Urgent Care/Triage & Transport of the Severe Stroke Patient in the Field. Robert Knight, BSN, RN, CEN, NRP, CCEMT/P INTEGRIS TeleStroke
|
|
|
- Mary Walsh
- 5 years ago
- Views:
Transcription
1 Urgent Care/Triage & Transport of the Severe Stroke Patient in the Field Robert Knight, BSN, RN, CEN, NRP, CCEMT/P INTEGRIS TeleStroke
2 Suggested Protocols Suggested protocols are just that. They are not intended to replace or supersede current or active protocols or orders. Oversight by local medical director is required. Financial Disclosure: None. Employee of INTEGRIS Health Center
3 Objectives Sections / Objectives Quick review of brain anatomy Briefly discuss recent endovascular stroke trials New treatment regime Why the need for a new stroke triage tool and the new paradigm shift Stroke screening tools for EMS
4 Objectives Large vessel stroke versus small vessel stroke Correlating LVO assessment in the brain What is and how to perform the VAN exam See one do one practical application Suggested Prehospital Stroke guidelines

5

6

7
8 WHY?

9 KILLS 140,000 People a year. That s about one out of every 20 deaths

10

11 Each Minute Time Frame Neurons Lost Ages the brain by Every Second 32, hours Every Minute 1.9 million 3.1 weeks Every Hour 120 million 3.6 years 10 Hours 1.2 billion 36 years
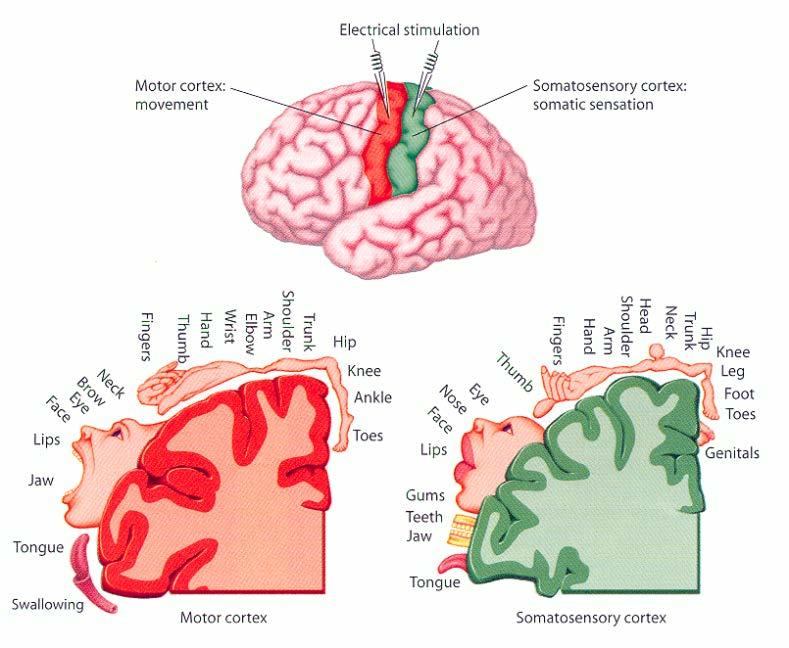
12 Anatomy 1. Brain Map 2. All mammal brains and spinal cord with sensory input in back and movement in front. Spinal cord, brain stem, same orientation 3. Right vs Left side (neglect vs aphasia) 4. Gaze center used as pseudo neglect 5. Center of cortex being involved in movement & is the starting point of VAN 6. Vision in back

13 Frontal gaze center N N V A
14 A

15

16 Brain: Blood Supply

17

18 Penumbra (at risk) Core (irreversibly damaged)
19 Optimizing revascularization Small vessel occlusions Location of vessel occlusion is important How do you know? Symptoms & imaging

20 Optimizing revascularization Medium and large vessel occlusions Location of vessel occlusion is important How do you know? Symptoms & imaging




21 Case Example

22 You re only as good as your Collaterals This is the reason for BP and volume support in acute stroke cases




23

24







25

26

27


28

29 STROKE is the new MI
30 NSTEMI MI MI Paradigm Shift is Needed Now Stroke STEMI NonLVO STROKE LVO Medical Txt Cath Lab TPA TPA & NeuroIR Suite LVO = Large Vessel Occlusion
31 Old Model CT of head 20 min IV & decide to go back for CTA 60 min NeuroIR team additional 30 min to come in now at 120 min New Model EMS notificatio n=fast- VAN TPA decision 45 min tpa started within min Transfer for NeuroIR Wait for read or call NeuroIR 60 to 90 min ED- CT/CTA 15 min TeleStrokenotification of NeuroIR Xfer Out of door after bolus (drip & ship)-30 minutes Retrieved from Teleb, M. J., Vertlage, A., Carter, J., Jayaraman, M. V., & McTaggart, R. A. (2016). Stroke vision, aphasia, neglect (VAN) assessment a novel emergent large vessel occlusion screening tool: pilot study and comparison with current clinical severity indices. NeuroIntervent Surg, 0, 1-5. doi: /neurintsurg

32 Assessment Tools Let s look on how we assess Stroke Patients

33


34 NIHSS Gold Standard Composed of 11 items Each of which score a specific ability between 0 & 4 0 typically indicates normal function Higher score is indicative of some level of impairment Maximum score is 42 with minimum being 0 Pictures-placards to assess Takes time to assess-lengthy Environment Ref: National Institutes of Health


35 Field/ED Triage CSS = FAST We need something : Fast Easy Immediate results 60% of stroke patients call EMS more than 1 hour into symptoms

36 Stroke Clinical Tools for EMS

37 How do they compare?

38 Triage- But Are we seeing everything?

39 Ref: American Heart/American Stroke Association; Mission Lifeline

40 What if we could be better in predicting large vessel strokes?
41 Let s review some basic types of strokes and compare some prehospital large artery screening tools
42 Small Vessel / Lacunar vs Large Artery 1. Lacunar usually are either pure motor or pure sensory 2. Large artery usually have associated cortical symptoms such as Visual Field Cut, Aphasia (inability to talk or understand), or Neglect (gaze preference and ignoring one side) 3. For practical purposes we have simplified: (there are subcortical aphasias & visual field cuts from small artery strokes, etc)

43 Motor weakness used in all large vessel screening tools due to central location as well as its link to functional independence on modified rankin scale used for all 5 endovascular stroke trials Frontal Gaze Center Ability to Talk Ability to Understand Vision
44 Motor weakness used in all large vessel screening tools due to central location as well as its link to functional independence on modified rankin scale used for all 5 endovascular stroke trials Frontal Gaze Center Ability to Talk Ability to Understand Vision RACE Mohamed S Teleb et al. J NeuroIntervent Surg 2017;9: Copyright Society of NeuroInterventional Surgery. All rights reserved
45 RACE
46 Motor weakness used in all large vessel screening tools due to central location as well as its link to functional independence on modified rankin scale used for all 5 endovascular stroke trials Frontal Gaze Center Ability to Talk Ability to Understand Vision LEGS Mohamed S Teleb et al. J NeuroIntervent Surg 2017;9:
47 LEGS
48 Motor weakness used in all large vessel screening tools due to central location as well as its link to functional independence on modified rankin scale used for all 5 endovascular stroke trials Frontal Gaze Center Ability to Talk Ability to Understand Vision LAMS Mohamed S Teleb et al. J NeuroIntervent Surg 2017;9:
49 LAMS
50 Motor weakness used in all large vessel screening tools due to central location as well as its link to functional independence on modified rankin scale used for all 5 endovascular stroke trials Frontal Gaze Center Ability to Talk Ability to Understand Vision CPSSS Mohamed S Teleb et al. J NeuroIntervent Surg 2017;9:
51 CPSSS
52 Motor weakness used in all large vessel screening tools due to central location as well as its link to functional independence on modified rankin scale used for all 5 endovascular stroke trials Frontal Gaze Center Ability to Talk Ability to Understand Vision FAST-ED Mohamed S Teleb et al. J NeuroIntervent Surg 2017;9:
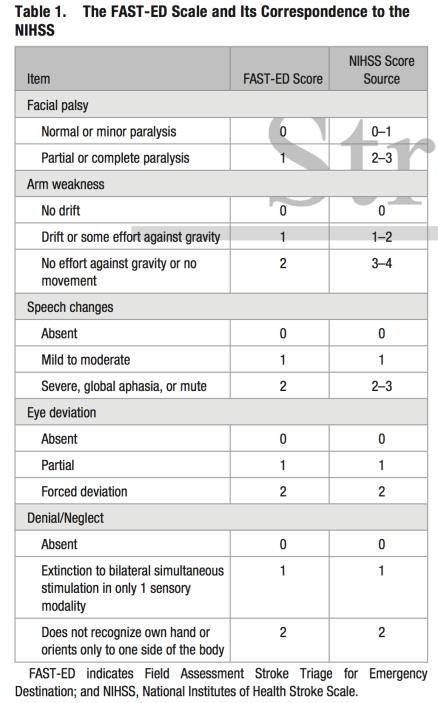
53 FAST ED

54

55
56 VAN Visual Aphasia Neglect (Large Vessel Occlusions)


57 Time is Brain

58 Motor weakness used in all large vessel screening tools due to central location as well as its link to functional independence on modified rankin scale used for all 5 endovascular stroke trials Frontal Gaze Center Ability to Talk Ability to Understand Vision VAN Mohamed S Teleb et al. J NeuroIntervent Surg 2017;9:

59

60 Why use V A N? VAN is Easy to do! Identifies the Cortical Symptoms Screens for large vessel occlusions 1. Weakness 2. Visual Disturbances 3. Aphasia 4. Neglect Early screening gets the patient to where they need to be for the best outcome.

