Evaluation Report Winnipeg Remand Centre
|
|
|
- Damon Wiggins
- 6 years ago
- Views:
Transcription
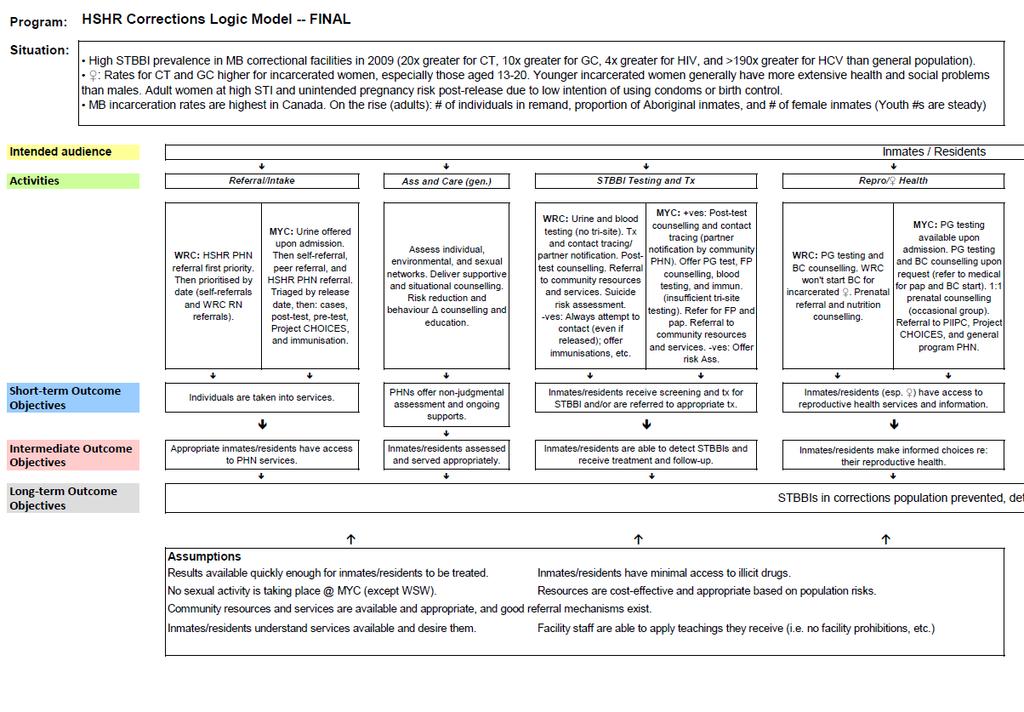
1 Evaluation Report Winnipeg Remand Centre Prepared for Winnipeg Regional Health Authority, Population and Public Health Program Healthy Sexuality and Harm Reduction Team Prepared by: Kellee Hodge, MPH Practicum Student Supervised by: Craig Ross, HSHR Program Specialist April 2014 Background and overview For approximately four years, Public Health Nurses (PHNs) from the Winnipeg Regional Health Authority s (WRHA) Health Sexuality and Harm Reduction (HSHR) team have been attending Winnipeg Remand Centre (WRC) and Manitoba outh Centre (MC) to provide sexually-transmitted and bloodborne infection (STBBI) prevention, screening, and care to those incarcerated there. The overall goal of these services is that STBBIs in [the] corrections population [are] prevented, detected and treated [and that] general health and quality of life are promoted (Program Logic Model; Appendix A). STBBIs would be prevented through: Access to condoms, lube, sex dams, and safer drug use supplies (where permitted) Access to knowledge and information Appropriate vaccination STBBIs would be detected through: Appropriate access to testing Contact tracing and identification of cases STBBIs would be treated through: Delivering results and administering appropriate treatment and counselling to those infected Appropriate linkages to community care Process of evaluation planning The evaluation of HSHR s corrections services was structured according to the evaluation tool developed by the Towards Evidence-Informed Practice program of the Ontario Public Health Association (2009), hybridized with tools developed by the Winnipeg-based agency Health in Common. 1
2 The process included: August 2012: Meeting of HSHR staff: team manager, program specialist, communicable disease coordinator, and corrections PHNs. The purpose of this meeting was to select outside representatives for the evaluation team. The Director of Health Services for Manitoba Justice was asked and agreed to participate. A local epidemiologist with expertise in corrections was asked but unfortunately was not able to participate. November 2012: Evaluation team met to brainstorm content to populate the program logic model. February 2013: Program logic model was finalised (Appendix A) and draft evaluation questions were identified. May 2013: MPH student joined the HSHR team and assumed responsibility for the evaluation. An evaluation framework (with finalised questions and indicators) was drafted and circulated to the evaluation team via . June July 2013: Evaluation framework finalised (Appendix B). Data collection was undertaken. Analyses were performed and final report written. April 2014 Reports approved by HSHR leadership. Context: Role of the PHN at WRC PHNs at WRC attend two full days a week. They are situated in the basement of the WRC, and inmates requiring services are brought down by Correctional Officers (COs). They are seen in a room with the door open, due to institutional guidelines. PHNs offer services related to the prevention, identification, and treatment of STBBIs, as well as serological and urine screening. Due to storage limitations, pharyngeal and rectal swabs are not available. The PHNs treat inmates who are symptomatic for gonorrhea and chlamydia, complete contact notification forms, and deliver results. They also provide condoms and lube to inmates, provide vaccinations, complete risk-reduction counselling, and facilitate referrals to public health in the community. Finally, PHNs are able to place resources in inmates storage, so it is available to them upon release. Inmates access PHNs in several ways. They are made aware of services by posters on the units and by word-of-mouth from other inmates. Inmates can fill out a form requesting services, or have a CO do this for them. The forms go to medical services at WRC, whose staff write the inmate name and DOB in the PHNs folders. The PHNs then obtain the inmates charts and have COs bring the inmates to the interview room. If the PHNs are seeking an inmate who has been named as a contact to an STBBI, they may also call the unit and ask for him/her to be brought down. Process of Evaluation PHNs currently document their visits on the standardised Sexually Transmitted & Blood Borne Infection Corrections form (Appendix C). The PHN will write open in the top corner of the form, which is then brought back to the HSHR office. Administrative staff enters the client information into the outreach 2
3 database and attach Manitoba Immunization Monitoring System (MIMS) records if requested. The forms are then returned to the PHNs to bring back to WRC. Subsequent results, vaccinations, etc. are then all documented on this form. Eventually, it is again transported back to the HSHR office to be marked as closed. Depending on both the presence of an STBBI and whether or not the client has an existing health record with HSHR, the documentation will be kept in a particular location: Client tests positive for an STBBI Client does not test positive for an STBBI Client has a previous health record with HSHR Form is filed in existing chart. Documentation in chart progress notes. An entry into the HSHR STI Database is created (indicated in a variety of ways as a WRC client). Form is filed in existing chart. No additional documentation occurs. No record in databases occurs. File may be located through the outreach database in HSHR, or the contacts database if the client was named a contact Client does not have a previous health record with HSHR HSHR chart is created and the form is filed there. Further documentation occurs in the chart. An entry into the HSHR STI Database is created (indicated in a variety of ways as a WRC client). Form is filed according to last name in a binder kept by HSHR admin staff. Client is completing his/her vaccine series Form is kept in an Immunizations binder until the series is completed (up to 6 months). Then filed based on STBBI positivity/ existence of HSHR health record. Additionally, the PHNs document all vaccine series, testing completed (including results), etc., into the charts maintained by corrections staff. 1 In certain instances (e.g. follow-up serology to assess titres, health information only, etc.), only the corrections chart is entered into, with no documentation on the HSHR form. Statistics and tracking are accomplished by two separate processes. First, the PHNs maintain a handwritten list of names on a Delegation of Function Tracking Log (Appendix D), organized by date seen, along with the particular testing and/or treatment that took place. Second, the PHNs also keep an anonymous list of clients seen and the reason for the visit, for the purpose of compiling statistics for Manitoba Justice. The multiple processes for both documentation and tracking were developed over time and serve to confound efforts to easily locate health records. For this reason, not all health records were found in time for inclusion in this report, as detailed below. 1 To avoid confusion, any reference to an inmate s chart or health record refers to the PHN/HSHR-maintained chart, unless the corrections chart (i.e. maintained by WRC medical staff) is explicitly referenced. 3
4 The writer began by creating a database in MS Excel with no fields for identifying information. The forms from the binder maintained by admin (for clients without a prior chart and with no diagnosed STBBI, as per above) were entered. All charts from clients listed in the HSHR STI database as WRC were then pulled and information from those forms was entered. Finally, cross-referencing was undertaken to seek out the remaining 150 inmates recorded in the daily tracking log but not found in the database or binder. Their charts were pulled and information entered from their forms. The student also elicited information from the PHNs directly, from policy and procedure manuals, from past available data, and from conversations with the HSHR communicable disease coordinator. Information was analysed using Epi Info 7. Number of records reviewed: The writer was able to obtain documentation for 380 unique individuals seen by the WRC PHNs between January 1 December 31, Taking into account charts that were not located (see below), the total number of individuals seen for testing is comparable to the PHNs own annual report for Of note, though, is that the number of infections detected during the year was greatly under-tracked in HSHR s Access database of STBBI-positive cases investigated by the team: PHNs detected almost double the infections originally reported, including one each of hepatitis C and HIV. This under-tracking may be attributable to inconsistencies in the entering of information into the database. 2 These data are also more in line with the records of Cadham Provincial Laboratory, the provincial agency that would have performed the actual analyses. PHNs 2012 stats report Evaluator chart review Evaluation + missing charts Cadham Provincial Laboratory records STI screening BBP Screening CT + GC + Hep C + Syphilis + HIV new 3 previously diagnosed but retested 0 1 previously known In the Doctor_Clinic field, Remand inmates may be indicated as WRC or Dr. Plourde (HSHR s Medical Officer of Health, whose name also appears next to cases generated in other outreach venues), or even Remand, etc. Without improvements in the consistency of these processes, only a chart audit reliably reports accurate numbers. 4
5 Number of visits recorded: 402 visits were documented and reviewed (representing the 380 individuals), from which are pulled the majority of data and analyses below. 57 instances of documentation (representing 46 individuals) were not located by the chart reviewer and therefore not included: Unable to locate chart Unable to locate documentation within chart STBBI testing Urine testing only Entry into Delegation of Function Tracking Log Test and Treat Test and treat (no BBP screening) Treatment for gc/ct (no testing) Hep Screen only HIV test only Total Total A subsequent investigation located the missing documentation in various locations, but after the evaluation analyses were completed. In order to facilitate future evaluations (and for general oversight), a process was implemented to assemble in one location copies of all documentation for clients seen at Remand (i.e. all categories contained within the table on p.3). This central repository will be managed by HSHR administrative staff. In addition to those missing, 270 individuals were documented as having at least two visits (mainly for testing, and then later to receive test results; these were considered together for the purposes of this evaluation). Taken all together (though excluding visits solely for vaccinations, pregnancy testing, health information, etc.), approximately 700 STBBI-related client visits occurred in 2012: i.e. 402 initial visits, 270 for follow-up/results, and 57 encounters whose nature is unknown due to the documentation not being found in time for inclusion. 5


6 Findings Client Demographics Age The Winnipeg Remand Centre being an adult detention facility, the age range of those seen was years old. The median age was 25 years old, indicating those seen tended generally to be younger. 75% of those seen were aged 30 years or younger. This was consistent across genders. Month of Contact The month of visit varied greatly, from 22 to 46 visits per month. 6
 self-identified as having used injection drugs, with a particularly high rate among women: 23 men (7.1%) and 15 women (19.7%). Injection drug-use was also more common among older inmates: 5.")
