Temperature Correction of Blood Gas Measurements during Therapeutic Hypothermia: Is it Time to Chill Out?
|
|
|
- Eugene Cannon
- 6 years ago
- Views:
Transcription
1 Temperature Correction of Blood Gas Measurements during Therapeutic Hypothermia: Is it Time to Chill Out? Dr. Elizabeth Zorn Dr. Gwenyth Fischer Dr. Martha Lyon
2 Disclosures (ML) Speaking Honoraria Radiometer Nova Biomedical Draeger Research Support (Reagents, Instrumentation, Travel) Nova Biomedical Roche Diagnostics (Canada) Radiometer Instrumentation Laboratories (Canada) ALOL Biomedical Inc Clinical Laboratory Consulting Business
3 Disclosures (EZ) Nothing to disclose
4 Disclosures (GF) Nothing to disclose
5 Objectives 1) To describe the pathophysiology of newborn hypoxic ischemic encephalopathy (HIE) 2) To discuss why therapeutic hypothermia is an effective treatment for HIE. 3) To review the alpha-stat versus the ph- stat strategies (and limitations of each) for measuring and reporting blood gas results during therapeutic hypothermia. 4) To outline the inconsistency in the measurement and reporting of blood gas parameters in the published clinical trials that demonstrated the efficacy of therapeutic hypothermia 5) To present clinical cases and discuss how the inconsistency in reporting blood gas results could influence the care of the neonate.
6 Clinical Case Example An outside hospital calls to request transport for a newborn 39w5d gestation female infant, birth weight 3050 g Mother presented to hospital with spontaneous rupture of membranes, meconium-stained fluid During fetal monitoring, noted to have down tones so stat C section was performed
7 Clinical Case Example At delivery, infant is limp, blue, and pulseless Immediately intubated, received chest compressions, epinephrine, bicarb, and calcium Required chest compressions for 20 minutes, multiple doses of epinephrine APGARs were 0, 1, 1, 1, 1 at 1, 5, 10, 15, and 20 minutes of age Arterial blood gas: ph 6.75, CO2 123, O2 108, HCO3 17
8 Clinical Case Example When our transport team arrived, infant was noted to be intubated and unresponsive Passive cooling initiated during transport to our facility Upon arrival, examination showed an unresponsive infant with no purposeful movements, minimal pupillary reaction to light, and intermittent lip-smacking and upper extremity jerking Admission temperature 32.7⁰C Seizure activity confirmed on a EEG
9 Clinical Case Example Admission laboratory data: Na 143, K 3.6, Cl 102, CO2 12, BUN 8, Creatinine 0.78, Glucose 165 ALT 142, AST 312 Lactate 19 ABG 7.11/38/87/12/-16 WBC 35.9, hgb 14.6, plt 142 INR 2.4, PTT 88, fibrinogen 98
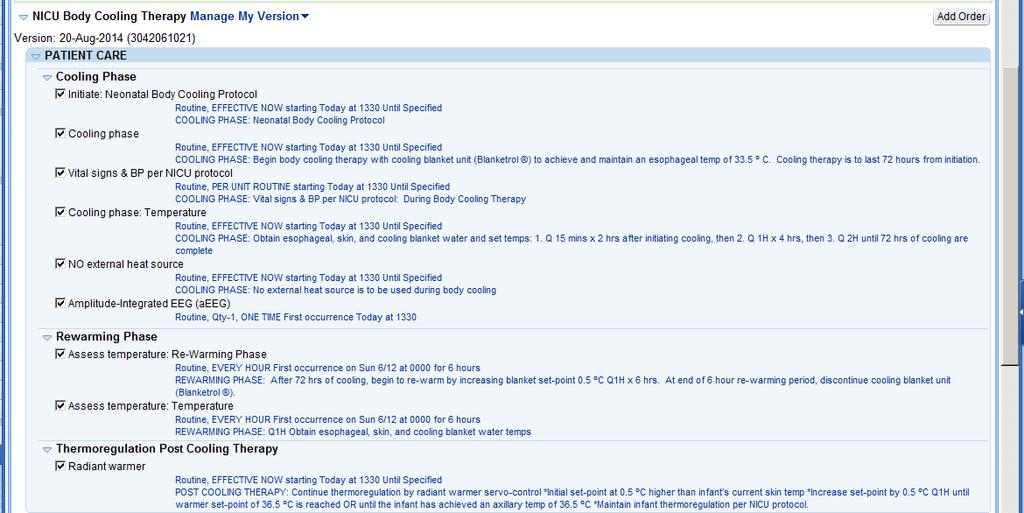
10 Clinical Case Example Plan: Neuro: Initiate therapeutic hypothermia (33.5 C for 72 hours). Loaded with phenobarbital x2 and keppra for seizures. FEN: TPN with total fluids written for 40 ml/kg/day due to anuria. Respiratory: Conventional mechanical ventilation CV: Dopamine and hydrocortisone started for hypotension ID: Started on ampicillin, gentamycin, and acyclovir (mother with HSV but treated during pregnancy and infant delivered via c-section) Heme: Coagulopathy treated with FFP and cryoprecipitate, continue to monitor coags Sedation: Fentanyl prn
11

12

13 Neonate Hypoxic Ischemic Encephalopathy (HIE) Lack of oxygen in the brain around the time of birth (perinatal asphyxia) affects 3-5 infants/1000 live births infants per 1000 live births develop brain damage in the form of HIE Up to 60% of infants with HIE will die and 25% of survivors will have long term neurodevelopmental sequelae
14 Therapeutic mild hypothermia (33.5⁰C) is currently the only neuroprotective treatment to have been clinically tested in large trials to minimize brain injury in term newborns Prior to the hypothermia clinical trials, supportive measures (no specific therapies) were only available for HIE
15 Which babies are eligible for therapeutic hypothermia? Therapeutic mild hypothermia (33.5⁰C) is currently the only neuroprotective treatment to have been clinically tested in large trials to minimize brain injury in term newborns Prior to the hypothermia clinical trials, supportive measures (no specific therapies) were only available for HIE
16 Which babies are eligible for therapeutic hypothermia? Based on inclusion criteria published in clinical trials Therapeutic mild hypothermia (33.5⁰C) is currently the only neuroprotective treatment to have been clinically tested in large trials to minimize brain injury in term newborns Prior to the hypothermia clinical trials, supportive measures (no specific therapies) were only available for HIE
17 Which babies are eligible for therapeutic hypothermia? Based on inclusion criteria published in clinical trials 36 weeks gestation and 6 hours of age Therapeutic mild hypothermia (33.5⁰C) is currently the only neuroprotective treatment to have been clinically tested in large trials to minimize brain injury in term newborns Prior to the hypothermia clinical trials, supportive measures (no specific therapies) were only available for HIE
18 Which babies are eligible for therapeutic hypothermia? Based on inclusion criteria published in clinical trials 36 weeks gestation and 6 hours of age ph 7.0 or a base deficit of 16 mmol/l (cord blood or blood collected within the first hour of birth) Therapeutic mild hypothermia (33.5⁰C) is currently the only neuroprotective treatment to have been clinically tested in large trials to minimize brain injury in term newborns Prior to the hypothermia clinical trials, supportive measures (no specific therapies) were only available for HIE
19 Which babies are eligible for therapeutic hypothermia? Based on inclusion criteria published in clinical trials 36 weeks gestation and 6 hours of age ph 7.0 or a base deficit of 16 mmol/l (cord blood or blood collected within the first hour of birth) History of an acute perinatal event Therapeutic mild hypothermia (33.5⁰C) is currently the only neuroprotective treatment to have been clinically tested in large trials to minimize brain injury in term newborns Prior to the hypothermia clinical trials, supportive measures (no specific therapies) were only available for HIE
20 Which babies are eligible for therapeutic hypothermia? Based on inclusion criteria published in clinical trials 36 weeks gestation and 6 hours of age ph 7.0 or a base deficit of 16 mmol/l (cord blood or blood collected within the first hour of birth) History of an acute perinatal event 10 minute APGAR score < 5 Therapeutic mild hypothermia (33.5⁰C) is currently the only neuroprotective treatment to have been clinically tested in large trials to minimize brain injury in term newborns Prior to the hypothermia clinical trials, supportive measures (no specific therapies) were only available for HIE
21 Which babies are eligible for therapeutic hypothermia? Based on inclusion criteria published in clinical trials 36 weeks gestation and 6 hours of age ph 7.0 or a base deficit of 16 mmol/l (cord blood or blood collected within the first hour of birth) History of an acute perinatal event 10 minute APGAR score < 5 Assisted ventilation initiated at birth and continued for at least 10 minutes Therapeutic mild hypothermia (33.5⁰C) is currently the only neuroprotective treatment to have been clinically tested in large trials to minimize brain injury in term newborns Prior to the hypothermia clinical trials, supportive measures (no specific therapies) were only available for HIE
22 Which babies are eligible for therapeutic hypothermia? Based on inclusion criteria published in clinical trials 36 weeks gestation and 6 hours of age ph 7.0 or a base deficit of 16 mmol/l (cord blood or blood collected within the first hour of birth) History of an acute perinatal event 10 minute APGAR score < 5 Assisted ventilation initiated at birth and continued for at least 10 minutes Neurologic examination demonstrating moderate to severe encephalopathy is essential Therapeutic mild hypothermia (33.5⁰C) is currently the only neuroprotective treatment to have been clinically tested in large trials to minimize brain injury in term newborns Prior to the hypothermia clinical trials, supportive measures (no specific therapies) were only available for HIE
23 Pathophysiology of HIE
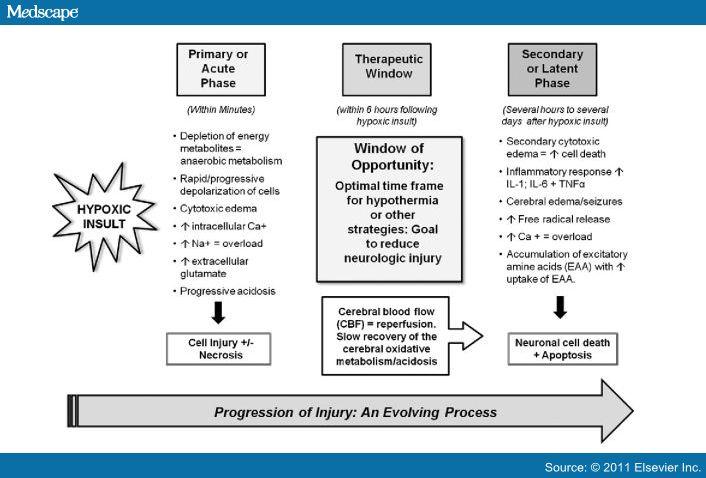
24 Pathophysiology of HIE
25 How/Why is Hypothermia Neuroprotective? Reducing brain perfusion and metabolism
26 How/Why is Hypothermia Neuroprotective? Reducing brain perfusion and metabolism Decrease of cellular oxygen and glucose requirements by 5-8% per ⁰C decrease in temperature This leads to a decrease in CO 2 production Hypocapnia with normoxemia induces cerebral vasoconstriction and decreases cerebral blood flow Mitigate reperfusion injury
27 How/Why is Hypothermia Neuroprotective? Reducing brain perfusion and metabolism Decrease free radical production
28 How/Why is Hypothermia Neuroprotective? Reducing brain perfusion and metabolism Decrease free radical production Decrease the immune response
29 How/Why is Hypothermia Neuroprotective? Reducing brain perfusion and metabolism Decrease free radical production Decrease the immune response Suppression of epileptic activity

30 Other Clinical Situations With Hypothermic Patients Cooling for head trauma in older children and adults Near drowning events Weather exposure Use of extracorporeal machines such as dialysis and ecmo

31 Cooling Older Patients External Cooling Ice Packs Water Immersion Cooling Blankets Conductive Pads Internal Cooling Ice Lavage Cooled IV Fluids Catheter Based Cooling Technologies Arctic Sun Device