61
 to Stroke care If")

 Aphasia (inability to")
")
.")

62 Perform FAST as usual and add VAN (FAST VAN) to Stroke care If patient has any weakness with any one of the below Visual Disturbance (cross eyed, double vision, or new blindness) Aphasia (inability to speak or understand) Neglect (gaze to one side or ignoring one side) These are likely to be a large artery clot (cortical symptoms). These patients should be considered to go to a facility with EVT Stroke and Neurovascular Services

63 Hold both arms up for 10 seconds palm up. Do they have drift or severe weakness?
64 Have patient look straight ahead and ask them to tell you number of fingers on left and then right Double vision meaning eyes semi crossed, one eye out or in. Have them track your hand to right then left
65 Ask them to repeat: today is a sunny day & name 2 objects Ask them to close eyes and make a fist? If they understand and follow commands and are making words. Do Not Count Slurring of Words. Paraphasic errors are expressive aphasia.
66 Neglect is the classic term; but we added forced gaze from frontal eye fields to get more parts of the brain. Frontal lobe in addition to parietal lobe. Touch patient on right then left and then both. Can they feel right and left at same time?

67 Time of on set: < 4 hrs; > 24 hrs, or unknown

68 Usage Permission: Teleb, M,. MD
69 Conducting the VAN properly Weakness is the essential question Why? It s the middle branch of the MCA, it affects disability scales and outcomes for independence. It warrants the risk of endovascular treatment (EVT) if there is permanent motor weakness.
70 Prehospital Scales for Large Vessel Occlusion RACE LEGS LAMS VAN 3I-SS CPSSS Need to calculate score Yes Yes Yes No Yes Yes # of tests Sensitivity Specificity Mohamed S Teleb et al. J NeuroIntervent Surg 2017;9:
71 Why VAN was chosen? No calculation of numerical score which potentially leads to less observer differences: RACE, CPSS, LAMS, LEGS Uses Motor Weakness as central point/triage like LAMS, Hemiparesis only screening, making it simple for 30% of stroke codes. You don t have to finish the exam if there is no arm weakness Uses Cortical symptoms without severity/scoring allowing to screen patients with LVO despite a lower NIH stroke scale score. VAN teaches what cortical symptoms are & also the medical lingo (aphasia, neglect) Pneumonic helps tester to remember aspects tested Does not over test one division of MCA ie face, arm, and leg weaknessthis can lead to having many lacunar strokes being false +
72 Why VAN? And finally All of Oklahoma s BIG 6 Stroke Hospitals (those with EVT/IR) AGREED to utilize it!

73 Stroke Care is a TEAM Effort

74
75 VAN

76 So Where Do I Go?
77 Suggested Transport Guidelines Patient presents with Stroke like symptoms LSW < 4.5 hours VAN Positive + Transport time is < 30 minutes to a Stroke Center with EVT clot removal capability Transport to the nearest Stroke Center with EVT capabilities
78 Suggested Transport Guidelines Patient presents with Stroke like symptoms Transport to the nearest Stroke Center with EVT capabilities LSW > 4.5 hours but < 24 hours VAN Positive + Transport time is < 30 minutes to a Stroke Center with EVT clot removal capability
79 Suggested Transport Guidelines Patient presents with Stroke like symptoms Transport to the nearest ED with thrombolytic capabilities (tpa) LSW < 4.5 hours VAN Positive + Transport time > 30 minutes to a Stroke Center with EVT clot removal capability
80 Suggested Transport Guidelines Patient presents with Stroke like symptoms Transport to the nearest ED with thrombolytic capabilities (tpa); if there is a LVO present prepare x-fer LSW > 4.5 hours and < 24 hours VAN Positive + or VAN - negative Transport time > 30 minutes to a EVT facility If dx. with LVO transport to Stroke Center w/evt capability
81 Suggested Transport Guidelines Patient presents with Stroke like symptoms LSW > 24 hours Transport to the nearest ED
82 True DRIP & SHIP (to a EVT facility) +VAN/LVO Notification for transfer/ transport Out of the ED < 30 minutes after tpa bolus/gtt started Transfer team educated in transfer of those w/htn & Thrombolytic infusions Protocols for transfer
83 Involvement Code Stroke Committee Involvement QI Community/Citizen/ Ist Responders/ EMS/ED/ ICU/ Rehabilitation Support Groups EMS/ED/ICU/Allied Health lab, radiology, hospitalist, rehab

