Hematologic Malignancies. Anna Schaal, RN, MSN, arnp Norris Cotton Cancer Center Lebanon, New Hampshire
|
|
|
- Briana Berry
- 5 years ago
- Views:
Transcription
1 Hematologic Malignancies Anna Schaal, RN, MSN, arnp Norris Cotton Cancer Center Lebanon, New Hampshire
2 Objectives At the end of the session, the oncology nurse will be able to: Explain the pathophysiology of hematologic malignancies Discuss the rationale for treating the client with a hematologic malignancy List common nursing interventions for patients with hematologic malignancies
3 Hematopoiesis
4 Hematologic Malignancy Risk Factors Cause is unknown Elevated risk associated with Immunodeficiency organ transplants, autoimmune disorders Infectious agents HIV/AIDS: adult T cell lymphoma EBV: Burkitt s lymphoma, PTLD HCV: Marginal zone lymphoma Helicobacter pylori: MALT lymphomas Environmental exposures Drugs, chemicals, radiation, occupational exposures Genetic Predisposition Downs syndrome
5 Leukemia Epidemiology Approximately 52,380 cases of leukemia will be diagnosed in 2014 (ACS, 2014) Leukemia occurs in more adults than children (ACS, 2014) More common in males ALL: most common form of childhood leukemia (ACS, 2014)
6 Pathophysiology of Leukemia Malignant disorder of blood cells and lymphatic tissues Leukemic, malignant cells excessively proliferate Leukemic cells capable of infiltrating and accumulating in other organs
7 Pathophysiology Symptoms of leukemia attributed to: Type of leukemia cell Degree of leukemic cell burden Degree of myelosuppression Effects of organ involvement
8 Types of Leukemia Acute leukemia: adults and children Acute Myelogenous Leukemia (AML) Acute Lymphocytic Leukemia (ALL) Chronic leukemia Chronic Myelogenous Leukemia (CML) Chronic Lymphocytic Leukemia (CLL) Hairy Cell Leukemia (HCL)
9 Types of Leukemia Has to do with cell lineage and maturity

10 V Faderl S, Talpaz M, Estrov Z, O Brien S, Kurzrock R, Kantarjian HM. N Engl J Med. 1999;341: Faderl S, Talpaz M, Estrov Z, Kantarjian HM. Ann Intern Med. 1999;131:
11
12
13 AML De novo vs. secondary (alkylating agents) Risk related to age and cellular biology Immunophenotyping, cytogenetics Initial remission rates 60 70% (adults) Median survival with treatment months
14 ALL Most common childhood leukemia Peak age 2 5 yrs 80% cured 80% are B cell, 20% T cell In adults is highly aggressive Long treatment programs 2 3 years CNS infiltration common



15 Leukemia: Clinical Presentation Usually associated with symptoms of cytopenias
16 Leukemia Management Depends on the type and stage AML Induction: Initial treatment with chemotherapy agents given at high doses to eradicate leukemia Consolidation,, which may include hematopoietic stem cell transplantation
17 Leukemia Management ALL Induction Initial treatment with chemotherapy agents given at high doses to eradicate leukemia Post remission therapy Consolidation therapy Intensification therapy Maintenance therapy +/ Stem cell transplant
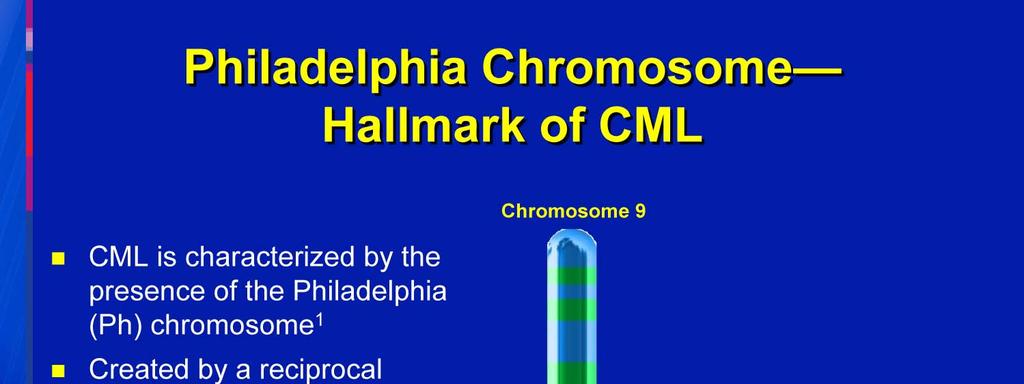
18 Leukemia Management CLL Watch and wait Chemotherapy and biotherapy May include allogeneic stem cell transplant CML Tyrosine Kinase Inhibitors (oral) May include allogeneic stem cell transplant
19 Leukemia Management: Stem Cell Transplant Autologous Patients own stem cells Is a rescue for high dose chemotherapy Allogeneic Donor cells Depends on graft vs. leukemia affect Myeloablative vs. non myeloablative

20 Non Hodgkin s Lymphomas: Overview Heterogeneous neoplasms Differing patterns of growth, treatment response Multiple sites, extranodal lesions common Reed-Sternberg cell, Wright-stained
 Digestive and respiratory tracts")
21 Lymphatic System Lymphatic vessels, nodes and organs Primary Lymphoid organs Bone marrow Thymus Secondary Lymphoid organs Lymph nodes Spleen Tonsils, adenoids (Waldeyer s ring) Digestive and respiratory tracts (MALT)
 cells Kill infected cells Attack cancer cells Non Hodgkin lymphoma 85% B cells 15%")
22 Pathophysiology: Lymphocytes T cells Release cytokines B cells Produce antibodies Natural killer (NK) cells Kill infected cells Attack cancer cells Non Hodgkin lymphoma 85% B cells 15% T cells
23 Incidence per 100, NHL: Age Demographics Age
24 Aggressiveness of Mature B Cell NHL Type Lymphomas Treatment Goals Indolent or slow-growing Aggressive CLL/SLL WM MZL FL MCL DLBCL PMBL Treatable, but not curable Goal is to control and minimize symptoms Waxing and waning course Transformation to large cell lymphoma can occur Without treatment, life expectancy is short Potential long-term survival with treatment Most treated with curative intent Cure rates vary CLL=chronic lymphocytic leukemia; DLBCL=diffuse large B-cell lymphoma; FL=follicular lymphoma; MCL=mantle cell lymphoma; B-lymphoblastic MZL=marginal zone lymphoma; PMBL=primary mediastinal large B-cell lymphoma; Treated SLL=small with lymphocytic curative leukemia; intent WM=Waldenstrom s macroglobulinemia. Very aggressive Precursor lymphoma/leukemia Burkitt s lymphoma/ B cell acute leukemia Cure rates vary
25 NHL: Common Subtypes BL (< 1%) Other subtypes (9%) MCL (6%) FL (22%) T and NK cell (12%) DLBCL (31%) SLL/CLL(7%) MALT-type MZL (7.5%) Nodal-type MZL (< 2%) Lymphoplasmacytic (1%) MCL = mantle cell lymphoma; FL = follicular lymphoma; SLL = small lymphocytic lymphoma; CLL = chronic lymphocytic leukemia; MALT = mucosa-associated lymphoid tissue; MZL = marginal zone lymphoma; BL = Burkitt lymphoma.
 Systemic symptoms (A or B) Bulk > 10 cm")
26 Ann Arbor Staging System Stage I Single lymph node group Stage II Multiple lymph nodes on same side of diaphragm Stage III Multiple lymph nodes on both sides of the diaphragm Stage IV Multiple extranodal sites or lymph nodes and extranodal disease Substaging: Extranodal extension (E) Systemic symptoms (A or B) Bulk > 10 cm (X)
27 International Prognostic Index Adverse Risk Factors Age >60 Stage 3 or 4 >2 extranodal sites Performance Status >2 LDH>normal Risk Category Low = 1 risk factor Low intermediate 2 High intermediate 3 High 4 or 5

28 Hodgkin s Disease Clonal lymphoid malignancy Characterized by Reed Sternberg cells
29 Epidemiology of Hodgkin s Disease Incidence: In 2018, approximately 8500 estimated new cases in USA Expect 1050 deaths HD comprises 16% of all lymphomas, but less than 1% of all new cancers Age: Incidence is bimodal (greatest peak in age range with a second smaller peak after age 60 years) Sex: Male to female ratio is 1.4 to 1
30 Prognostic factors Hemoglobin < 10.5g/dL Male Age < 45 years Stage IV disease Leukocytosis (WBC count > 15,000/mm 3 ) Lymphocytopenia (ALS < 600/mm 3 ) Freedom from disease progression at 5 years: 0 features = 84% (7%) 1 features = 77% (22%) 2 features = 67% (29%) 3 features = 60% (23% ) 4 features = 51% (12%) 5 or more = 42% (7%)

![loss Constitutional symptoms [fatigue] Bone marrow](/docs-images/96/127800502/images/31-5.jpg "involvement Site specific findings A Swollen Lymph")
31 Lymphoma: Clinical Presentation Painless lymphadenopathy B symptoms Fever, night sweats, weight loss Constitutional symptoms [fatigue] Bone marrow involvement Site specific findings A Swollen Lymph Node in the Neck 31
32 Treating Lymphoma
33 Multiple Myeloma Malignant proliferation of plasma cells in the bone marrow accompanied by an increased production of abnormal immunoglobulin (IgG, IgA, IgD, IgM) Destroys bone tissue Decreases bone marrow function Affects the immune system
34 Hematopoiesis
35 Pathophysiology: Plasma Cells Terminally differentiated cells of B lymphocyte lineage Cellular factories whose job is devoted to producing a single antibody protein Normally incapable of dividing Abundant in lymph nodes and bone marrow
36 Epidemiology Gender: Males > Females (1.3:1 ratio). Age: Onset of disease is late, with peak incidence at age > 60 years, fewer than 3% age <40 Race: Incidence is greater in African Americans than in Caucasians (2:1 ratio). Geography: No clear geographic distribution although higher relative incidence in more developed countries.

