Instellen van beademingsparameters bij de obese pa3ent. MDO Nynke Postma
|
|
|
- Kathlyn Sims
- 5 years ago
- Views:
Transcription
1 Instellen van beademingsparameters bij de obese pa3ent MDO Nynke Postma
2 1. Altered respiratory mechanics in obese 2. Transpulmonary pressure 3. PEEP volume 5. Effects of 6. Key messages

3 Obesity & respiratory mechanics Baseline in respiratory mechanics of the obese Decrease in TLC Decrease in FRC and VC Increase in pleural pressure Increase of upper and lower airway resistance.

4 Obesity: Increased weight of the chest wall Increased abdominal pressure } decrease in respir. system compliance
5 Obesity & respiratory mechanics of the small airways & expiratory flow PEEP i at rest Air trapping during exercise Intrinsic mechanical loading of inspiratory muscles Work of breathing & VO 2
6 Obesity & gas exchange Atelectasis with V/Q mismatch due to airway narrowing and in lung perfusion Arterial hypoxemia Elevated A- a gradient
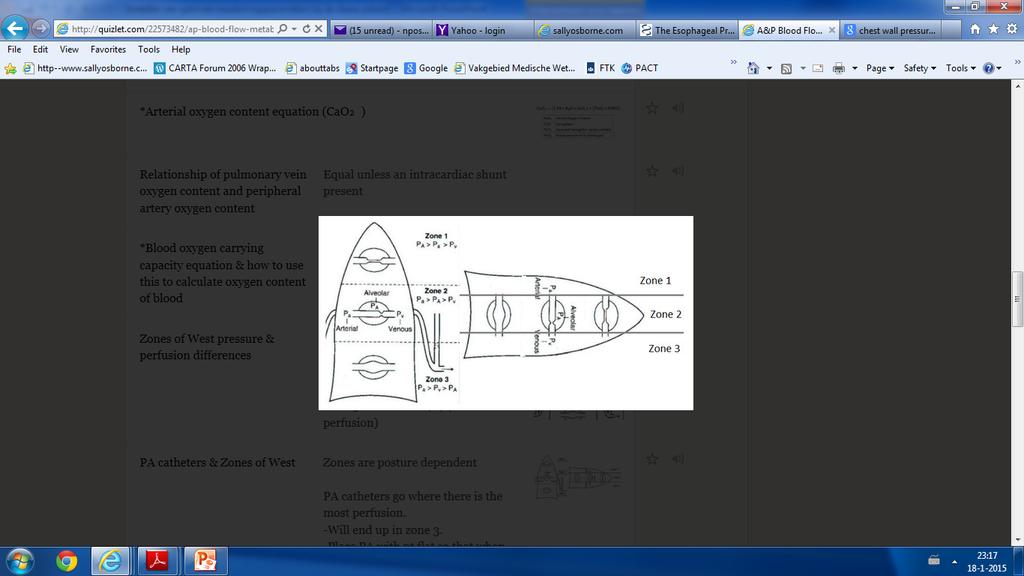
7 Transpulmonary pressure (P L ) Distending pressure across the lung P L =P A - P pl Obesity: P pl - - > P L - - > collapsing pressure - - > ATELECTASIS impaired gas exchange decreased lung compliance
8 Transpulmonary pressure (P L ) Hogere P pl ó lagere P L
9 Transpulmonary pressure (P L ) Safe upper limit: 25 cm H2O
10 Obesity & ARDS Obesity Heterogenic lung ARDS Heterogenic lung Obesity + ARDS Heterogenic lung +++
11 Obesity & ARDS Atelectasis & ARDS VALI Shear stresses at the of open and closed alveoli
12 Open lung strategy Agempts to create parenchymal homogeneity by: 1. Recruitment maneuvers 2. PEEP to respiratory mechanics 3. Minimize airway pressures
13 New focus: Reducing transpulmonary pressure Obese P pl à PEEP to overcome collapse and prevent derecruitment. High P peak ( 30 cmh2o) can be applied without lung overdisten@on P L <25 cmh2o at end inspira@on is considered safe (Mead J, Takishima T, Leith D. Stress distribu7on in lungs: a model of pulmonary elas7city. J Appl Physiol ; 28 ( 5 ): )
14 PEEP level? of PEEP: Collapse of alveoli during Atelectrauma lung injury. of PEEP: Hemodynamic compromise Increased dead space Overdistension of the lungs at end-
15 Methods of PEEPlevel 1. Using transpulmonary pressure by measuring P es 2. Using the airway curve profile (stress index) 3. compliance
16 PEEP level: esophageal pressure (P es ) P esophageal (P es ) es@mates P pl P L can be es@mated PEEP can be to achieve a posi@ve P L at end- exhala@on. Talmor et al. N Engl J Med : improvement of gas exchange and trend to improved 28- day mortality a primarily surgical ARDS popula7on

17 Obesity and Pes
18 Measurement of P es Lower 1/3 of oesofagus In sedated, paralyzed mechanically ven@lated pa@ents: cm distance from the nares transmission of the heartbeat
19 Effects of P es (supine) > P es (upright) (~5cmH2O) Medias@nal weight Much more fluctua@on in P es from cardiac ac@vity in supine posi@on compared with upright posi@on
20 PEEP with use of P es Technique: Increase PEEP un@l P L (end- expira@on) > 0 Goal: Preven@on of atelectrauma by preven@ng lung collapse Talmor et al. N Engl J Med : improvement of gas exchange and trend to improved 28- day mortality a primarily surgical ARDS popula7on
 Talmor et al. N Engl J Med.")
21 PEEP with use of P es Assump@ons: P es approximates P pl Expiratory airway collapse is not occurring in the lung regions in which local P pl < P es measured Risk: Severe overdistension in lung regions where P es overes@mates P pl (ventral regions) Talmor et al. N Engl J Med : improvement of gas exchange and trend to improved 28- day mortality a primarily surgical ARDS popula7on
22

23 Piralls Inter- individual variable of weight to P es Increasing PEEP to a target may cause injurious overdistension of other lung regions
24 PEEP compliance receiving a set V t, P plat is measured as PEEP is increased. 1. Pplat increase in PEEP : improved lung compliance and an element of recruitable lung. 2. Pplat increase in PEEP : no recruitment; areas of overdisten@on or hyperinfla@on
25 Tidal volume Based on ideal body weight 6 ml/kg IBW Hypercapnia Acute illness Chronic hypoven@la@on
26 prone Pro Allows the weight to be supported by the sternum Decrease of lung collapse Improvement of V/Q matching Decrease of shunt. Con Futher increase abdominal pressure Pressure ulcera Further studies in obese needed

27 Prone
28 reverse trendelenburg of weaning from the unloading: in trans - diaphragma@c pressure Decreased atelectasis, Improved gas exchange
29 Key messages Obese Altered respiratory mechanics Increased heterogeneity of the lung strategies that focus on P L as a measure of lung stress show promise in pilot studies

30
31 Literature
ARDS Management Protocol
 ARDS Management Protocol February 2018 ARDS Criteria Onset Within 1 week of a known clinical insult or new or worsening respiratory symptoms Bilateral opacities not fully explained by effusions, lobar/lung
ARDS Management Protocol February 2018 ARDS Criteria Onset Within 1 week of a known clinical insult or new or worsening respiratory symptoms Bilateral opacities not fully explained by effusions, lobar/lung
Management of refractory ARDS. Saurabh maji
 Management of refractory ARDS Saurabh maji Refractory hypoxemia as PaO2/FIO2 is less than 100 mm Hg, inability to keep plateau pressure below 30 cm H2O despite a VT of 4 ml/kg development of barotrauma
Management of refractory ARDS Saurabh maji Refractory hypoxemia as PaO2/FIO2 is less than 100 mm Hg, inability to keep plateau pressure below 30 cm H2O despite a VT of 4 ml/kg development of barotrauma
Ventilatory Management of ARDS. Alexei Ortiz Milan; MD, MSc
 Ventilatory Management of ARDS Alexei Ortiz Milan; MD, MSc 2017 Outline Ventilatory management of ARDS Protected Ventilatory Strategy Use of NMB Selection of PEEP Driving pressure Lung Recruitment Prone
Ventilatory Management of ARDS Alexei Ortiz Milan; MD, MSc 2017 Outline Ventilatory management of ARDS Protected Ventilatory Strategy Use of NMB Selection of PEEP Driving pressure Lung Recruitment Prone
1. When a patient fails to ventilate or oxygenate adequately, the problem is caused by pathophysiological factors such as hyperventilation.