84
Stroke Systems of Care Claire Corbett, MMS, NRP Manager of Neurodiagnostics and Stroke Center New Hanover Regional Medical Center. What do we know?
 Stroke Systems of Care Claire Corbett, MMS, NRP Manager of Neurodiagnostics and Stroke Center New Hanover Regional Medical Center What do we know? Stroke: Time is Brain Shorter onset to treatment times
Stroke Systems of Care Claire Corbett, MMS, NRP Manager of Neurodiagnostics and Stroke Center New Hanover Regional Medical Center What do we know? Stroke: Time is Brain Shorter onset to treatment times
Statewide Acute Stroke Triage The Washington Story
 Statewide Acute Stroke Triage The Washington Story David Tirschwell, MD, MSc Medical Director of Comprehensive Stroke Care Professor, Department of Neurology UW Medicine Comprehensive Stroke Center at
Statewide Acute Stroke Triage The Washington Story David Tirschwell, MD, MSc Medical Director of Comprehensive Stroke Care Professor, Department of Neurology UW Medicine Comprehensive Stroke Center at
North Carolina Stroke Systems of Care Survey. Presented on behalf of the Integrating & Accessing Care Work Group of the Stroke Advisory Council
 North Carolina Stroke Systems of Care Survey Presented on behalf of the Integrating & Accessing Care Work Group of the Stroke Advisory Council Survey Overview The survey was developed with input from the
North Carolina Stroke Systems of Care Survey Presented on behalf of the Integrating & Accessing Care Work Group of the Stroke Advisory Council Survey Overview The survey was developed with input from the
Code Stroke in real life. Disclosures. Parkland Memorial Hospital. I have no disclosures. Has 1 million patient visits annually. Level 1 Trauma Center
 Code Stroke in real life Alejandro Magadán, M.D. University of Texas Southwestern Medical Center Medical Director for Stroke Parkland Memorial Hospital Disclosures I have no disclosures Parkland Memorial
Code Stroke in real life Alejandro Magadán, M.D. University of Texas Southwestern Medical Center Medical Director for Stroke Parkland Memorial Hospital Disclosures I have no disclosures Parkland Memorial
Transport of Suspected Large Vessel Occlusion: What s the Right Protocol for Bypass?
 Transport of Suspected Large Vessel Occlusion: What s the Right Protocol for Bypass? Andrew W. Asimos, MD, FACEP Medical Director, Carolinas Stroke Network Carolinas Healthcare System Professor, Department
Transport of Suspected Large Vessel Occlusion: What s the Right Protocol for Bypass? Andrew W. Asimos, MD, FACEP Medical Director, Carolinas Stroke Network Carolinas Healthcare System Professor, Department
ND STROKE Coordinators Case Studies. STEMI and Stroke Conference, Fargo, ND, August 5, 2014
 ND STROKE Coordinators Case Studies STEMI and Stroke Conference, Fargo, ND, August 5, 2014 STROKE Coordinator Case Study Essentia Health, Fargo Essentia Health Stroke Alert Process Within 24 hours of Last
ND STROKE Coordinators Case Studies STEMI and Stroke Conference, Fargo, ND, August 5, 2014 STROKE Coordinator Case Study Essentia Health, Fargo Essentia Health Stroke Alert Process Within 24 hours of Last
Mission: Lifeline Stroke Nebraska
 Mission: Lifeline Stroke Nebraska What is Mission: Lifeline Stroke? Mission: Lifeline Stroke is the American Heart Association s national initiative to transform stroke care by focusing efforts on connecting
Mission: Lifeline Stroke Nebraska What is Mission: Lifeline Stroke? Mission: Lifeline Stroke is the American Heart Association s national initiative to transform stroke care by focusing efforts on connecting
ELVO update. Michael Wilder, MD Director, Neurointerventional Program PeaceHealth Sacred Heart Springfield, Oregon
 ELVO update Michael Wilder, MD Director, Neurointerventional Program PeaceHealth Sacred Heart Springfield, Oregon Riverbend 24/7 thrombectomy ELVO alert Access PH PACU Anesthesia Goyal et al. Lancet. 2016
ELVO update Michael Wilder, MD Director, Neurointerventional Program PeaceHealth Sacred Heart Springfield, Oregon Riverbend 24/7 thrombectomy ELVO alert Access PH PACU Anesthesia Goyal et al. Lancet. 2016
Better identification of patients who may benefit from therapy
 Jon Jui MD, MPH Large Vessel Occlusion Low rates of re-canalization after tpa Only 25 % of large vessel strokes re-canalization after tpa Newer invasive techniques Solitaire vs Merci Better identification
Jon Jui MD, MPH Large Vessel Occlusion Low rates of re-canalization after tpa Only 25 % of large vessel strokes re-canalization after tpa Newer invasive techniques Solitaire vs Merci Better identification
Acute Stroke Identification and Treatment
 Acute Stroke Identification and Treatment James S. McKinney, MD, FAHA Medical Director, NHRMC Stroke Center SE NC is located in the buckle of the Stroke Belt, seeing the highest stroke incidence and mortality
Acute Stroke Identification and Treatment James S. McKinney, MD, FAHA Medical Director, NHRMC Stroke Center SE NC is located in the buckle of the Stroke Belt, seeing the highest stroke incidence and mortality
ABNORMAL STROKE EXAM FINDINGS:
 Stroke Assessment Scenario Case Information PATIENT INFORMATION: 68-year-old male patient complaining of left sided weakness and an unsteady gait. Reported last normal time 3 minutes prior to EMS arrival
Stroke Assessment Scenario Case Information PATIENT INFORMATION: 68-year-old male patient complaining of left sided weakness and an unsteady gait. Reported last normal time 3 minutes prior to EMS arrival
Update on Neurologic Emergencies
 Update on Neurologic Emergencies KAREN GREENBERG, DO, FACOEP ARIA JEFFERSON HEALTH SYSTEM VIRTUA HEALTH SYSTEM KENNEDY HEALTH SYSTEM Disclosures Genentech Speakers Bureau I have disclosed a relevant relationship
Update on Neurologic Emergencies KAREN GREENBERG, DO, FACOEP ARIA JEFFERSON HEALTH SYSTEM VIRTUA HEALTH SYSTEM KENNEDY HEALTH SYSTEM Disclosures Genentech Speakers Bureau I have disclosed a relevant relationship
EVOLUTION IN SYSTEMS OF STROKE CARE RIDWAN LIN, MD, PHD STROKE & INTERVENTIONAL NEUROLOGY BROWARD HEALTH
 EVOLUTION IN SYSTEMS OF STROKE CARE RIDWAN LIN, MD, PHD STROKE & INTERVENTIONAL NEUROLOGY BROWARD HEALTH STROKE SYSTEMS OF CARE: 7. Secondary prevention 1. Primary prevention Patient 3. Emergency transport
EVOLUTION IN SYSTEMS OF STROKE CARE RIDWAN LIN, MD, PHD STROKE & INTERVENTIONAL NEUROLOGY BROWARD HEALTH STROKE SYSTEMS OF CARE: 7. Secondary prevention 1. Primary prevention Patient 3. Emergency transport
I n t e r h o s p i t a l Tr a n s fe r s o f t h e A c u t e S t r o ke Pat i e n t E M S G r a n d Ro u n d s : Febr u a r y 2 1,
 I n t e r h o s p i t a l Tr a n s fe r s o f t h e A c u t e S t r o ke Pat i e n t E M S G r a n d Ro u n d s : Febr u a r y 2 1, 2 0 1 8 Elaine Skalabrin, MD S t r o k e M e d i c a l D i r e c t o
I n t e r h o s p i t a l Tr a n s fe r s o f t h e A c u t e S t r o ke Pat i e n t E M S G r a n d Ro u n d s : Febr u a r y 2 1, 2 0 1 8 Elaine Skalabrin, MD S t r o k e M e d i c a l D i r e c t o
Code Stroke Intervention: Endovascular Therapies for Stroke J. DIEGO LOZANO MD INTERVENTIONAL NEURORADIOLOGY
 Code Stroke Intervention: Endovascular Therapies for Stroke J. DIEGO LOZANO MD INTERVENTIONAL NEURORADIOLOGY Disclosures None Part A. Objectives Epidemiology of AIS and of ELVO Concept: Acute Ischemic
Code Stroke Intervention: Endovascular Therapies for Stroke J. DIEGO LOZANO MD INTERVENTIONAL NEURORADIOLOGY Disclosures None Part A. Objectives Epidemiology of AIS and of ELVO Concept: Acute Ischemic
Top 5 Big Things in Acute Stroke Care! Raymond W. Grams II, DO Vascular Neurology Stroke Medical Director DRMC, Intermountain Healthcare
 Top 5 Big Things in Acute Stroke Care! Raymond W. Grams II, DO Vascular Neurology Stroke Medical Director DRMC, Intermountain Healthcare Late Time Window Endovascular Trials 48.6% WITH intervention vs
Top 5 Big Things in Acute Stroke Care! Raymond W. Grams II, DO Vascular Neurology Stroke Medical Director DRMC, Intermountain Healthcare Late Time Window Endovascular Trials 48.6% WITH intervention vs
Endovascular Treatment Updates in Stroke Care