37 International Staging System (ISS) Better Response to Therapy Stage I Factors: beta-2 microglobulin <3.5 mg/dl Albumin 3.5 g/dl Most Favorable Prognosis Stage II Factors: beta-2 microglobulin <3.5 mg/dl Albumin <3.5 g/dl or beta-2 microglobulin <5.5 mg/dl Lesser Response to Therapy Stage III Factors: beta-2 microglobulin 5.5 mg/dl Less Favorable Prognosis
38 CRAB Symptoms of MM C Calcium R Renal dysfunction A Anemia B Bone pain or lesions

39 Multiple Myeloma Clinical Presentation Back Pain Anemia Hypercalcemia Renal Failure Infections Fatigue

40 Treating Multiple Myeloma Approached as a chronic disease Treatable, but not curable
41 Diagnostic Evaluation: History and Physical Clinical evaluation Document onset of suspicious symptoms, acute episodes of illness, adenopathy, historical labs Review of medication profile Co-morbid conditions Physical exam Clinical significance May indicate onset of disease, rapidity of symptom onset and progression, presence of B-symptoms (fever, night sweats, weight loss, pruritus) Identification of any drug-induced cytopenias or symptoms, complexity of co-morbid conditions, potential drug interactions Effective management of co-morbid conditions may play a critical role in selecting therapies Underlying cardiovascular disease may require dose modification or omission of anthracyclines Establish a baseline for adenopathy, organomegaly, other extramedullary sites of disease, and identification of any abnormal findings which may require immediate intervention
42 Peripheral Blood Diagnostic study Clinical significance CBC + differential + platelets Reticulocyte count LDH, haptoglobin, coombs, and reticulocyte count LDH Serum β 2 m (lymphoma and MM) Hepatic profile Evaluate presence of cytopenias, lymphocytosis, morphological abnormalities, and bone marrow response to anemia Evaluate for underlying hemolysis Necessary for risk stratification using IPI Evaluate for aggressive disease, risk for TLS, and hemolysis Prognostic relevance Reflects WBC membrane turnover Levels are affected by renal function Treatments have potential renal and hepatic toxicities or may be affected by renal or hepatic insufficiencies Serum albumin reflects nutritional status and used to estimate prognosis
43 Diagnostic Evaluation: Peripheral Blood Diagnostic study Clinical significance Quantitative immunoglobulins UA, LDH, K+, PO 4, Ca++ Serum iron, ferritin, TIBC, folic acid, B12 Hepatitis B screen Lumbar puncture with cerebrospinal fluid analysis Hypogammaglobulinemia is common in aggressive disease and associated with an increased risk of infections Baseline tumor lysis screen Evaluate for other possible causes of anemia Risk of Hepatitis B reactivation a) HBsAg positive, particularly those who are HBeAg positive or have high levels of HBV DNA male gender b) Use of corticosteroids; use of rituximab Should be considered in patients with high LDH, multiple extranodal sites, epidural masses, testicular disease, paranasal or nasopharyngeal disease
44 Diagnostic Evaluation: Tissue Biopsy * Definitive diagnosis for lymphoma can only be made biopsy of pathologic LN or tumor tissues Diagnostic study Morphology Immunohistochemistry Flow cytometry Molecular profiling Clinical significance Review of cytology using low-power microscope to define basic architecture of the lymphatic tissue Excisional biopsy is the standard for initial diagnosis of NHL (fine needle aspirates are felt to be inadequate) Used to isolate cellular proteins which correlate with phases of B-cell differentiation Immunophenotyping used to describe antigen expression on B-cells using peripheral blood and bone marrow Used to correlate with the tissue biopsy for WHO classification of subtype Newer molecular profiling has identified key prognostic markers as well as potential targets for new therapies
45 Diagnostic Evaluation: Bone Marrow Diagnostic study Aspirate Should include spicules and be cellular enough to assess at least 500 cells Biopsy Should be of adequate size for evaluation (1 2 cm) Cytogenetics Clinical significance Evaluation of morphological abnormalities of hematopoietic precursors to allow WHO classification Used for flow cytometry, FISH analysis, and cytogenetics Evaluate cellularity, topography, presence of lymphocytic infiltrates, exclusion of other bone marrow disorders or bone marrow infiltration by solid tumors Evaluate for possible non-random chromosomal abnormalities Usually based on evaluation of 20 metaphases Greater than 2 metaphases is considered non-random
46 Diagnostic Evaluation: Imaging Diagnostic study MUGA scan or echocardiogram CT chest, abdomen, and pelvis Clinical significance _ Baseline evaluation for patients receiving anthracycline therapy Current standard of care for initial staging on NHL Estimation of anatomic extent of disease and areas of abnormal lymph nodes (> 1 cm) 18 FDG-PET PET with FDG shows functional metabolic status Useful in evaluation of lymph nodes < 1 cm Chest X-ray Skeletal Survey Baseline evaluation for any underlying disease Evaluate for lytic lesions, plasmacytomas, impending fractures
47 Supportive Therapy Nursing Interventions Infection Early recognition and prevention of infection IV immunoglobulin therapy for recurrent infections Consider yearly influenza vaccine Consider PCP, herpes, and antifungal prophylaxis with use of highdose Dexamethasone regimens Use of myeloid growth factors - neupogen Anemia Early recognition and treatment Erythropoietin therapy Red blood cell transfusions Thrombocytopenia Prevention of bleeding Platelet transfusions
 1.")
