensations over the levator ani muscles Diagnosis of paravaginal defects by physical examination is unreliable If a paravaginal defect is suspected, there usually is apical loss of support Apical support procedures may address most anterior vaginal wall defects, including paravaginal defects ACOG PB 176



53 Anterior vaginal wall repair Williams Gyn 3 rd ed

54 Paravaginal defect repair
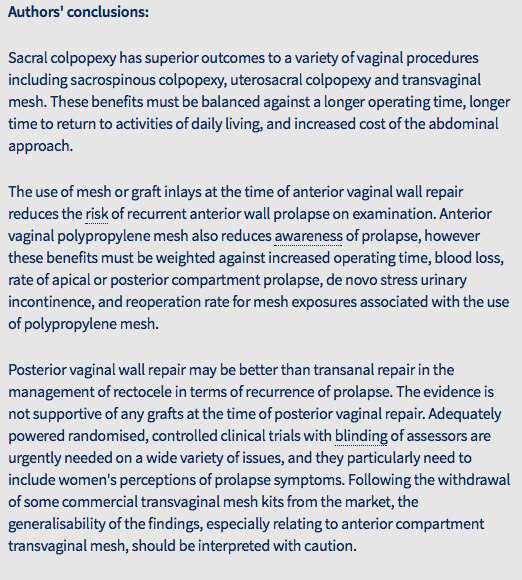
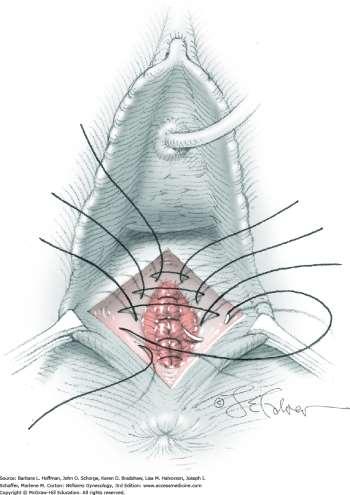
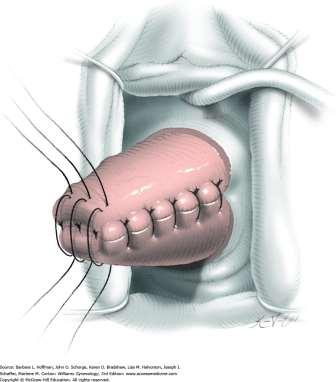
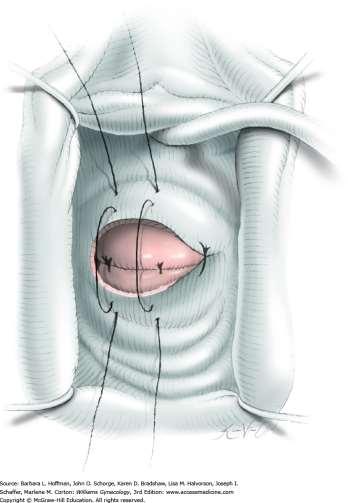
55 Posterior vaginal wall repair Posterior vaginal wall repair traditionally has been performed through a midline plication of the posterior vaginal wall fibromuscular connective tissue. The repair should be performed without placing tension on the levator ani muscles because this may lead to dyspareunia. Perineorrhaphy that results in reattachment of the perineal muscles to the rectovaginal septum can be performed as needed if a perineal defect is present. ACOG PB 176
56 Posterior vaginal wall repair An alternative technique for performing posterior vaginal wall repair is site-specific repair, which involves dissection of the vaginal epithelium off the underlying fibromuscular connective tissue and repair of localized tissue defects with sutures. Although a retrospective comparison of site-specific repair and midline colporrhaphy found that site-specific repair was associated with a higher rate of recurrence of a symptomatic bulge (11% versus 4%, P=.02) a prospective study showed comparable outcomes for the two techniques. ACOG PB 176


57 Posterior vaginal wall repair

58 Posterior vaginal wall repair
59 Perineorrhaphy
60 When is abdominal sacrocolpopexy indicated for the management of pelvic organ prolapse? Abdominal sacrocolpopexy is a proven and effective surgery for the treatment of POP. This procedure involves placement of a synthetic mesh or biologic graft from the apex of the vagina to the anterior longitudinal ligament of the sacrum. ACOG PB 176
61 When is abdominal sacrocolpopexy indicated for the management of pelvic organ prolapse? Women who may be candidates for abdominal sacrocolpopexy include those who have a shortened vaginal length, intra-abdominal pathology, or risk factors for recurrent POP (eg, age younger than 60 years, stage 3 or 4 prolapse, and body mass index greater than 26). In women who are at increased risk of synthetic mesh-related complications (eg, chronic steroid use, current smoker), sacrocolpopexy with a biologic graft or alternatives to a sacrocolpopexy could be considered. ACOG PB 176
62 Abdominal sacrocolpopexy Studies evaluating abdominal sacrocolpopexy with biologic grafts show conflicting results. Abdominal sacrocolpopexy with porcine dermis xenograft had efficacy similar to that of abdominal sacrocolpopexy with synthetic polypropylene mesh. However, the porcine dermal xenograft used in this study is no longer available. ACOG PB 176
63 Abdominal sacrocolpopexy In a study that evaluated the 5-year surgical outcomes of abdominal sacrocolpopexy among patients randomized to receive polypropylene mesh or cadaveric fascia lata, use of synthetic mesh resulted in better anatomic cure than use of cadaveric fascia lata grafts (93% [27 out of 29] versus 62% [18 out of 29], P=.02). Abdominal sacrocolpopexy with synthetic mesh has a lower risk of recurrent POP but is associated with more complications than vaginal apex repair with native tissue. ACOG PB 176
64 Abdominal sacrocolpopexy Data from randomized controlled trials also show a significantly greater likelihood of anatomic success with mesh abdominal sacrocolpopexy compared with vaginal apex repair with native tissue (pooled OR, 2.04; 95% CI, ). Surgical complications that are more common after abdominal sacrocolpopexy with mesh include ileus or small-bowel obstruction (2.7% versus 0.2%, P<.01), thromboembolic phenomena (0.6% versus 0.1%, P=.03), and mesh or suture complications (4.2% versus 0.04%, P<.01). ACOG PB 176
65 Sacrocolpopexy with mesh is associated with a significant reoperation rate due to mesh-related complications. Long-term (ie, 7-year) follow-up of participants of the Colpopexy and Urinary Reduction Efforts (CARE) trial found that the estimated rate of mesh complications (erosion into the vagina, visceral erosions, and sacral osteitis) was 10.5% (95% CI, ), with a significant number of reoperations. ACOG PB 176
66 Many of the CARE trial sacrocolpopexies, however, were performed with non-type 1 mesh, which may have increased the mesh complication rate. Because of complications attributed to multifilament and smallpore-size synthetic mesh, type 1 synthetic meshes (monofilament with large pore size) currently are used in the United States. ACOG PB 176
67 Do patients benefit from a minimally invasive approach to pelvic organ prolapse surgery? Sacrocolpopexy with or without supracervical hysterectomy or total hysterectomy can be performed laparoscopically with or without robotic assistance. Although open abdominal sacrocolpopexy is associated with shorter operative times (222 minutes versus 296 minutes; P<.02) minimally invasive sacrocolpopexy is associated with less blood loss (122 ± 146 ml versus 187 ± 142 ml; P<.01) shorter hospitalization (1.3 ± 1 days versus 2.9 ± 1.6 days; P<.01) ACOG PB 176
68 Do patients benefit from a minimally invasive approach to pelvic organ prolapse Similar results were seen in RCT that compared open ASC with laparoscopic sacrocolpopexy mean blood loss was significantly greater in the open arm (mean difference [MD] 184 ml; 95% CI, ) fewer inpatient days in the laparoscopic group (MD, 0.9 days; 95% CI, ). ACOG PB 176
69 Minimally Invasive Sacrocolpopexy Although robotic assistance shortens the learning curve for performing laparoscopic sacrocolpopexy and improves surgeon ergonomics, it has not been shown to improve short-term outcomes for patients. In two randomized controlled trials that compared robot-assisted sacrocolpopexy with laparoscopic sacrocolpopexy, operating time, postoperative pain, and cost were found to be significantly greater in the robot-assisted group. The groups had similar anatomic and functional outcomes 6 months to 1 year after surgery, although the robotic experience of the surgeons was low at the start of the study, which may have affected the results. ACOG PB 176
70 Minimally invasive Sacrocolpopexy Overall, the current literature is too scant to adequately indicate which minimally invasive approach should be recommended. Further comparative studies that assess long-term anatomic and functional outcomes and patient safety and that identify subgroups of patients who would benefit from a robotic approach are warranted. ACOG PB 176

71 Is posterior vaginal wall prolapse repair more effective with a transanal or transvaginal incision? Posterior vaginal wall prolapse repair is more effective when performed through a transvaginal incision than a transanal incision. Systematic review findings show that, compared with transanal incision, posterior vaginal repair results in fewer recurrent prolapse symptoms (relative risk [RR], 0.4; 95% CI, ), lower recurrence on clinical examination (RR, 0.2; 95% CI, ), and a smaller mean depth of rectocele on postoperative defecography (MD, 1.2 cm; 95% CI, 2.0 to 0.3). AOCG PB 176
72 Are surgical approaches available to treat pelvic organ prolapse in women with medical comorbidities? Obliterative procedures which narrow, shorten, or completely close the vagina are effective for the treatment of POP and should be considered a first-line surgical treatment for women with significant medical comorbidities who do not desire future vaginal intercourse or vaginal preservation. Obliterative procedures have high reported rates of objective and subjective improvement of POP (98% and 90%, respectively) and are associated with a low risk of recurrent POP. ACOG PB 176
73 Are surgical approaches available to treat pelvic organ prolapse in women with medical comorbidities? Because obliterative surgical procedures can be performed under local or regional anesthesia, these procedures may be especially beneficial for the treatment of POP in women with significant medical comorbidities that preclude general anesthesia or prolonged surgery, such as cardiac disease, chronic obstructive pulmonary disease, or thromboembolic disease. Le Fort-style partial colpocleisis Total colpectomy ACOG PB 176


74 Le Fort-style partial colpocleisis Williams Gyn 3 rd ed

75 Le Fort-style partial colpocleisis Williams Gyn 3 rd ed

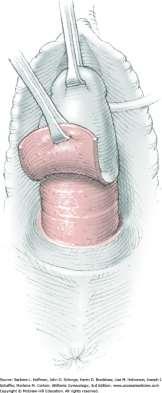
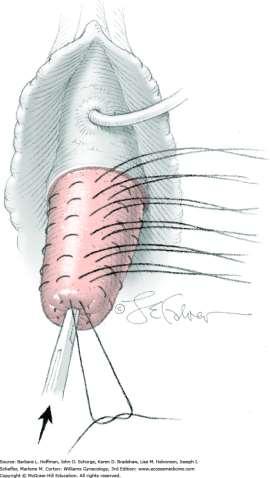
76 Williams Gyn 3 rd ed Colpocleisis - Complete colpectomy
77 Colpocleisis Are surgical approaches available to treat pelvic organ prolapse in women with medical comorbidities? Obliterative procedures are associated with low rates of: Complications - 6.8%, intensive care unit admissions, - 2.8%, Mortality 0.15% ACOG PB 176
78 Colpocleisis Patients undergoing obliterative procedures must be committed to no longer having vaginal sexual intercourse. In a multisite prospective study of older women (mean age 79 years) who underwent obliterative repair of POP, 95% of patients (125 out of 132) reported being satisfied or very satisfied with the results of the procedure 1 year after surgery. Patient regret also has been reported to be low. Among women interviewed more than 1 year after obliterative prolapse repair, only 9% (3 out of 32) reported they regretted having the procedure. ACOG PB 176
