A Review of Sleep Disorders in Neurology
|
|
|
- Gabriella Goodwin
- 5 years ago
- Views:
Transcription


1 A Review of Sleep Disorders in Neurology Chung-Yao Hsu, M.D., Ph.D. Section of Epilepsy and Sleep Disorders Department of Neurology Kaohsiung Medical University Hospital 1
, and would be missed on this")
2 Stage I sleep. Vertex waves are focal sharp transients typically best seen on transverse montages (through the midline), and would be missed on this longitudinal bipolar montage if it did not include midline channels (Fz-Cz-Pz). Vertex waves are seen in stages I and II sleep. 2

3 Stage I sleep. POSTS are seen in both occipital regions, with their typical characteristics contained in their name: Positive Occipital Sharp Transients of Sleep. They also have the morphology classically described as comparable to a reverse check mark, and often occur in consecutive runs of several seconds, as shown here. 3


4 Stage II sleep. On this transverse montage, there is a K-complex in the fifth second, with its typical broad duration (>500 ms), diphasic morphology, and overriding spindle. There are also abundant spindles before and after. 4


5 Slow wave sleep. There is predominantly delta activity. 5


6 REM sleep. Typical saccadic eye movements are shown, with lateral rectus spikes seen just preceding the lateral abducting eye movements. 6
 nuclei Copyright 2004 Allyn and")
7 Generation of REM sleep Lateral dorsal tegmental (LDT) nuclei Pedunculopontine tegmental (PPT) nuclei Copyright 2004 Allyn and Bacon 7
8 Biochemistry of REM Sleep 8
9 An EEG recording of a 24 year- old lady Fp1-F3 F3-C3 C3-P3 P3-O1 Fp2-F4 F4-C4 C4-P4 P4-O2 Fp1-F7 F7-T3 T3-T5 T5-O1 Fp2-F8 F8-T4 T4-T6 T6-O2 T3-C3 C3-Cz Cz-C4 C4-T4 LOC ROC CHIN
10 The following description is correct EXCEPT: (A) Positive occipital sharp transients (POSTs) usually coexist (B) Sleep spindles and K-complexes may follow (C) Rapid eye movement is evident in this stage (D) Slow eye movement (eye rolling) is evident in this stage (E) It can not be taken as epileptiform discharges 10

11 DSM-IV Diagnostic Criteria for Primary Insomnia 11
12 The Development of Psychophysiological Insomnia 12
13 Behavioral Treatment of Insomnia Sleep hygiene Relaxation training Stimulus control instructions Sleep restriction therapy 13
14 Mechanisms of Sleep-Promoting Agents Class Drug Mechanism Barbiturates Phenobarbital GABA A Sedatives & Hypnotics Benzodiazepine Imidazopyridine Flunitrazepam Nitrazepam Estazolam Zaleplon Zolpidem GABA A ω 1 + ω 2 GABA A ω 1 Anticonvulsant Gaboxadol Tiagabine GABA A gabapentin Antidepressant Mirtazapine Trazodone 5HT2 A Antihistamine Cyproheptadine Diphenhydramine H 1 14



15 Human Disasters due to Sleepiness 15
16 Epworth Sleepiness Scale (ESS) Situation Chance of dozing (0 3) Sitting and reading Watching television Sitting inactive in a public place for example, a theater or meeting As a passenger in a car for an hour without a break Lying down to rest in the afternoon Sitting and talking to someone Sitting quietly after lunch (when you ve had no alcohol) In a car, while stopped in traffic Total Score Johns MW. Sleep. 1991;14: = would never doze 1 = slight chance of dozing 2 = moderate chance of dozing 3 = high chance of dozing
17 Multiple Sleep Latency Test Series of naps, presented at 2-h intervals, beginning approx. 2-h after initial (morning) awakening. Normal MSLT: Mean sleep latency mins 2 Sleep onset REM period (SOREMP) 17
18 MSLT and Age 18

19 Obstructive Sleep Apnea (OSA) 19

20 Case Demo of OSA 20
21 21
22 Symptoms of OSA Excessive daytime sleepiness Habitual snoring Witnessed apneic episodes Choking or gasping in sleep Tiredness upon awakening Nocturia Morning headache 22

23 Continuous Positive Airway Pressure (CPAP) Flow Generator Nasal Mask Tubing Headgear 23

24 Mandibular Repositioning Appliance (MRA) 24
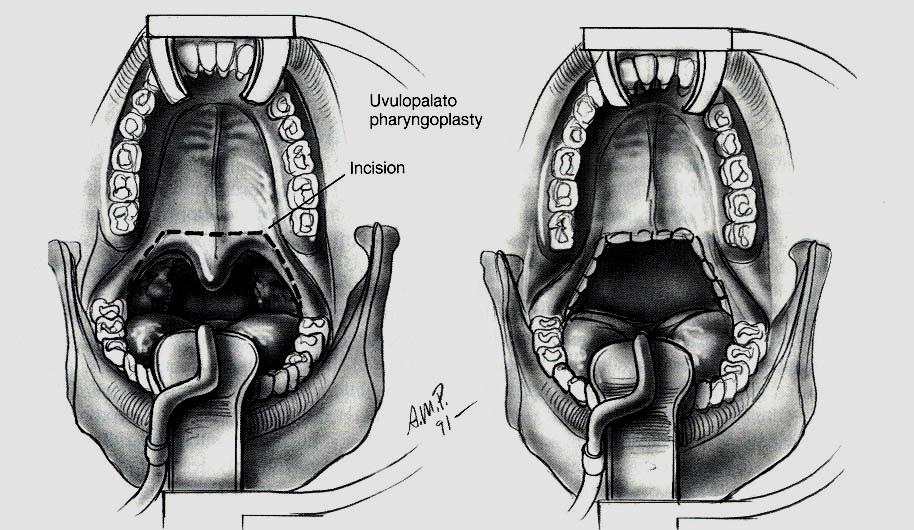
25 Uvulopalatopharyngoplasty (UPPP) 25

26 Mechanisms Associated With Obstructive Sleep Apnea That Potentially Contribute to Risk of Cardiovascular Disease Shamsuzzaman, A. S. M. et al. JAMA 2003;290:

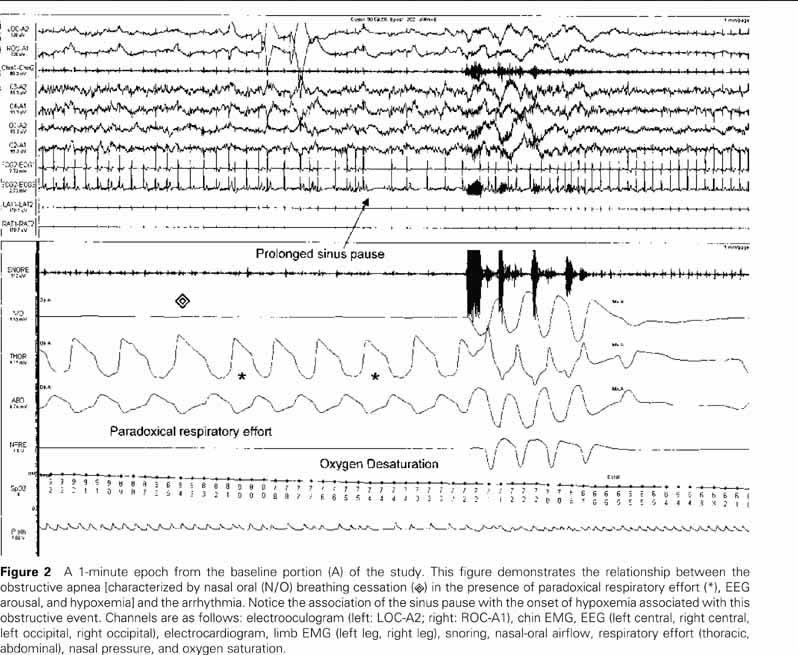
27 Polysomnography of a 46 yearold obese man 27
28 The following descriptions are correct EXCEPT: (A) Avoid alcohol or benzodiazepine should be suggested (B) MSLT is the next step to support the diagnosis (C) The treatment of choice is CPAP (D) Hypersomnia is a major daytime symptom (E) Hypertension is usually associated 28
29 Central Apnea with Age Prevalence (%) Age Category Bixler EO. Am J Respir Crit Care Med 1998;157:144 29

30 Lesions for Central Sleep Apnea A: Chemoreceptors B: Respiratory groups C: Cervico-medullary junction D: Anterior horn cells E: Phrenic nerve F: N-M junction G: Diaphragm 30
31 Two Types of CSA 1) Normocapnic or hypocapnic CSA (including Cheyne-Stoke breathing, idiopathic central sleep apnea and high altitude central sleep apnea) 2) Hypercapnic CSA (sleep-related hypoventilation/hypoxemic syndrome) 31
32 Diagnostic Criteria of CSR 1) Either congestive heart failure or neurological disease with respiratory monitoring that demonstrates at least three consecutive cycles of a cyclical crescendo and decrescendo change in breathing amplitude. 2) Either five or more central sleep apneashypopneas per hour of sleep or cyclic crescendo and decrescendo changes in breathing amplitude that have a duration of at least 10 consecutive minutes. 32

