PULMONARY INFECTIONS IN HEMATOLOGICAL MALIGNANCIES & POST STEM CELL TRANSPLANT SETTING Dr. Zia Hashim
|
|
|
- Theodore Carson
- 6 years ago
- Views:
Transcription
1 PULMONARY INFECTIONS IN HEMATOLOGICAL MALIGNANCIES & POST STEM CELL TRANSPLANT SETTING Dr. Zia Hashim
2 Hemopoietic stem cell transplant Types: Allogenic Autologous Source: Bone marrow Peripheral blood after priming with G-CSF Umbilical cord
3 Process Conditioning of recipient: high dose chemotherapy ± total body irradiation Infusion of stem cells Engraftment: ANC>500/cc and sustained platelet count >20,000/cc that lasts for 3 consecutive days without transfusions 3 weeks after HSCT
4 Immunosuppressive therapy After allogenic transplantation For GVHD prophylaxis Methotrexate Cyclosporin
5 Division of post-transplant period phase 1 (the first 30 days) Prolonged neutropenia: less severe in autologous SCT Disruption of mucosal barriers following cytoablative therapy phase 2 (Days 31 to 100): depressed cell mediated and humoral immunity phase 3 (more than100 days): chronic GVHD and GVHD prophylaxis
6 Phase 1 Gram-negative bacilli, Streptococci Staphylococcus epidermidis, Aspergillus spp Candida spp HSV NON INFECTIOUS Pulmonary edema DAH Drug reactions
7 Phase 2 S epidermidis, Aspergillus spp, Candida spp CMV EBV Pneumocystis jirovecii NON INFECTIOUS Idiopathic pneumonia syndrome Drug reactions
8 Phase 3 VZV Encapsulated bacteria Tuberculosis NTM Nocardia NON INFECTIOUS Bronchiolitis obliterans BOOP Chronic GVHD Secondary malignancies
9
10 Bacterial infections Neutropenia: bacteremia Mucositis and use of opiates predispose to aspiration Corticosteroid therapy used to treat Acute GVHD Use of various intravascular devices
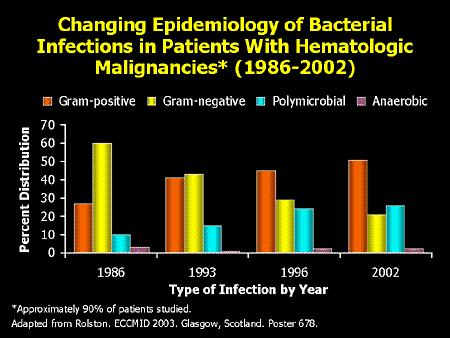
11 Bacterial infections Increase in gram-positive and polymicrobial(3x) infections Decrease in documented gram-negative infections from 60% in 1986 to 21% in 2002 Escherichia coli, Pseudomonas aeruginosa, and Klebsiella spp : constant Increase in percent of MRSA infection over the time Progressive rise in rate of resistance of enterococci to vancomycin
12
13 Aspergillosis Bimodal onset: 1 st peak median 16 d 2 nd peak median 96 d Symptoms triad: dyspnea, pleuritic chest pain, and hemoptysis Diagnostic yield of FOB low: <50% To distinguish infection from contamination, lavage from affected area may be compared with unaffected area

14
15
16 CT scan dense, well-circumscribed pulmonary infiltrate halo sign : present in all on day 0 22% by day 7 "crescent sign" (an air crescent caused by contracting infarcted tissue): appears day 3 28% day 7 63% day 14
17 Airway-invasive aspergillosis Patchy, peribronchial consolidation Small ill defined nodules centrilobular nodules or tree-in-bud GGO Lobar consolidation Yield of BAL high
18 Galactomannan assay Early detection: even before clinical features Sensitive (80%) and specific (90%) Negative test does not rule out and positive test should be judged in clinical setting Check same specimen: if first sample + follow with 2 nd specimen before therapy
19 Galactomannan assay When to use: pts at increased risk? biweekly monitor assess response to Rx False +ve Children Allo SCT (1 st 2wks) Piperacillin-Tazobactam Patients on antifungal Rx/Px: false ve Urine: lower sensitivity than serum
20 Treatment of fungal infections Definite: proven infection Empiric treatment: fever+neutropenia+ no response to proper antibiotics Pre-emptive Rx: similar to empiric + increased evidence of infection Prophylaxis
21 Voriconazole vs AmB Randomized, unblinded, multicenter trial Definite or probable aspergillosis n=277 Complete or partial response Voriconazole: 53% Amphotericin B: 32% Statistically significant difference 21% Significant difference in survival Fewer adverse effects in Voriconazole group Herbrect et al. NEJM 2002
22
23 Empiric antifungal therapy: is Amphotericin the only answer? open, randomized, controlled, multicenter trial 384 neutropenic patients with cancer and persistent fever unresponsive to antibiotics Itraconazole safe and effective as empirical therapy for suspected invasive fungal infection in febrile neutropenic patients Boogerts et al. Ann Int Med 2001 Voriconazole, Lipid AmB, Capsofungins: have not demonstrated complete success as empiric Rx
24 Candida 50% of disseminated disease have pulmonary involvement Symptoms of pulmonary involvement are cough, purulent expectoration, hemoptysis Most important clue is the presence of disseminated disease
25 Radiology U/L or B/L segmental or non-segmental consolidation Diffuse nodules, rarely miliary Pleural effusion 20% Screening scan for hepatosplenic candidiasis
26 Treatment Amphotericin B (AmB) ( mg/kg/day) Fluconazole (400 mg/day) Candida glabrata: resistant; HIGH DOSE AmB (0.7 mg/kg/day) C krusei > 1 mg/kg/d AmB Caspofungin Voriconazole Itraconazole?
27 Fluconazole prophylaxis 356 autologous and allogeneic HSCT Fluconazole (400 mg/day) vs placebo From the start of the conditioning period for a maximum of 10 weeks Systemic fungal infections: 3% vs 16% Fewer infection related deaths No effect on overall mortality Goodman et al. NEJM 1992 Fluconazole (400 mg/day for 75 days) does improve overall survival Slavin et al. J Infect Ds 1995

28
29 Zygomycosis Much less common than aspergillosis Occur in allograft patients during preengraftment or with corticosteroid therapy used to treat GVHD. Treatment is highest tolerable dose of AmB Voriconazole is not effective
30 Known gaps in antifungal coverage Fluconazole AmB Capsofungin Voriconazole C glabrata dose depedent C krusei Aspergillus terreus Fusarium, Scedoporium Cryptococcus Zygomycetes
31 Pneumocystis jirovecii Median time of onset: 60 d from Tx HRCT findings: Patchy or diffuse B/L GGO Central, perihilar or upper lobe prominence Thick walled, irregular septated cavities; thin walled cysts Pneumothorax related to cysts Bronchiectasis or bronchiolectasis
32 Pneumocystis jirovecii Diagnosis by BAL in 90%; obviating need of biopsy Role of adding steroids is not as clear as in patients with AIDS Rx: TMP 5 mg/kg-smx 25 mg/kg tds or Clinda 300mg qid + Primaquin 15mg OD
33 Herpes simplex pneumonitis Most common early infection Pulmonary involvement: 5-7% Herpes tracheitis or esophagitis commonly associated Unexplained pulmonary infiltrates along with mucocutaneous lesions: Tzanck smear BAL specimen alone may not be diagnostic: generous tissue biopsy is required
34 HSV Rx Aciclovir: 5-10 mg/kg TDS Resistant to Aciclovir: Foscarnet 60 mg/kg TDS Duration: d Prophylaxis (until engraftment): Aciclovir mg QID po 250 mg/m 2 TDS iv (severe mucositis) 500 mg/m 2 TDS for CMV+HSV
35 CMV Pneumonitis 6-12 wks post SCT; 90% within 100 d; later if Ganciclovir prophylaxis is used More common after allogenic transplants Fever, dry cough, dyspnea, and hypoxemia with diffuse interstitial infiltrates on CXR Other clues: vasculitis, esophagitis, retinitis, atypical lymphocytosis, leukopenia, thrombocytopenia
36 HRCT in CMV Patchy B/L foci of GGO Scattered poorly defined nodules Reticulation and septal thickening (resolving disease) Predilectation to lower lobes