 Chapter 1: Principles of Mechanical Ventilation TRUE/FALSE 1. When a patient fails to ventilate or oxygenate adequately, the problem is caused by pathophysiological factors such as hyperventilation. F
Chapter 1: Principles of Mechanical Ventilation TRUE/FALSE 1. When a patient fails to ventilate or oxygenate adequately, the problem is caused by pathophysiological factors such as hyperventilation. F
INTRODUCTION The effect of CPAP works on lung mechanics to improve oxygenation (PaO 2
 2 Effects of CPAP INTRODUCTION The effect of CPAP works on lung mechanics to improve oxygenation (PaO 2 ). The effect on CO 2 is only secondary to the primary process of improvement in lung volume and
2 Effects of CPAP INTRODUCTION The effect of CPAP works on lung mechanics to improve oxygenation (PaO 2 ). The effect on CO 2 is only secondary to the primary process of improvement in lung volume and
ARDS Assisted ventilation and prone position. ICU Fellowship Training Radboudumc
 ARDS Assisted ventilation and prone position ICU Fellowship Training Radboudumc Fig. 1 Physiological mechanisms controlling respiratory drive and clinical consequences of inappropriate respiratory drive
ARDS Assisted ventilation and prone position ICU Fellowship Training Radboudumc Fig. 1 Physiological mechanisms controlling respiratory drive and clinical consequences of inappropriate respiratory drive
Respiratory insufficiency in bariatric patients
 Respiratory insufficiency in bariatric patients Special considerations or just more of the same? Weaning and rehabilation conference 6th November 2015 Definition of obesity Underweight BMI< 18 Normal weight
Respiratory insufficiency in bariatric patients Special considerations or just more of the same? Weaning and rehabilation conference 6th November 2015 Definition of obesity Underweight BMI< 18 Normal weight
Dr. Yasser Fathi M.B.B.S, M.Sc, M.D. Anesthesia Consultant, Head of ICU King Saud Hospital, Unaizah
 BY Dr. Yasser Fathi M.B.B.S, M.Sc, M.D Anesthesia Consultant, Head of ICU King Saud Hospital, Unaizah Objectives For Discussion Respiratory Physiology Pulmonary Graphics BIPAP Graphics Trouble Shootings
BY Dr. Yasser Fathi M.B.B.S, M.Sc, M.D Anesthesia Consultant, Head of ICU King Saud Hospital, Unaizah Objectives For Discussion Respiratory Physiology Pulmonary Graphics BIPAP Graphics Trouble Shootings
APRV Ventilation Mode
 APRV Ventilation Mode Airway Pressure Release Ventilation A Type of CPAP Continuous Positive Airway Pressure (CPAP) with an intermittent release phase. Patient cycles between two levels of CPAP higher
APRV Ventilation Mode Airway Pressure Release Ventilation A Type of CPAP Continuous Positive Airway Pressure (CPAP) with an intermittent release phase. Patient cycles between two levels of CPAP higher
What s New About Proning?
 1 What s New About Proning? J. Brady Scott, MSc, RRT-ACCS, AE-C, FAARC Director of Clinical Education and Assistant Professor Department of Cardiopulmonary Sciences Division of Respiratory Care Rush University
1 What s New About Proning? J. Brady Scott, MSc, RRT-ACCS, AE-C, FAARC Director of Clinical Education and Assistant Professor Department of Cardiopulmonary Sciences Division of Respiratory Care Rush University
Application of Lung Protective Ventilation MUST Begin Immediately After Intubation
 Conflict of Interest Disclosure Robert M Kacmarek Managing Severe Hypoxemia!" 9-28-17 FOCUS Bob Kacmarek PhD, RRT Massachusetts General Hospital, Harvard Medical School, Boston, Massachusetts I disclose
Conflict of Interest Disclosure Robert M Kacmarek Managing Severe Hypoxemia!" 9-28-17 FOCUS Bob Kacmarek PhD, RRT Massachusetts General Hospital, Harvard Medical School, Boston, Massachusetts I disclose
ARDS: an update 6 th March A. Hakeem Al Hashim, MD, FRCP SQUH
 ARDS: an update 6 th March 2017 A. Hakeem Al Hashim, MD, FRCP SQUH 30M, previously healthy Hx: 1 week dry cough Gradually worsening SOB No travel Hx Case BP 130/70, HR 100/min ph 7.29 pco2 35 po2 50 HCO3
ARDS: an update 6 th March 2017 A. Hakeem Al Hashim, MD, FRCP SQUH 30M, previously healthy Hx: 1 week dry cough Gradually worsening SOB No travel Hx Case BP 130/70, HR 100/min ph 7.29 pco2 35 po2 50 HCO3
How ARDS should be treated in 2017
 How ARDS should be treated in 2017 2017, Ostrava Luciano Gattinoni, MD, FRCP Georg-August-Universität Göttingen Germany ARDS 1. Keep the patient alive respiration circulation 2. Cure the disease leading
How ARDS should be treated in 2017 2017, Ostrava Luciano Gattinoni, MD, FRCP Georg-August-Universität Göttingen Germany ARDS 1. Keep the patient alive respiration circulation 2. Cure the disease leading
Respiratory monitoring / Safe weaning of respiratory support
 Respiratory monitoring / Safe weaning of respiratory support Athavudh Deesomchok, MD Pulmonary, Cri9cal care and Allergy Medicine CMU CVT Short course 2013 Post- cardiac surgical care Opera9ng room ICU
Respiratory monitoring / Safe weaning of respiratory support Athavudh Deesomchok, MD Pulmonary, Cri9cal care and Allergy Medicine CMU CVT Short course 2013 Post- cardiac surgical care Opera9ng room ICU
C h a p t e r 1 4 Ventilator Support
 C h a p t e r 1 4 Ventilator Support Shirish Prayag Ex. Hon. Asst. Prof of Medicine, BJ Medical College and Sassoon Hospital, Pune; Chief Consultant in Internal Medicine and Critical Care, Shree Medical
C h a p t e r 1 4 Ventilator Support Shirish Prayag Ex. Hon. Asst. Prof of Medicine, BJ Medical College and Sassoon Hospital, Pune; Chief Consultant in Internal Medicine and Critical Care, Shree Medical
APRV: An Update CHLOE STEINSHOUER, MD PULMONARY & SLEEP CONSULTANTS OF KANSAS 04/06/2017
 APRV: An Update CHLOE STEINSHOUER, MD PULMONARY & SLEEP CONSULTANTS OF KANSAS 04/06/2017 Disclosures No conflicts of interest Objectives Attendees will be able to: Define the mechanism of APRV Describe
APRV: An Update CHLOE STEINSHOUER, MD PULMONARY & SLEEP CONSULTANTS OF KANSAS 04/06/2017 Disclosures No conflicts of interest Objectives Attendees will be able to: Define the mechanism of APRV Describe
Recruitment Maneuvers and Higher PEEP, the So-Called Open Lung Concept, in Patients with ARDS
 Zee and Gommers Critical Care (2019) 23:73 https://doi.org/10.1186/s13054-019-2365-1 REVIEW Recruitment Maneuvers and Higher PEEP, the So-Called Open Lung Concept, in Patients with ARDS Philip van der
Zee and Gommers Critical Care (2019) 23:73 https://doi.org/10.1186/s13054-019-2365-1 REVIEW Recruitment Maneuvers and Higher PEEP, the So-Called Open Lung Concept, in Patients with ARDS Philip van der
Prone Position in ARDS
 Prone Position in ARDS Rich Kallet MS RRT FAARC, FCCM Respiratory Care Services San Francisco General Hospital University of California, San Francisco, Case Study A 39 yo F admitted to SFGH TICU s/p hanging,
Prone Position in ARDS Rich Kallet MS RRT FAARC, FCCM Respiratory Care Services San Francisco General Hospital University of California, San Francisco, Case Study A 39 yo F admitted to SFGH TICU s/p hanging,
Landmark articles on ventilation
 Landmark articles on ventilation Dr Shrikanth Srinivasan MD,DNB,FNB,EDIC Consultant, Critical Care Medicine Medanta, The Medicity ARDS AECC DEFINITION-1994 ALI Acute onset Bilateral chest infiltrates PCWP
Landmark articles on ventilation Dr Shrikanth Srinivasan MD,DNB,FNB,EDIC Consultant, Critical Care Medicine Medanta, The Medicity ARDS AECC DEFINITION-1994 ALI Acute onset Bilateral chest infiltrates PCWP
«Best» PEEP? Physiologic? Therapeutic? Optimal? Super? Preferred? Minimal? Right? Protective? Prophylactic?
