Thyroid Neoplasm. ORL-Head and neck Surgery 2014
|
|
|
- Lora Oliver
- 5 years ago
- Views:
Transcription
1 In The Name of God
2 Thyroid Neoplasm ORL-Head and neck Surgery 2014
3 Malignant Neoplasm
4 By age 90, virtually everyone has nodules Estimates of cancer prevalence at autopsy 4% to 36%
5 Why these lesions are important?
6 Assessment of risk of thyroid nodules requires understanding of clinical, demographic, imaging, cytopathologic, and now biomarker profiles; none of these factors alone represents a sufficient decision-making factor.
7 The incidence of this malignancy has been increasing over the last decade.
8 Advanced radiologic imaging
9 These scans commonly reveal small, nonpalpable thyroid nodules, which in the past would never have been identified because they were too small to detect by palpation, and too small to cause symptoms to patients
10 What s the problem 1. These incidental findings unnecessarily create patients with cancer with all the attendant anxiety, surveillance needs, and financial ramifications. 2. Patients are exposed to harm from what is ultimately unnecessary treatment. 3. These patients affect the validity of studies designed to understand and mitigate the risks of death or recurrence from thyroid cancer by serving to falsely improve the results of clinical trials
11 The chief challenge to clinicians today is deciding which nodules require workup, and how aggressively to treat them
12
13 Risk Factors
14 Age Gender History of radiation exposure Family history of thyroid cancer Cancer syndromes
15
16 Workup of the thyoid nodule
17 Laboratory Examination
18 TSH Hyperthyroidism(15%) Hypothyroidism(2.3%) So: TSH assessment will allow identification of people with thyroid dysfunction requiring treatment regardless of the rest of the workup.
19 Calcitonin Measurment There is a high false positive rate (59% or more) in some studies. The serum calcitonin cutoff levels for sporadic medullary thyroid cancer have not been agreed on.
20 Antithyroid peroxidase antibodies Serum thyroglobulin
21 Scintigraphy
22 Identifying hyperfunctioning nodules when a low TSH is found on initial testing Determining which nodule to sample in patients with multiple nodules (Replace with US)
23 Hot Cold Indeterminate
24 Ultrasonography
25 Thyroid ultrasound is the first choice of imaging studies for thyroid gland evaluation
26 Ultrasound has been shown to be more accurate than physical examination in detecting nodules
27 Nodule size Detailed characteristics Anatomic location Condition of nearby structures are all clearly delineated
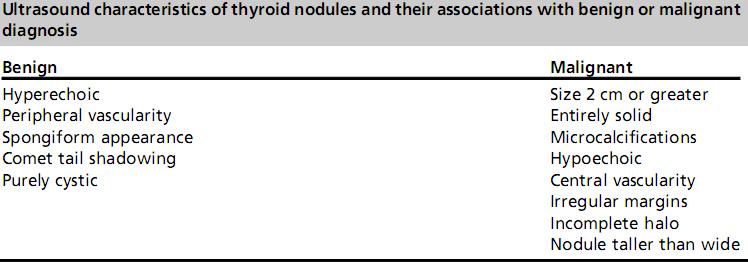
28 Ultrasound qualities of a nodule in isolation are not diagnostic of a malignancy They do indicate which nodules are more likely to harbor malignancy Can inform decision-making about nodule selection for biopsy.
29 1. Microcalcifications 2. Size greater than 2 cm 3. Nodules that are entirely solid composition
30
31 Both the American Association of Clinical Endocrinologists (AACE) and the American Thyroid Association (ATA) guidelines suggest nodules as small as 5 mm might be biopsied and should be followed based on risk factors alone
32 Nodules greater than 4 cm, needle biopsy results were frequently false negative They eventually affect speech and swallow function due to size, surgical intervention should be considered.
33 Who can do it?
34 Defining competency is one of the central issues in all of medical education Essential equipment and the economics of clinic-based US
35
36 1) Hypoechogenicity 2) Irregular (microlobulated) margins 3) Microcalcifications 4) Anteroposterior to transverse diameter ratio greater than 1 5) Intranodular vascularity 6) Size 7) Significant growth.
37 Ultrasound has proven to be the most sensitive imaging modality for detecting suspicious lateral neck nodes.
38 The characteristic findings of shape change, loss of the normal internal structure,, and change in blood flow all contribute to the identification of metastatic nodes as small as 3 mm
39 Fine Needle Aspiration Biopsy
40 Traditional FNA Is performed by method of manual palpation The size threshold for palpating thyroid nodules is 1.5 to 2.0 cm, and up to 30% of FNA biopsies without ultrasound guidance can be nondiagnostic
41 The ATA guidelines suggest biopsy of those nodules preferentially that have the most worrisome ultrasound characteristics
42 ATA 2009 Guidelines also suggest that if there are multiple nodules and none have characteristics indicative of malignancy, it is reasonable to biopsy the largest one
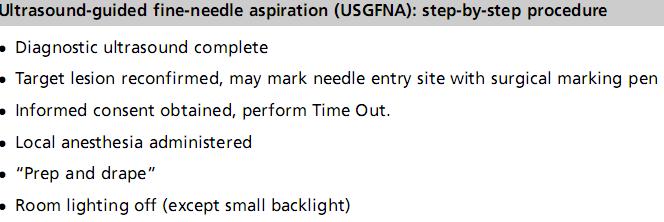
43 USGFNA Reduced the number of inadequate samples by half In one series, USGFNA, resulting in 14% reclassification to diagnoses of malignancies limit the number of needle passes required
44
45 Needle size 1.5-inch (38-mm) length, 25-gauge needles or longer (40 50 mm) needles for lesions at greater depth. Calcified masses may be more amenable to biopsy with a finer needle, such as a 2 7 gauge. Large needle for prior failed FNA

46

47
48 Number of needle passes
49 Staining Method Papanicolaou staining: nuclear chromatin, groundglass nuclei, and nuclear grooves Giemsa stain: characteristics of cytoplasm and colloid
 cyst fluid with or without")
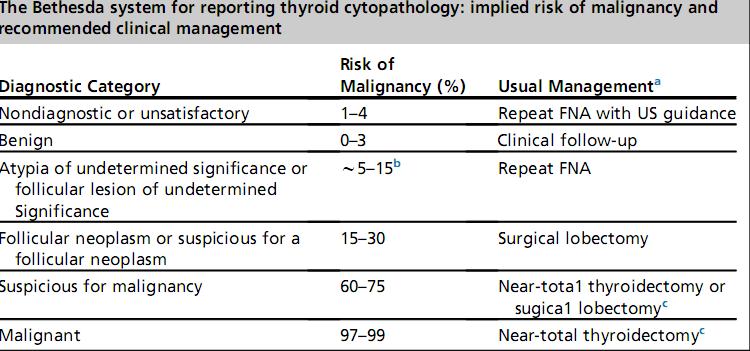
50 The Bethesda I (nondiagnostic/unsatisfact ory) Fewer than 6 groups of well-preserved, wellstained follicular cells; Poorly prepared, poorly stained, obscured follicular cells (excessively bloody specimens) cyst fluid with or without histiocytes
51 In inflammatory conditions of the thyroid, such as lymphocytic thyroiditis, abscess, and granulomatous thyroiditis, follicular cells may be sparse and there is no minimum requirement for adequacy for follicular cells when inflammation predominates.
 nodule 2. colloid nodule 3.")
52 The Bethesda II BENIGN THYROID LESIONS Nodular goiter: 1. hyperplastic (adenomatoid) nodule 2. colloid nodule 3. nodules in Graves disease

53 The Bethesda II Thyroiditis 1. Lymphocytic thyroiditis 2. Granulomatous thyroiditis 3. Acute thyroiditis

54 The Bethesda VI (malignant) 1. Papillary Ca 2. Medullary Ca 3. Poorly differentiated Ca 4. Anaplastic Ca 5. lymphoma 6. Various metastatic tumor
55 INDETERMINATE THYROID LESIONS
56 Cases diagnosed as atypical, follicular neoplasm, and suspicious for malignancy were lumped together in one category
57 The Bethesda III Atypia of Undetermined Significance/Follicular Lesion of Undetermined Significance The architectural and/or cytologic atypia is not sufficient to be classified as suspicious for follicular neoplasm, SFM, or malignant but is more than confidently diagnosed as benign

58 The Bethesda III 1. Clinicians should be aware that this is a category of last resort. 2. pathologists make significant efforts not to use this designation indiscriminately. 3. The frequency of AUS/FLUS interpretation should be approximately 7% of all thyroid FNA interpretations.
, usually in a highly cellular specimen 2.")
59 The Bethesda IV Follicular neoplasm / Suspicious for Follicular Neoplasm 1. The hallmark of this category is the presence of an abnormal architecture (architectural atypia), usually in a highly cellular specimen 2. FNHCT/SFNHTC should be used when at least 75% of the cells show Hurthle cell phenotype

60 Bethesda V Suspicious for Malignancy when some features of malignancy raise a strong suspicion for malignancy but the findings are not sufficient for a definitive diagnosis either qualitatively or quantitatively 1. uncommon variants of the respective malignancies 2. overlapping features with benign conditions (lymphocytic thyroiditis)suboptimal sampling.