37 CMV Diagnostic tests Serology: to evaluate the patient prior to transplantation Conventional cell culture: result by day 11 Shell vial culture: rapid results on day 2 Antigenemia (pp65): Direct fluorescent Ag detection. Requires enough no. of cells CMV DNA PCR BMT recipient CMV DNA, PCR is very useful for monitoring patients and the full risk stratification. Positive results in quantitative
38 Rx of CMV Pneumonitis Ganciclovir: 5 mg/kg BD + CMV hyperimmuneglobulin for 6 wks Maintainence therapy: Ganciclovir 6 mg/kg 5 times/wk Foscarnet 90 mg/kg 5 times/wk Prophylaxis: Started after engraftment Ganciclovir 5 mg/kg BD for 7 d 6 mg/kg 5 times/wk until day 100
39 Community respiratory viruses Increased morbidity and mortality in HSCT/hematological malignancies during community outbreaks RSV 35% Influenza 11% Parainfluenza 30% Rhinovirus 25%
40 RSV High proportion of LRTI Typically occurs in winters Mortality up to 100% Rx: Aerosolized ribavirin with IVIG Role of pre-emptive therapy with aerosolized ribavirin in patients with RSV +ve culture
41 Post Transplant Lymphoproliferative Syndrome Incidence: 1.5% Occur almost exclusively after allogenic SCT T cell depletion: ex-vivo of allograft and in-vivo following anti T-cell therapy for GVHD polyclonal expansion of B cells infected with EBV HRCT: multiple nodules peribronchial, subpleural + lymphadenopathy Rx: Humanized anti-cd 20 monoclonal antibody (Rituximab)
42 Tuberculosis post SCT Incidence from India? Risk factors Allogenic HSCT Total Body Irradiation Chronic GVHD Median time to onset: 150d & 324d in 2 series 20 cases of post SCT TB out of total 8013 de la Camara et al. BMT 2000

43
44 Important Non-infectious D/Ds
45 Pulmonary edema Onset rapid: 2 nd / 3 rd week post Tx Clinical features: orthopnea, wt gain, crackles Accompanying hepatic and renal dysfunction Radiological: enlarged pulm vs, smooth interlobular septal thickening, smooth peribronchovascular interstitial thickening, smooth subpleral or fissure thickening, patchy GGO Response to diuretics
46 Septic pulmonary emboli Setting: intra-vascular catheters HRCT: B/L peripheral nodules in varying stages of cavitation Peripheral wedge shaped triangular opacities abutting pleural surfaces with/without cavitation Associated pleural and/or pericardial effusion
47 Diffuse Alveolar Hemorrhage More common after autologous SCT Onset: 12 d (7-40 d) B/L GGO patchy or confluent air space consolidation involving perihilar or lower lung zones Successive aliquots of BAL fluid become increasingly hemorrhagic Drop in Hb
48 Engraftment syndrome Autologous BMT and peripheral stem cell transplantation Symptoms within 5 days after attaining an absolute neutrophil count that is greater than 500 The median time of onset was 7 days after BMT, with a median duration of 11 days. Fever, pulmonary infiltrates, skin rash, and hypoxia
49 Idiopathic pneumonia syndrome Incidence: 10% Median time: 2-7 wks B/L interstitial thickening associated with GGO and poorly defined small nodular opacities KL-6 mucinous HMW glycoprotein is elevated in BAL and serum
50 TBI and Drug Reactions Usually present within 90 d Fever, cough, dyspnea, hypoxemia Diffuse interstitial infiltrates Methotrexate: intestitial pneumonitis eosinophilic pneumonia
51 FOB Evaluation of pulmonary infiltrates which cannot be identified by imaging, microbiology Non responsive to antimicrobial therapy Findings at FOB provide specific diagnosis in appx 50% of allogenic HSCT TBLB adds to specific diagnosis in <10% Bronchoscopy led to change in treatment in 50% Establishing a specific diagnosis by FOB does not improve survival Naimish et al. Chest April 2005
52 Preparation from BAL samples Gram stain Giemsa (assessment of macrophages, ciliated epithelium, leucocytes) Calcofluor white (fungus & Pneumocystis) DIFT for Pneumocystis Stain for AFB Cytospin: for underlying malignancy
53 Transthoracic needle aspiration W/U of peripheral radiological abnormalities Positive diagnosis: 70% Correct diagnosis of fungal ds: 65% But there is possibility of missing fungal disease: 35% Most common complication: Pneumothorax (13-25%)
54 OLB In pts with diffuse infiltrates: OLB required when BAL is non diagnostic or technically impossible Suspected invasive aspergillosis: however false negative in 20% Non infectious lung infiltrates Severe thrombocytopenia: Platelet count <50,000 Complications: 10-15% 2 scenarios where OLB is beneficial BOOP Discrete solitary pulmonary nodule
55 D/D of consolidation Pseudomonas and E. coli : airspace consolidation with a patchy bronchopneumonic pattern Klebsiella and Enterobacter: confluent consolidation occupying a segment or lobe; bulging of the interlobar fissure Staph aureus: patchy consolidation in a bronchopneumonic pattern, bilateral; lung abscesses may develop in areas of consolidation where necrosis has occurred. Pneumatoceles
56 Consolidation Legionella pneumophilia: multilobar consolidation, nodules Malignancies: segmental or lobar consolidation, often with prominent air bronchograms. Focal infiltrates may also arise from leukemic deposits Haemorrhage: widespread consolidation ARDS(sepsis, cytotoxic drug rxn): widespread consolidation Peripheral, subpleural: Plum infarction, Drug rxn
57 GGO HSV CMV Pneumocystis BOOP Pulmonary edema DAH Idiopathic Pneumonia Syndrome Lymphoproliferative disorder
58 Nodules Aspergillosis: centrilobular with tree in bud Mucormycosis Tuberculosis; NTM Pulmonary edema: centrilobular without tree-inbud Lymphoproliferative disorder: perilymphatic Septic emboli Disseminated viral infection
59 Interlobular septal thickening Pulmonary edema: smooth Lymphoproliferative disorder: smooth/nodular Pneumocystis jirovecii
60 Infections in CLL Multifactorial pathogenesis Hypogammaglobinemia Decreased CMI Granulocytopenia -leukemic marrow -drug induced Increased incidence with -disease progression -repeated thearapy
61 Conventional therapies Chlorambucil, COP, CHOP Myelosuppression -Pneumonia most common and most severe -Bacteremia occurs with neutropenia -S pneumoniae > S aureus > H influenzae > Legionella > Salmonella - Localized Herpes common -Rare: Mycobacteria, fungi
62 Nucleoside analogs: Fludarabine Major infections 50% FUO 25% Pneumonia 24% Atypical: PCJ, TB, Listeria 5% Sepsis 11% Gm+ 5% Gm- 6% Others: Viral CMV, Herpes
63 Rituximab Profound B cell depletion Little effect on Ig or complement Occasional, mild neutropenia Infections mild responsive to Rx combination with Fludarabine increase in neutropenia no increased risk of infection
64 Alemtuzumab Monoclonal antibody specifically directed against CD52 This Ag is present on lymphocytes T and B and/or monocytes Results in profound prolonged lymphopenia CD4 comes back to normal in 2 years Decrease in NK-cell cytotoxicity
65 Infections in CLL treated with Alemtuzumab Untreated: Alemtuzumab well tolerated Previously treated: increased risk of infection Bacterial pneumonia, bacteremia Viral: HSV, VZV, CMV (20%) Pneumocystosis, fungal & mycobacterial
66 Infections in Multiple Myeloma Defects in humoral immunity Infection is the most common cause of death Early: S pneumoniae and other encapsulated bacteria Later: GNB and S aureus
67 Lymphoma Defect in T cell function Chemotherapy Steroids Intracellular pathogens: -Mycobacterium tuberculosis, M avium -Cryptococcosis -Listeria -Salmonella
