SCBT-MR 2015 Incidentaloma on Chest CT
|
|
|
- Godwin Dixon
- 5 years ago
- Views:
Transcription


1 SCBT-MR 2015 Incidentaloma on Chest CT Reginald F. Munden MD, DMD, MBA I have no conflicts of interest to report
2 Incidentaloma Pulmonary Nodule Mediastinal Lymph Node Coronary Artery Calcium
3 Incidental Nodule How big is the problem? Jacobs 2008 Retrospective review of 11 publications: CAC (7) and lung cancer screening (4) Clinically significant findings (required F/U) 3% to 41% 7.7% of CAD and 14.2% of Lung Cancer Screening studies required F/U Hall pulmonary CTAs from ED at UNC Pulmonary embolism 9% 24% incidental finding other than pe 13% pulmonary nodule (of which as per guidelines 96% needed follow-up) 9% - adenopathy Swensen Mayo Lung Cancer Screening 69% - 1 or more positive findings in chest or abdomen after 3 years Jacobs. JCAT 2008; Hall. Arch Int Med 2009; Swensen. Radiology, 2003
4 Incidental Findings Don t Touch
5 Classically Benign
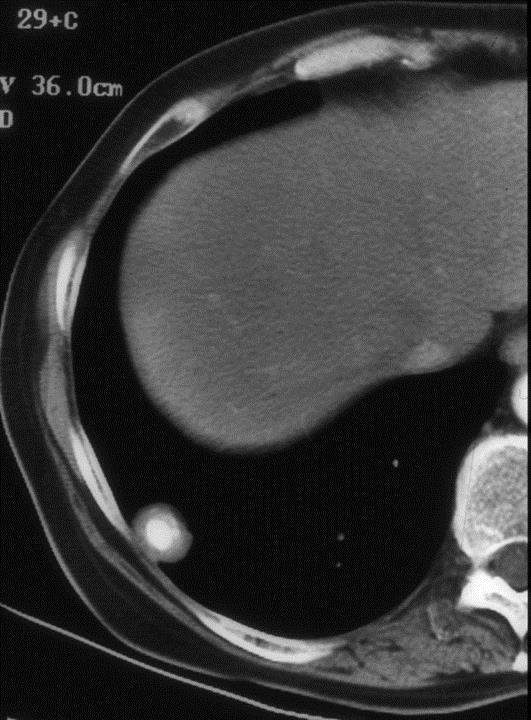
6 Benign Calcifications


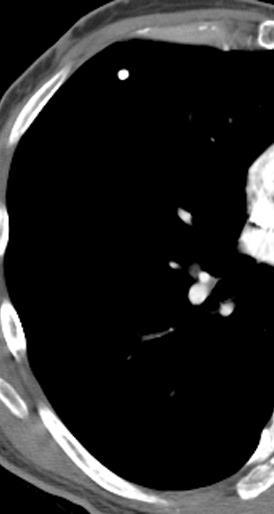
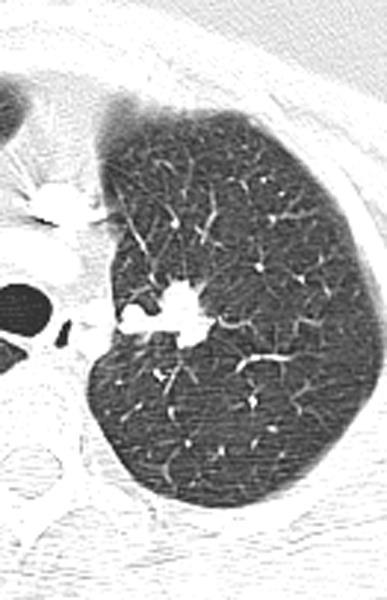
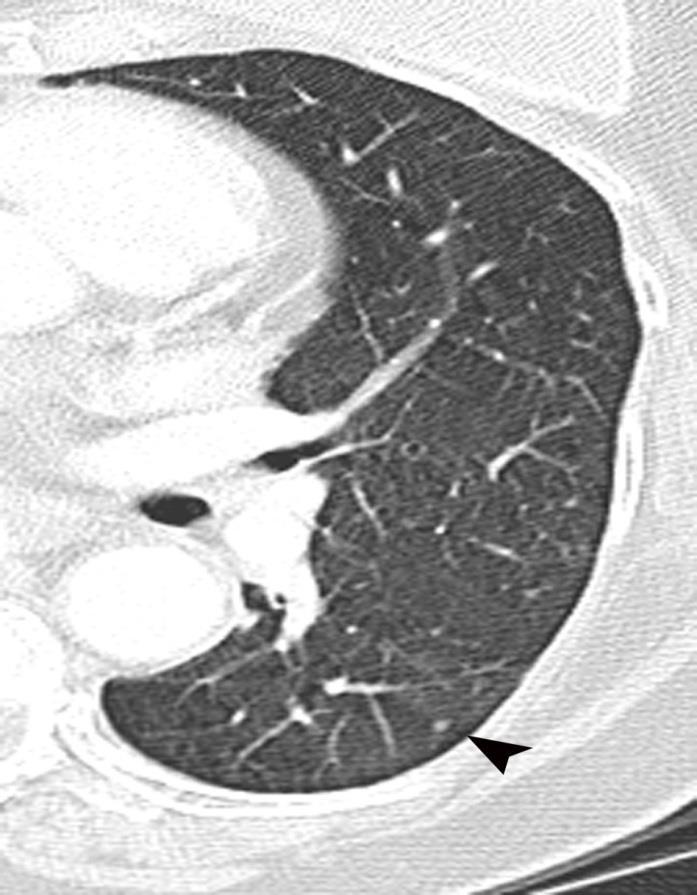
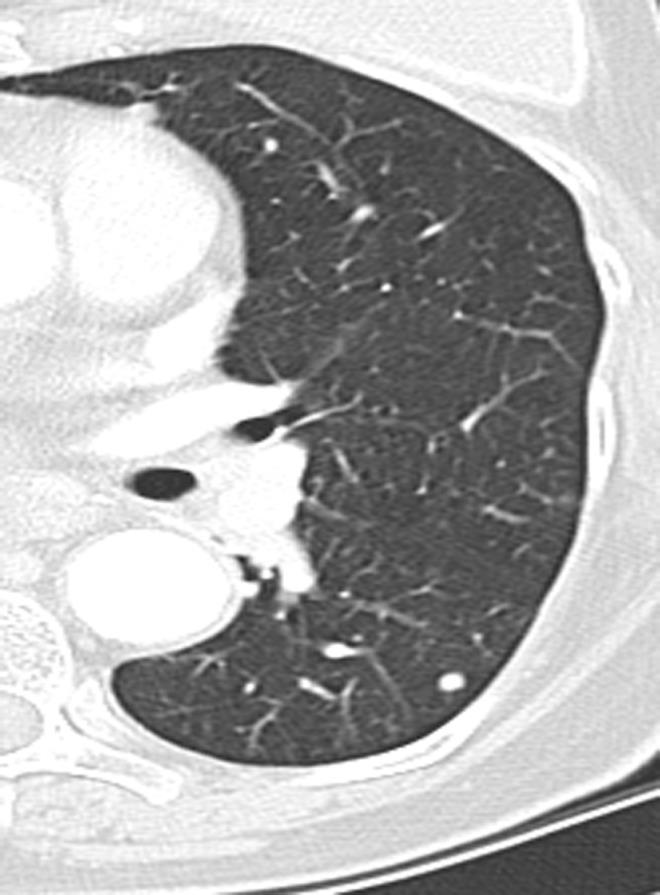
7 Perifissural lymph node Lung CA screen population 28% NCN adjacent to fissure 0% - became CA Ahn et al. Radiology. 2010
8 Incidental Findings Touch! Suspicious/Malignant

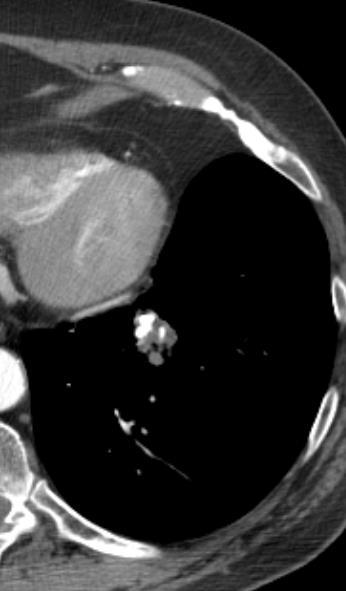
9 Worrisome Calcifications

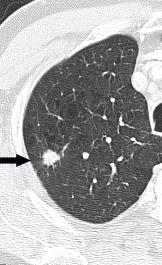
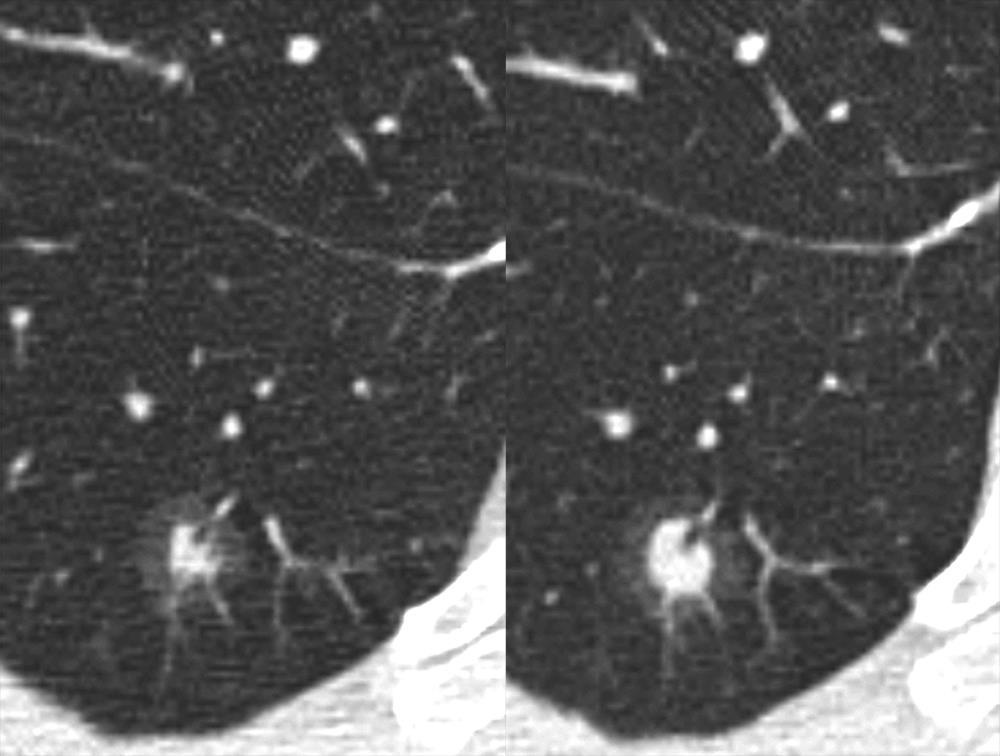
10 Edge Characteristics

