Appendiceal Pathology. Prof Ray McMahon Histopathology Department Manchester Royal Infirmary Bryan Warren School Sarajevo November 2016
|
|
|
- Magdalen Miles
- 5 years ago
- Views:
Transcription
1 Appendiceal Pathology Prof Ray McMahon Histopathology Department Manchester Royal Infirmary Bryan Warren School Sarajevo November 2016

2 Appendicitis

3 Appendicitis
4 Appendicitis Scattered groups of neutrophils in the mucosa alone do not indicate appendicitis Eosinophils are normal in the mucosa Neutrophils in the serosa alone do not indicate appendicitis - suggest an extraappendiceal cause Acute necrotising arteritis may be localised to the appendix Always think about actinomycosis Diverticulitis is quite common if you look for it



5




6 Ulcerative Colitis
7 Ulcerative Colitis Appendix involved in 50% cases of UC Skip lesion in 37% Active disease with ulceration in colectomy specimens predicts subsequent pouchitis Appendiceal carcinoma occurs in UC Appendicectomy protects against subsequent ulcerative colitis

8 Crohn s disease
9 Crohn s Disease Appendix involved in 40-50% cases of CD resections skip lesion in 20% 20% had previous appendicectomy Appendiceal involvement associated with more extensive colonic disease


10 Crohn s disease
11 Granulomatous Appendicitis Common in interval appendicectomies (60%) Other Crohn s-like changes in 50% Extra-appendiceal disease in <10% Consider other causes Yersinia (PCR +ve in 10/40 cases vs 0/60 controls) Tuberculosis Schistosomiasis


12


13
14 Yersinial infection Yersinia enterocolitica Yersinia pseudotuberculosis Meat (especially pork) and dairy products consumption and contact with untreated sewage Usually matted mesenteric lymphadenopathy May cause ileitis, appendicitis, colitis or enteric fever-like syndrome especially with Y enterocolitica Granulomatous inflammation especially with Y pseudotuberculosis
15 Four stages of Yersinial infection Lymphoid hyperplasia Histiocytic hyperplasia Epithelioid granuloma formation Central granulomatous necrosis



16




17

 with syncytial")
18 Measles Initial infection of respiratory lining cells followed by replication Primary viraemia leads to dissemination in lymphoid tissue with formation of Warthin-Finkeldey cells Secondary viraemia by infected lymphocytes giving epithelial infection (skin, gut, etc) with syncytial giant cells

")

19 Rarely causes clinical appendicitis Prodromal: Measles Appendicitis Hyperplasia of lymphoid tissue Warthin-Finkeldey giant cells (B-cells) in follicles Full-blown: Syncytial epithelial giant cells Mucosal necrosis and sloughing Few remaining W-F cells
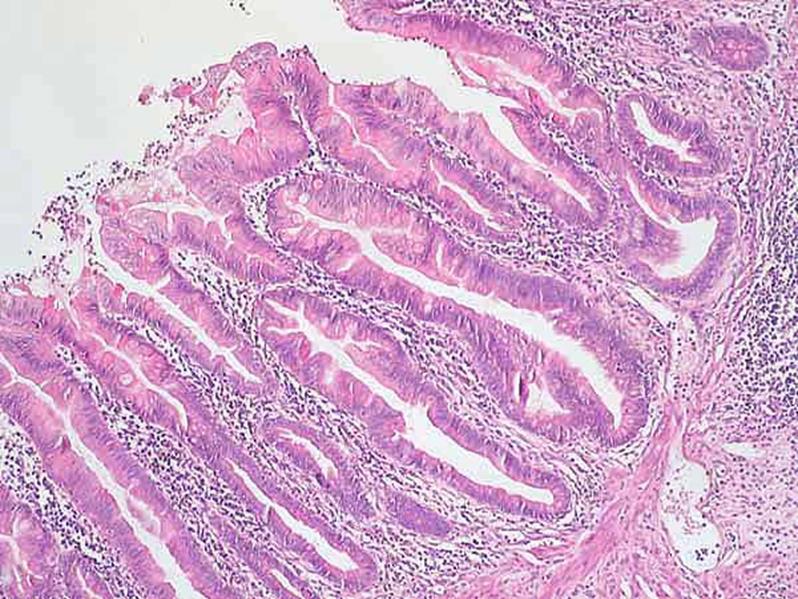
20 Appendiceal Adenomas Incidental (including FAP) Appendicitis Mucocoele

21


22 Appendiceal Adenoma - Carcinoma




23


24
25 Appendiceal Adenomas Women > men Synchronous ovarian mucinous tumours 10% Synchronous colorectal neoplasms 33-89% CK20+ 50% CK7+




26 Obstructive rare <1cm diameter epithelium flattened, devoid of atypia cystic fibrosis Neoplastic >1cm diameter Ulceration calcification Mucocoele




27
28 Mucinous adenoma If there is acellular mucin in the appendiceal wall, the diagnosis of adenoma should only be made if the muscularis mucosae is intact, since this implies that the lesion is curable by local excision WHO Classification of Tumours, 2000




29 Pseudomyxoma peritonei Mucinous material on peritoneal surfaces Spares intestinal serosa Involves omentum, around liver, pelvis Hernial sacs Pleura Retroperitoneum Splenic mucous cysts
30 Pseudomyxoma peritonei Progressive accumulation and recurrent intestinal obstruction, often over years Most cases related to appendiceal or ovarian mucinous tumours, many not overtly invasive (borderline tumours) Prognosis related to extent of disease cellularity degree of cytological atypia presence of overt carcinoma
31 Sugarbaker Technique combines complete surgical tumour removal (complete cytoreduction) with intraoperative heated chemotherapy (10 hours): removal of the right hemicolon, spleen, gallbladder, greater omentum and lesser omentum stripping of the peritoneum from the pelvis and diaphragm stripping of the tumour from the surface of the liver removal of the uterus and ovaries in women removal of the rectum in some cases followed by postoperative intraperitoneal chemotherapy
32 Misconceptions in Pseudomyxoma? only cases associated with an underlying carcinoma behave aggressively localised pseudomyxoma is always benign acellular mucous pools are always benign many cases arise from an ovarian mucinous tumour




33 Pseudomyxoma peritonei Great majority have an intestinal phenotype CK20 + CK7+ MUC2 + CDX-2 expression Nonaka D et al 2006 Histopathology 49: 381






34



35
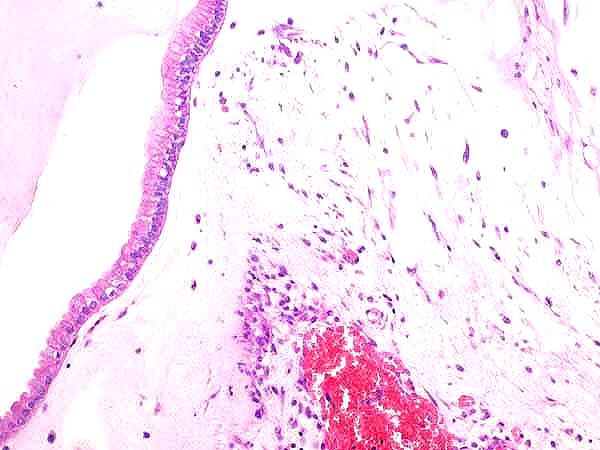
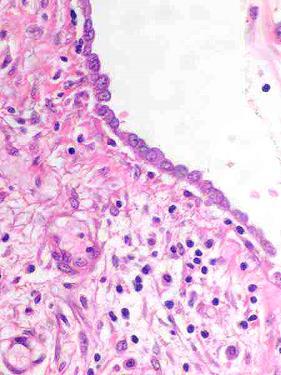
36 Appendiceal Mucinous Neoplasms LAMN - low grade appendiceal mucinous neoplasm low grade cytological atypia minimal architectural complexity no destructive invasion adenomucinosis MACA - mucinous adenocarcinoma of appendix destructive invasion of appendiceal wall OR high grade cytological atypia OR complex papillary fronds or cribriform glandular structures Misdraji J et al Am J Surg Pathol 2003; 27: 1089
37 Appendiceal Mucinous Neoplasms LAMN - low grade appendiceal mucinous neoplasm 88/107 50% confined to appendix - no recurrence 50% peritoneal mucinous tumour - 5 yr survival 86%, 10 yr 45% connection with intramural tumour not always apparent examples of acellular extracellular mucin with progression MACA - mucinous adenocarcinoma of appendix 16/107-5 yr survival 44% 75% peritoneal tumour 8 invasive 8 non-invasive Misdraji J et al Am J Surg Pathol 2003; 27: 1089
38 Appendiceal Mucinous Neoplasms Generous sampling essential LAMN - low grade appendiceal mucinous neoplasm confined to appendix - benign with extra-appendiceal peritoneal spread - guarded role of hemicolectomy unproven MACA - mucinous adenocarcinoma of appendix never benign invasive - adenocarcinoma non-invasive caution



39 Hyperplastic (metaplastic) Polyp

40 Appendiceal Mucosal Hyperplasia Diffuse flat mucosal changes resembling hyperplastic polyps Associated with mucocoele Results from appendiceal obstruction that is insufficient to compromise blood flow No dysplasia