 1936-2005 «Best» PEEP? Physiologic? Therapeutic? Optimal? Super? Preferred? Minimal? Right? Protective? Prophylactic? 1990-2000 Post cardiac arrest First day of mechanical ventilation 1990-1991 No patient
1936-2005 «Best» PEEP? Physiologic? Therapeutic? Optimal? Super? Preferred? Minimal? Right? Protective? Prophylactic? 1990-2000 Post cardiac arrest First day of mechanical ventilation 1990-1991 No patient
Monitor the patients disease pathology and response to therapy Estimate respiratory mechanics
 Understanding Graphics during Mechanical Ventilation Why Understand Ventilator Graphics? Waveforms are the graphic representation of the data collected by the ventilator and reflect the interaction between
Understanding Graphics during Mechanical Ventilation Why Understand Ventilator Graphics? Waveforms are the graphic representation of the data collected by the ventilator and reflect the interaction between
ARDS A Brief Overview. Lucas Pitts, M.D. Assistant Professor of Medicine Pulmonary and Critical Care Medicine University of Kansas School of Medicine
 ARDS A Brief Overview Lucas Pitts, M.D. Assistant Professor of Medicine Pulmonary and Critical Care Medicine University of Kansas School of Medicine Outline Definition of ARDS Epidemiology of ARDS Pathophysiology
ARDS A Brief Overview Lucas Pitts, M.D. Assistant Professor of Medicine Pulmonary and Critical Care Medicine University of Kansas School of Medicine Outline Definition of ARDS Epidemiology of ARDS Pathophysiology
Objec+ves: Respiratory Physiology Basics
 Noninvasive Posi+ve Pressure Ven+la+on: Applica+ons to Avoid Crisis Al Quinones, DHA, MA, RRT- NPS, RPFT, RPSGT, CCT, AE- C, FACHE Objec+ves: - Review basic respiratory physiology - Discuss essen;al aspects
Noninvasive Posi+ve Pressure Ven+la+on: Applica+ons to Avoid Crisis Al Quinones, DHA, MA, RRT- NPS, RPFT, RPSGT, CCT, AE- C, FACHE Objec+ves: - Review basic respiratory physiology - Discuss essen;al aspects
Prepared by : Bayan Kaddourah RN,MHM. GICU Clinical Instructor
 Mechanical Ventilation Prepared by : Bayan Kaddourah RN,MHM. GICU Clinical Instructor 1 Definition Is a supportive therapy to facilitate gas exchange. Most ventilatory support requires an artificial airway.
Mechanical Ventilation Prepared by : Bayan Kaddourah RN,MHM. GICU Clinical Instructor 1 Definition Is a supportive therapy to facilitate gas exchange. Most ventilatory support requires an artificial airway.
Ventilation de l obèse: les 10 points clés
 Ventilation de l obèse: les 10 points clés Samir JABER Department of Critical Care Medicine and Anesthesiology (DAR B) Saint Eloi University Hospital and Montpellier School of Medicine; INSERM U1046 University
Ventilation de l obèse: les 10 points clés Samir JABER Department of Critical Care Medicine and Anesthesiology (DAR B) Saint Eloi University Hospital and Montpellier School of Medicine; INSERM U1046 University
Analyzing Lung protective ventilation F Javier Belda MD, PhD Sº de Anestesiología y Reanimación. Hospital Clinico Universitario Valencia (Spain)
") Analyzing Lung protective ventilation F Javier Belda MD, PhD Sº de Anestesiología y Reanimación Hospital Clinico Universitario Valencia (Spain) ALI/ARDS Report of the American-European consensus conference
Analyzing Lung protective ventilation F Javier Belda MD, PhD Sº de Anestesiología y Reanimación Hospital Clinico Universitario Valencia (Spain) ALI/ARDS Report of the American-European consensus conference
Agenda. Mechanical Ventilation in Morbidly Obese Patients. Paolo Pelosi. ESPCOP, Ostend, Belgium Saturday, November 14, 2009.