68 Thank you!
Hospital-acquired Pneumonia
 Hospital-acquired Pneumonia Hospital-acquired pneumonia (HAP) Pneumonia that occurs at least 2 days after hospital admission. The second most common and the leading cause of death due to hospital-acquired
Hospital-acquired Pneumonia Hospital-acquired pneumonia (HAP) Pneumonia that occurs at least 2 days after hospital admission. The second most common and the leading cause of death due to hospital-acquired
Immunocompromised patients. Immunocompromised patients. Immunocompromised patients
 Value of CT in Early Pneumonia in Immunocompromised Patients Nantaka Kiranantawat, PSU Preventative Factors Phagocyts Cellular immunity Humoral immunity Predisposing Factors Infection, Stress, Poor nutrition,
Value of CT in Early Pneumonia in Immunocompromised Patients Nantaka Kiranantawat, PSU Preventative Factors Phagocyts Cellular immunity Humoral immunity Predisposing Factors Infection, Stress, Poor nutrition,
The Pulmonary Pathology of Iatrogenic Immunosuppression. Kevin O. Leslie, M.D. Mayo Clinic Scottsdale
 The Pulmonary Pathology of Iatrogenic Immunosuppression Kevin O. Leslie, M.D. Mayo Clinic Scottsdale The indications for iatrogenic immunosuppression Autoimmune/inflammatory disease Chemotherapy for malignant
The Pulmonary Pathology of Iatrogenic Immunosuppression Kevin O. Leslie, M.D. Mayo Clinic Scottsdale The indications for iatrogenic immunosuppression Autoimmune/inflammatory disease Chemotherapy for malignant
Complications after HSCT. ICU Fellowship Training Radboudumc
 Complications after HSCT ICU Fellowship Training Radboudumc Type of HSCT HSCT Improved outcome due to better HLA matching, conditioning regimens, post transplant supportive care Over one-third have pulmonary
Complications after HSCT ICU Fellowship Training Radboudumc Type of HSCT HSCT Improved outcome due to better HLA matching, conditioning regimens, post transplant supportive care Over one-third have pulmonary
Severe Viral Related Complications Following Allo-HCT for Severe Aplastic Anemia
 Severe Viral Related Complications Following Allo-HCT for Severe Aplastic Anemia Liat Shragian Alon, MD Rabin Medical Center, ISRAEL #EBMT15 www.ebmt.org Patient: 25-year-old male No prior medical history
Severe Viral Related Complications Following Allo-HCT for Severe Aplastic Anemia Liat Shragian Alon, MD Rabin Medical Center, ISRAEL #EBMT15 www.ebmt.org Patient: 25-year-old male No prior medical history
ESCMID Online Lecture Library. by author. CASE PRESENTATION ECCMID clinical grand round May Anat Stern, MD Rambam medical center Haifa, Israel
 CASE PRESENTATION ECCMID clinical grand round May 2014 Anat Stern, MD Rambam medical center Haifa, Israel An 18 years old Female, from Ukraine, diagnosed with acute lymphoblastic leukemia (ALL) in 2003.
CASE PRESENTATION ECCMID clinical grand round May 2014 Anat Stern, MD Rambam medical center Haifa, Israel An 18 years old Female, from Ukraine, diagnosed with acute lymphoblastic leukemia (ALL) in 2003.
Acute and Chronic Lung Disease
 KATHOLIEKE UNIVERSITEIT LEUVEN Faculty of Medicine Acute and Chronic Lung Disease W De Wever, JA Verschakelen Department of Radiology, University Hospitals Leuven, Belgium Clinical utility of HRCT To detect
KATHOLIEKE UNIVERSITEIT LEUVEN Faculty of Medicine Acute and Chronic Lung Disease W De Wever, JA Verschakelen Department of Radiology, University Hospitals Leuven, Belgium Clinical utility of HRCT To detect
Invasive Pulmonary Aspergillosis in
 Infection & Sepsis Symposium Porto, April 1-3, 2009 Invasive Pulmonary Aspergillosis in Non-Immunocompromised Patients Stijn BLOT, PhD General Internal Medicine & Infectious Diseases Ghent University Hospital,
Infection & Sepsis Symposium Porto, April 1-3, 2009 Invasive Pulmonary Aspergillosis in Non-Immunocompromised Patients Stijn BLOT, PhD General Internal Medicine & Infectious Diseases Ghent University Hospital,
Fungal Infections: Reporting. Marcie Tomblyn, MD, MS Associate Member, Moffitt Cancer Center
 Fungal Infections: Management and Reporting Marcie Tomblyn, MD, MS Associate Member, Moffitt Cancer Center February 25, 2010 Objectives Review common fungal infections in HCT patients Review current available
Fungal Infections: Management and Reporting Marcie Tomblyn, MD, MS Associate Member, Moffitt Cancer Center February 25, 2010 Objectives Review common fungal infections in HCT patients Review current available
HIV related pulmonary infections. A radiologic pictorial review.
 HIV related pulmonary infections. A radiologic pictorial review. Poster No.: C-0836 Congress: ECR 2013 Type: Educational Exhibit Authors: N. Arcalis, P. Trallero, L. Berrocal Morales, S. Medrano, S. 1
HIV related pulmonary infections. A radiologic pictorial review. Poster No.: C-0836 Congress: ECR 2013 Type: Educational Exhibit Authors: N. Arcalis, P. Trallero, L. Berrocal Morales, S. Medrano, S. 1
Radiological Imaging in pneumonia and its complications
 Radiological Imaging in pneumonia and its complications Cornelia Schaefer-Prokop Meander Medical Center Amersfoort Radboud University Nijmegen Netherlands Outline Radiographic patterns Infections in immunocompromised
Radiological Imaging in pneumonia and its complications Cornelia Schaefer-Prokop Meander Medical Center Amersfoort Radboud University Nijmegen Netherlands Outline Radiographic patterns Infections in immunocompromised
Uses, limitations and interpretation of CT in pulmonary infections: A practical approach
 Uses, limitations and interpretation of CT in pulmonary infections: A practical approach Canadian Association of Radiologists 2013 DISCLOSURES Speakers honorarium, Siemens Canada Objectives 1. Recognize
Uses, limitations and interpretation of CT in pulmonary infections: A practical approach Canadian Association of Radiologists 2013 DISCLOSURES Speakers honorarium, Siemens Canada Objectives 1. Recognize
Lung Injury after HCT
 Lung Injury after HCT J. Douglas Rizzo, MD, MS Financial Disclosure None SCS06_1.ppt Background HCT an important therapeutic modality for malignant and non-malignant diseases Pulmonary Toxicity common
Lung Injury after HCT J. Douglas Rizzo, MD, MS Financial Disclosure None SCS06_1.ppt Background HCT an important therapeutic modality for malignant and non-malignant diseases Pulmonary Toxicity common
2046: Fungal Infection Pre-Infusion Data
 2046: Fungal Infection Pre-Infusion Data Fungal infections are significant opportunistic infections affecting transplant patients. Because these infections are quite serious, it is important to collect
2046: Fungal Infection Pre-Infusion Data Fungal infections are significant opportunistic infections affecting transplant patients. Because these infections are quite serious, it is important to collect
PUO in the Immunocompromised Host: CMV and beyond
 PUO in the Immunocompromised Host: CMV and beyond PUO in the immunocompromised host: role of viral infections Nature of host defect T cell defects Underlying disease Treatment Nature of clinical presentation
PUO in the Immunocompromised Host: CMV and beyond PUO in the immunocompromised host: role of viral infections Nature of host defect T cell defects Underlying disease Treatment Nature of clinical presentation
Turkish Thoracic Society
 Türk Toraks Derneği Turkish Thoracic Society Turkish Thoracic Society Pocket Books Series Diagnosis and of Pneumonia in Immunocompromised Children Short Version (Handbook) in English www.toraks.org.tr
Türk Toraks Derneği Turkish Thoracic Society Turkish Thoracic Society Pocket Books Series Diagnosis and of Pneumonia in Immunocompromised Children Short Version (Handbook) in English www.toraks.org.tr
PROGRESSI NELLA TERAPIA ANTIFUNGINA. A tribute to Piero Martino
 PROGRESSI NELLA TERAPIA ANTIFUNGINA A tribute to Piero Martino 1946-2007 ITALIAN ICONS IERI, OGGI, E DOMANI IERI, OGGI, E DOMANI IERI, OGGI, E DOMANI 1961 CAUSES OF DEATH IN PATIENTS WITH MALIGNANCIES
PROGRESSI NELLA TERAPIA ANTIFUNGINA A tribute to Piero Martino 1946-2007 ITALIAN ICONS IERI, OGGI, E DOMANI IERI, OGGI, E DOMANI IERI, OGGI, E DOMANI 1961 CAUSES OF DEATH IN PATIENTS WITH MALIGNANCIES
Neutropenic Sepsis Guideline
 Neutropenic Sepsis Guideline Neutropenic Sepsis Guideline - definitions Suspected or proven infection in a neutropenic patient is a MEDICAL EMERGENCY and is an indication for immediate assessment and prompt