41 Sessile Serrated Adenoma Serrated, dilated and branched crypts with horizontal growth Microsatellite instability DNA methylation MLH1 inactivation BRAF mutation
42 NEUROENDOCRINE TUMOURS OF APPENDIX NORMAL STRUCTURE AND FUNCTION Enterochromaffin cells Originally thought to be of neural crest origin (APUD) Now known to be of endodermal origin, from gut stem cells Ganglion cells of neural crest origin

43 NEUROENDOCRINE TUMOURS OF APPENDIX GOBLET CELL ENTERO- STEM CELL ENTEROCYT ENDOCRINE CELL PANETH CELL
44 NEUROENDOCRINE TUMOURS OF APPENDIX NORMAL STRUCTURE AND FUNCTION Argyrophil cells (capable of reducing silver salts e.g. Grimelius) Argentaffin cells (require reducing agents e.g. Masson Fontana)
45 NEUROENDOCRINE TUMOURS OF APPENDIX NORMAL STRUCTURE AND FUNCTION Foregut (lung, stomach, 1 st part duodenum) Midgut (2 nd part duodenum +, jejunum, ileum, appendix, right colon) Hindgut (transverse colon, left colon, rectum)
46 NEUROENDOCRINE TUMOURS OF APPENDIX CARCINOID TUMOURS 74% GI, 25% lung, 1% other 2% of all malignant tumours (reported,? actual) Most indolent, capable of metastasis Functional consequences
47 NEUROENDOCRINE TUMOURS OF APPENDIX SECRETORY PRODUCTS Foregut: 5HT, tachykinins, gastrin, ACTH, HCG Carcinoid syndrome: flushing, diarrhoea, bronchoconstriction, cutaneous oedema Midgut: serotonin (5HT) Hindgut: tachykinins, somatostatin, PP, 5HT, dopamine, neurotensin

48 NEUROENDOCRINE TUMOURS OF APPENDIX CARCINOID SYNDROME Diarrhoea (83%), flushing (49%), dyspnoea (20%), wheezing (6%), right heart valve fibrosis Related to histamine, 5HT etc. Develops in metastatic disease (midgut, hindgut) Hepatic artery chemoembolisation Octreotide
49 NEUROENDOCRINE TUMOURS OF APPENDIX DISTRIBUTION Oesophagus 0.05% Stomach 4.3% Small bowel 39% (ileum 21%) Appendix 25.6% Colon 31% (rectum 17%)
50 NEUROENDOCRINE TUMOURS OF APPENDIX SITE Local 5YS Reg 5YS Dist 5YS STOMACH SMALL BOWEL APPENDIX COLON RECTUM
51 NEUROENDOCRINE TUMOURS OF APPENDIX IMMUNOHISTOCHEMISTRY Chromogranin A: 88% foregut, 100% midgut, 60% hindgut Synaptophysin (100%!) Neurone specific enolase (NSE) Cytokeratin 18 (not appendix, not CK 20) N-CAM (CD56): 77% foregut, 58% midgut, 20% hindgut CEA 26% S-100 protein 100% appendix
52 NEUROENDOCRINE TUMOURS OF APPENDIX APPENDIX CARCINOIDS 77% of tumours at this site Females 2 x male (others 1.15 M:F) Incidental gynae. procedures Most incidental at appendicitis 75% at tip, 10% at base
53 NEUROENDOCRINE TUMOURS OF APPENDIX APPENDIX CARCINOIDS Appendix reaches adult size at 4 years Epithelial NE cells uniform throughout life Deep subepithelial NE cells with age Presumed cell of origin 5HT+, Masson Fontana+ Yellow nodule Trabecular/nested, low mitoses <1cm:70-90%, 1-2cm: 4-25%, >2cm: rare
54 NEUROENDOCRINE TUMOURS OF APPENDIX GOBLET CELL CARCINOID Both glandular and neuroendocrine morphology More aggressive Increased atypia, mitoses Rare: most common in appendix, <5% of tumours at this site Also seen around ampulla Arise below crypts Goblet cells, tubular glands, mucin May be Paneth cells
55 NEUROENDOCRINE TUMOURS OF APPENDIX GOBLET CELL CARCINOID Symptomatic presentation Appendicitis, mass, obstruction Leads to recurrent disease Dissemination within abdomen Peritoneal, ovarian involvement Indication for right hemicolectomy If mitotically active, nuclear atypia, spread beyond appendix

56
57 NEUROENDOCRINE TUMOURS OF APPENDIX Grading system for gastrointestinal endocrine tumours Grade Mitotic count (10HPF)* Ki-67 index (%)** G1 <2 2 G >2 20 G3 >20 >20 * 10 HPF: high power field = 2 mm2, at least 40 fields evaluated in areas at highest mitotic density ** MIB1 antibody; % of tumour cells in a 2000 cell sample from the areas of highest nuclear labelling. Dataset for endocrine tumours of the gastrointestinal tract including pancreas.
58 Appendiceal Carcinoids EC-cell Carcinoids L-cell Carcinoids Goblet cell Carcinoids




59 EC-cell Carcinoids >95% Appendiceal Carcinoids insular pattern uncommon variants - clear cell, balloon cell, acinar may contain S-100-positive Schwann-like cells



60 <5% Appendiceal Carcinoids L-cell Carcinoids trabecular or tubular non-argentaffin but argyrophil contain enteroglucagons, PP or PYY usually chromogranin A negative chromogranin B and SV2 positive
61 Goblet Cell Carcinoids Females>males Incidental or appendicitis Often diffuse growth pattern, unsuspected grossly Genetically different from conventional carcinoids and adenocarcinomas (e.g. no K-ras mutations) Propensity for transcoelomic spread, especially to ovary Lymph node and liver metastases relatively unusual 80% 5 year survival
62 Goblet Cell Carcinoids Mucous cells Enterocytes/colonocytes Endocrine cells (EC-cells or L-cells) Paneth cells Aggressive features Nuclear pleomorphism Mitotic rate (>2/10 HPF) Carcinomatous growth: single file structures diffusely infiltrating signet ring cells cribriform glands solid sheets




63




64
65 Management Tumour confined to appendix with minimal invasion of mesoappendix Minority component carcinomatous Appendicectomy Extensive invasion of mesoappendix Involvement of resection line, invasion of caecum, lymph node involvement Majority component carcinomatous Right hemicolectomy

66 Signet Ring Carcinoma Rare Part of spectrum of goblet cell carcinoid and mucinous adenocarcinoma E-cadherin negative Beta-catenin negative Always consider metastasis stomach breast
 Modified Delphi Process. Carr et al. American Journal of Surgical Pathology. 40(1):14-26, January 2016. DOI: 10.1097/PAS.0000000000000535 FIGURE 1. PMP derived from an LAMN.")
67 FIGURE 1 A Consensus for Classification and Pathologic Reporting of Pseudomyxoma Peritonei and Associated Appendiceal Neoplasia: The Results of the Peritoneal Surface Oncology Group International (PSOGI) Modified Delphi Process. Carr et al. American Journal of Surgical Pathology. 40(1):14-26, January DOI: /PAS FIGURE 1. PMP derived from an LAMN. The specimen in (A) is from the right subphrenic space. The specimen in (B) is from the omentum and shows the hyaline fibrosis that is a common feature. Both specimens are classified as low-grade mucinous carcinoma peritonei/disseminated peritoneal adenomucinosis. Copyright 2016 Wolters Kluwer Health, Inc. All rights reserved. Published by Lippincott Williams & Wilkins, Inc. 2

68 FIGURE 2 FIGURE 2. This appendiceal mucinous lesion consists of epithelium showing minimal cytologic atypia that is pushing into the underling appendiceal wall but without an infiltrative invasive pattern. In the consensus classification, the lesion is an LAMN. Copyright 2016 Wolters Kluwer Health, Inc. All rights reserved. Published by Lippincott Williams & Wilkins, Inc. 3
69 TABLE 1 Copyright 2016 Wolters Kluwer Health, Inc. All rights reserved. Published by Lippincott Williams & Wilkins, Inc. 4

70 FIGURE 3 FIGURE 3. Infiltrative invasion in an appendiceal adenocarcinoma. Small, angulated glands are surrounded by desmoplasia. Copyright 2016 Wolters Kluwer Health, Inc. All rights reserved. Published by Lippincott Williams & Wilkins, Inc. 5

71 FIGURE 4 FIGURE 4. LAMN with hyaline fibrosis of the underlying tissue. Copyright 2016 Wolters Kluwer Health, Inc. All rights reserved. Published by Lippincott Williams & Wilkins, Inc. 6

72 FIGURE 5 FIGURE 5. HAMN resembles an LAMN at low power (A) but the cytologic atypia is marked (B). Copyright 2016 Wolters Kluwer Health, Inc. All rights reserved. Published by Lippincott Williams & Wilkins, Inc. 7

73 FIGURE 6 FIGURE 6. Serrated polyp of appendix without dysplasia. It closely resembles a sessile serrated adenoma of the colon. Note that the muscularis mucosae is intact. Copyright 2016 Wolters Kluwer Health, Inc. All rights reserved. Published by Lippincott Williams & Wilkins, Inc. 8
74 TABLE 2 TABLE 2 Classification of PMP (Peritoneal Disease Component) Copyright 2016 Wolters Kluwer Health, Inc. All rights reserved. Published by Lippincott Williams & Wilkins, Inc. 9
75 FIGURE 7 Copyright 2016 Wolters Kluwer Health, Inc. All rights reserved. Published by Lippincott Williams & Wilkins, Inc. 10