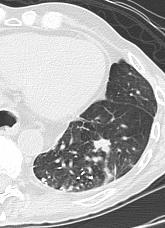
11 Lung Cancer/ TB?
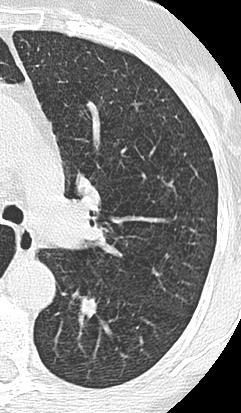
12 Incidental Findings Touch? Indeterminate
13 Indeterminate Solid Nodule What Next?
14 Fleischner Criteria Nodule size Low- risk High risk < 4mm No follow-up 12 months > 4-6 mm 12 months initial 6-12 months then months > 6-8mm initial 6-12 initial 3-6 months then , final 24 > 8mm 3, 9, and 24 Same as for low risk dynamic,pet,bx MacMahon et al. Radiology 237: , 2005

15 What next? PET/CT OR 8 weeks
16 Fleischner NOT for Oncology Patients
17 ACR LungRADS - Solid Nodules Category Category Descriptor Category Findings Fleischner Management Probability of Malignancy Negative Benign Appearance or Behavior Probably benign Suspicious No nodules and definitely benign nodules Nodules with a very low likelihood of becoming a clinically active cancer due to lack of size or growth Probably benign finding(s) short term follow up suggested; includes nodules with a low likelihood of becoming a clinically active cancer Findings for which additional diagnostic testing and/or tissue sampling is recommended A 4B 4x No lung nodules Nodule(s) with specific calcifications: complete, central, popcorn, concentric rings and fat containing nodules Solid nodule(s): < 6 mm New < 4 mm Category 3 or 4 nodules unchanged for > 3 months Solid nodule(s): > 6 mm to < 8 mm at baseline OR new 4 mm to < 6 mm Non solid nodule(s) (GGN) > 20 mm on baseline CT or new Solid nodule(s): 8 to < 15 mm at baseline OR growing < 8 mm OR new 6 to < 8 mm Solid nodule(s) 15 mm OR new or growing, and 8 mm Category 3 or 4 nodules with additional features or imaging findings that increases the suspicion of malignancy < 4 mm Continue annual screening with LDCT in 12 months < 1% > 4 mm 6 mm 6 month LDCT 1-2% > 6mm 8mm Initial 3-6 month CT Chest CT with or without contrast; PET/CT and/or tissue sampling depending on the *probability of malignancy and comorbidities; 8mm 3,9,24 CT, PET, PET/CT may be used when there is or bx a 8 mm solid component. > 15%

18 What next? Incidental Solid Nodule
19 Incidental Solid Nodule

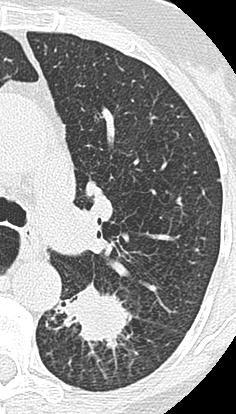
20 Incidental Non Solid Nodule What now?
21 Pulmonary Nodule: Subsolid Solitary Lesion Management GGO < 5-mm No follow-up > 5 mm Initial at 3 months (then annual for 3 or more years) Part solid Initial at 3 months. If persistent and solid component < 5 mm, then yearly. If solid > 5 mm, then biopsy/resect Multiple lesions GGO < 5mm Follow up 2 4 years > 5mm w/o Initial at 3 months, then annual for minimum 3 years dominant lesion with dominant Initial 3 months, if persistent then biopsy, especially if solid > 5mm Naidich. Radiology December, 2013
22
23 ACR LungRADS - Non Solid Category Category Descriptor Category Findings [Fleischner] Management Probability of Malignancy Nodules with a very low Benign likelihood of becoming a Appearance clinically active cancer or Behavior due to lack of size or growth Probably Benign Probably benign finding(s) short term follow up suggested; includes nodules with a low likelihood of becoming a clinically active cancer 2 3 Part solid nodule(s): < 6 mm total diameter on baseline screening Non solid nodules(s) (GGN ): < 20 mm OR > 20 mm and unchanged or slowly growing Part solid nodule(s): OR > 6 mm total diameter with solid component < 6mm new < 6mm total diameter Non solid nodule(s) (GGN) > 20 mm on baseline CT or new < 5 mm Continue annual screening with LDCT in 12 months < 1% Suspicious Findings for which additional diagnostic testing and/or tissue sampling is recommended 4A 4B Part-solid nodule(s): GGO > 5 mm Any PSN initial at 6 mm with solid component 6 mm to < 8 mm OR 3 months; If persistent and with a new or growing < 4 mm solid component solid < 5 mm, then yearly Part solid nodule(s) with a solid component 8 mm OR If solid > 5 mm then biopsy 3 month LDCT; PET/CT may be used when there is a 8 mm solid component 6 month LDCT Chest CT with or without contrast; PET/CT and/or tissue sampling depending on the *probability of malignancy and comorbidities; 5-15% > 15% a new or growing 4 mm solid component PET/CT may be used when there is a 8 mm solid component
 4B (PSN")
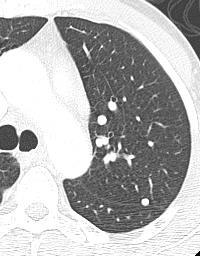
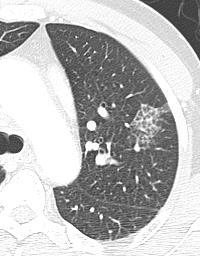
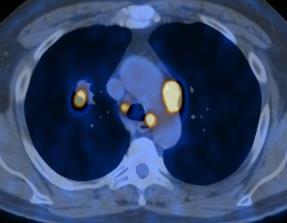
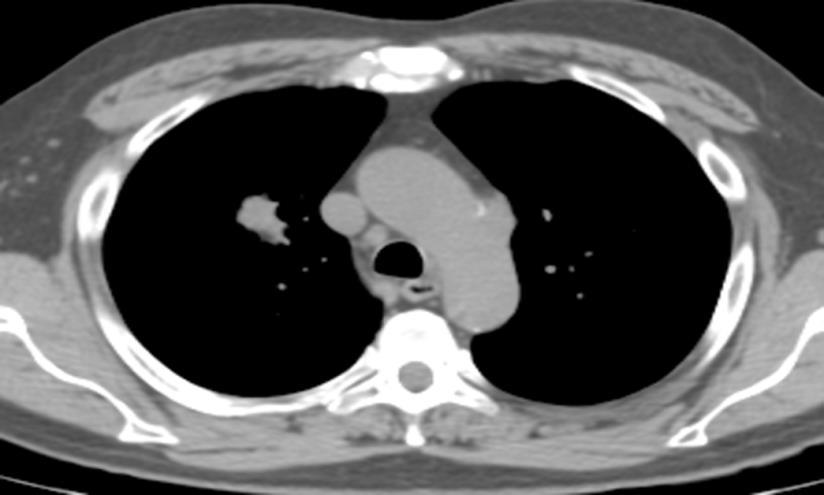
24 Pulmonary Nodule: Subsolid Category: 2 (GGN < 20mm) 4B (PSN Solid > 8mm)

25 Pulmonary Nodule: Subsolid
26 Incidental Nodule Review 1000 CTA chest CTs: Intermountain Health Care Rate of incidental nodule = 9.9% requiring follow-up Rate of appropriate follow-up when nodule noted 29% underwent recommended follow-up; 0% when mentioned in findings of report only Affect of radiology report: 68% reports had nodule follow-up recommendation 20 % in impression; 12% in findings only When in impression with specific recommendations 29% adherence When in findings 0% adherence Blagev. JACR, 2014
27 Incidental Nodule: Conclusion Incidental Nodules are not rare Management Most important - compare to prior studies Recommendations in the Impression For non-oncology patients Fleischner - solid nodule Fleischner - GGO ACR Incidental Chest White Paper - in development Oncology patients 3 month short term follow-up Lung Cancer Screening ACR LungRADS
28 Incidental Mediastinal Lymphadenopathy How big is the problem? Reported: % Variety of CAC and lung CA screening CTs Jacobs, 2008 Retrospective review of 11 CAD (7) and lung cancer screening (4) published studies Lymphadenopathy: 1 6% of studies Hall, CTAs for pulmonary embolus Positive = > 1cm node not associated with pneumonia; any > 3cm node; multiple nodes Mediastinal 29%; hilar 7% New adenopathy 9% of cases Thymoma SEER data = incidence 0.15 cases in 100, % of all thymic neoplasms; 0.2% of all malignancies Marom ; Engles,. Int J Cancer 2003