79 What can be recommended regarding currently available synthetic mesh and biologic graft materials for use in vaginal pelvic organ prolapse surgery? The use of synthetic mesh or biologic grafts in POP surgery is associated with unique complications not seen in POP repair with native tissue. A systematic review of seven randomized controlled trials that compared native tissue repair with synthetic mesh vaginal prolapse repair found that more women in the mesh group required repeat surgery for the combined outcome of prolapse, stress incontinence, or mesh exposure (RR, 2.40; 95% CI, ). The rate of mesh exposure was 12%, and 8% of women required repeat surgery for mesh exposure up to 3 years after the initial surgery. ACOG PB 176
80 What can be recommended regarding currently available synthetic mesh and biologic graft materials for use in vaginal pelvic organ prolapse surgery? Systematic review findings show that vaginal repair of prolapse with biologic grafts (tissue from human cadaver or other species) results in similar rates of awareness of prolapse and reoperation for prolapse compared with repairs using native tissue. However, it is difficult to make an overall recommendation about the use of biologic grafts for vaginal prolapse repair because the available evidence is of low quality, and most of the biologic grafts that were used in studies to date are no longer available. ACOG PB 176
81 Synthetic mesh placed through a transvaginal incision to correct POP has been studied extensively although there are few long-term (greater than 3 years) studies regarding the effectiveness of procedures currently being performed many transvaginal mesh products were removed from the market following the 2011 U.S. Food and Drug Administration (FDA) announcement that identified serious safety and effectiveness concerns over the use of transvaginal mesh to treat POP ACOG PB 176
82 In January 2016, the FDA issued two final orders regarding surgical mesh that is used to repair POP transvaginally : 1. The FDA reclassified this surgical mesh from class II, which generally includes moderate-risk devices, to class III, which generally includes highrisk devices. 2. The FDA required manufacturers to submit a premarket approval application to support the safety and effectiveness of surgical mesh for the transvaginal repair of POP. Subsequently, in January 2017, the FDA reclassified all urogynecologic surgical mesh instrumentation (whether used for transvaginal POP repair or other urogynecologic surgical mesh procedures) from class I (low risk) exempt from premarket notification to class II (moderate risk) and subject to premarket notification. ACOG PB 176
83 ACOG PB 176 Posterior Vaginal Repair The use of synthetic mesh or biologic grafts in transvaginal repair of posterior vaginal wall prolapse does not improve outcomes. In addition, there are increased complications (eg, mesh exposure) associated with placement of mesh through a posterior vaginal wall incision. In two randomized trials that compared native tissue with biologic graft material for the repair of posterior prolapse, the objective failure rate was significantly lower at the 1-year follow up in the native tissue group (10% [10 out of 98]) as compared with the biologic graft group (21% [20 out of 93]) (RR, 0.47; 95% CI, ), and the subjective failure rate was similar between the groups (RR, 1.09; 95% CI, ) (58, 75, 87). There was no difference in the rate of postoperative dyspareunia between the groups (RR, 1.26; 95% CI, ).
84 ACOG PB 176 Posterior Vaginal Repair Another trial that compared posterior biologic graft repair with traditional repair noted worse anatomic outcomes with posterior biologic graft repair than with traditional repair (46% versus 14%; P=0.02) (19, 58). Thus, synthetic mesh or biologic grafts should not be placed routinely through posterior vaginal wall incisions to correct POP for primary repair of posterior vaginal wall prolapse.
85 Anterior Vaginal Repair Polypropylene mesh improves anatomic and some subjective outcomes but does not affect reoperation rates for recurrent prolapse and is associated with a higher rate of complications compared with native tissue vaginal prolapse repair. ACOG PB 176



86 Transvaginal mesh for POP repair Pelvic organ prolapse vaginal mesh repair should be limited to high-risk individuals in whom the benefit of mesh placement may justify the risk, such as individuals with recurrent prolapse (particularly of the anterior or apical compartments) or with medical comorbidities that preclude more invasive and lengthier open and endoscopic procedures. Before placement of synthetic mesh grafts in the anterior vaginal wall, patients should provide their informed consent after reviewing the benefits and risks of the procedure and discussing alternative repairs. ACOG PB 176
87 Is special training required to perform pelvic organ prolapse procedures that use mesh or biologic grafts? Surgeons who perform POP surgery with biologic grafts or synthetic mesh grafts should have training specifically for these procedures and should be able to counsel patients regarding the risk benefit ratio for the use of mesh compared with native tissue repair. There are unique risks and complications associated with the use of mesh in surgeries to treat POP. ACOG PB 176
88 Is special training required to perform pelvic organ prolapse procedures that use mesh or biologic grafts? Special training regarding patient selection, anatomy, surgical technique, postoperative care, and management of complications is necessary for physicians who perform POP surgery using mesh or biologic grafts. The American Urogynecologic Society has published guidelines for training and privileging for the performance of abdominal sacrocolpopexy and vaginal mesh prolapse surgery. ACOG PB 176
89 Are there effective pelvic organ prolapse surgical treatment methods available for women who prefer to avoid hysterectomy? Women who desire surgical treatment of POP may choose to avoid hysterectomy for a variety of reasons, including preservation of fertility, maintenance of body image, and beliefs about adverse effects on sexual function. Alternatives to hysterectomy for the surgical treatment of POP include hysteropexy (ie, uterine suspension) and Le Fort colpocleisis. ACOG PB 176
90 Hysteropexy Hysteropexy is a viable alternative to hysterectomy in women with uterine prolapse, although there is less available evidence on safety and efficacy compared with hysterectomy. Hysteropexy may be performed through a vaginal incision by attaching the cervix to the sacrospinous ligament with sutures or mesh. Hysteropexy also may be performed abdominally or laparoscopically by placing a mesh or biologic graft from the cervix to the anterior longitudinal ligament. ACOG PB 176
91 Hysteropexy Shortening the uterosacral ligaments laparoscopically with or without robotic assistance or by an abdominal incision also can be performed. A 2016 cohort study that compared laparoscopic sacral hysteropexy with vaginal mesh hysteropexy found that, at 1- year follow-up, the two procedures had similar efficacy and no significant differences in the rate of complications, blood loss, or length of hospitalization. ACOG PB 176

92 Benefits of hysteropexy compared with total hysterectomy include shorter operative time and a lower incidence of mesh erosion if mesh augmentation is used. In comparison, women with uterine prolapse who choose hysterectomy will have a lower risk of uterine and cervical cancer or any procedures that involve abnormalities of the cervix or uterus (eg, endometrial biopsy). They will not become pregnant and will not have uterine bleeding or pain. ACOG PB 176


93 Can the occurrence of stress urinary incontinence after surgery for pelvic organ prolapse be anticipated and avoided? All women with significant apical prolapse, anterior prolapse, or both should have a preoperative evaluation for occult stress urinary incontinence, with cough stress testing or urodynamic testing with the prolapse reduced. ACOG PB 176
94 Summary of Recommendations and Conclusions The following recommendations and conclusions are based on good and consistent scientific evidence (Level A): Uterosacral and sacrospinous ligament suspension for apical POP with native tissue are equally effective surgical treatments of POP, with comparable anatomic, functional, and adverse outcomes. ACOG PB 176
95 The following recommendations and conclusions are based on good and consistent scientific evidence (Level A): The use of synthetic mesh or biologic grafts in transvaginal repair of posterior vaginal wall prolapse does not improve outcomes. ACOG PB 176
96 The following recommendations and conclusions are based on good and consistent scientific evidence (Level A): Polypropylene mesh augmentation of anterior vaginal wall prolapse repair improves anatomic and some subjective outcomes but does not affect reoperation rates for recurrent prolapse and is associated with a higher rate of complications compared with native tissue vaginal prolapse repair. ACOG PB 176
97 The following recommendations and conclusions are based on limited or inconsistent scientific evidence (Level B): Many women with POP on physical examination do not report symptoms of POP. Treatment is indicated only if prolapse is causing bothersome bulge and pressure symptoms, sexual dysfunction, lower urinary tract dysfunction, or defecatory dysfunction. Women considering treatment of POP should be offered a vaginal pessary as an alternative to surgery. ACOG PB 176
98 The following recommendations and conclusions are based on limited or inconsistent scientific evidence (Level B): Vaginal apex suspension should be performed at the time of hysterectomy for uterine prolapse to reduce the risk of recurrent POP. Abdominal sacrocolpopexy with synthetic mesh has a lower risk of recurrent POP but is associated with more complications than vaginal apex repair with native tissue. ACOG PB 176