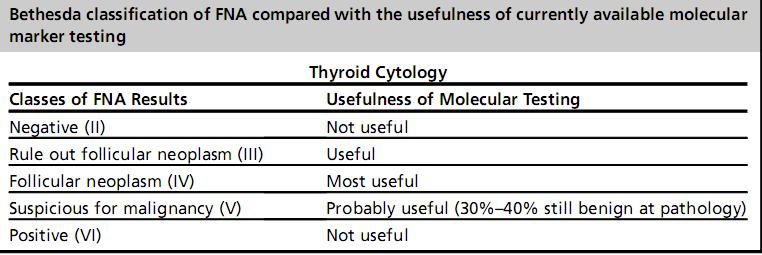
61 Needle biopsy results that are read as benign or malignant provide clear data on which to make clinical decisions. Up to nearly a third of needle biopsies will be returned as cytologically indeterminate.
62 Molecular Markers
63 Molecular testing of needle biopsy specimens read as malignant will not add useful information to the therapeutic decisionmaking process
64 BRAF RAS RET/PTC
65
66 Overall, tumor pathologic features continue to be most indicative of prognosis and therefore most clinically useful.
67
68 Treatment Modalities
69 Surgery Lobectomy ± Isthmectomy Total thyroidectomy Vs less than total Neck dissection
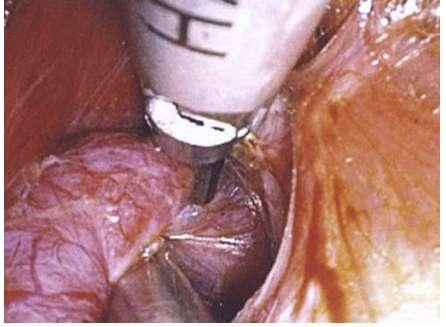
70 Surgical Technique Conventional thyroidectomy Minimally invasive cervical approach Remote access approaches
71 These alternative approaches have been applied to small, low-risk, well-differentiated thyroid cancers
72 Difficult or even unsafe in instances of large goiters, substernal or retropharyngeal extension, or thyroiditis. Furthermore, patients with thyroid malignancies need to be carefully considered to provide the most oncologically appropriate surgery for their disease.
73
74

75
76
77 The preoperative detection of lymph node involvement by either clinical examination or imaging can significantly clarify the goal of neck management and make clear the distinction between a prophylactic and therapeutic neck dissection.

78 Central Lymph Node Compartment Include the prelaryngeal (Delphian), pretracheal, and paratracheal nodes. An adequate unilateral central neck dissection, as defined by the ATA, should include the prelaryngeal, pretracheal, and the ipsilateral paratracheal nodal group. If performed with therapeutic intent, it is recommended that the dissection be extended to include bilateral paratracheal nodal groups.
79 Lateral compartment Meta-analysis data: high prevalence of multilevel disease: II 53%, III71%, IV 66% V 25% The ATA has further reviewed the lateral neck dissection and recommends a therapeutic dissection of levels IIa, III, IV, and Vb when suspicious
80 Prophylactic neck dissection Current guidelines recommend considering a prophylactic central neck dissection if other factors in patient presentation prompt a total thyroidectomy. ATA, which broadly suggest considering prophylactic central neck dissection, especially inpatients with advanced primary tumors larger than 4 cm
81 Consider a prophylactic central compartment neck dissection in papillary thyroid carcinomas that are either large tumors (>4 cm) or those with extrathyroidal extension
82 Routine prophylactic central neck dissections for follicular carcinomas are therefore not recommended
83 Hurthle cell carcinoma Literature and recommendations support a therapeutic central and/ or lateral compartment neck dissection for clinically involved nodes in Hurthle cell carcinoma and suggest considering a prophylactic central compartment neck dissection if a TT is prompted by other factors
84 Medullary Ca Routine central compartment neck dissection is recommended for patients with sporadic medullary thyroid cancer greater than 1 cm or patients with bilateral thyroid disease. Lateral neck dissection may be reserved for patients with clinically evident disease on preoperative examination or imaging. patients with even limited central involvement (1 3 positive nodes) have a high rate of lateral compartment disease. Thus, some clinicians have advocated for prophylactic lateral neck dissection when medullary carcinoma has spread to the central lymph node compartment.
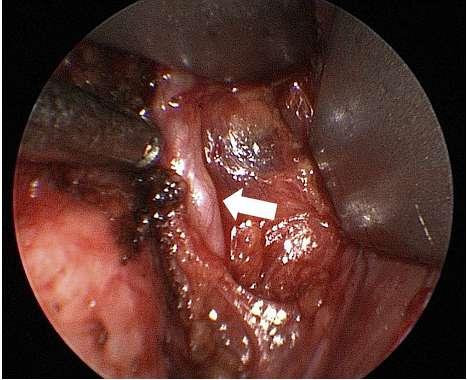
85 Surgical technique Central compartment Dissection begins at the innominate artery below and ends at the hyoid bone above. The lateral extent of the central compartment dissection is the medial border of the carotid sheath Once an indication for central compartment dissection has been confirmed, the surgeon should be as comprehensive as possible in removing nodes Preserve the anatomic integrity Minimize trauma to both the recurrent laryngeal nerves and vascularized parathyroid
86 Modified Radical Neck Dissection (Levels II, III, IV, and V) Direct invasion or true nodal fixation is uncommon for metastases of DTC Nodal berry-picking procedures are associated with unacceptably high levels of disease recurrence in the neck and should not be performed.
87 Surgical Notes Careful attention must be paid to the route of common metastatic spread: along the superior thyroid artery and the transverse cervical artery. Small nodes can be missed if the surgeon is rushed or not systematic in the dissection of this crucial area.
88 POSTOPERATIVE CARE AND MANAGEMENT
89 Hypoparathyroidism and Hypocalcemia Postoperative period strongly predict glandular function. Those in a low but detectable range predict a higher probability of transient or permanent hypocalcemia. Moreover, undetectable ipth levels are strongly correlated with hypocalcemia requiring intravenous infusion of calcium gluconate in the postoperative period.
90 Empiric oral supplementation with elemental calcium and vitamin D is generally warranted after paratracheal and mediastinal lymph node dissection. Intravenous calcium gluconate is reserved for patients with symptomatic hypocalcemia manifest by perioral numbness or tingling in the fingers or toes.
91 An infusion can be delivered by adding 10 ampoules of calcium gluconate to a 500-mL of normal saline and beginning at 30 ml/h, titrating up as needed to control symptoms.
92 Recurrent Laryngeal Nerve Injury The absence of voice disturbance does not guarantee normal nerve function; vocal cord paralysis (identified by laryngoscopy) is more sensitive at identifying recurrent laryngeal nerve defects caused by invasive thyroid malignancy.
93 Spinal Accessory Nerve Rehabilitation Even after preservation of the spinal accessory nerve, circumferential dissection can lead to devascularization and subsequent fibrosis. Therefore, early, if not immediate, postoperative rehabilitation is mandatory especially when level II-b is dissected.
94 Other Malignancies Anaplastic Ca Lymphoma Metastatic Ca
95 I-Ablation
96 Postoperative RT
97 CLOSING THOUGHTS ABOUT THYROID NODULE EVALUATION
98 Risk of Death for the Patient Found to Have a Thyroid Cancer
99 It has often been said that well-differentiated thyroid carcinoma is a disease of morbidity and not mortality
100 The point of evaluating a patient with a thyroid nodule is to determine whether a cancer is present. It is important to remember that, although everyone fears cancer, the outlook for patients diagnosed with papillary thyroid cancer, which is about 88% of thyroid cancers diagnosed in the United States, is excellent.
101 The 20-year survival for papillary thyroid cancer of any size confined to the thyroid gland at the time of diagnosis is 99%. For some patients, their competing risk of death from their other illnesses will be much greater, making workup of a thyroid nodule of lower utility to them. At a rate of 0.5 per 100,000 people, the mortality due to thyroid cancer is about the same as it is for tuberculosis that is, very rare.
102 In recent years, selected small cancers have been observed rather than operated on immediately Among those that grow or spread, surgical salvage has been successful, which means that delaying treatment will not necessarily present a problem for patients. These facts should be part of the mental algorithm used when talking with patients about the decision to evaluate a thyroid nodule.

103 Thanks for your patience
4/22/2010. Hakan Korkmaz, MD Assoc. Prof. of Otolaryngology Ankara Dıșkapı Training Hospital-Turkey.
