Preoperative Evaluation
|
|
|
- Donna Small
- 5 years ago
- Views:
Transcription

1
2 Preoperative Evaluation Lateral compartment lymph nodes are easier to detect and are amenable to FNA Central compartment lymph nodes are much more difficult to detect and FNA (Tg washout testing is compromised)

3 Surgical Levels of the Neck See insert in back of syllabus. Som et al, AJR 174:
4 Surgical Compartments of the Neck Compartment I Submandibular to the hyoid bone Compartments II, III, IV From the vascular bundle deep to the SCM Division by hyoid and cricoid Compartment V Posterior to the SCM Compartment VI The central compartment
5 Cervical Lymph Nodes Approximately 300 lymph nodes in the normal neck. Typically can identify 6 20 nodes by ultrasound. Nodes are more prominent following infections, mononucleosis, dental procedures and in Hashimoto s thyroiditis.
6 Differentiated Thyroid Cancer 63,000 New cases of DTC in ,890 Deaths predicted in 2014 Mortality essentially unchanged over past 30 years Unproved assumption: Early detection and treatment of cervical metastases will affect mortality Mortality versus Morbidity
7 Preoperative Imaging WDTC clinically involves lymph nodes in approximately 20% of patients. (Micrometastases in up to 90%) Pre-op US identifies suspicious Lateral neck nodes in approximately 14% of cases. Surgical management is altered in the presence of lateral neck metastases Near total Thyroidectomy Central Neck Dissection! (ATA Guidelines 2009) Lateral Neck Dissection Kouvaraki, Surgery :946; Stulak, Arch Surg :489
8 Preoperative Imaging Alternatives Ultrasound evaluation is uniquely operator dependent Sensitivity of CT, MRI and PET is less Ultrasound versus CT Characteristics of benign/suspicious nodules Contrast interference with RAI ablation Expense and time Visualization behind trachea and TE groove
9 RECOMMENDATION 6 Thyroid sonography with survey of the cervical lymph nodes should be performed in all patients with known or suspected thyroid nodules. (Strong recommendation, High-quality evidence) Haugen et al Thyroid 2016
10 And, if pre-op US NOT performed patients underwent reoperation for thyroid cancer MD Anderson <6months after initial surgery PRE-OP US would have prevented 70% or the reops!!! Kouvaraki Surgery :1183
11 Role for Preoperative Ultrasound Nodal Evaluation 560 patients underwent thyroidectomy and modified neck dissection US neg LNs 455 pts Recurrence rate US Neg 3.1% US + LNs 105 pts US Pos 24.8% Recurrences occurred significantly more often if ultrasound demonstrated abnormal nodes preoperatively 1 1 Ito, World J Surg 2005; 2 Ito, World J Surg 2004
12 Prophylactic lateral neck dissection does NOT improve recurrence free survival for patients with preoperative US negative for lymph nodes 1 Does lateral neck dissection alter the outcome for preoperative US positive for lymph nodes? 1 Ito, World J Surg 2004
13 For macroscopic lateral lymph node metastases, modified neck dissection at time of initial thyroidectomy improves survival Noguchi, Arch Surg,
14 Management Guidelines for Patients with Thyroid Nodules and Differentiated Thyroid Cancer 2015 RECOMMENDATION 32 A) Preoperative neck US for cervical (central and especially lateral neck compartments) lymph nodes is recommended for all patients undergoing thyroidectomy for malignant or suspicious for malignancy cytologic or molecular findings. (Strong recommendation, Moderate-quality evidence) RECOMMENDATION 33 A) Preoperative use of cross-sectional imaging studies (CT, MRI) with intravenous contrast is recommended as an adjunct to ultrasound for patients with clinical suspicion for advanced disease including invasive primary tumor, or clinically apparent multiple or bulky lymph node involvement. (Strong recommendation, lowquality evidence) Haugen et al Thyroid 2016

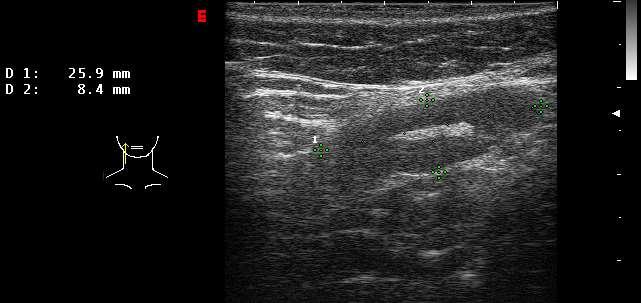
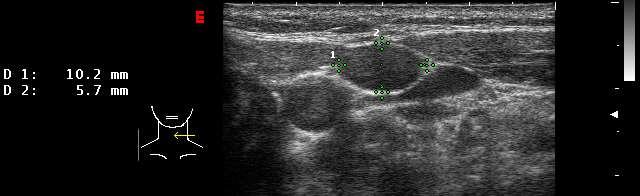
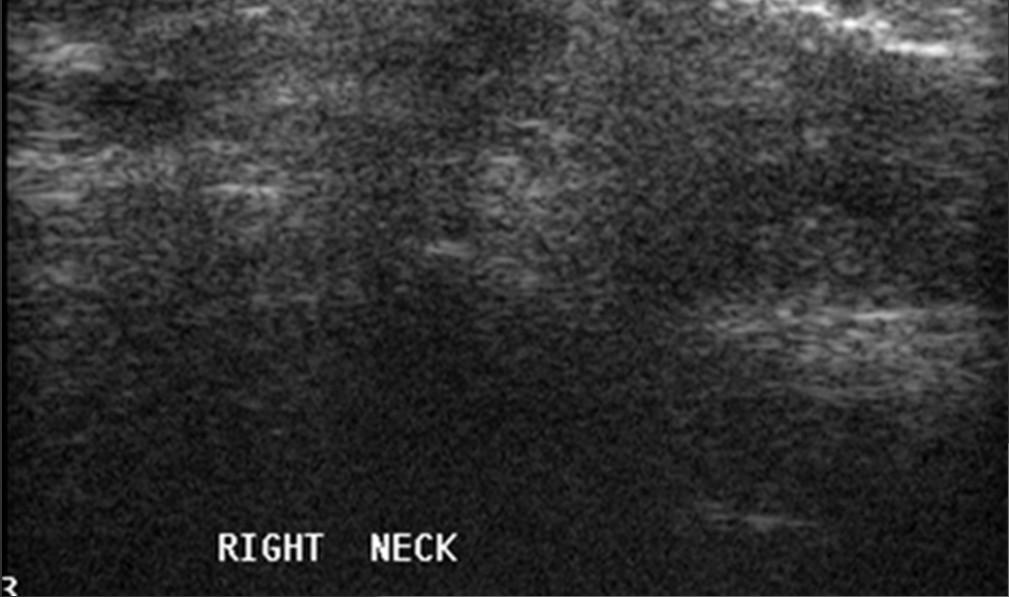
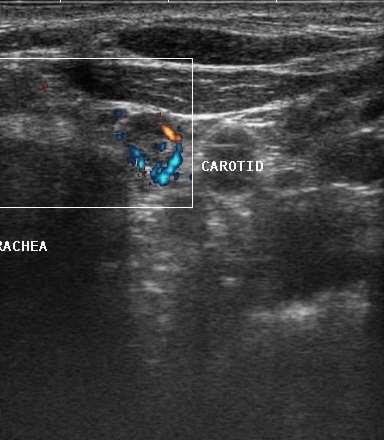
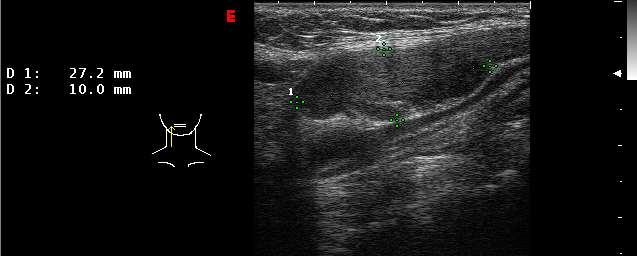
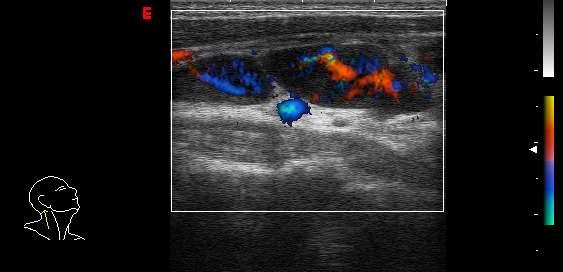
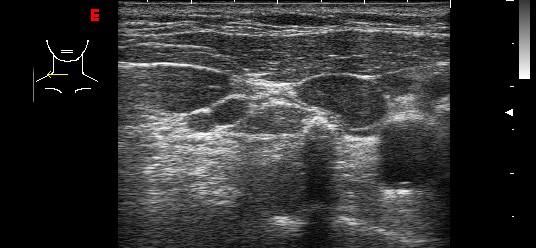
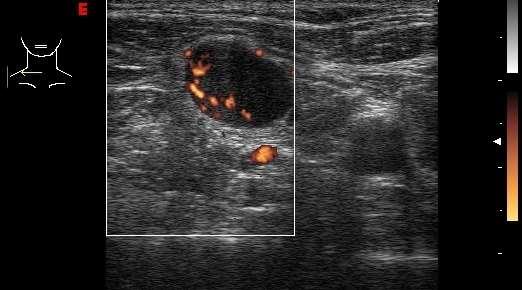
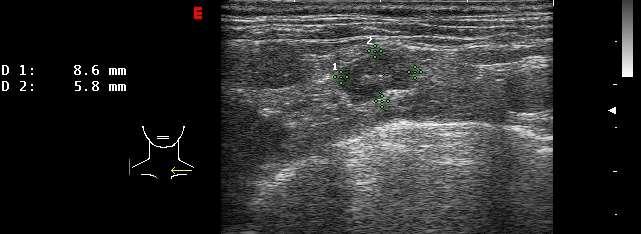
15 Pre-op evaluation of central compartment Carotid Thyroid nodule Metastatic paratrachael lymph node
 FNA cytology of nodule and lymph node negative LN C N Needle washout from lymph node Tg=24.")
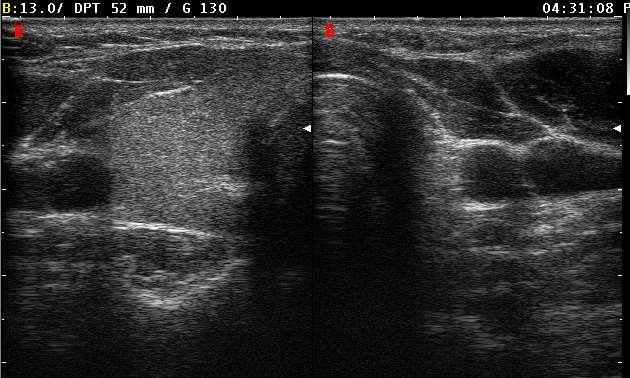
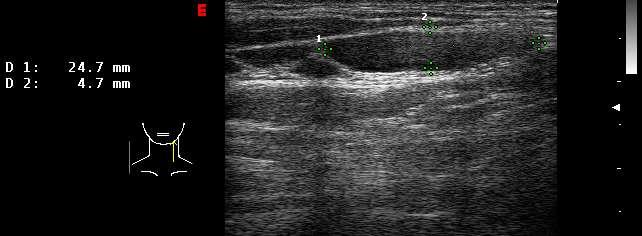
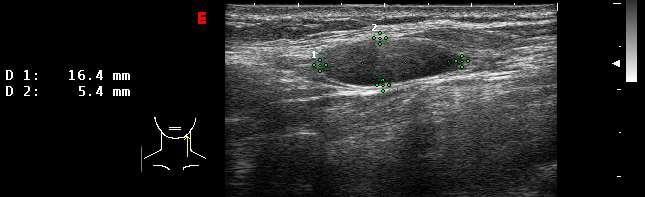
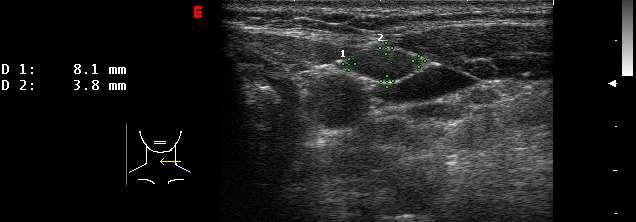
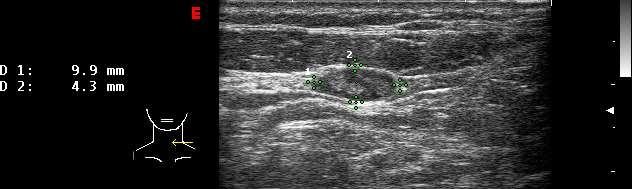
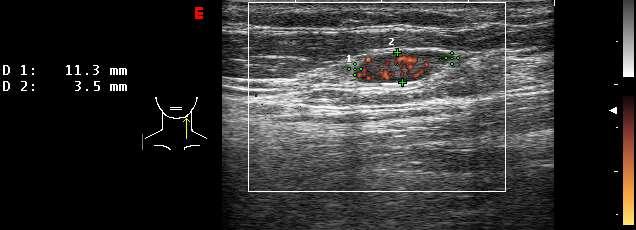
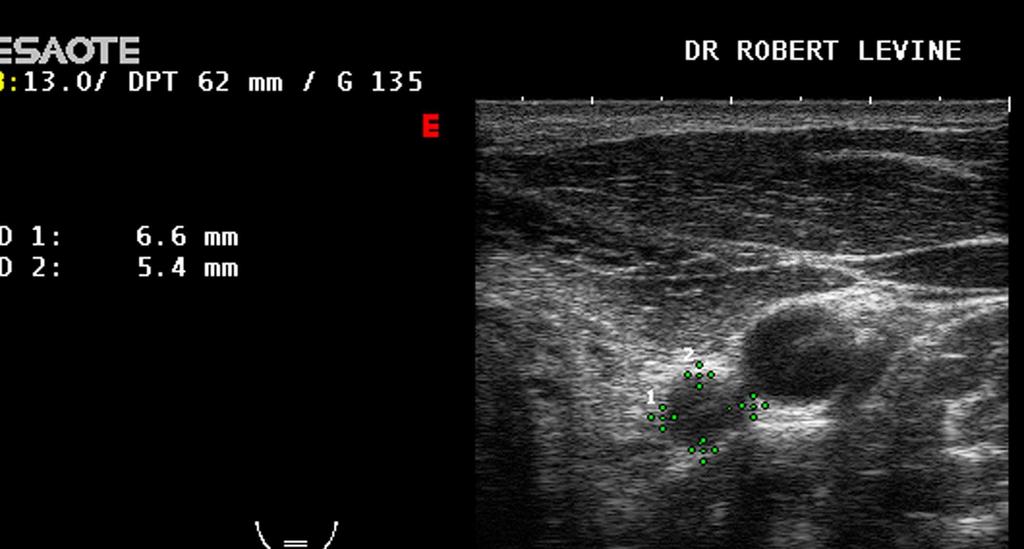
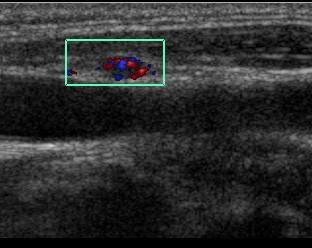
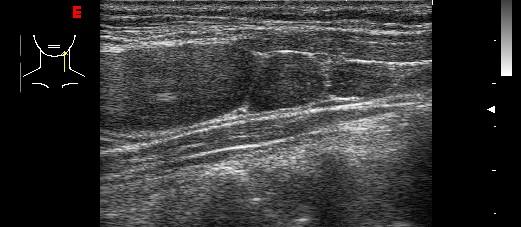
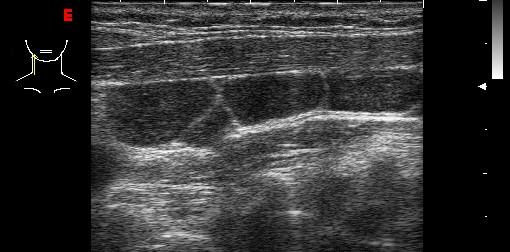
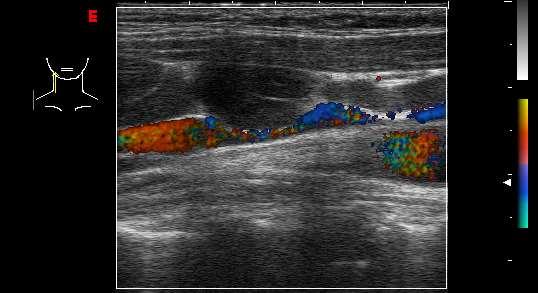
16 Preoperative Evaluation of Lateral Compartment 48yo female with cystic nodule right lobe (N) and lymph node in neck (LN) FNA cytology of nodule and lymph node negative LN C N Needle washout from lymph node Tg=24.3ng/ml
17 Post-operative Ultrasound Evaluation for the Surveillance of Patients with Low Risk (Stage I and II) Thyroid Cancer
18 Tests Used in Post-0perative Thyroid Cancer Surveillance Thyroglobulin 131 I or 123 I Whole Body Scan Ultrasound
19 Detection of LN metastases WBS vs. Neck US Sensitivity (%) WBS US Frasoldati Pacini Torlontano Frasoldati et al, Cancer 2003; Pacini et al, J Clin Endocrinol Metab 2003; Torlontano et al, J Clin Endocrinol Metab 2004
20 Diagnosis of Recurrent DTC in 51 of 494 Patients 131 I Whole Body Scan 23 (45%) Tg > 2ng/ml (off T4 therapy) 29 (57%) Tg detectable 34 (67%) Ultrasound 48 (94%) Frasoldati, et al; Cancer 2003
21 Limitations of Whole Body Scans Morbidity of thyroid withdrawal Expense Poor sensitivity (60-75%) lack of transmembrane sodium iodide symporter expression (especially with BRAF/RAS mutation) Iodine contamination Insufficient TSH stimulation Stunning Potential for causing growth? Withdrawal versus Thyrogen
22 RECOMMENDATION 65 A) Following surgery, cervical US to evaluate the thyroid bed and central and lateral cervical nodal compartments should be performed at 6 12 months and then periodically, depending on the patient s risk for recurrent disease and Tg status. (Strong recommendation, Moderatequality evidence) Haugen et al Thyroid 2016
23 Does US change surgery? Imaging of nonpalpable nodes MD Anderson Mayo Percent (%) Initial Surgery Reoperation Kouvaraki, Surgery :946; Stulak, Arch Surg :489
24 Where do we look for metastatic lymph nodes?
25 Locations of PTC nodal recurrences Ipsilateral ONLY, 12% skip metastases Central and bilateral, 13% Bilateral only, 1% 87% involve Central LNs Central ONLY, 22% Central and ipsilateral, 52% Leboulleux J Clin Endocrinol Metab 2005
26 Post-operative Ultrasound Evaluation Both the central compartment and the lateral compartments of the neck are easily surveyed with US in the post-op thyroid cancer patient FNA using US guidance allows both cytology and analysis for thyroglobulin without regard to thyroglobulin antibody
27 Post-operative Neck
28 Characteristics of Benign Lymph Nodes Flattened or oval shape (AP/T <0.5) Echogenic (hilar) line Hilar vascular flow on Doppler Size varies with compartment and is less important than morphology. Border definition also less important.
29 The Hilar Line A normal node can be split down the central hilum. Hilum contains fat and vessels A normal hilar line can be thin or thick, and can be central or eccentric/diagonal. The presence of a hilar line is reassuring.


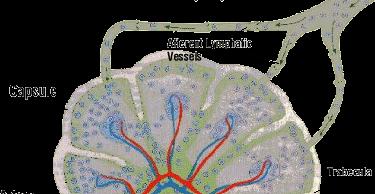

30 Normal lymph node- hilus

31 Normal Lymph Nodes


32 Normal Node with Broad Central Hilum

33 Normal Lymph Node


34 Normal Lymph Node Normal hilar blood flow
35 Node Shape Variations Central Compartment Paratracheal nodes Post surgical neck Loss of usual tissue planes Hashimoto s Matted Inflammatory

36 Paratracheal Nodes Hashimoto s Thyroiditis

37 Hashimoto s Thyroiditis
38 Node Size Variations Is there an absolute size limitation? Compartments III, IV 5 mm AP (?) NO!! Compartment II 8 10 mm AP (?) NO!!! Role for repeat evaluation over time Reactive nodes vary over time without progressive growth.

39 Large Benign Node - Compartment 2
40 Compartment 3 - Benign
41 Compartment 3 Benign 6 months later


42 Compartment 3 Benign 6 months later 10/07 4/08


43 Papillary Carcinoma Small round nodes - Benign

44 Papillary Carcinoma Small round nodes - Benign
45 Characteristics of Metastatic Lymph Nodes Absent echogenic (hilar) line Rounded appearance AP/T>.5 (transverse view) Jugular displacement Calcifications Cystic necrosis Chaotic vascularization
46 Characteristics of Malignant Nodes Sensitivity Specificity Disordered vascularity 86% 82% Microcalcifications 45% 100% Cystic Degeneration 11% 100% Absence of Hilar Line 95% 20% Hypoechoic Echotexture 39% 18% From Susan Mandel 2008 Leboulleux JCEM 2007 Ahuja, Clinical Radiology 2001

47 Malignant Node: AP/T >0.5

48 Malignant Nodes AP/TV >0.5

49 Malignant Node

50 Jugular Displacement Calcification
51 Jugular Displacement
52 Enhancement Cystic Necrosis

53 Heterogeneous Echogenicity Calcifications
54 Papillary Carcinoma Tall Cell Calcified Node

55 Papillary Carcinoma Node Chaotic Vascularity


56 Metastatic Papillary Carcinoma Central Lateral

57 Lymph node in central compartment
58 Compartment 3 - Malignant

59 Central Compartment Node hypoechoic

60 Malignant Node hyperechoic

61 Malignant Node Anaplastic CA

62 Malignant Node Hurthle Cell CA

63 Chaotic vascularization
64 What do we do when US detects an abnormal LN? RECOMMENDATION 65 B) If a positive result would change management, ultrasonographically suspicious lymph nodes > 8-10 mm (see Recommendation 71) in the smallest diameter should be biopsied for cytology with Tg measurement in the needle washout fluid. (Strong recommendation, Low-quality evidence) Haugen et al Thyroid 2016
65 Detection of malignancy in 40 LNs after US guided FNA Cyto FNA Tg Sensitivity (%) TG Ab+ TG Ab- Patients' Ab status Boi, J Clin Endocrinol Metab, 2006
66 143 Consecutive Patients with Stage I and II Papillary Cancer June 2003-November patients had 1 or more suspicious lymph nodes and underwent UG-FNA. 14 patients had positive cytology and/or Tg washout. Baskin, Thyroid 14:11:2004
67 Recurrent Cancer Patients Age/sex Years Tg Tg AB Cytology FNA-Tg 22 M M 13 < F 12 < F 20 < M 2 < M M M F 1 < F ,936 43F F 13 < F F



68 The challenge of minimal residual/recurrent disease right IJ CA left IJ CA
69 Recommendation 65 C) Suspicious lymph nodes less than 8-10 mm in smallest diameter may be followed without biopsy with consideration for FNA or intervention if there is growth or if the node threatens vital structures. (Weak recommendation, Low-quality evidence) Haugen et al Thyroid 2016
70 Differential Diagnosis of Cervical Lymph Nodes Benign Reactive Thyroid Cancers Cervical Lymphoma Chronic Lymphocytic Leukemia Metastases from other Cancers Sarcoid

71 Cervical Lymphoma

72 Cervical Lymphoma
73 Chronic Lymphocytic Leukemia
74 Chronic Lymphocytic Leukemia


75 Breast metastases to Cervical Compartment IV

76 Breast Cancer Compartment IV

77 Sarcoid Cervical Adenopathy NOT vascular
78 Role of cross sectional imaging in setting of rising thyroglobulin: Neck MRI or CT with contrast for clinically occult nodes Retropharynx Parapharyngeal space Low cervical lymph nodes Mediastinum Consider in patients with prior metastatic LNs in anterior cervical compartments Kaplan, Mandel J Neuroradiol, 2009



79 History of thyroid cancer, rising thyroglobulin Left retropharyngeal lymph node CT guided FNA Kaplan, Mandel J Neuroradiol, 2009
80 Conclusions Lymph node mets (esp micromets) are extremely common in PTC Preoperative recognition of CLINICALLY apparent lymph nodes with ultrasound changes the surgical approach and reduces the chance of reoperation Malignant nodes are often rounded (AP/T >0.5) with loss of visible hilum.
81 Conclusions Nodes with internal calcification or cystic changes are highly suspicious for malignancy Cytology and Tg needle washout are collected from LN FNA procedures Tg needle washout remains valid in presence of Tg Ab
82 Conclusions CT or MRI can be used preoperatively to define tissue planes in bulky or potentially invasive disease CT or MRI can be used postoperatively in patients with persistent Tg to look for retropharygeal or mediastinal nodes
Ultrasound for Pre-operative Evaluation of Well Differentiated Thyroid Cancer
 Ultrasound for Pre-operative Evaluation of Well Differentiated Thyroid Cancer Its Not Just About the Nodes AACE Advances in Medical and Surgical Management of Thyroid Cancer - 2017 Robert A. Levine, MD,
Ultrasound for Pre-operative Evaluation of Well Differentiated Thyroid Cancer Its Not Just About the Nodes AACE Advances in Medical and Surgical Management of Thyroid Cancer - 2017 Robert A. Levine, MD,
Pre-operative Ultrasound of Lymph Nodes in Thyroid Cancer
 Pre-operative Ultrasound of Lymph Nodes in Thyroid Cancer AACE - Advances in Medical and Surgical Management of Thyroid Cancer - 2018 Robert A. Levine, MD, FACE, ECNU Thyroid Center of New Hampshire Geisel
Pre-operative Ultrasound of Lymph Nodes in Thyroid Cancer AACE - Advances in Medical and Surgical Management of Thyroid Cancer - 2018 Robert A. Levine, MD, FACE, ECNU Thyroid Center of New Hampshire Geisel
Imaging in Thyroid Cancer
 Imaging in Thyroid Cancer Susan J. Mandel MD MPH University of Pennsylvania School of Medicine Philadelphia, PA I-123 Ultrasound Background Radioiodine ablation of thyroid remnants after surgery is a generally
Imaging in Thyroid Cancer Susan J. Mandel MD MPH University of Pennsylvania School of Medicine Philadelphia, PA I-123 Ultrasound Background Radioiodine ablation of thyroid remnants after surgery is a generally
WTC 2013 Panel Discussion: Minimal disease
 WTC 2013 Panel Discussion: Minimal disease Susan J. Mandel MD MPH Panelists Ken Ain Yasuhiro Ito Stephanie Lee Erich Sturgis Mark Urken Faculty/Presenter Disclosure Relationships with commercial interests
WTC 2013 Panel Discussion: Minimal disease Susan J. Mandel MD MPH Panelists Ken Ain Yasuhiro Ito Stephanie Lee Erich Sturgis Mark Urken Faculty/Presenter Disclosure Relationships with commercial interests
AACE/ACE Advanced Endocrine Neck Ultrasound Training Course 2016
 AACE/ACE Advanced Endocrine Neck Ultrasound Training Course 2016 This 9mm left inferior nodule should remind us all why we re here! There is no absolute number of images required for documentation
AACE/ACE Advanced Endocrine Neck Ultrasound Training Course 2016 This 9mm left inferior nodule should remind us all why we re here! There is no absolute number of images required for documentation
Cervical Lymph Nodes
 Cervical Lymph Nodes Diana Gaitini, MD Unit of Ultrasound, Department of Medical Imaging Rambam Medical Center and Faculty of Medicine Technion, Israel Institute of Technology Haifa, Israel Learning Targets
Cervical Lymph Nodes Diana Gaitini, MD Unit of Ultrasound, Department of Medical Imaging Rambam Medical Center and Faculty of Medicine Technion, Israel Institute of Technology Haifa, Israel Learning Targets
Overview. Extraglandular Thyroid Lymphatics. Management of the Lateral Neck in Well-Differentiated Thyroid Carcinoma. David W. Eisele, M.D., F.A.C.S.
 Management of the Lateral Neck in Well-Differentiated Thyroid Carcinoma David W. Eisele, M.D., F.A.C.S. Head and Neck Surgery and Oncology U.C.S.F. Comprehensive Cancer Center University of California,
Management of the Lateral Neck in Well-Differentiated Thyroid Carcinoma David W. Eisele, M.D., F.A.C.S. Head and Neck Surgery and Oncology U.C.S.F. Comprehensive Cancer Center University of California,
Sonographic Features of Thyroid Nodules & Guidelines for Management
 Sonographic Features of Thyroid Nodules & Guidelines for Management Mark A. Lupo, MD, FACE, ECNU Thyroid & Endocrine Center of Florida Assistant Clinical Professor of Medicine Florida State University,
Sonographic Features of Thyroid Nodules & Guidelines for Management Mark A. Lupo, MD, FACE, ECNU Thyroid & Endocrine Center of Florida Assistant Clinical Professor of Medicine Florida State University,
4/22/2010. Hakan Korkmaz, MD Assoc. Prof. of Otolaryngology Ankara Dıșkapı Training Hospital-Turkey.
 Management of Differentiated Thyroid Cancer: Head Neck Surgeon Perspective Hakan Korkmaz, MD Assoc. Prof. of Otolaryngology Ankara Dıșkapı Training Hospital-Turkey Thyroid gland Small endocrine gland:
Management of Differentiated Thyroid Cancer: Head Neck Surgeon Perspective Hakan Korkmaz, MD Assoc. Prof. of Otolaryngology Ankara Dıșkapı Training Hospital-Turkey Thyroid gland Small endocrine gland:
How Will (Should) the Latest Guidelines Affect the Endocrinologist s Management of Thyroid Cancer? AACE 2017
 the Latest Guidelines Affect the Endocrinologist s Management of Thyroid Cancer? AACE 2017") How Will (Should) the Latest Guidelines Affect the Endocrinologist s Management of Thyroid Cancer? AACE 2017 Bryan R. Haugen, MD University of Colorado, School of Medicine Outline Some statistics New guidelines
How Will (Should) the Latest Guidelines Affect the Endocrinologist s Management of Thyroid Cancer? AACE 2017 Bryan R. Haugen, MD University of Colorado, School of Medicine Outline Some statistics New guidelines
How good are we at finding nodules? Thyroid Nodules Thyroid Cancer Epidemiology Initial management Long-term follow up Disease-free status
 New Perspectives in Thyroid Cancer Jennifer Sipos, MD Assistant Professor of Medicine Division of Endocrinology The Ohio State University Outline Thyroid Nodules Thyroid Cancer Epidemiology Initial management
New Perspectives in Thyroid Cancer Jennifer Sipos, MD Assistant Professor of Medicine Division of Endocrinology The Ohio State University Outline Thyroid Nodules Thyroid Cancer Epidemiology Initial management
Persistent & Recurrent Differentiated Thyroid Cancer
 Persistent & Recurrent Differentiated Thyroid Cancer Electron Kebebew University of California, San Francisco Department of Surgery Objectives Risk factors for persistent & recurrent disease Causes of
Persistent & Recurrent Differentiated Thyroid Cancer Electron Kebebew University of California, San Francisco Department of Surgery Objectives Risk factors for persistent & recurrent disease Causes of
2015 American Thyroid Association Thyroid Nodule and Cancer Guidelines
 2015 American Thyroid Association Thyroid Nodule and Cancer Guidelines Angela M. Leung, MD, MSc, ECNU November 5, 2016 Outline Workup of nontoxic thyroid nodule(s) Ultrasound FNAB Management of FNAB results
2015 American Thyroid Association Thyroid Nodule and Cancer Guidelines Angela M. Leung, MD, MSc, ECNU November 5, 2016 Outline Workup of nontoxic thyroid nodule(s) Ultrasound FNAB Management of FNAB results
Thyroid Nodule. Disclosure. Learning Objectives P A P A P A 3/18/2014. Nothing to disclose.
 Thyroid Nodule Evaluating the patient with a thyroid nodule and some management options. Miguel V. Valdez PA C Disclosure Nothing to disclose. Learning Objectives Examination of thyroid gland Options for
Thyroid Nodule Evaluating the patient with a thyroid nodule and some management options. Miguel V. Valdez PA C Disclosure Nothing to disclose. Learning Objectives Examination of thyroid gland Options for
The International Federation of Head and Neck Oncologic Societies. Current Concepts in Head and Neck Surgery and Oncology
 The International Federation of Head and Neck Oncologic Societies Current Concepts in Head and Neck Surgery and Oncology www.ifhnos.net The International Federation of Head and Neck Oncologic Societies
The International Federation of Head and Neck Oncologic Societies Current Concepts in Head and Neck Surgery and Oncology www.ifhnos.net The International Federation of Head and Neck Oncologic Societies
Prophylactic Central Compartment Neck Dissection(CCND) for Papillary Thyroid Cancer: Con
 for Papillary Thyroid Cancer: Con") Prophylactic Central Compartment Neck Dissection(CCND) for Papillary Thyroid Cancer: Con Christopher R. McHenry, M.D. Vice Chairman Department of Surgery MetroHealth Medical Center Professor of Surgery
Prophylactic Central Compartment Neck Dissection(CCND) for Papillary Thyroid Cancer: Con Christopher R. McHenry, M.D. Vice Chairman Department of Surgery MetroHealth Medical Center Professor of Surgery
Thyroid Surgery: Lobectomy, total thyroidectomy, LN biopsies or only watchful waiting?
 Thyroid Surgery: Lobectomy, total thyroidectomy, LN biopsies or only watchful waiting? Jacob Moalem, MD, FACS Associate Professor Endocrine Surgery and Endocrinology URMC Agenda 1. When is lobectomy alone
Thyroid Surgery: Lobectomy, total thyroidectomy, LN biopsies or only watchful waiting? Jacob Moalem, MD, FACS Associate Professor Endocrine Surgery and Endocrinology URMC Agenda 1. When is lobectomy alone
Differentiated Thyroid Carcinoma
 Differentiated Thyroid Carcinoma The GOOD cancer? Jennifer Sipos, MD Associate Professor of Medicine Director, Benign Thyroid Program Division of Endocrinology, Diabetes and Metabolism The Ohio State University
Differentiated Thyroid Carcinoma The GOOD cancer? Jennifer Sipos, MD Associate Professor of Medicine Director, Benign Thyroid Program Division of Endocrinology, Diabetes and Metabolism The Ohio State University
Disclosures Nodal Management in Differentiated Thyroid Carcinoma
 Disclosures Nodal Management in Differentiated Thyroid Carcinoma Nothing to disclose Jonathan George, MD, MPH Assistant Professor UCSF Head and Neck Oncologic & Endocrine Surgery Objectives Overview Describe
Disclosures Nodal Management in Differentiated Thyroid Carcinoma Nothing to disclose Jonathan George, MD, MPH Assistant Professor UCSF Head and Neck Oncologic & Endocrine Surgery Objectives Overview Describe
Thyroid Nodules: US Risk Stratification. Alex Tessnow, MD, FACE, ECNU University of Texas Southwestern Associate Professor of Medicine Dallas, Texas
 Thyroid Nodules: US Risk Stratification Alex Tessnow, MD, FACE, ECNU University of Texas Southwestern Associate Professor of Medicine Dallas, Texas Which of the following is true? A. All echogenic foci
Thyroid Nodules: US Risk Stratification Alex Tessnow, MD, FACE, ECNU University of Texas Southwestern Associate Professor of Medicine Dallas, Texas Which of the following is true? A. All echogenic foci
Gerard M. Doherty, MD
 Surgical Management of Differentiated Thyroid Cancer: Update on 2015 ATA Guidelines Gerard M. Doherty, MD Chair of Surgery Utley Professor of Surgery and Medicine Boston University Surgeon-in-Chief Boston
Surgical Management of Differentiated Thyroid Cancer: Update on 2015 ATA Guidelines Gerard M. Doherty, MD Chair of Surgery Utley Professor of Surgery and Medicine Boston University Surgeon-in-Chief Boston
Management of Recurrent Thyroid Cancer
 Management of Recurrent Thyroid Cancer Eric Genden, MD, MHA Isidore Professor and Chairman Department of Otolaryngology- Head and Neck Surgery Senior Associate Dean for Clinical Affairs The Icahn School
Management of Recurrent Thyroid Cancer Eric Genden, MD, MHA Isidore Professor and Chairman Department of Otolaryngology- Head and Neck Surgery Senior Associate Dean for Clinical Affairs The Icahn School
Thyroid Cancer: When to Treat? MEGAN R. HAYMART, MD
 Thyroid Cancer: When to Treat? MEGAN R. HAYMART, MD ASSOCIATE PROFESSOR OF MEDICINE UNIVERSITY OF MICHIGAN MICHIGAN AACE 2018 ANNUAL MEETING Thyroid Cancer: When Not to Treat? FOCUS WILL BE ON LOW-RISK
Thyroid Cancer: When to Treat? MEGAN R. HAYMART, MD ASSOCIATE PROFESSOR OF MEDICINE UNIVERSITY OF MICHIGAN MICHIGAN AACE 2018 ANNUAL MEETING Thyroid Cancer: When Not to Treat? FOCUS WILL BE ON LOW-RISK
Differentiated Thyroid Cancer: Initial Management
 Page 1 ATA HOME GIVE ONLINE ABOUT THE ATA JOIN THE ATA MEMBER SIGN-IN INFORMATION FOR PATIENTS FIND A THYROID SPECIALIST Home Management Guidelines for Patients with Thyroid Nodules and Differentiated
Page 1 ATA HOME GIVE ONLINE ABOUT THE ATA JOIN THE ATA MEMBER SIGN-IN INFORMATION FOR PATIENTS FIND A THYROID SPECIALIST Home Management Guidelines for Patients with Thyroid Nodules and Differentiated
Approach to Thyroid Nodules
 Approach to Thyroid Nodules Alice Y.Y. Cheng, MD, FRCPC Twitter: @AliceYYCheng Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted
Approach to Thyroid Nodules Alice Y.Y. Cheng, MD, FRCPC Twitter: @AliceYYCheng Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted
Reoperative central neck surgery
 Reoperative central neck surgery R. Pandev, I. Tersiev, M. Belitova, A. Kouizi, D. Damyanov University Clinic of Surgery, Section Endocrine Surgery University Hospital Queen Johanna ISUL Medical University
Reoperative central neck surgery R. Pandev, I. Tersiev, M. Belitova, A. Kouizi, D. Damyanov University Clinic of Surgery, Section Endocrine Surgery University Hospital Queen Johanna ISUL Medical University
Objectives. 1)To recall thyroid nodule ultrasound characteristics that increase the risk of malignancy
To recall thyroid nodule ultrasound characteristics that increase the risk of malignancy") Evaluation and Management of Thyroid Nodules in Primary Care Chris Sadler, MA, PA C, CDE, DFAAPA Medical Science Outcomes Liaison Intarcia Diabetes and Endocrine Associates La Jolla, CA Past President
Evaluation and Management of Thyroid Nodules in Primary Care Chris Sadler, MA, PA C, CDE, DFAAPA Medical Science Outcomes Liaison Intarcia Diabetes and Endocrine Associates La Jolla, CA Past President
Case Papillary thyroid carcinoma(ptc):local recurrence post thyroidectomy
:local recurrence post thyroidectomy") Case 16070 Papillary thyroid carcinoma(ptc):local recurrence post thyroidectomy Dr Alka Ashmita Singhal, Dr Deepak Sarin 1, Dr Monika Aggarwal, Dr Haimanti Sarin2 Medanta The Medicity Hospital, Medanta
Case 16070 Papillary thyroid carcinoma(ptc):local recurrence post thyroidectomy Dr Alka Ashmita Singhal, Dr Deepak Sarin 1, Dr Monika Aggarwal, Dr Haimanti Sarin2 Medanta The Medicity Hospital, Medanta
Objectives. How to Investigate Thyroid Nodules like A Pro
 How to Investigate Thyroid Nodules like A Pro Chris Sadler, MA, PA C, CDE, DFAAPA Medical Science Outcomes Liaison Intarcia Diabetes and Endocrine Associates La Jolla, CA Past President ASEPA Disclosures
How to Investigate Thyroid Nodules like A Pro Chris Sadler, MA, PA C, CDE, DFAAPA Medical Science Outcomes Liaison Intarcia Diabetes and Endocrine Associates La Jolla, CA Past President ASEPA Disclosures
Ultrasonography of the Neck as an Adjunct to FNA. Nicole Massoll M.D.
 Ultrasonography of the Neck as an Adjunct to FNA Nicole Massoll M.D. Basic Features of Head and Neck Ultrasound and Anatomy Nicole Massoll M.D. University of Arkansas for Medical Sciences, Little Rock
Ultrasonography of the Neck as an Adjunct to FNA Nicole Massoll M.D. Basic Features of Head and Neck Ultrasound and Anatomy Nicole Massoll M.D. University of Arkansas for Medical Sciences, Little Rock
Long Term Follow-Up for Differentiated Thyroid Cancer: The Mayo Experience
 Long Term Follow-Up for Differentiated Thyroid Cancer: The Mayo Experience Geoffrey B. Thompson, MD Professor of Surgery College of Medicine, Mayo Clinic Differentiated Thyroid Cancer Objectives Overview
Long Term Follow-Up for Differentiated Thyroid Cancer: The Mayo Experience Geoffrey B. Thompson, MD Professor of Surgery College of Medicine, Mayo Clinic Differentiated Thyroid Cancer Objectives Overview
Thyroid US. Background: Thyroid/Neck US. Use of Office Ultrasound in the Thyroid Surgery Practice
 2010 UCSF Head and Neck Endocrine Surgery Course Use of Office Ultrasound in the Thyroid Surgery Practice Lisa A. Orloff, MD FACS Dept of Otolaryngology-Head and Neck Surgery University of California,
2010 UCSF Head and Neck Endocrine Surgery Course Use of Office Ultrasound in the Thyroid Surgery Practice Lisa A. Orloff, MD FACS Dept of Otolaryngology-Head and Neck Surgery University of California,
Case-Based Discussion of Thyroid Cancer Therapy
 Case-Based Discussion of Thyroid Cancer Therapy Matthew D. Ringel, MD Ralph W. Kurtz Chair and Professor of Medicine Director, Division of Endocrinology The Ohio State University Co-Leader, Molecular Biology
Case-Based Discussion of Thyroid Cancer Therapy Matthew D. Ringel, MD Ralph W. Kurtz Chair and Professor of Medicine Director, Division of Endocrinology The Ohio State University Co-Leader, Molecular Biology
5/3/2017. Ahn et al N Engl J Med 2014; 371
 Alan Failor, M.D. Clinical Professor of Medicine Division of Metabolism, Endocrinology and Nutrition University of Washington April 20, 2017 No disclosures to report 1. Appropriately evaluate s in adult
Alan Failor, M.D. Clinical Professor of Medicine Division of Metabolism, Endocrinology and Nutrition University of Washington April 20, 2017 No disclosures to report 1. Appropriately evaluate s in adult
Radiology- Pathology Conference 4/29/2012. Lymph Nodes. John McGrath
 Radiology- Pathology Conference 4/29/2012 Lymph Nodes John McGrath 1 Presentation material is for education purposes only. All rights reserved. 2012 URMC Radiology Page 1 of 24 Case 1: 51 year-old male
Radiology- Pathology Conference 4/29/2012 Lymph Nodes John McGrath 1 Presentation material is for education purposes only. All rights reserved. 2012 URMC Radiology Page 1 of 24 Case 1: 51 year-old male
A variation in recurrence patterns of papillary thyroid cancer with disease progression: A long-term follow-up study
 ORIGINAL ARTICLE A variation in recurrence patterns of papillary thyroid cancer with disease progression: A long-term follow-up study Joon-Hyop Lee, MD, Yoo Seung Chung, MD, PhD,* Young Don Lee, MD, PhD
ORIGINAL ARTICLE A variation in recurrence patterns of papillary thyroid cancer with disease progression: A long-term follow-up study Joon-Hyop Lee, MD, Yoo Seung Chung, MD, PhD,* Young Don Lee, MD, PhD
THYROID CANCER IN CHILDREN. Humberto Lugo-Vicente MD FACS FAAP Professor Pediatric Surgery UPR School of Medicine
 THYROID CANCER IN CHILDREN Humberto Lugo-Vicente MD FACS FAAP Professor Pediatric Surgery UPR School of Medicine Thyroid nodules Rare Female predominance 4-fold as likely to be malignant Hx Radiation exposure?
THYROID CANCER IN CHILDREN Humberto Lugo-Vicente MD FACS FAAP Professor Pediatric Surgery UPR School of Medicine Thyroid nodules Rare Female predominance 4-fold as likely to be malignant Hx Radiation exposure?
Thyroid nodules. Most thyroid nodules are benign
 Thyroid nodules Postgraduate Course in General Surgery Jessica E. Gosnell MD Assistant Professor March 22, 2011 Most thyroid nodules are benign thyroid nodules occur in 77% of the world s population palpable
Thyroid nodules Postgraduate Course in General Surgery Jessica E. Gosnell MD Assistant Professor March 22, 2011 Most thyroid nodules are benign thyroid nodules occur in 77% of the world s population palpable
Thyroid Neoplasm. ORL-Head and neck Surgery 2014
 In The Name of God Thyroid Neoplasm ORL-Head and neck Surgery 2014 Malignant Neoplasm By age 90, virtually everyone has nodules Estimates of cancer prevalence at autopsy 4% to 36% Why these lesions are
In The Name of God Thyroid Neoplasm ORL-Head and neck Surgery 2014 Malignant Neoplasm By age 90, virtually everyone has nodules Estimates of cancer prevalence at autopsy 4% to 36% Why these lesions are
Risk Adapted Follow-Up
 Risk Adapted Follow-Up Individualizing Follow- Up Strategies R Michael Tuttle, MD Clinical Director, Endocrinology Service Memorial Sloan Kettering Cancer Center Professor of Medicine Weill Medical College
Risk Adapted Follow-Up Individualizing Follow- Up Strategies R Michael Tuttle, MD Clinical Director, Endocrinology Service Memorial Sloan Kettering Cancer Center Professor of Medicine Weill Medical College
Thyroid nodules 3/22/2011. Most thyroid nodules are benign. Thyroid nodules: differential diagnosis
 Most thyroid nodules are benign Thyroid nodules Postgraduate Course in General Surgery thyroid nodules occur in 77% of the world s population palpable thyroid nodules occur in about 5% of women and 1%
Most thyroid nodules are benign Thyroid nodules Postgraduate Course in General Surgery thyroid nodules occur in 77% of the world s population palpable thyroid nodules occur in about 5% of women and 1%
42 yr old male with h/o Graves disease and prior I 131 treatment presents with hyperthyroidism and undetectable TSH. 2 hr uptake 20%, 24 hr uptake 50%
 Pinhole images of the neck are acquired in multiple projections, 24hrs after the oral administration of approximately 200 µci of I123. Usually, 24hr uptake value if also calculated (normal 24 hr uptake
Pinhole images of the neck are acquired in multiple projections, 24hrs after the oral administration of approximately 200 µci of I123. Usually, 24hr uptake value if also calculated (normal 24 hr uptake
Thyroid Nodules: US Risk Stratification and FNA Guidelines
 Thyroid Nodules: US Risk Stratification and FNA Guidelines Mark A. Lupo, MD, FACE, ECNU Thyroid & Endocrine Center of Florida Assistant Clinical Professor of Medicine Florida State University, College
Thyroid Nodules: US Risk Stratification and FNA Guidelines Mark A. Lupo, MD, FACE, ECNU Thyroid & Endocrine Center of Florida Assistant Clinical Professor of Medicine Florida State University, College
5/18/2013. Most thyroid nodules are benign. Thyroid nodules: new techniques in evaluation
 Most thyroid nodules are benign Thyroid nodules: new techniques in evaluation Incidence Etiology Risk factors Diagnosis Gene classification system Treatment Postgraduate Course in General Surgery Jessica
Most thyroid nodules are benign Thyroid nodules: new techniques in evaluation Incidence Etiology Risk factors Diagnosis Gene classification system Treatment Postgraduate Course in General Surgery Jessica
PAPILLARY THYROID CARCINOMA PRESENTING AS A LATERAL NECK MASS MASS. Dr. Pamela Hanson DO PGY3
 PAPILLARY THYROID CARCINOMA PRESENTING AS A LATERAL NECK MASS MASS Dr. Pamela Hanson DO PGY3 MK CASE PRESENTATION 28 yo Female presented to the ENT Clinic in October 2016, with the complaint of chronic
PAPILLARY THYROID CARCINOMA PRESENTING AS A LATERAL NECK MASS MASS Dr. Pamela Hanson DO PGY3 MK CASE PRESENTATION 28 yo Female presented to the ENT Clinic in October 2016, with the complaint of chronic
Strategies for detection of recurrent disease in longterm follow-up of differentiated thyroid cancer
 Strategies for detection of recurrent disease in longterm follow-up of differentiated thyroid cancer A rational approach to longterm follow-up based on dynamic risk assessment. World Congress on Thyroid
Strategies for detection of recurrent disease in longterm follow-up of differentiated thyroid cancer A rational approach to longterm follow-up based on dynamic risk assessment. World Congress on Thyroid
AACE/ACE Principles of Endocrine Neck Sonography Course
 AACE/ACE Principles of Endocrine Neck Sonography Course Primary objective of thyroid ultrasound: assess for malignant disease Nodular Disease Benign Malignant Goiter Iodine deficient Thyroiditis Organification
AACE/ACE Principles of Endocrine Neck Sonography Course Primary objective of thyroid ultrasound: assess for malignant disease Nodular Disease Benign Malignant Goiter Iodine deficient Thyroiditis Organification
Thyroid Nodule Risk Stratification and FNA Guidelines
 Thyroid Nodule Risk Stratification and FNA Guidelines Mark A. Lupo, MD, FACE, ECNU Thyroid & Endocrine Center of Florida Assistant Clinical Professor of Medicine Florida State University, College of Medicine
Thyroid Nodule Risk Stratification and FNA Guidelines Mark A. Lupo, MD, FACE, ECNU Thyroid & Endocrine Center of Florida Assistant Clinical Professor of Medicine Florida State University, College of Medicine
Pediatric Thyroid Cancer Lung Metastases. Liora Lazar MD
 Pediatric Thyroid Cancer Lung Metastases Liora Lazar MD Differentiated thyroid cancer (DTC) The 3rd most common solid tumor in childhood and adolescence Accounting for 1.5%-3% of all childhood cancers
Pediatric Thyroid Cancer Lung Metastases Liora Lazar MD Differentiated thyroid cancer (DTC) The 3rd most common solid tumor in childhood and adolescence Accounting for 1.5%-3% of all childhood cancers
Evaluation and Management of Thyroid Nodules. Nick Vernetti, MD, FACE Palm Medical Group Las Vegas, Nevada
 Evaluation and Management of Thyroid Nodules Nick Vernetti, MD, FACE Palm Medical Group Las Vegas, Nevada Disclosure Consulting Amgen Speaking Amgen Objectives Understand the significance of incidental
Evaluation and Management of Thyroid Nodules Nick Vernetti, MD, FACE Palm Medical Group Las Vegas, Nevada Disclosure Consulting Amgen Speaking Amgen Objectives Understand the significance of incidental
USGFNA of thyroid nodules
 US Guided FNA (USGFNA) of neck masses INTERVENTIONAL HEAD & NECK ULTRASOUND Brendan C. Stack, Jr., MD., FACS, FACE Professor Otolaryngology-Head and Neck Surgery Indications Technique Interpretation Results
US Guided FNA (USGFNA) of neck masses INTERVENTIONAL HEAD & NECK ULTRASOUND Brendan C. Stack, Jr., MD., FACS, FACE Professor Otolaryngology-Head and Neck Surgery Indications Technique Interpretation Results
I-131 ABLATION AND ADJUVANT THERAPY OF THYROID CANCER
 AMERICAN ASSOCIATION OF CLINICAL ENDOCRINOLOGISTS Advances in Medical and Surgical Management of Thyroid Cancer January 23-24, 2015 I-131 ABLATION AND ADJUVANT THERAPY OF THYROID CANCER 2015 Leonard Wartofsky,
AMERICAN ASSOCIATION OF CLINICAL ENDOCRINOLOGISTS Advances in Medical and Surgical Management of Thyroid Cancer January 23-24, 2015 I-131 ABLATION AND ADJUVANT THERAPY OF THYROID CANCER 2015 Leonard Wartofsky,
Thyroid Nodules. Dr. HAKIMI, SpAK Dr. MELDA DELIANA, SpAK Dr. SISKA MAYASARI LUBIS, SpA
 Thyroid Nodules ENDOCRINOLOGY DIVISION ENDOCRINOLOGY DIVISION Dr. HAKIMI, SpAK Dr. MELDA DELIANA, SpAK Dr. SISKA MAYASARI LUBIS, SpA Anatomical Considerations The Thyroid Nodule Congenital anomalies Thyroglossal
Thyroid Nodules ENDOCRINOLOGY DIVISION ENDOCRINOLOGY DIVISION Dr. HAKIMI, SpAK Dr. MELDA DELIANA, SpAK Dr. SISKA MAYASARI LUBIS, SpA Anatomical Considerations The Thyroid Nodule Congenital anomalies Thyroglossal
The International Federation of Head and Neck Oncologic Societies. Current Concepts in Head and Neck Surgery and Oncology
 The International Federation of Head and Neck Oncologic Societies Current Concepts in Head and Neck Surgery and Oncology www.ifhnos.net The International Federation of Head and Neck Oncologic Societies
The International Federation of Head and Neck Oncologic Societies Current Concepts in Head and Neck Surgery and Oncology www.ifhnos.net The International Federation of Head and Neck Oncologic Societies
3/29/2012. Thyroid cancer- what s new. Thyroid Cancer. Thyroid cancer is now the most rapidly increasing cancer in women
 Thyroid cancer- what s new Thyroid Cancer Changing epidemiology Molecular markers Lymph node dissection Technical advances rhtsh Genetic testing and prophylactic surgery Vandetanib What s new? Jessica
Thyroid cancer- what s new Thyroid Cancer Changing epidemiology Molecular markers Lymph node dissection Technical advances rhtsh Genetic testing and prophylactic surgery Vandetanib What s new? Jessica
Index. radiologic.theclinics.com. Note: Page numbers of article titles are in boldface type.
 Index Note: Page numbers of article titles are in boldface type. A ACC. See Adrenal cortical carcinoma. Acromegaly and the pituitary gland, 551 Acute suppurative thyroiditis, 405, 406 Addison, Thomas and
Index Note: Page numbers of article titles are in boldface type. A ACC. See Adrenal cortical carcinoma. Acromegaly and the pituitary gland, 551 Acute suppurative thyroiditis, 405, 406 Addison, Thomas and
(Not so) New Guidelines for Management of Thyroid Nodules and Differentiated Thyroid Cancer Minnesota/Midwest Chapter of AACE
 New Guidelines for Management of Thyroid Nodules and Differentiated Thyroid Cancer Minnesota/Midwest Chapter of AACE") (Not so) New Guidelines for Management of Thyroid Nodules and Differentiated Thyroid Cancer Minnesota/Midwest Chapter of AACE Bryan R. Haugen, MD University of Colorado, School of Medicine Outline Some
(Not so) New Guidelines for Management of Thyroid Nodules and Differentiated Thyroid Cancer Minnesota/Midwest Chapter of AACE Bryan R. Haugen, MD University of Colorado, School of Medicine Outline Some
PEDIATRIC Ariel Katz MD
 PEDIATRIC Ariel Katz MD Dept. Otolaryngology Head &Neck Surgery Wolfson Medical Center Holon, Israel OBJECTIVES Overview/Background Epidemiology/Etiology Intro to Guidelines Workup Treatment Follow-Up
PEDIATRIC Ariel Katz MD Dept. Otolaryngology Head &Neck Surgery Wolfson Medical Center Holon, Israel OBJECTIVES Overview/Background Epidemiology/Etiology Intro to Guidelines Workup Treatment Follow-Up
PARATHYROID IMAGING. James Lee, MD Chief, Endocrine Surgery Co-Director NY Thyroid-Parathyroid Center Columbia University Medical Center
 PARATHYROID IMAGING James Lee, MD Chief, Endocrine Surgery Co-Director NY Thyroid-Parathyroid Center Columbia University Medical Center NO DISCLOSURES Overview The hallmarks of the ideal test Benefits
PARATHYROID IMAGING James Lee, MD Chief, Endocrine Surgery Co-Director NY Thyroid-Parathyroid Center Columbia University Medical Center NO DISCLOSURES Overview The hallmarks of the ideal test Benefits
Thyroid Ultrasound Physics and Doppler
 Thyroid Ultrasound Physics and Doppler Advanced AACE-ACE US training course 2017 Dev Abraham MD, MRCP(UK), ECNU, FACE Professor of Medicine, University of Utah No Disclosures Natural Ability to see with
Thyroid Ultrasound Physics and Doppler Advanced AACE-ACE US training course 2017 Dev Abraham MD, MRCP(UK), ECNU, FACE Professor of Medicine, University of Utah No Disclosures Natural Ability to see with
Dr J K Jekel Dept. Surgery University of Pretoria
 Dr J K Jekel Dept. Surgery University of Pretoria No Maybe ( T`s and C`s apply ) 1. Total thyroidectomy 2. Neck dissection only if nodes are involved 3. Ablative dose or doses of Radioactive Iodine 4.
Dr J K Jekel Dept. Surgery University of Pretoria No Maybe ( T`s and C`s apply ) 1. Total thyroidectomy 2. Neck dissection only if nodes are involved 3. Ablative dose or doses of Radioactive Iodine 4.
High thyroglobulin (Tg) in a lymph node indicates metastatic
 in a lymph node indicates metastatic") ORIGINAL RESEARCH HEAD & NECK Optimized Cutoff Value and Indication for Washout Thyroglobulin Level According to Ultrasound Findings in Patients with Well-Differentiated Thyroid Cancer J.Y. Jung, J.H.
ORIGINAL RESEARCH HEAD & NECK Optimized Cutoff Value and Indication for Washout Thyroglobulin Level According to Ultrasound Findings in Patients with Well-Differentiated Thyroid Cancer J.Y. Jung, J.H.
Endocrinology and Metabolic Disorder Unit Regina Apostolorum Hospital
 Enrico Papini Endocrinology and Metabolic Disorder Unit Regina Apostolorum Hospital Albano Laziale, Italy The Following Faculty have provide no information regarding significant relationship with commercial
Enrico Papini Endocrinology and Metabolic Disorder Unit Regina Apostolorum Hospital Albano Laziale, Italy The Following Faculty have provide no information regarding significant relationship with commercial
40 TH EUROPEAN CONGRESS 0F CYTOLOGY LIVERPOOL, UK October 2-5, 2016
 Outcomes from the diagnostic approach of thyroid lesions using US-FNA and LBC in clinical practice Emmanouel Mastorakis MD PhD Cytopathologist Director in Cytopathology Laboratory Regional General Hospital
Outcomes from the diagnostic approach of thyroid lesions using US-FNA and LBC in clinical practice Emmanouel Mastorakis MD PhD Cytopathologist Director in Cytopathology Laboratory Regional General Hospital
34 year-old Female with Thyroid Cancer
 34 year-old Female with Thyroid Cancer KATIE O SULLIVAN, MD FELLOW, ADULT/PEDIATRIC ENDOCRINOLOGY UNIVERSITY OF CHICAGO ENDORAMA THURSDAY, SEPTEMBER 15 TH, 2016 Disclosures: I do not have any relevant
34 year-old Female with Thyroid Cancer KATIE O SULLIVAN, MD FELLOW, ADULT/PEDIATRIC ENDOCRINOLOGY UNIVERSITY OF CHICAGO ENDORAMA THURSDAY, SEPTEMBER 15 TH, 2016 Disclosures: I do not have any relevant
Dynamic Risk Stratification:
 Dynamic Risk Stratification: Using Risk Estimates to Guide Initial Management R Michael Tuttle, MD Clinical Director, Endocrinology Service Memorial Sloan Kettering Cancer Center Professor of Medicine
Dynamic Risk Stratification: Using Risk Estimates to Guide Initial Management R Michael Tuttle, MD Clinical Director, Endocrinology Service Memorial Sloan Kettering Cancer Center Professor of Medicine
Scientific Exhibit Authors:
 Real-time ultrasonography-guided fine needle non aspiration cytology of occult cervical lymphadenopathy in patients with thyroid malignancy without recurrent or residual thyroid cancer: accuracy and impact
Real-time ultrasonography-guided fine needle non aspiration cytology of occult cervical lymphadenopathy in patients with thyroid malignancy without recurrent or residual thyroid cancer: accuracy and impact
Current Issues in Thyroid Cancer Surgery in 2017
 Current Issues in Thyroid Cancer Surgery in 2017 Dr. David Goldstein MD Msc FRCSC FACS Associate Professor, Department Otolaryngology Head & Neck Surgery, U of T Department of Surgical Oncology, Princess
Current Issues in Thyroid Cancer Surgery in 2017 Dr. David Goldstein MD Msc FRCSC FACS Associate Professor, Department Otolaryngology Head & Neck Surgery, U of T Department of Surgical Oncology, Princess
Exercise 15: CSv2 Data Item Coding Instructions ANSWERS
 Exercise 15: CSv2 Data Item Coding Instructions ANSWERS CS Tumor Size Tumor size is the diameter of the tumor, not the depth or thickness of the tumor. Chest x-ray shows 3.5 cm mass; the pathology report
Exercise 15: CSv2 Data Item Coding Instructions ANSWERS CS Tumor Size Tumor size is the diameter of the tumor, not the depth or thickness of the tumor. Chest x-ray shows 3.5 cm mass; the pathology report
Adina Alazraki, MD, FAAP Assistant Professor Radiology and Pediatrics Emory University and Children s Healthcare of Atlanta
 Adina Alazraki, MD, FAAP Assistant Professor Radiology and Pediatrics Emory University and Children s Healthcare of Atlanta Review recently published pediatric guidelines for management of thyroid nodules
Adina Alazraki, MD, FAAP Assistant Professor Radiology and Pediatrics Emory University and Children s Healthcare of Atlanta Review recently published pediatric guidelines for management of thyroid nodules
Advanced Anatomy of the Neck
 AACE 2018 Advanced Anatomy of the Neck Alex Tessnow, MD, MBA, FACE, ECNU University of Texas Southwestern Dallas, TX Content contributed by: H. Jack Baskin, Daniel Duick, Diana Dean, Robert A. Levine,
AACE 2018 Advanced Anatomy of the Neck Alex Tessnow, MD, MBA, FACE, ECNU University of Texas Southwestern Dallas, TX Content contributed by: H. Jack Baskin, Daniel Duick, Diana Dean, Robert A. Levine,
Management of Thyroid Nodules. February 2 nd, 2018 Sarah Hopkins
 Management of Thyroid Nodules February 2 nd, 2018 Sarah Hopkins No disclosures Goals: Review Initial Evaluation of Thyroid Nodules Review Indications for Biopsy Approach to Multinodular Goiter Review Management
Management of Thyroid Nodules February 2 nd, 2018 Sarah Hopkins No disclosures Goals: Review Initial Evaluation of Thyroid Nodules Review Indications for Biopsy Approach to Multinodular Goiter Review Management
Management guideline for patients with differentiated thyroid cancer. Teeraporn Ratanaanekchai ENT, KKU 17 October 2007
 Management guideline for patients with differentiated thyroid Teeraporn Ratanaanekchai ENT, KKU 17 October 2007 Incidence (Srinagarind Hospital, 2005, both sex) Site (all) cases % 1. Liver 1178 27 2. Lung
Management guideline for patients with differentiated thyroid Teeraporn Ratanaanekchai ENT, KKU 17 October 2007 Incidence (Srinagarind Hospital, 2005, both sex) Site (all) cases % 1. Liver 1178 27 2. Lung
Carcinoma tiroideo differenziato: gestione della persistenza biochimica di malattia
 Carcinoma tiroideo differenziato: gestione della persistenza biochimica di malattia Massimo Torlontano U.O. Endocrinologia IRCCS Casa Sollievo della Sofferenza Thyroid cancer Incidence 1975-2009 (USA)
Carcinoma tiroideo differenziato: gestione della persistenza biochimica di malattia Massimo Torlontano U.O. Endocrinologia IRCCS Casa Sollievo della Sofferenza Thyroid cancer Incidence 1975-2009 (USA)
Treatment of Cervical Lymph Node Metastases Differentiated Thyroid Cancer
 Treatment of Cervical Lymph Node Metastases Differentiated Thyroid Cancer Well Differentiated Thyroid Cancer Natural History and Prognosis EORTC AGES AMES MACIS QuickTime and a TIFF (LZW) decompressor
Treatment of Cervical Lymph Node Metastases Differentiated Thyroid Cancer Well Differentiated Thyroid Cancer Natural History and Prognosis EORTC AGES AMES MACIS QuickTime and a TIFF (LZW) decompressor
Head & Neck Clinical Sub Group. Network Agreed Imaging Guidelines for UAT and Thyroid Cancer. Measure Nos: 11-1C-105i & 11-1C-106i
 Greater Manchester, Lancashire & South Cumbria Strategic Clinical Network & Senate Head & Neck Clinical Sub Group Network Agreed Imaging Guidelines for UAT and Thyroid Cancer Measure Nos: 11-1C-105i &
Greater Manchester, Lancashire & South Cumbria Strategic Clinical Network & Senate Head & Neck Clinical Sub Group Network Agreed Imaging Guidelines for UAT and Thyroid Cancer Measure Nos: 11-1C-105i &
131-I Therapy Planning in Thyroid Cancer: The role of diagnostic radioiodine scans
 131-I Therapy Planning in Thyroid Cancer: The role of diagnostic radioiodine scans Anca M. Avram, M.D. Associate Professor of Radiology Department of Nuclear Medicine University of Michigan Ann Arbor,
131-I Therapy Planning in Thyroid Cancer: The role of diagnostic radioiodine scans Anca M. Avram, M.D. Associate Professor of Radiology Department of Nuclear Medicine University of Michigan Ann Arbor,
Thyroid carcinoma. Assoc. prof. V. Marković, MD, PhD Assoc. prof. A. Punda, MD, PhD D. Brdar, MD, nucl. med. spec.
 Thyroid carcinoma Assoc. prof. V. Marković, MD, PhD Assoc. prof. A. Punda, MD, PhD D. Brdar, MD, nucl. med. spec. Thyroid tumors PRIMARY TUMORS Tumors of the follicular epithelium : - Tumors of the follicular
Thyroid carcinoma Assoc. prof. V. Marković, MD, PhD Assoc. prof. A. Punda, MD, PhD D. Brdar, MD, nucl. med. spec. Thyroid tumors PRIMARY TUMORS Tumors of the follicular epithelium : - Tumors of the follicular
Oncologist. The. Endocrinology. Use of Ultrasound in the Management of Thyroid Cancer. The Oncologist 2010;15:
 The Oncologist Endocrinology Use of Ultrasound in the Management of Thyroid Cancer JOHN I. LEW,CARMEN C. SOLORZANO Division of Endocrine Surgery, DeWitt Daughtry Family Department of Surgery, University
The Oncologist Endocrinology Use of Ultrasound in the Management of Thyroid Cancer JOHN I. LEW,CARMEN C. SOLORZANO Division of Endocrine Surgery, DeWitt Daughtry Family Department of Surgery, University
Thyroid and Parathyroid Ultrasound Protocol
 Thyroid and Parathyroid Ultrasound Protocol Reviewed By: Anna Ellermeier, MD Last Reviewed: December 2017 Contact: (866) 761-4200, Option 1 **NOTE for all examinations: 1. If documenting possible flow
Thyroid and Parathyroid Ultrasound Protocol Reviewed By: Anna Ellermeier, MD Last Reviewed: December 2017 Contact: (866) 761-4200, Option 1 **NOTE for all examinations: 1. If documenting possible flow
AACE Thyroid Cancer Tumor board 25 years of the Endocrine and Surgery collaboration
 AACE Thyroid Cancer Tumor board 25 years of the Endocrine and Surgery collaboration Dr. Peter Singer, Endocrinology Dr. Peter Sadow, Pathology Moderator Dr. Greg Randolph, Otolaryngology Relevant Financial
AACE Thyroid Cancer Tumor board 25 years of the Endocrine and Surgery collaboration Dr. Peter Singer, Endocrinology Dr. Peter Sadow, Pathology Moderator Dr. Greg Randolph, Otolaryngology Relevant Financial
Endocrine University, 2016 AACE-ACE-MAYO CLINIC
 Endocrine University, 2016 AACE-ACE-MAYO CLINIC Dev Abraham MD, MRCP (UK), ECNU Professor of Medicine (clinical), Division of Endocrinology Adjunct Professor of Surgery and Pathology Medical Director,
Endocrine University, 2016 AACE-ACE-MAYO CLINIC Dev Abraham MD, MRCP (UK), ECNU Professor of Medicine (clinical), Division of Endocrinology Adjunct Professor of Surgery and Pathology Medical Director,
THYROID CANCER IN CHILDREN
 THYROID CANCER IN CHILDREN Isabel ROCA, Montserrat NEGRE Joan CASTELL HU VALL HEBRON BARCELONA EPIDEMIOLOGY ADULTS males 1,2-2,6 cases /100.000 females 2,0-3,8 cases /100.000 0,02-0,3 / 100.000 children
THYROID CANCER IN CHILDREN Isabel ROCA, Montserrat NEGRE Joan CASTELL HU VALL HEBRON BARCELONA EPIDEMIOLOGY ADULTS males 1,2-2,6 cases /100.000 females 2,0-3,8 cases /100.000 0,02-0,3 / 100.000 children
RESEARCH ARTICLE. Hai-Shan Zhang 1, Ren-Jie Wang 2, Qing-Feng Fu 1, Shi Gao 2, Bu-Tong Sun 2, Hui Sun 1 *, Qing-Jie Ma 2 * Abstract.
 DOI:http://dx.doi.org/10.7314/APJCP.2014.15.24.10905 RESEARCH ARTICLE Diagnostic value of Thyroglobulin Measurement with Fineneedle Aspiration Biopsy for Lymph Node Metastases in Patients with a History
DOI:http://dx.doi.org/10.7314/APJCP.2014.15.24.10905 RESEARCH ARTICLE Diagnostic value of Thyroglobulin Measurement with Fineneedle Aspiration Biopsy for Lymph Node Metastases in Patients with a History
Key Topics in Thyroid Cancer Worldwide epidemic What Should the Endocrinologist and Surgeon do?
 Key Topics in Thyroid Cancer Worldwide epidemic What Should the Endocrinologist and Surgeon do? Martin Schlumberger Gustave Presenter Roussy Name and Université Paris Saclay, Villejuif, France 1 Disclosure
Key Topics in Thyroid Cancer Worldwide epidemic What Should the Endocrinologist and Surgeon do? Martin Schlumberger Gustave Presenter Roussy Name and Université Paris Saclay, Villejuif, France 1 Disclosure
Osman Ilkay Ozdamar, 1 Gul Ozbilen Acar, 1 Cigdem Kafkasli, 1 M. Tayyar Kalcioglu, 1 Tulay Zenginkinet, 2 and H. Gonca Tamer 3. 1.
 Case Reports in Otolaryngology Volume 2015, Article ID 79658, 4 pages http://dx.doi.org/10.1155/2015/79658 Case Report Papillary Thyroid Microcarcinoma with a Large Cystic Dilated Lymph Node Metastasis
Case Reports in Otolaryngology Volume 2015, Article ID 79658, 4 pages http://dx.doi.org/10.1155/2015/79658 Case Report Papillary Thyroid Microcarcinoma with a Large Cystic Dilated Lymph Node Metastasis
Imaging in Pediatric Thyroid disorders: US and Radionuclide imaging. Deepa R Biyyam, MD Attending Pediatric Radiologist
 Imaging in Pediatric Thyroid disorders: US and Radionuclide imaging Deepa R Biyyam, MD Attending Pediatric Radiologist Imaging in Pediatric Thyroid disorders: Imaging modalities Outline ACR-SNM-SPR guidelines
Imaging in Pediatric Thyroid disorders: US and Radionuclide imaging Deepa R Biyyam, MD Attending Pediatric Radiologist Imaging in Pediatric Thyroid disorders: Imaging modalities Outline ACR-SNM-SPR guidelines
Introduction: Ultrasound guided Fine Needle Aspiration: When and how
 International Course of Thyroid Ultrasonography and minimally invasive procedure 7-8 October 2016 University of Pisa, Italy Introduction: Ultrasound guided Fine Needle Aspiration: When and how Teresa Rago
International Course of Thyroid Ultrasonography and minimally invasive procedure 7-8 October 2016 University of Pisa, Italy Introduction: Ultrasound guided Fine Needle Aspiration: When and how Teresa Rago
Parathyroid Imaging: Current Concepts. Maria Gule-Monroe, M.D. Nancy Perrier, M.D.
 Parathyroid Imaging: Current Concepts Maria Gule-Monroe, M.D. Nancy Perrier, M.D. Disclosures None Objectives Ultrasound characteristics of parathyroid adenomas vs. lymph nodes 4D-CT evaluation of hyperparathyroidism
Parathyroid Imaging: Current Concepts Maria Gule-Monroe, M.D. Nancy Perrier, M.D. Disclosures None Objectives Ultrasound characteristics of parathyroid adenomas vs. lymph nodes 4D-CT evaluation of hyperparathyroidism
Contents. Basic Ultrasound Principles and Terminology. Ultrasound Nodule Characteristics
 Contents Basic Ultrasound Principles and Terminology Basic Ultrasound Principles... 1 Ultrasound System... 2 Linear Transducer for Superficial Images and Ultrasound-Guided FNA... 3 Scanning Planes... 4
Contents Basic Ultrasound Principles and Terminology Basic Ultrasound Principles... 1 Ultrasound System... 2 Linear Transducer for Superficial Images and Ultrasound-Guided FNA... 3 Scanning Planes... 4
Ultrasound-Guided Fine-Needle Aspiration of Thyroid Nodules: New events
 Ultrasound-Guided Fine-Needle Aspiration of Thyroid Nodules: New events Sandrine Rorive, M.D., PhD. Erasme Hospital - Université Libre de Bruxelles (ULB) INTRODUCTION The assessment of thyroid nodules
Ultrasound-Guided Fine-Needle Aspiration of Thyroid Nodules: New events Sandrine Rorive, M.D., PhD. Erasme Hospital - Université Libre de Bruxelles (ULB) INTRODUCTION The assessment of thyroid nodules
Management of Thyroid Nodules
 Management of Thyroid Nodules 38 y/o female with solid 1.5 cm right Thyroid nodule. TSH=0.68 Vincent J. Reid, MD., FACS Thyroid Cancer Incidence & Mortality 1974 to 2004 Overall Women Men Mortality 1 Cancer
Management of Thyroid Nodules 38 y/o female with solid 1.5 cm right Thyroid nodule. TSH=0.68 Vincent J. Reid, MD., FACS Thyroid Cancer Incidence & Mortality 1974 to 2004 Overall Women Men Mortality 1 Cancer
Oh, I get it, the TSH goes up and down
 Evaluation and Management of the Thyroid Nodule Oh, I get it, the TSH goes up and down UCSF Head and Neck Conference October 24, 2008 Peter A. Singer, M.D. Professor and Chief Clinical Endocrinology University
Evaluation and Management of the Thyroid Nodule Oh, I get it, the TSH goes up and down UCSF Head and Neck Conference October 24, 2008 Peter A. Singer, M.D. Professor and Chief Clinical Endocrinology University
Invited Commentary. From: Jill E. Langer, MD Department of Radiology, University of Pennsylvania Medical Center Philadelphia, Pennsylvania
 Note: This copy is for your personal non-commercial use only. To order presentation-ready copies for distribution to your colleagues or clients, contact us at www.rsna.org/rsnarights. RG f Volume 27 Number
Note: This copy is for your personal non-commercial use only. To order presentation-ready copies for distribution to your colleagues or clients, contact us at www.rsna.org/rsnarights. RG f Volume 27 Number
Shifting Paradigms and Debates in the Management of Well-differentiated Thyroid Cancer
 DEBATE WJOES Shifting Paradigms and Debates in the Management of Well-differentiated Thyroid Cancer Shifting Paradigms and Debates in the Management of Well-differentiated Thyroid Cancer Ashok R Shaha
DEBATE WJOES Shifting Paradigms and Debates in the Management of Well-differentiated Thyroid Cancer Shifting Paradigms and Debates in the Management of Well-differentiated Thyroid Cancer Ashok R Shaha
RESEARCH ARTICLE. Importance of Postoperative Stimulated Thyroglobulin Level at the Time of 131 I Ablation Therapy for Differentiated Thyroid Cancer
 RESEARCH ARTICLE Importance of Postoperative Stimulated Thyroglobulin Level at the Time of 131 I Ablation Therapy for Differentiated Thyroid Cancer Zekiye Hasbek 1 *, Bulent Turgut 1, Fatih Kilicli 2,
RESEARCH ARTICLE Importance of Postoperative Stimulated Thyroglobulin Level at the Time of 131 I Ablation Therapy for Differentiated Thyroid Cancer Zekiye Hasbek 1 *, Bulent Turgut 1, Fatih Kilicli 2,
American Thyroid Association Statement on Preoperative Imaging for Thyroid Cancer Surgery
 THYROID Volume X, Number X, 2014 ª Mary Ann Liebert, Inc., and the American Thyroid Association DOI: 10.1089/thy.2014.0096 STATEMENT American Thyroid Association Statement on Preoperative Imaging for Thyroid
THYROID Volume X, Number X, 2014 ª Mary Ann Liebert, Inc., and the American Thyroid Association DOI: 10.1089/thy.2014.0096 STATEMENT American Thyroid Association Statement on Preoperative Imaging for Thyroid
Thyroid Ultrasound for the Endocrine Surgeon: A Valuable Clinical Tool that Enhances Diagnostic and Therapeutic Outcomes
 Thyroid Ultrasound for the Endocrine Surgeon: A Valuable Clinical Tool that Enhances Diagnostic and Therapeutic Outcomes Allan Siperstein MD The Cleveland Clinic Audience Quiz Taken ultrasound course Perform
Thyroid Ultrasound for the Endocrine Surgeon: A Valuable Clinical Tool that Enhances Diagnostic and Therapeutic Outcomes Allan Siperstein MD The Cleveland Clinic Audience Quiz Taken ultrasound course Perform
Surgical Treatment for Papillary Thyroid Carcinoma in Japan: Differences from Other Countries
 REVIEW ARTICLE J Korean Thyroid Assoc Vol. 4, No. 2, November 2011 Surgical Treatment for Papillary Thyroid Carcinoma in Japan: Differences from Other Countries Yasuhiro Ito, MD and Akira Miyauchi, MD
REVIEW ARTICLE J Korean Thyroid Assoc Vol. 4, No. 2, November 2011 Surgical Treatment for Papillary Thyroid Carcinoma in Japan: Differences from Other Countries Yasuhiro Ito, MD and Akira Miyauchi, MD
Case Scenario #1 Larynx
 Case Scenario #1 Larynx 56 year old white female who presented with a 2 month history of hoarseness treated with antibiotics, but with no improvement. In the last 3 weeks, she has had a 15 lb weight loss,
Case Scenario #1 Larynx 56 year old white female who presented with a 2 month history of hoarseness treated with antibiotics, but with no improvement. In the last 3 weeks, she has had a 15 lb weight loss,