32 Will hypothermia affect blood gas parameters?
33 Henry s Law William Henry December 12, 1774 September 2, 1836 At a constant temperature, the amount of a given gas that dissolves in a given type and volume of liquid is directly proportional to the partial pressure of that gas in equilibrium with that liquid
34 Henry s Law William Henry December 12, 1774 September 2, 1836 C = K/P gas Mass of a gas dissolved in a solution
35 Henry s Law Solvent and temperature dependent Henry s Law Constant William Henry December 12, 1774 September 2, 1836 C = K/P gas Mass of a gas dissolved in a solution
36 Henry s Law Henry s Law Constant William Henry December 12, 1774 September 2, 1836 C = K/P gas Mass of a gas dissolved in a solution Partial Pressure of the gas
37 Mild therapeutic hypothermia to a rectal temperature of 34 ± 0.5⁰C initiated as soon as possible within the first 6 hours of life Cooling can be achieved by either total body or selective head cooling
38
39
40 Blood gas measurement in the clinical laboratory Blood gas instruments commonly conduct their analysis of blood gas parameters by warming the blood gas specimen to 37⁰C Most instruments can calculate and present temperature corrected values
41 Blood gas measurement in the clinical laboratory Blood gas instruments commonly conduct their analysis of blood gas parameters by warming the blood gas specimen to 37⁰C Most instruments can calculate temperature corrected values pco 2 (T) = pco 2 (37) X 10 [0.021X(t-37)]
42
43 HIE Neonate Which pco 2 is truth? DATE pco2 (37) pco2 (33.5) pco2 (34.5) Day 1 4:20:00 PM Day 1 10:05:00 PM Day 2 4:00:00 AM Day 2 10:05:00 AM Day 2 12:20:00 PM Day 2 3:10:00 PM Day 2 6:00:00 PM Day 2 10:30:00 PM Day 2 11:55:00 PM Day 3 4:00:00 AM Day 3 10:00:00 AM Day 3 4:00:00 PM Day 3 10:00:00 PM Day 4 4:00:00 AM Day 4 6:05:00 PM
44 HIE Neonate Which pco 2 is truth? DATE pco2 (37) pco2 (33.5) pco2 (34.5) Day 1 4:20:00 PM Day 1 10:05:00 PM Day 2 4:00:00 AM Day 2 10:05:00 AM Day 2 12:20:00 PM Day 2 3:10:00 PM Day 2 6:00:00 PM Day 2 10:30:00 PM Day 2 11:55:00 PM Day 3 4:00:00 AM Day 3 10:00:00 AM Day 3 4:00:00 PM Day 3 10:00:00 PM Day 4 4:00:00 AM Day 4 6:05:00 PM
45 Two Schools of Thought Alpha stat school Do not correct to body temperature ph stat school Do correct to body temperature
46 Two Schools of Thought Alpha stat versus ph stat controversy Should ventilation be adjusted to achieve a temperature uncorrected pco 2 of 40 mm Hg (alpha stat) or adjusted to achieve a temperature corrected pco 2 of 40 mm Hg (ph stat) - Chris Higgins, Jan 2016 Temperature Correction of Blood gas and ph measurementan unresolved controversy
47 Alpha Stat Do not correct to body temperature
48 Alpha Stat Do not correct to body temperature Initially based on the publications: Davis BD. On the importance of being ionized. Archives of Biochemistry and Biophysics 78: , 1958 Reeves RB. An imidazole alphastat hypothesis for vertebrate acid base regulation: Tissue carbon dioxide content and body temperature in bullfrogs Respiration Physiology 14: , 1972
49 Alpha Stat Do not correct to body temperature Initially based on the publications: Davis BD. On the importance of being ionized. Archives of Biochemistry and Biophysics 78: , 1958 Reeves RB. An imidazole alphastat hypothesis for vertebrate acid base regulation: Tissue carbon dioxide content and body temperature in bullfrogs Respiration Physiology 14: , 1972 Intracellular ph remains at or close to neutrality (with temperature) largely due to protein buffering (phosphate and bicarbonate buffers also functional)
50 Alpha Stat Do not correct to body temperature Initially based on the publications: Davis BD. On the importance of being ionized. Archives of Biochemistry and Biophysics 78: , 1958 Reeves RB. An imidazole alphastat hypothesis for vertebrate acid base regulation: Tissue carbon dioxide content and body temperature in bullfrogs Respiration Physiology 14: , 1972 Intracellular ph remains at or close to neutrality (with temperature) largely due to protein buffering (phosphate and bicarbonate buffers also functional) Established reference ranges for interpretation of blood gas values have been determined at 37⁰C
51 ph Stat Do correct to body temperature Level of CO 2 is externally controlled to maintain normal ph and CO 2 of the temperature corrected values It best represents what is happening in the patient Concerned about the application of Henry s law
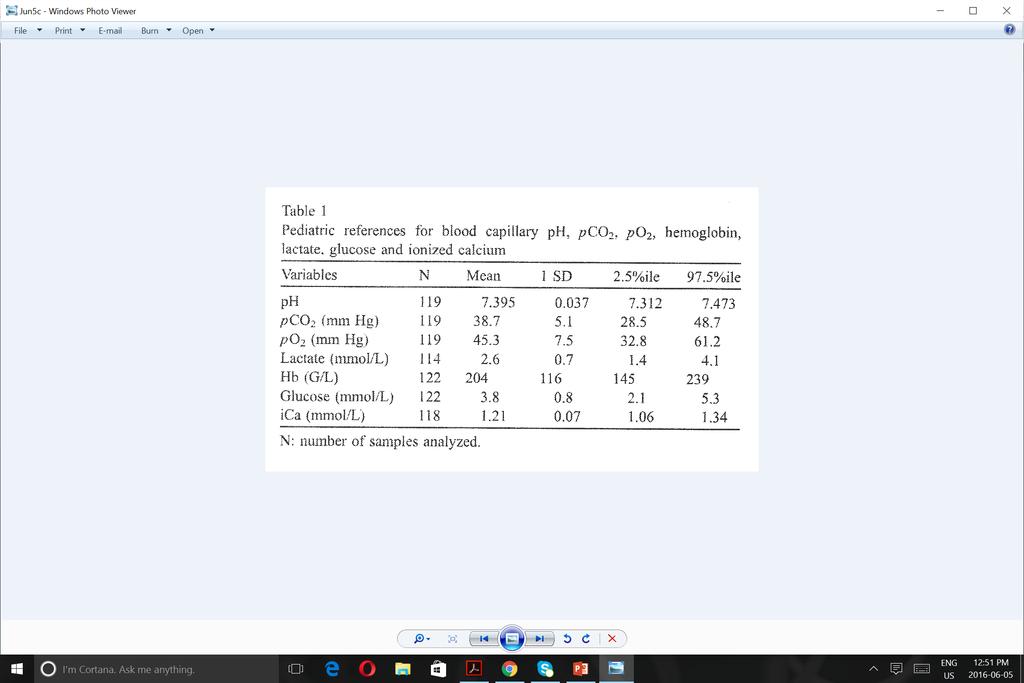
52 A closer look at blood gases reference ranges as it relates to HIE and therapeutic hypothermia
53 A closer look at blood gases reference ranges as it relates to HIE and therapeutic hypothermia 36 weeks gestation and 6 hours of age duration of the hypothermia is 72 hours (3 days post natal)
