Jean-Claude Theis. Section of Orthopaedics Department of Surgical Sciences Dunedin School of Medicine and Hospital Dunedin
|
|
|
- Herbert Brice Hamilton
- 5 years ago
- Views:
Transcription

1 Jean-Claude Theis Section of Orthopaedics Department of Surgical Sciences Dunedin School of Medicine and Hospital Dunedin South GP CME 2013
2 Rare Unstable pelvic fractures OC1C2 fracture dislocations Open arterial limb injuries Serious necrotising infections Spinal infections


3
4 More common Open fracture Knee dislocation Compartment syndrome Acute spinal cord/cauda equina compression Penetrating limb injuries

5 Common Fracture and dislocations Bone and joint infections Tendon and ligament injuries Nerve injuries
6 Priorities: 1. Save the patient s life 2. Save the endangered limb/spine 3. Save the function of the limb Most important MSK injury to detect quickly is an unstable pelvic fracture Can lead to massive life threatening internal bleeding
7 Bleeding control Restore circulation to limb Immobilisation Pain control Sterile dressing to open wounds Antibiotics Tetanus
8 Bleeding control by compression rather than tourniquet If no pulse correct limb deformity by traction Immobilise joint above and below Pain relief using narcotics and/or nerve blocs
9 Mortality rate 10-20% Mortality 38% if patient hypotensive and 50% if open fracture Neurologic damage 60% Associated injuries chest, abdominal, urological, spine etc Reduce pelvic volume via sheet wrap (applied level of trochanters)


10




11

12


13


14


15

16
17 ATLS = Advanced Trauma and Life Support Standardised protocol for the evaluation and treatment of victims of trauma Airway ( + cervical spine immobilisation) Breathing (+ high flow oxiygen) Circulation Disability Exposure
18 Rapid assessment of ABC s and adressing life threatening problems Large bore IV access for fluid replacement if haemodynamic instability Trauma Xrays: Chest Pelvis Lateral C spine
19 Other non life threatening injuries Orthopaedic assessment limbs, pelvis and spine Dress wounds Neurovascular assessment Splint fractures Obtain X-rays
20 AP and lateral X-rays showing joint above and below on 1 film No X-ray puzzles!! Beware of inadequate X-rays (cervical spine, shoulder, elbow, hip etc.) Repeat films if poor quality or not showing the entire bone
21 Open fracture versus closed fracture with overlying skin laceration? Bone visible in depth of wound Blood with fat globules oozing from wound Open joint injury Air in joint on radiographs Beware of pelvis fractures open into rectum/vagina

22
23 Soft tissue damage often more extensive than at first sight Wound coverage? Muscle/tendon injury Contamination Neurovascular injury Bone comminution/loss
24 Remove foreign material Reduce bacterial contamination by Irrigation Normal saline + antiseptic solution (Betadine) Large quantities up to 2 litres Apply sterile saline soaked dressing + compression bandage Immobilise Antibiotics and tetanus
25 Should cover Gram positive, negative and anaerobes in some situations Combination first generation cephalosporin (cefazolin) and aminoglycoside ( gentamycin, tobramycin) Substitutes for amynoglycoside: quinolones, 3 rd generation cephalosporin etc) Anaerobic cover for farm, vascular injuries etc: penicillin, ampicillin
26

27

28 cruciform ligament alar ligaments apical ligament

29 Cervical cord Nerve roots Vertebral artery

30 3 column concept

31 2 or 3 column injury

32 Spine potentially unstable if 2 or more columns are disrupted!

33 Flexion Compression Extension Rotation Combination Fall from height Direct blow to head Sports MVA
34 Roadside first aid principles apply ABCSL injured conscious - Neck pain? sensation/motor power limbs? if positive apply hard collar injured unconscious or decreased level of consciousness apply hard collar careful airway management safety position
35 Local hospital/gp surgery other acute injuries requiring transfer leave hard collar on and let them sort it out isolated injury you need to rule out neck injury
36 Medico legal! Cover yourself History and associated features MVA thrown out MBA helmet? Head/facial injury Sport Fall from height Intoxication/drugs etc
37 Electric shock type feeling Transient paraesthesiae/weakness shortly after injury Pain not always proportional to severity of injury Numbness/motor weakness limbs Able to stand up/hold head unsupported after injury
38 Clinical criteria to rule out serious injury ( NEXUS study NEJM 94: July 2000) no posterior midline tenderness no focal neurologic deficit normal level of consciousness no evidence of intoxication isolated injury
39 Remove cervical collar Look head position torticollis?c1c2 laceration face forehead?odontoid swelling back neck 3 column injury? Feel posterior midline tenderness Move active ROM Neuro exam
40 STANDARD VIEWS AP Lat Obliques left and right OTHER VIEWS Open Mouth (C1 C2) Swimmers (C7 T1) Flexion-Extension?
41 Interpretation of cervical spine Xrays is difficult Quality of acute films often poor Get help from Radiologist/orthopaedic surgeon Teleradiology useful

42 A=Anterior spinal line B=Posterior spinal line C=Spinolaminar curve
43 Displacement vertebral body Prevertebral swelling Shape vertebral body Kink posterior spinal line Increased interspinous distance Tear drop fractures Facet joints oblique views Spinous processes (use bright light) C1C2 AND C7T1

44
45 DIFFICULTIES! C1 C2 Unilateral facet dislocation C7 T1 CT SCAN MRI SCAN


46


47

48 # BODY FRAGMENT IN CANAL # LAMINA

49 SPINAL CORD
50 Flexion-extension views? Static Dynamic (under fluoroscopy) Safe in conscious patient Unconscious patient? Use fluoroscopy MRI safer option
51 Upper cervical C1 ant/post arch Jefferson lat mass blow out C2 dislocation C1 on C2 rupture transverse lig ( lat Xray distance peg ant arch C1 >5 mm) neural arch Hangmann s odontoid peg (type 1,2,3) C1C2 rotatory subluxation diagnosis difficult common in children

52

53

54
55 Mid and Lower cervical simple wedge compression # dislocations rotational # dislocations extension injuries burst # shear # Stable or unstable that s the question
56 Unilateral facet dislocation often associated with facet # 30% nerve root injury head tilted to the side of lesion x rays < 25% displacement spinous process deviated to the abnormal side Bilateral facet dislocation cord injury common xrays >50% displacement MRI prior to reduction disc disruption

57

58 National Pediatric Trauma Registry cases 1098 cervical spine injury 1.5% Mean age 11+/-5 years 61% boys 30% neurologic injury 50% no evidence of bony injury 24% complete 76% incomplete cord lesion Mortality upper 23% (atlanto axial dislocation) lower4%

59 Evaluation difficult numerous epiphyseal centres normal wedge shaped bodies pseudosubluxation due to horizontal angle of facet joints Get specialist advice
60 High dose IV methyl prednisolone in acute SCI remains controversial 1990 NASCIS study NEJM reported an increase in spinal cord recovery Findings and data interpretation has been questioned Recent systematic review does not support its use
61

62 Location: Leg Forearm Cause: Fracture Crush Reperfusion Closed muscle/tendon rupture

63
64 6 P s Pain Paraesthesia Puffiness Pallor Paralysis Pulselessness Pain with passive muscle stretch Limb tense wood like feeling Altered sensation Muscle weakness
65 High index of suspicion Presence of a distal pulse does not exclude compartment syndrome Compartment pressure measurements

