Salivary gland neoplasms: an update 29th Annual Meeting of Arab Division of the International Academy of Pathology MUSCAT, OMAN 2017
|
|
|
- Irene Sherman
- 6 years ago
- Views:
Transcription

1 Salivary gland neoplasms: an update 29th Annual Meeting of Arab Division of the International Academy of Pathology MUSCAT, OMAN 2017 Dr Mary Toner Consultant Pathologist St James Hospital Trinity College Dublin Dublin Dental University Hospital
2 WHO Blue Book 2017: salivary gland Some non neoplastic entities included Expanded molecular pathogenesis Newly defined entities: e.g. secretory carcinoma, polymorphous adenocarcinoma
3 New entities: Secretory Carcinoma Mammary analogue secretory carcinoma First recognised as tumour similar to secretory carcinoma of breast Defined by specific molecular finding of balanced chromosomal translocation t(12,15)(p13:q25) identical to secretory carcinoma of breast
4 Secretory carcinoma balanced chromosomal translocation t(12,15)(p13:q25) results in formation of ETV6-NTRK3 fusion gene (Also seen in infantile fibrosarcoma and others) Detected either by break-apart ETV6 FISH probe or RT-PCR for the fusion transcript
5 Variable fusion partners described Rather than ETV6-NTRK3 fusion there may be others e.g. ETV6-Xgene fusion Morphology may tend to be different - more infiltrative growth and sclerotic stroma
6 Secretory carcinoma Adults, wide age range mean 47y Male predominance Parotid > minor glands> submandibular gland Defined in molecular terms Characteristic morphology About 250 cases reported

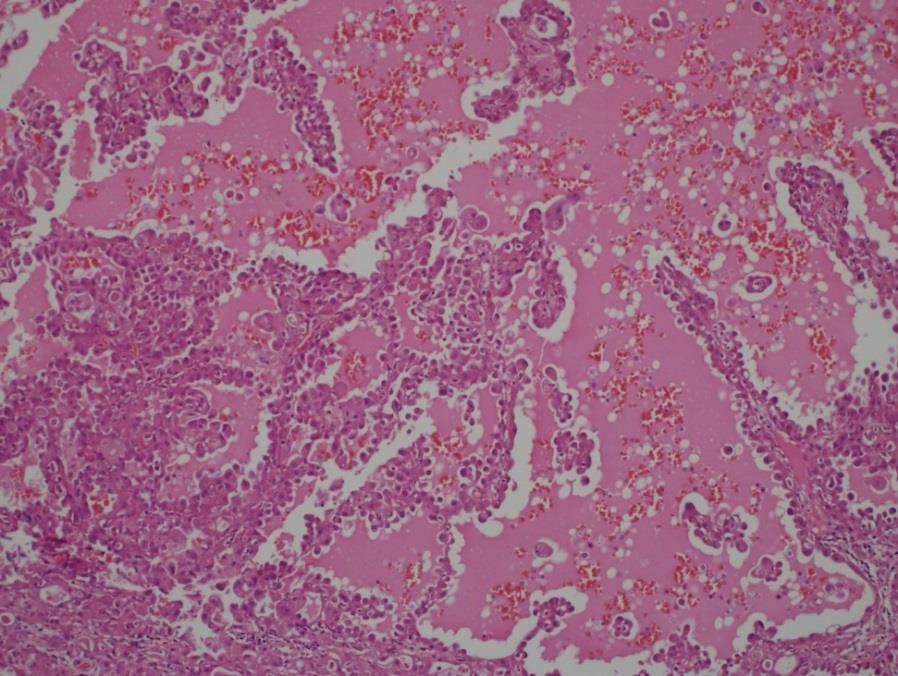
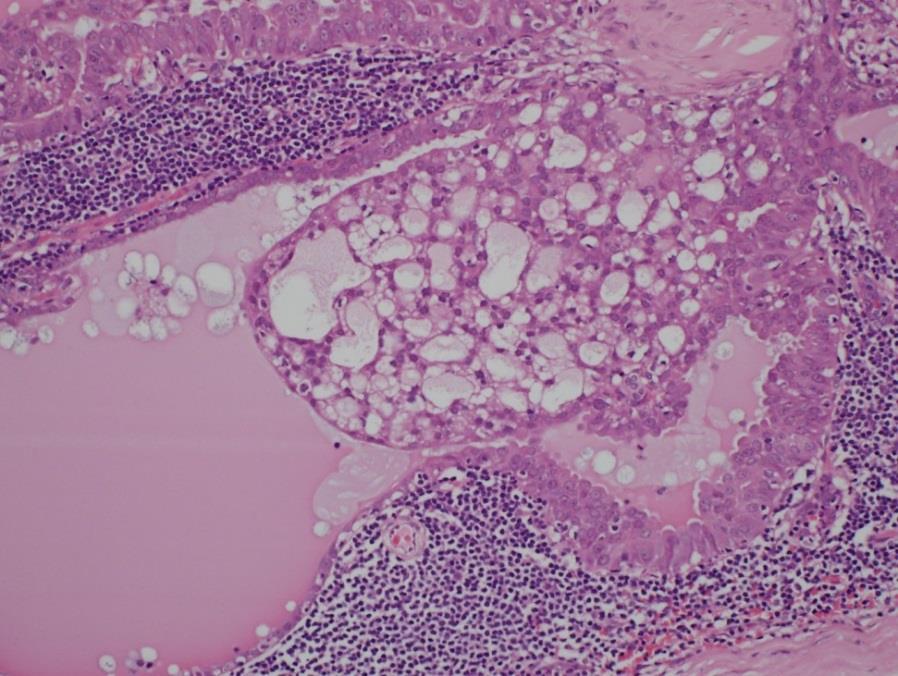
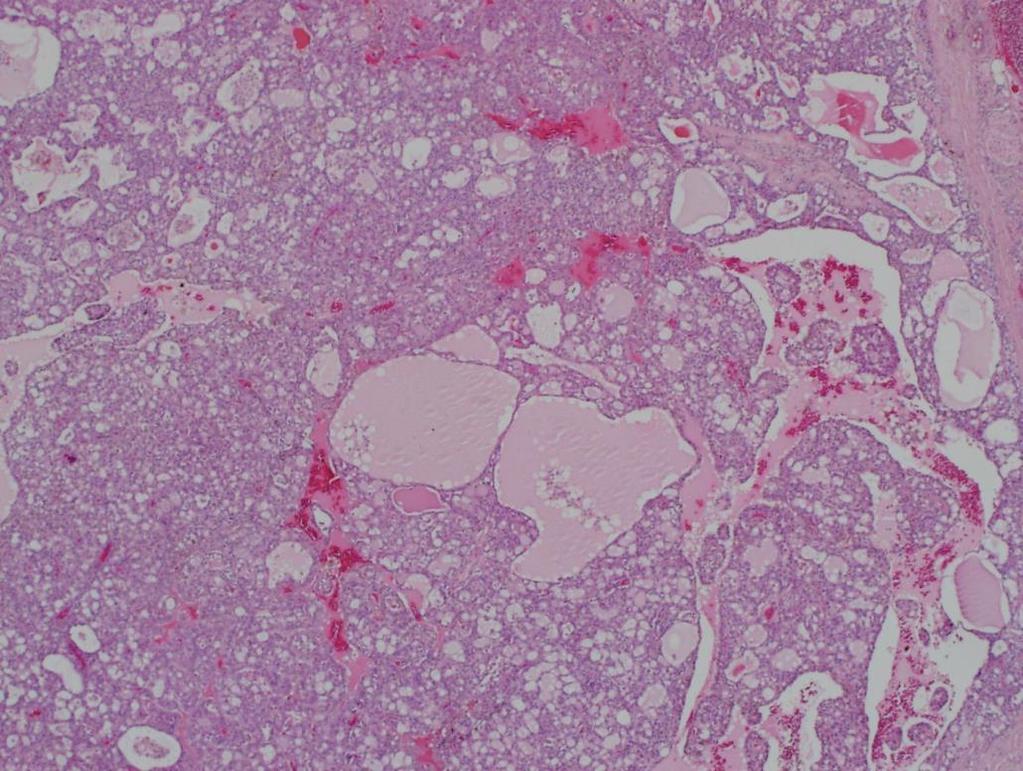
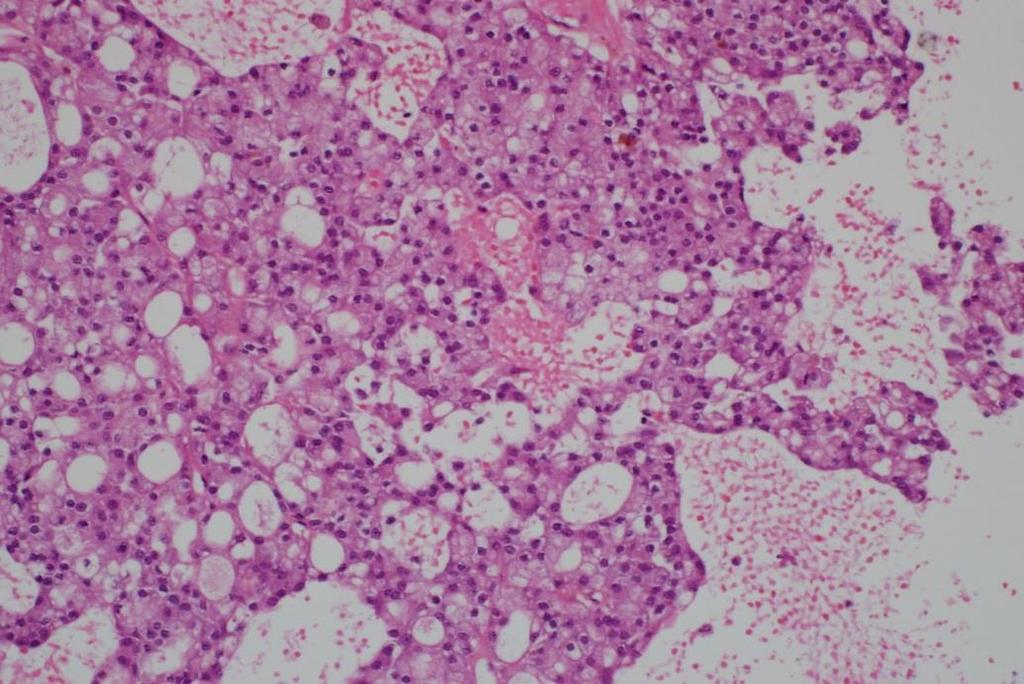
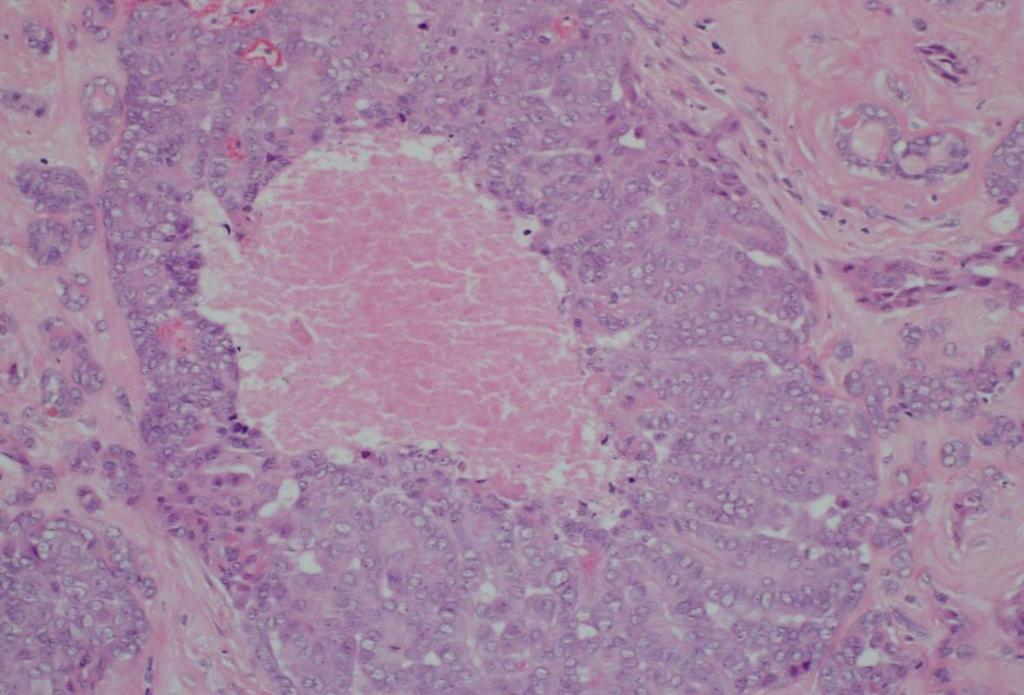
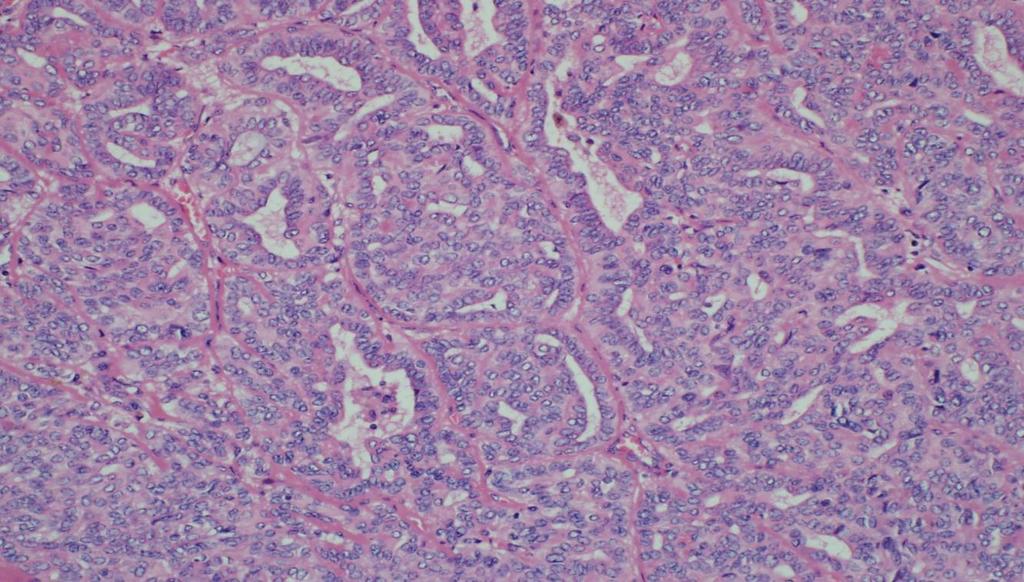
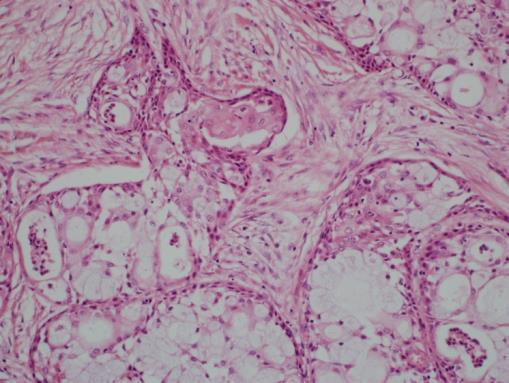
7 Secretory carcinoma Often lobules with thin septae Tubular, solid, microcystic, follicular or papillary growth patterns Fibrotic stroma less common Cystic less common