29 Incidental Mediastinal Lymphadenopathy Stigt, 2011 Patients with at least one incidental > 10 mm lymph node N = 83; 10mm - > 30mm; EUS or EBUS Results: 64 also hilar nodes Lymphocytes 55; sarcoid 18; granuloma 1; cyst 1; mets 1; inadequate - 7 Multiplicity, small size, coexistence with hilar lymphadenopathy Incidental lymph nodes mainly manifestation of reactive inflammation Stigt et al. JTO, 2011
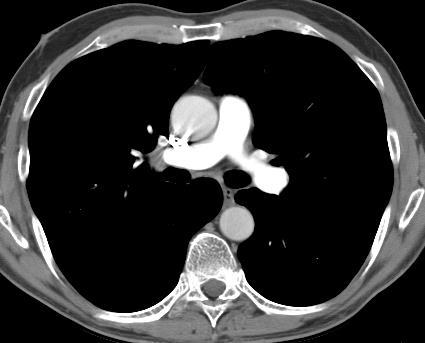

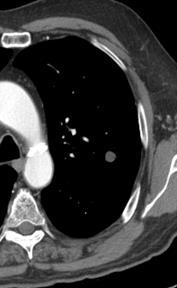
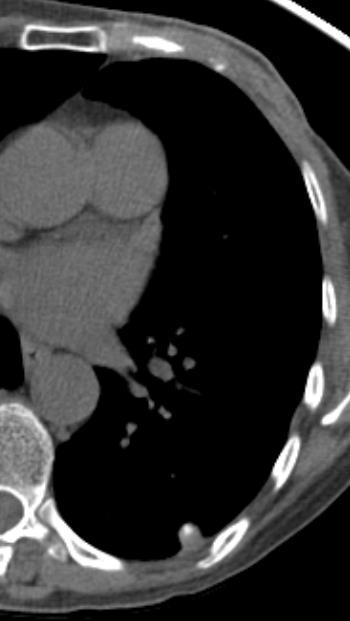
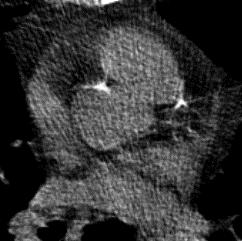
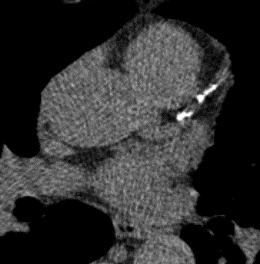
30 Mediastinal Lymph Nodes
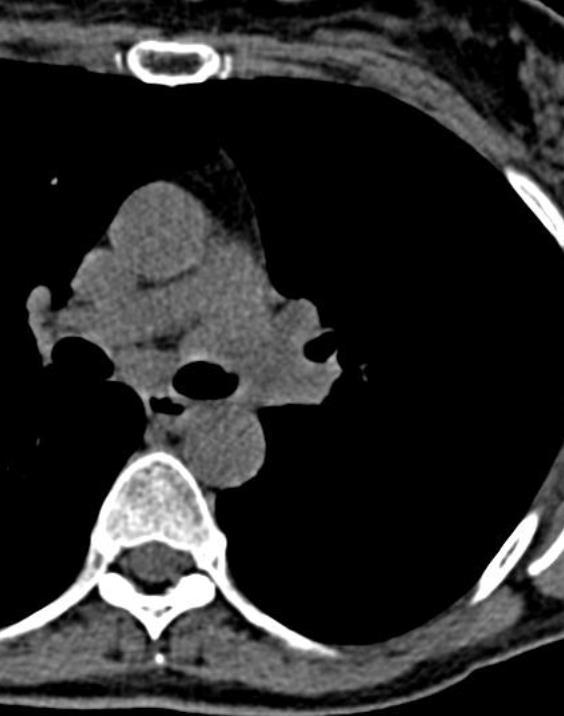
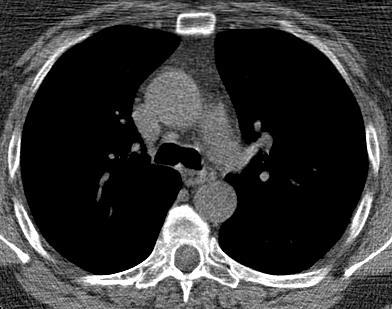
31 Mediastinal Lymph Nodes
32 Accuracy: CT 62-88% MR 50-82% PET 81-96% Staging - Lymph Nodes Webb et al. Radiology, 1991; Dietlein et al. Eur J Nucl Med, 2000; Steinert et al. Radiology, 1997
33 PET/CT (CT) NSCLC - Lymph Nodes Author Journal Year Sens Spec Accur Yi AJR (65) 100 (89) 90 (83) Kim Rad Antoch Rad (70) 94 (59) 93 (63) Birim ATS (70) 90 (70)

34 Lymph Nodes: PET/CT
35 Incidental Mediastinal Lymphadenopathy Conclusions: Size criteria: Not ideal, but the only reference In oncology patients Consider the malignancy Lung - Revised 8 th edition TNM - # nodes Esophageal, mesothelioma, lymphoma Testicular, Renal, Breast, Melanoma In screening Not uncommon reactive nodes In non-oncological patients Majority can be ignored size > 10 cm
36 Incidental Coronary Artery Calcification How big is the problem? Fluoroscopy 1 (for cardiac investigations) - 31% UK chest CTs - 26% of males, 15.6% of females; none in patients < 40 yrs old Prospective Army Coronary Calcium (PACC) year old: prevalence 17.3% 2009 Turkey thoracic CT, (31-92 yrs old; 72 male, 41 female) CAC = 33% Consecutive CTAs CAC detected on 46% 1. Eggan Circulation, 1965; 2. Callaway BJR, 1997; 3. Lee. US Army Research 2003; 4. Kihckesmez, MMJ 2009; 5. Foley. BMC Research News, 2010
37 Incidental Coronary Artery Calcification NLST: NLST (from 3856 death certificates) Cardiovascular disease 956 deaths [486 in CT group, 470 CXR group] Lung cancer deaths [427 in CT group, 503 in CXR group] NLST CAC study Agatston 1 100, HR 1.27; mild HR 2.09 Agatston 101-1,000, HR 3.57, moderate HR 3.86 Agatston > 1000, HR 6.63, heavy HR 6.95 Aberle & NLST Team, NEJM; Chiles. Radiology, In press


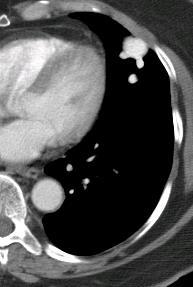
38 CAC Mild

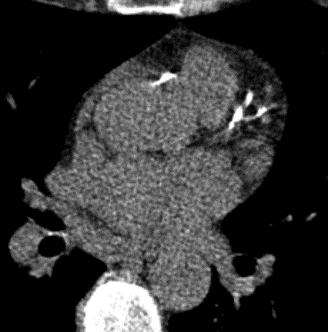
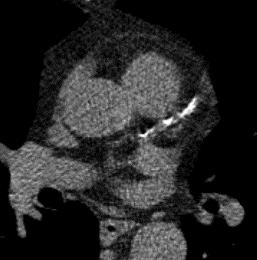
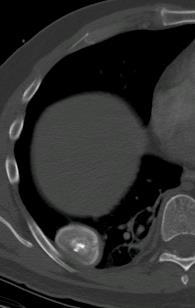
39 CAC Moderate

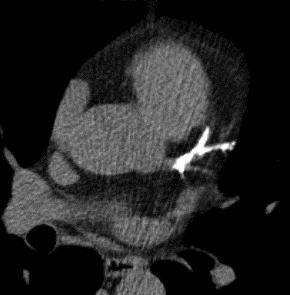
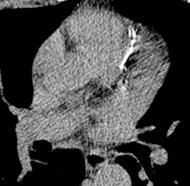
40 CAC Heavy
41 Incidental Coronary Artery Calcification Conclusions: Numerous studies indicate CAC should be reported NLST Report at least visual score mild, moderate, heavy
42 Thoracic Incidentaloma Thank You
SCBT-MR 2015 LungRADS : Basics
 SCBT-MR 2015 LungRADS : Basics Reginald F. Munden MD, DMD, MBA I have no conflicts of interest to report National Lung Cancer Screening Trial 20% lung cancer mortality reduction 6.9% all cause mortality
SCBT-MR 2015 LungRADS : Basics Reginald F. Munden MD, DMD, MBA I have no conflicts of interest to report National Lung Cancer Screening Trial 20% lung cancer mortality reduction 6.9% all cause mortality
SCBT-MR 2016 Lung Cancer Screening in Practice: State of the Art
 SCBT-MR 2016 Lung Cancer Screening in Practice: State of the Art Reginald F. Munden MD, DMD, MBA I have no conflicts of interest to report National Lung Cancer Screening Trial 20% lung cancer mortality
SCBT-MR 2016 Lung Cancer Screening in Practice: State of the Art Reginald F. Munden MD, DMD, MBA I have no conflicts of interest to report National Lung Cancer Screening Trial 20% lung cancer mortality
PULMONARY NODULES AND MASSES : DIAGNOSTIC APPROACH AND NEW MANAGEMENT GUIDELINES. https://tinyurl.com/hmpn2018
 PULMONARY NODULES AND MASSES : DIAGNOSTIC APPROACH AND NEW MANAGEMENT GUIDELINES Heber MacMahon MB, BCh Department of Radiology The University of Chicago https://tinyurl.com/hmpn2018 Disclosures Consultant
PULMONARY NODULES AND MASSES : DIAGNOSTIC APPROACH AND NEW MANAGEMENT GUIDELINES Heber MacMahon MB, BCh Department of Radiology The University of Chicago https://tinyurl.com/hmpn2018 Disclosures Consultant
GUIDELINES FOR PULMONARY NODULE MANAGEMENT : RECENT CHANGES AND UPDATES
 Venice 2017 GUIDELINES FOR PULMONARY NODULE MANAGEMENT : RECENT CHANGES AND UPDATES Heber MacMahon MB, BCh Department of Radiology The University of Chicago Disclosures Consultant for Riverain Medical
Venice 2017 GUIDELINES FOR PULMONARY NODULE MANAGEMENT : RECENT CHANGES AND UPDATES Heber MacMahon MB, BCh Department of Radiology The University of Chicago Disclosures Consultant for Riverain Medical
Learning Objectives. 1. Identify which patients meet criteria for annual lung cancer screening
 Disclosure I, Taylor Rowlett, DO NOT have a financial interest /arrangement or affiliation with one or more organizations that could be perceived as a real or apparent conflict of interest in the context
Disclosure I, Taylor Rowlett, DO NOT have a financial interest /arrangement or affiliation with one or more organizations that could be perceived as a real or apparent conflict of interest in the context
Pulmonary Nodules & Masses
 Pulmonary Nodules & Masses A Diagnostic Approach Heber MacMahon The University of Chicago Department of Radiology Disclosure Information Consultant for Riverain Technology Minor equity in Hologic Royalties
Pulmonary Nodules & Masses A Diagnostic Approach Heber MacMahon The University of Chicago Department of Radiology Disclosure Information Consultant for Riverain Technology Minor equity in Hologic Royalties
Current Approach to Screening for Lung Cancer. James R Jett M.D.