Neutropenic Sepsis Guideline Neutropenic Sepsis Guideline - definitions Suspected or proven infection in a neutropenic patient is a MEDICAL EMERGENCY and is an indication for immediate assessment and prompt
Surgical indications: Non-malignant pulmonary diseases. Punnarerk Thongcharoen
 Surgical indications: Non-malignant pulmonary diseases Punnarerk Thongcharoen Non-malignant Malignant as a pathological term: Cancer Non-malignant = not cancer Malignant as an adjective: Disposed to cause
Surgical indications: Non-malignant pulmonary diseases Punnarerk Thongcharoen Non-malignant Malignant as a pathological term: Cancer Non-malignant = not cancer Malignant as an adjective: Disposed to cause
Prophylaxis versus Diagnostics-driven approaches to treatment of Invasive fungal diseases. Y.L. Kwong Department of Medicine University of Hong Kong
 Prophylaxis versus Diagnostics-driven approaches to treatment of Invasive fungal diseases Y.L. Kwong Department of Medicine University of Hong Kong Pathogenic yeast Candida Cryptococcus Trichosporon Pathogenic
Prophylaxis versus Diagnostics-driven approaches to treatment of Invasive fungal diseases Y.L. Kwong Department of Medicine University of Hong Kong Pathogenic yeast Candida Cryptococcus Trichosporon Pathogenic
Case 1 : Question. 1.1 What is the intralobular distribution? 1. Centrilobular 2. Perilymphatic 3. Random
 Interesting case Case 1 Case 1 : Question 1.1 What is the intralobular distribution? 1. Centrilobular 2. Perilymphatic 3. Random Case 1: Answer 1.1 What is the intralobular distribution? 1. Centrilobular
Interesting case Case 1 Case 1 : Question 1.1 What is the intralobular distribution? 1. Centrilobular 2. Perilymphatic 3. Random Case 1: Answer 1.1 What is the intralobular distribution? 1. Centrilobular
Case 1: Question. 1.1 What is the main pattern of this HRCT? 1. Intralobular line 2. Groundglass opacity 3. Perilymphatic nodule
 HRCT WORK SHOP Case 1 Case 1: Question 1.1 What is the main pattern of this HRCT? 1. Intralobular line 2. Groundglass opacity 3. Perilymphatic nodule Case 1: Question 1.2 What is the diagnosis? 1. Hypersensitivity
HRCT WORK SHOP Case 1 Case 1: Question 1.1 What is the main pattern of this HRCT? 1. Intralobular line 2. Groundglass opacity 3. Perilymphatic nodule Case 1: Question 1.2 What is the diagnosis? 1. Hypersensitivity
ECMM Excellence Centers Quality Audit
 ECMM Excellence Centers Quality Audit Person in charge: Department: Head of Department: Laboratory is accredited according to ISO 15189 (Medical Laboratories Requirements for quality and competence) Inspected
ECMM Excellence Centers Quality Audit Person in charge: Department: Head of Department: Laboratory is accredited according to ISO 15189 (Medical Laboratories Requirements for quality and competence) Inspected
Pathology of Pneumonia
 Pathology of Pneumonia Dr. Atif Ali Bashir Assistant Professor of Pathology College of Medicine Majma ah University Introduction: 5000 sq meters of area.! (olympic track) Filters >10,000 L of air / day!
Pathology of Pneumonia Dr. Atif Ali Bashir Assistant Professor of Pathology College of Medicine Majma ah University Introduction: 5000 sq meters of area.! (olympic track) Filters >10,000 L of air / day!
Infections in immunocompromised host
 Infections in immunocompromised host Immunodeficiencies Primary immunodeficiencies Neutrophil defect Humoral: B cell defect Humoral: Complement Cellular: T cells Combined severe immunodeficiency Secondary
Infections in immunocompromised host Immunodeficiencies Primary immunodeficiencies Neutrophil defect Humoral: B cell defect Humoral: Complement Cellular: T cells Combined severe immunodeficiency Secondary
MANAGEMENT OF FEVER IN PEDIATRIC PATIENTS FOLLOWING HEMATOPOIETIC STEM CELL TRANSPLANTATION
 MANAGEMENT OF FEVER IN PEDIATRIC PATIENTS FOLLOWING HEMATOPOIETIC STEM CELL TRANSP There are no translations available. MANAGEMENT OF FEVER IN PEDIATRIC PATIENTS FOLLOWING HEMATOPOIETIC STEM CELL TRANSPLANTATION
MANAGEMENT OF FEVER IN PEDIATRIC PATIENTS FOLLOWING HEMATOPOIETIC STEM CELL TRANSP There are no translations available. MANAGEMENT OF FEVER IN PEDIATRIC PATIENTS FOLLOWING HEMATOPOIETIC STEM CELL TRANSPLANTATION
Eun-Young Kang, M.D., Jae Wook Lee, M.D., Ji Yung Choo, M.D., Hwan Seok Yong, M.D., Ki Yeol Lee, M.D., Yu-Whan Oh, M.D.
 Eun-Young Kang, M.D., Jae Wook Lee, M.D., Ji Yung Choo, M.D., Hwan Seok Yong, M.D., Ki Yeol Lee, M.D., Yu-Whan Oh, M.D. Department of Radiology, Korea University Guro Hospital, College of Medicine, Korea
Eun-Young Kang, M.D., Jae Wook Lee, M.D., Ji Yung Choo, M.D., Hwan Seok Yong, M.D., Ki Yeol Lee, M.D., Yu-Whan Oh, M.D. Department of Radiology, Korea University Guro Hospital, College of Medicine, Korea
Use of Antifungal Drugs in the Year 2006"
 Use of Antifungal Drugs in the Year 2006" Jose G. Montoya, MD Associate Professor of Medicine Associate Chief for Clinical Affairs Division of Infectious Diseases Stanford University School of Medicine
Use of Antifungal Drugs in the Year 2006" Jose G. Montoya, MD Associate Professor of Medicine Associate Chief for Clinical Affairs Division of Infectious Diseases Stanford University School of Medicine
PULMONARY EMERGENCIES
 EMERGENCIES I. Pneumonia A. Bacterial Pneumonia (most common cause of a focal infiltrate) 1. Epidemiology a. Accounts for up to 10% of hospital admissions in the U.S. b. Most pneumonias are the result
EMERGENCIES I. Pneumonia A. Bacterial Pneumonia (most common cause of a focal infiltrate) 1. Epidemiology a. Accounts for up to 10% of hospital admissions in the U.S. b. Most pneumonias are the result
Prophylaxis, Empirical, Pre-emptive Therapy of Aspergillosis in Hematological Patients: Which Strategy?
 TIMM-4 18-21 October 2009 Athens, Greece Prophylaxis, Empirical, Pre-emptive Therapy of Aspergillosis in Hematological Patients: Which Strategy? www.ichs.org Georg Maschmeyer Dept. of Hematology, Oncology
TIMM-4 18-21 October 2009 Athens, Greece Prophylaxis, Empirical, Pre-emptive Therapy of Aspergillosis in Hematological Patients: Which Strategy? www.ichs.org Georg Maschmeyer Dept. of Hematology, Oncology
Pulmonary Aspergillosis
 May 2005 Pulmonary Aspergillosis Nancy Wei, Harvard Medical School, Year III Overview Pulmonary aspergillosis background information Patient presentations Common radiographic findings for each type of
May 2005 Pulmonary Aspergillosis Nancy Wei, Harvard Medical School, Year III Overview Pulmonary aspergillosis background information Patient presentations Common radiographic findings for each type of
Unit II Problem 2 Pathology: Pneumonia
 Unit II Problem 2 Pathology: Pneumonia - Definition: pneumonia is the infection of lung parenchyma which occurs especially when normal defenses are impaired such as: Cough reflex. Damage of cilia in respiratory
Unit II Problem 2 Pathology: Pneumonia - Definition: pneumonia is the infection of lung parenchyma which occurs especially when normal defenses are impaired such as: Cough reflex. Damage of cilia in respiratory
DAYTON CHILDREN S HOSPITAL CLINICAL PRACTICE GUIDELINES
 DAYTON CHILDREN S HOSPITAL CLINICAL PRACTICE GUIDELINES DISCLAIMER: This Clinical Practice Guideline (CPG) generally describes a recommended course of treatment for patients with the identified health
DAYTON CHILDREN S HOSPITAL CLINICAL PRACTICE GUIDELINES DISCLAIMER: This Clinical Practice Guideline (CPG) generally describes a recommended course of treatment for patients with the identified health
Antimicrobial Management of Febrile Neutropenic Sepsis
 Antimicrobial Management of Febrile Neutropenic Sepsis Written by: Dr J Joseph, Consultant Haematologist Dr K Gajee, Consultant Microbiologist Amended by: Larissa Claybourn, Antimicrobial Pharmacist Date:
Antimicrobial Management of Febrile Neutropenic Sepsis Written by: Dr J Joseph, Consultant Haematologist Dr K Gajee, Consultant Microbiologist Amended by: Larissa Claybourn, Antimicrobial Pharmacist Date:
Diagnostic Procedures for Pulmonary Infiltrates in the Compromised Host
 Diagnostic Procedures for Pulmonary Infiltrates in the Compromised Host Michael Douvas, MD Heme/Onc Gerald Donowitz, MD - ID Eric Davis, MD - Pulmonary Disclosure Drs. Davis, Donowitz, and Douvas do not
Diagnostic Procedures for Pulmonary Infiltrates in the Compromised Host Michael Douvas, MD Heme/Onc Gerald Donowitz, MD - ID Eric Davis, MD - Pulmonary Disclosure Drs. Davis, Donowitz, and Douvas do not
Potential etiologies of infection in these patients are diverse, including common and uncommon opportunistic infections.
