Uses, limitations and interpretation of CT in pulmonary infections: A practical approach
|
|
|
- June Snow
- 5 years ago
- Views:
Transcription


1 Uses, limitations and interpretation of CT in pulmonary infections: A practical approach Canadian Association of Radiologists 2013
2 DISCLOSURES Speakers honorarium, Siemens Canada
3 Objectives 1. Recognize and differentiate the HCRT patterns of specific pulmonary infections, including those involving the immunocompromised host. 2. Identify non-infectious mimics of pulmonary infections and recognize the role of the radiologist in directing appropriate clinical work up and treatment. 3. Identify infectious mimics of neoplastic processes.

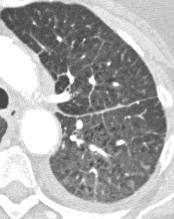
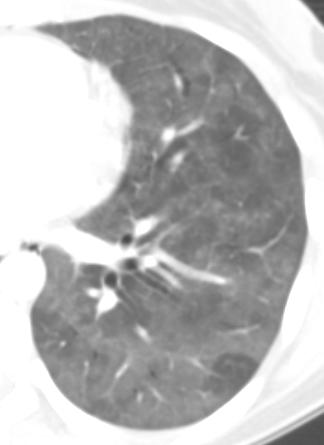
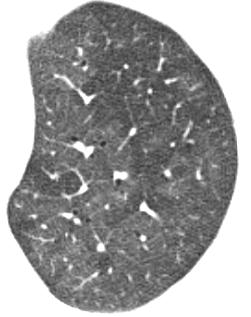
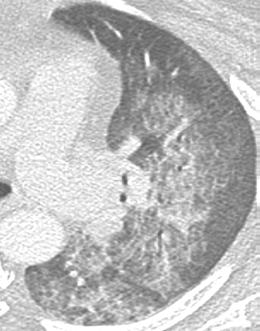
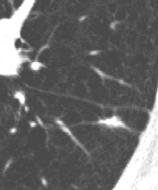
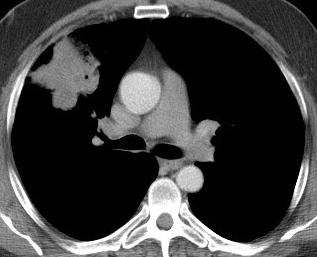
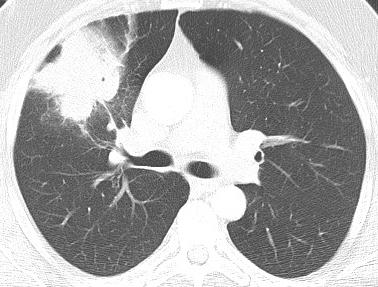
4 CASE 1 : Which is most likely to represent PCP? A B 50 yo male: chronic steroids 24 yo male: IVDU, HIV+ living on street C D Daria 38 yo Manos female: cachexia, 6 weeks of cough 60 yo female: 7 days post SCT

5 A 50 yo male: chronic steroids
6 B 24 yo male: IVDU, HIV+ living on street
7 C 38 yo female: cachexia, 6 weeks of cough

8 D 60 yo female: 7 days post SCT
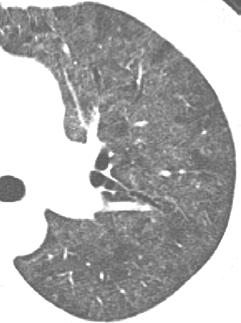
9 CASE 1: Answer Which is most likely to represent PCP? A B 50 yo male: chronic steroids 24 yo male: IVDU, HIV + living on street C D Daria 38 yo Manos female: cachexia, 6 weeks of cough 60 yo female: 7 days post SCT
10 Pneumocystis jiroveci pneumonia PCP no longer the most common respiratory infection in AIDS. Now with Septra prophylaxis changing demographic. HIV with poor health care (IVDU) HIV not yet diagnosed Non-HIV immunocompromised high dose corticosteroids, chemotherapy, transplant, hematologic malignancies 30% will have normal CXR Diagnosis: Induced sputum and PCR May need BAL



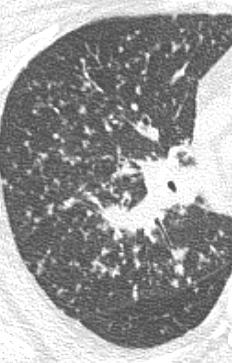
11 HISTORY: Few days of cough and fever. TRIAGE NOTE: often hypoxic PCP in 75 yo with CLL - Abnormal CXR in ED Progression over 3 days

12 Early bilateral perihilar ggo, interstitial thickening, hazy vessels. No effusion. QE


13 QE

14

15 QEII

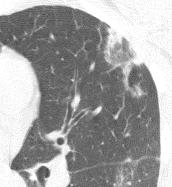
16 Patchy, often geographic Can see crazy paving. Why is this not alveolar proteinosis or HP?


17 Look for cysts or cavitation within ground glass Cysts/pneumatoceles in 10-38% QEII

18 Atypical QEII

19 VGH

20 QEII

21 Can be nodular QE II

22 atypical VGH but not pure tree in bud

23 VGH Dense air space consolidation possible

24 typical QE

25 atypical QE Lobar consolidation rare


26 PCP and Respiratory infections in HIV Bacterial Primary Tb PCP Post primary Tb Fungal Toxoplasmosis MAC CMV CD

27 Respiratory Infection post Stem cell transplant Course of events and risks associated with allogeneic transplantation. Léger C S, and Nevill T J CMAJ 2004;170:
28 CT for Immunocompromised Patients CT often adds little compared to CXR and clinical history. Weigh the risks of CT. Consider low dose. Indications for CT: normal CXR but high suspicion non-specific CXR pattern guiding invasive procedures assessing complications (eg effusion)
 PCP CMV Daria CMV Manos case courtesy Geoff")
29 Diffuse ggo in immunocompromised Infection clinically: PCP Viral (CMV, herpes, RSV) PCP CMV Daria CMV Manos case courtesy Geoff Marshall
30 Diffuse ggo in immunocompromised Infection clinically: PCP Viral (CMV, herpes, RSV) Specifically mention possibility of PCP and CMV. Induced sputum not very sensitive. Made need bronchoscopy to diagnose.
31 Diffuse ggo in immunocompromised If alternate clinical presentation: Consider other causes of ground glass opacity






