Alternative Routes of Drug Administration (analgesia) Dr Andrew Dickman Consultant Pharmacist
|
|
|
- Roger Sutton
- 5 years ago
- Views:
Transcription









1 Alternative Routes of Drug Administration (analgesia) Dr Andrew Dickman Consultant Pharmacist
2 Alternative Routes of Drug Administration Introduction Subcutaneous Route Contemporary Issues Compatibility Future Options
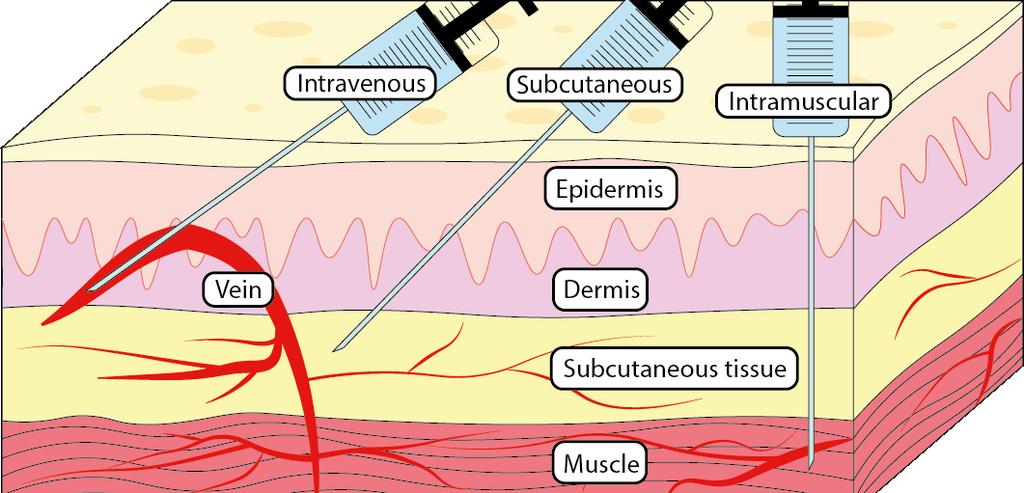
3 Classification Enteral Parenteral Topical Oral Sublingual Buccal Rectal Inhalation Injection Transdermal Intravenous Intramuscular Subcutaneous Intrathecal Skin Intranasal Ocular Mucosal throat ear mouth May have local and/or systemic effects

4 Choice of Route Condition of the patient unconscious, vomiting Available formulations Physical & chemical properties of drug solid/liquid/gas; solubility; stability; ph Rapidity of response Site of desired action E.g. localised or generalised; approachable?
5 Choice of Route When oral route no longer available: Buccal/SL PR Transdermal Intranasal IV IM SC
6 Sublingual and Buccal POSITIVES NEGATIVES Avoids first-pass metabolism Drug absorption is fast Rapid onset of action Generally considered unsuitable for prolonged administration Unpalatable & bitter drugs Irritation of oral mucosa Large quantities cannot be given Few drugs are absorbed Advantages lost if swallowed Dry mouth Few licensed products
7 Rectal POSITIVES NEGATIVES May circumvent first-pass elimination Effective absorption most meds used at end of life Uncomfortable (requires repeated movement) Ongoing invasion of privacy Low dose versatility usually one drug, one dose Time to onset of effect Limited options


8 Successful use of pregabalin by the rectal route to treat chronic neuropathic pain in a patient with complete intestinal failure. Doddrell et al. BMJ Case Rep 2015 pii: bcr year-old patient with chronic neuropathic pain and complete intestinal failure Unclear if capsule was used, or novel formulation Patient s pain scores improved after titration
9 Transdermal Opioids POSITIVES NEGATIVES Circumvents first-pass elimination Ease of use Extended duration of action Good patient compliance Painless administration Local irritation Use in patients with stable pain Temp affects absorption Patch may not adhere well Application may be difficult
10 Intranasal POSITIVES NEGATIVES Circumvents first-pass elimination Ease of use Rapid drug absorption and quick onset of action Painless administration Local irritation Small volume (0.2mL each nostril) May swallow dose loss of effect Drug suitability Lack of evidence
:390 401 There are no data on intranasal ketamine for cancer-related pain!")
11 Intranasal Intranasal Ketamine and Its Potential Role in Cancer-Related Pain Singh et al. Pharmacotherapy. 2018; 38(3): There are no data on intranasal ketamine for cancer-related pain! Intranasal ketamine may be an option for patients unable to tolerate oral administration


12 Not suitable for long-term management of cancer pain

13
14 Choice of Route Systematic review of the role of alternative application routes for opioid treatment for moderate to severe cancer pain: An EPCRC opioid guidelines project Radbruch et al. Palliat Med. 2010; 25(5) Good evidence that subcutaneous administration of morphine or other opioids is an effective alternative for cancer patients if oral treatment is not possible
 578 596 Intravenous, rectal or transdermal therapy will offer a good alternative to the subcutaneous route No significant differences in efficacy or adverse effects between the")
15 Choice of Route Systematic review of the role of alternative application routes for opioid treatment for moderate to severe cancer pain: An EPCRC opioid guidelines project Radbruch et al. Palliat Med. 2010; 25(5) Intravenous, rectal or transdermal therapy will offer a good alternative to the subcutaneous route No significant differences in efficacy or adverse effects between the alternative application routes
16 Choice of Route Subcutaneous Administration of Drugs in Palliative Care: Results of a Systematic Observational Study Bartz et al. J Pain Symptom Manage. 2014; 48(4) patients, 3957 applications Subcutaneous administration of medication is a very flexible, broadly feasible, rather safe, and nonburdensome method of drug administration Needs appropriate nursing care, and requires standardised policies and procedures.


17 Continuous Subcutaneous Infusions Embraced by palliative care services in the UK Rectal administration is not always practical, or acceptable Intramuscular administration will be painful, especially if the patient is cachectic Intravenous injections or infusions risk of infection CSCIs are less invasive, yet as effective Repeated intermittent SC bolus injections through indwelling subcutaneous cannula possible use of a CSCI is more practical

18 The Smiths Medical (formerly Graseby) devices have been the mainstay of palliative care provision across the UK for 30 years. Continuous Subcutaneous Infusions
19 Continuous Subcutaneous Infusions Syringe Driver in Terminal Care Dover S. Br Med J (Clin Res Ed) ;294(6571): The syringe driver is a valuable alternative to the less pleasant methods of drug administration The syringe driver is a major advance in the terminal care of patients

20 Continuous Subcutaneous Infusions Used in palliative care through serendipity Martin Wright s GP & neighbour was Dr Patrick Russell During usual friendly discussion, idea of CSCI in palliative care was born Russell described 1st CSCI in the hospice context in 1979 A CSCI remains popular to this day
21 Continuous Subcutaneous Infusions Popularity of MS26 undoubtedly due to several factors: small size and weight (190 mm x 53 mm x 30 mm; 300g) increased mobility and independence for patient relatively simple to use (after training) Manufactured in UK by Pye Dynamics (originally armaments); later Graseby (depth charges)


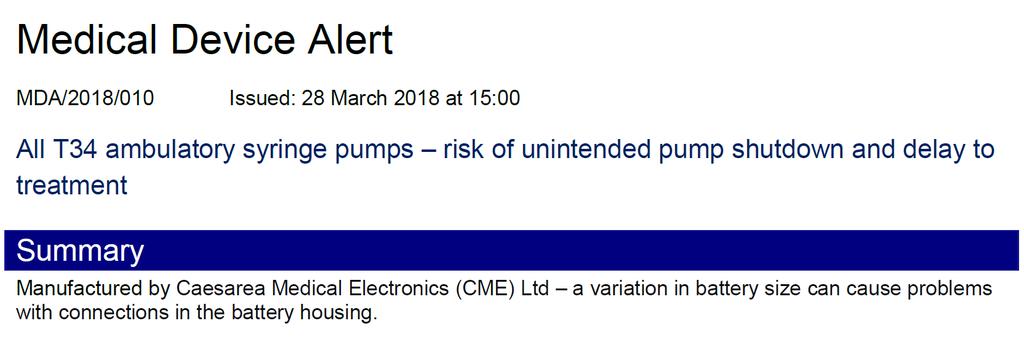
22 Continuous Subcutaneous Infusions 2003 Medical Devices Agency These devices do not include many of the safety features which would be expected of current infusion technology
23 Continuous Subcutaneous Infusions MS drivers did not comply with IEC Applied to the basic safety and essential performance of infusion pumps and controllers
24 Continuous Subcutaneous Infusions What did IEC stipulate? Allows the user to set up an infusion over 24 hours quickly and reliably Delivery rate is calculated by the device Safety alarms: power interruption a blocked line a displaced syringe tampering with the infusion end of infusion
 183 260 Lock box weight (g) 183 188 Battery 1x 9V Alkaline 1x 9V Alkaline Battery life (days) 50 7 Overall usability for palliative care")
25 Continuous Subcutaneous Infusions Device Graseby MS26/MS16A CME T34 List Price (ex VAT) Meets IEC UK Launch Size (H x W x D) 166 x 53 x x 53 x 23 Weight with battery (g) Lock box weight (g) Battery 1x 9V Alkaline 1x 9V Alkaline Battery life (days) 50 7 Overall usability for palliative care applications

