ESCALATING PATIENT & CARER NEEDS TOWARDS END OF LIFE; OVERVIEW OF END OF LIFE CARE IN THE COMMUNITY Renal Supportive Care Nursing Elizabeth Josland
|
|
|
- Rosalind Ball
- 5 years ago
- Views:
Transcription


1 ESCALATING PATIENT & CARER NEEDS TOWARDS END OF LIFE; OVERVIEW OF END OF LIFE CARE IN THE COMMUNITY Renal Supportive Care Nursing Elizabeth Josland CNC
2 Objectives Dialysis vs non-dialysis end of life picture Survival Causes of death Issues encountered community needs Case End of life
3 The Renal Supportive Care Client Dialysis Symptom Support Average age: 72 years When does end of life occur? Sentinel event Deterioration over time (age related or comorbidity related) QOL decision Prognosis on ceasing dialysis: days to months dependant on urine output and health Non-Dialysis Average age: 84 years When does end of life occur? Sentinel event Gradual deterioration (age, renal, other comorbidity) Prognosis if not for dialysis: Median survival was 16 months (CJASN 2015) No statistical significant survival if >75yrs with 2 or more comorbidities (one being IHD) for dialysis/nfd (CJASN 2015)
4 Why palliative care so early? Supportive/palliative care is appropriate for all chronic life limiting illnesses such as heart failure, respiratory failure, liver failure Early introduction to the team to avoid (some) anxiety at end of life Prevent avoidable admissions (fluid overload, SOB, carer acopia, pain crisis) Crisis planning (pre-empting what crisis may happen and plan for it with the carer or patient) End of life planning (ACPs, knowing place they prefer, knowing who the carer is and their capability, start conversations with GP) It takes time to develop a trusting relationship with clients
.")
5 Survival Median survival 16months mean age 82 SURVIVAL IN PATIENTS WHO REMAINED IN THE PRE-DIALYSIS CLINIC WITHOUT RECEIVING DIALYSIS (N=181) COMPARED WITH ALL THOSE RECEIVING DIALYSIS (N=164) AND PATIENTS IN THE RSC-Not for dialysis GROUP (N=122). (Arbitrarily defined as >70 years) Time zero is from first attendance at the Pre-dialysis or Renal Supportive Care clinic after a decision had been made to pursue dialysis or not. For the all dialysis group this time point includes the time at first dialysis for the 72 patients who had not attended the Pre-dialysis clinic.

6 Causes of death

7 Undecided Treatment Pathway
8 Cardio-renal picture




9 Cancer picture

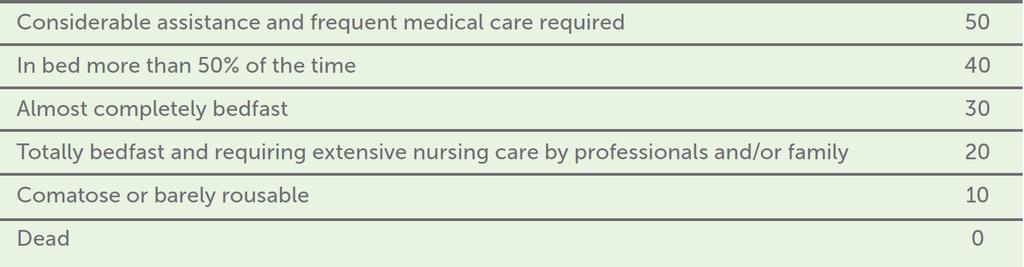
10 Functional Decline Australian-modified Karnofsky Performance Scale (AKPS)
11 Decline near end of life Functional decline in last 3 months before death We see the escalation of family stress Struggle to cope in last 2 months Potential for admissions due to carer stress and health issues and higher requirement for community resources
12 Common issues / fears Aging issues Increasing frailty Mobility issues, continence issues The ageing carer Transport issues, loss of independence, loss of health Financial stress Housing stress (i.e. stairs, public housing) Waiting time for services Inadequate services Cost of continence aids
13 Common issues / fears Health Issues Carer stress (work, financial, own health, other responsibilities) Wish to stay at home for as long as possible Wish to avoid nursing home Fears around discharge planning (can t stay in hospital, don t want NH, too unsafe for home, family friction around going home, rehabilitation issues (no clear goals, more palliative than intensive.) Managing medications (Webster pack) Increasing dementia issues
14 Common issues / fears Nearing End of Life Discussion on where the preferred place is (is it appropriate, crisis planning, discharge planning ) Time based bed pressure in hospital Criteria around hospice Conflict about what can be done and expectations Want to stay in hospital Want 24 nursing care at home Home vs hospital vs hospice Prognosis (dialysis vs non-dialysis)
15 Important notes There is no crisis palliative service for new patients in the community hence early involvement by us Can t call us when everything has fallen apart and expect someone to home visit that day even that week! Can t make first assessment on the phone Renal failure itself has few symptoms hence death can occur quickly at the end with no time for home death (organising takes time), and hospitalisation is likely Renal patients with low comorbidities on a conservative path rarely meet palliative criteria until they are dying Respite at Hospice admission unlikely not for aged care needs only, must have a complex symptom burden or be dying
16 The Carer Vitally important in all considerations for care Who they are and depth and breadth of role Sometimes they are caring for more than one person Are they the decision maker for medical care if the patient is not able to make decisions? How often are they at the home? Forward planning for when things become more difficult What are their wishes for future care, end of life care etc Allied health involvement early Dietitian to teach how to cheat with food restrictions Social worker for social/psychosocial assistance Respite care
17 Pre-crisis planning What do you expect the issues could be? SOB? Fluid overload? Pain? Profound weakness cannot perform ADLs What is something the family can do at home before things get frantic? How to manage SOB early Daily weigh and a Lasix plan How to use prn medicine and when to call for help Equipment early
18 Pre-crisis planning Encourage family to call early don t wait until they are already at breaking point Remind that there is a waiting time for community services early referral cannot be underestimated for its value Know the goals of care Comfort? Dialysis until the end? NFR? Don t make promises you can t keep i.e keeping out of nursing home
19 Community needs Social worker help with getting services Such as..myagedcare (MAC) When is community palliative care involved? Dependant on complexity of symptoms or prognosis Know your areas referral criteria and build a rapport with the team If only aged care needs, need to follow path of MAC referrals and may need nursing home.
20 Community resources GP Nursing Quick response program Continence Geriatric Flying Squad (nursing homes) Mental Health Palliative You need to know what is available in your area, referral criteria and guidelines, waiting times, how to escalate (if you can escalate), what they do.
21 Case Mr A has a history of severe heart failure and haemodialysis is now impossible due to hypotension and can only be carried out with inotrope support, but he is not for ICU and is unlikely to recover. A family meeting is held Mr A has been aware for a long time now that this time may come, his family are also very understanding. They are upset, but ask a lot of relevant questions.
22 Case Family have a choice for preferred place of death Hospital (time likely short but how short?) Home (need to be willing and able, have a home visiting GP that has known him approx 6 months, have equipment and CPCT in place before discharge) Hospice Nursing home What do we need to know as staff? Prognosis (important for planning place of death if likely to be prolonged) What is and is not possible (patient must be safe and cared for) NFR does everyone know what is happening?