32

33 Case 2: What is the most likely diagnosis? History: 65 yo man with productive cough 10 months earlier

34 Case 2: What is the most likely diagnosis? History: 65 yo man with productive cough 10 months earlier
35 Case 2: What is the most likely diagnosis? A. Tuberculosis. B. Central obstructing tumor. C. Mucinous adenocarcinoma. D. Organizing pneumonia.
36 10 months earlier

37 Non-resolving pneumonia Infectious Pathogen factors Host factors Inflammatory 20% Neoplastic Lipoid Pneumonia Organizing Pneumonia Eosinophilic Pneumonia Scar/radiation Consolidative adenocarcinoma Lymphoma Kaposi Sarcoma


38 Non resolving pneumonia Pathogen factors: actino severe up to 10 wks complex, abscess resistant penicillin 50% strep levofloxacin 5% strep misdiagnosed Host factors: tb, fungal, nocardia, DM, COPD, EtOh, age


39 Tuberculosis Dx may be difficult SNTB Altered in HIV Consider risk factors HIV endemic areas institutionalization



40 Lipoid Pneumonia Aspiration of oil/fat Consolidation may be fatty density Fibrosis Courtesy Geoff Marshall

41 Scar / radiation Radiation fibrosis 6 to 12 months post > 20Gy Stereotactic radiation: not as obvious

42 Chronic Eosinophilic pneumonia 3+ months Peripheral and upper Patchy Neg of pulm edema

43 Chronic Eosinophilic pneumonia 3+ months Peripheral and upper Patchy Neg of pulm edema

44 Chronic Eosinophilic pneumonia 3+ months Peripheral and upper Patchy Neg of pulm edema

45 Chronic Eosinophilic pneumonia 3+ months Peripheral and upper Patchy Neg of pulm edema

46 Cryptogenic organizing pneumonia Pattern of lung reaction Idiopathic (COP) or 2 o Patchy peripheral and peribronchovascuar consolidation and ggo Lower predominant Can recur Can migrate


47 CEP and OP Reverse halo, atoll sign, perilobular consolidation, lobular sparing




48 Lymphoma Extranodal NHL > HL In lung: consolidation masses nodules interstitial thickening 4 months later Progressive mass-like consolidation.

49 Adenocarcinoma- mucinous subtype mucinous BAC pneumonic BAC endobronchial spread

50 Adenocarcinoma- mucinous subtype mucinous BAC pneumonic BAC endobronchial spread

51 Adenocarcinoma- mucinous subtype mucinous BAC pneumonic BAC endobronchial spread
52 Progressive consolidation over months especially if mass-like consider lymphoma. middle aged, older consider mucinous adeno ca. Progressive consolidation over days/weeks consider Tb, resistant organism Peripheral consolidation in patient with unusual clinical story and otherwise healthy consider OP and EP Recurrent consolidation in same region abnormal underlying lung (obstruction, congenital) Migratory consolidation consider OP, EP, aspiration, vasculitis

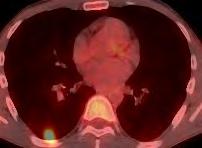
53 Case 3: Question What is your recommendation? 65 yo smoker: abnormality on CXR
54 Case 3: What is your recommendation? A. Follow up CT B. PET CT C. FNA or core D. Resection
55
56 When should the radiologist raise the possibility of infection as a cause of SPN?


57 Consider infection as cause of SPN when: 1. Infectious history on original requisition. 81 yo one week of dsypnea


58 Round pneumonia Typical and atypical bugs Slowly fades away CT delayed resolution lobular pattern often satellite nodules

59 Consider infection when: 2. Demographic clues: exposure < 50 years > 60 years Risk of infection immunocompromise smoker

60 34 year old

61 40 year old woman with fever and malaise Blastomycosis Serology core biopsy bronch VATS wedge. Fungal infection Endemic in Ohio and Mississippi River valleys



62 First 30 days post SCT angioinvasive aspergillosis Halo sign very specific but only in appropriate clinical context (severe neutropenia)

63 35 yo male HIV + : tuberculosis
64 Consider infection when: 3. Infectious CT features ground glass margin subsolid nodule/mass that has not been proven persistent multifocal satellite nodules air bronchograms in a solid lesion Not present on recent CT CT features alone only raise the possibility of infection. Neoplasm can not be excluded.

