Using syringe pumps in palliative care
|
|
|
- Malcolm Miller
- 5 years ago
- Views:
Transcription
1 Using syringe pumps in palliative care Facilitator: Barbara Stone RN

2 Ground rules

3 Medication matching game
4 Learning outcomes To identify the indications for using a syringe pump To discuss the general principles when caring for someone with a pump To identify your professional accountability To identify and understand medications commonly used To increase confidence and competence in assembling and setting up the McKinley T34 syringe pump correctly and knowing how to problem solve pump related problems To understand how to record the use of the pump
5 WHO Definition of Palliative care Palliative care is an approach that improves the quality of life of patients and their families facing the problem associated with life-threatening illness, through the prevention and relief of suffering by means of early identification and impeccable assessment and treatment of pain and other problems, physical, psychosocial and spiritual.
6 What are the legal considerations? NMC Your accountability Duty of care Best practice Evidence based v best established practice lack of research due to ethics Not always one solution discuss with other Heath Care Professionals Doctrine of double effect interventions need to be appropriate, proportionate and with the intent to treat symptoms.
7 Standards for medicines management (2007) The administration of medicines is an important aspect of the professional practice of persons whose name is on the register. It is not solely a mechanistic task to be performed in strict compliance with the written prescription of a medical practitioner (can now also be an independent and supplementary prescriber).. It requires thought and the exercise of professional judgement ndards/nmc-standards-for-medicines-management.pdf
8 The Consumer Protection Act 1987 and Medicines Act 1968 These acts require that in accordance with the directions of an appropriate practitioner the: Right Medicine is given To the right patient At the right time In the right forms of the drug At the right dose
9 Nice Guidance states Consider using a syringe pump to deliver medicines for continuous symptom control if more than 2 or 3 doses of any 'as required' (subcutaneous s/c) medicines have been given within 24 hours


10 Which patients do you consider would benefit from a syringe pump?
11 End of life patients (weak, cachetic) Uncontrolled nausea/vomiting Patients with impaired absorption due to vomiting or profuse diarrhoea Patients with bowel obstruction Patients with dysphagia Uncontrolled pain Not always associated with end of life scenarios
12 You visit your patient who appears uncomfortable Before considering a syringe pump, what else do you need to do/consider?
13 Consider Assess the situation and take a history. Has anything changed. What makes it better or worse Treatment related (chemo / radiotherapy, surgery) Full bladder? Loaded rectum? Reversible causes infection, constipation, hypercalcaemia, etc Position Not taking prescribed medication? Never assume!
14 What questions might you expect patients and families to ask? Does this mean I am dying? Does this hasten death/slow it down? How long will I have it? Can I Bath/Shower? (No) Can I go on holiday? What do I do if it stops working/who to contact? This will be a constant reminder of my illness?

15 What do you need to tell the patient &/or family/carer?
16 What do you need to tell the patient/family and carer? Explain rationale and seek consent. Explain likely effects of medication. Takes at least 4 hours to reach effective levels They will receive a daily visit (offer a time) to reassess We may need a period of time to reassess and readjust medication. We don t always get the dose right 1 st time. Stat injections available/given initially to manage this. Information re needle site/managing ADL s/battery/alarms/is dropped Ensure that they know who to call/contact if concerned

17 You have decided that a syringe pump is appropriate. How quickly will it work?

18 What kind of things do we need to think about/anticipate when setting up a pump?
19 Give a stat injection- consider use of just in case meds (may already be in home) Access a pump Discuss with prescriber Anticipatory prescribing (stat doses and dose ranges) especially for end of life care Correct documentation Access to pharmacy Check allergies Consider side effects of the drugs explain to patient and relatives.
20 Recording Prescription
21 Bolus Injections
22 Medication stock record
23 Administration record
24 Community Hospital Administration Record


25 What drugs are used in a syringe pump? Analgesics Consider the 4 A s Anti emetics Antispasmodics/anti secretion Agitation

26 Which drugs and what for?
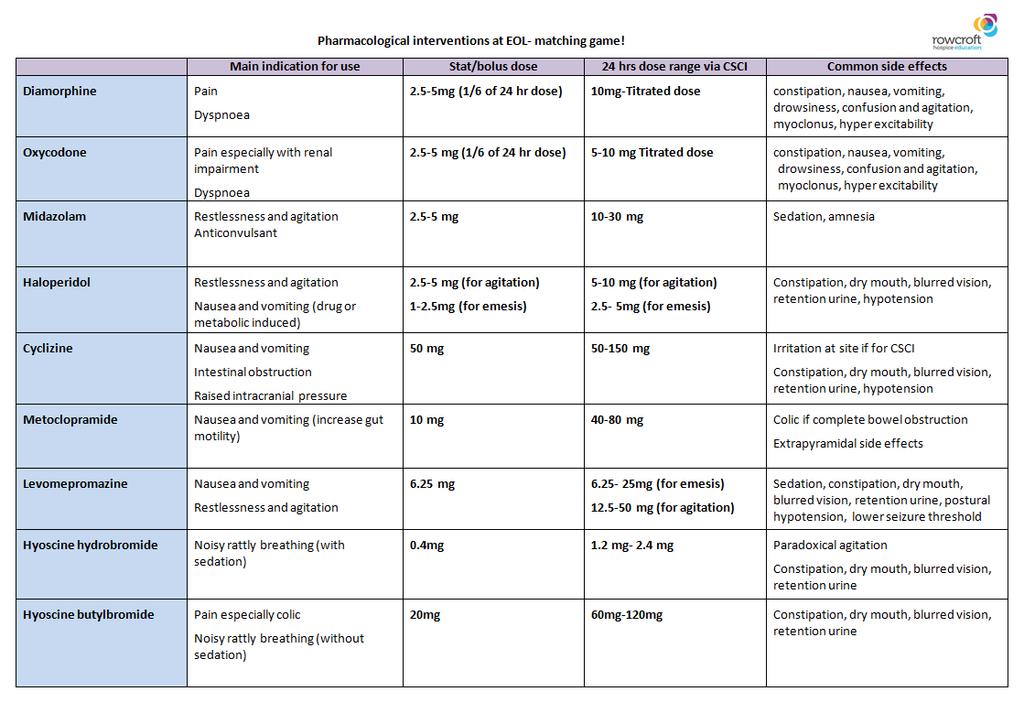
27 Pain Nausea and vomiting Restlessness/ agitation Noisy rattly breathing Morphine/diamorphine Midazolam Hyoscine butylbromide Levomepromazine Hyoscine hydrobromide Oxycodone Cyclizine Haloperidol Metoclopromide

