Evidence based approach to incidentally detected subsolid pulmonary nodule. DM SEMINAR July 27, 2018 Harshith Rao
|
|
|
- Geraldine Baker
- 5 years ago
- Views:
Transcription
1 Evidence based approach to incidentally detected subsolid pulmonary nodule DM SEMINAR July 27, 2018 Harshith Rao
2 Outline Definitions Etiologies Risk evaluation Clinical features Radiology Approach Modifications: new guidelines Management
3 Incidentally detected parenchymal lesion NODULE <30mm in size Well defined Round, single Completely surrounded by normal lung parenchyma MASS >30mm in size Solitary Pulmonary Nodule Tan BB, et al. The solitary pulmonary nodule. Chest. 2003;123(1):89S-96S.

4
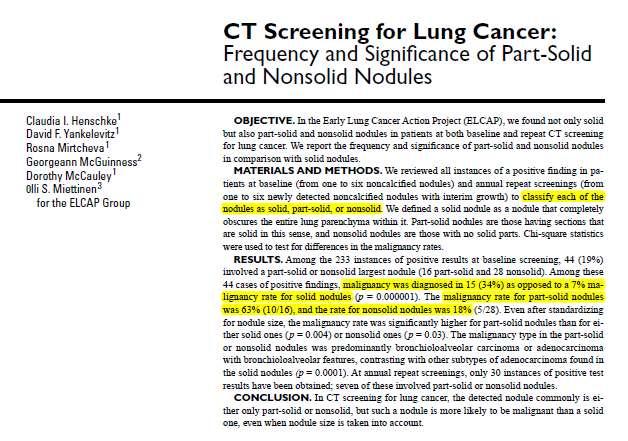
5 Pulmonary nodule-definition,types Solid Sub solid Partly solid Ground glass Solid nodule: completely obscures the entire lung parenchyma within it Partly solid nodule: patches of parenchyma that are completely obscured Ground glass nodule: NO patch of parenchyma that are completely obscured Henschke CI et al. CT screening for lung cancer: frequency and significance of part-solid and nonsolid nodules. AJR American journal of roentgenology. 2002;178(5):1053-7


6 PSN GGN Henschke CI et al. CT screening for lung cancer: frequency and significance of part-solid and nonsolid nodules. AJR American journal of roentgenology. 2002;178(5):1053-7
7
8 Prospective study to follow up incidentally detected nodules Low dose CT used 2 cohorts (Pan Can & BCCA) Total of 2961 patients, nodules were followed up 144 (1%) were malignant McWilliams A et al. Probability of cancer in pulmonary nodules detected on first screening CT. New England Journal of Medicine. 2013;369(10):910-9
9 Common Etiologies Benign Infectious granuloma (80%) Tuberculosis Benign tumours Hamartomas (10%) Vascular Pulmonary AVMs Others GPA, sarcoidosis, rh.arthritis Malignant Primary lung cancer Adenocarcinomas (50%) Squamous cell CA (25%) Metastatic Carcinoma Melanoma, sarcoma Colon, breast, kidney Carcinoid
10 Subsolid nodule Most common etiologies include Minimally invasive adenocarcinoma Adenocarcinoma insitu Atypical adenomatous hyperplasia Kim HY, et al. Persistent pulmonary nodular ground-glass opacity at thin-section CT: histopathologic comparisons. Radiology. 2007;245(1):267-75
11 APPROACH AND EVALUATION Clinical features Radiology Risk assesment
12 Clinical risk factors
13 Age Probability of lung cancer rises as age increases Rare below 35yrs Trunk G, et al. The management and evaluation of the solitary pulmonary nodule. Chest. 1974;66(3):236-9
14 Female gender risk factor in the PanCan trial, Odds ratio of 1.8 McWilliams A et al. Probability of cancer in pulmonary nodules detected on first screening CT. New England Journal of Medicine. 2013;369(10):910-9
15 Family history risk factor for both smokers and those who never smoked overall relative risk of 1.5 affected sibling: 1.8 Trunk G, et al. The management and evaluation of the solitary pulmonary nodule. Chest. 1974;66(3):236-9
16 Smoking and adeno CA Subsolid nodule (adeno CA) association with smoking is weak, not clearly established incidence of adenocarcinoma in non-smokers is increasing, with young female non-smokers being affected significantly more often than male non-smokers MacMahon H, et al. Guidelines for Management of Incidental Pulmonary Nodules Detected on CT Images: From the Fleischner Society 2017.Radiology. 2017;284(1):228-43
17 Smoking and adeno CA Recent recommendations (2017) do not differentiate smokers and nonsmokers No sufficient evidence to use a different management guidelines for smokers till date MacMahon H, et al. Guidelines for Management of Incidental Pulmonary Nodules Detected on CT Images: From the Fleischner Society 2017.Radiology. 2017;284(1):228-43
18 Risk factors in Radiology
19 Computed tomography Preferred for evaluation of a nodule for likelihood of malignancy Low dose radiation technique(1msv) Thin collimation(1mm) Non contrast scans
20 CT follow up 10% patients develop new nodule that requires independent assessment Swensen SJ, et al. CT screening for lung cancer: five-year prospective experience. Radiology. 2005;235(1):259-65
21 Nodule size size is an independent predictor for malignancy Dominant factor in management guidelines <5 mm 5 to 9 mm 8 to 20 mm >20 mm <1 percent 2 to 6 percent 18 percent >50 percent McWilliams A et al. Probability of cancer in pulmonary nodules detected on first screening CT. New England Journal of Medicine. 2013;369(10):910-9
22 Attenuation Solid nodule: more common Subsolid nodule: higher likelihood of malignancy Henschke CI et al. CT screening for lung cancer: frequency and significance of part-solid and nonsolid nodules. AJR American journal of roentgenology. 2002;178(5):1053-7
23
24 Location Upper lobe nodules Risk factor for malignancy odds ratio of 2 Lindell RM,et al. Five-year lung cancer screening experience: CT appearance, growth rate, location, and histologic features of 61 lung cancers. Radiology. 2007;242(2): McWilliams A, et al. Probability of cancer in pulmonary nodules detected on first screening CT. New England Journal of Medicine. 2013;369(10):910-9
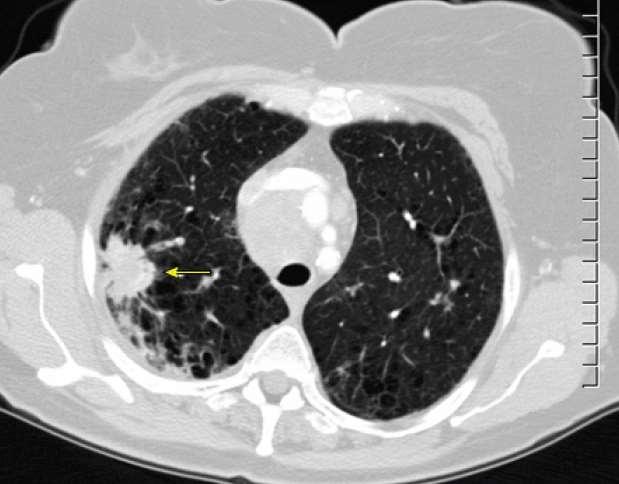
25 Border Well defined smooth border : benign Malignant Spiculated: growth of tumor cells along interstitium Lobulated: differential growth rates within nodules
26
27 Spiculated border risk factor for malignancy odds ratio in the range of McWilliams A et al. Probability of cancer in pulmonary nodules detected on first screening CT. New England Journal of Medicine. 2013;369(10):910-9
28
29 Number multiple nodules decreased the risk of malignancy McWilliams A et al. Probability of cancer in pulmonary nodules detected on first screening CT. New England Journal of Medicine. 2013;369(10):910-9
30 Number increased risk of malignancy as the total nodule count increased from 1 to 4 but decreased risk in patients with 5 or more nodules Peters R, et al. Prevalence of pulmonary multi-nodularity in CT lung cancer screening and lung cancer probability [abstr]. In: Radiological Society of North America Scientific Assembly and Annual Meeting Program. Oak Brook, Ill: Radiological Society of North America, 2015; 111.