 Management of Differentiated Thyroid Cancer: Head Neck Surgeon Perspective Hakan Korkmaz, MD Assoc. Prof. of Otolaryngology Ankara Dıșkapı Training Hospital-Turkey Thyroid gland Small endocrine gland:
Management of Differentiated Thyroid Cancer: Head Neck Surgeon Perspective Hakan Korkmaz, MD Assoc. Prof. of Otolaryngology Ankara Dıșkapı Training Hospital-Turkey Thyroid gland Small endocrine gland:
Thyroid nodules - medical and surgical management. Endocrinology and Endocrine Surgery Manchester Royal Infirmary
 Thyroid nodules - medical and surgical management JRE Davis NR Parrott Endocrinology and Endocrine Surgery Manchester Royal Infirmary Thyroid nodules - prevalence Thyroid nodules common, increase with
Thyroid nodules - medical and surgical management JRE Davis NR Parrott Endocrinology and Endocrine Surgery Manchester Royal Infirmary Thyroid nodules - prevalence Thyroid nodules common, increase with
Approach to Thyroid Nodules
 Approach to Thyroid Nodules Alice Y.Y. Cheng, MD, FRCPC Twitter: @AliceYYCheng Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted
Approach to Thyroid Nodules Alice Y.Y. Cheng, MD, FRCPC Twitter: @AliceYYCheng Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted
Thyroid Nodule. Disclosure. Learning Objectives P A P A P A 3/18/2014. Nothing to disclose.
 Thyroid Nodule Evaluating the patient with a thyroid nodule and some management options. Miguel V. Valdez PA C Disclosure Nothing to disclose. Learning Objectives Examination of thyroid gland Options for
Thyroid Nodule Evaluating the patient with a thyroid nodule and some management options. Miguel V. Valdez PA C Disclosure Nothing to disclose. Learning Objectives Examination of thyroid gland Options for
Reoperative central neck surgery
 Reoperative central neck surgery R. Pandev, I. Tersiev, M. Belitova, A. Kouizi, D. Damyanov University Clinic of Surgery, Section Endocrine Surgery University Hospital Queen Johanna ISUL Medical University
Reoperative central neck surgery R. Pandev, I. Tersiev, M. Belitova, A. Kouizi, D. Damyanov University Clinic of Surgery, Section Endocrine Surgery University Hospital Queen Johanna ISUL Medical University
40 TH EUROPEAN CONGRESS 0F CYTOLOGY LIVERPOOL, UK October 2-5, 2016
 Outcomes from the diagnostic approach of thyroid lesions using US-FNA and LBC in clinical practice Emmanouel Mastorakis MD PhD Cytopathologist Director in Cytopathology Laboratory Regional General Hospital
Outcomes from the diagnostic approach of thyroid lesions using US-FNA and LBC in clinical practice Emmanouel Mastorakis MD PhD Cytopathologist Director in Cytopathology Laboratory Regional General Hospital
2015 American Thyroid Association Thyroid Nodule and Cancer Guidelines
 2015 American Thyroid Association Thyroid Nodule and Cancer Guidelines Angela M. Leung, MD, MSc, ECNU November 5, 2016 Outline Workup of nontoxic thyroid nodule(s) Ultrasound FNAB Management of FNAB results
2015 American Thyroid Association Thyroid Nodule and Cancer Guidelines Angela M. Leung, MD, MSc, ECNU November 5, 2016 Outline Workup of nontoxic thyroid nodule(s) Ultrasound FNAB Management of FNAB results
Evaluation and Management of Thyroid Nodules. Nick Vernetti, MD, FACE Palm Medical Group Las Vegas, Nevada
 Evaluation and Management of Thyroid Nodules Nick Vernetti, MD, FACE Palm Medical Group Las Vegas, Nevada Disclosure Consulting Amgen Speaking Amgen Objectives Understand the significance of incidental
Evaluation and Management of Thyroid Nodules Nick Vernetti, MD, FACE Palm Medical Group Las Vegas, Nevada Disclosure Consulting Amgen Speaking Amgen Objectives Understand the significance of incidental
PEDIATRIC Ariel Katz MD
 PEDIATRIC Ariel Katz MD Dept. Otolaryngology Head &Neck Surgery Wolfson Medical Center Holon, Israel OBJECTIVES Overview/Background Epidemiology/Etiology Intro to Guidelines Workup Treatment Follow-Up
PEDIATRIC Ariel Katz MD Dept. Otolaryngology Head &Neck Surgery Wolfson Medical Center Holon, Israel OBJECTIVES Overview/Background Epidemiology/Etiology Intro to Guidelines Workup Treatment Follow-Up
5/3/2017. Ahn et al N Engl J Med 2014; 371
 Alan Failor, M.D. Clinical Professor of Medicine Division of Metabolism, Endocrinology and Nutrition University of Washington April 20, 2017 No disclosures to report 1. Appropriately evaluate s in adult
Alan Failor, M.D. Clinical Professor of Medicine Division of Metabolism, Endocrinology and Nutrition University of Washington April 20, 2017 No disclosures to report 1. Appropriately evaluate s in adult
THYROID CANCER IN CHILDREN. Humberto Lugo-Vicente MD FACS FAAP Professor Pediatric Surgery UPR School of Medicine
 THYROID CANCER IN CHILDREN Humberto Lugo-Vicente MD FACS FAAP Professor Pediatric Surgery UPR School of Medicine Thyroid nodules Rare Female predominance 4-fold as likely to be malignant Hx Radiation exposure?
THYROID CANCER IN CHILDREN Humberto Lugo-Vicente MD FACS FAAP Professor Pediatric Surgery UPR School of Medicine Thyroid nodules Rare Female predominance 4-fold as likely to be malignant Hx Radiation exposure?
Update on Thyroid FNA The Bethesda System. Shikha Bose M.D. Associate Professor Cedars Sinai Medical Center
 Update on Thyroid FNA The Bethesda System Shikha Bose M.D. Associate Professor Cedars Sinai Medical Center Thyroid Nodules Frequent occurrence Palpable: 4-7% of adults Ultrasound: 10-31% Majority benign
Update on Thyroid FNA The Bethesda System Shikha Bose M.D. Associate Professor Cedars Sinai Medical Center Thyroid Nodules Frequent occurrence Palpable: 4-7% of adults Ultrasound: 10-31% Majority benign
Persistent & Recurrent Differentiated Thyroid Cancer
 Persistent & Recurrent Differentiated Thyroid Cancer Electron Kebebew University of California, San Francisco Department of Surgery Objectives Risk factors for persistent & recurrent disease Causes of
Persistent & Recurrent Differentiated Thyroid Cancer Electron Kebebew University of California, San Francisco Department of Surgery Objectives Risk factors for persistent & recurrent disease Causes of
THYROID CYTOLOGY THYROID CYTOLOGY FINE-NEEDLE-ASPIRATION ANCILLARY TESTS IN THYROID FNA
 ANCILLARY TESTS IN THYROID FNA Prof. Fernando Schmitt Department of Pathology and Oncology, Medical Faculty of Porto University Head of Molecular Pathology Unit, IPATIMUP General-Secretary of the International
ANCILLARY TESTS IN THYROID FNA Prof. Fernando Schmitt Department of Pathology and Oncology, Medical Faculty of Porto University Head of Molecular Pathology Unit, IPATIMUP General-Secretary of the International
Differentiated Thyroid Carcinoma
 Differentiated Thyroid Carcinoma The GOOD cancer? Jennifer Sipos, MD Associate Professor of Medicine Director, Benign Thyroid Program Division of Endocrinology, Diabetes and Metabolism The Ohio State University
Differentiated Thyroid Carcinoma The GOOD cancer? Jennifer Sipos, MD Associate Professor of Medicine Director, Benign Thyroid Program Division of Endocrinology, Diabetes and Metabolism The Ohio State University
Disclosures Nodal Management in Differentiated Thyroid Carcinoma
 Disclosures Nodal Management in Differentiated Thyroid Carcinoma Nothing to disclose Jonathan George, MD, MPH Assistant Professor UCSF Head and Neck Oncologic & Endocrine Surgery Objectives Overview Describe
Disclosures Nodal Management in Differentiated Thyroid Carcinoma Nothing to disclose Jonathan George, MD, MPH Assistant Professor UCSF Head and Neck Oncologic & Endocrine Surgery Objectives Overview Describe
Building On The Best A Review and Update on Bethesda Thyroid 2017
 Building On The Best A Review and Update on Bethesda Thyroid 2017 Syed Z. Ali, MD, FRCPath, FIAC Professor of Pathology and Radiology The Johns Hopkins Hospital, Baltimore, Maryland USA TBSRTC Diagnostic
Building On The Best A Review and Update on Bethesda Thyroid 2017 Syed Z. Ali, MD, FRCPath, FIAC Professor of Pathology and Radiology The Johns Hopkins Hospital, Baltimore, Maryland USA TBSRTC Diagnostic
TBSRTC 1- Probabilistic approach and Relationship to Clinical Algorithms
 The Benefits of a Uniform Reporting System for Thyroid Cytopathology BETHESDA REPORTING SYSTEM Prof. Fernando Schmitt Department of Pathology and Oncology, Medical Faculty of Porto University Head of Molecular
The Benefits of a Uniform Reporting System for Thyroid Cytopathology BETHESDA REPORTING SYSTEM Prof. Fernando Schmitt Department of Pathology and Oncology, Medical Faculty of Porto University Head of Molecular
NCI Thyroid FNA State of the Science Conference. The Bethesda System For Reporting Thyroid Cytopathology
 The Bethesda System For Reporting Thyroid Cytopathology Towards a Uniform Terminology With Management Guidelines NCI Thyroid FNA State of the Science Conference Bethesda, MD October 22-23, 2007 154 registrants