48 Supportive Therapy Nursing Interventions Calculating the ANC WBC 0.8 Neutrophils 27 Immatures (bands) 1.2 (PMN s + Bands) X WBC
49 Supportive Therapy Nursing Interventions Constipation/Diarrhea Assessment of bowel habits changes in fluid and dietary intake and activity medication administration Pain Assessment and documentation Proper positioning and supports Consultation with PT/OT Analgesics Non-pharmacologic therapies Cord compression Proper positioning and supports Consultation with PT/OT Vertebroplasty
50 Supportive Therapy Nursing Interventions Nausea and Vomiting Anti-emetics remember anticipatory and delayed Monitor renal function/hydration status Complimentary non-pharmacologics ie.. Guided imagery, music therapy, accupressure Renal dysfunction (may occur in 25% MM patients) Maintain hydration to avoid renal failure Allopurinol Avoid NSAIDs and IV contrast dye Monitor for renal dysfunction with chronic use of bisphosphonates Not a contraindication to transplant Plasmapheresis may slow down/prevent renal failure by removal of M- protein from the blood
51 Supportive Therapy Nursing Interventions Cognitive impairment Counseling regarding injury prevention; anxiolytics, antidepressants Hypercalcemia (25% MM patients at presentation) Avoid/discontinue calcium supplements Hydration plus diuretics Bisphosphonates, steroids and//or calcitonin Bone disease (most common MM presenting symptom) Regular monitoring of bone lesions with skeletal survey or focused CT scan/mri Bisphosphonate administration intravenously q 3-4 weeks Regular exercise Avoid situations that put one at risk to fall Analgesia
52 Ann Arbor Staging is used in what type of malignancy? A. Lung Cancer B. Colon Cancer C. Breast Cancer D. Lymphoma
53 Mr. Jones has multiple myeloma and is currently in an unmaintained remission. Which of the following s/sx would indicate that his disease may be progressing? A. a drop in his total protein B. frequent urination C. pain in his right forearm D. an elevated BUN
54 Miss Jones has a total WBC of 2.0 with 48% neutrophils and 2% bands. What is her ANC? A. 550 B C. 100 D. 5000
55 Miss Jones has newly diagnosed NHL. She has a postive pet scan with adenopathy in the cervical, axillary and inguinal areas. Her bone marrow biopsy was negative for disease. She has no other extranodal disease sites. What stage of NHL does she have? A. 1 B. 2 C. 3 D. 4


56
LEUKAEMIA and LYMPHOMA. Dr Mubarak Abdelrahman Assistant Professor Jazan University
 LEUKAEMIA and LYMPHOMA Dr Mubarak Abdelrahman Assistant Professor Jazan University OBJECTIVES Identify etiology and epidemiology for leukemia and lymphoma. Discuss common types of leukemia. Distinguish
LEUKAEMIA and LYMPHOMA Dr Mubarak Abdelrahman Assistant Professor Jazan University OBJECTIVES Identify etiology and epidemiology for leukemia and lymphoma. Discuss common types of leukemia. Distinguish
Indolent Lymphomas. Dr. Melissa Toupin The Ottawa Hospital
 Indolent Lymphomas Dr. Melissa Toupin The Ottawa Hospital What does indolent mean? Slow growth Often asymptomatic Chronic disease with periods of relapse (long natural history possible) Incurable with
Indolent Lymphomas Dr. Melissa Toupin The Ottawa Hospital What does indolent mean? Slow growth Often asymptomatic Chronic disease with periods of relapse (long natural history possible) Incurable with
Lymphoma: What You Need to Know. Richard van der Jagt MD, FRCPC
 Lymphoma: What You Need to Know Richard van der Jagt MD, FRCPC Overview Concepts, classification, biology Epidemiology Clinical presentation Diagnosis Staging Three important types of lymphoma Conceptualizing
Lymphoma: What You Need to Know Richard van der Jagt MD, FRCPC Overview Concepts, classification, biology Epidemiology Clinical presentation Diagnosis Staging Three important types of lymphoma Conceptualizing
LYMPHOMA Joginder Singh, MD Medical Oncologist, Mercy Cancer Center
 LYMPHOMA Joginder Singh, MD Medical Oncologist, Mercy Cancer Center Lymphoma is cancer of the lymphatic system. The lymphatic system is made up of organs all over the body that make up and store cells
LYMPHOMA Joginder Singh, MD Medical Oncologist, Mercy Cancer Center Lymphoma is cancer of the lymphatic system. The lymphatic system is made up of organs all over the body that make up and store cells
Large cell immunoblastic Diffuse histiocytic (DHL) Lymphoblastic lymphoma Diffuse lymphoblastic Small non cleaved cell Burkitt s Non- Burkitt s
 Lymphoblastic lymphoma Diffuse lymphoblastic Small non cleaved cell Burkitt s Non- Burkitt s") Non Hodgkin s Lymphoma Introduction 6th most common cause of cancer death in United States. Increasing in incidence and mortality. Since 1970, the incidence of has almost doubled. Overview The types of
Non Hodgkin s Lymphoma Introduction 6th most common cause of cancer death in United States. Increasing in incidence and mortality. Since 1970, the incidence of has almost doubled. Overview The types of
What is a hematological malignancy? Hematology and Hematologic Malignancies. Etiology of hematological malignancies. Leukemias
 Hematology and Hematologic Malignancies Cancer of the formed elements of the blood What is a hematological malignancy? A hematologic malignancy is a malignancy (or cancer) of any of the formed elements
Hematology and Hematologic Malignancies Cancer of the formed elements of the blood What is a hematological malignancy? A hematologic malignancy is a malignancy (or cancer) of any of the formed elements
Indolent Lymphomas: Current. Dr. Laurie Sehn
 Indolent Lymphomas: Current Dr. Laurie Sehn Why does indolent mean? Slow growth Often asymptomatic Chronic disease with periods of relapse (long natural history possible) Incurable with current standard
Indolent Lymphomas: Current Dr. Laurie Sehn Why does indolent mean? Slow growth Often asymptomatic Chronic disease with periods of relapse (long natural history possible) Incurable with current standard
Lymphoma/CLL 101: Know your Subtype. Dr. David Macdonald Hematologist, The Ottawa Hospital
 Lymphoma/CLL 101: Know your Subtype Dr. David Macdonald Hematologist, The Ottawa Hospital Function of the Lymph System Lymph Node Lymphocytes B-cells develop in the bone marrow and influence the immune
Lymphoma/CLL 101: Know your Subtype Dr. David Macdonald Hematologist, The Ottawa Hospital Function of the Lymph System Lymph Node Lymphocytes B-cells develop in the bone marrow and influence the immune
7 Omar Abu Reesh. Dr. Ahmad Mansour Dr. Ahmad Mansour
 7 Omar Abu Reesh Dr. Ahmad Mansour Dr. Ahmad Mansour -Leukemia: neoplastic leukocytes circulating in the peripheral bloodstream. -Lymphoma: a neoplastic process in the lymph nodes, spleen or other lymphatic
7 Omar Abu Reesh Dr. Ahmad Mansour Dr. Ahmad Mansour -Leukemia: neoplastic leukocytes circulating in the peripheral bloodstream. -Lymphoma: a neoplastic process in the lymph nodes, spleen or other lymphatic
Lymphatic system component
 Introduction Lymphatic system component Statistics Overview Lymphoma Non Hodgkin s Lymphoma Non- Hodgkin's is a type of cancer that originates in the lymphatic system. It is estimated to be the sixth most
Introduction Lymphatic system component Statistics Overview Lymphoma Non Hodgkin s Lymphoma Non- Hodgkin's is a type of cancer that originates in the lymphatic system. It is estimated to be the sixth most
NON HODGKINS LYMPHOMA: INDOLENT Updated June 2015 by Dr. Manna (PGY-5 Medical Oncology Resident, University of Calgary)
") NON HODGKINS LYMPHOMA: INDOLENT Updated June 2015 by Dr. Manna (PGY-5 Medical Oncology Resident, University of Calgary) Reviewed by Dr. Michelle Geddes (Staff Hematologist, University of Calgary) and Dr.
NON HODGKINS LYMPHOMA: INDOLENT Updated June 2015 by Dr. Manna (PGY-5 Medical Oncology Resident, University of Calgary) Reviewed by Dr. Michelle Geddes (Staff Hematologist, University of Calgary) and Dr.
Non-Hodgkin lymphomas (NHLs) Hodgkin lymphoma )HL)
 Hodgkin lymphoma )HL)") Non-Hodgkin lymphomas (NHLs) Hodgkin lymphoma )HL) Lymphoid Neoplasms: 1- non-hodgkin lymphomas (NHLs) 2- Hodgkin lymphoma 3- plasma cell neoplasms Non-Hodgkin lymphomas (NHLs) Acute Lymphoblastic Leukemia/Lymphoma
Non-Hodgkin lymphomas (NHLs) Hodgkin lymphoma )HL) Lymphoid Neoplasms: 1- non-hodgkin lymphomas (NHLs) 2- Hodgkin lymphoma 3- plasma cell neoplasms Non-Hodgkin lymphomas (NHLs) Acute Lymphoblastic Leukemia/Lymphoma
Non-Hodgkin lymphoma