65




66 Value of short interval follow up CT


67
68 Role of FNA and PET? When infection is more likely, the yield of FNA is lower. When infection is a possibility, the specificity of PETCT is reduced.
69 Textbook list of infectious causes of SPN Round pneumonia Lung abscess Tb, NTMB Fungal Coccidiomycosis Histoplasmosis Blastomycosis. Cryptococcus Mycetoma Angioinvasive aspergillosis Dog heartworm Echinococcus Nocardia
70 Textbook list of infectious causes of SPN Round pneumonia Lung abscess Tb, NTMB Fungal Coccidiomycosis Histoplasmosis Blastomycosis. Cryptococcus Mycetoma Angioinvasive aspergillosis Dog heartworm Echinococcus Nocardia
71 Textbook list of infectious causes of SPN Round pneumonia Lung abscess Tb, NTMB Fungal Coccidiomycosis Histoplasmosis Blastomycosis. Cryptococcus Mycetoma Angioinvasive aspergillosis Dog heartworm Echinococcus Nocardia
72 Textbook list of infectious causes of SPN Round pneumonia Lung abscess Tb, NTMB Fungal Coccidiomycosis Histoplasmosis Blastomycosis. Cryptococcus Mycetoma Angioinvasive aspergillosis Dog heartworm Echinococcus Nocardia
73 Textbook list of infectious causes of SPN Round pneumonia Lung abscess Tb, NTMB Fungal Coccidiomycosis Histoplasmosis Blastomycosis. Cryptococcus Mycetoma Angioinvasive aspergillosis Dog heartworm Echinococcus Nocardia
74 Ruling out infectious cause of SPN Step 1 Is there infectious history? Step 2 If no infectious history but infectious CT features, do short interval follow up CT Step 3 If there is growth but still reasonable likelihood of infection, consider bronchoscopy or biopsy. Serology depending on risk factors (travel).
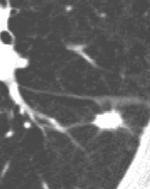
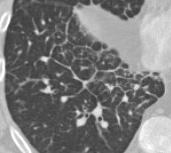
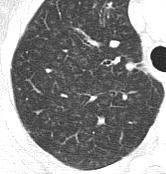
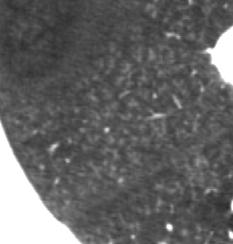
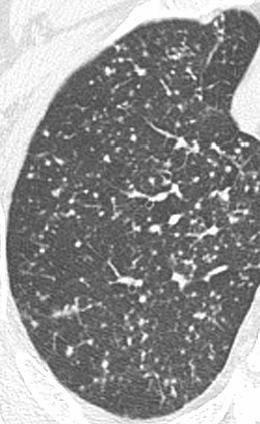
75 Case 4: Which micronodular pattern most likely represents infection? A B C D
76 A
77 B
78 C
79 D



80 Case 4: Answer Which micronodular pattern most likely represents infection? A B C D



81 Tree in bud Bronchiolar dilation and impaction Mucus, fluid, pus

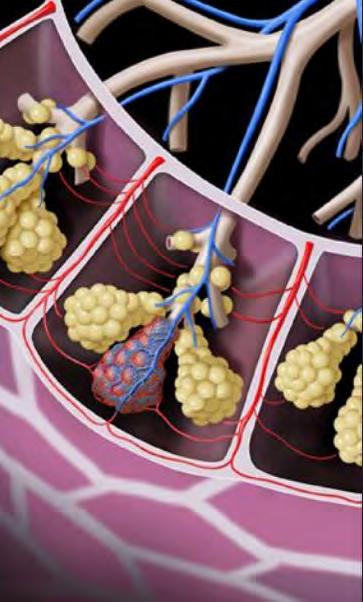
82 Secondary pulmonary lobule


83 Centilobular core Pulmonary artery Airway

84 Centrilobular Perilymphatic Random
85 Textbook causes of Tree in bud


86 Practical causes of tree in bud Acute bronchiolitis and Bronchopneumonia Majority of tree in bud is endobronchial infection. Bacterial, viral or fungal bronchopneumonia.


87 Practical causes of tree-in-bud Aspiration Inpatient Elderly Post operative Vomiting or bowel obstruction New NG tube At risk ED patient Overdose Friday night trauma Vomiting or bowel obstruction t
88 Practical causes of tree in bud Non-tuberculosis Mycobacterial Elderly women otherwise healthy Bronchiectasis especially RML and lingula TIB - may be infection or bland mucous plugs Small nodules Waxes and wanes


89 Practical causes of tree in bud Non-tuberculosis Mycobacterial Elderly women otherwise healthy Bronchiectasis especially RML and lingula TIB - may be infection or bland mucous plugs Small nodules Waxes and wanes



90 Practical causes of tree in bud When does Tree in bud = TB?? If clinical suspicion of Tb: tree-in-bud is an early and strong marker of active disease. Consider Tb: If cavitating focus. If evidence of prior disease. If risk factor. Appropriate clinical setting. Precautions and Induced sputum.
91 Does HIV + TIB = TB TIB in HIV often bacterial bronchiolitis / bronchopneumonia. Viral and bacterial TIB often basal predominant. TIB in TB often asymmetric and more often both upper and lower lung involved.


92 Practical causes of tree in bud Beware isolated TIB Possible obstructing tumor Look for subtle central mass If no infectious symptoms/high risk - do bronch If unclear follow up