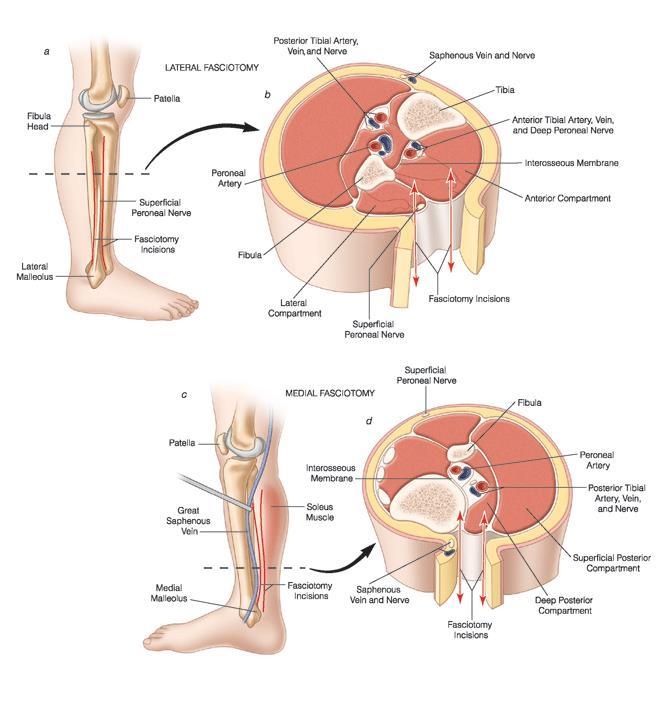
66 Split plaster, bandage down to skin Elevate limb to level of heart Urgent fasciotomies

67
68 Necrotising infections (gas gangrene, necrotising fasciitis) Spinal infections Septic arthritis Osteomyelitis Cellulitis
69 High mortality if delay in diagnosis and/or management Patient very unwell (high temperature, rigours etc) often with multiple co morbidities Very painful and swollen limb (sometimes skin breach in the area) No abscess formation Skin discolouration or necrosis ( late feature) Can lead to multi organ failure!
70 Bloods: High CRP, ESR WCC not always elevated Abnormal liver/renal function Myoglobinaemia/uria Cultures: Septicaemia in most cases Streptococcus pyogenes/beta haemolytic Clostridium if gas gangrene Invstigations: Xrays look for gas in the soft tissues Ultrasound to look for collection

71 .ed High index of suspicion required Differential diagnosis cellulitis Refer as soon as possible
72 Painful swollen joint in somebody feeling unwell Types: Haematogenous Direct seeding Surgery Artificial joint infection is a separate entity!!
73 Knee 50% Other joints: hip, shoulder, wrist, elbow, ankle (hip in new born and children beware!) Symptoms: acute pain, swelling, redness if joint superficial, movement painful in all directions, systemic symptoms with fever Bloods consistent with infection Aspirate to confirm diagnosis Common organism Staphylococcus aureus Differential diagnosis gout
74 Management: Joint wash out via arthrotomy Antibiotics Splinting Physiotherapy
75 Diagnosis difficult Often low grade infection Temperature often normal a painful joint replacement is infected until proven otherwise Diagnosis difficult in postoperative period Most commonly haematogenous infection
76 Diagnosis: Raised inflammatory markers X rays normal or loosening in chronic infections Joint aspiration ( easy for knee, image intensifier required for hip) Often few organisms difficult to grow (patient often been given antibiotics prior to aspiration!!) Organisms: staph aureus, strep, gram negative, staph epidermidis etc
77 Bacteria walled off from immune cells/antibiotics by glycocalix Removal of implant often required Antibiotics alone often not able to cure infection Prevention of infection following joint replacement surgery essential!!!

78 Acute OM in children rare except Polynesians Presents like septic arthritis High temperature Blood cultures positive in 50% Same organisms Xrays normal initially but will show bone destruction/periostal new bone formation after some weeks Ultrasound/MRI to confirm and localise High dose antibiotics and surgery if abscess formation Chronic osteomyelitis rare
79 Rare but serious Acute back pain and systemic symptoms (red flags) Diagnosis often delayed Types: Discitis Osteomyelitis Epidural abscess Serious infection with high morbidity Mortality in elderly and immuno compromised
80 Mainly haematogenous with positive blood cultures CT guided biopsy Organisms: staph aureus, gram neg etc (tuberculosis rare) Other concomitant sites of infection!! Refer early if red flags Treatment: High dose IV antibiotics Surgery if instability and neurological compromise
81 Acute compression cauda equina Large midline disc prolapse mainly Pain, numbness (including perianal), weakness (gait disturbance) both legs, urinary retention, absent reflexes Urgent referral for surgical decompression
82 Serious injury High velocity injury 3 out of 4 ligaments ruptured High incidence of popliteal artery and sciatic nerve injury (foot drop) injury Leg ischaemia if not recognised can lead to amputation Swollen knee+++ X rays often dislocation partially reduced Check circulation distal pulses (Doppler!) Refer urgently


83


84
85 Common If significant displacement risk of serious neuro vascular injury (brachial artery, median nerve) Extensive swelling elbow + deformity Ecchymosis above elbow crease 2 situations: No radial pulse white hand No radial pulse pink hand Check nerve function
86 Immobilise arm in extension Refer urgently particularly if no pulse and white hand!!! Can lead to compartment syndrome fore arm and muscle necrosis if treatment delayed Will require closed/open reduction + K wire fixation +/- vascular repair