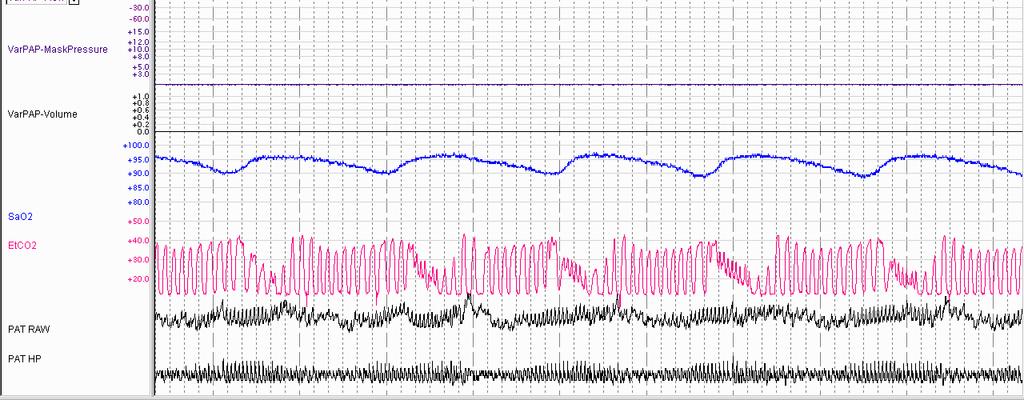
33 SaO2 and EtCo2 during Cheyne-Stokes Respiration 33
34 Diagnostic Criteria of SHHS Either erythrocytosis, cor pulmonale, pulmonary hypertension, or excessive daytime hypersomnolence not explained by other factors. Hypercapnia (PSG shows either an increase in PaCO2 greater than 55 mmhg for at least 10 minutes or an increase in PaCO2 during sleep greater than 10 mmhg from wake values to a value exceeding 50mmHg for at least 10 minutes). 34
35 SHHS not related with Respiratory Diseases Disorders of the sensory input systems Disorders of the central ventilatory control system Defects of the motor output system 35

36 MRI (T2WI) at C2-C3 Level 36

37 MRI (T2WI) at Medulla Level 37
38 The following diseases can cause OSA and CSA (including SHVS) EXCEPT: (A) Supratentorial stroke (B) Brain stem stroke (C) Myotonic dystrophy (D) Pompe disease (E) Cervical spinal cord injury 38

39 Narcolepsy (Tetrad) Excessive daytime sleepiness (EDS) Cataplexy Hypnagogic/ Hypnopompic hallucinations Sleep paralysis (Disrupted nocturnal sleep) 39

40 Case Demo of Cataplexy 40

41 Onset of Narcolepsy 41
42 MSLT Findings in Narcolepsy Mean sleep latency 8 minutes Sleep onset REM period (SOREMP) 2 42

43 Sleep Onset REM Period (SOREMP) Narcolepsy is characterized by a sudden transition from wake to REM sleep (sleep-onset-rapid-eyemovement period, SOREMP) 43
44 Kryger et al. Principle and Practice of Sleep Medicine 4 th edition 44

45 HLA Typing in Narcolepsy 45

46 Highly Selective CNS Activity Lin JS, et al. Potential brain neuronal targets for amphetamine, methylphenidate, and modafinil-induced wakefulness, evidenced by c-fos immunocytochemistry in the cat. Proc Natl Acad Sci USA. 1996;93:
47 Treatment of Cataplexy and REMrelated Phenomenon Tricyclic antidepressant (TCA) Selective serotonin reuptake inhibitors (SSRI) Sodium oxybate: a naturally occurring neurotransmitter in the brain involved in sleep regulation and a central nervous system depressant is used as a new anti-cataplatic agent with unkown mechanism 47
48 Which of the following statement about narcolepsy with cataplexy is CORRECT? (A) In most patients, it is associated with HLAB8 (B) Orexin/Hypocretin is produced by a group of neurons in the posterior lateral hypothalamus (C) CSF orexin/hypocretin level is elevated in most patients with narcolepsy (D) Sleep paralysis is usually the first symptom in patients with narcolepsy and cataplexy (E) Hypnagogic hallucinations are absent 48

49 REM Sleep Behavior Disorder 0.5% in the elderly Abnormal behavior associated with excess of EMG during REM sleep Sleep-related injury Male-predominant, age 50 or older Idiopathic Neurological disorders (alphasynucleinopathy): Parkinsonism, dementia with Lewy bodies, multiple system atrophy, stroke, antidepressants 49

50 Case Demo of RBD 50

51 REM Sleep Without Atonia 51
52 Management of RBD Environmental safety Clonazepam (Rivotril mg qhs): highly effective (90% or more) Levodopa or dopamine agonist: maybe effective in patients associated with Parkinson s disease Melatonin: case report 52

53 Polysomnography of a 68 Year- Old man with RBD 53
54 REM sleep behavior disorder can be found in: (A) Pontine infarction (B) Multiple system atrophy (C) Parkinson s disease (D) Dementia with Lewy bodies (E) All of above 54

55 Disorders of Arousal Somnabulism (sleep walking) Sleep terror Confusional arousals From ghoulies and ghosties, And three leggity beasties, And things that go bump in the night, Good Lord, deliver us. Old Scottish Prayer 55

56 Case Demo of Sleep Terror In a Child 56

57 Polysomnography of Somnabulism 57
58 Management of Sleep Walking Decrease deeper sleep: avoid sleep deprivation Decrease source of arousals: sleepdisordered breathing, RLS/PLM, external noise Good sleep hygiene Benzodiazipines Benign neglect: if mild, safe and not common (mostly for children) Respond to event: ensure safety, encourage return to sleep 58
59 Which of the following sleep disorders is (are) found in the NREM sleep stage? A. Sleep walking B. Nightmares (A) A only (B) B only (C) Both A and B (D) Neither A and B 59
60 Epilepsy Misdiagnosed as Sleep Disorders Nocturnal frontal lobe epilepsy (NFLE) Paroxysmal arousals (PA) Epileptic nocturnal wandering (ENW) Nocturnal paroxysmal dystonia (NPD) Supplementary motor seizures Nocturnal temporal lobe epilepsy 60
61 Which of the following statements is CORRECT about the differential diagnosis of nocturnal seizure and parasomnia? (A) Parasomnia usually presents as stereotypic behavior (B) Parasomnia is usually associated with dystonic or tonic posture (C) Patients with nocturnal seizure usually can remember the events (D) Nocturnal seizure usually occurs in clusters (E) The duration of attack of parasomnia is usually brief but nocturnal seizure is much longer 61
62 Restless Legs Syndrome (RLS) An urge to move the legs, usually accompanied or caused by uncomfortable and unpleasant sensations in the legs Begin or worsen during periods of rest or inactivity Partially or totally relieved by movement, such as walking or stretching Worse, or only occur, in the evening or night Cause secondary insomnia 62
63 Secondary RLS Iron deficiency anemia and low ferritin levels Polyneuropathy Uremia Folate/ Vitamin B12 deficiency Hypothyroidism Pregnancy Varicose veins Cigarette smoking and caffeine Obesity 63
64 Medications and Secondary RLS Psychotropic agents: dopamine antagonists, antidepressants, lithium (Bupropion with its dopaminergic activity may benefit RLS) Antihistamine, Antinausea/Antiemetics Alcohol and caffaine Beta blockers, CCBs 64
65 Periodic Limb Movement in Sleep (PLMS) Rhythmic dorsiflexion of the big toe and ankle with occasional flexions of the knee and hip Recording tibialis anterior EMG activity Duration: seconds Intermovement interval: 5 90 seconds (most frequently seconds) 4 leg movements in a series The amplitude of the EMG 25% of the amplitude reached during biological calibration 65

66 Case Demo of PLMS 66
")
67 PSG of PLMS (30 seconds) 67
68 Treatment for RLS and PLMS Dopamine agonists (Ropinirole, Pramipexole) Benzodiazepine: Clonazepam Anticonvulsant: Gabapentin Opiates 68
69 Which of the following conditions shows least association with secondary restless legs syndrome? (A) Motor neuron disease (B) Uremia (C) Iron deficiency (D) Pregnancy (E) Neuropathy 69
70 Which of the following medication is NOT indicated for the treatment of RLS? (A) Ropirinorole (B) Levodopa (C) Clonazepam (D) Gabapentin (E) Trazodone 70
71 Kleine-Levin Syndrome A rare condition almost exclusive to adolescent males that includes episodes of hypersomnia, cognitive changes, eating disturbances, hypersexuality, compulsions, and depressed mood. It can be idiopathic or secondary to infection, trauma, or alcohol consumption. When it occurs in females, it is more severe. Patients are normal in between episodes and it generally resolves over time. 71
72 Clock in the Brain Light Output Rhythms Physiology Behavior Suprachiasmatic Nuclei (SCN) 72

73 Free-running of Human Circadian Rhythm 73
74 Sleep Phase Syndromes SUMMARY ASPS Typical DSPS ASPS: advance sleep phase syndrome DSPS: delayed sleep phase syndrome 74
75 Bright Light The discovery that bright light (2,500-10,000 Lux) shifts human circadian rhythms and that the size and direction of the shift depends on time of exposure, has been a significant breakthrough in the management of circadian rhythm disorders. Light in the early morning (~6AM) advances rhythms, whereas, light in the evening (6-8 PM) delays circadian rhythms. Bright light therapy has been used successfully in several situations: 75