93 Practical causes of tree in bud? Active disease. Don t overcall Tree in bud can simply represent mucus impaction in bronchiectasis.
94 Radiologic pattern of disease Lobar pneumonia Bacteria, bacteria, bacteria. If immunocompromise consider TB. If organ transplant consider Nocardia. Multifocal airspace Type and level of immunocompromise become more important than radiologic pattern. Nodular fungal, mycobacteria, nocardia more likely. Interstitial or GGO PCP + viral more likely (especially in no effusion, no nodes)
95 If you are just waking up: ü History (type of immunocompromise and timing) may better predict specific infectious agent than CT appearance. ü A dominant pattern of GGO in an immunocompromised patient is worrisome for opportunistic infection, including PCP. ü Consider adenocarcinoma or lymphoma in air space consolidation progressing over months. ü Tree-in-bud nodularity is often infection or aspiration. ü When reporting a CT always review indication for the original CXR *Heussel et al. AJR 1997;169:
96 Thank you.
Resident Case Review CHEST. Daria Manos CAR 2016
 Resident Case Review CHEST CAR 2016 Daria Manos Disclosure Speakers bureau, Roche CAR 2016 Daria Manos 1. Recognize common and critical chest radiograph and computed tomography signs and use these clues
Resident Case Review CHEST CAR 2016 Daria Manos Disclosure Speakers bureau, Roche CAR 2016 Daria Manos 1. Recognize common and critical chest radiograph and computed tomography signs and use these clues
Acute and Chronic Lung Disease
 KATHOLIEKE UNIVERSITEIT LEUVEN Faculty of Medicine Acute and Chronic Lung Disease W De Wever, JA Verschakelen Department of Radiology, University Hospitals Leuven, Belgium Clinical utility of HRCT To detect
KATHOLIEKE UNIVERSITEIT LEUVEN Faculty of Medicine Acute and Chronic Lung Disease W De Wever, JA Verschakelen Department of Radiology, University Hospitals Leuven, Belgium Clinical utility of HRCT To detect
Immunocompromised patients. Immunocompromised patients. Immunocompromised patients
 Value of CT in Early Pneumonia in Immunocompromised Patients Nantaka Kiranantawat, PSU Preventative Factors Phagocyts Cellular immunity Humoral immunity Predisposing Factors Infection, Stress, Poor nutrition,
Value of CT in Early Pneumonia in Immunocompromised Patients Nantaka Kiranantawat, PSU Preventative Factors Phagocyts Cellular immunity Humoral immunity Predisposing Factors Infection, Stress, Poor nutrition,
11/10/2014. Multi-disciplinary Approach to Diffuse Lung Disease: The Imager s Perspective. Radiology
 Multi-disciplinary Approach to Diffuse Lung Disease: The Imager s Perspective Radiology Pathology Clinical 1 Role of HRCT Diagnosis Fibrosis vs. inflammation Next step in management Response to treatment
Multi-disciplinary Approach to Diffuse Lung Disease: The Imager s Perspective Radiology Pathology Clinical 1 Role of HRCT Diagnosis Fibrosis vs. inflammation Next step in management Response to treatment
Daria Manos RSNA 2016 RC 401. https://medicine.dal.ca/departments/depar tment-sites/radiology/contact/faculty/dariamanos.html
 Daria Manos RSNA 2016 RC 401 https://medicine.dal.ca/departments/depar tment-sites/radiology/contact/faculty/dariamanos.html STEP1: Is this fibrotic lung disease? STEP 2: Is this a UIP pattern? If yes:
Daria Manos RSNA 2016 RC 401 https://medicine.dal.ca/departments/depar tment-sites/radiology/contact/faculty/dariamanos.html STEP1: Is this fibrotic lung disease? STEP 2: Is this a UIP pattern? If yes:
Case 1 : Question. 1.1 What is the intralobular distribution? 1. Centrilobular 2. Perilymphatic 3. Random
 Interesting case Case 1 Case 1 : Question 1.1 What is the intralobular distribution? 1. Centrilobular 2. Perilymphatic 3. Random Case 1: Answer 1.1 What is the intralobular distribution? 1. Centrilobular
Interesting case Case 1 Case 1 : Question 1.1 What is the intralobular distribution? 1. Centrilobular 2. Perilymphatic 3. Random Case 1: Answer 1.1 What is the intralobular distribution? 1. Centrilobular
TB Intensive Houston, Texas
 TB Intensive Houston, Texas October 15-17, 17 2013 Diagnosis of TB: Radiology Rosa M Estrada-Y-Martin, MD MSc FCCP October 16, 2013 Rosa M Estrada-Y-Martin, MD MSc FCCP, has the following disclosures to
TB Intensive Houston, Texas October 15-17, 17 2013 Diagnosis of TB: Radiology Rosa M Estrada-Y-Martin, MD MSc FCCP October 16, 2013 Rosa M Estrada-Y-Martin, MD MSc FCCP, has the following disclosures to
HRCT in Diffuse Interstitial Lung Disease Steps in High Resolution CT Diagnosis. Where are the lymphatics? Anatomic distribution
 Steps in High Resolution CT Diagnosis Pattern of abnormality Distribution of disease Associated findings Clinical history Tomás Franquet MD What is the diagnosis? Hospital de Sant Pau. Barcelona Secondary
Steps in High Resolution CT Diagnosis Pattern of abnormality Distribution of disease Associated findings Clinical history Tomás Franquet MD What is the diagnosis? Hospital de Sant Pau. Barcelona Secondary
Financial disclosure COMMON DIAGNOSES IN HRCT. High Res Chest HRCT. HRCT Pre test. I have no financial relationships to disclose. Anatomy Nomenclature
 Financial disclosure I have no financial relationships to disclose. Douglas Johnson D.O. Cardiothoracic Imaging Gaston Radiology COMMON DIAGNOSES IN HRCT High Res Chest Anatomy Nomenclature HRCT Sampling
Financial disclosure I have no financial relationships to disclose. Douglas Johnson D.O. Cardiothoracic Imaging Gaston Radiology COMMON DIAGNOSES IN HRCT High Res Chest Anatomy Nomenclature HRCT Sampling
