Preventing Medication Related Falls
|
|
|
- Baldric Chapman
- 5 years ago
- Views:
Transcription

1 A Team Approach to Deprescribing and Preventing Medication Related Falls Wednesday, February 13 th 2019 Pam Howell THIS WEBINAR IS BEING RECORDED. THE SLIDE DECK AND RECORDING WILL BE ED AFTER THE WEBINAR. Webinar technology managed by:


2 A Team Approach to Deprescribing and Preventing Medication Related Falls LOOP: Fall Prevention Community of Practice Webinar February 13 th 2019 Pam Howell
3 Everyone has a story
4 Objectives Highlight key points about polypharmacy that relate to increased falls risk Present current deprescribing guidelines research Encourage participants to think about their role in medication management and how it fits within the healthcare team Engage participants to reflect how deprescribing could be managed within their expertise and in their care setting by using available tools and resources 15 February 2019

5 Medications can: Treat symptoms Slow the progression of disease Reduce the risk of complications from disease

6 Polypharmacy The use of more medications than are needed or for which harm outweighs benefit Increases the risk of: Drug interactions and adverse reactions Falls, fractures Functional and cognitive decline Nonadherence Hospitalizations and higher health care costs Particular risk for elderly individuals who handle and respond to drugs differently, are often frail, and are not typically represented in research

7 How big is the problem? 2/3 Canadian seniors are prescribed at least 5 prescription medications Who takes 10 or more? 27% over 65 years 40% over 85 years 66% in long-term care homes $419 million spent on PIMs $1.4 billion in incremental health care expenditure due to PIMs (CIHI 2014;

8 Who is most at risk of harmful effects of medication? 1. People with multiple chronic conditions 2. Women 3. People over the age of 65 Each year in Canada: 1 in 200 seniors are hospitalized due to harmful effects of their medication. Seniors are hospitalized 5 times more often than people under the age of 65 because of harmful medication effects Canadian Institute for Health Information Adverse Drug Reaction Related Hospitalizations Among Seniors, 2006 to
9 As we get older The brain becomes more sensitive to drug effects Some medications stay longer in our body because we have less muscle and more body fat Our liver and kidneys do not process medications as efficiently as when we were younger Our body contains less water and medications can become more concentrated 8

10 Which medications increase the risk of falls? Of note: -medications that are associated with falls are also often associated with decreasing cognition Sources: de Jong et al Therapeutic Advances in Drug Safety. 4(4): & Huang et al Drugs & Aging 29(5):



11 Higher risk of falling 1.5 X Higher risk 2 X Higher risk 2.5 X Higher risk Number of medications Adapted from Ziere et al., 2006
12 If we know so much, why does polypharmacy still happen? More medications available than ever before People are living longer (and acquiring more diseases with more medications) Guidelines tell prescribers when to start drugs but not when to stop them Increased hospital admissions (many prescribers) Fear of rocking the boat Culture of prescribing

13 Change in prescribing culture and patient attitudes to drugs is half the battle: In the late 1970s, benzodiazepines are the most prescribed medication in the world. Women are generally more frequent consumers. 12
14 Challenges and enablers in the literature Prescribers may: Not be aware polypharmacy is a problem Lack confidence for deprescribing Not have the time Be influenced by treatment guidelines Be more likely to deprescribe if raised by a patient And: Want to find ways to examine ongoing need for medication and ways to reduce burden Patients Vast majority willing to reduce or stop a medication if suggested by a prescriber Influenced by physicians, family, friends, media, previous experience May be fearful of deprescribing Supported by knowing there is a process 15 February 2019


15 The Deprescribing Project
16 Deprescribing The planned and supervised process of dose reduction or stopping of medication that may be causing harm or no longer be of benefit. The goal of deprescribing is to reduce medication burden and harm, while maintaining or improving quality of life. Deprescribing is part of good prescribing backing off when doses are too high, or stopping medications that are no longer needed.


17 Making deprescribing decisions Frailty
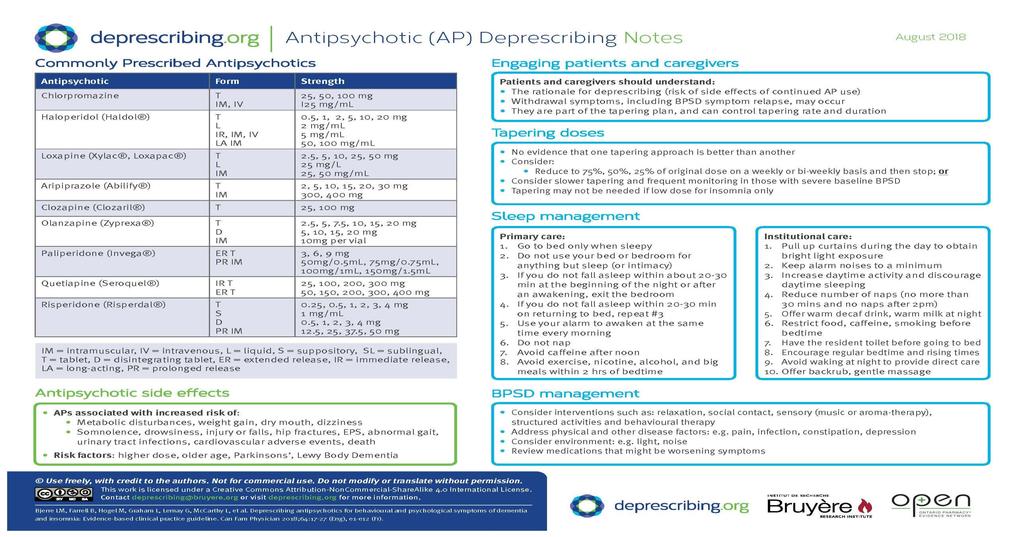
18 The work of the Bruyère Evidence-Based Deprescribing Guidelines team Evidence-based guidelines and algorithms that help health care providers decide when and how to reduce certain medications Benzodiazepine receptor agonists, Antipsychotics, Proton pump inhibitors, Cholinesterase inhibitors and Anti-hyperglycemics ( Spreading the word: reaching out to community groups, engaging policy makers, working with organizations (CaDeN) New research: community engagement, feasibility work in community pharmacy and LTC

19
20

21
22 That s all great, but I am not a pharmacist or doctor 15 February 2019

23 All of us have a role to play in improving medication management: Top Down Professional Bodies & Advisory Groups Policy Makers Administrators Prescribing and Deprescribing Frontline Healthcare Staff Support Staff e.g. PSW, volunteers Ground Up Patients and Caregivers Prescribers

24 The deprescribing process Steps in deprescribing 1. Compile a medication history 2. Identify potentially inappropriate medications, those with less evidence for benefit or those with harm 3. Assess each medication for eligibility for deprescribing 4. Prioritize medications for deprescribing 5. Develop a plan for tapering and monitoring 6. Monitor, support and document care With the patient Scott I et al, Reducing Inappropriate Polypharmacy The Process of Deprescribing, JAMA Int Med 2015 doi: /jamainternmed
25 Medication review identifies: Medications that might be causing problems Medications that are working well Medications that might be beneficial 15 February 2019

26 Steps in a medication review Ask: can this be caused by a drug? Ask: is this drug being used to treat the side effect of another drug? Screen for potentially inappropriate medications Ask: would a medication be useful? I E Indicated? Effective? Time to benefit Goals of care Goals of care Clinical status is the drug working? S Safe? Potential or actual adverse drug effects C Convenient? Pill burden Cost Route
27 Screening criteria Beers ces/uploads/files/pocket%20gui de%20to%202015%20beers%20c riteria.pdf STOPP /2016%20Stopp%20Start%2 0Cumbria.pdf Anticholinergic burden Examples of medications to avoid Benzodiazepines & Z drugs NSAIDs Tricyclic antidepressants (e.g. amitriptyline) First-generation antihistamines Antipsychotics Digoxin