76 Figure 5.3 People traveling east suffer more serious jet lag than people t li t 76

77 Figure 5.4 The graveyard shift is aptly named serious industrial accidents usually occur at night, when workers are least alert. Night-shift jobs providing emergency services are essential. But few people want to work permanently at night, so workers rotate among three shifts. As in jet lag, the direction of change is critical. Moving forward clockwise is easier than going backward. 77

78 Sleep Diary of a 23 year-old woman 78
79 Which one is the most likely diagnosis? (A) Advanced sleep phase syndrome (B) Delayed sleep phase syndrome (C) Non-entrained (free-running) sleepwake disorder (D) Irregular sleep-wake disorder (E) Primary insomnia 79

80 Treatment of Cataplexy and REMrelated Phenomenon Tricyclic antidepressant (TCA) Selective serotonin reuptake inhibitors (SSRI) Sodium oxybate: a naturally occurring neurotransmitter in the brain involved in sleep regulation and a central nervous system depressant is used as a new anticataplatic agent with unkown mechanism 80
Diagnosis and treatment of sleep disorders
 Diagnosis and treatment of sleep disorders Normal human sleep Sleep cycle occurs about every 90 minutes, approximately 4-6 cycles occur per major sleep episode NREM (70-80%) slow wave sleep heart rate,
Diagnosis and treatment of sleep disorders Normal human sleep Sleep cycle occurs about every 90 minutes, approximately 4-6 cycles occur per major sleep episode NREM (70-80%) slow wave sleep heart rate,
Assessment of Sleep Disorders DR HUGH SELSICK
 Assessment of Sleep Disorders DR HUGH SELSICK Goals Understand the importance of history taking Be able to take a basic sleep history Be aware the technology used to assess sleep disorders. Understand
Assessment of Sleep Disorders DR HUGH SELSICK Goals Understand the importance of history taking Be able to take a basic sleep history Be aware the technology used to assess sleep disorders. Understand
Help I Have Problems with My Sleep!
 Help I Have Problems with My Sleep! Over An 85 Year Lifespan Sleep 31% Work 21% Exercise 1% Food and Drink 11% Sleep Is Important! You can survive without food for up to 2 months Without water 3-5 days
Help I Have Problems with My Sleep! Over An 85 Year Lifespan Sleep 31% Work 21% Exercise 1% Food and Drink 11% Sleep Is Important! You can survive without food for up to 2 months Without water 3-5 days
Index. sleep.theclinics.com. Note: Page numbers of article titles are in boldface type.
 Note: Page numbers of article titles are in boldface type. A Actigraphy, 475, 485, 496 Adolescents, sleep disorders in, 576 578 Adults, sleep disorders in, 578 580 Advanced sleep phase disorder, 482 Age,
Note: Page numbers of article titles are in boldface type. A Actigraphy, 475, 485, 496 Adolescents, sleep disorders in, 576 578 Adults, sleep disorders in, 578 580 Advanced sleep phase disorder, 482 Age,
SLEEP DISORDERS. Kenneth C. Sassower, MD Division of Sleep Medicine; Department of Neurology Massachusetts General Hospital for Children
 SLEEP DISORDERS Kenneth C. Sassower, MD Division of Sleep Medicine; Department of Neurology Massachusetts General Hospital for Children Distinctive Features of Pediatric Sleep Daytime sleepiness uncommon
SLEEP DISORDERS Kenneth C. Sassower, MD Division of Sleep Medicine; Department of Neurology Massachusetts General Hospital for Children Distinctive Features of Pediatric Sleep Daytime sleepiness uncommon
Overview. Sleep Related Movement Disorders - Restless Leg Syndrome - Periodic Limb movements in Sleep
 The Structure of Sleep The Parasomnias - in REM - in Non-REM - Narcolepsy Overview Sleep Related Movement Disorders - Restless Leg Syndrome - Periodic Limb movements in Sleep Circadian Rhythm disorders
The Structure of Sleep The Parasomnias - in REM - in Non-REM - Narcolepsy Overview Sleep Related Movement Disorders - Restless Leg Syndrome - Periodic Limb movements in Sleep Circadian Rhythm disorders
Sleep disorders. Norbert Kozak
 Sleep disorders Norbert Kozak About the sleep Each of us will spend about 1/3 of our lifetime sleeping....and 1/3 part of the population has sleep complain Sleep is an essential biological function, but
Sleep disorders Norbert Kozak About the sleep Each of us will spend about 1/3 of our lifetime sleeping....and 1/3 part of the population has sleep complain Sleep is an essential biological function, but
Index. sleep.theclinics.com. Note: Page numbers of article titles are in boldface type.
 Note: Page numbers of article titles are in boldface type. A Accidents, risk of, with insufficient sleep, 318 Acquired immunodeficiency syndrome (AIDS), comorbid with narcolepsy, 298 299 Actigraphy, in
Note: Page numbers of article titles are in boldface type. A Accidents, risk of, with insufficient sleep, 318 Acquired immunodeficiency syndrome (AIDS), comorbid with narcolepsy, 298 299 Actigraphy, in
Index SLEEP MEDICINE CLINICS. Note: Page numbers of article titles are in boldface type. Cerebrospinal fluid analysis, for Kleine-Levin syndrome,
 165 SLEEP MEDICINE CLINICS Index Sleep Med Clin 1 (2006) 165 170 Note: Page numbers of article titles are in boldface type. A Academic performance, effects of sleepiness in children on, 112 Accidents,
165 SLEEP MEDICINE CLINICS Index Sleep Med Clin 1 (2006) 165 170 Note: Page numbers of article titles are in boldface type. A Academic performance, effects of sleepiness in children on, 112 Accidents,
Parkinson s Disease Associated Sleep Disturbance Ehsan M. Hadi, MD, MPH. Dignity Health Neurological Institute
 Parkinson s Disease Associated Sleep Disturbance Ehsan M. Hadi, MD, MPH. Dignity Health Neurological Institute Parkinson s Disease 2 nd most common neurodegenerative disorder Peak age at onset is 60 years
Parkinson s Disease Associated Sleep Disturbance Ehsan M. Hadi, MD, MPH. Dignity Health Neurological Institute Parkinson s Disease 2 nd most common neurodegenerative disorder Peak age at onset is 60 years
Sleep Medicine. Maintenance of Certification Examination Blueprint. Purpose of the exam
 Sleep Medicine Maintenance of Certification Examination Blueprint Purpose of the exam The exam is designed to evaluate the knowledge, diagnostic reasoning, and clinical judgment skills expected of the
Sleep Medicine Maintenance of Certification Examination Blueprint Purpose of the exam The exam is designed to evaluate the knowledge, diagnostic reasoning, and clinical judgment skills expected of the
TOP 10 LIST OF SLEEP QUESTIONS. Kenneth C. Sassower, MD Sleep Disorders Unit Massachusetts General Hospital for Children
 TOP 10 LIST OF SLEEP QUESTIONS Kenneth C. Sassower, MD Sleep Disorders Unit Massachusetts General Hospital for Children QUESTION #1: ARE SLEEP ISSUES IN CHILDREN THE SAME AS IN ADULTS? Distinctive Features
TOP 10 LIST OF SLEEP QUESTIONS Kenneth C. Sassower, MD Sleep Disorders Unit Massachusetts General Hospital for Children QUESTION #1: ARE SLEEP ISSUES IN CHILDREN THE SAME AS IN ADULTS? Distinctive Features
HEALTHY LIFESTYLE, HEALTHY SLEEP. There are many different sleep disorders, and almost all of them can be improved with lifestyle changes.
 HEALTHY LIFESTYLE, HEALTHY SLEEP There are many different sleep disorders, and almost all of them can be improved with lifestyle changes. HEALTHY LIFESTYLE, HEALTHY SLEEP There are many different sleep
HEALTHY LIFESTYLE, HEALTHY SLEEP There are many different sleep disorders, and almost all of them can be improved with lifestyle changes. HEALTHY LIFESTYLE, HEALTHY SLEEP There are many different sleep
Dr Alex Bartle. Medical Director Sleep Well Clinic Christchurch
 Dr Alex Bartle Medical Director Sleep Well Clinic Christchurch 8:30-9:25 WS #191: Sleep Disorders in The Elderly 9:35-10:30 WS #203: Sleep Disorders in The Elderly (Repeated) REM - Rapid Eye Movement
Dr Alex Bartle Medical Director Sleep Well Clinic Christchurch 8:30-9:25 WS #191: Sleep Disorders in The Elderly 9:35-10:30 WS #203: Sleep Disorders in The Elderly (Repeated) REM - Rapid Eye Movement
Corporate Medical Policy
 Corporate Medical Policy Polysomnography for Non Respiratory Sleep Disorders File Name: Origination: Last CAP Review: Next CAP Review: Last Review: polysomnography_for_non_respiratory_sleep_disorders 10/2015