23 Case Home: Equipment (OT) Community palliative care (send home with end of life medicine pack, GP aware and willing to visit and sign death certificate) may require community medication chart Home O 2 if required Authorised Adult Ambulance Care Plan Hospice Book bed with family permission once you know prognosis (may not be appropriate) Daily review until transfer or change plan to stay in hospital if deteriorates to unconsciousness before bed available
24 Case Hospital Continue palliative pathway explain everything to family / staff Leave after hours contact in case of distress Nursing home If from an aged care facility is a return appropriate? (prognosis is weeks/months) for permanent residents, hospice is not appropriate here. Send pack of medicines back with the patient and a palliative approach letter
25 Basic End of life medicines Hydromorphone (2mg/mL ampoule) mg SC Q2-4hrly PRN for SOB/pain (if already on regular pain relief change to subcut equivalent dose and make sure there is a breakthrough order also) Haloperidol (5mg / 1 ml) 0.5-1mg tds SC PRN for nausea/delirium Midazolam (5mg / 1 ml) 2.5-5mg SC Q2-4 hrly PRN for terminal agitation Glycopyrrolate (0.2mg/1 ml ampoule) mcg Q1-2hrly SC PRN for terminal secretions (can increase if very wet and gurgly to mcg) Lorazepam S/L (sublingual) 0.5mg tds PRN for anxiety Clonazepam drops (2.5mg / 1 ml) mg S/L (sublingual) bd prn for myoclonic jerks Sodibic mouthwash 1% po 10ml QID regular Aquaspray po 1 QID regular
26 End of life medicines if has Parkinsons or restless leg syndrome Hydromorphone (2mg/mL ampoule) mg sci Q2-4hrly PRN for SOB/pain Glycopyrrolate (0.2mg/1 ml ampoule) mcg q2hrly sci PRN for terminal secretions Midazolam (5mg / 1 ml) 2.5-5mg sci Q2-4 hrly PRN for terminal agitation Clonazepam drops (2.5mg / 1 ml) mg S/L (sublingual) bd prn for myoclonic jerks Lorazepam S/L (sublingual) 0.5mg bd-tds PRN for anxiety Sodibic mouthwash po 10ml QID Aquaspray po 1 QID Cyclizine 25mg tds sci prn for nausea Olanzapine AN ODT 2.5-5mg bd prn for delirium/agitation

27 Last 48 hours of life For every patient and family, the experience will be different Never presume what is the worst thing Ongoing assessment **The family will remember everything a bad death will be remembered and recounted in the family for a very long time


28 Symptoms and signs in CKD

29 Palliative Approach Letter

30 Ambulance palliative care plan
31 HYDROmorphone shortage Dilaudid is currently in shortage. Limit prescribing to prioritise patients with renal failure Morphine is avoided unless there is no alternative available Reduce dose (calculate dose from the renal appropriate HYDROmorphone dose) and time intervals watch for toxicity Can use Fentanyl (used in Broken Hill) If pain is under control, Panadol, Jurnista, Endone, Oxycontin, Fentanyl patch, Norspan patch, Tramadol Avoid NSAIDs
32 Conclusion Dialysis versus non dialysis end of life increasing frailty in both, end of life medications are the same but always look at co-morbidities and current pharmaceuticals Symptoms can be absent until very late, then deterioration occurs quickly Community resources early referral, escalating urgency, carer support paramount Good ongoing relationships with your local community resources with ongoing communication Treat symptoms to effect and side effect Always refer onwards where required Avoid conflicting information Have clear plans that are easy to follow for the families and teams
33 References Brown MA, Collett GK, Josland EA, Foote C, Qiang L, Brennan FP. CKD in Elderly Patients Managed without Dialysis: Survival, Symptoms, and Quality of Life. Clin J Am Soc Nephrol. 2015; 10: 1-9 Webster, A. C., Nagler, E. V., Morton, R. L., & Masson, P. (2017). Chronic Kidney Disease. Lancet, 389(10075), Murtagh, F. E., Addington-Hall, J. M., & Higginson, I. J. (2011). Endstage renal disease: a new trajectory of functional decline in the last year of life. Journal of the American Geriatrics Society, 59(2), Plan.pdf
Care of the dying in End Stage Kidney Disease (ESKD) - Conservative. Elizabeth Josland Renal Supportive Care CNC St George Hospital
 - Conservative. Elizabeth Josland Renal Supportive Care CNC St George Hospital") Care of the dying in End Stage Kidney Disease (ESKD) - Conservative Elizabeth Josland Renal Supportive Care CNC St George Hospital Introduction What does conservative management look like? How does the
Care of the dying in End Stage Kidney Disease (ESKD) - Conservative Elizabeth Josland Renal Supportive Care CNC St George Hospital Introduction What does conservative management look like? How does the
CARE OF THE DYING PATIENT WITH ESKD ELIZABETH JOSLAND - RSC CNC
 CARE OF THE DYING PATIENT WITH ESKD ELIZABETH JOSLAND - RSC CNC OBJECTIVES UNDERSTANDING OF: POTENTIAL COMPLEXITIES OF ESKD PATIENTS IMPORTANCE OF COMMUNICATION CONSIDERATIONS AT END-OF-LIFE END-OF-LIFE
CARE OF THE DYING PATIENT WITH ESKD ELIZABETH JOSLAND - RSC CNC OBJECTIVES UNDERSTANDING OF: POTENTIAL COMPLEXITIES OF ESKD PATIENTS IMPORTANCE OF COMMUNICATION CONSIDERATIONS AT END-OF-LIFE END-OF-LIFE
 The last days of life Linda Magann CNC Palliative Care St George Hospital I m not afraid of dying, I just don t want to be there when it happens Woody Allen Palliative Care is an approach that improves
The last days of life Linda Magann CNC Palliative Care St George Hospital I m not afraid of dying, I just don t want to be there when it happens Woody Allen Palliative Care is an approach that improves
Renal Supportive Care. Renal Supportive Care Symposium 2013 Elizabeth Josland CNC
 Renal Supportive Care. Renal Supportive Care Symposium 2013 Elizabeth Josland CNC Outline Background of Renal Supportive Care Conservative Management Symptom overview Reading What does conservative management
Renal Supportive Care. Renal Supportive Care Symposium 2013 Elizabeth Josland CNC Outline Background of Renal Supportive Care Conservative Management Symptom overview Reading What does conservative management
Introduction to the Concept of Renal Supportive Care. RSC Education Day Elizabeth Josland CNC 2016
 Introduction to the Concept of Renal Supportive Care RSC Education Day Elizabeth Josland CNC 2016 Objectives To understand the interface between Nephrology and Palliative Care and the role of Renal Supportive
Introduction to the Concept of Renal Supportive Care RSC Education Day Elizabeth Josland CNC 2016 Objectives To understand the interface between Nephrology and Palliative Care and the role of Renal Supportive
Supportive Care. End of Life Phase
 Supportive Care End of Life Phase Guidelines for Health Care Professionals In the care of patients with established renal failure who are in the last days of life References: Chambers E J (2004) End of
Supportive Care End of Life Phase Guidelines for Health Care Professionals In the care of patients with established renal failure who are in the last days of life References: Chambers E J (2004) End of
Regional Renal Training
 Regional Renal Training Palliative and End of Life Care Dr Clare Kendall North Bristol NHS Trust Advanced Kidney Disease Dialysis/Transplant Conservative Management Deteriorating despite dialysis/failing
Regional Renal Training Palliative and End of Life Care Dr Clare Kendall North Bristol NHS Trust Advanced Kidney Disease Dialysis/Transplant Conservative Management Deteriorating despite dialysis/failing
Integrating Renal & Palliative Care Nurse-Led Intervention
 Ballarat Hospice Care Inc. & Ballarat Health Service- Dialysis Shared Care Model Integrating Renal & Palliative Care Nurse-Led Intervention SMRPCC Clinical Forum, 20 th May 2016 Vicky Smith, RN MANP Palliative
Ballarat Hospice Care Inc. & Ballarat Health Service- Dialysis Shared Care Model Integrating Renal & Palliative Care Nurse-Led Intervention SMRPCC Clinical Forum, 20 th May 2016 Vicky Smith, RN MANP Palliative
For patients and their carers this means smoother symptom control, better support in a crisis, and avoidance of admission if that is their choice.