54
55
56
57
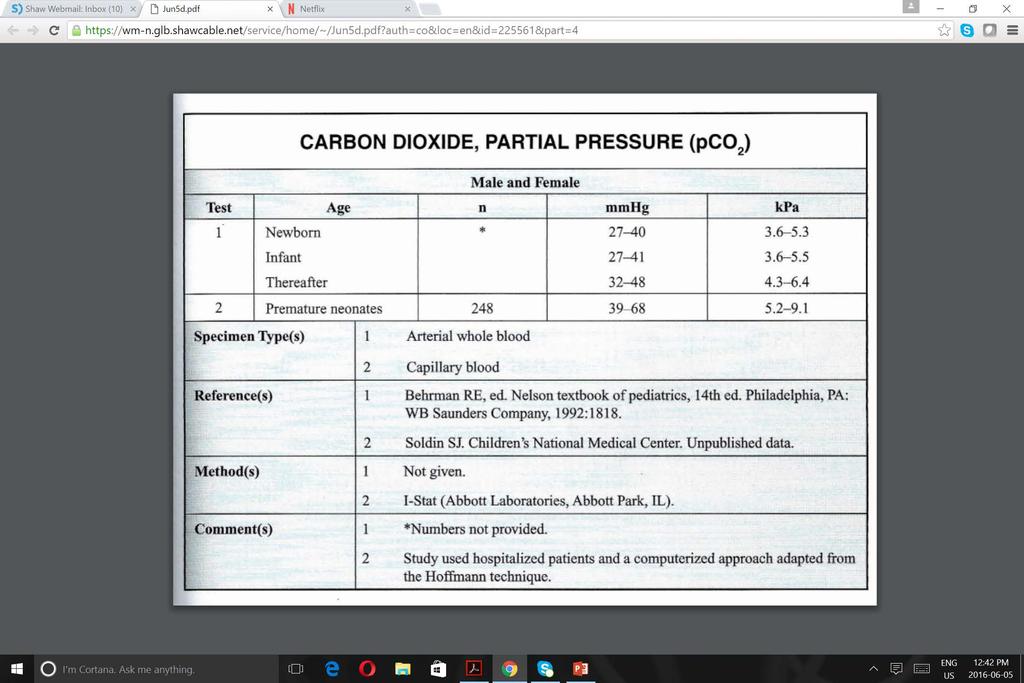
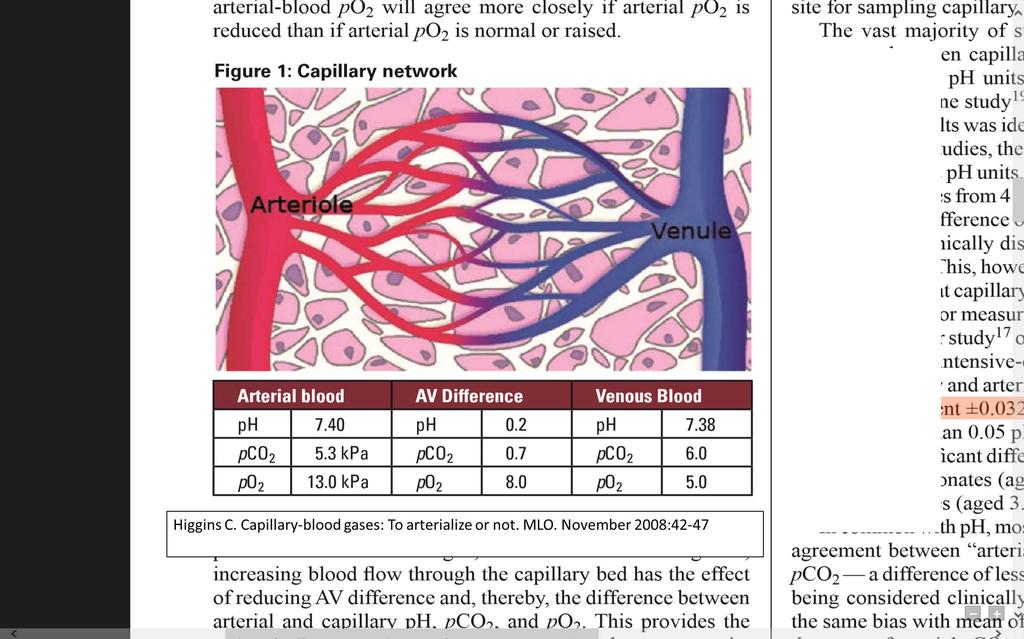
58 What differences can be expected between pco 2 values in different specimen types?
59 0.02
60
61

62 Arterial Venous pco 2 Difference ~ 7 mmhg Arterial Capillary pco 2 Difference ~ 6 mmhg
63 Will these pco 2 reference ranges be dependent upon the blood gas instrument used to measure the specimens?
64
65
66 All method mean (SD) 58.6 (4.4) mm Hg Lowest method mean (SD) 51.3 (2.4) mm Hg Highest method mean (SD) 67.6 (2.8) mm Hg
67 All method mean (SD) 58.6 (4.4) mm Hg Lowest method mean (SD) 51.3 (2.4) mm Hg Highest method mean (SD) 67.6 (2.8) mm Hg Can we use the same reference ranges for use with all blood gas instruments?
68
69 Can we use the same reference ranges for use with all blood gas instruments?
70 Clinical Trials Address the safety and efficacy of induced hypothermia in perinatal HIE Azzopardi D, Brocklehurst P, Edwards D. et al., The TOBY study. Whole body hypothermia for the treatment of perinatal asphyxia encephalopathy: a randomized control trial. BMC. Pediatr. 2008; 8:17 Azzopardi DV, Strohm B, Edwards AD., et al., TOBY study group. Moderate hypothermia to treat perinatal asphyxia encephalopathy. N Eng J Med. 2009; 361: Eicher DJ, Wagner CL, Katikaneni LP, et al., Moderate hypothermia in neonatal encephalopathy: efficacy outcomes. Pediatr Neurol 2005; 32:11-17 Gluckman PD, Wyatt JS, Azzopardi D., et al., Selective head cooling with mild systemic hypothermia after neonatal encephalopathy: a multicentre randomized trial. Lancet 2005; Shankaran S, Laptook AR, Ehrenkranz RA., et al., National Institute of Child Health and Human Development Neonatal Research Network. Whole blood hypothermia for neonates with hypoxic ischemic encephalopathy. N Eng J. Med. 2005; 353: Simbruner G, Mittal RA, Rohlmann F, Muche R. neo.neuro. Network Trial Participants. Systemic hypothermia after neonatal encephalopathy: outcomes of neo.neuro.network RCT. Pediatrics 2010; 126(4); e
71 Clinical Trials Address the safety and efficacy of induced hypothermia in perinatal HIE Azzopardi D, Brocklehurst P, Edwards D. et al., The TOBY study. Whole body hypothermia for the treatment of perinatal asphyxia encephalopathy: a randomized control trial. BMC. Pediatr. 2008; 8:17 Azzopardi DV, Strohm B, Edwards AD., et al., TOBY study group. Moderate hypothermia to treat perinatal asphyxia encephalopathy. N Eng J Med. 2009; 361: Eicher ph DJ, Wagner Stat: CL, Katikaneni Corrected LP, et al., Moderate for body hypothermia temperature in neonatal encephalopathy: efficacy outcomes. Pediatr Neurol 2005; 32:11-17 Gluckman PD, Wyatt JS, Azzopardi D., et al., Selective head cooling with mild systemic hypothermia after neonatal encephalopathy: a multicentre randomized trial. Lancet 2005; Shankaran S, Laptook AR, Ehrenkranz RA., et al., National Institute of Child Health and Human Development Neonatal Research Network. Whole blood hypothermia for neonates with hypoxic ischemic encephalopathy. N Eng J. Med. 2005; 353: Simbruner G, Mittal RA, Rohlmann F, Muche R. neo.neuro. Network Trial Participants. Systemic hypothermia after neonatal encephalopathy: outcomes of neo.neuro.network RCT. Pediatrics 2010; 126(4); e
72 Is there an association between hypocarbia and month outcome among neonates with HIE?
73

74 Evaluated the relationship between hypocarbia ( < 35 mm Hg) and outcome (disability/death at months Blood gases were corrected for body temperature Poor outcomes and death/disability increased with greater cumulative exposure to pco 2 < 35 mmhg
75 Clinical Case Wrap-up Patient underwent therapeutic hypothermia for 72 hours. No further seizures noted, Keppra stopped prior to discharge. Brain MRI consistent with profound hypoxic ischemic injury. Patient was successfully extubated after 6 days. Some difficulty handling secretions, managed with glycopyrrolate Unable to orally feed. Mother elected not to pursue G tube and patient was discharged on NG feeds. Neurologic exam at discharge was notable for hypertonicity in upper extremities and a weak suck reflex. Discharged from NICU at 5 weeks of age.
76 Clinical Case Wrap-up After discharge, patient had recurrent aspiration and stridor, at least one episode of aspiration pneumonia Tracheostomy and g tube were placed at 4 months of age Currently 5 months old, continues to have increased tone and spasticity in upper and lower extremities but does show good visual tracking and interaction with caregivers
77 Conclusions 1) Six clinical trails conducted between 2005 and 2012, demonstrated that mild hypothermia (33.5⁰C 34.5⁰C) for 72 hours is an effective treatment to help reduce morbidity and mortality associated with hypoxic ischemic encephalopathy (HIE). 2) During therapeutic hypothermia, it is critical to closely monitor pco 2 and ph to confirm adequate cerebral blood flow in the neonate. 3) Interpretation of blood gas results during therapeutic hypothermia is complicated because hypothermia can affect the solubility of CO 2 4) A controversy exists as to whether blood gas measurement should be corrected to the patient s actual body temperature or be consistently measured at 37⁰C
Objectives. Birth Depression Management. Birth Depression Terms
 Objectives Birth Depression Management Regional Perinatal Outreach Program 2016 Understand the terms and the clinical characteristics of birth depression. Be familiar with the evidence behind therapeutic
Objectives Birth Depression Management Regional Perinatal Outreach Program 2016 Understand the terms and the clinical characteristics of birth depression. Be familiar with the evidence behind therapeutic
Hypothermia in Neonates with HIE TARA JENDZIO, DNP(C), RN, RNC-NIC
, RN, RNC-NIC") Hypothermia in Neonates with HIE TARA JENDZIO, DNP(C), RN, RNC-NIC Objectives 1. Define Hypoxic-Ischemic Encephalopathy (HIE) 2. Identify the criteria used to determine if an infant qualifies for therapeutic
Hypothermia in Neonates with HIE TARA JENDZIO, DNP(C), RN, RNC-NIC Objectives 1. Define Hypoxic-Ischemic Encephalopathy (HIE) 2. Identify the criteria used to determine if an infant qualifies for therapeutic
Too Cool? Hypoxic Ischemic Encephalopathy and Therapeutic Hypothermia. Lauren Sacco DNP, ARNP, NNP-BC
 Too Cool? Hypoxic Ischemic Encephalopathy and Therapeutic Hypothermia Lauren Sacco DNP, ARNP, NNP-BC Pathophysiology of HIE Occurs in two energy failure phases: First phase happens during the initial insult
Too Cool? Hypoxic Ischemic Encephalopathy and Therapeutic Hypothermia Lauren Sacco DNP, ARNP, NNP-BC Pathophysiology of HIE Occurs in two energy failure phases: First phase happens during the initial insult
TOO COOL OR NOT TOO COOL- THERAPEUTIC HYPOTHERMIA IN THE ICU SCCM TX 2017 TED WU MD PEDIATRIC CRITICAL CARE UNIVERSITY OF TEXAS HEALTH SAN ANTONIO
 TOO COOL OR NOT TOO COOL- THERAPEUTIC HYPOTHERMIA IN THE ICU SCCM TX 2017 TED WU MD PEDIATRIC CRITICAL CARE UNIVERSITY OF TEXAS HEALTH SAN ANTONIO DISCLOSURE I have no relationships with commercial companies
TOO COOL OR NOT TOO COOL- THERAPEUTIC HYPOTHERMIA IN THE ICU SCCM TX 2017 TED WU MD PEDIATRIC CRITICAL CARE UNIVERSITY OF TEXAS HEALTH SAN ANTONIO DISCLOSURE I have no relationships with commercial companies
NEONATAL HYPOXIC-ISCHAEMIC ENCEPHALOPATHY (HIE) & COOLING THERAPY
 & COOLING THERAPY") Background NEONATAL HYPOXIC-ISCHAEMIC ENCEPHALOPATHY (HIE) & COOLING THERAPY A perinatal hypoxic-ischaemic insult may present with varying degrees of neonatal encephalopathy, neurological disorder and
Background NEONATAL HYPOXIC-ISCHAEMIC ENCEPHALOPATHY (HIE) & COOLING THERAPY A perinatal hypoxic-ischaemic insult may present with varying degrees of neonatal encephalopathy, neurological disorder and
State of Florida Hypothermia Protocol. Michael D. Weiss, M.D. Associate Professor of Pediatrics Division of Neonatology
 State of Florida Hypothermia Protocol Michael D. Weiss, M.D. Associate Professor of Pediatrics Division of Neonatology I. Entry Criteria 1. Gestational Age greater than or equal to 35 weeks gestation
State of Florida Hypothermia Protocol Michael D. Weiss, M.D. Associate Professor of Pediatrics Division of Neonatology I. Entry Criteria 1. Gestational Age greater than or equal to 35 weeks gestation
Queen Charlotte Hospital
 Queen Charlotte Hospital Neuroprotection for neonatal encephalopathy Neonatal encephalopathy accounts for 1 million deaths worldwide and even greater numbers of disabled survivors In countries with
Queen Charlotte Hospital Neuroprotection for neonatal encephalopathy Neonatal encephalopathy accounts for 1 million deaths worldwide and even greater numbers of disabled survivors In countries with
No social problems noted No past med hx Mother had spontaneous rupture of fetal membranes SB born on Needed to be resuscitated at birth
 No social problems noted No past med hx Mother had spontaneous rupture of fetal membranes SB born on 9-16-2011 Needed to be resuscitated at birth (included assisted vent) Had generalized edema and possible
No social problems noted No past med hx Mother had spontaneous rupture of fetal membranes SB born on 9-16-2011 Needed to be resuscitated at birth (included assisted vent) Had generalized edema and possible
Running head: THERAPEUTIC HYPOTHERMIA AND TRANSPORT 1
 Running head: THERAPEUTIC HYPOTHERMIA AND TRANSPORT 1 Therapeutic Hypothermia for Neonatal Encephalopathy: Preparation for Transport to Cooling Center Teresa Z. Baker, DNP-S Annie L. Addison, FNP-S NURS
Running head: THERAPEUTIC HYPOTHERMIA AND TRANSPORT 1 Therapeutic Hypothermia for Neonatal Encephalopathy: Preparation for Transport to Cooling Center Teresa Z. Baker, DNP-S Annie L. Addison, FNP-S NURS
This lecture will provide an overview of the neurologic exam of a neonate in the context of clinical cases.