Corporate Medical Policy Polysomnography for Non Respiratory Sleep Disorders File Name: Origination: Last CAP Review: Next CAP Review: Last Review: polysomnography_for_non_respiratory_sleep_disorders 10/2015
Sleep & Wakefulness Disorders in Parkinson s Disease: The Challenge of Getting a Good Night s Sleep
 Sleep & Wakefulness Disorders in Parkinson s Disease: The Challenge of Getting a Good Night s Sleep Helene A. Emsellem, MD March 25, 2017 The Center for Sleep & Wake Disorders PFNCA Symposium Sleep is
Sleep & Wakefulness Disorders in Parkinson s Disease: The Challenge of Getting a Good Night s Sleep Helene A. Emsellem, MD March 25, 2017 The Center for Sleep & Wake Disorders PFNCA Symposium Sleep is
Dr Alex Bartle. Director Sleep Well Clinic
 Dr Alex Bartle Director Sleep Well Clinic 1 Sleep Architecture REM NREM Rapid Eye Movement Non-Rapid Eye Movement Stages 1 and 2 light sleep Stages 3 and 4 deep sleep 25% REM, 50% Stage 2 and 25% stages
Dr Alex Bartle Director Sleep Well Clinic 1 Sleep Architecture REM NREM Rapid Eye Movement Non-Rapid Eye Movement Stages 1 and 2 light sleep Stages 3 and 4 deep sleep 25% REM, 50% Stage 2 and 25% stages
Pharmacy Benefit Determination Policy
 Policy Subject: CNS Stimulant Medications Policy Number: SHS PBD06 Category: CNS Drugs Policy Type: Medical Pharmacy Department: Pharmacy Product (check all that apply): Group HMO/POS ASO PPO Individual
Policy Subject: CNS Stimulant Medications Policy Number: SHS PBD06 Category: CNS Drugs Policy Type: Medical Pharmacy Department: Pharmacy Product (check all that apply): Group HMO/POS ASO PPO Individual
Sleep. Anil Rama, MD Medical Director, Division of Sleep Medicine The Permanente Medical Group
 Sleep Anil Rama, MD Medical Director, Division of Sleep Medicine The Permanente Medical Group Assistant Adjunct Clinical Faculty Stanford School of Medicine Circadian Rhythm of Sleep Body temperature 7
Sleep Anil Rama, MD Medical Director, Division of Sleep Medicine The Permanente Medical Group Assistant Adjunct Clinical Faculty Stanford School of Medicine Circadian Rhythm of Sleep Body temperature 7
A Scream in the Night. ARTP Conference 2010 Dr Christopher Kosky
 A Scream in the Night ARTP Conference 2010 Dr Christopher Kosky Parasomnia Slow Wave Sleep Arousal Disorder REM Sleep Behaviour Disorder Nocturnal Epilepsy Catathrenia Slow Wave Sleep Arousal Disorders
A Scream in the Night ARTP Conference 2010 Dr Christopher Kosky Parasomnia Slow Wave Sleep Arousal Disorder REM Sleep Behaviour Disorder Nocturnal Epilepsy Catathrenia Slow Wave Sleep Arousal Disorders
Sleep Complaints and Disorders in Epileptic Patients 순천향의대천안병원순천향의대천안병원신경과양광익
 Sleep Complaints and Disorders in Epileptic Patients 순천향의대천안병원순천향의대천안병원신경과양광익 Introduction The global physical, social and economic consequence of epilepsy are high. WHO 2000 study Improving QoL is increasingly
Sleep Complaints and Disorders in Epileptic Patients 순천향의대천안병원순천향의대천안병원신경과양광익 Introduction The global physical, social and economic consequence of epilepsy are high. WHO 2000 study Improving QoL is increasingly
Sleep Medicine Maintenance of Certification Examination Blueprint
 Sleep Medicine Maintenance of Certification Examination Blueprint Purpose of the exam The exam is designed to evaluate the knowledge, diagnostic reasoning, and clinical judgment skills expected of the
Sleep Medicine Maintenance of Certification Examination Blueprint Purpose of the exam The exam is designed to evaluate the knowledge, diagnostic reasoning, and clinical judgment skills expected of the
INTRINSIC SLEEP DISORDERS. Excessive daytime sleepiness (EDS) is a common complaint. Causes of EDS are numerous and include:
 is a common complaint. Causes of EDS are numerous and include:") INTRINSIC SLEEP DISORDERS Introduction Excessive daytime sleepiness (EDS) is a common complaint. Causes of EDS are numerous and include: Intrinsic sleep disorders (e.g. narcolepsy, obstructive sleep apnoea/hypopnea
INTRINSIC SLEEP DISORDERS Introduction Excessive daytime sleepiness (EDS) is a common complaint. Causes of EDS are numerous and include: Intrinsic sleep disorders (e.g. narcolepsy, obstructive sleep apnoea/hypopnea
WHY CAN T I SLEEP? Deepti Chandran, MD
 WHY CAN T I SLEEP? Deepti Chandran, MD Sleep and Aging How does sleep change as we age? Do we need less sleep as we get older? Can a person expect to experience more sleep problems or have a sleep disorder
WHY CAN T I SLEEP? Deepti Chandran, MD Sleep and Aging How does sleep change as we age? Do we need less sleep as we get older? Can a person expect to experience more sleep problems or have a sleep disorder
Polysomnography (PSG) (Sleep Studies), Sleep Center
 (Sleep Studies), Sleep Center") Policy Number: 1036 Policy History Approve Date: 07/09/2015 Effective Date: 07/09/2015 Preauthorization All Plans Benefit plans vary in coverage and some plans may not provide coverage for certain service(s)
Policy Number: 1036 Policy History Approve Date: 07/09/2015 Effective Date: 07/09/2015 Preauthorization All Plans Benefit plans vary in coverage and some plans may not provide coverage for certain service(s)
130 Preston Executive Drive Cary, NC Ph(919) Fax(919) Page 1 of 6. Patient History
 Fax(919) Page 1 of 6. Patient History") 130 Preston Executive Drive Cary, NC 27513 Ph(919)462-8081 Fax(919)462-8082 www.parkwaysleep.com Page 1 of 6 Patient History *Please fill out in dark BLACK INK only. General Information Name Sex: Male
130 Preston Executive Drive Cary, NC 27513 Ph(919)462-8081 Fax(919)462-8082 www.parkwaysleep.com Page 1 of 6 Patient History *Please fill out in dark BLACK INK only. General Information Name Sex: Male
Treating sleep disorders
 Treating sleep disorders Sue Wilson Centre for Neuropsychopharmacology Imperial College London sue.wilson@imperial.ac.uk Suggested algorithm for treatment of insomnia Diagnosis of insomnia Associated with
Treating sleep disorders Sue Wilson Centre for Neuropsychopharmacology Imperial College London sue.wilson@imperial.ac.uk Suggested algorithm for treatment of insomnia Diagnosis of insomnia Associated with
OBJECTIVES. The psychiatric, medical, and neurologic causes of sleep problems. Office-based and objective methods of evaluating sleep
 SLEEP ISSUES 1 OBJECTIVES 2 Know and understand: Age-related changes in sleep The psychiatric, medical, and neurologic causes of sleep problems Office-based and objective methods of evaluating sleep Appropriate
SLEEP ISSUES 1 OBJECTIVES 2 Know and understand: Age-related changes in sleep The psychiatric, medical, and neurologic causes of sleep problems Office-based and objective methods of evaluating sleep Appropriate
Managing Sleep Disorders in Primary Care. Objectives. Disclosures. Nancy Nadolski, FNP, MSN, M.Ed Insomnia Medicine of Idaho Boise Counseling Center
 Managing Sleep Disorders in Primary Care Nancy Nadolski, FNP, MSN, M.Ed Insomnia Medicine of Idaho Boise Counseling Center www.sleeplessinidaho.com 1 Objectives 1) Identify stages and behaviors for normal
Managing Sleep Disorders in Primary Care Nancy Nadolski, FNP, MSN, M.Ed Insomnia Medicine of Idaho Boise Counseling Center www.sleeplessinidaho.com 1 Objectives 1) Identify stages and behaviors for normal
ATHLETES & PRESCRIBING PHYSICIANS PLEASE READ
 ATHLETES & PRESCRIBING PHYSICIANS PLEASE READ USADA can grant a Therapeutic Use Exemption (TUE) in compliance with the World Anti- Doping Agency International Standard for TUEs. The TUE application process
ATHLETES & PRESCRIBING PHYSICIANS PLEASE READ USADA can grant a Therapeutic Use Exemption (TUE) in compliance with the World Anti- Doping Agency International Standard for TUEs. The TUE application process
PULMONARY & CRITICAL CARE CONSULTANTS OF AUSTIN 1305 West 34 th Street, Suite 400, Austin, TX Phone: Fax:
 Name: Sex: Age: Date: Date of Birth Height Weight Neck size Referring Physician: Primary Care MD: Main Sleep Complaint(s) trouble falling asleep trouble remaining asleep excessive sleepiness during the
Name: Sex: Age: Date: Date of Birth Height Weight Neck size Referring Physician: Primary Care MD: Main Sleep Complaint(s) trouble falling asleep trouble remaining asleep excessive sleepiness during the
SLEEP DISORDERS CENTER QUESTIONNAIRE