 Endovascular Treatment Updates in Stroke Care Autumn Graham, MD April 6-10, 2017 Phoenix, AZ Endovascular Treatment Updates in Stroke Care Autumn Graham, MD Associate Professor of Clinical Emergency Medicine
Endovascular Treatment Updates in Stroke Care Autumn Graham, MD April 6-10, 2017 Phoenix, AZ Endovascular Treatment Updates in Stroke Care Autumn Graham, MD Associate Professor of Clinical Emergency Medicine
CT Perfusion is Essential for Stroke Triage. Maarten Lansberg, MD PhD Associate Professor of Neurology Stanford University, Stanford Stroke Center
 CT Perfusion is Essential for Stroke Triage Maarten Lansberg, MD PhD Associate Professor of Neurology Stanford University, Stanford Stroke Center CT Perfusion is Essential for Stroke Triage Disclosures:
CT Perfusion is Essential for Stroke Triage Maarten Lansberg, MD PhD Associate Professor of Neurology Stanford University, Stanford Stroke Center CT Perfusion is Essential for Stroke Triage Disclosures:
Stroke in the Rural Setting: How You Can Make A Difference. Susie Fisher, RN, BSN Program Manager Providence Stroke Center Portland, OR
 Stroke in the Rural Setting: How You Can Make A Difference. Susie Fisher, RN, BSN Program Manager Providence Stroke Center Portland, OR Outline State Statistics The Oregon Problem Time & Treatments Steps
Stroke in the Rural Setting: How You Can Make A Difference. Susie Fisher, RN, BSN Program Manager Providence Stroke Center Portland, OR Outline State Statistics The Oregon Problem Time & Treatments Steps
what do the numbers really mean? NIHSS Timothy Hehr, RN MA Stroke Program Outreach Coordinator Allina Health
 what do the numbers really mean? NIHSS Timothy Hehr, RN MA Stroke Program Outreach Coordinator Allina Health NIHSS The National Institutes of Health Stroke Scale (NIHSS) is a tool used to objectively quantify
what do the numbers really mean? NIHSS Timothy Hehr, RN MA Stroke Program Outreach Coordinator Allina Health NIHSS The National Institutes of Health Stroke Scale (NIHSS) is a tool used to objectively quantify
WHY TIMELINESS MATTERS. W&M Wren Association Lecture Series
 WHY TIMELINESS MATTERS April 10, 2018 W&M Wren Association Lecture Series Pankajavalli Ramakrishnan, M.D., Ph.D. Stroke Neurologist and Neurointerventionalist Riverside Regional Medical Center Comprehensive
WHY TIMELINESS MATTERS April 10, 2018 W&M Wren Association Lecture Series Pankajavalli Ramakrishnan, M.D., Ph.D. Stroke Neurologist and Neurointerventionalist Riverside Regional Medical Center Comprehensive
Stroke: The First Critical Hour. Alina Candal, RN, PCC, MICN Kevin Andruss, MD, FACEP
 Stroke: The First Critical Hour Alina Candal, RN, PCC, MICN Kevin Andruss, MD, FACEP Disclosures We have no actual or potential conflicts of interest in relation to this presentation. Objectives Discuss
Stroke: The First Critical Hour Alina Candal, RN, PCC, MICN Kevin Andruss, MD, FACEP Disclosures We have no actual or potential conflicts of interest in relation to this presentation. Objectives Discuss
Code Stroke!! Amit Kansara, MD, FAHA. Joint EMS Conference Providence Brain and Spine Institute Providence Heart and Vascular Institute
 Code Stroke!! Amit Kansara, MD, FAHA Joint EMS Conference Providence Brain and Spine Institute Providence Heart and Vascular Institute February 22, 2019 Patient History: Dispatch 20:45: You are dispatched
Code Stroke!! Amit Kansara, MD, FAHA Joint EMS Conference Providence Brain and Spine Institute Providence Heart and Vascular Institute February 22, 2019 Patient History: Dispatch 20:45: You are dispatched
Drano vs. MR CLEAN Review of New Endovascular Therapy for Acute Ischemic Stroke Patients
 Drano vs. MR CLEAN Review of New Endovascular Therapy for Acute Ischemic Stroke Patients Peter Panagos, MD, FACEP, FAHA Associate Professor Emergency Medicine and Neurology Washington University School
Drano vs. MR CLEAN Review of New Endovascular Therapy for Acute Ischemic Stroke Patients Peter Panagos, MD, FACEP, FAHA Associate Professor Emergency Medicine and Neurology Washington University School
Slide 1. Slide 2. Slide 3 EMS STROKE CARE AND CSTAT OREGON STROKE NETWORK CONFERENCE 2018 SHAWN WOOD, CLINICAL MANAGER DISCLOSURES MY PATH TO EMS
 Slide 1 EMS STROKE CARE AND CSTAT OREGON STROKE NETWORK CONFERENCE 2018 SHAWN WOOD, CLINICAL MANAGER METRO WEST AMBULANCE Slide 2 DISCLOSURES No Financial Conflicts. I work as the Clinical Manager for
Slide 1 EMS STROKE CARE AND CSTAT OREGON STROKE NETWORK CONFERENCE 2018 SHAWN WOOD, CLINICAL MANAGER METRO WEST AMBULANCE Slide 2 DISCLOSURES No Financial Conflicts. I work as the Clinical Manager for
Code Stroke Optimizing Stroke Care in the Field: The Alberta Experience
 Code Stroke Optimizing Stroke Care in the Field: The Alberta Experience June 1st, 2018 Thomas Jeerakathil BSc, MD, MSc, FRCP(C) Professor Division of Neurology University of Alberta Northern Stroke Lead
Code Stroke Optimizing Stroke Care in the Field: The Alberta Experience June 1st, 2018 Thomas Jeerakathil BSc, MD, MSc, FRCP(C) Professor Division of Neurology University of Alberta Northern Stroke Lead
Shands at the University of Florida Stroke Program
 Shands at the University of Florida Stroke Program The only Comprehensive Stroke Center in north central Florida as designated by the Florida Agency for Health Care Administration. To transfer a stroke
Shands at the University of Florida Stroke Program The only Comprehensive Stroke Center in north central Florida as designated by the Florida Agency for Health Care Administration. To transfer a stroke
Size Matters: Differentiating Large Vessel Occlusion (LVO) and Small Vessel Occlusion (SVO) in Stroke
 and Small Vessel Occlusion (SVO) in Stroke") Size Matters: Differentiating Large Vessel Occlusion (LVO) and Small Vessel Occlusion (SVO) in Stroke Charles E. Romero, M.D. UPMC Hamot Great Lakes Neurosurgery & Neurointervention Case 1 83 yo RH F with
Size Matters: Differentiating Large Vessel Occlusion (LVO) and Small Vessel Occlusion (SVO) in Stroke Charles E. Romero, M.D. UPMC Hamot Great Lakes Neurosurgery & Neurointervention Case 1 83 yo RH F with
WV Appalachian Stroke Network 2016 State Stroke Conference The Big Decision Packaging the Patient for Transfer
 WV Appalachian Stroke Network 2016 State Stroke Conference The Big Decision Packaging the Patient for Transfer Dr. Jim Kyle, FACSM, FAAFP Regional Medical Director WVOEMS Executive Director, The Kyle Group
WV Appalachian Stroke Network 2016 State Stroke Conference The Big Decision Packaging the Patient for Transfer Dr. Jim Kyle, FACSM, FAAFP Regional Medical Director WVOEMS Executive Director, The Kyle Group
Case 1 5/26/2017 ENDOVASCULAR MECHANICAL THROMBECTOMY IN PATIENTS WITH ACUTE ISCHEMIC STROKE
 ENDOVASCULAR MECHANICAL THROMBECTOMY IN PATIENTS WITH ACUTE ISCHEMIC STROKE Rhonda Whiteman Racing Against the Clock Workshop June 1, 2017 Objectives To discuss the hyperacute ischemic stroke management
ENDOVASCULAR MECHANICAL THROMBECTOMY IN PATIENTS WITH ACUTE ISCHEMIC STROKE Rhonda Whiteman Racing Against the Clock Workshop June 1, 2017 Objectives To discuss the hyperacute ischemic stroke management
Acute Ischaemic Stroke Pathways Drip and Ship
 Acute Ischaemic Stroke Pathways Drip and Ship Professor Gary Ford Chief Executive Officer, Oxford Academic Health Science Network Consultant Stroke Physician, Oxford University Hospitals Visiting Professor
Acute Ischaemic Stroke Pathways Drip and Ship Professor Gary Ford Chief Executive Officer, Oxford Academic Health Science Network Consultant Stroke Physician, Oxford University Hospitals Visiting Professor
Interventional Treatment of Stroke
 Interventional Treatment of Stroke Andrew F. Ducruet, MD Barrow Neurological Institute 2018 BNI Stroke Rehab Symposium October 13, 2018 Disclosures Consultant: Medtronic, Penumbra, Cerenovus Lecture Overview
Interventional Treatment of Stroke Andrew F. Ducruet, MD Barrow Neurological Institute 2018 BNI Stroke Rehab Symposium October 13, 2018 Disclosures Consultant: Medtronic, Penumbra, Cerenovus Lecture Overview
Stroke Update Elaine J. Skalabrin MD Medical Director and Neurohospitalist Sacred Heart Medical Center Stroke Center