 Mechanical Ventilation in Morbidly Obese Patients t Paolo Pelosi Department of Ambient, Health and Safety University of Insubria - Varese, ITALY ppelosi@hotmail.com ESPCOP, Ostend, Belgium Saturday, November
Mechanical Ventilation in Morbidly Obese Patients t Paolo Pelosi Department of Ambient, Health and Safety University of Insubria - Varese, ITALY ppelosi@hotmail.com ESPCOP, Ostend, Belgium Saturday, November
Lung Recruitment Strategies in Anesthesia
 Lung Recruitment Strategies in Anesthesia Intraoperative ventilatory management to prevent Post-operative Pulmonary Complications Kook-Hyun Lee, MD, PhD Department of Anesthesiology Seoul National University
Lung Recruitment Strategies in Anesthesia Intraoperative ventilatory management to prevent Post-operative Pulmonary Complications Kook-Hyun Lee, MD, PhD Department of Anesthesiology Seoul National University
Part 2 of park s Ventilator and ARDS slides for syllabus
 Part 2 of park s Ventilator and ARDS slides for syllabus Early Neuromuscular Blockade Question 4 The early use of cis-atracurium in severe ARDS is: A. Contraindicated in patients with diabetes B. Associated
Part 2 of park s Ventilator and ARDS slides for syllabus Early Neuromuscular Blockade Question 4 The early use of cis-atracurium in severe ARDS is: A. Contraindicated in patients with diabetes B. Associated
Transpulmonary pressure measurement
 White Paper Transpulmonary pressure measurement Benefit of measuring transpulmonary pressure in mechanically ventilated patients Dr. Jean-Michel Arnal, Senior Intensivist, Hopital Sainte Musse, Toulon,
White Paper Transpulmonary pressure measurement Benefit of measuring transpulmonary pressure in mechanically ventilated patients Dr. Jean-Michel Arnal, Senior Intensivist, Hopital Sainte Musse, Toulon,
Recognizing and Correcting Patient-Ventilator Dysynchrony
 2019 KRCS Annual State Education Seminar Recognizing and Correcting Patient-Ventilator Dysynchrony Eric Kriner BS,RRT Pulmonary Critical Care Clinical Specialist MedStar Washington Hospital Center Washington,
2019 KRCS Annual State Education Seminar Recognizing and Correcting Patient-Ventilator Dysynchrony Eric Kriner BS,RRT Pulmonary Critical Care Clinical Specialist MedStar Washington Hospital Center Washington,
High Flow Nasal Cannula Oxygen HFNC. Dr I S Kalla Department of Pulmonology University of the Witwatersrand
 786 High Flow Nasal Cannula Oxygen HFNC Dr I S Kalla Department of Pulmonology University of the Witwatersrand Disclaimer I was a scep@c un@l I used it Now I am a firm believer HFNC The Fisher and Paykel
786 High Flow Nasal Cannula Oxygen HFNC Dr I S Kalla Department of Pulmonology University of the Witwatersrand Disclaimer I was a scep@c un@l I used it Now I am a firm believer HFNC The Fisher and Paykel
ARF, Mechaical Ventilation and PFTs: ACOI Board Review 2018
 ARF, Mechaical Ventilation and PFTs: ACOI Board Review 2018 Thomas F. Morley, DO, FACOI, FCCP, FAASM Professor of Medicine Chairman Department of Internal Medicine Director of the Division of Pulmonary,
ARF, Mechaical Ventilation and PFTs: ACOI Board Review 2018 Thomas F. Morley, DO, FACOI, FCCP, FAASM Professor of Medicine Chairman Department of Internal Medicine Director of the Division of Pulmonary,
Respiratory Mechanics
 Respiratory Mechanics Critical Care Medicine Specialty Board Tutorial Dr Arthur Chun-Wing LAU Associate Consultant Intensive Care Unit, Pamela Youde Nethersole Eastern Hospital, Hong Kong 17 th June 2014
Respiratory Mechanics Critical Care Medicine Specialty Board Tutorial Dr Arthur Chun-Wing LAU Associate Consultant Intensive Care Unit, Pamela Youde Nethersole Eastern Hospital, Hong Kong 17 th June 2014
Respiratory Complications of Obesity. Diana Wilson, M.D. ACP Educational Session September 16, 2017
 Respiratory Complications of Obesity Diana Wilson, M.D. ACP Educational Session September 16, 2017 1 Prevalence of Self-Reported Obesity Among U.S. Adults by State and Territory, BRFSS, 2011 Prevalence
Respiratory Complications of Obesity Diana Wilson, M.D. ACP Educational Session September 16, 2017 1 Prevalence of Self-Reported Obesity Among U.S. Adults by State and Territory, BRFSS, 2011 Prevalence
Lecture Notes. Chapter 2: Introduction to Respiratory Failure
 Lecture Notes Chapter 2: Introduction to Respiratory Failure Objectives Define respiratory failure, ventilatory failure, and oxygenation failure List the causes of respiratory failure Describe the effects
Lecture Notes Chapter 2: Introduction to Respiratory Failure Objectives Define respiratory failure, ventilatory failure, and oxygenation failure List the causes of respiratory failure Describe the effects
Cardiorespiratory Physiotherapy Tutoring Services 2017
 VENTILATOR HYPERINFLATION ***This document is intended to be used as an information resource only it is not intended to be used as a policy document/practice guideline. Before incorporating the use of
VENTILATOR HYPERINFLATION ***This document is intended to be used as an information resource only it is not intended to be used as a policy document/practice guideline. Before incorporating the use of
ACUTE RESPIRATORY DISTRESS SYNDROME
 ACUTE RESPIRATORY DISTRESS SYNDROME Angel Coz MD, FCCP, DCE Assistant Professor of Medicine UCSF Fresno November 4, 2017 No disclosures OBJECTIVES Identify current trends and risk factors of ARDS Describe
ACUTE RESPIRATORY DISTRESS SYNDROME Angel Coz MD, FCCP, DCE Assistant Professor of Medicine UCSF Fresno November 4, 2017 No disclosures OBJECTIVES Identify current trends and risk factors of ARDS Describe
Chronic Obstructive Pulmonary Disease
 136 PHYSIOLOGY CASES AND PROBLEMS Case 24 Chronic Obstructive Pulmonary Disease Bernice Betweiler is a 73-year-old retired seamstress who has never been married. She worked in the alterations department
136 PHYSIOLOGY CASES AND PROBLEMS Case 24 Chronic Obstructive Pulmonary Disease Bernice Betweiler is a 73-year-old retired seamstress who has never been married. She worked in the alterations department
ARDS and Lung Protection
 ARDS and Lung Protection Kristina Sullivan, MD Associate Professor University of California, San Francisco Department of Anesthesia and Perioperative Care Division of Critical Care Medicine Overview Low
ARDS and Lung Protection Kristina Sullivan, MD Associate Professor University of California, San Francisco Department of Anesthesia and Perioperative Care Division of Critical Care Medicine Overview Low
Capnography. Capnography. Oxygenation. Pulmonary Physiology 4/15/2018. non invasive monitor for ventilation. Edward C. Adlesic, DMD.