31 Growth Defined as Increase in size Increase in attenuation Increase in solid component Indication for biopsy/ resection during followup In solid lesions, increase in size more than 2 mm Bankier AA, et al. Recommendations for measuring pulmonary nodules at CT: a statement from the Fleischner Society. Radiology. 2017;285(2):
32 Stable subsolid nodule Same size for 5 years Considered to be benign 2 years for solid nodule Longer volume doubling time than solid lesions Usually 3-5 years Longer follow-up is necessary Hasegawa M, et al. Growth rate of small lung cancers detected on mass CT screening. The British journal of radiology. 2000;73(876):1252-9
33
34 Calcification / fat Presence of calcification or fat in the nodule suggests a benign etiology Sampling avoided Exceptions Carcinoid Mets from chondro/osteosarcomas

35
36 Emphysema presence of emphysema on a CT is an independent risk factor for lung cancer NLST trial shows incidence of 25 cancer per 1000 screened patients with emphysema, compared with 7.5 in those without emphysema de Torres JP, et al. Assessing the relationship between lung cancer risk and emphysema detected on low-dose CT of the chest. Chest. 2007;132(6):1932-8
37 Fibrosis Pulmonary fibrosis (particularly IPF) is also an independent risk factor hazard ratio of 4.2 compared with emphysema alone Kwak N, et al. Lung cancer risk among patients with combined pulmonary fibrosis and emphysema. Respiratory medicine. 2014;108(3):524-30
38 Role of CXR? insensitive for detection of small nodules most nodules less than 1 cm will not be seen Minimal increase in size of nodules not picked up Even though the radiation used in CT is higher than CXR, CT is the imaging modality of choice in evaluation and follow-up of pulmonary nodule CXR not to be used as it is insensitive Bankier AA, et al. Recommendations for measuring pulmonary nodules at CT: a statement from the Fleischner Society. Radiology. 2017;285(2):
39 Chest tomosynthesis Lower radiation dose (10-fold lower- 0.15mSv) not widely available more sensitive than CXR but less sensitive than CT half of nodules measuring 6 mm on CT are detected Not recommended as primary modality of imaging in pulmonary nodule Meltzer C, et al. Detection and characterization of solid pulmonary nodules at digital chest tomosynthesis: data from a cohort of the pilot Swedish Cardiopulmonary Bioimage Study. Radiology. 2018;287(3):
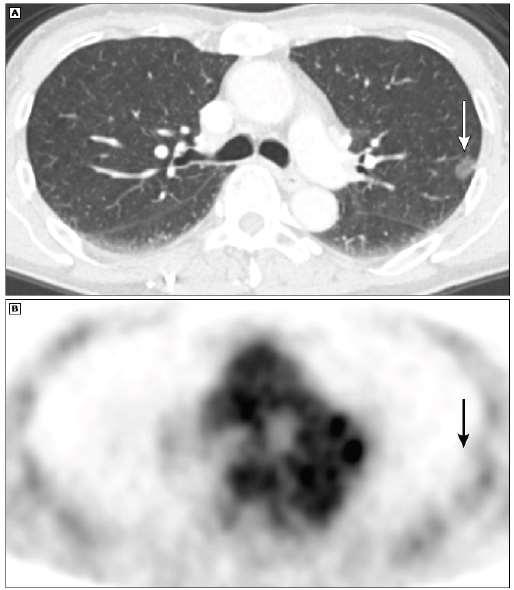
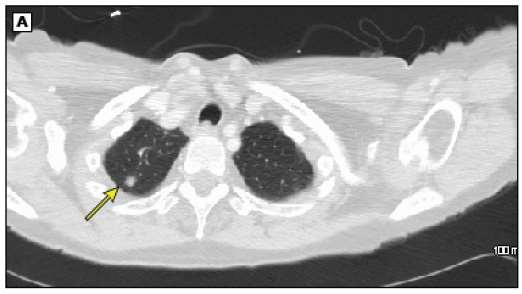
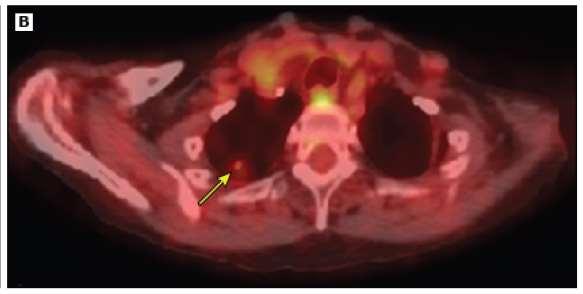
40 FDG PET/CT Poor characterization of subsolid nodules Sensitivity: 10% Specificity: 20% for detecting malignancy in a ground-glass nodule Nomori H, et al. Evaluation of F-18 fluorodeoxyglucose (FDG) PET scanning for pulmonary nodules less than 3 cm in diameter, with special reference to the CT images. Lung cancer. 2004;45(1):19-27
41
42 PET in solid nodule? Recommended for evaluation in solid nodules Helps in differentiating malignant nodules which are >8mm in size (SUVmax 2.5) Sensitivity 89%, specificity 75% Solid nodules measuring >8 mm that are not FDG-avid are likely to be benign used to evaluate for metastases and to select the safest target for biopsy Deppen SA, et al. Accuracy of FDG-PET to diagnose lung cancer in areas with infectious lung disease: a meta-analysis. Jama. 2014;312(12):
43
44 Risk evaluation Clinical and radiological features Predictive models and calculators
45 Brock University cancer prediction equation estimates the probability of a lung nodule to be diagnosed as cancer within a two- to fouryear follow-up period McWilliams A, et al. Probability of cancer in pulmonary nodules detected on first screening CT. N Engl J Med Sep 5;369(10):910
46 Probability Low Intermediate High <5 percent 5 to 65 percent >65 percent McWilliams A, et al. Probability of cancer in pulmonary nodules detected on first screening CT. N Engl J Med Sep 5;369(10):910
47 Why to evaluate risk? Lesion>3cm : high risk resection Lesion<6mm: low risk followed up with CT Role in deciding the management of those lesions which fall in between(indeterminate nodule) Assessing the pretest probability of the lesion being malignant
48 Why to evaluate risk? Achieve a balance between Life saving benefits of detecting resectable lung cancer Avoiding morbidity associated with procedure/intervention
49 Its role in subsolid nodules Used in individualizing the approach to a Whereas particular in a patient solid nodule (clinical judgement) Guidelines Not used in recommend the flow chart its use recommended in flow chart by the guidelines Used to categorize the solid nodule >8mm into low, intermediate and high risk and followed up, FDGPET/CT, biopsy are done respectively MacMahon H, et al. Guidelines for Management of Incidental Pulmonary Nodules Detected on CT Images: From the Fleischner Society Radiology. 2017;284(1):228-43

50 MacMahon H, et al. Guidelines for Management of Incidental Pulmonary Nodules Detected on CT Images: From the Fleischner Society Radiology. 2017;284(1):228-43
51 Used only for Incidentally detected nodules Age >35yrs No symptoms/signs attributable to lesion Baseline risk of lung CA equivalent to general population MacMahon H, et al. Guidelines for Management of Incidental Pulmonary Nodules Detected on CT Images: From the Fleischner Society Radiology. 2017;284(1):228-43
52 Exclusion Immunocompromised pts k/c/o malignancy Symptomatic due to lesion In whom screening for lung cancer is done MacMahon H, et al. Guidelines for Management of Incidental Pulmonary Nodules Detected on CT Images: From the Fleischner Society Radiology. 2017;284(1):228-43
53 Preliminary requirement
54 Principles of follow-up Stable nodule on follow up does not need any intervention Resolution of nodule doesnot need followup CT Any growth in the size of nodule on follow up CT warrants histological diagnosis
55 For pure ground-glass nodules smaller than 6 mm in diameter, no routine follow-up is recommended (grade 1B; strong recommendation, moderate-quality evidence). For pure ground-glass nodules 6 mm or larger, follow-up scanning is recommended at 6 12 months and then every 2 years thereafter until 5 years (grade 1B; strong recommendation, moderate-quality evidence).
56 For solitary partsolid nodules smaller than 6 mm, no routine follow-up is recommended (grade 1C; strong recommendation, low- or very-low-quality evidence) For solitary part-solid nodules 6 mm or larger with a solid component less than 6 mm in diameter, followup is recommended at 3 6 months and then annually for a minimum of 5 years For solitary part-solid nodules with a solid component 8 mm or larger, a short-term follow-up CT scan at 3 6 months should be considered. In high risk nodules with FDG avid, biopsy or resection are recommended (grade 1B; strong recommendation, moderate quality evidence).