Surgical indications: Non-malignant pulmonary diseases. Punnarerk Thongcharoen
 Surgical indications: Non-malignant pulmonary diseases Punnarerk Thongcharoen Non-malignant Malignant as a pathological term: Cancer Non-malignant = not cancer Malignant as an adjective: Disposed to cause
Surgical indications: Non-malignant pulmonary diseases Punnarerk Thongcharoen Non-malignant Malignant as a pathological term: Cancer Non-malignant = not cancer Malignant as an adjective: Disposed to cause
Pulmonary Aspergillosis
 May 2005 Pulmonary Aspergillosis Nancy Wei, Harvard Medical School, Year III Overview Pulmonary aspergillosis background information Patient presentations Common radiographic findings for each type of
May 2005 Pulmonary Aspergillosis Nancy Wei, Harvard Medical School, Year III Overview Pulmonary aspergillosis background information Patient presentations Common radiographic findings for each type of
Interesting Cases. Pulmonary
 Interesting Cases Pulmonary 54M with prior history of COPD, hep B/C, and possible history of TB presented with acute on chronic dyspnea, and productive cough Hazy opacity overlying the left hemithorax
Interesting Cases Pulmonary 54M with prior history of COPD, hep B/C, and possible history of TB presented with acute on chronic dyspnea, and productive cough Hazy opacity overlying the left hemithorax
Case 1: Question. 1.1 What is the main pattern of this HRCT? 1. Intralobular line 2. Groundglass opacity 3. Perilymphatic nodule
 HRCT WORK SHOP Case 1 Case 1: Question 1.1 What is the main pattern of this HRCT? 1. Intralobular line 2. Groundglass opacity 3. Perilymphatic nodule Case 1: Question 1.2 What is the diagnosis? 1. Hypersensitivity
HRCT WORK SHOP Case 1 Case 1: Question 1.1 What is the main pattern of this HRCT? 1. Intralobular line 2. Groundglass opacity 3. Perilymphatic nodule Case 1: Question 1.2 What is the diagnosis? 1. Hypersensitivity
Interstitial syndrome
 Interstitial syndrome Ground-glass attenuation Miliary and nodular images linear images Etienne Leroy Terquem Pierre L Her SPI / ISP Soutien Pneumologique International / International Support for Pulmonology
Interstitial syndrome Ground-glass attenuation Miliary and nodular images linear images Etienne Leroy Terquem Pierre L Her SPI / ISP Soutien Pneumologique International / International Support for Pulmonology
Chest Radiology Interpretation: Findings of Tuberculosis
 Chest Radiology Interpretation: Findings of Tuberculosis Get out your laptops, smart phones or other devices pollev.com/chestradiology Case #1 1 Plombage Pneumonia Cancer 2 Reading the TB CXR Be systematic!
Chest Radiology Interpretation: Findings of Tuberculosis Get out your laptops, smart phones or other devices pollev.com/chestradiology Case #1 1 Plombage Pneumonia Cancer 2 Reading the TB CXR Be systematic!
5/9/2015. Multi-disciplinary Approach to Diffuse Lung Disease: The Imager s Perspective. No, I am not a pulmonologist! Radiology
 Multi-disciplinary Approach to Diffuse Lung Disease: The Imager s Perspective No, I am not a pulmonologist! Radiology Pathology Clinical 1 Everyone needs a CT Confidence in diagnosis Definitive HRCT +
Multi-disciplinary Approach to Diffuse Lung Disease: The Imager s Perspective No, I am not a pulmonologist! Radiology Pathology Clinical 1 Everyone needs a CT Confidence in diagnosis Definitive HRCT +
objectives Pitfalls and Pearls in PET/CT imaging Kevin Robinson, DO Assistant Professor Department of Radiology Michigan State University
 objectives Pitfalls and Pearls in PET/CT imaging Kevin Robinson, DO Assistant Professor Department of Radiology Michigan State University To determine the regions of physiologic activity To understand
objectives Pitfalls and Pearls in PET/CT imaging Kevin Robinson, DO Assistant Professor Department of Radiology Michigan State University To determine the regions of physiologic activity To understand
Lung Injury after HCT
 Lung Injury after HCT J. Douglas Rizzo, MD, MS Financial Disclosure None SCS06_1.ppt Background HCT an important therapeutic modality for malignant and non-malignant diseases Pulmonary Toxicity common
Lung Injury after HCT J. Douglas Rizzo, MD, MS Financial Disclosure None SCS06_1.ppt Background HCT an important therapeutic modality for malignant and non-malignant diseases Pulmonary Toxicity common
Bronchiectasis: An Imaging Approach
 Bronchiectasis: An Imaging Approach Travis S Henry, MD Associate Professor of Clinical Radiology Cardiac and Pulmonary Imaging Section University of California, San Francisco Large Middle Small 1 Bronchiectasis
Bronchiectasis: An Imaging Approach Travis S Henry, MD Associate Professor of Clinical Radiology Cardiac and Pulmonary Imaging Section University of California, San Francisco Large Middle Small 1 Bronchiectasis
Manish Powari Regional Training Day 10/12/2014
 Manish Powari Regional Training Day 10/12/2014 Large number of different types of Interstitial Lung Disease (ILD). Most are very rare Most patients present with one of a smaller number of commoner diseases
Manish Powari Regional Training Day 10/12/2014 Large number of different types of Interstitial Lung Disease (ILD). Most are very rare Most patients present with one of a smaller number of commoner diseases
Radiological Imaging in pneumonia and its complications
 Radiological Imaging in pneumonia and its complications Cornelia Schaefer-Prokop Meander Medical Center Amersfoort Radboud University Nijmegen Netherlands Outline Radiographic patterns Infections in immunocompromised