99 The following recommendations and conclusions are based on limited or inconsistent scientific evidence (Level B): Obliterative procedures which narrow, shorten, or completely close the vagina are effective for the treatment of POP and should be considered a firstline surgical treatment for women with significant medical comorbidities who do not desire future vaginal intercourse or vaginal preservation. ACOG PB 176
100 The following recommendations and conclusions are based on limited or inconsistent scientific evidence (Level B): The use of synthetic mesh or biologic grafts in POP surgery is associated with unique complications not seen in POP repair with native tissue. Hysteropexy is a viable alternative to hysterectomy in women with uterine prolapse, although there is less available evidence on safety and efficacy compared with hysterectomy. ACOG PB 176
101 The following recommendations are based primarily on consensus and expert opinion (Level C): A POP-Q examination is recommended before treatment for the objective evaluation and documentation of the extent of prolapse. A pessary should be considered for a woman with symptomatic POP who wishes to become pregnant in the future. ACOG PB 176
102 The following recommendations are based primarily on consensus and expert opinion (Level C): Pelvic organ prolapse vaginal mesh repair should be limited to high-risk individuals in whom the benefit of mesh placement may justify the risk, such as individuals with recurrent prolapse (particularly of the anterior or apical compartments) or with medical comorbidities that preclude more invasive and lengthier open and endoscopic procedures. Before placement of synthetic mesh grafts in the anterior vaginal wall, patients should provide their informed consent after reviewing the benefits and risks of the procedure and discussing alternative repairs. ACOG PB 176
103 The following recommendations are based primarily on consensus and expert opinion (Level C): Surgeons who perform POP surgery with biologic grafts or synthetic mesh grafts should have training specifically for these procedures and should be able to counsel patients regarding the risk benefit ratio for the use of mesh compared with native tissue repair. ACOG PB 176
104 The following recommendations are based primarily on consensus and expert opinion (Level C): Routine intraoperative cystoscopy during POP surgery is recommended when the surgical procedure performed is associated with a significant risk of injury to the bladder or ureter. These procedures include suspension of the vaginal apex to the uterosacral ligaments, sacrocolpopexy, and anterior colporrhaphy and the placement of mesh in the anterior and apical compartments. ACOG PB 176
105 The following recommendations are based primarily on consensus and expert opinion (Level C): All women with significant apical prolapse, anterior prolapse, or both should have a preoperative evaluation for occult stress urinary incontinence, with cough stress testing or urodynamic testing with the prolapse reduced. ACOG PB 176
106 The following recommendations are based primarily on consensus and expert opinion (Level C): Patients with POP but without stress urinary incontinence who are undergoing either abdominal or vaginal prolapse repair should be counseled that postoperative stress urinary incontinence is more likely without a concomitant continence procedure but that the risk of adverse effects is increased with an additional procedure. ACOG PB 176
107 ACOG video of prolapse
108 ACOG Patient handouts

109

110 Pelvic organ prolapse (POP): the herniation of the pelvic organs to or beyond the vaginal walls
111 Resources: Utube video: Uterosacral Ligament Suspension, Walters and Schull Cleveland Clinic Uterosacral ligament Suspension, Karram Contemporary OBGYN AUGS video: Anatomy of Sacrospinous ligament, Delancy Resident membership to AUGS References ACOG Practice Bulletin 176, April 2017 Walters & Karram, Urogynecology and Reconstructive Surgery 4 Williams Gynecoloty 2 nd ed th ed
112 In the 2006 CARE Trial, sacrocolpopexies were done with and without Burch In women with POP having ASC who were continent before surgery, Burch decreased the rate of post-operative SUI (32% for Burch vs 45% for no Burch) For women with occult SUI on pre-testing, 37% had SUI after Burch and 60% had SUI after no Burch For women with no occult SUI on pre-testing, 20% had SUI after Burch and 39% had SUI after no Burch However, it is still controversial what to do to the bladder neck in women with symptomatic prolapse having vaginal surgery who have no SUI on preoperative testing with reduction
113 OPUS Trial In this multicenter RCT, 337 women without SUI but having vaginal surgery for POP were randomized to TVT or sham surgery The rate of UI at 12 months was 27.6% in the TVT group and 43.0% in the sham group (P=0.002) 6.3 slings were placed to prevent 1 case of UI at 12 months UTI s, bleeding complications (3.1%), and voiding disorders (3.7%) were all higher in the TVT group Wei JT, et al. N Engl J Med 2012; 366:
114 References Blaisdell FE. The anatomy of the sacro-uterine ligaments. Anat Record 1917;12:1 42. Campbell RM. The anatomy and histology of the sacrouterine ligaments. Am J Obstet Gynecol 1950;59:1 12. Umek WH, Morgan DM, Ashton-Miller JA, DeLancy JO. Quantitative analysis of uterosacral ligament origin and insertion points by magnetic resonance imaging. Obstetrics & Gynecology. 103(3):447-51, 2004 Mar. Nichols DH. Types of prolapse. In: Nichols DH, Randall CL, editors. Vaginal surgery. 4th ed. Baltimore (MD): Williams & Wilkins; p Buller JL, Thompson JR, Cundiff GW, Krueger Sullivan L, Schon Ybarra MA, et al. Uterosacral ligament: description of anatomic relationships to optimize surgical safety. Obstet Gynecol 2001;97: Fritsch H, Hotzinger H. Tomographical anatomy of the pelvis, visceral pelvic connective tissue, and its compartments. Clin Anat 1995;8: Siddiqui. Nerve Entrapment in Uterosacral Ligament Suspension. Obstet Gynecol Barber MD, Visco AG, Weidner AC, Amundsen CL, Bump RC. Bilateral uterosacral ligament vaginal vault suspension with site-specific endopelvic fascia defect repair for treatment of pelvic organ prolapse. Am J Obstet Gynecol 2000;183: Shull BL, Bachofen C, Coates KW, Kuehl TJ. A transvaginal approach to repair of apical and other associated sites of pelvic organ prolapse with uterosacral ligaments. Am J Obstet Gynecol 2000;183: Aronson MP, Aronson PK, Howard AE, Morse AN, Baker SP, Young SB. Low risk of ureteral obstruction with deep (dorsal/posterior) uterosacral ligament suture placement for transvaginal apical suspension. Am J Obstet Gynecol 2005;192: Buller JL, Thompson JR, Cundiff GW, Krueger Sullivan L, Schon Ybarra MA, Bent AE. Uterosacral ligament: description of anatomic relationships to optimize surgical safety. Obstet Gynecol 2001;97: Natale F, La Penna C, Padoa A, Agostini M, Panei M, Cervigni M (2010) High levator myorrhaphy versus uterosacral ligament sus- pension for vaginal vault fixation: a prospective, randomized study. Int Urogynecol J Pelvic Floor Dysfunct 21(5):
115 References Flynn MK, Weidner AC, Amundsen CL. Sensory nerve injury after uterosacral ligament suspension. Am J Obstet Gynecol 2006;195: Lowenstein L, Dooley Y, Kenton K, Mueller E, Brubaker L. Neural pain after uterosacral ligament vaginal suspension. Int Urogynecol J Pelvic Floor Dysfunct 2007;18: Wieslander CK, Roshanravan SM, Wai CY, Schaffer JI, Corton MM. Uterosacral ligament suspension sutures: anatomic relationships in unembalmed female cadavers. Am J Obstet Gynecol 2007;197:672e1 6. Siddique SA, Gutman RE, Schon Ybarra MA, Rojas F, Handa VL. Relationship of the uterosacral ligament to the sacral plexus and to the pudendal nerve. Int Urogynecol J Pelvic Floor Dysfunct 2006;17: Schon Ybarra MA, Gutman RE, Rini D, Handa VL. Etiology of post-uterosacral suspension neuropathies. Int Urogynecol J Pelvic Floor Dysfunct 2009;20: Collins SA, Downie SA, Olson TR, Mikhail MS. Nerve injury during uterosacral ligament fixation: a cadaver study. Int Urogynecol J Pelvic Floor Dysfynct 2009;20: Cheryl B. Iglesia, MD, Andrew I. Sokol, MD, Eric R. Sokol, MD, Bela I. Kudish, MD, Robert E. Gutman, MD, Joanna L. Peterson, RN, and Susan Shott, PhD, Vaginal Mesh for Prolapse A Randomized Controlled Trial Obstets & Gynecol VOL. 116, NO. 2, PART 1, AUGUST 2010 Robert E. Gutman, MD, Patrick A. Nosti, MD, Andrew I. Sokol, MD, Eric R. Sokol, MD, Joanna L. Peterson, RN, Hong Wang, PMD, MS, and Cheryl B. Iglesia, MD, Three-Year Outcomes of Vaginal Mesh for Prolapse A Randomized Controlled Trial. Obstet Gynecol 2013;122:770 7)
PRACTICE BULLETIN Female Pelvic Medicine & Reconstructive Surgery Volume 23, Number 4, July/August 2017
 PRACTICE BULLETIN Number 176, April 2017 (Replaces Committee Opinion Number 513, December 2011) Pelvic Organ Prolapse Pelvic organ prolapse (POP) is a common, benign condition in women. For many women
PRACTICE BULLETIN Number 176, April 2017 (Replaces Committee Opinion Number 513, December 2011) Pelvic Organ Prolapse Pelvic organ prolapse (POP) is a common, benign condition in women. For many women
International Federation of Gynecology and Obstetrics
 International Federation of Gynecology and Obstetrics COMMITTEE FOR UROGYNAECOLOGY AND PELVIC FLOOR MEMBER: TSUNG-HSIEN (CHARLES) SU, CHAIR (TAIWAN) DAVID RICHMOND, CO-CHAIR (UK) CHITTARANJAN PURANDARE,
International Federation of Gynecology and Obstetrics COMMITTEE FOR UROGYNAECOLOGY AND PELVIC FLOOR MEMBER: TSUNG-HSIEN (CHARLES) SU, CHAIR (TAIWAN) DAVID RICHMOND, CO-CHAIR (UK) CHITTARANJAN PURANDARE,
Understanding Pelvic Organ Prolapse. Stephanie Pickett, MD, MS Female Pelvic Medicine and Reconstructive Surgery
 Understanding Pelvic Organ Prolapse Stephanie Pickett, MD, MS Female Pelvic Medicine and Reconstructive Surgery Disclosures None I am the daughter of a physician assistant. Objectives List types of pelvic
Understanding Pelvic Organ Prolapse Stephanie Pickett, MD, MS Female Pelvic Medicine and Reconstructive Surgery Disclosures None I am the daughter of a physician assistant. Objectives List types of pelvic