57
58
59
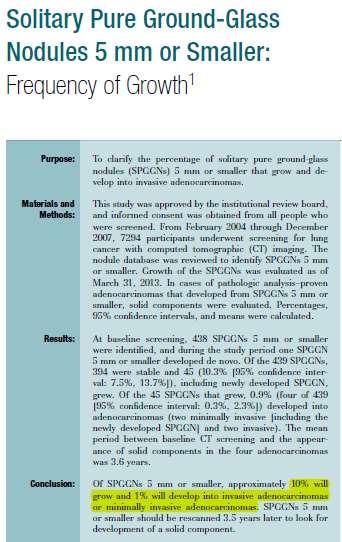
60 New modifications in 2017 guidelines? For pure ground-glass nodules smaller than 6 mm in diameter, no routine follow-up is recommended In case of nodule being suspicious for malignancy or with risk factors, then an option of 2 and 4 year follow up can be made Kakinuma R, et al. Solitary pure ground-glass nodules 5 mm or smaller: frequency of growth. Radiology 2015;276(3):
61
62 For pure ground-glass nodules 6 mm or larger, follow-up scanning is recommended at 6 12 months The previous recommendation of initial follow-up at 3 months has been changed to follow-up at 6 12 months because earlier follow-up is unlikely to affect the outcome of these characteristically indolent lesions. Naidich DP, et al. Recommendations for the management of subsolid pulmonary nodules detected at CT: a statement from the Fleischner Society. Radiology. 2013;266(1):304-17
63 New modifications in 2017 guidelines? Recommended follow-up intervals are now given as a range rather than as a precise time period to give radiologists, clinicians, and patients greater discretion to accommodate individual risk factors and preferences MacMahon H, et al. Guidelines for Management of Incidental Pulmonary Nodules Detected on CT Images: From the Fleischner Society Radiology. 2017;284(1):228-43
64 Multiple nodules MacMahon H, et al. Guidelines for Management of Incidental Pulmonary Nodules Detected on CT Images: From the Fleischner Society Radiology. 2017;284(1):228-43
65 Most of the incidentally detected multiple nodules are benign, resolution usually occurs within 3-6months, follow-up CT will help to avoid unnecessary sampling and assessment of resolution of subclinical pathology
66 Lung cancer screening? Every nodule must be evaluated Cutoff of 20mm used instead of 6mm <20mm CT f/u q 1year >20mm CT f/u q 6 month Naidich DP, et al. Recommendations for the management of subsolid pulmonary nodules detected at CT: a statement from the Fleischner Society. Radiology. 2013;266(1):304-17
67 Management
68 Excisional surgical biopsy Gold standard Diagnostic and therapeutic strategy 2 types Open VATS guided Diagnostic wedge resection by VATS(preferred, safe procedure)
69 Intraoperative frozen section analysis If positive, converted into VATS lobectomy with mediastinal lymph node sampling 50% required thoracotomy for complete resection and staging Allen M, et al. Video-assisted thoracoscopic stapled wedge excision for indeterminate pulmonary nodules. The Journal of thoracic and cardiovascular surgery. 1993;106(6):
70 Non surgical biopsy Preferred in Intermediate risk High risk non surgical candidates Sampling of nodule airway Bronchoscopic biopsy Large central chest wall Transthoracic needle biopsy Small peripheral
71 Transthoracic needle biopsy Under CT guidance Sensitivity >90% Specificity >99% Yield >90% nodules 1cm However, the rates of nondiagnostic biopsy do increase for nodules measuring 6 mm Lee SM, et al. C-arm cone-beam CT-guided percutaneous transthoracic needle biopsy of lung nodules: clinical experience in 1108 patients. Radiology. 2013;271(1):
72 Complications Pneumothorax (10-17%) Hemoptysis (1-7%) Lee SM, et al. C-arm cone-beam CT-guided percutaneous transthoracic needle biopsy of lung nodules: clinical experience in 1108 patients. Radiology. 2013;271(1):
73 Conventional TBLB Sensitivity 65 to 88 percent highest sensitivity for large, central lesions lower rates for peripheral nodules >2 cm: 63 percent <2 cm: 34 percent Rivera MP, et al. Establishing the diagnosis of lung cancer: Diagnosis and management of lung cancer: American College of Chest Physicians evidence-based clinical practice guidelines. Chest. 2013;143(5):e142S-e65S
74 Radial EBUS TBLB Sensitivity of 73-85% (larger central lesions) 70% if nodule <20mm 56% for peripheral nodules
75 EBUS TBB vs TBB Sensitivity 79% vs 55% Lesion >3cm : no significant difference <3cm: considerable fall in sensitivity of TBB(31%) EBUS TBB had similar sensitivity Paone G, et al. Endobronchial ultrasound-driven biopsy in the diagnosis of peripheral lung lesions. Chest. 2005;128(5):3551-7
76 Navigational bronchoscopy Using the CT guidance and electromagnetic radiation in navigation of bronchoscope to target small peripheral nodules Planning phase Preprocedure CT done 3D reconstruction of airways Target located Plan the approach
77 Navigation phase Software hybridises the CT images and realtime bronchoscope images Navigation of scanner probe and working channel to target Locking at target and sampling of nodule
78 Diagnostic yield: 70% Significantly higher than traditional bronchoscopy Increased as lesion size increased Wang Memoli JS, et al. Meta-analysis of guided bronchoscopy for the evaluation of the pulmonary nodule. Chest Aug;142(2):385-93
79 Take home message Subsolid: more malignant, low growth rate Risk factor assessment CXR, PET has not role in f/u Individualizing the approach Radial EBUS and navigation Bronchoscopy: better options
80 THANK YOU
GUIDELINES FOR PULMONARY NODULE MANAGEMENT : RECENT CHANGES AND UPDATES
 Venice 2017 GUIDELINES FOR PULMONARY NODULE MANAGEMENT : RECENT CHANGES AND UPDATES Heber MacMahon MB, BCh Department of Radiology The University of Chicago Disclosures Consultant for Riverain Medical
Venice 2017 GUIDELINES FOR PULMONARY NODULE MANAGEMENT : RECENT CHANGES AND UPDATES Heber MacMahon MB, BCh Department of Radiology The University of Chicago Disclosures Consultant for Riverain Medical
PULMONARY NODULES AND MASSES : DIAGNOSTIC APPROACH AND NEW MANAGEMENT GUIDELINES. https://tinyurl.com/hmpn2018
 PULMONARY NODULES AND MASSES : DIAGNOSTIC APPROACH AND NEW MANAGEMENT GUIDELINES Heber MacMahon MB, BCh Department of Radiology The University of Chicago https://tinyurl.com/hmpn2018 Disclosures Consultant
PULMONARY NODULES AND MASSES : DIAGNOSTIC APPROACH AND NEW MANAGEMENT GUIDELINES Heber MacMahon MB, BCh Department of Radiology The University of Chicago https://tinyurl.com/hmpn2018 Disclosures Consultant
OBJECTIVES. Solitary Solid Spiculated Nodule. What would you do next? Case Based Discussion: State of the Art Management of Lung Nodules.
 Organ Imaging : September 25 2015 OBJECTIVES Case Based Discussion: State of the Art Management of Lung Nodules Dr. Elsie T. Nguyen Dr. Kazuhiro Yasufuku 1. To review guidelines for follow up and management
Organ Imaging : September 25 2015 OBJECTIVES Case Based Discussion: State of the Art Management of Lung Nodules Dr. Elsie T. Nguyen Dr. Kazuhiro Yasufuku 1. To review guidelines for follow up and management
CT Screening for Lung Cancer for High Risk Patients
 CT Screening for Lung Cancer for High Risk Patients The recently published National Lung Cancer Screening Trial (NLST) showed that low-dose CT screening for lung cancer reduces mortality in high-risk patients
CT Screening for Lung Cancer for High Risk Patients The recently published National Lung Cancer Screening Trial (NLST) showed that low-dose CT screening for lung cancer reduces mortality in high-risk patients
Approach to Pulmonary Nodules
 Approach to Pulmonary Nodules Edwin Jackson, Jr., DO Assistant Professor-Clinical Director, James Early Detection Clinic Department of Internal Medicine Division of Pulmonary, Allergy, Critical Care and
Approach to Pulmonary Nodules Edwin Jackson, Jr., DO Assistant Professor-Clinical Director, James Early Detection Clinic Department of Internal Medicine Division of Pulmonary, Allergy, Critical Care and
Pulmonary Nodules & Masses
 Pulmonary Nodules & Masses A Diagnostic Approach Heber MacMahon The University of Chicago Department of Radiology Disclosure Information Consultant for Riverain Technology Minor equity in Hologic Royalties
Pulmonary Nodules & Masses A Diagnostic Approach Heber MacMahon The University of Chicago Department of Radiology Disclosure Information Consultant for Riverain Technology Minor equity in Hologic Royalties
Adam J. Hansen, MD UHC Thoracic Surgery
 Adam J. Hansen, MD UHC Thoracic Surgery Sometimes seen on Chest X-ray (CXR) Common incidental findings on computed tomography (CT) chest and abdomen done for other reasons Most lung cancers discovered
Adam J. Hansen, MD UHC Thoracic Surgery Sometimes seen on Chest X-ray (CXR) Common incidental findings on computed tomography (CT) chest and abdomen done for other reasons Most lung cancers discovered
LUNG NODULES: MODERN MANAGEMENT STRATEGIES
 Department of Radiology LUNG NODULES: MODERN MANAGEMENT STRATEGIES Christian J. Herold M.D. Department of Biomedical Imaging and Image-guided Therapy Medical University of Vienna Vienna, Austria Pulmonary
Department of Radiology LUNG NODULES: MODERN MANAGEMENT STRATEGIES Christian J. Herold M.D. Department of Biomedical Imaging and Image-guided Therapy Medical University of Vienna Vienna, Austria Pulmonary
Learning Objectives. 1. Identify which patients meet criteria for annual lung cancer screening
 Disclosure I, Taylor Rowlett, DO NOT have a financial interest /arrangement or affiliation with one or more organizations that could be perceived as a real or apparent conflict of interest in the context
Disclosure I, Taylor Rowlett, DO NOT have a financial interest /arrangement or affiliation with one or more organizations that could be perceived as a real or apparent conflict of interest in the context
Pulmonary Nodules. Michael Morris, MD
 Pulmonary Nodules Michael Morris, MD Case 45 year old healthy male Smokes socially Normal physical exam Pre-employment screening remote +PPD screening CXR nodular opacity Case 45 year old healthy male
Pulmonary Nodules Michael Morris, MD Case 45 year old healthy male Smokes socially Normal physical exam Pre-employment screening remote +PPD screening CXR nodular opacity Case 45 year old healthy male
The small subsolid pulmonary nodules. What radiologists need to know.
 The small subsolid pulmonary nodules. What radiologists need to know. Poster No.: C-1250 Congress: ECR 2016 Type: Educational Exhibit Authors: L. Fernandez Rodriguez, A. Martín Díaz, A. Linares Beltrán,
The small subsolid pulmonary nodules. What radiologists need to know. Poster No.: C-1250 Congress: ECR 2016 Type: Educational Exhibit Authors: L. Fernandez Rodriguez, A. Martín Díaz, A. Linares Beltrán,
DENOMINATOR: All final reports for CT imaging studies with a finding of an incidental pulmonary nodule for patients aged 35 years and older
 Quality ID #364: Optimizing Patient Exposure to Ionizing Radiation: Appropriateness: Follow-up CT Imaging for Incidentally Detected Pulmonary Nodules According to Recommended Guidelines National Quality
Quality ID #364: Optimizing Patient Exposure to Ionizing Radiation: Appropriateness: Follow-up CT Imaging for Incidentally Detected Pulmonary Nodules According to Recommended Guidelines National Quality
THE BENEFITS OF BIG DATA
 THE BENEFITS OF BIG DATA Disclosures I am a named inventor on a number of patents and patent applications relating to the evaluation of pulmonary nodules on CT scans of the chest which are owned by Cornell
THE BENEFITS OF BIG DATA Disclosures I am a named inventor on a number of patents and patent applications relating to the evaluation of pulmonary nodules on CT scans of the chest which are owned by Cornell
Lung Cancer Screening: To Screen or Not to Screen?