 Bedfordshire Palliative Care Palliative Care Medicines Guidance This folder has been produced to support professionals providing palliative care in any setting. Its aim is to make best practice in palliative
Bedfordshire Palliative Care Palliative Care Medicines Guidance This folder has been produced to support professionals providing palliative care in any setting. Its aim is to make best practice in palliative
Palliative Approach Toolkit: A framework for a palliative approach to care in residential aged care facilities
 Palliative Approach Toolkit: A framework for a palliative approach to care in residential aged care facilities Professor Liz Reymond MBBS (Hons), MSc, PhD, FRACGP, FAChPM Brisbane South Palliative Care
Palliative Approach Toolkit: A framework for a palliative approach to care in residential aged care facilities Professor Liz Reymond MBBS (Hons), MSc, PhD, FRACGP, FAChPM Brisbane South Palliative Care
PRESCRIBING GUIDELINES FOR SYMPTOM MANAGEMENT IN THE DYING PATIENT
 PRESCRIBING GUIDELINES FOR SYMPTOM MANAGEMENT IN THE DYING PATIENT A collaboration between: St. Rocco s Hospice, Bridgewater Community Healthcare NHS Trust, NHS Warrington Clinical Commissioning Group,
PRESCRIBING GUIDELINES FOR SYMPTOM MANAGEMENT IN THE DYING PATIENT A collaboration between: St. Rocco s Hospice, Bridgewater Community Healthcare NHS Trust, NHS Warrington Clinical Commissioning Group,
PAIN MANAGEMENT Patient established on oral morphine or opioid naive.
 PAIN MANAGEMENT Patient established on oral morphine or opioid naive. Important; It is the responsibility of the prescriber to ensure that guidelines are followed when prescribing opioids. Every member
PAIN MANAGEMENT Patient established on oral morphine or opioid naive. Important; It is the responsibility of the prescriber to ensure that guidelines are followed when prescribing opioids. Every member
HealthEd The Annual Women s Health Update 2016
 Presentation overview Background End of life planning for the woman with cancer Palliative Care Framework of care based on prognostication Key processes within the framework to meet emergent clinical needs
Presentation overview Background End of life planning for the woman with cancer Palliative Care Framework of care based on prognostication Key processes within the framework to meet emergent clinical needs
GUIDELINES FOR PRESCRIBING AT THE END OF LIFE FOR PATIENTS WITH RENAL IMPAIRMENT (estimated glomerular filtration rate<30)
") GUIDELINES FOR PRESCRIBING AT THE END OF LIFE FOR PATIENTS WITH RENAL IMPAIRMENT These guidelines have been produced in collaboration with Dr Lucy Smyth, Consultant in Renal Medicine, Royal Devon and Exeter
GUIDELINES FOR PRESCRIBING AT THE END OF LIFE FOR PATIENTS WITH RENAL IMPAIRMENT These guidelines have been produced in collaboration with Dr Lucy Smyth, Consultant in Renal Medicine, Royal Devon and Exeter
Renal Prescribing at End of Life Guidance for Anticipatory prescribing for patients in renal failure (egfr<30) at the end of life
 at the end of life") Guidance for Anticipatory prescribing for patients in renal failure (egfr
Guidance for Anticipatory prescribing for patients in renal failure (egfr
Renal Palliative Care Last Days of Life
 Renal Palliative Care Last Days of Life Introduction This guideline is an aid to clinical decision-making and good practice for patients with stage 4-5 chronic kidney disease (egfr
Renal Palliative Care Last Days of Life Introduction This guideline is an aid to clinical decision-making and good practice for patients with stage 4-5 chronic kidney disease (egfr
PAIN MANAGEMENT Person established taking oral morphine or opioid naive.
 PAIN MANAGEMENT Person established taking oral morphine or opioid naive. Important; it is the responsibility of the prescriber to ensure that guidelines are followed when prescribing opioids. Every member
PAIN MANAGEMENT Person established taking oral morphine or opioid naive. Important; it is the responsibility of the prescriber to ensure that guidelines are followed when prescribing opioids. Every member
HOSPICE My lecture outline
 Objectives: o Describe a brief history of the development of hospice care o Describe the hospice philosophy of care o Describe the referral process o Describe hospice services o Describe reimbursement
Objectives: o Describe a brief history of the development of hospice care o Describe the hospice philosophy of care o Describe the referral process o Describe hospice services o Describe reimbursement
Care of the Dying. For dosing in severe renal impairment see separate guidance for care of the dying in severe renal failure.