 Stroke Update 2015 Elaine J. Skalabrin MD Medical Director and Neurohospitalist Sacred Heart Medical Center Stroke Center Objectives 1. Review successes in systems of care approach to acute ischemic stroke
Stroke Update 2015 Elaine J. Skalabrin MD Medical Director and Neurohospitalist Sacred Heart Medical Center Stroke Center Objectives 1. Review successes in systems of care approach to acute ischemic stroke
Page 1 CVHNS Bulletin, Volume 13, Issue 1, Spring, 2018
 Page 1 CVHNS Bulletin, Volume 13, Issue 1, Spring, 2018 The Bulletin Welcome to the Cardiovascular Health Nova Scotia (CVHNS) e-mail bulletin, produced 3 times annually. The Bulletin has been created to
Page 1 CVHNS Bulletin, Volume 13, Issue 1, Spring, 2018 The Bulletin Welcome to the Cardiovascular Health Nova Scotia (CVHNS) e-mail bulletin, produced 3 times annually. The Bulletin has been created to
It s Not All One Sided. James Smith, MD (Smitty)
") It s Not All One Sided James Smith, MD (Smitty) Disclosures Chair, NE State EMS Board Medical Director, Emergency Services, GPH Medical Director, GPH LifeNet, NPFD, Maxwell, Tryon, Chase County, NP Rec
It s Not All One Sided James Smith, MD (Smitty) Disclosures Chair, NE State EMS Board Medical Director, Emergency Services, GPH Medical Director, GPH LifeNet, NPFD, Maxwell, Tryon, Chase County, NP Rec
Acute Stroke Rescue and Recovery
 Acute Stroke Rescue and Recovery Qaisar A. Shah, MD Director, Neurointerventional and Neurocritical care Nancy Arena Gogal,, RN Manager Cath/EPS/Neuro lab AMH Stroke Program Evolution 1997: Stroke Program
Acute Stroke Rescue and Recovery Qaisar A. Shah, MD Director, Neurointerventional and Neurocritical care Nancy Arena Gogal,, RN Manager Cath/EPS/Neuro lab AMH Stroke Program Evolution 1997: Stroke Program
Chinook Regional Hospital Stroke Alert Cases
 Chinook Regional Hospital Stroke Alert Cases Background 53,260 ED Department visits last year Stroke Alert started October 19, 2015 106 minutes Median DTN at beginning of QuiCR project 73 Stroke Alert
Chinook Regional Hospital Stroke Alert Cases Background 53,260 ED Department visits last year Stroke Alert started October 19, 2015 106 minutes Median DTN at beginning of QuiCR project 73 Stroke Alert
Getting the Right Stroke Patient to the Right Hospital: Pre-hospital Assessment Tools
 Getting the Right Stroke Patient to the Right Hospital: Pre-hospital Assessment Tools Francis X Guyette, MD, MPH Associate Professor of Emergency Medicine University of Pittsburgh School of Medicine Medical
Getting the Right Stroke Patient to the Right Hospital: Pre-hospital Assessment Tools Francis X Guyette, MD, MPH Associate Professor of Emergency Medicine University of Pittsburgh School of Medicine Medical
Advanced Stroke Care in the context of the Cardiovascular Patient
 EASTERN MAINE MEDICAL CENTER Advanced Stroke Care in the context of the Cardiovascular Patient Advancing Science in Cardiovascular Care Samoset Conference NOV 8, 2018 Dr. Gillian Gordon Perue Conflict
EASTERN MAINE MEDICAL CENTER Advanced Stroke Care in the context of the Cardiovascular Patient Advancing Science in Cardiovascular Care Samoset Conference NOV 8, 2018 Dr. Gillian Gordon Perue Conflict
Stroke Belt Consortium
 Field Triage And Diversion of Acute Stroke Charles Sand, MD Stroke Belt Consortium 10/26/12 WCF EMS Acute Stroke Advisory Committee Formed 2001 5 Original members Now > 100 members interdisciplinary expertise
Field Triage And Diversion of Acute Stroke Charles Sand, MD Stroke Belt Consortium 10/26/12 WCF EMS Acute Stroke Advisory Committee Formed 2001 5 Original members Now > 100 members interdisciplinary expertise
Alex Abou-Chebl, MD Associate Professor of Neurology and Neurosurgery Director of Neurointerventional Services Director of Vascular and
 Alex Abou-Chebl, MD Associate Professor of Neurology and Neurosurgery Director of Neurointerventional Services Director of Vascular and Interventional Neurology Fellowships University of Louisville School
Alex Abou-Chebl, MD Associate Professor of Neurology and Neurosurgery Director of Neurointerventional Services Director of Vascular and Interventional Neurology Fellowships University of Louisville School
Rural emergency department best practice for treatment of acute ischemic stroke
 Rural emergency department best practice for treatment of acute ischemic stroke Aubrey J. Hoye, DO Ministry Howard Young Medical Center, Woodruff, WI Ministry Eagle River Memorial Hospital, Eagle River,
Rural emergency department best practice for treatment of acute ischemic stroke Aubrey J. Hoye, DO Ministry Howard Young Medical Center, Woodruff, WI Ministry Eagle River Memorial Hospital, Eagle River,
5/31/2018. Interventional Therapies that Expand Time Windows for Acute Ischemic Stroke Treatment. Disclosures. Impact of clot burden
 Good Outcome (%) Rankin 0-2 at 90 days 5/31/2018 Interventional Therapies that Expand Time Windows for Acute Ischemic Stroke Treatment Disclosures Cerenovus: I am on Executive Committee for ARISE2 Trial
Good Outcome (%) Rankin 0-2 at 90 days 5/31/2018 Interventional Therapies that Expand Time Windows for Acute Ischemic Stroke Treatment Disclosures Cerenovus: I am on Executive Committee for ARISE2 Trial
Stroke Clinical Trials Update Transitioning to an Anatomic Diagnosis in Ischemic Stroke
 Stroke Clinical Trials Update Transitioning to an Anatomic Diagnosis in Ischemic Stroke Alexander A. Khalessi MD MS Director of Endovascular Neurosurgery Surgical Director of NeuroCritical Care University
Stroke Clinical Trials Update Transitioning to an Anatomic Diagnosis in Ischemic Stroke Alexander A. Khalessi MD MS Director of Endovascular Neurosurgery Surgical Director of NeuroCritical Care University
Update on Early Acute Ischemic Stroke Interventions
 Update on Early Acute Ischemic Stroke Interventions Diana Goodman MD Lead Neurohospitalist Maine Medical Center Assistant Professor of Neurology, Tufts University School of Medicine I have no disclosures
Update on Early Acute Ischemic Stroke Interventions Diana Goodman MD Lead Neurohospitalist Maine Medical Center Assistant Professor of Neurology, Tufts University School of Medicine I have no disclosures
AMSER Case of the Month: March 2019
 AMSER Case of the Month: March 2019 62 year-old male with left-sided weakness Ashley Graziano OMS IV, Lake Erie College of Osteopathic Medicine Erik Yannone MD, Charles Q. Li MD, Warren Chang MD, Matthew
AMSER Case of the Month: March 2019 62 year-old male with left-sided weakness Ashley Graziano OMS IV, Lake Erie College of Osteopathic Medicine Erik Yannone MD, Charles Q. Li MD, Warren Chang MD, Matthew
DISCLOSURES HUY TRAN MD UNM DEPARTMENT OF NEUROLOGY AND NEUROSURGERY NO DISCLOSURES
 DISCLOSURES ANDREW HARRELL MD FAEMS UNM DEPARTMENT OF EMERGENCY MEDICINEUNM EMS MEDICAL DIRECTION CONSORTIUM MEDICAL DIRECTOR, ALBUQUERQUE FIRE DEPARTMENT MEDICAL DIRECTOR, GRAND CANYON NATIONAL PARK TEMS
DISCLOSURES ANDREW HARRELL MD FAEMS UNM DEPARTMENT OF EMERGENCY MEDICINEUNM EMS MEDICAL DIRECTION CONSORTIUM MEDICAL DIRECTOR, ALBUQUERQUE FIRE DEPARTMENT MEDICAL DIRECTOR, GRAND CANYON NATIONAL PARK TEMS
Stroke Systems of Care
 Comprehensive Stroke and Cerebrovascular Center Stroke Systems of Care Dana Stradling RN MSN CNRN UC Irvine Stroke Manager dstradli@uci.edu Why Stroke Systems? No. 4 th 5 th cause of death in the U.S.
Comprehensive Stroke and Cerebrovascular Center Stroke Systems of Care Dana Stradling RN MSN CNRN UC Irvine Stroke Manager dstradli@uci.edu Why Stroke Systems? No. 4 th 5 th cause of death in the U.S.
Inside Your Patient s Brain Michelle Peterson, APRN, CNP Centracare Stroke and Vascular Neurology
 Inside Your Patient s Brain Michelle Peterson, APRN, CNP Centracare Stroke and Vascular Neurology Activity Everyone stand up, raise your right hand, tell your neighbors your name 1 What part of the brain
Inside Your Patient s Brain Michelle Peterson, APRN, CNP Centracare Stroke and Vascular Neurology Activity Everyone stand up, raise your right hand, tell your neighbors your name 1 What part of the brain