The Bethesda System For Reporting Thyroid Cytopathology Towards a Uniform Terminology With Management Guidelines NCI Thyroid FNA State of the Science Conference Bethesda, MD October 22-23, 2007 154 registrants
Thyroid Nodules. Family Medicine Refresher Course Geeta Lal MD, FACS April 2, No financial disclosures
 Thyroid Nodules Family Medicine Refresher Course Geeta Lal MD, FACS April 2, 2014 No financial disclosures Objectives Review epidemiology Work up of Thyroid nodules Indications for FNAB Evolving role of
Thyroid Nodules Family Medicine Refresher Course Geeta Lal MD, FACS April 2, 2014 No financial disclosures Objectives Review epidemiology Work up of Thyroid nodules Indications for FNAB Evolving role of
The Bethesda System for Reporting Thyroid Cytopathology, Laila Khazai 11/4/17
 The Bethesda System for Reporting Thyroid Cytopathology, 2017 Laila Khazai 11/4/17 In Summary No major changes for cytologists. The clinical team is faced with different risk of malignancies (ROM) associated
The Bethesda System for Reporting Thyroid Cytopathology, 2017 Laila Khazai 11/4/17 In Summary No major changes for cytologists. The clinical team is faced with different risk of malignancies (ROM) associated
5/18/2013. Most thyroid nodules are benign. Thyroid nodules: new techniques in evaluation
 Most thyroid nodules are benign Thyroid nodules: new techniques in evaluation Incidence Etiology Risk factors Diagnosis Gene classification system Treatment Postgraduate Course in General Surgery Jessica
Most thyroid nodules are benign Thyroid nodules: new techniques in evaluation Incidence Etiology Risk factors Diagnosis Gene classification system Treatment Postgraduate Course in General Surgery Jessica
Thyroid nodules 3/22/2011. Most thyroid nodules are benign. Thyroid nodules: differential diagnosis
 Most thyroid nodules are benign Thyroid nodules Postgraduate Course in General Surgery thyroid nodules occur in 77% of the world s population palpable thyroid nodules occur in about 5% of women and 1%
Most thyroid nodules are benign Thyroid nodules Postgraduate Course in General Surgery thyroid nodules occur in 77% of the world s population palpable thyroid nodules occur in about 5% of women and 1%
Management guideline for patients with differentiated thyroid cancer. Teeraporn Ratanaanekchai ENT, KKU 17 October 2007
 Management guideline for patients with differentiated thyroid Teeraporn Ratanaanekchai ENT, KKU 17 October 2007 Incidence (Srinagarind Hospital, 2005, both sex) Site (all) cases % 1. Liver 1178 27 2. Lung
Management guideline for patients with differentiated thyroid Teeraporn Ratanaanekchai ENT, KKU 17 October 2007 Incidence (Srinagarind Hospital, 2005, both sex) Site (all) cases % 1. Liver 1178 27 2. Lung
How good are we at finding nodules? Thyroid Nodules Thyroid Cancer Epidemiology Initial management Long-term follow up Disease-free status
 New Perspectives in Thyroid Cancer Jennifer Sipos, MD Assistant Professor of Medicine Division of Endocrinology The Ohio State University Outline Thyroid Nodules Thyroid Cancer Epidemiology Initial management
New Perspectives in Thyroid Cancer Jennifer Sipos, MD Assistant Professor of Medicine Division of Endocrinology The Ohio State University Outline Thyroid Nodules Thyroid Cancer Epidemiology Initial management
Preoperative Evaluation
 Preoperative Evaluation Lateral compartment lymph nodes are easier to detect and are amenable to FNA Central compartment lymph nodes are much more difficult to detect and FNA (Tg washout testing is compromised)
Preoperative Evaluation Lateral compartment lymph nodes are easier to detect and are amenable to FNA Central compartment lymph nodes are much more difficult to detect and FNA (Tg washout testing is compromised)
Objectives. 1)To recall thyroid nodule ultrasound characteristics that increase the risk of malignancy
To recall thyroid nodule ultrasound characteristics that increase the risk of malignancy") Evaluation and Management of Thyroid Nodules in Primary Care Chris Sadler, MA, PA C, CDE, DFAAPA Medical Science Outcomes Liaison Intarcia Diabetes and Endocrine Associates La Jolla, CA Past President
Evaluation and Management of Thyroid Nodules in Primary Care Chris Sadler, MA, PA C, CDE, DFAAPA Medical Science Outcomes Liaison Intarcia Diabetes and Endocrine Associates La Jolla, CA Past President
Thyroid nodules. Most thyroid nodules are benign
 Thyroid nodules Postgraduate Course in General Surgery Jessica E. Gosnell MD Assistant Professor March 22, 2011 Most thyroid nodules are benign thyroid nodules occur in 77% of the world s population palpable
Thyroid nodules Postgraduate Course in General Surgery Jessica E. Gosnell MD Assistant Professor March 22, 2011 Most thyroid nodules are benign thyroid nodules occur in 77% of the world s population palpable
The International Federation of Head and Neck Oncologic Societies. Current Concepts in Head and Neck Surgery and Oncology
 The International Federation of Head and Neck Oncologic Societies Current Concepts in Head and Neck Surgery and Oncology www.ifhnos.net The International Federation of Head and Neck Oncologic Societies
The International Federation of Head and Neck Oncologic Societies Current Concepts in Head and Neck Surgery and Oncology www.ifhnos.net The International Federation of Head and Neck Oncologic Societies
Thyroid INTRODUCTION ANATOMY SUMMARY OF CHANGES
 AJC 7/14/06 1:19 PM Page 67 Thyroid C73.9 Thyroid gland SUMMARY OF CHANGES Tumor staging (T) has been revised and the categories redefined. T4 is now divided into T4a and T4b. Nodal staging (N) has been
AJC 7/14/06 1:19 PM Page 67 Thyroid C73.9 Thyroid gland SUMMARY OF CHANGES Tumor staging (T) has been revised and the categories redefined. T4 is now divided into T4a and T4b. Nodal staging (N) has been
Cytology for the Endocrinologist. Nicole Massoll M.D
 Cytology for the Endocrinologist Nicole Massoll M.D Objectives Discuss slide preperation Definitions of adequacy ROSE (Rapid On-Site Evaluation) Thyroid Cytology Adequacy Nicole Massoll M.D. University
Cytology for the Endocrinologist Nicole Massoll M.D Objectives Discuss slide preperation Definitions of adequacy ROSE (Rapid On-Site Evaluation) Thyroid Cytology Adequacy Nicole Massoll M.D. University
MTP: Thyroid Nodules
 Canadian Endocrine Update MTP: Thyroid Nodules Deric Morrison MD, FRCP, ECNU Assistant Professor, Division of Endocrinology and Metabolism, Western University April 2014 Faculty/Presenter Disclosure Faculty:
Canadian Endocrine Update MTP: Thyroid Nodules Deric Morrison MD, FRCP, ECNU Assistant Professor, Division of Endocrinology and Metabolism, Western University April 2014 Faculty/Presenter Disclosure Faculty:
Thyroid Nodule Management
 Thyroid Nodule Management Shane O. LeBeau, MD Clinical Associate Professor of Medicine Clinical Lead, Endocrine Thyroid Unit Division of Endocrinology, Diabetes and Metabolism University of Pittsburgh
Thyroid Nodule Management Shane O. LeBeau, MD Clinical Associate Professor of Medicine Clinical Lead, Endocrine Thyroid Unit Division of Endocrinology, Diabetes and Metabolism University of Pittsburgh
Background to the Thyroid Nodule
 William C. Faquin, MD, PhD Professor of Pathology Harvard Medical School Director of Head and Neck Pathology Massachusetts Eye and Ear Massachusetts General Hospital THYROID FNA: PART I Background to the
William C. Faquin, MD, PhD Professor of Pathology Harvard Medical School Director of Head and Neck Pathology Massachusetts Eye and Ear Massachusetts General Hospital THYROID FNA: PART I Background to the
Thyroid Nodules. No conflicts. Overview 5/16/2017. UCSF Internal Medicine Updates May 22, 2017 Elizabeth Murphy, MD, DPhil
 Thyroid Nodules UCSF Internal Medicine Updates May 22, 2017 Elizabeth Murphy, MD, DPhil No conflicts Overview Thyroid nodule and cancer review Ultrasound FNA cytology Nodule follow up Putting it all together
Thyroid Nodules UCSF Internal Medicine Updates May 22, 2017 Elizabeth Murphy, MD, DPhil No conflicts Overview Thyroid nodule and cancer review Ultrasound FNA cytology Nodule follow up Putting it all together
Objectives. How to Investigate Thyroid Nodules like A Pro
 How to Investigate Thyroid Nodules like A Pro Chris Sadler, MA, PA C, CDE, DFAAPA Medical Science Outcomes Liaison Intarcia Diabetes and Endocrine Associates La Jolla, CA Past President ASEPA Disclosures
How to Investigate Thyroid Nodules like A Pro Chris Sadler, MA, PA C, CDE, DFAAPA Medical Science Outcomes Liaison Intarcia Diabetes and Endocrine Associates La Jolla, CA Past President ASEPA Disclosures
FNA of Thyroid. Toward a Uniform Terminology With Management Guidelines. NCI NCI Thyroid FNA State of the Science Conference
