Delving into Deprescription. Todd C. Lee MD MPH FRCPC Associate Professor of Medicine, McGill University With thanks to Dr. Emily G.
|
|
|
- Sheryl Underwood
- 5 years ago
- Views:
Transcription

1 Delving into Deprescription Todd C. Lee MD MPH FRCPC Associate Professor of Medicine, McGill University With thanks to Dr. Emily G. McDonald

2 Conflict of interest slide I don t think I have any conflicts of interest to declare But I have a software product in development to help physicians/patients deprescribe Sometimes I worry that pharma will take a contract out on me for my crusade for stopping medications (that s more of a confession)
3 Objectives Introduce the concept of deprescription and why it is important for your patients and for Canadians as a whole. Define the concepts of therapeutic and deprescribing cascades Provide an overview of the evidence in support of efforts to stop unnecessary or potentially harmful medications and point out specifically good examples of common drugs which would be appropriate to deprescribe. Give you resources you can turn to help you tackle these issues with your patients -- and, though it won't be an infomercial, perhaps empower you to set out to make this a regular part of your practice.
4 Polypharmacy: definition Five or more medications (40% of elderly) New terms on the horizon: extreme polypharmacy, mega-polypharmacy, polypharmacy+++ (I ve seen the residents write this in their admission note and it makes me so proud) 50% of our admitted elderly patients take 10 or more medications There are 10% of our patients on the ward who have more than 20 medications prescribed
 BEERS criteria, STOPP")
5 What s the problem with too many pills? Many medications are: Potentially inappropriate (NEW TERM: PIMs or potentially inappropriate medications are those which have a high probability of risk exceeding benefit) BEERS criteria, STOPP criteria, Choosing Wisely lists Continued beyond their original indication (a classic example is aspirin and clopidogrel continued together beyond 12 months following a stent or an acute coronary syndrome) Associated with harm in the form of Adverse Drug Events (ADEs) Estimate 27,000 ER visits in Canada per year due to ADE
6 What s the problem with too many pills? Complex interactions We know the simple ones of Drug A with B; but what about 10 in combination? Complex side effects We know the side effects of Drug A or Drug B; but what about 10 in combination? Therapeutic cascades Difficulty prioritizing the important pills Adherence
7 Therapeutic Cascades When a drug is given to manage/treat the side effect of another drug Give me some examples!
8 Therapeutic Cascades When a drug is given to manage/treat the side effect of another drug Furosemide for calcium channel blocker induced edema Magnesium for proton pump inhibitor related hypomagnesemia Laxatives for iron associated constipation Beta-blockers for beta-agonist induced palpitations Nystatin for inhaled steroid induced thrush Codeine for ACE inhibitor cough --- I m not joking I ve seen it!

9

10 Low value medications cost big bucks This says NOTHING about medications not on STOPP/BEERS which may also be inappropriate or low value
11 Defining deprescribing It is another relatively new term that first enters the research realm at most 5 years ago but certainly has been done It is the process of regular reassessment of medications for the purposes of discontinuing medications which are no longer considered necessary or are of low benefit compared to risk
12 Deprescribing It enters into the medical lexicon around Deprescribing has a wikipedia entry but it was not one of the 500 new words that were entered into the Oxford English Dictionary in 2016 (which included Oompa Loompa and Scrumdiddlyumptious) All this to say that children won t be asked to spell deprescribing at next year s spelling bee.
13 How would one consider deprescribing Low hanging fruit (PIMs) Higher hanging fruit (low benefit medications) Highest hanging fruit (medications which are no longer needed but once were)

14 PIMs Information on PIMs is expert-derived, freely available, widely publicized, and taught in medical school, medical residencies, and geriatrics/internal medicine training programs. BEERS criteria 2015, STOPP criteria, Choosing Wisely Canada There are many doctors who have a great command of this literature and who practice accordingly. There are others who know some of the basics but may forget some of the more complex or newer recommendations.
15 PIMs The care of the patient is highly dependent on being paired with a doctor who is more or less active in this area. Consider: Dr. B may frequently discuss with their patients stopping sedative-hypnotics to reduce the risk of falls. The patient chooses to continue them. Dr. A does not do this and continues the medications without reconsidering them. The patient has a hip fracture due to sedative-hypnotics
16 PIMs How to systematically address Interventions are needed that bring the overall level of knowledge on the issues of PIMs in the elderly to a more standardized level, to facilitate thinking about these issues through for example: computerized support evidence based solutions for helping patients stop these medications While we wait for many of these tools to be developed and deployed, we can still apply the concepts
17 Barbara Farrell- deprescribing research In 2013 Dr. Barbara Farrell (pharmd and assistant professor in the faculty of family medicine at the University of Ottawa) received a $ grant from the Ontario Ministry of Health and Long-term care to develop, implement and evaluate guidelines for deprescribing medications in primary and long-term care facilities CMAJ published a piece describing the goals of the grant Identified several classes of medications based on a modified Delphi approach
 What Are Priorities for Deprescribing for Elderly Patients? Capturing the Voice of Practitioners: A Modified Delphi Process. PLoS ONE 10(4): e0122246. doi:10.1371/journal.pone.")
18 Table 2. Round One Ranking: Drug/drug classes identified by 70% of participants as probably or definitely useful. Farrell B, Tsang C, Raman-Wilms L, Irving H, Conklin J, et al. (2015) What Are Priorities for Deprescribing for Elderly Patients? Capturing the Voice of Practitioners: A Modified Delphi Process. PLoS ONE 10(4): e doi: /journal.pone
19


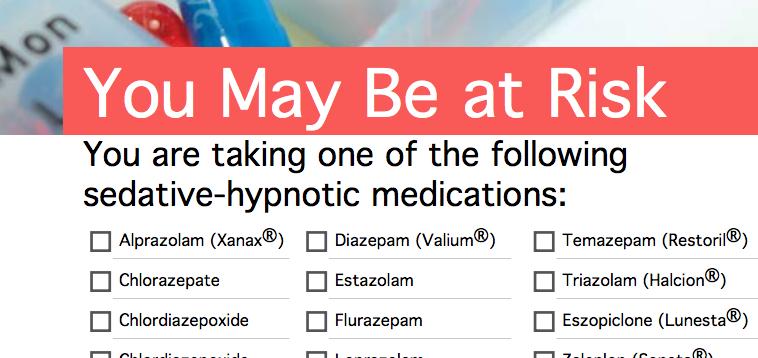
20 The number needed to treat with a sedative-hypnotic for improved sleep is 13. The average improvement in sleep is 8 minutes of latency and 14 minutes more sleep Number needed to harm is 6. Use of benzodiazepines should be reserved for alcohol withdrawal symptoms/delirium tremens or severe generalized anxiety disorder unresponsive to other therapies. Prescribing or discontinuing sedative-hypnotics in hospital can have substantial impact on long-term use.
21 Harms of inpatient benzodiazepines and Z- drugs Falls in hospital Hip fracture Cognitive impairment on MMSE/MOCA Length of stay increased Death Particular risk of death in CHF and COPD patients
22 Hospitalization confers increased risk of new outpatient benzodiazepine in elderly (OR) 3.09; 95% CI, Benzodiazepines prescribed to (3.1%) patients within 7 days of discharge Nearly half of these became new chronic benzodiazepine users.
23 So what s the problem then? Lets just stop some drugs! WELL there are several Physicians hesitate to bring up the topic of deprescribing as it may make their patients uncomfortable by implying reduced life expectancy Stopping medications is a complicated process REF: Schuling BMC Fam Pract 2012
24 Barriers Addressing polypharmacy requires some knowledge of the barriers and challenges of deprescribing Up until recent years the concept of less is more as it applies to medications (and indeed most realms of medicine) has been relatively unfamiliar to patients, pharmacists and clinicians.
25 Barriers Prescriber barriers: The medication is prescribed by another physician (missing information) There is no evidence to guide deprescribing Ageism (an ADE is thought to represent a normal symptom of aging) eg. decreased appetite or energy, falling down, agitation or alterations in sleep Pressure to prescribe according to guidelines Concern that rocking the boat will cause a problem Limited knowledge of how to stop Time
26 Barriers-consumer Patient/family barriers: Feeling of abandonment Medications represent hope Fear of rocking boat
27 Guidance from hit lists Lists of potentially inappropriate medications exist (Beers criteria and the STOP/START criteria; Choosing Wisely Canada) The first two do not give guidance on how to implement the process they merely list drugs Applications online ex. MedStopper.com give tapering instructions but do not link stopping medications with patient s underlying conditions (addresses the issue of lack of knowledge of how to stop or fear of side effects)

28
29
30 Addressing chronic medications What is the patient s prognosis? What was the INITIAL intention of the therapy? Is it being achieved? Is it still reasonable to attempt to achieve? What is the time until realizing benefits (or harms)?