28 Analgesics
29 Analgesics Diamorphine- drug of choice due to its solubility Morphine- same properties, larger volume in ampoules Oxycodone- synthetic opioid used as alternative to morphine
30 Diamorphine/ Morphine Indication Pain / Dyspnoea 24 hour dose 5 mg no max, need for titration Prn dose 2.5 mg 5 mg (6 th of 24 hr dose) Compatibility With most drugs Consider Gold standard opiate, constipation, nausea, confusion and agitation
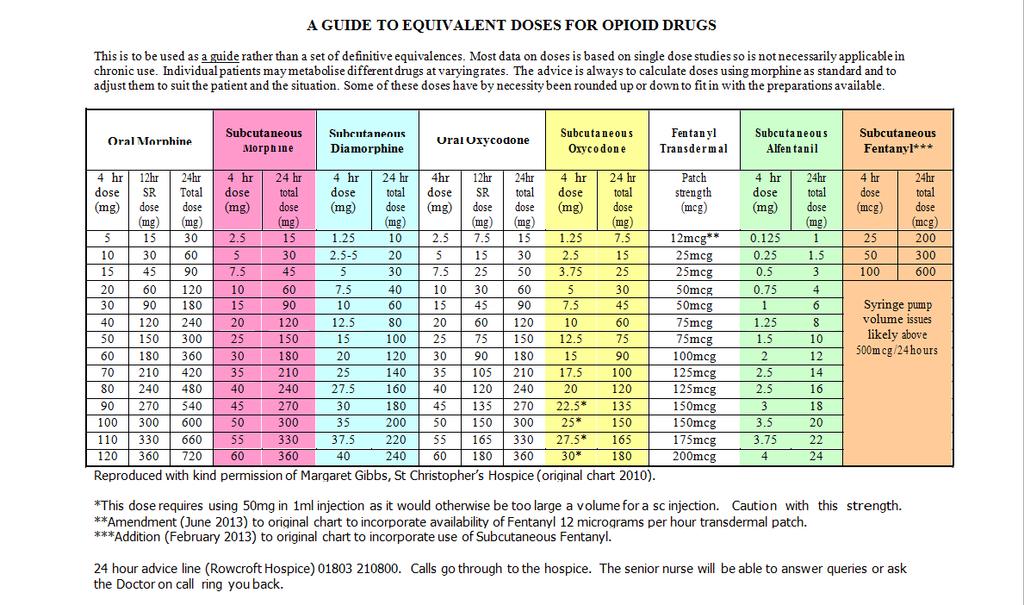
31 Conversions 30mg oral morphine mg s/c morphine 10 mg s/c diamorphine
32 Dose conversion Oral morphine to s/c morphine = half oral dose Oral morphine to s/c diamorphine = one third oral dose Back I (2001) Palliative Medicine Handbook Twycross R (1998) Palliative Care Formulary
33 Oxycodone Indications Pain/Dyspnoea 24 Hour dose mgs No max, Need for titration PRN dose 1/6 th of 24 hour dose Compatibility With most drugs Consider 2 nd line opiate. Double strength of morphine. Still constipating Available as 10mg/1ml ampoule 20mg/2ml ampoule 50mg/1ml ampoule Sometimes used as alternative to morphine e.g. if side effects undesirable and in renal impairment
34 Converting oxycodone Oral Oxycodone is twice the strength of oral morphine s/c oxycodone is twice the strength of oral oxycodone Therefore: 20mg of oral morphine = 10 mg of oral oxycodone = 5mg s/c oxycodone
35 Converting oxycodone 15mg oral oxycodone 7.5 mg s/c oxycodone 10mg s/c diamorphine 30mg oral morphine
36 Alternative opioids in use Fentanyl and alfentanyl are also available for use, sometimes when an opioid switch is desired or potentially for people with severe renal impairment. If someone is already using a fentanyl or buprenorphine patch - leave it on and give additional opiates via the syringe pump Contact Rowcroft for any further help
37
38 Antiemetics
39 Antiemetics, which would you use? levomepromazine haloperidol Which one metoclopramide cyclizine

40 What makes us sick?

41 The three b s! Biochemical Bowel Brain
42 Bowel Induced by stimulation of vagus nerve Causes include constipation, gastric stasis, obstruction, squashed stomach syndrome, hepatomegaly, ascites, and opioids that slow the gut Drug of choice 1 st line metoclopramide 30-80mg / 24hrs Stat dose of metoclopramide 10mg s/c
43 Biochemical Stimulation of dopamine receptors in the chemo receptor trigger zone (CTZ) Causes include toxins in blood, renal impairment, electrolyte imbalance, hypercalcaemia, infection. Drugs of choice Haloperidol or levomepromazine which block dopamine receptors in the brain. Haloperidol mg over 24 hours s/c 1-3mg s/c injection daily/b.d. Levomepromazine mg over 24 hours s/c Stat mg s/c injection 6-8 hourly
44 Brain Induced by direct pressure / stimulation on the vomiting centre Causes include brain tumours, raised intracranial pressure, motion sickness, radiotherapy (inflammation). Drug of choice cyclizine, antihistamine which blocks the M and H1 (muscarinic and histamine) receptors. Cyclizine mg over 24 hours s/c. Stat dose 50mg 8 hourly, max 150mg in 24 hours Observe for crystallisation, does not mix well with morphine. It can be used, but be aware.
45 Other drugs used as antiemetic's Dexamethasone reduces tumour pressure or oedema or damage from chemotherapy. Given as a stat rather than in a syringe pump. Ondansetron chemotherapy specific, targets one receptor site, 5HT3 antagonist.
46 Antispasmodics/antisecretory
47 Hyoscine Butylbromide Other name Buscopan Indication Antispasmodic (colic) / Antisecretory 24 hour dose mg over 24 hours PRN dose Compatibility 10 20mgs TDS Incompatible with Cyclizine Consider Constipation, as can dry the bowel and reduce peristalsis. Non-sedative.
48 Hyoscine Hydrobromide Indication Antisecretory 24 hour dose mg Prn dose mcg sc Consider It is sedative so be cautious and explain to patient and relatives. Can cause paradoxical agitation. Give with midazolam 2.5mg sc or levomepromazine 6.25mg sc (unless already in the pump)

49 Agitation and restlessness
50 Midazolam Benzodiazepine - in same group of medicines as diazepam and lorazepam. Indication Anxiety, fitting, sedation 24 hour dose 10mg 50mg Prn dose mg 4hrly Compatibility With most drugs Consider Sedative. Order 10mg/2ml as 5mg/5ml are large for stat doses.
51 Other drugs which may be used in syringe pumps Glycopyrronium for secretions Octreotide used in bowel obstruction and some fistulas to reduce gastric output
52 Which drugs are not suitable for use in a syringe pump? Diazepam Prochlorperazine Chlorpromazine Lorazepam

53 South & West Devon Formulary Chapter 16

54 Siting the cannula Where do you site them?
55 Sites Chest, arm, abdomen (caution if oedema or ascites present) Scapula useful in the agitated patient Avoid tumour site. As in breast cancer, for example, if considering chest placement. Consider body image Cachexia can limit options
56 What will you see if there are site problems? (continued) Infection Site reactions reduced since cannulas now mostly plastic Recommend to change site approximately every 72 hours


57 Saflo sizes 6mm green 9mm blue Use 100cm tubing
58 Saflo 90 Remove the Saflo 90 from its packaging. Ensure that the needle protector is in place and there are no visible signs of damage to the product. Note the product code and batch number if required for record keeping. Prime the infusion set Prepare the infusion site according to local guidelines.
59 Saflo 90 2: Remove the central portions of the tape from the infusion set 3: When ready to insert the infusion set, remove the needle protector
60 Saflo 90 4: Insert the infusion set into the tissue with a smooth downward motion. Press the central portion of the tape to ensure the infusion set is firmly attached to the skin 5: Remove the side portions of the tape backing and smooth the tape onto the skin surface
61 Saflo 90 6: Twist the cap of the device gently to the left through approximately ¼ turn. A click will be heard and a visible indicator will appear at the top of the cap to show that the needle has been withdrawn and is fully protected. 7: Hold down the tape of the infusion set and lift the needle assembly away from the site.

62 Saflo 90 Move the protective cover along the tubing and press gently down onto the infusion site Dispose of the protected needle assembly in a container suitable for contaminated waste according to local procedures

63 Saflo Needle Safe subcutaneous infusion system 45 Ideal for emaciated or cachexic patients Both 45, 90 need to be monitored and changed every 72 hours

64 What will you see if there are problems with the site? Redness Inflammation Hardness Irritation Pain Infection
65 What can be done about site problems Consider diluting further/using larger syringe Cyclizine and levomepromazine are particularly irritant Do not assume needle allergy Water for injection is the diluent of choice Saline is occasionally used if levomepromazine is the only drug used Generally limit to 3 drugs in the driver Change site more regularly Consider adding dexamethasone 0.5mg 1mg
66 Step by step guide Obtain informed consent. Provide information leaflet (A guide for patients & carers) Use a luer-lok syringe & draw up to 10ml in 10ml syringe, 17ml in 20ml syringe, 22ml in 30ml syringe Draw up medication checking against administration record: drug, dose, date& time, route & method, diluents, validity, legibility, signature of doctor/prescriber. Inspect for discolouration.
67
68 Rowcroft Community Team Who we are? Clinical Nurse Specialists Occupational Therapists Social Workers Medical Consultant and team Secretary
69 When should you consult with the Community Specialist Palliative Care Team? Complex symptom control problems Complex support issues Support at End of Life Needs led rather than diagnosis / extent of disease Patients should receive basic palliative care from all health and social care professionals Tel:
70 Rowcroft Hospice at Home Team Provide support and care for people in the community setting who are in the last two weeks of life Available 24/7/365 for telephone advice, to take referrals and provide direct care where appropriate Unable to take referrals just to recharge syringe pumps, but more than happy to give advice in their use Full referral details on the Rowcroft website Tel:
71

72 Free access to end of life e learning e-elca a free end of life care e learning site with syringe driver training module For local South West organisations some pathways have also been developed and can be found here:-

73 Our ambition is for everyone across Torbay and South Devon to view this short film. The purpose of the video is to discover people's comfort in talking about death and dying. Talking about dying may not be easy, but could be one of the most important conversations you will ever have. Click on the picture to go to the film
74 References Palliative Care Formulary 5, (2014), Ed. Twycross, R., Wilcock, A. & Howard, P. Palliativedrugs.com, Nottingham. Dickman, A. (2012) Drugs In Palliative Care (2nd Edition), Oxford University Press, Oxford. British National Formulary 70, (2016), BMJ Group & Pharmaceutical Press, London. Dickman, A. and Schneider, J. (2016) The Syringe Driver Continuous subcutaneous infusions in palliative care, (4 th Edition) Oxford University Press, Oxford.