7 Sex 76 visits were from females, 326 from males. Demographics Miscellany Thirty-eight (38) inmates (9.45%) self-identified as having used injection drugs, with a particularly high rate among women: 23 men (7.1%) and 15 women (19.7%). Injection drug-use was also more common among older inmates: 5.5% of year-olds, versus 13.37% of those aged 25+. Eleven (11) men identified as having sex with other men (3.37%). 6 women identified as having sex with other women (7.89%). Thirty-three (33) inmates self-identified as ever having traded sex for money, food, a place to stay, etc. (8.21%). 21 of these were female (27.63%), and 12 men (3.68%). Again, this was slightly more common among those 25+ than those aged years: 10.89% versus 5.50%, respectively. 7
 individuals screened had no results documented. Chlamydia There were 55 cases of urogenital chlamydia identified.")
8 STBBI Incidence Three hundred and eighty (380) individuals had urine screening for chlamydia (CT) and gonorrhea (GC) completed and documented; 346 also underwent serologic BBP screening. Twenty-one (21) individuals screened had no results documented. Chlamydia There were 55 cases of urogenital chlamydia identified. Of inmates assessed by PHNs, this indicates a percent-positive rate of 14.5%. While 42 cases (76.3%) were in those aged 18 24, there were 13 cases (23.6%) in those aged 25 and older. Forty (40) cases were identified in men, making the prevalence for men 12.9%. 15 cases were identified in females, making the female prevalence 21.1% Gonorrhea There were 18 cases of urogenital gonorrhea identified. Of inmates assessed by PHNs, this indicates an infection rate of 4.7%. 12 of these were in people under the age of 25 (66%). Ten (10) cases were identified in men, making the prevalence of gonorrhea for men tested by PHNs 3.2%. 8 cases were identified in women, resulting in a female prevalence of 11.3%. Gonorrhea and co-infections Half of gonorrhea cases (n=9) were co-infected with another STBBI. 8 individuals co-infected with GC/CT were identified, as well as 1 individual with GC/HIV co-infection. 8
9 HIV There were two identified cases of HIV, both in women, one aged 26 and one aged 30. One case selfidentified as IDU. Neither self-identified as being involved presently or in the past with sex work. Both cases were co-infected with a bacterial urogenital sexually-transmitted infection (STI) in one case gonorrhea, in the other chlamydia. Hepatitis C Three incident cases of hepatitis C were identified. 3 additional antibody tests came back positive, but for clients who had been identified through PHN documentation as already knowing their Hep C + status. 9
10 Evaluation Questions Evaluation Question 1 Are the PHNs roles in corrections clear, and are inmates aware of services and how to access them? An evaluation framework to answer this question will be developed and implemented during the next evaluation period. The PHNs offered some preliminary impressions: Indicator 1a COs will be aware of the PHNs roles and scope. It is unclear if the COs are aware of the PHNs precise role. Indicator 1b Inmates are aware of how to access the PHNs. PHNs have posters up on each unit, and there are referrals attributed to word-of-mouth between inmates. Health Services at WRC will forward any STBBI-related issues to the PHNs. Overall, the PHNs feel that the inmates are aware of how to access them. Indicator 1c - Health services in correctional facilities refers inmates appropriately. The PHNs feel that they receive appropriate referrals. There is no current system to monitor inappropriate referrals, although the PHNs report not feeling that this is currently an issue of concern. Evaluation Question 2 Are unvaccinated inmates being vaccinated against STBBIs, and are they completing their series? The descriptions of processes in Evaluation Question 2 are occasionally written in past tense to acknowledge that they were recently changed. In early 2013 (i.e. after the evaluation period), the PHNs were able to secure support from medical assistants at WRC. Before this i.e. with limited admin capacity MIMS could not previously be accessed reliably (including during the evaluation period). This greatly impacted the efficiency of the PHNs process for managing vaccinations, for example due to the risk that an inmate would be released before his/her titre results came back, as explained below. Future evaluations will undoubtedly demonstrate improvements reflecting this corresponding improvement in support infrastructure. Indicator 2a - PHNs will assess inmates immunization status. During the evaluation period, PHNs generally assessed hepatitis B vaccination eligibility via serologic testing. If there was no documented history of hepatitis vaccination in the corrections chart, and hepatitis B antibody returned negative, the PHN would then offer vaccination. If the inmate was agreeable, the PHN would then return to the HSHR office to request a copy of the inmate s vaccination history (via MIMS/eChart) from HSHR admin staff. If the inmate was indeed eligible, the PHN would return to WRC and offer vaccination, assuming the inmate was still incarcerated there. 10
; therefore this is likely a gross underrepresentation of PHNs actual assessing of MIMS and/or")
11 Forty-four (44) inmates (11%) had a MIMS report attached to their chart. As previously discussed, though, PHNs have access to corrections charts (not included in this evaluation); therefore this is likely a gross underrepresentation of PHNs actual assessing of MIMS and/or vaccination history. Two hundred and forty (240) inmates had documented hepatitis B titres checked as a proxy for determining sufficient protection against hepatitis B. Of the 150 inmates who tested negative for hepatitis B antibody, 91 (60%) were documented as offered hepatitis B vaccination. Of these, 35 (38.5%) were found via MIMS to have actually previously been fully vaccinated against hepatitis B, but it is unknown if these individuals had ever previously demonstrated an adequate antibody response. Despite antibody testing being used to determine eligibility for hepatitis B vaccination, 59 inmates tested negative for hepatitis B antibody but were not documented as having subsequently been offered vaccination. Of these, 54 were found via MIMS to have no or sub-optimally documented hepatitis B vaccination. It is unknown if these individuals were not offered immunization due to leaving the institution before results became available, if vaccination was offered but undocumented, or if vaccination was not offered. It is noteworthy, though, that only 72.8% of inmates seen by PHNs in WRC were able to receive blood test results before being discharged or moved (see indicator 3d), potentially contributing to this phenomenon (no dedicated resources exist for following up inmates in the community for initiation of vaccine series alone). The group of inmates for whom no offer of vaccination was documented included inmates seemingly at highest risk: 46% of injection drug-users (IDUs) with no documented vaccination or immunity to hepatitis B were not offered vaccination. 11

12 21% of inmates who had traded sex for money (etc.) with no documented vaccination or immunity to hepatitis B were not offered vaccination. These findings overall suggest that relying solely on antibody titres to determine vaccine eligibility was evident to the PHNs as being both insufficient and inefficient, spurring the procedure change in Indicator 2b - Immunizations against STBBIs will be initiated when indicated. Prior to November 2012 most inmates would not have been eligible for free vaccination with Gardasil. HPV vaccination was therefore not assessed in this evaluation. One hundred and twenty-five (125) individuals were both eligible for hepatitis B immunization (no documented history of vaccination in Manitoba, nor serologic confirmation of hepatitis B antibodies) and did not expressly refuse the vaccine (there were 43 documented refusals). Seventeen (17) of these (13.6%) were released prior to initiation of series. Of the remaining 108 eligible inmates, 48 (44.4%) were offered and initiated hepatitis B vaccination. Sixty (60) of 108 (55.5%) were not documented as having been offered vaccination. This number is likely due to factors not documented (e.g. inmate s belief that they had been vaccinated in the past) and/or lack of timely access to documentation regarding vaccination history. Recognising that an offer was likely made in all instances where possible, and in light of the recentlyimproved processes, a revised form may facilitate documenting: that MIMS was checked for an inmate, that serology (to assess hepatitis B antibody) was declined, and reason that no offer of vaccination was made (e.g. inmate was released before being seen, etc.). 12
13 Indicator 2c Inmates who initiate immunization series for hepatitis B and HPV will complete their series. Forty-eight (48) individuals initiated hepatitis B vaccination series, though 1 individual refused to see the PHN for completion. Of the remaining 47, 24 (51%) completed their series within a year. The 23 inmates who did not were generally either released or transferred to other institutions. In 13 cases where inmates were released, PHNs made effort through letters, phone calls, or both to reach them for completion (in the absence of a guideline either mandating or discouraging this). In all 9 cases where inmates were transferred to another institution, faxes were sent to make the new institution aware of the inmate s need to complete the vaccination series. Only 1 individual had no documented reason for discontinuation. Question 3 - Are those at risk of STBBIs being offered testing and receiving their results? Indicator 3a- Inmates requesting PHN services will be seen by PHNs prior to release. Inmates who request services are seen as promptly as possible. Corrections staff may filter inmate requests, meaning that not all requests for services may reach the PHN. Requests that do reach the PHNs must be prioritised due to the volume of those requesting services being larger at times than available capacity. Confirmed cases and contacts are prioritized first. Those requesting services are then added to the queue based on date the services were requested. Those requiring immunization are seen based on the date they are due. Inmates who request services but who are not able to be seen before being released or transferred have their request slips archived at WRC for five to seven years. Those slips were not included in this evaluation, and their inclusion in future evaluations may be complicated by the fact that a) slips archived include all unmet requests for services, above and beyond HSHR PHN services, and b) the slips are maintained by and are the property of WRC. Despite no ability to assess the volume of unmet requests nor the characteristics of those not seen, consideration could be given to more explicit prioritisation criteria. An American article (Barry et al., 2007), for example, concluded that STI screening priority be given to (in order of importance): females in youth detention first, women aged 30 years in adult jail second, and men aged 25 years in adult jail third. 13

14 Indicator 3b Rates/100,000 of positive tests will be similar to, or in excess of Manitoba rates. Percent positive rates are presented below: PHNs at WRC Percent positives, all MB STBBI in Corrections study 2 Male Female Total Male Female Total Chlamydia 12.9% 21.1% 14.5% 6.4% 7.0% 0.0% 6.0% Gonorrhea 3.2% 11.3% 4.7% 1.3% 0.6% 1.9% 0.8% HIV 0.0% 2.6% 0.5% 0.2% 0.6% 1.9% 0.8% Hepatitis C 3 3.5% 3.4% 8.1% 5.6% 7.7% 1 (Bullard, 2013) 2 (Beaudoin, 2009) 3 For Hepatitis C only, the percent positive rate is taken from Cadham Provincial Laboratory s (CPL) records of WRC testing in Individuals previously diagnosed with hepatitis C would not necessarily have this information recorded in their HSHR chart. Indeed, only three (3) individuals in 2012 were documented as receiving a new hepatitis C diagnosis, but in fact CPL recorded 14 HCV+ test results. For the purposes of comparing prevalence, the CPL number is therefore used, recognising that this still remains a likely underestimation due to the fact that HCV+ individuals generally would not ask for HCV testing in the first place. Because no denominator information is available from CPL, the high estimate of BBP screening from p.4 (395) is used. For all other infections, rates are calculated based on the evaluation chart review. *Bullard, 2013 Twenty-two (22) clients (approximately 6%) who underwent testing had no results documented. 14