 A11a Neuro Nuggets from the Trenches Michael D. Weiss, MD Associate Professor Department of Pediatrics, Division of Neonatology University of Florida, Gainesville, FL The speaker has signed a disclosure
A11a Neuro Nuggets from the Trenches Michael D. Weiss, MD Associate Professor Department of Pediatrics, Division of Neonatology University of Florida, Gainesville, FL The speaker has signed a disclosure
COOLING FOR HYPOXIC ISCHEMIC ENCEPHALOPATHY
 COOLING FOR HYPOXIC ISCHEMIC ENCEPHALOPATHY Roger F. Soll H. Wallace Professor of Neonatology University of Vermont 19 th International Symposium on Neonatology Sao Paulo, Brazil DISCLOSURE Roger F. Soll
COOLING FOR HYPOXIC ISCHEMIC ENCEPHALOPATHY Roger F. Soll H. Wallace Professor of Neonatology University of Vermont 19 th International Symposium on Neonatology Sao Paulo, Brazil DISCLOSURE Roger F. Soll
1/29/2014. Kimberly Johnson Hatchett, MD PGY-4 11/15/13
 Kimberly Johnson Hatchett, MD PGY-4 11/15/13 History of Present Illness 14 month old previously healthy infant boy presented via EMS after being found by his mother to be breathing loudly and non-responsive.
Kimberly Johnson Hatchett, MD PGY-4 11/15/13 History of Present Illness 14 month old previously healthy infant boy presented via EMS after being found by his mother to be breathing loudly and non-responsive.
State of Florida Systemic Supportive Care Guidelines. Michael D. Weiss, M.D. Associate Professor of Pediatrics Division of Neonatology
 State of Florida Systemic Supportive Care Guidelines Michael D. Weiss, M.D. Associate Professor of Pediatrics Division of Neonatology I. FEN 1. What intravenous fluids should be initiated upon admission
State of Florida Systemic Supportive Care Guidelines Michael D. Weiss, M.D. Associate Professor of Pediatrics Division of Neonatology I. FEN 1. What intravenous fluids should be initiated upon admission
Perinatal asphyxia: Pathophysiology and therapy
 Perinatal asphyxia: Pathophysiology and therapy Peter Davis Melbourne Australia With thanks to Dr Sue Jacobs Moderate or severe HIE Complicates ~1/1000 term live births: Mortality: >25% Major neurological
Perinatal asphyxia: Pathophysiology and therapy Peter Davis Melbourne Australia With thanks to Dr Sue Jacobs Moderate or severe HIE Complicates ~1/1000 term live births: Mortality: >25% Major neurological
Case Presentations. Anamika B. Mukherjee, MD September 13, 2017
 Case Presentations Anamika B. Mukherjee, MD September 13, 2017 Nothing to disclose Disclosures Learning Objectives Use the CPQCC Toolkit for therapeutic hypothermia to apply the guidelines for screening
Case Presentations Anamika B. Mukherjee, MD September 13, 2017 Nothing to disclose Disclosures Learning Objectives Use the CPQCC Toolkit for therapeutic hypothermia to apply the guidelines for screening
TREATMENT OF HYPOXIC ISCHEMIC ENCEPHALOPATHY WITH COOLING Children s Hospital & Research Center Oakland Guideline Revised by P.
 TREATMENT OF HYPOXIC ISCHEMIC ENCEPHALOPATHY WITH COOLING Children s Hospital & Research Center Oakland Guideline Revised 05-13-13 by P. Joe SCREENING FOR POTENTIAL COOLING PATIENTS Patients who are >
TREATMENT OF HYPOXIC ISCHEMIC ENCEPHALOPATHY WITH COOLING Children s Hospital & Research Center Oakland Guideline Revised 05-13-13 by P. Joe SCREENING FOR POTENTIAL COOLING PATIENTS Patients who are >
Therapeutic hypothermia for hypoxic ischemic encephalopathy using low-technology methods: A systematic review and meta-analysis
 Therapeutic hypothermia for hypoxic ischemic encephalopathy using low-technology methods: A systematic review and meta-analysis Rossouw G 1, Irlam J 2, Horn AR 1 1)Division of Neonatal Medicine, Department
Therapeutic hypothermia for hypoxic ischemic encephalopathy using low-technology methods: A systematic review and meta-analysis Rossouw G 1, Irlam J 2, Horn AR 1 1)Division of Neonatal Medicine, Department
Therapeutic Hypothermia for infants > 35 wks with moderate or severe Hypoxic Ischaemic Encephalopathy (HIE) Clinical Guideline Reference Number:
 Clinical Guideline Reference Number:") This is an official Northern Trust policy and should not be edited in any way Therapeutic Hypothermia for infants > 35 wks with moderate or severe Hypoxic Ischaemic Encephalopathy (HIE) Clinical Guideline
This is an official Northern Trust policy and should not be edited in any way Therapeutic Hypothermia for infants > 35 wks with moderate or severe Hypoxic Ischaemic Encephalopathy (HIE) Clinical Guideline
Kimberly M. Thornton, 1,2 Hongying Dai, 3 Seth Septer, 2,4 and Joshua E. Petrikin 1,2. 1. Introduction
 International Pediatrics, Article ID 643689, 7 pages http://dx.doi.org/10.1155/2014/643689 Research Article Effects of Whole Body Therapeutic Hypothermia on Gastrointestinal Morbidity and Feeding Tolerance
International Pediatrics, Article ID 643689, 7 pages http://dx.doi.org/10.1155/2014/643689 Research Article Effects of Whole Body Therapeutic Hypothermia on Gastrointestinal Morbidity and Feeding Tolerance
Birth Asphyxia - Summary of the previous meeting and protocol overview
 Birth Asphyxia - Summary of the previous meeting and protocol overview Dr Ornella Lincetto, WHO Geneve Milano, 11June 2007 Vilka är Personality egenskaper med den astrologiska Tvillingarna? Objective of
Birth Asphyxia - Summary of the previous meeting and protocol overview Dr Ornella Lincetto, WHO Geneve Milano, 11June 2007 Vilka är Personality egenskaper med den astrologiska Tvillingarna? Objective of
ETIOLOGY AND PATHOGENESIS OF HYPOXIC-ISCHEMIC ENCEPHALOPATHY
 ETIOLOGY AND PATHOGENESIS OF HYPOXIC-ISCHEMIC ENCEPHALOPATHY HYPOXIC-ISCHEMIC ENCEPHALOPATHY Hypoxic-İschemic Encephalopathy Encephalopathy due to hypoxic-ischemic injury [Hypoxic-ischemic encephalopathy
ETIOLOGY AND PATHOGENESIS OF HYPOXIC-ISCHEMIC ENCEPHALOPATHY HYPOXIC-ISCHEMIC ENCEPHALOPATHY Hypoxic-İschemic Encephalopathy Encephalopathy due to hypoxic-ischemic injury [Hypoxic-ischemic encephalopathy
Disclosures. Objectives. Definition: HIE. HIE: Incidence. Impact 9/10/2018. Hypoxic Ischemic Encephalopathy in the Neonate
 Disclosures Hypoxic Ischemic Encephalopathy in the Neonate No relevant financial relationships or conflicts of interest to disclose Franscesca Miquel-Verges MD 2018 Review therapies currently under research
Disclosures Hypoxic Ischemic Encephalopathy in the Neonate No relevant financial relationships or conflicts of interest to disclose Franscesca Miquel-Verges MD 2018 Review therapies currently under research
Review Article Current Controversies in Newer Therapies to Treat Birth Asphyxia
 International Pediatrics Volume 2011, Article ID 848413, 5 pages doi:10.1155/2011/848413 Review Article Current Controversies in Newer Therapies to Treat Birth Asphyxia Pia Wintermark Division of Newborn
International Pediatrics Volume 2011, Article ID 848413, 5 pages doi:10.1155/2011/848413 Review Article Current Controversies in Newer Therapies to Treat Birth Asphyxia Pia Wintermark Division of Newborn
Admission/Discharge Form for Infants Born in Please DO NOT mail or fax this form to the CPQCC Data Center. This form is for internal use ONLY.