Acute Stroke Systems of Care Optimizing Patient Care and Improving Outcomes
 Acute Stroke Systems of Care Optimizing Patient Care and Improving Outcomes Laurie Paletz, BSN PHN RN-BC SCRN Cedars-Sinai Medical Center Stroke Program Coordinator Disclosures Speaker s Bureau: Genentech
Acute Stroke Systems of Care Optimizing Patient Care and Improving Outcomes Laurie Paletz, BSN PHN RN-BC SCRN Cedars-Sinai Medical Center Stroke Program Coordinator Disclosures Speaker s Bureau: Genentech
Transport of Suspected Large Vessel Occlusion: What s the Right Protocol for Bypass?
 Transport of Suspected Large Vessel Occlusion: What s the Right Protocol for Bypass? Andrew W. Asimos, MD, FACEP Medical Director, Carolinas Stroke Network Carolinas Healthcare System Professor, Department
Transport of Suspected Large Vessel Occlusion: What s the Right Protocol for Bypass? Andrew W. Asimos, MD, FACEP Medical Director, Carolinas Stroke Network Carolinas Healthcare System Professor, Department
The DAWN of a New Era for Wake-up Stroke
 The DAWN of a New Era for Wake-up Stroke Alan H. Yee, D.O. Stroke and Critical Care Neurology Department of Neurology University of California Davis Medical Center Objectives Review Epidemiology and Natural
The DAWN of a New Era for Wake-up Stroke Alan H. Yee, D.O. Stroke and Critical Care Neurology Department of Neurology University of California Davis Medical Center Objectives Review Epidemiology and Natural
UPDATES IN INTRACRANIAL INTERVENTION Jordan Taylor DO Metro Health Neurology 2015
 UPDATES IN INTRACRANIAL INTERVENTION Jordan Taylor DO Metro Health Neurology 2015 NEW STUDIES FOR 2015 MR CLEAN ESCAPE EXTEND-IA REVASCAT SWIFT PRIME RECOGNIZED LIMITATIONS IV Alteplase proven benefit
UPDATES IN INTRACRANIAL INTERVENTION Jordan Taylor DO Metro Health Neurology 2015 NEW STUDIES FOR 2015 MR CLEAN ESCAPE EXTEND-IA REVASCAT SWIFT PRIME RECOGNIZED LIMITATIONS IV Alteplase proven benefit
Endovascular Neurointervention in Cerebral Ischemia
 Endovascular Neurointervention in Cerebral Ischemia Beyond Thrombolytics Curtis A. Given II, MD Co-Director, Neurointerventional Services Baptist Physician Lexington 72 y/o female with a recent diagnosis
Endovascular Neurointervention in Cerebral Ischemia Beyond Thrombolytics Curtis A. Given II, MD Co-Director, Neurointerventional Services Baptist Physician Lexington 72 y/o female with a recent diagnosis
KPNC Stroke EXPRESS EXpediting the PRocess of Evaluating & Stopping Stroke
 KPNC Stroke EXPRESS EXpediting the PRocess of Evaluating & Stopping Stroke Jeffrey G. Klingman, MD 1 Disclosures None 75% DTN < 60 50% DTN < 45 Why should we care about DTN?: Time is brain 2 million nerve
KPNC Stroke EXPRESS EXpediting the PRocess of Evaluating & Stopping Stroke Jeffrey G. Klingman, MD 1 Disclosures None 75% DTN < 60 50% DTN < 45 Why should we care about DTN?: Time is brain 2 million nerve
: STROKE. other pertinent information such as recent trauma, illicit drug use, pertinent medical history or use of oral contraceptives.
 INTRODUCTION A cerebral vascular accident (CVA) or stroke is a lack of blood supply to the brain as a result of either ischemia or hemorrhage. 80% of CVAs are a result of ischemia (embolic or thrombotic)
INTRODUCTION A cerebral vascular accident (CVA) or stroke is a lack of blood supply to the brain as a result of either ischemia or hemorrhage. 80% of CVAs are a result of ischemia (embolic or thrombotic)
Interventions to Improve Acute Ischemic Stroke Treatment Times
 Baptist Health South Florida Scholarly Commons @ Baptist Health South Florida All Publications 3-19-2018 Interventions to Improve Acute Ischemic Stroke Treatment Times Jayme Strauss Baptist Hospital of
Baptist Health South Florida Scholarly Commons @ Baptist Health South Florida All Publications 3-19-2018 Interventions to Improve Acute Ischemic Stroke Treatment Times Jayme Strauss Baptist Hospital of
ACUTE ISCHEMIC STROKE
 ENDOVASCULAR MECHANICAL THROMBECTOMY IN PATIENTS WITH ACUTE ISCHEMIC STROKE HHS Stroke Annual Review March 7 and March 8, 2018 Objectives To review the stroke endovascular mechanical thrombectomy evidence
ENDOVASCULAR MECHANICAL THROMBECTOMY IN PATIENTS WITH ACUTE ISCHEMIC STROKE HHS Stroke Annual Review March 7 and March 8, 2018 Objectives To review the stroke endovascular mechanical thrombectomy evidence
Stroke: clinical presentations, symptoms and signs
 Stroke: clinical presentations, symptoms and signs Professor Peter Sandercock University of Edinburgh EAN teaching course Burkina Faso 8 th November 2017 Clinical diagnosis is important to Ensure stroke
Stroke: clinical presentations, symptoms and signs Professor Peter Sandercock University of Edinburgh EAN teaching course Burkina Faso 8 th November 2017 Clinical diagnosis is important to Ensure stroke
Mechanical thrombectomy in Plymouth. Will Adams. Will Adams
 Mechanical thrombectomy in Plymouth Will Adams Will Adams History Intra-arterial intervention 1995 (NINDS) iv tpa improved clinical outcome in patients treated within 3 hours of ictus but limited recanalisation
Mechanical thrombectomy in Plymouth Will Adams Will Adams History Intra-arterial intervention 1995 (NINDS) iv tpa improved clinical outcome in patients treated within 3 hours of ictus but limited recanalisation
11/1/2018. Disclosure. Imaging in Acute Ischemic Stroke 2018 Neuro Symposium. Is NCCT good enough? Keystone Heart Consultant, Stock Options
 Disclosure Imaging in Acute Ischemic Stroke 2018 Neuro Symposium Keystone Heart Consultant, Stock Options Kevin Abrams, M.D. Chief of Radiology Medical Director of Neuroradiology Baptist Hospital, Miami,
Disclosure Imaging in Acute Ischemic Stroke 2018 Neuro Symposium Keystone Heart Consultant, Stock Options Kevin Abrams, M.D. Chief of Radiology Medical Director of Neuroradiology Baptist Hospital, Miami,
ACCESS CENTER:
 ACCESS CENTER: 1-877-367-8855 Emergency Specialty Services: BRAIN ATTACK Criteria: Stroke symptom onset time less than 6 hours Referring Emergency Department Patient Information Data: Time last known normal:
ACCESS CENTER: 1-877-367-8855 Emergency Specialty Services: BRAIN ATTACK Criteria: Stroke symptom onset time less than 6 hours Referring Emergency Department Patient Information Data: Time last known normal:
ACUTE STROKE IMAGING
 ACUTE STROKE IMAGING Mahesh V. Jayaraman M.D. Director, Inter ventional Neuroradiology Associate Professor Depar tments of Diagnostic Imaging and Neurosurger y Alper t Medical School at Brown University
ACUTE STROKE IMAGING Mahesh V. Jayaraman M.D. Director, Inter ventional Neuroradiology Associate Professor Depar tments of Diagnostic Imaging and Neurosurger y Alper t Medical School at Brown University
The Language of Stroke
 The Language of Stroke Examination / Imaging / Diagnosis / Treatment Dr Suzanne Busch A lot of letters! CBF CVA ICH CVD CBV DWI US MRI/MRA CAA CTA CTP ICA MCA SAH WMD TIA MCA Agnosia A lot of big words!
The Language of Stroke Examination / Imaging / Diagnosis / Treatment Dr Suzanne Busch A lot of letters! CBF CVA ICH CVD CBV DWI US MRI/MRA CAA CTA CTP ICA MCA SAH WMD TIA MCA Agnosia A lot of big words!
Objectives. Stroke Facts 2/27/2015. EMS in Stroke Care: A Critical Partnership
 EMS in Stroke Care: A Critical Partnership Spokane County EMS Objectives Identify the types and time limitations for acute ischemic stroke treatment options Identify the importance of early identification
EMS in Stroke Care: A Critical Partnership Spokane County EMS Objectives Identify the types and time limitations for acute ischemic stroke treatment options Identify the importance of early identification
Stroke School for Internists Part 1
 Stroke School for Internists Part 1 November 4, 2017 Dr. Albert Jin Dr. Gurpreet Jaswal Disclosures I receive a stipend for my role as Medical Director of the Stroke Network of SEO I have no commercial
Stroke School for Internists Part 1 November 4, 2017 Dr. Albert Jin Dr. Gurpreet Jaswal Disclosures I receive a stipend for my role as Medical Director of the Stroke Network of SEO I have no commercial
ACUTE STROKE INTERVENTION: THE ROLE OF THROMBECTOMY AND IA LYSIS
 Associate Professor of Neurology Director of Neurointerventional Services University of Louisville School of Medicine ACUTE STROKE INTERVENTION: THE ROLE OF THROMBECTOMY AND IA LYSIS Conflict of Interest
Associate Professor of Neurology Director of Neurointerventional Services University of Louisville School of Medicine ACUTE STROKE INTERVENTION: THE ROLE OF THROMBECTOMY AND IA LYSIS Conflict of Interest
Endovascular Treatment for Acute Ischemic Stroke: Curtis A. Given II, MD Co-Director, Neurointerventional Services Baptist Physician Lexington
 Endovascular Treatment for Acute Ischemic Stroke: Curtis A. Given II, MD Co-Director, Neurointerventional Services Baptist Physician Lexington Disclosures: SWIFT PRIME site (Medtronic) Physician Proctor
Endovascular Treatment for Acute Ischemic Stroke: Curtis A. Given II, MD Co-Director, Neurointerventional Services Baptist Physician Lexington Disclosures: SWIFT PRIME site (Medtronic) Physician Proctor
Mechanical Endovascular Reperfusion Therapy
 Get With the Guidelines Stroke Mechanical Endovascular Reperfusion Therapy February 1, 2017 Speaker Lee H. Schwamm, MD Executive Vice Chairman and Director of Stroke/TeleStroke Services, Department of
Get With the Guidelines Stroke Mechanical Endovascular Reperfusion Therapy February 1, 2017 Speaker Lee H. Schwamm, MD Executive Vice Chairman and Director of Stroke/TeleStroke Services, Department of
Unclogging The Pipes. Zahraa Rabeeah MD Chief Resident February 9,2018
 Unclogging The Pipes Zahraa Rabeeah MD Chief Resident February 9,2018 Please join Polleverywhere by texting: ZRABEEAH894 to 37607 Disclosures None Objectives Delineate the differences between TPA vs thrombectomy
Unclogging The Pipes Zahraa Rabeeah MD Chief Resident February 9,2018 Please join Polleverywhere by texting: ZRABEEAH894 to 37607 Disclosures None Objectives Delineate the differences between TPA vs thrombectomy
o Unenhanced Head CT
 Drip & Ship Protocol Acute Stroke Ready Hospital (ASRH) Duluth Area Primary Stroke Center (St. Luke s & St. Mary s Essentia) PATIENT LABEL Patient displays strokelike symptoms EMS/ED CSS > 0 Glucose >
Drip & Ship Protocol Acute Stroke Ready Hospital (ASRH) Duluth Area Primary Stroke Center (St. Luke s & St. Mary s Essentia) PATIENT LABEL Patient displays strokelike symptoms EMS/ED CSS > 0 Glucose >
IMAGING IN ACUTE ISCHEMIC STROKE
 IMAGING IN ACUTE ISCHEMIC STROKE Timo Krings MD, PhD, FRCP (C) Professor of Radiology & Surgery Braley Chair of Neuroradiology, Chief and Program Director of Diagnostic and Interventional Neuroradiology;
IMAGING IN ACUTE ISCHEMIC STROKE Timo Krings MD, PhD, FRCP (C) Professor of Radiology & Surgery Braley Chair of Neuroradiology, Chief and Program Director of Diagnostic and Interventional Neuroradiology;
Where are we heading and where are the big challenges?
 Where are we heading and where are the big challenges? Christopher Levi Neurologist, John Hunter Hospital, Newcastle & Liverpool Hospital, Sydney Executive Director, Sydney Partnership for Health Education
Where are we heading and where are the big challenges? Christopher Levi Neurologist, John Hunter Hospital, Newcastle & Liverpool Hospital, Sydney Executive Director, Sydney Partnership for Health Education
SARASOTA MEMORIAL HOSPITAL. NURSING PROCEDURE NATIONAL INSTITUTE OF HEALTH STROKE SCALE (neu04) Nursing
 Nursing") SARASOTA MEMORIAL HOSPITAL TITLE: ISSUED FOR: NURSING PROCEDURE NATIONAL INSTITUTE OF HEALTH Nursing DATE: REVIEWED: PAGES: PS1094 7/01 3/18 1 of 5 RESPONSIBILITY: RN, LPN PURPOSE: OBJECTIVE: DEFINITION:
SARASOTA MEMORIAL HOSPITAL TITLE: ISSUED FOR: NURSING PROCEDURE NATIONAL INSTITUTE OF HEALTH Nursing DATE: REVIEWED: PAGES: PS1094 7/01 3/18 1 of 5 RESPONSIBILITY: RN, LPN PURPOSE: OBJECTIVE: DEFINITION:
9/18/16. Setting: Community ED, 30k admissions per year Time: Friday night, 11pm. CC: Syncope
 William A. Knight IV MD, FACEP Associate Professor Emergency Medicine & Neurosurgery University of Cincinnati September 21, 2016 (William.knight@uc.edu) ED as the Front Door Spectrum of care with Endovascular
William A. Knight IV MD, FACEP Associate Professor Emergency Medicine & Neurosurgery University of Cincinnati September 21, 2016 (William.knight@uc.edu) ED as the Front Door Spectrum of care with Endovascular
Pre-Hospital Stroke Care: Bringing It To The Street. by Bob Atkins, NREMT-Paramedic AEMD EMS Director Bedford Regional Medical Center
 Pre-Hospital Stroke Care: Bringing It To The Street by Bob Atkins, NREMT-Paramedic AEMD EMS Director Bedford Regional Medical Center Overview/Objectives Explain the reasons or rational behind the importance
Pre-Hospital Stroke Care: Bringing It To The Street by Bob Atkins, NREMT-Paramedic AEMD EMS Director Bedford Regional Medical Center Overview/Objectives Explain the reasons or rational behind the importance
Advances in Neuro-Endovascular Care for Acute Stroke
 Advances in Neuro-Endovascular Care for Acute Stroke Ciarán J. Powers, MD, PhD, FAANS Associate Professor Program Director Department of Neurological Surgery Surgical Director Comprehensive Stroke Center
Advances in Neuro-Endovascular Care for Acute Stroke Ciarán J. Powers, MD, PhD, FAANS Associate Professor Program Director Department of Neurological Surgery Surgical Director Comprehensive Stroke Center
Primary Stroke Center Acute Stroke Transfer Guidelines When to Consider a Transfer:
 When to Consider a Transfer: Hemorrhagic Stroke Large volume intracerebral hematoma greater than 5cm on CT Concern for expanding hematoma Rapidly declining mental status, especially requiring intubation
When to Consider a Transfer: Hemorrhagic Stroke Large volume intracerebral hematoma greater than 5cm on CT Concern for expanding hematoma Rapidly declining mental status, especially requiring intubation
Acute Stroke Treatment KPNC Stroke EXPRESS
 Acute Stroke Treatment 2018 KPNC Stroke EXPRESS EXpediting the PRocess of Evaluating & Stopping Stroke 1 Jeffrey G. Klingman, MD The Permanente Medical Group Stroke Treatment in the old days Prior to 1996:
Acute Stroke Treatment 2018 KPNC Stroke EXPRESS EXpediting the PRocess of Evaluating & Stopping Stroke 1 Jeffrey G. Klingman, MD The Permanente Medical Group Stroke Treatment in the old days Prior to 1996:
Stroke Update. Lacunar 19% Thromboembolic 6% SAH 13% ICH 13% Unknown 32% Hemorrhagic 26% Ischemic 71% Other 3% Cardioembolic 14%
 Stroke Update Michel Torbey, MD, MPH, FAHA, FNCS Medical Director, Neurovascular Stroke Center Professor Department of Neurology and Neurosurgery The Ohio State University Wexner Medical Center Objectives
Stroke Update Michel Torbey, MD, MPH, FAHA, FNCS Medical Director, Neurovascular Stroke Center Professor Department of Neurology and Neurosurgery The Ohio State University Wexner Medical Center Objectives
Target: STROKE. The Team-Based Approached
 Target: STROKE The Team-Based Approached November 19, 2013 Tuesday 1300 1400 Thank you for joining today s webinar, the presentation will begin shortly. A special thank you to Cornerstone Therapeutics
Target: STROKE The Team-Based Approached November 19, 2013 Tuesday 1300 1400 Thank you for joining today s webinar, the presentation will begin shortly. A special thank you to Cornerstone Therapeutics
Ongoing Acute Stroke Studies 10/5/2015
 Ongoing Acute Stroke Studies 10/5/2015 Wade S. Smith, MD, PhD Director UCSF Neurovascular Service Daryl R. Gress Professor of Neurocritical Care and Stroke Disclosures NIH U10 NS 086494 (PI) NorCal RCC
Ongoing Acute Stroke Studies 10/5/2015 Wade S. Smith, MD, PhD Director UCSF Neurovascular Service Daryl R. Gress Professor of Neurocritical Care and Stroke Disclosures NIH U10 NS 086494 (PI) NorCal RCC
Stroke Transfer Checklist
 Stroke Transfer Checklist When preparing to transfer an acute stroke patient to the UF Health Shands Comprehensive Stroke Center, please make every attempt to include the following information: Results
Stroke Transfer Checklist When preparing to transfer an acute stroke patient to the UF Health Shands Comprehensive Stroke Center, please make every attempt to include the following information: Results