15 Indicator 3c Rates of BBP testing will be at an acceptable percentage to STI testing, based on institutional context. 93.0% of those seen by PHNs had documented BBP screening offered, and 92.5% of those offered BBP screening accepted it. Eleven (11) individuals had no documented offer of BBP screening, despite having been diagnosed with gonorrhea and/or chlamydia. This translates to 16.9% of inmates testing positive for an STI. Among those not diagnosed with an STI, only 2.5% had no documented offering of BBP screening. Inconsistencies in the current documentation do not currently allow for a definitive interpretation of these results. The revised form and/or guidelines should facilitate documenting both offers and refusals in order that these data may be interpreted, especially in light of much lower-than-expected prevalence of hepatitis C. For example, the cohort of STI-positive inmates may include many already aware of their hepatitis C+ status, in turn leading to a lower rate of serologic testing than their STI-negative peers. It is noteworthy, though, that the overall rate of urine-to-serology offering (93%) far exceeds the province-wide average for 2012 of 62.4% (see Bullard, 2013). Indicator 3d All positive cases of STBBIs will be notified of their results. Due to the transient nature of inmates in correctional facilities, many may not still be housed at WRC by the time results are received by the PHNs. 70.8% of inmates received their results from the PHN in-house following urine screening: 14 (of 55) individuals diagnosed with chlamydia had been released by the time results were available. 3 (of 18) individuals diagnosed with gonorrhea had been released by the time results were available. Despite this, 100% of these cases were followed-up by PHNs according to STI guidelines. Two cases (one gc/ct co-infected, and one CT mono-infected) required extensive follow-up by the PHNs in the community. 72.8% of inmates received their BBP screening results in-house following screening. Of the two HIV diagnoses, one was still incarcerated when the results became available, and one had been transferred to another facility. One new hepatitis C case remained in the facility when the results became available, one had been transferred, and one had been released. Of interest, around 30% of individuals who were released prior to receiving negative results received follow-up (phone call(s) and letter) to notify them to contact public health, whereas others did not. This practice seems to be inconsistent, but may be taking up considerable PHN time, likely necessitating a guideline. 15
16 Question 4 Are individuals being linked appropriately to continuing care in the community? Indicator 4a Evidence-based guidelines are in place to guide PHNs follow-up in the community. Currently, guidelines are in place governing STBBI testing done by all HSHR PHNs, via a Shared Competency (previously a Delegation of Function ) between the PHNs and the Medical Officer of Health (Appendix E). These guidelines mandate that PHNs make a plan with the client for the sharing of results. The HSHR communicable disease coordinator believes that the process for following up negative results is based primarily on the PHNs general practices and situational context. Importantly, there is no consistent guideline regarding if/how to notify incarcerated clients of negative results, especially considering a lack of dedicated PHN resources for community follow-up. Indicator 4b All positive cases of STBBIs will be notified of their results. 100% of positive cases were notified of their results. 70.8% of inmates received their results from the PHN in-house following urine screening. 72.8% of inmates received their BBP screening results in-house following screening. (See indicator 3d) Indicator 4c Inmates who initiate immunization series for hepatitis B and HPV will complete their series. Forty-eight (48) individuals initiated hepatitis B vaccination series, though 1 individual refused to see the PHN for completion. Of the remaining 47, 24 (51%) competed their series within a year. (See indicator 2c) Question 5 Are those found to have an STBBI treated appropriately, and have follow-up interviews and testing completed as per protocols? 5a) All positive cases of STBBIs will be notified of their results. 100% of positive cases were notified of their results. 70.8% of inmates received their results from the PHN in-house following urine screening. 72.8% of inmates received their BBP screening results in-house following screening. (See indicator 3d) 5b) All positive STI cases will be treated per guidelines. 100% of STI cases were treated as per the Canadian Sexually Transmitted Disease Guidelines (PHAC, 2006). 16
17 The Canadian Guidelines recommend unlike with chlamydia positives that all those found to be infected with gonorrhea undergo screening for HIV and syphilis. Of the 18 cases of gonorrhea, 13 (72%) had screening for HIV and syphilis. 2 individuals were offered screening and declined it. 3 individuals had no documented offer of BBP screening. It is also recommended that immunization against hepatitis B be undertaken for those who have tested positive for gonorrhea. 13 cases had documented hepatitis B immunity or completion of vaccination series. 1 individual was offered vaccination, but declined. 1 individual initiated their hepatitis vaccination series with the PHNs. 3 individuals had no documented offer of hepatitis B vaccination. 5c) All positive HIV and hepatitis C cases will be linked to medical care. Both new HIV diagnoses were linked to the Manitoba HIV program appropriately. Of the three new hepatitis C diagnoses, one case was linked to the community Hep C program at Mount Carmel Clinic. One was transferred to a new correctional facility, with documented contact with Southern Health Santé Sud PHNs to ensure appropriate follow-up. The remaining case was informed of their result, but no documented confirmation that the client was linked with a Hep C program was recorded. 17
18 Recommendations General All completed forms used for documentation by the PHNs should be photocopied and/or stored in a single location. Originals can be filed according to current processes, if these meet PHN needs. This process was implemented in late-2013 and should be periodically reviewed. Develop evidence-based guidelines specific to corrections (i.e. both MC and WRC, acknowledging differences between them) to ensure consistency and sustainability. These would include: o if/how to notify released clients of negative results, o if/how to follow up with released clients eligible for vaccination and/or in the process of completing a series, and o consistent documentation processes, as facilitated by improved forms. Revise the extant Sexually Transmitted & Blood Borne Infection Corrections form, in collaboration with the PHNs. Develop strategies, in collaboration with the PHNs and Manitoba Justice, to reduce the amount of duplicate charting required. The evaluation team should continue to meet regularly for the purposes of continual quality improvement. Related to Vaccination The PHNs should continue to have relatively easy access to MIMS/eChart in order to efficiently assess residents vaccination status. Currently, although PHNs have access to Correction s charts, their work takes place three floors below where the medical records are kept, which makes ideal access at the point of care impossible. Ensure that new/revised form facilitates documentation of assessment of confirmed immunity/previous completion of series for hepatitis vaccination. Related to STBBI testing, and treatment Continue exemplary offering of BBP screening. Ensure that new/revised form facilitates documentation of offering of BBP screening and/or reason for no offer. Consider the implementation of criteria to prioritise inmates seen for screening, based on the epidemiological profile of STBBIs in Manitoba. 18
19 Works Cited Barry, P. M., Kent, C. K., Scott, K. C., Snell, A., Goldenson, J., & Klausner, J. D. (2007). Optimising sexually transmitted infection screening in correctional facilities: San Francisco, Sexually Transmitted Infections 83(5), Beaudoin, C. (2009). The Epidemiology of Sexually Transmitted Infections and Blood Borne Pathogens in a Random Sample of Inmates in Manitoba Correctional Centres. Winnipeg: unpublished. Bullard, J. (2013). An STBBI Testing Update and the Quest for the 300. Winnipeg: Presentation to the WRHA 'Sex Matters' Conference. PHAC (Public Health Agency of Canada) (2006). Canadian Guidelines on Sexually Transmitted Infections. Ottawa: Government of Canada. Towards Evidence-Informed Practice (2009). Towards Evidence-Informed Practice (TEIP) Tools. Toronto: Ontario Public Health Association. 19
20 Appendix A HSHR Corrections Logic Model FINAL March
21 Page 1 21
22 Page 2 22
23 Appendix B Evaluation Framework Indicator Review * Worksheet courtesy of Health In Common 23
24 Adequate Culturally appropriate Practical Useful Specific Direct Currently Feasible? N N? N N N /N /N /N?? Worksheet 4b. Indicator Review Question 1. Are the PHNs roles in corrections clear, and are inmates aware of services and how to access them? Indicator(s) a. Correctional Officers will be aware of the PHNs roles and scope. b. Inmates are aware of how to access PHNs. c. Health services in correctional facilities refers inmates appropriately. 2. Are unvaccinated inmates being vaccinated against STBBIs, and are they completing their series? a. PHNs will assess inmates immunization status. b. Immunizations against STBBIs will be initiated when indicated. c. Inmates who initiate immunization series for hepatitis B and HPV will complete their series. 3. Are those at risk of STBBIs being offered testing and receiving their results? a. Inmates requesting PHN services will be seen by PHNs prior to release. b. Rates/100,000 of positive tests will be similar to, or in excess of Manitoba rates. 24
25 ? /N /N c. Rates of BBP testing will be at an acceptable percentage to STI testing, based on institutional context. d. All positive cases of STBBIs will be notified of their results. 4. Are individuals being linked appropriately to continuing care in the community? a. Evidence-based guidelines are in place to guide PHNs follow-up in the community. b. All positive cases of STBBIs will be notified of their results. c. Inmates who initiate immunization series for hepatitis B and HPV will complete their series. 5. Are those found to have an STBBI treated appropriately and have follow-up interviews and testing completed as per protocols? a. All positive cases of STBBIs will be notified of their results. b. All positive STI cases will be treated per guidelines. c. All positive HIV and hepatitis C cases will be linked to medical care. 25
26 Appendix C Sexually Transmitted & Blood-Borne Infection Corrections Form 26
27 CLIENT SURNAME GIVEN NAME DATE OF BIRTH MFRN PHIN Manitoba Corrections STI/BBP Counselling Gender: M h F h ERD/ Court Date: Alternate LocatingInformation Alias Risk Assessment: Contact for: Date of Last Sexual Exposure: Last Test: Number sexual contacts in last year: Sex with: Men Women Both Number of lifetime partners: Condom use: always most of the time some of the time never Age of Sexual Debut: Hx of Previous STI Sex Trade Worker/ Sex with Hx of Sexual Assault Sex Outside Manitoba Tattoo/piercing/acupuncture Scarification/ needle stick Injection Drug Use Other Substance Use Gang Involved/ Sex With Street Involved Recent Immigrant/ Sex With Fights Pregnant Birth Control Last Pap Test Self/ Partner Clinical: Symptoms Prevention Education: Condoms Oral barriers Chlamydia Gonorrhea Syphilis HIV HPV Herpes HBV HCV Trichomonas Transmission Incubation Period Complications Signs & symptoms Risk to newborn Testing Progress Notes: BBP Pre-test Counselling: Discuss transmission modes, signs & symptoms, prognosis, care, & treatment. Discuss harm reduction & prevention strategies. Discuss that a positive test means there is a presence of antibodies within 3 to 6 months. Discuss that a negative test means no antibodies were detected, meaning the person can be in the window period or the person is not affected. Discuss the confidentiality of the tests, provincial reporting requirements and partner notification. Discuss social supports and the stress related to waiting for test results and possible reactions to learning results. Discuss by whom and how test results will be communicated to offender. Obtain offender s consent for testing. [ GC CT VDRL HIV ANTI - HAV HBV HCV Hbsag ] 27
28 Completed (dd/mm/yy) Provider Signature and Professional Affiliation Initials of Provider Testing/Treatment: Allergies: dd/mm/yy Test Requisition/Code Result Treatment / Follow-up Chlamydia Gonorrhea HbsAG Anti-HBs Anti-HCV Anti-HAV HIV VDRL Pregnancy Test Post Test Counselling: Results of tests explained to offender. Re-test recommended in months. Test of cure recommended: yes no When NSTD completed and interviewed for contacts. Viral Hepatitis Investigation Form completed and interviewed for contacts Notification of HIV Infection completed and interviewed for contacts Discussed legal obligation to notify all sexual partners of HIV + status (for HIV cases/contacts) Immunization offered. Accepted Refused Referral to Completed (dd/mm/yy) Provider Signature and Professional Affiliation Initials of Provider Progress Notes: Immunization: dd/mm/yy Vaccine Lot # Dose Route/Site Signature Antibody : dd/mm/yy Test Result Plans Legend ERD-Expected Date of Release, Ag- antigen, Anti- antibody detection,, VDRL- screen, TP-PA-T palladium particle agglutination,, T-throat, R - rectal/anal, U-urethra Organism: HAV hepatitis A virus, HBV hepatitis B virus, HCV hepatitis C virus, HIV human immunodeficiency virus 28
29 Appendix D Delegation of Function Tracking Log 29