 Selection Criteria Admission/Discharge Form for Infants Born in 2016 To be eligible, you MUST answer YES to at least one of the possible criteria (A-C) A. 401 1500 grams o Yes B. GA range 22 0/7 31 6/7
Selection Criteria Admission/Discharge Form for Infants Born in 2016 To be eligible, you MUST answer YES to at least one of the possible criteria (A-C) A. 401 1500 grams o Yes B. GA range 22 0/7 31 6/7
Dysphagia in Encephalopathic Neonates Treated with Hypothermia
 Dysphagia in Encephalopathic Neonates Treated with Hypothermia A thesis submitted to the University of Arizona College of Medicine -- Phoenix in partial fulfillment of the requirements for the degree of
Dysphagia in Encephalopathic Neonates Treated with Hypothermia A thesis submitted to the University of Arizona College of Medicine -- Phoenix in partial fulfillment of the requirements for the degree of
Neonatal Therapeutic Hypothermia. A Wasunna Professor of Neonatal Medicine and Pediatrics School of Medicine, University of Nairobi
 Neonatal Therapeutic Hypothermia A Wasunna Professor of Neonatal Medicine and Pediatrics School of Medicine, University of Nairobi Definition of Perinatal Asphyxia *No agreed universal definition ACOG/AAP
Neonatal Therapeutic Hypothermia A Wasunna Professor of Neonatal Medicine and Pediatrics School of Medicine, University of Nairobi Definition of Perinatal Asphyxia *No agreed universal definition ACOG/AAP
Wales Neonatal Network Guideline Guideline for the management of Infants with Moderate or Severe Perinatal Asphyxia requiring cooling.
 Guideline for the management of Infants with Moderate or Severe Perinatal Asphyxia requiring cooling. (Including flowchart for infants fulfilling A criteria or A and B criteria only) Perinatal asphyxia
Guideline for the management of Infants with Moderate or Severe Perinatal Asphyxia requiring cooling. (Including flowchart for infants fulfilling A criteria or A and B criteria only) Perinatal asphyxia
Neonatal Life Support Provider (NLSP) Certification Preparatory Materials
 Certification Preparatory Materials") Neonatal Life Support Provider (NLSP) Certification Preparatory Materials NEONATAL LIFE SUPPORT PROVIDER (NRP) CERTIFICATION TABLE OF CONTENTS NEONATAL FLOW ALGORITHM.2 INTRODUCTION 3 ANTICIPATION OF RESUSCITATION
Neonatal Life Support Provider (NLSP) Certification Preparatory Materials NEONATAL LIFE SUPPORT PROVIDER (NRP) CERTIFICATION TABLE OF CONTENTS NEONATAL FLOW ALGORITHM.2 INTRODUCTION 3 ANTICIPATION OF RESUSCITATION
Inclusion criteria for cooling: Babies should be assessed for 3 criteria: A, B and C. See Appendix 1 for a decision making flowchart.
 Guideline for the management of Infants with Moderate or Severe Perinatal Asphyxia requiring cooling. (Including flowchart for infants fulfilling A criteria or A and B criteria only) Perinatal asphyxia
Guideline for the management of Infants with Moderate or Severe Perinatal Asphyxia requiring cooling. (Including flowchart for infants fulfilling A criteria or A and B criteria only) Perinatal asphyxia
TRAINING NEONATOLOGY SILVANA PARIS
 TRAINING ON NEONATOLOGY SILVANA PARIS RESUSCITATION IN DELIVERY ROOM INTRODUCTION THE GLOBAL RESUSCITATION BURDEN IN NEWBORN 136 MILL NEWBORN BABIES EACH YEAR (WHO WORLD REPORT) 5-8 MILL NEWBORN INFANTS
TRAINING ON NEONATOLOGY SILVANA PARIS RESUSCITATION IN DELIVERY ROOM INTRODUCTION THE GLOBAL RESUSCITATION BURDEN IN NEWBORN 136 MILL NEWBORN BABIES EACH YEAR (WHO WORLD REPORT) 5-8 MILL NEWBORN INFANTS
Too or Too Cold. Too Cold...Too Hot...Just Right. Temperature Control in Newborns. Temperature Balance in Newborns. Basics in the Delivery Room
 Too or Too Cold Neonatology Rediscovers Temperature Control Advances and Controversies in Clinical Pediatrics May 31, 2007 Terri A. Slagle Neonatology, CPMC Too Cold...Too Hot...Just Right Too Cold = Issues
Too or Too Cold Neonatology Rediscovers Temperature Control Advances and Controversies in Clinical Pediatrics May 31, 2007 Terri A. Slagle Neonatology, CPMC Too Cold...Too Hot...Just Right Too Cold = Issues
Initiation of passive cooling at referring centre is most predictive of achieving early therapeutic hypothermia in asphyxiated newborns
 Paediatrics & Child Health, 2017, 264 268 doi: 10.1093/pch/pxx062 Original Article Advance Access publication 23 May 2017 Original Article Initiation of passive cooling at referring centre is most predictive
Paediatrics & Child Health, 2017, 264 268 doi: 10.1093/pch/pxx062 Original Article Advance Access publication 23 May 2017 Original Article Initiation of passive cooling at referring centre is most predictive
TLC March 27, Shawn Hollinger-Neonatal Fellow CHEO
 TLC March 27, 2013 Presented/Prepared by: Shawn Hollinger, PGY5 Neonatal-Perinatal Medicine Resident - University of Ottawa With slides/images from Dr. Brigitte Lemyre Associate Professor of Pediatrics
TLC March 27, 2013 Presented/Prepared by: Shawn Hollinger, PGY5 Neonatal-Perinatal Medicine Resident - University of Ottawa With slides/images from Dr. Brigitte Lemyre Associate Professor of Pediatrics
Study of renal functions in neonatal asphyxia
 Original article: Study of renal functions in neonatal asphyxia *Dr. D.Y.Shrikhande, **Dr. Vivek Singh, **Dr. Amit Garg *Professor and Head, **Senior Resident Department of Pediatrics, Pravara Institute
Original article: Study of renal functions in neonatal asphyxia *Dr. D.Y.Shrikhande, **Dr. Vivek Singh, **Dr. Amit Garg *Professor and Head, **Senior Resident Department of Pediatrics, Pravara Institute
Hypoxic-Ischemic Encephalopathy. TW de Witt University of Pretoria Department of Paediatrics Neonatology
 Hypoxic-Ischemic Encephalopathy TW de Witt University of Pretoria Department of Paediatrics Neonatology Background HIE remains a serious condition that causes significant mortality and longterm morbidity.
Hypoxic-Ischemic Encephalopathy TW de Witt University of Pretoria Department of Paediatrics Neonatology Background HIE remains a serious condition that causes significant mortality and longterm morbidity.
NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE
 NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE INTERVENTIONAL PROCEDURES PROGRAMME Interventional procedure overview of therapeutic hypothermia with intracorporeal temperature monitoring for hypoxic
NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE INTERVENTIONAL PROCEDURES PROGRAMME Interventional procedure overview of therapeutic hypothermia with intracorporeal temperature monitoring for hypoxic
Guslihan Dasa Tjipta Division of Perinatology Department of Child Health Medical School University of Sumatera Utara
 Guslihan Dasa Tjipta Division of Perinatology Department of Child Health Medical School University of Sumatera Utara 1 Definition Perinatal asphyxia is a fetus/newborn, due to: is an insult to the Lack
Guslihan Dasa Tjipta Division of Perinatology Department of Child Health Medical School University of Sumatera Utara 1 Definition Perinatal asphyxia is a fetus/newborn, due to: is an insult to the Lack
Therapeutichypothermia headcooling and its Adverse Effects in Newborns with PerinatalAsphyxia
 International Research Journal of Applied and Basic Sciences 2013 Available online at www.irjabs.com ISSN 2251-838X / Vol, 5 (12): 1546-1551 Science Explorer Publications Therapeutichypothermia headcooling
International Research Journal of Applied and Basic Sciences 2013 Available online at www.irjabs.com ISSN 2251-838X / Vol, 5 (12): 1546-1551 Science Explorer Publications Therapeutichypothermia headcooling
University of Bristol - Explore Bristol Research
 Wang, H., Cheng, Z., Liao, Y., Li, J., Weber, J., Thomas, A., & Faul, C. FJ. (2017). Conjugated Microporous Polycarbazole Networks as Precursors for Nitrogen Enriched Microporous Carbons for CO2 Storage
Wang, H., Cheng, Z., Liao, Y., Li, J., Weber, J., Thomas, A., & Faul, C. FJ. (2017). Conjugated Microporous Polycarbazole Networks as Precursors for Nitrogen Enriched Microporous Carbons for CO2 Storage
PedsCases Podcast Scripts
 PedsCases Podcast Scripts This is a text version of a podcast from Pedscases.com on Hypoxic Ischemic Encephalopathy. These podcasts are designed to give medical students an overview of key topics in pediatrics.
PedsCases Podcast Scripts This is a text version of a podcast from Pedscases.com on Hypoxic Ischemic Encephalopathy. These podcasts are designed to give medical students an overview of key topics in pediatrics.
 NEONATAL LIFE SUPPORT PROVIDER (NLSP) CERTIFICATION EXAMINATION 1. To determine if an infant requires resuscitation, you must rapidly assess gestation period, presence of meconium in amniotic fluid, breaths
NEONATAL LIFE SUPPORT PROVIDER (NLSP) CERTIFICATION EXAMINATION 1. To determine if an infant requires resuscitation, you must rapidly assess gestation period, presence of meconium in amniotic fluid, breaths
Pathophysiology Review. Hypoxic-Ischemic Encephalopathy & Therapeutic Hypothermia. Objectives. What is Hypoxic-Ischemic Encephalopathy?