31 Example Donepezil to slow progression of mild Alzheimer s in a patient living in the community autonomously or semi-autonomously vs. Donepezil which has not been stopped in a patient residing in a nursing home with advanced dementia and limited life expectancy What are the harms? (Cardiac conduction. Anorexia and weight loss. Diarrhea, nausea, vomiting. Worsening of BPH symptom.) REF: Tija Clinics in Geriatric Medicine 2012
32 Framework The medical indication The patient s preference Quality of life Contextual issues
33 A deprescribing protocol (1) ascertain all drugs the patient is currently taking and the reasons for each one (2) consider overall risk of drug-induced harm in individual patients in determining the required intensity of deprescribing intervention REF: Scott JAMA int med 2015
34 A deprescribing protocol (3) assess each drug in regard to its current or future benefit potential compared with current or future harm or burden potential; (4) prioritize drugs for discontinuation that have the lowest benefit-harm ratio and lowest likelihood of adverse withdrawal reactions or disease rebound syndromes; and (5) implement a discontinuation regimen and monitor patients closely for improvement in outcomes or onset of adverse effects.
35 Has the medication already caused harm? Patients admitted to hospital with opioid overdose often leave the hospital on.
36 Similar considerations: What is the current indication for the drug? Is the patient actually taking the drug? Does the drug fit with the patient s circumstances? Does the likely benefit of the drug outweigh the potential harms?
37 Put the drug into one of two categories Disease or symptom control drug à controlling active disease or symptoms (anti-anginals, levothyroxine, heart failure medication etc ) Stopping these drugs may result in uncontrolled symptoms Preventive drug (statin, warfarin, bisphosphonates etc...) Stopping these drugs requires considering the absolute risks and benefits
38 Strategies Empower the patient Choosing wisely Canada what are the treatment options for my condition? What are the possible benefits and harms of each drug? What are reasonable grounds for discontinuing a medication?
39 Strategies Care provider should ask if any new symptoms at each visit Any problems taking your medications? Prediction tools and evidence tables if they exist Decision aids that estimate absolute risk of disease
40 CASES
41 Case 1 65 year old man admitted for weakness PMH: TIA in 2005 Atrial fibrillation since 2013 Diabetes Hypertension Meds: ASA Coumadin Omeprazole Sotalol Ramipril Pravastatin Hydrochlorothiazide Metformin Magnesium
42 Case 1 O/E: 140/80 HR 90 irregularly irregular, afebrile JVP ASA; no murmurs or extra sounds No edema Chest clear 4/5 power Brisk reflexes with clonus Positive Chvostek and Trousseau signs
43 LABS: Hemoglobin 135/WBC 9.5/Plt 340 AST/ALT normal A1c 9.5% TSH normal Na 135/ K+ 3.2/ Creatinine Normal Calcium total 1.6 Magnesium 0.15 CXR Normal ECG: Atrial fibrillation with adequate rate control and no ST-T changes PR 160 QRS 90 QTc 490
44 Introducing a counter-concept: The Deprescribing Cascade PRESCRIBING CASCADE Adding medications to deal with the side effects of other medications DEPRESCRIBING CASCADE Removing medications which are no longer necessary, which allows the removal of medications given to prevent/treat side effects of other medications
45 Taking the Ascent ASA and Coumadin together the ASA was for a remote TIA and the Coumadin for his atrial fibrillation. There is, in this patient, no compelling indication for both Markedly increases his risk of bleeding without significant benefit How common is this at MUHC: 40-50% (McDonald et.al,under review) If you stop the ASA, the indication for the proton pump inhibitor is no longer present (ASA + coumadin) and therefore without a history of complicated GI bleed the omeprazole can safely be stopped This is a good thing because it was likely the cause of the metabolic problem and we can also stop the magnesium soon
46 Can we cascade further? He is in atrial fibrillation (rate controlled) Why then is he still on sotalol for rhythm control (which has clearly failed) instead of a rate control agent? AFFIRM trial, RACE trial Sotolol HR 1.6 for death Am J Cardiol Sep 1;114(5): Sotolol + hypomagnesemia + hypokalemia = torsades de pointes Can thus change to alternative rate control agent (i.e. diltiazem, bisoprolol)
47 Net Result Adverse drug event recognized and offending medication stopped Potential ADE averted 3 fewer medications per day (a 33% reduction!)
48 Case of an adverse drug event 76 year old man who presents to the ER with a dizziness and an episode of syncope after passing bright red blood per rectum His hemoglobin is found to 45 g/l He has acute kidney injury with a creatinine of 200
49 Medications include: Metformin 850 mg po BI Nifedipine ER 60 mg po daily Quinine 200 mg po daily ISMN 60 mg po daily Asa 80 mg po daily Tamsulosin 0.4 mg po daily Simvastatin 40 mg po daily Pantoprazole 40 mg po daily Canagliflozin 300 po daily Amlodipine 2.5 mg po daily Azithromycine 250 mg po daily x 5 days Furosemide 80 mg po BID Clopidogrel 75 mg po daily Dutasteride 0.5 mg po daily
50 Additional information? Regarding metformin and canagliflozin Hemoglobin a1c History of hypoglycemia? Risks with canagliflozin? AKI, euglycemic DKA, genitourinary infections
51 Additional information Aspirin and clopidogrel Indication? Timing? DES in the right coronary artery 5 years ago (new risk calculators àdapt score calculator) REF: Mauri et al NEJM 2014 and Yeh et al JAMA 2016

52


53
54 Never drugs? They exist in my world Some examples: Quinine (only 2 health canada advisories saying please stop using) Colace (it doesn t work, sorry) Meperidine and Codeine (seizures and unpredictable pharmacokinetics) Chloral hydrate (it was cool back in Victorian England)
55 Deprescribing cascade Had his clopidogrel been stopped the pantoprazole could have been stopped Other examples include patients who are on magnesium supplements and a proton pump inhibitor

56 ISMN Other drugs to consider stopping
57 ISMN Other drugs to consider stopping
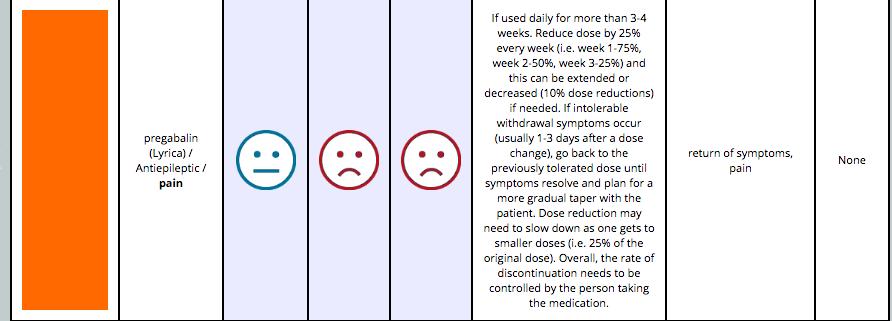
58 Final remarks before we conclude Don t forget that some drugs need to be tapered before stopping them Some because of rebound symptoms Some because of adverse effects from stopping the drug which could prove dangerous Some because a tapering regiment may improve your chances of the drug not being restarted (classic example is sleeping pills; less thought of example is PPIs).
59 For excellent patient directed resources (Because counselling a patient about deprescribing is time-consuming) Choosing Wisely Canada The deprescribing network: has a series of really excellent deprescribing pamphlets
60 Designed and tested with patient stakeholders They use patient friendly language They are freely available online They are translated in french and english They are validated They exist for benzos, sedative hypnotics, antipsychotics, antihistamines, sulfonylureas and PPIs Future pamphlets for general deprescribing and for statins
61

62
63

64
65 MedStopper Can enter drugs there; it tries to tell you risk:benefit and how one would stop for many drugs MedStopper McGill version 2.0 is the subject of a 1.8 million dollar 3 year CIHR funded RCT where it will combine patient comorbidities with recommendations and expanded ruleset
66 End on a quote rarely is it a good idea to substitute a big word, (like) deprescribe, when a small one, like stop, would do. But deprescribing is more than just stopping a therapy. It s more than just an action; it s a way of thinking, a mindset. It brings to the fore another important verb (and noun) need. The act of deprescribing offers an opportunity to inject care back into healthcare. Let s embrace the idea together. Please help me add the new verb to our language. Dr. John Mandrola from his editorial on deprescribing in 2014