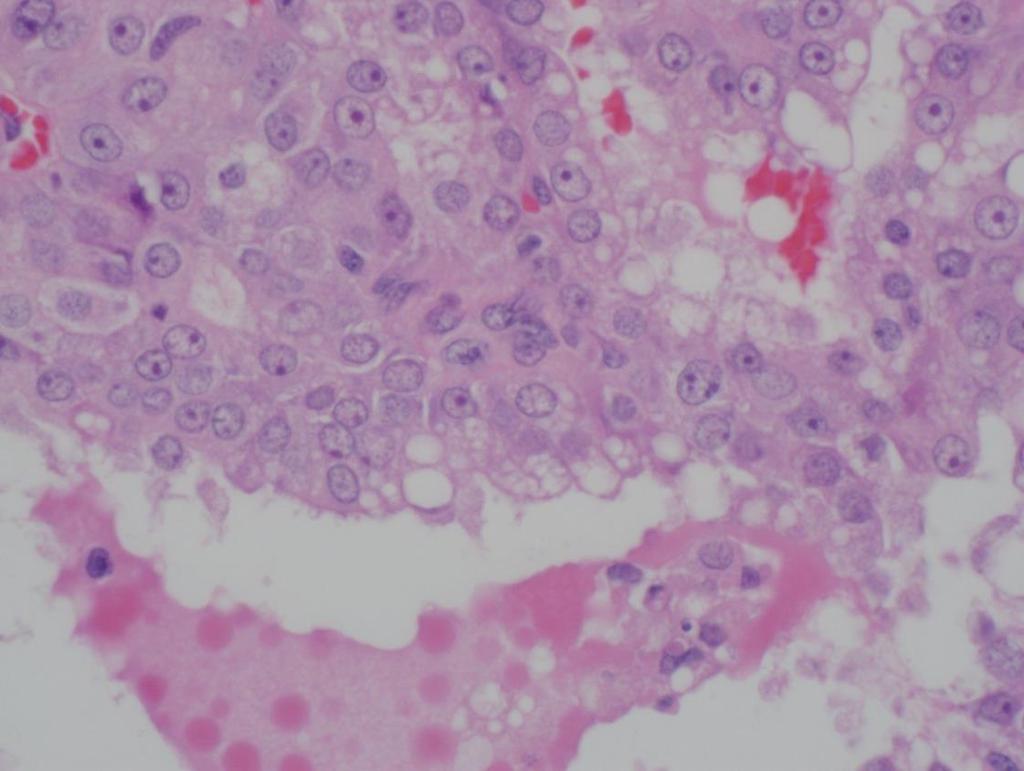
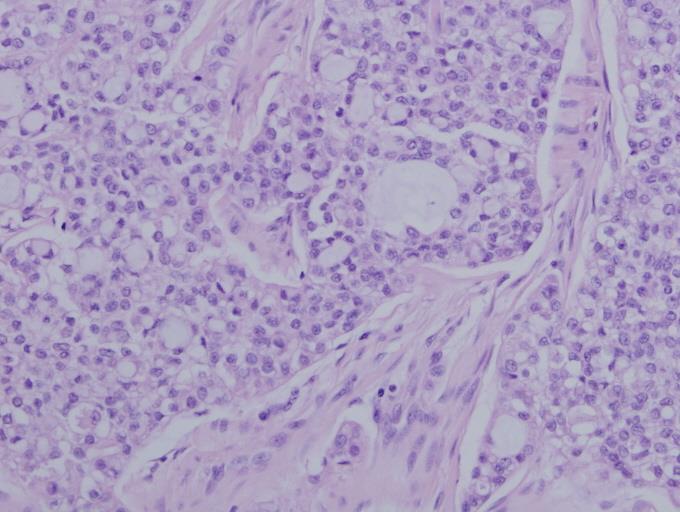
8 Secretory carcinoma Low grade vesicular nuclei Foamy/ granular/ vacuolated cytoplasm Bubbly secretions Atypia and mitoses rare
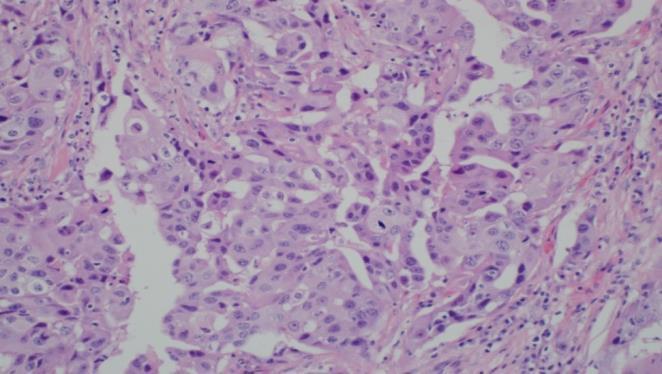
9

10
11
12
13
14
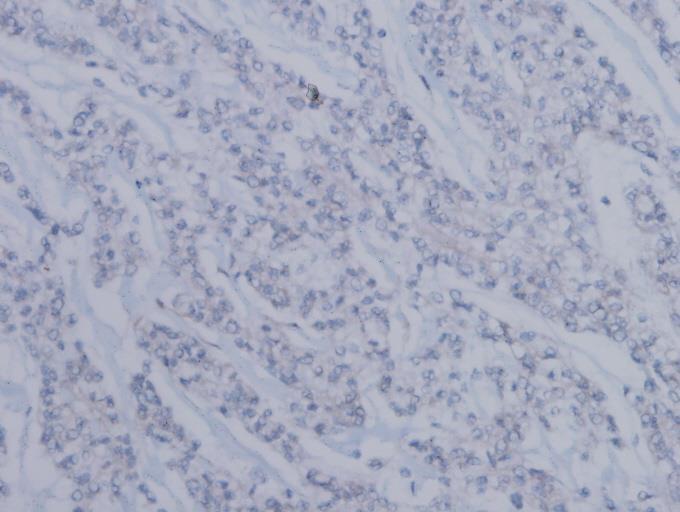
15 Secretory carcinoma versus acinic cell Secretory carcinoma Multiple growth patterns Papillary cystic More solid and bubbly Multivacuolated cytoplasm Luminal and cytoplasmic mucin DPAS+ globules No basophilic granules Diffuse S100, mammaglobin positive DOG1 negative carcinoma Acinic cell carcinoma Multiple growth patterns, rarely papillary Papillary cystic less likely DPAS: granular cytoplasmic positivity May have basophilic granules S100, mammaglobin negative DOG1 positive (intense apical membranous and variable cytoplasmic)
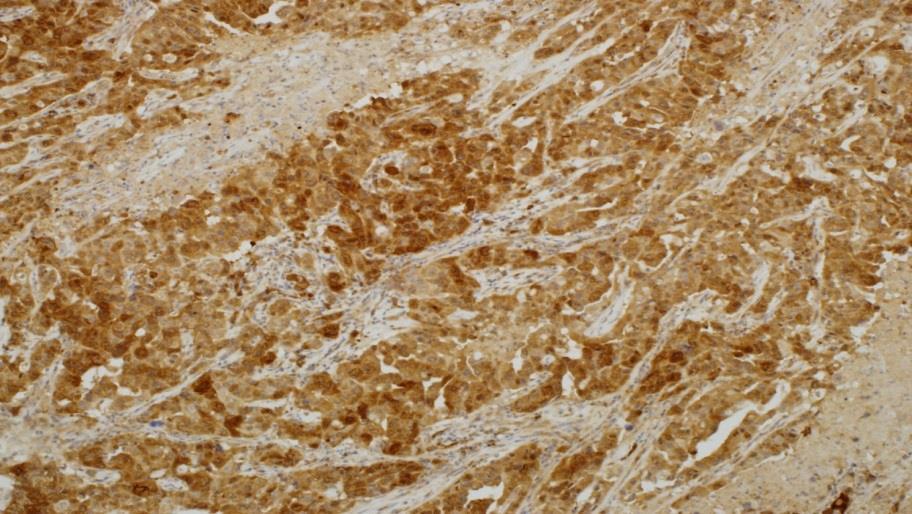
16 S100
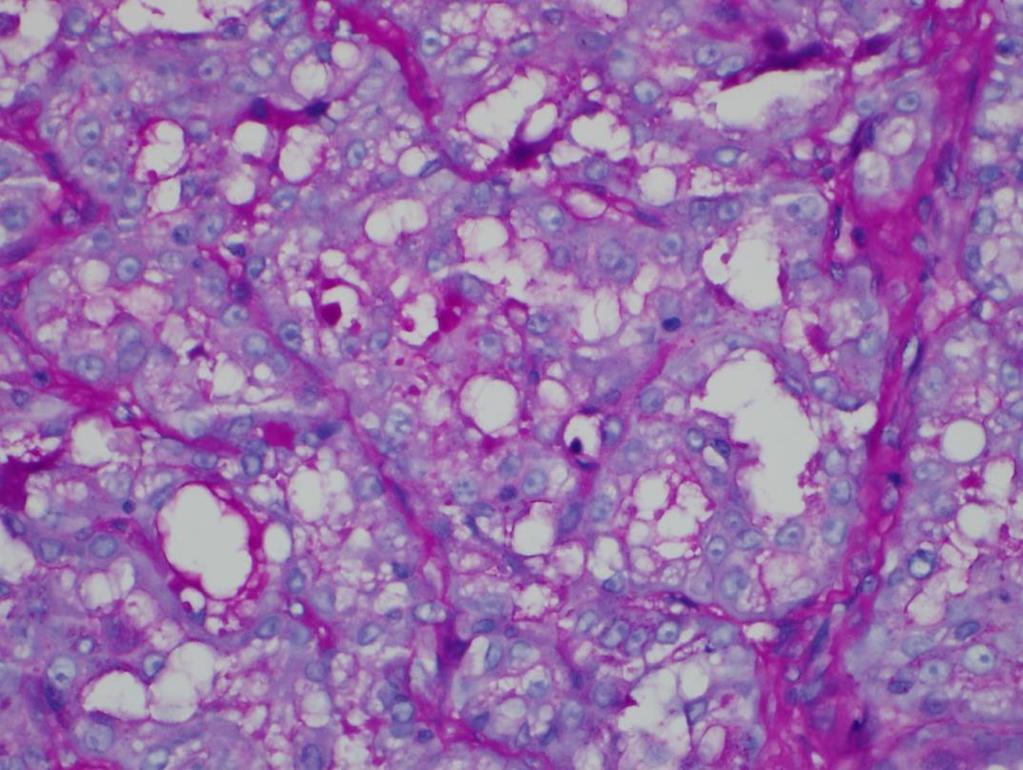
17 DPAS


18 Acinic cell carcinoma (zymogen rich)

19 DOG 1 in acinic cell carcinoma


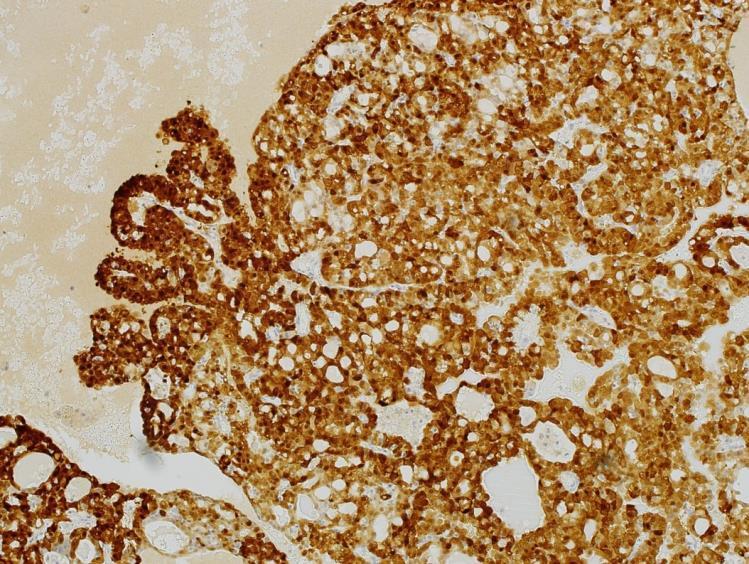
20 Secretory carcinoma Mammaglobin HE

21 Polymorphous low grade adenocarcinoma: 60% may have S100 and mammaglobin positivity Adenoid cystic: 13% mammoglobin positive Low grade salivary duct adenocarcinoma Salivary duct carcinoma Mammaglobin
22 Secretory carcinoma: differential Low grade ductal adenocarcinoma/ cystadenocarcinoma: S100 and mammaglobin diffusely positive Intraductal micropapillary or cribriform usually p63 positive myoepithelial layer help to distinguish Mucoepidermoid carcinoma: S100 and mammaglobin usually negative
23 Secretory carcinoma: Prognosis Usually indolent behaviour but may result in locoregional recurrence and metastasis Up to 25% nodal metastases described Prognosis: depends on stage High grade transformation has been described Due to nature of fusion: TRK inhibitors may have a role

24 Acinic cell carcinoma (after SC) >50% of zymogen granule poor acinic cell carcinomas are secretory carcinomas Secretory M:F ratio 8:2 Acinic M:F ratio 1:1.5
25 Secretory carcinoma in thyroid Recently 6 cases from 2 centres Morphologically like salivary counterpart Nodal metastases/ high stage S100 and mammaglobin positive ETV6 rearrangement confirmed by FISH Negative for thyroglobulin and TTF-1 ETV6-NTRK3 rearrangement also described in radiation associated thyroid PTC PAX8 was positive focally Probably true thyroid origin
26 New entity: polymorphous adenocarcinoma
27 Polymorphous adenocarcinoma New nomenclature 2017 probably most contentious area Includes cases previously called polymorphous low grade adenocarcinoma and cribriform adenocarcinoma of tongue(cat)/ cribriform adenocarcinoma of minor salivary glands (CAMSG) Low grade was dropped due to aggressive behaviour of some tumours, tumours with not so low grade appearance CAMSG - emerging entity, may be recognised as an entity in the future
28 PLGA and CAMSG -? distinct entities or variants on a spectrum Cribriform adenocarcinoma Base of tongue predominates Papillary/ glomeruloid structures Also cribriform, tubular, solid Optically clear/ ground glass nuclei Propensity for LVI PLGA Palate, buccal mucosa predominate Streaming columns of cells, concentric whorls, tubular, solid papillary and cribriform Pale vesicular nuclei PNI Rearrangements of PRKD1-3 in 80% PRKD1 E710D mutations 10% Early nodal metastasis common Rearrangements of PRKD1-3 in 10% PRKD1 E710D mutations 80% Nodal metastasis rare

29 Historically - polymorphous low grade adenocarcinoma Described in 1984 Infiltrative growth overlap with features of adenoid cystic carcinoma but much better prognosis Local recurrence 10-33% Distant metastases and death from disease rare
30


31 PLGA Adenoid cystic carcinoma
32 PLGA But historical difficulty over inclusion or exclusion of cases with prominent papillary growth pattern Some felt the papillary ones would be better categorised as adenocarcinoma, NOS associated with worse prognosis than PLGA without papillary growth Also cases with necrosis, higher grade areas Suggested since 2002 that low grade should be dropped
33
34 Cribriform adenocarcinoma of minor salivary gland Originally described as cribriform adenocarcinoma of the tongue (CAT) usually base of tongue Later expanded as seen in other sites CAMSG (minor salivary gland) Some base of tongue tumours were more papillary and more aggressive Growth pattern is mostly papillary/ glomeruloid despite the name

35 microcystic /cribriform
36
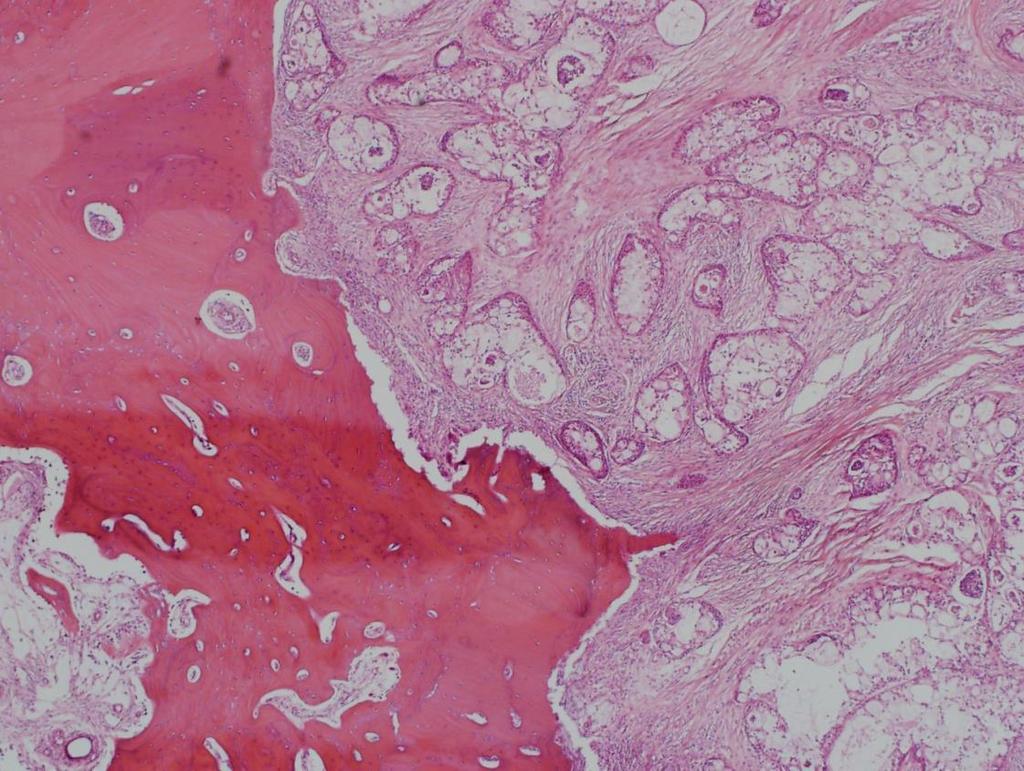
37 Infiltrative growth