Traditional Anterior, Posterior, and Apical Compartment Repairs A Technique Based Review
 Traditional Anterior, Posterior, and Apical Compartment Repairs A Technique Based Review Sandip Vasavada, MD Center for Female Urology and Pelvic Reconstructive Surgery The Glickman Urological and Kidney
Traditional Anterior, Posterior, and Apical Compartment Repairs A Technique Based Review Sandip Vasavada, MD Center for Female Urology and Pelvic Reconstructive Surgery The Glickman Urological and Kidney
Karanvir Virk M.D. Minimally Invasive & Pelvic Reconstructive Surgery 01/28/2015
 Karanvir Virk M.D. Minimally Invasive & Pelvic Reconstructive Surgery 01/28/2015 Disclosures I have none Objectives Identify the basic Anatomy and causes of Pelvic Organ Prolapse Examine office diagnosis
Karanvir Virk M.D. Minimally Invasive & Pelvic Reconstructive Surgery 01/28/2015 Disclosures I have none Objectives Identify the basic Anatomy and causes of Pelvic Organ Prolapse Examine office diagnosis
What are we talking about? Symptoms. Prolapse Risk Factors. Vaginal bulge 1 Splinting. ?? Pelvic pressure Back pain 1 Urinary complaints 2
 Options for Vaginal Prolapse What are we talking about? Michelle Y. Morrill, M.D. Director of Urogynecology The Permanente Medical Group Kaiser, San Francisco Assistant Professor, Volunteer Faculty Department
Options for Vaginal Prolapse What are we talking about? Michelle Y. Morrill, M.D. Director of Urogynecology The Permanente Medical Group Kaiser, San Francisco Assistant Professor, Volunteer Faculty Department
Interventional procedures guidance Published: 28 June 2017 nice.org.uk/guidance/ipg583
 Sacrocolpopexy using mesh to repair vaginal vault prolapse Interventional procedures guidance Published: 28 June 2017 nice.org.uk/guidance/ipg583 Your responsibility This guidance represents the view of
Sacrocolpopexy using mesh to repair vaginal vault prolapse Interventional procedures guidance Published: 28 June 2017 nice.org.uk/guidance/ipg583 Your responsibility This guidance represents the view of
SURGICAL. How to manage the cuff at vaginal hysterectomy. For personal use only. Copyright Dowden Health Media TECHNIQUES
 For mass reproduction, content licensing and permissions contact Dowden Health Media. How to manage the cuff at vaginal hysterectomy The high McCall culdoplasty and its modifications can prevent apical
For mass reproduction, content licensing and permissions contact Dowden Health Media. How to manage the cuff at vaginal hysterectomy The high McCall culdoplasty and its modifications can prevent apical
By:Dr:ISHRAQ MOHAMMED
 By:Dr:ISHRAQ MOHAMMED Protrusion of an organ or structure beyond its normal confines. Prolapses are classified according to their location and the organs contained within them. 1-Anterior vaginal wall
By:Dr:ISHRAQ MOHAMMED Protrusion of an organ or structure beyond its normal confines. Prolapses are classified according to their location and the organs contained within them. 1-Anterior vaginal wall
Gynecology Dr. Sallama Lecture 3 Genital Prolapse
 Gynecology Dr. Sallama Lecture 3 Genital Prolapse Genital(utero-vaginal )prolapse is extremely common, with an estimated 11% of women undergoing at least one operation for this condition. Definition: A
Gynecology Dr. Sallama Lecture 3 Genital Prolapse Genital(utero-vaginal )prolapse is extremely common, with an estimated 11% of women undergoing at least one operation for this condition. Definition: A
LAPAROSCOPIC REPAIR OF PELVIC FLOOR
 LAPAROSCOPIC REPAIR OF PELVIC FLOOR Dr. R. K. Mishra Elements comprising the Pelvis Bones Ilium, ischium and pubis fusion Ligaments Muscles Obturator internis muscle Arcus tendineus levator ani or white
LAPAROSCOPIC REPAIR OF PELVIC FLOOR Dr. R. K. Mishra Elements comprising the Pelvis Bones Ilium, ischium and pubis fusion Ligaments Muscles Obturator internis muscle Arcus tendineus levator ani or white
9/24/2015. Pelvic Floor Disorders. Agenda. What is the Pelvic Floor? Pelvic Floor Problems
 Management of Pelvic Floor Disorders Doctor, I don t want THAT mesh! Agenda What are pelvic floor disorders (PFDs)? What are the treatment options? Expectant. Conservative. Surgical. How and when are grafts
Management of Pelvic Floor Disorders Doctor, I don t want THAT mesh! Agenda What are pelvic floor disorders (PFDs)? What are the treatment options? Expectant. Conservative. Surgical. How and when are grafts
SACROSPINOUS LIGAMENT FIXATION, A SAFE AND EFFECTIVE WAY TO MANAGE VAGINAL VAULT PROLAPSE.A 10-YEAR OBSERVATIONAL STUDY OF CLINICAL PRACTICE
 Original Article, A SAFE AND EFFECTIVE WAY TO MANAGE VAGINAL VAULT PROLAPSE.A 10-YEAR OBSERVATIONAL STUDY OF CLINICAL PRACTICE * ** Fauzia Rasool Memon, Mohamed Matar * Consultant Obstetrician and Gynecologist
Original Article, A SAFE AND EFFECTIVE WAY TO MANAGE VAGINAL VAULT PROLAPSE.A 10-YEAR OBSERVATIONAL STUDY OF CLINICAL PRACTICE * ** Fauzia Rasool Memon, Mohamed Matar * Consultant Obstetrician and Gynecologist
Surgical repair of vaginal wall prolapse using mesh
 NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE Interventional procedure consultation document Surgical repair of vaginal wall prolapse using mesh Vaginal wall prolapse happens when the normal support
NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE Interventional procedure consultation document Surgical repair of vaginal wall prolapse using mesh Vaginal wall prolapse happens when the normal support
Long-Term Effectiveness of Uterosacral Colpopexy and Minimally Invasive Sacral Colpopexy for Treatment of Pelvic Organ Prolapse
 ORIGINAL ARTICLE Long-Term Effectiveness of Uterosacral Colpopexy and Minimally Invasive Sacral Colpopexy for Treatment of Pelvic Organ Prolapse Cecile A. Unger, MD, MPH, Matthew D. Barber, MD, MHS, Mark
ORIGINAL ARTICLE Long-Term Effectiveness of Uterosacral Colpopexy and Minimally Invasive Sacral Colpopexy for Treatment of Pelvic Organ Prolapse Cecile A. Unger, MD, MPH, Matthew D. Barber, MD, MHS, Mark
Prolapse & Stress Incontinence
 Advanced Pelvic Floor Course Prolapse & Stress Incontinence OVERVIEW Day One and morning of Day Two- Pelvic Organ Prolapse The Prolapse component covers the detailed anatomy of POP including the DeLancey
Advanced Pelvic Floor Course Prolapse & Stress Incontinence OVERVIEW Day One and morning of Day Two- Pelvic Organ Prolapse The Prolapse component covers the detailed anatomy of POP including the DeLancey
PL Narducci Department of Obstetrics and Gynecology General Hospital San Giovanni Battista Foligno, ITALY
 NESA DAYS 2018 New European Surgical Academy Perugia, April 19-21, 2018 EXCELLENCE IN FEMALE SURGERY PROLAPSE RECONSTRUCTIVE SURGERY IN SEXUALLY ACTIVE WOMEN LAPAROSCOPIC ANTERIOR ABDOMINAL WALL COLPOPEXY
NESA DAYS 2018 New European Surgical Academy Perugia, April 19-21, 2018 EXCELLENCE IN FEMALE SURGERY PROLAPSE RECONSTRUCTIVE SURGERY IN SEXUALLY ACTIVE WOMEN LAPAROSCOPIC ANTERIOR ABDOMINAL WALL COLPOPEXY
ROBOTIC MESH SACROCOLPOPEXY
 ROBOTIC MESH SACROCOLPOPEXY Philippe E. Zimmern, MD, FACS Professor of Urology Mesh sacrocolpopexy Background First described in 1962 by Lane Until then, treatment options were: Pessary Colpocleisis Vaginal
ROBOTIC MESH SACROCOLPOPEXY Philippe E. Zimmern, MD, FACS Professor of Urology Mesh sacrocolpopexy Background First described in 1962 by Lane Until then, treatment options were: Pessary Colpocleisis Vaginal
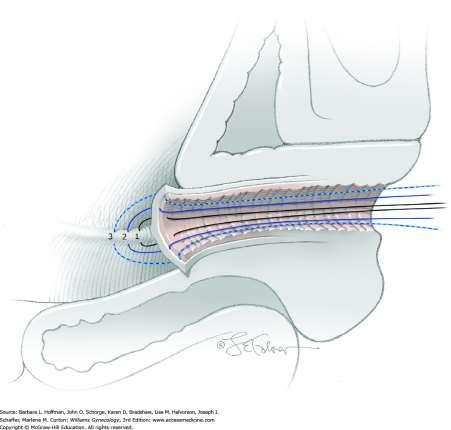
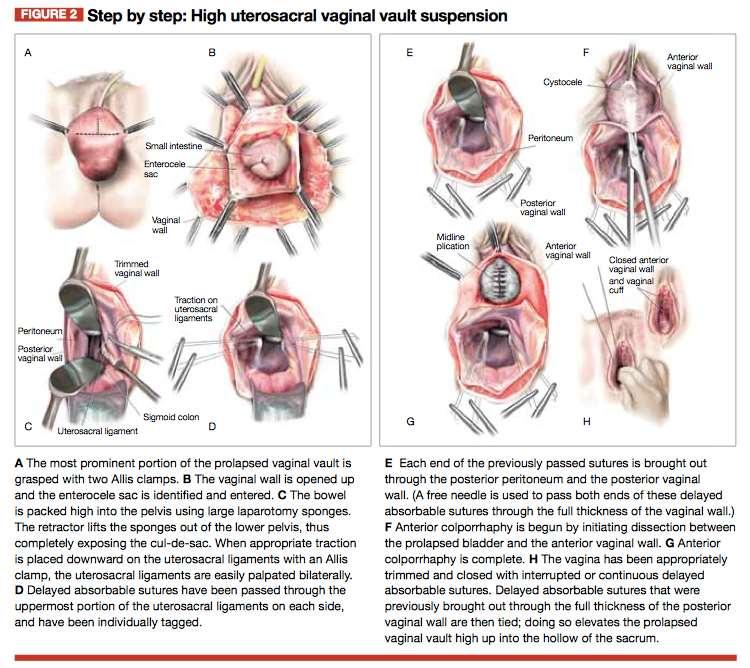
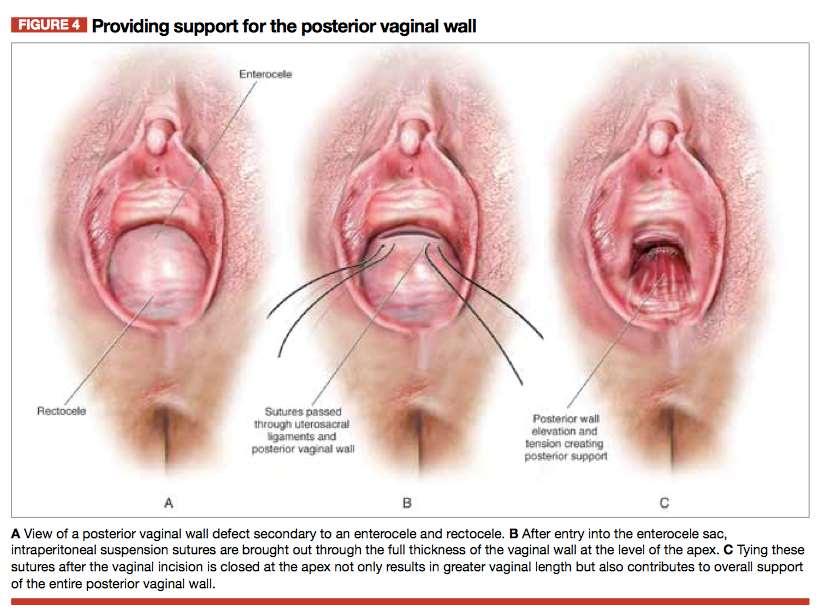
Step by step High uterosacral vaginal vault suspension to repair enterocele and apical prolapse
 When performing high uterosacral suspension, it is possible to pass sutures through the coccygeus muscle-sacrospinous ligament complex (arrow) because a segment of the uterosacral ligament inserts into
When performing high uterosacral suspension, it is possible to pass sutures through the coccygeus muscle-sacrospinous ligament complex (arrow) because a segment of the uterosacral ligament inserts into
Stop Coping. Start Living. Talk to your doctor about pelvic organ prolapse and sacrocolpopexy
 Stop Coping. Start Living Talk to your doctor about pelvic organ prolapse and sacrocolpopexy Did you know? One in three women will suffer from a pelvic health condition in her lifetime. Four of the most
Stop Coping. Start Living Talk to your doctor about pelvic organ prolapse and sacrocolpopexy Did you know? One in three women will suffer from a pelvic health condition in her lifetime. Four of the most
Index. Cyclical pelvic pain, 37 Cystocele, 22, 23, 25, 48, 51, 52, 54, 56, 124, 148, 160
 A Abdominal approach, 141 Abdominal hernia s surgery, 123, 124 Abdominal sacrocolpopexy (ASC), 116, 117 Abnormal uterine bleeding, 96 Anterior compartment repair, 101, 102 Apical compartment repair, 96
A Abdominal approach, 141 Abdominal hernia s surgery, 123, 124 Abdominal sacrocolpopexy (ASC), 116, 117 Abnormal uterine bleeding, 96 Anterior compartment repair, 101, 102 Apical compartment repair, 96
Clinical Curriculum: Urogynecology
 Updated July 201 Clinical Curriculum: Urogynecology GOAL: The primary goal of the Urogynecology rotation at the University of Alabama at Birmingham (UAB) is to train physicians to have a broad knowledge
Updated July 201 Clinical Curriculum: Urogynecology GOAL: The primary goal of the Urogynecology rotation at the University of Alabama at Birmingham (UAB) is to train physicians to have a broad knowledge
INTERNATIONAL UROGYNAECOLOGICAL ASSOCIATION (IUGA) JOINT REPORT ON THE TERMINOLOGY FOR SURGICAL PROCEDURES TO
 JOINT REPORT ON THE TERMINOLOGY FOR SURGICAL PROCEDURES TO") AN AMERICAN UROGYNECOLOGIC SOCIETY (AUGS) / INTERNATIONAL UROGYNAECOLOGICAL ASSOCIATION (IUGA) JOINT REPORT ON THE TERMINOLOGY FOR SURGICAL PROCEDURES TO TREAT PELVIC ORGAN PROLAPSE NEED FOR A WORKING