26 Continuous Subcutaneous Infusions 2002 Amended Medical Devices Legislation New regulatory system for medical devices Current standards retained for 5 years to cover existing products (i.e. MS drivers) October 2007 Smiths Medical voluntarily withdrew the devices from the Australian market At this time in the UK, ad hoc adoption causing problems across interfaces
27 Continuous Subcutaneous Infusions NPSA recommended syringe pumps with: rate settings in millilitres (ml) per hour mechanisms to stop infusion if the syringe is not properly and securely fitted alarms that activate if the syringe is removed before the infusion is stopped lock-box covers and/or lock out controlled by password provision of internal log memory to record all pump events

28 Continuous Subcutaneous Infusions For IMMEDIATE ACTION by all organisations in the NHS and independent sector who use ambulatory syringe drivers Introduction of syringe drivers with additional safety features by Dec 2015 This was EIGHT years after Australia & NZ acted


29 Continuous Subcutaneous Infusions


30 48.8mm 48.5mm 26mm 25.5mm
31 Thousands of elderly patients may have died prematurely because of cheap, faulty syringe pumps in a scandal described as one of the biggest cover-ups in NHS history
32 Graseby MS 16A & MS 26 syringe drivers were loaded with capsules and programmed to release drugs into a patient s bloodstream over an extended period so doctors and nurses did not have to inject manually

33 The whistleblower, a senior Department of Health official, said: Anyone who has lost their granny over the last 30 years when opiates were administered by this commonly used syringe driver will be asking themselves, Is that what killed Granny?

34 Continuous Subcutaneous Infusions Bishop James Jones chaired the Gosport independent panel: I understand the concerns about syringe drivers highlighted by The Sunday Times The panel was required to analyse historical documents relating to the early deaths from 1989 to None featured faulty syringe drivers.

35 Continuous Subcutaneous Infusions Scaremongering needs addressing Questions do need answering why did it take up to 8 years? what was the scale of the problem? who is the whistleblower and what facts/figures are being used?


36 Continuous Subcutaneous Infusions In 2007, the NPSA issued Patient Safety Alert 20 Full technical information about stability in solution and compatibility information for commonly used mixtures in should be readily available

37 Continuous Subcutaneous Infusions In 2008, MHRA issued a consultation document (MLX 356) The Commission on Human Medicine (CHM) advised the MHRA: research should be commissioned to develop authoritative national advice on mixing of medicines to encompass compatibility and stability data

38 ChemdEL Chemical compatibility of drugs administered by continuous subcutaneous infusion for end of life care
39 Drug Compatibility Incompatibility - a theoretically reversible physicochemical change that may result in precipitation or insolubility, which may not always be visible e.g. midazolam and dexamethasone Instability - irreversible chemical degradation of the active compound, resulting in loss of potency e.g. glycopyrronium and dexamethasone
40 Drug Compatibility A B Influence of ph on midazolam (A) and the more soluble open-ring benzophenone (B)
41 Drug Compatibility Salt Ion Suffix -ium ate (organic anion) -ium (base anion) -ate & -ide (acid cations) -ate ide -ide -ium ate -ium ide } denote quaternary ammonium cations Examples Dexamethasone sodium phosphate Diclofenac sodium, phenobarbital sodium Cyclizine lactate, fentanyl citrate, morphine sulphate, octreotide acetate, alfentanil hydrochloride, hyoscine hydrobromide, levomepromazine hydrochloride, metoclopramide hydrochloride, oxycodone hydrochloride Hyoscine butylbromide Glycopyrronium bromide

 Typically 2 or 3")
42 Drug Compatibility How many drug combinations are possible? 5 opioids (at least) 15 supportive drugs (at least) Typically 2 or 3 drugs plus opioid
43 Drug Compatibility
44 Drug Compatibility Identification of drug combinations administered by continuous subcutaneous infusion that require analysis for compatibility and stability Dickman et al. BMC Palliative Care (2017) 16:22 National survey identified 40 commonly used combinations from 2000 entries Delphi study identified 5 combinations Formed the basis of the analytical study
45 Drug Compatibility Analysis of the chemical compatibility and stability of drug combinations used in continuous subcutaneous infusions Dickman et al. Manuscript submitted A total of 30 discrete combinations were analysed 20 at max/min 9 min 1 max
46 Drug Compatibility Analysis of the chemical compatibility and stability of drug combinations used in continuous subcutaneous infusions Dickman et al. Manuscript submitted All 30 combinations were shown to be physically and chemically compatible and stable over an infusion period of 24 hours under normal fluorescent light at ambient room temperature.
47 ChemdEL Results Morphine Oxycodone Cyclizine Haloperidol Hyoscine butylbromide Metoclopramide (max only) Dexamethasone & Ranitidine Glycopyrronium Bromide & Midazolam Haloperidol & Hyoscine butylbromide Haloperidol & Midazolam (min only) Hyoscine butylbromide & Midazolam Levomepromazine & Midazolam (min only) Metoclopramide & Midazolam (min only) Glycopyrronium bromide & Midazolam Haloperidol & Hyoscine butylbromide Haloperidol & Midazolam (min only) Hyoscine butylbromide & Midazolam Hyoscine butylbromide & Octreotide Ketamine & Levomepromazine Levomepromazine & Midazolam (min only) Metoclopramide & Midazolam(min only)
48 ChemdEL Results Alfentanil Cyclizine Haloperidol Metoclopramide Midazolam Hyoscine butylbromide & Levomepromazine Hyoscine butylbromide & Octreotide Levomepromazine & Midazolam (min only) Metoclopramide & Midazolam Hyoscine butylbromide, Levomepromazine & Midazolam Diamorphine Haloperidol & Midazolam (min only) Levomepromazine & Midazolam (min only)

49 Equianalgesia 49
50 Equianalgesia Equaianalgesic dose:..that dose at which two opioids (at steady state) provide approximately the same pain relief. Shaheen et al. Opioid equianalgesic tables: are they all equally dangerous? J Pain Symptom Manage. 2009; 38(3):409-17
51 Equianalgesia Morphine has poor and variable oral absorption Complicates conversion values No equianalgesic table can fully address all clinical factors that influence opioid pharmacology Most of the tables are derived from single-dose studies, expert opinion and studies in non-cancer patients Designing a study to adequately address all variables that influence equianalgesia would be extremely difficult if not impossible
52 Equianalgesia Alfentanil:Diamorphine SC Expert opinion derived 1:10 (1) Based on 4 patients Adopted as canon Recent retrospective review suggests equianalgesic ratio is closer to 1:6 (2) Based on 35 patients 1. Kirkham SR, Pugh R. Opioid analgesia in uraemic patients. Lancet 1995;345: Cran A et al. Opioid rotation to alfentanil: comparative evaluation of conversion ratios. BMJ Support Palliat Care Sep;7(3):
53 Equianalgesia Bidirectional ratios safer? Alfentanil Diamorphine SC 1:6 Diamorphine Alfentanil 10:1
54 Equianalgesia Morphine:Oxycodone Is oxycodone more potent than morphine? No it isn t. Approaching 1:1 (1) Difference in oral conversion rate due to poor bioavailability of morphine Napp maintain 2:1 (25% vs 50%) BNF, PCF5 suggest 1.5:1 1. Dr K Smith. Director of Clinical Pharmacology Napp Personal communication. 2018



55 Equianalgesia Does cause confusion Several services produced 2 equianalgesic tables specialist generalist Equianalgesic ratio is simply a starting point Consider other factors before arriving at dose co-morbidity concurrent medication