75
Syringe driver in Palliative Care
 Syringe driver in Palliative Care Introduction: Syringe drivers are portable, battery operated devices widely used in palliative care to deliver medication as a continuous subcutaneous infusion over 24
Syringe driver in Palliative Care Introduction: Syringe drivers are portable, battery operated devices widely used in palliative care to deliver medication as a continuous subcutaneous infusion over 24
End of life prescribing guidance
 End of life prescribing guidance Introduction This guidance has been prepared to ASSIST IN DECISION MAKING for the prescribing and monitoring of medicines useful in the management of symptoms commonly
End of life prescribing guidance Introduction This guidance has been prepared to ASSIST IN DECISION MAKING for the prescribing and monitoring of medicines useful in the management of symptoms commonly
PAIN AND SYMPTOM MANAGEMENT GUIDANCE IN THE LAST DAYS OF LIFE
 PAIN AND SYMPTOM MANAGEMENT GUIDANCE IN THE LAST DAYS OF LIFE Reference: DCM029 Version: 1.1 This version issued: 07/06/18 Result of last review: Minor changes Date approved by owner (if applicable): N/A
PAIN AND SYMPTOM MANAGEMENT GUIDANCE IN THE LAST DAYS OF LIFE Reference: DCM029 Version: 1.1 This version issued: 07/06/18 Result of last review: Minor changes Date approved by owner (if applicable): N/A
Renal Prescribing at End of Life Guidance for Anticipatory prescribing for patients in renal failure (egfr<30) at the end of life
 at the end of life") Guidance for Anticipatory prescribing for patients in renal failure (egfr
Guidance for Anticipatory prescribing for patients in renal failure (egfr
[Type text] Anticipatory Medication STAT dose and Syringe Driver Guidance [Type text]
![[Type text] Anticipatory Medication STAT dose and Syringe Driver Guidance [Type text]](/thumbs/92/110296570.jpg "[Type text] Anticipatory Medication STAT dose and Syringe Driver Guidance [Type text]") [Type text] Anticipatory Medication STAT dose and Syringe Driver Guidance [Type text] Patients with egfr greater than 30mL/min Patients with egfr less than 30mL/min Symptom Drug Dose Symptom Drug Dose
[Type text] Anticipatory Medication STAT dose and Syringe Driver Guidance [Type text] Patients with egfr greater than 30mL/min Patients with egfr less than 30mL/min Symptom Drug Dose Symptom Drug Dose
MMG035 Symptom Management Guidelines for a Person thought to be in the Last Few Days and Hours of Life
 MMG035 Symptom Management Guidelines for a Person thought to be in the Last Few Days and Hours of Life The following pages are guidelines for the management of common symptoms for a person thought to be
MMG035 Symptom Management Guidelines for a Person thought to be in the Last Few Days and Hours of Life The following pages are guidelines for the management of common symptoms for a person thought to be
Clatterbridge Centre for Oncology
 Clatterbridge Centre for Oncology CONTENTS 1. Why and when to use a syringe driver 2. Siting the syringe driver 3. Mixing and measuring 4. Setting up the syringe driver 5. Drug information 6. Common problems
Clatterbridge Centre for Oncology CONTENTS 1. Why and when to use a syringe driver 2. Siting the syringe driver 3. Mixing and measuring 4. Setting up the syringe driver 5. Drug information 6. Common problems
Supporting Last Days of Life Symptom Control Medication Guidance: Algorithm. Agitation & Anxiety
 Agitation & Anxiety (Exclude or treat REVERSIBLE causes*) Patient is anxious / frightened, but lucid Patient is confused, agitated and / or hallucinating MIDAZOLAM 2.5-5mg s/c (Max total 24 hour dose of
Agitation & Anxiety (Exclude or treat REVERSIBLE causes*) Patient is anxious / frightened, but lucid Patient is confused, agitated and / or hallucinating MIDAZOLAM 2.5-5mg s/c (Max total 24 hour dose of
SYRINGE DRIVER MEDICATIONS
 SYRINGE DRIVER MEDICATIONS Christine Hull & Anita Webb Staff Nurses, Hospice in the Home 2015 Analgesics:- Groups of Medication used in Syringe Drivers Morphine sulphate Diamorphine Oxycodone Alfentanil
SYRINGE DRIVER MEDICATIONS Christine Hull & Anita Webb Staff Nurses, Hospice in the Home 2015 Analgesics:- Groups of Medication used in Syringe Drivers Morphine sulphate Diamorphine Oxycodone Alfentanil
PAIN MANAGEMENT Patient established on oral morphine or opioid naive.
 PAIN MANAGEMENT Patient established on oral morphine or opioid naive. Important; It is the responsibility of the prescriber to ensure that guidelines are followed when prescribing opioids. Every member
PAIN MANAGEMENT Patient established on oral morphine or opioid naive. Important; It is the responsibility of the prescriber to ensure that guidelines are followed when prescribing opioids. Every member
PAIN MANAGEMENT Person established taking oral morphine or opioid naive.
 PAIN MANAGEMENT Person established taking oral morphine or opioid naive. Important; it is the responsibility of the prescriber to ensure that guidelines are followed when prescribing opioids. Every member
PAIN MANAGEMENT Person established taking oral morphine or opioid naive. Important; it is the responsibility of the prescriber to ensure that guidelines are followed when prescribing opioids. Every member
Care in the Last Days of Life
 Care in the Last Days of Life Introduction This guideline is an aid to clinical decision making and good practice in person-centred care for patients who are deteriorating and at risk of dying. The patient
Care in the Last Days of Life Introduction This guideline is an aid to clinical decision making and good practice in person-centred care for patients who are deteriorating and at risk of dying. The patient
Renal Palliative Care Last Days of Life
 Renal Palliative Care Last Days of Life Introduction This guideline is an aid to clinical decision-making and good practice for patients with stage 4-5 chronic kidney disease (egfr
Renal Palliative Care Last Days of Life Introduction This guideline is an aid to clinical decision-making and good practice for patients with stage 4-5 chronic kidney disease (egfr
PRESCRIBING GUIDELINES FOR SYMPTOM MANAGEMENT IN THE DYING PATIENT
 PRESCRIBING GUIDELINES FOR SYMPTOM MANAGEMENT IN THE DYING PATIENT A collaboration between: St. Rocco s Hospice, Bridgewater Community Healthcare NHS Trust, NHS Warrington Clinical Commissioning Group,
PRESCRIBING GUIDELINES FOR SYMPTOM MANAGEMENT IN THE DYING PATIENT A collaboration between: St. Rocco s Hospice, Bridgewater Community Healthcare NHS Trust, NHS Warrington Clinical Commissioning Group,
Algorithms for Symptom Management. In End of Life Care
 Algorithms for Symptom Management In End of Life Care The Use of Drugs Beyond Licence (off label) -The Medicines and Healthcare Products Regulatory Agency (MHRA) in the UK regulates the activity of the
Algorithms for Symptom Management In End of Life Care The Use of Drugs Beyond Licence (off label) -The Medicines and Healthcare Products Regulatory Agency (MHRA) in the UK regulates the activity of the
SYMPTOM MANAGEMENT GUIDANCE FOR PATIENTS RECEIVING PALLIATIVE CARE AT ROYAL DERBY HOSPITAL
 SYMPTOM MANAGEMENT GUIDANCE FOR PATIENTS RECEIVING PALLIATIVE CARE AT ROYAL DERBY HOSPITAL If a patient is believed to be approaching the end of their life, medication should be prescribed in anticipation
SYMPTOM MANAGEMENT GUIDANCE FOR PATIENTS RECEIVING PALLIATIVE CARE AT ROYAL DERBY HOSPITAL If a patient is believed to be approaching the end of their life, medication should be prescribed in anticipation
Care of the Dying. For dosing in severe renal impairment see separate guidance for care of the dying in severe renal failure.
 Care of the Dying Early diagnosis of the dying process allows for adequate preparation of the patient, the family and the carers. This clinical guidance covers the prescribing and management of patients
Care of the Dying Early diagnosis of the dying process allows for adequate preparation of the patient, the family and the carers. This clinical guidance covers the prescribing and management of patients
Anticipatory Medications for End of Life Patients. Doses must be proportional to the current analgesic medication YES NO YES NO