87
88

89

90

91
92


93


94

95

96


97

98


99


100

101


102


103


104



105


106


107


108


109


110


111


112
Common fracture & dislocation of the cervical spine. Theerachai Apivatthakakul Department of Orthopaedic Chiangmai University
 Common fracture & dislocation of the cervical spine Theerachai Apivatthakakul Department of Orthopaedic Chiangmai University Objective Anatomy Mechanism and type of injury PE.and radiographic evaluation
Common fracture & dislocation of the cervical spine Theerachai Apivatthakakul Department of Orthopaedic Chiangmai University Objective Anatomy Mechanism and type of injury PE.and radiographic evaluation
SUBAXIAL CERVICAL SPINE TRAUMA- DIAGNOSIS AND MANAGEMENT
 SUBAXIAL CERVICAL SPINE TRAUMA- DIAGNOSIS AND MANAGEMENT 1 Anatomy 3 columns- Anterior, middle and Posterior Anterior- ALL, Anterior 2/3 rd body & disc. Middle- Posterior 1/3 rd of body & disc, PLL Posterior-
SUBAXIAL CERVICAL SPINE TRAUMA- DIAGNOSIS AND MANAGEMENT 1 Anatomy 3 columns- Anterior, middle and Posterior Anterior- ALL, Anterior 2/3 rd body & disc. Middle- Posterior 1/3 rd of body & disc, PLL Posterior-
Surgical Care at the District Hospital. EMERGENCY & ESSENTIAL SURGICAL CARE
 Surgical Care at the District Hospital 1 18 Orthopedic Trauma Key Points 2 18.1 Upper Extremity Injuries Clavicle Fractures Diagnose fractures from the history and by physical examination Treat with a
Surgical Care at the District Hospital 1 18 Orthopedic Trauma Key Points 2 18.1 Upper Extremity Injuries Clavicle Fractures Diagnose fractures from the history and by physical examination Treat with a
Spinal Cord Injuries: The Basics. Kadre Sneddon POS Rounds October 1, 2003
 Spinal Cord Injuries: The Basics Kadre Sneddon POS Rounds October 1, 2003 Anatomy Dorsal columntouch, vibration Corticospinal tract- UMN Anterior horn-lmn Spinothalamic tractpain, temperature (contralateral)
Spinal Cord Injuries: The Basics Kadre Sneddon POS Rounds October 1, 2003 Anatomy Dorsal columntouch, vibration Corticospinal tract- UMN Anterior horn-lmn Spinothalamic tractpain, temperature (contralateral)
Salisbury Foundation Trust Radiology Department Referral Guidelines for Primary Care: Musculoskeletal Imaging
 Salisbury Foundation Trust Radiology Department Referral Guidelines for Primary Care: Musculoskeletal Imaging These guidelines have been issued in conjunction with the Royal College of Radiology referral
Salisbury Foundation Trust Radiology Department Referral Guidelines for Primary Care: Musculoskeletal Imaging These guidelines have been issued in conjunction with the Royal College of Radiology referral
 International Trauma Life Support for Prehospital Care Providers Sixth Edition Patricia M. Hicks, MS, NREMTP Roy Alson, PhD, MD, FACEP Donna Hastings, EMT-P John Emory Campbell, MD, FACEP and Alabama Chapter,
International Trauma Life Support for Prehospital Care Providers Sixth Edition Patricia M. Hicks, MS, NREMTP Roy Alson, PhD, MD, FACEP Donna Hastings, EMT-P John Emory Campbell, MD, FACEP and Alabama Chapter,
Chapter 30 - Musculoskeletal_Trauma
 Introduction to Emergency Medical Care 1 OBJECTIVES 30.1 Define key terms introduced in this chapter. Slides 11 12, 19 20, 22 23, 37 30.2 Describe the anatomy of elements of the musculoskeletal system.
Introduction to Emergency Medical Care 1 OBJECTIVES 30.1 Define key terms introduced in this chapter. Slides 11 12, 19 20, 22 23, 37 30.2 Describe the anatomy of elements of the musculoskeletal system.
Surgery-Ortho. Fractures of the tibia and fibula. Management. Treatment of low energy fractures. Fifth stage. Lec-6 د.
 Fifth stage Lec-6 د. مثنى Surgery-Ortho 28/4/2016 Indirect force: (low energy) Fractures of the tibia and fibula Twisting: spiral fractures of both bones Angulatory: oblique fractures with butterfly segment.
Fifth stage Lec-6 د. مثنى Surgery-Ortho 28/4/2016 Indirect force: (low energy) Fractures of the tibia and fibula Twisting: spiral fractures of both bones Angulatory: oblique fractures with butterfly segment.
Imaging of Cervical Spine Trauma
 Imaging of Cervical Spine Trauma C Craig Blackmore, MD, MPH Professor of Radiology and Adjunct Professor of Health Services University of Washington, Harborview Medical Center Salary support: AHRQ grant
Imaging of Cervical Spine Trauma C Craig Blackmore, MD, MPH Professor of Radiology and Adjunct Professor of Health Services University of Washington, Harborview Medical Center Salary support: AHRQ grant
OBJECTIVES: Define basic assessments skills needed to identify orthopedic injuries. Differentiate when an orthopedic injury is a medical emergency
 1 2 How to Triage Orthopaedic Care David W. Gray, M.D. OBJECTIVES: Define basic assessments skills needed to identify orthopedic injuries Differentiate when an orthopedic injury is a medical emergency
1 2 How to Triage Orthopaedic Care David W. Gray, M.D. OBJECTIVES: Define basic assessments skills needed to identify orthopedic injuries Differentiate when an orthopedic injury is a medical emergency
1/3/2008. Karen Burke Priscilla LeMone Elaine Mohn-Brown. Medical-Surgical Nursing Care, 2e Karen Burke, Priscilla LeMone, and Elaine Mohn-Brown
 Medical-Surgical Nursing Care Second Edition Karen Burke Priscilla LeMone Elaine Mohn-Brown Chapter 42 Caring for Clients with Musculoskeletal Trauma Musculoskeletal Trauma Tissue is subjected to more
Medical-Surgical Nursing Care Second Edition Karen Burke Priscilla LeMone Elaine Mohn-Brown Chapter 42 Caring for Clients with Musculoskeletal Trauma Musculoskeletal Trauma Tissue is subjected to more
RED AND AMBER FLAG GUIDANCE ORTHOPAEDIC CONDITIONS
 RED AND AMBER FLAG GUIDANCE ORTHOPAEDIC CONDITIONS Distribution list: Clinical Commissioning Groups / All Worcestershire GP practices; Musculoskeletal Integrated Clinical and Assessment Services; Commissioning
RED AND AMBER FLAG GUIDANCE ORTHOPAEDIC CONDITIONS Distribution list: Clinical Commissioning Groups / All Worcestershire GP practices; Musculoskeletal Integrated Clinical and Assessment Services; Commissioning
Case. 5 year old with 2 weeks leg pain and now refusing to walk + Fevers, lower leg swelling, warmth Denies and history of trauma or wounds
 Case 5 year old with 2 weeks leg pain and now refusing to walk + Fevers, lower leg swelling, warmth Denies and history of trauma or wounds Exam I: Swelling over entire tibia extending to foot P: Tenderness
Case 5 year old with 2 weeks leg pain and now refusing to walk + Fevers, lower leg swelling, warmth Denies and history of trauma or wounds Exam I: Swelling over entire tibia extending to foot P: Tenderness
KNEE DISLOCATION. The most common injury will be an anterior dislocation, and this usually results from a hyperextension mechanism.
 KNEE DISLOCATION Introduction Dislocation of the knee is a severe injury associated with major soft tissue injury and a high incidence of damage to the popliteal artery. There is displacement of the tibia
KNEE DISLOCATION Introduction Dislocation of the knee is a severe injury associated with major soft tissue injury and a high incidence of damage to the popliteal artery. There is displacement of the tibia
Fractures of the shoulder girdle, elbow and fractures of the humerus. H. Sithebe 2012
 Fractures of the shoulder girdle, elbow and fractures of the humerus H. Sithebe 2012 Fractures of the Clavicle (mid-shaft). Fractures of the clavicle Fractures of the clavicle Treatment- conservative.
Fractures of the shoulder girdle, elbow and fractures of the humerus H. Sithebe 2012 Fractures of the Clavicle (mid-shaft). Fractures of the clavicle Fractures of the clavicle Treatment- conservative.
Disclosure. Pediatric Orthopedic Emergencies. I have no actual or potential conflict of interest in relation to this program or presentation.
 Pediatric Orthopedic Emergencies Robin Pearce MSN, RN-BC Trauma Performance Improvement Manager Henrico Doctors Hospital, Forest Disclosure I have no actual or potential conflict of interest in relation