38

39 CAMSG papillary with PTC like nuclei
40
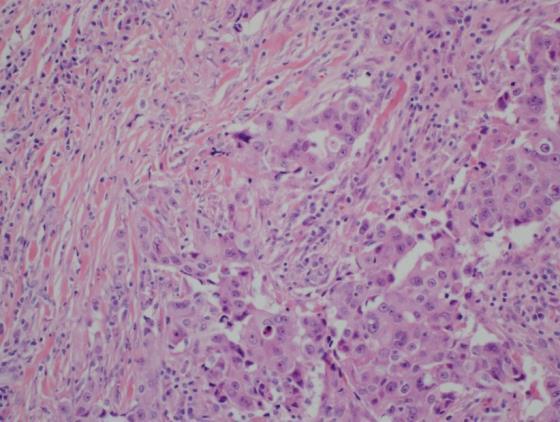
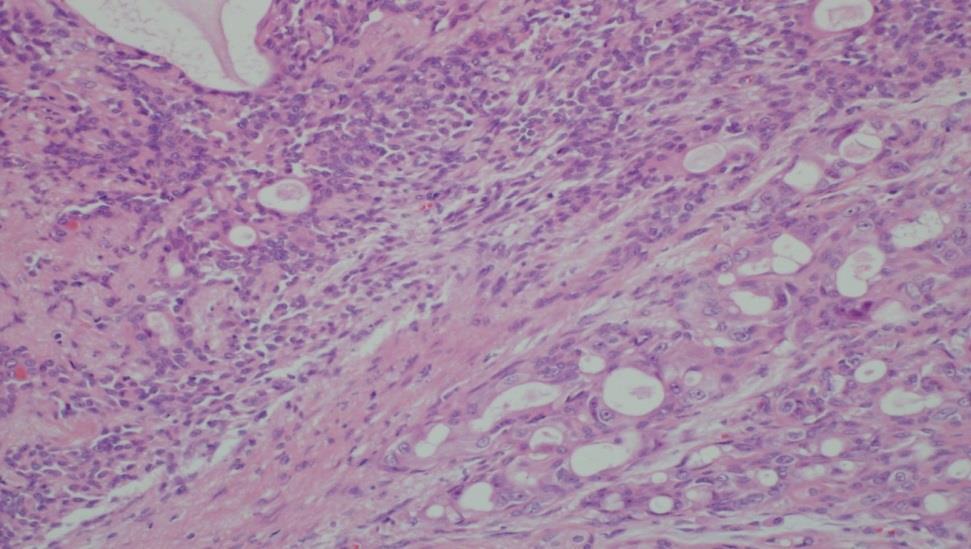
41 WHO 2017 Polymorphous adenocarcinoma Submucosal, unencapsulated, infiltrative Small bland cells Minimal hyperchromatism, many with pale washed out nuclei PNI common Mitoses uncommon, no necrosis Variability within and between tumours characteristic: lobular, trabecular, microcystic, cribriform, solid, papillary /cystic S100 often diffusely positive Do not have a prominent basal or myoepithelial phenotype although p63 seen (but not in biphasic pattern as in adenoid cystic )
42 Polymorphous adenocarcinoma versus adenoid cystic carcinoma Polymorphous adenocarcinoma Pale vesicular nuclei Multiple growth patterns, focally cribriform Monotypic cells PNI with perineural whorling at periphery MIB 1 <10% P63+p40- Adenoid cystic Hyperchromatic angulated nuclei Glandular / tubular, cribriform, solid Biphasic pattern usually seen, inner cells CD117 + PNI, often larger nerves MIB1 > 10% P63+p40+ MYB-NFIB fusion in 80%

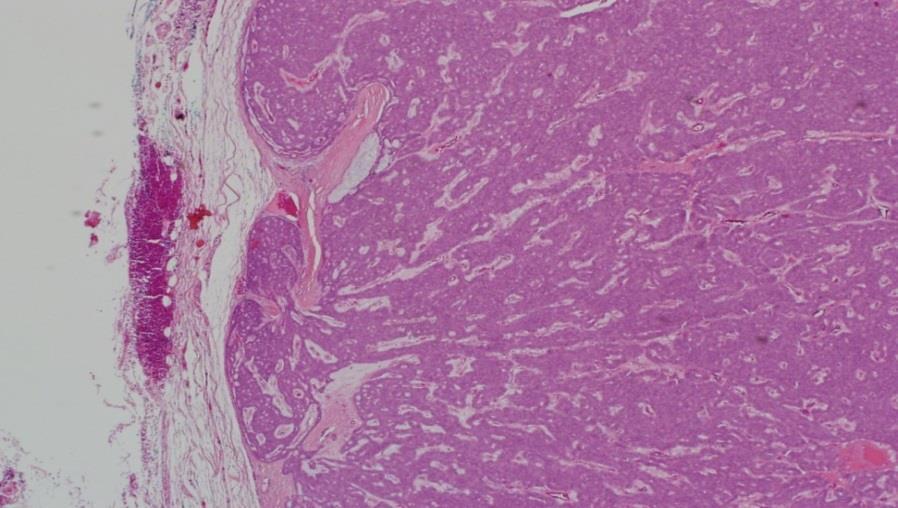
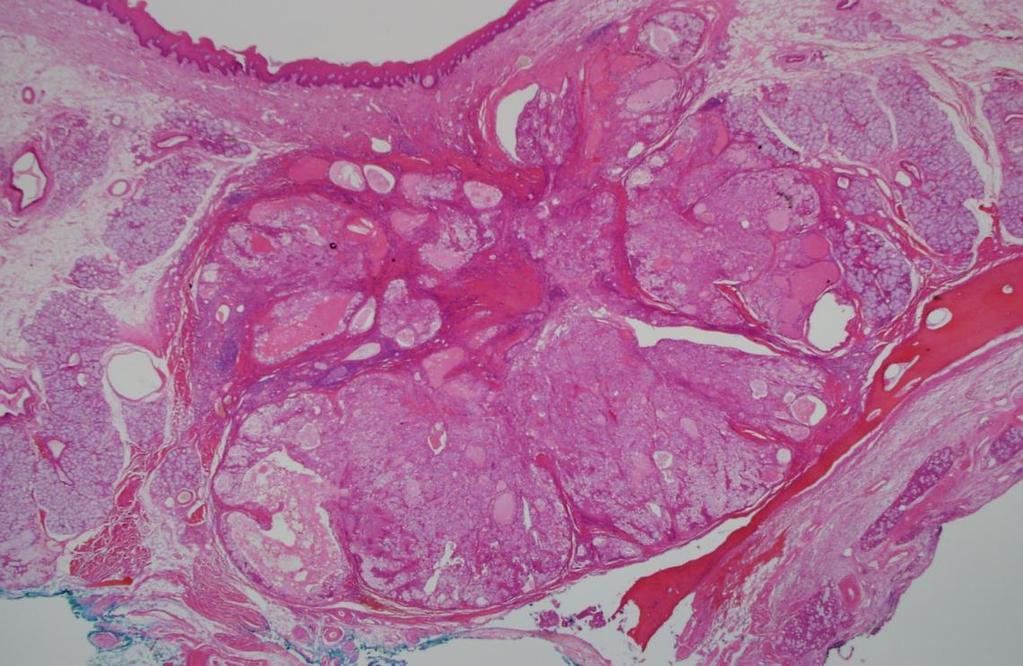
43 Tumour upper lip 35 year old female


44 Tumour of upper lip
45

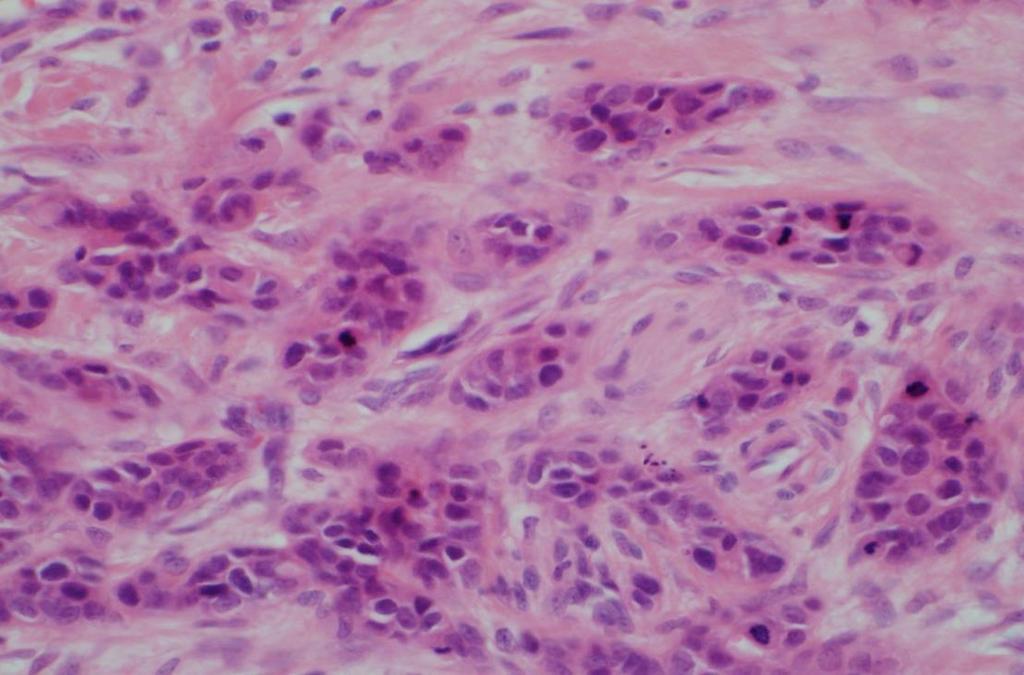
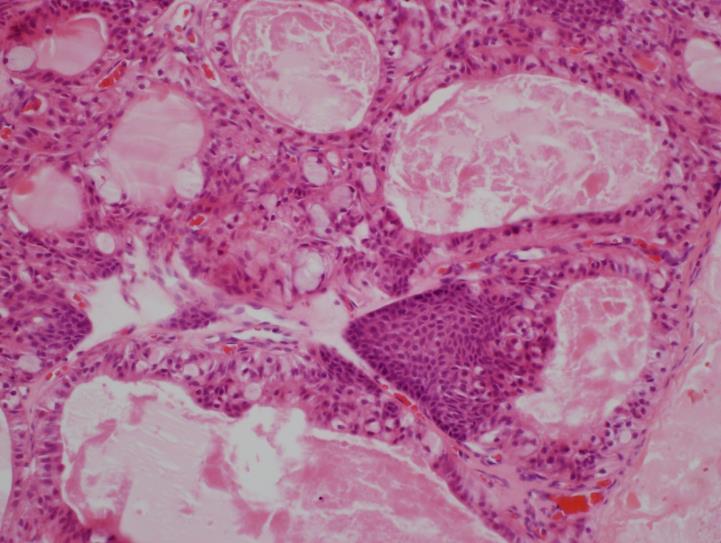
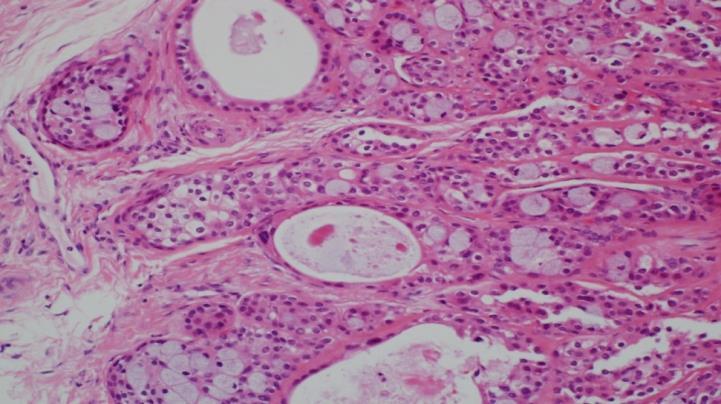
46 Mitoses, microcystic pattern
47
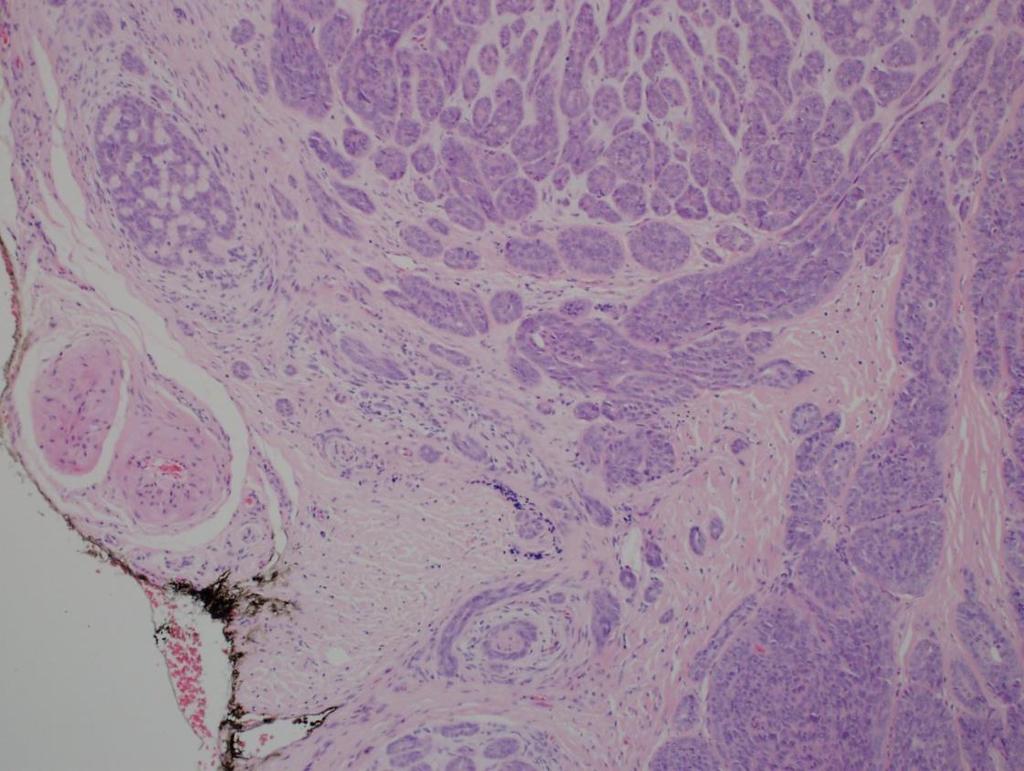
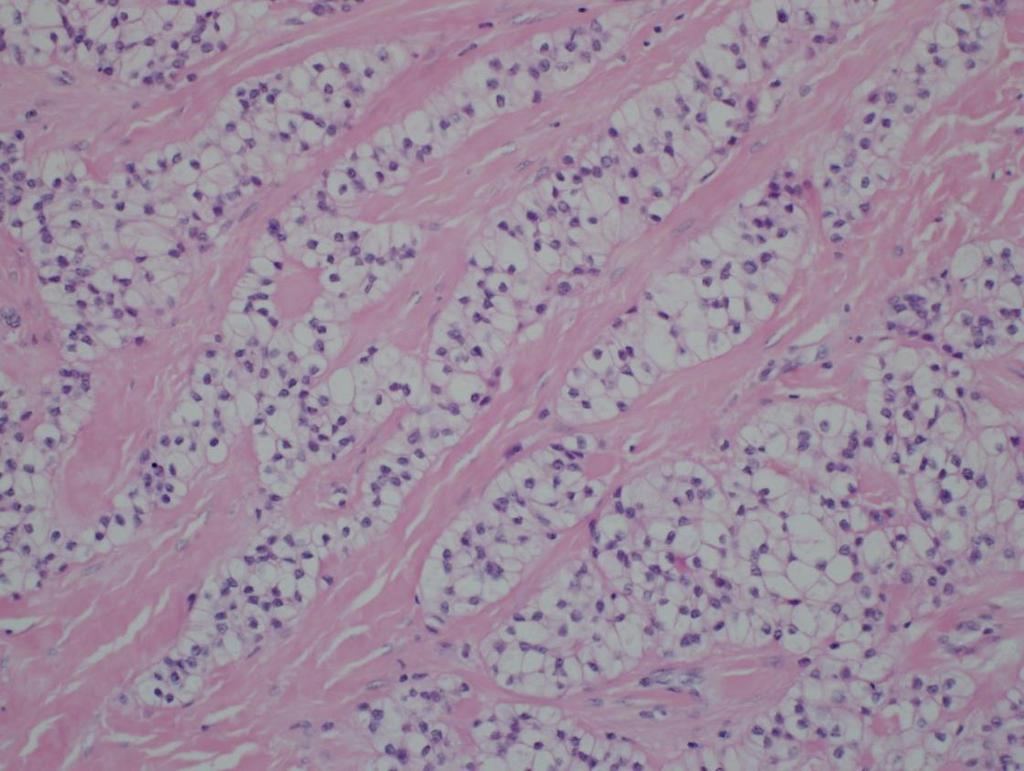
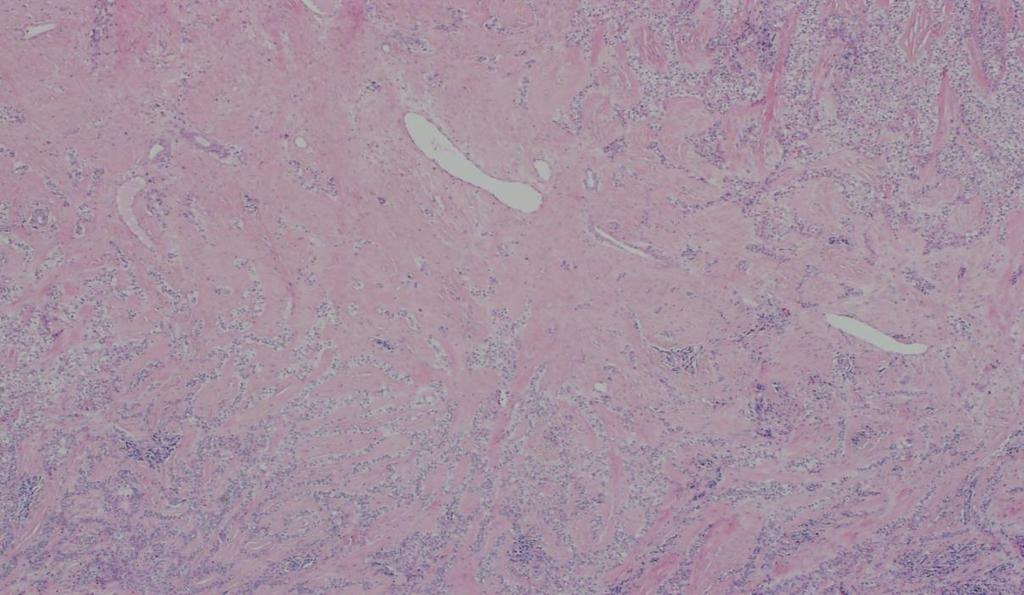
48 Polymorphous adenocarcinoma (CAMSG type)