 Current Approach to Screening for Lung Cancer James R Jett M.D. Potential Conflicts of Interest I am Chief Medical Officer for Oncimmune Ltd (Biomarkers of Cancer) Co-Editor of Lung Cancer Section of UP-TO-DATE
Current Approach to Screening for Lung Cancer James R Jett M.D. Potential Conflicts of Interest I am Chief Medical Officer for Oncimmune Ltd (Biomarkers of Cancer) Co-Editor of Lung Cancer Section of UP-TO-DATE
The Maine Lung Cancer Coalition. Working Together to Reduce Lung Cancer in Maine
 The Maine Lung Cancer Coalition Working Together to Reduce Lung Cancer in Maine funding Maine Lung Cancer Coalition (MLCC) Webinar Lung Cancer Screening: Following Up On Abnormal Low Dose CT Scans with
The Maine Lung Cancer Coalition Working Together to Reduce Lung Cancer in Maine funding Maine Lung Cancer Coalition (MLCC) Webinar Lung Cancer Screening: Following Up On Abnormal Low Dose CT Scans with
Approach to Pulmonary Nodules
 Approach to Pulmonary Nodules Edwin Jackson, Jr., DO Assistant Professor-Clinical Director, James Early Detection Clinic Department of Internal Medicine Division of Pulmonary, Allergy, Critical Care and
Approach to Pulmonary Nodules Edwin Jackson, Jr., DO Assistant Professor-Clinical Director, James Early Detection Clinic Department of Internal Medicine Division of Pulmonary, Allergy, Critical Care and
Screening Programs background and clinical implementation. Denise R. Aberle, MD Professor of Radiology and Engineering
 Screening Programs background and clinical implementation Denise R. Aberle, MD Professor of Radiology and Engineering disclosures I have no disclosures. I have no conflicts of interest relevant to this
Screening Programs background and clinical implementation Denise R. Aberle, MD Professor of Radiology and Engineering disclosures I have no disclosures. I have no conflicts of interest relevant to this
PULMONARY NODULES DETECTED INCIDENTALLY OR BY SCREENING: LOTS OF GUIDELINES BUT WHERE IS THE EVIDENCE?
 PULMONARY NODULES DETECTED INCIDENTALLY OR BY SCREENING: LOTS OF GUIDELINES BUT WHERE IS THE EVIDENCE? MICHAEL K. GOULD, MD SENIOR RESEARCH SCIENTIST DIRECTOR FOR HEALTH SCIENCES & IMPLEMENTATION SCIENCE
PULMONARY NODULES DETECTED INCIDENTALLY OR BY SCREENING: LOTS OF GUIDELINES BUT WHERE IS THE EVIDENCE? MICHAEL K. GOULD, MD SENIOR RESEARCH SCIENTIST DIRECTOR FOR HEALTH SCIENCES & IMPLEMENTATION SCIENCE
LUNG NODULES: MODERN MANAGEMENT STRATEGIES
 Department of Radiology LUNG NODULES: MODERN MANAGEMENT STRATEGIES Christian J. Herold M.D. Department of Biomedical Imaging and Image-guided Therapy Medical University of Vienna Vienna, Austria Pulmonary
Department of Radiology LUNG NODULES: MODERN MANAGEMENT STRATEGIES Christian J. Herold M.D. Department of Biomedical Imaging and Image-guided Therapy Medical University of Vienna Vienna, Austria Pulmonary
Pulmonary Nodules. Michael Morris, MD
 Pulmonary Nodules Michael Morris, MD Case 45 year old healthy male Smokes socially Normal physical exam Pre-employment screening remote +PPD screening CXR nodular opacity Case 45 year old healthy male
Pulmonary Nodules Michael Morris, MD Case 45 year old healthy male Smokes socially Normal physical exam Pre-employment screening remote +PPD screening CXR nodular opacity Case 45 year old healthy male
Evidence based approach to incidentally detected subsolid pulmonary nodule. DM SEMINAR July 27, 2018 Harshith Rao
 Evidence based approach to incidentally detected subsolid pulmonary nodule DM SEMINAR July 27, 2018 Harshith Rao Outline Definitions Etiologies Risk evaluation Clinical features Radiology Approach Modifications:
Evidence based approach to incidentally detected subsolid pulmonary nodule DM SEMINAR July 27, 2018 Harshith Rao Outline Definitions Etiologies Risk evaluation Clinical features Radiology Approach Modifications:
Lung Cancer Screening: To Screen or Not to Screen?
 Lung Cancer Screening: To Screen or Not to Screen? Lorriana Leard, MD Co-Director of UCSF Lung Cancer Screening Program Vice Chief of Clinical Activities UCSF Pulmonary, Critical Care, Allergy & Sleep
Lung Cancer Screening: To Screen or Not to Screen? Lorriana Leard, MD Co-Director of UCSF Lung Cancer Screening Program Vice Chief of Clinical Activities UCSF Pulmonary, Critical Care, Allergy & Sleep
American College of Radiology ACR Appropriateness Criteria
 American College of Radiology ACR Criteria Radiologic Management of Thoracic Nodules and Masses Variant 1: Middle-aged patient (35 60 years old) with an incidental 1.5-cm lung nodule. The lesion was smooth.
American College of Radiology ACR Criteria Radiologic Management of Thoracic Nodules and Masses Variant 1: Middle-aged patient (35 60 years old) with an incidental 1.5-cm lung nodule. The lesion was smooth.
Chest Radiology Interpretation: Findings of Tuberculosis
 Chest Radiology Interpretation: Findings of Tuberculosis Get out your laptops, smart phones or other devices pollev.com/chestradiology Case #1 1 Plombage Pneumonia Cancer 2 Reading the TB CXR Be systematic!
Chest Radiology Interpretation: Findings of Tuberculosis Get out your laptops, smart phones or other devices pollev.com/chestradiology Case #1 1 Plombage Pneumonia Cancer 2 Reading the TB CXR Be systematic!
CT Screening for Lung Cancer for High Risk Patients
 CT Screening for Lung Cancer for High Risk Patients The recently published National Lung Cancer Screening Trial (NLST) showed that low-dose CT screening for lung cancer reduces mortality in high-risk patients
CT Screening for Lung Cancer for High Risk Patients The recently published National Lung Cancer Screening Trial (NLST) showed that low-dose CT screening for lung cancer reduces mortality in high-risk patients
Published Pulmonary Nodule Guidelines A Synthesis
 Published Pulmonary Nodule Guidelines A Synthesis Dr A Devaraj Royal Brompton Hospital London 4/28/2015 1 And very soon to be published Published ^ Pulmonary Nodule Guidelines A Synthesis Dr A Devaraj
Published Pulmonary Nodule Guidelines A Synthesis Dr A Devaraj Royal Brompton Hospital London 4/28/2015 1 And very soon to be published Published ^ Pulmonary Nodule Guidelines A Synthesis Dr A Devaraj
DENOMINATOR: All final reports for CT imaging studies with a finding of an incidental pulmonary nodule for patients aged 35 years and older
 Quality ID #364: Optimizing Patient Exposure to Ionizing Radiation: Appropriateness: Follow-up CT Imaging for Incidentally Detected Pulmonary Nodules According to Recommended Guidelines National Quality
Quality ID #364: Optimizing Patient Exposure to Ionizing Radiation: Appropriateness: Follow-up CT Imaging for Incidentally Detected Pulmonary Nodules According to Recommended Guidelines National Quality
Positron Emission Tomography in Lung Cancer
 May 19, 2003 Positron Emission Tomography in Lung Cancer Andrew Wang, HMS III Patient DD 53 y/o gentleman presented with worsening dyspnea on exertion for the past two months 30 pack-year smoking Hx and
May 19, 2003 Positron Emission Tomography in Lung Cancer Andrew Wang, HMS III Patient DD 53 y/o gentleman presented with worsening dyspnea on exertion for the past two months 30 pack-year smoking Hx and
objectives Pitfalls and Pearls in PET/CT imaging Kevin Robinson, DO Assistant Professor Department of Radiology Michigan State University
 objectives Pitfalls and Pearls in PET/CT imaging Kevin Robinson, DO Assistant Professor Department of Radiology Michigan State University To determine the regions of physiologic activity To understand
objectives Pitfalls and Pearls in PET/CT imaging Kevin Robinson, DO Assistant Professor Department of Radiology Michigan State University To determine the regions of physiologic activity To understand
Lung Cancer Screening
 Lung Cancer Screening Steven Leh, MD, FCCP Diplomat of the American Association for Bronchology and Interventional Pulmonology Aurora Medical Group Pulmonary and Sleep Medicine February 10, 2018 Disclosures
Lung Cancer Screening Steven Leh, MD, FCCP Diplomat of the American Association for Bronchology and Interventional Pulmonology Aurora Medical Group Pulmonary and Sleep Medicine February 10, 2018 Disclosures
2018 OPTIONS FOR INDIVIDUAL MEASURES: REGISTRY ONLY. MEASURE TYPE: Process
 Quality ID #364: Optimizing Patient Exposure to Ionizing Radiation: Appropriateness: Follow-up CT Imaging for Incidentally Detected Pulmonary Nodules According to Recommended Guidelines National Quality
Quality ID #364: Optimizing Patient Exposure to Ionizing Radiation: Appropriateness: Follow-up CT Imaging for Incidentally Detected Pulmonary Nodules According to Recommended Guidelines National Quality
THE BENEFITS OF BIG DATA
 THE BENEFITS OF BIG DATA Disclosures I am a named inventor on a number of patents and patent applications relating to the evaluation of pulmonary nodules on CT scans of the chest which are owned by Cornell
THE BENEFITS OF BIG DATA Disclosures I am a named inventor on a number of patents and patent applications relating to the evaluation of pulmonary nodules on CT scans of the chest which are owned by Cornell
Lung Cancer Diagnosis for Primary Care
 Lung Cancer Diagnosis for Primary Care Daniel Nader, DO, FCCP Cancer Treatment Center of America Case 1 In which of the following situations would the U.S. Preventive Services Task Force (USPSTF) recommend
Lung Cancer Diagnosis for Primary Care Daniel Nader, DO, FCCP Cancer Treatment Center of America Case 1 In which of the following situations would the U.S. Preventive Services Task Force (USPSTF) recommend
Abstract Submission Form
 Abstract Submission Form All abstracts must be submitted to the AOCR by September 15 th. All information included must be the original work of the author(s) and be in typed form. Incomplete or handwritten
Abstract Submission Form All abstracts must be submitted to the AOCR by September 15 th. All information included must be the original work of the author(s) and be in typed form. Incomplete or handwritten
Early Detection of Lung Cancer. Amsterdam March 5 th 2010
 Early Detection of Lung Cancer Amsterdam March 5 th 2010 Rob J van Klaveren, MD, PhD Dept. of Pulmonology Erasmus MC Rotterdam, the Netherlands Early Detection and Screening - Questions to be addressed
Early Detection of Lung Cancer Amsterdam March 5 th 2010 Rob J van Klaveren, MD, PhD Dept. of Pulmonology Erasmus MC Rotterdam, the Netherlands Early Detection and Screening - Questions to be addressed
Respiratory Interactive Session. Elaine Borg
 Respiratory Interactive Session Elaine Borg Case 1 Respiratory Cytology 55 year old gentleman Anterior mediastinal mass EBUS FNA Case 1 Respiratory Cytology 55 year old gentleman with anterior mediastinal
Respiratory Interactive Session Elaine Borg Case 1 Respiratory Cytology 55 year old gentleman Anterior mediastinal mass EBUS FNA Case 1 Respiratory Cytology 55 year old gentleman with anterior mediastinal
Lung Cancer Screening: To screen or not to screen?