 Capnography Edward C. Adlesic, DMD University of Pittsburgh School of Dental Medicine 2018 North Carolina Program Capnography non invasive monitor for ventilation measures end tidal CO2 early detection
Capnography Edward C. Adlesic, DMD University of Pittsburgh School of Dental Medicine 2018 North Carolina Program Capnography non invasive monitor for ventilation measures end tidal CO2 early detection
Outline. Basic principles of lung protective ventilation. The challenging areas. Small tidal volumes Recruitment
 ARDS beyond 6/kg Gordon D. Rubenfeld, MD MSc Professor of Medicine, University of Toronto Chief, Program in Trauma, Emergency, and Critical Care Sunnybrook Health Sciences Centre Outline Basic principles
ARDS beyond 6/kg Gordon D. Rubenfeld, MD MSc Professor of Medicine, University of Toronto Chief, Program in Trauma, Emergency, and Critical Care Sunnybrook Health Sciences Centre Outline Basic principles
Refresher Course MYTHS AND REALITY ABOUT LUNG MECHANICS 5 RC 2. European Society of Anaesthesiologists FIGURE 1 STATIC MEASUREMENTS
 European Society of Anaesthesiologists Refresher Course S AND ABOUT LUNG MECHANICS 5 RC 2 Anders LARSSON Gentofte University Hospital Copenhagen University Hellerup, Denmark Saturday May 31, 2003 Euroanaesthesia
European Society of Anaesthesiologists Refresher Course S AND ABOUT LUNG MECHANICS 5 RC 2 Anders LARSSON Gentofte University Hospital Copenhagen University Hellerup, Denmark Saturday May 31, 2003 Euroanaesthesia
Respiratory System. Chapter 9
 Respiratory System Chapter 9 Air Intake Air in the atmosphere is mostly Nitrogen (78%) Only ~21% oxygen Carbon dioxide is less than 0.04% Air Intake Oxygen is required for Aerobic Cellular Respiration
Respiratory System Chapter 9 Air Intake Air in the atmosphere is mostly Nitrogen (78%) Only ~21% oxygen Carbon dioxide is less than 0.04% Air Intake Oxygen is required for Aerobic Cellular Respiration
Biomedical engineer s guide to the clinical aspects of intensive care mechanical ventilation
 https://doi.org/10.1186/s12938-018-0599-9 BioMedical Engineering OnLine REVIEW Open Access Biomedical engineer s guide to the clinical aspects of intensive care mechanical ventilation Vincent J. Major
https://doi.org/10.1186/s12938-018-0599-9 BioMedical Engineering OnLine REVIEW Open Access Biomedical engineer s guide to the clinical aspects of intensive care mechanical ventilation Vincent J. Major
ACUTE RESPIRATORY DISTRESS SYNDROME (ARDS) Rv
 Rv") ACUTE RESPIRATORY DISTRESS SYNDROME (ARDS) Rv.8.18.18 ACUTE RESPIRATORY DISTRESS SYNDROME (ARDS) SUDDEN PROGRESSIVE FORM OF ACUTE RESPIRATORY FAILURE ALVEOLAR CAPILLARY MEMBRANE BECOMES DAMAGED AND MORE
ACUTE RESPIRATORY DISTRESS SYNDROME (ARDS) Rv.8.18.18 ACUTE RESPIRATORY DISTRESS SYNDROME (ARDS) SUDDEN PROGRESSIVE FORM OF ACUTE RESPIRATORY FAILURE ALVEOLAR CAPILLARY MEMBRANE BECOMES DAMAGED AND MORE
Literature List Electrical Impedance Tomography
 Literature List Electrical Impedance Tomography 2017 Electrical Impedance Tomography (EIT) Literature List 2017 INDEX Writer Subject Publication Page Piraino T, Fan E Acute life-threatening hypoxemia during
Literature List Electrical Impedance Tomography 2017 Electrical Impedance Tomography (EIT) Literature List 2017 INDEX Writer Subject Publication Page Piraino T, Fan E Acute life-threatening hypoxemia during
The Prone Position Eliminates Compression of the Lungs by the Heart
 The Prone Position Eliminates Compression of the Lungs by the Heart RICHARD K. ALBERT and ROLF D. HUBMAYR Medical Service, Denver Health Medical Center, and Department of Medicine, University of Colorado
The Prone Position Eliminates Compression of the Lungs by the Heart RICHARD K. ALBERT and ROLF D. HUBMAYR Medical Service, Denver Health Medical Center, and Department of Medicine, University of Colorado
Introduction and Overview of Acute Respiratory Failure
 Introduction and Overview of Acute Respiratory Failure Definition: Acute Respiratory Failure Failure to oxygenate Inadequate PaO 2 to saturate hemoglobin PaO 2 of 60 mm Hg ~ SaO 2 of 90% PaO 2 of 50 mm
Introduction and Overview of Acute Respiratory Failure Definition: Acute Respiratory Failure Failure to oxygenate Inadequate PaO 2 to saturate hemoglobin PaO 2 of 60 mm Hg ~ SaO 2 of 90% PaO 2 of 50 mm
Airway pressure release ventilation (APRV) in PICU: Current evidence. Chor Yek Kee Sarawak General Hospital
 in PICU: Current evidence. Chor Yek Kee Sarawak General Hospital") Airway pressure release ventilation (APRV) in PICU: Current evidence Chor Yek Kee Sarawak General Hospital Outline Brief introduction of APRV History of APRV Common confusion in APRV Features of APRV and
Airway pressure release ventilation (APRV) in PICU: Current evidence Chor Yek Kee Sarawak General Hospital Outline Brief introduction of APRV History of APRV Common confusion in APRV Features of APRV and
THE ACUTE RESPIRATORY DISTRESS SYNDROME. Daniel Brockman, DO
 THE ACUTE RESPIRATORY DISTRESS SYNDROME Daniel Brockman, DO Objectives Describe the history and evolution of the diagnosis of ARDS Review the diagnostic criteria for ARDS Discuss the primary interventions
THE ACUTE RESPIRATORY DISTRESS SYNDROME Daniel Brockman, DO Objectives Describe the history and evolution of the diagnosis of ARDS Review the diagnostic criteria for ARDS Discuss the primary interventions
What is Acute Respiratory Distress Syndrome? Acute Respiratory Distress Syndrome (ARDS)
") Acute Respiratory Distress Syndrome (ARDS) Sonal Pannu, MD Clinical Assistant Professor Department of Internal Medicine Division of Pulmonary, Allergy, Critical Care and Sleep Medicine The Ohio State University
Acute Respiratory Distress Syndrome (ARDS) Sonal Pannu, MD Clinical Assistant Professor Department of Internal Medicine Division of Pulmonary, Allergy, Critical Care and Sleep Medicine The Ohio State University
Acute Respiratory Distress Syndrome (ARDS) What is Acute Respiratory Distress Syndrome?
 What is Acute Respiratory Distress Syndrome?") Acute Respiratory Distress Syndrome (ARDS) Sonal Pannu, MD Clinical Assistant Professor Department of Internal Medicine Division of Pulmonary, Allergy, Critical Care and Sleep Medicine The Ohio State University
Acute Respiratory Distress Syndrome (ARDS) Sonal Pannu, MD Clinical Assistant Professor Department of Internal Medicine Division of Pulmonary, Allergy, Critical Care and Sleep Medicine The Ohio State University
11 th Annual Congress Turkish Thoracic Society. Mechanical Ventilation in Acute Hypoxemic Respiratory Failure
 11 th Annual Congress Turkish Thoracic Society Mechanical Ventilation in Acute Hypoxemic Respiratory Failure Lluis Blanch MD PhD Senior Critical Care Center Scientific Director Corporació Parc Taulí Universitat
11 th Annual Congress Turkish Thoracic Society Mechanical Ventilation in Acute Hypoxemic Respiratory Failure Lluis Blanch MD PhD Senior Critical Care Center Scientific Director Corporació Parc Taulí Universitat
RESPIRATORY FAILURE. Michael Kelly, MD Division of Pediatric Critical Care Dept. of Pediatrics
 RESPIRATORY FAILURE Michael Kelly, MD Division of Pediatric Critical Care Dept. of Pediatrics What talk is he giving? DO2= CO * CaO2 CO = HR * SV CaO2 = (Hgb* SaO2 * 1.34) + (PaO2 * 0.003) Sound familiar??
RESPIRATORY FAILURE Michael Kelly, MD Division of Pediatric Critical Care Dept. of Pediatrics What talk is he giving? DO2= CO * CaO2 CO = HR * SV CaO2 = (Hgb* SaO2 * 1.34) + (PaO2 * 0.003) Sound familiar??