 Non-Hodgkin lymphoma Non-Hodgkin s lymphoma Definition: - clonal tumours of mature and immature B cells, T cells or NK cells - highly heterogeneous, both histologically and clinically Non-Hodgkin lymphoma
Non-Hodgkin lymphoma Non-Hodgkin s lymphoma Definition: - clonal tumours of mature and immature B cells, T cells or NK cells - highly heterogeneous, both histologically and clinically Non-Hodgkin lymphoma
Instructions for Chronic Lymphocytic Leukemia Post-HSCT Data (Form 2113)
") Instructions for Chronic Lymphocytic Leukemia Post-HSCT Data (Form 2113) This section of the CIBMTR Forms Instruction Manual is intended to be a resource for completing the CLL Post-HSCT Data Form. E-mail
Instructions for Chronic Lymphocytic Leukemia Post-HSCT Data (Form 2113) This section of the CIBMTR Forms Instruction Manual is intended to be a resource for completing the CLL Post-HSCT Data Form. E-mail
Lymphoma: The Basics. Dr. Douglas Stewart
 Lymphoma: The Basics Dr. Douglas Stewart Objectives What is lymphoma? How common is it? Why does it occur? How do you diagnose it? How do you manage it? How do you follow patients after treatment? What
Lymphoma: The Basics Dr. Douglas Stewart Objectives What is lymphoma? How common is it? Why does it occur? How do you diagnose it? How do you manage it? How do you follow patients after treatment? What
Aggressive Lymphomas - Current. Dr Kevin Imrie Physician-in-Chief, Sunnybrook Health Sciences Centre
 Aggressive Lymphomas - Current Dr Kevin Imrie Physician-in-Chief, Sunnybrook Health Sciences Centre Conflicts of interest I have no conflicts of interest to declare Outline What does aggressive lymphoma
Aggressive Lymphomas - Current Dr Kevin Imrie Physician-in-Chief, Sunnybrook Health Sciences Centre Conflicts of interest I have no conflicts of interest to declare Outline What does aggressive lymphoma
WHO Classification. B-cell chronic lymphocytic leukemia/small T-cell granular lymphocytic leukemia
 Blood Malignancies-II Prof. Dr. Herman Hariman, a Ph.D, SpPK (KH). Prof. Dr. Adikoesoema Aman, SpPK (KH) Dept. of Clinical Pathology, School of Medicine, University of North Sumatra WHO classification
Blood Malignancies-II Prof. Dr. Herman Hariman, a Ph.D, SpPK (KH). Prof. Dr. Adikoesoema Aman, SpPK (KH) Dept. of Clinical Pathology, School of Medicine, University of North Sumatra WHO classification
WHAT ARE PAEDIATRIC CANCERS
 WHAT ARE PAEDIATRIC CANCERS INTRODUCTION Childhood cancers are RARE 0.5% of all cancers in the West Overall risk that a child will develop cancer during first 15 years of life is 1 in 450 and 1 in 600
WHAT ARE PAEDIATRIC CANCERS INTRODUCTION Childhood cancers are RARE 0.5% of all cancers in the West Overall risk that a child will develop cancer during first 15 years of life is 1 in 450 and 1 in 600
1. Please review the following table, make any changes you think are necessary and highlight those changes. Feel free to put notes on the next page
 COME HOME Non-Hodgkin pathway development worksheet, v6 September 2014 1. Please review the following table, make any changes you think are necessary and highlight those changes. Feel free to put notes
COME HOME Non-Hodgkin pathway development worksheet, v6 September 2014 1. Please review the following table, make any changes you think are necessary and highlight those changes. Feel free to put notes
Pathology of Hematopoietic and Lymphoid tissue
 Pathology of Hematopoietic and Lymphoid tissue Peerayut Sitthichaiyakul, M.D. Department of Pathology and Forensic Medicine Faculty of Medicine, Naresuan University CONTENTS White blood cells and lymph
Pathology of Hematopoietic and Lymphoid tissue Peerayut Sitthichaiyakul, M.D. Department of Pathology and Forensic Medicine Faculty of Medicine, Naresuan University CONTENTS White blood cells and lymph
Burkitt lymphoma. Sporadic Endemic in Africa associated with EBV Translocations involving MYC gene on chromosome 8
 Heme 8 Burkitt lymphoma Sporadic Endemic in Africa associated with EBV Translocations involving MYC gene on chromosome 8 Most common is t(8;14) Believed to be the fastest growing tumor in humans!!!! Morphology
Heme 8 Burkitt lymphoma Sporadic Endemic in Africa associated with EBV Translocations involving MYC gene on chromosome 8 Most common is t(8;14) Believed to be the fastest growing tumor in humans!!!! Morphology
Hematology 101. Rachid Baz, M.D. 5/16/2014
 Hematology 101 Rachid Baz, M.D. 5/16/2014 Florida 101 Epidemiology Estimated prevalence 8,000 individuals in U.S (compare with 80,000 MM patients) Annual age adjusted incidence 3-8/million-year 1 More
Hematology 101 Rachid Baz, M.D. 5/16/2014 Florida 101 Epidemiology Estimated prevalence 8,000 individuals in U.S (compare with 80,000 MM patients) Annual age adjusted incidence 3-8/million-year 1 More
Pathology of Hematopoietic and Lymphoid tissue
 CONTENTS Pathology of Hematopoietic and Lymphoid tissue White blood cells and lymph nodes Quantitative disorder of white blood cells Reactive lymphadenopathies Infectious lymphadenitis Tumor metastasis
CONTENTS Pathology of Hematopoietic and Lymphoid tissue White blood cells and lymph nodes Quantitative disorder of white blood cells Reactive lymphadenopathies Infectious lymphadenitis Tumor metastasis
Understanding your diagnosis. Dr Graham Collins Consultant Haemtologist Oxford University Hospitals
 Understanding your diagnosis Dr Graham Collins Consultant Haemtologist Oxford University Hospitals Common questions I get asked What is lymphoma? What subtype do I have and what does that mean? What are
Understanding your diagnosis Dr Graham Collins Consultant Haemtologist Oxford University Hospitals Common questions I get asked What is lymphoma? What subtype do I have and what does that mean? What are
Leukemias. Prof. Mutti Ullah Khan Head of Department Medical Unit-II Holy Family Hospital Rawalpindi Medical College
 Leukemias Prof. Mutti Ullah Khan Head of Department Medical Unit-II Holy Family Hospital Rawalpindi Medical College Introduction Leukaemias are malignant disorders of the haematopoietic stem cell compartment,
Leukemias Prof. Mutti Ullah Khan Head of Department Medical Unit-II Holy Family Hospital Rawalpindi Medical College Introduction Leukaemias are malignant disorders of the haematopoietic stem cell compartment,
Lymphoma Read with the experts
 Lymphoma Read with the experts Marc Seltzer, MD Associate Professor of Radiology Geisel School of Medicine at Dartmouth Director, PET-CT Course American College of Radiology Learning Objectives Recognize
Lymphoma Read with the experts Marc Seltzer, MD Associate Professor of Radiology Geisel School of Medicine at Dartmouth Director, PET-CT Course American College of Radiology Learning Objectives Recognize
Lancashire and South Cumbria Haematology NSSG Guidelines for Follicular Lymphoma:
 1 Lancashire and South Cumbria Haematology NSSG Guidelines for Follicular Lymphoma: 2018-19 1.1 Pretreatment evaluation The following tests should be performed: FBC, U&Es, creat, LFTs, calcium, LDH, Igs/serum
1 Lancashire and South Cumbria Haematology NSSG Guidelines for Follicular Lymphoma: 2018-19 1.1 Pretreatment evaluation The following tests should be performed: FBC, U&Es, creat, LFTs, calcium, LDH, Igs/serum
If unqualified, Complete remission is considered to be Haematological complete remission
 Scroll right to see the database codes for Disease status and Response Diagnosis it refers to Disease status or response to treatment AML ALL CML CLL MDS or MD/MPN or acute leukaemia secondary to previous
Scroll right to see the database codes for Disease status and Response Diagnosis it refers to Disease status or response to treatment AML ALL CML CLL MDS or MD/MPN or acute leukaemia secondary to previous
WBCs Disorders 1. Dr. Nabila Hamdi MD, PhD
 WBCs Disorders 1 Dr. Nabila Hamdi MD, PhD ILOs Compare and contrast ALL, AML, CLL, CML in terms of age distribution, cytogenetics, morphology, immunophenotyping, laboratory diagnosis clinical features
WBCs Disorders 1 Dr. Nabila Hamdi MD, PhD ILOs Compare and contrast ALL, AML, CLL, CML in terms of age distribution, cytogenetics, morphology, immunophenotyping, laboratory diagnosis clinical features
If unqualified, Complete remission is considered to be Haematological complete remission
 Scroll right to see the database codes for Disease status and Response Diagnosis it refers to Disease status or response to treatment AML ALL CML CLL MDS or MD/MPN or acute leukaemia secondary to previous