 Care of the Dying Early diagnosis of the dying process allows for adequate preparation of the patient, the family and the carers. This clinical guidance covers the prescribing and management of patients
Care of the Dying Early diagnosis of the dying process allows for adequate preparation of the patient, the family and the carers. This clinical guidance covers the prescribing and management of patients
Waterloo Wellington (WW) Symptom Management Guideline for the End of Life (EOL) Medication Order Set for Long Term Care (LTC)
 Symptom Management Guideline for the End of Life (EOL) Medication Order Set for Long Term Care (LTC)") Waterloo Wellington (WW) Symptom Management Guideline for the End of Life (EOL) Medication Order Set for Long Term Care (LTC) May 2018 THE WATERLOO WELLINGTON SYMPTOM MANAGEMENT GUIDELINE FOR THE END OF
Waterloo Wellington (WW) Symptom Management Guideline for the End of Life (EOL) Medication Order Set for Long Term Care (LTC) May 2018 THE WATERLOO WELLINGTON SYMPTOM MANAGEMENT GUIDELINE FOR THE END OF
Palliative care for heart failure patients. Susan Addie
 Palliative care for heart failure patients Susan Addie Treatments The most common limiting and distressing complaint is of fatigue and breathlessness. Optimal treatment strategies relieve symptoms, improves
Palliative care for heart failure patients Susan Addie Treatments The most common limiting and distressing complaint is of fatigue and breathlessness. Optimal treatment strategies relieve symptoms, improves
Supporting Last Days of Life Symptom Control Medication Guidance: Algorithm. Agitation & Anxiety
 Agitation & Anxiety (Exclude or treat REVERSIBLE causes*) Patient is anxious / frightened, but lucid Patient is confused, agitated and / or hallucinating MIDAZOLAM 2.5-5mg s/c (Max total 24 hour dose of
Agitation & Anxiety (Exclude or treat REVERSIBLE causes*) Patient is anxious / frightened, but lucid Patient is confused, agitated and / or hallucinating MIDAZOLAM 2.5-5mg s/c (Max total 24 hour dose of
Symptom Management Guidelines for End of Life Care
 Symptom Management Guidelines for End of Life Care The following pages are guidelines for the management of common symptoms in the last few days of life. General principles: 1. Consider how symptoms can
Symptom Management Guidelines for End of Life Care The following pages are guidelines for the management of common symptoms in the last few days of life. General principles: 1. Consider how symptoms can
End of life prescribing guidance
 End of life prescribing guidance Introduction This guidance has been prepared to ASSIST IN DECISION MAKING for the prescribing and monitoring of medicines useful in the management of symptoms commonly
End of life prescribing guidance Introduction This guidance has been prepared to ASSIST IN DECISION MAKING for the prescribing and monitoring of medicines useful in the management of symptoms commonly
Care in the Last Days of Life
 Care in the Last Days of Life Introduction This guideline is an aid to clinical decision making and good practice in person-centred care for patients who are deteriorating and at risk of dying. The patient
Care in the Last Days of Life Introduction This guideline is an aid to clinical decision making and good practice in person-centred care for patients who are deteriorating and at risk of dying. The patient
Palliative Patient in Emergency Department
 Palliative Patient in Emergency Department Dr Thiru Thirukkumaran Palliative Care Services NW THO Northwest Regional Hospital, Burnie Northwest Tasmania Outline the Session Introduction What is palliative
Palliative Patient in Emergency Department Dr Thiru Thirukkumaran Palliative Care Services NW THO Northwest Regional Hospital, Burnie Northwest Tasmania Outline the Session Introduction What is palliative
MMG035 Symptom Management Guidelines for a Person thought to be in the Last Few Days and Hours of Life
 MMG035 Symptom Management Guidelines for a Person thought to be in the Last Few Days and Hours of Life The following pages are guidelines for the management of common symptoms for a person thought to be
MMG035 Symptom Management Guidelines for a Person thought to be in the Last Few Days and Hours of Life The following pages are guidelines for the management of common symptoms for a person thought to be
Our plan for giving better care to people with dementia Oxleas Dementia
 Our plan for giving better care to people with dementia Oxleas Dementia 2013-2016 November 2013 1 Contents 1. What is our plan about? 2. Finding out if someone has dementia 3. Finding out the care and
Our plan for giving better care to people with dementia Oxleas Dementia 2013-2016 November 2013 1 Contents 1. What is our plan about? 2. Finding out if someone has dementia 3. Finding out the care and
Palliative Care in a Dementia Unit: The Presbyterian Support Southland experience. Carla Arkless NP
 Palliative Care in a Dementia Unit: The Presbyterian Support Southland experience Carla Arkless NP Overview What the literature is saying Palliative Care challenges Our experiences Case example What is
Palliative Care in a Dementia Unit: The Presbyterian Support Southland experience Carla Arkless NP Overview What the literature is saying Palliative Care challenges Our experiences Case example What is
Algorithms for Symptom Management. In End of Life Care
 Algorithms for Symptom Management In End of Life Care The Use of Drugs Beyond Licence (off label) -The Medicines and Healthcare Products Regulatory Agency (MHRA) in the UK regulates the activity of the
Algorithms for Symptom Management In End of Life Care The Use of Drugs Beyond Licence (off label) -The Medicines and Healthcare Products Regulatory Agency (MHRA) in the UK regulates the activity of the
Conservative Care Pathway: A Client-Centred Approach
 2016 Conservative Care Pathway: A Client-Centred Approach Abbotsford Kidney Care Clinic October 7, 2016 Bobbi Preston, MSW, RCSW Jane Valcourt, RN Susan Cooper, MD, FRCP Goals of Session 1. Introduce the
2016 Conservative Care Pathway: A Client-Centred Approach Abbotsford Kidney Care Clinic October 7, 2016 Bobbi Preston, MSW, RCSW Jane Valcourt, RN Susan Cooper, MD, FRCP Goals of Session 1. Introduce the
Care of the Dying Management in Severe Renal Failure
 Care of the Dying Management in Severe Renal Failure Clinical Guideline Early diagnosis of the dying process allows for adequate preparation of the patient, the family and the carers. This clinical guidance
Care of the Dying Management in Severe Renal Failure Clinical Guideline Early diagnosis of the dying process allows for adequate preparation of the patient, the family and the carers. This clinical guidance
Pain and Chronic Kidney Disease
 Pain and Chronic Kidney Disease Frank Brennan Palliative Care Physician Department of Nephrology, St George Hospital Renal Supportive Care Symposium St George Hospital August 21 2015 Epidemiology Effect
Pain and Chronic Kidney Disease Frank Brennan Palliative Care Physician Department of Nephrology, St George Hospital Renal Supportive Care Symposium St George Hospital August 21 2015 Epidemiology Effect
Acceptance onto dialysis guidelines: St George Hospital
 Acceptance onto dialysis guidelines: St George Hospital The following information is a guideline to support clinicians in decision making regarding acceptance onto dialysis. A review of international guidelines
Acceptance onto dialysis guidelines: St George Hospital The following information is a guideline to support clinicians in decision making regarding acceptance onto dialysis. A review of international guidelines
Supportive and Palliative care for patients with Pancreatic Cancer. Dr Holly Taylor September 2018
 Supportive and Palliative care for patients with Pancreatic Cancer Dr Holly Taylor September 2018 Aims of this session To discuss the principles of supportive and palliative care Identification of patients
Supportive and Palliative care for patients with Pancreatic Cancer Dr Holly Taylor September 2018 Aims of this session To discuss the principles of supportive and palliative care Identification of patients
PATIENTS WHO WITHDRAW FROM DIALYSIS. Dr Katalin Urban Palliative Care Specialist Greenwich Hospital
 PATIENTS WHO WITHDRAW FROM DIALYSIS Dr Katalin Urban Palliative Care Specialist Greenwich Hospital Registrar project for FRACP Title: Patients who withdraw from dialysis in a Sydney centre with Palliative
PATIENTS WHO WITHDRAW FROM DIALYSIS Dr Katalin Urban Palliative Care Specialist Greenwich Hospital Registrar project for FRACP Title: Patients who withdraw from dialysis in a Sydney centre with Palliative
Care of the Dying Management in Severe Renal Failure