AN AMERICAN UROGYNECOLOGIC SOCIETY (AUGS) / INTERNATIONAL UROGYNAECOLOGICAL ASSOCIATION (IUGA) JOINT REPORT ON THE TERMINOLOGY FOR SURGICAL PROCEDURES TO TREAT PELVIC ORGAN PROLAPSE NEED FOR A WORKING
American Journal of Obstetrics and Gynecology
 American Journal of Obstetrics and Gynecology 1 2 3 Recurrence of vaginal prolapse after total vaginal hysterectomy with concurrent vaginal uterosacral ligament suspension: comparison between normal-weight
American Journal of Obstetrics and Gynecology 1 2 3 Recurrence of vaginal prolapse after total vaginal hysterectomy with concurrent vaginal uterosacral ligament suspension: comparison between normal-weight
Surgical treatments for vaginal apical prolapse
 Review Article Obstet Gynecol Sci 2016;59(4):253-260 http://dx.doi.org/10.5468/ogs.2016.59.4.253 pissn 2287-8572 eissn 2287-8580 Surgical treatments for vaginal apical prolapse Mi Kyung Kong, Sang Wook
Review Article Obstet Gynecol Sci 2016;59(4):253-260 http://dx.doi.org/10.5468/ogs.2016.59.4.253 pissn 2287-8572 eissn 2287-8580 Surgical treatments for vaginal apical prolapse Mi Kyung Kong, Sang Wook
Robotic-Assisted Surgery in Urogynecology: Beyond Sacrocolpopexy
 Robotic-Assisted Surgery in Urogynecology: Beyond Sacrocolpopexy Marie Fidela R. Paraiso, M.D. Professor of Surgery Section Head, Urogynecology and Reconstructive Pelvic Surgery Cleveland, OH Disclosures
Robotic-Assisted Surgery in Urogynecology: Beyond Sacrocolpopexy Marie Fidela R. Paraiso, M.D. Professor of Surgery Section Head, Urogynecology and Reconstructive Pelvic Surgery Cleveland, OH Disclosures
Current status in pelvic organ prolapse surgery: an evidence based review
 Current status in pelvic organ prolapse surgery: an evidence based review Christian Falconer, MD, PhD Department of Obstetrics and Gynecology Danderyd University Hospital Stockholm, Sweden Finnish Society
Current status in pelvic organ prolapse surgery: an evidence based review Christian Falconer, MD, PhD Department of Obstetrics and Gynecology Danderyd University Hospital Stockholm, Sweden Finnish Society
Pelvic Prolapse. A Patient Guide to Pelvic Floor Reconstruction
 Pelvic Prolapse A Patient Guide to Pelvic Floor Reconstruction Pelvic Prolapse When an organ becomes displaced, or slips down in the body, it is referred to as a prolapse. Your physician has diagnosed
Pelvic Prolapse A Patient Guide to Pelvic Floor Reconstruction Pelvic Prolapse When an organ becomes displaced, or slips down in the body, it is referred to as a prolapse. Your physician has diagnosed
Avoiding Mesh Disasters: Tips and Tricks for Success and Handling Complications
 Avoiding Mesh Disasters: Tips and Tricks for Success and Handling Complications Karyn S. Eilber, M.D. Cedars-Sinai FPMRS Associate Professor, Cedars-Sinai Dept of Surgery Associate Director, Urology Residency
Avoiding Mesh Disasters: Tips and Tricks for Success and Handling Complications Karyn S. Eilber, M.D. Cedars-Sinai FPMRS Associate Professor, Cedars-Sinai Dept of Surgery Associate Director, Urology Residency
Dr John Short. Obstetrician and Gynaecologist Christchurch Women s Hospital, Oxford Women's Health, Christchurch
 Dr John Short Obstetrician and Gynaecologist Christchurch Women s Hospital, Oxford Women's Health, Christchurch 8:30-9:25 WS #142: Peeling Back the Layers - The Pelvic Floor Uncovered 9:35-10:30 WS #152:
Dr John Short Obstetrician and Gynaecologist Christchurch Women s Hospital, Oxford Women's Health, Christchurch 8:30-9:25 WS #142: Peeling Back the Layers - The Pelvic Floor Uncovered 9:35-10:30 WS #152:
T h e C o m p l e t e Tr e a t m e n t o f P e l v i c F l o o r P r o l a p s e by Laparoscopy Technique, Tips and Tricks
 T h e C o m p l e t e Tr e a t m e n t o f P e l v i c F l o o r P r o l a p s e by Laparoscopy Technique, Tips and Tricks R Botchorishvili, A Wattiez, G Mage, M Canis, B Rabischong, K Jardon, C Rivoire,
T h e C o m p l e t e Tr e a t m e n t o f P e l v i c F l o o r P r o l a p s e by Laparoscopy Technique, Tips and Tricks R Botchorishvili, A Wattiez, G Mage, M Canis, B Rabischong, K Jardon, C Rivoire,
Prediction and prevention of stress urinary incontinence after prolapse surgery van der Ploeg, J.M.
 UvA-DARE (Digital Academic Repository) Prediction and prevention of stress urinary incontinence after prolapse surgery van der Ploeg, J.M. Link to publication Citation for published version (APA): van
UvA-DARE (Digital Academic Repository) Prediction and prevention of stress urinary incontinence after prolapse surgery van der Ploeg, J.M. Link to publication Citation for published version (APA): van
Original article J Bas Res Med Sci 2015; 2(2): The incidence of recurrent pelvic organ prolapse: A cross sectional study
: The incidence of recurrent pelvic organ prolapse: A cross sectional study") The incidence of recurrent pelvic organ prolapse: A cross sectional study Ashraf Direkvand-Moghadam 1, Ali Delpisheh 2, Azadeh Direkvand-Moghadam 3* 1. Psychosocial Injuries Research Center, Faculty of
The incidence of recurrent pelvic organ prolapse: A cross sectional study Ashraf Direkvand-Moghadam 1, Ali Delpisheh 2, Azadeh Direkvand-Moghadam 3* 1. Psychosocial Injuries Research Center, Faculty of
ISSN (o): Sacrospinous fixation: an efficient technique for prevention and treatment of vault prolapse
: Sacrospinous fixation: an efficient technique for prevention and treatment of vault prolapse") Original article www.ijrhs.com ISSN (o):2321 7251 Sacrospinous fixation: an efficient technique for prevention and treatment of vault Rajshree dayanand katke 1, Usha kiran. 2 1M.D.(Obstetrics & Gynecology),
Original article www.ijrhs.com ISSN (o):2321 7251 Sacrospinous fixation: an efficient technique for prevention and treatment of vault Rajshree dayanand katke 1, Usha kiran. 2 1M.D.(Obstetrics & Gynecology),
Introduction. Regarding the Section of the UPDATE Entitled Purpose
 Time to Rethink: an Evidence-Based Response from Pelvic Surgeons to the FDA Safety Communication: UPDATE on Serious Complications Associated with Transvaginal Placement of Surgical Mesh for Pelvic Organ
Time to Rethink: an Evidence-Based Response from Pelvic Surgeons to the FDA Safety Communication: UPDATE on Serious Complications Associated with Transvaginal Placement of Surgical Mesh for Pelvic Organ
Obliterative Procedures LeFort Colpocleisis Colpectomy (Vaginectomy) April 4, 2018
 April 4, 2018") Obliterative Procedures LeFort Colpocleisis Colpectomy (Vaginectomy) April 4, 2018 Obliterative Procedures for uterovaginal prolapse Total colpocleisis Partial colpocleisis (LeFort) Vaginectomy (colpectomy)-
Obliterative Procedures LeFort Colpocleisis Colpectomy (Vaginectomy) April 4, 2018 Obliterative Procedures for uterovaginal prolapse Total colpocleisis Partial colpocleisis (LeFort) Vaginectomy (colpectomy)-
A PATIENT GUIDE TO Understanding Stress Urinary Incontinence
 A PATIENT GUIDE TO Understanding Stress Urinary Incontinence Q: What is SUI? A: Stress urinary incontinence is defined as the involuntary leakage of urine. The problem afflicts approximately 18 million
A PATIENT GUIDE TO Understanding Stress Urinary Incontinence Q: What is SUI? A: Stress urinary incontinence is defined as the involuntary leakage of urine. The problem afflicts approximately 18 million
Posterior intravaginal slingplasty for vault and uterovaginal prolapse: an initial experience
 Gynecol Surg (2006) 3: 88 92 DOI 10.1007/s10397-005-0168-7 ORIGINAL ARTICLE R. Oliver. C. Dasgupta. A. Coker Posterior intravaginal slingplasty for vault and uterovaginal prolapse: an initial experience
Gynecol Surg (2006) 3: 88 92 DOI 10.1007/s10397-005-0168-7 ORIGINAL ARTICLE R. Oliver. C. Dasgupta. A. Coker Posterior intravaginal slingplasty for vault and uterovaginal prolapse: an initial experience
Suture complications in a teaching institution among patients undergoing uterosacral ligament suspension with permanent braided suture
 Int Urogynecol J (2010) 21:813 818 DOI 10.1007/s00192-010-1109-1 ORIGINAL ARTICLE Suture complications in a teaching institution among patients undergoing uterosacral ligament suspension with permanent
Int Urogynecol J (2010) 21:813 818 DOI 10.1007/s00192-010-1109-1 ORIGINAL ARTICLE Suture complications in a teaching institution among patients undergoing uterosacral ligament suspension with permanent
The UK National Prolapse Survey: 10 years on
 Int Urogynecol J (2018) 29:795 801 DOI 10.1007/s00192-017-3476-3 ORIGINAL ARTICLE The UK National Prolapse Survey: 10 years on Swati Jha 1 & Alfred Cutner 2 & Paul Moran 3 Received: 28 June 2017 /Accepted:
Int Urogynecol J (2018) 29:795 801 DOI 10.1007/s00192-017-3476-3 ORIGINAL ARTICLE The UK National Prolapse Survey: 10 years on Swati Jha 1 & Alfred Cutner 2 & Paul Moran 3 Received: 28 June 2017 /Accepted:
Long-term outcomes of modified high uterosacral ligament vault suspension (HUSLS) at vaginal hysterectomy
 at vaginal hysterectomy") Int Urogynecol J (2011) 22:577 584 DOI 10.1007/s00192-010-1325-8 ORIGINAL ARTICLE Long-term outcomes of modified high uterosacral ligament vault suspension (HUSLS) at vaginal hysterectomy Stergios K. Doumouchtsis
Int Urogynecol J (2011) 22:577 584 DOI 10.1007/s00192-010-1325-8 ORIGINAL ARTICLE Long-term outcomes of modified high uterosacral ligament vault suspension (HUSLS) at vaginal hysterectomy Stergios K. Doumouchtsis
Prospective study of an ultra-lightweight polypropylene Y mesh for robotic sacrocolpopexy
 Int Urogynecol J (2013) 24:1371 1375 DOI 10.1007/s00192-012-2021-7 ORIGINAL ARTICLE Prospective study of an ultra-lightweight polypropylene Y mesh for robotic sacrocolpopexy Charbel G. Salamon & Christa
Int Urogynecol J (2013) 24:1371 1375 DOI 10.1007/s00192-012-2021-7 ORIGINAL ARTICLE Prospective study of an ultra-lightweight polypropylene Y mesh for robotic sacrocolpopexy Charbel G. Salamon & Christa
ig. 2. The organs and their outlet tubes.