Pediatric Orthopedic Emergencies Robin Pearce MSN, RN-BC Trauma Performance Improvement Manager Henrico Doctors Hospital, Forest Disclosure I have no actual or potential conflict of interest in relation
Cervical Spine Injury Guidelines
 6/15/2018 Cervical Spine Injury Guidelines Benjamin Oshlag, MD, CAQSM Assistant Professor of Emergency Medicine Assistant Professor of Sports Medicine Columbia University Medical Center Nothing to Disclose
6/15/2018 Cervical Spine Injury Guidelines Benjamin Oshlag, MD, CAQSM Assistant Professor of Emergency Medicine Assistant Professor of Sports Medicine Columbia University Medical Center Nothing to Disclose
Imaging of Cervical Spine Trauma Tudor H Hughes, M.D.
 Imaging of Cervical Spine Trauma Tudor H Hughes, M.D. General Considerations Most spinal fractures are due to a single episode of major trauma. Fatigue fractures of the spine are unusual except in the
Imaging of Cervical Spine Trauma Tudor H Hughes, M.D. General Considerations Most spinal fractures are due to a single episode of major trauma. Fatigue fractures of the spine are unusual except in the
Chapter 29 Orthopaedic Injuries Principles of Splinting Types of Muscles
 1 2 3 4 5 6 7 Chapter 29 Orthopaedic Injuries Principles of Splinting Types of Muscles Striated Skeletal Smooth Anatomy and Physiology of the Musculoskeletal System Skeletal System Skeletal System Functions
1 2 3 4 5 6 7 Chapter 29 Orthopaedic Injuries Principles of Splinting Types of Muscles Striated Skeletal Smooth Anatomy and Physiology of the Musculoskeletal System Skeletal System Skeletal System Functions
Fractures of the Thoracic and Lumbar Spine
 A spinal fracture is a serious injury. Nader M. Hebela, MD Fellow of the American Academy of Orthopaedic Surgeons http://orthodoc.aaos.org/hebela Cleveland Clinic Abu Dhabi Cleveland Clinic Abu Dhabi Neurological
A spinal fracture is a serious injury. Nader M. Hebela, MD Fellow of the American Academy of Orthopaedic Surgeons http://orthodoc.aaos.org/hebela Cleveland Clinic Abu Dhabi Cleveland Clinic Abu Dhabi Neurological
Subaxial Cervical Spine Trauma
 Subaxial Cervical Spine Trauma Pooria Salari, MD Assistant Professor Of Orthopaedics Department of Orthopaedic Surgery St. Louis University School of Medicine St. Louis, Missouri, USA Initial Evaluation
Subaxial Cervical Spine Trauma Pooria Salari, MD Assistant Professor Of Orthopaedics Department of Orthopaedic Surgery St. Louis University School of Medicine St. Louis, Missouri, USA Initial Evaluation
Outline. Epidemiology Indications for C-spine imaging Modalities Interpretation Types of fractures
 C-Spine Plain Films Outline Epidemiology Indications for C-spine imaging Modalities Interpretation Types of fractures Epidemiology 7000-10000 c-spine injuries treated each year Additional 5000 die at the
C-Spine Plain Films Outline Epidemiology Indications for C-spine imaging Modalities Interpretation Types of fractures Epidemiology 7000-10000 c-spine injuries treated each year Additional 5000 die at the
Introduction to Fractures and Dislocations. CAPA 2016 Winnipeg, MB
 Introduction to Fractures and Dislocations CAPA 2016 Winnipeg, MB CAPA 2016 Dr. Chris Graham Orthopedic surgeon Practice primarily trauma related Assist. Prof. U of M Health Sciences Centre No conflicts
Introduction to Fractures and Dislocations CAPA 2016 Winnipeg, MB CAPA 2016 Dr. Chris Graham Orthopedic surgeon Practice primarily trauma related Assist. Prof. U of M Health Sciences Centre No conflicts
1 Chapter 29 Orthopaedic Injuries Principles of Splinting 2 Types of Muscles. Striated Skeletal. Smooth
 1 Chapter 29 Orthopaedic Injuries Principles of Splinting 2 Types of Muscles Striated Skeletal Smooth 3 Anatomy and Physiology of the Musculoskeletal System 4 Skeletal System 5 Skeletal System Functions
1 Chapter 29 Orthopaedic Injuries Principles of Splinting 2 Types of Muscles Striated Skeletal Smooth 3 Anatomy and Physiology of the Musculoskeletal System 4 Skeletal System 5 Skeletal System Functions
Spinal Trauma. Dr T G Kruger
 Spinal Trauma Dr T G Kruger Epidemiology Spine injury in 6% of trauma patients Multiple levels involved in 20% of cases 80% of spinal cord injury patients have concurrent other system injuries 41% have
Spinal Trauma Dr T G Kruger Epidemiology Spine injury in 6% of trauma patients Multiple levels involved in 20% of cases 80% of spinal cord injury patients have concurrent other system injuries 41% have
Basic Care of Common Fractures Utku Kandemir, MD
 Basic Care of Common Fractures Utku Kandemir, MD Assistant Clinical Professor Trauma & Sports Medicine Dept. of Orthopaedic Surgery UCSF / SFGH History Physical Exam Radiology Treatment History Acute trauma
Basic Care of Common Fractures Utku Kandemir, MD Assistant Clinical Professor Trauma & Sports Medicine Dept. of Orthopaedic Surgery UCSF / SFGH History Physical Exam Radiology Treatment History Acute trauma
Index. Note: Page numbers of article titles are in boldface type.
 Note: Page numbers of article titles are in boldface type. A Abscess, epidural, 822 824 Achilles tendon rupture, 894 895, 981 982 Acromioclavicular separations, shoulder pain in, 751 753 Adhesive capsulitis,
Note: Page numbers of article titles are in boldface type. A Abscess, epidural, 822 824 Achilles tendon rupture, 894 895, 981 982 Acromioclavicular separations, shoulder pain in, 751 753 Adhesive capsulitis,
VAriation. Orthotics and Me (?surgeons) Greg Etherington Spine Surgeon. Orthopaedic & Neurosurgery backgrounds. Subspeciality training
 Greg Etherington Spine Surgeon. Orthopaedic & Neurosurgery backgrounds. Subspeciality training") Orthotics and Me (?surgeons) Greg Etherington Spine Surgeon Orthopaedic & Neurosurgery backgrounds Subspeciality training spine, upper limb, trauma, pelvis. What do you do in spine? Lumbar Cervical Trauma
Orthotics and Me (?surgeons) Greg Etherington Spine Surgeon Orthopaedic & Neurosurgery backgrounds Subspeciality training spine, upper limb, trauma, pelvis. What do you do in spine? Lumbar Cervical Trauma
Subaxial Cervical Spine Trauma Dr Hesarikia BUMS
 Subaxial Cervical Spine Trauma Dr. Hesarikia BUMS Subaxial Cervical Spine From C3-C7 ROM Majority of cervical flexion Lateral bending Approximately 50% rotation Ligamentous Anatomy Anterior ALL, PLL, intervertebral
Subaxial Cervical Spine Trauma Dr. Hesarikia BUMS Subaxial Cervical Spine From C3-C7 ROM Majority of cervical flexion Lateral bending Approximately 50% rotation Ligamentous Anatomy Anterior ALL, PLL, intervertebral
Primary Care Office Orthopedic Emergencies/ Urgencies
 Primary Care Office Orthopedic Emergencies/ Urgencies Joshua Crum M.D. Hill Country Sports Medicine San Marcos, TX Goals Define what constitutes and orthopedic emergency/urgency Know what conditions need
Primary Care Office Orthopedic Emergencies/ Urgencies Joshua Crum M.D. Hill Country Sports Medicine San Marcos, TX Goals Define what constitutes and orthopedic emergency/urgency Know what conditions need
Trauma & Orthopaedic Undergraduate Syllabus
 Trauma & Orthopaedic Undergraduate Syllabus Introduction The purpose of this document is to provide a recommended syllabus for medical students in Trauma & Orthopaedics (T&0). It should help students on
Trauma & Orthopaedic Undergraduate Syllabus Introduction The purpose of this document is to provide a recommended syllabus for medical students in Trauma & Orthopaedics (T&0). It should help students on
Musculoskeletal System
 CHAPTER 28 Musculoskeletal Injuries Musculoskeletal System Anatomy & Physiology Bones provide framework. Joints allow for bending. Muscles allow for movement. Cartilage provides flexibility. Tendons connect
CHAPTER 28 Musculoskeletal Injuries Musculoskeletal System Anatomy & Physiology Bones provide framework. Joints allow for bending. Muscles allow for movement. Cartilage provides flexibility. Tendons connect
CHAPTER 28 Musculoskeletal Injuries