49 Small left lateral tongue tumour
50
51
52 Diagnosis: Metastatic adenocarcinoma from the oesophagus mimicking primary


53 Adenoid cystic carcinoma 2017

54 Adenoid cystic carcinoma 5 yr survival 90% 15 yr survival <70% Growth pattern and stage important Solid growth pattern > 30% - worse outcome
55 Adenoid cystic carcinoma: molecular t (6;9) translocation that joins the MYB (chros 6) and NFIB (chros 9) transcription factors into fusion gene product 80% of adenoid cystic carcinomas, not in HGT 6q22-23 translocations MYB fusion/activation 89% 8q13 translocations MYBLI fusion/ activation 10% NOTCH1 mutation 5-10% MYB antibody also available but not specific for diagnosis of ACC
56 Clear cell carcinoma Previously: clear cell carcinoma, NOS hyalinising clear cell carcinoma EWSR1-ATF1 fusion recently identified 85-90% of tumours
57 Clear cell carcinoma Rare low grade minor salivary gland carcinoma Lack of myoepithelial differentiation Until recently a diagnosis of exclusion Distinction from clear cell mucoepidermoid carcinoma, clear cell odontogenic carcinoma was not always possible

58 Clear cell carcinoma Palate tongue base, tongue Appear clinically and grossly circumscribed but infiltrative on histology Growth pattern: small nests, cords, thin trabeculae, single cells Pale uniform eosinophilic or clear cytoplasm Desmoplastic response most often in centre of tumour Infiltrative edge and can have pagetoid surface involvement PNI and intraneural involvement common
59
60
61

62 Calponin PAS
63 Clear cell carcinoma Foci of squamous differentiation may be seen Origin from surface epithelium can be seen No duct formation Diffuse p63 EM: features suggesting squamous differentiation At least not an adenocarcinoma Weinreb 2013
64 Clear cell carcinoma: molecular EWSR1-ATF1 fusion recently identified (85-90%) Also present in clear cell odontogenic carcinoma but not other clear cell mimics EWSR1 gene rearrangements are present in soft tissue myoepithelial tumours but fusions are distinct from salivary counterparts
65
66 Salivary duct carcinoma Papillary cribriform tumour with comedo necrosis, apocrine appearance High grade ER PR negative Androgen positivity discovered inadvertently (90%) Some PSA positive High grade carcinoma that is AR negative, non apocrine probably another type of carcinoma e.g. HGT of another type, SCC
67

68 Salivary duct carcinoma: androgen receptor positive androgen deprivation therapy under investigation

69 Salivary duct carcinoma: Her2 antibody (approximately 15%)
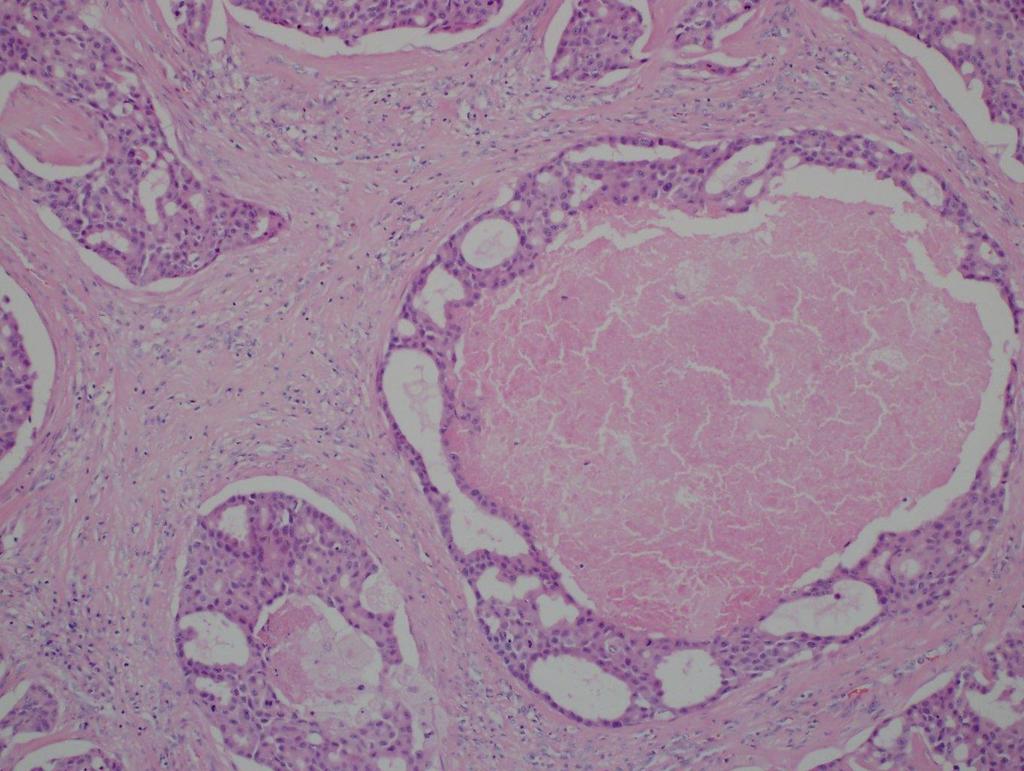
70 Intraductal carcinoma Intraductal carcinoma (low grade salivary duct adenocarcinoma/ low grade cribriform cystadenocarcinoma) Outer myoepithelial layer should be identifiable
71 Salivary duct carcinoma vs intraductal carcinoma Salivary duct carcinoma High grade, invasive AR positive S100 negative SOX10 negative P63, p40 negative Intraductal carcinoma Low grade, intraductal AR negative S100 positive SOX10 positive P63,p40 highlights intraductal component
72
73 Mucoepidermoid carcinoma
74 Grading in mucoepidermoid carcinoma AFIP: Goode/ Auclair/ Ellis 1998 Brandwein: modification of AFIP score 2001 Modified Healey (MD Anderson) 2009 Katabi/ MSKCC 2014 Low grade: local excision High grade: excision, neck dissection +/-radiotherapy
75 Quantitative grading systems AFIP Intracystic <20% +2 Neural invasion +2 Mitoses >4/10 hpf +3 Necrosis +3 Anaplasia +4 Low 0-4 Intermediate 5-6 High >7 Brandwein Intracystic <25% +2 Neural invasion +2 Mitoses >4/10 hpf +3 Necrosis +3 Nuclear atypia +3 Invades in small nests +2 Vascular invasion +3 Bone invasion +3 Low 0 Intermediate 2-3 High >4
76 Qualitative systems Modified Healey LG: macrocysts, minimal pleomorphism, circumscribed invasive edge IG: fewer microcysts, non macrocysts, more solid, mild moderate pleomorphism HG: solid, no macrocysts, easily found mitoses, cytologically high grade MSKCC LG: cystic, circumscribed, 0- mitoses1/10 hpf, no necrosis IG: mostly solid, circumscribed or infiltrative mitoses<4/10hpf, non necrosis HG: mitoses >4/10 hpf, necrosis present
77
78 Katabi (MSKCC) Compared grading systems with outcome Lack of consensus among grading systems AFIP more likely to downgrade, Brandwein more likely to upgrade (e.g. bone invasion) Modified Healey: descriptors too ambiguous Suggest MSKCC criteria are relatively more objective
79 High grade mucoepidermoid carcinoma is rare All scoring systems correlate with DSS and RFS No difference in outcome for low grade and intermediate grade (no matter which scoring system is used)
80 Mucoepidermoid carcinoma: unique translocation t(11;19)(q21;p13) results in MECT1-MAML2 fusion only seen in mucoepidermoid, but also at other sites e.g. lung useful in diagnosis >50% tumours show fusion Initially - fusion positive associated with better prognosis Associated with low/ intermediate grade tumours only Later fusion positive high grade carcinomas identified
81 Mucoepidermoid carcinoma Jee et al: genome wide copy number alterations study subdivide MEC into 3 groups Low grade, fusion positive, few genomic imbalances: favourable prognosis High grade, fusion positive, multiple genomic imbalances: unfavourable prognosis
 within infiltrative tumour")
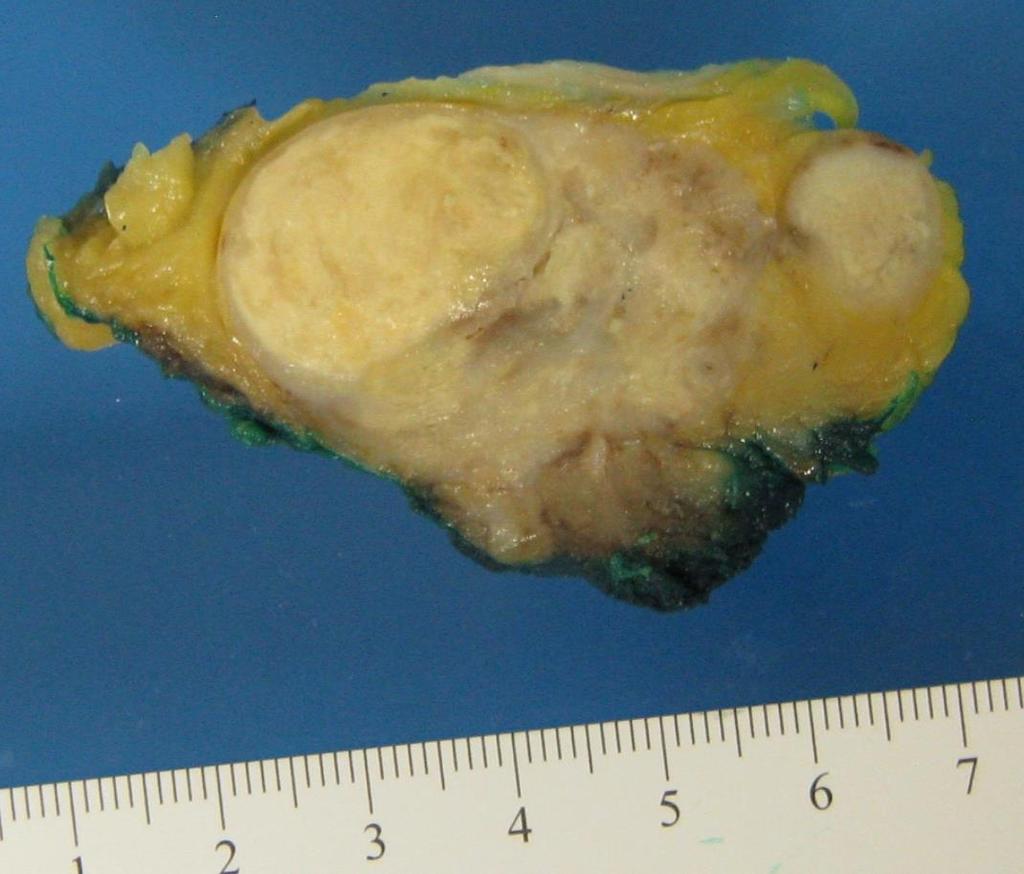
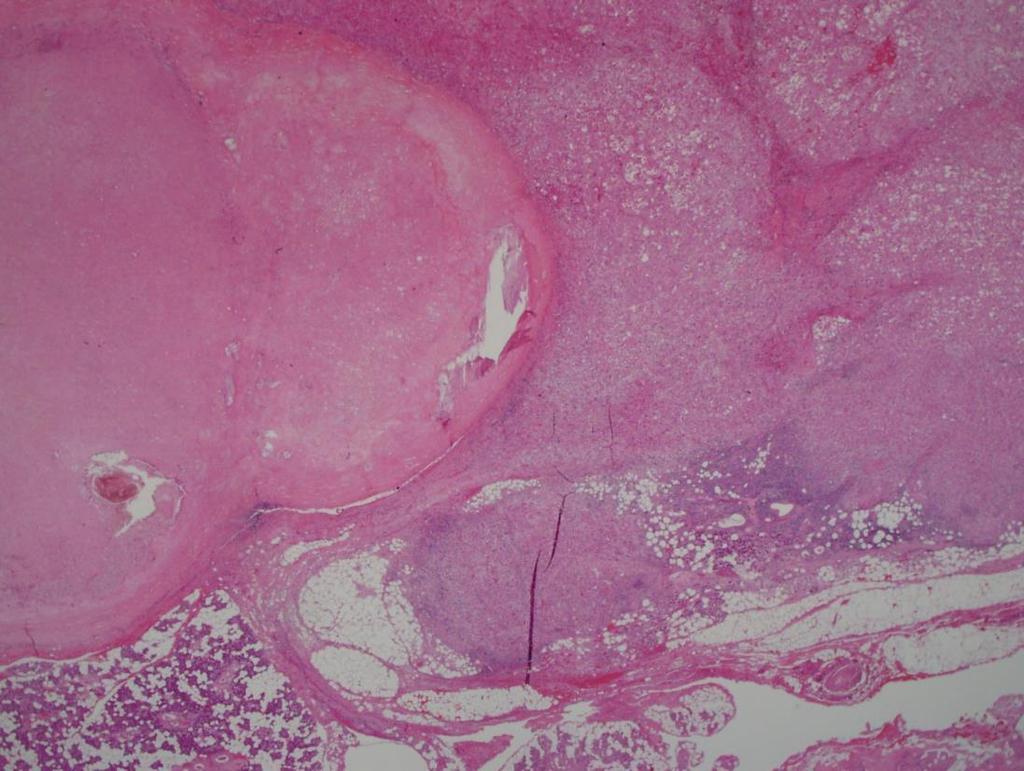
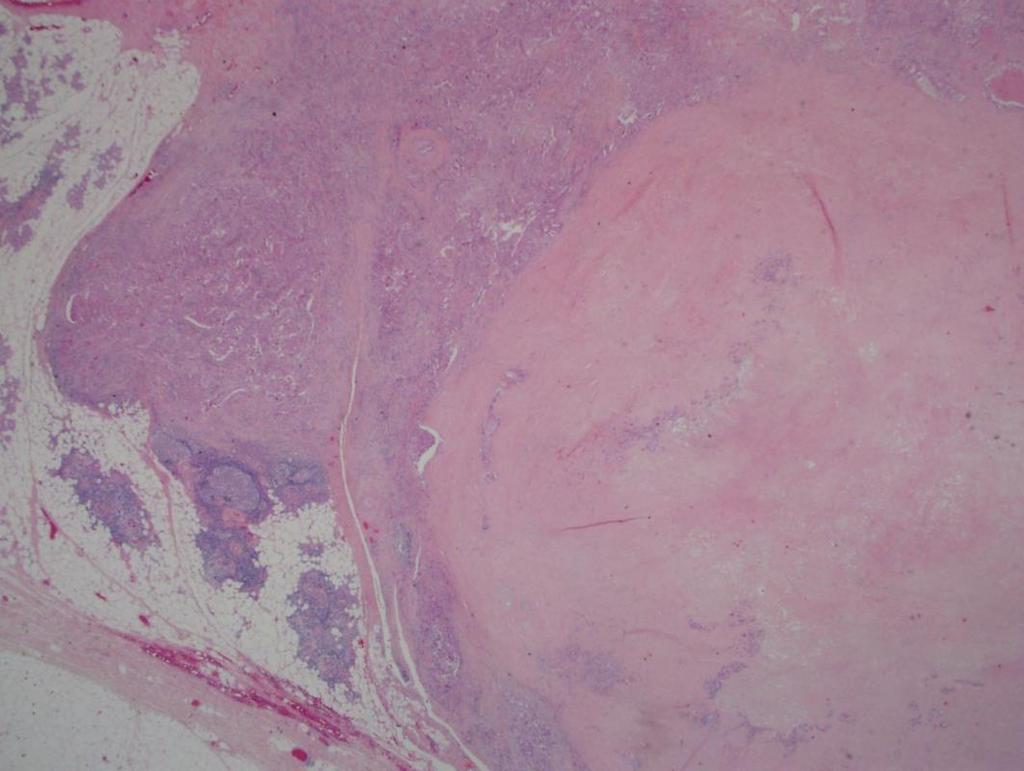
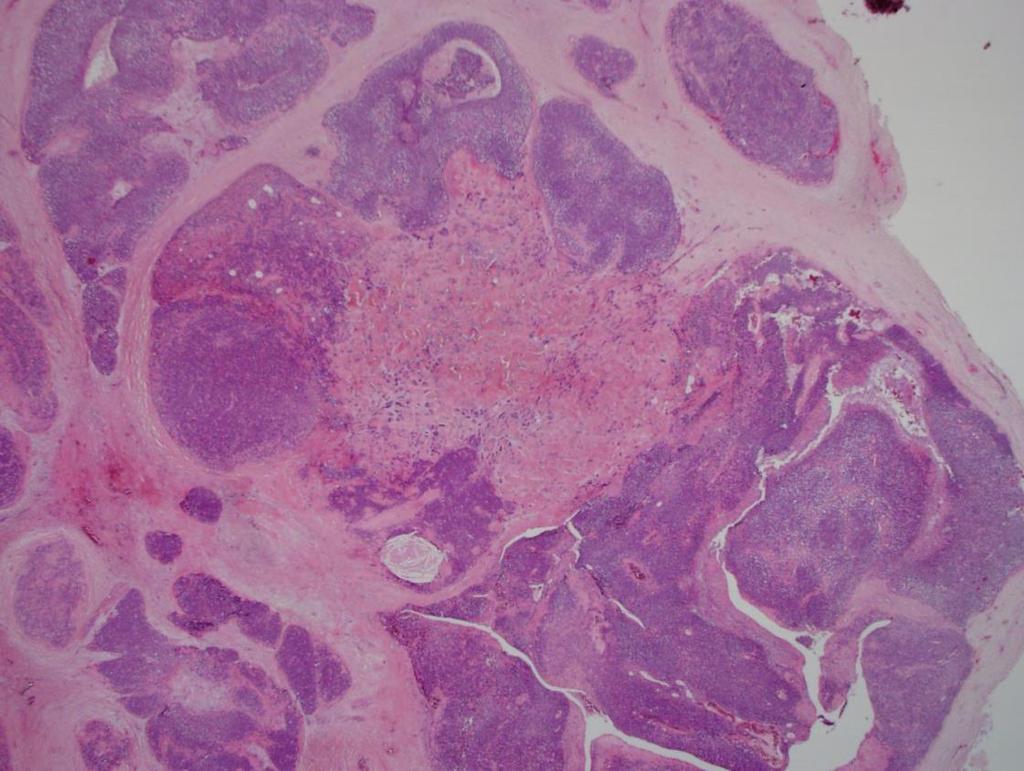
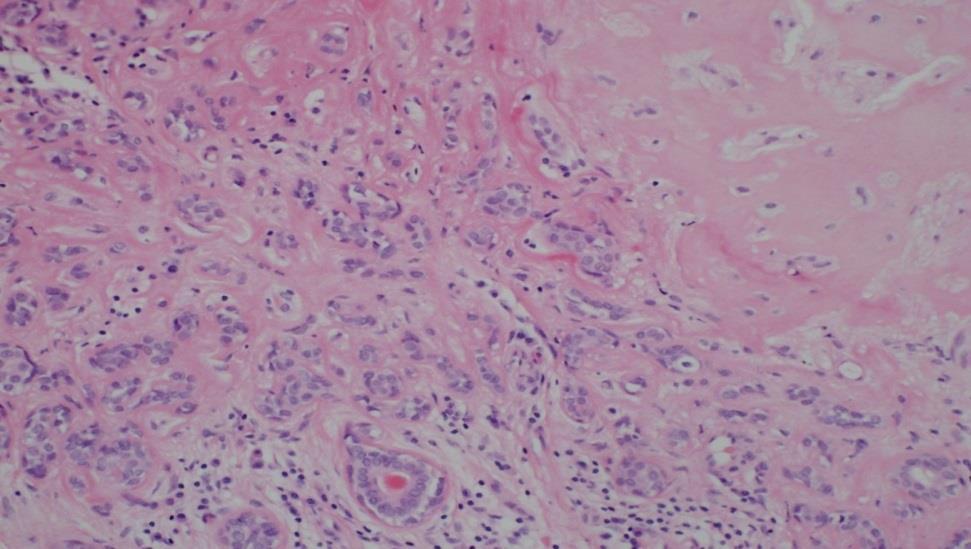
82 Carcinoma ex pleomorphic adenoma About 12% (7-27%) of all salivary carcinomas Often change in pre existing mass Grossly sclerotic nodule (pre existing PA) within infiltrative tumour
83
84
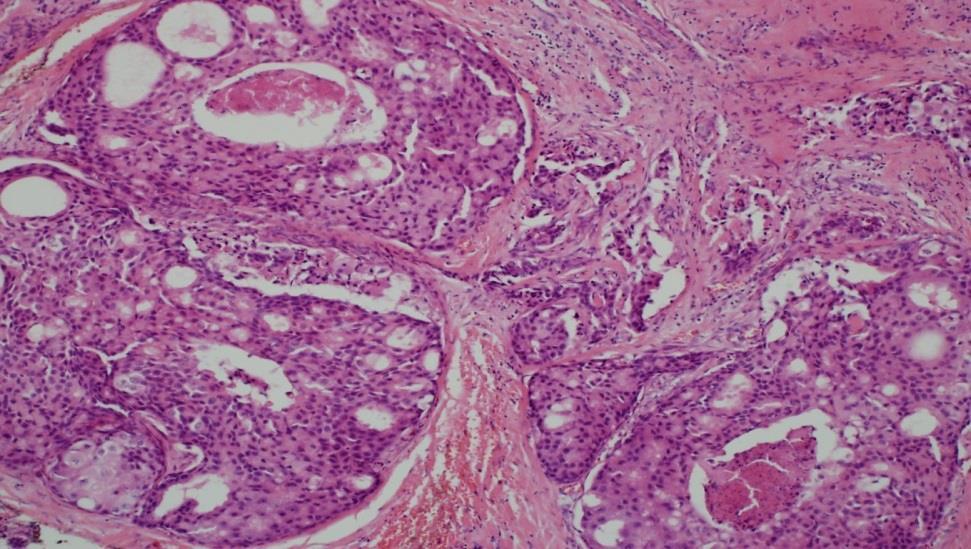
85 Carcinoma ex pleomorphic adenoma 1 -Must identify the subtype of carcinoma Many are salivary duct carcinoma but also less aggressive subtypes
86 Carcinoma ex pleomorphic adenoma 2- identify extent Intracapsular: abnormal proliferation within/ between ducts in PA, capsule not breached Minimally invasive: breach of capsule by carcinoma, measurable in mm unclear what cut off is associated with good prognosis - previously 1.5mm but possibly 4-6mm Widely invasive: extensive invasion outside capsule, may be hard to find PA
87

