Mining for Lost Memories: A Best Practice Approach for Alzheimer s Disease Diagnosis
|
|
|
- Daniela Roberts
- 6 years ago
- Views:
Transcription

1 Mining for Lost Memories: A Best Practice Approach for Alzheimer s Disease Diagnosis Michael Rosenbloom, MD and Terry Barclay, PhD HealthPartners Center for Dementia and Alzheimer s Care
2 Presentation Outline I. Diagnostic Challenges in Dementia II. Rational for Early Detection III. Practice Tips I. Typical and atypical dementia work-up IV. Sensitivity/Specificity of Popular Cognitive Screening Tools V. HealthPartners 6 th Vital Sign Project VI. Clinician Toolbox
3 Alzheimer s Diagnosis: Current Limitations Epidemiological Concerns Growing Epidemic Expected to Impact 13M Americans by 2050 and consume 40% of Healthcare Spending AD Diagnostic Limitations Diagnostic Accuracy 50% for AD Diagnosis Delayed by 6 Years Impairment of IADLs at Diagnosis

4 Beyond mountains, there are mountains. Haitian Proverb
5 Diagnostic Challenges Cultural Ageism and defining normal aging Fear of delivering bad news Associated stigma Implications for physician/patient relationship Medical Heterogeneous baseline Time No lab test Wrong diagnosis Treatment options/efficacy
6 Rational for Early Detection 1) Improve quality of life 2) Identify reversible causes 3) Maximize treatment response 4) Prevent diagnosis during crises 5) Identify strategies for medication adherence 6) Promote independence, lifestyle changes 7) Reduce cost of care by decreasing hospitalizations and ER visits
7 AD Diagnosis History Baseline premorbid cognitive state First symptom quality and onset Address memory, language, visuospatial, and executive function Evaluate AD risk factors Assess functional impairments Supplemental history from family/friend Neurological Exam Basic mental status Cranial nerve, motor, coordination, and gait testing to address pyramidal, extrapyramidal, or cerebellar tract findings
8 General Practice Tips Raise your expectation of the older patient Clinical interview Let patient answer questions without help Remember: Social skills remain intact Easy to be fooled by a sense of humor, irritability, reliance on old memories, or quiet/affable demeanor Subjective interviews FAIL to detect dementia in early stages
9 General Practice Tips Red flags Repetition (not normal in 7-10 min conversation) Tangential, circumstantial responses Losing track of conversation Frequently deferring to family Unexplained weight loss or failure to thrive Inattentive to appearance Unable to adapt to stressful circumstances (hospitalization)
10 General Practice Tips Family observations: ANY instances whatsoever of getting lost while driving, trouble following a recipe, asking same question repeatedly, mistakes paying bills Ask: Let s suppose your family member was alone on a domestic flight across the country and the trip required a layover with a gate change. Would he/she be able to manage that kind of mental task on his/her own?
11 Mental Status Exam Intact older adult should be able to: Describe 2 current events in some detail Describe what happened on 9/11, New Orleans disaster Name the current President and 2 immediate predecessors Describe medical history and names of some medications

12 AD Diagnosis Laboratory Studies CBC, BMP, LFTs, TSH, B12, Ca2+ Neuroimaging Brain MRI/CT
13 Dementia with Lewy Bodies Clinical Features Parkinsonism, hallucinations, cognitive fluctuations Neuropsychological Testing Predominant visuospatial dysfunction with relative sparing of verbal memory Neuroimaging Occipital hypometabolism on FDG-PET Non-specific MRI atrophy pattern
14 Frontotemporal Dementia Clinical Features Typical onset prior to age 65 Behavioral symptoms Disinhibition, apathy, loss of empathy, repetitive stereotyped movements, hyperorality Language symptoms Expressive aphasia, surface dyslexia Neuropsychological Testing Impairments on executive function/language with relative sparing of episodic memory and visuospatial function Neuroimaging Atrophy of frontal and anterior temporal cortex

15 Cognitive Screening
16 Objective Screening Measures Initial considerations Research findings re: early detection Balance b/w time and sensitivity/specificity How will your practice incorporate screening? Who will administer tests? MDs, Nurses, social workers, allied health professionals What happens once screen is positive?
17 Objective Screening Measures Wide range of options Mini-Cog Mini-Mental State Exam (MMSE) St. Louis University Mental Status Exam (SLUMS) Montreal Cognitive Assessment (MoCA) All but MMSE free online, in public domain AD Association Physician Toolkit
18 Objective Screening Measures Do NOT Allow patient to give up prematurely or skip questions Deviate from standardized instructions Offer multiple choice answers Bias score by coaching Be soft on scoring Score ranges already padded for normal errors Deduct points where necessary be strict
19 Mini-Cog Contents Verbal Recall (3 points) Clock Draw (2 points) Subject asked to recall 3 words Leader, Season, Table +3 Advantages Quick (2-3 min) Easy High yield (executive function, memory, visuospatial function) Subject asked to draw clock, set hands to 10 past 11 +2
20 Mini-Cog Pros Takes only 2-3 minutes to administer Clock drawing sensitive to both visuospatial & executive dysfunction Simple scoring and interpretation Cons Not considered as sensitive for MCI or early dementia when compared to longer screens Brevity means less information to interpret
21 Mini-Cog Performance unaffected by education or language Borson Int J Geriatr Psychiatry 2000 Sensitivity and Specificity similar to MMSE (76% vs. 79%; 89% vs. 88%) Borson JAGS 2003 Does not disrupt workflow & increases rate of diagnosis in primary care Borson JGIM 2007 Failure associated with inability to fill pillbox Anderson et al Am Soc Consult Pharmacists 2008
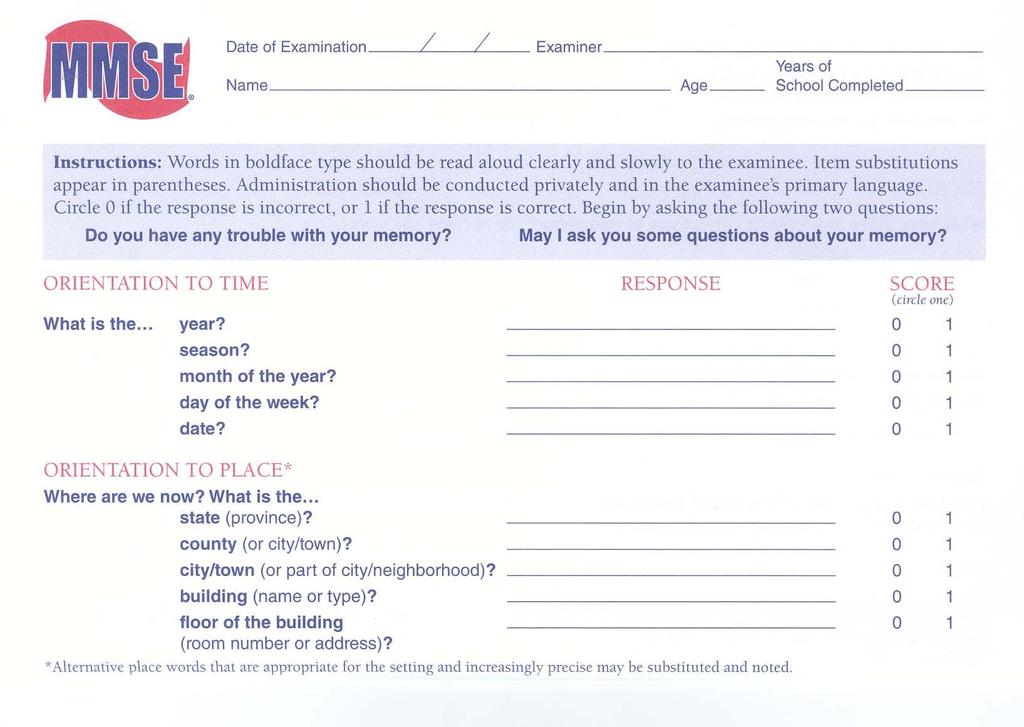
22 MMSE
23 MMSE Pros Widely accepted and validated tool for dementia screening 30-point scale well known and score is easily interpretable Measures orientation, working memory, recall, language, praxis Cons Scale developed 40 years ago, before MCI criteria and when early dementia less well understood Lacks sensitivity to MCI and early dementia Takes 7 min. to administer Copyright issues
24 SLUMS
25 SLUMS Pros More measures of executive functioning Good balance between easy and difficult items More sensitive than MMSE in detecting MCI and early dementia 30-point scale similar to MMSE Score range for MCI and dementia Free online Cons Takes 10 min. to administer Slightly more complex directions than MMSE Less name recognition than MMSE
26 MoCA
27 MoCA Pros Much more sensitive than MMSE in detecting MCI and early dementia More content tapping higher level executive functioning 30-point scale similar to MMSE Translations available in 35+ languages Free online Cons Takes min. to administer More complex administration and directions than MMSE
28 Screening Tool Selection Montreal Cognitive Assessment (MoCA) Sensitivity: 90% for MCI, 100% for dementia Specificity: 87% St. Louis University Mental Status (SLUMS) Sensitivity: 92% for MCI, 100% for dementia Specificity: 81% Mini-Mental Status Exam (MMSE) Sensitivity: 18% for MCI, 78% for dementia Specificity: 100% Larner et al Int Psychogeriatr 2012; Nasreddine et al J Am Geriatr Soc 2005; Tariq et al Am J Geriatr Psychiatry 2006; Ismail et al Int J Geriatr Psychiatry 2010
29 What about cognitive screening in patients without a history of cognitive disorder?
30 The 6 th Vital Sign Project HealthPartners Clinical Initiative to Address the Following: 1) Delays in AD diagnosis and growing geriatric population 2) Impaired management of chronic disease & medications in this population HTN Diabetes Hyperlipidemia Anticoagulation management

31 Lessons from Chronic Disease
32 MiniCog: Prior Studies Borson and colleagues administered MC to 524 patients 65 in primary care setting Screening did not disrupt clinic flow 18% screen failure rate (MC score<4) Only 17% of providers took appropriate action with screen fails» Borson et al. J. Gen. Intern. Med 2007 McCarten and colleagues administered MC to 8,342 patients aged 70 in VA setting Screen well-accepted by older veterans Testing completed between 1-3 minutes 25.8% failure rate among asymptomatic population» McCarten et al J Am Geriatr Soc

33 6 th Vital Sign Project: Clinical Setting HealthPartners Medical Group 640 physician multispecialty care delivery organization Health plan includes 750,000 members Tertiary care hospital serving an inner city population
34 6 th Vital Sign Project: Methods Rooming nurse staff Identifies patients aged 70 without history of MCI or dementia in chart review Administers MC to patients Alert provider for screen failures Physician provider Assesses patient for cognitive impairment Decides upon further diagnostic evaluation and/or referral
35
36 6 th Vital Sign Project: Preliminary Data Demographics Total Screened (246) Mean Age (78.5 yrs) %Male/Female (42.1%/57.9%) Results #Passes (151) #Fails (95) %Failures (38.6%)
37 6 th Vital Sign Project: Future Directions Clinical Goals Expand to ophthalmology in March 2012 Expand to a primary care clinic in April 2012 Research Goals Investigate screen feasibility and failure rate Retrospectively compare chronic disease management between screen passes and fails Prospectively compare markers of chronic disease management pre- and post-mc screen among screen failures
38 6 th Vital Sign Project: Research Plan Development of Screening Process Pilot Test Screen in Specialty Care Clinic >70 yr Pilot Test Screen in Primary Care Clinic >70 yr Expand Screen to Primary Care Throughout Primary Care Analysis 1. Measure prevalence of Mini-Cog screen fails and subsequent diagnosis of dementia 2. Measure feasibility of Mini-Cog as a screen in clinical care and acceptance of screen by nurses, providers, and leaders in each clinic 3. Identify impact of undiagnosed cognitive impairment on management of chronic disease and cost of care in each patient population by comparing 1 yr retrospective data from patients passing versus failing the screen 4. Identify potential benefits of screening on clinical outcomes and cost of care in each patient population by comparing 1 yr retrospective with 1 yr prospective data in screen fails
39 6 th Vital Sign Project: Limitations and Concerns Is the MC the Appropriate Screen? Does the MC favorably impact clinical care? What does one do with an abnormal MC screening test? How does one build the infrastructure to effectively handle patients failing the MC?
40 Clinician Toolbox Cognitive Impairment Detection Algorithm
41
42 Clinician Toolbox Standard Memory Loss Work-Up
43 Dementia Work-Up Provider Checklist Follow these diagnostic guidelines in response to patient failure on cognitive screening (e.g., Mini-cog) or other signs of possible cognitive impairment. History and Physical Review onset, course, and nature of memory and cognitive deficits (Alzheimer s Association Family Questionnaire may assist) and any associated behavioral, medical or psychosocial issues Assess ADLs and IADLs, including driving and possible medication and financial mismanagement Conduct structured mental status exam (e.g., MoCA, SLUMS, MMSE) 1 Assess mental health (consider depression, anxiety, chemical dependency) Perform neurological exam focusing on focal/lateralizing signs, vision, including visual fields and extraocular movements, hearing, speech, gait, coordination, and evidence of involuntary or impaired movements Diagnostics 1. Routine lab tests CBC, lytes, BUN, Cr, Ca, LFTs, Glucose 2. Neuroimaging CT or MRI when clinically indicated Dementia screening labs: TSH, B12 Contingent labs (per patient history) RPR or MHA-TP, HIV, heavy metals 3. Neuropsychological testing Indicated in cases of early or mild symptom presentation, for differential diagnosis, determination of nature and severity of cognitive functioning, and/or development of appropriate treatment plan Typically maximally beneficial in the following score ranges: MoCA 19-27; SLUMS 18-27; MMSE Diagnosis Mild Cognitive Impairment Mild deficit in 1 cognitive function: memory, executive, visuospatial, language, attention Intact ADLs and IADLs; does not meet criteria for dementia Alzheimer s disease Most common type of dementia (60-80% of cases) Memory loss, confusion, disorientation, dysnomia, impaired judgment/behavior, apathy/depression Dementia with Lewy Bodies / Parkinson s dementia Second most common type of dementia (up to 30% of cases) Hallmark symptoms include visual hallucinations, parkinsonism, and fluctuations in cognition Frontotemporal dementia Third most common type of dementia primarily affecting individuals in their 50s and 60s EITHER marked changes in behavior/personality OR language variant (difficulty with speech production or loss of word meaning) Vascular dementia Relatively rare in pure form (6-10% of cases) Symptoms often overlap with those of AD; frequently there is relative sparing of recognition memory Family Meeting Include family care partners Review diagnosis and intervention checklist (attached) Refer to Alzheimer s Association ( or
44 Clinician Toolbox Intervention Checklist
45
 Karen Ashe Kathleen Zahs Kamakshi")
46 Acknowledgements N. Bud Grossman Center for Memory Research and Care (UMN) Karen Ashe Kathleen Zahs Kamakshi Lakshminarayan Melanie Kiihn Minneapolis VA GRECC J. Riley McCarten James Cleary Maurice Dyken


47 The Center for Dementia and Alzheimer s Care Questions?
Clinical Provider Practice Tool
 Clinical Provider Practice Tool Cognitive Impairment Identification Annual Exam Mini Screen Tools Mini-Cog or GPCOG AND Family Questionniare (if family available) Normal Follow up in 1 year IF Mini-Cog
Clinical Provider Practice Tool Cognitive Impairment Identification Annual Exam Mini Screen Tools Mini-Cog or GPCOG AND Family Questionniare (if family available) Normal Follow up in 1 year IF Mini-Cog
Overview. Case #1 4/20/2012. Neuropsychological assessment of older adults: what, when and why?
 Neuropsychological assessment of older adults: what, when and why? Benjamin Mast, Ph.D. Associate Professor & Vice Chair, Psychological & Brain Sciences Associate Clinical Professor, Family & Geriatric
Neuropsychological assessment of older adults: what, when and why? Benjamin Mast, Ph.D. Associate Professor & Vice Chair, Psychological & Brain Sciences Associate Clinical Professor, Family & Geriatric
Information Gathering Obtaining history is the most critical first step Patient-provided history may not be reliable Need info from relatives, friends
 ASSESSING COMPETENCE Michael A Hill MD UNC Psychiatry 2008 Information Gathering Obtaining history is the most critical first step Patient-provided history may not be reliable Need info from relatives,
ASSESSING COMPETENCE Michael A Hill MD UNC Psychiatry 2008 Information Gathering Obtaining history is the most critical first step Patient-provided history may not be reliable Need info from relatives,
NEUROPSYCHOMETRIC TESTS
 NEUROPSYCHOMETRIC TESTS CAMCOG It is the Cognitive section of Cambridge Examination for Mental Disorders of the Elderly (CAMDEX) The measure assesses orientation, language, memory, praxis, attention, abstract
NEUROPSYCHOMETRIC TESTS CAMCOG It is the Cognitive section of Cambridge Examination for Mental Disorders of the Elderly (CAMDEX) The measure assesses orientation, language, memory, praxis, attention, abstract
As a general cognitive screening tool or as part of an annual exam (Medicare Annual Wellness Visit).
.") EMR DECISION SUPPORT TOOLS FOR ALZHEIMER S AND RELATED DEMENTIAS 1. Screening Tool Criteria For When to Use: As a general cognitive screening tool or as part of an annual exam (Medicare Annual Wellness
EMR DECISION SUPPORT TOOLS FOR ALZHEIMER S AND RELATED DEMENTIAS 1. Screening Tool Criteria For When to Use: As a general cognitive screening tool or as part of an annual exam (Medicare Annual Wellness
A Fresh View of Cognitive Disorders in Older Adults: New Classification and Screening Strategies
 A Fresh View of Cognitive Disorders in Older Adults: New Classification and Screening Strategies Lynda Mackin, PhD, AGPCNP-BC, CNS University of California San Francisco School of Nursing 1 Alzheimer s
A Fresh View of Cognitive Disorders in Older Adults: New Classification and Screening Strategies Lynda Mackin, PhD, AGPCNP-BC, CNS University of California San Francisco School of Nursing 1 Alzheimer s
Cognitive Screening in Risk Assessment. Geoffrey Tremont, Ph.D. Rhode Island Hospital & Alpert Medical School of Brown University.
 Cognitive Screening in Risk Assessment Geoffrey Tremont, Ph.D. Rhode Island Hospital & Alpert Medical School of Brown University Outline of Talk Definition of Dementia and MCI Incidence and Prevalence
Cognitive Screening in Risk Assessment Geoffrey Tremont, Ph.D. Rhode Island Hospital & Alpert Medical School of Brown University Outline of Talk Definition of Dementia and MCI Incidence and Prevalence
Alzheimer s disease dementia: a neuropsychological approach
 Alzheimer s disease dementia: a neuropsychological approach Dr. Roberta Biundo, PhD Neuropsychology Coordinator at Parkinson s disease and movement disorders unit of San Camillo rehabilitation hospital
Alzheimer s disease dementia: a neuropsychological approach Dr. Roberta Biundo, PhD Neuropsychology Coordinator at Parkinson s disease and movement disorders unit of San Camillo rehabilitation hospital
Objectives. My Patient: The story 10/6/2017
 Objectives Our Grey Matter Matters: A Case in Point Vivien Brown MDCM, CCFP,FCFP, NCMP Assistant Professor, University of Toronto Vice President, Medical Affairs, Medisys Healthy Group Past President,
Objectives Our Grey Matter Matters: A Case in Point Vivien Brown MDCM, CCFP,FCFP, NCMP Assistant Professor, University of Toronto Vice President, Medical Affairs, Medisys Healthy Group Past President,
Cognitive Evaluation in Primary Care. Scott T. Larson, MD Clinical Assistant Professor University of Iowa
 Cognitive Evaluation in Primary Care Scott T. Larson, MD Clinical Assistant Professor University of Iowa scott-larson@uiowa.edu Objectives Understand the subtypes of dementia, and the DSM-5 categorization
Cognitive Evaluation in Primary Care Scott T. Larson, MD Clinical Assistant Professor University of Iowa scott-larson@uiowa.edu Objectives Understand the subtypes of dementia, and the DSM-5 categorization
P20.2. Characteristics of different types of dementia and challenges for the clinician
 P20.2. Characteristics of different types of dementia and challenges for the clinician, professor Danish Dementia Research Center Rigshospitalet, University of Copenhagen (Denmark) This project has received
P20.2. Characteristics of different types of dementia and challenges for the clinician, professor Danish Dementia Research Center Rigshospitalet, University of Copenhagen (Denmark) This project has received
Introduction to Dementia: Diagnosis & Evaluation. Created in March 2005 Duration: about 15 minutes
 Introduction to Dementia: Diagnosis & Evaluation Created in March 2005 Duration: about 15 minutes Axel Juan, MD The Geriatrics Institute axel.juan@med.va.gov 305-575-3388 Credits Principal medical contributor:
Introduction to Dementia: Diagnosis & Evaluation Created in March 2005 Duration: about 15 minutes Axel Juan, MD The Geriatrics Institute axel.juan@med.va.gov 305-575-3388 Credits Principal medical contributor:
Implementation of a Dementia Screening Tool (Poster)
") Lehigh Valley Health Network LVHN Scholarly Works Patient Care Services / Nursing Implementation of a Dementia Screening Tool (Poster) Amanda Fougere Lehigh Valley Health Network, Amanda_A.Fougere@lvhn.org
Lehigh Valley Health Network LVHN Scholarly Works Patient Care Services / Nursing Implementation of a Dementia Screening Tool (Poster) Amanda Fougere Lehigh Valley Health Network, Amanda_A.Fougere@lvhn.org
Identification of Cognitive Impairment in HIV patients. Belinda Vicioso MD FACP, AGSF Jose Garcia Professor of Medicine UTSW
 Identification of Cognitive Impairment in HIV patients Belinda Vicioso MD FACP, AGSF Jose Garcia Professor of Medicine UTSW New emphasis on cognition Why? Common in our patient population Often overlooked
Identification of Cognitive Impairment in HIV patients Belinda Vicioso MD FACP, AGSF Jose Garcia Professor of Medicine UTSW New emphasis on cognition Why? Common in our patient population Often overlooked
Getting Help for Patients with Dementia and their Caregivers. Erica Salamida Associate Director of Programs and Services Alzheimer s Association-NENY
 Getting Help for Patients with Dementia and their Caregivers Erica Salamida Associate Director of Programs and Services Alzheimer s Association-NENY In this session you will learn about: Symptoms of dementia,
Getting Help for Patients with Dementia and their Caregivers Erica Salamida Associate Director of Programs and Services Alzheimer s Association-NENY In this session you will learn about: Symptoms of dementia,
ALZHEIMER S DISEASE OVERVIEW. Jeffrey Cummings, MD, ScD Cleveland Clinic Lou Ruvo Center for Brain Health
 ALZHEIMER S DISEASE OVERVIEW Jeffrey Cummings, MD, ScD Cleveland Clinic Lou Ruvo Center for Brain Health Prevalence AD: DEMOGRAPHY AND CLINICAL FEATURES Risk and protective factors Clinical features and
ALZHEIMER S DISEASE OVERVIEW Jeffrey Cummings, MD, ScD Cleveland Clinic Lou Ruvo Center for Brain Health Prevalence AD: DEMOGRAPHY AND CLINICAL FEATURES Risk and protective factors Clinical features and
The Person: Dementia Basics
 The Person: Dementia Basics Objectives 1. Discuss how expected age related changes in the brain might affect an individual's cognition and functioning 2. Discuss how changes in the brain due to Alzheimer
The Person: Dementia Basics Objectives 1. Discuss how expected age related changes in the brain might affect an individual's cognition and functioning 2. Discuss how changes in the brain due to Alzheimer
AGED SPECIFIC ASSESSMENT TOOLS. Anna Ciotta Senior Clinical Neuropsychologist Peninsula Mental Health Services
 AGED SPECIFIC ASSESSMENT TOOLS Anna Ciotta Senior Clinical Neuropsychologist Peninsula Mental Health Services Issues in assessing the Elderly Association between biological, psychological, social and cultural
AGED SPECIFIC ASSESSMENT TOOLS Anna Ciotta Senior Clinical Neuropsychologist Peninsula Mental Health Services Issues in assessing the Elderly Association between biological, psychological, social and cultural
The Basics of Alzheimer s Disease
 2017 Memory Loss Conference The Basics of Alzheimer s Disease Tom Ala, MD Center for Alzheimer s Disease and Related Disorders Southern Illinois University School of Medicine Springfield, Illinois SIU
2017 Memory Loss Conference The Basics of Alzheimer s Disease Tom Ala, MD Center for Alzheimer s Disease and Related Disorders Southern Illinois University School of Medicine Springfield, Illinois SIU
EMR DECISION SUPPORT TOOLS FOR ALZHEIMER S AND RELATED DEMENTIAS
 EMR DECISION SUPPORT TOOLS FOR ALZHEIMER S AND RELATED DEMENTIAS The ACT on Alzheimer s Electronic Medical Record (EMR) Decision Support Tools provide an evidence-based template to assist clinicians in
EMR DECISION SUPPORT TOOLS FOR ALZHEIMER S AND RELATED DEMENTIAS The ACT on Alzheimer s Electronic Medical Record (EMR) Decision Support Tools provide an evidence-based template to assist clinicians in
WHAT IS DEMENTIA? An acquired syndrome of decline in memory and other cognitive functions sufficient to affect daily life in an alert patient
 DEMENTIA WHAT IS DEMENTIA? An acquired syndrome of decline in memory and other cognitive functions sufficient to affect daily life in an alert patient Progressive and disabling Not an inherent aspect of
DEMENTIA WHAT IS DEMENTIA? An acquired syndrome of decline in memory and other cognitive functions sufficient to affect daily life in an alert patient Progressive and disabling Not an inherent aspect of
Assessing and Managing the Patient with Cognitive Decline
 Assessing and Managing the Patient with Cognitive Decline Center of Excellence For Alzheimer s Disease for State of NY Capital Region Alzheimer s Center of Albany Medical Center Earl A. Zimmerman, MD Professor
Assessing and Managing the Patient with Cognitive Decline Center of Excellence For Alzheimer s Disease for State of NY Capital Region Alzheimer s Center of Albany Medical Center Earl A. Zimmerman, MD Professor
3/6/2019 DIAGNOSIS OF DEMENTIA IN THE OUTPATIENT SETTING FINANCIAL DISCLOSURES LEARNING OBJECTIVES
 DIAGNOSIS OF DEMENTIA IN THE OUTPATIENT SETTING MILTA LITTLE, DO, CMD DUKE UNIVERSITY SCHOOL OF MEDICINE FINANCIAL DISCLOSURES Dr. Little has no relevant financial disclosures to report Dr. Little will
DIAGNOSIS OF DEMENTIA IN THE OUTPATIENT SETTING MILTA LITTLE, DO, CMD DUKE UNIVERSITY SCHOOL OF MEDICINE FINANCIAL DISCLOSURES Dr. Little has no relevant financial disclosures to report Dr. Little will
FTD basics! Etienne de Villers-Sidani, MD!
 FTD basics! Etienne de Villers-Sidani, MD! Frontotemporal lobar degeneration (FTLD) comprises 3 clinical syndromes! Frontotemporal dementia (behavioral variant FTD)! Semantic dementia (temporal variant
FTD basics! Etienne de Villers-Sidani, MD! Frontotemporal lobar degeneration (FTLD) comprises 3 clinical syndromes! Frontotemporal dementia (behavioral variant FTD)! Semantic dementia (temporal variant
DEMENTIA, THE BRAIN AND HOW IT WORKS AND WHY YOU MATTER
 OVERCOMING THE CHALLENGES OF MANAGING CHRONIC DISEASES IN PERSONS WITH DEMENTIA DEMENTIA, THE BRAIN AND HOW IT WORKS AND WHY YOU MATTER LEARNING OBJECTIVES Be familiar with the diagnostic criteria for
OVERCOMING THE CHALLENGES OF MANAGING CHRONIC DISEASES IN PERSONS WITH DEMENTIA DEMENTIA, THE BRAIN AND HOW IT WORKS AND WHY YOU MATTER LEARNING OBJECTIVES Be familiar with the diagnostic criteria for
Common Forms of Dementia Handout Package
 Common Forms of Dementia Handout Package Common Forms of Dementia 1 Learning Objectives As a result of working through this module, you should be better able to: 1. Describe clinical features of 4 major
Common Forms of Dementia Handout Package Common Forms of Dementia 1 Learning Objectives As a result of working through this module, you should be better able to: 1. Describe clinical features of 4 major
Screening for Cognitive Impairment
 Screening for Cognitive Impairment Screening for Cognitive Impairment. Educational Consultant Pearson April 27, 2017 Presentation Title Arial Bold 7 pt 1 Agenda What is Cognitive Impairment? Implications
Screening for Cognitive Impairment Screening for Cognitive Impairment. Educational Consultant Pearson April 27, 2017 Presentation Title Arial Bold 7 pt 1 Agenda What is Cognitive Impairment? Implications
Cognitive Assessment 4/29/2015. Learning Objectives To be able to:
 Supporting the Desire to Age in Place: Important Considerations for the Aging Population AGENDA 8:45 9:00 AM Geriatric Principles Robert L. Kane, MD *9:00 9:55 AM Cognitive Assessments Ed Ratner, MD 10:00
Supporting the Desire to Age in Place: Important Considerations for the Aging Population AGENDA 8:45 9:00 AM Geriatric Principles Robert L. Kane, MD *9:00 9:55 AM Cognitive Assessments Ed Ratner, MD 10:00
SECTION 1: as each other, or as me. THE BRAIN AND DEMENTIA. C. Boden *
 I read all the available books by other [people with] Alzheimer s disease but they never had quite the same problems as each other, or as me. I t s not like other diseases, where there is a standard set
I read all the available books by other [people with] Alzheimer s disease but they never had quite the same problems as each other, or as me. I t s not like other diseases, where there is a standard set
Case Presentation. Cognition: changes with Normal Aging? Synonyms
 Case Presentation 78 yr old new patient presenting for new PCP after discharge from hospital stay Discharged 3 days ago Summary : admitted with new atrial fibrillation, with history of DM, CHF. In hospital,
Case Presentation 78 yr old new patient presenting for new PCP after discharge from hospital stay Discharged 3 days ago Summary : admitted with new atrial fibrillation, with history of DM, CHF. In hospital,
Dementia and Driving Checklist
 6 Dementia and Driving Checklist 1. Questions to Ask the Patient and Family Patient Have you noticed any change or decreased confidence in your driving skills Have you had any accidents (or minor fender
6 Dementia and Driving Checklist 1. Questions to Ask the Patient and Family Patient Have you noticed any change or decreased confidence in your driving skills Have you had any accidents (or minor fender
DEMENTIA? 45 Million. What is. WHAT IS DEMENTIA Dementia is a disturbance in a group of mental processes including: 70% Dementia is not a disease
 What is PRESENTS DEMENTIA? WHAT IS DEMENTIA Dementia is a disturbance in a group of mental processes including: Memory Reasoning Planning Learning Attention Language Perception Behavior AS OF 2013 There
What is PRESENTS DEMENTIA? WHAT IS DEMENTIA Dementia is a disturbance in a group of mental processes including: Memory Reasoning Planning Learning Attention Language Perception Behavior AS OF 2013 There
Sorting Out the Three D s:
 Sorting Out the Three D s: Delirium, Depression & Dementia Teepa Snow, Positive Approach, LLC to be reused only with permission. Dementia Delirium Depression What s What? What s What For Each D Onset Hx
Sorting Out the Three D s: Delirium, Depression & Dementia Teepa Snow, Positive Approach, LLC to be reused only with permission. Dementia Delirium Depression What s What? What s What For Each D Onset Hx
02/04/2015. The structure of the talk. Dementia as a motor disorder. Movement, cognition & behaviour. Example 1. Example 2
 The th Annual Memory Clinic Conference Dublin, Trinity College, 27 March 1 The structure of the talk Dementia as a motor disorder Thomas H. Bak Human Cognitive Neuroscience & Centre for Clinical Brain
The th Annual Memory Clinic Conference Dublin, Trinity College, 27 March 1 The structure of the talk Dementia as a motor disorder Thomas H. Bak Human Cognitive Neuroscience & Centre for Clinical Brain
The current state of healthcare for Normal Aging, Mild Cognitive Impairment, & Alzheimer s Disease
 The current state of healthcare for Normal Aging, g, Mild Cognitive Impairment, & Alzheimer s Disease William Rodman Shankle, MS MD FACP Director, Alzheimer s Program, Hoag Neurosciences Institute Neurologist,
The current state of healthcare for Normal Aging, g, Mild Cognitive Impairment, & Alzheimer s Disease William Rodman Shankle, MS MD FACP Director, Alzheimer s Program, Hoag Neurosciences Institute Neurologist,
What if it s not Alzheimer s? Update on Lewy body dementia and frontotemporal dementia
 What if it s not Alzheimer s? Update on Lewy body dementia and frontotemporal dementia Dementia: broad term for any acquired brain condition impairing mental function such that ADLs are impaired. Includes:
What if it s not Alzheimer s? Update on Lewy body dementia and frontotemporal dementia Dementia: broad term for any acquired brain condition impairing mental function such that ADLs are impaired. Includes:
Recognizing Signs and Symptoms of Alzheimer's Disease in Earlier Stages Can Lead to Diagnosis
 A joint publication of the Illinois Health Care Association and CE Solutions November 2015 Recognizing Signs and Symptoms of Alzheimer's Disease in Earlier Stages Can Lead to Diagnosis Early diagnosis
A joint publication of the Illinois Health Care Association and CE Solutions November 2015 Recognizing Signs and Symptoms of Alzheimer's Disease in Earlier Stages Can Lead to Diagnosis Early diagnosis
Recognizing Dementia can be Tricky
 Dementia Abstract Recognizing Dementia can be Tricky Dementia is characterized by multiple cognitive impairments that cause significant functional decline. Based on this brief definition, the initial expectation
Dementia Abstract Recognizing Dementia can be Tricky Dementia is characterized by multiple cognitive impairments that cause significant functional decline. Based on this brief definition, the initial expectation
GERIATRIC MENTAL HEALTH AND MEDICATION TREATMENT
 Psychiatry and Addictions Case Conference UW Medicine Psychiatry and Behavioral Sciences GERIATRIC MENTAL HEALTH AND MEDICATION TREATMENT RUTH KOHEN ASSOCIATE PROFESSOR UW DEPARTMENT OF PSYCHIATRY 5-4-2017
Psychiatry and Addictions Case Conference UW Medicine Psychiatry and Behavioral Sciences GERIATRIC MENTAL HEALTH AND MEDICATION TREATMENT RUTH KOHEN ASSOCIATE PROFESSOR UW DEPARTMENT OF PSYCHIATRY 5-4-2017
Aging: Tools for Assessment
 Aging: Tools for Assessment Eugenia L. Siegler, MD Mason Adams Professor of Geriatric Medicine Weill Cornell Medicine New York, New York San Antonio, Texas: August 21 to 23, 2017 Learning Objectives After
Aging: Tools for Assessment Eugenia L. Siegler, MD Mason Adams Professor of Geriatric Medicine Weill Cornell Medicine New York, New York San Antonio, Texas: August 21 to 23, 2017 Learning Objectives After
Dementia. Aetiology, pathophysiology and the role of neuropsychological testing. Dr Sheng Ling Low Geriatrician
 Dementia Aetiology, pathophysiology and the role of neuropsychological testing Dr Sheng Ling Low Geriatrician Topics to cover Why is dementia important What is dementia Differentiate between dementia,
Dementia Aetiology, pathophysiology and the role of neuropsychological testing Dr Sheng Ling Low Geriatrician Topics to cover Why is dementia important What is dementia Differentiate between dementia,
DEMENTIA Dementia is NOT a normal part of aging Symptoms of dementia can be caused by different diseases Some symptoms of dementia may include:
 DEMENTIA Dementia is NOT a normal part of aging Symptoms of dementia can be caused by different diseases Some symptoms of dementia may include: 1. Memory loss The individual may repeat questions or statements,
DEMENTIA Dementia is NOT a normal part of aging Symptoms of dementia can be caused by different diseases Some symptoms of dementia may include: 1. Memory loss The individual may repeat questions or statements,
Review Evaluation of Residuals of Traumatic Brain Injury (R-TBI) Disability Benefits Questionnaire * Internal VA or DoD Use Only*
 Disability Benefits Questionnaire * Internal VA or DoD Use Only*") Review Evaluation of Residuals of Traumatic Brain Injury (R-TBI) Disability Benefits Questionnaire * Internal VA or DoD Use Only* Name of patient/veteran: SSN: Your patient is applying to the U. S. Department
Review Evaluation of Residuals of Traumatic Brain Injury (R-TBI) Disability Benefits Questionnaire * Internal VA or DoD Use Only* Name of patient/veteran: SSN: Your patient is applying to the U. S. Department
Delirium in the hospitalized patient
 Delirium in the hospitalized patient Jennifer A. Tarin, M.D. Department of Hospital Medicine Geriatric Health Safety Chair Colorado Permanente Medical Group UCLA Reynolds Scholar Delirium Preventing delirium
Delirium in the hospitalized patient Jennifer A. Tarin, M.D. Department of Hospital Medicine Geriatric Health Safety Chair Colorado Permanente Medical Group UCLA Reynolds Scholar Delirium Preventing delirium
The ABCs of Dementia Diagnosis
 The ABCs of Dementia Diagnosis Dr. Robin Heinrichs, Ph.D., ABPP Board Certified Clinical Neuropsychologist Associate Professor, Psychiatry & Behavioral Sciences Director of Neuropsychology Training What
The ABCs of Dementia Diagnosis Dr. Robin Heinrichs, Ph.D., ABPP Board Certified Clinical Neuropsychologist Associate Professor, Psychiatry & Behavioral Sciences Director of Neuropsychology Training What
Diagnosis and Treatment of Alzhiemer s Disease
 Diagnosis and Treatment of Alzhiemer s Disease Roy Yaari, MD, MAS Director, Memory Disorders Clinic, Banner Alzheimer s Institute 602-839-6900 Outline Introduction Alzheimer s disease (AD)Guidelines -revised
Diagnosis and Treatment of Alzhiemer s Disease Roy Yaari, MD, MAS Director, Memory Disorders Clinic, Banner Alzheimer s Institute 602-839-6900 Outline Introduction Alzheimer s disease (AD)Guidelines -revised
(5) Severe Alzheimer s Disease (SEV):
 Severe Alzheimer s Disease (SEV):") CST MEAN : () Severe Alzheimer s Disease (SEV): The severe AD group shows extreme deficits in all cognitive domains. This group in our database did not show symptoms of anosognosia. Numerous difficulties
CST MEAN : () Severe Alzheimer s Disease (SEV): The severe AD group shows extreme deficits in all cognitive domains. This group in our database did not show symptoms of anosognosia. Numerous difficulties
Version 4 River Nation Finger
 Mini-Cog Instructions for Administration & Scoring ID: Date: Step 1: Three Word Registration Look directly at person and say, Please listen carefully. I am going to say three words that I want you to repeat
Mini-Cog Instructions for Administration & Scoring ID: Date: Step 1: Three Word Registration Look directly at person and say, Please listen carefully. I am going to say three words that I want you to repeat
What APS Workers Need to Know about Frontotemporal, Lewy Body and Vascular Dementias
 What APS Workers Need to Know about Frontotemporal, Lewy Body and Vascular Dementias Presenter: Kim Bailey, MS Gerontology, Program & Education Specialist, Alzheimer s Orange County 1 1 Facts About Our
What APS Workers Need to Know about Frontotemporal, Lewy Body and Vascular Dementias Presenter: Kim Bailey, MS Gerontology, Program & Education Specialist, Alzheimer s Orange County 1 1 Facts About Our
Dementia and Alzheimer s disease
 Since 1960 Medicine Korat โรงพยาบาลมหาราชนครราชส มา Dementia and Alzheimer s disease Concise Reviews PAWUT MEKAWICHAI MD DEPARTMENT of MEDICINE MAHARAT NAKHON RATCHASIMA HOSPITAL 1 Prevalence Increase
Since 1960 Medicine Korat โรงพยาบาลมหาราชนครราชส มา Dementia and Alzheimer s disease Concise Reviews PAWUT MEKAWICHAI MD DEPARTMENT of MEDICINE MAHARAT NAKHON RATCHASIMA HOSPITAL 1 Prevalence Increase
Evaluation and Treatment of Dementia
 Evaluation and Treatment of Dementia Jeffrey M. Burns, MD Edward H. Hashinger Professor of Neurology Co-Director, KU Alzheimer s Disease Center Director, Clinical and Translational Science Unit Disclosures
Evaluation and Treatment of Dementia Jeffrey M. Burns, MD Edward H. Hashinger Professor of Neurology Co-Director, KU Alzheimer s Disease Center Director, Clinical and Translational Science Unit Disclosures
Just Clear Them The Approach to Medical Clearance
 Just Clear Them The Approach to Medical Clearance Dr. Nalin Ahluwalia MD CCFP(EM) Associate Chief of Staff Emergency Physician Oakville Trafalgar Memorial Hospital My Disclosures None! Exemplary patient
Just Clear Them The Approach to Medical Clearance Dr. Nalin Ahluwalia MD CCFP(EM) Associate Chief of Staff Emergency Physician Oakville Trafalgar Memorial Hospital My Disclosures None! Exemplary patient
Significance A Busy Clinician's Guide to Seniors with Memory Loss
 Significance A Busy Clinician's Guide to Seniors with Memory Loss Victoria Braund MD FACP CMD Division of Geriatrics. NorthShore University HealthSystem Alzheimer's disease is the sixth leading cause of
Significance A Busy Clinician's Guide to Seniors with Memory Loss Victoria Braund MD FACP CMD Division of Geriatrics. NorthShore University HealthSystem Alzheimer's disease is the sixth leading cause of
Dr. W. Dalziel Professor, Geriatric Medicine Ottawa Hospital. November /20/ Safety: Falls/Cooking/Unsafe Behaviour. 2.
 How To Decide if an Elderly Person Can Stay at Home: The Interval of Need Concept Dr. W. Dalziel Professor, Geriatric Medicine Ottawa Hospital November 2013 3 Factors 1. Safety: Falls/Cooking/Unsafe Behaviour
How To Decide if an Elderly Person Can Stay at Home: The Interval of Need Concept Dr. W. Dalziel Professor, Geriatric Medicine Ottawa Hospital November 2013 3 Factors 1. Safety: Falls/Cooking/Unsafe Behaviour
Assessment Toolkits for Lewy Body Dementia
 Study : Assessment Toolkits for Lewy Body Dementia There are two toolkits, depending on whether the patient is presenting with a primary cognitive problem or with cognitive decline in the context of established
Study : Assessment Toolkits for Lewy Body Dementia There are two toolkits, depending on whether the patient is presenting with a primary cognitive problem or with cognitive decline in the context of established
DEMENTIA ANDREA BERG, MD
 DEMENTIA ANDREA BERG, MD What Is Dementia? Decline in memory, language, problem-solving and other cognitive skills that affects a persons ability to perform everyday activities Progressive and disabling
DEMENTIA ANDREA BERG, MD What Is Dementia? Decline in memory, language, problem-solving and other cognitive skills that affects a persons ability to perform everyday activities Progressive and disabling
DBQ Initial Evaluation of Residuals of Traumatic Brain Injury (I-TBI) Disability
 Disability") DBQ Initial Evaluation of Residuals of Traumatic Brain Injury (I-TBI) Disability Name of patient/veteran: SSN: SECTION I 1. Diagnosis Does the Veteran now have or has he/she ever had a traumatic brain
DBQ Initial Evaluation of Residuals of Traumatic Brain Injury (I-TBI) Disability Name of patient/veteran: SSN: SECTION I 1. Diagnosis Does the Veteran now have or has he/she ever had a traumatic brain
CHAPTER 5 NEUROPSYCHOLOGICAL PROFILE OF ALZHEIMER S DISEASE
 CHAPTER 5 NEUROPSYCHOLOGICAL PROFILE OF ALZHEIMER S DISEASE 5.1 GENERAL BACKGROUND Neuropsychological assessment plays a crucial role in the assessment of cognitive decline in older age. In India, there
CHAPTER 5 NEUROPSYCHOLOGICAL PROFILE OF ALZHEIMER S DISEASE 5.1 GENERAL BACKGROUND Neuropsychological assessment plays a crucial role in the assessment of cognitive decline in older age. In India, there
Dementia and Delirium: A Neurologist s Approach to Altered Mental Status. Case 1 4/7/11. Which of the following evaluations is your next step?
 Dementia and Delirium: A Neurologist s Approach to Altered Mental Status S. Andrew Josephson, MD Director, Neurohospitalist Program Medical Director, Inpatient Neurology University of California San Francisco
Dementia and Delirium: A Neurologist s Approach to Altered Mental Status S. Andrew Josephson, MD Director, Neurohospitalist Program Medical Director, Inpatient Neurology University of California San Francisco
Dementia and Fall Geriatric Interprofessional Training. Wael Hamade, MD, FAAFP
 Dementia and Fall Geriatric Interprofessional Training Wael Hamade, MD, FAAFP Prevalence of Dementia Age range 65-74 5% % affected 75-84 15-25% 85 and older 36-50% 5.4 Million American have AD Dementia
Dementia and Fall Geriatric Interprofessional Training Wael Hamade, MD, FAAFP Prevalence of Dementia Age range 65-74 5% % affected 75-84 15-25% 85 and older 36-50% 5.4 Million American have AD Dementia
Imaging of Alzheimer s Disease: State of the Art
 July 2015 Imaging of Alzheimer s Disease: State of the Art Neir Eshel, Harvard Medical School Year IV Outline Our patient Definition of dementia Alzheimer s disease Epidemiology Diagnosis Stages of progression
July 2015 Imaging of Alzheimer s Disease: State of the Art Neir Eshel, Harvard Medical School Year IV Outline Our patient Definition of dementia Alzheimer s disease Epidemiology Diagnosis Stages of progression
DISCLOSURES. Objectives. THE EPIDEMIC of 21 st Century. Clinical Assessment of Cognition: New & Emerging Tools for Diagnosing Dementia NONE TO REPORT
 Clinical Assessment of Cognition: New & Emerging Tools for Diagnosing Dementia DISCLOSURES NONE TO REPORT Freddi Segal Gidan, PA, PhD USC Keck School of Medicine Rancho/USC California Alzheimers Disease
Clinical Assessment of Cognition: New & Emerging Tools for Diagnosing Dementia DISCLOSURES NONE TO REPORT Freddi Segal Gidan, PA, PhD USC Keck School of Medicine Rancho/USC California Alzheimers Disease
DISCLAIMER: ECHO Nevada emphasizes patient privacy and asks participants to not share ANY Protected Health Information during ECHO clinics.
 DISCLAIMER: Video will be taken at this clinic and potentially used in Project ECHO promotional materials. By attending this clinic, you consent to have your photo taken and allow Project ECHO to use this
DISCLAIMER: Video will be taken at this clinic and potentially used in Project ECHO promotional materials. By attending this clinic, you consent to have your photo taken and allow Project ECHO to use this
UNDERSTANDING CAPACITY & DECISION-MAKING VIDEO TRANSCRIPT
 I m Paul Bourque, President and CEO of the Investment Funds Institute of Canada. IFIC is preparing materials to assist advisors and firms in managing effective and productive relationships with their aging
I m Paul Bourque, President and CEO of the Investment Funds Institute of Canada. IFIC is preparing materials to assist advisors and firms in managing effective and productive relationships with their aging
The Neuropsychology of
 The Neuropsychology of Stroke Tammy Kordes, Ph.D. Northshore Neurosciences Outline What is the Role of Neuropsychology Purpose of Neuropsychological Assessments Common Neuropsychological Disorders Assessment
The Neuropsychology of Stroke Tammy Kordes, Ph.D. Northshore Neurosciences Outline What is the Role of Neuropsychology Purpose of Neuropsychological Assessments Common Neuropsychological Disorders Assessment
Clinical Differences Among Four Common Dementia Syndromes. a program of Morningside Ministries
 Clinical Differences Among Four Common Dementia Syndromes a program of Morningside Ministries Introduction Four clinical dementia syndromes account for 90% of all cases after excluding reversible causes
Clinical Differences Among Four Common Dementia Syndromes a program of Morningside Ministries Introduction Four clinical dementia syndromes account for 90% of all cases after excluding reversible causes
I do not have any disclosures
 Alzheimer s Disease: Update on Research, Treatment & Care Clinicopathological Classifications of FTD and Related Disorders Keith A. Josephs, MST, MD, MS Associate Professor & Consultant of Neurology Mayo
Alzheimer s Disease: Update on Research, Treatment & Care Clinicopathological Classifications of FTD and Related Disorders Keith A. Josephs, MST, MD, MS Associate Professor & Consultant of Neurology Mayo
Dementia Facts and Resources Dementia Warning Signs Getting a Diagnosis Dementia Communication Tips Dementia Risk Reduction.
 Dementia Facts and Resources Dementia Warning Signs Getting a Diagnosis Dementia Communication Tips Dementia Risk Reduction Intermission Dementia Stages and Behaviors Caregiving and Self-Care Overview
Dementia Facts and Resources Dementia Warning Signs Getting a Diagnosis Dementia Communication Tips Dementia Risk Reduction Intermission Dementia Stages and Behaviors Caregiving and Self-Care Overview
Dementia Update. October 1, 2013 Dylan Wint, M.D. Cleveland Clinic Lou Ruvo Center for Brain Health Las Vegas, Nevada
 Dementia Update October 1, 2013 Dylan Wint, M.D. Cleveland Clinic Lou Ruvo Center for Brain Health Las Vegas, Nevada Outline New concepts in Alzheimer disease Biomarkers and in vivo diagnosis Future trends
Dementia Update October 1, 2013 Dylan Wint, M.D. Cleveland Clinic Lou Ruvo Center for Brain Health Las Vegas, Nevada Outline New concepts in Alzheimer disease Biomarkers and in vivo diagnosis Future trends
Evaluations. Alzheimer s Disease A Public Health Response. Viewer Call-In. July 19, Guest Speakers. Thanks to our Sponsors:
 Alzheimer s Disease A Public Health Response July 19, 2007 1 2 Guest Speakers Thanks to our Sponsors: Earl A. Zimmerman, M.D. Bender Endowed Chair of Neurology and Director of the Alzheimer s Center at
Alzheimer s Disease A Public Health Response July 19, 2007 1 2 Guest Speakers Thanks to our Sponsors: Earl A. Zimmerman, M.D. Bender Endowed Chair of Neurology and Director of the Alzheimer s Center at
Clinical Diagnosis. Step 1: Dementia or not? Diagnostic criteria for dementia (DSM-IV)
") Step 1: Dementia or not? Diagnostic criteria for dementia (DSM-IV) A. The development of multiple cognitive deficits manifested by both 1 and 2 1 1. Memory impairment 2. One (or more) of the following
Step 1: Dementia or not? Diagnostic criteria for dementia (DSM-IV) A. The development of multiple cognitive deficits manifested by both 1 and 2 1 1. Memory impairment 2. One (or more) of the following
A Neurologist s Approach to Altered Mental Status
 A Neurologist s Approach to Altered Mental Status S. Andrew Josephson, MD Department of Neurology University of California San Francisco October 23, 2008 The speaker has no disclosures Case 1 A 71 year-old
A Neurologist s Approach to Altered Mental Status S. Andrew Josephson, MD Department of Neurology University of California San Francisco October 23, 2008 The speaker has no disclosures Case 1 A 71 year-old
United Council for Neurologic Subspecialties Geriatric Neurology Written Examination Content Outline
 United Council for Neurologic Subspecialties Geriatric Neurology Written Examination Content Outline REV 3/24/09 The UCNS Geriatric Neurology examination was established to determine the level of competence
United Council for Neurologic Subspecialties Geriatric Neurology Written Examination Content Outline REV 3/24/09 The UCNS Geriatric Neurology examination was established to determine the level of competence
Understanding the Progression of Alzheimer s and Related Dementias And Planning for Future Changes
 Town Hall Forum Making a Plan: The Smart Approach to Alzheimer s Care Needs May 25, 2017 Understanding the Progression of Alzheimer s and Related Dementias And Planning for Future Changes Daniel D. Sewell,
Town Hall Forum Making a Plan: The Smart Approach to Alzheimer s Care Needs May 25, 2017 Understanding the Progression of Alzheimer s and Related Dementias And Planning for Future Changes Daniel D. Sewell,
Neuroimaging for dementia diagnosis. Guidance from the London Dementia Clinical Network
 Neuroimaging for dementia diagnosis Guidance from the London Dementia Clinical Network Authors Dr Stephen Orleans-Foli Consultant Psychiatrist, West London Mental Health NHS Trust Dr Jeremy Isaacs Consultant
Neuroimaging for dementia diagnosis Guidance from the London Dementia Clinical Network Authors Dr Stephen Orleans-Foli Consultant Psychiatrist, West London Mental Health NHS Trust Dr Jeremy Isaacs Consultant
FRONTOTEMPORAL DEGENERATION: OVERVIEW, TRENDS AND DEVELOPMENTS
 FRONTOTEMPORAL DEGENERATION: OVERVIEW, TRENDS AND DEVELOPMENTS Norman L. Foster, M.D. Director, Center for Alzheimer s Care, Imaging and Research Chief, Division of Cognitive Neurology, Department of Neurology
FRONTOTEMPORAL DEGENERATION: OVERVIEW, TRENDS AND DEVELOPMENTS Norman L. Foster, M.D. Director, Center for Alzheimer s Care, Imaging and Research Chief, Division of Cognitive Neurology, Department of Neurology
David A Scott Lis Evered. Department of Anaesthesia and Acute Pain Medicine St Vincent s Hospital, Melbourne University of Melbourne
 David A Scott Lis Evered Department of Anaesthesia and Acute Pain Medicine St Vincent s Hospital, Melbourne University of Melbourne This talk will include live polling so please be sure to have the meeting
David A Scott Lis Evered Department of Anaesthesia and Acute Pain Medicine St Vincent s Hospital, Melbourne University of Melbourne This talk will include live polling so please be sure to have the meeting
What is Occupational Therapy? Introduction to Occupational Therapy. World Federation of Occupational Therapists 2012
 World Federation of Occupational Therapists 2012 Introduction to Occupational Therapy Suki HUI Occupational Therapist I Statement on Occupational Therapy Occupational therapy is a client-centred health
World Federation of Occupational Therapists 2012 Introduction to Occupational Therapy Suki HUI Occupational Therapist I Statement on Occupational Therapy Occupational therapy is a client-centred health
Diagnosing & Dealing with Dementia
 Diagnosing & Dealing with Dementia Robert G. Arias, PhD. I have no financial disclosures or conflicts of interest to report. Robert G. Arias, PhD. 1 Today We Will Learn About: Diagnosing dementia Characteristics
Diagnosing & Dealing with Dementia Robert G. Arias, PhD. I have no financial disclosures or conflicts of interest to report. Robert G. Arias, PhD. 1 Today We Will Learn About: Diagnosing dementia Characteristics
2016 Programs & Information
 Mayo Alzheimer s Disease Research Clinic Education Center 2016 Programs & Information BROCHURE TITLE FLUSH RIGHT for Persons & Families impacted by Mild Cognitive Impairment Alzheimer s Disease Dementia
Mayo Alzheimer s Disease Research Clinic Education Center 2016 Programs & Information BROCHURE TITLE FLUSH RIGHT for Persons & Families impacted by Mild Cognitive Impairment Alzheimer s Disease Dementia
Prof Tim Anderson. Neurologist University of Otago Christchurch
 Prof Tim Anderson Neurologist University of Otago Christchurch Tim Anderson Christchurch Insidious cognitive loss From subjective memory complaints (SMC) to dementia Case 1. AR. 64 yrs Male GP referral
Prof Tim Anderson Neurologist University of Otago Christchurch Tim Anderson Christchurch Insidious cognitive loss From subjective memory complaints (SMC) to dementia Case 1. AR. 64 yrs Male GP referral
The prevalence of YOD increases almost exponentially with age (as does the prevalence of late onset dementia).
.") Factsheet 1 Young Onset Dementia (YOD) Dementia is commonly seen as a health and social problem of older adults. Nevertheless dementia can occur earlier in life. Young onset dementia is defined by an onset
Factsheet 1 Young Onset Dementia (YOD) Dementia is commonly seen as a health and social problem of older adults. Nevertheless dementia can occur earlier in life. Young onset dementia is defined by an onset
Palliative Approach to the Person with Advanced Dementia
 Mid North Coast Rural Palliative Care Project Link Nurse Education 2004 Palliative Approach to the Person with Advanced Dementia Anne Sneesby CNC - ACAT To care for the dying is a very human opportunity
Mid North Coast Rural Palliative Care Project Link Nurse Education 2004 Palliative Approach to the Person with Advanced Dementia Anne Sneesby CNC - ACAT To care for the dying is a very human opportunity
What is dementia? What is dementia?
 What is dementia? What is dementia? What is dementia? Dementia is an umbrella term for a range of progressive conditions that affect the brain. It has been identified that there are over 200 subtypes of
What is dementia? What is dementia? What is dementia? Dementia is an umbrella term for a range of progressive conditions that affect the brain. It has been identified that there are over 200 subtypes of
Note: These are abbreviated slides with graphics and other protected content removed for electronic posting purposes with NAPSA.
 Note: These are abbreviated slides with graphics and other protected content removed for electronic posting purposes with NAPSA. Please attend the presentation for the full slideshow and information. Attendees
Note: These are abbreviated slides with graphics and other protected content removed for electronic posting purposes with NAPSA. Please attend the presentation for the full slideshow and information. Attendees
Latest Methods to Early Detection for Alzheimer's: Cognitive Assessments and Diagnostic Tools in Practice
 Transcript Details This is a transcript of an educational program accessible on the ReachMD network. Details about the program and additional media formats for the program are accessible by visiting: https://reachmd.com/programs/alzheimers-disease-towards-earlier-detection/latest-methods-earlydetection-alzheimers-cognitive-assessments-and-diagnostic-tools-practice/8321/
Transcript Details This is a transcript of an educational program accessible on the ReachMD network. Details about the program and additional media formats for the program are accessible by visiting: https://reachmd.com/programs/alzheimers-disease-towards-earlier-detection/latest-methods-earlydetection-alzheimers-cognitive-assessments-and-diagnostic-tools-practice/8321/
Form D1: Clinician Diagnosis
 Initial Visit Packet Form D: Clinician Diagnosis NACC Uniform Data Set (UDS) ADC name: Subject ID: Form date: / / Visit #: Examiner s initials: INSTRUCTIONS: This form is to be completed by the clinician.
Initial Visit Packet Form D: Clinician Diagnosis NACC Uniform Data Set (UDS) ADC name: Subject ID: Form date: / / Visit #: Examiner s initials: INSTRUCTIONS: This form is to be completed by the clinician.
Visual Dysfunction in Alzheimer s Disease and Parkinson s Disease
 Visual Dysfunction in Alzheimer s Disease and Parkinson s Disease Victoria S. Pelak, MD Professor of Neurology and Ophthalmology Divisions of Neuro-ophthalmology and Behavioral Neurology University of
Visual Dysfunction in Alzheimer s Disease and Parkinson s Disease Victoria S. Pelak, MD Professor of Neurology and Ophthalmology Divisions of Neuro-ophthalmology and Behavioral Neurology University of
Driving and Dementia Practical Tips for the Family Physician. L. Lee, MD, MClSc, CCFP, FCFP 2014
 Driving and Dementia Practical Tips for the Family Physician L. Lee, MD, MClSc, CCFP, FCFP 2014 Medico-legal problems related to fitness to drive CMPA experience, 2005-2009: 67 medico-legal cases Half
Driving and Dementia Practical Tips for the Family Physician L. Lee, MD, MClSc, CCFP, FCFP 2014 Medico-legal problems related to fitness to drive CMPA experience, 2005-2009: 67 medico-legal cases Half
Dementia: It s Not Always Alzheimer s
 Dementia: It s Not Always Alzheimer s A Caregiver s Perspective Diane E. Vance, Ph.D. Mid-America Institute on Aging and Wellness 2017 My Background Caregiver for my husband who had Lewy Body Dementia
Dementia: It s Not Always Alzheimer s A Caregiver s Perspective Diane E. Vance, Ph.D. Mid-America Institute on Aging and Wellness 2017 My Background Caregiver for my husband who had Lewy Body Dementia
Understanding Dementia
 Understanding Dementia Dr. Dallas Seitz MD FRCPC Assistant Professor, Department of Psychiatry, Queen s University, Kingston, Ontario, Canada What s Next Information about Dementia, Elder Care and Supports
Understanding Dementia Dr. Dallas Seitz MD FRCPC Assistant Professor, Department of Psychiatry, Queen s University, Kingston, Ontario, Canada What s Next Information about Dementia, Elder Care and Supports
Delirium Pilot Project
 CCU Nurses: Delirium Pilot Project Our unit has been selected to develop and implement a delirium assessment and intervention program. We are beginning Phase 1 with education and assessing for our baseline
CCU Nurses: Delirium Pilot Project Our unit has been selected to develop and implement a delirium assessment and intervention program. We are beginning Phase 1 with education and assessing for our baseline
Paying for Dementia Care. Mary Ann Forciea MD Clinical Professor of Medicine Division of Geriatric Medicine University of Pennsylvania Health System
 Paying for Dementia Care Mary Ann Forciea MD Clinical Professor of Medicine Division of Geriatric Medicine University of Pennsylvania Health System Audience: Possible concerns about dementia care in my
Paying for Dementia Care Mary Ann Forciea MD Clinical Professor of Medicine Division of Geriatric Medicine University of Pennsylvania Health System Audience: Possible concerns about dementia care in my
Understanding Dementia &
 Understanding Dementia & Care Options for Those Suffering with the Disease Paige Landry BSN Hospice Care Consultant SouthernCare New Beacon Hospice Objectives Understand Dementia Understand Common Problems
Understanding Dementia & Care Options for Those Suffering with the Disease Paige Landry BSN Hospice Care Consultant SouthernCare New Beacon Hospice Objectives Understand Dementia Understand Common Problems
Memory Loss, Dementia and Alzheimer's Disease: The Basics
 Memory Loss, Dementia and Alzheimer's Disease: The Basics What is memory loss? What is age-related memory loss? Typical changes Typical age-related changes involve: Making a bad decision once in a while
Memory Loss, Dementia and Alzheimer's Disease: The Basics What is memory loss? What is age-related memory loss? Typical changes Typical age-related changes involve: Making a bad decision once in a while
What is dementia? What is dementia?
 What is dementia? What is dementia? What is dementia? Dementia is an umbrella term for a range of progressive conditions that affect the brain. There are over 200 subtypes of dementia, but the five most
What is dementia? What is dementia? What is dementia? Dementia is an umbrella term for a range of progressive conditions that affect the brain. There are over 200 subtypes of dementia, but the five most
Geri R Hall, PhD, GCNS, FAAN Advanced Practice Nurse Emeritus Banner Alzheimer s Institute
 Geri R Hall, PhD, GCNS, FAAN Advanced Practice Nurse Emeritus Banner Alzheimer s Institute Anosognosia Purpose: To introduce caregivers and health professionals to symptoms of lack of awareness and other
Geri R Hall, PhD, GCNS, FAAN Advanced Practice Nurse Emeritus Banner Alzheimer s Institute Anosognosia Purpose: To introduce caregivers and health professionals to symptoms of lack of awareness and other
Objectives. Prevalence of AD by age. Diagnosing and Managing Dementia in Ambulatory Practice
 Diagnosing and Managing Dementia in Ambulatory Practice 35 th Annual Nurse Practitioners of Oregon Education Conference Elizabeth Eckstrom, MD, MPH Oregon Health & Science University Objectives Review
Diagnosing and Managing Dementia in Ambulatory Practice 35 th Annual Nurse Practitioners of Oregon Education Conference Elizabeth Eckstrom, MD, MPH Oregon Health & Science University Objectives Review
DEMENTIA 101: WHAT IS HAPPENING IN THE BRAIN? Philip L. Rambo, PhD
 DEMENTIA 101: WHAT IS HAPPENING IN THE BRAIN? Philip L. Rambo, PhD OBJECTIVES Terminology/Dementia Basics Most Common Types Defining features Neuro-anatomical/pathological underpinnings Neuro-cognitive
DEMENTIA 101: WHAT IS HAPPENING IN THE BRAIN? Philip L. Rambo, PhD OBJECTIVES Terminology/Dementia Basics Most Common Types Defining features Neuro-anatomical/pathological underpinnings Neuro-cognitive
CTFPHC Working Group Members:
 Cognitive Impairment - Guideline Presentation Speaker deck OVERVIEW We will review the following: 1. Background on Cognitive Impairment 2. Methods of the CTFPHC 3. Recommendations and Key Findings 4. Implementation
Cognitive Impairment - Guideline Presentation Speaker deck OVERVIEW We will review the following: 1. Background on Cognitive Impairment 2. Methods of the CTFPHC 3. Recommendations and Key Findings 4. Implementation