28 1. No benefit Significant toxicity OR no indication OR obvious contraindication OR cascade prescribing? YES Algorithm for deciding order and mode in which drug use could be discontinued Scott et al NO 2. Harm outweighs benefit Adverse effects outweigh symptomatic effect or potential future benefits? YES Withdrawal symptoms or disease recurrence likely if drug therapy discontinued? YES Taper dose and monitor for adverse drug withdrawal effects NO 3. Symptom or disease drugs Symptoms stable or nonexistent? YES NO NO Symptoms stable or nonexistent? 4. Preventive drugs Potential benefit unlikely to be realized because of limited life expectancy? YES YES NO NO Continue drug therapy Discontinue drug therapy Restart drug therapy
29 So what does applying all this information look like in real life? 15 February 2019
 referred to LTC Wheelchair-bound, heavily sedated, interviewing and")
30 Case #1: Tapering of a Benzodiazepine 77 year old woman Falls, pain, constipation, cognition, and polypharmacy PMH: CVD, CAD, hypertension, dementia, fibromyalgia, myositis, bipolar disorder, arthritis, remote duodenal ulcer, hypothyroidism Loss of independence (daily help with washing, dressing and medications) referred to LTC Wheelchair-bound, heavily sedated, interviewing and assessment difficult Near-falls attempting to self-transfer and could not stand unsupported CrCl 30 ml/min Farrell B, French Merkley V, Thompson W. Adding up the impact of medications from multiple prescribers managing polypharmacy. CMAJ 2013;185(14):
31 Her medication list Quinapril 40mg daily Amlodipine 5mg daily Diltiazem ER 360mg daily Acebutolol 200mg twice daily Nitroglycerin patch 0.6mg/h qhs Nitroglycerin 0.4mg spray prn Furosemide 40mg daily Dipyridamole/ASA 200/25 mg bid Rosuvastatin 20mg twice daily Levothyroxine 0.088mg daily Tiotropium 18mcg daily Salbutamol 100mcg, 2 puffs qid prn Galantamine ER 16mg daily Morphine 10mg qhs Acetaminophen 650mg q4-6h prn Cyclobenzaprine 5mg tid Glucosamine 500mg bid Amitriptyline 75mg qhs Oxazepam 15mg qhs Lactulose 15mL daily prn Mg hydroxide 311 mg 1-2 tablets qhs Fibre in water Carter s liver pill 2 pills prn Suppository Cranberry 500mg tid Carbamazepine 200mg bid Omeprazole 20mg daily

32 Interplay between the medications of a 77-year-old woman referred to a geriatric day hospital and their possible effects on sedation, cognition, constipation and risk of falls. Barbara Farrell et al. CMAJ 2013;185: by Canadian Medical Association
33 Making recommendations Identify the problem the patient is having Ask about drugs that might be contributing to that problem Suggest approaches to reducing or stopping the drug Include what you will do to monitor and follow-up on the patient 15 February 2019
34 What would you do? A. Leave everything as is (don t rock the boat) B. Taper the oxazepam C. Stop the amitriptyline D. Choose a different drug to deprescribe

 Overall health and well-being (e.g. general health perception)")
35 Thinking about goals in the elderly and engaging them in the conversation can help prioritize Maintain and improve Physical functioning (e.g. activities of daily living) Psychological functioning (e.g. cognition, depression) Social functioning (e.g. social activities, support systems) Overall health and well-being (e.g. general health perception)
36 What we know about BZRAs BZRA use is common in adults and expensive: In 2012 over 30% of Canadian seniors in LTC and over 15% living in the community used BZRAs ~100 million spent on BZRAs annually in Canada Guidance for use varies: Existing guidelines suggest BZRAs should be used short-term for treatment of insomnia (up to 4 weeks) Some groups recommend avoiding BZRAs all together in older persons, or as last resort for as short a duration as possible Studies detect loss of effect in 7 to 28 days although many stay on agent indefinitely BZRAs are not harmless Chronic BZRA may lead to physical and psychological dependence Associated with increased risk of: falls, motor vehicle accidents, memory problems and daytime sedation, risks that may be increased in the elderly Pottie K, Thompson W, Davies SJC, Grenier J, Sadowski CA, Welch V, Holbrook A, Boyd CM, Swenson JR, Ma A, Farrell B (2016). Evidencebased clinical practice guidelines for deprescribing benzodiazepine receptor agonists. CAN FAM Physician 2018,64:339-51

37 36

38 37

39 15 February 2019
40 Which healthcare provider would not need to consider medication side effects in their assessment of this patient? 1) Physiotherapist 2) Occupational Therapist 3) Speech Language Pathologist 4) None of the above 15 February 2019
41 Back to our patient Taking oxazepam for anxiety and sleep (plus amitriptyline) Before tapering oxazepam, need better approach to manage anxiety (Referrals? What is your expertise?) What non-drug options can you offer?
42 Monitoring when deprescribing It s a collaborative process with the patient, family and all healthcare staff involved with their care Know what should be monitored and when who can help? Communicate why the drug is being stopped Involve your colleagues who could offer nonpharmacological alternatives Document plan and progress for the patient and the care team members 15 February 2019

43 Patient outcome Reduced # from 27 to 17 Berg Balance Score from 18 to 31/56 Wheelchair walker cane No falls from 4th week onward No worsening of pain self-confidence and independence Constipation resolved Resumed old hobbies Improved social interaction Nightime sleeping improved; daytime napping eliminated Cognitive findings in keeping with stroke, not dementia
44 Case #2 87 year old, living independently at home is referred to your community falls program PMHx: HTN, OA, B12 deficiency She has no idea why she is meeting you Her daughter (who has come with her to the appointment) is more concerned about all the falls her mom has been having over the last 4 months 15 February 2019
45 Case #2 Upon further discussion about the falls, Mrs. PH tries to downplay them, but you were able to get the following history: First fall was about 4 months ago after she tripped on a rug At that time, she started having more pain, but reports that any X-ray done by her family doctor was normal Since then, she has had about 2 falls a month, usually in the morning or when she changes positions quickly; with the last one a week ago More and more she feels dizzy and foggy in her mind; her legs are also more swollen and feel very heavy when she moves 15 February 2019
46 Her medication list Amlodipine 5mg daily Lorazepam 2 mg at bedtime as needed Ibuprofen 200mg 3 times a day regularly (OTC) ASA 81mg daily (OTC) Omeprazole 20mg daily (OTC) Vitamin B mcg daily 15 February 2019
47 The trickle effect Decreased B12 absorption Vitamin B12 Increased fracture risk if use chronic ASA Amlodipine Lorazepam Fall Increased pain Ibuprofen Stomach upset BP increases Omeprazole Amlodipine increased Postural hypotension and falls risk Increased leg swelling 15 February 2019
48 Which drug would you think about starting a deprescribing conversation about first? 1) Lorazepam 2) Ibuprofen (switch to Acetaminophen instead) 3) Nothing as I am not a pharmacist

49 You are thinking that deprescribing her lorazepam is a good idea 15 February 2019



50 You are so excited to talk to her about stopping her lorazepam 15 February 2019


51 Collaborative Care: the Client and Caregiver experience We know stuff. Patient Lived Experience Professionals Illness Experts I know me.

52 Patient barriers Poor understanding of rationale and when appropriate Not being involved in planning Not knowing options if symptoms return Help patient/family understand why deprescribing is being considered and involve in planning Drugs Aging 2013;DOI /s
:7-9, Table 2.")
53 Examples of How to Discuss Deprescribing with Patients Barbara Farrell, Dee Mangin. Am Fam Physician Jan 1;99(1):7-9, Table February 2019
54 Advocating for clients: You know your patients in their home environment and know how to navigate the healthcare system Educate where you can to empower them or their caregivers about medication side effects Reach out where possible to the family physician identifying the concerns Involve your healthcare team where possible (e.g. pharmacist MedsCheck at Home for complex cases, involving OT, PT, SW to help with non-pharm options for pain) February 2019

 15")
55 Food for thought Know what motivates your patient Plant the seed -offer patient information sheets -rebook another appointment to revisit the issue Engage others to have the same message -family or caregivers -your clinic staff and colleagues -community healthcare providers that you make referrals to (RPh, PT, OT, CCAC) 15 February 2019

56 Food for thought Be transparent about the process -trial and error -offer alternatives Build on successes -pick the lowest hanging fruit first 15 February 2019


57 Food for thought Try to prevent the problem in the future: -set expectations with drug therapy initiation -ensure other HCPs in the circle of care are kept up to date -encourage patients to ask questions about their medications 15 February 2019
58 Further helpful resources Deprescribing Guidelines Research Website: Canadian Deprescribing Network Website: Choosing Wisely Canada Website: Institute of Safe Medication Practices Canada Website: 15 February 2019
59 So what is your story?










60 Acknowledgments Deprescribing guidelines developed with funding from the Government of Ontario*, the Ontario Pharmacy Research Collaboration and Canadian Institutes of Health Research *The views expressed in this presentation are the views of the author(s)/presenter(s) and do not necessarily reflect those of the Province.