 FNA of Thyroid NCI NCI Thyroid FNA State of the Science Conference Toward a Uniform Terminology With Management Guidelines Thyroid Thyroid FNA Cytomorphology NCI Thyroid FNA State of the Science Conference
FNA of Thyroid NCI NCI Thyroid FNA State of the Science Conference Toward a Uniform Terminology With Management Guidelines Thyroid Thyroid FNA Cytomorphology NCI Thyroid FNA State of the Science Conference
Tania Gallant MD, FRCPC Internal Medicine Update April
 Tania Gallant MD, FRCPC Internal Medicine Update April 28 2017 Disclosures Honoraria/Ad board: Sanofi-Aventis, Janssen, Merck Frosst, Eli-Lilly, Astra Zeneca, Boehringer-Ingelheim Objectives By the end
Tania Gallant MD, FRCPC Internal Medicine Update April 28 2017 Disclosures Honoraria/Ad board: Sanofi-Aventis, Janssen, Merck Frosst, Eli-Lilly, Astra Zeneca, Boehringer-Ingelheim Objectives By the end
ASCP Competency Assessment
 ASCP Competency Assessment Thyroid Cytopathology Ricardo R. Lastra, MD Michelle R. Pramick, MD Zubair W. Baloch, MD, PhD Department of Pathology & Laboratory Medicine University of Pennsylvania, Perelman
ASCP Competency Assessment Thyroid Cytopathology Ricardo R. Lastra, MD Michelle R. Pramick, MD Zubair W. Baloch, MD, PhD Department of Pathology & Laboratory Medicine University of Pennsylvania, Perelman
3/29/2012. Thyroid cancer- what s new. Thyroid Cancer. Thyroid cancer is now the most rapidly increasing cancer in women
 Thyroid cancer- what s new Thyroid Cancer Changing epidemiology Molecular markers Lymph node dissection Technical advances rhtsh Genetic testing and prophylactic surgery Vandetanib What s new? Jessica
Thyroid cancer- what s new Thyroid Cancer Changing epidemiology Molecular markers Lymph node dissection Technical advances rhtsh Genetic testing and prophylactic surgery Vandetanib What s new? Jessica
Index. radiologic.theclinics.com. Note: Page numbers of article titles are in boldface type.
 Index Note: Page numbers of article titles are in boldface type. A ACC. See Adrenal cortical carcinoma. Acromegaly and the pituitary gland, 551 Acute suppurative thyroiditis, 405, 406 Addison, Thomas and
Index Note: Page numbers of article titles are in boldface type. A ACC. See Adrenal cortical carcinoma. Acromegaly and the pituitary gland, 551 Acute suppurative thyroiditis, 405, 406 Addison, Thomas and
Women s Health in General Practice Symposium 2015 Thyroid & Parathyroid Cases
 Women s Health in General Practice Symposium 2015 Thyroid & Parathyroid Cases Bill Fleming Epworth Freemasons Hospital 1 Common Endocrine Presentations anatomical problems thyroid nodule / goitre embryological
Women s Health in General Practice Symposium 2015 Thyroid & Parathyroid Cases Bill Fleming Epworth Freemasons Hospital 1 Common Endocrine Presentations anatomical problems thyroid nodule / goitre embryological
Thyroid Surgery: Lobectomy, total thyroidectomy, LN biopsies or only watchful waiting?
 Thyroid Surgery: Lobectomy, total thyroidectomy, LN biopsies or only watchful waiting? Jacob Moalem, MD, FACS Associate Professor Endocrine Surgery and Endocrinology URMC Agenda 1. When is lobectomy alone
Thyroid Surgery: Lobectomy, total thyroidectomy, LN biopsies or only watchful waiting? Jacob Moalem, MD, FACS Associate Professor Endocrine Surgery and Endocrinology URMC Agenda 1. When is lobectomy alone
The Frozen Section: Diagnostic Challenges and Pitfalls
 The Frozen Section: Diagnostic Challenges and Pitfalls William C. Faquin, M.D., Ph.D. Director, Head and Neck Pathology Massachusetts General Hospital & Massachusetts Eye and Ear Infirmary Harvard Medical
The Frozen Section: Diagnostic Challenges and Pitfalls William C. Faquin, M.D., Ph.D. Director, Head and Neck Pathology Massachusetts General Hospital & Massachusetts Eye and Ear Infirmary Harvard Medical
Shifting Paradigms and Debates in the Management of Well-differentiated Thyroid Cancer
 DEBATE WJOES Shifting Paradigms and Debates in the Management of Well-differentiated Thyroid Cancer Shifting Paradigms and Debates in the Management of Well-differentiated Thyroid Cancer Ashok R Shaha
DEBATE WJOES Shifting Paradigms and Debates in the Management of Well-differentiated Thyroid Cancer Shifting Paradigms and Debates in the Management of Well-differentiated Thyroid Cancer Ashok R Shaha
- RET/PTC rearrangement: 20% papillary thyroid cancer - RET: medullary thyroid cancer
 Thyroid Cancer UpToDate: Introduction: Risk Factors: Biology: Symptoms: Diagnosis: 1. Lenvina is the first line therapy with powerful durable response and superior PFS in pts with RAI-refractory disease.
Thyroid Cancer UpToDate: Introduction: Risk Factors: Biology: Symptoms: Diagnosis: 1. Lenvina is the first line therapy with powerful durable response and superior PFS in pts with RAI-refractory disease.
Introduction: Ultrasound guided Fine Needle Aspiration: When and how
 International Course of Thyroid Ultrasonography and minimally invasive procedure 7-8 October 2016 University of Pisa, Italy Introduction: Ultrasound guided Fine Needle Aspiration: When and how Teresa Rago
International Course of Thyroid Ultrasonography and minimally invasive procedure 7-8 October 2016 University of Pisa, Italy Introduction: Ultrasound guided Fine Needle Aspiration: When and how Teresa Rago
A descriptive study on solitary nodular goitre
 Original Research Article A descriptive study on solitary nodular goitre T. Chitra 1*, Dorai D. 1, Aarthy G. 2 1 Associate Professor, 2 Post Graduate Department of General Surgery, Govt. Stanley Medical
Original Research Article A descriptive study on solitary nodular goitre T. Chitra 1*, Dorai D. 1, Aarthy G. 2 1 Associate Professor, 2 Post Graduate Department of General Surgery, Govt. Stanley Medical
Inter-observer reproducibility using The Besthesda System for Reporting Thyroid Cytopathology (TBSRTC)
") SHORT COMMUNICATION Inter-observer reproducibility in thyroid cytology reporting Inter-observer reproducibility using The Besthesda System for Reporting Thyroid Cytopathology (TBSRTC) Doshi Neena 1*, Jhabuawala
SHORT COMMUNICATION Inter-observer reproducibility in thyroid cytology reporting Inter-observer reproducibility using The Besthesda System for Reporting Thyroid Cytopathology (TBSRTC) Doshi Neena 1*, Jhabuawala
Work Up & Evaluation of Thyroid Nodules In 2013: State of The Art
 Work Up & Evaluation of Thyroid Nodules In 2013: State of The Art BC Surgical Oncology Network, Fall Update Todd McMullen MD PhD FRCSC FACS Endocrine Surgeon Divisions of General Surgery and Oncology Director,
Work Up & Evaluation of Thyroid Nodules In 2013: State of The Art BC Surgical Oncology Network, Fall Update Todd McMullen MD PhD FRCSC FACS Endocrine Surgeon Divisions of General Surgery and Oncology Director,
Ultrasound-Guided Fine-Needle Aspiration of Thyroid Nodules: New events
 Ultrasound-Guided Fine-Needle Aspiration of Thyroid Nodules: New events Sandrine Rorive, M.D., PhD. Erasme Hospital - Université Libre de Bruxelles (ULB) INTRODUCTION The assessment of thyroid nodules
Ultrasound-Guided Fine-Needle Aspiration of Thyroid Nodules: New events Sandrine Rorive, M.D., PhD. Erasme Hospital - Université Libre de Bruxelles (ULB) INTRODUCTION The assessment of thyroid nodules
Management of Thyroid Nodules. February 2 nd, 2018 Sarah Hopkins
 Management of Thyroid Nodules February 2 nd, 2018 Sarah Hopkins No disclosures Goals: Review Initial Evaluation of Thyroid Nodules Review Indications for Biopsy Approach to Multinodular Goiter Review Management
Management of Thyroid Nodules February 2 nd, 2018 Sarah Hopkins No disclosures Goals: Review Initial Evaluation of Thyroid Nodules Review Indications for Biopsy Approach to Multinodular Goiter Review Management
Imaging in Pediatric Thyroid disorders: US and Radionuclide imaging. Deepa R Biyyam, MD Attending Pediatric Radiologist
 Imaging in Pediatric Thyroid disorders: US and Radionuclide imaging Deepa R Biyyam, MD Attending Pediatric Radiologist Imaging in Pediatric Thyroid disorders: Imaging modalities Outline ACR-SNM-SPR guidelines
Imaging in Pediatric Thyroid disorders: US and Radionuclide imaging Deepa R Biyyam, MD Attending Pediatric Radiologist Imaging in Pediatric Thyroid disorders: Imaging modalities Outline ACR-SNM-SPR guidelines
Oh, I get it, the TSH goes up and down
 Evaluation and Management of the Thyroid Nodule Oh, I get it, the TSH goes up and down UCSF Head and Neck Conference October 24, 2008 Peter A. Singer, M.D. Professor and Chief Clinical Endocrinology University
Evaluation and Management of the Thyroid Nodule Oh, I get it, the TSH goes up and down UCSF Head and Neck Conference October 24, 2008 Peter A. Singer, M.D. Professor and Chief Clinical Endocrinology University
Section 2 Original Policy Date 2013 Last Review Status/Date September 1, 2014