Radiological Imaging in pneumonia and its complications Cornelia Schaefer-Prokop Meander Medical Center Amersfoort Radboud University Nijmegen Netherlands Outline Radiographic patterns Infections in immunocompromised
RADIOLOGIC EVALUATION OF PULMONARY NTM INFECTION. Tilman Koelsch, MD National Jewish Health - Department of Radiology
 Pr N op ot e fo rty rr o f ep Pr ro es du en ct te io r n RADIOLOGIC EVALUATION OF PULMONARY NTM INFECTION Tilman Koelsch, MD National Jewish Health - Department of Radiology Disclosures None Goals Identify
Pr N op ot e fo rty rr o f ep Pr ro es du en ct te io r n RADIOLOGIC EVALUATION OF PULMONARY NTM INFECTION Tilman Koelsch, MD National Jewish Health - Department of Radiology Disclosures None Goals Identify
Eun-Young Kang, M.D., Jae Wook Lee, M.D., Ji Yung Choo, M.D., Hwan Seok Yong, M.D., Ki Yeol Lee, M.D., Yu-Whan Oh, M.D.
 Eun-Young Kang, M.D., Jae Wook Lee, M.D., Ji Yung Choo, M.D., Hwan Seok Yong, M.D., Ki Yeol Lee, M.D., Yu-Whan Oh, M.D. Department of Radiology, Korea University Guro Hospital, College of Medicine, Korea
Eun-Young Kang, M.D., Jae Wook Lee, M.D., Ji Yung Choo, M.D., Hwan Seok Yong, M.D., Ki Yeol Lee, M.D., Yu-Whan Oh, M.D. Department of Radiology, Korea University Guro Hospital, College of Medicine, Korea
11/19/2012. The spectrum of pulmonary diseases in HIV-infected persons is broad.
 The spectrum of pulmonary diseases in HIV-infected persons is broad. HIV-associated Opportunistic infections Neoplasms Miscellaneous conditions Non HIV-associated Antiretroviral therapy (ART)-associated
The spectrum of pulmonary diseases in HIV-infected persons is broad. HIV-associated Opportunistic infections Neoplasms Miscellaneous conditions Non HIV-associated Antiretroviral therapy (ART)-associated
Eosinophilic lung diseases
 Eosinophilic lung diseases Chai Gin Tsen Department of Respiratory and Critical Care Medicine Tan Tock Seng Hospital The eyes do not see what the mind does not know Not very common A high index of suspicion
Eosinophilic lung diseases Chai Gin Tsen Department of Respiratory and Critical Care Medicine Tan Tock Seng Hospital The eyes do not see what the mind does not know Not very common A high index of suspicion
Pulmonary Nodules & Masses
 Pulmonary Nodules & Masses A Diagnostic Approach Heber MacMahon The University of Chicago Department of Radiology Disclosure Information Consultant for Riverain Technology Minor equity in Hologic Royalties
Pulmonary Nodules & Masses A Diagnostic Approach Heber MacMahon The University of Chicago Department of Radiology Disclosure Information Consultant for Riverain Technology Minor equity in Hologic Royalties
OBJECTIVES. Solitary Solid Spiculated Nodule. What would you do next? Case Based Discussion: State of the Art Management of Lung Nodules.
 Organ Imaging : September 25 2015 OBJECTIVES Case Based Discussion: State of the Art Management of Lung Nodules Dr. Elsie T. Nguyen Dr. Kazuhiro Yasufuku 1. To review guidelines for follow up and management
Organ Imaging : September 25 2015 OBJECTIVES Case Based Discussion: State of the Art Management of Lung Nodules Dr. Elsie T. Nguyen Dr. Kazuhiro Yasufuku 1. To review guidelines for follow up and management
The Dr. Jae Yang Lecture: An Overview of the Radiographic Picture of TB
 The Dr. Jae Yang Lecture: An Overview of the Radiographic Picture of TB Harvey H. Wong, MD FRCPC MScCH Assistant Professor Department of Medicine Division of Respirology University of Toronto Financial
The Dr. Jae Yang Lecture: An Overview of the Radiographic Picture of TB Harvey H. Wong, MD FRCPC MScCH Assistant Professor Department of Medicine Division of Respirology University of Toronto Financial
How to Analyse Difficult Chest CT
 How to Analyse Difficult Chest CT Complex diseases are:- - Large lesion - Unusual or atypical pattern - Multiple discordant findings Diffuse diseases are:- - Numerous findings in both sides 3 basic steps
How to Analyse Difficult Chest CT Complex diseases are:- - Large lesion - Unusual or atypical pattern - Multiple discordant findings Diffuse diseases are:- - Numerous findings in both sides 3 basic steps
The Pulmonary Pathology of Iatrogenic Immunosuppression. Kevin O. Leslie, M.D. Mayo Clinic Scottsdale
 The Pulmonary Pathology of Iatrogenic Immunosuppression Kevin O. Leslie, M.D. Mayo Clinic Scottsdale The indications for iatrogenic immunosuppression Autoimmune/inflammatory disease Chemotherapy for malignant
The Pulmonary Pathology of Iatrogenic Immunosuppression Kevin O. Leslie, M.D. Mayo Clinic Scottsdale The indications for iatrogenic immunosuppression Autoimmune/inflammatory disease Chemotherapy for malignant
CT findings in multifocal or diffuse non-mucinous bronchioloalveolar carcinoma (BAC)
") CT findings in multifocal or diffuse non-mucinous bronchioloalveolar carcinoma (BAC) Poster No.: C-2192 Congress: ECR 2014 Type: Educational Exhibit Authors: I. Sandu, A. R. Popita, I.-A. Brumboiu; Cluj-Napoca/RO
CT findings in multifocal or diffuse non-mucinous bronchioloalveolar carcinoma (BAC) Poster No.: C-2192 Congress: ECR 2014 Type: Educational Exhibit Authors: I. Sandu, A. R. Popita, I.-A. Brumboiu; Cluj-Napoca/RO
CT findings in multifocal or diffuse non-mucinous bronchioloalveolar carcinoma (BAC)
") CT findings in multifocal or diffuse non-mucinous bronchioloalveolar carcinoma (BAC) Poster No.: C-2192 Congress: ECR 2014 Type: Educational Exhibit Authors: I. Sandu, A. R. Popita, I.-A. Brumboiu; Cluj-Napoca/RO