 Lung Cancer Screening: To screen or not to screen? Dan J. Raz, M.D. Co Director, Lung Cancer Screening Program Co Director, LungCancer and Thoracic OncologyProgram Assistant Professor, Thoracic Surgery
Lung Cancer Screening: To screen or not to screen? Dan J. Raz, M.D. Co Director, Lung Cancer Screening Program Co Director, LungCancer and Thoracic OncologyProgram Assistant Professor, Thoracic Surgery
MANAGEMENT RECOMMENDATIONS
 1 MANAGEMENT RECOMMENDATIONS 1. Adrenal masses!!!!!!! page 2 2. Liver Masses!!!!!!! page 3 3. Obstetric US Soft Markers for Aneuploidy!! pages 4-6 4. Ovarian and Adnexal Cysts!!!!! pages 7-10 5. Pancreatic
1 MANAGEMENT RECOMMENDATIONS 1. Adrenal masses!!!!!!! page 2 2. Liver Masses!!!!!!! page 3 3. Obstetric US Soft Markers for Aneuploidy!! pages 4-6 4. Ovarian and Adnexal Cysts!!!!! pages 7-10 5. Pancreatic
CLINICAL GUIDELINES. Lung-Cancer Screening Program Guidelines Robert Y. Kanterman, M.D. and Thomas J. Gilbert, M.D., M.P.P.
 CLINICAL GUIDELINES Lung-Cancer Screening Program Guidelines Robert Y. Kanterman, M.D. and Thomas J. Gilbert, M.D., M.P.P. 3/14/2015 Introduction: The purpose of a lung-cancer screening program is to detect
CLINICAL GUIDELINES Lung-Cancer Screening Program Guidelines Robert Y. Kanterman, M.D. and Thomas J. Gilbert, M.D., M.P.P. 3/14/2015 Introduction: The purpose of a lung-cancer screening program is to detect
OBJECTIVES. Solitary Solid Spiculated Nodule. What would you do next? Case Based Discussion: State of the Art Management of Lung Nodules.
 Organ Imaging : September 25 2015 OBJECTIVES Case Based Discussion: State of the Art Management of Lung Nodules Dr. Elsie T. Nguyen Dr. Kazuhiro Yasufuku 1. To review guidelines for follow up and management
Organ Imaging : September 25 2015 OBJECTIVES Case Based Discussion: State of the Art Management of Lung Nodules Dr. Elsie T. Nguyen Dr. Kazuhiro Yasufuku 1. To review guidelines for follow up and management
Deppen S, et al. Annals of Thoracic Surgery 2011;92:
 Deppen S, et al. Annals of Thoracic Surgery 2011;92:428-33. http://www.nationmaster.com/graph/ mor_his-mortality-histoplasmosis http://www.humirarems.com/brochure.aspx Baddley, John W., et al. Emerging
Deppen S, et al. Annals of Thoracic Surgery 2011;92:428-33. http://www.nationmaster.com/graph/ mor_his-mortality-histoplasmosis http://www.humirarems.com/brochure.aspx Baddley, John W., et al. Emerging
Lung Cancer screening :
 Lung Cancer screening : Pro-Contra SAMO interdisciplinary workshop on chest tumors 27 and 28 january 2017 Prof L.P.Nicod Sevice de pneumologie CHUV-Lausanne -CH Lung Cancer How big is the problem? Epidemiology
Lung Cancer screening : Pro-Contra SAMO interdisciplinary workshop on chest tumors 27 and 28 january 2017 Prof L.P.Nicod Sevice de pneumologie CHUV-Lausanne -CH Lung Cancer How big is the problem? Epidemiology
Adam J. Hansen, MD UHC Thoracic Surgery
 Adam J. Hansen, MD UHC Thoracic Surgery Sometimes seen on Chest X-ray (CXR) Common incidental findings on computed tomography (CT) chest and abdomen done for other reasons Most lung cancers discovered
Adam J. Hansen, MD UHC Thoracic Surgery Sometimes seen on Chest X-ray (CXR) Common incidental findings on computed tomography (CT) chest and abdomen done for other reasons Most lung cancers discovered
Pulmonary Nodules: When to worry, when to chill. Douglas Arenberg Associate Professor Pulmonary & Critical Care
 Pulmonary Nodules: When to worry, when to chill Douglas Arenberg Associate Professor Pulmonary & Critical Care Disclosure MDCH Grant Funds to improve tobacco cessation service in the Michigan Medicine
Pulmonary Nodules: When to worry, when to chill Douglas Arenberg Associate Professor Pulmonary & Critical Care Disclosure MDCH Grant Funds to improve tobacco cessation service in the Michigan Medicine
Los Angeles Radiological Society 62 nd Annual Midwinter Radiology Conference January 31, 2010
 Los Angeles Radiological Society 62 nd Annual Midwinter Radiology Conference January 31, 2010 Self Assessment Module on Nuclear Medicine and PET/CT Case Review FDG PET/CT IN LYMPHOMA AND MELANOMA Submitted
Los Angeles Radiological Society 62 nd Annual Midwinter Radiology Conference January 31, 2010 Self Assessment Module on Nuclear Medicine and PET/CT Case Review FDG PET/CT IN LYMPHOMA AND MELANOMA Submitted
Radiological staging of lung cancer. Shukri Loutfi,MD,FRCR Consultant Thoracic Radiologist KAMC-Riyadh
 Radiological staging of lung cancer Shukri Loutfi,MD,FRCR Consultant Thoracic Radiologist KAMC-Riyadh Bronchogenic Carcinoma Accounts for 14% of new cancer diagnoses in 2012. Estimated to kill ~150,000
Radiological staging of lung cancer Shukri Loutfi,MD,FRCR Consultant Thoracic Radiologist KAMC-Riyadh Bronchogenic Carcinoma Accounts for 14% of new cancer diagnoses in 2012. Estimated to kill ~150,000
Robert J. McKenna M.D. Chief, Thoracic Surgery Cedars Sinai Medical Center
 You Smoke, You Get Lung Cancer, You Die: Can Screening Change this Paradigm? Robert J. McKenna M.D. Chief, Thoracic Surgery Cedars Sinai Medical Center AATS Saturday 4/28/2012 Cancer Screening Cancer
You Smoke, You Get Lung Cancer, You Die: Can Screening Change this Paradigm? Robert J. McKenna M.D. Chief, Thoracic Surgery Cedars Sinai Medical Center AATS Saturday 4/28/2012 Cancer Screening Cancer
The Spectrum of Management of Pulmonary Ground Glass Nodules
 The Spectrum of Management of Pulmonary Ground Glass Nodules Stanley S Siegelman CT Society 10/26/2011 No financial disclosures. Noguchi M et al. Cancer 75: 2844-2852, 1995. 236 surgically resected peripheral
The Spectrum of Management of Pulmonary Ground Glass Nodules Stanley S Siegelman CT Society 10/26/2011 No financial disclosures. Noguchi M et al. Cancer 75: 2844-2852, 1995. 236 surgically resected peripheral
Example of lung screening
 Justification of the use of CT for individual health assessment of asymptomatic people How to obtain evidence for IHA - Example of lung screening Mathias Prokop, MD PhD Professor of Radiology Radboud University
Justification of the use of CT for individual health assessment of asymptomatic people How to obtain evidence for IHA - Example of lung screening Mathias Prokop, MD PhD Professor of Radiology Radboud University
Charles Mulligan, MD, FACS, FCCP 26 March 2015
 Charles Mulligan, MD, FACS, FCCP 26 March 2015 Review lung cancer statistics Review the risk factors Discuss presentation and staging Discuss treatment options and outcomes Discuss the status of screening
Charles Mulligan, MD, FACS, FCCP 26 March 2015 Review lung cancer statistics Review the risk factors Discuss presentation and staging Discuss treatment options and outcomes Discuss the status of screening
Lung Cancer Screening:
 Lung Cancer Screening: Maximizing Gain and Dealing with Pandora s Box Mark M. Fuster, MD Division of Pulmonary & Critical Care UCSD Department of Medicine & VA San Diego Healthcare Service San Diego, CA
Lung Cancer Screening: Maximizing Gain and Dealing with Pandora s Box Mark M. Fuster, MD Division of Pulmonary & Critical Care UCSD Department of Medicine & VA San Diego Healthcare Service San Diego, CA
Lung Screening: Do s and Don t s
 18th Annual Interna3onal Symposium on Mul3detector-Row CT June 20-23 2015 HyaH Regency San Franciscio Wednesday June 22 7.00 AM Lung Screening: Do s and Don t s Mathias Prokop, MD PhD Department of Radiology
18th Annual Interna3onal Symposium on Mul3detector-Row CT June 20-23 2015 HyaH Regency San Franciscio Wednesday June 22 7.00 AM Lung Screening: Do s and Don t s Mathias Prokop, MD PhD Department of Radiology
ESUR 2018, Sept. 13 th.-16 th., 2018 Barcelona, Spain
 ESUR 2018, Sept. 13 th.-16 th., 2018 Barcelona, Spain OUR APPROACH Incidental adrenal nodule/mass Isaac R Francis, M.B;B.S University of Michigan, Ann Arbor, Michigan Disclosures None (in memory) M Korobkin,
ESUR 2018, Sept. 13 th.-16 th., 2018 Barcelona, Spain OUR APPROACH Incidental adrenal nodule/mass Isaac R Francis, M.B;B.S University of Michigan, Ann Arbor, Michigan Disclosures None (in memory) M Korobkin,
Diagnosis and Staging of Non-Small Cell Lung Cancer Carlos Eduardo Oliveira Baleeiro, MD. November 18, 2017
 Diagnosis and Staging of Non-Small Cell Lung Cancer Carlos Eduardo Oliveira Baleeiro, MD November 18, 2017 Disclosures I do not have a financial interest/arrangement or affiliation with one or more organizations
Diagnosis and Staging of Non-Small Cell Lung Cancer Carlos Eduardo Oliveira Baleeiro, MD November 18, 2017 Disclosures I do not have a financial interest/arrangement or affiliation with one or more organizations
Use of Integrated PET CT in the Clinical Staging of Non Small Cell Lung Cancer
 November 2010 Use of Integrated PET CT in the Clinical Staging of Non Small Cell Lung Cancer Laura Myers, Harvard Medical School, Year III Clinical Presentation 79yo woman with cough productive of green