 In the name of God Principles of post Tx infections 1: Potential etiologies of infection in these patients are diverse, including common and uncommon opportunistic infections. Infection processes can progress
In the name of God Principles of post Tx infections 1: Potential etiologies of infection in these patients are diverse, including common and uncommon opportunistic infections. Infection processes can progress
PAGL Inclusion Approved at January 2017 PGC
 Guideline for the prophylaxis and treatment of fungal infections in Haematology patients 1. Introduction PAGL Inclusion Approved at January 2017 PGC Haematology, CHUGGS June 2016 This guideline sets out
Guideline for the prophylaxis and treatment of fungal infections in Haematology patients 1. Introduction PAGL Inclusion Approved at January 2017 PGC Haematology, CHUGGS June 2016 This guideline sets out
Pneumonia in the Immunocompromised Host
 SIOP PODC Supportive Care Education Presentation Date: 26 th October 2015 Recording Link at www.cure4kids.org: https://www.cure4kids.org/ums/home/conference_rooms/enter.php?room=p1bk39ernlb Pneumonia in
SIOP PODC Supportive Care Education Presentation Date: 26 th October 2015 Recording Link at www.cure4kids.org: https://www.cure4kids.org/ums/home/conference_rooms/enter.php?room=p1bk39ernlb Pneumonia in
UPDATE ON FEBRILE NEUTROPENIA
 UPDATE ON FEBRILE NEUTROPENIA Clinical approach and management Dr.Shafiq A. Alimad Head of medical department at university of science and technology hospital YICID 15-December-2014 INTRODUCTION Cancer
UPDATE ON FEBRILE NEUTROPENIA Clinical approach and management Dr.Shafiq A. Alimad Head of medical department at university of science and technology hospital YICID 15-December-2014 INTRODUCTION Cancer
Pneumonia in immunosuppressed patients
 Blackwell Science, LtdOxford, UKRESRespirology1323-77992004 Blackwell Science Asia Pty LtdMarch 20049S1S25S29Original ArticlePneumonia in immunosuppressed patientss Kohno et al. Respirology (2004) 9, S25
Blackwell Science, LtdOxford, UKRESRespirology1323-77992004 Blackwell Science Asia Pty LtdMarch 20049S1S25S29Original ArticlePneumonia in immunosuppressed patientss Kohno et al. Respirology (2004) 9, S25
TOWARDS PRE-EMPTIVE? TRADITIONAL DIAGNOSIS. GALACTOMANNAN Sensitivity 61% Specificity 93% Neg Predict Value >95% β-d-glucan Neg Predict Value 100% PCR
 TOWARDS PRE-EMPTIVE? GALACTOMANNAN Sensitivity 61% Specificity 93% Neg Predict Value >95% TRADITIONAL DIAGNOSIS β-d-glucan Neg Predict Value 100% PCR diagnostics FUNGAL BURDEN FIRST TEST POSITIVE FOR ASPERGILLOSIS
TOWARDS PRE-EMPTIVE? GALACTOMANNAN Sensitivity 61% Specificity 93% Neg Predict Value >95% TRADITIONAL DIAGNOSIS β-d-glucan Neg Predict Value 100% PCR diagnostics FUNGAL BURDEN FIRST TEST POSITIVE FOR ASPERGILLOSIS
Treatment of febrile neutropenia in patients with neoplasia
 Treatment of febrile neutropenia in patients with neoplasia George Samonis MD, PhD Medical Oncologist Infectious Diseases Specialist Professor of Medicine The University of Crete, Heraklion,, Crete, Greece
Treatment of febrile neutropenia in patients with neoplasia George Samonis MD, PhD Medical Oncologist Infectious Diseases Specialist Professor of Medicine The University of Crete, Heraklion,, Crete, Greece
DAYTON CHILDREN S HOSPITAL CLINICAL PRACTICE GUIDELINES
 DAYTON CHILDREN S HOSPITAL CLINICAL PRACTICE GUIDELINES DISCLAIMER: This Clinical Practice Guideline (CPG) generally describes a recommended course of treatment for patients with the identified health
DAYTON CHILDREN S HOSPITAL CLINICAL PRACTICE GUIDELINES DISCLAIMER: This Clinical Practice Guideline (CPG) generally describes a recommended course of treatment for patients with the identified health
Pneumocystis Pneumonia. Dr. Pradeep kumar II yr Pulmonary Medicine
 Pneumocystis Pneumonia Dr. Pradeep kumar II yr Pulmonary Medicine PNEUMOCYSTIS CARINII PNEUMONIA Pneumocystis carinii pneumonia (PCP), is commonly termed Pneumocystis jiroveci pneumonia, is the 2 nd most
Pneumocystis Pneumonia Dr. Pradeep kumar II yr Pulmonary Medicine PNEUMOCYSTIS CARINII PNEUMONIA Pneumocystis carinii pneumonia (PCP), is commonly termed Pneumocystis jiroveci pneumonia, is the 2 nd most
An Introduction to Radiology for TB Nurses
 An Introduction to Radiology for TB Nurses Garold O. Minns, MD September 14, 2017 TB Nurse Case Management September 12 14, 2017 EXCELLENCE EXPERTISE INNOVATION Garold O. Minns, MD has the following disclosures
An Introduction to Radiology for TB Nurses Garold O. Minns, MD September 14, 2017 TB Nurse Case Management September 12 14, 2017 EXCELLENCE EXPERTISE INNOVATION Garold O. Minns, MD has the following disclosures
Pneumonia. Definition of pneumonia Infection of the lung parenchyma Usually bacterial
 Pneumonia Definition of pneumonia Infection of the lung parenchyma Usually bacterial Epidemiology of pneumonia Commonest infectious cause of death in the UK and USA Incidence - 5-11 per 1000 per year Worse
Pneumonia Definition of pneumonia Infection of the lung parenchyma Usually bacterial Epidemiology of pneumonia Commonest infectious cause of death in the UK and USA Incidence - 5-11 per 1000 per year Worse
PULMONARY MEDICINE BOARD REVIEW. Financial Conflicts of Interest. Question #1: Question #1 (Cont.): None. Christopher H. Fanta, M.D.