 Care of the Dying Management in Severe Renal Failure Clinical Guideline Early recognition of the dying process allows for adequate preparation of the patient, the family and the carers. This clinical guidance
Care of the Dying Management in Severe Renal Failure Clinical Guideline Early recognition of the dying process allows for adequate preparation of the patient, the family and the carers. This clinical guidance
Palliative and End of Life Care in End Stage Renal Disease
 Palliative and End of Life Care in End Stage Renal Disease Palliative and End of Life Care Priority for Action Regional Consensus Workshop 30.06.2010 Neal Morgan Consultant Nephrologist SHSCT Outline Introduction
Palliative and End of Life Care in End Stage Renal Disease Palliative and End of Life Care Priority for Action Regional Consensus Workshop 30.06.2010 Neal Morgan Consultant Nephrologist SHSCT Outline Introduction
Palliative Care Impact Survey
 September 2018 Contents Introduction...3 Headlines...3 Approach...4 Findings...4 Which guideline are used...4 How and where the guidelines are used...6 Alternative sources of information...7 Use of the
September 2018 Contents Introduction...3 Headlines...3 Approach...4 Findings...4 Which guideline are used...4 How and where the guidelines are used...6 Alternative sources of information...7 Use of the
GUIDELINES ON THE MANAGEMENT OF PAIN DUE TO CANCER IN ADULTS
 GUIDELINES ON THE MANAGEMENT OF PAIN DUE TO CANCER IN ADULTS Bristol Palliative Care Collaborative Contact Numbers: Hospital Specialist Palliative Care Teams: North Bristol 0117 4146392 UH Bristol 0117
GUIDELINES ON THE MANAGEMENT OF PAIN DUE TO CANCER IN ADULTS Bristol Palliative Care Collaborative Contact Numbers: Hospital Specialist Palliative Care Teams: North Bristol 0117 4146392 UH Bristol 0117
The last days of life in hospital and at home
 The last days of life in hospital and at home Beaumont Multi-disciplinary Palliative Care Study Day 28/9/2017 Dr Sarah McLean Consultant in Palliative Medicine St Francis Hospice Beaumont Hospital Overview
The last days of life in hospital and at home Beaumont Multi-disciplinary Palliative Care Study Day 28/9/2017 Dr Sarah McLean Consultant in Palliative Medicine St Francis Hospice Beaumont Hospital Overview
PALLIATIVE MEDICINE Nigel Sykes St Christopher s Hospice London UK
 Guttmann Conference June 2013 PALLIATIVE MEDICINE Nigel Sykes St Christopher s Hospice London UK Palliative Medicine What is Palliative Medicine and where did it come from? The extent and organisation
Guttmann Conference June 2013 PALLIATIVE MEDICINE Nigel Sykes St Christopher s Hospice London UK Palliative Medicine What is Palliative Medicine and where did it come from? The extent and organisation
Preventing harmful treatment
 Preventing harmful treatment How can Palliative Care prevent patients receiving overzealous or futile treatment? Antwerp, November 2010 Prof Scott A Murray, St Columba s Hospice Chair of Primary Palliative
Preventing harmful treatment How can Palliative Care prevent patients receiving overzealous or futile treatment? Antwerp, November 2010 Prof Scott A Murray, St Columba s Hospice Chair of Primary Palliative
Difficult conversations. Dr Amy Waters MBBS, FRACP Staff Specialist in Palliative Medicine, St George Hospital Conjoint Lecturer, UNSW
 Difficult conversations Dr Amy Waters MBBS, FRACP Staff Specialist in Palliative Medicine, St George Hospital Conjoint Lecturer, UNSW What are difficult conversations? Why are they difficult? Difficult
Difficult conversations Dr Amy Waters MBBS, FRACP Staff Specialist in Palliative Medicine, St George Hospital Conjoint Lecturer, UNSW What are difficult conversations? Why are they difficult? Difficult
Delivering personalised care to end of life patients. Jane Naismith Nurse Consultant in Palliative care St Joseph s Hospice London
 Delivering personalised care to end of life patients Jane Naismith Nurse Consultant in Palliative care St Joseph s Hospice London Over View This session will cover Supporting patients with long term conditions
Delivering personalised care to end of life patients Jane Naismith Nurse Consultant in Palliative care St Joseph s Hospice London Over View This session will cover Supporting patients with long term conditions
Conservative Management of Uraemia
 Conservative Management of Uraemia Information for Health Professionals Renal Department The York Hospital and Scarborough Hospital Tel: 01904 725370 For more information, please contact: The Renal Specialist
Conservative Management of Uraemia Information for Health Professionals Renal Department The York Hospital and Scarborough Hospital Tel: 01904 725370 For more information, please contact: The Renal Specialist
Three triggers that suggest that patients could benefit from a hospice palliative care approach
 Why is it important to identify people nearing the end of life? About 1% of the population dies each year. Although some deaths are unexpected, many more in fact can be predicted. This is inherently difficult,
Why is it important to identify people nearing the end of life? About 1% of the population dies each year. Although some deaths are unexpected, many more in fact can be predicted. This is inherently difficult,
PAIN AND SYMPTOM MANAGEMENT GUIDANCE IN THE LAST DAYS OF LIFE
 PAIN AND SYMPTOM MANAGEMENT GUIDANCE IN THE LAST DAYS OF LIFE Reference: DCM029 Version: 1.1 This version issued: 07/06/18 Result of last review: Minor changes Date approved by owner (if applicable): N/A
PAIN AND SYMPTOM MANAGEMENT GUIDANCE IN THE LAST DAYS OF LIFE Reference: DCM029 Version: 1.1 This version issued: 07/06/18 Result of last review: Minor changes Date approved by owner (if applicable): N/A
Specialist palliative care for patients with heart failure. Dr Katie Taylor Consultant in Palliative Medicine
 Specialist palliative care for patients with heart failure Dr Katie Taylor Consultant in Palliative Medicine Objectives Identify which patients to refer to hospice Review symptom management Think about
Specialist palliative care for patients with heart failure Dr Katie Taylor Consultant in Palliative Medicine Objectives Identify which patients to refer to hospice Review symptom management Think about
SERVICE SPECIFICATION 6 Conservative Management & End of Life Care
 SERVICE SPECIFICATION 6 Conservative Management & End of Life Care Table of Contents Page 1 Key Messages 2 2 Introduction & Background 2 3 Relevant Guidelines & Standards 2 4 Scope of Service 3 5 Interdependencies
SERVICE SPECIFICATION 6 Conservative Management & End of Life Care Table of Contents Page 1 Key Messages 2 2 Introduction & Background 2 3 Relevant Guidelines & Standards 2 4 Scope of Service 3 5 Interdependencies
ANTICIPATORY PRESCRIBING FOR PATIENTS AT END OF LIFE WITH RENAL IMPAIRMENT
 ANTICIPATORY PRESCRIBING FOR PATIENTS AT END OF LIFE WITH RENAL Doses of opiates must be proptional to current analgesic medication Please refer ALL patients on Methadone Ketamine to SPCT f advice. Patients
ANTICIPATORY PRESCRIBING FOR PATIENTS AT END OF LIFE WITH RENAL Doses of opiates must be proptional to current analgesic medication Please refer ALL patients on Methadone Ketamine to SPCT f advice. Patients
Palliative care for patients with brain cancer
 Palliative care for patients with brain cancer Lyn Cave Clinical Nurse Specialist Palliative Care Hospital2Home (H2H) Dr Jayne Wood Clinical Lead Palliative Care The Royal Marsden and Royal Brompton Palliative
Palliative care for patients with brain cancer Lyn Cave Clinical Nurse Specialist Palliative Care Hospital2Home (H2H) Dr Jayne Wood Clinical Lead Palliative Care The Royal Marsden and Royal Brompton Palliative
Palliative Prescribing - Pain
 Palliative Prescribing - Pain LAURA BARNFIELD 21/2/17 Aims To understand the classes of painkillers available in palliative care To gain confidence in counselling regarding opiates To gain confidence prescribing
Palliative Prescribing - Pain LAURA BARNFIELD 21/2/17 Aims To understand the classes of painkillers available in palliative care To gain confidence in counselling regarding opiates To gain confidence prescribing
Palliative care in long-term conditions Scottish Palliative Care Pharmacists Association
 Palliative care in long-term conditions 2011 2012 Scottish Palliative Care Pharmacists Association Aims & Objectives To explore symptoms, general management principles and appropriate palliative treatment
Palliative care in long-term conditions 2011 2012 Scottish Palliative Care Pharmacists Association Aims & Objectives To explore symptoms, general management principles and appropriate palliative treatment
Palliative Care: Improving quality of life when you re seriously ill.