30 DELEGATION OF FUNCTION TRACKING LOG MONTH PHN Date Client Name Sex CHL/GC TEST B PHN SPHILIS TEST B PHN HEP SCREEN TEST B PHN HIV TEST B PHN M F 1g 2g TREATMENT B PHN Zithro Suprax TOTAL 30
31 Appendix E Urine Testing for Chlamydia & Gonorrhea Genital Infections Practice Guideline with Delegation of Function 31
32 Purpose To increase testing options for marginalized, mobile and underserved populations at risk for gonorrhea and chlamydial trachomatis genital infections. Preamble The prevention and control of sexually transmitted infections (STIs) are important components of a comprehensive communicable disease control strategy. While it is beneficial for all citizens of the Winnipeg Health Region to have a regular primary care provider, many people do not access care due to health, social and/or economic inequities. Not accessing care poses a potential health risk to the individuals themselves and to the community. In order to improve and focus efforts to test and treat vulnerable and mobile populations at risk for chlamydia and gonorrhea infections, designated Public Health Nurses (PHNs) may offer urine testing for chlamydia and gonorrhea to eligible clients. Delegation of Function The Medical Officer of Health (MOH), Winnipeg Regional Health Authority (WRHA), delegates to designated PHNs, the authority to administer chlamydia and gonorrhea urine testing and communicate these results to clients. These guidelines have been developed using the principles recommended in the Guideline for Shared Competencies and Delegated Physician Services (College of Physicians and Surgeons of Manitoba and College of Registered Nurses of Manitoba, 2002) as indicated in the following 6 sections. 1. Patients/Clients Appropriateness of the client: Clients who meet Urine Testing Eligibility Criteria (outlined below) are those in need of specialized sexual health, harm reduction, and/or STI-related public health assessment or education from PHNs within the WRHA Healthy Sexuality and Harm Reduction team These clients expect the public health practitioner to be competent & current. They expect to have urine testing for gonorrhea and chlamydia infections, and receive the test results with referral for appropriate treatment and/or primary care and support services as necessary. 32
33 Winnipeg Regional Health Authority Healthy Sexuality and Harm Reduction Team Date Issued: April 3, 2003 Practice Guideline with Delegation of Function Urine Testing for Chlamydia & Gonorrhea Genital Infections Reviewed and accepted by Dr. P. Plourde (original signed by Dr. Plourde & Registered Nurses to whom function is delegated) Date Revised: Sept 30, 2010 Appropriateness of the service delegation: Testing of urine specimens will be delegated to PHNs with advanced education and experience in public health who are working within the WRHA Healthy Sexuality and Harm Reduction team 2. Collaboration between the delegating MOH and registered nurse This document, when signed by the delegating MOH and PHN, is a clear agreement regarding delegation of function This delegation does not apply in the following situations. Referral to appropriate medical practitioner/rn(ep) needed: o Client with symptoms that suggest Pelvic Inflammatory Disease (PID), urinary tract infection (UTI) or other clinical findings beyond the usual scope of practice in the course of offering STI screening o Client does not provide informed consent to testing o Client not able to independently provide urine sample 3. Competence Physician competence: The MOH s (Dr. Pierre Plourde) professional qualifications include a Certificate of Special Competence, Infectious Diseases, Royal College of Physicians of Canada (FRCPC); Associate Professor, University of Manitoba Departments of Medical Microbiology and Community Health Sciences In the absence of the above-named MOH, consultation is available through any of the other MOH s at the WRHA. All WRHA MOHs have advanced professional qualifications including Certificates of Special Competence with the Royal College of Physicians of Canada (FRCPC) Public Health Nurse Competence: PHN competence will include an orientation to specialized Healthy Sexuality and Harm Reduction services including delegated urine testing for uncomplicated chlamydia and gonorrhea infections, followed by ongoing continuing education. Competency will initially be achieved over a 4-8 week period of apprenticeship with an experienced PHN. Maintenance of 33
34 Winnipeg Regional Health Authority Healthy Sexuality and Harm Reduction Team Date Issued: April 3, 2003 Practice Guideline with Delegation of Function Urine Testing for Chlamydia & Gonorrhea Genital Infections Reviewed and accepted by Dr. P. Plourde (original signed by Dr. Plourde & Registered Nurses to whom function is delegated) Date Revised: Sept 30, 2010 competency will be achieved through ongoing review of practice in regular team meetings with the Manager, MOH, Clinical Nurse Specialist and Communicable Disease Control (CD) Coordinator 4. Context Supports include access to all current STI guidelines and resources (Healthy Sexuality and Harm Reduction team s practice guidelines, Manitoba Health and Health Living s Communicable Diseases Management Protocols, Public Health Agency of Canada s Canadian Guidelines on Sexually Transmitted Infections). Where there are differences between provincial and national guidelines, provincial guidelines apply. The MOH or designated back-up MOH is available by pager for immediate consultation as required. Mechanisms to maintain quality and safety will include regular peer review at team meetings, regular consultation with the MOH through the CD Coordinator, and an annual random chart audit by the CD Coordinator (at least 5 charts per nurse to be reviewed). Every 3 months, the PHN will send to the CD Coordinator, a list of clients who received a delegated function by the PHN. When guidelines and delegations are not followed, this will be documented, investigated and evaluated with the PHN by the MOH in collaboration (as appropriate) with a designated individual (Team Manager, Clinical Nurse Specialist, CD Coordinator). Bi-annual performance reviews with manager are required. All WRHA guidelines for documentation and storage of records will be followed according to existing WRHA standards and protocols 5. Education Continued and ongoing competence will be maintained through ongoing education and review of practice. Reliable provincial and national guidelines are available and updated regularly, and are used by PHNs for each delegated function. PHNs are competent healthcare professionals with skills in teaching about risks, benefits, side effects and reporting of adverse events 34
35 Winnipeg Regional Health Authority Healthy Sexuality and Harm Reduction Team Date Issued: April 3, 2003 Practice Guideline with Delegation of Function Urine Testing for Chlamydia & Gonorrhea Genital Infections Reviewed and accepted by Dr. P. Plourde (original signed by Dr. Plourde & Registered Nurses to whom function is delegated) Date Revised: Sept 30, Evaluation This delegation of function process will be reviewed every 2 years or more frequently if needed (e.g., change in delegating physician). Guideline Urine testing to screen for chlamydia and gonorrhea may be offered by PHNs who have current signed delegation agreements, to eligible clients who meet the Urine Testing Eligibility Criteria Procedure Determine client s eligibility with the Urine Testing Eligibility Criteria Assess client s health status Ensure the standards of care (below) are met Complete appropriate requisition & enter taken by [nurse s name and phone number] into the other requests sections at bottom right side of requisition PHN may interview client for sex contacts at this time for the purposes of partner notification if results are positive PHN may assess eligibility as per the Antibiotic Treatment for Uncomplicated Chlamydia and Gonorrhea Practice Guideline with Delegation of Function Standards of Care The PHN will: Offer chlamydia and gonorrhea urine testing to clients who meet the Urine Testing Eligibility Criteria review risks of infection along with the risks/benefits of testing/ treatment and the value of Primary Care for all health/stbbi needs Review the testing process 35
36 Winnipeg Regional Health Authority Healthy Sexuality and Harm Reduction Team Date Issued: April 3, 2003 Practice Guideline with Delegation of Function Urine Testing for Chlamydia & Gonorrhea Genital Infections Reviewed and accepted by Dr. P. Plourde (original signed by Dr. Plourde & Registered Nurses to whom function is delegated) Date Revised: Sept 30, 2010 Obtain informed consent ensuring appropriate information & capacity Make a plan with the client for the sharing of results Offer risk/harm reduction and prevention information and resources Manage results as follows: o original test results will be retained in the client record o no results will be given to third parties except as required by law or with the informed consent of the client in accordance with PHIA o arrangements will be made for medical follow-up/referral as needed o arrange/refer for social support services as needed with client s consent Document on the WRHA Client Record: o Urine Testing Eligibility Criteria reviewed o Primary Care for STBBI recommended/supported by PHN o Client provided informed consent o Date and time that specimen obtained o Plan for follow-up and sharing of results o Risk/harm reduction education and resources offered and/or provided Urine Testing Eligibility Criteria AT LEAST 1 OF THE FOLLOWING 3 CRITERIA Client did not attend a primary care provider for testing, due to health, social and/or economic inequities Incarcerated persons to whom the Healthy Sexuality and Harm Reduction team is making a special effort to reach because they are members of a spread network Persons to whom the Healthy Sexuality and Harm Reduction team is making a special effort to reach because they are patrons of venues with significant risk of STI transmission (e.g., bathhouse patrons) AND Client is able to understand the information, benefits and risks that are relevant to making a decision to be tested. If there are any doubts about the individual s 36
37 Winnipeg Regional Health Authority Healthy Sexuality and Harm Reduction Team Date Issued: April 3, 2003 Practice Guideline with Delegation of Function Urine Testing for Chlamydia & Gonorrhea Genital Infections Reviewed and accepted by Dr. P. Plourde (original signed by Dr. Plourde & Registered Nurses to whom function is delegated) Date Revised: Sept 30, 2010 capacity to consent, the testing should not be performed by the PHN, and the client should be referred to a physician/nurse practitioner for medical assessment AND Client is at least 16 years of age. Note: For those clients between the ages of 13 and 15, a reasonable attempt must be made by the nurse to obtain parental/legal guardian consent prior to testing. For street involved youth, the persistent refusal to disclose guardianship will be considered a reasonable attempt to locate parents/guardians, and the mature minor provision will be followed AND Client is able to independently provide his/her own urine sample AND AT LEAST 1 OF THE FOLLOWING Client presents to the PHN with clinical symptoms of uncomplicated gonorrhea and/or chlamydia, as per the Communicable Disease Management Protocols (Manitoba Health and Healthy Living, 2008) Client has been named as a contact to a case of gonorrhea and/or chlamydia Client is identified as being at risk for an STI as per Communicable Disease Management Protocols (Manitoba Health and Healthy Living, 2008) References College of Physicians and Surgeons of Manitoba and College of Registered Nurses of Manitoba (2002), (Guideline No. 132) Guidelines for Shared Competencies and 37
38 Winnipeg Regional Health Authority Healthy Sexuality and Harm Reduction Team Date Issued: April 3, 2003 Practice Guideline with Delegation of Function Urine Testing for Chlamydia & Gonorrhea Genital Infections Reviewed and accepted by Dr. P. Plourde (original signed by Dr. Plourde & Registered Nurses to whom function is delegated) Date Revised: Sept 30, 2010 Delegated Physician Services revised. Retrieved February 5, 2009 from: Manitoba Health and Healthy Living (2008), Communicable Disease Management Protocols. Retrieved February 5, 2009 from: Public Health Agency of Canada (2006). Canadian Guidelines on Sexually Transmitted Infections. Retrieved February 5, 2009 from: 38
Evaluation Report Manitoba Youth Centre
 Evaluation Report Manitoba outh Centre Prepared for Winnipeg Regional Health Authority, Population and Public Health Program Healthy Sexuality and Harm Reduction Team Prepared by: Kellee Hodge, MPH Practicum
Evaluation Report Manitoba outh Centre Prepared for Winnipeg Regional Health Authority, Population and Public Health Program Healthy Sexuality and Harm Reduction Team Prepared by: Kellee Hodge, MPH Practicum
Clinical Practice Guideline with Delegation of Function
 1 of 8 1.0 Purpose 1.1 To improve and focus efforts to treat those at risk for undiagnosed/untreated incubating, primary, secondary, or early latent infectious syphilis. 2.0 Scope and Goal 2.1 Antibiotic