 Carteret Health Care Patient's name DOB Gender: M F Date of Visit _ Referring physicians: Primary care providers: Please complete the following questionnaire by filling in the blanks and placing a check
Carteret Health Care Patient's name DOB Gender: M F Date of Visit _ Referring physicians: Primary care providers: Please complete the following questionnaire by filling in the blanks and placing a check
노인병원에서 Light Therapy 의 활용 박 기 형 진주삼성병원 송도병원 신경과
 Light Therapy 1 : 15 / 63 (23.8%) 1 : 7 2 : 8 : 6 / 86 (7%) 1, : 48 / 205 (23.4%) 1 : 43 2 : 5 Sleep in Geriatrics Prevalence NIH survey of 9000 american senior above age 65 ; 88% had sleep disturbances
Light Therapy 1 : 15 / 63 (23.8%) 1 : 7 2 : 8 : 6 / 86 (7%) 1, : 48 / 205 (23.4%) 1 : 43 2 : 5 Sleep in Geriatrics Prevalence NIH survey of 9000 american senior above age 65 ; 88% had sleep disturbances
A Medical Approach to Sleep Disorders in School-Aged Children and Adolescents.
 A Medical Approach to Sleep Disorders in School-Aged Children and Adolescents. Akinyemi Ajayi, MD, FAAP, FCCP, D,ABSM, FAASM. Children s Lung, Asthma and Sleep Specialists Children s Sleep Laboratory Sleep
A Medical Approach to Sleep Disorders in School-Aged Children and Adolescents. Akinyemi Ajayi, MD, FAAP, FCCP, D,ABSM, FAASM. Children s Lung, Asthma and Sleep Specialists Children s Sleep Laboratory Sleep
Sleep Medicine Questionnaire
 Please bring this completed questionnaire with you to your sleep medicine appointment. Our sleep medicine staff strives to understand your sleep symptoms, which may be complex in nature. Thank you for
Please bring this completed questionnaire with you to your sleep medicine appointment. Our sleep medicine staff strives to understand your sleep symptoms, which may be complex in nature. Thank you for
Narcolepsy. Jon R. Doud, MD Pulmonary Physician Midwest Center for Sleep Disorders Aurora, IL
 Narcolepsy Jon R. Doud, MD Pulmonary Physician Midwest Center for Sleep Disorders Aurora, IL Narcolepsy A central nervous system disorder that is an important cause of persistent sleepiness. The second
Narcolepsy Jon R. Doud, MD Pulmonary Physician Midwest Center for Sleep Disorders Aurora, IL Narcolepsy A central nervous system disorder that is an important cause of persistent sleepiness. The second
Sleep - Definition. Slide 1 Sleep & Developmental Disabilities: Lessons for All Children. Slide 2 Importance of Sleep. Slide 3. Lawrence W.
 1 Sleep & Developmental Disabilities: Lessons for All Children March 28, 2012 Lawrence W. Brown, MD Pediatric Neuropsychiatry Program Sleep Disorders Center The Children s Hospital of Philadelphia 2 Importance
1 Sleep & Developmental Disabilities: Lessons for All Children March 28, 2012 Lawrence W. Brown, MD Pediatric Neuropsychiatry Program Sleep Disorders Center The Children s Hospital of Philadelphia 2 Importance
Index. baclofen 73 basal forebrain nuclei 174
 Index acetazolamide 33 acetylcholine esterase inhibitor 174 actigraphy 14 activity meter 226 acute insomnia 4 α1 adrenergic activity 88 α 1 containing receptor 211 adenosine 108 advanced sleep phase syndrome
Index acetazolamide 33 acetylcholine esterase inhibitor 174 actigraphy 14 activity meter 226 acute insomnia 4 α1 adrenergic activity 88 α 1 containing receptor 211 adenosine 108 advanced sleep phase syndrome
Chapter Eleven. Sleep and Waking
 Chapter Eleven Sleep and Waking Sleep Are we getting enough. How z it work? Sleep Deprivation contributed to the Exxon Valdez, Challenger Explosion, and 3 Mile Island Deprivation is VERY common, and quite
Chapter Eleven Sleep and Waking Sleep Are we getting enough. How z it work? Sleep Deprivation contributed to the Exxon Valdez, Challenger Explosion, and 3 Mile Island Deprivation is VERY common, and quite
Sleep, Dreaming and Circadian Rhythms
 Sleep, Dreaming and Circadian Rhythms People typically sleep about 8 hours per day, and spend 16 hours awake. Most people sleep over 175,000 hours in their lifetime. The vast amount of time spent sleeping
Sleep, Dreaming and Circadian Rhythms People typically sleep about 8 hours per day, and spend 16 hours awake. Most people sleep over 175,000 hours in their lifetime. The vast amount of time spent sleeping
Healthy Sleep Tips Along the Way!
 Women and Sleep What You Will Learn The Benefits and Importance of Sleep States and Stages of the Sleep Cycle Unique Physiology of Women s Sleep Common Disorders in Women that Affect Sleep Women s Role
Women and Sleep What You Will Learn The Benefits and Importance of Sleep States and Stages of the Sleep Cycle Unique Physiology of Women s Sleep Common Disorders in Women that Affect Sleep Women s Role
Emergency Contact Information Name: Phone: Address: Employer Information Employer Name: Address/Street: City: Zip: Phone: Fax:
 SUNSET SLEEP LABS PATIENT INFORMATION FORM Patient Information Name: Sex: M F Date of Birth: Address/Street: City: Zip: Phone: Alt Phone: Parent/Guardian: Phone: Social Security Number: Drivers License:
SUNSET SLEEP LABS PATIENT INFORMATION FORM Patient Information Name: Sex: M F Date of Birth: Address/Street: City: Zip: Phone: Alt Phone: Parent/Guardian: Phone: Social Security Number: Drivers License:
Diana Corzine, MD ABMS Sleep Chief MT VA Sleep Medicine Common Sleep Disorders
 Diana Corzine, MD ABMS Sleep Chief MT VA Sleep Medicine 2018 Common Sleep Disorders Objectives: Understand Understand how Sleep Disorders affects health. Describe Describe some Common Sleep Disorders.
Diana Corzine, MD ABMS Sleep Chief MT VA Sleep Medicine 2018 Common Sleep Disorders Objectives: Understand Understand how Sleep Disorders affects health. Describe Describe some Common Sleep Disorders.
Sleep History Questionnaire
 Sleep History Questionnaire Name: DOB: Phone: Date of Consultation: Consultation is requested by: Primary care provider: _ Preferred pharmacy: Chief complaint: Please tell us why you are here: How long
Sleep History Questionnaire Name: DOB: Phone: Date of Consultation: Consultation is requested by: Primary care provider: _ Preferred pharmacy: Chief complaint: Please tell us why you are here: How long
Sleep Center. Have you had a previous sleep study? Yes No If so, when and where? Name of facility Address
 Patient Label For office use only Appt date: Clinician: Sleep Center Main Campus Highlands Ranch Location 1400 Jackson Street 8671 S. Quebec St., Ste 120 Denver, CO 80206 Highlands Ranch, CO 80130 Leading
Patient Label For office use only Appt date: Clinician: Sleep Center Main Campus Highlands Ranch Location 1400 Jackson Street 8671 S. Quebec St., Ste 120 Denver, CO 80206 Highlands Ranch, CO 80130 Leading
John McLachlan. Clinical Lead Pulmonary Physiology & Sleep Medicine. President Elect, WA Branch Thoracic Society of Australia & NZ
 John McLachlan Respiratory & Sleep Physician @FSH Clinical Lead Pulmonary Physiology & Sleep Medicine Sleep Physician x 27 years Interest in Insomnia management President Elect, WA Branch Thoracic Society
John McLachlan Respiratory & Sleep Physician @FSH Clinical Lead Pulmonary Physiology & Sleep Medicine Sleep Physician x 27 years Interest in Insomnia management President Elect, WA Branch Thoracic Society
Disorders of Sleep: An Overview 305 Leon Ting and Atul Malhotra
 SLEEP MEDICINE Preface Robert D. Ballard and Teofilo L. Lee-Chiong Jr xiii Disorders of Sleep: An Overview 305 Leon Ting and Atul Malhotra Only recently has the medical profession focused on the importance
SLEEP MEDICINE Preface Robert D. Ballard and Teofilo L. Lee-Chiong Jr xiii Disorders of Sleep: An Overview 305 Leon Ting and Atul Malhotra Only recently has the medical profession focused on the importance
Insomnia. Learning Objectives. Disclosure 6/7/11. Research funding: NIH, Respironics, Embla Consulting: Elsevier
 Insomnia Teofilo Lee-Chiong MD Professor of Medicine National Jewish Health University of Colorado Denver School of Medicine Learning Objectives Learn about the causes of transient and chronic Learn how
Insomnia Teofilo Lee-Chiong MD Professor of Medicine National Jewish Health University of Colorado Denver School of Medicine Learning Objectives Learn about the causes of transient and chronic Learn how
SLEEP HISTORY QUESTIONNAIRE