56
57 Equianalgesia Oral Morphine 4-hr dose (mg) 12-hr dose (mg) Oral Oxycodone 4-hr dose (mg) 12-hr dose (mg) Transdermal Buprenorphine BuTrans (mcg/hr) Change every 7 days Transtec (mcg/hr) Change every 4 days Transdermal Fentanyl (mcg/hr) Change patch every 3 days Subcutaneous Morphine Subcutaneous Oxycodone Subcutaneous Diamorphine CONSIDER SEEKING SPECIALIST PALLIATIVE CARE ADVICE IF DOSES >120mg/24hours ORAL MORPHINE (OR EQUIVALENT) ARE NOT CONTROLLING PAIN hr Dose (mg) 24-hr dose (mg) 4-hr Dose (mg) 24-hr dose (mg) 4-hr Dose (mg) 24-hr dose (mg) Ensure advice given about doses >120mg PO morphine/24hrs
SYRINGE DRIVER MEDICATIONS
 SYRINGE DRIVER MEDICATIONS Christine Hull & Anita Webb Staff Nurses, Hospice in the Home 2015 Analgesics:- Groups of Medication used in Syringe Drivers Morphine sulphate Diamorphine Oxycodone Alfentanil
SYRINGE DRIVER MEDICATIONS Christine Hull & Anita Webb Staff Nurses, Hospice in the Home 2015 Analgesics:- Groups of Medication used in Syringe Drivers Morphine sulphate Diamorphine Oxycodone Alfentanil
PHARMACY SERVICE ARRANGEMENTS FOR THE SUPPLY OF PALLIATIVE CARE SYRINGES AND MEDICINES FOR COMMUNITY PATIENTS
 PHARMACY SERVICE ARRANGEMENTS FOR THE SUPPLY OF PALLIATIVE CARE SYRINGES AND MEDICINES FOR COMMUNITY PATIENTS The benefits of prefilled syringes for palliative care from the hospital pharmacy service In
PHARMACY SERVICE ARRANGEMENTS FOR THE SUPPLY OF PALLIATIVE CARE SYRINGES AND MEDICINES FOR COMMUNITY PATIENTS The benefits of prefilled syringes for palliative care from the hospital pharmacy service In
Syringe driver in Palliative Care
 Syringe driver in Palliative Care Introduction: Syringe drivers are portable, battery operated devices widely used in palliative care to deliver medication as a continuous subcutaneous infusion over 24
Syringe driver in Palliative Care Introduction: Syringe drivers are portable, battery operated devices widely used in palliative care to deliver medication as a continuous subcutaneous infusion over 24
PRESCRIBING GUIDELINES FOR SYMPTOM MANAGEMENT IN THE DYING PATIENT
 PRESCRIBING GUIDELINES FOR SYMPTOM MANAGEMENT IN THE DYING PATIENT A collaboration between: St. Rocco s Hospice, Bridgewater Community Healthcare NHS Trust, NHS Warrington Clinical Commissioning Group,
PRESCRIBING GUIDELINES FOR SYMPTOM MANAGEMENT IN THE DYING PATIENT A collaboration between: St. Rocco s Hospice, Bridgewater Community Healthcare NHS Trust, NHS Warrington Clinical Commissioning Group,
For patients and their carers this means smoother symptom control, better support in a crisis, and avoidance of admission if that is their choice.
 Bedfordshire Palliative Care Palliative Care Medicines Guidance This folder has been produced to support professionals providing palliative care in any setting. Its aim is to make best practice in palliative
Bedfordshire Palliative Care Palliative Care Medicines Guidance This folder has been produced to support professionals providing palliative care in any setting. Its aim is to make best practice in palliative
Algorithms for Symptom Management. In End of Life Care
 Algorithms for Symptom Management In End of Life Care The Use of Drugs Beyond Licence (off label) -The Medicines and Healthcare Products Regulatory Agency (MHRA) in the UK regulates the activity of the
Algorithms for Symptom Management In End of Life Care The Use of Drugs Beyond Licence (off label) -The Medicines and Healthcare Products Regulatory Agency (MHRA) in the UK regulates the activity of the
GUIDELINES ON THE MANAGEMENT OF PAIN DUE TO CANCER IN ADULTS
 GUIDELINES ON THE MANAGEMENT OF PAIN DUE TO CANCER IN ADULTS Bristol Palliative Care Collaborative Contact Numbers: Hospital Specialist Palliative Care Teams: North Bristol 0117 4146392 UH Bristol 0117
GUIDELINES ON THE MANAGEMENT OF PAIN DUE TO CANCER IN ADULTS Bristol Palliative Care Collaborative Contact Numbers: Hospital Specialist Palliative Care Teams: North Bristol 0117 4146392 UH Bristol 0117
Isle of Wight Syringe Driver Compatibility Guidelines
 Isle of Wight Syringe Driver Compatibility Guidelines Produced by The Earl Mountbatten Hospice, Isle of Wight Written January 2015, revision due January 2018 This guideline is available as a paper pocketbook
Isle of Wight Syringe Driver Compatibility Guidelines Produced by The Earl Mountbatten Hospice, Isle of Wight Written January 2015, revision due January 2018 This guideline is available as a paper pocketbook
Palliative Care Impact Survey
 September 2018 Contents Introduction...3 Headlines...3 Approach...4 Findings...4 Which guideline are used...4 How and where the guidelines are used...6 Alternative sources of information...7 Use of the
September 2018 Contents Introduction...3 Headlines...3 Approach...4 Findings...4 Which guideline are used...4 How and where the guidelines are used...6 Alternative sources of information...7 Use of the
Supporting Last Days of Life Symptom Control Medication Guidance: Algorithm. Agitation & Anxiety
 Agitation & Anxiety (Exclude or treat REVERSIBLE causes*) Patient is anxious / frightened, but lucid Patient is confused, agitated and / or hallucinating MIDAZOLAM 2.5-5mg s/c (Max total 24 hour dose of
Agitation & Anxiety (Exclude or treat REVERSIBLE causes*) Patient is anxious / frightened, but lucid Patient is confused, agitated and / or hallucinating MIDAZOLAM 2.5-5mg s/c (Max total 24 hour dose of
End of life prescribing guidance
 End of life prescribing guidance Introduction This guidance has been prepared to ASSIST IN DECISION MAKING for the prescribing and monitoring of medicines useful in the management of symptoms commonly
End of life prescribing guidance Introduction This guidance has been prepared to ASSIST IN DECISION MAKING for the prescribing and monitoring of medicines useful in the management of symptoms commonly
Renal Prescribing at End of Life Guidance for Anticipatory prescribing for patients in renal failure (egfr<30) at the end of life
 at the end of life") Guidance for Anticipatory prescribing for patients in renal failure (egfr
Guidance for Anticipatory prescribing for patients in renal failure (egfr
SYMPTOM MANAGEMENT GUIDANCE FOR PATIENTS RECEIVING PALLIATIVE CARE AT ROYAL DERBY HOSPITAL
 SYMPTOM MANAGEMENT GUIDANCE FOR PATIENTS RECEIVING PALLIATIVE CARE AT ROYAL DERBY HOSPITAL If a patient is believed to be approaching the end of their life, medication should be prescribed in anticipation
SYMPTOM MANAGEMENT GUIDANCE FOR PATIENTS RECEIVING PALLIATIVE CARE AT ROYAL DERBY HOSPITAL If a patient is believed to be approaching the end of their life, medication should be prescribed in anticipation
GUIDELINES FOR PRESCRIBING AT THE END OF LIFE FOR PATIENTS WITH RENAL IMPAIRMENT (estimated glomerular filtration rate<30)
") GUIDELINES FOR PRESCRIBING AT THE END OF LIFE FOR PATIENTS WITH RENAL IMPAIRMENT These guidelines have been produced in collaboration with Dr Lucy Smyth, Consultant in Renal Medicine, Royal Devon and Exeter
GUIDELINES FOR PRESCRIBING AT THE END OF LIFE FOR PATIENTS WITH RENAL IMPAIRMENT These guidelines have been produced in collaboration with Dr Lucy Smyth, Consultant in Renal Medicine, Royal Devon and Exeter
Supportive Care. End of Life Phase
 Supportive Care End of Life Phase Guidelines for Health Care Professionals In the care of patients with established renal failure who are in the last days of life References: Chambers E J (2004) End of
Supportive Care End of Life Phase Guidelines for Health Care Professionals In the care of patients with established renal failure who are in the last days of life References: Chambers E J (2004) End of
Care in the Last Days of Life
 Care in the Last Days of Life Introduction This guideline is an aid to clinical decision making and good practice in person-centred care for patients who are deteriorating and at risk of dying. The patient
Care in the Last Days of Life Introduction This guideline is an aid to clinical decision making and good practice in person-centred care for patients who are deteriorating and at risk of dying. The patient
Renal Palliative Care Last Days of Life
 Renal Palliative Care Last Days of Life Introduction This guideline is an aid to clinical decision-making and good practice for patients with stage 4-5 chronic kidney disease (egfr