 Lung Cancer Screening: To Screen or Not to Screen? Lorriana Leard, MD Co-Director of UCSF Lung Cancer Screening Program Vice Chief of Clinical Activities UCSF Pulmonary, Critical Care, Allergy & Sleep
Lung Cancer Screening: To Screen or Not to Screen? Lorriana Leard, MD Co-Director of UCSF Lung Cancer Screening Program Vice Chief of Clinical Activities UCSF Pulmonary, Critical Care, Allergy & Sleep
2018 OPTIONS FOR INDIVIDUAL MEASURES: REGISTRY ONLY. MEASURE TYPE: Process
 Quality ID #364: Optimizing Patient Exposure to Ionizing Radiation: Appropriateness: Follow-up CT Imaging for Incidentally Detected Pulmonary Nodules According to Recommended Guidelines National Quality
Quality ID #364: Optimizing Patient Exposure to Ionizing Radiation: Appropriateness: Follow-up CT Imaging for Incidentally Detected Pulmonary Nodules According to Recommended Guidelines National Quality
The Spectrum of Management of Pulmonary Ground Glass Nodules
 The Spectrum of Management of Pulmonary Ground Glass Nodules Stanley S Siegelman CT Society 10/26/2011 No financial disclosures. Noguchi M et al. Cancer 75: 2844-2852, 1995. 236 surgically resected peripheral
The Spectrum of Management of Pulmonary Ground Glass Nodules Stanley S Siegelman CT Society 10/26/2011 No financial disclosures. Noguchi M et al. Cancer 75: 2844-2852, 1995. 236 surgically resected peripheral
Endobronchial Ultrasound in the Diagnosis & Staging of Lung Cancer
 Endobronchial Ultrasound in the Diagnosis & Staging of Lung Cancer Dr Richard Booton PhD FRCP Lead Lung Cancer Clinician, Consultant Respiratory Physician & Speciality Director Manchester University NHS
Endobronchial Ultrasound in the Diagnosis & Staging of Lung Cancer Dr Richard Booton PhD FRCP Lead Lung Cancer Clinician, Consultant Respiratory Physician & Speciality Director Manchester University NHS
SCBT-MR 2015 Incidentaloma on Chest CT
 SCBT-MR 2015 Incidentaloma on Chest CT Reginald F. Munden MD, DMD, MBA I have no conflicts of interest to report Incidentaloma Pulmonary Nodule Mediastinal Lymph Node Coronary Artery Calcium Incidental
SCBT-MR 2015 Incidentaloma on Chest CT Reginald F. Munden MD, DMD, MBA I have no conflicts of interest to report Incidentaloma Pulmonary Nodule Mediastinal Lymph Node Coronary Artery Calcium Incidental
Published Pulmonary Nodule Guidelines A Synthesis
 Published Pulmonary Nodule Guidelines A Synthesis Dr A Devaraj Royal Brompton Hospital London 4/28/2015 1 And very soon to be published Published ^ Pulmonary Nodule Guidelines A Synthesis Dr A Devaraj
Published Pulmonary Nodule Guidelines A Synthesis Dr A Devaraj Royal Brompton Hospital London 4/28/2015 1 And very soon to be published Published ^ Pulmonary Nodule Guidelines A Synthesis Dr A Devaraj
Small Pulmonary Nodules: Our Preliminary Experience in Volumetric Analysis of Doubling Times
 Small Pulmonary Nodules: Our Preliminary Experience in Volumetric Analysis of Doubling Times Andrea Borghesi, MD Davide Farina, MD Roberto Maroldi, MD Department of Radiology University of Brescia Brescia,
Small Pulmonary Nodules: Our Preliminary Experience in Volumetric Analysis of Doubling Times Andrea Borghesi, MD Davide Farina, MD Roberto Maroldi, MD Department of Radiology University of Brescia Brescia,
Low-dose CT Lung Cancer Screening Guidelines for Pulmonary Nodules Management Version 2
 Low-dose CT Lung Cancer Screening Guidelines for Pulmonary Nodules Management Version 2 The Committee for Management of CT-screening-detected Pulmonary Nodules 2009-2011 The Japanese Society of CT Screening
Low-dose CT Lung Cancer Screening Guidelines for Pulmonary Nodules Management Version 2 The Committee for Management of CT-screening-detected Pulmonary Nodules 2009-2011 The Japanese Society of CT Screening
Screening for Lung Cancer: New Guidelines, Old Problems
 Screening for Lung Cancer: New Guidelines, Old Problems Robert Schilz DO, PhD Associate Professor of Medicine Interim Chief of the Division of Pulmonary, Critical Care and Sleep Medicine University Hospitals
Screening for Lung Cancer: New Guidelines, Old Problems Robert Schilz DO, PhD Associate Professor of Medicine Interim Chief of the Division of Pulmonary, Critical Care and Sleep Medicine University Hospitals
I appreciate the courtesy of Kusumoto at NCC for this presentation. What is Early Lung Cancers. Early Lung Cancers. Early Lung Cancers 18/10/55
 I appreciate the courtesy of Kusumoto at NCC for this presentation. Dr. What is Early Lung Cancers DEATH Early period in its lifetime Curative period in its lifetime Early Lung Cancers Early Lung Cancers
I appreciate the courtesy of Kusumoto at NCC for this presentation. Dr. What is Early Lung Cancers DEATH Early period in its lifetime Curative period in its lifetime Early Lung Cancers Early Lung Cancers
PULMONARY NODULES DETECTED INCIDENTALLY OR BY SCREENING: LOTS OF GUIDELINES BUT WHERE IS THE EVIDENCE?
 PULMONARY NODULES DETECTED INCIDENTALLY OR BY SCREENING: LOTS OF GUIDELINES BUT WHERE IS THE EVIDENCE? MICHAEL K. GOULD, MD SENIOR RESEARCH SCIENTIST DIRECTOR FOR HEALTH SCIENCES & IMPLEMENTATION SCIENCE
PULMONARY NODULES DETECTED INCIDENTALLY OR BY SCREENING: LOTS OF GUIDELINES BUT WHERE IS THE EVIDENCE? MICHAEL K. GOULD, MD SENIOR RESEARCH SCIENTIST DIRECTOR FOR HEALTH SCIENCES & IMPLEMENTATION SCIENCE
The solitary pulmonary nodule: Assessing the success of predicting malignancy
 The solitary pulmonary nodule: Assessing the success of predicting malignancy Poster No.: C-0829 Congress: ECR 2010 Type: Scientific Exhibit Topic: Chest Authors: R. W. K. Lindsay, J. Foster, K. McManus;
The solitary pulmonary nodule: Assessing the success of predicting malignancy Poster No.: C-0829 Congress: ECR 2010 Type: Scientific Exhibit Topic: Chest Authors: R. W. K. Lindsay, J. Foster, K. McManus;
THORACIK RICK. Lungs. Outline and objectives Richard A. Malthaner MD MSc FRCSC FACS
 THORACIK RICK Outline and objectives Lungs Management of a solitary lung nodule Mediastinum Management of a mediastinal mass Pleura Management of a pleural fluid & pneumothorax Esophagus & Stomach Management
THORACIK RICK Outline and objectives Lungs Management of a solitary lung nodule Mediastinum Management of a mediastinal mass Pleura Management of a pleural fluid & pneumothorax Esophagus & Stomach Management
Best Medical Practices: Maximizing Skills, Minimizing Risk Lung Cancer
 Best Medical Practices: Maximizing Skills, Minimizing Risk Lung Cancer Optimal Management of Incidental Pulmonary Nodule Ramin Khorasani, MD, MPH Vice Chair, Department of Radiology Director, Center for
Best Medical Practices: Maximizing Skills, Minimizing Risk Lung Cancer Optimal Management of Incidental Pulmonary Nodule Ramin Khorasani, MD, MPH Vice Chair, Department of Radiology Director, Center for
Lung Cancer Diagnosis for Primary Care
 Lung Cancer Diagnosis for Primary Care Daniel Nader, DO, FCCP Cancer Treatment Center of America Case 1 In which of the following situations would the U.S. Preventive Services Task Force (USPSTF) recommend
Lung Cancer Diagnosis for Primary Care Daniel Nader, DO, FCCP Cancer Treatment Center of America Case 1 In which of the following situations would the U.S. Preventive Services Task Force (USPSTF) recommend
Comparison of three mathematical prediction models in patients with a solitary pulmonary nodule
 Original Article Comparison of three mathematical prediction models in patients with a solitary pulmonary nodule Xuan Zhang*, Hong-Hong Yan, Jun-Tao Lin, Ze-Hua Wu, Jia Liu, Xu-Wei Cao, Xue-Ning Yang From
Original Article Comparison of three mathematical prediction models in patients with a solitary pulmonary nodule Xuan Zhang*, Hong-Hong Yan, Jun-Tao Lin, Ze-Hua Wu, Jia Liu, Xu-Wei Cao, Xue-Ning Yang From
Evaluation of Individuals With Pulmonary Nodules: When Is It Lung Cancer?