Oxygenation Failure. Increase FiO2. Titrate end-expiratory pressure. Adjust duty cycle to increase MAP. Patient Positioning. Inhaled Vasodilators
 Oxygenation Failure Increase FiO2 Titrate end-expiratory pressure Adjust duty cycle to increase MAP Patient Positioning Inhaled Vasodilators Extracorporeal Circulation ARDS Radiology Increasing Intensity
Oxygenation Failure Increase FiO2 Titrate end-expiratory pressure Adjust duty cycle to increase MAP Patient Positioning Inhaled Vasodilators Extracorporeal Circulation ARDS Radiology Increasing Intensity
VENTILATOR GRAPHICS ver.2.0. Charles S. Williams RRT, AE-C
 VENTILATOR GRAPHICS ver.2.0 Charles S. Williams RRT, AE-C Purpose Graphics are waveforms that reflect the patientventilator system and their interaction. Purposes of monitoring graphics: Allow users to
VENTILATOR GRAPHICS ver.2.0 Charles S. Williams RRT, AE-C Purpose Graphics are waveforms that reflect the patientventilator system and their interaction. Purposes of monitoring graphics: Allow users to
Case discussion Acute severe asthma during pregnancy. J.G. van der Hoeven
 Case discussion Acute severe asthma during pregnancy J.G. van der Hoeven Case (1) 32-year-old female - gravida 3 - para 2 Previous medical history - asthma Pregnant (33 w) Acute onset fever with wheezing
Case discussion Acute severe asthma during pregnancy J.G. van der Hoeven Case (1) 32-year-old female - gravida 3 - para 2 Previous medical history - asthma Pregnant (33 w) Acute onset fever with wheezing
Prone Position in ARDS
 Prone Position in ARDS Rich Kallet MS RRT FAARC, FCCM Respiratory Care Services Department of Anesthesia & Perioperative Care University of California, San Francisco, San Francisco General Hospital Case
Prone Position in ARDS Rich Kallet MS RRT FAARC, FCCM Respiratory Care Services Department of Anesthesia & Perioperative Care University of California, San Francisco, San Francisco General Hospital Case
Teacher : Dorota Marczuk Krynicka, MD., PhD. Coll. Anatomicum, Święcicki Street no. 6, Dept. of Physiology
 Title: Spirometry Teacher : Dorota Marczuk Krynicka, MD., PhD. Coll. Anatomicum, Święcicki Street no. 6, Dept. of Physiology I. Measurements of Ventilation Spirometry A. Pulmonary Volumes 1. The tidal
Title: Spirometry Teacher : Dorota Marczuk Krynicka, MD., PhD. Coll. Anatomicum, Święcicki Street no. 6, Dept. of Physiology I. Measurements of Ventilation Spirometry A. Pulmonary Volumes 1. The tidal
9/5/2018. Conflicts of Interests. Pediatric Acute Respiratory Distress Syndrome. Objectives ARDS ARDS. Definitions. None
 Pediatric Acute Respiratory Distress Syndrome Conflicts of Interests Diane C Lipscomb, MD Director Inpatient Pediatric Medical Director Mercy Springfield Associate Clerkship Clinical Director University
Pediatric Acute Respiratory Distress Syndrome Conflicts of Interests Diane C Lipscomb, MD Director Inpatient Pediatric Medical Director Mercy Springfield Associate Clerkship Clinical Director University
APPENDIX VI HFOV Quick Guide
 APPENDIX VI HFOV Quick Guide Overall goal: Maintain PH in the target range at the minimum tidal volume. This is achieved by favoring higher frequencies over lower P (amplitude). This goal is also promoted
APPENDIX VI HFOV Quick Guide Overall goal: Maintain PH in the target range at the minimum tidal volume. This is achieved by favoring higher frequencies over lower P (amplitude). This goal is also promoted
The Art and Science of Weaning from Mechanical Ventilation
 The Art and Science of Weaning from Mechanical Ventilation Shekhar T. Venkataraman M.D. Professor Departments of Critical Care Medicine and Pediatrics University of Pittsburgh School of Medicine Some definitions
The Art and Science of Weaning from Mechanical Ventilation Shekhar T. Venkataraman M.D. Professor Departments of Critical Care Medicine and Pediatrics University of Pittsburgh School of Medicine Some definitions
The use of proning in the management of Acute Respiratory Distress Syndrome
 Case 3 The use of proning in the management of Acute Respiratory Distress Syndrome Clinical Problem This expanded case summary has been chosen to explore the rationale and evidence behind the use of proning
Case 3 The use of proning in the management of Acute Respiratory Distress Syndrome Clinical Problem This expanded case summary has been chosen to explore the rationale and evidence behind the use of proning
Mechanical Ventilation 1. Shari McKeown, RRT Respiratory Services - VGH
 Mechanical Ventilation 1 Shari McKeown, RRT Respiratory Services - VGH Objectives Describe indications for mcvent Describe types of breaths and modes of ventilation Describe compliance and resistance and
Mechanical Ventilation 1 Shari McKeown, RRT Respiratory Services - VGH Objectives Describe indications for mcvent Describe types of breaths and modes of ventilation Describe compliance and resistance and
Lecture Notes. Chapter 3: Asthma
 Lecture Notes Chapter 3: Asthma Objectives Define asthma and status asthmaticus List the potential causes of asthma attacks Describe the effect of asthma attacks on lung function List the clinical features
Lecture Notes Chapter 3: Asthma Objectives Define asthma and status asthmaticus List the potential causes of asthma attacks Describe the effect of asthma attacks on lung function List the clinical features
How the Knowledge Proceeds in Intensive Care: the ARDS Example
 How the Knowledge Proceeds in Intensive Care: the ARDS Example 2016, Antalya Luciano Gattinoni, MD, FRCP Georg-August-Universität Göttingen Germany INDUCTION: From particular (application) to general (law/theory)
How the Knowledge Proceeds in Intensive Care: the ARDS Example 2016, Antalya Luciano Gattinoni, MD, FRCP Georg-August-Universität Göttingen Germany INDUCTION: From particular (application) to general (law/theory)
a. Describe the physiological consequences of intermittent positive pressure ventilation and positive end-expiratory pressure.
 B. 10 Applied Respiratory Physiology a. Describe the physiological consequences of intermittent positive pressure ventilation and positive end-expiratory pressure. Intermittent positive pressure ventilation
B. 10 Applied Respiratory Physiology a. Describe the physiological consequences of intermittent positive pressure ventilation and positive end-expiratory pressure. Intermittent positive pressure ventilation
We are IntechOpen, the world s leading publisher of Open Access books Built by scientists, for scientists. International authors and editors
 We are IntechOpen, the world s leading publisher of Open Access books Built by scientists, for scientists 3,800 116,000 120M Open access books available International authors and editors Downloads Our
We are IntechOpen, the world s leading publisher of Open Access books Built by scientists, for scientists 3,800 116,000 120M Open access books available International authors and editors Downloads Our
Tracking lung recruitment and regional tidal volume at the bedside. Antonio Pesenti
 Tracking lung recruitment and regional tidal volume at the bedside Antonio Pesenti Conflicts of Interest Maquet: Received research support and consultation fees Drager: Received research support and consultation
Tracking lung recruitment and regional tidal volume at the bedside Antonio Pesenti Conflicts of Interest Maquet: Received research support and consultation fees Drager: Received research support and consultation
MECHANICAL VENTILATION PROTOCOLS
 GENERAL or SURGICAL Initial Ventilator Parameters Ventilator Management (see appendix I) Assess Patient Data (see appendix II) Data Collection Mode: Tidal Volume: FIO2: PEEP: Rate: I:E Ratio: ACUTE PHASE
GENERAL or SURGICAL Initial Ventilator Parameters Ventilator Management (see appendix I) Assess Patient Data (see appendix II) Data Collection Mode: Tidal Volume: FIO2: PEEP: Rate: I:E Ratio: ACUTE PHASE
Pulmonary & Extra-pulmonary ARDS: FIZZ or FUSS?