Renal Palliative Care Last Days of Life Introduction This guideline is an aid to clinical decision-making and good practice for patients with stage 4-5 chronic kidney disease (egfr
PAIN AND SYMPTOM MANAGEMENT GUIDANCE IN THE LAST DAYS OF LIFE
 PAIN AND SYMPTOM MANAGEMENT GUIDANCE IN THE LAST DAYS OF LIFE Reference: DCM029 Version: 1.1 This version issued: 07/06/18 Result of last review: Minor changes Date approved by owner (if applicable): N/A
PAIN AND SYMPTOM MANAGEMENT GUIDANCE IN THE LAST DAYS OF LIFE Reference: DCM029 Version: 1.1 This version issued: 07/06/18 Result of last review: Minor changes Date approved by owner (if applicable): N/A
ALLERGIES/ SENSITIVITIES This section must be completed before prescribing/administering any drug
 COMMUNITY PRESCRIPTION CHART All entries should be in CAPITAL letters and in indelible black ink. If medications/ doses are stopped, cross through the relevant line clearly to avoid error. GP: PRESCRIBER
COMMUNITY PRESCRIPTION CHART All entries should be in CAPITAL letters and in indelible black ink. If medications/ doses are stopped, cross through the relevant line clearly to avoid error. GP: PRESCRIBER
PAIN MANAGEMENT Person established taking oral morphine or opioid naive.
 PAIN MANAGEMENT Person established taking oral morphine or opioid naive. Important; it is the responsibility of the prescriber to ensure that guidelines are followed when prescribing opioids. Every member
PAIN MANAGEMENT Person established taking oral morphine or opioid naive. Important; it is the responsibility of the prescriber to ensure that guidelines are followed when prescribing opioids. Every member
PAIN MANAGEMENT Patient established on oral morphine or opioid naive.
 PAIN MANAGEMENT Patient established on oral morphine or opioid naive. Important; It is the responsibility of the prescriber to ensure that guidelines are followed when prescribing opioids. Every member
PAIN MANAGEMENT Patient established on oral morphine or opioid naive. Important; It is the responsibility of the prescriber to ensure that guidelines are followed when prescribing opioids. Every member
[Type text] Anticipatory Medication STAT dose and Syringe Driver Guidance [Type text]
![[Type text] Anticipatory Medication STAT dose and Syringe Driver Guidance [Type text]](/thumbs/92/110296570.jpg "[Type text] Anticipatory Medication STAT dose and Syringe Driver Guidance [Type text]") [Type text] Anticipatory Medication STAT dose and Syringe Driver Guidance [Type text] Patients with egfr greater than 30mL/min Patients with egfr less than 30mL/min Symptom Drug Dose Symptom Drug Dose
[Type text] Anticipatory Medication STAT dose and Syringe Driver Guidance [Type text] Patients with egfr greater than 30mL/min Patients with egfr less than 30mL/min Symptom Drug Dose Symptom Drug Dose
ANTICIPATORY PRESCRIBING FOR PATIENTS AT END OF LIFE WITH RENAL IMPAIRMENT
 ANTICIPATORY PRESCRIBING FOR PATIENTS AT END OF LIFE WITH RENAL Doses of opiates must be proptional to current analgesic medication Please refer ALL patients on Methadone Ketamine to SPCT f advice. Patients
ANTICIPATORY PRESCRIBING FOR PATIENTS AT END OF LIFE WITH RENAL Doses of opiates must be proptional to current analgesic medication Please refer ALL patients on Methadone Ketamine to SPCT f advice. Patients
MMG035 Symptom Management Guidelines for a Person thought to be in the Last Few Days and Hours of Life
 MMG035 Symptom Management Guidelines for a Person thought to be in the Last Few Days and Hours of Life The following pages are guidelines for the management of common symptoms for a person thought to be
MMG035 Symptom Management Guidelines for a Person thought to be in the Last Few Days and Hours of Life The following pages are guidelines for the management of common symptoms for a person thought to be
Doncaster & Bassetlaw Cancer Locality. Palliative Care Core Formulary
 Doncaster & Bassetlaw Cancer Locality Palliative Core Formulary Approved by Doncaster & Bassetlaw Hospitals NHS Foundation Trust Drugs and Therapeutics Committee. DJ14/2155 Oct 2014 Review date: Oct 2017
Doncaster & Bassetlaw Cancer Locality Palliative Core Formulary Approved by Doncaster & Bassetlaw Hospitals NHS Foundation Trust Drugs and Therapeutics Committee. DJ14/2155 Oct 2014 Review date: Oct 2017
Mid Essex Locality Guideline for Management of Adult Acute and Chronic Non-Cancer Pain in Primary care
 Guideline for Management of Adult Acute and Chronic Non-Cancer Pain in Primary care If possible patients should be assessed using a simple visual analogue scale VAS to determine the most appropriate stage
Guideline for Management of Adult Acute and Chronic Non-Cancer Pain in Primary care If possible patients should be assessed using a simple visual analogue scale VAS to determine the most appropriate stage
What s New 2003? What new treatments? What have you discontinued? More information please!
 What s New 2003? What new treatments? What have you discontinued? More information please! 1 What s New 2003? Submissions = 137 UK = 52 (38%) Doctors = 60% Nurses = 25% Pharmacists = 15% 2 What s New?
What s New 2003? What new treatments? What have you discontinued? More information please! 1 What s New 2003? Submissions = 137 UK = 52 (38%) Doctors = 60% Nurses = 25% Pharmacists = 15% 2 What s New?
Diamorphine 4 hour. alfentanil (500microgram/mL) Calculated by dividing 24 hour oral morphine dose by 30
 Calculated by dividing 24 hour oral morphine dose by 30") If more information is required please seek help from specialist palliative care pioid dose conversion chart, syringe driver doses, rescue/prn doses and opioid patches Use the conversion chart to work
If more information is required please seek help from specialist palliative care pioid dose conversion chart, syringe driver doses, rescue/prn doses and opioid patches Use the conversion chart to work
In our patients the cause of seizures can be broadly divided into structural and systemic causes.
 Guidelines for the management of Seizures Amalgamation and update of previous policies 7 (Seizure guidelines, ND, 2015) and 9 (Status epilepticus, KJ, 2011) Seizures can occur in up to 15% of the Palliative
Guidelines for the management of Seizures Amalgamation and update of previous policies 7 (Seizure guidelines, ND, 2015) and 9 (Status epilepticus, KJ, 2011) Seizures can occur in up to 15% of the Palliative
Palliative Care and the Critical Role of the Pharmacist. Arti Thakerar Education/ Palliative Care Peter MacCallum Cancer Centre
 Palliative Care and the Critical Role of the Pharmacist Arti Thakerar Education/ Palliative Care Peter MacCallum Cancer Centre Overview What is palliative care Role of a pharmacist in palliative care Issues
Palliative Care and the Critical Role of the Pharmacist Arti Thakerar Education/ Palliative Care Peter MacCallum Cancer Centre Overview What is palliative care Role of a pharmacist in palliative care Issues
Anticipatory Medications for End of Life Patients. Doses must be proportional to the current analgesic medication YES NO YES NO
 Anticipatory Medications for End of Life Patients oses must be proportional to the current analgesic medication Please refer ALL patients on Methadone or Ketamine to palliative care team for advice. Patients
Anticipatory Medications for End of Life Patients oses must be proportional to the current analgesic medication Please refer ALL patients on Methadone or Ketamine to palliative care team for advice. Patients
EAST LANCASHIRE GUIDELINES FOR THE MANAGEMENT OF SYMPTOMS IN THE LAST DAYS OF LIFE
 EAST LANCASHIRE SPECIALIST PALLIATIVE CARE TEAM EAST LANCASHIRE GUIDELINES FOR THE MANAGEMENT OF SYMPTOMS IN THE LAST DAYS OF LIFE Reviewed and updated August 2009 Next review date August 2011 Approved
EAST LANCASHIRE SPECIALIST PALLIATIVE CARE TEAM EAST LANCASHIRE GUIDELINES FOR THE MANAGEMENT OF SYMPTOMS IN THE LAST DAYS OF LIFE Reviewed and updated August 2009 Next review date August 2011 Approved
Care of the Dying Management in Severe Renal Failure
 Care of the Dying Management in Severe Renal Failure Clinical Guideline Early recognition of the dying process allows for adequate preparation of the patient, the family and the carers. This clinical guidance