67 Questions?
Deconstructing Polypharmacy. Alan B. Douglass, M.D. Director
 Deconstructing Polypharmacy Alan B. Douglass, M.D. Director Recognize this patient? Mrs. Brown- 82 years young Active Medical Problems Hypertension Hyperlipidemia Type 2 Diabetes Peripheral edema Osteoarthritis
Deconstructing Polypharmacy Alan B. Douglass, M.D. Director Recognize this patient? Mrs. Brown- 82 years young Active Medical Problems Hypertension Hyperlipidemia Type 2 Diabetes Peripheral edema Osteoarthritis
DEPRESCRIBING IN THE ELDERLY
 DEPRESCRIBING IN THE ELDERLY G E R I A T R I C S R E F R E S H E R D A Y W E D N E S D A Y, A P R I L 5 TH, 2 0 1 7 V É R O N I Q U E F R E N C H M E R K L E Y, M D, C C F P ( C O E ) B R U Y È R E C O
DEPRESCRIBING IN THE ELDERLY G E R I A T R I C S R E F R E S H E R D A Y W E D N E S D A Y, A P R I L 5 TH, 2 0 1 7 V É R O N I Q U E F R E N C H M E R K L E Y, M D, C C F P ( C O E ) B R U Y È R E C O
Deprescribing Unnecessary Medications: A Four-Part Process
 Deprescribing Unnecessary Medications: A Four-Part Process Scott Endsley, MD Fam Pract Manag. 2018;25(3):28-32. Abstract and Introduction Introduction www.medscape.com Ms. Horatio is a 76-year-old patient
Deprescribing Unnecessary Medications: A Four-Part Process Scott Endsley, MD Fam Pract Manag. 2018;25(3):28-32. Abstract and Introduction Introduction www.medscape.com Ms. Horatio is a 76-year-old patient
Disclosure. The elderly at risk: reducing medications safely to meet life s changes. Relevant financial relationships.
 The elderly at risk: reducing medications safely to meet life s changes Barbara Farrell BScPhm, PharmD, FCSHP European Society of Hospital Pharmacists Conference March 2017 Disclosure Relevant financial
The elderly at risk: reducing medications safely to meet life s changes Barbara Farrell BScPhm, PharmD, FCSHP European Society of Hospital Pharmacists Conference March 2017 Disclosure Relevant financial
Polypharmacy & De-prescribing In Older Adults
 Polypharmacy & De-prescribing In Older Adults Maryland Association of Osteopathic Physicians Annual Meeting September 15, 2018 Elizabeth Phung, DO Lead Clinical Associate Physician Beacham Center for Geriatric
Polypharmacy & De-prescribing In Older Adults Maryland Association of Osteopathic Physicians Annual Meeting September 15, 2018 Elizabeth Phung, DO Lead Clinical Associate Physician Beacham Center for Geriatric
Health Outcome Prioritization as a Tool for Decision Making Among Older Persons With Multiple Chronic Conditions
 Health Outcome Prioritization as a Tool for Decision Making Among Older Persons With Multiple Chronic Conditions Mary Tinetti, M.D. Canadian Geriatrics Society May, 2013 CFPC CoI Templates: Slide 1 Faculty/Presenter
Health Outcome Prioritization as a Tool for Decision Making Among Older Persons With Multiple Chronic Conditions Mary Tinetti, M.D. Canadian Geriatrics Society May, 2013 CFPC CoI Templates: Slide 1 Faculty/Presenter
Deprescribing in CKD patients: Is less more? Speaker: Dr. Judith G. Marin, PharmD
 2016 Deprescribing in CKD patients: Is less more? Speaker: Dr. Judith G. Marin, PharmD Case Mr. Kid Ney is a 75 y/o patient who has been on dialysis for the last 4 years (PD, then HD). PMHx: HTN, DM,
2016 Deprescribing in CKD patients: Is less more? Speaker: Dr. Judith G. Marin, PharmD Case Mr. Kid Ney is a 75 y/o patient who has been on dialysis for the last 4 years (PD, then HD). PMHx: HTN, DM,
About ISMP Canada. Analysis Outputs: Safety Bulletins. Less is More: An Introduction to Deprescribing. canada.org
 Less is More: An Introduction to Deprescribing Lindsay Yoo, BSc, BScPhm, RPh, CDE, CGP, PharmD Medication Safety Analyst, ISMP Canada About ISMP Canada The Institute for Safe Medication Practices Canada
Less is More: An Introduction to Deprescribing Lindsay Yoo, BSc, BScPhm, RPh, CDE, CGP, PharmD Medication Safety Analyst, ISMP Canada About ISMP Canada The Institute for Safe Medication Practices Canada
David Gardner, BSc Pharm, MSc CH&E, PharmD Professor, Department of Psychiatry & College of Pharmacy
 David Gardner, BSc Pharm, MSc CH&E, PharmD Professor, Department of Psychiatry & College of Pharmacy It s no dream. Sleep well without sleeping pills. Outline Baby boomers & beyond: medication use Deprescribing
David Gardner, BSc Pharm, MSc CH&E, PharmD Professor, Department of Psychiatry & College of Pharmacy It s no dream. Sleep well without sleeping pills. Outline Baby boomers & beyond: medication use Deprescribing
Polypharmacy. A CPPE distance learning programme
 A CPPE distance learning programme DLP 177 January 2016 Contents About CPPE distance learning programmes About this learning programme Glossary of key terms v vii ix Contents Section 1 The problem with
A CPPE distance learning programme DLP 177 January 2016 Contents About CPPE distance learning programmes About this learning programme Glossary of key terms v vii ix Contents Section 1 The problem with
A C A D E M I C D E TA I L I N G C H O O S I N G W I S E LY C O N F E R E N C E O C T 2 1, PA M M C L E A N - V E Y S E Y B S C P H A R M D R
 PPI DEPRESCRIBING Canadian Deprescribing Network (CaDeN) goals are to: Reduce harm by raising awareness and cutting risky prescriptions for seniors by 50% by 2020. Promote health by ensuring access to
PPI DEPRESCRIBING Canadian Deprescribing Network (CaDeN) goals are to: Reduce harm by raising awareness and cutting risky prescriptions for seniors by 50% by 2020. Promote health by ensuring access to
BLCS 1-Clinical Overview. Dr. Chris Rauscher Clinical Lead Shared Care Polypharmacy Risk Reduction Initiative
 BLCS 1-Clinical Overview Dr. Chris Rauscher Clinical Lead Shared Care Polypharmacy Risk Reduction Initiative Fraser Health Guide To Person-Centered Medication Decisions Factors to Consider When Systematically
BLCS 1-Clinical Overview Dr. Chris Rauscher Clinical Lead Shared Care Polypharmacy Risk Reduction Initiative Fraser Health Guide To Person-Centered Medication Decisions Factors to Consider When Systematically
Less is More: Introduction to Deprescribing
 Less is More: Introduction to Deprescribing 7th Annual Pharmaceutical Care Conference Muscat, Oman Feb 23, 2017 Lindsay Yoo, BSc, BScPhm, RPh, CDE, CGP, PharmD Medication Safety Analyst, ISMP Canada About
Less is More: Introduction to Deprescribing 7th Annual Pharmaceutical Care Conference Muscat, Oman Feb 23, 2017 Lindsay Yoo, BSc, BScPhm, RPh, CDE, CGP, PharmD Medication Safety Analyst, ISMP Canada About
Polypharmacy and Polymorbid Patients: Practical Tips and Tricks
 Polypharmacy and Polymorbid Patients: Practical Tips and Tricks November 2, 2013 Faculty/Presenter Disclosure Faculty: Chris Fan-Lun, BScPhm, ACPR, CGP Pharmacist - Geriatric Medicine Clinical Practice
Polypharmacy and Polymorbid Patients: Practical Tips and Tricks November 2, 2013 Faculty/Presenter Disclosure Faculty: Chris Fan-Lun, BScPhm, ACPR, CGP Pharmacist - Geriatric Medicine Clinical Practice
START, STOPP, Beers Oh My! Navigating the World of Geriatric Pharmacy
 START, STOPP, Beers Oh My! Navigating the World of Geriatric Pharmacy Jessica DiLeo, PharmD Kate Murphy, PharmD OBJECTIVES Identify pharmacodynamic and pharmacokinetic parameters that may influence treatment
START, STOPP, Beers Oh My! Navigating the World of Geriatric Pharmacy Jessica DiLeo, PharmD Kate Murphy, PharmD OBJECTIVES Identify pharmacodynamic and pharmacokinetic parameters that may influence treatment
If a bad thing is happening to a patient, a drug did it until proven otherwise
 Dr Vicki s First Rule of Geriatrics Deprescribing in the Elderly Victoria Braund MD, FACP, CMD Director, Division of Geriatrics NorthShore University HealthSystem Medical Director, Brandel Health & Rehab
Dr Vicki s First Rule of Geriatrics Deprescribing in the Elderly Victoria Braund MD, FACP, CMD Director, Division of Geriatrics NorthShore University HealthSystem Medical Director, Brandel Health & Rehab
Let it go! Rationalising medicines for patients with life limiting illness
 Let it go! Rationalising medicines for patients with life limiting illness Inga Andrew Senior Clinical Pharmacist Northumbria Healthcare Trust E-mail: inga_andrew@northumbria-healthcare.nhs.uk Welcome
Let it go! Rationalising medicines for patients with life limiting illness Inga Andrew Senior Clinical Pharmacist Northumbria Healthcare Trust E-mail: inga_andrew@northumbria-healthcare.nhs.uk Welcome
Update in Geriatrics: Choosing Wisely Primum Non Nocere