CT findings in multifocal or diffuse non-mucinous bronchioloalveolar carcinoma (BAC) Poster No.: C-2192 Congress: ECR 2014 Type: Educational Exhibit Authors: I. Sandu, A. R. Popita, I.-A. Brumboiu; Cluj-Napoca/RO
Lung Cancer - Suspected
 Lung Cancer - Suspected Shared Decision Making Lung Cancer: http://www.enhertsccg.nhs.uk/ Patient presents with abnormal CXR Lung cancer - clinical presentation History and Examination Incidental finding
Lung Cancer - Suspected Shared Decision Making Lung Cancer: http://www.enhertsccg.nhs.uk/ Patient presents with abnormal CXR Lung cancer - clinical presentation History and Examination Incidental finding
HYPERSENSITIVITY PNEUMONITIS
 HYPERSENSITIVITY PNEUMONITIS A preventable fibrosis MOSAVIR ANSARIE MB., FCCP INTERSTITIAL LUNG DISEASES A heterogeneous group of non infectious, non malignant diffuse parenchymal disorders of the lower
HYPERSENSITIVITY PNEUMONITIS A preventable fibrosis MOSAVIR ANSARIE MB., FCCP INTERSTITIAL LUNG DISEASES A heterogeneous group of non infectious, non malignant diffuse parenchymal disorders of the lower
INTERSTITIAL LUNG DISEASE. Radhika Reddy MD Pulmonary/Critical Care Long Beach VA Medical Center January 5, 2018
 INTERSTITIAL LUNG DISEASE Radhika Reddy MD Pulmonary/Critical Care Long Beach VA Medical Center January 5, 2018 Interstitial Lung Disease Interstitial Lung Disease Prevalence by Diagnosis: Idiopathic Interstitial
INTERSTITIAL LUNG DISEASE Radhika Reddy MD Pulmonary/Critical Care Long Beach VA Medical Center January 5, 2018 Interstitial Lung Disease Interstitial Lung Disease Prevalence by Diagnosis: Idiopathic Interstitial
Differential diagnosis
 Differential diagnosis Idiopathic pulmonary fibrosis (IPF) is part of a large family of idiopathic interstitial pneumonias (IIP), one of four subgroups of interstitial lung disease (ILD). Differential
Differential diagnosis Idiopathic pulmonary fibrosis (IPF) is part of a large family of idiopathic interstitial pneumonias (IIP), one of four subgroups of interstitial lung disease (ILD). Differential
Pulmonary Alveolar Proteinosis
 January 2001 Pulmonary Alveolar Proteinosis Brady Case, Harvard Medical School 1 Our Patient Nelson is a 40 year-old male who presents with a 6 month history of: progressive dyspnea on exertion dry cough
January 2001 Pulmonary Alveolar Proteinosis Brady Case, Harvard Medical School 1 Our Patient Nelson is a 40 year-old male who presents with a 6 month history of: progressive dyspnea on exertion dry cough
Case of the Day Chest
 Case of the Day Chest Darin White MDCM FRCPC Department of Radiology, Mayo Clinic 76 th Annual Scientific Meeting Canadian Association of Radiologists Montreal, QC April 26, 2013 2013 MFMER slide-1 Disclosures
Case of the Day Chest Darin White MDCM FRCPC Department of Radiology, Mayo Clinic 76 th Annual Scientific Meeting Canadian Association of Radiologists Montreal, QC April 26, 2013 2013 MFMER slide-1 Disclosures
Interstitial Syndrome Ground glass attenuation miliary and nodular images Linear images
 Interstitial Syndrome Ground glass attenuation miliary and nodular images Linear images Dr Etienne Leroy-Terquem Centre hospitalier de Meulan les Mureaux. France French-cambodian association for pneumology
Interstitial Syndrome Ground glass attenuation miliary and nodular images Linear images Dr Etienne Leroy-Terquem Centre hospitalier de Meulan les Mureaux. France French-cambodian association for pneumology
Joseph Garland, HMS IV Gillian Lieberman, MD. Round Pneumonia. Joseph Garland, HMS IV Gillian Lieberman, MD
 Round Pneumonia Joseph Garland, HMS IV Case 1: Mr. H Mr. H is a 45-year-old man who presents with a 4 day history of full-body myalgias, headaches and fever to 103 F. He also complains of sharp leftsided
Round Pneumonia Joseph Garland, HMS IV Case 1: Mr. H Mr. H is a 45-year-old man who presents with a 4 day history of full-body myalgias, headaches and fever to 103 F. He also complains of sharp leftsided
Micronodular Lung Disease an algorithm
 Micronodular Lung Disease an algorithm H. Page McAdams, MD Department of Radiology Duke University Medical Center Durham, NC USA page.mcadams@duke.edu Question Which of the following lung diseases is MOST
Micronodular Lung Disease an algorithm H. Page McAdams, MD Department of Radiology Duke University Medical Center Durham, NC USA page.mcadams@duke.edu Question Which of the following lung diseases is MOST
TB Radiology for Nurses Garold O. Minns, MD
 TB Nurse Case Management Salina, Kansas March 31-April 1, 2010 TB Radiology for Nurses Garold O. Minns, MD April 1, 2010 TB Radiology for Nurses Highway Patrol Training Center Salina, KS April 1, 2010
TB Nurse Case Management Salina, Kansas March 31-April 1, 2010 TB Radiology for Nurses Garold O. Minns, MD April 1, 2010 TB Radiology for Nurses Highway Patrol Training Center Salina, KS April 1, 2010
Cryptogenic Organizing Pneumonia Diagnosis Approach Based on a Clinical-Radiologic-Pathologic Consensus
 Cryptogenic Organizing Pneumonia Diagnosis Approach Based on a Clinical-Radiologic-Pathologic Consensus Poster No.: C-1622 Congress: ECR 2012 Type: Scientific Exhibit Authors: C. Cordero Lares, E. Zorita
Cryptogenic Organizing Pneumonia Diagnosis Approach Based on a Clinical-Radiologic-Pathologic Consensus Poster No.: C-1622 Congress: ECR 2012 Type: Scientific Exhibit Authors: C. Cordero Lares, E. Zorita
An Image Repository for Chest CT
 An Image Repository for Chest CT Francesco Frajoli for the Chest CT in Antibody Deficiency Group An Image Repository for Chest CT he Chest CT in Antibody Deficiency Group is an international and interdisciplinary