 Fig. 1. Birth-related laxity. The diagram shows the baby s head severely stretching ligaments and other tissues in and outside the vagina. This may cause various degrees of looseness, prolapse of the bladder
Fig. 1. Birth-related laxity. The diagram shows the baby s head severely stretching ligaments and other tissues in and outside the vagina. This may cause various degrees of looseness, prolapse of the bladder
Surgery for women with apical vaginal prolapse(review)
") Cochrane Database of Systematic Reviews (Review) Maher C, Feiner B, Baessler K, Christmann-Schmid C, Haya N, Brown J Maher C, Feiner B, Baessler K, Christmann-Schmid C, Haya N, Brown J.. Cochrane Database
Cochrane Database of Systematic Reviews (Review) Maher C, Feiner B, Baessler K, Christmann-Schmid C, Haya N, Brown J Maher C, Feiner B, Baessler K, Christmann-Schmid C, Haya N, Brown J.. Cochrane Database
Management of Vaginal Prolapse
 Information for Patients Saint Mary s Hospital/Trafford General Hospital Uro-gynaecology Service Management of Vaginal Prolapse Before reading this leaflet you should read What is vaginal prolapse? If
Information for Patients Saint Mary s Hospital/Trafford General Hospital Uro-gynaecology Service Management of Vaginal Prolapse Before reading this leaflet you should read What is vaginal prolapse? If
Options for Vaginal Prolapse. What is prolapse? What is prolapse? Disclosures 10/23/2013. Michelle Y. Morrill, M.D. None
 Options for Vaginal Prolapse Disclosures None Michelle Y. Morrill, M.D. Director of Urogynecology Kaiser, San Francisco Assistant Professor, Volunteer Faculty Department of Ob/Gyn, UCSF What is prolapse?
Options for Vaginal Prolapse Disclosures None Michelle Y. Morrill, M.D. Director of Urogynecology Kaiser, San Francisco Assistant Professor, Volunteer Faculty Department of Ob/Gyn, UCSF What is prolapse?
High levator myorraphy versus uterosacral ligament suspension for vaginal vault fixation: a prospective, randomized study
 Int Urogynecol J (2010) 21:515 522 DOI 10.1007/s00192-009-1064-x ORIGINAL ARTICLE High levator myorraphy versus uterosacral ligament suspension for vaginal vault fixation: a prospective, randomized study
Int Urogynecol J (2010) 21:515 522 DOI 10.1007/s00192-009-1064-x ORIGINAL ARTICLE High levator myorraphy versus uterosacral ligament suspension for vaginal vault fixation: a prospective, randomized study
Functional anatomy of the female pelvic floor and lower urinary tract Stefano Floris, MD, PhD Department of Obstetrics and Gynaecology
 Functional anatomy of the female pelvic floor and lower urinary tract Stefano Floris, MD, PhD Department of Obstetrics and Gynaecology Ospedale San Giovanni di Dio, Gorizia, Italy ANATOMY URINARY CONTINENCE
Functional anatomy of the female pelvic floor and lower urinary tract Stefano Floris, MD, PhD Department of Obstetrics and Gynaecology Ospedale San Giovanni di Dio, Gorizia, Italy ANATOMY URINARY CONTINENCE
Eric R. Sokol, MD. Bio. CLINICAL OFFICES Gynecology Clinic 900 Blake Wilbur Dr. Palo Alto, CA Tel (650) Fax (650) BIO
 Fax (650) BIO") CLINICAL OFFICES Gynecology Clinic 900 Blake Wilbur Dr Bio Palo Alto, CA 94304 Associate Professor of Obstetrics and Gynecology (Gynecology-Urogynecology) and, by courtesy, of Urology at the Stanford University
CLINICAL OFFICES Gynecology Clinic 900 Blake Wilbur Dr Bio Palo Alto, CA 94304 Associate Professor of Obstetrics and Gynecology (Gynecology-Urogynecology) and, by courtesy, of Urology at the Stanford University
Medium-term follow-up on use of freeze-dried, irradiated donor fascia for sacrocolpopexy and sling procedures
 Int Urogynecol J (2004) 15: 238 242 DOI 10.1007/s00192-004-1146-8 ORIGINAL ARTICLE Mary Pat FitzGerald Æ S. Renee Edwards Æ Dee Fenner Medium-term follow-up on use of freeze-dried, irradiated donor fascia
Int Urogynecol J (2004) 15: 238 242 DOI 10.1007/s00192-004-1146-8 ORIGINAL ARTICLE Mary Pat FitzGerald Æ S. Renee Edwards Æ Dee Fenner Medium-term follow-up on use of freeze-dried, irradiated donor fascia
Development of the pelvic floor : implications for clinical anatomy Wallner, C.
 UvA-DARE (Digital Academic Repository) Development of the pelvic floor : implications for clinical anatomy Wallner, C. Link to publication Citation for published version (APA): Wallner, C. (2008). Development
UvA-DARE (Digital Academic Repository) Development of the pelvic floor : implications for clinical anatomy Wallner, C. Link to publication Citation for published version (APA): Wallner, C. (2008). Development
FDA & Transvaginal Mesh: What Happened? What s Next?
 FDA & Transvaginal Mesh: What Happened? What s Next? Matthew D. Barber, MD MHS Professor & Vice Chair for Clinical Research Obstetrics Gynecology & Women s Health Institute Disclosures I receive no grants,
FDA & Transvaginal Mesh: What Happened? What s Next? Matthew D. Barber, MD MHS Professor & Vice Chair for Clinical Research Obstetrics Gynecology & Women s Health Institute Disclosures I receive no grants,
Anatomical and functional results of McCall culdoplasty in the prevention of enteroceles and vaginal vault prolapse after vaginal hysterectomy
 Int Urogynecol J (2008) 19:1007 1011 DOI 10.1007/s00192-007-0549-8 ORIGINAL ARTICLE Anatomical and functional results of McCall culdoplasty in the prevention of enteroceles and vaginal vault prolapse after
Int Urogynecol J (2008) 19:1007 1011 DOI 10.1007/s00192-007-0549-8 ORIGINAL ARTICLE Anatomical and functional results of McCall culdoplasty in the prevention of enteroceles and vaginal vault prolapse after
We welcome comments and corrections which will be used to improve the system annually.
 ACGME Case Log Instructions: Female Pelvic Medicine and Reconstructive Surgery (FPMRS) Review Committees for Obstetrics and Gynecology, and Urology Updated July 2013 BACKGROUND The ACGME Case Log System
ACGME Case Log Instructions: Female Pelvic Medicine and Reconstructive Surgery (FPMRS) Review Committees for Obstetrics and Gynecology, and Urology Updated July 2013 BACKGROUND The ACGME Case Log System
Innovations in mesh kit technology for vaginal wall prolapse
 Available at www.obgmanagement.com s u p p l e m e n t t o This supplement is supported by American Medical Systems, Inc., and has been peer reviewed by the editors of OBG Management. J a n u a r y 2 0
Available at www.obgmanagement.com s u p p l e m e n t t o This supplement is supported by American Medical Systems, Inc., and has been peer reviewed by the editors of OBG Management. J a n u a r y 2 0
NOTES FROM GUTMAN LECTURE 10/26 Use this outline to study from. As you go through Gutman s lecture, fill in the topics.
 NOTES FROM GUTMAN LECTURE 10/26 Use this outline to study from. As you go through Gutman s lecture, fill in the topics. Anatomy above the arcuate line Skin Camper s fascia Scarpa s fascia External oblique
NOTES FROM GUTMAN LECTURE 10/26 Use this outline to study from. As you go through Gutman s lecture, fill in the topics. Anatomy above the arcuate line Skin Camper s fascia Scarpa s fascia External oblique
Pelvic Organ Prolapse and Urinary Incontinence
 Pelvic Organ Prolapse and Urinary Incontinence A E U M U R O G. L A K E, M D F E M A L E P E L V I C M E D I C I N E & R E C O N S T R U C T I V E S U R G E R Y W O M E N S H E A L T H S P E C I A L T
Pelvic Organ Prolapse and Urinary Incontinence A E U M U R O G. L A K E, M D F E M A L E P E L V I C M E D I C I N E & R E C O N S T R U C T I V E S U R G E R Y W O M E N S H E A L T H S P E C I A L T
Complications from permanent synthetic mesh
 Original Research Symptom Resolution After Operative Management of Complications From Transvaginal Mesh Erin C. Crosby, MD, Melinda Abernethy, MD, MPH, Mitchell B. Berger, MD, PhD, John O. DeLancey, MD,
Original Research Symptom Resolution After Operative Management of Complications From Transvaginal Mesh Erin C. Crosby, MD, Melinda Abernethy, MD, MPH, Mitchell B. Berger, MD, PhD, John O. DeLancey, MD,
Female Pelvic Medicine & Reconstructive Surgery
 Female Pelvic Medicine & Reconstructive Surgery APPLICATION FOR NEW FELLOWSHIP Name of Institution: McGill University Location: Royal Victoria Hospital (Glen Site), St Mary s Hospital Centre Type of Fellowship:
Female Pelvic Medicine & Reconstructive Surgery APPLICATION FOR NEW FELLOWSHIP Name of Institution: McGill University Location: Royal Victoria Hospital (Glen Site), St Mary s Hospital Centre Type of Fellowship:
Ina S. Irabon, MD, FPOGS, FPSRM, FPSGE Obstetrics and Gynecology Reproductive Endocrinology and Infertility Laparoscopy and Hysteroscopy
 Ina S. Irabon, MD, FPOGS, FPSRM, FPSGE Obstetrics and Gynecology Reproductive Endocrinology and Infertility Laparoscopy and Hysteroscopy Comprehensive Gynecology 7 th edition, 2017 (Lobo RA, Gershenson
Ina S. Irabon, MD, FPOGS, FPSRM, FPSGE Obstetrics and Gynecology Reproductive Endocrinology and Infertility Laparoscopy and Hysteroscopy Comprehensive Gynecology 7 th edition, 2017 (Lobo RA, Gershenson
Laparoscopic Sacrocolpopexy with & without the Robot: Tips and Tricks for success and avoidance / management of complications
 Laparoscopic Sacrocolpopexy with & without the Robot: Tips and Tricks for success and avoidance / management of complications Course Faculty: Patrick Culligan, MD Peter Rosenblatt, MD What is a Sacrocolpopexy?