 Pulmonary & Extra-pulmonary ARDS: FIZZ or FUSS? Dr. Rajagopala Srinivas Senior Resident, Dept. Pulmonary Medicine, PGIMER, Chandigarh. The beginning.. "The etiology of this respiratory distress syndrome
Pulmonary & Extra-pulmonary ARDS: FIZZ or FUSS? Dr. Rajagopala Srinivas Senior Resident, Dept. Pulmonary Medicine, PGIMER, Chandigarh. The beginning.. "The etiology of this respiratory distress syndrome
RESCUE VENTILATION SUMMARY
 DISCLAIMER: These guidelines were prepared by the Department of Surgical Education, Orlando Regional Medical Center. They are intended to serve as a general statement regarding appropriate patient care
DISCLAIMER: These guidelines were prepared by the Department of Surgical Education, Orlando Regional Medical Center. They are intended to serve as a general statement regarding appropriate patient care
Effects of patient positioning on respiratory mechanics in mechanically ventilated ICU patients
 Review Article Page 1 of 9 Effects of patient positioning on respiratory mechanics in mechanically ventilated ICU patients Mehdi Mezidi 1,2, Claude Guérin 1,2,3 1 Service de réanimation médicale, Hôpital
Review Article Page 1 of 9 Effects of patient positioning on respiratory mechanics in mechanically ventilated ICU patients Mehdi Mezidi 1,2, Claude Guérin 1,2,3 1 Service de réanimation médicale, Hôpital
Severe Hypoxemic Respiratory Failure
 CHEST Postgraduate Education Corner CONTEMPORARY REVIEWS IN CRITICAL CARE MEDICINE Severe Hypoxemic Respiratory Failure Part 1 Ventilatory Strategies Adebayo Esan, MD ; Dean R. Hess, PhD, RRT, FCCP ; Suhail
CHEST Postgraduate Education Corner CONTEMPORARY REVIEWS IN CRITICAL CARE MEDICINE Severe Hypoxemic Respiratory Failure Part 1 Ventilatory Strategies Adebayo Esan, MD ; Dean R. Hess, PhD, RRT, FCCP ; Suhail
Ventilator Waveforms: Interpretation
 Ventilator Waveforms: Interpretation Albert L. Rafanan, MD, FPCCP Pulmonary, Critical Care and Sleep Medicine Chong Hua Hospital, Cebu City Types of Waveforms Scalars are waveform representations of pressure,
Ventilator Waveforms: Interpretation Albert L. Rafanan, MD, FPCCP Pulmonary, Critical Care and Sleep Medicine Chong Hua Hospital, Cebu City Types of Waveforms Scalars are waveform representations of pressure,
One Lung Ventilation in Obese patients
 One Lung Ventilation in Obese patients YUSNI PUSPITA DEPARTEMEN ANESTESIOLOGI DAN TERAPI INTENSIF FAKULTAS KEDOKTERAN UNIVERSITAS SRIWIJAYA/RSMH PALEMBANG One Lung Ventilation Lung isolation techniques
One Lung Ventilation in Obese patients YUSNI PUSPITA DEPARTEMEN ANESTESIOLOGI DAN TERAPI INTENSIF FAKULTAS KEDOKTERAN UNIVERSITAS SRIWIJAYA/RSMH PALEMBANG One Lung Ventilation Lung isolation techniques
Surviving Sepsis Campaign. Guidelines for Management of Severe Sepsis/Septic Shock. An Overview
 Surviving Sepsis Campaign Guidelines for Management of Severe Sepsis/Septic Shock An Overview Mechanical Ventilation of Sepsis-Induced ALI/ARDS ARDSnet Mechanical Ventilation Protocol Results: Mortality
Surviving Sepsis Campaign Guidelines for Management of Severe Sepsis/Septic Shock An Overview Mechanical Ventilation of Sepsis-Induced ALI/ARDS ARDSnet Mechanical Ventilation Protocol Results: Mortality
Variation in lung with normal, quiet breathing. Minimal lung volume (residual volume) at maximum deflation. Total lung capacity at maximum inflation
 at maximum deflation. Total lung capacity at maximum inflation") r Total lung capacity at maximum inflation Variation in lung with normal, quiet breathing Volume of lungs at end of normal inspiration (average 2,200 ml) Minimal lung volume (residual volume) at maximum
r Total lung capacity at maximum inflation Variation in lung with normal, quiet breathing Volume of lungs at end of normal inspiration (average 2,200 ml) Minimal lung volume (residual volume) at maximum
Proportional Assist Ventilation (PAV) (NAVA) Younes ARRD 1992;145:114. Ventilator output :Triggering, Cycling Control of flow, rise time and pressure
 (NAVA) Younes ARRD 1992;145:114. Ventilator output :Triggering, Cycling Control of flow, rise time and pressure") Conflict of Interest Disclosure Robert M Kacmarek Unconventional Techniques Using Your ICU Ventilator!" 5-5-17 FOCUS Bob Kacmarek PhD, RRT Massachusetts General Hospital, Harvard Medical School, Boston,
Conflict of Interest Disclosure Robert M Kacmarek Unconventional Techniques Using Your ICU Ventilator!" 5-5-17 FOCUS Bob Kacmarek PhD, RRT Massachusetts General Hospital, Harvard Medical School, Boston,
Bi-Level Therapy: Boosting Comfort & Compliance in Apnea Patients
 Bi-Level Therapy: Boosting Comfort & Compliance in Apnea Patients Objectives Describe nocturnal ventilation characteristics that may indicate underlying conditions and benefits of bilevel therapy for specific
Bi-Level Therapy: Boosting Comfort & Compliance in Apnea Patients Objectives Describe nocturnal ventilation characteristics that may indicate underlying conditions and benefits of bilevel therapy for specific
NIV use in ED. Dr. Khalfan AL Amrani Emergency Resuscitation Symposium 2 nd May 2016 SQUH
 NIV use in ED Dr. Khalfan AL Amrani Emergency Resuscitation Symposium 2 nd May 2016 SQUH Outline History & Introduction Overview of NIV application Review of proven uses of NIV History of Ventilation 1940
NIV use in ED Dr. Khalfan AL Amrani Emergency Resuscitation Symposium 2 nd May 2016 SQUH Outline History & Introduction Overview of NIV application Review of proven uses of NIV History of Ventilation 1940
Sub-category: Intensive Care for Respiratory Distress
 Course n : Course 3 Title: RESPIRATORY PHYSIOLOGY, PHYSICS AND PATHOLOGY IN RELATION TO ANAESTHESIA AND INTENSIVE CARE Sub-category: Intensive Care for Respiratory Distress Topic: Acute Respiratory Distress
Course n : Course 3 Title: RESPIRATORY PHYSIOLOGY, PHYSICS AND PATHOLOGY IN RELATION TO ANAESTHESIA AND INTENSIVE CARE Sub-category: Intensive Care for Respiratory Distress Topic: Acute Respiratory Distress
Seminar. Current Concepts
 Seminar Current Concepts In ARDS What I think is possible to cover in 40 minutes- Definition Management Ventilatory strategies Conventional LPV Rescue therapy Non Ventilatory strategies Definition and
Seminar Current Concepts In ARDS What I think is possible to cover in 40 minutes- Definition Management Ventilatory strategies Conventional LPV Rescue therapy Non Ventilatory strategies Definition and
ARDS & TBI - Trading Off Ventilation Targets
 ARDS & TBI - Trading Off Ventilation Targets Salvatore M. Maggiore, MD, PhD Rome, Italy smmaggiore@rm.unicatt.it Conflict of interest Principal Investigator: RINO trial o Nasal high-flow vs Venturi mask
ARDS & TBI - Trading Off Ventilation Targets Salvatore M. Maggiore, MD, PhD Rome, Italy smmaggiore@rm.unicatt.it Conflict of interest Principal Investigator: RINO trial o Nasal high-flow vs Venturi mask