Care of the Dying Management in Severe Renal Failure Clinical Guideline Early recognition of the dying process allows for adequate preparation of the patient, the family and the carers. This clinical guidance
Clatterbridge Centre for Oncology
 Clatterbridge Centre for Oncology CONTENTS 1. Why and when to use a syringe driver 2. Siting the syringe driver 3. Mixing and measuring 4. Setting up the syringe driver 5. Drug information 6. Common problems
Clatterbridge Centre for Oncology CONTENTS 1. Why and when to use a syringe driver 2. Siting the syringe driver 3. Mixing and measuring 4. Setting up the syringe driver 5. Drug information 6. Common problems
Care of the Dying. For dosing in severe renal impairment see separate guidance for care of the dying in severe renal failure.
 Care of the Dying Early diagnosis of the dying process allows for adequate preparation of the patient, the family and the carers. This clinical guidance covers the prescribing and management of patients
Care of the Dying Early diagnosis of the dying process allows for adequate preparation of the patient, the family and the carers. This clinical guidance covers the prescribing and management of patients
SUBCUTANEOUS AS REQUIRED & SYRINGE PUMP PRESCRIPTION & ADMINISTRATION RECORD (SPAR) Name: Address: Postcode: Date of Birth: NHS Number:
 Name: Address: Postcode: Date of Birth: NHS Number:") FILE IN PATIENT S COMMUNITY HEALTH RECORD FOLDER : SUBCUTANEOUS AS REQUIRED & SYRINGE PUMP PRERIPTION & ADMINISTRATION RECORD (SPAR) Abbreviations used in this document to be listed here with the full
FILE IN PATIENT S COMMUNITY HEALTH RECORD FOLDER : SUBCUTANEOUS AS REQUIRED & SYRINGE PUMP PRERIPTION & ADMINISTRATION RECORD (SPAR) Abbreviations used in this document to be listed here with the full
SCHEDULE 2 THE SERVICES
 SCHEDULE 2 THE SERVICES A. Service Specifications Mandatory headings 1 4: mandatory but detail for local determination and agreement Optional headings 5-7: optional to use, detail for local determination
SCHEDULE 2 THE SERVICES A. Service Specifications Mandatory headings 1 4: mandatory but detail for local determination and agreement Optional headings 5-7: optional to use, detail for local determination
Palliative care for heart failure patients. Susan Addie
 Palliative care for heart failure patients Susan Addie Treatments The most common limiting and distressing complaint is of fatigue and breathlessness. Optimal treatment strategies relieve symptoms, improves
Palliative care for heart failure patients Susan Addie Treatments The most common limiting and distressing complaint is of fatigue and breathlessness. Optimal treatment strategies relieve symptoms, improves
Palliative Care Out-of-hours. A resource pack for West Dorset. Contents:
 Palliative Care Out-of-hours. A resource pack for West Dorset Contents: Section 1 Supply of drugs DCH Pharmacy hours and arrangements How to contact a community pharmacist out of hours Palliative care
Palliative Care Out-of-hours. A resource pack for West Dorset Contents: Section 1 Supply of drugs DCH Pharmacy hours and arrangements How to contact a community pharmacist out of hours Palliative care
End Stage Liver Disease Regional Audit Casenote Survey
 1. This questionnaire is an audit of clinical documentation of patients who have died of end stage liver disease. If you have any questions about how this form should be completed please contact Dr Grace
1. This questionnaire is an audit of clinical documentation of patients who have died of end stage liver disease. If you have any questions about how this form should be completed please contact Dr Grace
Pharmaceutics I صيدالنيات 1. Unit 2 Route of Drug Administration
 Pharmaceutics I صيدالنيات 1 Unit 2 Route of Drug Administration 1 Routs of Drug administration The possible routes of drug entry into the body may be divided into two classes: Parenteral Rout Enteral Rout
Pharmaceutics I صيدالنيات 1 Unit 2 Route of Drug Administration 1 Routs of Drug administration The possible routes of drug entry into the body may be divided into two classes: Parenteral Rout Enteral Rout
Syringe Drivers. Back to top
 Page 1 of 8 Syringe Drivers Introduction Indications for use Advantages Method Siting syringe driver Boost facility Transfer to hospital/hospice syringe driver drugs Drug compatibility P.r.n medication
Page 1 of 8 Syringe Drivers Introduction Indications for use Advantages Method Siting syringe driver Boost facility Transfer to hospital/hospice syringe driver drugs Drug compatibility P.r.n medication
Coversheet for Network Site Specific Group Agreed Documentation
 Coversheet for Network Site Specific Group Agreed Documentation This sheet is to accompany all documentation agreed by Pan Birmingham Cancer Network Site Specific Groups. This will assist the Network Governance
Coversheet for Network Site Specific Group Agreed Documentation This sheet is to accompany all documentation agreed by Pan Birmingham Cancer Network Site Specific Groups. This will assist the Network Governance
THE EAPC OPIOID GUIDELINES: PROCESS, RESULTS AND FUTURE DEVELOPMENT
 1 THE EAPC OPIOID GUIDELINES: PROCESS, RESULTS AND FUTURE DEVELOPMENT Jaegtvolden 4-5 June 2012 14. 12. 2012 2 1 3 WHO ANALGESIC LADDER (1996) NSAID +/- Adjuvant STEP II OPIODS Opids for mild to moderate
1 THE EAPC OPIOID GUIDELINES: PROCESS, RESULTS AND FUTURE DEVELOPMENT Jaegtvolden 4-5 June 2012 14. 12. 2012 2 1 3 WHO ANALGESIC LADDER (1996) NSAID +/- Adjuvant STEP II OPIODS Opids for mild to moderate
PENNINE LANCASHIRE GUIDELINES FOR THE MANAGEMENT OF SYMPTOMS IN THE LAST DAYS OF LIFE
 PENNINE LANCASHIRE GUIDELINES FOR THE MANAGEMENT OF SYMPTOMS IN THE LAST DAYS OF LIFE Originally produced: July 2006 First Review: August 2009 Second Review: November 2011 For review November 2013 Approved
PENNINE LANCASHIRE GUIDELINES FOR THE MANAGEMENT OF SYMPTOMS IN THE LAST DAYS OF LIFE Originally produced: July 2006 First Review: August 2009 Second Review: November 2011 For review November 2013 Approved
Care of the Dying Management in Severe Renal Failure
 Care of the Dying Management in Severe Renal Failure Clinical Guideline Early diagnosis of the dying process allows for adequate preparation of the patient, the family and the carers. This clinical guidance
Care of the Dying Management in Severe Renal Failure Clinical Guideline Early diagnosis of the dying process allows for adequate preparation of the patient, the family and the carers. This clinical guidance
MORPHINE ADMINISTRATION
 Introduction Individualised Administration Drug of Choice Route of Administration & Doses Monitoring of Neonates & high risk patients Team Management Responsibility Morphine Protocol Flow Chart Introduction
Introduction Individualised Administration Drug of Choice Route of Administration & Doses Monitoring of Neonates & high risk patients Team Management Responsibility Morphine Protocol Flow Chart Introduction
Q&A: Opioid Prescribing for Chronic Non-Malignant Pain
 NHS Hastings and Rother Clinical Commissioning Group Chair Dr David Warden Chief Officer Amanda Philpott NHS Eastbourne, Hailsham and Seaford Clinical Commissioning Group Chair Dr Martin Writer Chief Officer
NHS Hastings and Rother Clinical Commissioning Group Chair Dr David Warden Chief Officer Amanda Philpott NHS Eastbourne, Hailsham and Seaford Clinical Commissioning Group Chair Dr Martin Writer Chief Officer
Care of dying adults in the last days of life. Improving care at the very end of life.
 Care of dying adults in the last days of life Improving care at the very end of life. Foreword We will all experience death, whether it is our own or that of a loved one. The bereaved person s perception
Care of dying adults in the last days of life Improving care at the very end of life. Foreword We will all experience death, whether it is our own or that of a loved one. The bereaved person s perception
Long Term Care Formulary HCD - 08
 1 of 5 PREAMBLE Opioids are an important component of the pharmaceutical armamentarium for management of chronic pain. The superiority of analgesic effect of one narcotic over another is not generally