61

62
63 Questions? Type your questions into the chat box. OR Dial *7 on your telephone to unmute. Dial *6 when you are finished speaking to re-mute. THIS WEBINAR IS BEING RECORDED. THE SLIDE DECK AND RECORDING WILL BE ED AFTER THE WEBINAR. THIS WEBINAR IS BEING RECORDED. Webinar technology managed by:
DEPRESCRIBING IN THE ELDERLY
 DEPRESCRIBING IN THE ELDERLY G E R I A T R I C S R E F R E S H E R D A Y W E D N E S D A Y, A P R I L 5 TH, 2 0 1 7 V É R O N I Q U E F R E N C H M E R K L E Y, M D, C C F P ( C O E ) B R U Y È R E C O
DEPRESCRIBING IN THE ELDERLY G E R I A T R I C S R E F R E S H E R D A Y W E D N E S D A Y, A P R I L 5 TH, 2 0 1 7 V É R O N I Q U E F R E N C H M E R K L E Y, M D, C C F P ( C O E ) B R U Y È R E C O
Disclosure. The elderly at risk: reducing medications safely to meet life s changes. Relevant financial relationships.
 The elderly at risk: reducing medications safely to meet life s changes Barbara Farrell BScPhm, PharmD, FCSHP European Society of Hospital Pharmacists Conference March 2017 Disclosure Relevant financial
The elderly at risk: reducing medications safely to meet life s changes Barbara Farrell BScPhm, PharmD, FCSHP European Society of Hospital Pharmacists Conference March 2017 Disclosure Relevant financial
David Gardner, BSc Pharm, MSc CH&E, PharmD Professor, Department of Psychiatry & College of Pharmacy
 David Gardner, BSc Pharm, MSc CH&E, PharmD Professor, Department of Psychiatry & College of Pharmacy It s no dream. Sleep well without sleeping pills. Outline Baby boomers & beyond: medication use Deprescribing
David Gardner, BSc Pharm, MSc CH&E, PharmD Professor, Department of Psychiatry & College of Pharmacy It s no dream. Sleep well without sleeping pills. Outline Baby boomers & beyond: medication use Deprescribing
Polypharmacy and Polymorbid Patients: Practical Tips and Tricks
 Polypharmacy and Polymorbid Patients: Practical Tips and Tricks November 2, 2013 Faculty/Presenter Disclosure Faculty: Chris Fan-Lun, BScPhm, ACPR, CGP Pharmacist - Geriatric Medicine Clinical Practice
Polypharmacy and Polymorbid Patients: Practical Tips and Tricks November 2, 2013 Faculty/Presenter Disclosure Faculty: Chris Fan-Lun, BScPhm, ACPR, CGP Pharmacist - Geriatric Medicine Clinical Practice
Deconstructing Polypharmacy. Alan B. Douglass, M.D. Director
 Deconstructing Polypharmacy Alan B. Douglass, M.D. Director Recognize this patient? Mrs. Brown- 82 years young Active Medical Problems Hypertension Hyperlipidemia Type 2 Diabetes Peripheral edema Osteoarthritis
Deconstructing Polypharmacy Alan B. Douglass, M.D. Director Recognize this patient? Mrs. Brown- 82 years young Active Medical Problems Hypertension Hyperlipidemia Type 2 Diabetes Peripheral edema Osteoarthritis
About ISMP Canada. Analysis Outputs: Safety Bulletins. Less is More: An Introduction to Deprescribing. canada.org
 Less is More: An Introduction to Deprescribing Lindsay Yoo, BSc, BScPhm, RPh, CDE, CGP, PharmD Medication Safety Analyst, ISMP Canada About ISMP Canada The Institute for Safe Medication Practices Canada
Less is More: An Introduction to Deprescribing Lindsay Yoo, BSc, BScPhm, RPh, CDE, CGP, PharmD Medication Safety Analyst, ISMP Canada About ISMP Canada The Institute for Safe Medication Practices Canada
If a bad thing is happening to a patient, a drug did it until proven otherwise
 Dr Vicki s First Rule of Geriatrics Deprescribing in the Elderly Victoria Braund MD, FACP, CMD Director, Division of Geriatrics NorthShore University HealthSystem Medical Director, Brandel Health & Rehab
Dr Vicki s First Rule of Geriatrics Deprescribing in the Elderly Victoria Braund MD, FACP, CMD Director, Division of Geriatrics NorthShore University HealthSystem Medical Director, Brandel Health & Rehab
Deprescribing Unnecessary Medications: A Four-Part Process
 Deprescribing Unnecessary Medications: A Four-Part Process Scott Endsley, MD Fam Pract Manag. 2018;25(3):28-32. Abstract and Introduction Introduction www.medscape.com Ms. Horatio is a 76-year-old patient
Deprescribing Unnecessary Medications: A Four-Part Process Scott Endsley, MD Fam Pract Manag. 2018;25(3):28-32. Abstract and Introduction Introduction www.medscape.com Ms. Horatio is a 76-year-old patient
Less is More: Introduction to Deprescribing
 Less is More: Introduction to Deprescribing 7th Annual Pharmaceutical Care Conference Muscat, Oman Feb 23, 2017 Lindsay Yoo, BSc, BScPhm, RPh, CDE, CGP, PharmD Medication Safety Analyst, ISMP Canada About
Less is More: Introduction to Deprescribing 7th Annual Pharmaceutical Care Conference Muscat, Oman Feb 23, 2017 Lindsay Yoo, BSc, BScPhm, RPh, CDE, CGP, PharmD Medication Safety Analyst, ISMP Canada About
START, STOPP, Beers Oh My! Navigating the World of Geriatric Pharmacy
 START, STOPP, Beers Oh My! Navigating the World of Geriatric Pharmacy Jessica DiLeo, PharmD Kate Murphy, PharmD OBJECTIVES Identify pharmacodynamic and pharmacokinetic parameters that may influence treatment
START, STOPP, Beers Oh My! Navigating the World of Geriatric Pharmacy Jessica DiLeo, PharmD Kate Murphy, PharmD OBJECTIVES Identify pharmacodynamic and pharmacokinetic parameters that may influence treatment
A C A D E M I C D E TA I L I N G C H O O S I N G W I S E LY C O N F E R E N C E O C T 2 1, PA M M C L E A N - V E Y S E Y B S C P H A R M D R
 PPI DEPRESCRIBING Canadian Deprescribing Network (CaDeN) goals are to: Reduce harm by raising awareness and cutting risky prescriptions for seniors by 50% by 2020. Promote health by ensuring access to
PPI DEPRESCRIBING Canadian Deprescribing Network (CaDeN) goals are to: Reduce harm by raising awareness and cutting risky prescriptions for seniors by 50% by 2020. Promote health by ensuring access to
GRADE, EBM and Deprescribing. Kevin Pottie MD CCFP, MClSc, FCFP Associate Professor, Family Medicine, University of Ottawa
 GRADE, EBM and Deprescribing Kevin Pottie MD CCFP, MClSc, FCFP Associate Professor, Family Medicine, University of Ottawa Research is like turning on the light before you clean up the room: it doesn t
GRADE, EBM and Deprescribing Kevin Pottie MD CCFP, MClSc, FCFP Associate Professor, Family Medicine, University of Ottawa Research is like turning on the light before you clean up the room: it doesn t
BLCS 1-Clinical Overview. Dr. Chris Rauscher Clinical Lead Shared Care Polypharmacy Risk Reduction Initiative
 BLCS 1-Clinical Overview Dr. Chris Rauscher Clinical Lead Shared Care Polypharmacy Risk Reduction Initiative Fraser Health Guide To Person-Centered Medication Decisions Factors to Consider When Systematically
BLCS 1-Clinical Overview Dr. Chris Rauscher Clinical Lead Shared Care Polypharmacy Risk Reduction Initiative Fraser Health Guide To Person-Centered Medication Decisions Factors to Consider When Systematically
Optimizing medication in caring for seniors living with frailty: Five perspectives
 Optimizing medication in caring for seniors living with frailty: Five perspectives Community Care Shanna Trenaman BScH, BScPharm, MAHSR, ACPR, PhD(student) Project Manager for A Collaborative Intervention
Optimizing medication in caring for seniors living with frailty: Five perspectives Community Care Shanna Trenaman BScH, BScPharm, MAHSR, ACPR, PhD(student) Project Manager for A Collaborative Intervention
Deprescribing in CKD patients: Is less more? Speaker: Dr. Judith G. Marin, PharmD
 2016 Deprescribing in CKD patients: Is less more? Speaker: Dr. Judith G. Marin, PharmD Case Mr. Kid Ney is a 75 y/o patient who has been on dialysis for the last 4 years (PD, then HD). PMHx: HTN, DM,
2016 Deprescribing in CKD patients: Is less more? Speaker: Dr. Judith G. Marin, PharmD Case Mr. Kid Ney is a 75 y/o patient who has been on dialysis for the last 4 years (PD, then HD). PMHx: HTN, DM,
Geriatric Pharmacology
 Geriatric Pharmacology Janice Scheufler R.Ph.,PharmD, FASCP Clinical Pharmacist Hospice of the Western Reserve Objectives List three risk factors for adverse drug events in the elderly Discuss two physiological
Geriatric Pharmacology Janice Scheufler R.Ph.,PharmD, FASCP Clinical Pharmacist Hospice of the Western Reserve Objectives List three risk factors for adverse drug events in the elderly Discuss two physiological
Polypharmacy & De-prescribing In Older Adults