 Anticipatory Medications for End of Life Patients oses must be proportional to the current analgesic medication Please refer ALL patients on Methadone or Ketamine to palliative care team for advice. Patients
Anticipatory Medications for End of Life Patients oses must be proportional to the current analgesic medication Please refer ALL patients on Methadone or Ketamine to palliative care team for advice. Patients
Syringe Drivers. Back to top
 Page 1 of 8 Syringe Drivers Introduction Indications for use Advantages Method Siting syringe driver Boost facility Transfer to hospital/hospice syringe driver drugs Drug compatibility P.r.n medication
Page 1 of 8 Syringe Drivers Introduction Indications for use Advantages Method Siting syringe driver Boost facility Transfer to hospital/hospice syringe driver drugs Drug compatibility P.r.n medication
ALLERGIES/ SENSITIVITIES This section must be completed before prescribing/administering any drug
 COMMUNITY PRESCRIPTION CHART All entries should be in CAPITAL letters and in indelible black ink. If medications/ doses are stopped, cross through the relevant line clearly to avoid error. GP: PRESCRIBER
COMMUNITY PRESCRIPTION CHART All entries should be in CAPITAL letters and in indelible black ink. If medications/ doses are stopped, cross through the relevant line clearly to avoid error. GP: PRESCRIBER
ANTICIPATORY PRESCRIBING FOR PATIENTS AT END OF LIFE WITH RENAL IMPAIRMENT
 ANTICIPATORY PRESCRIBING FOR PATIENTS AT END OF LIFE WITH RENAL Doses of opiates must be proptional to current analgesic medication Please refer ALL patients on Methadone Ketamine to SPCT f advice. Patients
ANTICIPATORY PRESCRIBING FOR PATIENTS AT END OF LIFE WITH RENAL Doses of opiates must be proptional to current analgesic medication Please refer ALL patients on Methadone Ketamine to SPCT f advice. Patients
Supportive Care. End of Life Phase
 Supportive Care End of Life Phase Guidelines for Health Care Professionals In the care of patients with established renal failure who are in the last days of life References: Chambers E J (2004) End of
Supportive Care End of Life Phase Guidelines for Health Care Professionals In the care of patients with established renal failure who are in the last days of life References: Chambers E J (2004) End of
Symptom Management Guidelines for End of Life Care
 Symptom Management Guidelines for End of Life Care The following pages are guidelines for the management of common symptoms in the last few days of life. General principles: 1. Consider how symptoms can
Symptom Management Guidelines for End of Life Care The following pages are guidelines for the management of common symptoms in the last few days of life. General principles: 1. Consider how symptoms can
Care of the Dying Management in Severe Renal Failure
 Care of the Dying Management in Severe Renal Failure Clinical Guideline Early recognition of the dying process allows for adequate preparation of the patient, the family and the carers. This clinical guidance
Care of the Dying Management in Severe Renal Failure Clinical Guideline Early recognition of the dying process allows for adequate preparation of the patient, the family and the carers. This clinical guidance
Care of the Dying Management in Severe Renal Failure
 Care of the Dying Management in Severe Renal Failure Clinical Guideline Early diagnosis of the dying process allows for adequate preparation of the patient, the family and the carers. This clinical guidance
Care of the Dying Management in Severe Renal Failure Clinical Guideline Early diagnosis of the dying process allows for adequate preparation of the patient, the family and the carers. This clinical guidance
For patients and their carers this means smoother symptom control, better support in a crisis, and avoidance of admission if that is their choice.
 Bedfordshire Palliative Care Palliative Care Medicines Guidance This folder has been produced to support professionals providing palliative care in any setting. Its aim is to make best practice in palliative
Bedfordshire Palliative Care Palliative Care Medicines Guidance This folder has been produced to support professionals providing palliative care in any setting. Its aim is to make best practice in palliative
GUIDELINES FOR PRESCRIBING AT THE END OF LIFE FOR PATIENTS WITH RENAL IMPAIRMENT (estimated glomerular filtration rate<30)
") GUIDELINES FOR PRESCRIBING AT THE END OF LIFE FOR PATIENTS WITH RENAL IMPAIRMENT These guidelines have been produced in collaboration with Dr Lucy Smyth, Consultant in Renal Medicine, Royal Devon and Exeter
GUIDELINES FOR PRESCRIBING AT THE END OF LIFE FOR PATIENTS WITH RENAL IMPAIRMENT These guidelines have been produced in collaboration with Dr Lucy Smyth, Consultant in Renal Medicine, Royal Devon and Exeter
Essential Syringe Driver Training for T 34. Elaine Bird St Luke s Hospice
 Essential Syringe Driver Training for T 34 Elaine Bird St Luke s Hospice Aim For all practitioners to be accountable for their individual competence and capability when caring for a resident with a T34
Essential Syringe Driver Training for T 34 Elaine Bird St Luke s Hospice Aim For all practitioners to be accountable for their individual competence and capability when caring for a resident with a T34
Diamorphine 4 hour. alfentanil (500microgram/mL) Calculated by dividing 24 hour oral morphine dose by 30
 Calculated by dividing 24 hour oral morphine dose by 30") If more information is required please seek help from specialist palliative care pioid dose conversion chart, syringe driver doses, rescue/prn doses and opioid patches Use the conversion chart to work
If more information is required please seek help from specialist palliative care pioid dose conversion chart, syringe driver doses, rescue/prn doses and opioid patches Use the conversion chart to work
Doncaster & Bassetlaw Cancer Locality. Palliative Care Core Formulary
 Doncaster & Bassetlaw Cancer Locality Palliative Core Formulary Approved by Doncaster & Bassetlaw Hospitals NHS Foundation Trust Drugs and Therapeutics Committee. DJ14/2155 Oct 2014 Review date: Oct 2017
Doncaster & Bassetlaw Cancer Locality Palliative Core Formulary Approved by Doncaster & Bassetlaw Hospitals NHS Foundation Trust Drugs and Therapeutics Committee. DJ14/2155 Oct 2014 Review date: Oct 2017
We would like to thank you for completing this audit questionnaire which looks at how you manage nausea and vomiting in palliative care patients.
 We would like to thank you for completing this audit questionnaire which looks at how you manage nausea and vomiting in palliative care patients. The closing date for responses is 19th December The results
We would like to thank you for completing this audit questionnaire which looks at how you manage nausea and vomiting in palliative care patients. The closing date for responses is 19th December The results
Guidelines: EOLC Symptom Control for Patients with Normal Renal Function (in Wandsworth)
") Guidelines: EOLC Symptom Control for Patients with Normal Renal Function (in Wandsworth) Policy Number : DC020 Issue Date: October 2014 Review date: October 2016 Policy Owner: Head Community Services Monitor:
Guidelines: EOLC Symptom Control for Patients with Normal Renal Function (in Wandsworth) Policy Number : DC020 Issue Date: October 2014 Review date: October 2016 Policy Owner: Head Community Services Monitor:
PHARMACY SERVICE ARRANGEMENTS FOR THE SUPPLY OF PALLIATIVE CARE SYRINGES AND MEDICINES FOR COMMUNITY PATIENTS
 PHARMACY SERVICE ARRANGEMENTS FOR THE SUPPLY OF PALLIATIVE CARE SYRINGES AND MEDICINES FOR COMMUNITY PATIENTS The benefits of prefilled syringes for palliative care from the hospital pharmacy service In
PHARMACY SERVICE ARRANGEMENTS FOR THE SUPPLY OF PALLIATIVE CARE SYRINGES AND MEDICINES FOR COMMUNITY PATIENTS The benefits of prefilled syringes for palliative care from the hospital pharmacy service In
Palliative care for heart failure patients. Susan Addie
 Palliative care for heart failure patients Susan Addie Treatments The most common limiting and distressing complaint is of fatigue and breathlessness. Optimal treatment strategies relieve symptoms, improves