88 Carcinoma ex pleomorphic adenoma
89
90

91 Tumour nodules
92 58 year old male FNA neck mass Poorly differentiated carcinoma p16 antibody positive No primary Treated as p16 positive metastatic squamous carcinoma with unknown primary
93
94 p16
95 Metastasising pleomorphic adenoma Histologically identical to PA but metastases: regional or distant Arises after multiple recurrences Spreads to lung and bone 40% die of disease previously under malignant category now under benign Still considered biologically aggressive
96 Summary Secretory carcinoma Polymorphous adenocarcinoma (combined PLGA and CAMSG) More definition required in carcinoma ex PA Increasing molecular signatures: secretory, adenoid cystic, mucoepidermoid, clear cell carcinoma Grading in mucoepidermoid remains a problem
97

98

99
WHO 2017: New Classification of Head and Neck Tumours
 WHO 2017: New Classification of Head and Neck Tumours Ilmo Leivo Department of Pathology University of Turku & Turku University Hospital FINLAND Suomen IAP Aulanko 18.05.2018 WHO 2017 New entities Simplification
WHO 2017: New Classification of Head and Neck Tumours Ilmo Leivo Department of Pathology University of Turku & Turku University Hospital FINLAND Suomen IAP Aulanko 18.05.2018 WHO 2017 New entities Simplification
Update in Salivary Gland Pathology. Benjamin L. Witt University of Utah/ARUP Laboratories February 9, 2016
 Update in Salivary Gland Pathology Benjamin L. Witt University of Utah/ARUP Laboratories February 9, 2016 Objectives Review the different appearances of a selection of salivary gland tumor types Establish
Update in Salivary Gland Pathology Benjamin L. Witt University of Utah/ARUP Laboratories February 9, 2016 Objectives Review the different appearances of a selection of salivary gland tumor types Establish
Salivary Glands 3/7/2017
 Salivary Glands 3/7/2017 Goals and objectives Focus on the entities unique to H&N Common board type facts Information for your future practice Salivary Glands Salivary Glands Major gland. Paratid. Submandibular.
Salivary Glands 3/7/2017 Goals and objectives Focus on the entities unique to H&N Common board type facts Information for your future practice Salivary Glands Salivary Glands Major gland. Paratid. Submandibular.
04/09/2018. Salivary Gland Pathology in the Molecular Era Old Friends, Old Foes, & New Acquaintances
 Salivary Gland Pathology in the Molecular Era Old Friends, Old Foes, & New Acquaintances Jennifer L. Hunt, MD, MEd Aubrey J. Hough Jr, MD, Endowed Professor of Pathology Chair of Pathology and Laboratory
Salivary Gland Pathology in the Molecular Era Old Friends, Old Foes, & New Acquaintances Jennifer L. Hunt, MD, MEd Aubrey J. Hough Jr, MD, Endowed Professor of Pathology Chair of Pathology and Laboratory
PRELIMINARY CYTOLOGIC DIAGNOSIS: Suspicious for Acinic Cell Carcinoma. Cell Block: Immunohistochemical Studies CYTOLOGIC DIAGNOSIS:
 1 PRELIMINARY CYTOLOGIC DIAGNOSIS: Suspicious for Acinic Cell Carcinoma. Cell Block: Immunohistochemical Studies GCDFP-15 S-100 CYTOLOGIC DIAGNOSIS: Consistent with mammary analogue secretory carcinoma.
1 PRELIMINARY CYTOLOGIC DIAGNOSIS: Suspicious for Acinic Cell Carcinoma. Cell Block: Immunohistochemical Studies GCDFP-15 S-100 CYTOLOGIC DIAGNOSIS: Consistent with mammary analogue secretory carcinoma.
Oncocytic-Appearing Salivary Gland Tumors. Oncocytic, Cystic, Mucinous, and High Grade Salivary Gland Tumors SALIVARY GLAND FNA: PART II
 William C. Faquin, MD, PhD Professor of Pathology Harvard Medical School Director of Head and Neck Pathology Massachusetts Eye and Ear Massachusetts General Hospital SALIVARY GLAND FNA: PART II Oncocytic,
William C. Faquin, MD, PhD Professor of Pathology Harvard Medical School Director of Head and Neck Pathology Massachusetts Eye and Ear Massachusetts General Hospital SALIVARY GLAND FNA: PART II Oncocytic,
Mammary analogue secretory carcinoma of salivary gland A case report of new entity
 Case Report Mammary analogue secretory carcinoma of salivary gland A case report of new entity Vaibhav Bhika Bari 1*, Sandhya Unmesh Bholay 2 1 Assistant Professor, 2 Associate Professor Rajiv Gandhi Medical
Case Report Mammary analogue secretory carcinoma of salivary gland A case report of new entity Vaibhav Bhika Bari 1*, Sandhya Unmesh Bholay 2 1 Assistant Professor, 2 Associate Professor Rajiv Gandhi Medical
Molecular Diagnostics of Head and Neck Tumors Justin A. Bishop, M.D. Associate Professor of Pathology The Johns Hopkins University Baltimore, Maryland
 Molecular Diagnostics of Head and Neck Tumors Justin A. Bishop, M.D. Associate Professor of Pathology The Johns Hopkins University Baltimore, Maryland Two Main Topics Molecular insights in salivary gland
Molecular Diagnostics of Head and Neck Tumors Justin A. Bishop, M.D. Associate Professor of Pathology The Johns Hopkins University Baltimore, Maryland Two Main Topics Molecular insights in salivary gland
Review and Updates of Immunohistochemistry in Selected Salivary Gland and Head and Neck Tumors
 Review and Updates of Immunohistochemistry in Selected Salivary Gland and Head and Neck Tumors. Monophasic tumors : myoepithelioma, acinic cell carcinoma, and salivary duct carcinoma. Biphasic tumors includes
Review and Updates of Immunohistochemistry in Selected Salivary Gland and Head and Neck Tumors. Monophasic tumors : myoepithelioma, acinic cell carcinoma, and salivary duct carcinoma. Biphasic tumors includes
Salivary Gland Neoplasms. Napa Valley Pathology Conference Silverado Resort & Spa May 18, /22/2018. Salivary Gland Neoplasms Outline
 Salivary Gland Neoplasms Napa Valley Pathology Conference Silverado Resort & Spa May 18, 2018 Bruce M. Wenig, MD Moffitt Cancer Center Tampa, FL Salivary Gland Neoplasms Outline Basic concepts of salivary
Salivary Gland Neoplasms Napa Valley Pathology Conference Silverado Resort & Spa May 18, 2018 Bruce M. Wenig, MD Moffitt Cancer Center Tampa, FL Salivary Gland Neoplasms Outline Basic concepts of salivary
Objectives. Salivary Gland FNA: The Milan System. Role of Salivary Gland FNA 04/26/2018
 Salivary Gland FNA: The Milan System Dr. Jennifer Brainard Section Head Cytopathology Cleveland Clinic Objectives Introduce the Milan System for reporting salivary gland cytopathology Define cytologic
Salivary Gland FNA: The Milan System Dr. Jennifer Brainard Section Head Cytopathology Cleveland Clinic Objectives Introduce the Milan System for reporting salivary gland cytopathology Define cytologic
Salivary Gland Neoplasms. Salivary Gland Neoplasms Outline 4/16/2018. MUSC Pathology Multi-Specialty Course Kiawah Island, SC April 19, 2018
 Salivary Gland Neoplasms MUSC Pathology Multi-Specialty Course Kiawah Island, SC April 19, 2018 Bruce M. Wenig, MD Moffitt Cancer Center Tampa, FL Salivary Gland Neoplasms Outline Basic concepts of salivary
Salivary Gland Neoplasms MUSC Pathology Multi-Specialty Course Kiawah Island, SC April 19, 2018 Bruce M. Wenig, MD Moffitt Cancer Center Tampa, FL Salivary Gland Neoplasms Outline Basic concepts of salivary
5/22/2017. An Aggressive Nasopharyngeal Tumor. Case History
 An Aggressive Nasopharyngeal Tumor Head & Neck/Endocrine Evening Specialty Conference Martin Bullock, MD, FRCPC Dalhousie University, Halifax, Nova Scotia Case History 52-year-old male, 6 month history
An Aggressive Nasopharyngeal Tumor Head & Neck/Endocrine Evening Specialty Conference Martin Bullock, MD, FRCPC Dalhousie University, Halifax, Nova Scotia Case History 52-year-old male, 6 month history
New/Emerging Entities in Salivary Gland Pathology
 New/Emerging Entities in Salivary Gland Pathology Alena Skalova, MD, PhD Professor of Pathology Charles University, Faculty of Medicine in Plzen, Czech Republic 2018 IAP Congress; Jordan, 14 18 October
New/Emerging Entities in Salivary Gland Pathology Alena Skalova, MD, PhD Professor of Pathology Charles University, Faculty of Medicine in Plzen, Czech Republic 2018 IAP Congress; Jordan, 14 18 October
Lesions Mimicking Adenoid Cystic Carcinoma. Diagnostic Problems in Salivary Gland Pathology An Update 5/29/2009
 Diagnostic Problems in Salivary Gland Pathology An Update Lesions Mimicking Adenoid Cystic Carcinoma Stacey E. Mills, M.D. W.S. Royster Professor of Pathology Director of Surgical and Cytopathology University
Diagnostic Problems in Salivary Gland Pathology An Update Lesions Mimicking Adenoid Cystic Carcinoma Stacey E. Mills, M.D. W.S. Royster Professor of Pathology Director of Surgical and Cytopathology University
4/17/2015. Case 1. A 37 year old man with a 2.2 cm solitary left thyroid mass.
 Case 1 A 37 year old man with a 2.2 cm solitary left thyroid mass. Case 1 Case 1 1 Case 1: Diagnosis? A. Benign B. Atypia of undetermined significance/follicular lesion of undetermined significance C.
Case 1 A 37 year old man with a 2.2 cm solitary left thyroid mass. Case 1 Case 1 1 Case 1: Diagnosis? A. Benign B. Atypia of undetermined significance/follicular lesion of undetermined significance C.
Los Angeles Society Of Pathologists Dr. Shobha Castelino Prabhu
 Los Angeles Society Of Pathologists Dr. Shobha Castelino Prabhu Loma Linda University Medical Center June 12, 2007 CASE 1 76 year-old gentleman Status post right parotidectomy 1 year ago for a rare tumor
Los Angeles Society Of Pathologists Dr. Shobha Castelino Prabhu Loma Linda University Medical Center June 12, 2007 CASE 1 76 year-old gentleman Status post right parotidectomy 1 year ago for a rare tumor
Salivary Gland FNA ATYPICAL : Criteria and Controversies
 Salivary Gland FNA ATYPICAL : Criteria and Controversies W.C. Faquin, M.D., Ph.D. Director, Head and Neck Pathology Massachusetts General Hospital Massachusetts Eye and Ear Infirmary Harvard Medical School
Salivary Gland FNA ATYPICAL : Criteria and Controversies W.C. Faquin, M.D., Ph.D. Director, Head and Neck Pathology Massachusetts General Hospital Massachusetts Eye and Ear Infirmary Harvard Medical School
Enterprise Interest None
 Enterprise Interest None What are triple negative breast cancers? A synopsis of their histological patterns Ian Ellis Molecular Medical Sciences, University of Nottingham Department of Histopathology,
Enterprise Interest None What are triple negative breast cancers? A synopsis of their histological patterns Ian Ellis Molecular Medical Sciences, University of Nottingham Department of Histopathology,
ARIZONA SOCIETY OF PATHOLOGISTS 13 TH APRIL 2013 HEAD AND NECK CYTOPATHOLOGY. F ZAHRA ALY, MD, PhD
 ARIZONA SOCIETY OF PATHOLOGISTS 13 TH APRIL 2013 HEAD AND NECK CYTOPATHOLOGY F ZAHRA ALY, MD, PhD The main areas sites amenable for cytopathology include lymph nodes, thyroid, major salivary glands especially
ARIZONA SOCIETY OF PATHOLOGISTS 13 TH APRIL 2013 HEAD AND NECK CYTOPATHOLOGY F ZAHRA ALY, MD, PhD The main areas sites amenable for cytopathology include lymph nodes, thyroid, major salivary glands especially
My Journey into the World of Salivary Gland Sebaceous Neoplasms
 My Journey into the World of Salivary Gland Sebaceous Neoplasms Douglas R. Gnepp Warren Alpert Medical School at Brown University Rhode Island Hospital Pathology Department Providence RI Asked to present
My Journey into the World of Salivary Gland Sebaceous Neoplasms Douglas R. Gnepp Warren Alpert Medical School at Brown University Rhode Island Hospital Pathology Department Providence RI Asked to present
Papillary Lesions of the breast
 Papillary Lesions of the breast Emad Rakha Professor of Breast Pathology The University of Nottingham Papillary lesions of the breast are a heterogeneous group of disease, which are characterised by neoplastic
Papillary Lesions of the breast Emad Rakha Professor of Breast Pathology The University of Nottingham Papillary lesions of the breast are a heterogeneous group of disease, which are characterised by neoplastic
Notice of Faculty Disclosure
 California Society of Pathology Diagnostic Problems in Surgical Pathology December 2015 Case 2 Laura C. Collins, M.D. Associate Professor of Pathology Associate Director of Anatomic Pathology Beth Israel
California Society of Pathology Diagnostic Problems in Surgical Pathology December 2015 Case 2 Laura C. Collins, M.D. Associate Professor of Pathology Associate Director of Anatomic Pathology Beth Israel
Carcinoma mammario: le istologie non frequenti. Valentina Guarneri Università di Padova IOV-IRCCS
 Carcinoma mammario: le istologie non frequenti Valentina Guarneri Università di Padova IOV-IRCCS Histological diversity of breast adenocarcinomas Different histological types are defined according to specific