Scroll right to see the database codes for Disease status and Response Diagnosis it refers to Disease status or response to treatment AML ALL CML CLL MDS or MD/MPN or acute leukaemia secondary to previous
Chronic Lymphocytic Leukemia (CLL)
") Page 1 of 10 PATIENT EDUCATION Chronic Lymphocytic Leukemia (CLL) Introduction Chronic lymphocytic leukemia (CLL) is a type of cancer of the lymphocytes (a kind of white blood cell). It is also referred
Page 1 of 10 PATIENT EDUCATION Chronic Lymphocytic Leukemia (CLL) Introduction Chronic lymphocytic leukemia (CLL) is a type of cancer of the lymphocytes (a kind of white blood cell). It is also referred
Pathology #07. Hussein Al-Sa di. Dr. Sohaib Al-Khatib. Mature B-Cell Neoplasm. 0 P a g e
 Pathology #07 Mature B-Cell Neoplasm Hussein Al-Sa di Dr. Sohaib Al-Khatib 0 P a g e Thursday 18/2/2016 Our lecture today (with the next 2 lectures) will be about lymphoid tumors This is a little bit long
Pathology #07 Mature B-Cell Neoplasm Hussein Al-Sa di Dr. Sohaib Al-Khatib 0 P a g e Thursday 18/2/2016 Our lecture today (with the next 2 lectures) will be about lymphoid tumors This is a little bit long
HAEMATOLOGICAL MALIGNANCY
 HAEMATOLOGICAL MALIGNANCY Reference Compulsory reading Haematology at Glance 2 nd ed. Atul Mehta & Victor Hoffbrand Chapters: 20 to 31 Pages: 46 to 69 Pathogenesis of Haematological Malignancy Figure (a)
HAEMATOLOGICAL MALIGNANCY Reference Compulsory reading Haematology at Glance 2 nd ed. Atul Mehta & Victor Hoffbrand Chapters: 20 to 31 Pages: 46 to 69 Pathogenesis of Haematological Malignancy Figure (a)
2013 AAIM Pathology Workshop
 2013 AAIM Pathology Workshop John Schmieg, M.D., Ph.D. None Disclosures 1 Pathology Workshop Objectives Define the general philosophy of reviewing pathology reports Review the various components of Bone
2013 AAIM Pathology Workshop John Schmieg, M.D., Ph.D. None Disclosures 1 Pathology Workshop Objectives Define the general philosophy of reviewing pathology reports Review the various components of Bone
Plasma cell myeloma (multiple myeloma)
") Plasma cell myeloma (multiple myeloma) Common lymphoid neoplasm, present at old age (70 years average) Remember: plasma cells are terminally differentiated B-lymphocytes that produces antibodies. B-cells
Plasma cell myeloma (multiple myeloma) Common lymphoid neoplasm, present at old age (70 years average) Remember: plasma cells are terminally differentiated B-lymphocytes that produces antibodies. B-cells
CHAPTER:4 LEUKEMIA. BY Mrs. K.SHAILAJA., M. PHARM., LECTURER DEPT OF PHARMACY PRACTICE, SRM COLLEGE OF PHARMACY 8/12/2009
 LEUKEMIA CHAPTER:4 1 BY Mrs. K.SHAILAJA., M. PHARM., LECTURER DEPT OF PHARMACY PRACTICE, SRM COLLEGE OF PHARMACY Leukemia A group of malignant disorders affecting the blood and blood-forming tissues of
LEUKEMIA CHAPTER:4 1 BY Mrs. K.SHAILAJA., M. PHARM., LECTURER DEPT OF PHARMACY PRACTICE, SRM COLLEGE OF PHARMACY Leukemia A group of malignant disorders affecting the blood and blood-forming tissues of
NAACCR Webinar Series 1
 COLLECTING CANCER DATA: HEMATOPOIETIC AND LYMPHOID NEOPLASMS Jim Hofferkamp, CTR (jhofferkam@naaccr.org) Shannon Vann, CTR (svann@naaccr.org) Q&A Please submit all questions concerning webinar content
COLLECTING CANCER DATA: HEMATOPOIETIC AND LYMPHOID NEOPLASMS Jim Hofferkamp, CTR (jhofferkam@naaccr.org) Shannon Vann, CTR (svann@naaccr.org) Q&A Please submit all questions concerning webinar content
Pediatric Oncology. Vlad Radulescu, MD
 Pediatric Oncology Vlad Radulescu, MD Objectives Review the epidemiology of childhood cancer Discuss the presenting signs and symptoms, general treatment principles and overall prognosis of the most common
Pediatric Oncology Vlad Radulescu, MD Objectives Review the epidemiology of childhood cancer Discuss the presenting signs and symptoms, general treatment principles and overall prognosis of the most common
The Lymphomas. An overview..
 The Lymphomas An overview.. Peter Anglin MD, FRCPC, MBA Stronach Regional Cancer Centre Newmarket, ON The lymphomas are an important part of the history of medicine 1666 Magpighi publishes first recorded
The Lymphomas An overview.. Peter Anglin MD, FRCPC, MBA Stronach Regional Cancer Centre Newmarket, ON The lymphomas are an important part of the history of medicine 1666 Magpighi publishes first recorded
Pathology. #11 Acute Leukemias. Farah Banyhany. Dr. Sohaib Al- Khatib 23/2/16
 35 Pathology #11 Acute Leukemias Farah Banyhany Dr. Sohaib Al- Khatib 23/2/16 1 Salam First of all, this tafreegh is NOT as long as you may think. If you just focus while studying this, everything will
35 Pathology #11 Acute Leukemias Farah Banyhany Dr. Sohaib Al- Khatib 23/2/16 1 Salam First of all, this tafreegh is NOT as long as you may think. If you just focus while studying this, everything will
Molecular Pathology of Lymphoma (Part 1) Rex K.H. Au-Yeung Department of Pathology, HKU
 Rex K.H. Au-Yeung Department of Pathology, HKU") Molecular Pathology of Lymphoma (Part 1) Rex K.H. Au-Yeung Department of Pathology, HKU Lecture outline Time 10:00 11:00 11:15 12:10 12:20 13:15 Content Introduction to lymphoma Review of lymphocyte biology
Molecular Pathology of Lymphoma (Part 1) Rex K.H. Au-Yeung Department of Pathology, HKU Lecture outline Time 10:00 11:00 11:15 12:10 12:20 13:15 Content Introduction to lymphoma Review of lymphocyte biology
Update in Lymphoma Imaging
 Update in Lymphoma Imaging Victorine V. Muse, MD Lymphoma Update in Lymphoma Imaging Victorine V Muse, MD Heterogeneous group of lymphoid neoplasms divided into two broad histological categories Hodgkin
Update in Lymphoma Imaging Victorine V. Muse, MD Lymphoma Update in Lymphoma Imaging Victorine V Muse, MD Heterogeneous group of lymphoid neoplasms divided into two broad histological categories Hodgkin
Head and Neck: DLBCL
 Head and Neck: DLBCL Nikhil G. Thaker Chelsea C. Pinnix Valerie K. Reed Bouthaina S. Dabaja Department of Radiation Oncology MD Anderson Cancer Center Case 60 yo male Presented with right cervical LAD
Head and Neck: DLBCL Nikhil G. Thaker Chelsea C. Pinnix Valerie K. Reed Bouthaina S. Dabaja Department of Radiation Oncology MD Anderson Cancer Center Case 60 yo male Presented with right cervical LAD
Aggressive NHL and Hodgkin Lymphoma. Dr. Carolyn Faught November 10, 2017
 Aggressive NHL and Hodgkin Lymphoma Dr. Carolyn Faught November 10, 2017 What does aggressive mean? Shorter duration of symptoms Generally need treatment at time of diagnosis Immediate, few days, few weeks
Aggressive NHL and Hodgkin Lymphoma Dr. Carolyn Faught November 10, 2017 What does aggressive mean? Shorter duration of symptoms Generally need treatment at time of diagnosis Immediate, few days, few weeks
UPDATE Autologous Stem Cell Transplantation for Lymphoma and Myeloma
 UPDATE Autologous Stem Cell Transplantation for Lymphoma and Myeloma Supported by a grant from Supported by a grant from UPDATE Autologous Stem Cell Transplantation for Lymphoma and Myeloma Jonathan W.
UPDATE Autologous Stem Cell Transplantation for Lymphoma and Myeloma Supported by a grant from Supported by a grant from UPDATE Autologous Stem Cell Transplantation for Lymphoma and Myeloma Jonathan W.
Blood Cancers. Blood Cells. Blood Cancers: Progress and Promise. Bone Marrow and Blood. Lymph Nodes and Spleen
 Blood Cancers: Progress and Promise Mike Barnett & Khaled Ramadan Division of Hematology Department of Medicine Providence Health Care & UBC Blood Cancers Significant health problem Arise from normal cells
Blood Cancers: Progress and Promise Mike Barnett & Khaled Ramadan Division of Hematology Department of Medicine Providence Health Care & UBC Blood Cancers Significant health problem Arise from normal cells
Myelodysplasia/Myeloproliferative Neoplasms (MDS/MPN) Post-HCT Data
 Post-HCT Data") Instructions for Myelodysplasia/Myeloproliferative Neoplasms (MDS/MPN) Post-HCT Data (Form 2114) This section of the CIBMTR Forms Instruction Manual is intended to be a resource for completing the Myelodysplasia/Myeloproliferative
Instructions for Myelodysplasia/Myeloproliferative Neoplasms (MDS/MPN) Post-HCT Data (Form 2114) This section of the CIBMTR Forms Instruction Manual is intended to be a resource for completing the Myelodysplasia/Myeloproliferative
Lymphoma is a cancer that develops in the white blood cells (lymphocytes) of the lymphatic system, which is part of the body's immune system.