: None. Christopher H. Fanta, M.D.") PULMONARY MEDICINE BOARD REVIEW Christopher H. Fanta, M.D. Pulmonary and Critical Care Division Brigham and Women s Hospital Partners Asthma Center Harvard Medical School Financial Conflicts of Interest
PULMONARY MEDICINE BOARD REVIEW Christopher H. Fanta, M.D. Pulmonary and Critical Care Division Brigham and Women s Hospital Partners Asthma Center Harvard Medical School Financial Conflicts of Interest
How to Analyse Difficult Chest CT
 How to Analyse Difficult Chest CT Complex diseases are:- - Large lesion - Unusual or atypical pattern - Multiple discordant findings Diffuse diseases are:- - Numerous findings in both sides 3 basic steps
How to Analyse Difficult Chest CT Complex diseases are:- - Large lesion - Unusual or atypical pattern - Multiple discordant findings Diffuse diseases are:- - Numerous findings in both sides 3 basic steps
Interesting Cases. Pulmonary
 Interesting Cases Pulmonary 54M with prior history of COPD, hep B/C, and possible history of TB presented with acute on chronic dyspnea, and productive cough Hazy opacity overlying the left hemithorax
Interesting Cases Pulmonary 54M with prior history of COPD, hep B/C, and possible history of TB presented with acute on chronic dyspnea, and productive cough Hazy opacity overlying the left hemithorax
HAEMATOLOGY ANTIFUNGAL POLICY
 HAEMATOLOGY ANTIFUNGAL POLICY PROPHYLAXIS Primary Prophylaxis Patient Group Patients receiving intensive remissioninduction chemotherapy for Acute Leukaemia (excluding patients receiving vinca alkaloids)
HAEMATOLOGY ANTIFUNGAL POLICY PROPHYLAXIS Primary Prophylaxis Patient Group Patients receiving intensive remissioninduction chemotherapy for Acute Leukaemia (excluding patients receiving vinca alkaloids)
Antimicrobial prophylaxis for transplant recipients. Peter Chin-Hong, MD MAS February 4, 2015
 Antimicrobial prophylaxis for transplant recipients Peter Chin-Hong, MD MAS February 4, 2015 Objective To list and understand the approach to three prevention strategies used to prevent infections in transplant
Antimicrobial prophylaxis for transplant recipients Peter Chin-Hong, MD MAS February 4, 2015 Objective To list and understand the approach to three prevention strategies used to prevent infections in transplant
Infectious Complications in Patients with Chronic Lymphocytic Leukemia Pathogenesis, Spectrum, Treatment
 Infectious Complications in Patients with Chronic Lymphocytic Leukemia Pathogenesis, Spectrum, Treatment Vicki A. Morrison, MD Professor of Medicine, University of Minnesota Staff Physician, Sections of
Infectious Complications in Patients with Chronic Lymphocytic Leukemia Pathogenesis, Spectrum, Treatment Vicki A. Morrison, MD Professor of Medicine, University of Minnesota Staff Physician, Sections of
Top 5 papers in clinical mycology
 Top 5 papers in clinical mycology Dirk Vogelaers Department of General Internal Medicine University Hospital Ghent Joint symposium BVIKM/BSIMC and SBMHA/BVMDM Influenza-associated aspergillosis in critically
Top 5 papers in clinical mycology Dirk Vogelaers Department of General Internal Medicine University Hospital Ghent Joint symposium BVIKM/BSIMC and SBMHA/BVMDM Influenza-associated aspergillosis in critically
PNEUMONIA. I. Background 6 th most common cause of death in U.S. Most common cause of infection related mortality
 Page 1 of 8 September 4, 2001 Donald P. Levine, M.D. University Health Center Suite 5C Office: 577-0348 dlevine@intmed.wayne.edu Assigned reading: pages 153-160; 553-563 PNEUMONIA the most widespread and
Page 1 of 8 September 4, 2001 Donald P. Levine, M.D. University Health Center Suite 5C Office: 577-0348 dlevine@intmed.wayne.edu Assigned reading: pages 153-160; 553-563 PNEUMONIA the most widespread and
Case Studies in Fungal Infections and Antifungal Therapy
 Case Studies in Fungal Infections and Antifungal Therapy Wayne L. Gold MD, FRCPC Annual Meeting of the Canadian Society of Internal Medicine November 4, 2017 Disclosures No financial disclosures or industry
Case Studies in Fungal Infections and Antifungal Therapy Wayne L. Gold MD, FRCPC Annual Meeting of the Canadian Society of Internal Medicine November 4, 2017 Disclosures No financial disclosures or industry
Antifungals in Invasive Fungal Infections: Antifungals in neutropenic patients
 BVIKM-SBIMC La Hulpe, 6 November 2008 Antifungals in Invasive Fungal Infections: Antifungals in neutropenic patients Johan Maertens, MD Acute Leukemia and SCT Unit University Hospital Gasthuisberg Catholic
BVIKM-SBIMC La Hulpe, 6 November 2008 Antifungals in Invasive Fungal Infections: Antifungals in neutropenic patients Johan Maertens, MD Acute Leukemia and SCT Unit University Hospital Gasthuisberg Catholic
Diagnosis of TB: Radiology David Finlay, MD
 TB Intensive Tyler, Texas June 2-4, 2010 Diagnosis of TB: Radiology David Finlay, MD June 3, 2010 2stages stages- Tuberculosis 1. primary infection 2. reactivation, or post primary disease 2 1 Primary
TB Intensive Tyler, Texas June 2-4, 2010 Diagnosis of TB: Radiology David Finlay, MD June 3, 2010 2stages stages- Tuberculosis 1. primary infection 2. reactivation, or post primary disease 2 1 Primary
Invasive Aspergillosis in India: Unique Challenges. Dr Rajeev Soman Consultant Physician PD Hinduja Hospital Mumbai
 Invasive Aspergillosis in India: Unique Challenges Dr Rajeev Soman Consultant Physician PD Hinduja Hospital Mumbai Aspergillus Challenges Capable of surviving & thriving in all the diverse environmental
Invasive Aspergillosis in India: Unique Challenges Dr Rajeev Soman Consultant Physician PD Hinduja Hospital Mumbai Aspergillus Challenges Capable of surviving & thriving in all the diverse environmental
Common Fungi. Catherine Diamond MD MPH
 Common Fungi Catherine Diamond MD MPH Birth Month and Day & Last Four Digits of Your Cell Phone # BEFORE: http://tinyurl.com/kvfy3ts AFTER: http://tinyurl.com/lc4dzwr Clinically Common Fungi Yeast Mold
Common Fungi Catherine Diamond MD MPH Birth Month and Day & Last Four Digits of Your Cell Phone # BEFORE: http://tinyurl.com/kvfy3ts AFTER: http://tinyurl.com/lc4dzwr Clinically Common Fungi Yeast Mold
TB Radiology for Nurses Garold O. Minns, MD
 TB Nurse Case Management Salina, Kansas March 31-April 1, 2010 TB Radiology for Nurses Garold O. Minns, MD April 1, 2010 TB Radiology for Nurses Highway Patrol Training Center Salina, KS April 1, 2010
TB Nurse Case Management Salina, Kansas March 31-April 1, 2010 TB Radiology for Nurses Garold O. Minns, MD April 1, 2010 TB Radiology for Nurses Highway Patrol Training Center Salina, KS April 1, 2010
MICROBIOLOGICAL TESTING IN PICU
 MICROBIOLOGICAL TESTING IN PICU This is a guideline for the taking of microbiological samples in PICU to diagnose or exclude infection. The diagnosis of infection requires: Ruling out non-infectious causes
MICROBIOLOGICAL TESTING IN PICU This is a guideline for the taking of microbiological samples in PICU to diagnose or exclude infection. The diagnosis of infection requires: Ruling out non-infectious causes
Antimicrobial prophylaxis in liver transplant A multicenter survey endorsed by the European Liver and Intestine Transplant Association
 Antimicrobial prophylaxis in liver transplant A multicenter survey endorsed by the European Liver and Intestine Transplant Association Els Vandecasteele, Jan De Waele, Dominique Vandijck, Stijn Blot, Dirk
Antimicrobial prophylaxis in liver transplant A multicenter survey endorsed by the European Liver and Intestine Transplant Association Els Vandecasteele, Jan De Waele, Dominique Vandijck, Stijn Blot, Dirk
TREATMENT STRATEGIES FOR INVASIVE FUNGAL INFECTIONS. Part I: EMPIRICAL THERAPY
 TREATMENT STRATEGIES FOR INVASIVE FUNGAL INFECTIONS Part I: EMPIRICAL THERAPY CAUSES OF DEATH IN PATIENTS WITH MALIGNANCIES NIJMEGEN, THE NETHERLANDS n = 328 BACTERIAL INFECTION FUNGAL INFECTION 7% 36%
TREATMENT STRATEGIES FOR INVASIVE FUNGAL INFECTIONS Part I: EMPIRICAL THERAPY CAUSES OF DEATH IN PATIENTS WITH MALIGNANCIES NIJMEGEN, THE NETHERLANDS n = 328 BACTERIAL INFECTION FUNGAL INFECTION 7% 36%
PULMONARY TUBERCULOSIS RADIOLOGY
 PULMONARY TUBERCULOSIS RADIOLOGY RADIOLOGICAL MODALITIES Medical radiophotography Radiography Fluoroscopy Linear (conventional) tomography Computed tomography Pulmonary angiography, bronchography Ultrasonography,
PULMONARY TUBERCULOSIS RADIOLOGY RADIOLOGICAL MODALITIES Medical radiophotography Radiography Fluoroscopy Linear (conventional) tomography Computed tomography Pulmonary angiography, bronchography Ultrasonography,
8/11/2015. Febrile neutropenia Bone marrow transplant Immunosuppressant medications
 Dean Van Loo Pharm.D. Febrile neutropenia Bone marrow transplant Immunosuppressant medications Steroids Biologics Antineoplastic Most data from cancer chemotherapy Bone marrow suppression Fever is the
Dean Van Loo Pharm.D. Febrile neutropenia Bone marrow transplant Immunosuppressant medications Steroids Biologics Antineoplastic Most data from cancer chemotherapy Bone marrow suppression Fever is the
Severe β-lactam allergy. Alternative (use for mild-moderate β-lactam allergy) therapy
 therapy") Recommended Empirical Antibiotic Regimens for MICU Patients Notes: The antibiotic regimens shown are general guidelines and should not replace clinical judgment. Always assess for antibiotic allergies.