 Joseph G. Ouslander, M.D. Professor of Clinical Biomedical Science Senior Associate Dean for Geriatric Programs Chair, Department of Integrated Medical Science Charles E. Schmidt College of Medicine Professor
Joseph G. Ouslander, M.D. Professor of Clinical Biomedical Science Senior Associate Dean for Geriatric Programs Chair, Department of Integrated Medical Science Charles E. Schmidt College of Medicine Professor
Transitions of Care & Medication Reconciliation Ashley King, PharmD, BCGP Clinical Pharmacist LECOM Health March 2018
 Transitions of Care & Medication Reconciliation Ashley King, PharmD, BCGP Clinical Pharmacist LECOM Health March 2018 Objectives Identify when to complete medication reconciliation Understand the importance
Transitions of Care & Medication Reconciliation Ashley King, PharmD, BCGP Clinical Pharmacist LECOM Health March 2018 Objectives Identify when to complete medication reconciliation Understand the importance
Appropriate prescribing and deprescribing for older people getting it right. Alan Davis Northland District Health Board
 Appropriate prescribing and deprescribing for older people getting it right Alan Davis Northland District Health Board Unused returns Potentially inappropriate medication use in the elderly 15% of older
Appropriate prescribing and deprescribing for older people getting it right Alan Davis Northland District Health Board Unused returns Potentially inappropriate medication use in the elderly 15% of older
MEDICATION APPROPRIATENESS FOR THE AGING POPULATION. Building Partnerships for Successful Aging
 MEDICATION APPROPRIATENESS FOR THE AGING POPULATION Building Partnerships for Successful Aging Learning objectives Appreciate complexities involved in making appropriate clinical decisions in older adults
MEDICATION APPROPRIATENESS FOR THE AGING POPULATION Building Partnerships for Successful Aging Learning objectives Appreciate complexities involved in making appropriate clinical decisions in older adults
Atrial fibrillation. Understanding NICE guidance
 Understanding NICE guidance Information for people who use NHS services Atrial fibrillation NICE clinical guidelines advise the NHS on caring for people with specific conditions or diseases and the treatments
Understanding NICE guidance Information for people who use NHS services Atrial fibrillation NICE clinical guidelines advise the NHS on caring for people with specific conditions or diseases and the treatments
COMMON DRUG RELATED PROBLEMS SEEN IN PACE AND MECHANISMS TO MITIGATE RISK
 COMMON DRUG RELATED PROBLEMS SEEN IN PACE AND MECHANISMS TO MITIGATE RISK Robert L Alesiani, PharmD, CGP Chief Pharmacotherapy Officer CareKinesis, Inc. (a Tabula Rasa Healthcare Company) 2 3 4 5 Pharmacogenomics
COMMON DRUG RELATED PROBLEMS SEEN IN PACE AND MECHANISMS TO MITIGATE RISK Robert L Alesiani, PharmD, CGP Chief Pharmacotherapy Officer CareKinesis, Inc. (a Tabula Rasa Healthcare Company) 2 3 4 5 Pharmacogenomics
Geriatric Pharmacology
 Geriatric Pharmacology Janice Scheufler R.Ph.,PharmD, FASCP Clinical Pharmacist Hospice of the Western Reserve Objectives List three risk factors for adverse drug events in the elderly Discuss two physiological
Geriatric Pharmacology Janice Scheufler R.Ph.,PharmD, FASCP Clinical Pharmacist Hospice of the Western Reserve Objectives List three risk factors for adverse drug events in the elderly Discuss two physiological
Polypharmacy in the Elderly
 Polypharmacy in the Elderly Or How Scotland invented the Modern World Sir William Ferguson Anderson 1914-2001 Became the first Professor of Geriatrics in the world when he was appointed to the David Cargill
Polypharmacy in the Elderly Or How Scotland invented the Modern World Sir William Ferguson Anderson 1914-2001 Became the first Professor of Geriatrics in the world when he was appointed to the David Cargill
Evidence-Based Clinical Practice Guideline for Deprescribing Cholinesterase Inhibitors and Memantine in People with Dementia
 Evidence-Based Clinical Practice Guideline for Deprescribing Cholinesterase Inhibitors and Memantine in People with Dementia ADI 2018, Chicago FACULTY OF MEDICINE Dr Emily Reeve NHMRC Cognitive Decline
Evidence-Based Clinical Practice Guideline for Deprescribing Cholinesterase Inhibitors and Memantine in People with Dementia ADI 2018, Chicago FACULTY OF MEDICINE Dr Emily Reeve NHMRC Cognitive Decline
Shared decision making for stepdown and stopping decisions. Michael R. Gionfriddo Pharm.D, Ph.D Geisinger Center for Pharmacy Innovation and Outcomes
 Shared decision making for stepdown and stopping decisions Michael R. Gionfriddo Pharm.D, Ph.D Geisinger Center for Pharmacy Innovation and Outcomes 1 Disclosures I have had travel and lodging paid for
Shared decision making for stepdown and stopping decisions Michael R. Gionfriddo Pharm.D, Ph.D Geisinger Center for Pharmacy Innovation and Outcomes 1 Disclosures I have had travel and lodging paid for
Preventing Medication Related Falls
 A Team Approach to Deprescribing and Preventing Medication Related Falls Wednesday, February 13 th 2019 Pam Howell THIS WEBINAR IS BEING RECORDED. THE SLIDE DECK AND RECORDING WILL BE EMAILED AFTER THE
A Team Approach to Deprescribing and Preventing Medication Related Falls Wednesday, February 13 th 2019 Pam Howell THIS WEBINAR IS BEING RECORDED. THE SLIDE DECK AND RECORDING WILL BE EMAILED AFTER THE
Thank You to Our Sponsors: Evaluations & CE Credits. Featured Speakers. Conflict of Interest & Disclosure Statements 10/18/2016
 Thank You to Our Sponsors: University at Albany School of Public Health NYS Department of Health Conflict of Interest & Disclosure Statements The planners and presenters do not have any financial arrangements
Thank You to Our Sponsors: University at Albany School of Public Health NYS Department of Health Conflict of Interest & Disclosure Statements The planners and presenters do not have any financial arrangements
TOP 5 DRUGS.. TO AVOID IN THE ELDERLY
 TOP 5 DRUGS.. TO AVOID IN THE ELDERLY Debbie Kwan, BScPhm., MSc., FCSHP Canadian Geriatrics Society, April 20, 2013 Disclosure of Potential for Conflict of Interest: Financial Disclosure: None Mar 26,
TOP 5 DRUGS.. TO AVOID IN THE ELDERLY Debbie Kwan, BScPhm., MSc., FCSHP Canadian Geriatrics Society, April 20, 2013 Disclosure of Potential for Conflict of Interest: Financial Disclosure: None Mar 26,
DRUG THERAPY CHOICES FOR THE DEMENTED PATIENT Past, Present and Future
 DRUG THERAPY CHOICES FOR THE DEMENTED PATIENT Past, Present and Future Daniel S. Sitar Professor Emeritus University of Manitoba Email: Daniel.Sitar@umanitoba.ca March 6, 2018 INTRODUCTION EPIDEMIOLOGY
DRUG THERAPY CHOICES FOR THE DEMENTED PATIENT Past, Present and Future Daniel S. Sitar Professor Emeritus University of Manitoba Email: Daniel.Sitar@umanitoba.ca March 6, 2018 INTRODUCTION EPIDEMIOLOGY
Targeted Deprescribing in Patients on Hemodialysis to Decrease Polypharmacy
 Targeted Deprescribing in Patients on Hemodialysis to Decrease Polypharmacy Presentation Objectives Discuss Polypharmacy In HD patients Define Deprescribing Review results of the pilot study on deprescribing
Targeted Deprescribing in Patients on Hemodialysis to Decrease Polypharmacy Presentation Objectives Discuss Polypharmacy In HD patients Define Deprescribing Review results of the pilot study on deprescribing
Akinbolade O, Husband A, Forrest S, Todd A. Deprescribing in advanced illness. Progress in Palliative Care 2016, 24(5),
,") Akinbolade O, Husband A, Forrest S, Todd A. Deprescribing in advanced illness. Progress in Palliative Care 2016, 24(5), 268-271 Copyright: This is an Accepted Manuscript of an article published by Taylor
Akinbolade O, Husband A, Forrest S, Todd A. Deprescribing in advanced illness. Progress in Palliative Care 2016, 24(5), 268-271 Copyright: This is an Accepted Manuscript of an article published by Taylor
Polypharmacy and Deprescribing for Older People
 Polypharmacy and Deprescribing for Older People Sarah Hilmer Head of Department, Clinical Pharmacology and Senior Staff Specialist Aged Care, RNSH Conjoint Professor of Geriatric Pharmacology, Sydney University
Polypharmacy and Deprescribing for Older People Sarah Hilmer Head of Department, Clinical Pharmacology and Senior Staff Specialist Aged Care, RNSH Conjoint Professor of Geriatric Pharmacology, Sydney University
Heart Failure Clinician Guide JANUARY 2018
 Kaiser Permanente National CLINICAL PRACTICE GUIDELINES Heart Failure Clinician Guide JANUARY 2018 Introduction This evidence-based guideline summary is based on the 2018 National Heart Failure Guideline.