Palliative care for heart failure patients Susan Addie Treatments The most common limiting and distressing complaint is of fatigue and breathlessness. Optimal treatment strategies relieve symptoms, improves
SUBCUTANEOUS AS REQUIRED & SYRINGE PUMP PRESCRIPTION & ADMINISTRATION RECORD (SPAR) Name: Address: Postcode: Date of Birth: NHS Number:
 Name: Address: Postcode: Date of Birth: NHS Number:") FILE IN PATIENT S COMMUNITY HEALTH RECORD FOLDER : SUBCUTANEOUS AS REQUIRED & SYRINGE PUMP PRERIPTION & ADMINISTRATION RECORD (SPAR) Abbreviations used in this document to be listed here with the full
FILE IN PATIENT S COMMUNITY HEALTH RECORD FOLDER : SUBCUTANEOUS AS REQUIRED & SYRINGE PUMP PRERIPTION & ADMINISTRATION RECORD (SPAR) Abbreviations used in this document to be listed here with the full
Conservative Management of Uraemia
 Conservative Management of Uraemia Information for Health Professionals Renal Department The York Hospital and Scarborough Hospital Tel: 01904 725370 For more information, please contact: The Renal Specialist
Conservative Management of Uraemia Information for Health Professionals Renal Department The York Hospital and Scarborough Hospital Tel: 01904 725370 For more information, please contact: The Renal Specialist
Care of dying adults in the last days of life. Improving care at the very end of life.
 Care of dying adults in the last days of life Improving care at the very end of life. Foreword We will all experience death, whether it is our own or that of a loved one. The bereaved person s perception
Care of dying adults in the last days of life Improving care at the very end of life. Foreword We will all experience death, whether it is our own or that of a loved one. The bereaved person s perception
EAST LANCASHIRE GUIDELINES FOR THE MANAGEMENT OF SYMPTOMS IN THE LAST DAYS OF LIFE
 EAST LANCASHIRE SPECIALIST PALLIATIVE CARE TEAM EAST LANCASHIRE GUIDELINES FOR THE MANAGEMENT OF SYMPTOMS IN THE LAST DAYS OF LIFE Reviewed and updated August 2009 Next review date August 2011 Approved
EAST LANCASHIRE SPECIALIST PALLIATIVE CARE TEAM EAST LANCASHIRE GUIDELINES FOR THE MANAGEMENT OF SYMPTOMS IN THE LAST DAYS OF LIFE Reviewed and updated August 2009 Next review date August 2011 Approved
SYMPTOM CONTROL IN THE LAST DAYS OF LIFE. Bradford, Airedale, Wharfedale & Craven
 Bradford, Airedale, Wharfedale & Craven Managed Clinical Network SYMPTOM CONTROL IN THE LAST DAYS OF LIFE Guidelines for Healthcare Professionals Bradford, Airedale, Wharfedale & Craven Signs and symptoms
Bradford, Airedale, Wharfedale & Craven Managed Clinical Network SYMPTOM CONTROL IN THE LAST DAYS OF LIFE Guidelines for Healthcare Professionals Bradford, Airedale, Wharfedale & Craven Signs and symptoms
Palliative Care Impact Survey
 September 2018 Contents Introduction...3 Headlines...3 Approach...4 Findings...4 Which guideline are used...4 How and where the guidelines are used...6 Alternative sources of information...7 Use of the
September 2018 Contents Introduction...3 Headlines...3 Approach...4 Findings...4 Which guideline are used...4 How and where the guidelines are used...6 Alternative sources of information...7 Use of the
BACKGROUND Measuring renal function :
 A GUIDE TO USE OF COMMON PALLIATIVE CARE DRUGS IN RENAL IMPAIRMENT These guidelines bring together information and recommendations from the Palliative Care formulary (PCF5 ) BACKGROUND Measuring renal
A GUIDE TO USE OF COMMON PALLIATIVE CARE DRUGS IN RENAL IMPAIRMENT These guidelines bring together information and recommendations from the Palliative Care formulary (PCF5 ) BACKGROUND Measuring renal
Isle of Wight Syringe Driver Compatibility Guidelines
 Isle of Wight Syringe Driver Compatibility Guidelines Produced by The Earl Mountbatten Hospice, Isle of Wight Written January 2015, revision due January 2018 This guideline is available as a paper pocketbook
Isle of Wight Syringe Driver Compatibility Guidelines Produced by The Earl Mountbatten Hospice, Isle of Wight Written January 2015, revision due January 2018 This guideline is available as a paper pocketbook
GUIDELINES ON THE MANAGEMENT OF PAIN DUE TO CANCER IN ADULTS
 GUIDELINES ON THE MANAGEMENT OF PAIN DUE TO CANCER IN ADULTS Bristol Palliative Care Collaborative Contact Numbers: Hospital Specialist Palliative Care Teams: North Bristol 0117 4146392 UH Bristol 0117
GUIDELINES ON THE MANAGEMENT OF PAIN DUE TO CANCER IN ADULTS Bristol Palliative Care Collaborative Contact Numbers: Hospital Specialist Palliative Care Teams: North Bristol 0117 4146392 UH Bristol 0117
PENNINE LANCASHIRE GUIDELINES FOR THE MANAGEMENT OF SYMPTOMS IN THE LAST DAYS OF LIFE
 PENNINE LANCASHIRE GUIDELINES FOR THE MANAGEMENT OF SYMPTOMS IN THE LAST DAYS OF LIFE Originally produced: July 2006 First Review: August 2009 Second Review: November 2011 For review November 2013 Approved
PENNINE LANCASHIRE GUIDELINES FOR THE MANAGEMENT OF SYMPTOMS IN THE LAST DAYS OF LIFE Originally produced: July 2006 First Review: August 2009 Second Review: November 2011 For review November 2013 Approved
MND Just in Case kit Information for GPs
 MND Just in Case kit Information for GPs What is the MND Just in Case kit? 2 Motor neurone disease (MND) is a progressive and terminal disease that results in degeneration of the motor neurones in the
MND Just in Case kit Information for GPs What is the MND Just in Case kit? 2 Motor neurone disease (MND) is a progressive and terminal disease that results in degeneration of the motor neurones in the
Palliative care for patients with brain cancer
 Palliative care for patients with brain cancer Lyn Cave Clinical Nurse Specialist Palliative Care Hospital2Home (H2H) Dr Jayne Wood Clinical Lead Palliative Care The Royal Marsden and Royal Brompton Palliative
Palliative care for patients with brain cancer Lyn Cave Clinical Nurse Specialist Palliative Care Hospital2Home (H2H) Dr Jayne Wood Clinical Lead Palliative Care The Royal Marsden and Royal Brompton Palliative
Palliative Prescribing - Pain
 Palliative Prescribing - Pain LAURA BARNFIELD 21/2/17 Aims To understand the classes of painkillers available in palliative care To gain confidence in counselling regarding opiates To gain confidence prescribing
Palliative Prescribing - Pain LAURA BARNFIELD 21/2/17 Aims To understand the classes of painkillers available in palliative care To gain confidence in counselling regarding opiates To gain confidence prescribing
Palliative Care and the Critical Role of the Pharmacist. Arti Thakerar Education/ Palliative Care Peter MacCallum Cancer Centre
 Palliative Care and the Critical Role of the Pharmacist Arti Thakerar Education/ Palliative Care Peter MacCallum Cancer Centre Overview What is palliative care Role of a pharmacist in palliative care Issues
Palliative Care and the Critical Role of the Pharmacist Arti Thakerar Education/ Palliative Care Peter MacCallum Cancer Centre Overview What is palliative care Role of a pharmacist in palliative care Issues
Palliative Care Out-of-hours. A resource pack for West Dorset. Contents:
 Palliative Care Out-of-hours. A resource pack for West Dorset Contents: Section 1 Supply of drugs DCH Pharmacy hours and arrangements How to contact a community pharmacist out of hours Palliative care
Palliative Care Out-of-hours. A resource pack for West Dorset Contents: Section 1 Supply of drugs DCH Pharmacy hours and arrangements How to contact a community pharmacist out of hours Palliative care
End Stage Liver Disease Regional Audit Casenote Survey
 1. This questionnaire is an audit of clinical documentation of patients who have died of end stage liver disease. If you have any questions about how this form should be completed please contact Dr Grace
1. This questionnaire is an audit of clinical documentation of patients who have died of end stage liver disease. If you have any questions about how this form should be completed please contact Dr Grace
Implementing the recommendation on medication management and symptom control