 CHEST Supplement DIAGNOSIS AND MANAGEMENT OF LUNG CANCER, 3RD ED: ACCP GUIDELINES Evaluation of Individuals With Pulmonary Nodules: When Is It Lung Cancer? Diagnosis and Management of Lung Cancer, 3rd
CHEST Supplement DIAGNOSIS AND MANAGEMENT OF LUNG CANCER, 3RD ED: ACCP GUIDELINES Evaluation of Individuals With Pulmonary Nodules: When Is It Lung Cancer? Diagnosis and Management of Lung Cancer, 3rd
Rodney C Richie MD FACP FCCP DBIM Texas Life and EMSI
 Rodney C Richie MD FACP FCCP DBIM Texas Life and EMSI Pulmonary Nodules Well-circumscribed, radiographic opacities measuring 3 cm in diameter Surrounded by aerated lung Not associated with atelectesis
Rodney C Richie MD FACP FCCP DBIM Texas Life and EMSI Pulmonary Nodules Well-circumscribed, radiographic opacities measuring 3 cm in diameter Surrounded by aerated lung Not associated with atelectesis
Charles Mulligan, MD, FACS, FCCP 26 March 2015
 Charles Mulligan, MD, FACS, FCCP 26 March 2015 Review lung cancer statistics Review the risk factors Discuss presentation and staging Discuss treatment options and outcomes Discuss the status of screening
Charles Mulligan, MD, FACS, FCCP 26 March 2015 Review lung cancer statistics Review the risk factors Discuss presentation and staging Discuss treatment options and outcomes Discuss the status of screening
GROUP 1: Peripheral tumour with normal hilar and mediastinum on staging CT with no disant metastases. Including: Excluding:
 GROUP 1: Including: Excluding: Peripheral tumour with normal hilar and mediastinum on staging CT with no disant metastases Solid pulmonary nodules 8mm diameter / 300mm3 volume and BROCK risk of malignancy
GROUP 1: Including: Excluding: Peripheral tumour with normal hilar and mediastinum on staging CT with no disant metastases Solid pulmonary nodules 8mm diameter / 300mm3 volume and BROCK risk of malignancy
What to Do with Small Lung Nodules Hanh Vu Nghiem, MD William Beaumont Hospital Royal Oak, Michigan
 What to Do with Small Lung Nodules Hanh Vu Nghiem, MD William Beaumont Hospital Royal Oak, Michigan Small Lung Nodules What to do with small lung nodules? We biopsy them when requested What are our accuracy
What to Do with Small Lung Nodules Hanh Vu Nghiem, MD William Beaumont Hospital Royal Oak, Michigan Small Lung Nodules What to do with small lung nodules? We biopsy them when requested What are our accuracy
The Maine Lung Cancer Coalition. Working Together to Reduce Lung Cancer in Maine
 The Maine Lung Cancer Coalition Working Together to Reduce Lung Cancer in Maine funding Maine Lung Cancer Coalition (MLCC) Webinar Lung Cancer Screening: Following Up On Abnormal Low Dose CT Scans with
The Maine Lung Cancer Coalition Working Together to Reduce Lung Cancer in Maine funding Maine Lung Cancer Coalition (MLCC) Webinar Lung Cancer Screening: Following Up On Abnormal Low Dose CT Scans with
Imaging Decisions Start Here SM
 Owing to its high resolution and wide anatomic coverage, dynamic first-pass perfusion 320-detector-row CT outperforms PET/CT for distinguishing benign from malignant lung nodules, researchers from Japan
Owing to its high resolution and wide anatomic coverage, dynamic first-pass perfusion 320-detector-row CT outperforms PET/CT for distinguishing benign from malignant lung nodules, researchers from Japan
Larry Tan, MD Thoracic Surgery, HSC. Community Cancer Care Educational Conference October 27, 2017
 Larry Tan, MD Thoracic Surgery, HSC Community Cancer Care Educational Conference October 27, 2017 To describe patient referral & triage for the patient with suspected lung cancer To describe the initial
Larry Tan, MD Thoracic Surgery, HSC Community Cancer Care Educational Conference October 27, 2017 To describe patient referral & triage for the patient with suspected lung cancer To describe the initial
Screening Programs background and clinical implementation. Denise R. Aberle, MD Professor of Radiology and Engineering
 Screening Programs background and clinical implementation Denise R. Aberle, MD Professor of Radiology and Engineering disclosures I have no disclosures. I have no conflicts of interest relevant to this
Screening Programs background and clinical implementation Denise R. Aberle, MD Professor of Radiology and Engineering disclosures I have no disclosures. I have no conflicts of interest relevant to this
Xiaohuan Pan 1,2 *, Xinguan Yang 1,2 *, Jingxu Li 1,2, Xiao Dong 1,2, Jianxing He 2,3, Yubao Guan 1,2. Original Article
 Original Article Is a 5-mm diameter an appropriate cut-off value for the diagnosis of atypical adenomatous hyperplasia and adenocarcinoma in situ on chest computed tomography and pathological examination?
Original Article Is a 5-mm diameter an appropriate cut-off value for the diagnosis of atypical adenomatous hyperplasia and adenocarcinoma in situ on chest computed tomography and pathological examination?
Management of Multiple Pure Ground-Glass Opacity Lesions in Patients with Bronchioloalveolar Carcinoma
 ORIGINAL ARTICLE Management of Multiple Pure Ground-Glass Opacity Lesions in Patients with Bronchioloalveolar Carcinoma Hong Kwan Kim, MD,* Yong Soo Choi, MD,* Jhingook Kim, MD, PhD,* Young Mog Shim, MD,
ORIGINAL ARTICLE Management of Multiple Pure Ground-Glass Opacity Lesions in Patients with Bronchioloalveolar Carcinoma Hong Kwan Kim, MD,* Yong Soo Choi, MD,* Jhingook Kim, MD, PhD,* Young Mog Shim, MD,
Screening for Lung Cancer: Are We There Yet?
 Screening for Lung Cancer: Are We There Yet? Kavita Garg, MD Professor of Radiology University of CO, Denver Mountain States Cancer Conference Nov 6 th 2010 The Epidemiology of Lung Cancer Tobacco is the
Screening for Lung Cancer: Are We There Yet? Kavita Garg, MD Professor of Radiology University of CO, Denver Mountain States Cancer Conference Nov 6 th 2010 The Epidemiology of Lung Cancer Tobacco is the
With recent advances in diagnostic imaging technologies,
 ORIGINAL ARTICLE Management of Ground-Glass Opacity Lesions Detected in Patients with Otherwise Operable Non-small Cell Lung Cancer Hong Kwan Kim, MD,* Yong Soo Choi, MD,* Kwhanmien Kim, MD,* Young Mog
ORIGINAL ARTICLE Management of Ground-Glass Opacity Lesions Detected in Patients with Otherwise Operable Non-small Cell Lung Cancer Hong Kwan Kim, MD,* Yong Soo Choi, MD,* Kwhanmien Kim, MD,* Young Mog
Guidelines for the Management of Pulmonary Nodules Detected by Low-dose CT Lung Cancer Screening
 Guidelines for the Management of Pulmonary Nodules Detected by Low-dose CT Lung Cancer Screening 1. Introduction In January 2005, the Committee for Preparation of Clinical Practice Guidelines for the Management
Guidelines for the Management of Pulmonary Nodules Detected by Low-dose CT Lung Cancer Screening 1. Introduction In January 2005, the Committee for Preparation of Clinical Practice Guidelines for the Management
American College of Radiology ACR Appropriateness Criteria
 American College of Radiology ACR Criteria Radiologic Management of Thoracic Nodules and Masses Variant 1: Middle-aged patient (35 60 years old) with an incidental 1.5-cm lung nodule. The lesion was smooth.
American College of Radiology ACR Criteria Radiologic Management of Thoracic Nodules and Masses Variant 1: Middle-aged patient (35 60 years old) with an incidental 1.5-cm lung nodule. The lesion was smooth.
PET/CT in lung cancer
 PET/CT in lung cancer Andrei Šamarin North Estonia Medical Centre 3 rd Baltic Congress of Radiology 08.10.2010 Imaging in lung cancer Why do we need PET/CT? CT is routine imaging modality for staging of
PET/CT in lung cancer Andrei Šamarin North Estonia Medical Centre 3 rd Baltic Congress of Radiology 08.10.2010 Imaging in lung cancer Why do we need PET/CT? CT is routine imaging modality for staging of
Educational Objectives. Managing Lung Cancer From the Solitary Pulmonary Nodule to Complex Cases: A Multidisciplinary Approach.