 Hypoxic-Ischemic Encephalopathy & Therapeutic Hypothermia Nancy Couto Nurse Practitioner, NICU London Health Sciences Centre, Children s Hospital nancy.couto@lhsc.on.ca 2014 12 17 Objectives Review Pathophysiology
Hypoxic-Ischemic Encephalopathy & Therapeutic Hypothermia Nancy Couto Nurse Practitioner, NICU London Health Sciences Centre, Children s Hospital nancy.couto@lhsc.on.ca 2014 12 17 Objectives Review Pathophysiology
Predicting Outcomes in HIE. Naaz Merchant Consultant Neonatologist Beds & Herts Meeting 17/03/2016
 Predicting Outcomes in HIE Naaz Merchant Consultant Neonatologist Beds & Herts Meeting 17/03/2016 Interactive please! Case 1 Term, 3.5 kg Antenatal: Breech Labour/Delivery: Em CS failure to progress, mec
Predicting Outcomes in HIE Naaz Merchant Consultant Neonatologist Beds & Herts Meeting 17/03/2016 Interactive please! Case 1 Term, 3.5 kg Antenatal: Breech Labour/Delivery: Em CS failure to progress, mec
Running head: CASE STUDY NEONATAL HEAD COOLING 1
 Running head: CASE STUDY NEONATAL HEAD COOLING 1 Case Study 1: Head Cooling as Treatment for Neonatal Encephalopathy NURS 6035 Practicum I Teresa Z. Baker Texas Woman s University CASE STUDY NEONATAL HEAD
Running head: CASE STUDY NEONATAL HEAD COOLING 1 Case Study 1: Head Cooling as Treatment for Neonatal Encephalopathy NURS 6035 Practicum I Teresa Z. Baker Texas Woman s University CASE STUDY NEONATAL HEAD
Effect of ALlopurinol in addition to hypothermia for hypoxic-ischemic Brain Injury on Neurocognitive Outcome. Axel Franz, Tübingen
 Effect of ALlopurinol in addition to hypothermia for hypoxic-ischemic Brain Injury on Neurocognitive Outcome Axel Franz, Tübingen Hypoxic-ischemic encephalopathy 1-2 / 1000 newborn suffer from moderate
Effect of ALlopurinol in addition to hypothermia for hypoxic-ischemic Brain Injury on Neurocognitive Outcome Axel Franz, Tübingen Hypoxic-ischemic encephalopathy 1-2 / 1000 newborn suffer from moderate
NEONATOLOGY Healthy newborn. Neonatal sequelaes
 NEONATOLOGY Healthy newborn. Neonatal sequelaes Ágnes Harmath M.D. Ph.D. senior lecturer 11. November 2016. Tasks of the neonatologist Prenatal diagnosed condition Inform parents, preparation of necessary
NEONATOLOGY Healthy newborn. Neonatal sequelaes Ágnes Harmath M.D. Ph.D. senior lecturer 11. November 2016. Tasks of the neonatologist Prenatal diagnosed condition Inform parents, preparation of necessary
Study of role of MRI brain in evaluation of hypoxic ischemic encephalopathy
 Original article: Study of role of MRI brain in evaluation of hypoxic ischemic encephalopathy *Dr Harshad Bhagat, ** Dr Ravindra Kawade, ***Dr Y.P.Sachdev *Junior Resident, Department Of Radiodiagnosis,
Original article: Study of role of MRI brain in evaluation of hypoxic ischemic encephalopathy *Dr Harshad Bhagat, ** Dr Ravindra Kawade, ***Dr Y.P.Sachdev *Junior Resident, Department Of Radiodiagnosis,
Addendum to the NRP Provider Textbook 6 th Edition Recommendations for specific modifications in the Canadian context
 Addendum to the NRP Provider Textbook 6 th Edition Recommendations for specific modifications in the Canadian context A subcommittee of the Canadian Neonatal Resuscitation Program (NRP) Steering Committee
Addendum to the NRP Provider Textbook 6 th Edition Recommendations for specific modifications in the Canadian context A subcommittee of the Canadian Neonatal Resuscitation Program (NRP) Steering Committee
Simulation 3: Post-term Baby in Labor and Delivery
 Simulation 3: Post-term Baby in Labor and Delivery Opening Scenario (Links to Section 1) You are an evening-shift respiratory therapist in a large hospital with a level III neonatal unit. You are paged
Simulation 3: Post-term Baby in Labor and Delivery Opening Scenario (Links to Section 1) You are an evening-shift respiratory therapist in a large hospital with a level III neonatal unit. You are paged
Hypothermia: Neuroprotective Treatment of Hypoxic-Ischemic Encephalopathy. Serious perinatal asphyxia. Therapeutic hypothermia
 Therapeutic hypothermia Hypothermia: Neuroprotective Treatment of Hypoxic-Ischemic Encephalopathy Background of hypothermia Clinical application Floris Groenendaal Department of Neonatology Complications
Therapeutic hypothermia Hypothermia: Neuroprotective Treatment of Hypoxic-Ischemic Encephalopathy Background of hypothermia Clinical application Floris Groenendaal Department of Neonatology Complications
SWISS SOCIETY OF NEONATOLOGY. Supercarbia in an infant with meconium aspiration syndrome
 SWISS SOCIETY OF NEONATOLOGY Supercarbia in an infant with meconium aspiration syndrome January 2006 2 Wilhelm C, Frey B, Department of Intensive Care and Neonatology, University Children s Hospital Zurich,
SWISS SOCIETY OF NEONATOLOGY Supercarbia in an infant with meconium aspiration syndrome January 2006 2 Wilhelm C, Frey B, Department of Intensive Care and Neonatology, University Children s Hospital Zurich,
Correlation of Neurodevelopmental Outcome and brain MRI/EEG findings in term HIE infants
 Correlation of Neurodevelopmental Outcome and brain MRI/EEG findings in term HIE infants Ajou University School of Medicine Department of Pediatrics Moon Sung Park M.D. Hee Cheol Jo, M.D., Jang Hoon Lee,
Correlation of Neurodevelopmental Outcome and brain MRI/EEG findings in term HIE infants Ajou University School of Medicine Department of Pediatrics Moon Sung Park M.D. Hee Cheol Jo, M.D., Jang Hoon Lee,
Infection. Risk factor for infection ACoRN alerting sign with * Clinical deterioration. Problem List. Respiratory. Cardiovascular
 The ACoRN Process Baby at risk Unwell Risk factors Post-resuscitation requiring stabilization Resuscitation Ineffective breathing Heart rate < 100 bpm Central cyanosis Support Infection Risk factor for
The ACoRN Process Baby at risk Unwell Risk factors Post-resuscitation requiring stabilization Resuscitation Ineffective breathing Heart rate < 100 bpm Central cyanosis Support Infection Risk factor for
Post-Cardiac Arrest Syndrome. MICU Lecture Series
 Post-Cardiac Arrest Syndrome MICU Lecture Series Case 58 y/o female collapses at home, family attempts CPR, EMS arrives and notes VF, defibrillation x 3 with return of spontaneous circulation, brought
Post-Cardiac Arrest Syndrome MICU Lecture Series Case 58 y/o female collapses at home, family attempts CPR, EMS arrives and notes VF, defibrillation x 3 with return of spontaneous circulation, brought
Does phenobarbital improve the effectiveness of therapeutic hypothermia in infants with hypoxic-ischemic encephalopathy?
 (2012) 32, 15 20 r 2012 Nature America, Inc. All rights reserved. 0743-8346/12 www.nature.com/jp ORIGINAL ARTICLE Does phenobarbital improve the effectiveness of therapeutic hypothermia in infants with
(2012) 32, 15 20 r 2012 Nature America, Inc. All rights reserved. 0743-8346/12 www.nature.com/jp ORIGINAL ARTICLE Does phenobarbital improve the effectiveness of therapeutic hypothermia in infants with
Blood Gases For beginners
 Blood Gases For beginners Lynsey ward th February 2008 4 th Aims To have a basic understanding of Blood Gas analysis. Objectives To state what acid and alkaline in the value of PH When analysing a blood
Blood Gases For beginners Lynsey ward th February 2008 4 th Aims To have a basic understanding of Blood Gas analysis. Objectives To state what acid and alkaline in the value of PH When analysing a blood
Stayin Alive: Pediatric Advanced Life Support (PALS) Updated Guidelines
 Updated Guidelines") Stayin Alive: Pediatric Advanced Life Support (PALS) Updated Guidelines Margaret Oates, PharmD, BCPPS Pediatric Critical Care Specialist GSHP Summer Meeting July 16, 2016 Disclosures I have nothing to
Stayin Alive: Pediatric Advanced Life Support (PALS) Updated Guidelines Margaret Oates, PharmD, BCPPS Pediatric Critical Care Specialist GSHP Summer Meeting July 16, 2016 Disclosures I have nothing to
Birth Asphyxia. Perinatal Depression. Birth Asphyxia. Risk Factors maternal. Risk Factors fetal. Risk Factors Intrapartum 2/12/2011
 Birth Asphyxia Perinatal Depression Sara Brown, ARNP Children s Hospital and Regional Medical Center May occur in utero, during labor/delivery or during the neonatal period Condition of impaired blood
Birth Asphyxia Perinatal Depression Sara Brown, ARNP Children s Hospital and Regional Medical Center May occur in utero, during labor/delivery or during the neonatal period Condition of impaired blood
Total Body Cooling & Hypoxic Ischemic Encephalopathy in the Neonate Kaleidoscope 2017
 Total Body Cooling & Hypoxic Ischemic Encephalopathy in the Neonate Kaleidoscope 2017 LEIGH ANN CATES PHD, APRN, NNP -BC, RRT-NPS, CHSE N E O N ATA L N U R S E P R A C T I T I O N E R - T E X A S C H I
Total Body Cooling & Hypoxic Ischemic Encephalopathy in the Neonate Kaleidoscope 2017 LEIGH ANN CATES PHD, APRN, NNP -BC, RRT-NPS, CHSE N E O N ATA L N U R S E P R A C T I T I O N E R - T E X A S C H I
Number: Policy *Please see amendment for Pennsylvania Medicaid at the end of this CPB.