 Policy Number 2.04.82 Molecular Markers in Fine Needle Aspirates of the Thyroid Medical Policy Section 2 Original Policy Date 2013 Last Review Status/Date September 1, 2014 Disclaimer Our medical policies
Policy Number 2.04.82 Molecular Markers in Fine Needle Aspirates of the Thyroid Medical Policy Section 2 Original Policy Date 2013 Last Review Status/Date September 1, 2014 Disclaimer Our medical policies
Repeat Thyroid Nodule Fine-Needle Aspiration in Patients With Initial Benign Cytologic Results
 Anatomic Pathology / REPEAT THYROID FINE-NEEDLE ASPIRATION Repeat Thyroid Nodule Fine-Needle Aspiration in Patients With Initial Benign Cytologic Results Melina B. Flanagan, MD, MSPH, 1 N. Paul Ohori,
Anatomic Pathology / REPEAT THYROID FINE-NEEDLE ASPIRATION Repeat Thyroid Nodule Fine-Needle Aspiration in Patients With Initial Benign Cytologic Results Melina B. Flanagan, MD, MSPH, 1 N. Paul Ohori,
Journal of Diagnostic Pathology 2011 (6); 1: Leading Article
; 1: Leading Article") Leading Article Beyond the horizon of current thyroid cytology reporting in Sri Lanka... Lokuhetty MDS Thyroid enlargement is a commonly encountered clinical problem among Sri Lankan patients, be it diffuse
Leading Article Beyond the horizon of current thyroid cytology reporting in Sri Lanka... Lokuhetty MDS Thyroid enlargement is a commonly encountered clinical problem among Sri Lankan patients, be it diffuse
CAP Cancer Protocol and ecc Summary of Changes for August 2014 Thyroid Agile Release
 CAP Cancer Protocol and ecc Summary of Changes for August 2014 Thyroid Agile Release 2 REVISION HISTORY Date Author / Editor Comments 5/19/2014 Jaleh Mirza Created the document 8/12/2014 Samantha Spencer/Jaleh
CAP Cancer Protocol and ecc Summary of Changes for August 2014 Thyroid Agile Release 2 REVISION HISTORY Date Author / Editor Comments 5/19/2014 Jaleh Mirza Created the document 8/12/2014 Samantha Spencer/Jaleh
Papillary Thyroid Microcarcinoma Presenting as Horner s Syndrome: A Novel Clinical Presentation
 Case Report American Journal of Cancer Case Reports http://ivyunion.org/index.php/ajccr/ Page 1 of 6 Papillary Thyroid Microcarcinoma Presenting as Horner s Syndrome: A Novel Clinical Presentation Ammara
Case Report American Journal of Cancer Case Reports http://ivyunion.org/index.php/ajccr/ Page 1 of 6 Papillary Thyroid Microcarcinoma Presenting as Horner s Syndrome: A Novel Clinical Presentation Ammara
Thyroid Nodules: Understanding FNA Cytology (The Bethesda System for Reporting of Thyroid Cytopathology) Shamlal Mangray, MB, BS
 Shamlal Mangray, MB, BS") Thyroid Nodules: Understanding FNA Cytology (The Bethesda System for Reporting of Thyroid Cytopathology) Shamlal Mangray, MB, BS Attending Pathologist Rhode Island Hospital, Providence, RI DISCLOSURE:
Thyroid Nodules: Understanding FNA Cytology (The Bethesda System for Reporting of Thyroid Cytopathology) Shamlal Mangray, MB, BS Attending Pathologist Rhode Island Hospital, Providence, RI DISCLOSURE:
Management of Neck Metastasis from Unknown Primary
 Management of Neck Metastasis from Unknown Primary.. Definition Histologic evidence of malignancy in the cervical lymph node (s) with no apparent primary site of original tumour Diagnosis after a thorough
Management of Neck Metastasis from Unknown Primary.. Definition Histologic evidence of malignancy in the cervical lymph node (s) with no apparent primary site of original tumour Diagnosis after a thorough
Thyroid Pathology: It starts and ends with the gross. Causes of Thyrophobia. Agenda. Diagnostic ambiguity. Treatment/prognosis disconnect
 Thyroid Pathology: It starts and ends with the gross Jennifer L. Hunt, MD, MEd Aubrey J. Hough Jr, MD, Endowed Professor of Pathology Chair of Pathology and Laboratory Medicine University of Arkansas for
Thyroid Pathology: It starts and ends with the gross Jennifer L. Hunt, MD, MEd Aubrey J. Hough Jr, MD, Endowed Professor of Pathology Chair of Pathology and Laboratory Medicine University of Arkansas for
Volume 2 Issue ISSN
 Volume 2 Issue 3 2012 ISSN 2250-0359 Correlation of fine needle aspiration and final histopathology in thyroid disease: a series of 702 patients managed in an endocrine surgical unit *Chandrasekaran Maharajan
Volume 2 Issue 3 2012 ISSN 2250-0359 Correlation of fine needle aspiration and final histopathology in thyroid disease: a series of 702 patients managed in an endocrine surgical unit *Chandrasekaran Maharajan
Pediatric Thyroid Cancer Lung Metastases. Liora Lazar MD
 Pediatric Thyroid Cancer Lung Metastases Liora Lazar MD Differentiated thyroid cancer (DTC) The 3rd most common solid tumor in childhood and adolescence Accounting for 1.5%-3% of all childhood cancers
Pediatric Thyroid Cancer Lung Metastases Liora Lazar MD Differentiated thyroid cancer (DTC) The 3rd most common solid tumor in childhood and adolescence Accounting for 1.5%-3% of all childhood cancers
Thyroid and Parathyroid Surgery
 Med 5 Surgery Refresher Course 2013 2014 Thyroid and Parathyroid Surgery Dr Shirley Liu Resident Specialist Honorary Clinical Assistant Professor Team 2 Surgery Prince of Wales Hospital Case scenario:
Med 5 Surgery Refresher Course 2013 2014 Thyroid and Parathyroid Surgery Dr Shirley Liu Resident Specialist Honorary Clinical Assistant Professor Team 2 Surgery Prince of Wales Hospital Case scenario:
A Study of Thyroid Swellings and Correlation between FNAC and Histopathology Results
 International Journal of Current Microbiology and Applied Sciences ISSN: 2319-7706 Volume 6 Number 4 (2017) pp. 265-269 Journal homepage: http://www.ijcmas.com Original Research Article https://doi.org/10.20546/ijcmas.2017.604.030
International Journal of Current Microbiology and Applied Sciences ISSN: 2319-7706 Volume 6 Number 4 (2017) pp. 265-269 Journal homepage: http://www.ijcmas.com Original Research Article https://doi.org/10.20546/ijcmas.2017.604.030
Sonographic Features of Thyroid Nodules & Guidelines for Management
 Sonographic Features of Thyroid Nodules & Guidelines for Management Mark A. Lupo, MD, FACE, ECNU Thyroid & Endocrine Center of Florida Assistant Clinical Professor of Medicine Florida State University,
Sonographic Features of Thyroid Nodules & Guidelines for Management Mark A. Lupo, MD, FACE, ECNU Thyroid & Endocrine Center of Florida Assistant Clinical Professor of Medicine Florida State University,
"Atypical": Criteria and
 "Atypical": Criteria and Controversies Esther Rossi MD PhD MIAC Division of Anatomic Pathology and Cytology Catholic University of Sacred Heart Rome, Italy CASE HISTORY In 2015, 45 y/o woman underwent
"Atypical": Criteria and Controversies Esther Rossi MD PhD MIAC Division of Anatomic Pathology and Cytology Catholic University of Sacred Heart Rome, Italy CASE HISTORY In 2015, 45 y/o woman underwent
 To the Patient and Family This booklet has been written for people who have received a diagnosis of thyroid cancer or who are being tested for this illness. If you have questions that are not answered
To the Patient and Family This booklet has been written for people who have received a diagnosis of thyroid cancer or who are being tested for this illness. If you have questions that are not answered
Chapter 14: Thyroid Cancer
 The American Academy of Otolaryngology Head and Neck Surgery Foundation (AAO-HNSF) Presents... Chapter 14: Thyroid Cancer Daiichi Pharmaceutical Corporation, marketers and distributors of FLOXIN Otic (ofloxacin
The American Academy of Otolaryngology Head and Neck Surgery Foundation (AAO-HNSF) Presents... Chapter 14: Thyroid Cancer Daiichi Pharmaceutical Corporation, marketers and distributors of FLOXIN Otic (ofloxacin
AGGRESSIVE VARIANTS OF PAPILLARY THYROID CARCINOMA DIAGNOSIS AND PROGNOSIS
 AGGRESSIVE VARIANTS OF PAPILLARY THYROID CARCINOMA DIAGNOSIS AND PROGNOSIS PAPILLARY THYROID CARCINOMA Clinical Any age Microscopic to large Female: Male= 2-4:1 Radiation history Lymph nodes Prognosis
AGGRESSIVE VARIANTS OF PAPILLARY THYROID CARCINOMA DIAGNOSIS AND PROGNOSIS PAPILLARY THYROID CARCINOMA Clinical Any age Microscopic to large Female: Male= 2-4:1 Radiation history Lymph nodes Prognosis
The International Federation of Head and Neck Oncologic Societies. Current Concepts in Head and Neck Surgery and Oncology
 The International Federation of Head and Neck Oncologic Societies Current Concepts in Head and Neck Surgery and Oncology www.ifhnos.net The International Federation of Head and Neck Oncologic Societies
The International Federation of Head and Neck Oncologic Societies Current Concepts in Head and Neck Surgery and Oncology www.ifhnos.net The International Federation of Head and Neck Oncologic Societies
Thyroid Gland. Protocol applies to all malignant tumors of the thyroid gland, except lymphomas.