1 of 8 1.0 Purpose 1.1 To improve and focus efforts to treat those at risk for undiagnosed/untreated incubating, primary, secondary, or early latent infectious syphilis. 2.0 Scope and Goal 2.1 Antibiotic
Clinical Practice Guideline
 1 of 10 1.0 Purpose 1.1 To improve and focus efforts to respond to clusters and outbreaks of infectious syphilis and reduce transmission in the Winnipeg Health Region by enhancing treatment options for
1 of 10 1.0 Purpose 1.1 To improve and focus efforts to respond to clusters and outbreaks of infectious syphilis and reduce transmission in the Winnipeg Health Region by enhancing treatment options for
Descriptive Epidemiology of STBBIs in the Winnipeg Health Region
 Descriptive Epidemiology of STBBIs in the Winnipeg Health Region Pierre Plourde Souradet Shaw Debbie Nowicki Mandy Whitlock March 22, 211 Methods Case definitions and case reporting In Manitoba, all confirmed
Descriptive Epidemiology of STBBIs in the Winnipeg Health Region Pierre Plourde Souradet Shaw Debbie Nowicki Mandy Whitlock March 22, 211 Methods Case definitions and case reporting In Manitoba, all confirmed
An STBBI Testing Update and the Quest for the 300
 An STBBI Testing Update and the Quest for the 300 Jared Bullard MD FRCPC Paediatric Infectious Diseases & Medical Microbiology Associate Medical Director Cadham Provincial Laboratory WRHA STBBI Conference
An STBBI Testing Update and the Quest for the 300 Jared Bullard MD FRCPC Paediatric Infectious Diseases & Medical Microbiology Associate Medical Director Cadham Provincial Laboratory WRHA STBBI Conference
New Brunswick Report on Sexually Transmitted and Blood Borne Infections, 2016
 New Brunswick Report on Sexually Transmitted and Blood Borne Infections, 6 Table of Contents. Introduction.... Methodology... 3. Data Limitations.... Definitions used... 3 5. Overview of STBBI epidemiology
New Brunswick Report on Sexually Transmitted and Blood Borne Infections, 6 Table of Contents. Introduction.... Methodology... 3. Data Limitations.... Definitions used... 3 5. Overview of STBBI epidemiology
Survey questionnaire on STI. surveillance, care and prevention. in European countries SAMPLE APPENDIX
 European Surveillance of Sexually Transmitted Infections Survey questionnaire on STI surveillance, care and prevention in European countries APPENDIX Detailed questionnaire on clinician and laboratory
European Surveillance of Sexually Transmitted Infections Survey questionnaire on STI surveillance, care and prevention in European countries APPENDIX Detailed questionnaire on clinician and laboratory
Manitoba Health Statistical Update on HIV/AIDS
 Manitoba Health Statistical Update on HIV/AIDS 1985-2002 Communicable Disease Control Unit Public Health MANITOBA HEALTH STATISTICAL UPDATE ON HIV/AIDS 1985 TO December 2002 HIV January 1, 1985 to December
Manitoba Health Statistical Update on HIV/AIDS 1985-2002 Communicable Disease Control Unit Public Health MANITOBA HEALTH STATISTICAL UPDATE ON HIV/AIDS 1985 TO December 2002 HIV January 1, 1985 to December
Gonorrhea, Chlamydia, and Syphilis in Alaska
 Department of Health and Social Services Division of Public Health Section of Epidemiology Karen Perdue, Commissioner Karen Pearson, Director John Middaugh, MD, Editor 361 C Street, Suite 54, P.O. Box
Department of Health and Social Services Division of Public Health Section of Epidemiology Karen Perdue, Commissioner Karen Pearson, Director John Middaugh, MD, Editor 361 C Street, Suite 54, P.O. Box
Immunization of Adults in High Risk Populations. Carol A. Kurbis MD, CCFP, FRCPC WRHA Medical Officer of Health
 Immunization of Adults in High Risk Populations Carol A. Kurbis MD, CCFP, FRCPC WRHA Medical Officer of Health OBJECTIVES To review recommendations for immunization in adult populations, with a focus on
Immunization of Adults in High Risk Populations Carol A. Kurbis MD, CCFP, FRCPC WRHA Medical Officer of Health OBJECTIVES To review recommendations for immunization in adult populations, with a focus on
IDU Outreach Project. Program Guidelines
 Ministry of Health and Long-Term Care Ministère de la Santé et des Soins de longue dureé Prepared by: AIDS Bureau Revision Date: April 2001 TABLE OF CONTENTS 1 Introduction...1 1.1 Program Goals... 2 1.2
Ministry of Health and Long-Term Care Ministère de la Santé et des Soins de longue dureé Prepared by: AIDS Bureau Revision Date: April 2001 TABLE OF CONTENTS 1 Introduction...1 1.1 Program Goals... 2 1.2
Mahoning County Public Health. Epidemiology Response Annex
 Mahoning County Public Health Epidemiology Response Annex Created: May 2006 Updated: February 2015 Mahoning County Public Health Epidemiology Response Annex Table of Contents Epidemiology Response Document
Mahoning County Public Health Epidemiology Response Annex Created: May 2006 Updated: February 2015 Mahoning County Public Health Epidemiology Response Annex Table of Contents Epidemiology Response Document
Manitoba Health Statistical Update on HIV/AIDS
 Manitoba Health Statistical Update on HIV/AIDS 1985 - Dec 2001 Communicable Disease Control Unit Public Health Branch MANITOBA HEALTH STATISTICAL UPDATE ON HIV/AIDS 1985 TO DECEMBER 2001 HIV January 1,
Manitoba Health Statistical Update on HIV/AIDS 1985 - Dec 2001 Communicable Disease Control Unit Public Health Branch MANITOBA HEALTH STATISTICAL UPDATE ON HIV/AIDS 1985 TO DECEMBER 2001 HIV January 1,
Safety Regulations and Procedures Occupational Health Bloodborne Pathogens Exposure Control Plan S80.10, updated, May Contains information for:
 APPENDIX A Safety Regulations and Procedures Occupational Health Bloodborne Pathogens Exposure Control Plan S80.10, updated, May 2018 BLOODBORNE PATHOGEN EXPOSURE INCIDENT PACKET Contains information for:
APPENDIX A Safety Regulations and Procedures Occupational Health Bloodborne Pathogens Exposure Control Plan S80.10, updated, May 2018 BLOODBORNE PATHOGEN EXPOSURE INCIDENT PACKET Contains information for:
Sexually Transmitted Infections In Manitoba
 Sexually Transmitted Infections In Manitoba 2014 A focus on bacterial sexually transmitted infections Data reported to December 31, 2014 Epidemiology & Surveillance Public Health Branch Public Health and
Sexually Transmitted Infections In Manitoba 2014 A focus on bacterial sexually transmitted infections Data reported to December 31, 2014 Epidemiology & Surveillance Public Health Branch Public Health and
FY 2018 PERFORMANCE PLAN. Public Health/ CHSB
 Sexually Transmitted Infections Clinic Public Health/ CHSB Lilibeth Grandas x1211 Sharron Martin x1239 Program Purpose Program Information Reduce and prevent the incidence of sexually transmitted infections
Sexually Transmitted Infections Clinic Public Health/ CHSB Lilibeth Grandas x1211 Sharron Martin x1239 Program Purpose Program Information Reduce and prevent the incidence of sexually transmitted infections
Summary Report: Survey of Hepatitis C Virus counseling and testing services at HIV counseling and testing sites, and health service sites.
 Summary Report: Survey of Hepatitis C Virus counseling and testing services at HIV counseling and testing sites, and health service sites. Sharon Adler MD, MPH Tomás Aragón MD, MPH Preventive Medicine
Summary Report: Survey of Hepatitis C Virus counseling and testing services at HIV counseling and testing sites, and health service sites. Sharon Adler MD, MPH Tomás Aragón MD, MPH Preventive Medicine
Sexually Transmitted & Blood-Borne Infections in LGL ( )
") Sexually Transmitted & Blood-Borne Infections in LGL (2006 2015) Some Highlights: Chlamydia, Hepatitis C and Gonorrhoea were the sexually transmitted infections with the highest incidences in LGL in 2015.
Sexually Transmitted & Blood-Borne Infections in LGL (2006 2015) Some Highlights: Chlamydia, Hepatitis C and Gonorrhoea were the sexually transmitted infections with the highest incidences in LGL in 2015.
STI Prevention: Housekeeping and How We Use Public Health. M. Terry Hogan, MPH Johns Hopkins University
 This work is licensed under a Creative Commons Attribution-NonCommercial-ShareAlike License. Your use of this material constitutes acceptance of that license and the conditions of use of materials on this
This work is licensed under a Creative Commons Attribution-NonCommercial-ShareAlike License. Your use of this material constitutes acceptance of that license and the conditions of use of materials on this
COMMUNICABLE DISEASE REPORT
 June 2011 Department of Health and Community Services Government of Newfoundland and Labrador COMMUNICABLE DISEASE REPORT Reporting Sexually Transmitted and Bloodborne Infections All laboratory-confirmed
June 2011 Department of Health and Community Services Government of Newfoundland and Labrador COMMUNICABLE DISEASE REPORT Reporting Sexually Transmitted and Bloodborne Infections All laboratory-confirmed
CHAPTER 1: SEXUALLY TRANSMITTED AND BLOODBORNE INFECTIONS
 CHAPTER : SEXUALLY TRANSMITTED AND BLOODBORNE INFECTIONS Highlights In Peel, the incidence of Acquired Immunodeficiency Syndrome (AIDS) has remained low (. to. cases per,) since the introduction of the
CHAPTER : SEXUALLY TRANSMITTED AND BLOODBORNE INFECTIONS Highlights In Peel, the incidence of Acquired Immunodeficiency Syndrome (AIDS) has remained low (. to. cases per,) since the introduction of the
Note: Staff who work in case management programs should attend the AIDS Institute training, "Addressing Prevention in HIV Case Management.
 Addressing Prevention with HIV Positive Clients This one-day training will prepare participants to help people living with HIV to avoid sexual and substance use behaviors that can result in transmitting
Addressing Prevention with HIV Positive Clients This one-day training will prepare participants to help people living with HIV to avoid sexual and substance use behaviors that can result in transmitting
ACKNOWLEDGEMENTS FOR FURTHER INFORMATION
 ACKNOWLEDGEMENTS This report details the descriptive epidemiology of chlamydia and gonorrhea in the Winnipeg Health Region. Special gratitude is extended to the following individuals: Communicable Disease
ACKNOWLEDGEMENTS This report details the descriptive epidemiology of chlamydia and gonorrhea in the Winnipeg Health Region. Special gratitude is extended to the following individuals: Communicable Disease
What You Need to Know. Sexually Transmitted Infections (STIs)
") What You Need to Know Sexually Transmitted Infections (STIs) What You Need to Know About STIs What are STIs? Sexually transmitted infections (STIs) are diseases that spread through sexual contact. If you
What You Need to Know Sexually Transmitted Infections (STIs) What You Need to Know About STIs What are STIs? Sexually transmitted infections (STIs) are diseases that spread through sexual contact. If you
HIV Point of Care Testing in Manitoba Report
 CADHAM PROVINCIAL LABORATORY HIV Point of Care Testing in Manitoba Report 2016 to 2017 APRIL 2018 1 HIV POINT OF CARE TESTING IN MANITOBA REPORT, 2016 TO 2017 Report prepared by: Jared Bullard Cadham Provincial
CADHAM PROVINCIAL LABORATORY HIV Point of Care Testing in Manitoba Report 2016 to 2017 APRIL 2018 1 HIV POINT OF CARE TESTING IN MANITOBA REPORT, 2016 TO 2017 Report prepared by: Jared Bullard Cadham Provincial
Appendix 11 Roles and Responsibilities October, 2013 Page 1 of 5
 October, 2013 Page 1 of 5 Exposed Person To present to a health care facility as soon as possible following the exposure (ideally within 2 hours). To answer assessment questions. (Refer to Appendix 15
October, 2013 Page 1 of 5 Exposed Person To present to a health care facility as soon as possible following the exposure (ideally within 2 hours). To answer assessment questions. (Refer to Appendix 15
ALASKA NATIVE MEDICAL CENTER SEXUALLY TRANSMITTED DISEASE SCREENING AND TREATMENT GUIDELINES
 ALASKA NATIVE MEDICAL CENTER SEXUALLY TRANSMITTED DISEASE SCREENING AND TREATMENT GUIDELINES A. Screening Page Chlamydia and Gonorrhea 1 HIV 1 Syphilis 1 Genital Herpes 2 Hepatitis A 2 Hepatitis B 2 Hepatitis
ALASKA NATIVE MEDICAL CENTER SEXUALLY TRANSMITTED DISEASE SCREENING AND TREATMENT GUIDELINES A. Screening Page Chlamydia and Gonorrhea 1 HIV 1 Syphilis 1 Genital Herpes 2 Hepatitis A 2 Hepatitis B 2 Hepatitis
Coding for Preventive Services A Guide for HIV Providers
 Coding for Preventive Services A Guide for HIV Providers Jessie Murphy, MPH and Michelle Cataldo, LCSW, April 2016 Implementation of the Patient Protection and Affordable Care Act and other regulatory
Coding for Preventive Services A Guide for HIV Providers Jessie Murphy, MPH and Michelle Cataldo, LCSW, April 2016 Implementation of the Patient Protection and Affordable Care Act and other regulatory
Practice Steps for Implementation of Guidelines Recommendations The guideline recommendations are shown schematically -
 ASK SCREEN Test for HIV and STI Practice Steps for Implementation of Guidelines Recommendations The guideline recommendations are shown schematically - Routinely obtain a thorough sexual history from all
ASK SCREEN Test for HIV and STI Practice Steps for Implementation of Guidelines Recommendations The guideline recommendations are shown schematically - Routinely obtain a thorough sexual history from all
2016 SATURDAY SERVICES TRAINING INFORMATION Applications are due Tuesday, March 1, 2016 at 11:59pm. Early submission is highly recommended!