 Polypharmacy & De-prescribing In Older Adults Maryland Association of Osteopathic Physicians Annual Meeting September 15, 2018 Elizabeth Phung, DO Lead Clinical Associate Physician Beacham Center for Geriatric
Polypharmacy & De-prescribing In Older Adults Maryland Association of Osteopathic Physicians Annual Meeting September 15, 2018 Elizabeth Phung, DO Lead Clinical Associate Physician Beacham Center for Geriatric
Meds and Falls: Keep in Step with your Meds
 Meds and Falls: Keep in Step with your Meds Donna Bartlett PharmD, CGP, RPh Associate Professor-Pharmacy Practice MCPHS University Clinical Pharmacist-MCPHS University- Pharmacy Outreach Program donna.bartlett@mcphs.edu
Meds and Falls: Keep in Step with your Meds Donna Bartlett PharmD, CGP, RPh Associate Professor-Pharmacy Practice MCPHS University Clinical Pharmacist-MCPHS University- Pharmacy Outreach Program donna.bartlett@mcphs.edu
Katee Kindler, PharmD, BCACP
 Speaker Introduction Katee Kindler, PharmD, BCACP Current Practice: Clinical Pharmacy Specialist Ambulatory Care, St. Vincent Indianapolis Assistant Professor of Pharmacy Practice, Manchester University,
Speaker Introduction Katee Kindler, PharmD, BCACP Current Practice: Clinical Pharmacy Specialist Ambulatory Care, St. Vincent Indianapolis Assistant Professor of Pharmacy Practice, Manchester University,
Shared decision making for stepdown and stopping decisions. Michael R. Gionfriddo Pharm.D, Ph.D Geisinger Center for Pharmacy Innovation and Outcomes
 Shared decision making for stepdown and stopping decisions Michael R. Gionfriddo Pharm.D, Ph.D Geisinger Center for Pharmacy Innovation and Outcomes 1 Disclosures I have had travel and lodging paid for
Shared decision making for stepdown and stopping decisions Michael R. Gionfriddo Pharm.D, Ph.D Geisinger Center for Pharmacy Innovation and Outcomes 1 Disclosures I have had travel and lodging paid for
Geriatric Pharmacology. Kwi Bulow, M.D. Clinical Professor of Medicine Director, Academic Geriatric Resource Center
 Geriatric Pharmacology Kwi Bulow, M.D. Clinical Professor of Medicine Director, Academic Geriatric Resource Center Silver Tsunami 2010: 40 million (13%) 2030: 72 million (20%) Baby Boomers (1946-1964)
Geriatric Pharmacology Kwi Bulow, M.D. Clinical Professor of Medicine Director, Academic Geriatric Resource Center Silver Tsunami 2010: 40 million (13%) 2030: 72 million (20%) Baby Boomers (1946-1964)
POLYPHARMACY. A practical approach to deprescribing in care homes. Care Home Pharmacy Team. Herts Valleys Clinical Commissioning Group
 POLYPHARMACY A practical approach to deprescribing in care homes. Care Home Pharmacy Team Herts Valleys Clinical Commissioning Group Neeta Gulhane Specialist Pharmaceutical Advisor Care Homes The Care
POLYPHARMACY A practical approach to deprescribing in care homes. Care Home Pharmacy Team Herts Valleys Clinical Commissioning Group Neeta Gulhane Specialist Pharmaceutical Advisor Care Homes The Care
Transitions of Care & Medication Reconciliation Ashley King, PharmD, BCGP Clinical Pharmacist LECOM Health March 2018
 Transitions of Care & Medication Reconciliation Ashley King, PharmD, BCGP Clinical Pharmacist LECOM Health March 2018 Objectives Identify when to complete medication reconciliation Understand the importance
Transitions of Care & Medication Reconciliation Ashley King, PharmD, BCGP Clinical Pharmacist LECOM Health March 2018 Objectives Identify when to complete medication reconciliation Understand the importance
Preventing Falls in Older Adults A Matter of Safety
 Preventing Falls in Older Adults A Matter of Safety Roger Tam, BSc. Pharm. Wal-Mart Clinical Designated Pharmacist Falls Prevention Pharmacist Specialist NCCHC-Pre/Post Test Educator Q.U.I.T Educator Overview
Preventing Falls in Older Adults A Matter of Safety Roger Tam, BSc. Pharm. Wal-Mart Clinical Designated Pharmacist Falls Prevention Pharmacist Specialist NCCHC-Pre/Post Test Educator Q.U.I.T Educator Overview
TOP 5 DRUGS.. TO AVOID IN THE ELDERLY
 TOP 5 DRUGS.. TO AVOID IN THE ELDERLY Debbie Kwan, BScPhm., MSc., FCSHP Canadian Geriatrics Society, April 20, 2013 Disclosure of Potential for Conflict of Interest: Financial Disclosure: None Mar 26,
TOP 5 DRUGS.. TO AVOID IN THE ELDERLY Debbie Kwan, BScPhm., MSc., FCSHP Canadian Geriatrics Society, April 20, 2013 Disclosure of Potential for Conflict of Interest: Financial Disclosure: None Mar 26,
Reviewing Medicines in at risk patients care homes
 Reviewing Medicines in at risk patients care homes Clinical Medication Reviews by Pharmacists in Collaboration with GP Surgeries across Brighton and Hove CCG Liz Butterfield FRPharmS 19th April 2016 NICE:
Reviewing Medicines in at risk patients care homes Clinical Medication Reviews by Pharmacists in Collaboration with GP Surgeries across Brighton and Hove CCG Liz Butterfield FRPharmS 19th April 2016 NICE:
Mucky Meds: A (practical) approach the nightmare med list. Michelle Gibson, MD, CCFP (COE), FCFP and Erin Beattie, MD, CCFP
 approach the nightmare med list. Michelle Gibson, MD, CCFP (COE), FCFP and Erin Beattie, MD, CCFP") Mucky Meds: A (practical) approach the nightmare med list Michelle Gibson, MD, CCFP (COE), FCFP and Erin Beattie, MD, CCFP Faculty/Presenter Disclosure Faculty: Michelle Gibson Relationships with financial
Mucky Meds: A (practical) approach the nightmare med list Michelle Gibson, MD, CCFP (COE), FCFP and Erin Beattie, MD, CCFP Faculty/Presenter Disclosure Faculty: Michelle Gibson Relationships with financial
Polypharmacy in the Elderly
 Polypharmacy in the Elderly Physiotherapy Alberta Conference September 24 th 2016 Lesley Charles Associate Professor and Program Director Division of Care of the Elderly Department of Family Medicine,
Polypharmacy in the Elderly Physiotherapy Alberta Conference September 24 th 2016 Lesley Charles Associate Professor and Program Director Division of Care of the Elderly Department of Family Medicine,
Doreen Wan-Chow-Wah, MD, FRCPC Assistant Professor, Division of Geriatric Medicine, Department of Medicine McGill University Health Center Associate
 Doreen Wan-Chow-Wah, MD, FRCPC Assistant Professor, Division of Geriatric Medicine, Department of Medicine McGill University Health Center Associate member, Department of Oncology McGill University Medical
Doreen Wan-Chow-Wah, MD, FRCPC Assistant Professor, Division of Geriatric Medicine, Department of Medicine McGill University Health Center Associate member, Department of Oncology McGill University Medical
Early Intervention the Key to Geriatric Assessment: Geriatric Assessment Outreach Teams
 Early Intervention the Key to Geriatric Assessment: Geriatric Assessment Outreach Teams Regional Geriatric Program of Eastern Ontario Outpatient Clinics Geriatric Rehabilitation Unit Community Referrals
Early Intervention the Key to Geriatric Assessment: Geriatric Assessment Outreach Teams Regional Geriatric Program of Eastern Ontario Outpatient Clinics Geriatric Rehabilitation Unit Community Referrals
Optimising Safe & Appropriate Medicines Use and Deprescribing. Katie Smith, Director, East Anglia Medicines Information Service February 2014
 Optimising Safe & Appropriate Medicines Use and Deprescribing Katie Smith, Director, East Anglia Medicines Information Service February 2014 Background Objectives How & why the OSAMU document was developed
Optimising Safe & Appropriate Medicines Use and Deprescribing Katie Smith, Director, East Anglia Medicines Information Service February 2014 Background Objectives How & why the OSAMU document was developed
The Use of Sleep Aids in Our Society Today
 The Use of Sleep Aids in Our Society Today Kathryn Hansen, BS, CPC, CPMA, REEGT Integration Consultants, LLC Sleep Education Partners Executive Director Kentucky Sleep Society Executive Director Society
The Use of Sleep Aids in Our Society Today Kathryn Hansen, BS, CPC, CPMA, REEGT Integration Consultants, LLC Sleep Education Partners Executive Director Kentucky Sleep Society Executive Director Society
Taking the harm out of Polypharmacy Step by step. Karen Reid and Claire Stein Lead Integrated Care Pharmacist NHS Lothian
 Taking the harm out of Polypharmacy Step by step Karen Reid and Claire Stein Lead Integrated Care Pharmacist NHS Lothian Presentation: Polypharmacy Overview of the 2015 guidelines The Seven Steps Application