Carcinoma mammario: le istologie non frequenti Valentina Guarneri Università di Padova IOV-IRCCS Histological diversity of breast adenocarcinomas Different histological types are defined according to specific
USCAP 2012: Companion Meeting of the AAOOP. Update on lacrimal gland neoplasms: Molecular pathology of interest
 USCAP 2012: Companion Meeting of the AAOOP Vancouver BC, Canada, March 17, 2012 Update on lacrimal gland neoplasms: Molecular pathology of interest Valerie A. White MD, MHSc, FRCPC Department of Pathology
USCAP 2012: Companion Meeting of the AAOOP Vancouver BC, Canada, March 17, 2012 Update on lacrimal gland neoplasms: Molecular pathology of interest Valerie A. White MD, MHSc, FRCPC Department of Pathology
Evening Specialty Conference: Cytopathology
 : Cytopathology N. Paul Ohori, M.D. University of Pittsburgh Medical Center Disclosure of Relevant Financial Relationships Disclosure of Relevant Financial Relationships USCAP requires that all planners
: Cytopathology N. Paul Ohori, M.D. University of Pittsburgh Medical Center Disclosure of Relevant Financial Relationships Disclosure of Relevant Financial Relationships USCAP requires that all planners
Fine-Needle Aspiration Cytology of Low-Grade Cribriform Cystadenocarcinoma with Many Psammoma Bodies of the Salivary Gland
 The Korean Journal of Pathology 2013; 47: 481-485 CASE STUDY Fine-Needle Aspiration Cytology of Low-Grade Cribriform Cystadenocarcinoma with Many Psammoma Bodies of the Salivary Gland Ji Yun Jeong Dongbin
The Korean Journal of Pathology 2013; 47: 481-485 CASE STUDY Fine-Needle Aspiration Cytology of Low-Grade Cribriform Cystadenocarcinoma with Many Psammoma Bodies of the Salivary Gland Ji Yun Jeong Dongbin
Differential Diagnosis of Oral Masses. Palatal Lesions
 Differential Diagnosis of Oral Masses Palatal Lesions Palatal Masses Periapical Abscess Torus Palatinus Mucocele Lymphoid Hyperplasia Adenomatous Hyperplasia Benign Salivary Neoplasms Malignant Salivary
Differential Diagnosis of Oral Masses Palatal Lesions Palatal Masses Periapical Abscess Torus Palatinus Mucocele Lymphoid Hyperplasia Adenomatous Hyperplasia Benign Salivary Neoplasms Malignant Salivary
WHO classification salivary tumours: What's new?
 WHO classification salivary tumours: What's new? Alena Skalova, MD, PhD Professor of Pathology Charles University, Faculty of Medicine in Plzen, Czech Republic An update on Histopathology of Salivary Gland
WHO classification salivary tumours: What's new? Alena Skalova, MD, PhD Professor of Pathology Charles University, Faculty of Medicine in Plzen, Czech Republic An update on Histopathology of Salivary Gland
DISCUSSION: PLGA accounts for about 2% of all salivary gland tumours and occurs almost exclusively in the minor salivary glands.
 SWELLING ON THE HARD PALATE PRESENTING AS POLYMORPHOUS LOW GRADE ADENOCARCINOMA: A AND REVIEW OF LITERATURE Swapnil D. Chandekar 1, Sunita S. Dantkale 2, Rahul R. Narkhede 3, Snehal V. Chavhan 4, Khushboo
SWELLING ON THE HARD PALATE PRESENTING AS POLYMORPHOUS LOW GRADE ADENOCARCINOMA: A AND REVIEW OF LITERATURE Swapnil D. Chandekar 1, Sunita S. Dantkale 2, Rahul R. Narkhede 3, Snehal V. Chavhan 4, Khushboo
Salivary Gland Cytology
 Salivary Gland Cytology Diagnostic challenges and potential pitfalls Tarik M. Elsheikh, MD Professor and Medical Director Anatomic Pathology Cleveland Clinic FNA Salivary Gland Lesions Indications Distinguish
Salivary Gland Cytology Diagnostic challenges and potential pitfalls Tarik M. Elsheikh, MD Professor and Medical Director Anatomic Pathology Cleveland Clinic FNA Salivary Gland Lesions Indications Distinguish
Educational Cases EQA November T.J. Palmer Raigmore Hospital Inverness
 Educational Cases EQA November 2013 T.J. Palmer Raigmore Hospital Inverness Case 2 Clinical Details Dob 11 February 1951 PMH: 1964 Extraction of 45 aet 13 yr 1966 Cyst between 44 and 46 enucleated 1973
Educational Cases EQA November 2013 T.J. Palmer Raigmore Hospital Inverness Case 2 Clinical Details Dob 11 February 1951 PMH: 1964 Extraction of 45 aet 13 yr 1966 Cyst between 44 and 46 enucleated 1973
POLYMORPHOUS LOW GRADE ADENOCARCINOMA - CASE REPORT AND REVIEW OF LITERATURE
 POLYMORPHOUS LOW GRADE ADENOCARCINOMA - CASE REPORT AND REVIEW OF LITERATURE S.Sunil 1 B.S. Sreenivasan 2 Jisha Titus 3 Soma Susan 4 Jubin Thomas 4 Antony George 4 Devi Gopakumar 5 1 Reader, 2 Professor,
POLYMORPHOUS LOW GRADE ADENOCARCINOMA - CASE REPORT AND REVIEW OF LITERATURE S.Sunil 1 B.S. Sreenivasan 2 Jisha Titus 3 Soma Susan 4 Jubin Thomas 4 Antony George 4 Devi Gopakumar 5 1 Reader, 2 Professor,
Salivary gland tumor cytologic and histologic correlation: Algorithmic and risk stratification based approaches
 Salivary gland tumor cytologic and histologic correlation: Algorithmic and risk stratification based approaches Christopher C. Griffith, MD, PhD Raja R. Seethala, MD 1. Salivary gland tumor cytology: A
Salivary gland tumor cytologic and histologic correlation: Algorithmic and risk stratification based approaches Christopher C. Griffith, MD, PhD Raja R. Seethala, MD 1. Salivary gland tumor cytology: A
AGGRESSIVE VARIANTS OF PAPILLARY THYROID CARCINOMA DIAGNOSIS AND PROGNOSIS
 AGGRESSIVE VARIANTS OF PAPILLARY THYROID CARCINOMA DIAGNOSIS AND PROGNOSIS PAPILLARY THYROID CARCINOMA Clinical Any age Microscopic to large Female: Male= 2-4:1 Radiation history Lymph nodes Prognosis
AGGRESSIVE VARIANTS OF PAPILLARY THYROID CARCINOMA DIAGNOSIS AND PROGNOSIS PAPILLARY THYROID CARCINOMA Clinical Any age Microscopic to large Female: Male= 2-4:1 Radiation history Lymph nodes Prognosis
Basaloid neoplasms of the head and neck. Basaloid SCC. Clinico-pathologic features 5/5/11. Basaloid Tumors Head and Neck
 Basaloid neoplasms of the head and neck Richard Jordan DDS PhD FRCPath Professor & Director UCSF Oral Pathology Laboratory University of California San Francisco Basaloid Tumors Head and Neck Basaloid
Basaloid neoplasms of the head and neck Richard Jordan DDS PhD FRCPath Professor & Director UCSF Oral Pathology Laboratory University of California San Francisco Basaloid Tumors Head and Neck Basaloid
A 60-year old Man with Left Jaw Mass. Simon Chiosea, MD University of Pittsburgh medical Center 3/15/2016
 ACCME/Disclosures The USCAP requires that anyone in a position to influence or control the content of CME disclose any relevant financial relationship WITH COMMERCIAL INTERESTS which they or their spouse/partner
ACCME/Disclosures The USCAP requires that anyone in a position to influence or control the content of CME disclose any relevant financial relationship WITH COMMERCIAL INTERESTS which they or their spouse/partner
Rare Breast Tumours. 1. Breast Tumours. 1.1 General Results. 1.2 Incidence
 Rare Breast Tumours 1. Breast Tumours 1.1 General Results Table 1. Epithelial Tumours of Breast: Incidence, Trends, Survival Flemish Region 2001-2010 Incidence Trend Survival Females EAPC Relative survival
Rare Breast Tumours 1. Breast Tumours 1.1 General Results Table 1. Epithelial Tumours of Breast: Incidence, Trends, Survival Flemish Region 2001-2010 Incidence Trend Survival Females EAPC Relative survival
Diagnostically relevant molecular alterations in salivary glandtumours
 Diagnostically relevant molecular alterations in salivary glandtumours Alena Skalova, MD, PhD Professor of Pathology Charles University, Faculty of Medicine in Plzen, Czech Republic An update on Histopathology
Diagnostically relevant molecular alterations in salivary glandtumours Alena Skalova, MD, PhD Professor of Pathology Charles University, Faculty of Medicine in Plzen, Czech Republic An update on Histopathology
Polymorphous Low-Grade. December 5 th, 2008
 Polymorphous Low-Grade Adenocarcinoma December 5 th, 2008 Epidemiology Represents 2 nd or 3 rd most common minor salivary gland malignancy (17-26%) 1 st mucoepidermoid carcinoma Rare in reported Asian
Polymorphous Low-Grade Adenocarcinoma December 5 th, 2008 Epidemiology Represents 2 nd or 3 rd most common minor salivary gland malignancy (17-26%) 1 st mucoepidermoid carcinoma Rare in reported Asian
Papillary Lesions of the Breast A Practical Approach to Diagnosis. (Arch Pathol Lab Med. 2016;140: ; doi: /arpa.
 Papillary Lesions of the Breast A Practical Approach to Diagnosis (Arch Pathol Lab Med. 2016;140:1052 1059; doi: 10.5858/arpa.2016-0219-RA) Papillary lesions of the breast Span the spectrum of benign,
Papillary Lesions of the Breast A Practical Approach to Diagnosis (Arch Pathol Lab Med. 2016;140:1052 1059; doi: 10.5858/arpa.2016-0219-RA) Papillary lesions of the breast Span the spectrum of benign,
Basement membrane in lobule.
 Bahram Memar, MD Basement membrane in lobule. Normal lobule-luteal phase Normal lobule-follicular phase Lactating breast Greater than 95% are adenocarcinomas in situ carcinomas and invasive carcinomas.
Bahram Memar, MD Basement membrane in lobule. Normal lobule-luteal phase Normal lobule-follicular phase Lactating breast Greater than 95% are adenocarcinomas in situ carcinomas and invasive carcinomas.
DIAGNOSTIC SLIDE SEMINAR: PART 1 RENAL TUMOUR BIOPSY CASES
 DIAGNOSTIC SLIDE SEMINAR: PART 1 RENAL TUMOUR BIOPSY CASES Dr. Andrew J. Evans MD, PhD, FACP, FRCPC Consultant in Genitourinary Pathology University Health Network, Toronto, ON Case 1 43 year-old female,
DIAGNOSTIC SLIDE SEMINAR: PART 1 RENAL TUMOUR BIOPSY CASES Dr. Andrew J. Evans MD, PhD, FACP, FRCPC Consultant in Genitourinary Pathology University Health Network, Toronto, ON Case 1 43 year-old female,
FNA OF SALIVARY GLANDS: A PRACTICAL APPROACH
 FNA OF SALIVARY GLANDS: A PRACTICAL APPROACH FNA of Salivary Glands: Challenges Wide range of neoplastic and non-neoplastic lesions Cytological overlap between the different benign and malignant tumors
FNA OF SALIVARY GLANDS: A PRACTICAL APPROACH FNA of Salivary Glands: Challenges Wide range of neoplastic and non-neoplastic lesions Cytological overlap between the different benign and malignant tumors
Case year old female presented with asymmetric enlargement of the left lobe of the thyroid
 Case 4 22 year old female presented with asymmetric enlargement of the left lobe of the thyroid gland. No information available relative to a prior fine needle aspiration biopsy. A left lobectomy was performed.
Case 4 22 year old female presented with asymmetric enlargement of the left lobe of the thyroid gland. No information available relative to a prior fine needle aspiration biopsy. A left lobectomy was performed.
Salivary gland carcinomas-update
 Salivary gland carcinomas-update Alena Skalova, MD, PhD Professor of Pathology Charles University, Faculty of Medicine in Plzen, Czech Republic An update on Histopathology of Salivary Gland Tumors, La
Salivary gland carcinomas-update Alena Skalova, MD, PhD Professor of Pathology Charles University, Faculty of Medicine in Plzen, Czech Republic An update on Histopathology of Salivary Gland Tumors, La
Case 4 Diagnosis 2/21/2011 TGB
 Case 4 22 year old female presented with asymmetric enlargement of the left lobe of the thyroid gland. No information available relative to a prior fine needle aspiration biopsy. A left lobectomy was performed.
Case 4 22 year old female presented with asymmetric enlargement of the left lobe of the thyroid gland. No information available relative to a prior fine needle aspiration biopsy. A left lobectomy was performed.
04/10/2018. Intraductal Papillary Neoplasms Of Breast INTRADUCTAL PAPILLOMA
 Intraductal Papillary Neoplasms Of Breast Savitri Krishnamurthy MD Professor of Pathology Deputy Division Head The University of Texas MD Anderson Cancer Center 25 th Annual Seminar in Pathology Pittsburgh,
Intraductal Papillary Neoplasms Of Breast Savitri Krishnamurthy MD Professor of Pathology Deputy Division Head The University of Texas MD Anderson Cancer Center 25 th Annual Seminar in Pathology Pittsburgh,
Disclosure of Relevant Financial Relationships
 Squamous entities of the thyroid: Reactive to Neoplastic Michelle D. Williams Associate Professor Dept of Pathology, Head & Neck Section University of Texas MD Anderson Cancer Center Disclosure of Relevant
Squamous entities of the thyroid: Reactive to Neoplastic Michelle D. Williams Associate Professor Dept of Pathology, Head & Neck Section University of Texas MD Anderson Cancer Center Disclosure of Relevant
An Update on Grading of Salivary Gland Carcinomas