 BERKELEY FREE CLINIC, SATURDAY SERVICES COLLECTIVE Clinic Address: 2339 Durant Avenue, Berkeley, CA 94704. Clinic Number: (510) 548 2570 saturdayservicestc@gmail.com 2016 SATURDAY SERVICES TRAINING INFORMATION
BERKELEY FREE CLINIC, SATURDAY SERVICES COLLECTIVE Clinic Address: 2339 Durant Avenue, Berkeley, CA 94704. Clinic Number: (510) 548 2570 saturdayservicestc@gmail.com 2016 SATURDAY SERVICES TRAINING INFORMATION
Sexually Transmitted Diseases This publication was made possible by Grant Number TP1AH from the Department of Health and Human Services,
 Sexually Transmitted Diseases This publication was made possible by Grant Number TP1AH000081-01-01 from the Department of Health and Human Services, Office of Adolescent Health; its contents are solely
Sexually Transmitted Diseases This publication was made possible by Grant Number TP1AH000081-01-01 from the Department of Health and Human Services, Office of Adolescent Health; its contents are solely
Infectious and Communicable Diseases Prevention and Control Program Annual Service Plan A. Community Need and Priorities We are situated rurally with
 Infectious and Communicable Diseases Prevention and Control Program Annual Service Plan A. Community Need and Priorities We are situated rurally with no access to walk in clinics and access to health care
Infectious and Communicable Diseases Prevention and Control Program Annual Service Plan A. Community Need and Priorities We are situated rurally with no access to walk in clinics and access to health care
As a result of this training, participants will be able to:
 Addressing Sexual Risk with Drug Users and their Partners 1 Day Training This one-day training will build participant knowledge and skills in offering sexual harm reduction options to substance users.
Addressing Sexual Risk with Drug Users and their Partners 1 Day Training This one-day training will build participant knowledge and skills in offering sexual harm reduction options to substance users.
IMPORTANT HEALTH INFORMATION
 IMPORTANT HEALTH INFORMATION SU-6523MI Page 1 of 8 Table of Contents Page What is an HIV test?..........................................1 Will the HIV test tell me if I have AIDS?............................1
IMPORTANT HEALTH INFORMATION SU-6523MI Page 1 of 8 Table of Contents Page What is an HIV test?..........................................1 Will the HIV test tell me if I have AIDS?............................1
As a result of this training, participants will be able to:
 Addressing Prevention with HIV Positive Clients 1 Day Training This one-day training will prepare participants to help people living with HIV to avoid sexual and substance use behaviors that can result
Addressing Prevention with HIV Positive Clients 1 Day Training This one-day training will prepare participants to help people living with HIV to avoid sexual and substance use behaviors that can result
Biology 3201 Unit 2 Reproduction: Sexually Transmitted Infections (STD s/sti s)
") Biology 3201 Unit 2 Reproduction: Sexually Transmitted Infections (STD s/sti s) STI s once called venereal diseases More than 20 STIs have now been identified most prevalent among teenagers and young adults.
Biology 3201 Unit 2 Reproduction: Sexually Transmitted Infections (STD s/sti s) STI s once called venereal diseases More than 20 STIs have now been identified most prevalent among teenagers and young adults.
Primary Care Services for blood borne viral hepatitis prevention, treatment and care
 Primary Care Services for blood borne viral hepatitis prevention, treatment and care Author: Josie Smith, Marion Lyons Page 1 of 13 October 2006 Status : Final Contents: Page: Executive Summary 3 Introduction
Primary Care Services for blood borne viral hepatitis prevention, treatment and care Author: Josie Smith, Marion Lyons Page 1 of 13 October 2006 Status : Final Contents: Page: Executive Summary 3 Introduction
HIV/AIDS. Saskatchewan. Saskatchewan Health Population Health Branch
 HIV/AIDS In Saskatchewan 26 Saskatchewan Health Population Health Branch HIV/AIDS in Saskatchewan to December 31, 26 This epidemiological report profiles HIV and AIDS in Saskatchewan from the commencement
HIV/AIDS In Saskatchewan 26 Saskatchewan Health Population Health Branch HIV/AIDS in Saskatchewan to December 31, 26 This epidemiological report profiles HIV and AIDS in Saskatchewan from the commencement
STI & HIV PRE-TEST ANSWER KEY
 Name: STI & HIV PRE-TEST ANSWER KEY 1. You can catch a STI or HIV from door knobs, toilet seats, or FALSE drinking fountains. STIs are transmitted sexually, requiring sexual contact. Some STIs can be transmitted
Name: STI & HIV PRE-TEST ANSWER KEY 1. You can catch a STI or HIV from door knobs, toilet seats, or FALSE drinking fountains. STIs are transmitted sexually, requiring sexual contact. Some STIs can be transmitted
The objectives of this presentation are; to increase awareness of the issue of antimicrobial resistant gonorrhea, and to inform primary care and
 1 Antimicrobial resistant gonorrhea is an emerging public health threat that needs to be addressed. Neisseria gonorrhoeae is able to develop resistance to antimicrobials quickly. Effective antibiotic stewardship
1 Antimicrobial resistant gonorrhea is an emerging public health threat that needs to be addressed. Neisseria gonorrhoeae is able to develop resistance to antimicrobials quickly. Effective antibiotic stewardship
Dear Parent or Guardian,
 Dear Parent or Guardian, This summer may be a period of transition for you and your child. For a lot of our students it may even be the first time they are taking the lead in their personal care, including
Dear Parent or Guardian, This summer may be a period of transition for you and your child. For a lot of our students it may even be the first time they are taking the lead in their personal care, including
SUBJECT: Hepatitis C Virus (HCV) Counseling/Education, Testing, Referral, and Partner Notification
 Counseling/Education, Testing, Referral, and Partner Notification") SUBJECT: Hepatitis C Virus (HCV) Counseling/Education, Testing, Referral, and Partner Notification Hepatitis C virus (HCV) infection is the most common chronic bloodborne infection in the United States.
SUBJECT: Hepatitis C Virus (HCV) Counseling/Education, Testing, Referral, and Partner Notification Hepatitis C virus (HCV) infection is the most common chronic bloodborne infection in the United States.
Annual Statistical Update on HIV and AIDS 2013
 Annual Statistical Update on HIV and AIDS 2013 Data reported to December 31, 2013 Epidemiology & Surveillance Public Health Branch Public Health and Primary Health Care Division Manitoba Health, Healthy
Annual Statistical Update on HIV and AIDS 2013 Data reported to December 31, 2013 Epidemiology & Surveillance Public Health Branch Public Health and Primary Health Care Division Manitoba Health, Healthy
Toronto Public Health HCV Outbreak Investigation Ontario Endoscopy Clinic 1315 Finch Avenue West, Suite 302, Toronto Final Report April 24, 2015
 Toronto Public Health HCV Outbreak Investigation Ontario Endoscopy Clinic 1315 Finch Avenue West, Suite 302, Toronto Final Report April 24, 2015 Initial Case Identification On May 24, 2013, a 60 year old
Toronto Public Health HCV Outbreak Investigation Ontario Endoscopy Clinic 1315 Finch Avenue West, Suite 302, Toronto Final Report April 24, 2015 Initial Case Identification On May 24, 2013, a 60 year old
Guidelines for Implementing Pre-Exposure Prophylaxis For The Prevention of HIV in Youth Peter Havens, MD MS Draft:
 Guidelines for Implementing Pre-Exposure Prophylaxis For The Prevention of HIV in Youth Peter Havens, MD MS Draft: 10-2-2015 Clinical studies demonstrate that when a person without HIV infection takes
Guidelines for Implementing Pre-Exposure Prophylaxis For The Prevention of HIV in Youth Peter Havens, MD MS Draft: 10-2-2015 Clinical studies demonstrate that when a person without HIV infection takes
The epidemiology of hepatitis C in Canada
 The epidemiology of hepatitis C in Canada FACT SHEET Published 2017 This fact sheet provides a snapshot of the hepatitis C epidemic in Canada. It is one of a series of fact sheets providing epidemiological
The epidemiology of hepatitis C in Canada FACT SHEET Published 2017 This fact sheet provides a snapshot of the hepatitis C epidemic in Canada. It is one of a series of fact sheets providing epidemiological
ANNOUNCEMENT. Navy and Marine Corps Public Health Center 1
 ANNOUNCEMENT Register for the Monthly Disease SurveillanceTrainings: Contact your Service surveillance hub Log-on or Request log-on ID/password: https://tiny.army.mil/r/zb8a/cme and Register for Epi-Tech
ANNOUNCEMENT Register for the Monthly Disease SurveillanceTrainings: Contact your Service surveillance hub Log-on or Request log-on ID/password: https://tiny.army.mil/r/zb8a/cme and Register for Epi-Tech
iphis Case ID #: Reported Date: Reporting Source: Diagnosing Health Unit: Branch Office: Outbreak Number:
 Case Investigation Form: Hepatitis C Legend iphis system mandatory Required Case Information (add dates as YYYY-MM-DD) Case s Last Name: Case s First Name: Middle Name: Birth Date: Male Gender: Female
Case Investigation Form: Hepatitis C Legend iphis system mandatory Required Case Information (add dates as YYYY-MM-DD) Case s Last Name: Case s First Name: Middle Name: Birth Date: Male Gender: Female
Responsibilities in a sexual relationship - Contact tracing
 P a g e 1 Responsibilities in a sexual relationship - Contact tracing This activity has been designed increase student familiarity with the NSW Health Play Safe website. Suggested duration: 50-60 minutes
P a g e 1 Responsibilities in a sexual relationship - Contact tracing This activity has been designed increase student familiarity with the NSW Health Play Safe website. Suggested duration: 50-60 minutes
Annual Statistical Update: HIV and AIDS
 Annual Statistical Update: HIV and AIDS 2015 Data reported to December 31, 2015 Epidemiology & Surveillance Public Health Branch Public Health and Primary Health Care Division Manitoba Health, Seniors
Annual Statistical Update: HIV and AIDS 2015 Data reported to December 31, 2015 Epidemiology & Surveillance Public Health Branch Public Health and Primary Health Care Division Manitoba Health, Seniors
Prevalence of Hepatitis B and C in an Urban General Medicine Practice
 Prevalence of Hepatitis B and C in an Urban General Medicine Practice Juliet Jacobsen A. Study Purpose and Rationale Hepatitis B and C are the major causes of acute and chronic hepatitis, cirrhosis and
Prevalence of Hepatitis B and C in an Urban General Medicine Practice Juliet Jacobsen A. Study Purpose and Rationale Hepatitis B and C are the major causes of acute and chronic hepatitis, cirrhosis and
Howard Brown Health Center
 Howard Brown Health Center STI Annual Report, Background Howard Brown is the largest LGBT health center in the Midwest, providing comprehensive medical and behavioral health services to over, adults and
Howard Brown Health Center STI Annual Report, Background Howard Brown is the largest LGBT health center in the Midwest, providing comprehensive medical and behavioral health services to over, adults and
Clinical Practice Guideline. APPROVED BY: Healthy Sexuality and Harm Reduction Working Group
 1 of 18 Purpose To ensure an appropriate and consistent approach to the public health management of HIV-positive clients who do not disclose their HIV status before engaging in activities that put others
1 of 18 Purpose To ensure an appropriate and consistent approach to the public health management of HIV-positive clients who do not disclose their HIV status before engaging in activities that put others
Annual Statistical Update: HIV and AIDS
 Annual Statistical Update: HIV and AIDS 2014 Data reported to December 31, 2014 Epidemiology & Surveillance Public Health Branch Public Health and Primary Health Care Division Manitoba Health, Healthy
Annual Statistical Update: HIV and AIDS 2014 Data reported to December 31, 2014 Epidemiology & Surveillance Public Health Branch Public Health and Primary Health Care Division Manitoba Health, Healthy
Department of Dental Hygiene Policy on Bloodborne Pathogens
 Department of Dental Hygiene Policy on Bloodborne Pathogens The Bridgemont Department of Dental Hygiene Policy on Bloodborne Pathogens is modeled after the policy statement published by the American Dental
Department of Dental Hygiene Policy on Bloodborne Pathogens The Bridgemont Department of Dental Hygiene Policy on Bloodborne Pathogens is modeled after the policy statement published by the American Dental
In Canada and around the world, the trend is clear: sexually transmitted infections (STIs) are on the rise.
 are on the rise.") Adapted From: Sexually Transmitted Infections Pamphlet. Public Health Agency of Canada, 2007 In Canada and around the world, the trend is clear: sexually transmitted infections (STIs) are on the rise.