76 THANK YOU FOR YOUR ATTENTION ANY QUESTIONS?
Joseph Misdraji, M.D. GI pathology Unit Massachusetts General Hospital
 Joseph Misdraji, M.D. GI pathology Unit Massachusetts General Hospital jmisdraji@partners.org Low-grade appendiceal mucinous neoplasm (LAMN) High-grade appendiceal mucinous neoplasm (HAMN) Adenocarcinoma
Joseph Misdraji, M.D. GI pathology Unit Massachusetts General Hospital jmisdraji@partners.org Low-grade appendiceal mucinous neoplasm (LAMN) High-grade appendiceal mucinous neoplasm (HAMN) Adenocarcinoma
GOBLET CELL CARCINOID. Hanlin L. Wang, MD, PhD University of California Los Angeles
 GOBLET CELL CARCINOID Hanlin L. Wang, MD, PhD University of California Los Angeles Disclosure of Relevant Financial Relationships USCAP requires that all planners (Education Committee) in a position to
GOBLET CELL CARCINOID Hanlin L. Wang, MD, PhD University of California Los Angeles Disclosure of Relevant Financial Relationships USCAP requires that all planners (Education Committee) in a position to
GOBLET CELL CARCINOID
 GOBLET CELL CARCINOID Hanlin L. Wang, MD, PhD University of California Los Angeles Disclosure of Relevant Financial Relationships USCAP requires that all planners (Education Committee) in a position to
GOBLET CELL CARCINOID Hanlin L. Wang, MD, PhD University of California Los Angeles Disclosure of Relevant Financial Relationships USCAP requires that all planners (Education Committee) in a position to
Joseph Misdraji, M.D. GI pathology Unit Massachusetts General Hospital
 Joseph Misdraji, M.D. GI pathology Unit Massachusetts General Hospital jmisdraji@partners.org Adenoma Low-grade appendiceal mucinous neoplasm High-grade appendiceal mucinous neoplasm Adenocarcinoma Serrated
Joseph Misdraji, M.D. GI pathology Unit Massachusetts General Hospital jmisdraji@partners.org Adenoma Low-grade appendiceal mucinous neoplasm High-grade appendiceal mucinous neoplasm Adenocarcinoma Serrated
Community Case. Saeed Awan R5
 Community Case Saeed Awan R5 18 year old presents to ER with history of pain right lower quadrant for three days. Nauseated, denies vomiting and bowel movements normal and no urinary complaint. Admitted
Community Case Saeed Awan R5 18 year old presents to ER with history of pain right lower quadrant for three days. Nauseated, denies vomiting and bowel movements normal and no urinary complaint. Admitted
Syllabus. Appendiceal GCC and LAMN Navigating the Alphabet Soup in the Appendix. Appendiceal tumors. Summary provided Complete presentation
 2016 Current Issues in Surgical Pathology Appendiceal GCC and LAMN Navigating the Alphabet Soup in the Appendix Syllabus Summary provided Complete presentation sanjay.kakar@ucsf.edu Sanjay Kakar, MD University
2016 Current Issues in Surgical Pathology Appendiceal GCC and LAMN Navigating the Alphabet Soup in the Appendix Syllabus Summary provided Complete presentation sanjay.kakar@ucsf.edu Sanjay Kakar, MD University
Despite advances in our understanding of appendiceal. An Update on the Diagnosis, Grading, and Staging of Appendiceal Mucinous Neoplasms
 REVIEW ARTICLE An Update on the Diagnosis, Grading, and Staging of Appendiceal Mucinous Neoplasms Mark A. Valasek, MD, PhD* and Reetesh K. Pai, MD Abstract: Despite advances in our understanding of appendiceal
REVIEW ARTICLE An Update on the Diagnosis, Grading, and Staging of Appendiceal Mucinous Neoplasms Mark A. Valasek, MD, PhD* and Reetesh K. Pai, MD Abstract: Despite advances in our understanding of appendiceal
Chapter 6 Frozen Section Evaluation of the Appendix
 Chapter 6 Frozen Section Evaluation of the Appendix Abstract Appendiceal tumors are rarely diagnosed preoperatively, and their classification is both challenging and controversial owing to their tendency
Chapter 6 Frozen Section Evaluation of the Appendix Abstract Appendiceal tumors are rarely diagnosed preoperatively, and their classification is both challenging and controversial owing to their tendency
Fig. 59 Malignant phaeochromocytoma, hepatic metastasis.
 Fig. 59 Malignant phaeochromocytoma, hepatic metastasis. X 120 Hyperte nsion Fig. 60 Malignant sympathetic paraganglioma, lymph node metastasis Primary in bladder. x 1 20 Hypertension Fig. 61 Malignant
Fig. 59 Malignant phaeochromocytoma, hepatic metastasis. X 120 Hyperte nsion Fig. 60 Malignant sympathetic paraganglioma, lymph node metastasis Primary in bladder. x 1 20 Hypertension Fig. 61 Malignant
GOBLET CELL CARCINOID. Hanlin L. Wang, MD, PhD University of California Los Angeles
 GOBLET CELL CARCINOID Hanlin L. Wang, MD, PhD University of California Los Angeles hanlinwang@mednet.ucla.edu Goblet cell carcinoid (GCC) is a unique type of mixed endocrine-exocrine neoplasm, almost exclusively
GOBLET CELL CARCINOID Hanlin L. Wang, MD, PhD University of California Los Angeles hanlinwang@mednet.ucla.edu Goblet cell carcinoid (GCC) is a unique type of mixed endocrine-exocrine neoplasm, almost exclusively
The pathology of neuroendocrine tumours of the gut
 The pathology of neuroendocrine tumours of the gut Professor Neil A Shepherd Gloucester & Cheltenham, UK Histopathology Regional Teaching Bristol May 11 2016 The pathology of neuroendocrine tumours (NETs)
The pathology of neuroendocrine tumours of the gut Professor Neil A Shepherd Gloucester & Cheltenham, UK Histopathology Regional Teaching Bristol May 11 2016 The pathology of neuroendocrine tumours (NETs)
Management of an Appendiceal Mass - Approach to acute presentation of appendiceal neoplasms
 Management of an Appendiceal Mass - Approach to acute presentation of appendiceal neoplasms Dr. Claudia LY WONG, Department of Surgery, Kwong Wah Hospital Joint Hospital Surgical Grand Round Presentation,
Management of an Appendiceal Mass - Approach to acute presentation of appendiceal neoplasms Dr. Claudia LY WONG, Department of Surgery, Kwong Wah Hospital Joint Hospital Surgical Grand Round Presentation,
Unexpected Findings at Endoscopy
 The Endoscopic Incidentaloma: What to Tell Your Patient t with Unexpected Endoscopic Findings: Gastric Intestinal Metaplasia, Silent Ileitis, Carcinoid David Greenwald, MD Montefiore Medical Center Albert
The Endoscopic Incidentaloma: What to Tell Your Patient t with Unexpected Endoscopic Findings: Gastric Intestinal Metaplasia, Silent Ileitis, Carcinoid David Greenwald, MD Montefiore Medical Center Albert
Specialespecifikt kursus i Patologisk Anatomi 2009: Fordøjelseskanalens patologi APPENDIX
 Specialespecifikt kursus i Patologisk Anatomi 2009: Fordøjelseskanalens patologi APPENDIX Appendix Occurrence of lesions (%) Acute appendicitis 72 Normal 16 Fibrosis 3 (Cyst-)Adenoma 3 Diverticulitis
Specialespecifikt kursus i Patologisk Anatomi 2009: Fordøjelseskanalens patologi APPENDIX Appendix Occurrence of lesions (%) Acute appendicitis 72 Normal 16 Fibrosis 3 (Cyst-)Adenoma 3 Diverticulitis
Salivary Glands 3/7/2017
 Salivary Glands 3/7/2017 Goals and objectives Focus on the entities unique to H&N Common board type facts Information for your future practice Salivary Glands Salivary Glands Major gland. Paratid. Submandibular.
Salivary Glands 3/7/2017 Goals and objectives Focus on the entities unique to H&N Common board type facts Information for your future practice Salivary Glands Salivary Glands Major gland. Paratid. Submandibular.
Neoplasias Quisticas del Páncreas
 SEAP -Aproximación Práctica a la Patología Gastrointestinal- Madrid, 26 de mayo, 2006 Neoplasias Quisticas del Páncreas Gregory Y. Lauwers, M.D. Director, Service Massachusetts General Hospital Harvard
SEAP -Aproximación Práctica a la Patología Gastrointestinal- Madrid, 26 de mayo, 2006 Neoplasias Quisticas del Páncreas Gregory Y. Lauwers, M.D. Director, Service Massachusetts General Hospital Harvard
SCOPE TODAYS SESSION. Case 1: Case 2. Basic Theory Stuff: Heavy Stuff. Basic Questions. Basic Questions
 MONDAY TEACHING SCOPE TODAYS SESSION Case 1: Basic Questions Case 2 Basic Questions Basic Theory Stuff: AJCC TNM + Stage Group for Carcinoid of the Appendix Management of Carcinoid of the Appendix (NCCN)
MONDAY TEACHING SCOPE TODAYS SESSION Case 1: Basic Questions Case 2 Basic Questions Basic Theory Stuff: AJCC TNM + Stage Group for Carcinoid of the Appendix Management of Carcinoid of the Appendix (NCCN)