 CHAPTER 28 Musculoskeletal Injuries Musculoskeletal System Anatomy & Physiology Bones provide framework. Joints allow for bending. Muscles allow for movement. Cartilage provides flexibility. Tendons connect
CHAPTER 28 Musculoskeletal Injuries Musculoskeletal System Anatomy & Physiology Bones provide framework. Joints allow for bending. Muscles allow for movement. Cartilage provides flexibility. Tendons connect
Trauma Films for Upper Body. LCDR. Naruebade Rungrattanawilai RTN M.D., LL.B. FRCOST, DMOC
 Trauma Films for Upper Body LCDR. Naruebade Rungrattanawilai RTN M.D., LL.B. FRCOST, DMOC Objective A 42 year-old housekeeper with history of motorcycle accident. There was no external wound but she have
Trauma Films for Upper Body LCDR. Naruebade Rungrattanawilai RTN M.D., LL.B. FRCOST, DMOC Objective A 42 year-old housekeeper with history of motorcycle accident. There was no external wound but she have
HIGH LEVEL - Science
 Learning Outcomes HIGH LEVEL - Science Describe the structure and function of the back and spine (8a) Outline the functional anatomy and physiology of the spinal cord and peripheral nerves (8a) Describe
Learning Outcomes HIGH LEVEL - Science Describe the structure and function of the back and spine (8a) Outline the functional anatomy and physiology of the spinal cord and peripheral nerves (8a) Describe
Subaxial Cervical Spine Trauma. Introduction. Anatomic Considerations 7/23/2018
 Subaxial Cervical Spine Trauma Sheyan J. Armaghani, MD Florida Orthopedic Institute Assistant Professor USF Dept of Orthopedics Introduction Trauma to the cervical spine accounts for 5 of all spine injuries
Subaxial Cervical Spine Trauma Sheyan J. Armaghani, MD Florida Orthopedic Institute Assistant Professor USF Dept of Orthopedics Introduction Trauma to the cervical spine accounts for 5 of all spine injuries
Assessment of limping child (beware the child who does not weight bear at all):
:") Department of Paediatrics Clinical Guideline Acutely Limping Child and Septic Arthritis Assessment of limping child (beware the child who does not weight bear at all): History Careful history of any significant
Department of Paediatrics Clinical Guideline Acutely Limping Child and Septic Arthritis Assessment of limping child (beware the child who does not weight bear at all): History Careful history of any significant
3/10/2014. Occurs in 70-80% of patients with blunt trauma. Rarely causes immediate threat to life or limb. Orthopedic Trauma. Musculoskeletal Trauma
 Orthopedic Trauma Douglas D. Presta, D.P.M., FACFAS, NREMT-P Spokane County EMS Musculoskeletal Trauma Introduction Primary Assessment Secondary Survey Musculoskeletal assessment Life threatening injuries
Orthopedic Trauma Douglas D. Presta, D.P.M., FACFAS, NREMT-P Spokane County EMS Musculoskeletal Trauma Introduction Primary Assessment Secondary Survey Musculoskeletal assessment Life threatening injuries
Primary care referral criteria for musculoskeletal MRI scans
 Appendix 1 Primary care referral criteria for musculoskeletal MRI scans Accepted Criteria for Direct Access MRI Body Part Symptoms Imaging indicated Lumbar Spine Low Back Pain with adverse symptoms or
Appendix 1 Primary care referral criteria for musculoskeletal MRI scans Accepted Criteria for Direct Access MRI Body Part Symptoms Imaging indicated Lumbar Spine Low Back Pain with adverse symptoms or
Aviation Rescue Swimmer Course
 Aviation Rescue Swimmer Course Primary Survey LT 5.4 December 2003 1 Objectives List the procedures used in a primary survey. Demonstrate primary survey procedures used in a mock trauma (moulage) scenario
Aviation Rescue Swimmer Course Primary Survey LT 5.4 December 2003 1 Objectives List the procedures used in a primary survey. Demonstrate primary survey procedures used in a mock trauma (moulage) scenario
Bone Injuries and Treatment. Fractures and Dislocations
 Bone Injuries and Treatment Fractures and Dislocations Bellwork Research the small bones in the foot and wrist. Draw them in your notes. State Standards 16) Understand principles of and successfully perform
Bone Injuries and Treatment Fractures and Dislocations Bellwork Research the small bones in the foot and wrist. Draw them in your notes. State Standards 16) Understand principles of and successfully perform
MUSCULOSKELETAL INJURIES
 WHAT ARE THEY They are injuries to muscles, nerves, tendons ligaments, joints, cartilage and spinal discs. WHAT KIND OF INJURIES ARE MUSCULOSKELETAL INJURIES 1. Fractures- -Open -Closed 2. Dislocations
WHAT ARE THEY They are injuries to muscles, nerves, tendons ligaments, joints, cartilage and spinal discs. WHAT KIND OF INJURIES ARE MUSCULOSKELETAL INJURIES 1. Fractures- -Open -Closed 2. Dislocations
Upper Cervical Spine - Occult Injury and Trigger for CT Exam
 Upper Cervical Spine - Occult Injury and Trigger for CT Exam Main Menu Introduction Clinical clearance of C-SpineC Radiographic evaluation Norms for C-spineC Triggers for CT exam: Odontoid Lateral view
Upper Cervical Spine - Occult Injury and Trigger for CT Exam Main Menu Introduction Clinical clearance of C-SpineC Radiographic evaluation Norms for C-spineC Triggers for CT exam: Odontoid Lateral view
Nursing Management: Musculoskeletal Trauma and Orthopedic Surgery. By: Aun Lauriz E. Macuja SAC_SN4
 Nursing Management: Musculoskeletal Trauma and Orthopedic Surgery By: Aun Lauriz E. Macuja SAC_SN4 The most common cause of musculoskeletal injuries is a traumatic event resulting in fracture, dislocation,
Nursing Management: Musculoskeletal Trauma and Orthopedic Surgery By: Aun Lauriz E. Macuja SAC_SN4 The most common cause of musculoskeletal injuries is a traumatic event resulting in fracture, dislocation,
REFERRAL GUIDELINES: ORTHOPAEDIC SURGERY
 All patients referred to specialist clinics are assigned to a priority category based on their clinical need and related psychosocial factors. The examples given are indicative only and the clinician reviewing
All patients referred to specialist clinics are assigned to a priority category based on their clinical need and related psychosocial factors. The examples given are indicative only and the clinician reviewing
Page 1 of 6. Appendix 1
 Page 1 Appendix 1 Rotation Objectives and Schedule 1. Introductory Month 4 weeks 2. Total Joints 4 weeks a. Diagnosis and management of hip and knee arthritis b. Indications for surgery c. Implant selection;
Page 1 Appendix 1 Rotation Objectives and Schedule 1. Introductory Month 4 weeks 2. Total Joints 4 weeks a. Diagnosis and management of hip and knee arthritis b. Indications for surgery c. Implant selection;
Knee Dislocation: Spectrum of Injury, Evolution of Treatment & Modern Outcomes
 Knee Dislocation: Spectrum of Injury, Evolution of Treatment & Modern Outcomes William M Weiss, MD MSc FRCSC Orthopedic Surgery & Rehabilitation Sports Medicine, Arthroscopy & Extremity Reconstruction
Knee Dislocation: Spectrum of Injury, Evolution of Treatment & Modern Outcomes William M Weiss, MD MSc FRCSC Orthopedic Surgery & Rehabilitation Sports Medicine, Arthroscopy & Extremity Reconstruction
Fractures and dislocations around elbow in adult
 Lec: 3 Fractures and dislocations around elbow in adult These include fractures of distal humerus, fracture of the capitulum, fracture of the radial head, fracture of the olecranon & dislocation of the
Lec: 3 Fractures and dislocations around elbow in adult These include fractures of distal humerus, fracture of the capitulum, fracture of the radial head, fracture of the olecranon & dislocation of the
A Patient s Guide to Diffuse Idiopathic Skeletal Hyperostosis (DISH)
") A Patient s Guide to Diffuse Idiopathic Skeletal Hyperostosis (DISH) 6565 Fannin Street Houston, TX 77030 Phone: 713-790-3333 DISCLAIMER: The information in this booklet is compiled from a variety of sources.
A Patient s Guide to Diffuse Idiopathic Skeletal Hyperostosis (DISH) 6565 Fannin Street Houston, TX 77030 Phone: 713-790-3333 DISCLAIMER: The information in this booklet is compiled from a variety of sources.
How to Triage Orthopaedic Care. David W. Gray, M.D.