 Number: 0812 Policy *Please see amendment for Pennsylvania Medicaid at the end of this CPB. Aetna considers total body cooling (TBC, also known as whole body cooling) and/or selective head cooling (SHC)
Number: 0812 Policy *Please see amendment for Pennsylvania Medicaid at the end of this CPB. Aetna considers total body cooling (TBC, also known as whole body cooling) and/or selective head cooling (SHC)
Prevalence and outcomes of acute kidney injury in term neonates with perinatal asphyxia
 Prevalence and outcomes of acute kidney injury in term neonates with perinatal asphyxia Dan Alaro¹, Admani Bashir¹ ², Rachel Musoke¹, Lucy Wanaiana¹ 1. Department of Paediatrics and Child Health, University
Prevalence and outcomes of acute kidney injury in term neonates with perinatal asphyxia Dan Alaro¹, Admani Bashir¹ ², Rachel Musoke¹, Lucy Wanaiana¹ 1. Department of Paediatrics and Child Health, University
Neuroprotection strategies in neonates with
 Neuroprotection strategies in neonates with encephalopathy Dr. Khorshid Mohammad, MD, MSc(Pediatrics), FABP, FRCP(Edin) NICU lead, Neuro-Critical Care Program, University of Calgary Disclosure I have no
Neuroprotection strategies in neonates with encephalopathy Dr. Khorshid Mohammad, MD, MSc(Pediatrics), FABP, FRCP(Edin) NICU lead, Neuro-Critical Care Program, University of Calgary Disclosure I have no
1 Pediatric Advanced Life Support Science Update What s New for 2010? 3 CPR. 4 4 Steps of BLS Survey 5 CPR 6 CPR.
 1 Pediatric Advanced Life Support Science Update 2010 2 What s New for 2010? 3 CPR Take no longer than seconds for pulse check Rate at least on per minute (instead of around 100 per minute ) Depth change:
1 Pediatric Advanced Life Support Science Update 2010 2 What s New for 2010? 3 CPR Take no longer than seconds for pulse check Rate at least on per minute (instead of around 100 per minute ) Depth change:
HIE (Hypoxic Ischaemic Encephalopathy)
") HIE (Hypoxic Ischaemic Encephalopathy) Document Title and Reference : HIE (Hypoxic Ischaemic Encephalopathy Main Auth (s) Kiran Yajamanyam Consultant LWH Ratified by: CM NSG Date Ratified: May 2017 Review
HIE (Hypoxic Ischaemic Encephalopathy) Document Title and Reference : HIE (Hypoxic Ischaemic Encephalopathy Main Auth (s) Kiran Yajamanyam Consultant LWH Ratified by: CM NSG Date Ratified: May 2017 Review
Serum Lactate, Brain Magnetic Resonance Imaging and Outcome of Neonatal Hypoxic Ischemic Encephalopathy after Therapeutic Hypothermia
 Pediatrics and Neonatology (2016) 57, 35e40 Available online at www.sciencedirect.com ScienceDirect journal homepage: http://www.pediatr-neonatol.com ORIGINAL ARTICLE Serum Lactate, Brain Magnetic Resonance
Pediatrics and Neonatology (2016) 57, 35e40 Available online at www.sciencedirect.com ScienceDirect journal homepage: http://www.pediatr-neonatol.com ORIGINAL ARTICLE Serum Lactate, Brain Magnetic Resonance
ACoRN Workbook 2012 Update
 ACoRN Neonatal Society Société néonatale ACoRN www.acornprogram.net A Canadian non-profit Society Vancouver, British Columbia ACoRN Workbook 2012 Update Name: The ACoRN Process The Resuscitation Sequence
ACoRN Neonatal Society Société néonatale ACoRN www.acornprogram.net A Canadian non-profit Society Vancouver, British Columbia ACoRN Workbook 2012 Update Name: The ACoRN Process The Resuscitation Sequence
NRP Raising the Bar for Providers and Instructors
 NRP 2011 Raising the Bar for Providers and Instructors What is the same? 1. Minimum course requirement is Lessons 1 through 4 and Lesson 9. The NRP Provider Card requires renewal every 2 years. Your facility
NRP 2011 Raising the Bar for Providers and Instructors What is the same? 1. Minimum course requirement is Lessons 1 through 4 and Lesson 9. The NRP Provider Card requires renewal every 2 years. Your facility
ADMISSION/DISCHARGE FORM FOR INFANTS BORN IN 2019 DO NOT mail or fax this form to the CPQCC Data Center. This form is for internal use ONLY.
 1 Any eligible inborn infant who dies in the delivery room or at any other location in your hospital within 12 hours after birth and prior to admission to the NICU is defined as a "Delivery Room Death."
1 Any eligible inborn infant who dies in the delivery room or at any other location in your hospital within 12 hours after birth and prior to admission to the NICU is defined as a "Delivery Room Death."
Patient Case. Post cardiac arrest pathophysiology 10/19/2017. Disclosure. Objectives. Patient Case-TM
 Disclosure TARGETED TEMPERATURE MANAGEMENT POST CARDIAC ARREST I have nothing to disclose concerning possible financial or personal relationships with commercial entities that may have a direct or indirect
Disclosure TARGETED TEMPERATURE MANAGEMENT POST CARDIAC ARREST I have nothing to disclose concerning possible financial or personal relationships with commercial entities that may have a direct or indirect
Acid-base management during hypothermic CPB alpha-stat and ph-stat models of blood gas interpretation
 Acid-base management during hypothermic CPB alpha-stat and ph-stat models of blood gas interpretation Michael Kremke Department of Anaesthesiology and Intensive Care Aarhus University Hospital, Denmark
Acid-base management during hypothermic CPB alpha-stat and ph-stat models of blood gas interpretation Michael Kremke Department of Anaesthesiology and Intensive Care Aarhus University Hospital, Denmark
COOLING FOR NEONATAL HYPOXIC ISCHAEMIC ENCEPHALOPATHY (HIE) - GUIDELINE
 - GUIDELINE") Background Objective Equipment Indications Contraindications When to initiate cooling in NPICU Procedure for therapeutic cooling NETS Transfer Issues Follow-up References Acknowledgements Related Documents
Background Objective Equipment Indications Contraindications When to initiate cooling in NPICU Procedure for therapeutic cooling NETS Transfer Issues Follow-up References Acknowledgements Related Documents
Serum creatine kinase and lactic dehydrogenase levels as useful markers of immediate and long-term outcome of perinatal asphyxia
 Serum creatine kinase and lactic dehydrogenase levels as useful markers of immediate and long-term outcome of perinatal asphyxia D H Karunatilaka 1, G W D S Amaratunga 2, K D N I Perera 3, V Caldera 4
Serum creatine kinase and lactic dehydrogenase levels as useful markers of immediate and long-term outcome of perinatal asphyxia D H Karunatilaka 1, G W D S Amaratunga 2, K D N I Perera 3, V Caldera 4
INDUCED HYPOTHERMIA A Hot Topic. R. Darrell Nelson, MD, FACEP Emergency Medicine Wake Forest University Health Sciences
 INDUCED HYPOTHERMIA A Hot Topic R. Darrell Nelson, MD, FACEP Emergency Medicine Wake Forest University Health Sciences Conflicts of Interest Sadly, we have no financial or industrial conflicts of interest
INDUCED HYPOTHERMIA A Hot Topic R. Darrell Nelson, MD, FACEP Emergency Medicine Wake Forest University Health Sciences Conflicts of Interest Sadly, we have no financial or industrial conflicts of interest
Stabilization of the Newborn for Transport. Relevant Disclosure. Learning Objectives
 Stabilization of the Newborn for Transport Arlen Foulks, DO FAAP FACOP Medical Director, CCMH Level II NICU Medical Director, NeoFlight Assistant Professor of Pediatrics Neonatal Perinatal Medicine Section,
Stabilization of the Newborn for Transport Arlen Foulks, DO FAAP FACOP Medical Director, CCMH Level II NICU Medical Director, NeoFlight Assistant Professor of Pediatrics Neonatal Perinatal Medicine Section,
The Pharmacokinetics of Antiepileptics Drugs in Neonates with Hypoxic Ischemic Encephalopathy
 The Pharmacokinetics of Antiepileptics Drugs in Neonates with Hypoxic Ischemic Encephalopathy KELIANA O MARA, PHARMD FLORIDA NEONATAL NEUROLOGIC NETWORK STATE MEETING Objectives Describe seizures in hypoxic
The Pharmacokinetics of Antiepileptics Drugs in Neonates with Hypoxic Ischemic Encephalopathy KELIANA O MARA, PHARMD FLORIDA NEONATAL NEUROLOGIC NETWORK STATE MEETING Objectives Describe seizures in hypoxic
Relationship between acute kidney injury and brain MRI findings in asphyxiated newborns after therapeutic hypothermia
 nature publishing group Clinical Investigation Relationship between acute kidney injury and brain MRI findings in asphyxiated newborns after therapeutic hypothermia Subrata Sarkar 1, David J. Askenazi
nature publishing group Clinical Investigation Relationship between acute kidney injury and brain MRI findings in asphyxiated newborns after therapeutic hypothermia Subrata Sarkar 1, David J. Askenazi
Therapeutic Hypothermia: Treatment for Hypoxic-Ischemic Encephalopathy in the NICU
 Therapeutic Hypothermia: Treatment for Hypoxic-Ischemic Encephalopathy in the NICU Denise M. Casey, RN, MS, CCRN, CPNP Nancy Tella, RN, BSN, CCRN Rachel Turesky, RN, BSN Michelle Labrecque, RN, MSN, CCRN
Therapeutic Hypothermia: Treatment for Hypoxic-Ischemic Encephalopathy in the NICU Denise M. Casey, RN, MS, CCRN, CPNP Nancy Tella, RN, BSN, CCRN Rachel Turesky, RN, BSN Michelle Labrecque, RN, MSN, CCRN
Patient: 55 y female (ambulatory)
") Disclosures Speaking Honoraria Radiometer (Canada) Nova Biomedical, Draeger Roche Diagnostics (Canada) Research Support (Reagents, Instrumentation, Travel) Nova Biomedical Abbott Laboratories (Canada)
Disclosures Speaking Honoraria Radiometer (Canada) Nova Biomedical, Draeger Roche Diagnostics (Canada) Research Support (Reagents, Instrumentation, Travel) Nova Biomedical Abbott Laboratories (Canada)
Standardize comprehensive care of the patient with severe traumatic brain injury
 Trauma Center Practice Management Guideline Iowa Methodist Medical Center Des Moines Management of Patients with Severe Traumatic Brain Injury (GCS < 9) ADULT Practice Management Guideline Contact: Trauma
Trauma Center Practice Management Guideline Iowa Methodist Medical Center Des Moines Management of Patients with Severe Traumatic Brain Injury (GCS < 9) ADULT Practice Management Guideline Contact: Trauma
What is symptomatic? Neonatal hypoglycemia: how low can you go? Hypoglycemia and MRI. Conflicts. What s the problem? Hypoglycemia and MRI
 Neonatal hypoglycemia: how low can you go? Kristi Watterberg, MD Professor of Pediatrics, UNM What is symptomatic? Jitteriness Cyanosis Poor feeding Weak, high-pitched cry Seizures Apnea Lethargy, low
Neonatal hypoglycemia: how low can you go? Kristi Watterberg, MD Professor of Pediatrics, UNM What is symptomatic? Jitteriness Cyanosis Poor feeding Weak, high-pitched cry Seizures Apnea Lethargy, low
Post-Arrest Care: Beyond Hypothermia
 Post-Arrest Care: Beyond Hypothermia Damon Scales MD PhD Department of Critical Care Medicine Sunnybrook Health Sciences Centre University of Toronto Disclosures CIHR Physicians Services Incorporated Main
Post-Arrest Care: Beyond Hypothermia Damon Scales MD PhD Department of Critical Care Medicine Sunnybrook Health Sciences Centre University of Toronto Disclosures CIHR Physicians Services Incorporated Main
University of Bristol - Explore Bristol Research
 Elstad, M., Liu, X., & Thoresen, M. (2016). Heart rate response to therapeutic hypothermia in infants with hypoxic-ischaemic encephalopathy. Resuscitation, 106, 53-57. DOI: 10.1016/j.resuscitation.2016.06.023
Elstad, M., Liu, X., & Thoresen, M. (2016). Heart rate response to therapeutic hypothermia in infants with hypoxic-ischaemic encephalopathy. Resuscitation, 106, 53-57. DOI: 10.1016/j.resuscitation.2016.06.023
Swiss neonatal network and Follow up Group
 Swiss neonatal network and Follow up Group March 2011 Barbara Brotschi and Cornelia Hagmann Hypoxic ischaemic encephalopathy Neonatal encephalopathy due to perinatal hypoxiaischaemia: clinically defined
Swiss neonatal network and Follow up Group March 2011 Barbara Brotschi and Cornelia Hagmann Hypoxic ischaemic encephalopathy Neonatal encephalopathy due to perinatal hypoxiaischaemia: clinically defined
Neonatal Seizure. Dr.Nawar Yahya. Presented by: Sarah Khalil Zeina Shamil Zainab Waleed Zainab Qahtan. Supervised by:
 Neonatal Seizure Supervised by: Dr.Nawar Yahya Presented by: Sarah Khalil Zeina Shamil Zainab Waleed Zainab Qahtan Objectives: What is neonatal seizure Etiology Clinical presentation Differential diagnosis
Neonatal Seizure Supervised by: Dr.Nawar Yahya Presented by: Sarah Khalil Zeina Shamil Zainab Waleed Zainab Qahtan Objectives: What is neonatal seizure Etiology Clinical presentation Differential diagnosis
Therapeutic Hypothermia
 Objectives Overview Therapeutic Hypothermia Nerissa U. Ko, MD, MAS UCSF Department of Neurology Critical Care Medicine and Trauma June 4, 2011 Hypothermia as a neuroprotectant Proven indications: Adult
Objectives Overview Therapeutic Hypothermia Nerissa U. Ko, MD, MAS UCSF Department of Neurology Critical Care Medicine and Trauma June 4, 2011 Hypothermia as a neuroprotectant Proven indications: Adult
Neonatal Hypoxic-Ischemic Injury: Ultrasound and Dynamic Color Doppler Sonography perfusion of the Brain and Abdomen with pathologic correlation.