Urinary Bladder: WHO Classification and AJCC Staging Update 2017
 Urinary Bladder: WHO Classification and AJCC Staging Update 2017 Houston Society of Clinical Pathologists 58 th Annual Spring Symposium Houston, TX April 8, 2017 Jesse K. McKenney, MD Classification
Urinary Bladder: WHO Classification and AJCC Staging Update 2017 Houston Society of Clinical Pathologists 58 th Annual Spring Symposium Houston, TX April 8, 2017 Jesse K. McKenney, MD Classification
Specialised Services Policy: CP02 Hyperthermic Intraperitoneal Chemotherapy (HIPEC) and Cytoreductive Surgery for treatment of Pseudomyxoma Peritonei
 and Cytoreductive Surgery for treatment of Pseudomyxoma Peritonei") Specialised Services Policy: CP02 Hyperthermic Intraperitoneal Chemotherapy (HIPEC) of Pseudomyxoma Peritonei Document Author: Assistant Medical Director Executive Lead: Medical Director Approved by: Management
Specialised Services Policy: CP02 Hyperthermic Intraperitoneal Chemotherapy (HIPEC) of Pseudomyxoma Peritonei Document Author: Assistant Medical Director Executive Lead: Medical Director Approved by: Management
Colon and Rectum: 2018 Solid Tumor Rules
 2018 SEER Solid Tumor Manual 2018 KCR SPRING TRAINING Colon and Rectum: 2018 Solid Tumor Rules 1 Colon and Rectum Solid Tumor Rules Separate sections for: Introduction Changes from 2007 MP/H rules Equivalent
2018 SEER Solid Tumor Manual 2018 KCR SPRING TRAINING Colon and Rectum: 2018 Solid Tumor Rules 1 Colon and Rectum Solid Tumor Rules Separate sections for: Introduction Changes from 2007 MP/H rules Equivalent
Surgical Management of Neuroendocrine Tumors of the Gut. Richard Hodin MD Professor of Surgery Massachusetts General Hospital Harvard Medical School
 Surgical Management of Neuroendocrine Tumors of the Gut Richard Hodin MD Professor of Surgery Massachusetts General Hospital Harvard Medical School Sites of GI Carcinoid Tumors Small intestine 44% Rectum
Surgical Management of Neuroendocrine Tumors of the Gut Richard Hodin MD Professor of Surgery Massachusetts General Hospital Harvard Medical School Sites of GI Carcinoid Tumors Small intestine 44% Rectum
Select problems in cystic pancreatic lesions
 Disclosure Select problems in cystic pancreatic lesions Five Prime Therapeutics shareholder Adicet Bio shareholder Bristol-Meyer Squibb advisory board grace.kim@ucsf.edu Pancreatic cystic lesions Intraductal
Disclosure Select problems in cystic pancreatic lesions Five Prime Therapeutics shareholder Adicet Bio shareholder Bristol-Meyer Squibb advisory board grace.kim@ucsf.edu Pancreatic cystic lesions Intraductal
COLON AND RECTUM SOLID TUMOR RULES ABSTRACTORS TRAINING
 COLON AND RECTUM SOLID TUMOR RULES ABSTRACTORS TRAINING COLON AND RECTUM SOLID TUMOR RULES Separate sections for: Introduction Changes from 2007 MP/H rules Equivalent Terms Terms that are NOT Equivalent
COLON AND RECTUM SOLID TUMOR RULES ABSTRACTORS TRAINING COLON AND RECTUM SOLID TUMOR RULES Separate sections for: Introduction Changes from 2007 MP/H rules Equivalent Terms Terms that are NOT Equivalent
colorectal cancer Colorectal cancer hereditary sporadic Familial 1/12/2018
 colorectal cancer Adenocarcinoma of the colon and rectum is the third most common site of new cancer cases and deaths in men (following prostate and lung or bronchus cancer) and women (following breast
colorectal cancer Adenocarcinoma of the colon and rectum is the third most common site of new cancer cases and deaths in men (following prostate and lung or bronchus cancer) and women (following breast
Neoplasms of the Canine, Feline and Lemur Liver:
 Neoplasms of the Canine, Feline and Lemur Liver: Classification and Prognosis Annual Seminar of the French Society of Veterinary Pathology John M. Cullen VMD PhD DACVP North Carolina State University Primary
Neoplasms of the Canine, Feline and Lemur Liver: Classification and Prognosis Annual Seminar of the French Society of Veterinary Pathology John M. Cullen VMD PhD DACVP North Carolina State University Primary
Bowel obstruction and tumors
 Bowel obstruction and tumors Intestinal Obstruction Obstruction of the GI tract may occur at any level, but the small intestine is most often involved because of its relatively narrow lumen. Causes: Hernias
Bowel obstruction and tumors Intestinal Obstruction Obstruction of the GI tract may occur at any level, but the small intestine is most often involved because of its relatively narrow lumen. Causes: Hernias
Pre-operative assessment of patients for cytoreduction and HIPEC
 Pre-operative assessment of patients for cytoreduction and HIPEC Washington Hospital Center Washington, DC, USA Ovarian Cancer Surgery New Strategies Bergamo, Italy May 5, 2011 Background Cytoreductive
Pre-operative assessment of patients for cytoreduction and HIPEC Washington Hospital Center Washington, DC, USA Ovarian Cancer Surgery New Strategies Bergamo, Italy May 5, 2011 Background Cytoreductive
Pancreatic Cytopathology: The Solid Neoplasms
 Pancreatic Cytopathology: The Solid Neoplasms Syed Z. Ali, M.D. Professor of Pathology and Radiology Director of Cytopathology The Johns Hopkins Hospital Baltimore, Maryland Pancreatic Cytopathology: Past,
Pancreatic Cytopathology: The Solid Neoplasms Syed Z. Ali, M.D. Professor of Pathology and Radiology Director of Cytopathology The Johns Hopkins Hospital Baltimore, Maryland Pancreatic Cytopathology: Past,
Disorders of Cell Growth & Neoplasia. Histopathology Lab
 Disorders of Cell Growth & Neoplasia Histopathology Lab Paul Hanna April 2010 Case #84 Clinical History: 5 yr-old, West Highland White terrier. skin mass from axillary region. has been present for the
Disorders of Cell Growth & Neoplasia Histopathology Lab Paul Hanna April 2010 Case #84 Clinical History: 5 yr-old, West Highland White terrier. skin mass from axillary region. has been present for the
Synonyms. Nephrogenic metaplasia Mesonephric adenoma
 Nephrogenic Adenoma Synonyms Nephrogenic metaplasia Mesonephric adenoma Definition Benign epithelial lesion of urinary tract with tubular, glandular, papillary growth pattern Most frequently in the urinary
Nephrogenic Adenoma Synonyms Nephrogenic metaplasia Mesonephric adenoma Definition Benign epithelial lesion of urinary tract with tubular, glandular, papillary growth pattern Most frequently in the urinary
APPENDIX 5 PATHOLOGY 1. Handling and gross examination of gastrointestinal and pancreatic NETs
 APPENDIX 5 PATHOLOGY 1. Handling and gross examination of gastrointestinal and pancreatic NETs Specimen handling and gross examination should be performed according to the Royal College of Pathologists
APPENDIX 5 PATHOLOGY 1. Handling and gross examination of gastrointestinal and pancreatic NETs Specimen handling and gross examination should be performed according to the Royal College of Pathologists
Section 1. Biology of gynaecological cancers: our current understanding
 Section 1 Biology of gynaecological cancers: our current understanding Chapter 1 Morphological sub-types of ovarian carcinoma: new developments and pathogenesis W Glenn McCluggage 1 Introduction In most
Section 1 Biology of gynaecological cancers: our current understanding Chapter 1 Morphological sub-types of ovarian carcinoma: new developments and pathogenesis W Glenn McCluggage 1 Introduction In most
Information for health professionals - pseudomyxoma peritonei
 Colorectal and peritoneal oncology centre Information for health professionals - pseudomyxoma peritonei What is it? Pseudomyxoma Peritonei (PMP) is often a slowly progressive disease that produces extensive
Colorectal and peritoneal oncology centre Information for health professionals - pseudomyxoma peritonei What is it? Pseudomyxoma Peritonei (PMP) is often a slowly progressive disease that produces extensive
Adenocarcinoid Tumor of the Colon Arising in Preexisting Ulcera tive Colitis
 Adenocarcinoid Tumor of the Colon Arising in Preexisting Ulcera tive Colitis ALAN P. LYSS, MD,* JOHN J. THOMPSON, MD,t AND JOHN H. GLICK, MD* F Patients with ulcerative colitis are at increased risk of