 of the lymphatic system, which is part of the body's immune system.") Scan for mobile link. Lymphoma Lymphoma is a cancer that develops in the white blood cells of the lymphatic system. Symptoms may include enlarged lymph nodes, unexplained weight loss, fatigue, night sweats
Scan for mobile link. Lymphoma Lymphoma is a cancer that develops in the white blood cells of the lymphatic system. Symptoms may include enlarged lymph nodes, unexplained weight loss, fatigue, night sweats
12 Dynamic Interactions between Hematopoietic Stem and Progenitor Cells and the Bone Marrow: Current Biology of Stem Cell Homing and Mobilization
 Table of Contents: PART I: Molecular and Cellular Basis of Hematology 1 Anatomy and Pathophysiology of the Gene 2 Genomic Approaches to Hematology 3 Regulation of Gene Expression, Transcription, Splicing,
Table of Contents: PART I: Molecular and Cellular Basis of Hematology 1 Anatomy and Pathophysiology of the Gene 2 Genomic Approaches to Hematology 3 Regulation of Gene Expression, Transcription, Splicing,
New Evidence reports on presentations given at EHA/ICML Bendamustine in the Treatment of Lymphoproliferative Disorders
 New Evidence reports on presentations given at EHA/ICML 2011 Bendamustine in the Treatment of Lymphoproliferative Disorders Report on EHA/ICML 2011 presentations Efficacy and safety of bendamustine plus
New Evidence reports on presentations given at EHA/ICML 2011 Bendamustine in the Treatment of Lymphoproliferative Disorders Report on EHA/ICML 2011 presentations Efficacy and safety of bendamustine plus
CLL & SLL: Current Management & Treatment. Dr. Isabelle Bence-Bruckler
 CLL & SLL: Current Management & Treatment Dr. Isabelle Bence-Bruckler Chronic Lymphocytic Leukemia Prolonged clinical course Chronic A particular type of white blood cell B lymphocyte Lymphocytic Cancer
CLL & SLL: Current Management & Treatment Dr. Isabelle Bence-Bruckler Chronic Lymphocytic Leukemia Prolonged clinical course Chronic A particular type of white blood cell B lymphocyte Lymphocytic Cancer
Case Workshop of Society for Hematopathology and European Association for Haematopathology
 Case 24 2007 Workshop of Society for Hematopathology and European Association for Haematopathology Aliyah Rahemtullah 1, Martin K Selig 1, Paola Dal Cin 2 and Robert P Hasserjian 1 Departments of Pathology,
Case 24 2007 Workshop of Society for Hematopathology and European Association for Haematopathology Aliyah Rahemtullah 1, Martin K Selig 1, Paola Dal Cin 2 and Robert P Hasserjian 1 Departments of Pathology,
Corporate Medical Policy
 Corporate Medical Policy Hematopoietic Stem-Cell Transplant for Non-Hodgkin Lymphomas File Name: Origination: Last CAP Review: Next CAP Review: Last Review: hematopoietic_stem-cell_transplant_for_non_hodgkin_lymphomas
Corporate Medical Policy Hematopoietic Stem-Cell Transplant for Non-Hodgkin Lymphomas File Name: Origination: Last CAP Review: Next CAP Review: Last Review: hematopoietic_stem-cell_transplant_for_non_hodgkin_lymphomas
Multiple Myeloma 101: Understanding Your Labs
 Multiple Myeloma 101: Understanding Your Labs Tim Wassenaar MD MS Hematologist, Director of Clinical Trials UW Cancer Center at ProHealth Care None Disclosures Outline Define hematopoiesis WBCs, RBCs,
Multiple Myeloma 101: Understanding Your Labs Tim Wassenaar MD MS Hematologist, Director of Clinical Trials UW Cancer Center at ProHealth Care None Disclosures Outline Define hematopoiesis WBCs, RBCs,
Easy Trick to Spot Leukemia for Pediatricians
 Easy Trick to Spot Leukemia for Pediatricians Piya Rujkijyanont, MD Division of Hematology-Oncology Department of Pediatrics Phramongkutklao Hospital Most Common Pediatric Cancers Age 0-14 Leukemia 32%
Easy Trick to Spot Leukemia for Pediatricians Piya Rujkijyanont, MD Division of Hematology-Oncology Department of Pediatrics Phramongkutklao Hospital Most Common Pediatric Cancers Age 0-14 Leukemia 32%
Leukocytosis - Some Learning Points
 Leukocytosis - Some Learning Points Koh Liang Piu Department of Hematology-Oncology National University Cancer Institute National University Health System Objectives of this talk: 1. To provide some useful
Leukocytosis - Some Learning Points Koh Liang Piu Department of Hematology-Oncology National University Cancer Institute National University Health System Objectives of this talk: 1. To provide some useful
Hodgkin's Lymphoma. Symptoms. Types
 Hodgkin's lymphoma (Hodgkin's disease) usually develops in the lymphatic system, a part of the body's immune system. This system carries disease-fighting white blood cells throughout the body. Lymph tissue
Hodgkin's lymphoma (Hodgkin's disease) usually develops in the lymphatic system, a part of the body's immune system. This system carries disease-fighting white blood cells throughout the body. Lymph tissue
Differential diagnosis of hematolymphoid tumors composed of medium-sized cells. Brian Skinnider B.C. Cancer Agency, Vancouver General Hospital
 Differential diagnosis of hematolymphoid tumors composed of medium-sized cells Brian Skinnider B.C. Cancer Agency, Vancouver General Hospital Lymphoma classification Lymphoma diagnosis starts with morphologic
Differential diagnosis of hematolymphoid tumors composed of medium-sized cells Brian Skinnider B.C. Cancer Agency, Vancouver General Hospital Lymphoma classification Lymphoma diagnosis starts with morphologic
Classification of Hematologic Malignancies. Patricia Aoun MD MPH
 Classification of Hematologic Malignancies Patricia Aoun MD MPH Objectives Know the basic principles of the current classification system for hematopoietic and lymphoid malignancies Understand the differences
Classification of Hematologic Malignancies Patricia Aoun MD MPH Objectives Know the basic principles of the current classification system for hematopoietic and lymphoid malignancies Understand the differences
Lymphoid Neoplasms. Sylvie Freeman Department of Clinical Immunology, University of Birmingham
 Lymphoid Neoplasms Sylvie Freeman Department of Clinical Immunology, University of Birmingham Incidence of Haematological Malignancies UK2001 (CRUK) Malignancy New Cases All Cancers 271,000 Leukaemia 6,760
Lymphoid Neoplasms Sylvie Freeman Department of Clinical Immunology, University of Birmingham Incidence of Haematological Malignancies UK2001 (CRUK) Malignancy New Cases All Cancers 271,000 Leukaemia 6,760
Leukemia and Myelodysplastic Syndromes
 Leukemia and Myelodysplastic Syndromes Lenise Taylor, RN, MN, AOCNS Heme Malignancies/BMT CNS Seattle Cancer Care Alliance/UWMC Lymphoid 1 Myeloid 2 Presenting Signs and Symptoms Diagnostic Evaluation
Leukemia and Myelodysplastic Syndromes Lenise Taylor, RN, MN, AOCNS Heme Malignancies/BMT CNS Seattle Cancer Care Alliance/UWMC Lymphoid 1 Myeloid 2 Presenting Signs and Symptoms Diagnostic Evaluation
Blood Cancers in the Community
 Over to you, mate Blood Cancers in the Community National Rural Health Conference NZ Rural General Practice Network April 7, 2018 Brian Grainger Haematology Registrar Auckland Acknowledgements Dr James
Over to you, mate Blood Cancers in the Community National Rural Health Conference NZ Rural General Practice Network April 7, 2018 Brian Grainger Haematology Registrar Auckland Acknowledgements Dr James
Lymphoma and Myeloma Kris3ne Kra4s, M.D.
 Lymphoma and Myeloma Kris3ne Kra4s, M.D. Hematologic Malignancies Leukemia Malignancy of hematopoie3c cells Starts in bone marrow, can spread to blood, nodes Myeloid or lymphoid Acute or chronic Lymphoma
Lymphoma and Myeloma Kris3ne Kra4s, M.D. Hematologic Malignancies Leukemia Malignancy of hematopoie3c cells Starts in bone marrow, can spread to blood, nodes Myeloid or lymphoid Acute or chronic Lymphoma
Low grade High grade , immune suppression chronic persistent inflammation viruses B-symptoms
 We've one category for lymphoid neoplasm which is the lymphoma in contrast to that of myeloid which has three categories; acute myeloid leukemias, myeloproliferative & myelodysplastic disorders. Lymphoma
We've one category for lymphoid neoplasm which is the lymphoma in contrast to that of myeloid which has three categories; acute myeloid leukemias, myeloproliferative & myelodysplastic disorders. Lymphoma
CELL-MEDIATED IMMUNITY
 LECTURE #4 1 LYMPHATIC SYSTEM 2 CELL-MEDIATED IMMUNITY T-lymphocytes (activated in the thymus) identify aggressors and try to destroy them through the production of lymphokines (synthesized proteins) Killer
LECTURE #4 1 LYMPHATIC SYSTEM 2 CELL-MEDIATED IMMUNITY T-lymphocytes (activated in the thymus) identify aggressors and try to destroy them through the production of lymphokines (synthesized proteins) Killer
Immunopathology of Lymphoma
 Immunopathology of Lymphoma Noraidah Masir MBBCh, M.Med (Pathology), D.Phil. Department of Pathology Faculty of Medicine Universiti Kebangsaan Malaysia Lymphoma classification has been challenging to pathologists.
Immunopathology of Lymphoma Noraidah Masir MBBCh, M.Med (Pathology), D.Phil. Department of Pathology Faculty of Medicine Universiti Kebangsaan Malaysia Lymphoma classification has been challenging to pathologists.