 How to Triage Orthopaedic Care David W. Gray, M.D. OBJECTIVES: Define basic assessments skills needed to identify orthopedic injuries Differentiate when an orthopedic injury is a medical emergency Determine
How to Triage Orthopaedic Care David W. Gray, M.D. OBJECTIVES: Define basic assessments skills needed to identify orthopedic injuries Differentiate when an orthopedic injury is a medical emergency Determine
Common Elbow Problems
 Common Elbow Problems Duncan Ferguson FRACS Knee and Shoulder Specialist Elbow Instability Common 10-25% of elbow injuries Median age 30 yrs Most simple dislocations are stable after reduction recurrence
Common Elbow Problems Duncan Ferguson FRACS Knee and Shoulder Specialist Elbow Instability Common 10-25% of elbow injuries Median age 30 yrs Most simple dislocations are stable after reduction recurrence
 55-year-old male with 2nd and 3rd degree burns to face, chest, and arms on 25% of the body Respirations: 34 Pulse: 120 Mental Status: moans to painful stimulus Mucous membranes charred Stridor 10 cm scalp
55-year-old male with 2nd and 3rd degree burns to face, chest, and arms on 25% of the body Respirations: 34 Pulse: 120 Mental Status: moans to painful stimulus Mucous membranes charred Stridor 10 cm scalp
Cheyenne Kate P. Rebosura, MD Clinical Associate Orthopaedic Surgery KhooTeck PuatHospital
 Cheyenne Kate P. Rebosura, MD Clinical Associate Orthopaedic Surgery KhooTeck PuatHospital Outline I. Principles of Assessment II. Flexor Tenosynovitis III. Fight Bite IV. Animal Bite V. Compartment Syndrome
Cheyenne Kate P. Rebosura, MD Clinical Associate Orthopaedic Surgery KhooTeck PuatHospital Outline I. Principles of Assessment II. Flexor Tenosynovitis III. Fight Bite IV. Animal Bite V. Compartment Syndrome
Surgical Care at the District Hospital. EMERGENCY & ESSENTIAL SURGICAL CARE
 Surgical Care at the District Hospital 1 17 Orthopedic Techniques Key Points 2 17.1 Traction Use an appropriate method of traction to treat fractures of the extremities and cervical spine Apply extremity
Surgical Care at the District Hospital 1 17 Orthopedic Techniques Key Points 2 17.1 Traction Use an appropriate method of traction to treat fractures of the extremities and cervical spine Apply extremity
NOTE If it is necessary to perform abdominal thrusts, expose the abdominal area prior to pressing on the abdomen.
 ENABLING OBJECTIVES: 4.7 List the procedures used in a primary survey. 4.8 Demonstrate primary survey procedures used in a mock trauma (moulage) scenario without injury to personnel or damage to equipment.
ENABLING OBJECTIVES: 4.7 List the procedures used in a primary survey. 4.8 Demonstrate primary survey procedures used in a mock trauma (moulage) scenario without injury to personnel or damage to equipment.
Imaging of Trauma to the Spine. Orthopedic Diplomate Program University of Bridgeport College of Chiropractic
 Imaging of Trauma to the Spine Orthopedic Diplomate Program University of Bridgeport College of Chiropractic Jefferson Fracture Yee, LL: The Jefferson Fracture, Radiology Cases in Pediatric Emergency Medicine.
Imaging of Trauma to the Spine Orthopedic Diplomate Program University of Bridgeport College of Chiropractic Jefferson Fracture Yee, LL: The Jefferson Fracture, Radiology Cases in Pediatric Emergency Medicine.
SCIWORA Rozlyn McTeer BSN, RN, CEN Pediatric Trauma Coordinator Trauma Services OBJECTIVES DEFINITION 11/8/2017. Identify SCIWORA.
 SCIWORA Rozlyn McTeer BSN, RN, CEN Pediatric Trauma Coordinator Trauma Services Identify SCIWORA. OBJECTIVES Identify the population at risk. To identify anatomic and physiologic reasons for SCIWORA. To
SCIWORA Rozlyn McTeer BSN, RN, CEN Pediatric Trauma Coordinator Trauma Services Identify SCIWORA. OBJECTIVES Identify the population at risk. To identify anatomic and physiologic reasons for SCIWORA. To
Treatment of Acute Traumatic Knee Dislocations
 Treatment of Acute Traumatic Knee Dislocations Angelo J. Colosimo, MD Head Orthopaedic Surgeon University of Cincinnati Athletics Director of Sports Medicine University of Cincinnati Medical Center Associate
Treatment of Acute Traumatic Knee Dislocations Angelo J. Colosimo, MD Head Orthopaedic Surgeon University of Cincinnati Athletics Director of Sports Medicine University of Cincinnati Medical Center Associate
Diagnostic Imaging Exams
 Guide for Chiropractors Diagnostic Imaging Exams CREATED FOR OUR CHIROPRACTIC PARTNERS This document has been prepared by the specialized, board-certified radiologists who interpret patient exams for Center
Guide for Chiropractors Diagnostic Imaging Exams CREATED FOR OUR CHIROPRACTIC PARTNERS This document has been prepared by the specialized, board-certified radiologists who interpret patient exams for Center
OUTLINE SHEET 5.4 PRIMARY SURVEY
 ENABLING OBJECTIVES: 4.7 List the procedures used in a primary survey. 4.8 Demonstrate primary survey procedures used in a mock trauma (moulage) scenario without injury to personnel or damage to equipment.
ENABLING OBJECTIVES: 4.7 List the procedures used in a primary survey. 4.8 Demonstrate primary survey procedures used in a mock trauma (moulage) scenario without injury to personnel or damage to equipment.
Acute spinal cord injury
 Acute spinal cord injury Thakul Oearsakul Songklanagarind hospital Hat Yai Songkhla Introduction New SCI 10000-12000 cases Approximately 4.0-5.3 per 100000 population Common causes of traumatic SCI :Motor
Acute spinal cord injury Thakul Oearsakul Songklanagarind hospital Hat Yai Songkhla Introduction New SCI 10000-12000 cases Approximately 4.0-5.3 per 100000 population Common causes of traumatic SCI :Motor
OSTEOMYELITIS. If it occurs in adults, then the axial skeleton is the usual site.
 OSTEOMYELITIS Introduction Osteomyelitis is an acute or chronic inflammatory process of the bone and its structures secondary to infection with pyogenic organisms. Pathophysiology Osteomyelitis may be
OSTEOMYELITIS Introduction Osteomyelitis is an acute or chronic inflammatory process of the bone and its structures secondary to infection with pyogenic organisms. Pathophysiology Osteomyelitis may be
Dupuytrens contracture
 OA Wrist Ganglion/Cysts Dupuytrens contracture Carpal Tunnel Syndrome Carpal Tunnel pathway For advice on management of CTS please follow link to Map of Medicine Trigger Finger Trigger finger pathway For
OA Wrist Ganglion/Cysts Dupuytrens contracture Carpal Tunnel Syndrome Carpal Tunnel pathway For advice on management of CTS please follow link to Map of Medicine Trigger Finger Trigger finger pathway For
EVALUATE, TREAT AND WHEN TO REFER RED FLAGS Mid Atlantic Occupational Regional Conference and Environmental Medicine October 6, 2018
 EVALUATE, TREAT AND WHEN TO REFER RED FLAGS Mid Atlantic Occupational Regional Conference and Environmental Medicine October 6, 2018 Marc J. Levine, MD Rothman Institute Director Spine Surgery Program
EVALUATE, TREAT AND WHEN TO REFER RED FLAGS Mid Atlantic Occupational Regional Conference and Environmental Medicine October 6, 2018 Marc J. Levine, MD Rothman Institute Director Spine Surgery Program
Open Fractures. Ria Dindial. Photo courtesy pic2fly.com
 Open Fractures Ria Dindial Photo courtesy pic2fly.com CLINICAL PEARL TYPE WOUND DESCRIPTION OTHER CRITERIA I < 1cm (puncture wounds) - II 1-10 cm - IIIA >10 cm, coverage available Segmental fractures,
Open Fractures Ria Dindial Photo courtesy pic2fly.com CLINICAL PEARL TYPE WOUND DESCRIPTION OTHER CRITERIA I < 1cm (puncture wounds) - II 1-10 cm - IIIA >10 cm, coverage available Segmental fractures,
MANAGEMENT OF FRACTURE. Sudi maiteh (seminar 2 )
") MANAGEMENT OF FRACTURE Sudi maiteh (seminar 2 ) Management of fracture Subjects : _ general management of fractures & Orthopedic patient evaluation _ Closed and open fractures management (Conservative,
MANAGEMENT OF FRACTURE Sudi maiteh (seminar 2 ) Management of fracture Subjects : _ general management of fractures & Orthopedic patient evaluation _ Closed and open fractures management (Conservative,