Adenocarcinoid Tumor of the Colon Arising in Preexisting Ulcera tive Colitis ALAN P. LYSS, MD,* JOHN J. THOMPSON, MD,t AND JOHN H. GLICK, MD* F Patients with ulcerative colitis are at increased risk of
Polyps in general: is a descriptive term of forming a mass that is exophytic & polypoid.
 ميحرلا نمحرلا هللا مسب Gastric Tumors: Benign tumours & tumor-like conditions: -Mucosal: Gastric polyps (they are uncommon) -Mesenchymal tumours: Leiomyoma & Lipoma (can occur anywhere in the body) Malignant:
ميحرلا نمحرلا هللا مسب Gastric Tumors: Benign tumours & tumor-like conditions: -Mucosal: Gastric polyps (they are uncommon) -Mesenchymal tumours: Leiomyoma & Lipoma (can occur anywhere in the body) Malignant:
Basic Data. Birthday: Gender:Female Admission date:
 Basic Data Birthday:1951-07-02 Gender:Female Admission date:2004-06-28 Chief Complaint A protruding mass over RLQ abdomen for many years. Present Illness & Past History Pseudomyxoma peritonei s/p laparotomy
Basic Data Birthday:1951-07-02 Gender:Female Admission date:2004-06-28 Chief Complaint A protruding mass over RLQ abdomen for many years. Present Illness & Past History Pseudomyxoma peritonei s/p laparotomy
Case year old female presented with asymmetric enlargement of the left lobe of the thyroid
 Case 4 22 year old female presented with asymmetric enlargement of the left lobe of the thyroid gland. No information available relative to a prior fine needle aspiration biopsy. A left lobectomy was performed.
Case 4 22 year old female presented with asymmetric enlargement of the left lobe of the thyroid gland. No information available relative to a prior fine needle aspiration biopsy. A left lobectomy was performed.
Case 4 Diagnosis 2/21/2011 TGB
 Case 4 22 year old female presented with asymmetric enlargement of the left lobe of the thyroid gland. No information available relative to a prior fine needle aspiration biopsy. A left lobectomy was performed.
Case 4 22 year old female presented with asymmetric enlargement of the left lobe of the thyroid gland. No information available relative to a prior fine needle aspiration biopsy. A left lobectomy was performed.
Neuroendocrine tumors of GI and Pancreatobiliary tracts. N. Volkan Adsay, MD
 Neuroendocrine tumors of GI and Pancreatobiliary tracts N. Volkan Adsay, MD New (2017) WHO WHO 2017 (endocrine book; for pancreas) WHO 2017 (endocrine book; for pancreas) PD-NE ca WD-NE Tumor Intended
Neuroendocrine tumors of GI and Pancreatobiliary tracts N. Volkan Adsay, MD New (2017) WHO WHO 2017 (endocrine book; for pancreas) WHO 2017 (endocrine book; for pancreas) PD-NE ca WD-NE Tumor Intended
1. Esophageal diverticulum located above the upper esophageal sphincter is called
 Test Bank for Robbins Basic Pathology 9th Edition by Kumar Link full download: http://testbankair.com/download/test-bank-for-robbins-basic-pathology-9thedition-by-kumar/ Chapter 14: Oral Cavity and Gastrointestinal
Test Bank for Robbins Basic Pathology 9th Edition by Kumar Link full download: http://testbankair.com/download/test-bank-for-robbins-basic-pathology-9thedition-by-kumar/ Chapter 14: Oral Cavity and Gastrointestinal
Mody. AIS vs. Invasive Adenocarcinoma of the Cervix
 Common Problems in Gynecologic Pathology Michael T. Deavers, M.D. Houston Methodist Hospital, Houston, Texas Common Problems in Gynecologic Pathology Adenocarcinoma in-situ (AIS) of the Cervix vs. Invasive
Common Problems in Gynecologic Pathology Michael T. Deavers, M.D. Houston Methodist Hospital, Houston, Texas Common Problems in Gynecologic Pathology Adenocarcinoma in-situ (AIS) of the Cervix vs. Invasive
Tumors of the Intestines. Malignant Lesion. Adenocarcinoma. sessile Serrated Adenomas
 Tumors of the Intestines Non-Neoplastic Polyps Neoplastic Epithelial Polyps Other Tumors Hyperplastic, Hamartomatous, Juvenile, Peutz-Jeghers, Inflammatory abd Lymphoid Polyphs Benign Polyphs Malignant
Tumors of the Intestines Non-Neoplastic Polyps Neoplastic Epithelial Polyps Other Tumors Hyperplastic, Hamartomatous, Juvenile, Peutz-Jeghers, Inflammatory abd Lymphoid Polyphs Benign Polyphs Malignant
Goblet Cell Carcinoids of the Appendix
 40 Ulster Med J 2006; 75 (1) 40-45 The Ulster Medical Journal Review Goblet Cell Carcinoids of the Appendix R Arnold, K McCallion, C McGailie Accepted 14 October 2005 INTRODUCTION Carcinoid tumours are
40 Ulster Med J 2006; 75 (1) 40-45 The Ulster Medical Journal Review Goblet Cell Carcinoids of the Appendix R Arnold, K McCallion, C McGailie Accepted 14 October 2005 INTRODUCTION Carcinoid tumours are
Objectives. Terminology 03/11/2013. Pitfalls in the diagnosis of Gastroenteropancreatic Neuroendocrine Tumors. Pathology Update 2013
 Pitfalls in the diagnosis of Gastroenteropancreatic Neuroendocrine Tumors Pathology Update 2013 Ozgur Mete, MD Consultant in Endocrine Pathology, Department of Pathology, University Health Network Assistant
Pitfalls in the diagnosis of Gastroenteropancreatic Neuroendocrine Tumors Pathology Update 2013 Ozgur Mete, MD Consultant in Endocrine Pathology, Department of Pathology, University Health Network Assistant
Serrated Lesions in the Bowel Cancer Screening Programme
 Serrated Lesions in the Bowel Cancer Screening Programme Mark Arends Cambridge & Edinburgh Serrated Lesions of Large Bowel 1. Hyperplastic polyp 2. Serrated adenoma 3. Mixed polyp 4. Sessile serrated lesion
Serrated Lesions in the Bowel Cancer Screening Programme Mark Arends Cambridge & Edinburgh Serrated Lesions of Large Bowel 1. Hyperplastic polyp 2. Serrated adenoma 3. Mixed polyp 4. Sessile serrated lesion
LOINC. Clinical information. RCPA code. Record if different to report header Operating surgeon name and contact details. Absent.
 Complete as narrative or use the structured format below 55752-0 17.02.28593 Clinical information 22027-7 17.02.30001 Record if different to report header Operating surgeon name and contact details 52101004
Complete as narrative or use the structured format below 55752-0 17.02.28593 Clinical information 22027-7 17.02.30001 Record if different to report header Operating surgeon name and contact details 52101004
Colorectal Cancer Structured Pathology Reporting Proforma DD MM YYYY
 Colorectal Cancer Structured Pathology Reporting Proforma Mandatory questions (i.e. protocol standards) are in bold (e.g. S1.03). Family name Given name(s) Date of birth DD MM YYYY S1.02 Clinical details
Colorectal Cancer Structured Pathology Reporting Proforma Mandatory questions (i.e. protocol standards) are in bold (e.g. S1.03). Family name Given name(s) Date of birth DD MM YYYY S1.02 Clinical details
Anatomy of the biliary tract
 Harvard-MIT Division of Health Sciences and Technology HST.121: Gastroenterology, Fall 2005 Instructors: Dr. Jonathan Glickman Anatomy of the biliary tract Figure removed due to copyright reasons. Biliary
Harvard-MIT Division of Health Sciences and Technology HST.121: Gastroenterology, Fall 2005 Instructors: Dr. Jonathan Glickman Anatomy of the biliary tract Figure removed due to copyright reasons. Biliary
International Society of Gynecological Pathologists Symposium 2007
 International Society of Gynecological Pathologists Symposium 2007 Anais Malpica, M.D. Department of Pathology The University of Texas M.D. Anderson Cancer Center Grading of Ovarian Cancer Histologic grade
International Society of Gynecological Pathologists Symposium 2007 Anais Malpica, M.D. Department of Pathology The University of Texas M.D. Anderson Cancer Center Grading of Ovarian Cancer Histologic grade
Gastrointestinal pathology 2018 lecture 4. Dr Heyam Awad FRCPath
 Gastrointestinal pathology 2018 lecture 4 Dr Heyam Awad FRCPath Topics to be covered Peptic ulcer disease Hiatal hernia Gastric neoplasms Peptic ulcer disease (PUD)= chronic gastric ulcer Causes H pylori
Gastrointestinal pathology 2018 lecture 4 Dr Heyam Awad FRCPath Topics to be covered Peptic ulcer disease Hiatal hernia Gastric neoplasms Peptic ulcer disease (PUD)= chronic gastric ulcer Causes H pylori
Enterprise Interest Nothing to declare
 Enterprise Interest Nothing to declare Update of mixed tumours of the GI tract, the pancreas and the liver Introduction to the concept of mixed tumours and clinical implication Jean-Yves SCOAZEC Surgical