Taking the harm out of Polypharmacy Step by step Karen Reid and Claire Stein Lead Integrated Care Pharmacist NHS Lothian Presentation: Polypharmacy Overview of the 2015 guidelines The Seven Steps Application
A Geriatrician s Perspective on Successful Aging. Ariel Green, MD, MPH Assistant Professor of Medicine
 A Geriatrician s Perspective on Successful Aging Ariel Green, MD, MPH Assistant Professor of Medicine 1 Disclosures Johns Hopkins Clinical Research Scholars Program American College of Cardiology Foundation
A Geriatrician s Perspective on Successful Aging Ariel Green, MD, MPH Assistant Professor of Medicine 1 Disclosures Johns Hopkins Clinical Research Scholars Program American College of Cardiology Foundation
< = > less is more. De-diagnosing De-prescribing Non-testing
 < = > less is more De-diagnosing De-prescribing Non-testing Who says? Overdiagnosis Polypharmacy False positives Too much medicine Risk aversion $$$ Sources Prof David Le Couteur, Clin Pharm and Aged Care
< = > less is more De-diagnosing De-prescribing Non-testing Who says? Overdiagnosis Polypharmacy False positives Too much medicine Risk aversion $$$ Sources Prof David Le Couteur, Clin Pharm and Aged Care
Evidence-Based Clinical Practice Guideline for Deprescribing Cholinesterase Inhibitors and Memantine in People with Dementia
 Evidence-Based Clinical Practice Guideline for Deprescribing Cholinesterase Inhibitors and Memantine in People with Dementia ADI 2018, Chicago FACULTY OF MEDICINE Dr Emily Reeve NHMRC Cognitive Decline
Evidence-Based Clinical Practice Guideline for Deprescribing Cholinesterase Inhibitors and Memantine in People with Dementia ADI 2018, Chicago FACULTY OF MEDICINE Dr Emily Reeve NHMRC Cognitive Decline
Managing Polypharmacy in the Elderly March 21, Barbara Farrell BScPhm, PharmD, FCSHP Pharmacist, Bruyère Geriatric Day Hospital
 Managing Polypharmacy in the Elderly March 21, 2012 Barbara Farrell BScPhm, PharmD, FCSHP Pharmacist, Bruyère Geriatric Day Hospital Objectives Participants will be able to: Describe the impact of polypharmacy
Managing Polypharmacy in the Elderly March 21, 2012 Barbara Farrell BScPhm, PharmD, FCSHP Pharmacist, Bruyère Geriatric Day Hospital Objectives Participants will be able to: Describe the impact of polypharmacy
Supplemental materials for:
 Supplemental materials for: Wallis KA, Andrews A, Henderson M. Swimming against the tide: primary care physicians views on deprescribing in everyday practice. Ann Fam Med. 2017;15(4):341-346. General Practice
Supplemental materials for: Wallis KA, Andrews A, Henderson M. Swimming against the tide: primary care physicians views on deprescribing in everyday practice. Ann Fam Med. 2017;15(4):341-346. General Practice
Polypharmacy and the Older Adult. Leslie Baker, PharmD, BCGP Umanga Sharma, MD
 Polypharmacy and the Older Adult Leslie Baker, PharmD, BCGP Umanga Sharma, MD Objectives Identify what polypharmacy is Identify factors leading to polypharmacy Discuss consequences of polypharmacy Identify
Polypharmacy and the Older Adult Leslie Baker, PharmD, BCGP Umanga Sharma, MD Objectives Identify what polypharmacy is Identify factors leading to polypharmacy Discuss consequences of polypharmacy Identify
PRESCRIBING IN THE ELDERLY. CARE HOME PHARMACY TEAM Bhavini Shah, Eleesha Pentiah & Puja Vyas
 PRESCRIBING IN THE ELDERLY CARE HOME PHARMACY TEAM Bhavini Shah, Eleesha Pentiah & Puja Vyas LEARNING OUTCOMES Medicines Optimisation The effects of aging on health and medicines. Polypharmacy Acute Kidney
PRESCRIBING IN THE ELDERLY CARE HOME PHARMACY TEAM Bhavini Shah, Eleesha Pentiah & Puja Vyas LEARNING OUTCOMES Medicines Optimisation The effects of aging on health and medicines. Polypharmacy Acute Kidney
Let it go! Rationalising medicines for patients with life limiting illness
 Let it go! Rationalising medicines for patients with life limiting illness Inga Andrew Senior Clinical Pharmacist Northumbria Healthcare Trust E-mail: inga_andrew@northumbria-healthcare.nhs.uk Welcome
Let it go! Rationalising medicines for patients with life limiting illness Inga Andrew Senior Clinical Pharmacist Northumbria Healthcare Trust E-mail: inga_andrew@northumbria-healthcare.nhs.uk Welcome
A Step Forward: Promoting Independence through Falls Prevention
 A Step Forward: Promoting Independence through Falls Prevention 2014 Geriatric Update Meharry Consortium Geriatric Education Center A Step Forward: Promoting Independence through Falls Prevention Moderator:
A Step Forward: Promoting Independence through Falls Prevention 2014 Geriatric Update Meharry Consortium Geriatric Education Center A Step Forward: Promoting Independence through Falls Prevention Moderator:
Transforming Care for the Elderly
 Transforming Care for the Elderly Session 2: Engaging Pharmacists & Interdisciplinary Care Teams to Improve Prescribing of Antipsychotics & to Reduce Polypharmacy January 11, 2017 3 @cfhi_fcass Welcome
Transforming Care for the Elderly Session 2: Engaging Pharmacists & Interdisciplinary Care Teams to Improve Prescribing of Antipsychotics & to Reduce Polypharmacy January 11, 2017 3 @cfhi_fcass Welcome
Potentially Inappropriate Medications in Elderly Patients: Prevalence at Admission and Changes During Hospital Stay
 Potentially Inappropriate Medications in Elderly Patients: Prevalence at Admission and Changes During Hospital Stay Background Polypharmacy in the Elderly 40% seniors are using 5-9 different classes of
Potentially Inappropriate Medications in Elderly Patients: Prevalence at Admission and Changes During Hospital Stay Background Polypharmacy in the Elderly 40% seniors are using 5-9 different classes of
Post Fall- Preventing Future Falls. A look at process- everyone's responsibility.
 Post Fall- Preventing Future Falls. A look at process- everyone's responsibility. Thursday, November 15, 2018 Daphne Kemp THIS WEBINAR IS BEING RECORDED. THE SLIDE DECK AND RECORDING WILL BE EMAILED AFTER
Post Fall- Preventing Future Falls. A look at process- everyone's responsibility. Thursday, November 15, 2018 Daphne Kemp THIS WEBINAR IS BEING RECORDED. THE SLIDE DECK AND RECORDING WILL BE EMAILED AFTER
IMPROVING MEDICATION SAFETY AMONG ELDERLY PATIENTS IN AN AMBULATORY SETTING. Alyssa Berry, Rebecca Burgett, Erin Day, Aron Hrubetz
 IMPROVING MEDICATION SAFETY AMONG ELDERLY PATIENTS IN AN AMBULATORY SETTING Alyssa Berry, Rebecca Burgett, Erin Day, Aron Hrubetz Improving Medication Safety Among Elderly Patients in an Ambulatory Setting
IMPROVING MEDICATION SAFETY AMONG ELDERLY PATIENTS IN AN AMBULATORY SETTING Alyssa Berry, Rebecca Burgett, Erin Day, Aron Hrubetz Improving Medication Safety Among Elderly Patients in an Ambulatory Setting
DEPRESCRIBING. Phil St John CSIM Workshop
 DEPRESCRIBING Phil St John CSIM Workshop Conflict of Interest Disclosure Consultant for: none Speaker for: none Received grant/research support from: CIHR, MHRC, Riverview Foundation Received honoraria
DEPRESCRIBING Phil St John CSIM Workshop Conflict of Interest Disclosure Consultant for: none Speaker for: none Received grant/research support from: CIHR, MHRC, Riverview Foundation Received honoraria
Using Deprescribing Guidelines in Long-Term Care: The Ottawa Experience
 Using Deprescribing Guidelines in Long-Term Care: The Ottawa Experience Barbara Farrell, BScPhm, Pharm D, FCSHP James Conklin, PhD Bruyère Research Institute, Ottawa Co-authors: Hannah Irving, Lalitha
Using Deprescribing Guidelines in Long-Term Care: The Ottawa Experience Barbara Farrell, BScPhm, Pharm D, FCSHP James Conklin, PhD Bruyère Research Institute, Ottawa Co-authors: Hannah Irving, Lalitha
Demystifying the Complex Patient
 Demystifying the Complex Patient Jay Reaume, BSc, BScPhm, RPh, CDE Suzanne Singh, BScPhm, ACPR, PharmD, RPh May 30, 2015 Disclosures Jay Reaume No conflicts of interest to disclose Suzanne Singh No conflicts
Demystifying the Complex Patient Jay Reaume, BSc, BScPhm, RPh, CDE Suzanne Singh, BScPhm, ACPR, PharmD, RPh May 30, 2015 Disclosures Jay Reaume No conflicts of interest to disclose Suzanne Singh No conflicts
Polypharmacy. in the Elderly. Lesley Charles, MBChB, CCFP
 Polypharmacy in the Elderly Lesley Charles, MBChB, CCFP Associate Professor and Program Director Division of Care of the Elderly Department of Family Medicine, University of Alberta March 06, 2016 1 Faculty/Presenter