 Date of birth: Today s date: Dear Patient: SLEEP HISTORY QUESTIONNAIRE Thank you for taking the time to fill out a sleep history questionnaire. This will help our healthcare team to provide the best possible
Date of birth: Today s date: Dear Patient: SLEEP HISTORY QUESTIONNAIRE Thank you for taking the time to fill out a sleep history questionnaire. This will help our healthcare team to provide the best possible
Associated Neurological Specialties and Sleep Disorder Center
 Sleep Center Questionnaire Name: Sex: Age: Date: Date of Birth: Height: Weight: Neck Size: Primary Care Physician: Referring Physician: Main Sleep Issues/Complaints Trouble falling asleep Trouble staying
Sleep Center Questionnaire Name: Sex: Age: Date: Date of Birth: Height: Weight: Neck Size: Primary Care Physician: Referring Physician: Main Sleep Issues/Complaints Trouble falling asleep Trouble staying
Index 265. Feeding bottle, 37 methods, 37
 Index 263 Index A Actigraphy delayed sleep phase syndrome, 66f Activity, 19 Adenoidectomy OSAHS, 121 Adolescents insomnia, 71 81 assessment and treatment, 76 78 etiology, 75, 76 female, 74, 75 sleep need
Index 263 Index A Actigraphy delayed sleep phase syndrome, 66f Activity, 19 Adenoidectomy OSAHS, 121 Adolescents insomnia, 71 81 assessment and treatment, 76 78 etiology, 75, 76 female, 74, 75 sleep need
Overview of Sleep Medicine
 Overview of Sleep Medicine Rodney Smith. New York Times 11-18-2007 James E. Mojica, MD, FAASM Pulmonary, Sleep, Critical Care Massachusetts General Hospital Sleep Reversible state Perceptual disengagement
Overview of Sleep Medicine Rodney Smith. New York Times 11-18-2007 James E. Mojica, MD, FAASM Pulmonary, Sleep, Critical Care Massachusetts General Hospital Sleep Reversible state Perceptual disengagement
Sleep Apnea. Herbert A Berger, MD Pulmonary Division Department of Internal Medicine University of Iowa
 Sleep Apnea Herbert A Berger, MD Pulmonary Division Department of Internal Medicine University of Iowa Disclosures No Relevant Financial Interests to Report Objectives Learn the history and physical examination
Sleep Apnea Herbert A Berger, MD Pulmonary Division Department of Internal Medicine University of Iowa Disclosures No Relevant Financial Interests to Report Objectives Learn the history and physical examination
PATIENT DEMOGRAPHICS
 PATIENT DEMOGRAPHICS NPSG CPAP CPAP Retitration Split Night PATIENT INFORMATION: Name: Last First Middle Initial Address: City: State: Zip: Social Security #: DOB: Gender: Age: Phone Number: Cell: Work:
PATIENT DEMOGRAPHICS NPSG CPAP CPAP Retitration Split Night PATIENT INFORMATION: Name: Last First Middle Initial Address: City: State: Zip: Social Security #: DOB: Gender: Age: Phone Number: Cell: Work:
Sleep Questionnaire Name: Sex: Age: Da te: Da te of birth: Height: Weight: Neck siz e: Ref erring Physician: Primary Car e MD:
 www.myvcmf.com 1133 E. Stanley Blvd., Suite 101 Livermore, CA 94550 925 454-4280 5725 W. Las Positas Blvd., Suite 110 Pleasanton, CA 94588 925-416-6767 Sleep Questionnaire Name: Sex: Age: Da te: Da te
www.myvcmf.com 1133 E. Stanley Blvd., Suite 101 Livermore, CA 94550 925 454-4280 5725 W. Las Positas Blvd., Suite 110 Pleasanton, CA 94588 925-416-6767 Sleep Questionnaire Name: Sex: Age: Da te: Da te
Insomnia. Dr Terri Henderson MBChB FCPsych
 Insomnia Dr Terri Henderson MBChB FCPsych Plan Basics of insomnia Pharmacology Medication CBT Details of insomnia Unsatisfactory sleep that impairs daytime well-being Starts with specific problem or change
Insomnia Dr Terri Henderson MBChB FCPsych Plan Basics of insomnia Pharmacology Medication CBT Details of insomnia Unsatisfactory sleep that impairs daytime well-being Starts with specific problem or change
Participant ID: If you had no responsibilities, what time would your body tell you to go to sleep and wake up?
 What does your sleep look like on a typical week? Total Sleep Time: Bedtime:, Sleep onset latency:, Number of Awakenings:, Wake time after sleep onset:, Rise time:, Out of bed:, Naps:? Notes: Is your sleep
What does your sleep look like on a typical week? Total Sleep Time: Bedtime:, Sleep onset latency:, Number of Awakenings:, Wake time after sleep onset:, Rise time:, Out of bed:, Naps:? Notes: Is your sleep
Sleep and the Heart Reversing the Effects of Sleep Apnea to Better Manage Heart Disease
 1 Sleep and the Heart Reversing the Effects of Sleep Apnea to Better Manage Heart Disease Rami Khayat, MD Professor of Internal Medicine Director, OSU Sleep Heart Program Medical Director, Department of
1 Sleep and the Heart Reversing the Effects of Sleep Apnea to Better Manage Heart Disease Rami Khayat, MD Professor of Internal Medicine Director, OSU Sleep Heart Program Medical Director, Department of
Modern Management of Sleep Disorders
 Modern Management of Sleep Disorders Douglas C. Bauer, MD University of California, San Francisco No Disclosures Case 68 yr. old WF with >15 yr. of poor sleep Difficulty with both initiation and maintenance
Modern Management of Sleep Disorders Douglas C. Bauer, MD University of California, San Francisco No Disclosures Case 68 yr. old WF with >15 yr. of poor sleep Difficulty with both initiation and maintenance
Home Sleep Testing Questionnaire
 Home Sleep Testing Questionnaire Patient Name: DOB: / / Gender: Male Female Study Date: / / Marital Status: Married Cohabitate Single Divorced Widow/Widower Email: Phone: Height: Weight: Neck Size: What
Home Sleep Testing Questionnaire Patient Name: DOB: / / Gender: Male Female Study Date: / / Marital Status: Married Cohabitate Single Divorced Widow/Widower Email: Phone: Height: Weight: Neck Size: What
14. Percent Mellinger GD et al. Arch Gen Psychiatry. 1985;42: ICSD III
 4:45 5:45 pm Management of Insomnia and Other Disorders Presenter Disclosure Information The following relationships exist related to this presentation: Alon Y. Avidan, MD, MPH, FAAN, FAASM: Speakers Bureau
4:45 5:45 pm Management of Insomnia and Other Disorders Presenter Disclosure Information The following relationships exist related to this presentation: Alon Y. Avidan, MD, MPH, FAAN, FAASM: Speakers Bureau
Beyond Sleep Apnoea. Dr Justin Pepperell DA SODIT 2017
 Beyond Sleep Apnoea Dr Justin Pepperell DA SODIT 2017 disclosures Introduction Sleep and its disorders Obstructive sleep apnea Other common sleep disorders Critical illness sleep disorders Bonus BIS monitoring
Beyond Sleep Apnoea Dr Justin Pepperell DA SODIT 2017 disclosures Introduction Sleep and its disorders Obstructive sleep apnea Other common sleep disorders Critical illness sleep disorders Bonus BIS monitoring
Sleep Disorders. Sleep. Circadian Rhythms
 Sleep Disorders Sleep The Sleep Wakefulness Cycle: Circadian Rhythms Internally generated patterns of bodily functions that vary over a ~24-hour period Function even in the absence of normal cues 2 Circadian
Sleep Disorders Sleep The Sleep Wakefulness Cycle: Circadian Rhythms Internally generated patterns of bodily functions that vary over a ~24-hour period Function even in the absence of normal cues 2 Circadian
New Patient Sleep Intake
 New Patient Sleep Intake Name: Date of Birth: Primary Care Physician: Date of Visit: Referring Physician and/or Other Physicians: Retail Pharmacy: Mail Order Pharmacy: Address: Mail Order Phone #: Phone
New Patient Sleep Intake Name: Date of Birth: Primary Care Physician: Date of Visit: Referring Physician and/or Other Physicians: Retail Pharmacy: Mail Order Pharmacy: Address: Mail Order Phone #: Phone
Sleep Dysfunction in Multiple System Atrophy DR CALLUM DUPRE NEUROLOGY/SLEEP MEDICINE CAPITAL HEALTH SYSTEM
 Sleep Dysfunction in Multiple System Atrophy DR CALLUM DUPRE NEUROLOGY/SLEEP MEDICINE CAPITAL HEALTH SYSTEM Categories of Disturbance Sleep Breathing Disorders Parasomnias Sleepiness Insomnia Breathing?
Sleep Dysfunction in Multiple System Atrophy DR CALLUM DUPRE NEUROLOGY/SLEEP MEDICINE CAPITAL HEALTH SYSTEM Categories of Disturbance Sleep Breathing Disorders Parasomnias Sleepiness Insomnia Breathing?
WELCOME TO THE NORTHSHORE UNIVERSITY HEALTHSYSTEM SLEEP CENTERS
 WELCOME TO THE NORTHSHORE UNIVERSITY HEALTHSYSTEM SLEEP CENTERS Prior to your office visit, we request that you complete this questionnaire. It asks questions not only about your sleeping habits and behavior