Respiratory Physiology
 Respiratory Physiology Dr. Aida Korish Associate Prof. Physiology KSU The main goal of respiration is to 1-Provide oxygen to tissues 2- Remove CO2 from the body. Respiratory system consists of: Passages
Respiratory Physiology Dr. Aida Korish Associate Prof. Physiology KSU The main goal of respiration is to 1-Provide oxygen to tissues 2- Remove CO2 from the body. Respiratory system consists of: Passages
A simple case of.. Acute severe asthma. MasterclassIC Schiermonnikoog 2017
 A simple case of.. Acute severe asthma MasterclassIC Schiermonnikoog 2017 Case (1) Female, 27 - G1P0 (26 weeks) PMH - several admissions for severe acute asthma (no MV) Progressive dyspnea for 1 week Admitted
A simple case of.. Acute severe asthma MasterclassIC Schiermonnikoog 2017 Case (1) Female, 27 - G1P0 (26 weeks) PMH - several admissions for severe acute asthma (no MV) Progressive dyspnea for 1 week Admitted
Experience with Low Flow ECCO2R device on a CRRT platform : CO2 removal
 Experience with Low Flow ECCO2R device on a CRRT platform : CO2 removal Alain Combes, MD, PhD, Hôpital Pitié-Salpêtrière, AP-HP Inserm UMRS 1166, ican, Institute of Cardiometabolism and Nutrition Pierre
Experience with Low Flow ECCO2R device on a CRRT platform : CO2 removal Alain Combes, MD, PhD, Hôpital Pitié-Salpêtrière, AP-HP Inserm UMRS 1166, ican, Institute of Cardiometabolism and Nutrition Pierre
Omar Sami. Mustafa Khader. Yanal Shafaqouj
 8 Omar Sami Mustafa Khader Yanal Shafaqouj Let us retrieve our discussion about the ventilation-perfusion ratio (V/Q). - When (V/Q) is Zero this means that no ventilation is taking place, V is Zero; bronchial
8 Omar Sami Mustafa Khader Yanal Shafaqouj Let us retrieve our discussion about the ventilation-perfusion ratio (V/Q). - When (V/Q) is Zero this means that no ventilation is taking place, V is Zero; bronchial
EFFECT OF NASAL-CPAP ON PATIENTS WITH CHRONIC OBSTRUCTIVE PULMONARY DISEASE
 EFFECT OF NASAL-CPAP ON PATIENTS WITH CHRONIC OBSTRUCTIVE PULMONARY DISEASE TKLim ABSTRACT Patients with chronic obstructive pulmonary disease [COPD] breath at large lung volumes because of dynamic hyperinflation.
EFFECT OF NASAL-CPAP ON PATIENTS WITH CHRONIC OBSTRUCTIVE PULMONARY DISEASE TKLim ABSTRACT Patients with chronic obstructive pulmonary disease [COPD] breath at large lung volumes because of dynamic hyperinflation.
7 Initial Ventilator Settings, ~05
 Abbreviations (inside front cover and back cover) PART 1 Basic Concepts and Core Knowledge in Mechanical -- -- -- -- 1 Oxygenation and Acid-Base Evaluation, 1 Review 01Arterial Blood Gases, 2 Evaluating
Abbreviations (inside front cover and back cover) PART 1 Basic Concepts and Core Knowledge in Mechanical -- -- -- -- 1 Oxygenation and Acid-Base Evaluation, 1 Review 01Arterial Blood Gases, 2 Evaluating
Foundation in Critical Care Nursing. Airway / Respiratory / Workbook
 Foundation in Critical Care Nursing Airway / Respiratory / Workbook Airway Anatomy: Please label the following: Tongue Larynx Epiglottis Pharynx Trachea Vertebrae Oesophagus Where is the ET (endotracheal)
Foundation in Critical Care Nursing Airway / Respiratory / Workbook Airway Anatomy: Please label the following: Tongue Larynx Epiglottis Pharynx Trachea Vertebrae Oesophagus Where is the ET (endotracheal)
Pro - Con Debate APRV vs Conventional Ventilation. Pro Jon Marinaro, MD
 Pro - Con Debate APRV vs Conventional Ventilation Pro Jon Marinaro, MD PRO CON Volume Assist Control Mode ARDS MORTALITY OVER LAST 50 YEARS 53 year old female with 50% Flame Burn to Chest, Flanks & Buttocks
Pro - Con Debate APRV vs Conventional Ventilation Pro Jon Marinaro, MD PRO CON Volume Assist Control Mode ARDS MORTALITY OVER LAST 50 YEARS 53 year old female with 50% Flame Burn to Chest, Flanks & Buttocks
Author: Thomas Sisson, MD, 2009
 Author: Thomas Sisson, MD, 2009 License: Unless otherwise noted, this material is made available under the terms of the Creative Commons Attribution Non-commercial Share Alike 3.0 License: http://creativecommons.org/licenses/by-nc-sa/3.0/
Author: Thomas Sisson, MD, 2009 License: Unless otherwise noted, this material is made available under the terms of the Creative Commons Attribution Non-commercial Share Alike 3.0 License: http://creativecommons.org/licenses/by-nc-sa/3.0/
Respiratory System. BSC 2086 A&P 2 Professor Tcherina Duncombe Palm Beach State College
 Respiratory System BSC 2086 A&P 2 Professor Tcherina Duncombe Palm Beach State College Respiration Ventilation of lungs Gas exchange between air/bld and bld/tissue Use of oxygen in cellular respiration
Respiratory System BSC 2086 A&P 2 Professor Tcherina Duncombe Palm Beach State College Respiration Ventilation of lungs Gas exchange between air/bld and bld/tissue Use of oxygen in cellular respiration
Weaning from Mechanical Ventilation. Dr Azmin Huda Abdul Rahim
 Weaning from Mechanical Ventilation Dr Azmin Huda Abdul Rahim Content Definition Classification Weaning criteria Weaning methods Criteria for extubation Introduction Weaning comprises 40% of the duration
Weaning from Mechanical Ventilation Dr Azmin Huda Abdul Rahim Content Definition Classification Weaning criteria Weaning methods Criteria for extubation Introduction Weaning comprises 40% of the duration
Principles of Mechanical Ventilation
 47 Principles of Mechanical Ventilation Jonathan E. Sevransky, MD, MHS Objectives Understand the indications for treatment with mechanical ventilation Describe ventilator strategies that will minimize
47 Principles of Mechanical Ventilation Jonathan E. Sevransky, MD, MHS Objectives Understand the indications for treatment with mechanical ventilation Describe ventilator strategies that will minimize
How to Do PAP Therapy: VAPS, Trilogy
 Workshop: Non- Invasive Ven?la?on October 9, 2014 How to Do PAP Therapy: VAPS, Trilogy Lisa F. Wolfe Associate Professor of Medicine Northwestern University Feinberg School of Medicine Chicago, Illinois
Workshop: Non- Invasive Ven?la?on October 9, 2014 How to Do PAP Therapy: VAPS, Trilogy Lisa F. Wolfe Associate Professor of Medicine Northwestern University Feinberg School of Medicine Chicago, Illinois
Critical Care Monitoring. Assessing the Adequacy of Tissue Oxygenation. Tissue Oxygenation - Step 1. Tissue Oxygenation
 Critical Care Monitoring 1 Assessing the Adequacy of Tissue oxygenation is the end-product of many complex steps 2 - Step 1 Oxygen must be made available to alveoli 3 1 - Step 2 Oxygen must cross the alveolarcapillary
Critical Care Monitoring 1 Assessing the Adequacy of Tissue oxygenation is the end-product of many complex steps 2 - Step 1 Oxygen must be made available to alveoli 3 1 - Step 2 Oxygen must cross the alveolarcapillary