November 2010 Use of Integrated PET CT in the Clinical Staging of Non Small Cell Lung Cancer Laura Myers, Harvard Medical School, Year III Clinical Presentation 79yo woman with cough productive of green
PET/CT in lung cancer
 PET/CT in lung cancer Andrei Šamarin North Estonia Medical Centre 3 rd Baltic Congress of Radiology 08.10.2010 Imaging in lung cancer Why do we need PET/CT? CT is routine imaging modality for staging of
PET/CT in lung cancer Andrei Šamarin North Estonia Medical Centre 3 rd Baltic Congress of Radiology 08.10.2010 Imaging in lung cancer Why do we need PET/CT? CT is routine imaging modality for staging of
8/3/2016. Consultant for / research support from: Astellas Bayer Bracco GE Healthcare Guerbet Medrad Siemens Healthcare. Single Energy.
 U. Joseph Schoepf, MD Prof. (h.c.), FAHA, FSCBT-MR, FNASCI, FSCCT Professor of Radiology, Medicine, and Pediatrics Director, Division of Cardiovascular Imaging Consultant for / research support from: Astellas
U. Joseph Schoepf, MD Prof. (h.c.), FAHA, FSCBT-MR, FNASCI, FSCCT Professor of Radiology, Medicine, and Pediatrics Director, Division of Cardiovascular Imaging Consultant for / research support from: Astellas
What to Do with Small Lung Nodules Hanh Vu Nghiem, MD William Beaumont Hospital Royal Oak, Michigan
 What to Do with Small Lung Nodules Hanh Vu Nghiem, MD William Beaumont Hospital Royal Oak, Michigan Small Lung Nodules What to do with small lung nodules? We biopsy them when requested What are our accuracy
What to Do with Small Lung Nodules Hanh Vu Nghiem, MD William Beaumont Hospital Royal Oak, Michigan Small Lung Nodules What to do with small lung nodules? We biopsy them when requested What are our accuracy
Endobronchial Ultrasound in the Diagnosis & Staging of Lung Cancer
 Endobronchial Ultrasound in the Diagnosis & Staging of Lung Cancer Dr Richard Booton PhD FRCP Lead Lung Cancer Clinician, Consultant Respiratory Physician & Speciality Director Manchester University NHS
Endobronchial Ultrasound in the Diagnosis & Staging of Lung Cancer Dr Richard Booton PhD FRCP Lead Lung Cancer Clinician, Consultant Respiratory Physician & Speciality Director Manchester University NHS
Christine Argento, MD Interventional Pulmonology Emory University
 Christine Argento, MD Interventional Pulmonology Emory University Outline Lung Cancer Statistics Prior Studies for Lung Cancer Screening NLST Studies Following NLST Future Directions Lung Cancer American
Christine Argento, MD Interventional Pulmonology Emory University Outline Lung Cancer Statistics Prior Studies for Lung Cancer Screening NLST Studies Following NLST Future Directions Lung Cancer American
Assessing the lung and mediastinum in cancer-is tissue the issue? George Santis
 1 Assessing the lung and mediastinum in cancer-is tissue the issue? George Santis Optimal management of Cancer Histological diagnosis & accurate staging at presentation Molecular analysis of primary tumour
1 Assessing the lung and mediastinum in cancer-is tissue the issue? George Santis Optimal management of Cancer Histological diagnosis & accurate staging at presentation Molecular analysis of primary tumour
Right infrahilar nodule
 Right infrahilar nodule Search Infrahilar nodule Nov 9, 2015.. CT chest showed a right infrahilar mass 3.5 2.5 cm along with multiple bilateral lung nodules of size 9 to 11 mm. Bronchoscopy. Jun 13, 2015.
Right infrahilar nodule Search Infrahilar nodule Nov 9, 2015.. CT chest showed a right infrahilar mass 3.5 2.5 cm along with multiple bilateral lung nodules of size 9 to 11 mm. Bronchoscopy. Jun 13, 2015.
Lung. 10/24/13 Chest X-ray: 2.9 cm mass like density in the inferior lingular segment worrisome for neoplasm. Malignancy cannot be excluded.
 Lung Case Scenario 1 A 54 year white male presents with a recent abnormal CT of the chest. The patient has a history of melanoma, kidney, and prostate cancers. 10/24/13 Chest X-ray: 2.9 cm mass like density
Lung Case Scenario 1 A 54 year white male presents with a recent abnormal CT of the chest. The patient has a history of melanoma, kidney, and prostate cancers. 10/24/13 Chest X-ray: 2.9 cm mass like density
Objectives. Why? Why? Background 11/5/ % incurable disease at presentation Locally advanced disease Metastasis. 14% 5 year survival
 Objectives Appraise lung cancer screening trials results Review screening guidelines Lung Cancer Screening: Past, Present and Future Chi Wan Koo, MD Koo.chiwan@mayo.edu Discuss recommendations essential
Objectives Appraise lung cancer screening trials results Review screening guidelines Lung Cancer Screening: Past, Present and Future Chi Wan Koo, MD Koo.chiwan@mayo.edu Discuss recommendations essential
11/1/2014. Radiologic incidentalomas Ordering pitfalls Newer technology and applications
 Bilal Tahir, MD Gitasree Borthakur, MD Indiana University School of Medicine Department of Radiology & Imaging Sciences October 31, 2014 ACP 2014 Dr. V. Aaron Nuclear (vaaron@iupui.edu) Dr. S. Westphal
Bilal Tahir, MD Gitasree Borthakur, MD Indiana University School of Medicine Department of Radiology & Imaging Sciences October 31, 2014 ACP 2014 Dr. V. Aaron Nuclear (vaaron@iupui.edu) Dr. S. Westphal
The solitary pulmonary nodule: Assessing the success of predicting malignancy
 The solitary pulmonary nodule: Assessing the success of predicting malignancy Poster No.: C-0829 Congress: ECR 2010 Type: Scientific Exhibit Topic: Chest Authors: R. W. K. Lindsay, J. Foster, K. McManus;
The solitary pulmonary nodule: Assessing the success of predicting malignancy Poster No.: C-0829 Congress: ECR 2010 Type: Scientific Exhibit Topic: Chest Authors: R. W. K. Lindsay, J. Foster, K. McManus;
None
 2014 None rosemary clooney Cancer is one of the most common diseases in the developed world: 1 in 4 deaths are due to cancer 1 in 17 deaths are due to lung cancer Lung cancer is the most common
2014 None rosemary clooney Cancer is one of the most common diseases in the developed world: 1 in 4 deaths are due to cancer 1 in 17 deaths are due to lung cancer Lung cancer is the most common
Understanding the Diagnostic and Prognostic Role of Imaging in the Evaluation of an Anterior Mediastinal Mass
 Understanding the Diagnostic and Prognostic Role of Imaging in the Evaluation of an Anterior Mediastinal Mass Daniel W. Kim, Harvard Medical School Year III Agenda Mediastinum Menu of tests Anatomy Normal
Understanding the Diagnostic and Prognostic Role of Imaging in the Evaluation of an Anterior Mediastinal Mass Daniel W. Kim, Harvard Medical School Year III Agenda Mediastinum Menu of tests Anatomy Normal
Rodney C Richie MD FACP FCCP DBIM Texas Life and EMSI
 Rodney C Richie MD FACP FCCP DBIM Texas Life and EMSI Pulmonary Nodules Well-circumscribed, radiographic opacities measuring 3 cm in diameter Surrounded by aerated lung Not associated with atelectesis
Rodney C Richie MD FACP FCCP DBIM Texas Life and EMSI Pulmonary Nodules Well-circumscribed, radiographic opacities measuring 3 cm in diameter Surrounded by aerated lung Not associated with atelectesis
PET CT for Staging Lung Cancer
 PET CT for Staging Lung Cancer Rohit Kochhar Consultant Radiologist Disclosures Neither I nor my immediate family members have financial relationships with commercial organizations that may have a direct
PET CT for Staging Lung Cancer Rohit Kochhar Consultant Radiologist Disclosures Neither I nor my immediate family members have financial relationships with commercial organizations that may have a direct
Mediastinal Tumors: Imaging
 Mediastinal Tumors: Imaging References Imaging in Oncology, Husband and Reznek Computed Tomography and Magnetic Resonance of the thorax, Naidich, Zerhouni, Siegelman, Mediastinal compartments Anterior:
Mediastinal Tumors: Imaging References Imaging in Oncology, Husband and Reznek Computed Tomography and Magnetic Resonance of the thorax, Naidich, Zerhouni, Siegelman, Mediastinal compartments Anterior:
Lung Cancer Screening in the Midwest of the US: When Histoplasmosis Complicates the Picture
 Cronicon OPEN ACCESS EC PULMONOLOGY AND RESPIRATORY MEDICINE Case Report Lung Cancer Screening in the Midwest of the US: When Histoplasmosis Complicates the Picture Swan Lee 1 and Rolando Sanchez Sanchez
Cronicon OPEN ACCESS EC PULMONOLOGY AND RESPIRATORY MEDICINE Case Report Lung Cancer Screening in the Midwest of the US: When Histoplasmosis Complicates the Picture Swan Lee 1 and Rolando Sanchez Sanchez
Projected Outcomes Using Different Nodule Sizes to Define a Positive CT Lung Cancer Screening Examination
 DOI:10.1093/jnci/dju284 First published online October 20, 2014 The Author 2014. Published by Oxford University Press. All rights reserved. For Permissions, please e-mail: journals.permissions@oup.com.