1 of 5 PREAMBLE Opioids are an important component of the pharmaceutical armamentarium for management of chronic pain. The superiority of analgesic effect of one narcotic over another is not generally
Opioid Conversion Guidelines
 Opioid Conversion Guidelines March 2015 Gippsland Region Palliative Care Consortium Clinical Practice Group Title Keywords Ratified Opioid, Conversion, Drug, Therapy, Palliative, Guideline, Palliative,
Opioid Conversion Guidelines March 2015 Gippsland Region Palliative Care Consortium Clinical Practice Group Title Keywords Ratified Opioid, Conversion, Drug, Therapy, Palliative, Guideline, Palliative,
Analgesia. This is widely used in palliative care. It has antipyretic and analgesic effects but no anti-
 Page 1 of 8 Analgesia The World Health Organisation (WHO, 1990) has devised a model to assist health care professionals in the management of cancer pain. The recommendations include managing pain, by the
Page 1 of 8 Analgesia The World Health Organisation (WHO, 1990) has devised a model to assist health care professionals in the management of cancer pain. The recommendations include managing pain, by the
Routes of drug administration
 Routes of drug administration Definition:- A route of administration in pharmacy is the path by which a drug is taken into the body. Classification:- The various routes of administrations are classified
Routes of drug administration Definition:- A route of administration in pharmacy is the path by which a drug is taken into the body. Classification:- The various routes of administrations are classified
Palliative Prescribing - Pain
 Palliative Prescribing - Pain LAURA BARNFIELD 21/2/17 Aims To understand the classes of painkillers available in palliative care To gain confidence in counselling regarding opiates To gain confidence prescribing
Palliative Prescribing - Pain LAURA BARNFIELD 21/2/17 Aims To understand the classes of painkillers available in palliative care To gain confidence in counselling regarding opiates To gain confidence prescribing
GUIDELINES AND AUDIT IMPLEMENTATION NETWORK
 GUIDELINES AND AUDIT IMPLEMENTATION NETWORK General Palliative Care Guidelines The Management of Pain at the End Of Life November 2010 Aim To provide a user friendly, evidence based guide for the management
GUIDELINES AND AUDIT IMPLEMENTATION NETWORK General Palliative Care Guidelines The Management of Pain at the End Of Life November 2010 Aim To provide a user friendly, evidence based guide for the management
Opioid Pearls and Acute Pain Management
 Opioid Pearls and Acute Pain Management Jeanie Youngwerth, MD University of Colorado Denver Assistant Professor of Medicine, Hospitalist Associate Director, Colorado Palliative Medicine Fellowship Program
Opioid Pearls and Acute Pain Management Jeanie Youngwerth, MD University of Colorado Denver Assistant Professor of Medicine, Hospitalist Associate Director, Colorado Palliative Medicine Fellowship Program
Intranasal Medications
 Intranasal Medications Mike Harlos MD, CCFP, FCFP Professor and Section Head, Palliative Medicine, University of Manitoba Medical Director, WRHA Adult and Pediatric Palliative Care The presenter has no
Intranasal Medications Mike Harlos MD, CCFP, FCFP Professor and Section Head, Palliative Medicine, University of Manitoba Medical Director, WRHA Adult and Pediatric Palliative Care The presenter has no
Howida Kamal, Ph.D Ass. Prof. of Pharmaceutics, Cairo University
 Pharmacy Howida Kamal, Ph.D Ass. Prof. of Pharmaceutics, Cairo University Pharmacy Pharmacy Pharmaceutics The science of dosage form design. Pharmacy 1. 2. 3. Dosage forms Information Resources Use of
Pharmacy Howida Kamal, Ph.D Ass. Prof. of Pharmaceutics, Cairo University Pharmacy Pharmacy Pharmaceutics The science of dosage form design. Pharmacy 1. 2. 3. Dosage forms Information Resources Use of
MND Just in Case kit Information for GPs
 MND Just in Case kit Information for GPs What is the MND Just in Case kit? 2 Motor neurone disease (MND) is a progressive and terminal disease that results in degeneration of the motor neurones in the
MND Just in Case kit Information for GPs What is the MND Just in Case kit? 2 Motor neurone disease (MND) is a progressive and terminal disease that results in degeneration of the motor neurones in the
Berkshire West Area Prescribing Committee Guidance
 Guideline Name Berkshire West Area Prescribing Committee Guidance Date of Issue: September 2015 Review Date: September 2017 Date taken to APC: 2 nd September 2015 Date Ratified by GP MOC: Guidelines for
Guideline Name Berkshire West Area Prescribing Committee Guidance Date of Issue: September 2015 Review Date: September 2017 Date taken to APC: 2 nd September 2015 Date Ratified by GP MOC: Guidelines for
Conservative Management of Uraemia
 Conservative Management of Uraemia Information for Health Professionals Renal Department The York Hospital and Scarborough Hospital Tel: 01904 725370 For more information, please contact: The Renal Specialist
Conservative Management of Uraemia Information for Health Professionals Renal Department The York Hospital and Scarborough Hospital Tel: 01904 725370 For more information, please contact: The Renal Specialist
BACKGROUND Measuring renal function :
 A GUIDE TO USE OF COMMON PALLIATIVE CARE DRUGS IN RENAL IMPAIRMENT These guidelines bring together information and recommendations from the Palliative Care formulary (PCF5 ) BACKGROUND Measuring renal
A GUIDE TO USE OF COMMON PALLIATIVE CARE DRUGS IN RENAL IMPAIRMENT These guidelines bring together information and recommendations from the Palliative Care formulary (PCF5 ) BACKGROUND Measuring renal
Community Pharmacy Enhanced Service. Just In Case 4 Core Drugs supply. Stock Holding of Palliative Care Medicines
 Community Pharmacy Enhanced Service Just In Case 4 Core Drugs supply Stock Holding of Palliative Care Medicines Parties to the Agreement Provider: Purchaser: NHS Blackpool 1. Service description 1.1 This
Community Pharmacy Enhanced Service Just In Case 4 Core Drugs supply Stock Holding of Palliative Care Medicines Parties to the Agreement Provider: Purchaser: NHS Blackpool 1. Service description 1.1 This
Anticipatory prescribing and end of life considerations. Dr Stephanie Lippett
 Anticipatory prescribing and end of life considerations Dr Stephanie Lippett contents Pain Restlessness/agitation Nausea/vomiting Secretions Syringe driver Anticipatory prescribing Important things to
Anticipatory prescribing and end of life considerations Dr Stephanie Lippett contents Pain Restlessness/agitation Nausea/vomiting Secretions Syringe driver Anticipatory prescribing Important things to
This survey aims to look at individual practice and can be completed by any healthcare professional.
 This survey aims to look at individual practice and can be completed by any healthcare professional. If you have any questions about how this form should be completed please contact Dr Grace Ting (ghlting@doctors.net.uk)
This survey aims to look at individual practice and can be completed by any healthcare professional. If you have any questions about how this form should be completed please contact Dr Grace Ting (ghlting@doctors.net.uk)
Policy/Standard Operating Procedure/ Clinical Guideline. ELHT/CP22 Version 5.1. ELHT/CP22 Version 4.1
 TRUST WIDE/DIVISIONAL DOCUMENT Delete as appropriate Policy/Standard Operating Procedure/ Clinical Guideline DOCUMENT TITLE: Policy and Procedure for the T34 Ambulatory Syringe Pump in adults (Palliative
TRUST WIDE/DIVISIONAL DOCUMENT Delete as appropriate Policy/Standard Operating Procedure/ Clinical Guideline DOCUMENT TITLE: Policy and Procedure for the T34 Ambulatory Syringe Pump in adults (Palliative
Guidance for the Use of Subcutaneous Furosemide by Continuous Infusion for Heart Failure in Community Settings
 Guidance for the Use of Subcutaneous Furosemide by Continuous Infusion for Heart Failure in Community Settings NHS Highland Authorised by: Planning For Fairness: Yes/No (Formerly EQIA) Distribution Consultant
Guidance for the Use of Subcutaneous Furosemide by Continuous Infusion for Heart Failure in Community Settings NHS Highland Authorised by: Planning For Fairness: Yes/No (Formerly EQIA) Distribution Consultant
Drug Prescription and Administration Record