Enterprise Interest Nothing to declare Update of mixed tumours of the GI tract, the pancreas and the liver Introduction to the concept of mixed tumours and clinical implication Jean-Yves SCOAZEC Surgical
Imaging Evaluation of Polyps. CT Colonography: Sessile Adenoma. Polyps, DALMs & Megacolon Objectives
 Polyps, DALMs & Megacolon: Pathology and Imaging of the Colon and Rectum Angela D. Levy and Leslie H. Sobin Washington, DC Drs. Levy and Sobin have indicated that they have no relationships which, in the
Polyps, DALMs & Megacolon: Pathology and Imaging of the Colon and Rectum Angela D. Levy and Leslie H. Sobin Washington, DC Drs. Levy and Sobin have indicated that they have no relationships which, in the
Wendy L Frankel. Chair and Distinguished Professor
 1 Wendy L Frankel Chair and Distinguished Professor Case 1 59 y/o woman Abdominal pain No personal or family history of cancer History of colon polyps Colonoscopy Polypoid rectosigmoid mass Biopsy 3 4
1 Wendy L Frankel Chair and Distinguished Professor Case 1 59 y/o woman Abdominal pain No personal or family history of cancer History of colon polyps Colonoscopy Polypoid rectosigmoid mass Biopsy 3 4
Gross appearance of nodular hyperplasia in material obtained from suprapubic prostatectomy. Note the multinodular appearance and the admixture of
 Tiền liệt tuyến Tiền liệt tuyến Gross appearance of nodular hyperplasia in material obtained from suprapubic prostatectomy. Note the multinodular appearance and the admixture of solid and microcystic areas.
Tiền liệt tuyến Tiền liệt tuyến Gross appearance of nodular hyperplasia in material obtained from suprapubic prostatectomy. Note the multinodular appearance and the admixture of solid and microcystic areas.
05/07/2018. Types of challenges. Challenging cases in uterine pathology. Case 1 ` 65 year old female Post menopausal bleeding Uterine Polyp
 Types of challenges Challenging cases in uterine pathology Nafisa Wilkinson Gynaecological Pathologist UCLH London Lack of complete history often, NO clinical history at all! Cases from other centres often
Types of challenges Challenging cases in uterine pathology Nafisa Wilkinson Gynaecological Pathologist UCLH London Lack of complete history often, NO clinical history at all! Cases from other centres often
EDUCATIONAL CASES E1 & E2. Natasha Inglis 20/03/15
 EDUCATIONAL CASES E1 & E2 Natasha Inglis 20/03/15 CASE E1 79 year old female Rectum. Altemeier operation Histology Superficial erosions and mucosal congestion volcano lesion and pseudomembrane formation
EDUCATIONAL CASES E1 & E2 Natasha Inglis 20/03/15 CASE E1 79 year old female Rectum. Altemeier operation Histology Superficial erosions and mucosal congestion volcano lesion and pseudomembrane formation
ONCOLOGY. Csaba Bödör. Department of Pathology and Experimental Cancer Research november 19., ÁOK, III.
 ONCOLOGY Csaba Bödör Department of Pathology and Experimental Cancer Research 2018. november 19., ÁOK, III. bodor.csaba1@med.semmelweis-univ.hu ONCOLOGY Characteristics of Benign and Malignant Neoplasms
ONCOLOGY Csaba Bödör Department of Pathology and Experimental Cancer Research 2018. november 19., ÁOK, III. bodor.csaba1@med.semmelweis-univ.hu ONCOLOGY Characteristics of Benign and Malignant Neoplasms
World Journal of Colorectal Surgery
 World Journal of Colorectal Surgery Volume 6, Issue 4 2016 Article 3 Laparoscopic Right Colectomy For Appendiceal Mucinous Cystadenoma: A Case Report Dion A. Putra Adianto Nugroho Ibrahim Basir University
World Journal of Colorectal Surgery Volume 6, Issue 4 2016 Article 3 Laparoscopic Right Colectomy For Appendiceal Mucinous Cystadenoma: A Case Report Dion A. Putra Adianto Nugroho Ibrahim Basir University
Polypoid lesions of the gastrointestinal tract
 Polypoid lesions of the gastrointestinal tract Professor Neil A Shepherd Gloucester & Cheltenham, UK 27 th IAP-AD Congress 2 nd Emirates Surgical Pathology Conference Dubai, 26 November 2015 Polypoid lesions
Polypoid lesions of the gastrointestinal tract Professor Neil A Shepherd Gloucester & Cheltenham, UK 27 th IAP-AD Congress 2 nd Emirates Surgical Pathology Conference Dubai, 26 November 2015 Polypoid lesions
GASTROINTESTINAL IMAGING STUDY GUIDE
 GASTROINTESTINAL IMAGING STUDY GUIDE Pharynx Diverticula Foreign bodies Trauma o Motility Disorders Esophagus Diverticula Trauma Esophagitis Barrett esophagus Rings, webs, and strictures Varices Benign
GASTROINTESTINAL IMAGING STUDY GUIDE Pharynx Diverticula Foreign bodies Trauma o Motility Disorders Esophagus Diverticula Trauma Esophagitis Barrett esophagus Rings, webs, and strictures Varices Benign
Appendix 4: WHO Classification of Tumours of the pancreas 17
 S3.01 The WHO histological tumour type must be recorded. CS3.01a The histological type of the tumour should be recorded based on the current WHO classification 17 (refer to Appendices 4-7). Appendix 4:
S3.01 The WHO histological tumour type must be recorded. CS3.01a The histological type of the tumour should be recorded based on the current WHO classification 17 (refer to Appendices 4-7). Appendix 4:
Epithelial tumors. Dr. F.F. Khuzin, PhD Dr. M.O. Mavlikeev
 Epithelial tumors Dr. F.F. Khuzin, PhD Dr. M.O. Mavlikeev Epithelial tumors Tumors from the epithelium are the most frequent among tumors. There are 2 group features of these tumors: The presence in most
Epithelial tumors Dr. F.F. Khuzin, PhD Dr. M.O. Mavlikeev Epithelial tumors Tumors from the epithelium are the most frequent among tumors. There are 2 group features of these tumors: The presence in most
COLORECTAL PATHWAY GROUP, MANCHESTER CANCER. Guidelines for the assessment of mismatch. Colorectal Cancer
 COLORECTAL PATHWAY GROUP, MANCHESTER CANCER Guidelines for the assessment of mismatch repair (MMR) status in Colorectal Cancer January 2015 1 Background Mismatch repair (MMR) deficiency is seen in approximately
COLORECTAL PATHWAY GROUP, MANCHESTER CANCER Guidelines for the assessment of mismatch repair (MMR) status in Colorectal Cancer January 2015 1 Background Mismatch repair (MMR) deficiency is seen in approximately
12/7/2011. Pathological mimics of malignancy in the GI tract. Professor Neil A Shepherd President, British Division of the IAP
 Pathological mimics of malignancy in the GI tract Professor Neil A Shepherd President, British Division of the IAP IAP-AD, Beirut, Lebanon 1 December 2011 How do we become aware of the problems and the
Pathological mimics of malignancy in the GI tract Professor Neil A Shepherd President, British Division of the IAP IAP-AD, Beirut, Lebanon 1 December 2011 How do we become aware of the problems and the
Normal endometrium: A, proliferative. B, secretory.
 Normal endometrium: A, proliferative. B, secretory. Nội mạc tử cung Nội mạc tử cung Cyclic changes in endometrium.. Approximate relationship of useful microscopic changes. Arias-Stella reaction in endometrial
Normal endometrium: A, proliferative. B, secretory. Nội mạc tử cung Nội mạc tử cung Cyclic changes in endometrium.. Approximate relationship of useful microscopic changes. Arias-Stella reaction in endometrial
Colonic Polyp. Najmeh Aletaha. MD
 Colonic Polyp Najmeh Aletaha. MD 1 Polyps & classification 2 Colorectal cancer risk factors 3 Pathogenesis 4 Surveillance polyp of the colon refers to a protuberance into the lumen above the surrounding
Colonic Polyp Najmeh Aletaha. MD 1 Polyps & classification 2 Colorectal cancer risk factors 3 Pathogenesis 4 Surveillance polyp of the colon refers to a protuberance into the lumen above the surrounding
FINAL HISTOLOGICAL DIAGNOSIS: Villo-adenomatous polyp with in-situ-carcinomatous foci (involving both adenomatous and villous component).
.") SOLITARY VILLO ADENOMATOUS POLYP WITH CARCINOMATOUS CHANGES RECTUM: A Divvya B 1, M. Valluvan 2, Rehana Tippoo 3, P. Viswanathan 4, R. Baskaran 5 HOW TO CITE THIS ARTICLE: Divvya B, M. Valluvan, Rehana
SOLITARY VILLO ADENOMATOUS POLYP WITH CARCINOMATOUS CHANGES RECTUM: A Divvya B 1, M. Valluvan 2, Rehana Tippoo 3, P. Viswanathan 4, R. Baskaran 5 HOW TO CITE THIS ARTICLE: Divvya B, M. Valluvan, Rehana