 Managing Lung Cancer From the Solitary Pulmonary Nodule to Complex Cases: A Multidisciplinary Approach Robert A. Meguid, MD, MPH, FACS Assistant Professor of Cardiothoracic Surgery Surgical Director, Surgical
Managing Lung Cancer From the Solitary Pulmonary Nodule to Complex Cases: A Multidisciplinary Approach Robert A. Meguid, MD, MPH, FACS Assistant Professor of Cardiothoracic Surgery Surgical Director, Surgical
Role of CT imaging to evaluate solitary pulmonary nodule with extrapulmonary neoplasms
 Original Research Article Role of CT imaging to evaluate solitary pulmonary nodule with extrapulmonary neoplasms Anand Vachhani 1, Shashvat Modia 1*, Varun Garasia 1, Deepak Bhimani 1, C. Raychaudhuri
Original Research Article Role of CT imaging to evaluate solitary pulmonary nodule with extrapulmonary neoplasms Anand Vachhani 1, Shashvat Modia 1*, Varun Garasia 1, Deepak Bhimani 1, C. Raychaudhuri
PET CT for Staging Lung Cancer
 PET CT for Staging Lung Cancer Rohit Kochhar Consultant Radiologist Disclosures Neither I nor my immediate family members have financial relationships with commercial organizations that may have a direct
PET CT for Staging Lung Cancer Rohit Kochhar Consultant Radiologist Disclosures Neither I nor my immediate family members have financial relationships with commercial organizations that may have a direct
Thoracic CT pattern in lung cancer: correlation of CT and pathologic diagnosis
 19 th Congress of APSR PG of Lung Cancer (ESAP): Update of Lung Cancer Thoracic CT pattern in lung cancer: correlation of CT and pathologic diagnosis Kazuma Kishi, M.D. Department of Respiratory Medicine,
19 th Congress of APSR PG of Lung Cancer (ESAP): Update of Lung Cancer Thoracic CT pattern in lung cancer: correlation of CT and pathologic diagnosis Kazuma Kishi, M.D. Department of Respiratory Medicine,
Malignant solitary pulmonary nodules: assessment of mass growth rate and doubling time at follow-up CT
 Original Article Malignant solitary pulmonary nodules: assessment of mass growth rate and doubling time at follow-up CT Jingxu Li*, Tingting Xia*, Xinguan Yang, Xiao Dong, Jiamin Liang, Nanshan Zhong,
Original Article Malignant solitary pulmonary nodules: assessment of mass growth rate and doubling time at follow-up CT Jingxu Li*, Tingting Xia*, Xinguan Yang, Xiao Dong, Jiamin Liang, Nanshan Zhong,
SCBT-MR 2016 Lung Cancer Screening in Practice: State of the Art
 SCBT-MR 2016 Lung Cancer Screening in Practice: State of the Art Reginald F. Munden MD, DMD, MBA I have no conflicts of interest to report National Lung Cancer Screening Trial 20% lung cancer mortality
SCBT-MR 2016 Lung Cancer Screening in Practice: State of the Art Reginald F. Munden MD, DMD, MBA I have no conflicts of interest to report National Lung Cancer Screening Trial 20% lung cancer mortality
Robert J. McKenna M.D. Chief, Thoracic Surgery Cedars Sinai Medical Center
 You Smoke, You Get Lung Cancer, You Die: Can Screening Change this Paradigm? Robert J. McKenna M.D. Chief, Thoracic Surgery Cedars Sinai Medical Center AATS Saturday 4/28/2012 Cancer Screening Cancer
You Smoke, You Get Lung Cancer, You Die: Can Screening Change this Paradigm? Robert J. McKenna M.D. Chief, Thoracic Surgery Cedars Sinai Medical Center AATS Saturday 4/28/2012 Cancer Screening Cancer
May-Lin Wilgus. A. Study Purpose and Rationale
 Utility of a Computer-Aided Diagnosis Program in the Evaluation of Solitary Pulmonary Nodules Detected on Computed Tomography Scans: A Prospective Observational Study May-Lin Wilgus A. Study Purpose and
Utility of a Computer-Aided Diagnosis Program in the Evaluation of Solitary Pulmonary Nodules Detected on Computed Tomography Scans: A Prospective Observational Study May-Lin Wilgus A. Study Purpose and
Guidelines for Management of Incidental Pulmonary Nodules Detected on CT Images: From the Fleischner Society
 This copy is for personal use only. To order printed copies, contact reprints@rsna.org Heber MacMahon, MB, BCh David P. Naidich, MD Jin Mo Goo, MD, PhD Kyung Soo Lee, MD, PhD Ann N. C. Leung, MD John R.
This copy is for personal use only. To order printed copies, contact reprints@rsna.org Heber MacMahon, MB, BCh David P. Naidich, MD Jin Mo Goo, MD, PhD Kyung Soo Lee, MD, PhD Ann N. C. Leung, MD John R.
Pulmonary Nodules: When to worry, when to chill. Douglas Arenberg Associate Professor Pulmonary & Critical Care
 Pulmonary Nodules: When to worry, when to chill Douglas Arenberg Associate Professor Pulmonary & Critical Care Disclosure MDCH Grant Funds to improve tobacco cessation service in the Michigan Medicine
Pulmonary Nodules: When to worry, when to chill Douglas Arenberg Associate Professor Pulmonary & Critical Care Disclosure MDCH Grant Funds to improve tobacco cessation service in the Michigan Medicine
Erica Giblin, MD Holy Family Hospital
 Erica Giblin, MD Holy Family Hospital Electromagnetic Navigation Bronchoscopy A New Treatment for Patients with Peripheral Lung Lesions Lung Cancer: An Epidemic? In the U.S.: #1 cause of cancer-related
Erica Giblin, MD Holy Family Hospital Electromagnetic Navigation Bronchoscopy A New Treatment for Patients with Peripheral Lung Lesions Lung Cancer: An Epidemic? In the U.S.: #1 cause of cancer-related
Noninvasive Differential Diagnosis of Pulmonary Nodules Using the Standardized Uptake Value Index
 doi: 10.5761/atcs.oa.14-00241 Original Article Noninvasive Differential Diagnosis of Pulmonary Nodules Using the Standardized Uptake Value Index Satoshi Shiono, MD, 1 Naoki Yanagawa, MD, 2 Masami Abiko,
doi: 10.5761/atcs.oa.14-00241 Original Article Noninvasive Differential Diagnosis of Pulmonary Nodules Using the Standardized Uptake Value Index Satoshi Shiono, MD, 1 Naoki Yanagawa, MD, 2 Masami Abiko,
Corporate Medical Policy Electromagnetic Navigation Bronchoscopy
 Corporate Medical Policy Electromagnetic Navigation Bronchoscopy File Name: Origination: Last CAP Review: Next CAP Review: Last Review: electromagnetic_navigation_bronchoscopy 1/2010 3/2017 3/2018 9/2017
Corporate Medical Policy Electromagnetic Navigation Bronchoscopy File Name: Origination: Last CAP Review: Next CAP Review: Last Review: electromagnetic_navigation_bronchoscopy 1/2010 3/2017 3/2018 9/2017
Lung. 10/24/13 Chest X-ray: 2.9 cm mass like density in the inferior lingular segment worrisome for neoplasm. Malignancy cannot be excluded.
 Lung Case Scenario 1 A 54 year white male presents with a recent abnormal CT of the chest. The patient has a history of melanoma, kidney, and prostate cancers. 10/24/13 Chest X-ray: 2.9 cm mass like density
Lung Case Scenario 1 A 54 year white male presents with a recent abnormal CT of the chest. The patient has a history of melanoma, kidney, and prostate cancers. 10/24/13 Chest X-ray: 2.9 cm mass like density
PET/CT Frequently Asked Questions
 PET/CT Frequently Asked Questions General Q: Is FDG PET specific for cancer? A: No, it is a marker of metabolism. In general, any disease that causes increased metabolism can result in increased FDG uptake
PET/CT Frequently Asked Questions General Q: Is FDG PET specific for cancer? A: No, it is a marker of metabolism. In general, any disease that causes increased metabolism can result in increased FDG uptake
VATS Metastasectomy. Inderpal (Netu) S. Sarkaria, MD, FACS
 S. Sarkaria, MD, FACS") VATS Metastasectomy Inderpal (Netu) S. Sarkaria, MD, FACS Vice Chairman, Clinical Affairs Director, Robotic Thoracic Surgery Co-Director, Esophageal and Lung Surgery Institute Disclosures Speaking & Education:
VATS Metastasectomy Inderpal (Netu) S. Sarkaria, MD, FACS Vice Chairman, Clinical Affairs Director, Robotic Thoracic Surgery Co-Director, Esophageal and Lung Surgery Institute Disclosures Speaking & Education:
A Chronology of Advancements in the Diagnosing of Lung Nodules
 November 17, 2017 A Chronology of Advancements in the Diagnosing of Lung Nodules Presenter: Daniel P. Harley, MD, MSB, FACS Surgical Director of the Angelos Center for Lung Diseases 1 Pulmonary Nodules
November 17, 2017 A Chronology of Advancements in the Diagnosing of Lung Nodules Presenter: Daniel P. Harley, MD, MSB, FACS Surgical Director of the Angelos Center for Lung Diseases 1 Pulmonary Nodules
Lung Cancer screening :
 Lung Cancer screening : Pro-Contra SAMO interdisciplinary workshop on chest tumors 27 and 28 january 2017 Prof L.P.Nicod Sevice de pneumologie CHUV-Lausanne -CH Lung Cancer How big is the problem? Epidemiology
Lung Cancer screening : Pro-Contra SAMO interdisciplinary workshop on chest tumors 27 and 28 january 2017 Prof L.P.Nicod Sevice de pneumologie CHUV-Lausanne -CH Lung Cancer How big is the problem? Epidemiology
Example of lung screening
 Justification of the use of CT for individual health assessment of asymptomatic people How to obtain evidence for IHA - Example of lung screening Mathias Prokop, MD PhD Professor of Radiology Radboud University
Justification of the use of CT for individual health assessment of asymptomatic people How to obtain evidence for IHA - Example of lung screening Mathias Prokop, MD PhD Professor of Radiology Radboud University
What to know and what to make of it
 Lung Cancer Screening: What to know and what to make of it J. Matthew Reinersman, MD Assistant Professor of Surgery Division of Thoracic and Cardiovascular Surgery Department of Surgery University of Oklahoma
Lung Cancer Screening: What to know and what to make of it J. Matthew Reinersman, MD Assistant Professor of Surgery Division of Thoracic and Cardiovascular Surgery Department of Surgery University of Oklahoma
FDG PET/CT STAGING OF LUNG CANCER. Dr Shakher Ramdave
 FDG PET/CT STAGING OF LUNG CANCER Dr Shakher Ramdave FDG PET/CT STAGING OF LUNG CANCER FDG PET/CT is used in all patients with lung cancer who are considered for curative treatment to exclude occult disease.