Kaiser Permanente National CLINICAL PRACTICE GUIDELINES Heart Failure Clinician Guide JANUARY 2018 Introduction This evidence-based guideline summary is based on the 2018 National Heart Failure Guideline.
PRESCRIBING IN THE ELDERLY. CARE HOME PHARMACY TEAM Bhavini Shah, Eleesha Pentiah & Puja Vyas
 PRESCRIBING IN THE ELDERLY CARE HOME PHARMACY TEAM Bhavini Shah, Eleesha Pentiah & Puja Vyas LEARNING OUTCOMES Medicines Optimisation The effects of aging on health and medicines. Polypharmacy Acute Kidney
PRESCRIBING IN THE ELDERLY CARE HOME PHARMACY TEAM Bhavini Shah, Eleesha Pentiah & Puja Vyas LEARNING OUTCOMES Medicines Optimisation The effects of aging on health and medicines. Polypharmacy Acute Kidney
Heart Failure Clinician Guide JANUARY 2016
 Kaiser Permanente National CLINICAL PRACTICE GUIDELINES Heart Failure Clinician Guide JANUARY 2016 Introduction This evidence-based guideline summary is based on the 2016 National Heart Failure Guideline.
Kaiser Permanente National CLINICAL PRACTICE GUIDELINES Heart Failure Clinician Guide JANUARY 2016 Introduction This evidence-based guideline summary is based on the 2016 National Heart Failure Guideline.
STOPP and START criteria October 2011
 # START and STOPP are newer criteria to identify potentially inappropriate medications in elderly, including drug drug and drug disease interactions, drugs which increase risk of falls and drugs which
# START and STOPP are newer criteria to identify potentially inappropriate medications in elderly, including drug drug and drug disease interactions, drugs which increase risk of falls and drugs which
From medicines reconciliation to medicines review. Dr. Fatma Karapinar Hospital pharmacistepidemiologist
 From medicines reconciliation to medicines review Dr. Fatma Karapinar Hospital pharmacistepidemiologist Conflict of interest Nothing to disclose Questions Medication review is more important than medicines
From medicines reconciliation to medicines review Dr. Fatma Karapinar Hospital pharmacistepidemiologist Conflict of interest Nothing to disclose Questions Medication review is more important than medicines
Case Study #1 GUIDING PRINCIPLES FOR THE CARE OF OLDER ADULTS WITH MULTIMORBIDITY
 Case Study #1 GUIDING PRINCIPLES FOR THE CARE OF OLDER ADULTS WITH MULTIMORBIDITY Panel Moderator & Panelists: Edward Perrin, MD Banner icare Scott Bolhack, MD, MBA Sandra Brownstein, PharmD Paige Hector,
Case Study #1 GUIDING PRINCIPLES FOR THE CARE OF OLDER ADULTS WITH MULTIMORBIDITY Panel Moderator & Panelists: Edward Perrin, MD Banner icare Scott Bolhack, MD, MBA Sandra Brownstein, PharmD Paige Hector,
Controlled Substance and Wellness Agreement
 Controlled Substance and Wellness Agreement You and your provider have agreed on the use of controlled substance medications to treat your: We want to make sure you know how to manage your new prescription(s)
Controlled Substance and Wellness Agreement You and your provider have agreed on the use of controlled substance medications to treat your: We want to make sure you know how to manage your new prescription(s)
AF in the ER: Common Scenarios CASE 1. Fast facts. Diagnosis. Management
 AF in the ER: Common Scenarios Atrial fibrillation is a common problem with a wide spectrum of presentations. Below are five common emergency room scenarios and the management strategies for each. Evan
AF in the ER: Common Scenarios Atrial fibrillation is a common problem with a wide spectrum of presentations. Below are five common emergency room scenarios and the management strategies for each. Evan
2/1/2013. Poisoning pitfalls. The original pitfall
 The original pitfall Poisoning pitfalls Craig Smollin MD Associate Medical Director, California Poison Control System - SF Division Assistant Professor of Emergency Medicine, UCSF What will we talk about?
The original pitfall Poisoning pitfalls Craig Smollin MD Associate Medical Director, California Poison Control System - SF Division Assistant Professor of Emergency Medicine, UCSF What will we talk about?
Screening tools for elderly patients in primary care
 Screening tools for elderly patients in primary care Cristín Ryan 1 Prof. Julia Kennedy 1 Dr. Denis O Mahony 2 Dr. Stephen Byrne 1 Co-Investigator: Dr. Paul Gallagher 2 1 Pharmaceutical Care Research Group,
Screening tools for elderly patients in primary care Cristín Ryan 1 Prof. Julia Kennedy 1 Dr. Denis O Mahony 2 Dr. Stephen Byrne 1 Co-Investigator: Dr. Paul Gallagher 2 1 Pharmaceutical Care Research Group,
DEPRESCRIBING. Phil St John CSIM Workshop
 DEPRESCRIBING Phil St John CSIM Workshop Conflict of Interest Disclosure Consultant for: none Speaker for: none Received grant/research support from: CIHR, MHRC, Riverview Foundation Received honoraria
DEPRESCRIBING Phil St John CSIM Workshop Conflict of Interest Disclosure Consultant for: none Speaker for: none Received grant/research support from: CIHR, MHRC, Riverview Foundation Received honoraria
Polypharmacy: Guidance for Prescribing in Frail Adults
 Polypharmacy: Guidance for Prescribing in Frail Adults Why is reviewing polypharmacy important? Medication is by far the most common form of medical intervention. Four out of five people aged over 75 years
Polypharmacy: Guidance for Prescribing in Frail Adults Why is reviewing polypharmacy important? Medication is by far the most common form of medical intervention. Four out of five people aged over 75 years
Preventing Falls in Older Adults A Matter of Safety
 Preventing Falls in Older Adults A Matter of Safety Roger Tam, BSc. Pharm. Wal-Mart Clinical Designated Pharmacist Falls Prevention Pharmacist Specialist NCCHC-Pre/Post Test Educator Q.U.I.T Educator Overview
Preventing Falls in Older Adults A Matter of Safety Roger Tam, BSc. Pharm. Wal-Mart Clinical Designated Pharmacist Falls Prevention Pharmacist Specialist NCCHC-Pre/Post Test Educator Q.U.I.T Educator Overview
CHAPTER 2. GERIATRICS, SELF-ASSESSMENT QUESTIONS
 CHAPTER 2. GERIATRICS, SELF-ASSESSMENT QUESTIONS 1. The following is an accurate description of the aging population: A. The number of older adults will reach 17 million in 2030 B. The ratio of women to
CHAPTER 2. GERIATRICS, SELF-ASSESSMENT QUESTIONS 1. The following is an accurate description of the aging population: A. The number of older adults will reach 17 million in 2030 B. The ratio of women to
Meds and Falls: Keep in Step with your Meds
 Meds and Falls: Keep in Step with your Meds Donna Bartlett PharmD, CGP, RPh Associate Professor-Pharmacy Practice MCPHS University Clinical Pharmacist-MCPHS University- Pharmacy Outreach Program donna.bartlett@mcphs.edu
Meds and Falls: Keep in Step with your Meds Donna Bartlett PharmD, CGP, RPh Associate Professor-Pharmacy Practice MCPHS University Clinical Pharmacist-MCPHS University- Pharmacy Outreach Program donna.bartlett@mcphs.edu
Optimising Safe & Appropriate Medicines Use and Deprescribing. Katie Smith, Director, East Anglia Medicines Information Service February 2014
 Optimising Safe & Appropriate Medicines Use and Deprescribing Katie Smith, Director, East Anglia Medicines Information Service February 2014 Background Objectives How & why the OSAMU document was developed
Optimising Safe & Appropriate Medicines Use and Deprescribing Katie Smith, Director, East Anglia Medicines Information Service February 2014 Background Objectives How & why the OSAMU document was developed
Travel Health Conference. April 27, 2018 Jamie Falk, BScPharm, PharmD
 Travel Health Conference April 27, 2018 Jamie Falk, BScPharm, PharmD Presenter: Jamie Falk Drug interactions in travelers with chronic conditions I have no conflicts to disclose By attending this session
Travel Health Conference April 27, 2018 Jamie Falk, BScPharm, PharmD Presenter: Jamie Falk Drug interactions in travelers with chronic conditions I have no conflicts to disclose By attending this session
Prescribing Drugs to the Elderly