Allogeneic Hematopoietic Stem-Cell Transplantation for Myelodysplastic Syndromes and Myeloproliferative Neoplasms. Policy Specific Section:
 Medical Policy Allogeneic Hematopoietic Stem-Cell Transplantation for Myelodysplastic Syndromes and Myeloproliferative Type: Medical Necessity and Investigational / Experimental Policy Specific Section:
Medical Policy Allogeneic Hematopoietic Stem-Cell Transplantation for Myelodysplastic Syndromes and Myeloproliferative Type: Medical Necessity and Investigational / Experimental Policy Specific Section:
MECHANISMS OF HUMAN DISEASE: LABORATORY SESSIONS LYMPHOMA. April 16, 2008
 MECHANISMS OF HUMAN DISEASE: LABORATORY SESSIONS LYMPHOMA April 16, 2008 FACULTY COPY GOAL: Learn the appearance of normal peripheral blood elements and lymph nodes. Recognize abnormal peripheral blood
MECHANISMS OF HUMAN DISEASE: LABORATORY SESSIONS LYMPHOMA April 16, 2008 FACULTY COPY GOAL: Learn the appearance of normal peripheral blood elements and lymph nodes. Recognize abnormal peripheral blood
Lymphatic System Disorders
 Lymphatic System Disorders Lymphomas Malignant neoplasms involving lymphocyte proliferation in lymph nodes Specific causes not identified // Higher risk in adults who received radiation during childhood
Lymphatic System Disorders Lymphomas Malignant neoplasms involving lymphocyte proliferation in lymph nodes Specific causes not identified // Higher risk in adults who received radiation during childhood
2012 by American Society of Hematology
 2012 by American Society of Hematology Common Types of HIV-Associated Lymphomas DLBCL includes primary CNS lymphoma (PCNSL) Burkitt Lymphoma HIV-positive patients have a 60-200 fold increased incidence
2012 by American Society of Hematology Common Types of HIV-Associated Lymphomas DLBCL includes primary CNS lymphoma (PCNSL) Burkitt Lymphoma HIV-positive patients have a 60-200 fold increased incidence
Lymphoma John P. Leonard, M.D.
 Lymphoma 2017 John P. Leonard, M.D. Richard T. Silver Distinguished Professor of Hematology and Medical Oncology Associate Dean for Clinical Research Vice Chairman, Department of Medicine Disclosures Consulting
Lymphoma 2017 John P. Leonard, M.D. Richard T. Silver Distinguished Professor of Hematology and Medical Oncology Associate Dean for Clinical Research Vice Chairman, Department of Medicine Disclosures Consulting
Disclosures/COI. Cases in Hematopathology. Outline. Heme Path Findings Not to Miss. Normal Peripheral Smear 6/30/2016
 Disclosures/COI Cases in Hematopathology Vamsi Kota Assistant Professor Department of Hematology & Medical Oncology Leukemia/BMT I have no disclosures or conflicts of interest regarding this presentation.
Disclosures/COI Cases in Hematopathology Vamsi Kota Assistant Professor Department of Hematology & Medical Oncology Leukemia/BMT I have no disclosures or conflicts of interest regarding this presentation.
Done By : WESSEN ADNAN BUTHAINAH AL-MASAEED
 Done By : WESSEN ADNAN BUTHAINAH AL-MASAEED Acute Myeloid Leukemia Firstly we ll start with this introduction then enter the title of the lecture, so be ready and let s begin by the name of Allah : We
Done By : WESSEN ADNAN BUTHAINAH AL-MASAEED Acute Myeloid Leukemia Firstly we ll start with this introduction then enter the title of the lecture, so be ready and let s begin by the name of Allah : We
Abstracting Hematopoietic Neoplasms
 CASE 1: LYMPHOMA PHYSICAL EXAMINATION 43yo male with a history of lower gastrointestinal bleeding and melena undergoing colonoscopy and biopsy to rule out neoplasm versus inflammation. Patient had no other
CASE 1: LYMPHOMA PHYSICAL EXAMINATION 43yo male with a history of lower gastrointestinal bleeding and melena undergoing colonoscopy and biopsy to rule out neoplasm versus inflammation. Patient had no other
Harmesh Naik, MD. GME Presentation to Family Practice Residents October 16, 2013.
 Harmesh Naik, MD. GME Presentation to Family Practice Residents October 16, 2013. Lymphoma: Lympho-proliferative disorders arising from lymphocytes Heterogeneous group of disorders Differing patterns of
Harmesh Naik, MD. GME Presentation to Family Practice Residents October 16, 2013. Lymphoma: Lympho-proliferative disorders arising from lymphocytes Heterogeneous group of disorders Differing patterns of
Myeloproliferative Disorders - D Savage - 9 Jan 2002
 Disease Usual phenotype acute leukemia precursor chronic leukemia low grade lymphoma myeloma differentiated Total WBC > 60 leukemoid reaction acute leukemia Blast Pro Myel Meta Band Seg Lymph 0 0 0 2
Disease Usual phenotype acute leukemia precursor chronic leukemia low grade lymphoma myeloma differentiated Total WBC > 60 leukemoid reaction acute leukemia Blast Pro Myel Meta Band Seg Lymph 0 0 0 2
Patterns of Lymphoid Neoplasia in Peripheral Blood. Leon F. Baltrucki, M.D. Leon F. Baltrucki, M.D. Disclosure
 Patterns of Lymphoid Neoplasia in Peripheral Blood Leon F. Baltrucki, M.D. Leon F. Baltrucki, M.D. Disclosure Dr Baltrucki has received an honorarium for his participation as a faculty presenter in this
Patterns of Lymphoid Neoplasia in Peripheral Blood Leon F. Baltrucki, M.D. Leon F. Baltrucki, M.D. Disclosure Dr Baltrucki has received an honorarium for his participation as a faculty presenter in this
Treatment of Waldenström s Macroglobulinemia Mayo Consensus
 Treatment of Waldenström s Macroglobulinemia Mayo Consensus Scottsdale, Arizona Rochester, Minnesota Jacksonville, Florida Mayo Clinic College of Medicine Mayo Clinic Comprehensive Cancer Center Mayo Clinic
Treatment of Waldenström s Macroglobulinemia Mayo Consensus Scottsdale, Arizona Rochester, Minnesota Jacksonville, Florida Mayo Clinic College of Medicine Mayo Clinic Comprehensive Cancer Center Mayo Clinic
Charles Mxxx DCEM2 Toulouse Purpan Medical School 01/26/2012 ECN Item 162
 Charles Mxxx DCEM2 Toulouse Purpan Medical School 01/26/2012 ECN Item 162 Definition Pathophysiology Clinical signs and symptoms Biology and Diagnosis Different types of AL Prognosis and Treatment Malignant
Charles Mxxx DCEM2 Toulouse Purpan Medical School 01/26/2012 ECN Item 162 Definition Pathophysiology Clinical signs and symptoms Biology and Diagnosis Different types of AL Prognosis and Treatment Malignant
Case Study Discussions on the Nurse s Role in Caring for Patients With Hematologic Malignancies
 Case Study Discussions on the Nurse s Role in Caring for Patients With Hematologic Malignancies Case Study Discussions on the Nurse s Role in Caring for Patients With Hematologic Malignancies Welcome and
Case Study Discussions on the Nurse s Role in Caring for Patients With Hematologic Malignancies Case Study Discussions on the Nurse s Role in Caring for Patients With Hematologic Malignancies Welcome and
Chronic Lymphocytic Leukemia Early Detection, Diagnosis, and Staging
 Chronic Lymphocytic Leukemia Early Detection, Diagnosis, and Staging Detection and Diagnosis Catching cancer early often allows for more treatment options. Some early cancers may have signs and symptoms
Chronic Lymphocytic Leukemia Early Detection, Diagnosis, and Staging Detection and Diagnosis Catching cancer early often allows for more treatment options. Some early cancers may have signs and symptoms
Understanding the role of ex vivo T cell depletion
 Prevention of graftversus-host disease (GVHD) Understanding the role of ex vivo T cell depletion Information for patients undergoing allogeneic stem cell transplantation in AML and their families 2 This
Prevention of graftversus-host disease (GVHD) Understanding the role of ex vivo T cell depletion Information for patients undergoing allogeneic stem cell transplantation in AML and their families 2 This
Waldenstrom s Macroglobulinemia
 Waldenstrom s Macroglobulinemia : Introduction Waldenstrom s macroglobulinemia (WM) is a lymphoma, or cancer of the lymphatic system. It occurs in a type of white blood cell called a B-lymphocyte or B-cell,
Waldenstrom s Macroglobulinemia : Introduction Waldenstrom s macroglobulinemia (WM) is a lymphoma, or cancer of the lymphatic system. It occurs in a type of white blood cell called a B-lymphocyte or B-cell,
Q&A Session Collecting Cancer Data: Hematopoietic and Lymphoid Neoplasms Thursday, November 6, 2014
 Q&A Session Collecting Cancer Data: Hematopoietic and Lymphoid Neoplasms Thursday, November 6, 2014 Q: If polycythemia ruba vera (PRV) or essential thrombocythemia (ET) is diagnosed by peripheral smear,
Q&A Session Collecting Cancer Data: Hematopoietic and Lymphoid Neoplasms Thursday, November 6, 2014 Q: If polycythemia ruba vera (PRV) or essential thrombocythemia (ET) is diagnosed by peripheral smear,
Contents. vii. Preface... Acknowledgments... v xiii
 Contents Preface... Acknowledgments... v xiii SECTION I 1. Introduction... 3 Knowledge-Based Diagnosis... 4 Systematic Examination of the Lymph Node... 7 Cell Type Identification... 9 Cell Size and Cellularity...