The Spine.
 The Spine www.fisiokinesiterapia.biz Characteristics of Vertebrae Cervical Spine 1 and 2 Sacrum and Coccyx Curves Lordotic in the Spine Kyphotic Lordotic Ligamentous Support Muscles of the Spine Spinal
The Spine www.fisiokinesiterapia.biz Characteristics of Vertebrae Cervical Spine 1 and 2 Sacrum and Coccyx Curves Lordotic in the Spine Kyphotic Lordotic Ligamentous Support Muscles of the Spine Spinal
Post test for O&P 2 Hrs CE. The Exam
 Post test for O&P 2 Hrs CE The Exam This examination is taken in "open book" format. That means you are free to answer the questions after research or discussion with your fellow workers. We feel this
Post test for O&P 2 Hrs CE The Exam This examination is taken in "open book" format. That means you are free to answer the questions after research or discussion with your fellow workers. We feel this
Activity Three: Where s the Bleeding?
 Activity Three: Where s the Bleeding? There are five main sites of potentially fatal bleeding in trauma, remembered by the phrase on the floor and four more. On the floor refers to losing blood externally
Activity Three: Where s the Bleeding? There are five main sites of potentially fatal bleeding in trauma, remembered by the phrase on the floor and four more. On the floor refers to losing blood externally
The Positive Findings In Neck Injuries. American Journal of Orthopedics. August-September, 1964, pp
 The Positive Findings In Neck Injuries 1 American Journal of Orthopedics August-September, 1964, pp. 178-187 Ruth Jackson, MD This author analyzed 5,000 patients with disorders and found the following:
The Positive Findings In Neck Injuries 1 American Journal of Orthopedics August-September, 1964, pp. 178-187 Ruth Jackson, MD This author analyzed 5,000 patients with disorders and found the following:
Fractures of the thoracic and lumbar spine and thoracolumbar transition
 Most spinal column injuries occur in the thoracolumbar transition, the area between the lower thoracic spine and the upper lumbar spine; over half of all vertebral fractures involve the 12 th thoracic
Most spinal column injuries occur in the thoracolumbar transition, the area between the lower thoracic spine and the upper lumbar spine; over half of all vertebral fractures involve the 12 th thoracic
Involvement of the spine is common in rheumatoid. Incidence been reported to be 85% radiologically but only 30% have neurological signs and symptoms.
 RHEUMATOID SPINE Involvement of the spine is common in rheumatoid. Incidence been reported to be 85% radiologically but only 30% have neurological signs and symptoms. When neurology is present it may manifest
RHEUMATOID SPINE Involvement of the spine is common in rheumatoid. Incidence been reported to be 85% radiologically but only 30% have neurological signs and symptoms. When neurology is present it may manifest
SMF PCP Treatment & Referral Guideline Orthopedics Developed February 1, 2003 Revised: October, 2011
 SUTTER MEDICAL FOUNDATION (SMF) 2800 L Street, 7 th Floor Sacramento, CA 95816 SMF PCP Treatment & Referral Guideline Orthopedics Developed February 1, 2003 Revised: October, 2011 I. Shoulder Pain...Page
SUTTER MEDICAL FOUNDATION (SMF) 2800 L Street, 7 th Floor Sacramento, CA 95816 SMF PCP Treatment & Referral Guideline Orthopedics Developed February 1, 2003 Revised: October, 2011 I. Shoulder Pain...Page
Indications for cervical spine immobilisation: -
 Paediatric Trauma Cervical Spine Guidelines UHW Traumatic injuries of the cervical spine (C-spine) are uncommon in children. However, it is safer assume there is a cervical spine injury until examination
Paediatric Trauma Cervical Spine Guidelines UHW Traumatic injuries of the cervical spine (C-spine) are uncommon in children. However, it is safer assume there is a cervical spine injury until examination
Musculoskeletal Injuries
 Chapter 3 Musculoskeletal Injuries This chapter describes how to recognize and treat injuries to the musculoskeletal system, and the best methods for preventing problems of this nature: Recognize signs
Chapter 3 Musculoskeletal Injuries This chapter describes how to recognize and treat injuries to the musculoskeletal system, and the best methods for preventing problems of this nature: Recognize signs
Spine Trauma- Part B
 Spine Trauma- Part B Cervical Spine Injuries Atlanto- Occipital Dislocation Hyperextension and distraction mechanism Down s syndrome, RA more susceptible Asymmetric lateral masses on odontoid view Widened
Spine Trauma- Part B Cervical Spine Injuries Atlanto- Occipital Dislocation Hyperextension and distraction mechanism Down s syndrome, RA more susceptible Asymmetric lateral masses on odontoid view Widened
Objectives. Comprehension of the common spine disorder
 Objectives Comprehension of the common spine disorder Disc degeneration/hernia Spinal stenosis Common spinal deformity (Spondylolisthesis, Scoliosis) Osteoporotic fracture Destructive spinal lesions Anatomy
Objectives Comprehension of the common spine disorder Disc degeneration/hernia Spinal stenosis Common spinal deformity (Spondylolisthesis, Scoliosis) Osteoporotic fracture Destructive spinal lesions Anatomy
Musculoskeletal System Objectives:
 Lemone and Burke Chapters 40-41 Musculoskeletal System Objectives: Review Anatomy and physiology Describe normal MS assessment Describe age related changes Discuss tests and nursing interventions Recognize
Lemone and Burke Chapters 40-41 Musculoskeletal System Objectives: Review Anatomy and physiology Describe normal MS assessment Describe age related changes Discuss tests and nursing interventions Recognize
Lumbar Disc Prolapse. Dr. Ahmed Salah Eldin Hassan. Professor of Neurosurgery & Consultant spinal surgeon
 Lumbar Disc Prolapse By Dr. Ahmed Salah Eldin Hassan Professor of Neurosurgery & Consultant spinal surgeon 1-What are the Functions of the Spine Structural support for upright posture Protection of Spinal
Lumbar Disc Prolapse By Dr. Ahmed Salah Eldin Hassan Professor of Neurosurgery & Consultant spinal surgeon 1-What are the Functions of the Spine Structural support for upright posture Protection of Spinal
This presentation is the intellectual property of the author. Contact them for permission to reprint and/or distribute.
 Introduction Compartment Syndromes of the Leg Related to Athletic Activity Mark M. Casillas, M.D. Consequences of a misdiagnosis persistence of a performance limitation loss of function/compartment loss
Introduction Compartment Syndromes of the Leg Related to Athletic Activity Mark M. Casillas, M.D. Consequences of a misdiagnosis persistence of a performance limitation loss of function/compartment loss
Orthopedics - Dr. Ahmad - Lecture 2 - Injuries of the Upper Limb
 The shoulder and the upper arm Fractures of the clavicle 1. Fall on the shoulder. 2. Fall on outstretched hand. In mid shaft fractures, the outer fragment is pulled down by the weight of the arm and the
The shoulder and the upper arm Fractures of the clavicle 1. Fall on the shoulder. 2. Fall on outstretched hand. In mid shaft fractures, the outer fragment is pulled down by the weight of the arm and the
Title Protocol for the Management of Shoulder Injuries in MIUs and WICs
 Document Control Title in MIUs and WICs Author Author s job title Professional Lead, Minor Injuries Unit Directorate, Logistics and Resilience Department Emergency Department Version Date Issued Status
Document Control Title in MIUs and WICs Author Author s job title Professional Lead, Minor Injuries Unit Directorate, Logistics and Resilience Department Emergency Department Version Date Issued Status
102 Results RESULTS. Age Mean=S.D Range 42= years -84 years Number % <30 years years >50 years
 102 Results RESULTS A total of 50 cases were studied 39 males and 11females.Their age ranged between 16 years and 84 years (mean 42years). T1 and T2WI were acquired for all cases in sagittal and axial