 Answers to your questions from University of Toronto experts Prescribing Drugs to the Elderly Can drugs do more harm than good? M.A. is a 90-year-old man living at home. He has dementia and due to wandering
Answers to your questions from University of Toronto experts Prescribing Drugs to the Elderly Can drugs do more harm than good? M.A. is a 90-year-old man living at home. He has dementia and due to wandering
Medication Management When Caring for Seniors at Home
 Medication Management When Caring for Seniors at Home White Paper May 24, 2013 2013 Physician s Choice Private Duty http://private-duty.pchhc.com 1 Proper medication management for seniors who live at
Medication Management When Caring for Seniors at Home White Paper May 24, 2013 2013 Physician s Choice Private Duty http://private-duty.pchhc.com 1 Proper medication management for seniors who live at
ten questions you might have about tapering (and room for your own) an informational booklet for opioid pain treatment
 an informational booklet for opioid pain treatment") ten questions you might have about tapering (and room for your own) an informational booklet for opioid pain treatment This booklet was created to help you learn about tapering. You probably have lots
ten questions you might have about tapering (and room for your own) an informational booklet for opioid pain treatment This booklet was created to help you learn about tapering. You probably have lots
Adjusting and Withdrawing Medications in the Elderly
 Adjusting and Withdrawing Medications in the Elderly Louise Mallet, B.Sc.Pharm., Pharm.D., CGP Professor in Clinical Pharmacy, Faculty of Pharmacy, University of Montreal Clinical Pharmacist in Geriatrics,
Adjusting and Withdrawing Medications in the Elderly Louise Mallet, B.Sc.Pharm., Pharm.D., CGP Professor in Clinical Pharmacy, Faculty of Pharmacy, University of Montreal Clinical Pharmacist in Geriatrics,
Cost and Prevalence of A fib. Atrial Fibrillation: Guideline Directed Treatment. Prevalence of A Fib. Risk Factors for A Fib. Risk Factors for A Fib
 Atrial Fibrillation: Guideline Directed Treatment Melissa Wendell, FNP-C, MSN Heart Failure - Lead Nurse Practitioner, Aspirus Wausau Hospital and Aspirus Cardiology Cost and Prevalence of A fib 33.5 million
Atrial Fibrillation: Guideline Directed Treatment Melissa Wendell, FNP-C, MSN Heart Failure - Lead Nurse Practitioner, Aspirus Wausau Hospital and Aspirus Cardiology Cost and Prevalence of A fib 33.5 million
Individualizing Treatment Plans for Older Adults With T2DM
 Individualizing Treatment Plans for Older Adults With T2DM Key Slides from the Interactive Newsletter Hypoglycemia y in Older Adults Particularly dangerous, especially for those on insulin or secretagogues
Individualizing Treatment Plans for Older Adults With T2DM Key Slides from the Interactive Newsletter Hypoglycemia y in Older Adults Particularly dangerous, especially for those on insulin or secretagogues
Supplemental materials for:
 Supplemental materials for: Wallis KA, Andrews A, Henderson M. Swimming against the tide: primary care physicians views on deprescribing in everyday practice. Ann Fam Med. 2017;15(4):341-346. General Practice
Supplemental materials for: Wallis KA, Andrews A, Henderson M. Swimming against the tide: primary care physicians views on deprescribing in everyday practice. Ann Fam Med. 2017;15(4):341-346. General Practice
Instruct patient and caregivers: Need for constant monitoring Potential complications of drug therapy
 Assessment Prior to administration: Assess patient for chest pain, dysrhythmias, and vital signs (initially and throughout therapy) Obtain complete medical history, including allergies, especially heart
Assessment Prior to administration: Assess patient for chest pain, dysrhythmias, and vital signs (initially and throughout therapy) Obtain complete medical history, including allergies, especially heart
Murthy Gokula MD,CMD
 Murthy Gokula MD,CMD MEDICATIONS & LIFE EXPECTANCY DON T ROUTINELY PRESCRIBE LIPID-LOWERING MEDICATIONS IN INDIVIDUALS WITH A LIMITED LIFE EXPECTANCY: AAHPM About Choosing Wisely First conceived by the
Murthy Gokula MD,CMD MEDICATIONS & LIFE EXPECTANCY DON T ROUTINELY PRESCRIBE LIPID-LOWERING MEDICATIONS IN INDIVIDUALS WITH A LIMITED LIFE EXPECTANCY: AAHPM About Choosing Wisely First conceived by the
5AB Dysrhythmia Interpretation and Management 2016
 5AB Dysrhythmia Interpretation and Management 2016 How to complete your biennial ECG review: A website has been created that contains the basic review information. Use this as a reference during your review.
5AB Dysrhythmia Interpretation and Management 2016 How to complete your biennial ECG review: A website has been created that contains the basic review information. Use this as a reference during your review.
Objectives. Case Ruby. 1- Warfarin. 1- Warfarin. Warfarin discontinuation 8/13/ DRUGS TO STOP GIVING HOSPICE PATIENTS
 Objectives 10 DRUGS TO STOP GIVING HOSPICE PATIENTS Richard E. Allen MD, MPH Hospice Medical Director Family Medicine Residency Director Salt Lake City, Utah 2 Recognize 10 commonly prescribed medications
Objectives 10 DRUGS TO STOP GIVING HOSPICE PATIENTS Richard E. Allen MD, MPH Hospice Medical Director Family Medicine Residency Director Salt Lake City, Utah 2 Recognize 10 commonly prescribed medications
University of Hawaii Center on Aging
 University of Hawaii Center on Aging. Supported in part by a cooperative agreement No. 90AL0011-01-00 from the Administration on Aging, Administration for Community Living, U.S. Department of Health and
University of Hawaii Center on Aging. Supported in part by a cooperative agreement No. 90AL0011-01-00 from the Administration on Aging, Administration for Community Living, U.S. Department of Health and
Optimising prescribing in primary care in the face of multimorbidity and polypharmacy
 University of Dundee School of Medicine Optimising prescribing in primary care in the face of multimorbidity and polypharmacy Bruce Guthrie Professor of Primary Care Medicine, University of Dundee NICE
University of Dundee School of Medicine Optimising prescribing in primary care in the face of multimorbidity and polypharmacy Bruce Guthrie Professor of Primary Care Medicine, University of Dundee NICE
David Dosa MD, MPH Assistant Professor of Medicine and Community Health The Warren Alpert School of Medicine, Brown University Director, Primary Care
 David Dosa MD, MPH Assistant Professor of Medicine and Community Health The Warren Alpert School of Medicine, Brown University Director, Primary Care Geriatrics Clinic- Providence VAMC VA Grand Rounds
David Dosa MD, MPH Assistant Professor of Medicine and Community Health The Warren Alpert School of Medicine, Brown University Director, Primary Care Geriatrics Clinic- Providence VAMC VA Grand Rounds
Appropriate Use of Proton Pump Inhibitors (PPIs) Anderson Mabour, Pharm.D., BCPS Clinical Pharmacy Specialist
 Anderson Mabour, Pharm.D., BCPS Clinical Pharmacy Specialist") Appropriate Use of Proton Pump Inhibitors (PPIs) Anderson Mabour, Pharm.D., BCPS Clinical Pharmacy Specialist Disclosures I have no actual or potential conflicts of interest to report in relation to this
Appropriate Use of Proton Pump Inhibitors (PPIs) Anderson Mabour, Pharm.D., BCPS Clinical Pharmacy Specialist Disclosures I have no actual or potential conflicts of interest to report in relation to this
Mucky Meds: A (practical) approach the nightmare med list. Michelle Gibson, MD, CCFP (COE), FCFP and Erin Beattie, MD, CCFP
 approach the nightmare med list. Michelle Gibson, MD, CCFP (COE), FCFP and Erin Beattie, MD, CCFP") Mucky Meds: A (practical) approach the nightmare med list Michelle Gibson, MD, CCFP (COE), FCFP and Erin Beattie, MD, CCFP Faculty/Presenter Disclosure Faculty: Michelle Gibson Relationships with financial
Mucky Meds: A (practical) approach the nightmare med list Michelle Gibson, MD, CCFP (COE), FCFP and Erin Beattie, MD, CCFP Faculty/Presenter Disclosure Faculty: Michelle Gibson Relationships with financial