 Head and Neck Pathol (2009) 3:69 77 DOI 10.1007/s12105-009-0102-9 PROCEEDINGS OF THE 2009 NORTH AMERICAN SOCIETY OF HEAD AND NECK PATHOLOGY COMPANION MEETING ( BOSTON, MA) An Update on Grading of Salivary
Head and Neck Pathol (2009) 3:69 77 DOI 10.1007/s12105-009-0102-9 PROCEEDINGS OF THE 2009 NORTH AMERICAN SOCIETY OF HEAD AND NECK PATHOLOGY COMPANION MEETING ( BOSTON, MA) An Update on Grading of Salivary
Slide seminar. Asist. Prof. Jože Pižem, MD, PhD Institute of Pathology Medical Faculty, University of Ljubljana
 Slide seminar Asist. Prof. Jože Pižem, MD, PhD Institute of Pathology Medical Faculty, University of Ljubljana Case 5 A 57-year-old man with a dermal/subcutaneous lesion on the scalp, which was interpreted
Slide seminar Asist. Prof. Jože Pižem, MD, PhD Institute of Pathology Medical Faculty, University of Ljubljana Case 5 A 57-year-old man with a dermal/subcutaneous lesion on the scalp, which was interpreted
PLEOMORPHIC ADENOMA ( BENIGN MIXED TUMOR )
") ( BENIGN MIXED TUMOR ) Grossly, the tumor is freely movable, solid, sometimes lobulated and occasionally cystic. If recurrent, multinodular masses are common. Histologically, within a fibrous capsule,
( BENIGN MIXED TUMOR ) Grossly, the tumor is freely movable, solid, sometimes lobulated and occasionally cystic. If recurrent, multinodular masses are common. Histologically, within a fibrous capsule,
See the latest estimates for new cases of salivary gland cancers in the US and what research is currently being done.
 About Salivary Gland Cancer Overview and Types If you have been diagnosed with salivary gland cancer or are worried about it, you likely have a lot of questions. Learning some basics is a good place to
About Salivary Gland Cancer Overview and Types If you have been diagnosed with salivary gland cancer or are worried about it, you likely have a lot of questions. Learning some basics is a good place to
(CYLINDROMA) ATLAS OF HEAD AND NECK PATHOLOGY ADENOID CYSTIC CARCINOMA
 ATLAS OF HEAD AND NECK PATHOLOGY ADENOID CYSTIC CARCINOMA") (CYLINDROMA) This malignant tumor is poorly encapsulated and while seemingly well defined within the affected gland, there is usually infiltration of surrounding tissue on closer examination. The cut surface
(CYLINDROMA) This malignant tumor is poorly encapsulated and while seemingly well defined within the affected gland, there is usually infiltration of surrounding tissue on closer examination. The cut surface
EQA Circulation 43 Educational Cases
 EQA Circulation 43 Educational Cases E1-E2 Monica Agarwal Monklands Hospital E1 38 yrs male Submandibular gland tumour E1 Formal excision following diagnosis of poorly differentiated carcinoma on core
EQA Circulation 43 Educational Cases E1-E2 Monica Agarwal Monklands Hospital E1 38 yrs male Submandibular gland tumour E1 Formal excision following diagnosis of poorly differentiated carcinoma on core
Case 1. ACCME/Disclosure. Clinical History. Dr. Mulligan has nothing to disclose
 Breast Evening Specialty Conference USCAP, 2016 Case 1 Anna Marie Mulligan University Health Network, Toronto University of Toronto ACCME/Disclosure Dr. Mulligan has nothing to disclose Clinical History
Breast Evening Specialty Conference USCAP, 2016 Case 1 Anna Marie Mulligan University Health Network, Toronto University of Toronto ACCME/Disclosure Dr. Mulligan has nothing to disclose Clinical History
DISORDERS OF THE SALIVARY GLANDS Neoplasms Dr.M.Baskaran Selvapathy S IV
 DISORDERS OF THE SALIVARY GLANDS Neoplasms Dr.M.Baskaran Selvapathy S IV NEOPLASMS A) Epithelial I. Benign Pleomorphic adenoma( Mixed tumour) Adenolymphoma (Warthin s tumour) Oxyphil adenoma (Oncocytoma)
DISORDERS OF THE SALIVARY GLANDS Neoplasms Dr.M.Baskaran Selvapathy S IV NEOPLASMS A) Epithelial I. Benign Pleomorphic adenoma( Mixed tumour) Adenolymphoma (Warthin s tumour) Oxyphil adenoma (Oncocytoma)
Papillary Lesions of the Breast
 Papillary Lesions of the Breast Laura C. Collins, M.D. Associate Professor of Pathology Associate Director, Division of Anatomic Pathology Beth Israel Deaconess Medical Center and Harvard Medical School
Papillary Lesions of the Breast Laura C. Collins, M.D. Associate Professor of Pathology Associate Director, Division of Anatomic Pathology Beth Israel Deaconess Medical Center and Harvard Medical School
Oncocytic carcinoma: A rare malignancy of the parotid gland
 ISPUB.COM The Internet Journal of Pathology Volume 8 Number 2 Oncocytic carcinoma: A rare malignancy of the parotid gland K Mardi, J Sharma Citation K Mardi, J Sharma.. The Internet Journal of Pathology.
ISPUB.COM The Internet Journal of Pathology Volume 8 Number 2 Oncocytic carcinoma: A rare malignancy of the parotid gland K Mardi, J Sharma Citation K Mardi, J Sharma.. The Internet Journal of Pathology.
They Do Look Alike : Mimics of Prostate Cancer in Biopsy Samples
 They Do Look Alike : in Biopsy Samples Gladell P. Paner, MD Departments of Pathology and Surgery (Urology) University of Chicago, IL USA Gladell.paner@uchospitals.edu Benign in Needle Biopsy 1. Benign
They Do Look Alike : in Biopsy Samples Gladell P. Paner, MD Departments of Pathology and Surgery (Urology) University of Chicago, IL USA Gladell.paner@uchospitals.edu Benign in Needle Biopsy 1. Benign
Ductal Carcinoma in Situ. Laura C. Collins, M.D. Department of Pathology Beth Israel Deaconess Medical Center and Harvard Medical School Boston, MA
 Ductal Carcinoma in Situ Laura C. Collins, M.D. Department of Pathology Beth Israel Deaconess Medical Center and Harvard Medical School Boston, MA Definition of DCIS WHO 2012 A neoplastic proliferation
Ductal Carcinoma in Situ Laura C. Collins, M.D. Department of Pathology Beth Israel Deaconess Medical Center and Harvard Medical School Boston, MA Definition of DCIS WHO 2012 A neoplastic proliferation
Salivary Duct Carcinoma: An Update on Morphologic Mimics and Diagnostic Use of Androgen Receptor Immunohistochemistry
 Manuscript Click here to view linked References 1 1 1 1 1 1 1 1 1 0 1 0 1 0 1 0 1 0 1 Click here to download Manuscript Salivary Duct Carcinoma.docx Salivary Duct Carcinoma: An Update on Morphologic Mimics
Manuscript Click here to view linked References 1 1 1 1 1 1 1 1 1 0 1 0 1 0 1 0 1 0 1 Click here to download Manuscript Salivary Duct Carcinoma.docx Salivary Duct Carcinoma: An Update on Morphologic Mimics
3/28/2017. Head and Neck/Endocrine Pathology Specialty Conference Case 4 Raja R. Seethala, M.D. University of Pittsburgh Medical Center
 Head and Neck/Endocrine Pathology Specialty Conference Case 4 Raja R. Seethala, M.D. University of Pittsburgh Medical Center Disclosure of Relevant Financial Relationships Disclosure of Relevant Financial
Head and Neck/Endocrine Pathology Specialty Conference Case 4 Raja R. Seethala, M.D. University of Pittsburgh Medical Center Disclosure of Relevant Financial Relationships Disclosure of Relevant Financial
Gross appearance of nodular hyperplasia in material obtained from suprapubic prostatectomy. Note the multinodular appearance and the admixture of
 Tiền liệt tuyến Tiền liệt tuyến Gross appearance of nodular hyperplasia in material obtained from suprapubic prostatectomy. Note the multinodular appearance and the admixture of solid and microcystic areas.
Tiền liệt tuyến Tiền liệt tuyến Gross appearance of nodular hyperplasia in material obtained from suprapubic prostatectomy. Note the multinodular appearance and the admixture of solid and microcystic areas.
Pitfalls in thyroid tumor pathology. Prof.Valdi Pešutić-Pisac MD, PhD
 Pitfalls in thyroid tumor pathology Prof.Valdi Pešutić-Pisac MD, PhD Too many or... Tumour herniation through a torn capsule simulating capsular invasion fibrous capsule with a sharp discontinuity, suggestive
Pitfalls in thyroid tumor pathology Prof.Valdi Pešutić-Pisac MD, PhD Too many or... Tumour herniation through a torn capsule simulating capsular invasion fibrous capsule with a sharp discontinuity, suggestive
Urinary Bladder: WHO Classification and AJCC Staging Update 2017
 Urinary Bladder: WHO Classification and AJCC Staging Update 2017 Houston Society of Clinical Pathologists 58 th Annual Spring Symposium Houston, TX April 8, 2017 Jesse K. McKenney, MD Classification
Urinary Bladder: WHO Classification and AJCC Staging Update 2017 Houston Society of Clinical Pathologists 58 th Annual Spring Symposium Houston, TX April 8, 2017 Jesse K. McKenney, MD Classification
PROSTATIC ADENOCARCINOMA: DIAGNOSTIC CRITERIA AND IMPORTANT MIMICKERS PROSTATIC ADENOCARCINOMA: DIAGNOSTIC CRITERIA
 PROSTATIC ADENOCARCINOMA: DIAGNOSTIC CRITERIA AND IMPORTANT MIMICKERS PROSTATIC ADENOCARCINOMA: DIAGNOSTIC CRITERIA 1 A good H & E helps! ADENOCARCINOMA DIAGNOSTIC CRITERIA Relatively uniform proliferation
PROSTATIC ADENOCARCINOMA: DIAGNOSTIC CRITERIA AND IMPORTANT MIMICKERS PROSTATIC ADENOCARCINOMA: DIAGNOSTIC CRITERIA 1 A good H & E helps! ADENOCARCINOMA DIAGNOSTIC CRITERIA Relatively uniform proliferation
Papillary Lesions of the Breast: WHO Update
 Papillary Lesions of the Breast: WHO Update Stuart J. Schnitt, M.D. Department of Pathology Beth Israel Deaconess Medical Center and Harvard Medical School Boston, MA, USA Papillary Lesions of the Breast
Papillary Lesions of the Breast: WHO Update Stuart J. Schnitt, M.D. Department of Pathology Beth Israel Deaconess Medical Center and Harvard Medical School Boston, MA, USA Papillary Lesions of the Breast
Histological Type. Morphological and Molecular Typing of breast Cancer. Nottingham Tenovus Primary Breast Cancer Study. Survival (%) Ian Ellis
 Ian Ellis") Morphological and Molecular Typing of breast Cancer Ian Ellis Molecular Medical Sciences, University of Nottingham Department of Histopathology, Nottingham University Hospitals NHS Trust Histological Type
Morphological and Molecular Typing of breast Cancer Ian Ellis Molecular Medical Sciences, University of Nottingham Department of Histopathology, Nottingham University Hospitals NHS Trust Histological Type
Diseases of the breast (1 of 2)
") Diseases of the breast (1 of 2) Introduction A histology introduction Normal ducts and lobules of the breast are lined by two layers of cells a layer of luminal cells overlying a second layer of myoepithelial
Diseases of the breast (1 of 2) Introduction A histology introduction Normal ducts and lobules of the breast are lined by two layers of cells a layer of luminal cells overlying a second layer of myoepithelial
Breast pathology. 2nd Department of Pathology Semmelweis University
 Breast pathology 2nd Department of Pathology Semmelweis University Breast pathology - Summary - Benign lesions - Acute mastitis - Plasma cell mastitis / duct ectasia - Fat necrosis - Fibrocystic change/
Breast pathology 2nd Department of Pathology Semmelweis University Breast pathology - Summary - Benign lesions - Acute mastitis - Plasma cell mastitis / duct ectasia - Fat necrosis - Fibrocystic change/
Maram Abdaljaleel, MD Dermatopathologist and Neuropathologist University of Jordan, School of Medicine
 Maram Abdaljaleel, MD Dermatopathologist and Neuropathologist University of Jordan, School of Medicine The most common non-skin malignancy of women 2 nd most common cause of cancer deaths in women, following
Maram Abdaljaleel, MD Dermatopathologist and Neuropathologist University of Jordan, School of Medicine The most common non-skin malignancy of women 2 nd most common cause of cancer deaths in women, following
Recent advances in breast cancers
 Recent advances in breast cancers Breast cancer is a hetrogenous disease due to distinct genetic alterations. Similar morphological subtypes show variation in clinical behaviour especially in response
Recent advances in breast cancers Breast cancer is a hetrogenous disease due to distinct genetic alterations. Similar morphological subtypes show variation in clinical behaviour especially in response
Small Cell Carcinoma ex-pleomorphic Adenoma of the Parotid Gland
 Head and Neck Pathol (2012) 6:502 506 DOI 10.1007/s12105-012-0376-1 CASE REPORT Small Cell Carcinoma ex-pleomorphic Adenoma of the Parotid Gland Ashley Cimino-Mathews Brian M. Lin Steven S. Chang Kofi
Head and Neck Pathol (2012) 6:502 506 DOI 10.1007/s12105-012-0376-1 CASE REPORT Small Cell Carcinoma ex-pleomorphic Adenoma of the Parotid Gland Ashley Cimino-Mathews Brian M. Lin Steven S. Chang Kofi
Mody. AIS vs. Invasive Adenocarcinoma of the Cervix