 Thyroid Gland Protocol applies to all malignant tumors of the thyroid gland, except lymphomas. Procedures Cytology (No Accompanying Checklist) Partial Thyroidectomy Total Thyroidectomy With/Without Lymph
Thyroid Gland Protocol applies to all malignant tumors of the thyroid gland, except lymphomas. Procedures Cytology (No Accompanying Checklist) Partial Thyroidectomy Total Thyroidectomy With/Without Lymph
Mandana Moosavi 1 and Stuart Kreisman Background
 Case Reports in Endocrinology Volume 2016, Article ID 6471081, 4 pages http://dx.doi.org/10.1155/2016/6471081 Case Report A Case Report of Dramatically Increased Thyroglobulin after Lymph Node Biopsy in
Case Reports in Endocrinology Volume 2016, Article ID 6471081, 4 pages http://dx.doi.org/10.1155/2016/6471081 Case Report A Case Report of Dramatically Increased Thyroglobulin after Lymph Node Biopsy in
Adina Alazraki, MD, FAAP Assistant Professor Radiology and Pediatrics Emory University and Children s Healthcare of Atlanta
 Adina Alazraki, MD, FAAP Assistant Professor Radiology and Pediatrics Emory University and Children s Healthcare of Atlanta Review recently published pediatric guidelines for management of thyroid nodules
Adina Alazraki, MD, FAAP Assistant Professor Radiology and Pediatrics Emory University and Children s Healthcare of Atlanta Review recently published pediatric guidelines for management of thyroid nodules
Calcitonin. 1
 Calcitonin Medullary thyroid carcinoma (MTC) is characterized by a high concentration of serum calcitonin. Routine measurement of serum calcitonin concentration has been advocated for detection of MTC
Calcitonin Medullary thyroid carcinoma (MTC) is characterized by a high concentration of serum calcitonin. Routine measurement of serum calcitonin concentration has been advocated for detection of MTC
DOWNLOAD ENTIRE DOCUMENT FROM
 PREVIEW ONLY 1 Atlas on Bethesda system for reporting Thyroid Cytology PREVIEW ONLY 2 OVERVIEW 1. Indications and goal of thyroid FNA 2. Contraindications 3. Procurement of cell sample 4. Staining methods
PREVIEW ONLY 1 Atlas on Bethesda system for reporting Thyroid Cytology PREVIEW ONLY 2 OVERVIEW 1. Indications and goal of thyroid FNA 2. Contraindications 3. Procurement of cell sample 4. Staining methods
Cytomorphologic Thresholds for Classifying Thyroid FNAs as Suspicious and Positive for PTC
 Cytomorphologic Thresholds for Classifying Thyroid FNAs as Suspicious and Positive for PTC Tarik M. Elsheikh, MD Professor and Medical Director Anatomic Pathology Cleveland Clinic Laboratories Case Study
Cytomorphologic Thresholds for Classifying Thyroid FNAs as Suspicious and Positive for PTC Tarik M. Elsheikh, MD Professor and Medical Director Anatomic Pathology Cleveland Clinic Laboratories Case Study
B. Environmental Factors. a. The major risk factor to papillary thyroid cancer is exposure to ionizing radiation, during the first 2 decades of life.
 B. Environmental Factors. a. The major risk factor to papillary thyroid cancer is exposure to ionizing radiation, during the first 2 decades of life. b. Deficiency of dietary iodine: - Is linked with a
B. Environmental Factors. a. The major risk factor to papillary thyroid cancer is exposure to ionizing radiation, during the first 2 decades of life. b. Deficiency of dietary iodine: - Is linked with a
Thyroid Cancer: When to Treat? MEGAN R. HAYMART, MD
 Thyroid Cancer: When to Treat? MEGAN R. HAYMART, MD ASSOCIATE PROFESSOR OF MEDICINE UNIVERSITY OF MICHIGAN MICHIGAN AACE 2018 ANNUAL MEETING Thyroid Cancer: When Not to Treat? FOCUS WILL BE ON LOW-RISK
Thyroid Cancer: When to Treat? MEGAN R. HAYMART, MD ASSOCIATE PROFESSOR OF MEDICINE UNIVERSITY OF MICHIGAN MICHIGAN AACE 2018 ANNUAL MEETING Thyroid Cancer: When Not to Treat? FOCUS WILL BE ON LOW-RISK
Evaluation and Management of Thyroid Nodules. Overview of Thyroid Nodules and Their Management. Thyroid Nodule detection: U/S versus Exam
 Overview of Thyroid Nodules and Their Management Matthew D. Ringel, M.D. Professor of Medicine Divisions of Endocrinology and Oncology, The Ohio State University Co-Director, Thyroid Cancer Unit Arthur
Overview of Thyroid Nodules and Their Management Matthew D. Ringel, M.D. Professor of Medicine Divisions of Endocrinology and Oncology, The Ohio State University Co-Director, Thyroid Cancer Unit Arthur
Thyroid and Parathyroid Disease. RTC Conference Christina Edwards Bailey Faculty: Dr. Carmen Solorzano April 2, 2010
 Thyroid and Parathyroid Disease RTC Conference Christina Edwards Bailey Faculty: Dr. Carmen Solorzano April 2, 2010 Case Presentation # 1 CC: Neck Mass HPI: 51f found to have a neck mass on routine PE.
Thyroid and Parathyroid Disease RTC Conference Christina Edwards Bailey Faculty: Dr. Carmen Solorzano April 2, 2010 Case Presentation # 1 CC: Neck Mass HPI: 51f found to have a neck mass on routine PE.
AACE-AME 2016 Thyroid Nodule Update
 AACE-AME 2016 Thyroid Nodule Update 26 th Annual AACE Meeting & Clinical Congress Austin May 1-5, 2017 Hossein Gharib, MD, MACP, MACE Professor, Mayo Clinic College of Medicine Past President, American
AACE-AME 2016 Thyroid Nodule Update 26 th Annual AACE Meeting & Clinical Congress Austin May 1-5, 2017 Hossein Gharib, MD, MACP, MACE Professor, Mayo Clinic College of Medicine Past President, American
Research Article Papillary Thyroid Cancer, Macrofollicular Variant: The Follow-Up and Analysis of Prognosis of 5 Patients
 yroid Research, Article ID 818134, 4 pages http://dx.doi.org/10.1155/2014/818134 Research Article Papillary Thyroid Cancer, Macrofollicular Variant: The Follow-Up and Analysis of Prognosis of 5 Patients
yroid Research, Article ID 818134, 4 pages http://dx.doi.org/10.1155/2014/818134 Research Article Papillary Thyroid Cancer, Macrofollicular Variant: The Follow-Up and Analysis of Prognosis of 5 Patients
An Alphabet Soup of Thyroid Neoplasms
 Overall Objectives An Alphabet Soup of Thyroid Neoplasms Lester D. R. Thompson www.lester-thompson.com What is the current management of papillary carcinoma? What are the trends and what can we do differently?