STOPP START Toolkit Supporting Medication Review in the Older Person
 STOPP START Toolkit Supporting Medication Review in the Older Person STOPP: Screening Tool of Older People s potentially inappropriate Prescriptions START: Screening Tool to Alert doctors to Right (appropriate,
STOPP START Toolkit Supporting Medication Review in the Older Person STOPP: Screening Tool of Older People s potentially inappropriate Prescriptions START: Screening Tool to Alert doctors to Right (appropriate,
Delirium. A Geriatric Syndrome. Jonathan McCaleb, MD, CMD, HMDC UNSOM, Assistant Professor of Medicine Geriatrics / Hospice & Palliative Medicine
 Delirium A Geriatric Syndrome Jonathan McCaleb, MD, CMD, HMDC UNSOM, Assistant Professor of Medicine Geriatrics / Hospice & Palliative Medicine Introduction Common Serious Unrecognized: a medical emergency
Delirium A Geriatric Syndrome Jonathan McCaleb, MD, CMD, HMDC UNSOM, Assistant Professor of Medicine Geriatrics / Hospice & Palliative Medicine Introduction Common Serious Unrecognized: a medical emergency
There s A Pill For That (But should my patient be on it?) A Review of Tools for the Evaluation of Optimal Prescribing in Geriatric Patients
 A Review of Tools for the Evaluation of Optimal Prescribing in Geriatric Patients") There s A Pill For That (But should my patient be on it?) A Review of Tools for the Evaluation of Optimal Prescribing in Geriatric Patients Marilyn N. Bulloch, PharmD, BCPS Assistant Clinical Professor
There s A Pill For That (But should my patient be on it?) A Review of Tools for the Evaluation of Optimal Prescribing in Geriatric Patients Marilyn N. Bulloch, PharmD, BCPS Assistant Clinical Professor
A Case of Severe Hypomagnesemia with Long-term Use of a Proton Pump Inhibitor
 A Case of Severe Hypomagnesemia with Long-term Use of a Proton Pump Inhibitor Amy Trottier University of Calgary Internal Medicine, PGY1 November 14, 2013 2013 Rocky Mountain/ACP Internal Medicine Conference
A Case of Severe Hypomagnesemia with Long-term Use of a Proton Pump Inhibitor Amy Trottier University of Calgary Internal Medicine, PGY1 November 14, 2013 2013 Rocky Mountain/ACP Internal Medicine Conference
Polypharmacy: Making it all Work Kathy Wilson, RPh, RWSIR Director of Pharmacy
 Polypharmacy: Making it all Work Kathy Wilson, RPh, RWSIR Director of Pharmacy Polypharmacy can be defined as the use of multiple medications for the treatment of a patient s medical conditions. The term
Polypharmacy: Making it all Work Kathy Wilson, RPh, RWSIR Director of Pharmacy Polypharmacy can be defined as the use of multiple medications for the treatment of a patient s medical conditions. The term
Potentially Inappropriate Medications in Elderly Patients: Prevalence at Admission and Changes During Hospital Stay
 Potentially Inappropriate Medications in Elderly Patients: Prevalence at Admission and Changes During Hospital Stay Background Polypharmacy in the Elderly 40% seniors are using 5-9 different classes of
Potentially Inappropriate Medications in Elderly Patients: Prevalence at Admission and Changes During Hospital Stay Background Polypharmacy in the Elderly 40% seniors are using 5-9 different classes of
Medication Use in Older Adults
 Medication Use in Older Adults F. Michael Gloth, III, MD, AGSF, FACP, CMD Clinical Professor Department of Geriatrics, Florida State University College of Medicine Associate Professor of Medicine Division
Medication Use in Older Adults F. Michael Gloth, III, MD, AGSF, FACP, CMD Clinical Professor Department of Geriatrics, Florida State University College of Medicine Associate Professor of Medicine Division
Interdisciplinary detection of potential drug related problems in older people
 Interdisciplinary detection of potential drug related problems in older people Prof. dr. Mirko Petrovic Department of Internal Medicine, Ghent University Department of Geriatrics, Ghent University Hospital,
Interdisciplinary detection of potential drug related problems in older people Prof. dr. Mirko Petrovic Department of Internal Medicine, Ghent University Department of Geriatrics, Ghent University Hospital,
Medication Reviews within Care Homes. Catherine Armstrong
 Medication Reviews within Care Homes Catherine Armstrong What is a Medication Review? A structured, critical examination of a patient s medicines with the objective of reaching an agreement with the patient
Medication Reviews within Care Homes Catherine Armstrong What is a Medication Review? A structured, critical examination of a patient s medicines with the objective of reaching an agreement with the patient
Polypharmacy. in the Elderly. Lesley Charles, MBChB, CCFP
 Polypharmacy in the Elderly Lesley Charles, MBChB, CCFP Associate Professor and Program Director Division of Care of the Elderly Department of Family Medicine, University of Alberta March 06, 2016 1 Faculty/Presenter
Polypharmacy in the Elderly Lesley Charles, MBChB, CCFP Associate Professor and Program Director Division of Care of the Elderly Department of Family Medicine, University of Alberta March 06, 2016 1 Faculty/Presenter
ATRIAL FIBRILLATION: REVISITING CONTROVERSIES IN AN ERA OF INNOVATION
 ATRIAL FIBRILLATION: REVISITING CONTROVERSIES IN AN ERA OF INNOVATION Frederick Schaller, DO, MACOI,FACP Adjunct Clinical Professor Touro University Nevada DISCLOSURES I have no financial relationships
ATRIAL FIBRILLATION: REVISITING CONTROVERSIES IN AN ERA OF INNOVATION Frederick Schaller, DO, MACOI,FACP Adjunct Clinical Professor Touro University Nevada DISCLOSURES I have no financial relationships
GRADE, EBM and Deprescribing. Kevin Pottie MD CCFP, MClSc, FCFP Associate Professor, Family Medicine, University of Ottawa
 GRADE, EBM and Deprescribing Kevin Pottie MD CCFP, MClSc, FCFP Associate Professor, Family Medicine, University of Ottawa Research is like turning on the light before you clean up the room: it doesn t
GRADE, EBM and Deprescribing Kevin Pottie MD CCFP, MClSc, FCFP Associate Professor, Family Medicine, University of Ottawa Research is like turning on the light before you clean up the room: it doesn t
Difficult to Treat Hypertension
 Difficult to Treat Hypertension According to Goldilocks JNC 8 Blood Pressure Goals (2014) BP Goal 60 years old and greater*- systolic < 150 and diastolic < 90. (Grade A)** BP Goal 18-59 years old* diastolic
Difficult to Treat Hypertension According to Goldilocks JNC 8 Blood Pressure Goals (2014) BP Goal 60 years old and greater*- systolic < 150 and diastolic < 90. (Grade A)** BP Goal 18-59 years old* diastolic
The patient with multiple chronic conditions: balancing guidelines and patient preference
 The patient with multiple chronic conditions: balancing guidelines and patient preference Sid Feldman MD CCFP FCFP Associate Professor, Department of Family and Community Medicine, University of Toronto
The patient with multiple chronic conditions: balancing guidelines and patient preference Sid Feldman MD CCFP FCFP Associate Professor, Department of Family and Community Medicine, University of Toronto
Atrial Fibrillation Cases. Dr Paul Broadhurst Consultant Cardiologist
 Atrial Fibrillation Cases Dr Paul Broadhurst Consultant Cardiologist November 2011 Mr TH age 72 Routine medical for hypertension check Denies any symptoms despite close questioning PMH: hypertension, MI,
Atrial Fibrillation Cases Dr Paul Broadhurst Consultant Cardiologist November 2011 Mr TH age 72 Routine medical for hypertension check Denies any symptoms despite close questioning PMH: hypertension, MI,
Anthony J. Caprio, MD, CMD, AGSF 1
 Objectives 1) Discuss the dangers of polypharmacy 2) Review potentially inappropriate medications for older adults Doc, I think I am taking too many medications! 3) Develop strategies for prioritizing