Polypharmacy in the Elderly Lesley Charles, MBChB, CCFP Associate Professor and Program Director Division of Care of the Elderly Department of Family Medicine, University of Alberta March 06, 2016 1 Faculty/Presenter
Anthony J. Caprio, MD, CMD, AGSF 1
 Objectives 1) Discuss the dangers of polypharmacy 2) Review potentially inappropriate medications for older adults Doc, I think I am taking too many medications! 3) Develop strategies for prioritizing
Objectives 1) Discuss the dangers of polypharmacy 2) Review potentially inappropriate medications for older adults Doc, I think I am taking too many medications! 3) Develop strategies for prioritizing
Rebecca Rottman-Sagebiel, Pharm.D., BCPS Sharon Jung Tschirhart, Pharm.D., BCPS Geriatric Clinical Pharmacy Specialists STVHCS, Audie L.
 Rebecca Rottman-Sagebiel, Pharm.D., BCPS Sharon Jung Tschirhart, Pharm.D., BCPS Geriatric Clinical Pharmacy Specialists STVHCS, Audie L. Murphy Division Clinical Assistant Professors, University of Texas/UTHSCSA
Rebecca Rottman-Sagebiel, Pharm.D., BCPS Sharon Jung Tschirhart, Pharm.D., BCPS Geriatric Clinical Pharmacy Specialists STVHCS, Audie L. Murphy Division Clinical Assistant Professors, University of Texas/UTHSCSA
Polypharmacy. A CPPE distance learning programme
 A CPPE distance learning programme DLP 177 January 2016 Contents About CPPE distance learning programmes About this learning programme Glossary of key terms v vii ix Contents Section 1 The problem with
A CPPE distance learning programme DLP 177 January 2016 Contents About CPPE distance learning programmes About this learning programme Glossary of key terms v vii ix Contents Section 1 The problem with
Dementia is an overall term for a set of symptoms that is caused by disorders affecting the brain.
 Vascular Dementia Vascular Dementia Other Dementias This information sheet provides an overview of a type of dementia known as vascular dementia. In this information sheet you will find: An overview of
Vascular Dementia Vascular Dementia Other Dementias This information sheet provides an overview of a type of dementia known as vascular dementia. In this information sheet you will find: An overview of
Deprescribing with Confidence Dr Sanjay Suman MD FRCP
 Deprescribing with Confidence Dr Sanjay Suman MD FRCP Clinical Director Elderly Care and Stroke Medway NHS Foundation Trust Kent 45% of all medications prescribed for 65 years 1 1. Wynne et al Maturitas
Deprescribing with Confidence Dr Sanjay Suman MD FRCP Clinical Director Elderly Care and Stroke Medway NHS Foundation Trust Kent 45% of all medications prescribed for 65 years 1 1. Wynne et al Maturitas
Medications for Alzheimer s disease: are they right for you?
 Medications for Alzheimer s disease: are they right for you? There are no medications today that can cure Alzheimer s disease. But there are currently four medications approved by Health Canada which can
Medications for Alzheimer s disease: are they right for you? There are no medications today that can cure Alzheimer s disease. But there are currently four medications approved by Health Canada which can
Multifactorial risk assessments and evidence-based interventions to address falls in primary care. Objectives. Importance
 Multifactorial risk assessments and evidence-based interventions to address falls in primary care Sarah Ross, DO, MS Assistant Professor Internal Medicine, Geriatrics Nicoleta Bugnariu, PT, PhD Associate
Multifactorial risk assessments and evidence-based interventions to address falls in primary care Sarah Ross, DO, MS Assistant Professor Internal Medicine, Geriatrics Nicoleta Bugnariu, PT, PhD Associate
Polypharmacy in the Elderly
 Polypharmacy in the Elderly Or How Scotland invented the Modern World Sir William Ferguson Anderson 1914-2001 Became the first Professor of Geriatrics in the world when he was appointed to the David Cargill
Polypharmacy in the Elderly Or How Scotland invented the Modern World Sir William Ferguson Anderson 1914-2001 Became the first Professor of Geriatrics in the world when he was appointed to the David Cargill
The Use, Misuse and Abuse of Alcohol, and Psychoactive Drugs among Older Persons
 The Use, Misuse and Abuse of Alcohol, and Psychoactive Drugs among Older Persons Alison A. Moore, MD, MPH Division of Geriatric Medicine David Geffen School of Medicine at UCLA Drinking in Older Adults:
The Use, Misuse and Abuse of Alcohol, and Psychoactive Drugs among Older Persons Alison A. Moore, MD, MPH Division of Geriatric Medicine David Geffen School of Medicine at UCLA Drinking in Older Adults:
Thank You to Our Sponsors: Evaluations & CE Credits. Featured Speakers. Conflict of Interest & Disclosure Statements 10/18/2016
 Thank You to Our Sponsors: University at Albany School of Public Health NYS Department of Health Conflict of Interest & Disclosure Statements The planners and presenters do not have any financial arrangements
Thank You to Our Sponsors: University at Albany School of Public Health NYS Department of Health Conflict of Interest & Disclosure Statements The planners and presenters do not have any financial arrangements
Medication Use in Older Adults
 Medication Use in Older Adults F. Michael Gloth, III, MD, AGSF, FACP, CMD Clinical Professor Department of Geriatrics, Florida State University College of Medicine Associate Professor of Medicine Division
Medication Use in Older Adults F. Michael Gloth, III, MD, AGSF, FACP, CMD Clinical Professor Department of Geriatrics, Florida State University College of Medicine Associate Professor of Medicine Division
Medication Management When Caring for Seniors at Home
 Medication Management When Caring for Seniors at Home White Paper May 24, 2013 2013 Physician s Choice Private Duty http://private-duty.pchhc.com 1 Proper medication management for seniors who live at
Medication Management When Caring for Seniors at Home White Paper May 24, 2013 2013 Physician s Choice Private Duty http://private-duty.pchhc.com 1 Proper medication management for seniors who live at
Diagnostics and therapeutic decision making. Linda Nazarko. London Northwest Healthcare NHS Trust
 Diagnostics and therapeutic decision making Linda Nazarko London Northwest Healthcare NHS Trust Aims and objectives To be aware of: The value of consultation models The importance of history taking How
Diagnostics and therapeutic decision making Linda Nazarko London Northwest Healthcare NHS Trust Aims and objectives To be aware of: The value of consultation models The importance of history taking How
Adjusting and Withdrawing Medications in the Elderly
 Adjusting and Withdrawing Medications in the Elderly Louise Mallet, B.Sc.Pharm., Pharm.D., CGP Professor in Clinical Pharmacy, Faculty of Pharmacy, University of Montreal Clinical Pharmacist in Geriatrics,
Adjusting and Withdrawing Medications in the Elderly Louise Mallet, B.Sc.Pharm., Pharm.D., CGP Professor in Clinical Pharmacy, Faculty of Pharmacy, University of Montreal Clinical Pharmacist in Geriatrics,
Canadian Deprescribing Network
 Canadian Deprescribing Network 2017 Annual Report 1 What s deprescribing? Deprescribing is the planned and supervised process of reducing or stopping medications that may no longer be of benefit or may
Canadian Deprescribing Network 2017 Annual Report 1 What s deprescribing? Deprescribing is the planned and supervised process of reducing or stopping medications that may no longer be of benefit or may
Akinbolade O, Husband A, Forrest S, Todd A. Deprescribing in advanced illness. Progress in Palliative Care 2016, 24(5),
,") Akinbolade O, Husband A, Forrest S, Todd A. Deprescribing in advanced illness. Progress in Palliative Care 2016, 24(5), 268-271 Copyright: This is an Accepted Manuscript of an article published by Taylor
Akinbolade O, Husband A, Forrest S, Todd A. Deprescribing in advanced illness. Progress in Palliative Care 2016, 24(5), 268-271 Copyright: This is an Accepted Manuscript of an article published by Taylor
Ontario Deprescribing Project Update - July 2014
 Subscribe Share Past Issues Translate Ontario Deprescribing Project Update - July 2014 View this email in your browser Ontario Deprescribing Project Update July 2014 The evidence based Deprescribing guidelines