 Implementing the recommendation on medication management and symptom control Mike Grocott Professor of Anaesthesia and Critical Care Medicine University of Southampton Consultant in Critical Care Medicine
Implementing the recommendation on medication management and symptom control Mike Grocott Professor of Anaesthesia and Critical Care Medicine University of Southampton Consultant in Critical Care Medicine
Anticipatory prescribing and end of life considerations. Dr Stephanie Lippett
 Anticipatory prescribing and end of life considerations Dr Stephanie Lippett contents Pain Restlessness/agitation Nausea/vomiting Secretions Syringe driver Anticipatory prescribing Important things to
Anticipatory prescribing and end of life considerations Dr Stephanie Lippett contents Pain Restlessness/agitation Nausea/vomiting Secretions Syringe driver Anticipatory prescribing Important things to
Symptom Control in the Community Setting. Dr Andrew Tysoe-Calnon
 Symptom Control in the Community Setting Dr Andrew Tysoe-Calnon Lead Consultant t Common symptoms Pain Agitation Shortness of breath Nausea and vomiting Intestinal obstruction Confusion Pain Occurs in
Symptom Control in the Community Setting Dr Andrew Tysoe-Calnon Lead Consultant t Common symptoms Pain Agitation Shortness of breath Nausea and vomiting Intestinal obstruction Confusion Pain Occurs in
Policy/Standard Operating Procedure/ Clinical Guideline. ELHT/CP22 Version 5.1. ELHT/CP22 Version 4.1
 TRUST WIDE/DIVISIONAL DOCUMENT Delete as appropriate Policy/Standard Operating Procedure/ Clinical Guideline DOCUMENT TITLE: Policy and Procedure for the T34 Ambulatory Syringe Pump in adults (Palliative
TRUST WIDE/DIVISIONAL DOCUMENT Delete as appropriate Policy/Standard Operating Procedure/ Clinical Guideline DOCUMENT TITLE: Policy and Procedure for the T34 Ambulatory Syringe Pump in adults (Palliative
CONTROLLED DOCUMENT. Guidelines for the use of subcutaneous hydration in palliative care (hypodermoclysis) Controlled Document Number: CG259
 Controlled Document Number: CG259") Guidelines for the use of subcutaneous hydration in palliative care (hypodermoclysis) CONTROLLED DOCUMENT CATEGORY: CLASSIFICATION: Controlled Document Number: Version Number: 1 Controlled Document Sponsor:
Guidelines for the use of subcutaneous hydration in palliative care (hypodermoclysis) CONTROLLED DOCUMENT CATEGORY: CLASSIFICATION: Controlled Document Number: Version Number: 1 Controlled Document Sponsor:
End of Life Care. Dr Anne Garry Consultant in Palliative Medicine
 End of Life Care Dr Anne Garry Consultant in Palliative Medicine Concerns voiced both by public and professionals.. Implementation and on-going training highly variable across country Decisions made by
End of Life Care Dr Anne Garry Consultant in Palliative Medicine Concerns voiced both by public and professionals.. Implementation and on-going training highly variable across country Decisions made by
1. GUIDELINES FOR THE MANAGEMENT OF AGITATION IN ADVANCED CANCER
 1. GUIDELINES FOR THE MANAGEMENT OF AGITATION IN ADVANCED CANCER 1.1 GENERAL PRINCIPLES There are many causes of agitation in palliative care patients, which makes recommendations for treatment difficult.
1. GUIDELINES FOR THE MANAGEMENT OF AGITATION IN ADVANCED CANCER 1.1 GENERAL PRINCIPLES There are many causes of agitation in palliative care patients, which makes recommendations for treatment difficult.
SCHEDULE 2 THE SERVICES
 SCHEDULE 2 THE SERVICES A. Service Specifications Mandatory headings 1 4: mandatory but detail for local determination and agreement Optional headings 5-7: optional to use, detail for local determination
SCHEDULE 2 THE SERVICES A. Service Specifications Mandatory headings 1 4: mandatory but detail for local determination and agreement Optional headings 5-7: optional to use, detail for local determination
Palliative Care. Pocketbook 4
 Nottinghamshire STP EOL Programme Board 2019 Review 2022 Palliative Care Pocketbook 4 Contents Pain Guidelines page 2 Nausea and Vomiting page 9 Inoperable Bowel Obstruction page 10 Constipation page 11
Nottinghamshire STP EOL Programme Board 2019 Review 2022 Palliative Care Pocketbook 4 Contents Pain Guidelines page 2 Nausea and Vomiting page 9 Inoperable Bowel Obstruction page 10 Constipation page 11
Palliative care in long-term conditions Scottish Palliative Care Pharmacists Association
 Palliative care in long-term conditions 2011 2012 Scottish Palliative Care Pharmacists Association Aims & Objectives To explore symptoms, general management principles and appropriate palliative treatment
Palliative care in long-term conditions 2011 2012 Scottish Palliative Care Pharmacists Association Aims & Objectives To explore symptoms, general management principles and appropriate palliative treatment
Berkshire Adult Palliative Care Guidelines - End of Life Care GL110
 Berkshire Adult Palliative Care Guidelines - End of Life Care GL110 Approval Approval Group Job Title, Chair of Committee Date Drugs & Therapeutic Committee Chair, Drugs & Therapeutic Committee October
Berkshire Adult Palliative Care Guidelines - End of Life Care GL110 Approval Approval Group Job Title, Chair of Committee Date Drugs & Therapeutic Committee Chair, Drugs & Therapeutic Committee October
What else is new (other symptoms) DR ANDREW DAVIES
 DR ANDREW DAVIES") What else is new (other symptoms) DR ANDREW DAVIES Outline Nausea & vomiting Petroleum jelly (and oxygen) Nausea & vomiting MASCC / ESMO recommendations MASCC / ESMO recommendations General: The anti-emetic
What else is new (other symptoms) DR ANDREW DAVIES Outline Nausea & vomiting Petroleum jelly (and oxygen) Nausea & vomiting MASCC / ESMO recommendations MASCC / ESMO recommendations General: The anti-emetic
Guidelines for Syringe Driver Management in Palliative Care in New Zealand
 Guidelines for Syringe Driver Management in Palliative Care in New Zealand i Citation: Ministry of Health. 2009. Guidelines for Syringe Driver Management in Palliative Care in New Zealand. Wellington:
Guidelines for Syringe Driver Management in Palliative Care in New Zealand i Citation: Ministry of Health. 2009. Guidelines for Syringe Driver Management in Palliative Care in New Zealand. Wellington:
BREATHLESSNESS MANAGEMENT
 Guideline Name: Breathlessness BACKGROUND Breathlessness is a common symptom in patients with cancer, end-stage heart failure and end-stage chronic obstructive pulmonary disease (COPD). There are many
Guideline Name: Breathlessness BACKGROUND Breathlessness is a common symptom in patients with cancer, end-stage heart failure and end-stage chronic obstructive pulmonary disease (COPD). There are many
Palliative Care Formulary
 Palliative Care Formulary 2016-2019 This formulary for pain and symptom management in adults is intended as a guide for prescribers in hospital and community. Special care should be taken when prescribing
Palliative Care Formulary 2016-2019 This formulary for pain and symptom management in adults is intended as a guide for prescribers in hospital and community. Special care should be taken when prescribing
Palliative Care. Anticipatory Prescribing Guidelines & June Gippsland Region Palliative Care Consortium Clinical Practice Group
 Palliative Care Anticipatory Prescribing Guidelines June 2016 Gippsland Region Palliative Care Consortium Clinical Practice Group Policy No. Title Keywords Ratified GRPCC-CPG008_1.1_2016 Anticipatory Prescribing
Palliative Care Anticipatory Prescribing Guidelines June 2016 Gippsland Region Palliative Care Consortium Clinical Practice Group Policy No. Title Keywords Ratified GRPCC-CPG008_1.1_2016 Anticipatory Prescribing
Treating the symptoms of kidney failure
 Treating the symptoms of kidney failure Information for patients, relatives and carers Renal Department The York Hospital and Scarborough Hospital Tel: 01904 725370 For more information, please contact:
Treating the symptoms of kidney failure Information for patients, relatives and carers Renal Department The York Hospital and Scarborough Hospital Tel: 01904 725370 For more information, please contact:
Planning for the future; A guide to symptom control at end of life in advanced dementia