 Palliative Care The Relief You Need When You re Experiencing the Symptoms of Serious Illness Palliative Care: Improving quality of life when you re seriously ill. Dealing with the symptoms of any painful
Palliative Care The Relief You Need When You re Experiencing the Symptoms of Serious Illness Palliative Care: Improving quality of life when you re seriously ill. Dealing with the symptoms of any painful
Treating the symptoms of kidney failure
 Treating the symptoms of kidney failure Information for patients, relatives and carers Renal Department The York Hospital and Scarborough Hospital Tel: 01904 725370 For more information, please contact:
Treating the symptoms of kidney failure Information for patients, relatives and carers Renal Department The York Hospital and Scarborough Hospital Tel: 01904 725370 For more information, please contact:
A tale of two specialties
 A tale of two specialties United Kingdom Annual Symposia on Renal-Palliative Care co-organised by both disciplines National Service Framework for Renal Services Part 2 (UK) - 2005 Concentrated on the
A tale of two specialties United Kingdom Annual Symposia on Renal-Palliative Care co-organised by both disciplines National Service Framework for Renal Services Part 2 (UK) - 2005 Concentrated on the
Overview of Essentials of Pain Management. Updated 11/2016
 0 Overview of Essentials of Pain Management Updated 11/2016 1 Overview of Essentials of Pain Management 1. Assess pain intensity on a 0 10 scale in which 0 = no pain at all and 10 = the worst pain imaginable.
0 Overview of Essentials of Pain Management Updated 11/2016 1 Overview of Essentials of Pain Management 1. Assess pain intensity on a 0 10 scale in which 0 = no pain at all and 10 = the worst pain imaginable.
ADVANCE CARE PLANNING FOR KIDNEY PATIENTS: THE IMPORTANCE OF AN ONGOING DISCUSSION
 ADVANCE CARE PLANNING FOR KIDNEY PATIENTS: THE IMPORTANCE OF AN ONGOING DISCUSSION Melissa Hale, MSW, LCSW Advance Care Planning Coordinator ProHealth Care Thank You. CMS: Conditions for Coverage Renal
ADVANCE CARE PLANNING FOR KIDNEY PATIENTS: THE IMPORTANCE OF AN ONGOING DISCUSSION Melissa Hale, MSW, LCSW Advance Care Planning Coordinator ProHealth Care Thank You. CMS: Conditions for Coverage Renal
Road Blocks in Non-Cancer Palliative Care Obstacles observed from outpatient non-cancer palliative practice.
 Road Blocks in Non-Cancer Palliative Care Obstacles observed from outpatient non-cancer palliative practice. 25th Annual Palliative Education and Research Days, West Edmonton Mall. Edmonton. 2014 Amanda
Road Blocks in Non-Cancer Palliative Care Obstacles observed from outpatient non-cancer palliative practice. 25th Annual Palliative Education and Research Days, West Edmonton Mall. Edmonton. 2014 Amanda
[Type text] Anticipatory Medication STAT dose and Syringe Driver Guidance [Type text]
![[Type text] Anticipatory Medication STAT dose and Syringe Driver Guidance [Type text]](/thumbs/92/110296570.jpg "[Type text] Anticipatory Medication STAT dose and Syringe Driver Guidance [Type text]") [Type text] Anticipatory Medication STAT dose and Syringe Driver Guidance [Type text] Patients with egfr greater than 30mL/min Patients with egfr less than 30mL/min Symptom Drug Dose Symptom Drug Dose
[Type text] Anticipatory Medication STAT dose and Syringe Driver Guidance [Type text] Patients with egfr greater than 30mL/min Patients with egfr less than 30mL/min Symptom Drug Dose Symptom Drug Dose
Geriatric Nephrology. Murtener Tage
 Geriatric Nephrology Murtener Tage 2014 Isabelle.Binet@kssg.ch www.nierenstiftung.ch Plan Geriatric nephrology The elderly with CKD The elderly on dialysis The elderly in transplantation Plan Geriatric
Geriatric Nephrology Murtener Tage 2014 Isabelle.Binet@kssg.ch www.nierenstiftung.ch Plan Geriatric nephrology The elderly with CKD The elderly on dialysis The elderly in transplantation Plan Geriatric
5 key areas for research, and how to go forward. Primary Palliative Care Research Forum, University of Capetown, September, 2010
 5 key areas for research, and how to go forward Primary Palliative Care Research Forum, University of Capetown, September, 2010 Scott A Murray St Columba s Hospice Chair of Primary Palliative Care Primary
5 key areas for research, and how to go forward Primary Palliative Care Research Forum, University of Capetown, September, 2010 Scott A Murray St Columba s Hospice Chair of Primary Palliative Care Primary
Heart Failure Vital steps for palliative care. Dr Karen J Hogg Glasgow Royal Infirmary
 Heart Failure Vital steps for palliative care Dr Karen J Hogg Glasgow Royal Infirmary Overview Why is heart failure a problem? Why do we need integrated cardiology and palliative care services? Cardiology
Heart Failure Vital steps for palliative care Dr Karen J Hogg Glasgow Royal Infirmary Overview Why is heart failure a problem? Why do we need integrated cardiology and palliative care services? Cardiology
Unmet palliative care needs in heart failure heart failure. Dr Claire Hookey
 Unmet palliative care needs in heart failure heart failure Dr Claire Hookey Discomfort was not necessarily greatest in those dying from cancer; patients dying of heart failure, or renal failure, or both,
Unmet palliative care needs in heart failure heart failure Dr Claire Hookey Discomfort was not necessarily greatest in those dying from cancer; patients dying of heart failure, or renal failure, or both,
4/3/2018. Management of Acute Pain Crises. Five Mistakes I ve made and why you shouldn t
 Management of Acute Pain Crises Maggie O Connor, M.D. Retired Palliative Care Physician Hope is not the conviction that something will turn out well, but the certainty that something makes sense, regardless
Management of Acute Pain Crises Maggie O Connor, M.D. Retired Palliative Care Physician Hope is not the conviction that something will turn out well, but the certainty that something makes sense, regardless
Community and Mental Health Services. Palliative Care. Criteria and
 Community and Mental Health Services Specialist Palliative Care Service Referral Criteria and Guidance November 2018 Specialist Palliative Care Service Referrals These guidelines cover referrals for patients
Community and Mental Health Services Specialist Palliative Care Service Referral Criteria and Guidance November 2018 Specialist Palliative Care Service Referrals These guidelines cover referrals for patients
Guidelines: EOLC Symptom Control for Patients with Normal Renal Function (in Wandsworth)
") Guidelines: EOLC Symptom Control for Patients with Normal Renal Function (in Wandsworth) Policy Number : DC020 Issue Date: October 2014 Review date: October 2016 Policy Owner: Head Community Services Monitor:
Guidelines: EOLC Symptom Control for Patients with Normal Renal Function (in Wandsworth) Policy Number : DC020 Issue Date: October 2014 Review date: October 2016 Policy Owner: Head Community Services Monitor:
POsitive mental health for young people. What you need to know about Children and Adolescent s Mental Health Services (CAMHS) in Buckinghamshire
 in Buckinghamshire") POsitive mental health for young people What you need to know about Children and Adolescent s Mental Health Services (CAMHS) in Buckinghamshire 1 CONTENTS PAGE 3 AND 4 When to ask for help PAGE 5 AND 6