Adapted From: Sexually Transmitted Infections Pamphlet. Public Health Agency of Canada, 2007 In Canada and around the world, the trend is clear: sexually transmitted infections (STIs) are on the rise.
Appendix A: Disease-Specific Chapters
 Infectious Diseases Protocol Appendix A: Disease-Specific Chapters Chapter: Gonorrhoea Revised January 2014 Gonorrhoea Communicable Virulent Health Protection and Promotion Act, Section 1 (1) Health Protection
Infectious Diseases Protocol Appendix A: Disease-Specific Chapters Chapter: Gonorrhoea Revised January 2014 Gonorrhoea Communicable Virulent Health Protection and Promotion Act, Section 1 (1) Health Protection
HIV and STD Integration: Using Data to Power the Program
 HIV and STD Integration: Using Data to Power the Program Focus: Prevention and Surveillance Moderator: Romni Neiman, MPH, Assistant Branch Chief, CDPH STD Control Branch Speakers: Terri Lopez, HIV Surveillance
HIV and STD Integration: Using Data to Power the Program Focus: Prevention and Surveillance Moderator: Romni Neiman, MPH, Assistant Branch Chief, CDPH STD Control Branch Speakers: Terri Lopez, HIV Surveillance
HIV Partner Services in HIV Care Programs
 Welcome HIV Partner Services in HIV Care Programs Building the Care Continuum: Comprehensive Approaches to HIV Care in California Manny Rios HIV Partner Services Specialist CDPH: Office of AIDS Brett AugsJoost
Welcome HIV Partner Services in HIV Care Programs Building the Care Continuum: Comprehensive Approaches to HIV Care in California Manny Rios HIV Partner Services Specialist CDPH: Office of AIDS Brett AugsJoost
SECTION 11 IMMUNIZATION WORK PLANS
 SECTION 11 IMMUNIZATION WORK PLANS Table of Contents 1.0 ALL NURSES WHO ARE AUTHORIZED TO PROVIDE IMMUNIZATION IN THE YUKON WILL MAINTAIN COMPETENCE IN IMMUNIZATION AND ADHERE, TO ALL COLDS CHAIN PROCEDURES...
SECTION 11 IMMUNIZATION WORK PLANS Table of Contents 1.0 ALL NURSES WHO ARE AUTHORIZED TO PROVIDE IMMUNIZATION IN THE YUKON WILL MAINTAIN COMPETENCE IN IMMUNIZATION AND ADHERE, TO ALL COLDS CHAIN PROCEDURES...
Emergency, Community and Health Outreach
 ECHO Q&A Emergency, Community and Health Outreach Draft 4 FINAL DRAFT June 16, 2009 ECHO Questions and Answers 10 Minute Conversation STD Prevention and Treatment GUEST: Please modify question #2 for your
ECHO Q&A Emergency, Community and Health Outreach Draft 4 FINAL DRAFT June 16, 2009 ECHO Questions and Answers 10 Minute Conversation STD Prevention and Treatment GUEST: Please modify question #2 for your
Cost-effectiveness of Hepatitis A and Hepatitis B Vaccination for Jail Inmates
 Yale University EliScholar A Digital Platform for Scholarly Publishing at Yale Yale Medicine Thesis Digital Library School of Medicine 2007 Cost-effectiveness of Hepatitis A and Hepatitis B Vaccination
Yale University EliScholar A Digital Platform for Scholarly Publishing at Yale Yale Medicine Thesis Digital Library School of Medicine 2007 Cost-effectiveness of Hepatitis A and Hepatitis B Vaccination
Action Item for 2019 Review of Tool. Maintain (add include oral cavity) Maintain. Archive. Archive. 12 creatinine)
 Maintain. Archive. Archive. 12 creatinine)") NEWLY DIAGNOSED/ NEW TO CARE PROGRAM SITE: REVIEWER(S): REVIEW DATE: CORE SERVICES Outpatient/Ambulatory Health Services Tool - 2018 (OLD) SECTION 1: CHART REVIEW Review for newly diagnosed HIV patients
NEWLY DIAGNOSED/ NEW TO CARE PROGRAM SITE: REVIEWER(S): REVIEW DATE: CORE SERVICES Outpatient/Ambulatory Health Services Tool - 2018 (OLD) SECTION 1: CHART REVIEW Review for newly diagnosed HIV patients
THE CENTER FOR ADVANCED REPRODUCTIVE SERVICES (CARS) (The Center) CONSENT TO PERFORM THERAPEUTIC DONOR INSEMINATION WITH IDENTIFIED DONOR SPERM
 (The Center) CONSENT TO PERFORM THERAPEUTIC DONOR INSEMINATION WITH IDENTIFIED DONOR SPERM") THE CENTER FOR ADVANCED REPRODUCTIVE SERVICES (CARS) (The Center) CONSENT TO PERFORM THERAPEUTIC DONOR INSEMINATION WITH IDENTIFIED DONOR SPERM Partner #1 Last Name (Surname): Partner #1 First Name: Partner
THE CENTER FOR ADVANCED REPRODUCTIVE SERVICES (CARS) (The Center) CONSENT TO PERFORM THERAPEUTIC DONOR INSEMINATION WITH IDENTIFIED DONOR SPERM Partner #1 Last Name (Surname): Partner #1 First Name: Partner
Opportunities and Challenges for HIV and STD Data Sharing: Data to Care Realities PLENARY 4 11/28/2017
 Opportunities and Challenges for HIV and STD Data Sharing: Data to Care Realities PLENARY 4 11/28/2017 Julie Arena, J.D. Health Program Specialist, CDPH Office of AIDS Will Wheeler, Ph.D., MPH Clinical
Opportunities and Challenges for HIV and STD Data Sharing: Data to Care Realities PLENARY 4 11/28/2017 Julie Arena, J.D. Health Program Specialist, CDPH Office of AIDS Will Wheeler, Ph.D., MPH Clinical
PrEP for HIV Prevention. Adult Clinical Guideline from the New York State Department of Health AIDS Institute
 PrEP for HIV Prevention Adult Clinical Guideline from the New York State Department of Health AIDS Institute www.hivguidelines.org Purpose of the PrEP Guideline Raise awareness of PrEP among healthcare
PrEP for HIV Prevention Adult Clinical Guideline from the New York State Department of Health AIDS Institute www.hivguidelines.org Purpose of the PrEP Guideline Raise awareness of PrEP among healthcare
MANITOBA HIV REPORT 2015
 MANITOBA HIV REPORT 2015 The Manitoba HIV Program provides information, specialized care, treatment, and support to approximately 1,250 people living with HIV across the province. The Program has two Winnipeg-based
MANITOBA HIV REPORT 2015 The Manitoba HIV Program provides information, specialized care, treatment, and support to approximately 1,250 people living with HIV across the province. The Program has two Winnipeg-based
Epidemiology of Acute Hepatitis C Infection in Canada Results from the Enhanced Hepatitis Strain Surveillance System (EHSSS)
") Epidemiology of Acute Hepatitis C Infection in Canada Results from the Enhanced Hepatitis Strain Surveillance System (EHSSS) At a Glance Reported rates of acute HCV declined from.5 per, population in to.
Epidemiology of Acute Hepatitis C Infection in Canada Results from the Enhanced Hepatitis Strain Surveillance System (EHSSS) At a Glance Reported rates of acute HCV declined from.5 per, population in to.
School Nursing and Health. Standard Precautions. (aka Universal Precautions)
") School Nursing and Health Standard Precautions (aka Universal Precautions) August 2016 1 Standard Precautions Occupational Safety and Health Administration Federal Law 29 CFR bloodborne Pathogens 1910.1030(g)(2)(i)
School Nursing and Health Standard Precautions (aka Universal Precautions) August 2016 1 Standard Precautions Occupational Safety and Health Administration Federal Law 29 CFR bloodborne Pathogens 1910.1030(g)(2)(i)
Nursing and Midwifery students only. Section 1: Information
 Nursing and Midwifery students only. Section 1: Information Students enrolled in programs offered by our School are REQUIRED to provide evidence of their immunisation status for the diseases listed in
Nursing and Midwifery students only. Section 1: Information Students enrolled in programs offered by our School are REQUIRED to provide evidence of their immunisation status for the diseases listed in
City and County of Denver Sexually Transmitted Infections Surveillance Report 2005
 City and County of Denver Sexually Transmitted Infections Surveillance Report 2005 Denver Public Health Department Sexually Transmitted Disease Control Program November 2006 This report was prepared by:
City and County of Denver Sexually Transmitted Infections Surveillance Report 2005 Denver Public Health Department Sexually Transmitted Disease Control Program November 2006 This report was prepared by:
INFECTIOUS SYPHILIS NOTIFICATION FORM
 INFECTIOUS SYPHILIS NOTIFICATION FORM This is a Schedule 1, Section C disease notifiable to the Medical Officer of Health under Sections 74 and 74AA of the Health Act 1956 using non-identifiable data.
INFECTIOUS SYPHILIS NOTIFICATION FORM This is a Schedule 1, Section C disease notifiable to the Medical Officer of Health under Sections 74 and 74AA of the Health Act 1956 using non-identifiable data.
Bloodborne Pathogens. Post-Exposure Incident Packet. An Informational Guide
 Bloodborne Pathogens Post-Exposure Incident Packet An Informational Guide Faribault Public Schools Bloodborne Pathogens Post-Exposure Incident Packet This packet has been developed as an informational
Bloodborne Pathogens Post-Exposure Incident Packet An Informational Guide Faribault Public Schools Bloodborne Pathogens Post-Exposure Incident Packet This packet has been developed as an informational
All four components must be present, but Part A funds to be used for HIV testing only as necessary to supplement, not supplant, existing funding.
 EARLY INTERVENTION SERVICES I. DEFINITION OF SERVICE Support of Early Intervention Services (EIS) that include identification of individuals at points of entry and access to services and provision of:
EARLY INTERVENTION SERVICES I. DEFINITION OF SERVICE Support of Early Intervention Services (EIS) that include identification of individuals at points of entry and access to services and provision of:
Evidence Summary Title: Abstinence-plus HIV prevention programs in high-income countries: Evidence and implications for public health
 Date this evidence summary was written: January 2010 Evidence Summary Title: Abstinence-plus HIV prevention programs in high-income countries: Evidence and implications for public health Quality Assessment
Date this evidence summary was written: January 2010 Evidence Summary Title: Abstinence-plus HIV prevention programs in high-income countries: Evidence and implications for public health Quality Assessment
What you need to know to: Keep Yourself SAFE!