FDG PET/CT STAGING OF LUNG CANCER Dr Shakher Ramdave FDG PET/CT STAGING OF LUNG CANCER FDG PET/CT is used in all patients with lung cancer who are considered for curative treatment to exclude occult disease.
Electromagnetic navigational bronchoscopy in patients with solitary pulmonary nodules
 Original article Electromagnetic navigational bronchoscopy in patients with solitary pulmonary nodules Samuel Copeland MD, Shrinivas Kambali MD, Gilbert Berdine MD, Raed Alalawi MD Abstract Background:
Original article Electromagnetic navigational bronchoscopy in patients with solitary pulmonary nodules Samuel Copeland MD, Shrinivas Kambali MD, Gilbert Berdine MD, Raed Alalawi MD Abstract Background:
Bronchogenic Carcinoma
 A 55-year-old construction worker has smoked 2 packs of ciggarettes daily for the past 25 years. He notes swelling in his upper extremity & face, along with dilated veins in this region. What is the most
A 55-year-old construction worker has smoked 2 packs of ciggarettes daily for the past 25 years. He notes swelling in his upper extremity & face, along with dilated veins in this region. What is the most
objectives Pitfalls and Pearls in PET/CT imaging Kevin Robinson, DO Assistant Professor Department of Radiology Michigan State University
 objectives Pitfalls and Pearls in PET/CT imaging Kevin Robinson, DO Assistant Professor Department of Radiology Michigan State University To determine the regions of physiologic activity To understand
objectives Pitfalls and Pearls in PET/CT imaging Kevin Robinson, DO Assistant Professor Department of Radiology Michigan State University To determine the regions of physiologic activity To understand
SCBT-MR 2015 LungRADS : Basics
 SCBT-MR 2015 LungRADS : Basics Reginald F. Munden MD, DMD, MBA I have no conflicts of interest to report National Lung Cancer Screening Trial 20% lung cancer mortality reduction 6.9% all cause mortality
SCBT-MR 2015 LungRADS : Basics Reginald F. Munden MD, DMD, MBA I have no conflicts of interest to report National Lung Cancer Screening Trial 20% lung cancer mortality reduction 6.9% all cause mortality
Lung Cancer Screening in the Midwest of the US: When Histoplasmosis Complicates the Picture
 Cronicon OPEN ACCESS EC PULMONOLOGY AND RESPIRATORY MEDICINE Case Report Lung Cancer Screening in the Midwest of the US: When Histoplasmosis Complicates the Picture Swan Lee 1 and Rolando Sanchez Sanchez
Cronicon OPEN ACCESS EC PULMONOLOGY AND RESPIRATORY MEDICINE Case Report Lung Cancer Screening in the Midwest of the US: When Histoplasmosis Complicates the Picture Swan Lee 1 and Rolando Sanchez Sanchez
RF Ablation: indication, technique and imaging follow-up
 RF Ablation: indication, technique and imaging follow-up Trongtum Tongdee, M.D. Radiology Department, Faculty of Medicine, Siriraj Hospital, Mahidol University, Bangkok, Thailand Objective Basic knowledge
RF Ablation: indication, technique and imaging follow-up Trongtum Tongdee, M.D. Radiology Department, Faculty of Medicine, Siriraj Hospital, Mahidol University, Bangkok, Thailand Objective Basic knowledge
Radial endobronchial ultrasound (EBUS), performed during
, performed during") Original Article Can Computed Tomography Characteristics Predict Outcomes in Patients Undergoing Radial Endobronchial Ultrasound-Guided Biopsy of Peripheral Lung Lesions? Matthew Evison,* Philip A.J. Crosbie,*
Original Article Can Computed Tomography Characteristics Predict Outcomes in Patients Undergoing Radial Endobronchial Ultrasound-Guided Biopsy of Peripheral Lung Lesions? Matthew Evison,* Philip A.J. Crosbie,*
Lung Cancer-a primer. Sai Yendamuri, MD Professor and Chair, Dept of Thoracic Surgery,RPCI,Buffalo
 Lung Cancer-a primer Sai Yendamuri, MD Professor and Chair, Dept of Thoracic Surgery,RPCI,Buffalo CLINICAL CATEGORIES THE SOLITARY PULMONARY NODULE MULTIPLE PULMONARY NODULES Differential Diagnosis Malignant
Lung Cancer-a primer Sai Yendamuri, MD Professor and Chair, Dept of Thoracic Surgery,RPCI,Buffalo CLINICAL CATEGORIES THE SOLITARY PULMONARY NODULE MULTIPLE PULMONARY NODULES Differential Diagnosis Malignant
None
 2014 None rosemary clooney Cancer is one of the most common diseases in the developed world: 1 in 4 deaths are due to cancer 1 in 17 deaths are due to lung cancer Lung cancer is the most common
2014 None rosemary clooney Cancer is one of the most common diseases in the developed world: 1 in 4 deaths are due to cancer 1 in 17 deaths are due to lung cancer Lung cancer is the most common
LUNG CANCER SCREENING WHAT S THE IMPACT? Nitra Piyavisetpat, MD Department of Radiology Chulalongkorn University
 LUNG CANCER SCREENING WHAT S THE IMPACT? Nitra Piyavisetpat, MD Department of Radiology Chulalongkorn University Objective LDCT lung cancer screening (LCS) Potential Benefits & Harms Recommendation of
LUNG CANCER SCREENING WHAT S THE IMPACT? Nitra Piyavisetpat, MD Department of Radiology Chulalongkorn University Objective LDCT lung cancer screening (LCS) Potential Benefits & Harms Recommendation of
Volume and Mass Doubling Times of Persistent Pulmonary Subsolid Nodules Detected in Patients without Known Malignancy 1
 Note: This copy is for your personal non-commercial use only. To order presentation-ready copies for distribution to your colleagues or clients, contact us at www.rsna.org/rsnarights. Original Research
Note: This copy is for your personal non-commercial use only. To order presentation-ready copies for distribution to your colleagues or clients, contact us at www.rsna.org/rsnarights. Original Research
Chest Radiology Interpretation: Findings of Tuberculosis
 Chest Radiology Interpretation: Findings of Tuberculosis Get out your laptops, smart phones or other devices pollev.com/chestradiology Case #1 1 Plombage Pneumonia Cancer 2 Reading the TB CXR Be systematic!
Chest Radiology Interpretation: Findings of Tuberculosis Get out your laptops, smart phones or other devices pollev.com/chestradiology Case #1 1 Plombage Pneumonia Cancer 2 Reading the TB CXR Be systematic!
Deppen S, et al. Annals of Thoracic Surgery 2011;92:
 Deppen S, et al. Annals of Thoracic Surgery 2011;92:428-33. http://www.nationmaster.com/graph/ mor_his-mortality-histoplasmosis http://www.humirarems.com/brochure.aspx Baddley, John W., et al. Emerging
Deppen S, et al. Annals of Thoracic Surgery 2011;92:428-33. http://www.nationmaster.com/graph/ mor_his-mortality-histoplasmosis http://www.humirarems.com/brochure.aspx Baddley, John W., et al. Emerging
Owing to the recent attention given to lung cancer
 Electromagnetic : A Surgeon s Perspective Todd S. Weiser, MD, Kevin Hyman, MD, Jaime Yun, MD, Virginia Litle, MD, Cythinia Chin, MD, and Scott J. Swanson, MD Department of Cardiothoracic Surgery, Mount
Electromagnetic : A Surgeon s Perspective Todd S. Weiser, MD, Kevin Hyman, MD, Jaime Yun, MD, Virginia Litle, MD, Cythinia Chin, MD, and Scott J. Swanson, MD Department of Cardiothoracic Surgery, Mount
Utility of PET-CT for detection of N2 or N3 nodal mestastases in the mediastinum in patients with non-small cell lung cancer (NSCLC)
") Utility of PET-CT for detection of N2 or N3 nodal mestastases in the mediastinum in patients with non-small cell lung cancer (NSCLC) Poster No.: C-1360 Congress: ECR 2015 Type: Scientific Exhibit Authors:
Utility of PET-CT for detection of N2 or N3 nodal mestastases in the mediastinum in patients with non-small cell lung cancer (NSCLC) Poster No.: C-1360 Congress: ECR 2015 Type: Scientific Exhibit Authors:
Positron Emission Tomography in Lung Cancer
 May 19, 2003 Positron Emission Tomography in Lung Cancer Andrew Wang, HMS III Patient DD 53 y/o gentleman presented with worsening dyspnea on exertion for the past two months 30 pack-year smoking Hx and
May 19, 2003 Positron Emission Tomography in Lung Cancer Andrew Wang, HMS III Patient DD 53 y/o gentleman presented with worsening dyspnea on exertion for the past two months 30 pack-year smoking Hx and
performed to help sway the clinician in what the appropriate diagnosis is, which can substantially alter the treatment of management.