Laparoscopic Sacrocolpopexy with & without the Robot: Tips and Tricks for success and avoidance / management of complications Course Faculty: Patrick Culligan, MD Peter Rosenblatt, MD What is a Sacrocolpopexy?
Does trocar-guided tension-free vaginal mesh (Prolift ) repair provoke prolapse of the unaffected compartments?
 repair provoke prolapse of the unaffected compartments?") Int Urogynecol J (2010) 21:271 278 DOI 10.1007/s00192-009-1028-1 ORIGINAL ARTICLE Does trocar-guided tension-free vaginal mesh (Prolift ) repair provoke prolapse of the unaffected compartments? Mariëlla
Int Urogynecol J (2010) 21:271 278 DOI 10.1007/s00192-009-1028-1 ORIGINAL ARTICLE Does trocar-guided tension-free vaginal mesh (Prolift ) repair provoke prolapse of the unaffected compartments? Mariëlla
Polypropylene vaginal mesh implants for vaginal prolapse
 Polypropylene vaginal mesh implants for vaginal prolapse This statement has been developed and reviewed by the Women s Health Committee and approved by the RANZCOG Board and Council. A list of Women s
Polypropylene vaginal mesh implants for vaginal prolapse This statement has been developed and reviewed by the Women s Health Committee and approved by the RANZCOG Board and Council. A list of Women s
Moneli Golara Consultant Obstetrician and Gynaecologist Royal Free NHS Trust Barnet Hospital
 Moneli Golara Consultant Obstetrician and Gynaecologist Royal Free NHS Trust Barnet Hospital Pelvic Organ Prolapse (POP)- herniation of pelvic organs into vaginal walls Common Huge impact on daily activities
Moneli Golara Consultant Obstetrician and Gynaecologist Royal Free NHS Trust Barnet Hospital Pelvic Organ Prolapse (POP)- herniation of pelvic organs into vaginal walls Common Huge impact on daily activities
Paravaginal Repair: A Laparoscopic Approach
 44 Paravaginal Repair: A Laparoscopic Approach John R. Miklos and Robert Moore Atlanta Urogynecology Associates, Atlanta, Georgia, U.S.A. Neeraj Kohli Harvard University, Boston, Massachusetts, U.S.A.
44 Paravaginal Repair: A Laparoscopic Approach John R. Miklos and Robert Moore Atlanta Urogynecology Associates, Atlanta, Georgia, U.S.A. Neeraj Kohli Harvard University, Boston, Massachusetts, U.S.A.
Female Urology. The Results of Grade IV Cystocele Repair Using Mesh. Introduction ZARGAR MA, EMAMI M*, ZARGAR K, JAMSHIDI M
 Urology Journal UNRC/IUA Vol. 1, No. 4, 263-267 Autumn 2004 Printed in IRAN Female Urology The Results of Grade IV Cystocele Repair Using Mesh ZARGAR MA, EMAMI M*, ZARGAR K, JAMSHIDI M Department of Urology,
Urology Journal UNRC/IUA Vol. 1, No. 4, 263-267 Autumn 2004 Printed in IRAN Female Urology The Results of Grade IV Cystocele Repair Using Mesh ZARGAR MA, EMAMI M*, ZARGAR K, JAMSHIDI M Department of Urology,
Table 2. First Generated List of Expert Responses. Likert-Type Scale. Category or Criterion. Rationale or Comments (1) (2) (3) (4)
 (2) (3) (4)") Table 2. First Generated List of Expert Responses. Likert-Type Scale Category or Criterion Anatomical Structures and Features Skeletal Structures and Features (1) (2) (3) (4) Rationale or Comments 1. Bones
Table 2. First Generated List of Expert Responses. Likert-Type Scale Category or Criterion Anatomical Structures and Features Skeletal Structures and Features (1) (2) (3) (4) Rationale or Comments 1. Bones
Gökmen Sukgen, 1 Esra SaygJlJ YJlmaz, 2 and Eralp BaGer Introduction. 2. Case Presentation
 Case Reports in Obstetrics and Gynecology Volume 2016, Article ID 2906596, 4 pages http://dx.doi.org/10.1155/2016/2906596 Case Report Vaginal Hysterectomy with Anterior Four-Arm Mesh Implant Technique
Case Reports in Obstetrics and Gynecology Volume 2016, Article ID 2906596, 4 pages http://dx.doi.org/10.1155/2016/2906596 Case Report Vaginal Hysterectomy with Anterior Four-Arm Mesh Implant Technique
Recent advances in POP. Dr. Bernhard Uhl Department for Obstetrics and Gynecology St. Vinzenz-Hospital Dinslaken Germany
 Recent advances in POP Dr. Bernhard Uhl Department for Obstetrics and Gynecology St. Vinzenz-Hospital Dinslaken Germany Level of pelvic floor support Level I apical Level II transverse/ horizontal Level
Recent advances in POP Dr. Bernhard Uhl Department for Obstetrics and Gynecology St. Vinzenz-Hospital Dinslaken Germany Level of pelvic floor support Level I apical Level II transverse/ horizontal Level
Index. Note: Page numbers of article titles are in boldface type.
 Index Note: Page numbers of article titles are in boldface type. A Abdominal mesh background of, 84 85 Age as factor in PFDs, 8 Anal plugs in FI management in women, 107 Anterior compartment native tissue
Index Note: Page numbers of article titles are in boldface type. A Abdominal mesh background of, 84 85 Age as factor in PFDs, 8 Anal plugs in FI management in women, 107 Anterior compartment native tissue
Subjective and objective results 1 year after robotic sacrocolpopexy using a lightweight Y-mesh
 DOI 10.1007/s00192-013-2265-x ORIGINAL ARTICLE Subjective and objective results 1 year after robotic sacrocolpopexy using a lightweight Y-mesh Patrick J. Culligan & Emil Gurshumov & Christa Lewis & Jennifer
DOI 10.1007/s00192-013-2265-x ORIGINAL ARTICLE Subjective and objective results 1 year after robotic sacrocolpopexy using a lightweight Y-mesh Patrick J. Culligan & Emil Gurshumov & Christa Lewis & Jennifer
12/1/13. What are Pelvic Floor Disorders? What is the Pelvic Floor? Facts. Prevalence of Urinary InconOnence. What s New in Pelvic Floor Disorders?
 What are Pelvic Floor Disorders? Urinary Control Problems - InconOnence or leakage of urine Prolapse of pelvic organs - Vagina, bladder, rectum What s New in Pelvic Floor Disorders? Kimberly Kenton MD,
What are Pelvic Floor Disorders? Urinary Control Problems - InconOnence or leakage of urine Prolapse of pelvic organs - Vagina, bladder, rectum What s New in Pelvic Floor Disorders? Kimberly Kenton MD,
Urethrolysis; When, Why & How. M Karram Professor of Ob/Gyn & Urology University of Cincinnati
 Urethrolysis; When, Why & How M Karram Professor of Ob/Gyn & Urology University of Cincinnati Anatomy Urethra may be fixed to the pubic bone with dense scar tissue Goal of urethrolysis is to completely
Urethrolysis; When, Why & How M Karram Professor of Ob/Gyn & Urology University of Cincinnati Anatomy Urethra may be fixed to the pubic bone with dense scar tissue Goal of urethrolysis is to completely
Considering Surgery for Pelvic Prolapse? Learn about minimally invasive da Vinci Surgery
 Considering Surgery for Pelvic Prolapse? Learn about minimally invasive da Vinci Surgery The Surgery: Pelvic Prolapse Surgery If you have pelvic prolapse symptoms, your doctor may suggest medicine or lifestyle
Considering Surgery for Pelvic Prolapse? Learn about minimally invasive da Vinci Surgery The Surgery: Pelvic Prolapse Surgery If you have pelvic prolapse symptoms, your doctor may suggest medicine or lifestyle
NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE
 NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE INTERVENTIONAL PROCEDURES PROGRAMME Interventional procedure overview of infracoccygeal sacropexy using mesh to repair vaginal vault prolapse The vaginal
NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE INTERVENTIONAL PROCEDURES PROGRAMME Interventional procedure overview of infracoccygeal sacropexy using mesh to repair vaginal vault prolapse The vaginal
Vaginal McCall culdoplasty versus laparoscopic uterosacral plication to prophylactically address vaginal vault prolapse
 Vaginal McCall culdoplasty versus laparoscopic uterosacral to prophylactically address vaginal vault prolapse Niblock, K., Bailie, E., McCracken, G., & Johnston, K. (2017). Vaginal McCall culdoplasty versus
Vaginal McCall culdoplasty versus laparoscopic uterosacral to prophylactically address vaginal vault prolapse Niblock, K., Bailie, E., McCracken, G., & Johnston, K. (2017). Vaginal McCall culdoplasty versus
Considering Surgery for Vaginal or Uterine Prolapse? Learn why da Vinci Surgery may be your best treatment option.
 Considering Surgery for Vaginal or Uterine Prolapse? Learn why da Vinci Surgery may be your best treatment option. The Condition(s): Vaginal Prolapse, Uterine Prolapse Vaginal prolapse occurs when the
Considering Surgery for Vaginal or Uterine Prolapse? Learn why da Vinci Surgery may be your best treatment option. The Condition(s): Vaginal Prolapse, Uterine Prolapse Vaginal prolapse occurs when the
EndoFast Reliant System vs. Tension- free Mesh in a Sheep Model; three arm Comparative Study Assessing the Mechanical Pullout Force of Mesh Over Time
 EndoFast Reliant System vs. Tension- free Mesh in a Sheep Model; three arm Comparative Study Assessing the Mechanical Pullout Force of Mesh Over Time Menachem Alcalay,M.D, Urogynecology unit, Sheba Medical
EndoFast Reliant System vs. Tension- free Mesh in a Sheep Model; three arm Comparative Study Assessing the Mechanical Pullout Force of Mesh Over Time Menachem Alcalay,M.D, Urogynecology unit, Sheba Medical
SGS Annual Course in Advanced Gynecologic Surgery New Orleans, LA
 SGS Annual Course in Advanced Gynecologic Surgery New Orleans, LA Thursday, November 29 Royal Sonesta New Orleans 7:00 7:20 am Registration and Continental Breakfast 7:20 7:30 am Welcome and Opening Remarks
SGS Annual Course in Advanced Gynecologic Surgery New Orleans, LA Thursday, November 29 Royal Sonesta New Orleans 7:00 7:20 am Registration and Continental Breakfast 7:20 7:30 am Welcome and Opening Remarks
High risk of complications with a single incision pelvic floor repair kit: results of a retrospective case series
 Int Urogynecol J (2014) 25:109 116 DOI 10.1007/s00192-013-2156-1 ORIGINAL ARTICLE High risk of complications with a single incision pelvic floor repair kit: results of a retrospective case series Stephen
Int Urogynecol J (2014) 25:109 116 DOI 10.1007/s00192-013-2156-1 ORIGINAL ARTICLE High risk of complications with a single incision pelvic floor repair kit: results of a retrospective case series Stephen
Tian-Ni Kuo 1, Ming-Ping Wu 1,2 *
 RESEARCH LETTER THE USE OF A CONCOMITANT TENSION-FREE VAGINAL MESH TECHNIQUE AND A TENSION-FREE MIDURETHRAL SLING IN TREATING PELVIC ORGAN PROLAPSE AND OCCULT STRESS URINARY INCONTINENCE Tian-Ni Kuo 1,
RESEARCH LETTER THE USE OF A CONCOMITANT TENSION-FREE VAGINAL MESH TECHNIQUE AND A TENSION-FREE MIDURETHRAL SLING IN TREATING PELVIC ORGAN PROLAPSE AND OCCULT STRESS URINARY INCONTINENCE Tian-Ni Kuo 1,
Surgical management of pelvic organ prolapse in women(review)
") Cochrane Database of Systematic Reviews Surgical management of pelvic organ prolapse in women (Review) MaherC,FeinerB,BaesslerK,SchmidC MaherC,FeinerB,BaesslerK,SchmidC. Surgical management of pelvic organ
Cochrane Database of Systematic Reviews Surgical management of pelvic organ prolapse in women (Review) MaherC,FeinerB,BaesslerK,SchmidC MaherC,FeinerB,BaesslerK,SchmidC. Surgical management of pelvic organ
Total vs Subtotal Hysterectomy
 Total vs Subtotal Hysterectomy AN UNSOLVED PROBLEM? G Centini, E Zupi, A Wattiez 153 patient with 15 years of follow-up The Timeline The first successful hysterectomy (Subtotal)! First Laparoscopic Hysterectomy!