 What you need to know to: Keep Yourself SAFE! What are sexually transmitted diseases (STDs)? How are they spread? What are the different types of STDs? How do I protect myself? STDs are infections or diseases
What you need to know to: Keep Yourself SAFE! What are sexually transmitted diseases (STDs)? How are they spread? What are the different types of STDs? How do I protect myself? STDs are infections or diseases
Here are a few resources you may want to refer to in order to learn more about Applied Behaviour Analysis (ABA) and our program:
 and our program:") Dear Parent/Guardian: Thank you for your interest in the St.Amant Autism Programs. Please find enclosed is the application package for the St.Amant Autism Early Learning Program. Here are a few resources
Dear Parent/Guardian: Thank you for your interest in the St.Amant Autism Programs. Please find enclosed is the application package for the St.Amant Autism Early Learning Program. Here are a few resources
Syphilis Outbreak Investigation Report
 ` Office of the Chief Medical Officer of Health Syphilis Outbreak Investigation Report Office of the Chief Medical Officer of Health Health il 2014 Table of Contents Summary... 1 Acronyms... 1 Introduction...
` Office of the Chief Medical Officer of Health Syphilis Outbreak Investigation Report Office of the Chief Medical Officer of Health Health il 2014 Table of Contents Summary... 1 Acronyms... 1 Introduction...
Chapter 5 Serology Testing
 Chapter 5 Serology Testing 49 50 This page intentionally left blank. Diagnostic Tests for Hepatitis B Virus (HBV) Diagnosis of HBV infection (acute vs. chronic) is based on clinical, laboratory, and epidemiologic
Chapter 5 Serology Testing 49 50 This page intentionally left blank. Diagnostic Tests for Hepatitis B Virus (HBV) Diagnosis of HBV infection (acute vs. chronic) is based on clinical, laboratory, and epidemiologic
The new German strategy on HIV, Hepatitis B, C and STI, an integrated approach. Ines Perea Ministry of Health, Germany
 The new German strategy on HIV, Hepatitis B, C and STI, an integrated approach Ines Perea Ministry of Health, Germany Reasons for a new strategy in 2016 New international agreements (SDG s) Renewed political
The new German strategy on HIV, Hepatitis B, C and STI, an integrated approach Ines Perea Ministry of Health, Germany Reasons for a new strategy in 2016 New international agreements (SDG s) Renewed political
The Hepatitis C Action Plan for Scotland: Draft Guidelines for Hepatitis C Care Networks
 The Hepatitis C Action Plan for Scotland: Draft Guidelines for Hepatitis C Care Networks Royal College of Physicians of Edinburgh Friday 12 October 2007 CONTENTS 1.0 ACCOUNTABILITY AND ORGANISATION 2.0
The Hepatitis C Action Plan for Scotland: Draft Guidelines for Hepatitis C Care Networks Royal College of Physicians of Edinburgh Friday 12 October 2007 CONTENTS 1.0 ACCOUNTABILITY AND ORGANISATION 2.0
Becoming a harm reduction distribution agency in Toronto - information session
 Becoming a harm reduction distribution agency in Toronto - information session Kris Guthrie, RN BScN Health Promotion Specialist, The Works Toronto Public Health May 2016 Overview Brief backgrounder Harm
Becoming a harm reduction distribution agency in Toronto - information session Kris Guthrie, RN BScN Health Promotion Specialist, The Works Toronto Public Health May 2016 Overview Brief backgrounder Harm
Sexually Transmitted Infections. Kim Dawson October 2010
 Sexually Transmitted Infections Kim Dawson October 2010 Objectives: You will learn about: Sexually Transmitted Infections (STI s). How they are transferred. High risk behavior. The most common STI s. How
Sexually Transmitted Infections Kim Dawson October 2010 Objectives: You will learn about: Sexually Transmitted Infections (STI s). How they are transferred. High risk behavior. The most common STI s. How
Teacher Resource: Anecdotal Recording Chart. Class: Specific Expectations: Success Criteria: (Page 1 of 2) Student Name. Observation.
 Student Name. Observation.") Teacher Resource: Anecdotal Recording Chart (Page 1 of 2) Class: Specific Expectations: Success Criteria: Student Name Observation Student Name Observation Student Name Observation Teacher Resource: Anecdotal
Teacher Resource: Anecdotal Recording Chart (Page 1 of 2) Class: Specific Expectations: Success Criteria: Student Name Observation Student Name Observation Student Name Observation Teacher Resource: Anecdotal
AIDS and insurance. Information about the necessity of AIDS testing Implications of undergoing an AIDS test The choices available to you INSURANCE
 INSURANCE AIDS and insurance Information about the necessity of AIDS testing Implications of undergoing an AIDS test The choices available to you Please read carefully NSW and TAS only What is AIDS? AIDS
INSURANCE AIDS and insurance Information about the necessity of AIDS testing Implications of undergoing an AIDS test The choices available to you Please read carefully NSW and TAS only What is AIDS? AIDS
San Francisco Department of Public Health Program Collaboration and Service Integration Surveillance Baseline Assessment
 Background and Purpose San Francisco Department of Public Health This syndemics assessment is the first step in developing a sustainable system of primary prevention and clinical care in San Francisco
Background and Purpose San Francisco Department of Public Health This syndemics assessment is the first step in developing a sustainable system of primary prevention and clinical care in San Francisco
OF THE REPUBLIC OF ARMENIA DECREE. 316 of 1 April 2002 Yerevan
 Ratified President of the Republic of Armenia R. Kocharyan 1 April 2002 GOVERNMENT OF THE REPUBLIC OF ARMENIA DECREE 316 of 1 April 2002 Yerevan On ratification of the National Programme on HIV/AIDS Prevention
Ratified President of the Republic of Armenia R. Kocharyan 1 April 2002 GOVERNMENT OF THE REPUBLIC OF ARMENIA DECREE 316 of 1 April 2002 Yerevan On ratification of the National Programme on HIV/AIDS Prevention
HIV AIDS and Other Infectious Diseases
 HIV AIDS and Other Infectious Diseases Multiple Choice Identify the choice that best completes the statement or answers the question. 1. Chapter 1 - Introduction Despite the availability of a vaccine since
HIV AIDS and Other Infectious Diseases Multiple Choice Identify the choice that best completes the statement or answers the question. 1. Chapter 1 - Introduction Despite the availability of a vaccine since
The HIV testing process
 FACTSHEET The HIV testing process Summary There are a few steps that a person will take in the HIV testing process. To access an HIV test, people can request a test or may be offered a test. There are
FACTSHEET The HIV testing process Summary There are a few steps that a person will take in the HIV testing process. To access an HIV test, people can request a test or may be offered a test. There are
2018 POLQM Conference
 Lower Mainland Pathology & Laboratory Medicine 2018 POLQM Conference Medical Laboratory Quality Improvement: Knowing your customers A storytelling session Lower Mainland Pathology and Laboratory Medicine
Lower Mainland Pathology & Laboratory Medicine 2018 POLQM Conference Medical Laboratory Quality Improvement: Knowing your customers A storytelling session Lower Mainland Pathology and Laboratory Medicine
Diabetes in Manitoba: Trends among Adults
 Diabetes Among Adults in Manitoba (1989-2013) Diabetes in Manitoba: Trends among Adults 1989-2013 1989-2013 Epidemiology & Surveillance Active Living, Population and Public Health Branch Manitoba Health,
Diabetes Among Adults in Manitoba (1989-2013) Diabetes in Manitoba: Trends among Adults 1989-2013 1989-2013 Epidemiology & Surveillance Active Living, Population and Public Health Branch Manitoba Health,
THE POWER OF UNDETECTABLE. What you need to know about HIV treatment as prevention
 THE POWER OF UNDETECTABLE What you need to know about HIV treatment as prevention CONTENTS 3 Treatment as prevention First, a few basics: What is an undetectable viral load? How do I know if I m undetectable?
THE POWER OF UNDETECTABLE What you need to know about HIV treatment as prevention CONTENTS 3 Treatment as prevention First, a few basics: What is an undetectable viral load? How do I know if I m undetectable?
Operational Guideline
 1 of 6 PURPOSE Prevention of the spread of sexually transmitted and blood-borne infections (STBBI) through distribution of harm reduction supplies SCOPE & GOAL Harm reduction supplies and condoms will
1 of 6 PURPOSE Prevention of the spread of sexually transmitted and blood-borne infections (STBBI) through distribution of harm reduction supplies SCOPE & GOAL Harm reduction supplies and condoms will
Sexually Transmitted Infections. Naluce Manuela Morris, MPH, CHES
 Sexually Transmitted Infections Naluce Manuela Morris, MPH, CHES Handshake Activity Handshake Activity Mrs. or Mr. X Mrs. or Mr. Y Carry this glove but do not put it on Put this glove on before shaking
Sexually Transmitted Infections Naluce Manuela Morris, MPH, CHES Handshake Activity Handshake Activity Mrs. or Mr. X Mrs. or Mr. Y Carry this glove but do not put it on Put this glove on before shaking
For People Who Have Been Sexually Assaulted... What You Need To Know about STDs and Emergency Contraception
 For People Who Have Been Sexually Assaulted... What You Need To Know about STDs and Emergency Contraception FOR PEOPLE WHO HAVE BEEN SEXUALLY ASSAULTED What You Need to Know about STDs and Emergency Contraception
For People Who Have Been Sexually Assaulted... What You Need To Know about STDs and Emergency Contraception FOR PEOPLE WHO HAVE BEEN SEXUALLY ASSAULTED What You Need to Know about STDs and Emergency Contraception
Questions may be directed totamara Chipperfield, Director of Mental Health and Addictions
 Position Title: Classification: Department: Reporting to: Type: Location: Harm Reduction Peer Worker Support Worker ($20.26 - $24.40 per hour) Harm Reduction Practice Facilitator, Harm Reduction Contract/Term
Position Title: Classification: Department: Reporting to: Type: Location: Harm Reduction Peer Worker Support Worker ($20.26 - $24.40 per hour) Harm Reduction Practice Facilitator, Harm Reduction Contract/Term
GLOBAL AIDS MONITORING REPORT
 KINGDOM OF SAUDI ARABIA MINISTRY OF HEALTH GLOBAL AIDS MONITORING REPORT COUNTRY PROGRESS REPORT 2017 KINGDOM OF SAUDI ARABIA Submission date: March 29, 2018 1 Overview The Global AIDS Monitoring 2017
KINGDOM OF SAUDI ARABIA MINISTRY OF HEALTH GLOBAL AIDS MONITORING REPORT COUNTRY PROGRESS REPORT 2017 KINGDOM OF SAUDI ARABIA Submission date: March 29, 2018 1 Overview The Global AIDS Monitoring 2017
Student Immunisation Record Faculty of Medicine. Section 1: Information. Notes
 Student Immunisation Record Faculty of Section 1: Information Students enrolled in programs offered by the Faculty of are REQUIRED to provide evidence of their immunisation status for the diseases listed
Student Immunisation Record Faculty of Section 1: Information Students enrolled in programs offered by the Faculty of are REQUIRED to provide evidence of their immunisation status for the diseases listed
Section 5. Study Procedures
 Section 5. Study Procedures 5. Introduction 5-1 5.1 Visit Locations... 5-1 5.2 Eligibility Determination SOP... 5-1 5.3 Screening Visit... 5-2 5.3.1 Screening and Enrollment Timeframe... 5-2 5.3.2 Screening
Section 5. Study Procedures 5. Introduction 5-1 5.1 Visit Locations... 5-1 5.2 Eligibility Determination SOP... 5-1 5.3 Screening Visit... 5-2 5.3.1 Screening and Enrollment Timeframe... 5-2 5.3.2 Screening
Answers to those burning questions -
 Answers to those burning questions - Ann Avery MD Infectious Diseases Physician-MetroHealth Medical Center Assistant Professor- Case Western Reserve University SOM Medical Director -Cleveland Department
Answers to those burning questions - Ann Avery MD Infectious Diseases Physician-MetroHealth Medical Center Assistant Professor- Case Western Reserve University SOM Medical Director -Cleveland Department