Contents Preface... Acknowledgments... v xiii SECTION I 1. Introduction... 3 Knowledge-Based Diagnosis... 4 Systematic Examination of the Lymph Node... 7 Cell Type Identification... 9 Cell Size and Cellularity...
Idelalisib treatment is associated with improved cytopenias in patients with relapsed/refractory inhl and CLL
 Idelalisib treatment is associated with improved cytopenias in patients with relapsed/refractory inhl and CLL Susan M O Brien, Andrew J Davies, Ian W Flinn, Ajay K Gopal, Thomas J Kipps, Gilles A Salles,
Idelalisib treatment is associated with improved cytopenias in patients with relapsed/refractory inhl and CLL Susan M O Brien, Andrew J Davies, Ian W Flinn, Ajay K Gopal, Thomas J Kipps, Gilles A Salles,
Corporate Medical Policy
 Corporate Medical Policy Hematopoietic Cell Transplantation for CLL and SLL File Name: Origination: Last CAP Review: Next CAP Review: Last Review: hematopoietic_cell_transplantation_for_cll_and_sll 2/2001
Corporate Medical Policy Hematopoietic Cell Transplantation for CLL and SLL File Name: Origination: Last CAP Review: Next CAP Review: Last Review: hematopoietic_cell_transplantation_for_cll_and_sll 2/2001
LYMPHOMAS an overview of some subtypes of NHLs
 One of the confusing aspects of the lymphoid neoplasms concerns the use of the descriptive terms "leukemia" and "lymphoma." LYMPHOMAS an overview of some subtypes of NHLs Leukemia is used for lymphoid
One of the confusing aspects of the lymphoid neoplasms concerns the use of the descriptive terms "leukemia" and "lymphoma." LYMPHOMAS an overview of some subtypes of NHLs Leukemia is used for lymphoid
Candidates must answer ALL questions
 Time allowed: Three hours. Part 1 examination Haematology: First paper Tuesday 22 March 2016 Candidates must answer ALL questions Question 1: General Haematology A 16 year old non-european is referred
Time allowed: Three hours. Part 1 examination Haematology: First paper Tuesday 22 March 2016 Candidates must answer ALL questions Question 1: General Haematology A 16 year old non-european is referred
Lymphoma: What You Need to Know
 Lymphoma: What You Need to Know www.lymphoma.org.au Lymphoma What You Need to Know Whilst Lymphoma Australia (LA) has made every effort to confirm the accuracy of the information contained herein, it makes
Lymphoma: What You Need to Know www.lymphoma.org.au Lymphoma What You Need to Know Whilst Lymphoma Australia (LA) has made every effort to confirm the accuracy of the information contained herein, it makes
HENATOLYMPHOID SYSTEM THIRD YEAR MEDICAL STUDENTS- UNIVERSITY OF JORDAN AHMAD T. MANSOUR, MD. Parts 2 and 3
 HENATOLYMPHOID SYSTEM THIRD YEAR MEDICAL STUDENTS- UNIVERSITY OF JORDAN AHMAD T. MANSOUR, MD Parts 2 and 3 NEOPLASTIC LYMPHOID DISEASES Introduction o The bone marrow is the source of all cells in the
HENATOLYMPHOID SYSTEM THIRD YEAR MEDICAL STUDENTS- UNIVERSITY OF JORDAN AHMAD T. MANSOUR, MD Parts 2 and 3 NEOPLASTIC LYMPHOID DISEASES Introduction o The bone marrow is the source of all cells in the
Hematologic Malignancies. Kim Noonan, RN, ANP, AOCN
 Hematologic Malignancies Kim Noonan, RN, ANP, AOCN Hematologic Malignancies Cancers that affect blood, bone marrow and lymphatic system. Liquid tumors vs solid tumors Leukemia Lymphoma Multiple Myeloma
Hematologic Malignancies Kim Noonan, RN, ANP, AOCN Hematologic Malignancies Cancers that affect blood, bone marrow and lymphatic system. Liquid tumors vs solid tumors Leukemia Lymphoma Multiple Myeloma
LYMPHOMA DIAGNOSIS and PROGNOSIS. LC Lim Dept of Hematology Singapore General Hospital
 LYMPHOMA DIAGNOSIS and PROGNOSIS LC Lim Dept of Hematology Singapore General Hospital OUTLINE Accurate diagnosis Define subtype : WHO classification Staging : Defines extent of involvement Prognosis Determining
LYMPHOMA DIAGNOSIS and PROGNOSIS LC Lim Dept of Hematology Singapore General Hospital OUTLINE Accurate diagnosis Define subtype : WHO classification Staging : Defines extent of involvement Prognosis Determining
Appendix 6: Indications for adult allogeneic bone marrow transplant in New Zealand
 Appendix 6: Indications for adult allogeneic bone marrow transplant in New Zealand This list provides indications for the majority of adult BMTs that are performed in New Zealand. A small number of BMTs
Appendix 6: Indications for adult allogeneic bone marrow transplant in New Zealand This list provides indications for the majority of adult BMTs that are performed in New Zealand. A small number of BMTs
Myeloid neoplasms. Early arrest in the blast cell or immature cell "we call it acute leukemia" Myoid neoplasm divided in to 3 major categories:
 Myeloid neoplasms Note: Early arrest in the blast cell or immature cell "we call it acute leukemia" Myoid neoplasm divided in to 3 major categories: 1. AML : Acute myeloid leukemia(stem cell with myeloid
Myeloid neoplasms Note: Early arrest in the blast cell or immature cell "we call it acute leukemia" Myoid neoplasm divided in to 3 major categories: 1. AML : Acute myeloid leukemia(stem cell with myeloid
PROBLEMS OF THE HEMATOLOGICAL SYSTEM
 PROBLEMS OF THE HEMATOLOGICAL SYSTEM UNIT 5 Review A & P of Hematological system Outline focused exam Differentiate and start to evaluate diagnostic exams used to assess problems of the hematological system
PROBLEMS OF THE HEMATOLOGICAL SYSTEM UNIT 5 Review A & P of Hematological system Outline focused exam Differentiate and start to evaluate diagnostic exams used to assess problems of the hematological system
Index. Note: Page numbers of article titles are in boldface type.
 Index Note: Page numbers of article titles are in boldface type. A Anemia(s), 412 426 categories in morphologic approach to, macrocytic, 412 414 microcytic, 412 414 normocytic, 412 413 categorizing, 412
Index Note: Page numbers of article titles are in boldface type. A Anemia(s), 412 426 categories in morphologic approach to, macrocytic, 412 414 microcytic, 412 414 normocytic, 412 413 categorizing, 412
Acute myeloid leukemia. M. Kaźmierczak 2016
 Acute myeloid leukemia M. Kaźmierczak 2016 Acute myeloid leukemia Malignant clonal disorder of immature hematopoietic cells characterized by clonal proliferation of abnormal blast cells and impaired production
Acute myeloid leukemia M. Kaźmierczak 2016 Acute myeloid leukemia Malignant clonal disorder of immature hematopoietic cells characterized by clonal proliferation of abnormal blast cells and impaired production
Lymphoma 101. Nathalie Johnson, MDPhD. Division of Hematology Jewish General Hospital Associate Professor of Medicine, McGill University
 Lymphoma 101 Nathalie Johnson, MDPhD Division of Hematology Jewish General Hospital Associate Professor of Medicine, McGill University Disclosures Consultant and Advisory boards for multiple companies
Lymphoma 101 Nathalie Johnson, MDPhD Division of Hematology Jewish General Hospital Associate Professor of Medicine, McGill University Disclosures Consultant and Advisory boards for multiple companies
NON HODGKINS LYMPHOMA: AGGRESSIVE Updated June 2015 by Dr. Manna (PGY-5 Medical Oncology Resident, University of Calgary)
") NON HODGKINS LYMPHOMA: AGGRESSIVE Updated June 2015 by Dr. Manna (PGY-5 Medical Oncology Resident, University of Calgary) Reviewed by Dr. Michelle Geddes (Staff Hematologist, University of Calgary) and
NON HODGKINS LYMPHOMA: AGGRESSIVE Updated June 2015 by Dr. Manna (PGY-5 Medical Oncology Resident, University of Calgary) Reviewed by Dr. Michelle Geddes (Staff Hematologist, University of Calgary) and