DOI:10.1093/jnci/dju284 First published online October 20, 2014 The Author 2014. Published by Oxford University Press. All rights reserved. For Permissions, please e-mail: journals.permissions@oup.com.
10/17/16. Lung Cancer Screening. Question 1: Does lung cancer screening make sense? 3rd lung cancer third most prevalent tumor type
 Lung Cancer Screening Greg Rogalski Mercy Radiology Group greg@grogo.org Question 1: Does lung cancer screening make sense? 2 Requirements for successful screening process Sufficiently high prevalence
Lung Cancer Screening Greg Rogalski Mercy Radiology Group greg@grogo.org Question 1: Does lung cancer screening make sense? 2 Requirements for successful screening process Sufficiently high prevalence
Screening for Lung Cancer: Are We There Yet?
 Screening for Lung Cancer: Are We There Yet? Kavita Garg, MD Professor of Radiology University of CO, Denver Mountain States Cancer Conference Nov 6 th 2010 The Epidemiology of Lung Cancer Tobacco is the
Screening for Lung Cancer: Are We There Yet? Kavita Garg, MD Professor of Radiology University of CO, Denver Mountain States Cancer Conference Nov 6 th 2010 The Epidemiology of Lung Cancer Tobacco is the
Diagnostic Value of EBUS-TBNA in Various Lung Diseases (Lymphoma, Tuberculosis, Sarcoidosis)
") Diagnostic Value of EBUS-TBNA in Various Lung Diseases (Lymphoma, Tuberculosis, Sarcoidosis) Sevda Sener Cömert, MD, FCCP. SBU, Kartal Dr.Lütfi Kırdar Training and Research Hospital Department of Pulmonary
Diagnostic Value of EBUS-TBNA in Various Lung Diseases (Lymphoma, Tuberculosis, Sarcoidosis) Sevda Sener Cömert, MD, FCCP. SBU, Kartal Dr.Lütfi Kırdar Training and Research Hospital Department of Pulmonary
Role of CT in Lung Cancer Screening: 2010 Stuart S. Sagel, M.D.
 Role of CT in Lung Cancer Screening: 2010 Stuart S. Sagel, M.D. Lung Cancer 219,440 new cases/year in U.S. (2009) 169,390 deaths/year in U.S. mortality greater than from breast, colon, prostate CA combined
Role of CT in Lung Cancer Screening: 2010 Stuart S. Sagel, M.D. Lung Cancer 219,440 new cases/year in U.S. (2009) 169,390 deaths/year in U.S. mortality greater than from breast, colon, prostate CA combined
Lung Cancer Risk Associated With New Solid Nodules in the National Lung Screening Trial
 Cardiopulmonary Imaging Original Research Pinsky et al. Lung Cancer Risk Associated With New Nodules Cardiopulmonary Imaging Original Research Paul F. Pinsky 1 David S. Gierada 2 P. Hrudaya Nath 3 Reginald
Cardiopulmonary Imaging Original Research Pinsky et al. Lung Cancer Risk Associated With New Nodules Cardiopulmonary Imaging Original Research Paul F. Pinsky 1 David S. Gierada 2 P. Hrudaya Nath 3 Reginald
LUNG CANCER SCREENING WHAT S THE IMPACT? Nitra Piyavisetpat, MD Department of Radiology Chulalongkorn University
 LUNG CANCER SCREENING WHAT S THE IMPACT? Nitra Piyavisetpat, MD Department of Radiology Chulalongkorn University Objective LDCT lung cancer screening (LCS) Potential Benefits & Harms Recommendation of
LUNG CANCER SCREENING WHAT S THE IMPACT? Nitra Piyavisetpat, MD Department of Radiology Chulalongkorn University Objective LDCT lung cancer screening (LCS) Potential Benefits & Harms Recommendation of
PET/CT Frequently Asked Questions
 PET/CT Frequently Asked Questions General Q: Is FDG PET specific for cancer? A: No, it is a marker of metabolism. In general, any disease that causes increased metabolism can result in increased FDG uptake
PET/CT Frequently Asked Questions General Q: Is FDG PET specific for cancer? A: No, it is a marker of metabolism. In general, any disease that causes increased metabolism can result in increased FDG uptake
Pulmonologist s Perspective
 Low-dose CT for lung cancer screening Pulmonologist s Perspective Literature Review Kang-Yun Lee, MD PhD Department of Thoracic Medicine Taipei Medical University- Shuang Ho Hospital Taiwan Local vs. Advanced
Low-dose CT for lung cancer screening Pulmonologist s Perspective Literature Review Kang-Yun Lee, MD PhD Department of Thoracic Medicine Taipei Medical University- Shuang Ho Hospital Taiwan Local vs. Advanced
Diagnostic and Prognostic Value of Coronary Ca Score
 Diagnostic and Prognostic Value of Coronary Ca Score Dr. Ghormallah Alzahrani Cardiac imaging division, Adult Cardiology department Prince Sultan Cardiac Center ( PSCC) Madina, June 2 Coronary Calcium
Diagnostic and Prognostic Value of Coronary Ca Score Dr. Ghormallah Alzahrani Cardiac imaging division, Adult Cardiology department Prince Sultan Cardiac Center ( PSCC) Madina, June 2 Coronary Calcium
UCLA General Surgery Residency Program Rotation Educational Policy Goals and Objectives
 UPDATED: July 2009 ROTATION: THORACIC SURGERY UCLA General Surgery Residency Program ROTATION DIRECTOR: Mary Maish, M.D. CHIEF OF CARDIAC SURGERY: Robert Cameron, M.D. SITES: UCLA Medical Center - Westwood
UPDATED: July 2009 ROTATION: THORACIC SURGERY UCLA General Surgery Residency Program ROTATION DIRECTOR: Mary Maish, M.D. CHIEF OF CARDIAC SURGERY: Robert Cameron, M.D. SITES: UCLA Medical Center - Westwood
The Itracacies of Staging Patients with Suspected Lung Cancer
 The Itracacies of Staging Patients with Suspected Lung Cancer Gerard A. Silvestri, MD,MS, FCCP Professor of Medicine Medical University of South Carolina Charleston, SC silvestri@musc.edu Staging Lung
The Itracacies of Staging Patients with Suspected Lung Cancer Gerard A. Silvestri, MD,MS, FCCP Professor of Medicine Medical University of South Carolina Charleston, SC silvestri@musc.edu Staging Lung
Larry Tan, MD Thoracic Surgery, HSC. Community Cancer Care Educational Conference October 27, 2017
 Larry Tan, MD Thoracic Surgery, HSC Community Cancer Care Educational Conference October 27, 2017 To describe patient referral & triage for the patient with suspected lung cancer To describe the initial
Larry Tan, MD Thoracic Surgery, HSC Community Cancer Care Educational Conference October 27, 2017 To describe patient referral & triage for the patient with suspected lung cancer To describe the initial
May-Lin Wilgus. A. Study Purpose and Rationale
 Utility of a Computer-Aided Diagnosis Program in the Evaluation of Solitary Pulmonary Nodules Detected on Computed Tomography Scans: A Prospective Observational Study May-Lin Wilgus A. Study Purpose and
Utility of a Computer-Aided Diagnosis Program in the Evaluation of Solitary Pulmonary Nodules Detected on Computed Tomography Scans: A Prospective Observational Study May-Lin Wilgus A. Study Purpose and
Thyroid Nodule. Disclosure. Learning Objectives P A P A P A 3/18/2014. Nothing to disclose.
 Thyroid Nodule Evaluating the patient with a thyroid nodule and some management options. Miguel V. Valdez PA C Disclosure Nothing to disclose. Learning Objectives Examination of thyroid gland Options for
Thyroid Nodule Evaluating the patient with a thyroid nodule and some management options. Miguel V. Valdez PA C Disclosure Nothing to disclose. Learning Objectives Examination of thyroid gland Options for
Detecting Lung Nodules: Challenges and Solutions. Geoffrey D. Rubin, MD, MBA, FACR, FSCBTMR
 Detecting Lung Nodules: Challenges and Solutions Geoffrey D. Rubin, MD, MBA, FACR, FSCBTMR Learning Objectives Awareness of lung nodule detection performance Apply best practice for detection of lung nodules
Detecting Lung Nodules: Challenges and Solutions Geoffrey D. Rubin, MD, MBA, FACR, FSCBTMR Learning Objectives Awareness of lung nodule detection performance Apply best practice for detection of lung nodules
Educational Objectives. Managing Lung Cancer From the Solitary Pulmonary Nodule to Complex Cases: A Multidisciplinary Approach.