 Planning for the future; A guide to symptom control at end of life in advanced dementia Item Type Guideline Authors Irish Hospice Foundation;St Vincent's Hospital, Athy;St Brigid's Hospice Publisher Irish
Planning for the future; A guide to symptom control at end of life in advanced dementia Item Type Guideline Authors Irish Hospice Foundation;St Vincent's Hospital, Athy;St Brigid's Hospice Publisher Irish
Target audience: The target audience for this guidance are: GPs Care home managers and nurses, District nurses, and Specialist Palliative Care teams.
 Anticipatory medication guidance for the last days of life for frail older people being care for in care homes who do not have Specialist Palliative Care needs Purpose of guidance: The purpose of this
Anticipatory medication guidance for the last days of life for frail older people being care for in care homes who do not have Specialist Palliative Care needs Purpose of guidance: The purpose of this
Nausea and Vomiting in Palliative Care
 Nausea and Vomiting in Palliative Care Definitions Nausea - an unpleasant feeling of the need to vomit Vomiting - the expulsion of gastric contents through the mouth, caused by forceful and sustained contraction
Nausea and Vomiting in Palliative Care Definitions Nausea - an unpleasant feeling of the need to vomit Vomiting - the expulsion of gastric contents through the mouth, caused by forceful and sustained contraction
This survey aims to look at individual practice and can be completed by any healthcare professional.
 This survey aims to look at individual practice and can be completed by any healthcare professional. If you have any questions about how this form should be completed please contact Dr Grace Ting (ghlting@doctors.net.uk)
This survey aims to look at individual practice and can be completed by any healthcare professional. If you have any questions about how this form should be completed please contact Dr Grace Ting (ghlting@doctors.net.uk)
Specialist Palliative Care Audit and Guidelines Group (SPAGG)
") Specialist Palliative Care Audit and Guidelines Group (SPAGG) Clinical Guideline for the Prescribing and Administration of Furosemide via continuous subcutaneous infusion (CSCI) for Heart Failure Patients
Specialist Palliative Care Audit and Guidelines Group (SPAGG) Clinical Guideline for the Prescribing and Administration of Furosemide via continuous subcutaneous infusion (CSCI) for Heart Failure Patients
GG&C Chronic Non Malignant Pain Opioid Prescribing Guideline
 GG&C Chronic Non Malignant Pain Opioid Prescribing Guideline Background Persistent pain is common, affecting around five million people in the UK. For many sufferers, pain can be frustrating and disabling,
GG&C Chronic Non Malignant Pain Opioid Prescribing Guideline Background Persistent pain is common, affecting around five million people in the UK. For many sufferers, pain can be frustrating and disabling,
Analgesia. This is widely used in palliative care. It has antipyretic and analgesic effects but no anti-
 Page 1 of 8 Analgesia The World Health Organisation (WHO, 1990) has devised a model to assist health care professionals in the management of cancer pain. The recommendations include managing pain, by the
Page 1 of 8 Analgesia The World Health Organisation (WHO, 1990) has devised a model to assist health care professionals in the management of cancer pain. The recommendations include managing pain, by the
ADULT SYRINGE DRIVER PROTOCOL (T34)
") ADULT SYRINGE DRIVER PROTOCOL (T34) Version Date Purpose of Issue/Description of Change Review Date 3 May 2016 Guidelines for T34 syringe driver May 2018 Status Publication Scheme FOI Classification Function/Activity
ADULT SYRINGE DRIVER PROTOCOL (T34) Version Date Purpose of Issue/Description of Change Review Date 3 May 2016 Guidelines for T34 syringe driver May 2018 Status Publication Scheme FOI Classification Function/Activity
Palliative Patient in Emergency Department
 Palliative Patient in Emergency Department Dr Thiru Thirukkumaran Palliative Care Services NW THO Northwest Regional Hospital, Burnie Northwest Tasmania Outline the Session Introduction What is palliative
Palliative Patient in Emergency Department Dr Thiru Thirukkumaran Palliative Care Services NW THO Northwest Regional Hospital, Burnie Northwest Tasmania Outline the Session Introduction What is palliative
Managing Respiratory Symptoms - Breathlessness, Cough and Secretions. Dr Laura Healy. Palliative Medicine Registrar, Beaumont Hospital.
 Managing Respiratory Symptoms - Breathlessness, Cough and Secretions. Dr Laura Healy. Palliative Medicine Registrar, Beaumont Hospital. Things to consider: 1. Very common symptoms. 2. Can occur in any
Managing Respiratory Symptoms - Breathlessness, Cough and Secretions. Dr Laura Healy. Palliative Medicine Registrar, Beaumont Hospital. Things to consider: 1. Very common symptoms. 2. Can occur in any
Controlled Document Number: Version Number: 1. Controlled Document Sponsor: Controlled Document Lead (Author): On: July Review Date: July 2020
: On: July Review Date: July 2020") Guidelines for the Use of Naloxone in Palliative Care in Adult Patients CONTROLLED DOCUMENT CATEGORY: CLASSIFICATION: Controlled Document Number: Version Number: 1 Controlled Document Sponsor: Controlled
Guidelines for the Use of Naloxone in Palliative Care in Adult Patients CONTROLLED DOCUMENT CATEGORY: CLASSIFICATION: Controlled Document Number: Version Number: 1 Controlled Document Sponsor: Controlled
The last days of life in hospital and at home
 The last days of life in hospital and at home Beaumont Multi-disciplinary Palliative Care Study Day 28/9/2017 Dr Sarah McLean Consultant in Palliative Medicine St Francis Hospice Beaumont Hospital Overview
The last days of life in hospital and at home Beaumont Multi-disciplinary Palliative Care Study Day 28/9/2017 Dr Sarah McLean Consultant in Palliative Medicine St Francis Hospice Beaumont Hospital Overview
Understanding pain in 5 minutes
 Pain Management- PallCare Definition of Pain Pain is what the patient says hurts. Dr Simon Allan Director of Palliative Care Arohanui Hospice An unpleasant sensory and emotional experience associated with
Pain Management- PallCare Definition of Pain Pain is what the patient says hurts. Dr Simon Allan Director of Palliative Care Arohanui Hospice An unpleasant sensory and emotional experience associated with
Cardiac Catheter Labs Intravenous Drug Therapy Guide
 Title of Guideline (must include the word Guideline (not protocol, policy, procedure etc) Contact Name and Job Title (author) Cardiac Catheter Lab IV Medicines Guideline Helen Buxton ( Senior Cath Lab
Title of Guideline (must include the word Guideline (not protocol, policy, procedure etc) Contact Name and Job Title (author) Cardiac Catheter Lab IV Medicines Guideline Helen Buxton ( Senior Cath Lab
In our patients the cause of seizures can be broadly divided into structural and systemic causes.
 Guidelines for the management of Seizures Amalgamation and update of previous policies 7 (Seizure guidelines, ND, 2015) and 9 (Status epilepticus, KJ, 2011) Seizures can occur in up to 15% of the Palliative
Guidelines for the management of Seizures Amalgamation and update of previous policies 7 (Seizure guidelines, ND, 2015) and 9 (Status epilepticus, KJ, 2011) Seizures can occur in up to 15% of the Palliative
Lothian Palliative Care Guidelines POCKET EDITION 2004
 Lothian Palliative Care Guidelines POCKET EDITION 2004 These guidelines have been developed by a multidisciplinary group of specialist and non-specialist health professionals from hospital, community and
Lothian Palliative Care Guidelines POCKET EDITION 2004 These guidelines have been developed by a multidisciplinary group of specialist and non-specialist health professionals from hospital, community and
Pain relief after major surgery
 Page 1 of 6 Pain relief after major surgery Introduction The aim of this leaflet is to tell you about the main pain relief options available after major surgery. You will probably only need this for the