Overall Objectives An Alphabet Soup of Thyroid Neoplasms Lester D. R. Thompson www.lester-thompson.com What is the current management of papillary carcinoma? What are the trends and what can we do differently?
OUTLINE. Regulation of Thyroid Hormone Production Common Tests to Evaluate the Thyroid Hyperthyroidism - Graves disease, toxic nodules, thyroiditis
 THYROID DISEASE OUTLINE Regulation of Thyroid Hormone Production Common Tests to Evaluate the Thyroid Hyperthyroidism - Graves disease, toxic nodules, thyroiditis OUTLINE Hypothyroidism - Hashimoto s thyroiditis,
THYROID DISEASE OUTLINE Regulation of Thyroid Hormone Production Common Tests to Evaluate the Thyroid Hyperthyroidism - Graves disease, toxic nodules, thyroiditis OUTLINE Hypothyroidism - Hashimoto s thyroiditis,
Pathology of the Thyroid
 Pathology of the Thyroid Thyroid Carcinoma Arising from Follicular Cells 2015-01-19 Prof. Dr. med. Katharina Glatz Pathologie Carcinomas Arising from Follicular Cells Differentiated Carcinoma Papillary
Pathology of the Thyroid Thyroid Carcinoma Arising from Follicular Cells 2015-01-19 Prof. Dr. med. Katharina Glatz Pathologie Carcinomas Arising from Follicular Cells Differentiated Carcinoma Papillary
Ultrasound for Pre-operative Evaluation of Well Differentiated Thyroid Cancer
 Ultrasound for Pre-operative Evaluation of Well Differentiated Thyroid Cancer Its Not Just About the Nodes AACE Advances in Medical and Surgical Management of Thyroid Cancer - 2017 Robert A. Levine, MD,
Ultrasound for Pre-operative Evaluation of Well Differentiated Thyroid Cancer Its Not Just About the Nodes AACE Advances in Medical and Surgical Management of Thyroid Cancer - 2017 Robert A. Levine, MD,
Avi Khafif, MD, Rami Ben-Yosef, MD, Avrum Abergel, MD, Ada Kesler, MD, Roee Landsberg, MD, Dan M. Fliss, MD
 ORIGINAL ARTICLE ELECTIVE PARATRACHEAL NECK DISSECTION FOR LATERAL METASTASES FROM PAPILLARY CARCINOMA OF THE THYROID: IS IT INDICATED? Avi Khafif, MD, Rami Ben-Yosef, MD, Avrum Abergel, MD, Ada Kesler,
ORIGINAL ARTICLE ELECTIVE PARATRACHEAL NECK DISSECTION FOR LATERAL METASTASES FROM PAPILLARY CARCINOMA OF THE THYROID: IS IT INDICATED? Avi Khafif, MD, Rami Ben-Yosef, MD, Avrum Abergel, MD, Ada Kesler,
THYROID NODULES: THE ROLE OF ULTRASOUND
 THYROID NODULES: THE ROLE OF ULTRASOUND NOVEMBER 2017 DR. DEAN DURANT DEFINITION Thyroid nodule: Focal area within the thyroid gland with echogenicity different from surrounding parenchyma. THYROID NODULES
THYROID NODULES: THE ROLE OF ULTRASOUND NOVEMBER 2017 DR. DEAN DURANT DEFINITION Thyroid nodule: Focal area within the thyroid gland with echogenicity different from surrounding parenchyma. THYROID NODULES
NIFTP Cytologic Aspects
 NIFTP Cytologic Aspects William C. Faquin, MD PhD Director, Head and Neck Pathology Massachusetts General Hospital & Massachusetts Eye and Ear Infirmary Boston, MA USA So, what is the story about FVPTC
NIFTP Cytologic Aspects William C. Faquin, MD PhD Director, Head and Neck Pathology Massachusetts General Hospital & Massachusetts Eye and Ear Infirmary Boston, MA USA So, what is the story about FVPTC
Clinical and Molecular Approach to Using Thyroid Needle Biopsy for Nodular Disease
 Clinical and Molecular Approach to Using Thyroid Needle Biopsy for Nodular Disease Robert L. Ferris, MD, PhD Department of Otolaryngology/Head and Neck Surgery and Yuri E. Nikiforov, MD, PhD Division of
Clinical and Molecular Approach to Using Thyroid Needle Biopsy for Nodular Disease Robert L. Ferris, MD, PhD Department of Otolaryngology/Head and Neck Surgery and Yuri E. Nikiforov, MD, PhD Division of
42 yr old male with h/o Graves disease and prior I 131 treatment presents with hyperthyroidism and undetectable TSH. 2 hr uptake 20%, 24 hr uptake 50%
 Pinhole images of the neck are acquired in multiple projections, 24hrs after the oral administration of approximately 200 µci of I123. Usually, 24hr uptake value if also calculated (normal 24 hr uptake
Pinhole images of the neck are acquired in multiple projections, 24hrs after the oral administration of approximately 200 µci of I123. Usually, 24hr uptake value if also calculated (normal 24 hr uptake
Thyroid Cancer (Carcinoma)
") Information for Patients Thyroid Cancer (Carcinoma) Prepared by the American Association of Clinical Endocrinologists (AACE), a not-for-profit national organization of highly qualified specialists in hormonal
Information for Patients Thyroid Cancer (Carcinoma) Prepared by the American Association of Clinical Endocrinologists (AACE), a not-for-profit national organization of highly qualified specialists in hormonal
Medullary Thyroid Carcinoma. This case was provided by Treant Hospital, Bethesda, Hoogeveen, The Netherlands
 Medullary Thyroid Carcinoma This case was provided by Treant Hospital, Bethesda, Hoogeveen, The Netherlands ADS-01504 Rev. 001 2016 Hologic, Inc. All rights reserved. Overview Medullary Thyroid Carcinoma
Medullary Thyroid Carcinoma This case was provided by Treant Hospital, Bethesda, Hoogeveen, The Netherlands ADS-01504 Rev. 001 2016 Hologic, Inc. All rights reserved. Overview Medullary Thyroid Carcinoma
Pitfalls in thyroid tumor pathology. Prof.Valdi Pešutić-Pisac MD, PhD
 Pitfalls in thyroid tumor pathology Prof.Valdi Pešutić-Pisac MD, PhD Too many or... Tumour herniation through a torn capsule simulating capsular invasion fibrous capsule with a sharp discontinuity, suggestive
Pitfalls in thyroid tumor pathology Prof.Valdi Pešutić-Pisac MD, PhD Too many or... Tumour herniation through a torn capsule simulating capsular invasion fibrous capsule with a sharp discontinuity, suggestive
CN 925/15 History. Microscopic Findings
 CN 925/15 History 78 year old female. FNA indeterminate lesion right thyroid lobe. Previous THY1C (UK) Bethesda category 1 cyst fluid. Ultrasound showed part solid/cystic changes, indeterminate in nature
CN 925/15 History 78 year old female. FNA indeterminate lesion right thyroid lobe. Previous THY1C (UK) Bethesda category 1 cyst fluid. Ultrasound showed part solid/cystic changes, indeterminate in nature
The incidence of thyroid cancer has increased exponentially over
 FEATURE THYROID Papillary thyroid cancer: the most common endocrine malignancy JAMES C. LEE FRACS STANLEY B. SIDHU FRACS, PhD Papillary thyroid cancer has an excellent prognosis and over 90% of affected
FEATURE THYROID Papillary thyroid cancer: the most common endocrine malignancy JAMES C. LEE FRACS STANLEY B. SIDHU FRACS, PhD Papillary thyroid cancer has an excellent prognosis and over 90% of affected
Management of Thyroid Nodules
 Management of Thyroid Nodules 38 y/o female with solid 1.5 cm right Thyroid nodule. TSH=0.68 Vincent J. Reid, MD., FACS Thyroid Cancer Incidence & Mortality 1974 to 2004 Overall Women Men Mortality 1 Cancer
Management of Thyroid Nodules 38 y/o female with solid 1.5 cm right Thyroid nodule. TSH=0.68 Vincent J. Reid, MD., FACS Thyroid Cancer Incidence & Mortality 1974 to 2004 Overall Women Men Mortality 1 Cancer
Correspondence should be addressed to David N. Bimston; Received 23 January 2017; Accepted 20 March 2017; Published 13 April 2017
 Hindawi International Surgical Oncology Volume 2017, Article ID 4689465, 6 pages https://doi.org/10.1155/2017/4689465 Research Article Noninvasive Encapsulated Follicular Variant of Papillary Thyroid Cancer:
Hindawi International Surgical Oncology Volume 2017, Article ID 4689465, 6 pages https://doi.org/10.1155/2017/4689465 Research Article Noninvasive Encapsulated Follicular Variant of Papillary Thyroid Cancer: