Evaluation Report Manitoba Youth Centre
|
|
|
- Junior Hodge
- 6 years ago
- Views:
Transcription
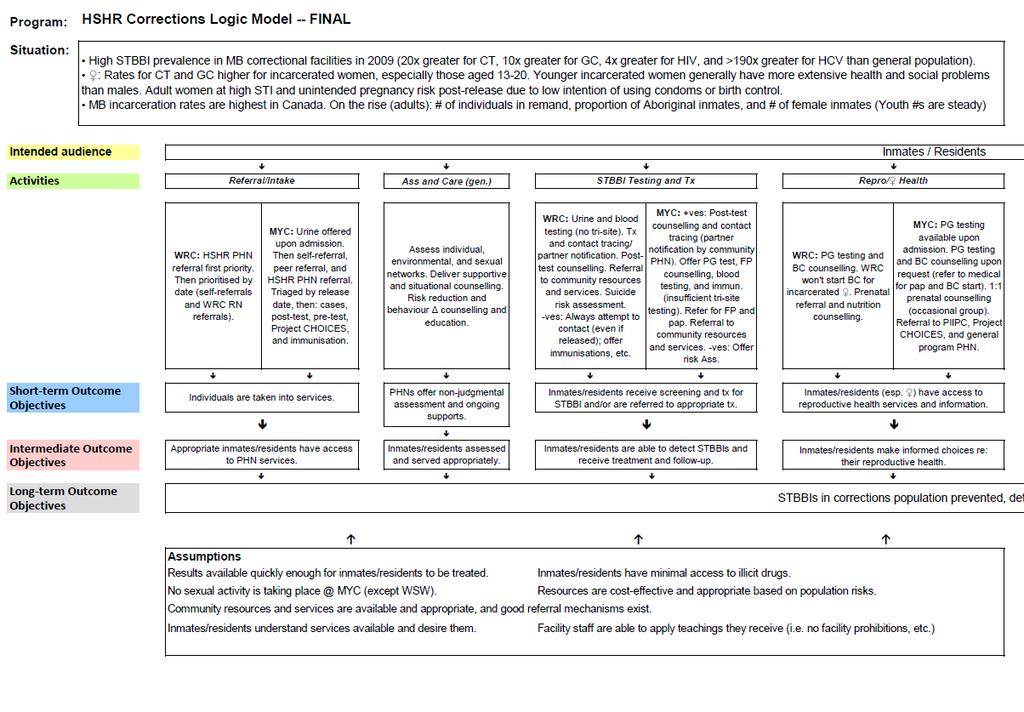
1 Evaluation Report Manitoba outh Centre Prepared for Winnipeg Regional Health Authority, Population and Public Health Program Healthy Sexuality and Harm Reduction Team Prepared by: Kellee Hodge, MPH Practicum Student Supervised by: Craig Ross, HSHR Program Specialist April 2014 Background and overview For approximately four years, Public Health Nurses (PHNs) from the Winnipeg Regional Health Authority s (WRHA) Health Sexuality and Harm Reduction (HSHR) team have been attending Winnipeg Remand Centre (WRC) and Manitoba outh Centre (MC) to provide sexually-transmitted and bloodborne infection (STBBI) prevention, screening, and care to those incarcerated there. The overall goal of these services is that STBBIs in [the] corrections population [are] prevented, detected and treated [and that g]eneral health and quality of life are promoted (Program Logic Model; Appendix A). STBBIs would be prevented through: Access to condoms, lube, sex dams, and safer drug use supplies (where permitted) Access to knowledge and information Appropriate vaccination STBBIs would be detected through: Appropriate access to testing Contact tracing and identification of cases STBBIs would be treated through: Delivering results and administering appropriate treatment and counselling to those infected Appropriate linkages to community care Process of evaluation planning The evaluation of HSHR s corrections services was structured according to the evaluation tool developed by the Towards Evidence-Informed Practice program of the Ontario Public Health Association (2009), hybridized with tools developed by the Winnipeg-based agency Health in Common. 1
2 The process included: August 2012: Meeting of HSHR staff: team manager, program specialist, communicable disease coordinator, and corrections PHNs. The purpose of this meeting was to select outside representatives for the evaluation team. The Director of Health Services for Manitoba Justice was asked and agreed to participate. A local epidemiologist with expertise in corrections was asked but unfortunately was not able to participate. November 2012: Evaluation team met to brainstorm content to populate the program logic model. February 2013: Program logic model was finalised (Appendix A) and draft evaluation questions were identified. May 2013: MPH student joined the HSHR team and assumed responsibility for the evaluation. An evaluation framework (with finalised questions and indicators) was drafted and circulated to the evaluation team via . June July 2013: Evaluation framework finalised (Appendix B). Data collection was undertaken. Analyses were performed and final report written. April 2014 Reports approved by HSHR leadership. Context: Role of the PHN at MC The PHN at MC attends two or three full days per week. She has an office in the building, though is unable to see clients there. She sees clients in a variety of locales: interview rooms, program rooms, the library, and the cottages. Upon intake at MC, all youth are offered urine screening for sexuallytransmitted infections (STIs) and pregnancy testing by the medical staff at MC. The PHN delivers urine testing results to residents if they are still incarcerated when the results come in, though treatment is usually administered by MC medical staff, due to high resident turnover (necessitating a quick response). The PHN does contact tracing, as well as pre- and post-test counselling for blood-borne pathogens (BBPs), though medical staff draws the blood for serology. 1 The PHN also administers vaccinations, counsels on family planning and prenatal issues, and delivers general counselling. The PHN also completes numerous referrals to medical care, Project CHOICES, the FASD program, community public health, and others. The PHN ideally wishes to deliver educational sessions to the youth, as well as to the Juvenile outh Counsellors (JCs), but does not currently feel that time allows for this. Process of evaluation All youth seen have their visits documented on the Sexually Transmitted & Blood Borne Infection Corrections form (Appendix C). Given the particular role of the PHN at MC (which differs greatly compared with WRC), the form is often filled with writing and documentation in the margins to capture data fields not included on the form. All forms are filed in a binder at MC, organised by year of visit. If a youth is released from the facility but later returns, their forms are stapled together and filed based on the year of the most recent visit. 1 Although not routinely offered by MC medical staff, throat and rectal swabbing is done by the PHN when indicated (currently infrequently). 2
 in the 2013 binder. The writer created a database in MS Excel.")
3 The writer attended MC to observe the function of the PHN and to pull data from the forms. The writer did not access corrections charts (i.e. maintained by MC staff). All forms filed in the 2012 binder were tabulated, as well as forms dating from 2012 but filed (as per above) in the 2013 binder. The writer created a database in MS Excel. Data from the forms were entered, sans identifiers, and then analysed using Epi Info 7. The writer was able to obtain documentation for 199 unique individuals seen by the PHN at MC between January 1 and December 31, Many of these youth were seen multiple times, for a total of approximately 700 visits. Findings Client Demographics Age outh seen had ages ranging from years old. 3


4 Sex 47% of those seen were male (n=94), 53 % female (n=105). Month of visit Month of visit varied greatly, from 10 visits in March to 30 in April, though it is important to note that many visits (e.g. administration of vaccine doses only) were not included in this evaluation (see footnote, p. 6). 4
. As above, this does not include visits not included in this evaluation. Demographics Miscellany Six (6) youth self-identified as injection drug users.")
5 Reason for Visit The most frequently reported reason for visit was related to STIs (50%), followed by vaccine initiation (25%), family planning (11%), provision of negative results (8%), other (4%), and prenatal issues (2%). As above, this does not include visits not included in this evaluation. Demographics Miscellany Six (6) youth self-identified as injection drug users. 2 All of these youth were female and between the ages of years old. No male youth identified as having sex with other men. Twenty-eight (28) female youth identified as having sex with other women. 3 Nineteen (19) youth self-identified as having ever traded sex for money, food, a place to stay, etc. 18 of these were female, and 1 male. They were all between the ages of years old. 2 Typical question phrasing: What drugs have you ever used?, and follow-up prompts. 3 Typical question phrasing: Do you have sex with men, women, or both? 5
 cases were in females, 34 were in males.")
6 STBBI Incidence 4 The PHN documented 208 urine STI test results. Sixty-three (63) youth tested positive for at least one STI. There were 56 cases of urogenital chlamydia identified, translating to a percent positive rate of 26.9%. Twenty-two (22) cases were in females, 34 were in males. There were 15 cases of urogenital gonorrhea identified, translating to a percent positive rate of 7.2%. Seven (7) cases were in females, 8 were in males. Two individuals had more than one urogenital gonorrhoea infection in In 8 instances, the youth was co-infected with both gonorrhea and chlamydia. Four (4) cases were female and 4 male. BBPs There were no cases of syphilis, hepatitis C, or HIV detected in Due to time restraints and limited access to off-site records, approximately 70 individuals charts were not reviewed due to their form containing only minimal information (for example, when the youth was incarcerated for such a brief period that they were not even seen by the PHN, etc.). In certain instances, these excluded forms may have contained (only) negative test results, which would not be factored into the denominator used to calculate the percent positive rates. The rates given therefore reflect the best estimate possible based on the information available, but should not be considered research-quality (for the purposes of comparison with studies, etc.). 6
7 Evaluation Questions Evaluation Question 1 Is the Public Health Nurse s role in corrections clear, and are the residents aware of services and how to access them? An evaluation framework to answer this question will be developed and implemented during the next evaluation period. The PHN offered some preliminary impressions: Indicator 1a Juvenile outh Counsellors (JCs) will be aware of the public health nurse s role and scope. The PHN feels that, due to high turnover of staff, there may be some JCs who are unaware of her role. Indicator 1b Residents are aware of how to access the PHN. The PHN feels that youth are aware of how to access her. Because she delivers results of STI tests, and all youth are offered STI testing on admission, the PHN sees a large number of the residents. Indicator 1c - Health services in correctional facilities refers residents appropriately. The PHN feels that referrals are appropriate. Evaluation Question 2 Are unvaccinated residents being vaccinated against STBBIs, and are they completing their series? Indicator 2a The PHN will assess residents immunization status. Currently, the PHN is unable to access the Manitoba Immunization Monitoring System (MIMS) records or echart Manitoba consistently within MC. The PHN can access a youth s immunization history documented in their corrections chart, but this is only pulled upon the youth s first intake into MC (for the purpose of accessing their Manitoba Health Personal Health Identification Number) and so is potentially out-of-date. When no history exists in the chart, the PHN requests MIMS report from the MC nursing staff. The PHN notes known vaccination history, documented immunity to hepatitis B, or point in vaccine schedule for all the youth she encounters. Due to the high number of youth that the PHN endeavours to complete vaccinations for, the process of obtaining MIMS/eChart was identified as arduous by the PHN. Additionally, the process of documentation in multiple places was deemed to occupy a large portion of time. Despite this, 100% of youth seen had their immunization status assessed (either through past documentation or MIMS) and documented. 7
8 Indicator 2b - Immunizations against STBBIs will be initiated when indicated. Prior to November 2012 most residents would not have been eligible for free vaccination with Gardasil. Regardless, 37 female youth were documented as having initiated Gardasil in 2012, representing 35% of female youth seen. With the expansion of criteria for free vaccination, the number of youth to whom Gardasil is offered will undoubtedly increase for 2013 and beyond. Eighty-nine percent (89%) of those eligible for and requiring hepatitis B immunization were documented as being offered the series. Recognising that an offer was likely made in all instances where possible, this may reflect a need for a revised form to facilitate documenting reason for no offer (e.g. youth was released before being seen, etc.) and refusals. Almost all individuals documented as being offered vaccination consented to initiate the series. In rare instances, when requested by the youth, the PHN will also obtain parental consent. Indicator 2c Residents who initiate immunization series for hepatitis B and HPV will complete their series. Although even a single vaccine dose offers some degree of protection, it is still noteworthy that 72% of those who initiated hepatitis B vaccination completed the series within one year (as per guidelines). 5 To compare, the rate of completion for Grade 4 students in Winnipeg was 59.2% for the 2011/12 school year (PPH 2012a). Seventy-nine percent (79%) of those who had Gardasil vaccination initiated completed their series within one year (as per guidelines). To compare, the rate of completion for Grade 6 girls in Winnipeg was 60.8% for the 2011/12 school year (PPH 2012b). Rates of completion are especially impressive in the context of youth being released and later reincarcerated, with the series generally not interrupted due to the strength of the documentation (tracking and reminder) infrastructure (see indicator 3a). Although the evaluation was not equipped to capture the amount of community-based (post-release) follow-up done by HSHR PHNs for series completion, it is almost certainly in excess of the 16% of youth who required community follow-up to receive serologic STBBI results (see indicator 4b), due to the fact that most vaccine series require 6 months to complete, as opposed to one-time sharing of results. 5 It should be noted that, for hepatitis B vaccination but not Gardasil the 2 nd and 3 rd injections are done by MC nursing staff (i.e. after the series is initiated by the PHN). 8

9 Question 3 - Are those at risk of STBBIs being offered testing and receiving their results? Indicator 3a- Residents requesting PHN services will be seen by the PHN prior to release. There were 21 residents documented as released prior to being seen by the PHN. The PHN currently has a system whereby residents who request to be seen (or are due to be seen for vaccination, etc.) have flags placed in their corrections charts, so MC nursing staff will alert the PHN should the youth return to the facility. Indicator 3b Rates/100,000 of positive tests will be similar to, or in excess of Manitoba rates. This indicator is not necessarily as relevant at MC (compared to WRC), as the PHN does not perform actual STI testing. STI testing, and often treatment, is done by the correctional nurses. However, it is worth noting again the striking STI incidence among youth at MC, reinforcing the extent to which this is a priority population for public health. Of those seen by the PHN with documented urine testing completed by correctional staff, 27% tested positive for chlamydia, and 7.2% tested positive for gonorrhea. * (Bullard, 2013) 9
10 Indicator 3c Rates of BBP testing will be at an acceptable percentage to STI testing, based on institutional context. Of the 210 visits related in some way to STI testing, in 174 (82.3%) instances the youth was documented as being offered BBP screening. 5 youth were documented to have recently completed BBP screening, with no new exposures, and 2 were advised that they were at very low risk for BBPs and were thus advised not to have screening done at that time. No rationale was documented for the remaining 29, though the likelihood is that the PHN determined or the youth expressed that BBP screening had occurred recently enough that a new test was not warranted. A revised documentation form would facilitate the documentation of this fact. Indicator 3d All positive cases of STBBIs will be notified of their results. Due to urine STI testing being offered upon intake at MC, 99% of positive cases of STIs were documented as having been notified of their results by either the PHN or MC nurses. One individual was not documented as having been confirmed treated, though documentation suggested that the youth was referred and followed up by public health outside of MC. On the other hand, serologic testing (for HIV, hepatitis, and syphilis) is done only after meeting with the PHN and receiving pre-test counselling, with the turn-around time for results closer to 7 days. As such, 16% of youth were released or transferred to another institution prior to receiving these results at MC. The responsibility of contacting these youth would fall to HSHR community PHNs, despite an absence of dedicated resources for this. Question 4 Are individuals being linked appropriately to continuing care in the community? Indicator 4a Evidence-based guidelines are in place to guide the PHN s follow-up in the community. Although less relevant at MC (due to the fact that the PHN does not perform actual STBBI testing), it is worth noting that no HSHR guidelines exist specific to corrections nursing. When developed, these should include community follow-up (to deliver results, etc., particularly in the context of negative results at WRC), but indicating where they may or may not be relevant to the MC role. Indicator 4b All positive cases of STBBIs will be notified of their results. 99% of positive cases of STIs were documented as having been notified of their results by either the PHN or MC nurses. (See indicator 3d). 10
11 Indicator 4c Residents who initiate immunization series for hepatitis B and HPV will complete their series. Seventy-two percent (72%) of those who initiated hepatitis B vaccination completed the series within one year (as per guidelines). Seventy-nine percent (79%) of those who had Gardasil vaccination initiated completed their series within one year (as per guidelines). Question 5 Are those found to have an STBBI treated appropriately and have follow-up interviews and testing completed as per protocols? 5a - All positive cases of STBBIs will be notified of their results. 99% of positive cases of STIs were documented as having been notified of their results by either the PHN or MC nurses. (See indicator 3d) 5b - All positive STI cases will be treated per guidelines. 100% of STI cases were treated per the Canadian Sexually Transmitted Disease Guidelines (PHAC, 2006). The Canadian Guidelines recommend that all those found to be infected with gonorrhea unlike with chlamydia positives undergo screening for HIV and syphilis, as well as immunization against hepatitis B. Three (3) of 15 individuals who were gonorrhea positive did not have documented offering of serology for HIV or syphilis. Upon review of these individuals HSHR/WRHA health records, one was to be imminently released (i.e. before being able to meet with the PHN), one had already been given a requisition for serologic testing from their primary care provider, and the third had undergone serologic testing only two months prior. A revised Corrections form would facilitate the documentation of offer/reason for no offer/refusal of BBP screening (see also indicator 3c). Two (2) of 15 individuals who were gonorrhea positive did not have documented confirmation of immunity or offering of vaccination. A revised Corrections form would facilitate the documentation of offer/reason for no offer/refusal of vaccination (see also indicator 2b). 5c - All positive HIV and hepatitis C cases will be linked to medical care. There were no new identified cases of HIV and hepatitis C in 2012 at MC. In the event of a confirmed new case, HSHR clinical practice guidelines exist that would dictate appropriate follow-up. 11
12 Recommendations Precise recommendations will be developed through discussion with the evaluation team. The writer recommends that the following represent the most salient findings of the evaluation: General Develop separate evidence-based guidelines for each corrections site (i.e. MC and WRC) to ensure consistency and sustainability. These would include: o if/how to notify released clients of negative results, o if/how to follow up with released clients eligible for vaccination and/or in the process of completing a series, and o consistent documentation processes, as facilitated by improved forms. The need for additional or dedicated resources must be considered in the context of the processes developed as per above. Develop a new Sexually Transmitted & Blood Borne Infection Corrections form specific to MC, in collaboration with the PHN and based on an established model, that better meets program needs. Develop strategies, in collaboration with the PHN and Manitoba Justice, to reduce the amount of duplicate charting required. Although the youth population at MC is largely male, young women comprised the majority of clients accessing PHN services. Strategies to engage with male youth should be considered. The evaluation team should continue to meet regularly for the purposes of continual quality improvement. Related to vaccination Continue very impressive assessment, offering, and completion of vaccinations. The PHN should have prompt, easy access to MIMS/eChart in order to efficiently assess residents vaccination status. Ensure that new/revised form facilitates documentation of assessment of confirmed immunity/previous completion of series for hepatitis vaccination. Related to STIBBI testing, and treatment Continue exemplary offering of BBP screening. Ensure that new/revised form facilitates documentation of offering of BBP screening and/or reason for no offer. 12
13 Works Cited Bullard, J. (2013). An STBBI Testing Update and the Quest for the 300. Winnipeg: Presentation to the WRHA 'Sex Matters' Conference. National Advisory Committee on Immunization (2012). Canadian Immunization Guide, Part 4, Active Vaccines, Hepatitis B Vaccine. Ottawa: Health Canada. PHAC (Public Health Agency of Canada) (2006). Canadian Guidelines on Sexually Transmitted Infections. Ottawa: Government of Canada. PPH (Population and Public Health program) (2012a). WRHA Grade 4 Hepatitis B Immunization Program: Public Health-Administered Vaccine by ear of Campaign. Winnipeg: WRHA. Unpublished. PPH (Population and Public Health program) (2012b). WRHA Grade 6 HPV Immunization Program: Public Health-Administered Vaccine by ear of Campaign. Winnipeg: WRHA. Unpublished. Towards Evidence-Informed Practice (2009). Towards Evidence-Informed Practice (TEIP) Tools. Toronto: Ontario Public Health Association. 13
14 Appendix A HSHR Corrections Logic Model FINAL March
15 Page 1 15
16 Page 2 16
17 Appendix B Evaluation Framework Indicator Review * Worksheet courtesy of Health In Common 17
18 Adequate Culturally appropriate Practical Useful Specific Direct Currently Feasible? N N? N N N /N /N /N Worksheet 4b. Indicator Review Question 1. Are the PHNs roles in corrections clear, and are inmates 6 aware of services and how to access them? Indicator(s) a. Correctional Officers 7 will be aware of the PHNs roles and scope. b. Inmates are aware of how to access PHNs. c. Health services in correctional facilities refers inmates appropriately. 2. Are unvaccinated inmates being vaccinated against STBBIs, and are they completing their series? a. PHNs will assess inmates immunization status. b. Immunizations against STBBIs will be initiated when indicated. c. Inmates who initiate immunization series for hepatitis B and HPV will complete their series. 6 Incarcerated youth at MC are generally referred to as residents ; therefore, that language is substituted for inmates throughout the MC evaluation report. 7 Likewise, frontline staff at MC are generally referred to as Juvenile outh Counsellors (JCs); therefore, that language is substituted for Correctional Officers throughout the MC evaluation report. 18
19 ??? /N /N 3. Are those at risk of STBBIs being offered testing and receiving their results? a. Inmates requesting PHN services will be seen by PHNs prior to release. b. Rates/100,000 of positive tests will be similar to, or in excess of Manitoba rates. c. Rates of BBP testing will be at an acceptable percentage to STI testing, based on institutional context. d. All positive cases of STBBIs will be notified of their results. 4. Are individuals being linked appropriately to continuing care in the community? a. Evidence-based guidelines are in place to guide PHNs follow-up in the community. b. All positive cases of STBBIs will be notified of their results. c. Inmates who initiate immunization series for hepatitis B and HPV will complete their series. 5. Are those found to have an STBBI treated appropriately and have follow-up interviews and testing completed as per protocols? a. All positive cases of STBBIs will be notified of their results. b. All positive STI cases will be treated per guidelines. c. All positive HIV and hepatitis C cases will be linked to medical care. 19
20 Appendix C Sexually Transmitted & Blood-Borne Infection Corrections Form 20
21 CLIENT SURNAME GIVEN NAME DATE OF BIRTH MFRN PHIN Manitoba Corrections STI/BBP Counselling Alternate LocatingInformation Alias Risk Assessment: Contact for: Date of Last Sexual Exposure: Last Test: Number sexual contacts in last year: Sex with: Men Women Both Number of lifetime partners: Condom use: always most of the time some of the time never Age of Sexual Debut: Hx of Previous STI Sex Trade Worker/ Sex with Hx of Sexual Assault Sex Outside Manitoba Tattoo/piercing/acupuncture Scarification/ needle stick Injection Drug Use Other Substance Use Gang Involved/ Sex With Street Involved Recent Immigrant/ Sex With Fights Pregnant Birth Control Last Pap Test Self/ Partner Clinical: Symptoms Prevention Education: Condoms Oral barriers Chlamydia Gonorrhea Syphilis HIV HPV Herpes HBV HCV Trichomonas Transmission Incubation Period Complications Signs & symptoms Risk to newborn Testing Progress Notes: BBP Pre-test Counselling: Discuss transmission modes, signs & symptoms, prognosis, care, & treatment. Discuss harm reduction & prevention strategies. Discuss that a positive test means there is a presence of antibodies within 3 to 6 months. Discuss that a negative test means no antibodies were detected, meaning the person can be in the window period or the person is not affected. Discuss the confidentiality of the tests, provincial reporting requirements and partner notification. Discuss social supports and the stress related to waiting for test results and possible reactions to learning results. Discuss by whom and how test results will be communicated to offender. Gender: M h F h ERD/ Court Date: Obtain offender s consent for testing. [ GC CT VDRL HIV ANTI - HAV HBV HCV Hbsag ] Completed (dd/mm/yy) Provider Signature and Professional Affiliation Initials of Provider 21
22 Testing/Treatment: Allergies: dd/mm/yy Test Requisition/Code Result Treatment / Follow-up Chlamydia Gonorrhea HbsAG Anti-HBs Anti-HCV Anti-HAV HIV VDRL Pregnancy Test Post Test Counselling: Results of tests explained to offender. Re-test recommended in months. Test of cure recommended: yes no When NSTD completed and interviewed for contacts. Viral Hepatitis Investigation Form completed and interviewed for contacts Notification of HIV Infection completed and interviewed for contacts Discussed legal obligation to notify all sexual partners of HIV + status (for HIV cases/contacts) Immunization offered. Accepted Refused Referral to Completed (dd/mm/yy) Provider Signature and Professional Affiliation Initials of Provider Progress Notes: Immunization: dd/mm/yy Vaccine Lot # Dose Route/Site Signature Antibody : dd/mm/yy Test Result Plans Legend ERD-Expected Date of Release, Ag- antigen, Anti- antibody detection,, VDRL- screen, TP-PA-T palladium particle agglutination,, T-throat, R - rectal/anal, U-urethra Organism: HAV hepatitis A virus, HBV hepatitis B virus, HCV hepatitis C virus, HIV human immunodeficiency virus 22
Evaluation Report Winnipeg Remand Centre
 Evaluation Report Winnipeg Remand Centre Prepared for Winnipeg Regional Health Authority, Population and Public Health Program Healthy Sexuality and Harm Reduction Team Prepared by: Kellee Hodge, MPH Practicum
Evaluation Report Winnipeg Remand Centre Prepared for Winnipeg Regional Health Authority, Population and Public Health Program Healthy Sexuality and Harm Reduction Team Prepared by: Kellee Hodge, MPH Practicum
Clinical Practice Guideline with Delegation of Function
 1 of 8 1.0 Purpose 1.1 To improve and focus efforts to treat those at risk for undiagnosed/untreated incubating, primary, secondary, or early latent infectious syphilis. 2.0 Scope and Goal 2.1 Antibiotic
1 of 8 1.0 Purpose 1.1 To improve and focus efforts to treat those at risk for undiagnosed/untreated incubating, primary, secondary, or early latent infectious syphilis. 2.0 Scope and Goal 2.1 Antibiotic
New Brunswick Report on Sexually Transmitted and Blood Borne Infections, 2016
 New Brunswick Report on Sexually Transmitted and Blood Borne Infections, 6 Table of Contents. Introduction.... Methodology... 3. Data Limitations.... Definitions used... 3 5. Overview of STBBI epidemiology
New Brunswick Report on Sexually Transmitted and Blood Borne Infections, 6 Table of Contents. Introduction.... Methodology... 3. Data Limitations.... Definitions used... 3 5. Overview of STBBI epidemiology
Practice Steps for Implementation of Guidelines Recommendations The guideline recommendations are shown schematically -
 ASK SCREEN Test for HIV and STI Practice Steps for Implementation of Guidelines Recommendations The guideline recommendations are shown schematically - Routinely obtain a thorough sexual history from all
ASK SCREEN Test for HIV and STI Practice Steps for Implementation of Guidelines Recommendations The guideline recommendations are shown schematically - Routinely obtain a thorough sexual history from all
An STBBI Testing Update and the Quest for the 300
 An STBBI Testing Update and the Quest for the 300 Jared Bullard MD FRCPC Paediatric Infectious Diseases & Medical Microbiology Associate Medical Director Cadham Provincial Laboratory WRHA STBBI Conference
An STBBI Testing Update and the Quest for the 300 Jared Bullard MD FRCPC Paediatric Infectious Diseases & Medical Microbiology Associate Medical Director Cadham Provincial Laboratory WRHA STBBI Conference
Descriptive Epidemiology of STBBIs in the Winnipeg Health Region
 Descriptive Epidemiology of STBBIs in the Winnipeg Health Region Pierre Plourde Souradet Shaw Debbie Nowicki Mandy Whitlock March 22, 211 Methods Case definitions and case reporting In Manitoba, all confirmed
Descriptive Epidemiology of STBBIs in the Winnipeg Health Region Pierre Plourde Souradet Shaw Debbie Nowicki Mandy Whitlock March 22, 211 Methods Case definitions and case reporting In Manitoba, all confirmed
Clinical Practice Guideline
 1 of 10 1.0 Purpose 1.1 To improve and focus efforts to respond to clusters and outbreaks of infectious syphilis and reduce transmission in the Winnipeg Health Region by enhancing treatment options for
1 of 10 1.0 Purpose 1.1 To improve and focus efforts to respond to clusters and outbreaks of infectious syphilis and reduce transmission in the Winnipeg Health Region by enhancing treatment options for
Clinical Practice Guideline. APPROVED BY: Healthy Sexuality and Harm Reduction Working Group
 1 of 18 Purpose To ensure an appropriate and consistent approach to the public health management of HIV-positive clients who do not disclose their HIV status before engaging in activities that put others
1 of 18 Purpose To ensure an appropriate and consistent approach to the public health management of HIV-positive clients who do not disclose their HIV status before engaging in activities that put others
Survey questionnaire on STI. surveillance, care and prevention. in European countries SAMPLE APPENDIX
 European Surveillance of Sexually Transmitted Infections Survey questionnaire on STI surveillance, care and prevention in European countries APPENDIX Detailed questionnaire on clinician and laboratory
European Surveillance of Sexually Transmitted Infections Survey questionnaire on STI surveillance, care and prevention in European countries APPENDIX Detailed questionnaire on clinician and laboratory
Immunization of Adults in High Risk Populations. Carol A. Kurbis MD, CCFP, FRCPC WRHA Medical Officer of Health
 Immunization of Adults in High Risk Populations Carol A. Kurbis MD, CCFP, FRCPC WRHA Medical Officer of Health OBJECTIVES To review recommendations for immunization in adult populations, with a focus on
Immunization of Adults in High Risk Populations Carol A. Kurbis MD, CCFP, FRCPC WRHA Medical Officer of Health OBJECTIVES To review recommendations for immunization in adult populations, with a focus on
HIV Point of Care Testing in Manitoba Report
 CADHAM PROVINCIAL LABORATORY HIV Point of Care Testing in Manitoba Report 2016 to 2017 APRIL 2018 1 HIV POINT OF CARE TESTING IN MANITOBA REPORT, 2016 TO 2017 Report prepared by: Jared Bullard Cadham Provincial
CADHAM PROVINCIAL LABORATORY HIV Point of Care Testing in Manitoba Report 2016 to 2017 APRIL 2018 1 HIV POINT OF CARE TESTING IN MANITOBA REPORT, 2016 TO 2017 Report prepared by: Jared Bullard Cadham Provincial
IDU Outreach Project. Program Guidelines
 Ministry of Health and Long-Term Care Ministère de la Santé et des Soins de longue dureé Prepared by: AIDS Bureau Revision Date: April 2001 TABLE OF CONTENTS 1 Introduction...1 1.1 Program Goals... 2 1.2
Ministry of Health and Long-Term Care Ministère de la Santé et des Soins de longue dureé Prepared by: AIDS Bureau Revision Date: April 2001 TABLE OF CONTENTS 1 Introduction...1 1.1 Program Goals... 2 1.2
Gonorrhea, Chlamydia, and Syphilis in Alaska
 Department of Health and Social Services Division of Public Health Section of Epidemiology Karen Perdue, Commissioner Karen Pearson, Director John Middaugh, MD, Editor 361 C Street, Suite 54, P.O. Box
Department of Health and Social Services Division of Public Health Section of Epidemiology Karen Perdue, Commissioner Karen Pearson, Director John Middaugh, MD, Editor 361 C Street, Suite 54, P.O. Box
ALASKA NATIVE MEDICAL CENTER SEXUALLY TRANSMITTED DISEASE SCREENING AND TREATMENT GUIDELINES
 ALASKA NATIVE MEDICAL CENTER SEXUALLY TRANSMITTED DISEASE SCREENING AND TREATMENT GUIDELINES A. Screening Page Chlamydia and Gonorrhea 1 HIV 1 Syphilis 1 Genital Herpes 2 Hepatitis A 2 Hepatitis B 2 Hepatitis
ALASKA NATIVE MEDICAL CENTER SEXUALLY TRANSMITTED DISEASE SCREENING AND TREATMENT GUIDELINES A. Screening Page Chlamydia and Gonorrhea 1 HIV 1 Syphilis 1 Genital Herpes 2 Hepatitis A 2 Hepatitis B 2 Hepatitis
Infectious and Communicable Diseases Prevention and Control Program Annual Service Plan A. Community Need and Priorities We are situated rurally with
 Infectious and Communicable Diseases Prevention and Control Program Annual Service Plan A. Community Need and Priorities We are situated rurally with no access to walk in clinics and access to health care
Infectious and Communicable Diseases Prevention and Control Program Annual Service Plan A. Community Need and Priorities We are situated rurally with no access to walk in clinics and access to health care
Guidelines for Implementing Pre-Exposure Prophylaxis For The Prevention of HIV in Youth Peter Havens, MD MS Draft:
 Guidelines for Implementing Pre-Exposure Prophylaxis For The Prevention of HIV in Youth Peter Havens, MD MS Draft: 10-2-2015 Clinical studies demonstrate that when a person without HIV infection takes
Guidelines for Implementing Pre-Exposure Prophylaxis For The Prevention of HIV in Youth Peter Havens, MD MS Draft: 10-2-2015 Clinical studies demonstrate that when a person without HIV infection takes
As a result of this training, participants will be able to:
 Addressing Sexual Risk with Drug Users and their Partners 1 Day Training This one-day training will build participant knowledge and skills in offering sexual harm reduction options to substance users.
Addressing Sexual Risk with Drug Users and their Partners 1 Day Training This one-day training will build participant knowledge and skills in offering sexual harm reduction options to substance users.
Toronto Declaration: Strategies to control and eliminate viral hepatitis globally. A call for coordinated action
 Toronto Declaration: Strategies to control and eliminate viral hepatitis globally A call for coordinated action Hepatitis B National Action Plan All countries should develop a national and/or regional
Toronto Declaration: Strategies to control and eliminate viral hepatitis globally A call for coordinated action Hepatitis B National Action Plan All countries should develop a national and/or regional
Chapter 5 Serology Testing
 Chapter 5 Serology Testing 49 50 This page intentionally left blank. Diagnostic Tests for Hepatitis B Virus (HBV) Diagnosis of HBV infection (acute vs. chronic) is based on clinical, laboratory, and epidemiologic
Chapter 5 Serology Testing 49 50 This page intentionally left blank. Diagnostic Tests for Hepatitis B Virus (HBV) Diagnosis of HBV infection (acute vs. chronic) is based on clinical, laboratory, and epidemiologic
iphis Case ID #: Reported Date: Reporting Source: Diagnosing Health Unit: Branch Office: Outbreak Number:
 Case Investigation Form: Hepatitis C Legend iphis system mandatory Required Case Information (add dates as YYYY-MM-DD) Case s Last Name: Case s First Name: Middle Name: Birth Date: Male Gender: Female
Case Investigation Form: Hepatitis C Legend iphis system mandatory Required Case Information (add dates as YYYY-MM-DD) Case s Last Name: Case s First Name: Middle Name: Birth Date: Male Gender: Female
Manitoba Health Statistical Update on HIV/AIDS
 Manitoba Health Statistical Update on HIV/AIDS 1985-2002 Communicable Disease Control Unit Public Health MANITOBA HEALTH STATISTICAL UPDATE ON HIV/AIDS 1985 TO December 2002 HIV January 1, 1985 to December
Manitoba Health Statistical Update on HIV/AIDS 1985-2002 Communicable Disease Control Unit Public Health MANITOBA HEALTH STATISTICAL UPDATE ON HIV/AIDS 1985 TO December 2002 HIV January 1, 1985 to December
Provincial Infectious Diseases Advisory Committee Public Health Response to Hepatitis C
 Provincial Infectious Diseases Advisory Committee Public Health Response to Hepatitis C Dr. Doug Sider, Medical Director, Public Health Ontario Dr. Peggy Millson, Professor Emeritus, Dalla Lana School
Provincial Infectious Diseases Advisory Committee Public Health Response to Hepatitis C Dr. Doug Sider, Medical Director, Public Health Ontario Dr. Peggy Millson, Professor Emeritus, Dalla Lana School
As a result of this training, participants will be able to:
 Addressing Prevention with HIV Positive Clients 1 Day Training This one-day training will prepare participants to help people living with HIV to avoid sexual and substance use behaviors that can result
Addressing Prevention with HIV Positive Clients 1 Day Training This one-day training will prepare participants to help people living with HIV to avoid sexual and substance use behaviors that can result
Note: Staff who work in case management programs should attend the AIDS Institute training, "Addressing Prevention in HIV Case Management.
 Addressing Prevention with HIV Positive Clients This one-day training will prepare participants to help people living with HIV to avoid sexual and substance use behaviors that can result in transmitting
Addressing Prevention with HIV Positive Clients This one-day training will prepare participants to help people living with HIV to avoid sexual and substance use behaviors that can result in transmitting
FY 2018 PERFORMANCE PLAN. Public Health/ CHSB
 Sexually Transmitted Infections Clinic Public Health/ CHSB Lilibeth Grandas x1211 Sharron Martin x1239 Program Purpose Program Information Reduce and prevent the incidence of sexually transmitted infections
Sexually Transmitted Infections Clinic Public Health/ CHSB Lilibeth Grandas x1211 Sharron Martin x1239 Program Purpose Program Information Reduce and prevent the incidence of sexually transmitted infections
Annual Statistical Update on HIV and AIDS 2013
 Annual Statistical Update on HIV and AIDS 2013 Data reported to December 31, 2013 Epidemiology & Surveillance Public Health Branch Public Health and Primary Health Care Division Manitoba Health, Healthy
Annual Statistical Update on HIV and AIDS 2013 Data reported to December 31, 2013 Epidemiology & Surveillance Public Health Branch Public Health and Primary Health Care Division Manitoba Health, Healthy
Hepatitis Case Investigation
 * indicates required fields Does patient also have: Hepatitis Case Investigation West Virginia Electronic Disease Surveillance System Division of Surveillance and Disease Control Infectious Disease Epidemiology
* indicates required fields Does patient also have: Hepatitis Case Investigation West Virginia Electronic Disease Surveillance System Division of Surveillance and Disease Control Infectious Disease Epidemiology
Manitoba Health Statistical Update on HIV/AIDS
 Manitoba Health Statistical Update on HIV/AIDS 1985 - Dec 2001 Communicable Disease Control Unit Public Health Branch MANITOBA HEALTH STATISTICAL UPDATE ON HIV/AIDS 1985 TO DECEMBER 2001 HIV January 1,
Manitoba Health Statistical Update on HIV/AIDS 1985 - Dec 2001 Communicable Disease Control Unit Public Health Branch MANITOBA HEALTH STATISTICAL UPDATE ON HIV/AIDS 1985 TO DECEMBER 2001 HIV January 1,
STI & HIV PRE-TEST ANSWER KEY
 Name: STI & HIV PRE-TEST ANSWER KEY 1. You can catch a STI or HIV from door knobs, toilet seats, or FALSE drinking fountains. STIs are transmitted sexually, requiring sexual contact. Some STIs can be transmitted
Name: STI & HIV PRE-TEST ANSWER KEY 1. You can catch a STI or HIV from door knobs, toilet seats, or FALSE drinking fountains. STIs are transmitted sexually, requiring sexual contact. Some STIs can be transmitted
Responsibilities in a sexual relationship - Contact tracing
 P a g e 1 Responsibilities in a sexual relationship - Contact tracing This activity has been designed increase student familiarity with the NSW Health Play Safe website. Suggested duration: 50-60 minutes
P a g e 1 Responsibilities in a sexual relationship - Contact tracing This activity has been designed increase student familiarity with the NSW Health Play Safe website. Suggested duration: 50-60 minutes
What You Need to Know. Sexually Transmitted Infections (STIs)
") What You Need to Know Sexually Transmitted Infections (STIs) What You Need to Know About STIs What are STIs? Sexually transmitted infections (STIs) are diseases that spread through sexual contact. If you
What You Need to Know Sexually Transmitted Infections (STIs) What You Need to Know About STIs What are STIs? Sexually transmitted infections (STIs) are diseases that spread through sexual contact. If you
The HIV testing process
 FACTSHEET The HIV testing process Summary There are a few steps that a person will take in the HIV testing process. To access an HIV test, people can request a test or may be offered a test. There are
FACTSHEET The HIV testing process Summary There are a few steps that a person will take in the HIV testing process. To access an HIV test, people can request a test or may be offered a test. There are
The objectives of this presentation are; to increase awareness of the issue of antimicrobial resistant gonorrhea, and to inform primary care and
 1 Antimicrobial resistant gonorrhea is an emerging public health threat that needs to be addressed. Neisseria gonorrhoeae is able to develop resistance to antimicrobials quickly. Effective antibiotic stewardship
1 Antimicrobial resistant gonorrhea is an emerging public health threat that needs to be addressed. Neisseria gonorrhoeae is able to develop resistance to antimicrobials quickly. Effective antibiotic stewardship
MANITOBA HIV REPORT 2015
 MANITOBA HIV REPORT 2015 The Manitoba HIV Program provides information, specialized care, treatment, and support to approximately 1,250 people living with HIV across the province. The Program has two Winnipeg-based
MANITOBA HIV REPORT 2015 The Manitoba HIV Program provides information, specialized care, treatment, and support to approximately 1,250 people living with HIV across the province. The Program has two Winnipeg-based
Coding for Preventive Services A Guide for HIV Providers
 Coding for Preventive Services A Guide for HIV Providers Jessie Murphy, MPH and Michelle Cataldo, LCSW, April 2016 Implementation of the Patient Protection and Affordable Care Act and other regulatory
Coding for Preventive Services A Guide for HIV Providers Jessie Murphy, MPH and Michelle Cataldo, LCSW, April 2016 Implementation of the Patient Protection and Affordable Care Act and other regulatory
HIV Partner Services in HIV Care Programs
 Welcome HIV Partner Services in HIV Care Programs Building the Care Continuum: Comprehensive Approaches to HIV Care in California Manny Rios HIV Partner Services Specialist CDPH: Office of AIDS Brett AugsJoost
Welcome HIV Partner Services in HIV Care Programs Building the Care Continuum: Comprehensive Approaches to HIV Care in California Manny Rios HIV Partner Services Specialist CDPH: Office of AIDS Brett AugsJoost
Ask at Least Annually. Ask Older Adults. Have you been sexually active in the last year? Have you ever been sexually active?
 Essential Sexual Health Questions to Ask Adults Ask all of your adult patients the sexual health questions on this card. They will help you assess the patient s level of sexual risk and determine whether
Essential Sexual Health Questions to Ask Adults Ask all of your adult patients the sexual health questions on this card. They will help you assess the patient s level of sexual risk and determine whether
GLOBAL AIDS MONITORING REPORT
 KINGDOM OF SAUDI ARABIA MINISTRY OF HEALTH GLOBAL AIDS MONITORING REPORT COUNTRY PROGRESS REPORT 2017 KINGDOM OF SAUDI ARABIA Submission date: March 29, 2018 1 Overview The Global AIDS Monitoring 2017
KINGDOM OF SAUDI ARABIA MINISTRY OF HEALTH GLOBAL AIDS MONITORING REPORT COUNTRY PROGRESS REPORT 2017 KINGDOM OF SAUDI ARABIA Submission date: March 29, 2018 1 Overview The Global AIDS Monitoring 2017
HIV/AIDS. Saskatchewan. Saskatchewan Health Population Health Branch
 HIV/AIDS In Saskatchewan 26 Saskatchewan Health Population Health Branch HIV/AIDS in Saskatchewan to December 31, 26 This epidemiological report profiles HIV and AIDS in Saskatchewan from the commencement
HIV/AIDS In Saskatchewan 26 Saskatchewan Health Population Health Branch HIV/AIDS in Saskatchewan to December 31, 26 This epidemiological report profiles HIV and AIDS in Saskatchewan from the commencement
THE POWER OF UNDETECTABLE. What you need to know about HIV treatment as prevention
 THE POWER OF UNDETECTABLE What you need to know about HIV treatment as prevention CONTENTS 3 Treatment as prevention First, a few basics: What is an undetectable viral load? How do I know if I m undetectable?
THE POWER OF UNDETECTABLE What you need to know about HIV treatment as prevention CONTENTS 3 Treatment as prevention First, a few basics: What is an undetectable viral load? How do I know if I m undetectable?
Evidence Summary Title: Abstinence-plus HIV prevention programs in high-income countries: Evidence and implications for public health
 Date this evidence summary was written: January 2010 Evidence Summary Title: Abstinence-plus HIV prevention programs in high-income countries: Evidence and implications for public health Quality Assessment
Date this evidence summary was written: January 2010 Evidence Summary Title: Abstinence-plus HIV prevention programs in high-income countries: Evidence and implications for public health Quality Assessment
Item 4. Sexual Health and Blood Borne Virus Strategy Strategy for Sexual Health and Blood Borne Viruses. Background
 Item 4 Strategy for Sexual Health and Blood Borne Viruses Background 1. In August 2011 the Scottish Government launched a joint Sexual Health and Blood Borne Virus Framework. This brought four policy areas
Item 4 Strategy for Sexual Health and Blood Borne Viruses Background 1. In August 2011 the Scottish Government launched a joint Sexual Health and Blood Borne Virus Framework. This brought four policy areas
OB Provider Guide to Alaska s Perinatal Hepatitis B Prevention Program
 OB Provider Guide to Alaska s Perinatal Hepatitis B Prevention Program Dear Colleague, This letter is to introduce myself and explain the role I play with the Alaska Perinatal Hepatitis B Program. Alaska
OB Provider Guide to Alaska s Perinatal Hepatitis B Prevention Program Dear Colleague, This letter is to introduce myself and explain the role I play with the Alaska Perinatal Hepatitis B Program. Alaska
Today s Webinar will be approximately 1 hour long including breaks for Q and A one in the middle, and one at the end. In order to receive Continuing
 1 Today s Webinar will be approximately 1 hour long including breaks for Q and A one in the middle, and one at the end. In order to receive Continuing Nursing Education, participants must attend the entire
1 Today s Webinar will be approximately 1 hour long including breaks for Q and A one in the middle, and one at the end. In order to receive Continuing Nursing Education, participants must attend the entire
COMMUNICABLE DISEASE REPORT
 June 2011 Department of Health and Community Services Government of Newfoundland and Labrador COMMUNICABLE DISEASE REPORT Reporting Sexually Transmitted and Bloodborne Infections All laboratory-confirmed
June 2011 Department of Health and Community Services Government of Newfoundland and Labrador COMMUNICABLE DISEASE REPORT Reporting Sexually Transmitted and Bloodborne Infections All laboratory-confirmed
Sexually Transmitted & Blood-Borne Infections in LGL ( )
") Sexually Transmitted & Blood-Borne Infections in LGL (2006 2015) Some Highlights: Chlamydia, Hepatitis C and Gonorrhoea were the sexually transmitted infections with the highest incidences in LGL in 2015.
Sexually Transmitted & Blood-Borne Infections in LGL (2006 2015) Some Highlights: Chlamydia, Hepatitis C and Gonorrhoea were the sexually transmitted infections with the highest incidences in LGL in 2015.
QuADS Organisational Standards and Professional Competencies in needle exchange
 QuADS Organisational Standards and Professional Competencies in needle exchange N This briefing paper was funded by the Department of Health as part of their 'Making Harm Reduction Work' initiative. DrugScope/Department
QuADS Organisational Standards and Professional Competencies in needle exchange N This briefing paper was funded by the Department of Health as part of their 'Making Harm Reduction Work' initiative. DrugScope/Department
Microbes at Our Doorstep: Emerging issues in infection control and travel-related infections
 Microbes at Our Doorstep: Emerging issues in infection control and travel-related infections Peel November 2, 2016 Learning Objectives At the end of this session, participants will be able to: 1. Identify
Microbes at Our Doorstep: Emerging issues in infection control and travel-related infections Peel November 2, 2016 Learning Objectives At the end of this session, participants will be able to: 1. Identify
Appendix A: Disease-Specific Chapters
 Infectious Diseases Protocol Appendix A: Disease-Specific Chapters Chapter: Gonorrhoea Revised January 2014 Gonorrhoea Communicable Virulent Health Protection and Promotion Act, Section 1 (1) Health Protection
Infectious Diseases Protocol Appendix A: Disease-Specific Chapters Chapter: Gonorrhoea Revised January 2014 Gonorrhoea Communicable Virulent Health Protection and Promotion Act, Section 1 (1) Health Protection
Summary Report: Survey of Hepatitis C Virus counseling and testing services at HIV counseling and testing sites, and health service sites.
 Summary Report: Survey of Hepatitis C Virus counseling and testing services at HIV counseling and testing sites, and health service sites. Sharon Adler MD, MPH Tomás Aragón MD, MPH Preventive Medicine
Summary Report: Survey of Hepatitis C Virus counseling and testing services at HIV counseling and testing sites, and health service sites. Sharon Adler MD, MPH Tomás Aragón MD, MPH Preventive Medicine
Prevalence of Hepatitis B and C in an Urban General Medicine Practice
 Prevalence of Hepatitis B and C in an Urban General Medicine Practice Juliet Jacobsen A. Study Purpose and Rationale Hepatitis B and C are the major causes of acute and chronic hepatitis, cirrhosis and
Prevalence of Hepatitis B and C in an Urban General Medicine Practice Juliet Jacobsen A. Study Purpose and Rationale Hepatitis B and C are the major causes of acute and chronic hepatitis, cirrhosis and
HIV/AIDS Prevention, Treatment and Care among Injecting Drug Users and in Prisons
 HIV/AIDS Prevention, Treatment and Care among Injecting Drug Users and in Prisons Ministerial Meeting on Urgent response to the HIV/AIDS epidemics in the Commonwealth of Independent States Moscow, 31 March
HIV/AIDS Prevention, Treatment and Care among Injecting Drug Users and in Prisons Ministerial Meeting on Urgent response to the HIV/AIDS epidemics in the Commonwealth of Independent States Moscow, 31 March
Sexual Health Services (Emergency Hormonal Contraception, Chlamydia Screening, Condom Distribution & Pregnancy Testing) in Pharmacies.
 in Pharmacies.") Local Enhanced Service (LES) Specification for: Sexual Health Services (Emergency Hormonal Contraception, Chlamydia Screening, Condom Distribution & Pregnancy Testing) in Pharmacies. 1. Introduction 2.
Local Enhanced Service (LES) Specification for: Sexual Health Services (Emergency Hormonal Contraception, Chlamydia Screening, Condom Distribution & Pregnancy Testing) in Pharmacies. 1. Introduction 2.
Sexually Transmitted Infections. Naluce Manuela Morris, MPH, CHES
 Sexually Transmitted Infections Naluce Manuela Morris, MPH, CHES Handshake Activity Handshake Activity Mrs. or Mr. X Mrs. or Mr. Y Carry this glove but do not put it on Put this glove on before shaking
Sexually Transmitted Infections Naluce Manuela Morris, MPH, CHES Handshake Activity Handshake Activity Mrs. or Mr. X Mrs. or Mr. Y Carry this glove but do not put it on Put this glove on before shaking
Action Item for 2019 Review of Tool. Maintain (add include oral cavity) Maintain. Archive. Archive. 12 creatinine)
 Maintain. Archive. Archive. 12 creatinine)") NEWLY DIAGNOSED/ NEW TO CARE PROGRAM SITE: REVIEWER(S): REVIEW DATE: CORE SERVICES Outpatient/Ambulatory Health Services Tool - 2018 (OLD) SECTION 1: CHART REVIEW Review for newly diagnosed HIV patients
NEWLY DIAGNOSED/ NEW TO CARE PROGRAM SITE: REVIEWER(S): REVIEW DATE: CORE SERVICES Outpatient/Ambulatory Health Services Tool - 2018 (OLD) SECTION 1: CHART REVIEW Review for newly diagnosed HIV patients
IMPORTANT HEALTH INFORMATION
 IMPORTANT HEALTH INFORMATION SU-6523MI Page 1 of 8 Table of Contents Page What is an HIV test?..........................................1 Will the HIV test tell me if I have AIDS?............................1
IMPORTANT HEALTH INFORMATION SU-6523MI Page 1 of 8 Table of Contents Page What is an HIV test?..........................................1 Will the HIV test tell me if I have AIDS?............................1
Part 1: Introduction & Overview
 Part 1: Introduction & Overview We envision a collaborative, participative partnership around IDU that: Provides all relevant and interested stakeholders with a voice and role. Promotes awareness of the
Part 1: Introduction & Overview We envision a collaborative, participative partnership around IDU that: Provides all relevant and interested stakeholders with a voice and role. Promotes awareness of the
Annual Statistical Update: HIV and AIDS
 Annual Statistical Update: HIV and AIDS 2014 Data reported to December 31, 2014 Epidemiology & Surveillance Public Health Branch Public Health and Primary Health Care Division Manitoba Health, Healthy
Annual Statistical Update: HIV and AIDS 2014 Data reported to December 31, 2014 Epidemiology & Surveillance Public Health Branch Public Health and Primary Health Care Division Manitoba Health, Healthy
STI Prevention: Housekeeping and How We Use Public Health. M. Terry Hogan, MPH Johns Hopkins University
 This work is licensed under a Creative Commons Attribution-NonCommercial-ShareAlike License. Your use of this material constitutes acceptance of that license and the conditions of use of materials on this
This work is licensed under a Creative Commons Attribution-NonCommercial-ShareAlike License. Your use of this material constitutes acceptance of that license and the conditions of use of materials on this
All four components must be present, but Part A funds to be used for HIV testing only as necessary to supplement, not supplant, existing funding.
 EARLY INTERVENTION SERVICES I. DEFINITION OF SERVICE Support of Early Intervention Services (EIS) that include identification of individuals at points of entry and access to services and provision of:
EARLY INTERVENTION SERVICES I. DEFINITION OF SERVICE Support of Early Intervention Services (EIS) that include identification of individuals at points of entry and access to services and provision of:
Annual Statistical Update: HIV and AIDS
 Annual Statistical Update: HIV and AIDS 2015 Data reported to December 31, 2015 Epidemiology & Surveillance Public Health Branch Public Health and Primary Health Care Division Manitoba Health, Seniors
Annual Statistical Update: HIV and AIDS 2015 Data reported to December 31, 2015 Epidemiology & Surveillance Public Health Branch Public Health and Primary Health Care Division Manitoba Health, Seniors
CHAPTER 1: SEXUALLY TRANSMITTED AND BLOODBORNE INFECTIONS
 CHAPTER : SEXUALLY TRANSMITTED AND BLOODBORNE INFECTIONS Highlights In Peel, the incidence of Acquired Immunodeficiency Syndrome (AIDS) has remained low (. to. cases per,) since the introduction of the
CHAPTER : SEXUALLY TRANSMITTED AND BLOODBORNE INFECTIONS Highlights In Peel, the incidence of Acquired Immunodeficiency Syndrome (AIDS) has remained low (. to. cases per,) since the introduction of the
Authorization for vaccination
 FOR USE BY CLSC INFORMATION RELATING TO VACCINATION Free Vaccination programs File no FIRST dose in grade 4 elementary school CONTRAINDICATION TO VACCINATION (specify) You must fill out the vaccination
FOR USE BY CLSC INFORMATION RELATING TO VACCINATION Free Vaccination programs File no FIRST dose in grade 4 elementary school CONTRAINDICATION TO VACCINATION (specify) You must fill out the vaccination
Australian Research Centre in Sex, Health & Society. EMBARGOED until am 4/8/09 Secondary Students and Sexual Health 2008
 Australian Research Centre in Sex, Health & Society EMBARGOED until 10.30 am 4/8/09 Secondary Students and Sexual Health 2008 Melbourne, Australia Sample 2002 2008 Jurisdictions All All School sectors
Australian Research Centre in Sex, Health & Society EMBARGOED until 10.30 am 4/8/09 Secondary Students and Sexual Health 2008 Melbourne, Australia Sample 2002 2008 Jurisdictions All All School sectors
School Nursing and Health. Standard Precautions. (aka Universal Precautions)
") School Nursing and Health Standard Precautions (aka Universal Precautions) August 2016 1 Standard Precautions Occupational Safety and Health Administration Federal Law 29 CFR bloodborne Pathogens 1910.1030(g)(2)(i)
School Nursing and Health Standard Precautions (aka Universal Precautions) August 2016 1 Standard Precautions Occupational Safety and Health Administration Federal Law 29 CFR bloodborne Pathogens 1910.1030(g)(2)(i)
ANNOUNCEMENT. Navy and Marine Corps Public Health Center 1
 ANNOUNCEMENT Register for the Monthly Disease SurveillanceTrainings: Contact your Service surveillance hub Log-on or Request log-on ID/password: https://tiny.army.mil/r/zb8a/cme and Register for Epi-Tech
ANNOUNCEMENT Register for the Monthly Disease SurveillanceTrainings: Contact your Service surveillance hub Log-on or Request log-on ID/password: https://tiny.army.mil/r/zb8a/cme and Register for Epi-Tech
The new German strategy on HIV, Hepatitis B, C and STI, an integrated approach. Ines Perea Ministry of Health, Germany
 The new German strategy on HIV, Hepatitis B, C and STI, an integrated approach Ines Perea Ministry of Health, Germany Reasons for a new strategy in 2016 New international agreements (SDG s) Renewed political
The new German strategy on HIV, Hepatitis B, C and STI, an integrated approach Ines Perea Ministry of Health, Germany Reasons for a new strategy in 2016 New international agreements (SDG s) Renewed political
The Hepatitis C Action Plan for Scotland: Draft Guidelines for Hepatitis C Care Networks
 The Hepatitis C Action Plan for Scotland: Draft Guidelines for Hepatitis C Care Networks Royal College of Physicians of Edinburgh Friday 12 October 2007 CONTENTS 1.0 ACCOUNTABILITY AND ORGANISATION 2.0
The Hepatitis C Action Plan for Scotland: Draft Guidelines for Hepatitis C Care Networks Royal College of Physicians of Edinburgh Friday 12 October 2007 CONTENTS 1.0 ACCOUNTABILITY AND ORGANISATION 2.0
Time to Eliminate Hepatitis B John W. Ward, M.D. Division of Viral Hepatitis Centers for Disease Control and Prevention
 Time to Eliminate Hepatitis B John W. Ward, M.D. Division of Viral Hepatitis Centers for Disease Control and Prevention Division of Viral Hepatitis National Center for HIV/AIDS, Viral Hepatitis, STD, and
Time to Eliminate Hepatitis B John W. Ward, M.D. Division of Viral Hepatitis Centers for Disease Control and Prevention Division of Viral Hepatitis National Center for HIV/AIDS, Viral Hepatitis, STD, and
San Francisco Department of Public Health Program Collaboration and Service Integration Surveillance Baseline Assessment
 Background and Purpose San Francisco Department of Public Health This syndemics assessment is the first step in developing a sustainable system of primary prevention and clinical care in San Francisco
Background and Purpose San Francisco Department of Public Health This syndemics assessment is the first step in developing a sustainable system of primary prevention and clinical care in San Francisco
Technical Guidance Note for Global Fund HIV Proposals
 Technical Guidance Note for Global Fund HIV Proposals UNAIDS I World Health Organization I 2011 Rationale for including this activity in the proposal The World Health Organization (WHO), the Joint United
Technical Guidance Note for Global Fund HIV Proposals UNAIDS I World Health Organization I 2011 Rationale for including this activity in the proposal The World Health Organization (WHO), the Joint United
Ontario Harm Reduction Conference April 30 to May 2, 2017 Toronto, Ontario
 Ontario Harm Reduction Conference April 30 to May 2, 2017 Toronto, Ontario Views expressed in the attached document do not necessarily represent those of the Ministry of Health and Long Term Care or those
Ontario Harm Reduction Conference April 30 to May 2, 2017 Toronto, Ontario Views expressed in the attached document do not necessarily represent those of the Ministry of Health and Long Term Care or those
CALM LEARNER OUTCOMES 1 :
 CALM STI AND HIV LESSON 2 STI AND HIV Lesson 2 GRADE CALM LEARNER OUTCOMES 1 : Examine aspects of healthy sexuality, sexual wellness and responsible sexual behaviour. Describe sexually healthy choices
CALM STI AND HIV LESSON 2 STI AND HIV Lesson 2 GRADE CALM LEARNER OUTCOMES 1 : Examine aspects of healthy sexuality, sexual wellness and responsible sexual behaviour. Describe sexually healthy choices
COFM Immunization Policy 2016
 COFM Immunization Policy 2016 Council of Ontario Faculties of Medicine June 2016 COUNCIL OF ONTARIO FACULTIES OF MEDICINE An affiliate of the Council of Ontario Universities COFM Immunization Policy 2016
COFM Immunization Policy 2016 Council of Ontario Faculties of Medicine June 2016 COUNCIL OF ONTARIO FACULTIES OF MEDICINE An affiliate of the Council of Ontario Universities COFM Immunization Policy 2016
Reproductive and Sexual Health
 Reproductive and Sexual Health Webinar: Navy Preventive Medicine and Management of the STI Patient 27 April 2016 The views expressed in this briefing are those of the authors and do not necessarily reflect
Reproductive and Sexual Health Webinar: Navy Preventive Medicine and Management of the STI Patient 27 April 2016 The views expressed in this briefing are those of the authors and do not necessarily reflect
SUBJECT: Hepatitis C Virus (HCV) Counseling/Education, Testing, Referral, and Partner Notification
 Counseling/Education, Testing, Referral, and Partner Notification") SUBJECT: Hepatitis C Virus (HCV) Counseling/Education, Testing, Referral, and Partner Notification Hepatitis C virus (HCV) infection is the most common chronic bloodborne infection in the United States.
SUBJECT: Hepatitis C Virus (HCV) Counseling/Education, Testing, Referral, and Partner Notification Hepatitis C virus (HCV) infection is the most common chronic bloodborne infection in the United States.
Yakima Health District BULLETIN
 Yakima Health District BULLETIN Volume 12, Issue 4 December, 2013 Overview Prevention of Perinatal Hepatitis B Transmission Perinatal transmission of hepatitis B virus (HBV) is preventable through universal
Yakima Health District BULLETIN Volume 12, Issue 4 December, 2013 Overview Prevention of Perinatal Hepatitis B Transmission Perinatal transmission of hepatitis B virus (HBV) is preventable through universal
Syphilis Outbreak Investigation Report
 ` Office of the Chief Medical Officer of Health Syphilis Outbreak Investigation Report Office of the Chief Medical Officer of Health Health il 2014 Table of Contents Summary... 1 Acronyms... 1 Introduction...
` Office of the Chief Medical Officer of Health Syphilis Outbreak Investigation Report Office of the Chief Medical Officer of Health Health il 2014 Table of Contents Summary... 1 Acronyms... 1 Introduction...
Becoming a harm reduction distribution agency in Toronto - information session
 Becoming a harm reduction distribution agency in Toronto - information session Kris Guthrie, RN BScN Health Promotion Specialist, The Works Toronto Public Health May 2016 Overview Brief backgrounder Harm
Becoming a harm reduction distribution agency in Toronto - information session Kris Guthrie, RN BScN Health Promotion Specialist, The Works Toronto Public Health May 2016 Overview Brief backgrounder Harm
Outline. Successful Integration of Hepatitis Vaccination Services into Programs for High-Risk Adults An Update of State-Based Programs
 Successful Integration of Hepatitis Vaccination Services into Programs for High-Risk Adults An Update of State-Based Programs Joanna Buffington, MD, MPH Division of Viral Hepatitis National Immunization
Successful Integration of Hepatitis Vaccination Services into Programs for High-Risk Adults An Update of State-Based Programs Joanna Buffington, MD, MPH Division of Viral Hepatitis National Immunization
Consultation on the Draft National Strategies for Blood Borne Viruses and Sexually Transmissible Infections
 Consultation on the Draft National Strategies for Blood Borne Viruses and Sexually Transmissible Infections AFAO comments on draft Third National Sexually Transmissible Infections Strategy 2014 2017 AFAO
Consultation on the Draft National Strategies for Blood Borne Viruses and Sexually Transmissible Infections AFAO comments on draft Third National Sexually Transmissible Infections Strategy 2014 2017 AFAO
The epidemiology of hepatitis C in Canada
 The epidemiology of hepatitis C in Canada FACT SHEET Published 2017 This fact sheet provides a snapshot of the hepatitis C epidemic in Canada. It is one of a series of fact sheets providing epidemiological
The epidemiology of hepatitis C in Canada FACT SHEET Published 2017 This fact sheet provides a snapshot of the hepatitis C epidemic in Canada. It is one of a series of fact sheets providing epidemiological
ACKNOWLEDGEMENTS FOR FURTHER INFORMATION
 ACKNOWLEDGEMENTS This report details the descriptive epidemiology of chlamydia and gonorrhea in the Winnipeg Health Region. Special gratitude is extended to the following individuals: Communicable Disease
ACKNOWLEDGEMENTS This report details the descriptive epidemiology of chlamydia and gonorrhea in the Winnipeg Health Region. Special gratitude is extended to the following individuals: Communicable Disease
STI Prevention and Screening. Molly McHenry Fenway Health May 2016
 STI Prevention and Screening Molly McHenry Fenway Health May 2016 Presentation Overview CDC Surveillance data Risk Assessment Special Populations and Barriers to Care STI Prevention STI Screening Treatment
STI Prevention and Screening Molly McHenry Fenway Health May 2016 Presentation Overview CDC Surveillance data Risk Assessment Special Populations and Barriers to Care STI Prevention STI Screening Treatment
Annex A: Impact, Outcome and Coverage Indicators (including Glossary of Terms)
") IMPACT INDICATORS (INDICATORS PER GOAL) HIV/AIDS TUBERCULOSIS MALARIA Reduced HIV prevalence among sexually active population Reduced HIV prevalence in specific groups (sex workers, clients of sex workers,
IMPACT INDICATORS (INDICATORS PER GOAL) HIV/AIDS TUBERCULOSIS MALARIA Reduced HIV prevalence among sexually active population Reduced HIV prevalence in specific groups (sex workers, clients of sex workers,
Primary Care Services for blood borne viral hepatitis prevention, treatment and care
 Primary Care Services for blood borne viral hepatitis prevention, treatment and care Author: Josie Smith, Marion Lyons Page 1 of 13 October 2006 Status : Final Contents: Page: Executive Summary 3 Introduction
Primary Care Services for blood borne viral hepatitis prevention, treatment and care Author: Josie Smith, Marion Lyons Page 1 of 13 October 2006 Status : Final Contents: Page: Executive Summary 3 Introduction
HIV, HBV and HCV testing policy experiences and lessons learned.
 HIV, HBV and HCV testing policy experiences and lessons learned. Contents HIV and viral hepatitis: distinct epidemics at different stages of evolution Epidemiology: transmission, prevalence, incidence
HIV, HBV and HCV testing policy experiences and lessons learned. Contents HIV and viral hepatitis: distinct epidemics at different stages of evolution Epidemiology: transmission, prevalence, incidence
FAMILY LIFE Education. Fifth Grade Instructional lessons
 FAMILY LIFE Education Fifth Grade Instructional lessons As new and updated videos and instructional materials become available the Family Life Supervisor may include them where appropriate without altering
FAMILY LIFE Education Fifth Grade Instructional lessons As new and updated videos and instructional materials become available the Family Life Supervisor may include them where appropriate without altering
The Ethics of Notifiable STIs
 The Ethics of Notifiable STIs Does Public Health Trump Privacy? Temberly Mitchell Leigh E. Rich How far have we come? A brief history of reporting Getting tested today Ethical concerns Suggestions Outline
The Ethics of Notifiable STIs Does Public Health Trump Privacy? Temberly Mitchell Leigh E. Rich How far have we come? A brief history of reporting Getting tested today Ethical concerns Suggestions Outline
Version for the Silent Procedure 29 April Agenda item January Hepatitis
 Version for the Silent Procedure 29 April 2014 134th session EB134.R18 Agenda item 10.5 25 January 2014 Hepatitis The Executive Board, Having considered the report on hepatitis, 1 RECOMMENDS to the Sixty-seventh
Version for the Silent Procedure 29 April 2014 134th session EB134.R18 Agenda item 10.5 25 January 2014 Hepatitis The Executive Board, Having considered the report on hepatitis, 1 RECOMMENDS to the Sixty-seventh
Sexually Transmitted Infections. Kim Dawson October 2010
 Sexually Transmitted Infections Kim Dawson October 2010 Objectives: You will learn about: Sexually Transmitted Infections (STI s). How they are transferred. High risk behavior. The most common STI s. How
Sexually Transmitted Infections Kim Dawson October 2010 Objectives: You will learn about: Sexually Transmitted Infections (STI s). How they are transferred. High risk behavior. The most common STI s. How
Management of Needlestick and Mucous Membrane Exposures To Blood/Body Fluids
 Management of Needlestick and Mucous Membrane Exposures To Blood/Body Fluids August 2004 Table Of Contents Protocol - Management of Needlestick and Mucous Membrane Exposures to Blood/Body Fluids Assessment
Management of Needlestick and Mucous Membrane Exposures To Blood/Body Fluids August 2004 Table Of Contents Protocol - Management of Needlestick and Mucous Membrane Exposures to Blood/Body Fluids Assessment
Operational Guideline
 1 of 6 PURPOSE Prevention of the spread of sexually transmitted and blood-borne infections (STBBI) through distribution of harm reduction supplies SCOPE & GOAL Harm reduction supplies and condoms will
1 of 6 PURPOSE Prevention of the spread of sexually transmitted and blood-borne infections (STBBI) through distribution of harm reduction supplies SCOPE & GOAL Harm reduction supplies and condoms will
Cost-effectiveness of Hepatitis A and Hepatitis B Vaccination for Jail Inmates
 Yale University EliScholar A Digital Platform for Scholarly Publishing at Yale Yale Medicine Thesis Digital Library School of Medicine 2007 Cost-effectiveness of Hepatitis A and Hepatitis B Vaccination
Yale University EliScholar A Digital Platform for Scholarly Publishing at Yale Yale Medicine Thesis Digital Library School of Medicine 2007 Cost-effectiveness of Hepatitis A and Hepatitis B Vaccination
Fax completed form to: (204) Further inquiries: your CD Coordinator
 Further inquiries: your CD Coordinator") Population and Public Health Program Acute Hepatitis B Virus (HBV) Enhanced Surveillance Case Report Form Fax completed form to: (204) 940-2690 Further inquiries: your CD Coordinator PERSON REPORTING Last
Population and Public Health Program Acute Hepatitis B Virus (HBV) Enhanced Surveillance Case Report Form Fax completed form to: (204) 940-2690 Further inquiries: your CD Coordinator PERSON REPORTING Last
Welcome to 4 th Syphilis Report to the Community. May 18, 2016
 Welcome to 4 th Syphilis Report to the Community May 18, 2016 Syphilis and STDs in Bexar County Anil T. Mangla, MS, PhD, MPH, FRIPH Assistant Director of Health Syphilis Update to the Community May 18,
Welcome to 4 th Syphilis Report to the Community May 18, 2016 Syphilis and STDs in Bexar County Anil T. Mangla, MS, PhD, MPH, FRIPH Assistant Director of Health Syphilis Update to the Community May 18,
STIs and BBVs. The facts
 EASY ENGLISH STIs and BBVs Some people say sex germs The facts New words There may be words in this factsheet that are new to you and you may not know what they mean or you may be unsure what they mean.
EASY ENGLISH STIs and BBVs Some people say sex germs The facts New words There may be words in this factsheet that are new to you and you may not know what they mean or you may be unsure what they mean.
Primary Health Networks
 Primary Health Networks Drug and Alcohol Treatment Activity Work Plan 2016-17 to 2018-19 Hunter New England & Central Coast Please note: This Activity Work Plan was developed in response to the HNECC PHN
Primary Health Networks Drug and Alcohol Treatment Activity Work Plan 2016-17 to 2018-19 Hunter New England & Central Coast Please note: This Activity Work Plan was developed in response to the HNECC PHN
Sexually Transmitted Diseases This publication was made possible by Grant Number TP1AH from the Department of Health and Human Services,
 Sexually Transmitted Diseases This publication was made possible by Grant Number TP1AH000081-01-01 from the Department of Health and Human Services, Office of Adolescent Health; its contents are solely
Sexually Transmitted Diseases This publication was made possible by Grant Number TP1AH000081-01-01 from the Department of Health and Human Services, Office of Adolescent Health; its contents are solely
University Health Services at CMU STI Awareness Month specials for students:
 University Health Services at CMU STI Awareness Month specials for students: -Free condoms during April (10 per student) -Free walk-in rapid HIV testing April 22-27 (no appointment needed) -STI Screening
University Health Services at CMU STI Awareness Month specials for students: -Free condoms during April (10 per student) -Free walk-in rapid HIV testing April 22-27 (no appointment needed) -STI Screening