POsitive mental health for young people What you need to know about Children and Adolescent s Mental Health Services (CAMHS) in Buckinghamshire 1 CONTENTS PAGE 3 AND 4 When to ask for help PAGE 5 AND 6
Palliative Care Asking the questions that matter to me
 Palliative Care Asking the questions that matter to me THE PALLIATIVE HUB Adult This booklet has been developed by the Palliative Care Senior Nurses Network and adapted with permission from Palliative
Palliative Care Asking the questions that matter to me THE PALLIATIVE HUB Adult This booklet has been developed by the Palliative Care Senior Nurses Network and adapted with permission from Palliative
Outcomes of dialysis in the elderly. DNT March 2011 Dr Céline Foote
 Outcomes of dialysis in the elderly DNT March 2011 Dr Céline Foote Increasing number of elderly patients on renal replacement therapy 500 500 Patients per million 400 300 200 100 400 300 200 100 TOTAL
Outcomes of dialysis in the elderly DNT March 2011 Dr Céline Foote Increasing number of elderly patients on renal replacement therapy 500 500 Patients per million 400 300 200 100 400 300 200 100 TOTAL
Palliative Care. Anticipatory Prescribing Guidelines & June Gippsland Region Palliative Care Consortium Clinical Practice Group
 Palliative Care Anticipatory Prescribing Guidelines June 2016 Gippsland Region Palliative Care Consortium Clinical Practice Group Policy No. Title Keywords Ratified GRPCC-CPG008_1.1_2016 Anticipatory Prescribing
Palliative Care Anticipatory Prescribing Guidelines June 2016 Gippsland Region Palliative Care Consortium Clinical Practice Group Policy No. Title Keywords Ratified GRPCC-CPG008_1.1_2016 Anticipatory Prescribing
The Palliative Care Journey. By Sandra O Sullivan Clinical Nurse Manager 1 St Luke's home
 The Palliative Care Journey By Sandra O Sullivan Clinical Nurse Manager 1 St Luke's home Aims 1. To provide an overview of what palliative care involves. 2. Identify, at what stage should Dementia be acknowledged
The Palliative Care Journey By Sandra O Sullivan Clinical Nurse Manager 1 St Luke's home Aims 1. To provide an overview of what palliative care involves. 2. Identify, at what stage should Dementia be acknowledged
Palliative Care & Hospice
 Palliative Care & Hospice Kenneth Brummel-Smith, M.D. Charlotte Edwards Maguire Professor, Department of Geriatrics Florida State University College of Medicine 1 Diane Meier, MD Director, Center to Advance
Palliative Care & Hospice Kenneth Brummel-Smith, M.D. Charlotte Edwards Maguire Professor, Department of Geriatrics Florida State University College of Medicine 1 Diane Meier, MD Director, Center to Advance
THE CONSERVATIVE CARE PATHWAY
 THE CONSERVATIVE CARE PATHWAY Dr. Gaylene Hargrove Sept. 19, 2015 Island Health Renal Program End of Life Conference Learning Objectives Describe and discuss what defines conservative care. Identify key
THE CONSERVATIVE CARE PATHWAY Dr. Gaylene Hargrove Sept. 19, 2015 Island Health Renal Program End of Life Conference Learning Objectives Describe and discuss what defines conservative care. Identify key
Palliative and Hospice Care of the Terminally Ill Introduction
 Palliative and Hospice Care of the Terminally Ill Introduction There has been an increase in life expectancy for men and women of all races to 77.6 years Leading causes of death in older patients are chronic
Palliative and Hospice Care of the Terminally Ill Introduction There has been an increase in life expectancy for men and women of all races to 77.6 years Leading causes of death in older patients are chronic
End of life. care planning. in dementia. Dr Victor Pace St Christopher s Hospice February 2018
 Dr Victor Pace St Christopher s Hospice February 2018 It s making the headlines Why does advance matter in dementia? Why does this matter? Since 2015, dementia has become the leading cause of death in
Dr Victor Pace St Christopher s Hospice February 2018 It s making the headlines Why does advance matter in dementia? Why does this matter? Since 2015, dementia has become the leading cause of death in
We need to talk about Palliative Care. Parkinson s UK
 We need to talk about Palliative Care Parkinson s UK Introduction Parkinson s UK strongly welcomes the Committee s Inquiry, and hope that it will help to address inequalities in access to palliative and
We need to talk about Palliative Care Parkinson s UK Introduction Parkinson s UK strongly welcomes the Committee s Inquiry, and hope that it will help to address inequalities in access to palliative and
The Mid Yorkshire Macmillan Specialist Palliative Care Team
 The Mid Yorkshire Macmillan Specialist Palliative Care Team Morphine and Strong Opioid information leaflet Information for patients/carers The mere mention of Morphine can be enough to conjure up all sorts
The Mid Yorkshire Macmillan Specialist Palliative Care Team Morphine and Strong Opioid information leaflet Information for patients/carers The mere mention of Morphine can be enough to conjure up all sorts
9 End of life issues
 9 End of life issues In this part Key points: End of life issues 132 Palliative care 134 Grief and bereavement 136 130 131 Key points: End of life issues As a person with dementia approaches the end of
9 End of life issues In this part Key points: End of life issues 132 Palliative care 134 Grief and bereavement 136 130 131 Key points: End of life issues As a person with dementia approaches the end of
Management of the Frail Older Patients: What Are the Outcomes
 Management of the Frail Older Patients: What Are the Outcomes Professor Edwina Brown Imperial College Renal and Transplant Centre Hammersmith Hospital, London Increasing prevalence of old old on RRT RRT
Management of the Frail Older Patients: What Are the Outcomes Professor Edwina Brown Imperial College Renal and Transplant Centre Hammersmith Hospital, London Increasing prevalence of old old on RRT RRT
End of Life Care. Dr Anne Garry Consultant in Palliative Medicine
 End of Life Care Dr Anne Garry Consultant in Palliative Medicine Concerns voiced both by public and professionals.. Implementation and on-going training highly variable across country Decisions made by
End of Life Care Dr Anne Garry Consultant in Palliative Medicine Concerns voiced both by public and professionals.. Implementation and on-going training highly variable across country Decisions made by
Specialist Palliative Care Service Referral Criteria and Guidance
 Specialist Palliative Care Service Referral Criteria and Guidance Specialist Palliative Care Service Referrals These guidelines cover referrals for patients with progressive terminal illness, whether
Specialist Palliative Care Service Referral Criteria and Guidance Specialist Palliative Care Service Referrals These guidelines cover referrals for patients with progressive terminal illness, whether
Mental Health Strategy. Easy Read
 Mental Health Strategy Easy Read Mental Health Strategy Easy Read The Scottish Government, Edinburgh 2012 Crown copyright 2012 You may re-use this information (excluding logos and images) free of charge