 Chart No. this admission Drug Prescription and Administration Record Patient s Name: of Admission: Chart Start : Chart Finish : NHS No: Consultant Code: Ward: ALERT: of Birth: ADDITIONAL CAUTIONS FOR PRESCRIBING
Chart No. this admission Drug Prescription and Administration Record Patient s Name: of Admission: Chart Start : Chart Finish : NHS No: Consultant Code: Ward: ALERT: of Birth: ADDITIONAL CAUTIONS FOR PRESCRIBING
Pharmacokinetics of strong opioids. Susan Addie Specialist palliative care pharmacist
 Pharmacokinetics of strong opioids Susan Addie Specialist palliative care pharmacist What is the difference between pharmacokinetics and pharmacodynamics? Definitions Pharmacokinetics = what the body does
Pharmacokinetics of strong opioids Susan Addie Specialist palliative care pharmacist What is the difference between pharmacokinetics and pharmacodynamics? Definitions Pharmacokinetics = what the body does
The last days of life in hospital and at home
 The last days of life in hospital and at home Beaumont Multi-disciplinary Palliative Care Study Day 28/9/2017 Dr Sarah McLean Consultant in Palliative Medicine St Francis Hospice Beaumont Hospital Overview
The last days of life in hospital and at home Beaumont Multi-disciplinary Palliative Care Study Day 28/9/2017 Dr Sarah McLean Consultant in Palliative Medicine St Francis Hospice Beaumont Hospital Overview
Adult Palliative and Supportive Care: Ambulatory Syringe Pump Policy including Symptom Management Guidelines
 The States of Jersey Department for H ealth & Social Services Adult Palliative and Supportive Care: Ambulatory Syringe Pump Policy including Symptom Management Guidelines [CME McKinley T34 (ml/hour)] March
The States of Jersey Department for H ealth & Social Services Adult Palliative and Supportive Care: Ambulatory Syringe Pump Policy including Symptom Management Guidelines [CME McKinley T34 (ml/hour)] March
Symptom Management Challenges at End-of-Life
 Symptom Management Challenges at End-of-Life Amanda Lovell, PharmD, BCGP Clinical Pharmacist- Inpatient Units Optum Hospice Pharmacy Services February 15, 2018 Hospice Pharmacy Services Objectives Identify
Symptom Management Challenges at End-of-Life Amanda Lovell, PharmD, BCGP Clinical Pharmacist- Inpatient Units Optum Hospice Pharmacy Services February 15, 2018 Hospice Pharmacy Services Objectives Identify
1. GUIDELINES FOR THE MANAGEMENT OF AGITATION IN ADVANCED CANCER
 1. GUIDELINES FOR THE MANAGEMENT OF AGITATION IN ADVANCED CANCER 1.1 GENERAL PRINCIPLES There are many causes of agitation in palliative care patients, which makes recommendations for treatment difficult.
1. GUIDELINES FOR THE MANAGEMENT OF AGITATION IN ADVANCED CANCER 1.1 GENERAL PRINCIPLES There are many causes of agitation in palliative care patients, which makes recommendations for treatment difficult.
GUIDELINES FOR STRONG OPIOID SUBSTITUITION IN PALLIATIVE CARE
 GUIDELINES FOR STRONG OPIOID SUBSTITUITION IN PALLIATIVE CARE 30.1 GENERAL PRINCIPLES Morphine is the strong opioid of choice in palliative care. 1, 2 Options for opioid substitution include oxycodone,
GUIDELINES FOR STRONG OPIOID SUBSTITUITION IN PALLIATIVE CARE 30.1 GENERAL PRINCIPLES Morphine is the strong opioid of choice in palliative care. 1, 2 Options for opioid substitution include oxycodone,
DRUG COMBINATIONS IN PALLIATIVE CARE: A COMPATIBILITY STUDY
 DRUG COMBINATIONS IN PALLIATIVE CARE: A COMPATIBILITY STUDY HEATHER LOUISE KEAN A thesis submitted in partial fulfilment of the requirements of Liverpool John Moores University for the degree of Master
DRUG COMBINATIONS IN PALLIATIVE CARE: A COMPATIBILITY STUDY HEATHER LOUISE KEAN A thesis submitted in partial fulfilment of the requirements of Liverpool John Moores University for the degree of Master
Guidelines: EOLC Symptom Control for Patients with Normal Renal Function (in Wandsworth)
") Guidelines: EOLC Symptom Control for Patients with Normal Renal Function (in Wandsworth) Policy Number : DC020 Issue Date: October 2014 Review date: October 2016 Policy Owner: Head Community Services Monitor:
Guidelines: EOLC Symptom Control for Patients with Normal Renal Function (in Wandsworth) Policy Number : DC020 Issue Date: October 2014 Review date: October 2016 Policy Owner: Head Community Services Monitor:
Essential Syringe Driver Training for T 34. Elaine Bird St Luke s Hospice
 Essential Syringe Driver Training for T 34 Elaine Bird St Luke s Hospice Aim For all practitioners to be accountable for their individual competence and capability when caring for a resident with a T34
Essential Syringe Driver Training for T 34 Elaine Bird St Luke s Hospice Aim For all practitioners to be accountable for their individual competence and capability when caring for a resident with a T34
New Medicines Committee Briefing November 2011 Abstral (sublingual fentanyl citrate tablet) for the management of breakthrough cancer pain
 for the management of breakthrough cancer pain") New Medicines Committee Briefing November 2011 Abstral (sublingual fentanyl citrate tablet) for the management of breakthrough cancer pain Abstral is to be reviewed for use within: Primary Care Secondary
New Medicines Committee Briefing November 2011 Abstral (sublingual fentanyl citrate tablet) for the management of breakthrough cancer pain Abstral is to be reviewed for use within: Primary Care Secondary
PHAR 7632 Chapter 7. Table Market and Share of Pharmaceuticals by ROA Data from Viswanathan, 2004
 Student Objectives for this Chapter After completing the material in this chapter each student should:- be able to describe various routes of drug administration including the concentration versus time
Student Objectives for this Chapter After completing the material in this chapter each student should:- be able to describe various routes of drug administration including the concentration versus time
SYMPTOM CONTROL IN THE LAST DAYS OF LIFE. Bradford, Airedale, Wharfedale & Craven
 Bradford, Airedale, Wharfedale & Craven Managed Clinical Network SYMPTOM CONTROL IN THE LAST DAYS OF LIFE Guidelines for Healthcare Professionals Bradford, Airedale, Wharfedale & Craven Signs and symptoms
Bradford, Airedale, Wharfedale & Craven Managed Clinical Network SYMPTOM CONTROL IN THE LAST DAYS OF LIFE Guidelines for Healthcare Professionals Bradford, Airedale, Wharfedale & Craven Signs and symptoms
Implementing the recommendation on medication management and symptom control
 Implementing the recommendation on medication management and symptom control Mike Grocott Professor of Anaesthesia and Critical Care Medicine University of Southampton Consultant in Critical Care Medicine
Implementing the recommendation on medication management and symptom control Mike Grocott Professor of Anaesthesia and Critical Care Medicine University of Southampton Consultant in Critical Care Medicine
Guidelines for the Management of Chronic Non-Malignant Pain (CNMP) in Primary Care (not including neuropathic pain (NeP).
 in Primary Care (not including neuropathic pain (NeP).") Surrey (East Surrey CCG, Guildford & Waverley CCG, North West Surrey CCG, Surrey Downs CCG & Surrey Heath CCG) North East Hampshire & Farnham CCG and Crawley, Horsham & Mid-Sussex CCG Guidelines for the
Surrey (East Surrey CCG, Guildford & Waverley CCG, North West Surrey CCG, Surrey Downs CCG & Surrey Heath CCG) North East Hampshire & Farnham CCG and Crawley, Horsham & Mid-Sussex CCG Guidelines for the
Scottish Medicines Consortium
 Scottish Medicines Consortium fentanyl 50 micrograms / dose, 100 micrograms/dose, 200 micrograms / dose nasal spray (Instanyl ) No. (579/09) Nycomed UK Ltd 09 October 2009 The Scottish Medicines Consortium
Scottish Medicines Consortium fentanyl 50 micrograms / dose, 100 micrograms/dose, 200 micrograms / dose nasal spray (Instanyl ) No. (579/09) Nycomed UK Ltd 09 October 2009 The Scottish Medicines Consortium
BJF Acute Pain Team Formulary Group
 Title Analgesia Guidelines for Acute Pain Management (Adults) in BGH Document Type Issue no Clinical guideline Clinical Governance Support Team Use Issue date April 2013 Review date April 2015 Distribution
Title Analgesia Guidelines for Acute Pain Management (Adults) in BGH Document Type Issue no Clinical guideline Clinical Governance Support Team Use Issue date April 2013 Review date April 2015 Distribution