Recommended Empirical Antibiotic Regimens for MICU Patients Notes: The antibiotic regimens shown are general guidelines and should not replace clinical judgment. Always assess for antibiotic allergies.
Therapy of Hematologic Malignancies Period at high risk of IFI
 Therapy of Hematologic Malignancies Period at high risk of IFI Neutrophils (/mm 3 ) 5 Chemotherapy Conditioning Regimen HSCT Engraftment GVHD + Immunosuppressive Treatment Cutaneous and mucositis : - Direct
Therapy of Hematologic Malignancies Period at high risk of IFI Neutrophils (/mm 3 ) 5 Chemotherapy Conditioning Regimen HSCT Engraftment GVHD + Immunosuppressive Treatment Cutaneous and mucositis : - Direct
Approach to the Transplant Patient. Amy Musiek, MD AAD Annual Meeting 2018
 Approach to the Transplant Patient Amy Musiek, MD AAD Annual Meeting 2018 Disclosures Actelion: speaker, advisory board, investigator Elorac: investigator Kyowa: investigator, advisory board Seattle genetics:
Approach to the Transplant Patient Amy Musiek, MD AAD Annual Meeting 2018 Disclosures Actelion: speaker, advisory board, investigator Elorac: investigator Kyowa: investigator, advisory board Seattle genetics:
Disorders of immune system in hematology Stomatologic complications of treatment in hematology. Semminar for students E.Faber
 Disorders of immune system in hematology Stomatologic complications of treatment in hematology Semminar for students E.Faber Topics Disorders of immune system in hematology Principles of treatment in hematology
Disorders of immune system in hematology Stomatologic complications of treatment in hematology Semminar for students E.Faber Topics Disorders of immune system in hematology Principles of treatment in hematology
Neutropenic Fever. CID 2011; 52 (4):e56-e93
:e56-e93") Neutropenic Fever www.idsociety.org CID 2011; 52 (4):e56-e93 Definitions Fever: Single oral temperature of 101 F (38.3 C) Temperature 100.4 F (38.0 C) over 1 hour Neutropenia: ANC < 500 cells/mm 3 Expected
Neutropenic Fever www.idsociety.org CID 2011; 52 (4):e56-e93 Definitions Fever: Single oral temperature of 101 F (38.3 C) Temperature 100.4 F (38.0 C) over 1 hour Neutropenia: ANC < 500 cells/mm 3 Expected
When is failure failure?
 When is failure failure? Bart-Jan Kullberg, M.D. Radboud University Nijmegen The Netherlands The ICU patient with candidemia!! Female, 39 years old!! Multiple abdominal surgeries for Crohn's disease!!
When is failure failure? Bart-Jan Kullberg, M.D. Radboud University Nijmegen The Netherlands The ICU patient with candidemia!! Female, 39 years old!! Multiple abdominal surgeries for Crohn's disease!!
Interpretation of Chest Radiographs Paul Christensen, MD 10/21/09. Diagnostic Evaluation. Medical Evaluation & CXR Interpretation.
 Diagnostic Evaluation Medical Evaluation & CXR Interpretation University of Michigan TB Consultant Washtenaw County Medical history Physical examination Testing for TB exposure (previously covered) Radiologic
Diagnostic Evaluation Medical Evaluation & CXR Interpretation University of Michigan TB Consultant Washtenaw County Medical history Physical examination Testing for TB exposure (previously covered) Radiologic
We are IntechOpen, the world s leading publisher of Open Access books Built by scientists, for scientists. International authors and editors
 We are IntechOpen, the world s leading publisher of Open Access books Built by scientists, for scientists 3,800 116,000 120M Open access books available International authors and editors Downloads Our
We are IntechOpen, the world s leading publisher of Open Access books Built by scientists, for scientists 3,800 116,000 120M Open access books available International authors and editors Downloads Our
General History. 林陳 珠 Female 69 years old 住院期間 : ~ Chief Complaint : sudden loss of conscious 5 minutes in the morning.
 General History 林陳 珠 Female 69 years old 住院期間 : 93.5.8~93.5.15 Chief Complaint : sudden loss of conscious for 2-52 5 minutes in the morning. General History DM under regular medical control for 10 years.
General History 林陳 珠 Female 69 years old 住院期間 : 93.5.8~93.5.15 Chief Complaint : sudden loss of conscious for 2-52 5 minutes in the morning. General History DM under regular medical control for 10 years.
Key Difference - Pleural Effusion vs Pneumonia
 Difference Between Pleural Effusion and Pneumonia www.differencebetween.com Key Difference - Pleural Effusion vs Pneumonia Pleural effusion and pneumonia are two conditions that affect our respiratory
Difference Between Pleural Effusion and Pneumonia www.differencebetween.com Key Difference - Pleural Effusion vs Pneumonia Pleural effusion and pneumonia are two conditions that affect our respiratory
Management Strategies For Invasive Mycoses: An MD Anderson Perspective
 Management Strategies For Invasive Mycoses: An MD Anderson Perspective Dimitrios P. Kontoyiannis, MD, ScD, FACP, FIDSA Professor of Medicine Director of Mycology Research Program M. D. Anderson Cancer
Management Strategies For Invasive Mycoses: An MD Anderson Perspective Dimitrios P. Kontoyiannis, MD, ScD, FACP, FIDSA Professor of Medicine Director of Mycology Research Program M. D. Anderson Cancer
Fever in Lupus. 21 st April 2014
 Fever in Lupus 21 st April 2014 Fever in lupus Cause of fever N= 487 % SLE fever 206 42 Infection in SLE 265 54.5 Active SLE and infection 8 1.6 Tumor fever 4 0.8 Miscellaneous 4 0.8 Crucial Question Infection
Fever in Lupus 21 st April 2014 Fever in lupus Cause of fever N= 487 % SLE fever 206 42 Infection in SLE 265 54.5 Active SLE and infection 8 1.6 Tumor fever 4 0.8 Miscellaneous 4 0.8 Crucial Question Infection
Infections after stem cell transplantation
 Infections after stem cell transplantation Lidia Gil Poznan, Poland No conflict of interest Lisbon, Portugal 20/03/2018 #EBMT18 www.ebmt.or Infections after HSCT Infectious complications universal problem
Infections after stem cell transplantation Lidia Gil Poznan, Poland No conflict of interest Lisbon, Portugal 20/03/2018 #EBMT18 www.ebmt.or Infections after HSCT Infectious complications universal problem
HRCT in Diffuse Interstitial Lung Disease Steps in High Resolution CT Diagnosis. Where are the lymphatics? Anatomic distribution
 Steps in High Resolution CT Diagnosis Pattern of abnormality Distribution of disease Associated findings Clinical history Tomás Franquet MD What is the diagnosis? Hospital de Sant Pau. Barcelona Secondary
Steps in High Resolution CT Diagnosis Pattern of abnormality Distribution of disease Associated findings Clinical history Tomás Franquet MD What is the diagnosis? Hospital de Sant Pau. Barcelona Secondary
A CASE OF UNFORTUNATE
 A CASE OF UNFORTUNATE TAPER Hélène Schoemans, MD University Hospitals Leuven, Belgium EBMT Complications and Quality of Life Working Party Educational Course Warsaw, October 24 th 2014 Company name No
A CASE OF UNFORTUNATE TAPER Hélène Schoemans, MD University Hospitals Leuven, Belgium EBMT Complications and Quality of Life Working Party Educational Course Warsaw, October 24 th 2014 Company name No
Immune-mediated lung disease. Ian Sabroe
 Immune-mediated lung disease Ian Sabroe It s all immune? Diseases that doesn t have immune involvement? The processes of response to injury and tissue repair are key homeostatic pathways involved in all
Immune-mediated lung disease Ian Sabroe It s all immune? Diseases that doesn t have immune involvement? The processes of response to injury and tissue repair are key homeostatic pathways involved in all
Financial disclosure COMMON DIAGNOSES IN HRCT. High Res Chest HRCT. HRCT Pre test. I have no financial relationships to disclose. Anatomy Nomenclature
 Financial disclosure I have no financial relationships to disclose. Douglas Johnson D.O. Cardiothoracic Imaging Gaston Radiology COMMON DIAGNOSES IN HRCT High Res Chest Anatomy Nomenclature HRCT Sampling
Financial disclosure I have no financial relationships to disclose. Douglas Johnson D.O. Cardiothoracic Imaging Gaston Radiology COMMON DIAGNOSES IN HRCT High Res Chest Anatomy Nomenclature HRCT Sampling
Condition First line Alternative Comments Candidemia Nonneutropenic adults