Subscribe Share Past Issues Translate Ontario Deprescribing Project Update - July 2014 View this email in your browser Ontario Deprescribing Project Update July 2014 The evidence based Deprescribing guidelines
Psychotropic Medication. Including Role of Gradual Dose Reductions
 Psychotropic Medication Including Role of Gradual Dose Reductions What are they? The phrase psychotropic drugs is a technical term for psychiatric medicines that alter chemical levels in the brain which
Psychotropic Medication Including Role of Gradual Dose Reductions What are they? The phrase psychotropic drugs is a technical term for psychiatric medicines that alter chemical levels in the brain which
Deprescribing benzodiazepine receptor agonists
 Deprescribing benzodiazepine receptor agonists Evidence-based clinical practice guideline CLINICAL PRACICE GUIDELINES Kevin Pottie MD MClSc CCFP FCFP Wade hompson RPh MSc Simon Davies DM MB BS MSc Jean
Deprescribing benzodiazepine receptor agonists Evidence-based clinical practice guideline CLINICAL PRACICE GUIDELINES Kevin Pottie MD MClSc CCFP FCFP Wade hompson RPh MSc Simon Davies DM MB BS MSc Jean
Presented by: Ontario s Geriatric Steering Committee
 Polypharmacy: A Medication Management Opportunity Chris Fan-Lun, BScPhm, ACPR, CGP Clinical Practice Leader, Dept. of Pharmacy Services Mount Sinai Hospital, Sinai Health system Learning Objectives Provide
Polypharmacy: A Medication Management Opportunity Chris Fan-Lun, BScPhm, ACPR, CGP Clinical Practice Leader, Dept. of Pharmacy Services Mount Sinai Hospital, Sinai Health system Learning Objectives Provide
Appropriate prescribing and deprescribing for older people getting it right. Alan Davis Northland District Health Board
 Appropriate prescribing and deprescribing for older people getting it right Alan Davis Northland District Health Board Unused returns Potentially inappropriate medication use in the elderly 15% of older
Appropriate prescribing and deprescribing for older people getting it right Alan Davis Northland District Health Board Unused returns Potentially inappropriate medication use in the elderly 15% of older
From MCI to Dementia DR YU- MIN LIN GERIATRICIAN AUG 2018
 From MCI to Dementia DR YU- MIN LIN GERIATRICIAN AUG 2018 Overview What is dementia? Common causes Normal cognitive decline Abnormal decline and mild cognitive impairment How do we manage dementia Can
From MCI to Dementia DR YU- MIN LIN GERIATRICIAN AUG 2018 Overview What is dementia? Common causes Normal cognitive decline Abnormal decline and mild cognitive impairment How do we manage dementia Can
Medication rationalization in patients with advanced medical illness
 Medication rationalization in patients with advanced medical illness Kiran Battu, BScPhm, RPh Sandra Porter, BScPhm, RPh Rachel Whitty, BScPhm, RPh, ACPR James Downar, MDCM, MHSc, FRCPC CHPC September
Medication rationalization in patients with advanced medical illness Kiran Battu, BScPhm, RPh Sandra Porter, BScPhm, RPh Rachel Whitty, BScPhm, RPh, ACPR James Downar, MDCM, MHSc, FRCPC CHPC September
SAFETY CONCERNS WITH MULTIPLE MEDICATIONS AND BEYOND. Sandra Brownstein, PharmD, CGP
 SAFETY CONCERNS WITH MULTIPLE MEDICATIONS AND BEYOND Sandra Brownstein, PharmD, CGP Objectives: List potential medication related problems that increase in the frail elderly with acute illness Differentiate
SAFETY CONCERNS WITH MULTIPLE MEDICATIONS AND BEYOND Sandra Brownstein, PharmD, CGP Objectives: List potential medication related problems that increase in the frail elderly with acute illness Differentiate
Friend or Foe? Review of the Regulations & Benefits: Risk Profiles of the Benzodiazepines
 Friend or Foe? Review of the Regulations & Benefits: Risk Profiles of the Benzodiazepines Program Learning Objectives At the conclusion of the activity, participants should be able to: Have a basic understanding
Friend or Foe? Review of the Regulations & Benefits: Risk Profiles of the Benzodiazepines Program Learning Objectives At the conclusion of the activity, participants should be able to: Have a basic understanding
MOTIVATING BEHAVIOUR CHANGE IN PATIENTS USING OPIOIDS
 MOTIVATING BEHAVIOUR CHANGE IN PATIENTS USING OPIOIDS Opioid Webinar Series Laura Murphy, PharmD Disclosures No conflict of interest Acknowledgements Andrea Fernandes Anne Kalvik Pearl Isaac Karen Ng Beth
MOTIVATING BEHAVIOUR CHANGE IN PATIENTS USING OPIOIDS Opioid Webinar Series Laura Murphy, PharmD Disclosures No conflict of interest Acknowledgements Andrea Fernandes Anne Kalvik Pearl Isaac Karen Ng Beth
COMMON DRUG RELATED PROBLEMS SEEN IN PACE AND MECHANISMS TO MITIGATE RISK
 COMMON DRUG RELATED PROBLEMS SEEN IN PACE AND MECHANISMS TO MITIGATE RISK Robert L Alesiani, PharmD, CGP Chief Pharmacotherapy Officer CareKinesis, Inc. (a Tabula Rasa Healthcare Company) 2 3 4 5 Pharmacogenomics
COMMON DRUG RELATED PROBLEMS SEEN IN PACE AND MECHANISMS TO MITIGATE RISK Robert L Alesiani, PharmD, CGP Chief Pharmacotherapy Officer CareKinesis, Inc. (a Tabula Rasa Healthcare Company) 2 3 4 5 Pharmacogenomics
ARE YOUR LEVODOPA PILLS WORKING LIKE THEY USED TO?
 ARE YOUR LEVODOPA PILLS WORKING LIKE THEY USED TO? You may have noticed a change... Levodopa is a common treatment for Parkinson s, and doctors have relied on it for decades. Over time as Parkinson s progresses,
ARE YOUR LEVODOPA PILLS WORKING LIKE THEY USED TO? You may have noticed a change... Levodopa is a common treatment for Parkinson s, and doctors have relied on it for decades. Over time as Parkinson s progresses,
ten questions you might have about tapering (and room for your own) an informational booklet for opioid pain treatment
 an informational booklet for opioid pain treatment") ten questions you might have about tapering (and room for your own) an informational booklet for opioid pain treatment This booklet was created to help you learn about tapering. You probably have lots
ten questions you might have about tapering (and room for your own) an informational booklet for opioid pain treatment This booklet was created to help you learn about tapering. You probably have lots
Geri-PARDY! (2015 Beers Criteria) Pharmacology Edition
 Pharmacology Edition") Geri-PARDY! Pharmacology Edition (2015 Beers Criteria) Aurelio Muyot, MD, AGSF, FACP Assistant Professor College of Osteopathic Medicine Touro University Nevada Objectives Review the 2015 Beers Criteria
Geri-PARDY! Pharmacology Edition (2015 Beers Criteria) Aurelio Muyot, MD, AGSF, FACP Assistant Professor College of Osteopathic Medicine Touro University Nevada Objectives Review the 2015 Beers Criteria
You May Be at Risk. You are currently taking a sedative-hypnotic drug. Please Bring This Information With You To Your Next Medical Appointment
 You are currently taking a sedative-hypnotic drug Alprazolam Chlordiazepoxide Clonazepam Diazepam Estazolam Flurazepam Lorazepam Oxazepam Temazepam Triazolam Eszopiclone Zaleplon Zolpidem Please Bring
You are currently taking a sedative-hypnotic drug Alprazolam Chlordiazepoxide Clonazepam Diazepam Estazolam Flurazepam Lorazepam Oxazepam Temazepam Triazolam Eszopiclone Zaleplon Zolpidem Please Bring
Each Home Instead Senior Care franchise office is independently owned and operated Home Instead, Inc.
 Each Home Instead Senior Care franchise office is independently owned and operated. 2011 Home Instead, Inc. Modern medicine continues to give us new drugs to ease our pain, cure our ills and extend our
Each Home Instead Senior Care franchise office is independently owned and operated. 2011 Home Instead, Inc. Modern medicine continues to give us new drugs to ease our pain, cure our ills and extend our
Palliative Care In Respirology: Who s job is it, anyway?! Everyones!
 Palliative Care In Respirology: Who s job is it, anyway?! Everyones! Dr. Shalini Nayar MD Respiratory Medicine Palliative Medicine Clinical Assistant Professor, Dept of Medicine, UBC Canadian Cancer Society
Palliative Care In Respirology: Who s job is it, anyway?! Everyones! Dr. Shalini Nayar MD Respiratory Medicine Palliative Medicine Clinical Assistant Professor, Dept of Medicine, UBC Canadian Cancer Society
Prevention of Medication-Related Falls Through Appropriate Medication Use. Clay Sprouse, MEd., CPhT Piedmont Technical College