102 Results RESULTS A total of 50 cases were studied 39 males and 11females.Their age ranged between 16 years and 84 years (mean 42years). T1 and T2WI were acquired for all cases in sagittal and axial
ACDF. Anterior Cervical Discectomy and Fusion. An introduction to
 An introduction to ACDF Anterior Cervical Discectomy and Fusion This booklet provides general information on ACDF. It is not meant to replace any personal conversations that you might wish to have with
An introduction to ACDF Anterior Cervical Discectomy and Fusion This booklet provides general information on ACDF. It is not meant to replace any personal conversations that you might wish to have with
Review date: February Lumbar Discectomy
 Review date: February 2019 Lumbar Discectomy Following your recent MRI scan and consultation with your spinal surgeon, you have been diagnosed as having a lumbar disc protrusion, resulting in nerve root
Review date: February 2019 Lumbar Discectomy Following your recent MRI scan and consultation with your spinal surgeon, you have been diagnosed as having a lumbar disc protrusion, resulting in nerve root
Thorasic and lumbar spinal injury. Dr.Abrisham
 Thorasic and lumbar spinal injury Dr.Abrisham Goal : alignment Stability Preserve neuologic function early mobilization Incidence: most site is thoraco lumbar 50% T 11 to L 1 30% L 2 to L 5 Motor vehicle
Thorasic and lumbar spinal injury Dr.Abrisham Goal : alignment Stability Preserve neuologic function early mobilization Incidence: most site is thoraco lumbar 50% T 11 to L 1 30% L 2 to L 5 Motor vehicle
Paediatric fractures in the Emergency Department. October 2012
 Paediatric fractures in the Emergency Department October 2012 Victorian Paediatric Orthopaedic Network What this presentation covers Paediatric bone anatomy Buckle injury of distal radius Supracondylar
Paediatric fractures in the Emergency Department October 2012 Victorian Paediatric Orthopaedic Network What this presentation covers Paediatric bone anatomy Buckle injury of distal radius Supracondylar
Posterior Lumbar Decompression for Spinal Stenosis
 Posterior Lumbar Decompression for Spinal Stenosis Issue 6: March 2016 Review date: February 2019 Following your recent MRI scan and consultation with your spinal surgeon you have been diagnosed with
Posterior Lumbar Decompression for Spinal Stenosis Issue 6: March 2016 Review date: February 2019 Following your recent MRI scan and consultation with your spinal surgeon you have been diagnosed with
Cervical Spine in Baseball
 Cervical Spine in Baseball Robert G Watkins, IV, MD Co-Director, Marina Spine Center Marina del Rey, CA Vice Chief of Staff Cedars-Marina del Rey Hospital Disclosures n Pioneer / RTI Consulting, Royalties
Cervical Spine in Baseball Robert G Watkins, IV, MD Co-Director, Marina Spine Center Marina del Rey, CA Vice Chief of Staff Cedars-Marina del Rey Hospital Disclosures n Pioneer / RTI Consulting, Royalties
Injuries to Muscles, Bones and Joints. Emergency Medical Response
 Injuries to Muscles, Bones and Joints Lesson 33: Injuries to Muscles, Bones and Joints You Are the Emergency Medical Responder You are patrolling the state park where you are the emergency medical responder
Injuries to Muscles, Bones and Joints Lesson 33: Injuries to Muscles, Bones and Joints You Are the Emergency Medical Responder You are patrolling the state park where you are the emergency medical responder
11. Spinal cord injury
 11. Spinal cord injury Introduction Always think spinal (vertebral) and/or spinal cord injury (SCI) in children with trauma. Remember SCIWORA cord injury may be present without abnormalities on routine
11. Spinal cord injury Introduction Always think spinal (vertebral) and/or spinal cord injury (SCI) in children with trauma. Remember SCIWORA cord injury may be present without abnormalities on routine
Peggers Super Summaries: The Aging Spine
 Aging Spine: AGING PROCESS Osteopenia 10% of 50 year old males and 25% of 50 year females Disc dehydration Facet degeneration Soft tissue hypertrophy 2 0 deformity Leg pain worse than back pain from nerve
Aging Spine: AGING PROCESS Osteopenia 10% of 50 year old males and 25% of 50 year females Disc dehydration Facet degeneration Soft tissue hypertrophy 2 0 deformity Leg pain worse than back pain from nerve
Goals. Initial management skeletal trauma. Physical Exam ABC OF PRIMARY CARE MEDICINE FRACTURE MANAGEMENT 12/4/2010
 ABC OF PRIMARY CARE MEDICINE FRACTURE MANAGEMENT Brian Feeley, MD UCSF Sports Medicine and Shoulder Surgery Goals Discuss common fractures and initial management, treatment guidelines Let your patients
ABC OF PRIMARY CARE MEDICINE FRACTURE MANAGEMENT Brian Feeley, MD UCSF Sports Medicine and Shoulder Surgery Goals Discuss common fractures and initial management, treatment guidelines Let your patients
POSTERIOR CERVICAL FUSION
 AN INTRODUCTION TO PCF POSTERIOR CERVICAL FUSION This booklet provides general information on the Posterior Cervical Fusion (PCF) surgical procedure for you to discuss with your physician. It is not meant
AN INTRODUCTION TO PCF POSTERIOR CERVICAL FUSION This booklet provides general information on the Posterior Cervical Fusion (PCF) surgical procedure for you to discuss with your physician. It is not meant
Physical and Radiographic Examination of the Spine
 Physical and Radiographic Examination of the Spine Christopher M. Bono, MD Assistant Professor, Department of Orthopaedic Surgery Boston University School of Medicine, Boston Medical Center, Boston, MA
Physical and Radiographic Examination of the Spine Christopher M. Bono, MD Assistant Professor, Department of Orthopaedic Surgery Boston University School of Medicine, Boston Medical Center, Boston, MA
Complications of Treatment: Nonsurgical and Surgical
 Complications of Treatment: Nonsurgical and Surgical Whenever orthopedic surgeons discuss a treatment with patients we must always consider the risks and complications of any treatment we recommend. Part
Complications of Treatment: Nonsurgical and Surgical Whenever orthopedic surgeons discuss a treatment with patients we must always consider the risks and complications of any treatment we recommend. Part
Tibial Shaft Fractures
 Tibial Shaft Fractures Mr Krishna Vemulapalli Consultant Orthopaedics Surgeon Queens & King George Hospitals Queens Hospital 14/03/2018 Google Maps Map data 2018 Google 10 km Orthopaedics Department Covers
Tibial Shaft Fractures Mr Krishna Vemulapalli Consultant Orthopaedics Surgeon Queens & King George Hospitals Queens Hospital 14/03/2018 Google Maps Map data 2018 Google 10 km Orthopaedics Department Covers
1/19/2018. Winter injuries to the shoulder and elbow. Highgate Private Hospital (Whittington Health NHS Trust)
") Winter injuries to the shoulder and elbow Omar Haddo Consultant Orthopaedic Surgeon, Shoulder, Elbow, Hand & Wrist Specialist MBBS, BmedSci, FRCS(Orth) Highgate Private Hospital (Whittington Health NHS
Winter injuries to the shoulder and elbow Omar Haddo Consultant Orthopaedic Surgeon, Shoulder, Elbow, Hand & Wrist Specialist MBBS, BmedSci, FRCS(Orth) Highgate Private Hospital (Whittington Health NHS
CERVICAL SPINE EVALUATION MARK FIGUEROA PHYSICAL THERAPIST
 CERVICAL SPINE EVALUATION MARK FIGUEROA PHYSICAL THERAPIST OVERVIEW OF CLINICAL REASONING Stage of disorder Pathoanatomical diagnosis Signs and symptoms Consideration of the evidence gathered Common sense
CERVICAL SPINE EVALUATION MARK FIGUEROA PHYSICAL THERAPIST OVERVIEW OF CLINICAL REASONING Stage of disorder Pathoanatomical diagnosis Signs and symptoms Consideration of the evidence gathered Common sense
Surgical Complications
 Surgical Complications Complications are common even with ideal management. Recently, Bashyal performed a retrospective review of 622 patients treated for supracondylar fractures and evaluated the complications
Surgical Complications Complications are common even with ideal management. Recently, Bashyal performed a retrospective review of 622 patients treated for supracondylar fractures and evaluated the complications