 Common Problems in Gynecologic Pathology Michael T. Deavers, M.D. Houston Methodist Hospital, Houston, Texas Common Problems in Gynecologic Pathology Adenocarcinoma in-situ (AIS) of the Cervix vs. Invasive
Common Problems in Gynecologic Pathology Michael T. Deavers, M.D. Houston Methodist Hospital, Houston, Texas Common Problems in Gynecologic Pathology Adenocarcinoma in-situ (AIS) of the Cervix vs. Invasive
Salivary Gland Pathology
 IN THE NAME OF GOD Salivary Gland Pathology CHAPTER 11 Dr.kheirandish Oral and maxillofacial pathology Sialadenosis Adenomatoid Hyperplasia of the Minor Salivary Glands Necrotizing Sialometaplasia Pleomorphic
IN THE NAME OF GOD Salivary Gland Pathology CHAPTER 11 Dr.kheirandish Oral and maxillofacial pathology Sialadenosis Adenomatoid Hyperplasia of the Minor Salivary Glands Necrotizing Sialometaplasia Pleomorphic
Pathology of the Thyroid
 Pathology of the Thyroid Thyroid Carcinoma Arising from Follicular Cells 2015-01-19 Prof. Dr. med. Katharina Glatz Pathologie Carcinomas Arising from Follicular Cells Differentiated Carcinoma Papillary
Pathology of the Thyroid Thyroid Carcinoma Arising from Follicular Cells 2015-01-19 Prof. Dr. med. Katharina Glatz Pathologie Carcinomas Arising from Follicular Cells Differentiated Carcinoma Papillary
Salivary gland Workshop Trondheim 31th may 2012
 Salivary gland Workshop Trondheim 31th may 2012 Peter Jebsen cytopathologist Oslo University Hospital Rikshospitalet Anna Bofin ass. Professor St. Olavs Hospital, Trondheim Drying artifacts Lymfocytes
Salivary gland Workshop Trondheim 31th may 2012 Peter Jebsen cytopathologist Oslo University Hospital Rikshospitalet Anna Bofin ass. Professor St. Olavs Hospital, Trondheim Drying artifacts Lymfocytes
Low-grade cribriform cystadenocarcinoma arising from a minor salivary gland: a case report
 145 Journal of Oral Science, Vol. 58, No. 1, 145-149, 2016 Case Report Low-grade cribriform cystadenocarcinoma arising from a minor salivary gland: a case report Masashi Kimura 1), Shinji Mii 2), Shinichi
145 Journal of Oral Science, Vol. 58, No. 1, 145-149, 2016 Case Report Low-grade cribriform cystadenocarcinoma arising from a minor salivary gland: a case report Masashi Kimura 1), Shinji Mii 2), Shinichi
POORLY DIFFERENTIATED, HIGH GRADE AND ANAPLASTIC CARCINOMAS: WHAT IS EVERYONE TALKING ABOUT?
 POORLY DIFFERENTIATED, HIGH GRADE AND ANAPLASTIC CARCINOMAS: WHAT IS EVERYONE TALKING ABOUT? AGGRESSIVE THYROID CANCERS PAPILLARY CARCINOMA CERTAIN SUBTYPES POORLY DIFFERENTIATED CARCINOMA HIGH GRADE DIFFERENTIATED
POORLY DIFFERENTIATED, HIGH GRADE AND ANAPLASTIC CARCINOMAS: WHAT IS EVERYONE TALKING ABOUT? AGGRESSIVE THYROID CANCERS PAPILLARY CARCINOMA CERTAIN SUBTYPES POORLY DIFFERENTIATED CARCINOMA HIGH GRADE DIFFERENTIATED
Proliferative Epithelial lesions of the Breast. Sami Shousha, MD, FRCPath Charing Cross Hospital & Imperial College, London
 Proliferative Epithelial lesions of the Breast Sami Shousha, MD, FRCPath Charing Cross Hospital & Imperial College, London Amman, November2013 Proliferative Epithelial Lesions of the Breast Usual type
Proliferative Epithelial lesions of the Breast Sami Shousha, MD, FRCPath Charing Cross Hospital & Imperial College, London Amman, November2013 Proliferative Epithelial Lesions of the Breast Usual type
XXV Congreso de la Sociedad Española de Anatomía Patológica y División Española de la International Academy of Pathology
 XXV Congreso de la Sociedad Española de Anatomía Patológica y División Española de la International Academy of Pathology NUEVOS FENOTIPOS DEL CÁNCER DE MAMA: NUEVOS PROBLEMAS PARA EL PATÓLOGO? Tienen actualmente
XXV Congreso de la Sociedad Española de Anatomía Patológica y División Española de la International Academy of Pathology NUEVOS FENOTIPOS DEL CÁNCER DE MAMA: NUEVOS PROBLEMAS PARA EL PATÓLOGO? Tienen actualmente
BREAST PATHOLOGY. Fibrocystic Changes
 BREAST PATHOLOGY Lesions of the breast are very common, and they present as palpable, sometimes painful, nodules or masses. Most of these lesions are benign. Breast cancer is the 2 nd most common cause
BREAST PATHOLOGY Lesions of the breast are very common, and they present as palpable, sometimes painful, nodules or masses. Most of these lesions are benign. Breast cancer is the 2 nd most common cause
Journal of International Academy of Forensic Science & Pathology (JIAFP)
") Journal of International Academy of Forensic Science & Pathology (JIAFP) ISSN 2395-0722 MICROCYSTIC ADNEXAL CARCINOMA-A CASE REPORT WITH REVIEW OF LITERATURE Case Report Sulakshana M S 1,Natarajan M 2
Journal of International Academy of Forensic Science & Pathology (JIAFP) ISSN 2395-0722 MICROCYSTIC ADNEXAL CARCINOMA-A CASE REPORT WITH REVIEW OF LITERATURE Case Report Sulakshana M S 1,Natarajan M 2
Neoplasms of the salivary glands account for 2% to 7%
 Update on Selected Salivary Gland Neoplasms Jonathan B. McHugh, MD; Daniel W. Visscher, MD; E. Leon Barnes, MD N Context. Malignancies of the salivary gland are uncommon and account for 0.3% of all malignancies.
Update on Selected Salivary Gland Neoplasms Jonathan B. McHugh, MD; Daniel W. Visscher, MD; E. Leon Barnes, MD N Context. Malignancies of the salivary gland are uncommon and account for 0.3% of all malignancies.
Non Small Cell Lung Cancer Histopathology ד"ר יהודית זנדבנק
 Non Small Cell Lung Cancer Histopathology ד"ר יהודית זנדבנק 26.06.09 Lecture outlines WHO histological classification Macro/Micro assessment Early diagnosis Minimal pathology Main subtypes SCC, AdCa, LCLC
Non Small Cell Lung Cancer Histopathology ד"ר יהודית זנדבנק 26.06.09 Lecture outlines WHO histological classification Macro/Micro assessment Early diagnosis Minimal pathology Main subtypes SCC, AdCa, LCLC
Review of the AP Part II Practical Examination. Dr David Clift Co Chief Examiner
 Review of the AP Part II Practical Examination Dr David Clift Co Chief Examiner General Remarks The part II practical examination involved 15 cases which were presented with sufficient clinical data to
Review of the AP Part II Practical Examination Dr David Clift Co Chief Examiner General Remarks The part II practical examination involved 15 cases which were presented with sufficient clinical data to
Neoplasia 2018 Lecture 2. Dr Heyam Awad MD, FRCPath
 Neoplasia 2018 Lecture 2 Dr Heyam Awad MD, FRCPath ILOS 1. List the differences between benign and malignant tumors. 2. Recognize the histological features of malignancy. 3. Define dysplasia and understand
Neoplasia 2018 Lecture 2 Dr Heyam Awad MD, FRCPath ILOS 1. List the differences between benign and malignant tumors. 2. Recognize the histological features of malignancy. 3. Define dysplasia and understand
PSA. HMCK, p63, Racemase. HMCK, p63, Racemase
 Case 1 67 year old male presented with gross hematuria H/o acute prostatitis & BPH Urethroscopy: small, polypoid growth with a broad base emanating from the left side of the verumontanum Serum PSA :7 ng/ml
Case 1 67 year old male presented with gross hematuria H/o acute prostatitis & BPH Urethroscopy: small, polypoid growth with a broad base emanating from the left side of the verumontanum Serum PSA :7 ng/ml
Disclosures. Parathyroid Pathology. Objectives. The normal parathyroid 11/10/2012
 Disclosures Parathyroid Pathology I have nothing to disclose Annemieke van Zante MD/PhD Assistant Professor of Clinical Pathology Associate Chief of Cytopathology Objectives 1. Review the pathologic features
Disclosures Parathyroid Pathology I have nothing to disclose Annemieke van Zante MD/PhD Assistant Professor of Clinical Pathology Associate Chief of Cytopathology Objectives 1. Review the pathologic features
BSD 2015 Case 19. Female 21. Nodule on forehead. The best diagnosis is:
 BSD 2015 Case 19 Female 21. Nodule on forehead. The best diagnosis is: A. mixed tumour of skin B. porocarcinoma C. nodular hidradenoma D. metastatic adenocarcinoma BSD 2015 Case 19 Female 21 Nodule on
BSD 2015 Case 19 Female 21. Nodule on forehead. The best diagnosis is: A. mixed tumour of skin B. porocarcinoma C. nodular hidradenoma D. metastatic adenocarcinoma BSD 2015 Case 19 Female 21 Nodule on
A Cutaneous Facial Mass Identified as the New Entity Mammary Analogue Secretory Carcinoma of Probable Salivary Gland Origin
 A Cutaneous Facial Mass Identified as the New Entity Mammary Analogue Secretory Carcinoma of Probable Salivary Gland Origin Scott W. Binder, MD Professor and Senior Vice Chair Chief, Dermatopathology Geffen/UCLA
A Cutaneous Facial Mass Identified as the New Entity Mammary Analogue Secretory Carcinoma of Probable Salivary Gland Origin Scott W. Binder, MD Professor and Senior Vice Chair Chief, Dermatopathology Geffen/UCLA
Note: The cause of testicular neoplasms remains unknown
 - In the 15- to 34-year-old age group, they are the most common tumors of men. - Tumors of the testis are a heterogeneous group of neoplasms that include: I. Germ cell tumors : 95%; all are malignant.
- In the 15- to 34-year-old age group, they are the most common tumors of men. - Tumors of the testis are a heterogeneous group of neoplasms that include: I. Germ cell tumors : 95%; all are malignant.
What is ACC? (Adenoid Cystic Carcinoma)
") What is ACC? (Adenoid Cystic Carcinoma) 10-9-10 Where ACC Occurs ACC (Adenoid Cystic Carcinoma) is a rare and unique form of cancer that is known to be unpredictable in nature, with a typical growth pattern
What is ACC? (Adenoid Cystic Carcinoma) 10-9-10 Where ACC Occurs ACC (Adenoid Cystic Carcinoma) is a rare and unique form of cancer that is known to be unpredictable in nature, with a typical growth pattern
Disclosure. Relevant Financial Relationship(s) None. Off Label Usage None MFMER slide-1
 None. Off Label Usage None MFMER slide-1") Disclosure Relevant Financial Relationship(s) None Off Label Usage None 2013 MFMER slide-1 Case Presentation A 43 year old male, with partial nephrectomy for a right kidney mass 2013 MFMER slide-2 2013
Disclosure Relevant Financial Relationship(s) None Off Label Usage None 2013 MFMER slide-1 Case Presentation A 43 year old male, with partial nephrectomy for a right kidney mass 2013 MFMER slide-2 2013
Adenoid Cystic Carcinoma Minor Salivary Gland Origin
 Adenoid Cystic Carcinoma Minor Salivary Gland Origin Educational Session Presenter: Smith JA Supervisors: Palme CE, Gupta R Content Case report Imaging Primary Therapy Surgery Adjuvant Therapy Radiotherapy
Adenoid Cystic Carcinoma Minor Salivary Gland Origin Educational Session Presenter: Smith JA Supervisors: Palme CE, Gupta R Content Case report Imaging Primary Therapy Surgery Adjuvant Therapy Radiotherapy
The Pathology and Surgery of the Salivary Glands. R. A. Cawson, M. J. Gleeson, J. W. Eveson. Chapter 7: Carcinoma of salivary glands.
 The Pathology and Surgery of the Salivary Glands R. A. Cawson, M. J. Gleeson, J. W. Eveson Chapter 7: Carcinoma of salivary glands Introduction In terms of registration in England and Wales, cancers of
The Pathology and Surgery of the Salivary Glands R. A. Cawson, M. J. Gleeson, J. W. Eveson Chapter 7: Carcinoma of salivary glands Introduction In terms of registration in England and Wales, cancers of
Neoplasias Quisticas del Páncreas
 SEAP -Aproximación Práctica a la Patología Gastrointestinal- Madrid, 26 de mayo, 2006 Neoplasias Quisticas del Páncreas Gregory Y. Lauwers, M.D. Director, Service Massachusetts General Hospital Harvard
SEAP -Aproximación Práctica a la Patología Gastrointestinal- Madrid, 26 de mayo, 2006 Neoplasias Quisticas del Páncreas Gregory Y. Lauwers, M.D. Director, Service Massachusetts General Hospital Harvard
40th European Congress of Cytology Liverpool, UK, 2-5 th October 2016
 40th European Congress of Cytology Liverpool, UK, 2-5 th October 2016 EUS FNA of abdominal organs: An approach to reporting and triage for ancillary testing Date and time: Sunday 2 nd October 2016 15.00-16.30
40th European Congress of Cytology Liverpool, UK, 2-5 th October 2016 EUS FNA of abdominal organs: An approach to reporting and triage for ancillary testing Date and time: Sunday 2 nd October 2016 15.00-16.30
Triple Negative Breast Cancer
 Triple Negative Breast Cancer Prof. Dr. Pornchai O-charoenrat Division of Head-Neck & Breast Surgery Department of Surgery Faculty of Medicine Siriraj Hospital Breast Cancer Classification Traditional
Triple Negative Breast Cancer Prof. Dr. Pornchai O-charoenrat Division of Head-Neck & Breast Surgery Department of Surgery Faculty of Medicine Siriraj Hospital Breast Cancer Classification Traditional