Mental Health Strategy Easy Read Mental Health Strategy Easy Read The Scottish Government, Edinburgh 2012 Crown copyright 2012 You may re-use this information (excluding logos and images) free of charge
BACK TO THE FUTURE: Palliative Care in the 21 st Century
 BACK TO THE FUTURE: Palliative Care in the 21 st Century Section 3: Hospice 101 I m not afraid of death; I just don t want to be there when it happens. -Woody Allen A Century of Change 1900 2000 Age at
BACK TO THE FUTURE: Palliative Care in the 21 st Century Section 3: Hospice 101 I m not afraid of death; I just don t want to be there when it happens. -Woody Allen A Century of Change 1900 2000 Age at
COMMUNICATION ISSUES IN PALLIATIVE CARE
 COMMUNICATION ISSUES IN PALLIATIVE CARE Palliative Care: Communication, Communication, Communication! Key Features of Communication in Appropriate setting Permission Palliative Care Be clear about topic
COMMUNICATION ISSUES IN PALLIATIVE CARE Palliative Care: Communication, Communication, Communication! Key Features of Communication in Appropriate setting Permission Palliative Care Be clear about topic
Call the National Dementia Helpline on
 128 Call the National Dementia Helpline on 1800 100 500 End of life issues 9 9 End of life issues In this part Key points: End of life issues 130 Palliative care 132 Grief and bereavement 134 For more
128 Call the National Dementia Helpline on 1800 100 500 End of life issues 9 9 End of life issues In this part Key points: End of life issues 130 Palliative care 132 Grief and bereavement 134 For more
Talking with your doctors about palliative care Dr. Mary Anne Huggins and Barbara Pidcock
 Talking with your doctors about palliative care Dr. Mary Anne Huggins and Barbara Pidcock You will have appointments with your family doctor, and with specialists. It will help you if you write your brief
Talking with your doctors about palliative care Dr. Mary Anne Huggins and Barbara Pidcock You will have appointments with your family doctor, and with specialists. It will help you if you write your brief
15mg oxycodone is equivalent to how much morphine
 15mg oxycodone is equivalent to how much morphine The Borg System is 100 % 15mg oxycodone is equivalent to how much morphine nursing home activity director cover letter 15 mg oxycodone equal to how much
15mg oxycodone is equivalent to how much morphine The Borg System is 100 % 15mg oxycodone is equivalent to how much morphine nursing home activity director cover letter 15 mg oxycodone equal to how much
Emergency Palliative Care
 Emergency Palliative Care Dr Jenny Hynson Consultant Paediatrician Victorian Paediatric Palliative Care Program (VPPCP) Royal Children s Hospital, Melbourne Points of discussion What is palliative care?
Emergency Palliative Care Dr Jenny Hynson Consultant Paediatrician Victorian Paediatric Palliative Care Program (VPPCP) Royal Children s Hospital, Melbourne Points of discussion What is palliative care?
Support for Kidney Cancer
 Page 1 Fact sheet Introduction Our series of kidney cancer fact sheets have been developed to help you understand more about kidney cancer. This fact sheet provides support information for people affected
Page 1 Fact sheet Introduction Our series of kidney cancer fact sheets have been developed to help you understand more about kidney cancer. This fact sheet provides support information for people affected
Northumbria Healthcare NHS Foundation Trust. Your guide to understanding Delirium. Issued by Department of Medicine
 Northumbria Healthcare NHS Foundation Trust Your guide to understanding Delirium Issued by Department of Medicine Purpose of this leaflet This leaflet is for patients and carers and aims to give you information
Northumbria Healthcare NHS Foundation Trust Your guide to understanding Delirium Issued by Department of Medicine Purpose of this leaflet This leaflet is for patients and carers and aims to give you information
12/6/2016. Objective PALLIATIVE CARE IN THE NURSING HOME. Medical Care in the US. Palliative Care
 Objective PALLIATIVE CARE IN THE NURSING HOME Deborah Morris, M.D., M.H.S. Assistant Professor of Medicine The Glennan Center for Geriatrics and Gerontology Eastern Virginia Medical School Describe program
Objective PALLIATIVE CARE IN THE NURSING HOME Deborah Morris, M.D., M.H.S. Assistant Professor of Medicine The Glennan Center for Geriatrics and Gerontology Eastern Virginia Medical School Describe program
Chapter 6. Hospice: A Team Approach to Care
 Chapter 6 Hospice: A Team Approach to Care Chapter 6: Hospice: A Team Approach to Care Comfort, Respect and Dignity in Dying Hospice care provides patients and family members with hope, comfort, respect,
Chapter 6 Hospice: A Team Approach to Care Chapter 6: Hospice: A Team Approach to Care Comfort, Respect and Dignity in Dying Hospice care provides patients and family members with hope, comfort, respect,
Outcome Measures in Palliative Care. Outcome Measures in
 From noon to six o'clock we ran thirty miles to the northward, skirting a sandy shore at the distance of five, and thence iles; the depth was then 5 to eight m fathoms, and we dropped the anchor upon a
From noon to six o'clock we ran thirty miles to the northward, skirting a sandy shore at the distance of five, and thence iles; the depth was then 5 to eight m fathoms, and we dropped the anchor upon a
Approach to symptom control near the end-of-life
 Approach to symptom control near the end-of-life 18 Sept 2011 Dr Alethea Yee Senior Consultant, Department of Palliative Medicine National Cancer Centre,Singapore What is end of life? No precise definition
Approach to symptom control near the end-of-life 18 Sept 2011 Dr Alethea Yee Senior Consultant, Department of Palliative Medicine National Cancer Centre,Singapore What is end of life? No precise definition
Lumbar Fusion. Reference Guide for PACU CLINICAL PATHWAY. All patient variances to the pathway are to be circled and addressed in the progress notes.
 Reference Guide for PACU Lumbar Fusion CLINICAL PATHWAY All patient variances to the pathway are to be circled and addressed in the progress notes. This Clinical Pathway is intended to assist in clinical
Reference Guide for PACU Lumbar Fusion CLINICAL PATHWAY All patient variances to the pathway are to be circled and addressed in the progress notes. This Clinical Pathway is intended to assist in clinical
Agitation. Susan Emmens Palliative Care Clinical Nurse Specialist
 Agitation Susan Emmens Palliative Care Clinical Nurse Specialist Definitions Restlessness finding or affording no rest, uneasy, agitated. Constantly in motion fidgeting Agitation shaking, moving, mental
Agitation Susan Emmens Palliative Care Clinical Nurse Specialist Definitions Restlessness finding or affording no rest, uneasy, agitated. Constantly in motion fidgeting Agitation shaking, moving, mental
Dying in the 21 st Century
 Dying in the 21 st Century ensuring appropriate care at the end of life is everyone s business Dr Will Cairns Statewide Clinical Lead for Care at the End of Life Qld Statewide Strategy for E-o-L Care State
Dying in the 21 st Century ensuring appropriate care at the end of life is everyone s business Dr Will Cairns Statewide Clinical Lead for Care at the End of Life Qld Statewide Strategy for E-o-L Care State