Total vs Subtotal Hysterectomy AN UNSOLVED PROBLEM? G Centini, E Zupi, A Wattiez 153 patient with 15 years of follow-up The Timeline The first successful hysterectomy (Subtotal)! First Laparoscopic Hysterectomy!
Dana Alrafaiah. - Amani Nofal. - Ahmad Alsalman. 1 P a g e
 - 2 - Dana Alrafaiah - Amani Nofal - Ahmad Alsalman 1 P a g e This lecture will discuss five topics as follows: 1- Arrangement of pelvic viscera. 2- Muscles of Pelvis. 3- Blood Supply of pelvis. 4- Nerve
- 2 - Dana Alrafaiah - Amani Nofal - Ahmad Alsalman 1 P a g e This lecture will discuss five topics as follows: 1- Arrangement of pelvic viscera. 2- Muscles of Pelvis. 3- Blood Supply of pelvis. 4- Nerve
ORIENTING TO BISECTED SPECIMENS ON THE PELVIS PRACTICAL
 ORIENTING TO BISECTED SPECIMENS ON THE PELVIS PRACTICAL The Pelvis is just about as complicated as head and neck and considerably more mysterious. You have to be able to visualize (imagine) the underlying
ORIENTING TO BISECTED SPECIMENS ON THE PELVIS PRACTICAL The Pelvis is just about as complicated as head and neck and considerably more mysterious. You have to be able to visualize (imagine) the underlying
Site-specific fascial defects in the diagnosis and surgical management of enterocele
 Site-specific fascial defects in the diagnosis and surgical management of enterocele John R. Miklos, MD,a Neeraj Kohli, MD,b Vincent Lucente, MD,c and William B. Safe, MDd Atlanta and Marietta, GeO1gia,
Site-specific fascial defects in the diagnosis and surgical management of enterocele John R. Miklos, MD,a Neeraj Kohli, MD,b Vincent Lucente, MD,c and William B. Safe, MDd Atlanta and Marietta, GeO1gia,
W23: Approaches to pelvic organ prolapse surgery Workshop Chair: Philippe Zimmern, United States 21 October :00-12:00
 W23: Approaches to pelvic organ prolapse surgery Workshop Chair: Philippe Zimmern, United States 21 October 2014 09:00-12:00 Start End Topic Speakers 09:00 09:30 Goals of repair and anatomical principles
W23: Approaches to pelvic organ prolapse surgery Workshop Chair: Philippe Zimmern, United States 21 October 2014 09:00-12:00 Start End Topic Speakers 09:00 09:30 Goals of repair and anatomical principles
CHAU KHAC TU M.D., Ph.D.
 CHAU KHAC TU M.D., Ph.D. Hue Central Hospital Vietnam LAPAROSCOPIC PROMONTOFIXATION FOR THE GENITAL PROLAPSE TREATMENT Chau Khac Tu MD.PhD. Hue central hospital CONTENT 3 1 INTRODUCTION 2 OBJECTIVE AND
CHAU KHAC TU M.D., Ph.D. Hue Central Hospital Vietnam LAPAROSCOPIC PROMONTOFIXATION FOR THE GENITAL PROLAPSE TREATMENT Chau Khac Tu MD.PhD. Hue central hospital CONTENT 3 1 INTRODUCTION 2 OBJECTIVE AND
Pelvic Organ Prolapse: Diagnosis, Treatment, and Avoiding Complications
 Pelvic Organ Prolapse: Diagnosis, Treatment, and Avoiding Complications Christina Dancz and Morgan Fullerton Contents 1 Introduction... 2 2 Anatomy/Pathophysiology... 2 2.1 Level 1: The Cardinal and Uterosacral
Pelvic Organ Prolapse: Diagnosis, Treatment, and Avoiding Complications Christina Dancz and Morgan Fullerton Contents 1 Introduction... 2 2 Anatomy/Pathophysiology... 2 2.1 Level 1: The Cardinal and Uterosacral
Laparoscopic sacrocolpopexy: an observational study of functional and anatomical outcomes
 DOI 10.1007/s00192-010-1241-y ORIGINAL ARTICLE Laparoscopic sacrocolpopexy: an observational study of functional and anatomical outcomes Natalia Price & Alex Slack & Simon R. Jackson Received: 26 April
DOI 10.1007/s00192-010-1241-y ORIGINAL ARTICLE Laparoscopic sacrocolpopexy: an observational study of functional and anatomical outcomes Natalia Price & Alex Slack & Simon R. Jackson Received: 26 April
Surgical management of pelvic organ prolapse in women (Review)
") Surgical management of pelvic organ prolapse in women (Review) Maher C, Feiner B, Baessler K, Glazener CMA This is a reprint of a Cochrane review, prepared and maintained by The Cochrane Collaboration
Surgical management of pelvic organ prolapse in women (Review) Maher C, Feiner B, Baessler K, Glazener CMA This is a reprint of a Cochrane review, prepared and maintained by The Cochrane Collaboration
Dear Mrs. Burch and editors of the BMJ,
 Dear Mrs. Burch and editors of the BMJ, We are pleased that our manuscript entitled: Sacrospinous hysteropexy versus vaginal hysterectomy with uterosacral ligament suspension in women with uterine prolapse
Dear Mrs. Burch and editors of the BMJ, We are pleased that our manuscript entitled: Sacrospinous hysteropexy versus vaginal hysterectomy with uterosacral ligament suspension in women with uterine prolapse
1) What conditions is vaginal mesh used to commonly treat? Vaginal mesh is used to treat two different health issues in women:
 What conditions is vaginal mesh used to commonly treat? Vaginal mesh is used to treat two different health issues in women:") Vaginal Mesh Frequently Asked Questions 1) What conditions is vaginal mesh used to commonly treat? Vaginal mesh is used to treat two different health issues in women: a) stress urinary incontinence (SUI)
Vaginal Mesh Frequently Asked Questions 1) What conditions is vaginal mesh used to commonly treat? Vaginal mesh is used to treat two different health issues in women: a) stress urinary incontinence (SUI)
Posterior Deep Endometriosis. What is the best approach? Posterior Deep Endometriosis. Should we perform a routine excision of the vagina??
 Posterior Deep Endometriosis What is the best approach? Dept Gyn Obst Polyclinique Hotel Dieu CHU Clermont Ferrand France Posterior Deep Endometriosis Organs involved - Peritoneum - Uterine cervix -Rectum
Posterior Deep Endometriosis What is the best approach? Dept Gyn Obst Polyclinique Hotel Dieu CHU Clermont Ferrand France Posterior Deep Endometriosis Organs involved - Peritoneum - Uterine cervix -Rectum
This information is intended as an overview only
 This information is intended as an overview only Please refer to the INSTRUCTIONS FOR USE included with this device for indications, contraindications, warnings, precautions and other important information
This information is intended as an overview only Please refer to the INSTRUCTIONS FOR USE included with this device for indications, contraindications, warnings, precautions and other important information
Stephen T Jeffery. University of Cape Town, South Africa
 Stephen T Jeffery University of Cape Town, South Africa I still think there s a role for mesh in Prolapse surgery Examples of my most recent mesh cases Case 1 62 yr old Sacrocolpopexy for vault prolapse
Stephen T Jeffery University of Cape Town, South Africa I still think there s a role for mesh in Prolapse surgery Examples of my most recent mesh cases Case 1 62 yr old Sacrocolpopexy for vault prolapse
University College Hospital
 University College Hospital Surgery for prolapse Helping you to make the right choice Urogynaecology and Pelvic Floor Unit, Women s Health Contents Page 1. What type of surgery should I choose? 2 2. What
University College Hospital Surgery for prolapse Helping you to make the right choice Urogynaecology and Pelvic Floor Unit, Women s Health Contents Page 1. What type of surgery should I choose? 2 2. What
Introduction to GYN Specialties
 Outline Introduction to GYN Specialties Gynecologic Oncology* Female Pelvic Medicine and Reconstructive Surgery* Reproductive Endocrinology and Infertility* Pediatric and Adolescent Gynecology** Family
Outline Introduction to GYN Specialties Gynecologic Oncology* Female Pelvic Medicine and Reconstructive Surgery* Reproductive Endocrinology and Infertility* Pediatric and Adolescent Gynecology** Family
30/06/2014. Gynaecological Surgery. Mr Alfred Cutner, Consultant Gynaecologist, University College Hospital, London WHAT IS LAPAROSCOPIC SURGERY?
 Gynaecological Surgery Mr Alfred Cutner, Consultant Gynaecologist, University College Hospital, London Laparoscopic surgery techniques Common complications of laparoscopic surgery Intra-operative injuries:
Gynaecological Surgery Mr Alfred Cutner, Consultant Gynaecologist, University College Hospital, London Laparoscopic surgery techniques Common complications of laparoscopic surgery Intra-operative injuries:
Laparoscopic Sacrocolpopexy vs Robotic Sacrocolpopexy
 Laparoscopic Sacrocolpopexy vs Robotic Sacrocolpopexy Magnus Murphy FRCSC Clinical Assistant Professor Department of Obstetrics and Gynecology University of Calgary Division of Urogynecology www.pelvicfloor.com
Laparoscopic Sacrocolpopexy vs Robotic Sacrocolpopexy Magnus Murphy FRCSC Clinical Assistant Professor Department of Obstetrics and Gynecology University of Calgary Division of Urogynecology www.pelvicfloor.com