 Neonatal Hypoxic-Ischemic Injury: Ultrasound and Dynamic Color Doppler Sonography perfusion of the Brain and Abdomen with pathologic correlation. Ricardo Faingold,MD Montreal Children s Hospital Medical
Neonatal Hypoxic-Ischemic Injury: Ultrasound and Dynamic Color Doppler Sonography perfusion of the Brain and Abdomen with pathologic correlation. Ricardo Faingold,MD Montreal Children s Hospital Medical
REVIEW ARTICLE. Hypothermia to Treat Neonatal Hypoxic Ischemic Encephalopathy
 REVIEW ARTICLE Hypothermia to Treat Neonatal Hypoxic Ischemic Encephalopathy Systematic Review Prakesh S. Shah, MD, MSc, FRCPC; Arne Ohlsson, FRCPC, MSc; Max Perlman, FRCPC Objectives: To systematically
REVIEW ARTICLE Hypothermia to Treat Neonatal Hypoxic Ischemic Encephalopathy Systematic Review Prakesh S. Shah, MD, MSc, FRCPC; Arne Ohlsson, FRCPC, MSc; Max Perlman, FRCPC Objectives: To systematically
These signs should lead to the administration of high concentrations of
 Hypoxic-ischemic encephalopathy (HIE); (cont.) Clinical manifestations; *Intrauterine; growth restriction and increased vascular resistances may be the st manifestation of fetal hypoxia. *During labor;
Hypoxic-ischemic encephalopathy (HIE); (cont.) Clinical manifestations; *Intrauterine; growth restriction and increased vascular resistances may be the st manifestation of fetal hypoxia. *During labor;
UNIT VI: ACID BASE IMBALANCE
 UNIT VI: ACID BASE IMBALANCE 1 Objectives: Review the physiological mechanism responsible to regulate acid base balance in the body i.e.: Buffers (phosphate, hemoglobin, carbonate) Renal mechanism Respiratory
UNIT VI: ACID BASE IMBALANCE 1 Objectives: Review the physiological mechanism responsible to regulate acid base balance in the body i.e.: Buffers (phosphate, hemoglobin, carbonate) Renal mechanism Respiratory
12/4/2017. Disclosure. Educational Objectives. Has been consultant for Bard, Chiesi
 Temperature Management in Neuro ICU Kiwon Lee, MD, FACP, FAHA, FCCM Professor of Neurology, RWJ Medical School Chief of Neurology, RWJ University Hospital Director, RWJ Comprehensive Stroke Center Director,
Temperature Management in Neuro ICU Kiwon Lee, MD, FACP, FAHA, FCCM Professor of Neurology, RWJ Medical School Chief of Neurology, RWJ University Hospital Director, RWJ Comprehensive Stroke Center Director,
New Therapeutic Hypothermia Techniques
 New Therapeutic Hypothermia Techniques Joseph P. Ornato, MD, FACP, FACC, FACEP Professor & Chairman, Emergency Medicine Virginia Commonwealth University Health System Richmond, VA Medical Director Richmond
New Therapeutic Hypothermia Techniques Joseph P. Ornato, MD, FACP, FACC, FACEP Professor & Chairman, Emergency Medicine Virginia Commonwealth University Health System Richmond, VA Medical Director Richmond
Fetal Heart Rate Monitoring Myths and Misperceptions s: Electronic Fetal Heart Rate Monitoring (EFM): Baseline Assumptions.
: Baseline Assumptions.") Can FHR Monitoring Prevent Hypoxic-Ischemic Encephalopathy in the Newborn? Fetal Heart Rate Monitoring Myths and Misperceptions 1. Yes 2. No 72% Tekoa L. King CNM, MPH June 6, 2008 28% Yes No Objectives
Can FHR Monitoring Prevent Hypoxic-Ischemic Encephalopathy in the Newborn? Fetal Heart Rate Monitoring Myths and Misperceptions 1. Yes 2. No 72% Tekoa L. King CNM, MPH June 6, 2008 28% Yes No Objectives
Provide guidelines for the management of mechanical ventilation in infants <34 weeks gestation.
 Page 1 of 5 PURPOSE: Provide guidelines for the management of mechanical ventilation in infants
Page 1 of 5 PURPOSE: Provide guidelines for the management of mechanical ventilation in infants
(31189) Hypothermia Initiation Phase One
 Hypothermia Initiation Phase One") Hypothermia Initiation Phase One Diagnosis Allergies For hypothermia tracking purposes only. Please do not uncheck.- Required Cardiac Emergency Tracking For hypothermia tracking purposes only. Consults
Hypothermia Initiation Phase One Diagnosis Allergies For hypothermia tracking purposes only. Please do not uncheck.- Required Cardiac Emergency Tracking For hypothermia tracking purposes only. Consults
The Blue Baby. Network Stabilisation of the Term Infant Study Day 15 th March 2017 Joanna Behrsin
 The Blue Baby Network Stabilisation of the Term Infant Study Day 15 th March 2017 Joanna Behrsin Session Structure Definitions and assessment of cyanosis Causes of blue baby Structured approach to assessing
The Blue Baby Network Stabilisation of the Term Infant Study Day 15 th March 2017 Joanna Behrsin Session Structure Definitions and assessment of cyanosis Causes of blue baby Structured approach to assessing
Experience. Initials Medical Staffing Network Rev. 06/15 F01201 NNICU 2 of 5
 Neonatal Intensive Care Unit Self Assessment Directions Please circle a value for each question to provide us and the interested facilities with an assessment of your clinical experience. These values
Neonatal Intensive Care Unit Self Assessment Directions Please circle a value for each question to provide us and the interested facilities with an assessment of your clinical experience. These values
Cooling guidance for babies presenting with moderate to severe hypoxic ischaemic encephalopathy within the North West London Perinatal Network
 Cooling guidance for babies presenting with moderate to severe hypoxic ischaemic encephalopathy within the North West London Perinatal Network 1. INTRODUCTION Perinatal asphyxia severe enough to cause
Cooling guidance for babies presenting with moderate to severe hypoxic ischaemic encephalopathy within the North West London Perinatal Network 1. INTRODUCTION Perinatal asphyxia severe enough to cause
DOWNLOAD OR READ : PERINATAL EVENTS AND BRAIN DAMAGE IN SURVIVING CHILDREN BASED ON PAPERS PRESENTED AT AN INTERNATIONA PDF EBOOK EPUB MOBI
 DOWNLOAD OR READ : PERINATAL EVENTS AND BRAIN DAMAGE IN SURVIVING CHILDREN BASED ON PAPERS PRESENTED AT AN INTERNATIONA PDF EBOOK EPUB MOBI Page 1 Page 2 perinatal events and brain damage in surviving
DOWNLOAD OR READ : PERINATAL EVENTS AND BRAIN DAMAGE IN SURVIVING CHILDREN BASED ON PAPERS PRESENTED AT AN INTERNATIONA PDF EBOOK EPUB MOBI Page 1 Page 2 perinatal events and brain damage in surviving
Neonatal/Pediatric Cardiopulmonary Care
 Neonatal/Pediatric Cardiopulmonary Care Resuscitation 2 When To Resuscitate Need usually related Combination of Can occur in 3 Causes of Fetal Asphyxia 1 4 Apnea Hypoxia Stimulates chemoreceptors & baroreceptors
Neonatal/Pediatric Cardiopulmonary Care Resuscitation 2 When To Resuscitate Need usually related Combination of Can occur in 3 Causes of Fetal Asphyxia 1 4 Apnea Hypoxia Stimulates chemoreceptors & baroreceptors
The Evidence Base. Stephan A. Mayer, MD. Columbia University New York, NY
 Hypothermic for Cardiac Arrest The Evidence Base Stephan A. Mayer, MD Director, Neuro-ICU Columbia University New York, NY Disclosures Columbia University Clinical Trials Pilot Award Radiant Medical, Inc.
Hypothermic for Cardiac Arrest The Evidence Base Stephan A. Mayer, MD Director, Neuro-ICU Columbia University New York, NY Disclosures Columbia University Clinical Trials Pilot Award Radiant Medical, Inc.