Page 1 of 6 Pain relief after major surgery Introduction The aim of this leaflet is to tell you about the main pain relief options available after major surgery. You will probably only need this for the
Eastern Health and Social Services Board Palliative Care
 Eastern Health and Social Services Board Palliative Care Out of Hours Symptom advice leaflets Adult Palliative care patients (Compiled by Macmillan GP Facilitators March 2008) 1 CONTENTS PAIN Control of
Eastern Health and Social Services Board Palliative Care Out of Hours Symptom advice leaflets Adult Palliative care patients (Compiled by Macmillan GP Facilitators March 2008) 1 CONTENTS PAIN Control of
Symptom Management in the last weeks & days of life. Facilitator: Vernon Davis RN/Community Team Leader Rowcroft Community Team
 Symptom Management in the last weeks & days of life Facilitator: Vernon Davis RN/Community Team Leader Rowcroft Community Team Session objectives To identify common symptoms at the end of life To increase
Symptom Management in the last weeks & days of life Facilitator: Vernon Davis RN/Community Team Leader Rowcroft Community Team Session objectives To identify common symptoms at the end of life To increase
Facts About Morphine and Other Opioid Medicines In Palliative Care. Find out more at: palliativecare.my. Prepared by: Printing sponsored by:
 Facts About Morphine and Other Opioid Medicines In Palliative Care Find out more at: palliativecare.my Prepared by: Printing sponsored by: What is this brochure about? Opioid medicines are pain relievers.
Facts About Morphine and Other Opioid Medicines In Palliative Care Find out more at: palliativecare.my Prepared by: Printing sponsored by: What is this brochure about? Opioid medicines are pain relievers.
Mid Essex Locality Guideline for Management of Adult Acute and Chronic Non-Cancer Pain in Primary care
 Guideline for Management of Adult Acute and Chronic Non-Cancer Pain in Primary care If possible patients should be assessed using a simple visual analogue scale VAS to determine the most appropriate stage
Guideline for Management of Adult Acute and Chronic Non-Cancer Pain in Primary care If possible patients should be assessed using a simple visual analogue scale VAS to determine the most appropriate stage
Nausea and Vomiting. Principles and Practice in End of Life Care November 2018
 Nausea and Vomiting Principles and Practice in End of Life Care November 2018 Overview Aims and Objectives Why is managing nausea and vomiting important? Definitions Causes Interventions pharmacological
Nausea and Vomiting Principles and Practice in End of Life Care November 2018 Overview Aims and Objectives Why is managing nausea and vomiting important? Definitions Causes Interventions pharmacological
BJF Acute Pain Team Formulary Group
 Title Analgesia Guidelines for Acute Pain Management (Adults) in BGH Document Type Issue no Clinical guideline Clinical Governance Support Team Use Issue date April 2013 Review date April 2015 Distribution
Title Analgesia Guidelines for Acute Pain Management (Adults) in BGH Document Type Issue no Clinical guideline Clinical Governance Support Team Use Issue date April 2013 Review date April 2015 Distribution
Pain management in palliative care. Dr. Stepanie Lippett and Sister Karen Davies-Linihan
 Pain management in palliative care Dr. Stepanie Lippett and Sister Karen Davies-Linihan contents Concept of total pain Steps in pain management Recognising neuropathic pain WHO analgesic ladder Common
Pain management in palliative care Dr. Stepanie Lippett and Sister Karen Davies-Linihan contents Concept of total pain Steps in pain management Recognising neuropathic pain WHO analgesic ladder Common
Regional Renal Training
 Regional Renal Training Palliative and End of Life Care Dr Clare Kendall North Bristol NHS Trust Advanced Kidney Disease Dialysis/Transplant Conservative Management Deteriorating despite dialysis/failing
Regional Renal Training Palliative and End of Life Care Dr Clare Kendall North Bristol NHS Trust Advanced Kidney Disease Dialysis/Transplant Conservative Management Deteriorating despite dialysis/failing
Guidance for the Use of Subcutaneous Furosemide by Continuous Infusion for Heart Failure in Community Settings
 Guidance for the Use of Subcutaneous Furosemide by Continuous Infusion for Heart Failure in Community Settings NHS Highland Authorised by: Planning For Fairness: Yes/No (Formerly EQIA) Distribution Consultant
Guidance for the Use of Subcutaneous Furosemide by Continuous Infusion for Heart Failure in Community Settings NHS Highland Authorised by: Planning For Fairness: Yes/No (Formerly EQIA) Distribution Consultant
SPAGG. Coversheet for Specialist Palliative Audit and Guideline Group Agreed Documentation
 SPAGG Coversheet for Specialist Palliative Audit and Guideline Group Agreed Documentation This sheet is to accompany all documentation agreed by SPAGG. This will assist maintenance of the guidelines as
SPAGG Coversheet for Specialist Palliative Audit and Guideline Group Agreed Documentation This sheet is to accompany all documentation agreed by SPAGG. This will assist maintenance of the guidelines as
Nausea & Vomiting. Dr Eve Lyn TAN Liverpool Hospital NSW, AUSTRALIA
 Nausea & Vomiting Dr Eve Lyn TAN Liverpool Hospital NSW, AUSTRALIA Prevalence prevalence varies *, systemic review 2007 : overall prevalence : nausea 30%, vomiting 20% in last 1-2 weeks of life : nausea
Nausea & Vomiting Dr Eve Lyn TAN Liverpool Hospital NSW, AUSTRALIA Prevalence prevalence varies *, systemic review 2007 : overall prevalence : nausea 30%, vomiting 20% in last 1-2 weeks of life : nausea
Agitation. Susan Emmens Palliative Care Clinical Nurse Specialist
 Agitation Susan Emmens Palliative Care Clinical Nurse Specialist Definitions Restlessness finding or affording no rest, uneasy, agitated. Constantly in motion fidgeting Agitation shaking, moving, mental
Agitation Susan Emmens Palliative Care Clinical Nurse Specialist Definitions Restlessness finding or affording no rest, uneasy, agitated. Constantly in motion fidgeting Agitation shaking, moving, mental
GI Pharmacology -4 Irritable Bowel Syndrome and Antiemetics. Dr. Alia Shatanawi
 GI Pharmacology -4 Irritable Bowel Syndrome and Antiemetics Dr. Alia Shatanawi 11-04-2018 Drugs used in Irritable Bowel Syndrome Idiopathic, chronic, relapsing disorder characterized by abdominal discomfort
GI Pharmacology -4 Irritable Bowel Syndrome and Antiemetics Dr. Alia Shatanawi 11-04-2018 Drugs used in Irritable Bowel Syndrome Idiopathic, chronic, relapsing disorder characterized by abdominal discomfort
Coversheet for Network Site Specific Group Agreed Documentation
 Coversheet for Network Site Specific Group Agreed Documentation This sheet is to accompany all documentation agreed by Pan Birmingham Cancer Network Site Specific Groups. This will assist the Network Governance
Coversheet for Network Site Specific Group Agreed Documentation This sheet is to accompany all documentation agreed by Pan Birmingham Cancer Network Site Specific Groups. This will assist the Network Governance
GUIDELINES AND AUDIT IMPLEMENTATION NETWORK
 GUIDELINES AND AUDIT IMPLEMENTATION NETWORK General Palliative Care Guidelines The Management of Pain at the End Of Life November 2010 Aim To provide a user friendly, evidence based guide for the management
GUIDELINES AND AUDIT IMPLEMENTATION NETWORK General Palliative Care Guidelines The Management of Pain at the End Of Life November 2010 Aim To provide a user friendly, evidence based guide for the management
Waterloo Wellington (WW) Symptom Management Guideline for the End of Life (EOL) Medication Order Set for Long Term Care (LTC)
 Symptom Management Guideline for the End of Life (EOL) Medication Order Set for Long Term Care (LTC)") Waterloo Wellington (WW) Symptom Management Guideline for the End of Life (EOL) Medication Order Set for Long Term Care (LTC) May 2018 THE WATERLOO WELLINGTON SYMPTOM MANAGEMENT GUIDELINE FOR THE END OF
Waterloo Wellington (WW) Symptom Management Guideline for the End of Life (EOL) Medication Order Set for Long Term Care (LTC) May 2018 THE WATERLOO WELLINGTON SYMPTOM MANAGEMENT GUIDELINE FOR THE END OF