WELCOME TO THE NORTHSHORE UNIVERSITY HEALTHSYSTEM SLEEP CENTERS Prior to your office visit, we request that you complete this questionnaire. It asks questions not only about your sleeping habits and behavior
SLEEP APNEA IN THE ELDERLY SLEEP THAT KNITS UP THE RAVELED SLEEVE OF CARE
 SLEEP APNEA IN THE ELDERLY SLEEP THAT KNITS UP THE RAVELED SLEEVE OF CARE OBJECTIVES 1. TO DESCRIBE THE NORMAL AGE RELATED CHANGES TO SLEEP 2. TO DESCRIBE THE SPECTRUM OF SLEEP-DISORDERED BREATHING. 3.
SLEEP APNEA IN THE ELDERLY SLEEP THAT KNITS UP THE RAVELED SLEEVE OF CARE OBJECTIVES 1. TO DESCRIBE THE NORMAL AGE RELATED CHANGES TO SLEEP 2. TO DESCRIBE THE SPECTRUM OF SLEEP-DISORDERED BREATHING. 3.
Sleep Disorders in Adolescents and Young Adults
 Sleep Disorders in Adolescents and Young Adults Deborah Layden 9/9/2014 Arousal MT Wake REM S1 S2 S3 S4 00:00 01:00 02:00 03:00 04:00 05:00 Button Supine Left Prone Right Upright SpO2 [%] Desat 100 90
Sleep Disorders in Adolescents and Young Adults Deborah Layden 9/9/2014 Arousal MT Wake REM S1 S2 S3 S4 00:00 01:00 02:00 03:00 04:00 05:00 Button Supine Left Prone Right Upright SpO2 [%] Desat 100 90
AGING CHANGES IN SLEEP
 OBJECTIVES: Understand the common age-related changes in sleep Discuss the evaluation of the older person with sleep complaints Identify sleep apnea, PLMS, RLS, and REM sleep disorders and their treatments
OBJECTIVES: Understand the common age-related changes in sleep Discuss the evaluation of the older person with sleep complaints Identify sleep apnea, PLMS, RLS, and REM sleep disorders and their treatments
FEP Medical Policy Manual
 FEP Medical Policy Manual Effective Date: October 15, 2018 Related Policies: 2.01.18 Diagnosis and Medical Management of Obstructive Sleep Apnea Syndrome Polysomnography for Non-Respiratory Sleep Disorders
FEP Medical Policy Manual Effective Date: October 15, 2018 Related Policies: 2.01.18 Diagnosis and Medical Management of Obstructive Sleep Apnea Syndrome Polysomnography for Non-Respiratory Sleep Disorders
Sleep Disorders. Anneka Rose ST5 Psychiatrist
 Sleep Disorders Anneka Rose ST5 Psychiatrist Agenda Basic overview of sleep structure Interactive case based discussions 5 min interventions MCQs Questions Hypnogram Actigraphy Common Scenario Patient
Sleep Disorders Anneka Rose ST5 Psychiatrist Agenda Basic overview of sleep structure Interactive case based discussions 5 min interventions MCQs Questions Hypnogram Actigraphy Common Scenario Patient
SLEEP APNOEA DR TAN KAH LEONG ALVIN CO-DIRECTOR SLEEP LABORATORY SITE CHIEF SDDC (SLEEP) DEPARTMENT OF OTORHINOLARYNGOLOGY, HEAD & NECK SURGERY
 DEPARTMENT OF OTORHINOLARYNGOLOGY, HEAD & NECK SURGERY") SLEEP APNOEA DR TAN KAH LEONG ALVIN CO-DIRECTOR SLEEP LABORATORY SITE CHIEF SDDC (SLEEP) DEPARTMENT OF OTORHINOLARYNGOLOGY, HEAD & NECK SURGERY
SLEEP APNOEA DR TAN KAH LEONG ALVIN CO-DIRECTOR SLEEP LABORATORY SITE CHIEF SDDC (SLEEP) DEPARTMENT OF OTORHINOLARYNGOLOGY, HEAD & NECK SURGERY
Are you skimping on sleep, or could you have a sleep disorder?
 Are you skimping on sleep, or could you have a sleep disorder? Look around you: the guy nodding off on the bus, the co-worker snoozing during a dull presentation, the people with heavy eyelids lined up
Are you skimping on sleep, or could you have a sleep disorder? Look around you: the guy nodding off on the bus, the co-worker snoozing during a dull presentation, the people with heavy eyelids lined up
For more than 25 million Americans, including surgical technologists, who have nontraditional
 RICHARD EVANS WILLS, MD, MA, FACSM JAMES A WOODMANSEE, MD MICHAEL NORTON, DC For more than 25 million Americans, including surgical technologists, who have nontraditional work schedules, sleep deprivation
RICHARD EVANS WILLS, MD, MA, FACSM JAMES A WOODMANSEE, MD MICHAEL NORTON, DC For more than 25 million Americans, including surgical technologists, who have nontraditional work schedules, sleep deprivation
Marieb, E.N. (2004), Human Anatomy & Physiology, Pearson Education, Inc, San Francisco, CA, USA, p459
, Human Anatomy & Physiology, Pearson Education, Inc, San Francisco, CA, USA, p459") Neuroscience Tutorial: Sleep and Dreams Discuss the following diagram with the students: Marieb, E.N. (2004), Human Anatomy & Physiology, Pearson Education, Inc, San Francisco, CA, USA, p459 1 Purves,
Neuroscience Tutorial: Sleep and Dreams Discuss the following diagram with the students: Marieb, E.N. (2004), Human Anatomy & Physiology, Pearson Education, Inc, San Francisco, CA, USA, p459 1 Purves,
Modern Management of Sleep Disorders. If Only I Could Sleep Like I Did Before
 Modern Management of Sleep Disorders Douglas C. Bauer, MD University of California, San Francisco No Disclosures If Only I Could Sleep Like I Did Before Sleep Case 52 yr. old WF with >4 yr. of poor sleep
Modern Management of Sleep Disorders Douglas C. Bauer, MD University of California, San Francisco No Disclosures If Only I Could Sleep Like I Did Before Sleep Case 52 yr. old WF with >4 yr. of poor sleep
INSOMNIA IN GERIATRICS. Presented By: Sara Kamalfar MD, Geriatrics Medicine Fellow
 INSOMNIA IN GERIATRICS Presented By: Sara Kamalfar MD, Geriatrics Medicine Fellow Insomnia Insomnia is the inability to fall asleep, the inability to stay asleep, or waking up earlier than desired. To
INSOMNIA IN GERIATRICS Presented By: Sara Kamalfar MD, Geriatrics Medicine Fellow Insomnia Insomnia is the inability to fall asleep, the inability to stay asleep, or waking up earlier than desired. To
Modern Management of Sleep Disorders. Case. Introduction. Topics Covered. Douglas C. Bauer, MD University of California, San Francisco
 Modern Management of Sleep Disorders Douglas C. Bauer, MD University of California, San Francisco No Disclosures Case 68 yr. old WF with >15 yr. of poor sleep Difficulty with both initiation and maintenance
Modern Management of Sleep Disorders Douglas C. Bauer, MD University of California, San Francisco No Disclosures Case 68 yr. old WF with >15 yr. of poor sleep Difficulty with both initiation and maintenance
Sleep: A Forgotten Component of Overall Health Demarcus Sneed Health and Human Sciences Educator Madison County October 5, 2016
 Sleep: A Forgotten Component of Overall Health Demarcus Sneed Health and Human Sciences Educator Madison County October 5, 2016 Lesson Objectives Understand the importance of having consistent, quality
Sleep: A Forgotten Component of Overall Health Demarcus Sneed Health and Human Sciences Educator Madison County October 5, 2016 Lesson Objectives Understand the importance of having consistent, quality
Sleep and a Healthy Heart
 Sleep and a Healthy Heart Dr. R. John Kimoff, MD, FRCP(C) Professor of Medicine, Respiratory Division Director, Sleep Laboratory, MCI-McGill University Health Centre Montréal, Québec, Canada Women s Healthy
Sleep and a Healthy Heart Dr. R. John Kimoff, MD, FRCP(C) Professor of Medicine, Respiratory Division Director, Sleep Laboratory, MCI-McGill University Health Centre Montréal, Québec, Canada Women s Healthy
MLA HASS LUNG. SLEEP CENTER, Leominster Campus 100 Erdman Way, Leomjnster, MA Phone: Fax:
 MLA HASS LUNG SLEEP CENTER, Leominster Campus 100 Erdman Way, Leomjnster, MA 01453 Phone: 978-728-4641 Fax: 978-978-1382 MEICAL IRECTOR: Payam Aghassi, M, FCCP Thank you for your sleep study order! Attached
MLA HASS LUNG SLEEP CENTER, Leominster Campus 100 Erdman Way, Leomjnster, MA 01453 Phone: 978-728-4641 Fax: 978-978-1382 MEICAL IRECTOR: Payam Aghassi, M, FCCP Thank you for your sleep study order! Attached
Overview. Surviving shift work. What is the circadian rhythm? Components of a Generic Biological Timing System 31/10/2017
 Overview Surviving shift work Dr Claire M. Ellender Respiratory and Sleep Physician Princess Alexandra Hospital Conflicts nil relevant Circadian rhythm Impacts of shift work on health Case example Circadian
Overview Surviving shift work Dr Claire M. Ellender Respiratory and Sleep Physician Princess Alexandra Hospital Conflicts nil relevant Circadian rhythm Impacts of shift work on health Case example Circadian
Article printed from
 What Are Sleep Disorders? Sleep disorders are conditions that affect how much and how well you sleep. The causes range from poor habits that keep you awake to medical problems that disrupt your sleep cycle.