Antithrombotics: Percent of patients with an ischemic stroke or TIA prescribed antithrombotic therapy at discharge. Corresponding
 Get With The Guidelines -Stroke is the American Heart Association s collaborative performance improvement program, demonstrated to improve adherence to evidence-based care of patients hospitalized with
Get With The Guidelines -Stroke is the American Heart Association s collaborative performance improvement program, demonstrated to improve adherence to evidence-based care of patients hospitalized with
Acute Stroke Management LUKE BRADBURY, MD 10/8/14 FALL WAPA CONFERENCE
 Objectives Acute Stroke Management LUKE BRADBURY, MD 10/8/14 FALL WAPA CONFERENCE Recognize the clinical signs of acute stroke Differentiate between stroke and some of the more common stroke mimics Review
Objectives Acute Stroke Management LUKE BRADBURY, MD 10/8/14 FALL WAPA CONFERENCE Recognize the clinical signs of acute stroke Differentiate between stroke and some of the more common stroke mimics Review
The Nervous System. Divisions of the Nervous System. Branches of the Autonomic Nervous System. Central versus Peripheral
 The Nervous System Divisions of the Nervous System Central versus Peripheral Central Brain and spinal cord Peripheral Everything else Somatic versus Autonomic Somatic Nerves serving conscious sensations
The Nervous System Divisions of the Nervous System Central versus Peripheral Central Brain and spinal cord Peripheral Everything else Somatic versus Autonomic Somatic Nerves serving conscious sensations
Optimizing Care for Patients with Acute Ischemic Stroke Thrombolytic Therapy for Low NIHSS
 Optimizing Care for Patients with Acute Ischemic Stroke Thrombolytic Therapy for Low NIHSS Nerses Sanossian, MD, FAHA Presentation not eligible for CME credit Disclosures Today s objectives Case study:
Optimizing Care for Patients with Acute Ischemic Stroke Thrombolytic Therapy for Low NIHSS Nerses Sanossian, MD, FAHA Presentation not eligible for CME credit Disclosures Today s objectives Case study:
Acute Stroke Treatment: Current Trends 2010
 Acute Stroke Treatment: Current Trends 2010 Helmi L. Lutsep, MD Oregon Stroke Center Oregon Health & Science University Overview Ischemic Stroke Neuroprotectant trials to watch for IV tpa longer treatment
Acute Stroke Treatment: Current Trends 2010 Helmi L. Lutsep, MD Oregon Stroke Center Oregon Health & Science University Overview Ischemic Stroke Neuroprotectant trials to watch for IV tpa longer treatment
GUIDELINES FOR THE EARLY MANAGEMENT OF PATIENTS WITH ACUTE ISCHEMIC STROKE
 2018 UPDATE QUICK SHEET 2018 American Heart Association GUIDELINES FOR THE EARLY MANAGEMENT OF PATIENTS WITH ACUTE ISCHEMIC STROKE A Summary for Healthcare Professionals from the American Heart Association/American
2018 UPDATE QUICK SHEET 2018 American Heart Association GUIDELINES FOR THE EARLY MANAGEMENT OF PATIENTS WITH ACUTE ISCHEMIC STROKE A Summary for Healthcare Professionals from the American Heart Association/American
TRANSPORT OF PATIENTS WITH SUSPECTED ACUTE STROKE
 TRANSPORT OF PATIENTS WITH SUSPECTED ACUTE STROKE I. Patients with stroke symptoms 24 hours in duration or of unknown time of last known normal shall be assessed using the Cincinnati Stroke Scale (CSS
TRANSPORT OF PATIENTS WITH SUSPECTED ACUTE STROKE I. Patients with stroke symptoms 24 hours in duration or of unknown time of last known normal shall be assessed using the Cincinnati Stroke Scale (CSS
On Call Guide to CT Perfusion. Updated: March 2011
 On Call Guide to CT Perfusion Updated: March 2011 CT Stroke Protocol 1. Non contrast CT brain 2. CT perfusion: contrast 40cc bolus dynamic imaging at 8 slice levels ~ 60 sec creates perfusion color maps
On Call Guide to CT Perfusion Updated: March 2011 CT Stroke Protocol 1. Non contrast CT brain 2. CT perfusion: contrast 40cc bolus dynamic imaging at 8 slice levels ~ 60 sec creates perfusion color maps
Interventional Neuroradiology. & Stroke INR PROCEDURES INR PROCEDURES. Dr Steve Chryssidis. 25-Sep-17. Interventional Neuroradiology
 Interventional Neuroradiology Interventional Neuroradiology & Stroke Dr Steve Chryssidis Interventional Neuroradiology (INR) is a subspecialty within Radiology INR -- broadly defined as treatment by endovascular
Interventional Neuroradiology Interventional Neuroradiology & Stroke Dr Steve Chryssidis Interventional Neuroradiology (INR) is a subspecialty within Radiology INR -- broadly defined as treatment by endovascular
Thrombolysis Assessment
 Thrombolysis Assessment Brief Clinical Summary of symptom onset of arrival of patient of assessment BP GCS BM If BM
Thrombolysis Assessment Brief Clinical Summary of symptom onset of arrival of patient of assessment BP GCS BM If BM
Mechanical thrombectomy beyond the 6 hours. Mahmoud Rayes, MD Medical Director, Stroke program Greenville Memorial Hospital
 Mechanical thrombectomy beyond the 6 hours Mahmoud Rayes, MD Medical Director, Stroke program Greenville Memorial Hospital Disclosures None Worldwide statistics 1 IN 6 people will have a stroke at some
Mechanical thrombectomy beyond the 6 hours Mahmoud Rayes, MD Medical Director, Stroke program Greenville Memorial Hospital Disclosures None Worldwide statistics 1 IN 6 people will have a stroke at some
Broadening the Stroke Window in Light of the DAWN Trial
 Broadening the Stroke Window in Light of the DAWN Trial South Jersey Neurovascular and Stroke Symposium April 26, 2018 Rohan Chitale, MD Assistant Professor of Neurological Surgery Vanderbilt University
Broadening the Stroke Window in Light of the DAWN Trial South Jersey Neurovascular and Stroke Symposium April 26, 2018 Rohan Chitale, MD Assistant Professor of Neurological Surgery Vanderbilt University
Imaging Stroke: Is There a Stroke Equivalent of the ECG? Albert J. Yoo, MD Director of Acute Stroke Intervention Massachusetts General Hospital
 Imaging Stroke: Is There a Stroke Equivalent of the ECG? Albert J. Yoo, MD Director of Acute Stroke Intervention Massachusetts General Hospital Disclosures Penumbra, Inc. research grant (significant) for
Imaging Stroke: Is There a Stroke Equivalent of the ECG? Albert J. Yoo, MD Director of Acute Stroke Intervention Massachusetts General Hospital Disclosures Penumbra, Inc. research grant (significant) for
DISCLOSURES OBJECTIVES 11/18/2014. Stroke Network Update. None. Discuss
 Stroke Network Update MOUHAMMAD A. JUMAA MD ASSISTANT PROFESSOR VASCULAR & INTERVENTIONAL NEUROLOGY UNIVERSITY OF TOLEDO DISCLOSURES None OBJECTIVES Discuss Regional stroke systems of care in NW OHIO Evolution
Stroke Network Update MOUHAMMAD A. JUMAA MD ASSISTANT PROFESSOR VASCULAR & INTERVENTIONAL NEUROLOGY UNIVERSITY OF TOLEDO DISCLOSURES None OBJECTIVES Discuss Regional stroke systems of care in NW OHIO Evolution
BY: Ramon Medina EMT-LP/RN
 BY: Ramon Medina EMT-LP/RN Discuss types of strokes Discuss the physical and neurological assessment of stroke patients Discuss pertinent historical findings Discuss pre-hospital and emergency management
BY: Ramon Medina EMT-LP/RN Discuss types of strokes Discuss the physical and neurological assessment of stroke patients Discuss pertinent historical findings Discuss pre-hospital and emergency management
Brain Injury and Epilepsy
 Slide 1 Brain Injury and Epilepsy Presented by: Paula St. John, MA Education and Community Outreach Manager Minnesota Brain injury Alliance www.braininjurymn.org l 612-378-2742 800-669-6442 Slide 2 Objectives:
Slide 1 Brain Injury and Epilepsy Presented by: Paula St. John, MA Education and Community Outreach Manager Minnesota Brain injury Alliance www.braininjurymn.org l 612-378-2742 800-669-6442 Slide 2 Objectives:
IMAGING IN ACUTE ISCHEMIC STROKE
 IMAGING IN ACUTE ISCHEMIC STROKE Timo Krings MD, PhD, FRCP (C) Professor of Radiology & Surgery Braley Chair of Neuroradiology, Chief and Program Director of Diagnostic and Interventional Neuroradiology;
IMAGING IN ACUTE ISCHEMIC STROKE Timo Krings MD, PhD, FRCP (C) Professor of Radiology & Surgery Braley Chair of Neuroradiology, Chief and Program Director of Diagnostic and Interventional Neuroradiology;