Objectives 1) Discuss the dangers of polypharmacy 2) Review potentially inappropriate medications for older adults Doc, I think I am taking too many medications! 3) Develop strategies for prioritizing
Bulletin Independent prescribing information for NHS Wales
 Bulletin Independent prescribing information for NHS Wales July 2016 Optimising medicines use in care homes There are currently over 22 000 resident places in older adult care homes in Wales. 1 An ageing
Bulletin Independent prescribing information for NHS Wales July 2016 Optimising medicines use in care homes There are currently over 22 000 resident places in older adult care homes in Wales. 1 An ageing
STATS, FACTS & TALKING POINTS ABOUT ALCOHOL AND OTHER DRUGS PARENT ACTION PACK
 ARE YOU PREPARED TO HELP YOUR TEEN MAKE GOOD DECISIONS? STATS, FACTS & TALKING POINTS ABOUT ALCOHOL AND OTHER DRUGS PARENT ACTION PACK facebook.com/parentactionondrugs @PAD_Ontario YOU ARE YOUR TEEN S
ARE YOU PREPARED TO HELP YOUR TEEN MAKE GOOD DECISIONS? STATS, FACTS & TALKING POINTS ABOUT ALCOHOL AND OTHER DRUGS PARENT ACTION PACK facebook.com/parentactionondrugs @PAD_Ontario YOU ARE YOUR TEEN S
Webinar Series April 11, 2018
 Webinar Series April 11, 2018 Reducing post-discharge potentially inappropriate medications amongst the elderly: a multi-centre electronic deprescribing intervention Todd Lee, MD, MPH, FRCPC McGill University
Webinar Series April 11, 2018 Reducing post-discharge potentially inappropriate medications amongst the elderly: a multi-centre electronic deprescribing intervention Todd Lee, MD, MPH, FRCPC McGill University
Taking the harm out of Polypharmacy Step by step. Karen Reid and Claire Stein Lead Integrated Care Pharmacist NHS Lothian
 Taking the harm out of Polypharmacy Step by step Karen Reid and Claire Stein Lead Integrated Care Pharmacist NHS Lothian Presentation: Polypharmacy Overview of the 2015 guidelines The Seven Steps Application
Taking the harm out of Polypharmacy Step by step Karen Reid and Claire Stein Lead Integrated Care Pharmacist NHS Lothian Presentation: Polypharmacy Overview of the 2015 guidelines The Seven Steps Application
Family Medicine Clinical Pharmacy Forum Vol. 4, Issue 5 (September/October 2008)
") 1 Family Medicine Clinical Pharmacy Forum Vol. 4, Issue 5 (September/October 2008) Family Medicine Clinical Pharmacy Forum is a brief bi-monthly publication from the Family Medicine clinical pharmacists
1 Family Medicine Clinical Pharmacy Forum Vol. 4, Issue 5 (September/October 2008) Family Medicine Clinical Pharmacy Forum is a brief bi-monthly publication from the Family Medicine clinical pharmacists
Opioid de-prescribing guidelines?
 Opioid de-prescribing guidelines? Feng Chang, RPh, BScPhm, PharmD Associate Professor University of Waterloo, School of Pharmacy Waterloo, Canada #derx2018 Outline Introduction De-prescribing guideline
Opioid de-prescribing guidelines? Feng Chang, RPh, BScPhm, PharmD Associate Professor University of Waterloo, School of Pharmacy Waterloo, Canada #derx2018 Outline Introduction De-prescribing guideline
Palliative Medicine in Critical Care Not Just Hospice. Robin. Truth or Myth 6/11/2015. Francine Arneson, MD Palliative Medicine
 Palliative Medicine in Critical Care Not Just Hospice Francine Arneson, MD Palliative Medicine Robin 45 year old female married, husband in Afghanistan. 4 children ages 17-24. Mother has been providing
Palliative Medicine in Critical Care Not Just Hospice Francine Arneson, MD Palliative Medicine Robin 45 year old female married, husband in Afghanistan. 4 children ages 17-24. Mother has been providing
TELUS Health Conference Toronto
 TELUS Health Conference Toronto Dr. Wendy Levinson, MD, OC Chair, Choosing Wisely Canada & International Professor of Medicine, University of Toronto March 23rd, 2016 Wedges of Waste 2 I ve always done
TELUS Health Conference Toronto Dr. Wendy Levinson, MD, OC Chair, Choosing Wisely Canada & International Professor of Medicine, University of Toronto March 23rd, 2016 Wedges of Waste 2 I ve always done
High Alert Medications in the long-term care setting. Carrie Allen PharmD, CGP, BCPS, CCHP
 High Alert Medications in the long-term care setting Carrie Allen PharmD, CGP, BCPS, CCHP Who does this involve? Nurses Medication aides Pharmacies/pharmacists Medical Records and Data Entry Personnel
High Alert Medications in the long-term care setting Carrie Allen PharmD, CGP, BCPS, CCHP Who does this involve? Nurses Medication aides Pharmacies/pharmacists Medical Records and Data Entry Personnel
Rationalizing Medications. Tan Jianming Senior Pharmacist KTPH
 Rationalizing Medications Tan Jianming Senior Pharmacist KTPH + Older patients are more likely to: 2 Have multiple co-morbid diseases Have age-related physiological changes that result in a reduced tolerance
Rationalizing Medications Tan Jianming Senior Pharmacist KTPH + Older patients are more likely to: 2 Have multiple co-morbid diseases Have age-related physiological changes that result in a reduced tolerance
Review guidance for patients on long-term amiodarone treatment
 Review guidance for patients on long-term amiodarone treatment This review guidance document has been produced in response to: 1. Current supply shortages of branded and generic versions of 100mg and 200mg
Review guidance for patients on long-term amiodarone treatment This review guidance document has been produced in response to: 1. Current supply shortages of branded and generic versions of 100mg and 200mg
PPIs: Good or Bad? 1. Basics of PPIs. Gastric Acid Basics. Outline. Gastric Acid Basics. Proton Pump Inhibitors (PPI)
") Outline Quick basics on Proton Pump Inhibitors (PPIs) PPIs: Good or Bad? What are potential risks of PPI therapy? How to approach your patients American Gastroenterology Association (AGA) recommendations
Outline Quick basics on Proton Pump Inhibitors (PPIs) PPIs: Good or Bad? What are potential risks of PPI therapy? How to approach your patients American Gastroenterology Association (AGA) recommendations
Doreen Wan-Chow-Wah, MD, FRCPC Assistant Professor, Division of Geriatric Medicine, Department of Medicine McGill University Health Center Associate
 Doreen Wan-Chow-Wah, MD, FRCPC Assistant Professor, Division of Geriatric Medicine, Department of Medicine McGill University Health Center Associate member, Department of Oncology McGill University Medical
Doreen Wan-Chow-Wah, MD, FRCPC Assistant Professor, Division of Geriatric Medicine, Department of Medicine McGill University Health Center Associate member, Department of Oncology McGill University Medical
Pharmaceutical Care for Geriatrics
 Continuing Professional Pharmacy Development Program Pharmaceutical Care for Geriatrics Presented by: Alla El-Awaisi; MPharm, MRPharmS, MSc Event Organizer: Dr. Nadir Kheir; PhD Disclaimer: PRESENTING
Continuing Professional Pharmacy Development Program Pharmaceutical Care for Geriatrics Presented by: Alla El-Awaisi; MPharm, MRPharmS, MSc Event Organizer: Dr. Nadir Kheir; PhD Disclaimer: PRESENTING
Diabetes and the Elderly: Medication Considerations When Determining Benefits and Risks
 Diabetes and the Elderly: Medication Considerations When Determining Benefits and Risks Gretchen M. Ray, PharmD, PhC, BCACP, CDE Associate Professor UNM College of Pharmacy September 7 th, 2018 DISCLOSURES
Diabetes and the Elderly: Medication Considerations When Determining Benefits and Risks Gretchen M. Ray, PharmD, PhC, BCACP, CDE Associate Professor UNM College of Pharmacy September 7 th, 2018 DISCLOSURES
Choosing Wisely Long Term Care Uniquely Canadian
 Choosing Wisely Long Term Care Uniquely Canadian Family Medicine Forum, Montreal November 11, 2017 Session ID S460 Room 512 ABEF Conflict of interest Dr. Fred Mather Waterloo Ontario Amgen Dr. Serge Gingras
Choosing Wisely Long Term Care Uniquely Canadian Family Medicine Forum, Montreal November 11, 2017 Session ID S460 Room 512 ABEF Conflict of interest Dr. Fred Mather Waterloo Ontario Amgen Dr. Serge Gingras