 Hello, I am Maura Polansky at the University of Texas MD Anderson Cancer Center. I am a Physician Assistant in the Department of Gastrointestinal Medical Oncology and the Program Director for Physician
Hello, I am Maura Polansky at the University of Texas MD Anderson Cancer Center. I am a Physician Assistant in the Department of Gastrointestinal Medical Oncology and the Program Director for Physician
CT Screening for Lung Cancer: Implication of Lung Biopsy Recommendations
 Cardiopulmonary Imaging Original Research Wagnetz et al. Lung Biopsy and CT Screening for Lung Cancer Cardiopulmonary Imaging Original Research Ute Wagnetz 1 Ravi J. Menezes 2 Scott Boerner 3 Narinder
Cardiopulmonary Imaging Original Research Wagnetz et al. Lung Biopsy and CT Screening for Lung Cancer Cardiopulmonary Imaging Original Research Ute Wagnetz 1 Ravi J. Menezes 2 Scott Boerner 3 Narinder
A Practical Algorithmic Approach to the Diagnosis and Management of Solitary Pulmonary Nodules. Part 2: Pretest Probability and Algorithm
 CHEST Special Features A Practical Algorithmic Approach to the Diagnosis and Management of Solitary Pulmonary Nodules Part 2: Pretest Probability and Algorithm Vishal K. Patel, MBBS ; Sagar K. Naik, MBBS
CHEST Special Features A Practical Algorithmic Approach to the Diagnosis and Management of Solitary Pulmonary Nodules Part 2: Pretest Probability and Algorithm Vishal K. Patel, MBBS ; Sagar K. Naik, MBBS
Research Article The Advantage of PET and CT Integration in Examination of Lung Tumors
 Hindawi Publishing Corporation International Journal of Biomedical Imaging Volume 2007, Article ID 17131, 5 pages doi:10.1155/2007/17131 Research Article The Advantage of PET and CT Integration in Examination
Hindawi Publishing Corporation International Journal of Biomedical Imaging Volume 2007, Article ID 17131, 5 pages doi:10.1155/2007/17131 Research Article The Advantage of PET and CT Integration in Examination
The Various Methods to Biopsy the Lung PROF SHITRIT DAVID HEAD, PULMONARY DEPARTMENT MEIR MEDICAL CENTER, ISRAEL
 The Various Methods to Biopsy the Lung PROF SHITRIT DAVID HEAD, PULMONARY DEPARTMENT MEIR MEDICAL CENTER, ISRAEL Conflict of Interest This presentation is supported by AstraZeneca Two main steps before
The Various Methods to Biopsy the Lung PROF SHITRIT DAVID HEAD, PULMONARY DEPARTMENT MEIR MEDICAL CENTER, ISRAEL Conflict of Interest This presentation is supported by AstraZeneca Two main steps before
Lung Cancer. Current Therapy JEREMIAH MARTIN MBBCh FRCSI MSCRD
 Lung Cancer Current Therapy JEREMIAH MARTIN MBBCh FRCSI MSCRD Objectives Describe risk factors, early detection & work-up of lung cancer. Define the role of modern treatment options, minimally invasive
Lung Cancer Current Therapy JEREMIAH MARTIN MBBCh FRCSI MSCRD Objectives Describe risk factors, early detection & work-up of lung cancer. Define the role of modern treatment options, minimally invasive
Will CT screening reduce overall lung cancer mortality? Associate Professor of Radiology Department of Medical Imaging UHN / MSH / WCH
 Will CT screening reduce overall lung cancer mortality? Heidi Roberts MD FRCP(C) Heidi Roberts, MD, FRCP(C) Associate Professor of Radiology Department of Medical Imaging UHN / MSH / WCH Screening - Requirements
Will CT screening reduce overall lung cancer mortality? Heidi Roberts MD FRCP(C) Heidi Roberts, MD, FRCP(C) Associate Professor of Radiology Department of Medical Imaging UHN / MSH / WCH Screening - Requirements
Lung Cancer Update. Disclosures. None
 Lung Cancer Update Ronald J Servi DO FCCP Adjunct Assistant Professor Department of Pulmonary Medicine University of Texas MD Anderson Cancer Center Banner MD Anderson Cancer Center Gilbert, Arizona Disclosures
Lung Cancer Update Ronald J Servi DO FCCP Adjunct Assistant Professor Department of Pulmonary Medicine University of Texas MD Anderson Cancer Center Banner MD Anderson Cancer Center Gilbert, Arizona Disclosures
CT Screening for Lung Cancer: Frequency and Significance of Part-Solid and Nonsolid Nodules
 Claudia I. Henschke 1 David F. Yankelevitz 1 Rosna Mirtcheva 1 Georgeann McGuinness 2 Dorothy McCauley 1 0lli S. Miettinen 3 for the ELCAP Group Received June 19, 2001; accepted after revision November
Claudia I. Henschke 1 David F. Yankelevitz 1 Rosna Mirtcheva 1 Georgeann McGuinness 2 Dorothy McCauley 1 0lli S. Miettinen 3 for the ELCAP Group Received June 19, 2001; accepted after revision November
Navigational bronchoscopy-guided dye marking to assist resection of a small lung nodule
 Case Report on Aerodigestive Endoscopy Navigational bronchoscopy-guided dye marking to assist resection of a small lung nodule Jennifer L. Sullivan 1, Michael G. Martin 2, Benny Weksler 1 1 Division of
Case Report on Aerodigestive Endoscopy Navigational bronchoscopy-guided dye marking to assist resection of a small lung nodule Jennifer L. Sullivan 1, Michael G. Martin 2, Benny Weksler 1 1 Division of
Abstract Submission Form
 Abstract Submission Form All abstracts must be submitted to the AOCR by September 15 th. All information included must be the original work of the author(s) and be in typed form. Incomplete or handwritten
Abstract Submission Form All abstracts must be submitted to the AOCR by September 15 th. All information included must be the original work of the author(s) and be in typed form. Incomplete or handwritten
Innovations in Lung Cancer Diagnosis and Surgical Treatment
 Transcript Details This is a transcript of a continuing medical education (CME) activity accessible on the ReachMD network. Additional media formats for the activity and full activity details (including
Transcript Details This is a transcript of a continuing medical education (CME) activity accessible on the ReachMD network. Additional media formats for the activity and full activity details (including
The revised lung adenocarcinoma classification an imaging guide
 Review Article The revised lung adenocarcinoma classification an imaging guide Natasha Gardiner 1, Sanjay Jogai 2, Adam Wallis 3 1 Specialty Registrar in Clinical Radiology, Wessex Deanery, UK; 2 Consultant
Review Article The revised lung adenocarcinoma classification an imaging guide Natasha Gardiner 1, Sanjay Jogai 2, Adam Wallis 3 1 Specialty Registrar in Clinical Radiology, Wessex Deanery, UK; 2 Consultant
Projected Outcomes Using Different Nodule Sizes to Define a Positive CT Lung Cancer Screening Examination
 DOI:10.1093/jnci/dju284 First published online October 20, 2014 The Author 2014. Published by Oxford University Press. All rights reserved. For Permissions, please e-mail: journals.permissions@oup.com.
DOI:10.1093/jnci/dju284 First published online October 20, 2014 The Author 2014. Published by Oxford University Press. All rights reserved. For Permissions, please e-mail: journals.permissions@oup.com.
I9 COMPLETION INSTRUCTIONS
 The I9 Form is completed for each screening exam at T0, T1, and T2. At T0 (baseline), the I9 documents comparison review of the baseline screen (C2 Form) with any historical images available. At T1 and
The I9 Form is completed for each screening exam at T0, T1, and T2. At T0 (baseline), the I9 documents comparison review of the baseline screen (C2 Form) with any historical images available. At T1 and
The Role of PET / CT in Lung Cancer Staging
 July 2004 The Role of PET / CT in Lung Cancer Staging Vlad Vinarsky, Harvard Medical School Year IV Patient AM HPI: 81 yo F p/w hemoptysis x 1 month LLL lesion on CXR, not responsive to Abx 35 pack-year
July 2004 The Role of PET / CT in Lung Cancer Staging Vlad Vinarsky, Harvard Medical School Year IV Patient AM HPI: 81 yo F p/w hemoptysis x 1 month LLL lesion on CXR, not responsive to Abx 35 pack-year
Diagnostic challenge: Sclerosing Hemangioma of the Lung. Department of Medicine, Division of Pulmonary and Critical Care, Lincoln Medical and
 Diagnostic challenge: Sclerosing Hemangioma of the Lung. S. Arias M.D, R. Loganathan M.D, FCCP Department of Medicine, Division of Pulmonary and Critical Care, Lincoln Medical and Mental Health Center/Weill
Diagnostic challenge: Sclerosing Hemangioma of the Lung. S. Arias M.D, R. Loganathan M.D, FCCP Department of Medicine, Division of Pulmonary and Critical Care, Lincoln Medical and Mental Health Center/Weill
New Horizons in the Imaging of the Lung
 New Horizons in the Imaging of the Lung Postprocessing. How to do it and when do we need it? Peter M.A. van Ooijen, MSc, PhD Principal Investigator, Radiology, UMCG Discipline Leader Medical Imaging Informatics
New Horizons in the Imaging of the Lung Postprocessing. How to do it and when do we need it? Peter M.A. van Ooijen, MSc, PhD Principal Investigator, Radiology, UMCG Discipline Leader Medical Imaging Informatics