 Prevention of Medication-Related Falls Through Appropriate Medication Use Clay Sprouse, MEd., CPhT Piedmont Technical College Disclosure I have no relevant financial or nonfinancial relationships to disclose
Prevention of Medication-Related Falls Through Appropriate Medication Use Clay Sprouse, MEd., CPhT Piedmont Technical College Disclosure I have no relevant financial or nonfinancial relationships to disclose
Opioid Prescribing for Acute Pain
 Patient Reference Guide Opioid Prescribing for Acute Pain Care for People 15 Years of Age and Older Quality standards outline what high-quality care looks like. They focus on conditions or topics where
Patient Reference Guide Opioid Prescribing for Acute Pain Care for People 15 Years of Age and Older Quality standards outline what high-quality care looks like. They focus on conditions or topics where
Targeted Deprescribing in Patients on Hemodialysis to Decrease Polypharmacy
 Targeted Deprescribing in Patients on Hemodialysis to Decrease Polypharmacy Presentation Objectives Discuss Polypharmacy In HD patients Define Deprescribing Review results of the pilot study on deprescribing
Targeted Deprescribing in Patients on Hemodialysis to Decrease Polypharmacy Presentation Objectives Discuss Polypharmacy In HD patients Define Deprescribing Review results of the pilot study on deprescribing
POLYPHARMACY IN OLDER ADULTS AND BEERS CRITERIA UPDATE
 POLYPHARMACY IN OLDER ADULTS AND BEERS CRITERIA UPDATE Jeannie Kim Lee, PharmD, BCPS, CGP Clinical Pharmacy Director College of Pharmacy The University of Arizona Learning Objectives: State the risks of
POLYPHARMACY IN OLDER ADULTS AND BEERS CRITERIA UPDATE Jeannie Kim Lee, PharmD, BCPS, CGP Clinical Pharmacy Director College of Pharmacy The University of Arizona Learning Objectives: State the risks of
OBJECTIVES. Achieving Success in Reducing Inappropriate Use of Antipsychotic Medication in Patients with Dementia
 Achieving Success in Reducing Inappropriate Use of Antipsychotic Medication in Patients with Dementia Amy J. Osborn, NHA, PMP Executive Director, Health Services Advisory Group (HSAG) Rick Foley, PharmD,
Achieving Success in Reducing Inappropriate Use of Antipsychotic Medication in Patients with Dementia Amy J. Osborn, NHA, PMP Executive Director, Health Services Advisory Group (HSAG) Rick Foley, PharmD,
Medication Information for Parents and Teachers
 Medication Information for Parents and Teachers General Information About Medication Hydroxyzine Vistaril Each child and adolescent is different. No one has exactly the same combination of medical and
Medication Information for Parents and Teachers General Information About Medication Hydroxyzine Vistaril Each child and adolescent is different. No one has exactly the same combination of medical and
Great Low Cost in SNF-NF Jabbar Fazeli, MD Maine Medical Directors Association
 Great Care @ Low Cost in SNF-NF Jabbar Fazeli, MD Maine Medical Directors Association Principles Best interest of the patient (SNF) and resident (NF) comes first. Lowest cost to achieve the same care.
Great Care @ Low Cost in SNF-NF Jabbar Fazeli, MD Maine Medical Directors Association Principles Best interest of the patient (SNF) and resident (NF) comes first. Lowest cost to achieve the same care.
Don t Blame it on Aging. Nancy Stiles, MD Associate Professor Geriatrics Dept of Physical Medicine and Rehabilitation University of Kentucky
 Don t Blame it on Aging Nancy Stiles, MD Associate Professor Geriatrics Dept of Physical Medicine and Rehabilitation University of Kentucky Normal Aging Typical Aging Age-related disease Aging is not a
Don t Blame it on Aging Nancy Stiles, MD Associate Professor Geriatrics Dept of Physical Medicine and Rehabilitation University of Kentucky Normal Aging Typical Aging Age-related disease Aging is not a
Michelle Greiver Simone Dahrouge Patricia O Brien Donna Manca Marie-Thérèse Lussier
 Michelle Greiver Simone Dahrouge Patricia O Brien Donna Manca Marie-Thérèse Lussier University of Toronto Practice Based Research Network Ottawa Practice Enhancement Network Quality & Innovation Program,
Michelle Greiver Simone Dahrouge Patricia O Brien Donna Manca Marie-Thérèse Lussier University of Toronto Practice Based Research Network Ottawa Practice Enhancement Network Quality & Innovation Program,
AGS Annual Meeting May Sponsored by the Polypharmacy Special Interest Group and the Pharmacists Section
 AGS Annual Meeting May 2010 Sponsored by the Polypharmacy Special Interest Group and the Pharmacists Section No financial conflicts of interest Sponsored by the Polypharmacy Special Interest Group Thanks
AGS Annual Meeting May 2010 Sponsored by the Polypharmacy Special Interest Group and the Pharmacists Section No financial conflicts of interest Sponsored by the Polypharmacy Special Interest Group Thanks
Black holes taped on floor Redirection Music and activities Yellow straps across the door Remind other residents to use call bell when she comes in
 Intrusive Wandering Case study........................................... A 97 year old woman with dementia lives in a mixed 23 bed LTC unit. She is independently mobile in her wheelchair and goes in and
Intrusive Wandering Case study........................................... A 97 year old woman with dementia lives in a mixed 23 bed LTC unit. She is independently mobile in her wheelchair and goes in and
Polypharmacy and Deprescribing for Older People
 Polypharmacy and Deprescribing for Older People Sarah Hilmer Head of Department, Clinical Pharmacology and Senior Staff Specialist Aged Care, RNSH Conjoint Professor of Geriatric Pharmacology, Sydney University
Polypharmacy and Deprescribing for Older People Sarah Hilmer Head of Department, Clinical Pharmacology and Senior Staff Specialist Aged Care, RNSH Conjoint Professor of Geriatric Pharmacology, Sydney University
Polypharmacy and Elders. Leslie Baker, Pharm. D., RPh, CGP Sanford Center for Aging
 Polypharmacy and Elders Leslie Baker, Pharm. D., RPh, CGP Sanford Center for Aging Prescription Medication Use In Elders 1 13% of the US population is age 65+ Age 65 years 13% Age 65+ account for 34% of
Polypharmacy and Elders Leslie Baker, Pharm. D., RPh, CGP Sanford Center for Aging Prescription Medication Use In Elders 1 13% of the US population is age 65+ Age 65 years 13% Age 65+ account for 34% of
Medicines in Scotland: What s the right treatment for me? Information for patients and the public
 Medicines in Scotland: What s the right treatment for me? Information for patients and the public You can read and download this document from our website. We are happy to consider requests for other languages
Medicines in Scotland: What s the right treatment for me? Information for patients and the public You can read and download this document from our website. We are happy to consider requests for other languages
Polypharmacy: Making it all Work Kathy Wilson, RPh, RWSIR Director of Pharmacy
 Polypharmacy: Making it all Work Kathy Wilson, RPh, RWSIR Director of Pharmacy Polypharmacy can be defined as the use of multiple medications for the treatment of a patient s medical conditions. The term
Polypharmacy: Making it all Work Kathy Wilson, RPh, RWSIR Director of Pharmacy Polypharmacy can be defined as the use of multiple medications for the treatment of a patient s medical conditions. The term
Patient Safety in Older Adults
 Patient Safety in Older Adults Scott Martin Vouri, PharmD, MSCI, BCPS, BCGP, FASCP St. Louis College of Pharmacy Faculty Disclosure Dr. Vouri is funded by the Washington University Institute of Clinical
Patient Safety in Older Adults Scott Martin Vouri, PharmD, MSCI, BCPS, BCGP, FASCP St. Louis College of Pharmacy Faculty Disclosure Dr. Vouri is funded by the Washington University Institute of Clinical
Safe Prescribing of Drugs with Potential for Misuse/Diversion
 College of Physicians and Surgeons of British Columbia Safe Prescribing of Drugs with Potential for Misuse/Diversion Preamble This document establishes both professional standards as well as guidelines
College of Physicians and Surgeons of British Columbia Safe Prescribing of Drugs with Potential for Misuse/Diversion Preamble This document establishes both professional standards as well as guidelines