What Are Sleep Disorders? Sleep disorders are conditions that affect how much and how well you sleep. The causes range from poor habits that keep you awake to medical problems that disrupt your sleep cycle.
Sleep and Parkinson's Disease
 Parkinson s Disease Clinic and Research Center University of California, San Francisco 505 Parnassus Ave., Rm. 795-M, Box 0114 San Francisco, CA 94143-0114 (415) 476-9276 http://pdcenter.neurology.ucsf.edu
Parkinson s Disease Clinic and Research Center University of California, San Francisco 505 Parnassus Ave., Rm. 795-M, Box 0114 San Francisco, CA 94143-0114 (415) 476-9276 http://pdcenter.neurology.ucsf.edu
EEG Electrode Placement
 EEG Electrode Placement Classifying EEG brain waves Frequency: the number of oscillations/waves per second, measured in Hertz (Hz) reflects the firing rate of neurons alpha, beta, theta, delta Amplitude:
EEG Electrode Placement Classifying EEG brain waves Frequency: the number of oscillations/waves per second, measured in Hertz (Hz) reflects the firing rate of neurons alpha, beta, theta, delta Amplitude:
Occupation: Usual Work Hours/Days: Referring Physician: Family Physician (PCP): Marital status: Single Married Divorced Widowed
: Marital status: Single Married Divorced Widowed") Name Social Security No. Last First MI Address Phone No. ( ) City State Zip Secondary No. ( ) Date of Birth Sex (M/F) Race Email County Primary Care Marital Status Single Divorced Married Widowed Employer
Name Social Security No. Last First MI Address Phone No. ( ) City State Zip Secondary No. ( ) Date of Birth Sex (M/F) Race Email County Primary Care Marital Status Single Divorced Married Widowed Employer
1960 FP CENTER FOR SLEEP DISORDERS
 1960 FP CENTER FOR SLEEP DISORDERS Sleep Questionnaire Name: Date: Date of Birth: / / Age: Gender: Height: Weight: lbs. Referring Physician: Occupation: Please give a brief description of your sleep problem
1960 FP CENTER FOR SLEEP DISORDERS Sleep Questionnaire Name: Date: Date of Birth: / / Age: Gender: Height: Weight: lbs. Referring Physician: Occupation: Please give a brief description of your sleep problem
FEP Medical Policy Manual
 FEP Medical Policy Manual Effective Date: January 15, 2018 Related Policies: 2.01.18 Diagnosis and Medical Management of Obstructive Sleep Apnea Syndrome Diagnosis and Medical Management of Obstructive
FEP Medical Policy Manual Effective Date: January 15, 2018 Related Policies: 2.01.18 Diagnosis and Medical Management of Obstructive Sleep Apnea Syndrome Diagnosis and Medical Management of Obstructive
1/28/2015 EVALUATION OF SLEEP THROUGH SCALES AND LABORATORY TOOLS. Marco Zucconi
 EVALUATION OF SLEEP THROUGH SCALES AND LABORATORY TOOLS Marco Zucconi Sleep Disorders Centre, Dept of Clinical Neurosciences, San Raffaele Hospital, Milan, Italy INDAGINI STRUMENTALI DEL CICLO SONNO-VEGLIA
EVALUATION OF SLEEP THROUGH SCALES AND LABORATORY TOOLS Marco Zucconi Sleep Disorders Centre, Dept of Clinical Neurosciences, San Raffaele Hospital, Milan, Italy INDAGINI STRUMENTALI DEL CICLO SONNO-VEGLIA
Sleep History Questionnaire B/P / Pulse: Neck Circum Wgt: Pulse Ox
 2700 Campus Drive, Ste 100 2412 E 117 th Street Plymouth, MN 55441 Burnsville, MN 55337 P 763.519.0634 F 763.519.0636 P 952.431.5011 F 952.431.5013 www.whitneysleepcenter.com Sleep History Questionnaire
2700 Campus Drive, Ste 100 2412 E 117 th Street Plymouth, MN 55441 Burnsville, MN 55337 P 763.519.0634 F 763.519.0636 P 952.431.5011 F 952.431.5013 www.whitneysleepcenter.com Sleep History Questionnaire
Parkinson s Founda.on
 Parkinson s Founda.on PD ExpertBriefing: Sleep and Parkinson s Led By: Aleksandar Videnovic, M.D., M.Sc. Associate Professor of Neurology; Director, MGH Program on Sleep, Circadian Biology and NeurodegeneraDon
Parkinson s Founda.on PD ExpertBriefing: Sleep and Parkinson s Led By: Aleksandar Videnovic, M.D., M.Sc. Associate Professor of Neurology; Director, MGH Program on Sleep, Circadian Biology and NeurodegeneraDon
14. Percent
 4:30 5:45 pm Management of Insomnia and Other Disorders Presenter Disclosure Information The following relationships exist related to this presentation: Alon Y. Avidan, MD, MPH, FAAN, FAASM: Speakers Bureau
4:30 5:45 pm Management of Insomnia and Other Disorders Presenter Disclosure Information The following relationships exist related to this presentation: Alon Y. Avidan, MD, MPH, FAAN, FAASM: Speakers Bureau
Patient Adult Information History
 Patient Adult Information History Patient name: Age: Date: What is the main reason for today s evaluation? Infant History Birth delivery: Normal C-section Delayed Epidural Premature: No Yes If yes, how
Patient Adult Information History Patient name: Age: Date: What is the main reason for today s evaluation? Infant History Birth delivery: Normal C-section Delayed Epidural Premature: No Yes If yes, how
SLEEP UPDATE 2008 SLEEP HYPNOGRAM. David Claman, MD UCSF Sleep Disorders Center
 SLEEP UPDATE 2008 SLEEP HYPNOGRAM David Claman, MD UCSF Sleep Disorders Center Insomnia Case A 40 year old man c/o insomnia at sleep onset. He worries about sleep at night, and takes 2-3 hrs to fall asleep.
SLEEP UPDATE 2008 SLEEP HYPNOGRAM David Claman, MD UCSF Sleep Disorders Center Insomnia Case A 40 year old man c/o insomnia at sleep onset. He worries about sleep at night, and takes 2-3 hrs to fall asleep.
Symptoms of Narcolepsy
 Symptoms of Narcolepsy v Sleep attacks Brief episodes of sleep that occur many times a day May occur without warning or be preceded by drowsiness Patient usually feels refreshed afterwards Refractory period
Symptoms of Narcolepsy v Sleep attacks Brief episodes of sleep that occur many times a day May occur without warning or be preceded by drowsiness Patient usually feels refreshed afterwards Refractory period
Disclosures. Speaker: Teva, UCB, Purdue Advisory Board: Welltrinsic Sleep Network Consultant: Vapotherm, Inc. National Interpretor: Novasom
 So PAP Doesn t Work Rochelle Goldberg, MD, FAASM, FCCP Diplomat, American Board of Sleep Medicine Director Sleep Medicine Services Main Line Health Systems Lankenau Medical Center and Paoli Hospital Disclosures
So PAP Doesn t Work Rochelle Goldberg, MD, FAASM, FCCP Diplomat, American Board of Sleep Medicine Director Sleep Medicine Services Main Line Health Systems Lankenau Medical Center and Paoli Hospital Disclosures
Original Sleep Hygiene Rules*
 Original Sleep Hygiene Rules* 1. Sleep as much as needed to feel refreshed and healthy during the following day, but not more. Curtailing time in bed a bit seems to solidify sleep; excessively long times
Original Sleep Hygiene Rules* 1. Sleep as much as needed to feel refreshed and healthy during the following day, but not more. Curtailing time in bed a bit seems to solidify sleep; excessively long times
PHARMACOLOGY OF SLEEP
 NAMS REGIONAL SYMPOSIUM ON SLEEP MEDICINE PHARMACOLOGY OF SLEEP DR. K.K. SHARMA Department of Pharmacology School of Medical Sciences & Research (SMSR) Sharda University, Greater Noida- 201306. 1 Introduction
NAMS REGIONAL SYMPOSIUM ON SLEEP MEDICINE PHARMACOLOGY OF SLEEP DR. K.K. SHARMA Department of Pharmacology School of Medical Sciences & Research (SMSR) Sharda University, Greater Noida- 201306. 1 Introduction
Chapter 5. Variations in Consciousness 8 th Edition
 Chapter 5 Variations in Consciousness 8 th Edition Consciousness: Personal Awareness Awareness of Internal and External Stimuli Levels of awareness James stream of consciousness Freud unconscious Sleep/dreaming
Chapter 5 Variations in Consciousness 8 th Edition Consciousness: Personal Awareness Awareness of Internal and External Stimuli Levels of awareness James stream of consciousness Freud unconscious Sleep/dreaming
Balboa Island Dentistry (949)
") Do You Snore? Are you always tired? Snoring is no laughing matter! It may be more than an annoying habit. It may be a sign of. How well do you sleep? Just about everyone snores occasionally. Even a baby
Do You Snore? Are you always tired? Snoring is no laughing matter! It may be more than an annoying habit. It may be a sign of. How well do you sleep? Just about everyone snores occasionally. Even a baby