 Recommendations for the treatment of candidiasis. Clinical Practice Guidelines for the Management of Candidiasis: 2009 Update by the Infectious Diseases Society of America. Condition First line Alternative
Recommendations for the treatment of candidiasis. Clinical Practice Guidelines for the Management of Candidiasis: 2009 Update by the Infectious Diseases Society of America. Condition First line Alternative
Systemic lupus erythematosus (SLE): Pleuropulmonary Manifestations
: Pleuropulmonary Manifestations") 08/30/10 09/26/10 Systemic lupus erythematosus (SLE): Pleuropulmonary Manifestations Camila Downey S. Universidad de Chile, School of Medicine, Year VII Harvard University, School of Medicine Sept 17,
08/30/10 09/26/10 Systemic lupus erythematosus (SLE): Pleuropulmonary Manifestations Camila Downey S. Universidad de Chile, School of Medicine, Year VII Harvard University, School of Medicine Sept 17,
Chapter 22. Pulmonary Infections
 Chapter 22 Pulmonary Infections Objectives State the incidence of pneumonia in the United States and its economic impact. Discuss the current classification scheme for pneumonia and be able to define hospital-acquired
Chapter 22 Pulmonary Infections Objectives State the incidence of pneumonia in the United States and its economic impact. Discuss the current classification scheme for pneumonia and be able to define hospital-acquired
New respiratory symptoms and lung imaging findings in a woman with polymyositis
 Maria Bolaki 1, Konstantinos Karagiannis 1, George Bertsias 2, Ioanna Mitrouska 1, Nikolaos Tzanakis 1, Katerina M. Antoniou 1 kantoniou@uoc.gr 1 Dept of Thoracic Medicine, Heraklion University Hospital,
Maria Bolaki 1, Konstantinos Karagiannis 1, George Bertsias 2, Ioanna Mitrouska 1, Nikolaos Tzanakis 1, Katerina M. Antoniou 1 kantoniou@uoc.gr 1 Dept of Thoracic Medicine, Heraklion University Hospital,
Case 1. Background. Presenting Symptoms. Schecter Case1 Differential Diagnosis of TB 1
 TB or Not TB? Case 1 Gisela Schecter, M.D., M.P.H. California Department of Public Health Background 26 year old African American male Born and raised in Bay Area of California Convicted of cocaine trafficking
TB or Not TB? Case 1 Gisela Schecter, M.D., M.P.H. California Department of Public Health Background 26 year old African American male Born and raised in Bay Area of California Convicted of cocaine trafficking
Pneumocystis jirovecci pneumonia: from mild disease to a real disaster. A pictorial review of the different radiologic patterns in acute settings
 Pneumocystis jirovecci pneumonia: from mild disease to a real disaster. A pictorial review of the different radiologic patterns in acute settings Poster No.: C-1425 Congress: ECR 2017 Type: Educational
Pneumocystis jirovecci pneumonia: from mild disease to a real disaster. A pictorial review of the different radiologic patterns in acute settings Poster No.: C-1425 Congress: ECR 2017 Type: Educational
MANAGEMENT OF HOSPITAL-ACQUIRED FUNGAL INFECTIONS
 MANAGEMENT OF HOSPITAL-ACQUIRED FUNGAL INFECTIONS Paul D. Holtom, MD Associate Professor of Medicine and Orthopaedics USC Keck School of Medicine Numbers of Cases of Sepsis in the United States, According
MANAGEMENT OF HOSPITAL-ACQUIRED FUNGAL INFECTIONS Paul D. Holtom, MD Associate Professor of Medicine and Orthopaedics USC Keck School of Medicine Numbers of Cases of Sepsis in the United States, According
Pneumonia. Dr. Rami M Adil Al-Hayali Assistant professor in medicine
 Pneumonia Dr. Rami M Adil Al-Hayali Assistant professor in medicine Definition Pneumonia is an acute respiratory illness caused by an infection of the lung parenchyma, associated with recently developed
Pneumonia Dr. Rami M Adil Al-Hayali Assistant professor in medicine Definition Pneumonia is an acute respiratory illness caused by an infection of the lung parenchyma, associated with recently developed
Infection in the (non-hiv) Immunocompromised Host
 Immunocompromised Host") Infection in the (non-hiv) Immunocompromised Host No financial relationships to disclose Brian S. Schwartz, MD UCSF, Division of Infectious Diseases Lecture outline Background/why is this topic important?
Infection in the (non-hiv) Immunocompromised Host No financial relationships to disclose Brian S. Schwartz, MD UCSF, Division of Infectious Diseases Lecture outline Background/why is this topic important?
Lecture Notes. Chapter 16: Bacterial Pneumonia
 Lecture Notes Chapter 16: Bacterial Pneumonia Objectives Explain the epidemiology Identify the common causes Explain the pathological changes in the lung Identify clinical features Explain the treatment
Lecture Notes Chapter 16: Bacterial Pneumonia Objectives Explain the epidemiology Identify the common causes Explain the pathological changes in the lung Identify clinical features Explain the treatment
PNEUMONIA IN CHILDREN. IAP UG Teaching slides
 PNEUMONIA IN CHILDREN 1 INTRODUCTION 156 million new episodes / yr. worldwide 151 million episodes developing world 95% in developing countries 19% of all deaths in children
PNEUMONIA IN CHILDREN 1 INTRODUCTION 156 million new episodes / yr. worldwide 151 million episodes developing world 95% in developing countries 19% of all deaths in children
Outline. Cryptococcosis Pneumocystosis Diarrhea. Case Histories: HIV Related- Opportunistic Infections in 2015
 AU Edited: 05/06/15 Case Histories: HIV Related- Opportunistic Infections in 2015 Henry Masur, MD Clinical Professor of Medicine George Washington University School of Medicine Bethesda, Maryland Washington,
AU Edited: 05/06/15 Case Histories: HIV Related- Opportunistic Infections in 2015 Henry Masur, MD Clinical Professor of Medicine George Washington University School of Medicine Bethesda, Maryland Washington,
Radiological Aspects of Pulmonary Tuberculosis in Immunocompetent Hosts
 Nov 2003 Radiological Aspects of Pulmonary Tuberculosis in Immunocompetent Hosts Josh Rempell, Harvard Medical School Year III Tuberculosis: the captain of all (wo)men of death Overall, one third of the
Nov 2003 Radiological Aspects of Pulmonary Tuberculosis in Immunocompetent Hosts Josh Rempell, Harvard Medical School Year III Tuberculosis: the captain of all (wo)men of death Overall, one third of the
Is pre-emptive therapy a realistic approach?
 Is pre-emptive therapy a realistic approach? J Peter Donnelly PhD, FRCPath Department of Haematology Radboud University Nijmegen Medical Centre Nijmegen, The Netherlands Is pre-emptive therapy a realistic
Is pre-emptive therapy a realistic approach? J Peter Donnelly PhD, FRCPath Department of Haematology Radboud University Nijmegen Medical Centre Nijmegen, The Netherlands Is pre-emptive therapy a realistic
Pulmonary Pathology II. William Bligh-Glover M.D. Department of Anatomy, CWRU
 Pulmonary Pathology II William Bligh-Glover M.D. Department of Anatomy, CWRU Goals and Objectives Comprehend the etiology, pathogenesis/pathopysiology and consequences of pulmonary hypertension Distinguish
Pulmonary Pathology II William Bligh-Glover M.D. Department of Anatomy, CWRU Goals and Objectives Comprehend the etiology, pathogenesis/pathopysiology and consequences of pulmonary hypertension Distinguish
TB Intensive Houston, Texas
 TB Intensive Houston, Texas October 15-17, 17 2013 Diagnosis of TB: Radiology Rosa M Estrada-Y-Martin, MD MSc FCCP October 16, 2013 Rosa M Estrada-Y-Martin, MD MSc FCCP, has the following disclosures to
TB Intensive Houston, Texas October 15-17, 17 2013 Diagnosis of TB: Radiology Rosa M Estrada-Y-Martin, MD MSc FCCP October 16, 2013 Rosa M Estrada-Y-Martin, MD MSc FCCP, has the following disclosures to
POLICY FOR TREATMENT OF LOWER RESPIRATORY TRACT INFECTIONS
 POLICY F TREATMENT OF LOWER RESPIRATY TRACT INFECTIONS Written by: Dr M Milupi, Consultant Microbiologist Date: June 2018 Approved by: The Drugs & Therapeutics Committee Date: July 2018 Implementation
POLICY F TREATMENT OF LOWER RESPIRATY TRACT INFECTIONS Written by: Dr M Milupi, Consultant Microbiologist Date: June 2018 Approved by: The Drugs & Therapeutics Committee Date: July 2018 Implementation