 Managing Lung Cancer From the Solitary Pulmonary Nodule to Complex Cases: A Multidisciplinary Approach Robert A. Meguid, MD, MPH, FACS Assistant Professor of Cardiothoracic Surgery Surgical Director, Surgical
Managing Lung Cancer From the Solitary Pulmonary Nodule to Complex Cases: A Multidisciplinary Approach Robert A. Meguid, MD, MPH, FACS Assistant Professor of Cardiothoracic Surgery Surgical Director, Surgical
Lung Cancer Staging: The Revised TNM Classification
 Norwegian Society of Thoracic Imaging Oslo, October 2011 Lung Cancer Staging: The Revised TNM Classification Sujal R Desai King s College Hospital, London Lung Cancer The Scale of the Problem Leading cause
Norwegian Society of Thoracic Imaging Oslo, October 2011 Lung Cancer Staging: The Revised TNM Classification Sujal R Desai King s College Hospital, London Lung Cancer The Scale of the Problem Leading cause
Role of CT imaging to evaluate solitary pulmonary nodule with extrapulmonary neoplasms
 Original Research Article Role of CT imaging to evaluate solitary pulmonary nodule with extrapulmonary neoplasms Anand Vachhani 1, Shashvat Modia 1*, Varun Garasia 1, Deepak Bhimani 1, C. Raychaudhuri
Original Research Article Role of CT imaging to evaluate solitary pulmonary nodule with extrapulmonary neoplasms Anand Vachhani 1, Shashvat Modia 1*, Varun Garasia 1, Deepak Bhimani 1, C. Raychaudhuri
Case Scenario 1 Worksheet. Primary Site C44.4 Morphology 8743/3 Laterality 0 Stage/ Prognostic Factors
 CASE SCENARIO 1 9/10/13 HISTORY: Patient is a 67-year-old white male and presents with lesion located 4-5cm above his right ear. The lesion has been present for years. No lymphadenopathy. 9/10/13 anterior
CASE SCENARIO 1 9/10/13 HISTORY: Patient is a 67-year-old white male and presents with lesion located 4-5cm above his right ear. The lesion has been present for years. No lymphadenopathy. 9/10/13 anterior
I9 COMPLETION INSTRUCTIONS
 The I9 Form is completed for each screening exam at T0, T1, and T2. At T0 (baseline), the I9 documents comparison review of the baseline screen (C2 Form) with any historical images available. At T1 and
The I9 Form is completed for each screening exam at T0, T1, and T2. At T0 (baseline), the I9 documents comparison review of the baseline screen (C2 Form) with any historical images available. At T1 and
Observer variability for Lung-RADS categorisation of lung cancer screening CTs: impact on patient management
 European Radiology https://doi.org/10.1007/s00330-018-5599-4 CHEST Observer variability for Lung-RADS categorisation of lung cancer screening CTs: impact on patient management Sarah J. van Riel 1 & Colin
European Radiology https://doi.org/10.1007/s00330-018-5599-4 CHEST Observer variability for Lung-RADS categorisation of lung cancer screening CTs: impact on patient management Sarah J. van Riel 1 & Colin
Mediastinal Incidentalomas
 ORIGINAL ARTICLE Jos A. Stigt, MD,* James E. Boers, MD, PhD, Ad H. Oostdijk, MD, Jan-Willem K. van den Berg, MD, PhD,* and Harry J. M. Groen, MD, PhD Introduction: Incidental mediastinal lymphadenopathy
ORIGINAL ARTICLE Jos A. Stigt, MD,* James E. Boers, MD, PhD, Ad H. Oostdijk, MD, Jan-Willem K. van den Berg, MD, PhD,* and Harry J. M. Groen, MD, PhD Introduction: Incidental mediastinal lymphadenopathy
Veterans Health Administration Lung Cancer Screening Demonstration Project: Results & Lessons Learned
 Veterans Health Administration Lung Cancer Screening Demonstration Project: Results & Lessons Learned Jane Kim, MD, MPH Acting Chief Consultant for Preventive Medicine National Center for Health Promotion
Veterans Health Administration Lung Cancer Screening Demonstration Project: Results & Lessons Learned Jane Kim, MD, MPH Acting Chief Consultant for Preventive Medicine National Center for Health Promotion
Lung Cancer Screening: Evidence and current recommendations
 Lung Cancer Screening: Evidence and current recommendations 20 th March 2018 Dr Annette McWilliams Fiona Stanley Hospital University of Western Australia WA Cancer & Palliative Care Network I have no financial
Lung Cancer Screening: Evidence and current recommendations 20 th March 2018 Dr Annette McWilliams Fiona Stanley Hospital University of Western Australia WA Cancer & Palliative Care Network I have no financial
I appreciate the courtesy of Kusumoto at NCC for this presentation. What is Early Lung Cancers. Early Lung Cancers. Early Lung Cancers 18/10/55
 I appreciate the courtesy of Kusumoto at NCC for this presentation. Dr. What is Early Lung Cancers DEATH Early period in its lifetime Curative period in its lifetime Early Lung Cancers Early Lung Cancers
I appreciate the courtesy of Kusumoto at NCC for this presentation. Dr. What is Early Lung Cancers DEATH Early period in its lifetime Curative period in its lifetime Early Lung Cancers Early Lung Cancers
Best Medical Practices: Maximizing Skills, Minimizing Risk Lung Cancer
 Best Medical Practices: Maximizing Skills, Minimizing Risk Lung Cancer Optimal Management of Incidental Pulmonary Nodule Ramin Khorasani, MD, MPH Vice Chair, Department of Radiology Director, Center for
Best Medical Practices: Maximizing Skills, Minimizing Risk Lung Cancer Optimal Management of Incidental Pulmonary Nodule Ramin Khorasani, MD, MPH Vice Chair, Department of Radiology Director, Center for
FDG PET/CT STAGING OF LUNG CANCER. Dr Shakher Ramdave
 FDG PET/CT STAGING OF LUNG CANCER Dr Shakher Ramdave FDG PET/CT STAGING OF LUNG CANCER FDG PET/CT is used in all patients with lung cancer who are considered for curative treatment to exclude occult disease.
FDG PET/CT STAGING OF LUNG CANCER Dr Shakher Ramdave FDG PET/CT STAGING OF LUNG CANCER FDG PET/CT is used in all patients with lung cancer who are considered for curative treatment to exclude occult disease.
A Comprehensive Cancer Center Designated by the National Cancer Institute
 N C I C C C A Comprehensive Cancer Center Designated by the National Cancer Institute Screening and Early Detection of Lung Cancer: Ready for Practice? David S. Ettinger, MD, FACP, FCCP Alex Grass Professor
N C I C C C A Comprehensive Cancer Center Designated by the National Cancer Institute Screening and Early Detection of Lung Cancer: Ready for Practice? David S. Ettinger, MD, FACP, FCCP Alex Grass Professor
The Virtual Lung Nodule Clinic
 The Virtual Lung Nodule Clinic Poster No.: C-1023 Congress: ECR 2016 Type: Educational Exhibit Authors: S. Higgins, F. C. Lyall, J. Taylor, J. goldman, S. Rolin, B. 1 2 1 2 2 3 2 2 3 Soar ; Torbay/UK,
The Virtual Lung Nodule Clinic Poster No.: C-1023 Congress: ECR 2016 Type: Educational Exhibit Authors: S. Higgins, F. C. Lyall, J. Taylor, J. goldman, S. Rolin, B. 1 2 1 2 2 3 2 2 3 Soar ; Torbay/UK,
Boot Camp Case Scenarios
 Boot Camp Case Scenarios Case Scenario 1 Patient is a 69-year-old white female. She presents with dyspnea on exertion, cough, and right rib pain. Patient is a smoker. 9/21/12 CT Chest FINDINGS: There is
Boot Camp Case Scenarios Case Scenario 1 Patient is a 69-year-old white female. She presents with dyspnea on exertion, cough, and right rib pain. Patient is a smoker. 9/21/12 CT Chest FINDINGS: There is
Small Pulmonary Nodules: Our Preliminary Experience in Volumetric Analysis of Doubling Times
 Small Pulmonary Nodules: Our Preliminary Experience in Volumetric Analysis of Doubling Times Andrea Borghesi, MD Davide Farina, MD Roberto Maroldi, MD Department of Radiology University of Brescia Brescia,
Small Pulmonary Nodules: Our Preliminary Experience in Volumetric Analysis of Doubling Times Andrea Borghesi, MD Davide Farina, MD Roberto Maroldi, MD Department of Radiology University of Brescia Brescia,
The Role of PET / CT in Lung Cancer Staging
 July 2004 The Role of PET / CT in Lung Cancer Staging Vlad Vinarsky, Harvard Medical School Year IV Patient AM HPI: 81 yo F p/w hemoptysis x 1 month LLL lesion on CXR, not responsive to Abx 35 pack-year
July 2004 The Role of PET / CT in Lung Cancer Staging Vlad Vinarsky, Harvard Medical School Year IV Patient AM HPI: 81 yo F p/w hemoptysis x 1 month LLL lesion on CXR, not responsive to Abx 35 pack-year
VHA Demonstration Project for Lung Cancer Screening Using Low-Dose Chest CT Screening
 VHA Demonstration Project for Lung Cancer Screening Using Low-Dose Chest CT Screening ATS San Francisco 2016 James K. Brown MD 1, Kathryn L. Rice, MD 2 (1) San Francisco VA (2) Minneapolis VAMC Disclosures
VHA Demonstration Project for Lung Cancer Screening Using Low-Dose Chest CT Screening ATS San Francisco 2016 James K. Brown MD 1, Kathryn L. Rice, MD 2 (1) San Francisco VA (2) Minneapolis VAMC Disclosures
Zurich, January 19, 2018
 Brain metastases as first presentation of malignancy: Immediate management, differential diagnosis; prevalence of primaries and suggested work-up Symposium on Brain Metastasis Cancer Center Zurich Zurich,
Brain metastases as first presentation of malignancy: Immediate management, differential diagnosis; prevalence of primaries and suggested work-up Symposium on Brain Metastasis Cancer Center Zurich Zurich,