Sedation in children and young people. Appendix J. Sedation for diagnostic and therapeutic procedures in children and young people
 SEDATION IN CHILDREN AND YOUNG PEOPLE 1 Sedation in children and young people Sedation for diagnostic and therapeutic procedures in children and young people Appendix J 2 SEDATION IN CHILDREN AND YOUNG
SEDATION IN CHILDREN AND YOUNG PEOPLE 1 Sedation in children and young people Sedation for diagnostic and therapeutic procedures in children and young people Appendix J 2 SEDATION IN CHILDREN AND YOUNG
CLINICAL POLICY FOR THE USE OF INTRANASAL DIAMORPHINE FOR ANALGESIA IN CHILDREN ATTENDING THE PAEDIATRIC EMERGENCY DEPARTMENT, SASH
 CLINICAL POLICY FOR THE USE OF INTRANASAL DIAMORPHINE FOR ANALGESIA IN CHILDREN ATTENDING THE PAEDIATRIC EMERGENCY DEPARTMENT, SASH Background Adequate analgesia is a vital aspect of early management of
CLINICAL POLICY FOR THE USE OF INTRANASAL DIAMORPHINE FOR ANALGESIA IN CHILDREN ATTENDING THE PAEDIATRIC EMERGENCY DEPARTMENT, SASH Background Adequate analgesia is a vital aspect of early management of
Using syringe pumps in palliative care
 Using syringe pumps in palliative care Facilitator: Barbara Stone RN Ground rules Medication matching game Learning outcomes To identify the indications for using a syringe pump To discuss the general
Using syringe pumps in palliative care Facilitator: Barbara Stone RN Ground rules Medication matching game Learning outcomes To identify the indications for using a syringe pump To discuss the general
Policy on Pharmacological Therapies Practice Guidance Note Reducing Dosing Errors with Opioid Medicines V04
 Policy on Pharmacological Therapies Practice Guidance Note Reducing Dosing Errors with Opioid Medicines V04 Date issued Issue 1 Nov 2018 Planned review Nov 2021 PPT-PGN 18 part of NTW(C)38 Pharmaceutical
Policy on Pharmacological Therapies Practice Guidance Note Reducing Dosing Errors with Opioid Medicines V04 Date issued Issue 1 Nov 2018 Planned review Nov 2021 PPT-PGN 18 part of NTW(C)38 Pharmaceutical
Symptom Control in the Community Setting. Dr Andrew Tysoe-Calnon
 Symptom Control in the Community Setting Dr Andrew Tysoe-Calnon Lead Consultant t Common symptoms Pain Agitation Shortness of breath Nausea and vomiting Intestinal obstruction Confusion Pain Occurs in
Symptom Control in the Community Setting Dr Andrew Tysoe-Calnon Lead Consultant t Common symptoms Pain Agitation Shortness of breath Nausea and vomiting Intestinal obstruction Confusion Pain Occurs in
Pain. Christine Illingworth. Community Nurse St Luke s Hospice 17/5/17
 Pain Christine Illingworth Community Nurse St Luke s Hospice 17/5/17 What is pain? Pain is an unpleasant sensory and emotional experience associated with actual or potential tissue damage Pain is whatever
Pain Christine Illingworth Community Nurse St Luke s Hospice 17/5/17 What is pain? Pain is an unpleasant sensory and emotional experience associated with actual or potential tissue damage Pain is whatever
Opioid Conversion Ratios - Guide to Practice 2010
 Opioid Conversion Ratios - Guide to Practice 2010 Released December 2010. 2010. The EMR PCC grants permission to reproduce parts of this publication for clinical and educational use only, provided that
Opioid Conversion Ratios - Guide to Practice 2010 Released December 2010. 2010. The EMR PCC grants permission to reproduce parts of this publication for clinical and educational use only, provided that
NOVIDADES NO TRATAMENTO COM OPIOIDES. Novelties in therapeutic with opioids. V Congresso National de Cuidados Palliativos Marco 2010, Lisboa
 NOVIDADES NO TRATAMENTO COM OPIOIDES Novelties in therapeutic with opioids V Congresso National de Cuidados Palliativos 11 12 Marco 2010, Lisboa Friedemann Nauck Department Palliative Medicine Center Anesthesiology,
NOVIDADES NO TRATAMENTO COM OPIOIDES Novelties in therapeutic with opioids V Congresso National de Cuidados Palliativos 11 12 Marco 2010, Lisboa Friedemann Nauck Department Palliative Medicine Center Anesthesiology,
Access to Palliative Care Drugs and Advice through Lothian Primary Care NHS Trust Community Pharmacy Palliative Care Network
 Access to Palliative Care Drugs and Advice through Lothian Primary Care NHS Trust Community Pharmacy Palliative Care Network Information for GPs, community pharmacists and district nurses First issued
Access to Palliative Care Drugs and Advice through Lothian Primary Care NHS Trust Community Pharmacy Palliative Care Network Information for GPs, community pharmacists and district nurses First issued
Opioid rotation or switching may be considered if a patient obtains pain relief with one opioid and is suffering severe adverse effects.
 Dose equivalence and switching between opioids Key Messages Switching from one opioid to another should only be recommended or supervised by a healthcare practitioner with adequate competence and sufficient
Dose equivalence and switching between opioids Key Messages Switching from one opioid to another should only be recommended or supervised by a healthcare practitioner with adequate competence and sufficient
Report to: Public Board of Directors Agenda item: 11 Date of Meeting: 25 July Gosport Hospital Report & RUH Assurance
 Report to: Public Board of Directors Agenda item: 11 Date of Meeting: 25 July 2018 Title of Report: Status: Board Sponsor: Author: Appendices Gosport Hospital Report & RUH Assurance For Information Dr
Report to: Public Board of Directors Agenda item: 11 Date of Meeting: 25 July 2018 Title of Report: Status: Board Sponsor: Author: Appendices Gosport Hospital Report & RUH Assurance For Information Dr
Controlled Document Number: Version Number: 1. Controlled Document Sponsor: Controlled Document Lead (Author): On: July Review Date: July 2020
: On: July Review Date: July 2020") Guidelines for the Use of Naloxone in Palliative Care in Adult Patients CONTROLLED DOCUMENT CATEGORY: CLASSIFICATION: Controlled Document Number: Version Number: 1 Controlled Document Sponsor: Controlled
Guidelines for the Use of Naloxone in Palliative Care in Adult Patients CONTROLLED DOCUMENT CATEGORY: CLASSIFICATION: Controlled Document Number: Version Number: 1 Controlled Document Sponsor: Controlled
Respiratory Secretions. Care in the last 72 hours of life Paul Tait, pharmacist
 Respiratory Secretions Care in the last 72 hours of life Paul Tait, pharmacist 50% Why? Inability to swallow & clear secretions Ineffective cough Reduced consciousness Pooling of secretions in the throat
Respiratory Secretions Care in the last 72 hours of life Paul Tait, pharmacist 50% Why? Inability to swallow & clear secretions Ineffective cough Reduced consciousness Pooling of secretions in the throat
Pharmacokinetics I. Dr. M.Mothilal Assistant professor
 Pharmacokinetics I Dr. M.Mothilal Assistant professor DRUG TRANSPORT For a drug to produce a therapeutic effect, it must reach to its target and it must accumulate at that site to reach to the minimum
Pharmacokinetics I Dr. M.Mothilal Assistant professor DRUG TRANSPORT For a drug to produce a therapeutic effect, it must reach to its target and it must accumulate at that site to reach to the minimum
POLICY / PROCEDURE FOR THE USE OF THE McKinley T34 SYRINGE DRIVER
 POLICY / PROCEDURE FOR THE USE OF THE McKinley T34 SYRINGE DRIVER This is a working document and any changes that become necessary to this policy must be notified in writing to the Macmillan Pharmacist
POLICY / PROCEDURE FOR THE USE OF THE McKinley T34 SYRINGE DRIVER This is a working document and any changes that become necessary to this policy must be notified in writing to the Macmillan Pharmacist
SPAGG. Coversheet for Specialist Palliative Audit and Guideline Group Agreed Documentation
 SPAGG Coversheet for Specialist Palliative Audit and Guideline Group Agreed Documentation This sheet is to accompany all documentation agreed by SPAGG. This will assist maintenance of the guidelines as
SPAGG Coversheet for Specialist Palliative Audit and Guideline Group Agreed Documentation This sheet is to accompany all documentation agreed by SPAGG. This will assist maintenance of the guidelines as