COLORECTAL PATHWAY GROUP, MANCHESTER CANCER. Guidelines for the assessment of mismatch. Colorectal Cancer
 COLORECTAL PATHWAY GROUP, MANCHESTER CANCER Guidelines for the assessment of mismatch repair (MMR) status in Colorectal Cancer March 2017 1 Background Mismatch repair (MMR) deficiency is seen in approximately
COLORECTAL PATHWAY GROUP, MANCHESTER CANCER Guidelines for the assessment of mismatch repair (MMR) status in Colorectal Cancer March 2017 1 Background Mismatch repair (MMR) deficiency is seen in approximately
Neoplasia 2018 Lecture 2. Dr Heyam Awad MD, FRCPath
 Neoplasia 2018 Lecture 2 Dr Heyam Awad MD, FRCPath ILOS 1. List the differences between benign and malignant tumors. 2. Recognize the histological features of malignancy. 3. Define dysplasia and understand
Neoplasia 2018 Lecture 2 Dr Heyam Awad MD, FRCPath ILOS 1. List the differences between benign and malignant tumors. 2. Recognize the histological features of malignancy. 3. Define dysplasia and understand
Hyperplastische Polyps Innocent bystanders?
 Hyperplastische Polyps Innocent bystanders?? K. Geboes P th l i h O tl dk d Pathologische Ontleedkunde, KULeuven Content Historical Classification Relation Hyperplastic polyps carcinoma The concept cept
Hyperplastische Polyps Innocent bystanders?? K. Geboes P th l i h O tl dk d Pathologische Ontleedkunde, KULeuven Content Historical Classification Relation Hyperplastic polyps carcinoma The concept cept
Colorectal adenocarcinoma leading cancer in developed countries In US, annual deaths due to colorectal adenocarcinoma 57,000.
 Colonic Neoplasia Remotti Colorectal adenocarcinoma leading cancer in developed countries In US, annual incidence of colorectal adenocarcinoma 150,000. In US, annual deaths due to colorectal adenocarcinoma
Colonic Neoplasia Remotti Colorectal adenocarcinoma leading cancer in developed countries In US, annual incidence of colorectal adenocarcinoma 150,000. In US, annual deaths due to colorectal adenocarcinoma
Carcinoembryonic Antigen
 Other Names/Abbreviations CEA 190.26 - Carcinoembryonic Antigen Carcinoembryonic antigen (CEA) is a protein polysaccharide found in some carcinomas. It is effective as a biochemical marker for monitoring
Other Names/Abbreviations CEA 190.26 - Carcinoembryonic Antigen Carcinoembryonic antigen (CEA) is a protein polysaccharide found in some carcinomas. It is effective as a biochemical marker for monitoring
Gross appearance of peritoneal cysts. They have a thin, translucent wall and contain a clear fluid.
 Gross appearance of peritoneal cysts. They have a thin, translucent wall and contain a clear fluid. So-called multicystic benign mesothelioma. A, Gross appearance. So-called multicystic benign mesothelioma.
Gross appearance of peritoneal cysts. They have a thin, translucent wall and contain a clear fluid. So-called multicystic benign mesothelioma. A, Gross appearance. So-called multicystic benign mesothelioma.
Pancreatitis: A Potential Pitfall in Endoscopic Ultrasound Guided Pancreatic FNA
 Pancreatitis: A Potential Pitfall in Endoscopic Ultrasound Guided Pancreatic FNA Jack Yang, MD Department of Pathology, Medical University of South Carolina Objectives Understand the indication of EUS
Pancreatitis: A Potential Pitfall in Endoscopic Ultrasound Guided Pancreatic FNA Jack Yang, MD Department of Pathology, Medical University of South Carolina Objectives Understand the indication of EUS
Staging Challenges in Lower GI Cancers. Disclosure of Relevant Financial Relationships. AJCC 8 th edition and CAP protocol updates
 Staging Challenges in Lower GI Cancers Sanjay Kakar, MD University of California, San Francisco March 05, 2017 Disclosure of Relevant Financial Relationships USCAP requires that all planners (Education
Staging Challenges in Lower GI Cancers Sanjay Kakar, MD University of California, San Francisco March 05, 2017 Disclosure of Relevant Financial Relationships USCAP requires that all planners (Education
Part 3. Case #7 History:
 Part 3 Case #7 History: The patient is a 25 year old woman who had a colectomy for familial adenomatous polyposis 2 years ago. No carcinoma was found in her colectomy specimen. She presents now with 2
Part 3 Case #7 History: The patient is a 25 year old woman who had a colectomy for familial adenomatous polyposis 2 years ago. No carcinoma was found in her colectomy specimen. She presents now with 2
Gastrointestinal Malignancies. Dr Rodney ITAKI Pathology Division, SMHS, UPNG Anatomical Pathology Discipline
 Gastrointestinal Malignancies Dr Rodney ITAKI Pathology Division, SMHS, UPNG Anatomical Pathology Discipline Esophagus normal anatomy Hollow tube 23-25cm long in adults Extends from pharynx to level of
Gastrointestinal Malignancies Dr Rodney ITAKI Pathology Division, SMHS, UPNG Anatomical Pathology Discipline Esophagus normal anatomy Hollow tube 23-25cm long in adults Extends from pharynx to level of
SAMs Guidelines DEVELOPING SELF-ASSESSMENT MODULES TEST QUESTIONS. Ver. #
 SAMs Guidelines DEVELOPING SELF-ASSESSMENT MODULES TEST Ver. #5-02.12.17 GUIDELINES FOR DEVELOPING SELF-ASSESSMENT MODULES TEST The USCAP is accredited by the American Board of Pathology (ABP) to offer
SAMs Guidelines DEVELOPING SELF-ASSESSMENT MODULES TEST Ver. #5-02.12.17 GUIDELINES FOR DEVELOPING SELF-ASSESSMENT MODULES TEST The USCAP is accredited by the American Board of Pathology (ABP) to offer
8. The polyp in the illustration can be described as (circle all that apply) a. Exophytic b. Pedunculated c. Sessile d. Frank
 a. Exophytic b. Pedunculated c. Sessile d. Frank") Quiz 1 Overview 1. Beginning with the cecum, which is the correct sequence of colon subsites? a. Cecum, ascending, splenic flexure, transverse, hepatic flexure, descending, sigmoid. b. Cecum, ascending,
Quiz 1 Overview 1. Beginning with the cecum, which is the correct sequence of colon subsites? a. Cecum, ascending, splenic flexure, transverse, hepatic flexure, descending, sigmoid. b. Cecum, ascending,
Greater Manchester and Cheshire HPB Unit Guidelines for the Assessment & Management of Hepatobiliary and Pancreatic Disease Chapter 14
 Greater Manchester and Cheshire HPB Unit Guidelines for the Assessment & Management of Hepatobiliary and Pancreatic Disease Chapter 14 Contents 14. Neuroendocrine Tumours 161 14.1. Diagnostic algorithm
Greater Manchester and Cheshire HPB Unit Guidelines for the Assessment & Management of Hepatobiliary and Pancreatic Disease Chapter 14 Contents 14. Neuroendocrine Tumours 161 14.1. Diagnostic algorithm
3/30/2017. Disclosure of Relevant Financial Relationships. Case 5: Polypoid mass in ulcerative colitis. Case 5. TC Smyrk
 Case 5: Polypoid mass in ulcerative colitis TC Smyrk Disclosure of Relevant Financial Relationships USCAP requires that all faculty in a position to influence or control the content of CME disclose any
Case 5: Polypoid mass in ulcerative colitis TC Smyrk Disclosure of Relevant Financial Relationships USCAP requires that all faculty in a position to influence or control the content of CME disclose any
Gastric and Oesophageal Neuroendocrine tumours. Dr Tim Bracey, Consultant Pathologist MBChB PhD MRCS FRCPath
 Gastric and Oesophageal Neuroendocrine tumours Dr Tim Bracey, Consultant Pathologist MBChB PhD MRCS FRCPath Intestinal (and BO) endocrine cells in crypt bases NE cell (granules towards vessels) Paneth
Gastric and Oesophageal Neuroendocrine tumours Dr Tim Bracey, Consultant Pathologist MBChB PhD MRCS FRCPath Intestinal (and BO) endocrine cells in crypt bases NE cell (granules towards vessels) Paneth
POORLY DIFFERENTIATED, HIGH GRADE AND ANAPLASTIC CARCINOMAS: WHAT IS EVERYONE TALKING ABOUT?
 POORLY DIFFERENTIATED, HIGH GRADE AND ANAPLASTIC CARCINOMAS: WHAT IS EVERYONE TALKING ABOUT? AGGRESSIVE THYROID CANCERS PAPILLARY CARCINOMA CERTAIN SUBTYPES POORLY DIFFERENTIATED CARCINOMA HIGH GRADE DIFFERENTIATED
POORLY DIFFERENTIATED, HIGH GRADE AND ANAPLASTIC CARCINOMAS: WHAT IS EVERYONE TALKING ABOUT? AGGRESSIVE THYROID CANCERS PAPILLARY CARCINOMA CERTAIN SUBTYPES POORLY DIFFERENTIATED CARCINOMA HIGH GRADE DIFFERENTIATED
NEOPLASIA-I CANCER. Nam Deuk Kim, Ph.D.
 NEOPLASIA-I CANCER Nam Deuk Kim, Ph.D. 1 2 Tumor in the hieroglyphics of the Edwin Smith papyrus (1,600 B.C., Breasted s translation 1930) 3 War on Cancer (National Cancer Act, 1971) 4 Cancer Acts in Korea
NEOPLASIA-I CANCER Nam Deuk Kim, Ph.D. 1 2 Tumor in the hieroglyphics of the Edwin Smith papyrus (1,600 B.C., Breasted s translation 1930) 3 War on Cancer (National Cancer Act, 1971) 4 Cancer Acts in Korea
Biliary tract tumors
 Short Course 2010 Annual Fall Meeting of the Korean Society for Pathologists Biliary tract tumors Joon Hyuk Choi, M.D., Ph.D. Professor, Department of Pathology, Yeungnam Univ. College of Medicine, Daegu,
Short Course 2010 Annual Fall Meeting of the Korean Society for Pathologists Biliary tract tumors Joon Hyuk Choi, M.D., Ph.D. Professor, Department of Pathology, Yeungnam Univ. College of Medicine, Daegu,
Rectal biopsy as an aid to cancer control in ulcerative colitis
 Rectal biopsy as an aid to cancer control in ulcerative colitis B. C. MORSON AND LILLIAN S. C. PANG From the Research Department, St. Mark's Hospital, London Gut, 1967, 8, 423 EDITORIAL COMMENT This is
Rectal biopsy as an aid to cancer control in ulcerative colitis B. C. MORSON AND LILLIAN S. C. PANG From the Research Department, St. Mark's Hospital, London Gut, 1967, 8, 423 EDITORIAL COMMENT This is
04/10/2018. Intraductal Papillary Neoplasms Of Breast INTRADUCTAL PAPILLOMA
 Intraductal Papillary Neoplasms Of Breast Savitri Krishnamurthy MD Professor of Pathology Deputy Division Head The University of Texas MD Anderson Cancer Center 25 th Annual Seminar in Pathology Pittsburgh,
Intraductal Papillary Neoplasms Of Breast Savitri Krishnamurthy MD Professor of Pathology Deputy Division Head The University of Texas MD Anderson Cancer Center 25 th Annual Seminar in Pathology Pittsburgh,
COLORECTAL CANCER FAISALGHANISIDDIQUI MBBS; FCPS; PGDIP-BIOETHICS; MCPS-HPE
 COLORECTAL CANCER FAISALGHANISIDDIQUI MBBS; FCPS; PGDIP-BIOETHICS; MCPS-HPE PROFESSOR OF SURGERY & DIRECTOR, PROFESSIONAL DEVELOPMENT CENTRE J I N N A H S I N D H M E D I C A L U N I V E R S I T Y faisal.siddiqui@jsmu.edu.pk
COLORECTAL CANCER FAISALGHANISIDDIQUI MBBS; FCPS; PGDIP-BIOETHICS; MCPS-HPE PROFESSOR OF SURGERY & DIRECTOR, PROFESSIONAL DEVELOPMENT CENTRE J I N N A H S I N D H M E D I C A L U N I V E R S I T Y faisal.siddiqui@jsmu.edu.pk
NET und NEC. Endoscopic and oncologic therapy
 NET und NEC Endoscopic and oncologic therapy Classification well-differentiated NET - G1 and G2 - carcinoid poorly-differentiated NEC - G3 - like SCLC well differentiated NET G3 -> elevated proliferation
NET und NEC Endoscopic and oncologic therapy Classification well-differentiated NET - G1 and G2 - carcinoid poorly-differentiated NEC - G3 - like SCLC well differentiated NET G3 -> elevated proliferation
Proceedings of the 36th World Small Animal Veterinary Congress WSAVA
 www.ivis.org Proceedings of the 36th World Small Animal Veterinary Congress WSAVA Oct. 14-17, 2011 Jeju, Korea Next Congress: Reprinted in IVIS with the permission of WSAVA http://www.ivis.org 14(Fri)
www.ivis.org Proceedings of the 36th World Small Animal Veterinary Congress WSAVA Oct. 14-17, 2011 Jeju, Korea Next Congress: Reprinted in IVIS with the permission of WSAVA http://www.ivis.org 14(Fri)
Pancreatic Cystic Lesions 원자력병원
 Pancreatic Cystic Lesions 원자력병원 박선 후 Lines of cellular differentiation Ductal Acinar Undetermined Ductal adenocarcinoma Serous/ mucinous tumor Intraductal papillary mucinous neoplasm Acinar cell carcinoma
Pancreatic Cystic Lesions 원자력병원 박선 후 Lines of cellular differentiation Ductal Acinar Undetermined Ductal adenocarcinoma Serous/ mucinous tumor Intraductal papillary mucinous neoplasm Acinar cell carcinoma
5/21/2018. Prostate Adenocarcinoma vs. Urothelial Carcinoma. Common Differential Diagnoses in Urological Pathology. Jonathan I.
 Common Differential Diagnoses in Urological Pathology Jonathan I. Epstein Prostate Adenocarcinoma vs. Urothelial Carcinoma 1 2 NKX3.1 NKX3.1 3 4 5 6 Proposed ISUP Recommendations Option to use PSA as a
Common Differential Diagnoses in Urological Pathology Jonathan I. Epstein Prostate Adenocarcinoma vs. Urothelial Carcinoma 1 2 NKX3.1 NKX3.1 3 4 5 6 Proposed ISUP Recommendations Option to use PSA as a
Guidelines for the assessment of mismatch repair (MMR) status in Colorectal Cancer
 status in Colorectal Cancer") Guidelines for the assessment of mismatch repair (MMR) status in Colorectal Cancer Start date: May 2015 Review date: April 2018 1 Background Mismatch repair (MMR) deficiency is seen in approximately 15%
Guidelines for the assessment of mismatch repair (MMR) status in Colorectal Cancer Start date: May 2015 Review date: April 2018 1 Background Mismatch repair (MMR) deficiency is seen in approximately 15%
General Session 7: Controversies in Screening and Surveillance in Colorectal Cancer
 General Session 7: Controversies in Screening and Surveillance in Colorectal Cancer Complexities of Pathological Assessment: Serrated Polyps/Adenomas Carolyn Compton, MD, PhD Professor of Life Sciences,
General Session 7: Controversies in Screening and Surveillance in Colorectal Cancer Complexities of Pathological Assessment: Serrated Polyps/Adenomas Carolyn Compton, MD, PhD Professor of Life Sciences,
Disseminated Peritoneal Adenomucinosis Associated with a Panperitonitis-Like Onset: Report of a Case
 Surg Today (2001) 31:646 650 Disseminated Peritoneal Adenomucinosis Associated with a Panperitonitis-Like Onset: Report of a Case Yoshito Kuroki 1, Shunyou Otagiri 1, and Kazuhiro Tsukada 2 1 Department
Surg Today (2001) 31:646 650 Disseminated Peritoneal Adenomucinosis Associated with a Panperitonitis-Like Onset: Report of a Case Yoshito Kuroki 1, Shunyou Otagiri 1, and Kazuhiro Tsukada 2 1 Department
Gastroenterology Tutorial
 Gastroenterology Tutorial Gastritis Poorly defined term that refers to inflammation of the stomach. Infection with H. pylori is the most common cause of gastritis. Most patients remain asymptomatic Some
Gastroenterology Tutorial Gastritis Poorly defined term that refers to inflammation of the stomach. Infection with H. pylori is the most common cause of gastritis. Most patients remain asymptomatic Some
TUMOR AND TUMOR-LIKE CONDITIONS OF THE PERITONEUM AND OMENTUM/MESENTERY 40 th. Annual Meeting SCBTMR September 9-13, 2017, Nashville, Tennessee
 TUMOR AND TUMOR-LIKE CONDITIONS OF THE PERITONEUM AND OMENTUM/MESENTERY 40 th. Annual Meeting SCBTMR September 9-13, 2017, Nashville, Tennessee Isaac R Francis University of Michigan Department of Radiology
TUMOR AND TUMOR-LIKE CONDITIONS OF THE PERITONEUM AND OMENTUM/MESENTERY 40 th. Annual Meeting SCBTMR September 9-13, 2017, Nashville, Tennessee Isaac R Francis University of Michigan Department of Radiology
Appendix cancer mimicking ovarian cancer
 Int J Gynecol Cancer 2002, 12, 768 772 CORRESPONDENCE AND BRIEF REPORTS Appendix cancer mimicking ovarian cancer P. A. GEHRIG *, J. F. BOGGESS*, D. W. OLLILA, P. A. GROBEN & L. VAN LE* *Division of Gynecologic
Int J Gynecol Cancer 2002, 12, 768 772 CORRESPONDENCE AND BRIEF REPORTS Appendix cancer mimicking ovarian cancer P. A. GEHRIG *, J. F. BOGGESS*, D. W. OLLILA, P. A. GROBEN & L. VAN LE* *Division of Gynecologic
Disclosure of Relevant Financial Relationships
 Disclosure of Relevant Financial Relationships USCAP requires that all faculty in a position to influence or control the content of CME disclose any relevant financial relationship WITH COMMERCIAL INTERESTS
Disclosure of Relevant Financial Relationships USCAP requires that all faculty in a position to influence or control the content of CME disclose any relevant financial relationship WITH COMMERCIAL INTERESTS
Solid pseudopapillary tumour of the pancreas: Report of five cases
 ISPUB.COM The Internet Journal of Pathology Volume 8 Number 2 Solid pseudopapillary tumour of the pancreas: Report of five cases P Srilatha, V Manna, P Kanthilatha Citation P Srilatha, V Manna, P Kanthilatha..
ISPUB.COM The Internet Journal of Pathology Volume 8 Number 2 Solid pseudopapillary tumour of the pancreas: Report of five cases P Srilatha, V Manna, P Kanthilatha Citation P Srilatha, V Manna, P Kanthilatha..