An Image Repository for Chest CT Francesco Frajoli for the Chest CT in Antibody Deficiency Group An Image Repository for Chest CT he Chest CT in Antibody Deficiency Group is an international and interdisciplinary
RADIOLOGIC EVALUATION OF PULMONARY NTM INFECTION. Tilman Koelsch, MD National Jewish Health - Department of Radiology
 Pr N op ot er fo ty r R of ep Pr ro es du en ct te io r n RADIOLOGIC EVALUATION OF PULMONARY NTM INFECTION Tilman Koelsch, MD National Jewish Health - Department of Radiology Disclosures No relevant financial
Pr N op ot er fo ty r R of ep Pr ro es du en ct te io r n RADIOLOGIC EVALUATION OF PULMONARY NTM INFECTION Tilman Koelsch, MD National Jewish Health - Department of Radiology Disclosures No relevant financial
HIV related pulmonary infections. A radiologic pictorial review.
 HIV related pulmonary infections. A radiologic pictorial review. Poster No.: C-0836 Congress: ECR 2013 Type: Educational Exhibit Authors: N. Arcalis, P. Trallero, L. Berrocal Morales, S. Medrano, S. 1
HIV related pulmonary infections. A radiologic pictorial review. Poster No.: C-0836 Congress: ECR 2013 Type: Educational Exhibit Authors: N. Arcalis, P. Trallero, L. Berrocal Morales, S. Medrano, S. 1
Respiratory Pathology. Kristine Krafts, M.D.
 Respiratory Pathology Kristine Krafts, M.D. Normal lung: alveolar spaces Respiratory Pathology Outline Acute respiratory distress syndrome Obstructive lung diseases Restrictive lung diseases Vascular
Respiratory Pathology Kristine Krafts, M.D. Normal lung: alveolar spaces Respiratory Pathology Outline Acute respiratory distress syndrome Obstructive lung diseases Restrictive lung diseases Vascular
Pneumocystis jirovecci pneumonia: from mild disease to a real disaster. A pictorial review of the different radiologic patterns in acute settings
 Pneumocystis jirovecci pneumonia: from mild disease to a real disaster. A pictorial review of the different radiologic patterns in acute settings Poster No.: C-1425 Congress: ECR 2017 Type: Educational
Pneumocystis jirovecci pneumonia: from mild disease to a real disaster. A pictorial review of the different radiologic patterns in acute settings Poster No.: C-1425 Congress: ECR 2017 Type: Educational
An Introduction to Radiology for TB Nurses
 An Introduction to Radiology for TB Nurses Garold O. Minns, MD September 14, 2017 TB Nurse Case Management September 12 14, 2017 EXCELLENCE EXPERTISE INNOVATION Garold O. Minns, MD has the following disclosures
An Introduction to Radiology for TB Nurses Garold O. Minns, MD September 14, 2017 TB Nurse Case Management September 12 14, 2017 EXCELLENCE EXPERTISE INNOVATION Garold O. Minns, MD has the following disclosures
Outline Definition of Terms: Lexicon. Traction Bronchiectasis
 HRCT OF IDIOPATHIC INTERSTITIAL PNEUMONIAS Disclosures Genentech, Inc. Speakers Bureau Tadashi Allen, MD University of Minnesota Assistant Professor Diagnostic Radiology 10/29/2016 Outline Definition of
HRCT OF IDIOPATHIC INTERSTITIAL PNEUMONIAS Disclosures Genentech, Inc. Speakers Bureau Tadashi Allen, MD University of Minnesota Assistant Professor Diagnostic Radiology 10/29/2016 Outline Definition of
Case 1. Background. Presenting Symptoms. Schecter Case1 Differential Diagnosis of TB 1
 TB or Not TB? Case 1 Gisela Schecter, M.D., M.P.H. California Department of Public Health Background 26 year old African American male Born and raised in Bay Area of California Convicted of cocaine trafficking
TB or Not TB? Case 1 Gisela Schecter, M.D., M.P.H. California Department of Public Health Background 26 year old African American male Born and raised in Bay Area of California Convicted of cocaine trafficking
Usual Interstitial pneumonia and Nonspecific Interstitial Pneumonia. Nitra and the Gangs.
 Usual Interstitial pneumonia and Nonspecific Interstitial Pneumonia Nitra and the Gangs. บทน ำและบทท ๓, ๑๐, ๑๒, ๑๓, ๑๔, ๑๕, ๑๗ Usual Interstitial Pneumonia (UIP) Most common & basic pathologic pattern
Usual Interstitial pneumonia and Nonspecific Interstitial Pneumonia Nitra and the Gangs. บทน ำและบทท ๓, ๑๐, ๑๒, ๑๓, ๑๔, ๑๕, ๑๗ Usual Interstitial Pneumonia (UIP) Most common & basic pathologic pattern
Liebow and Carrington's original classification of IIP
 Liebow and Carrington's original classification of IIP-- 1969 Eric J. Stern MD University of Washington UIP Usual interstitial pneumonia DIP Desquamative interstitial pneumonia BIP Bronchiolitis obliterans
Liebow and Carrington's original classification of IIP-- 1969 Eric J. Stern MD University of Washington UIP Usual interstitial pneumonia DIP Desquamative interstitial pneumonia BIP Bronchiolitis obliterans
Thoracic CT pattern in lung cancer: correlation of CT and pathologic diagnosis
 19 th Congress of APSR PG of Lung Cancer (ESAP): Update of Lung Cancer Thoracic CT pattern in lung cancer: correlation of CT and pathologic diagnosis Kazuma Kishi, M.D. Department of Respiratory Medicine,
19 th Congress of APSR PG of Lung Cancer (ESAP): Update of Lung Cancer Thoracic CT pattern in lung cancer: correlation of CT and pathologic diagnosis Kazuma Kishi, M.D. Department of Respiratory Medicine,
Pathology of Pneumonia
 Pathology of Pneumonia Dr. Atif Ali Bashir Assistant Professor of Pathology College of Medicine Majma ah University Introduction: 5000 sq meters of area.! (olympic track) Filters >10,000 L of air / day!
Pathology of Pneumonia Dr. Atif Ali Bashir Assistant Professor of Pathology College of Medicine Majma ah University Introduction: 5000 sq meters of area.! (olympic track) Filters >10,000 L of air / day!
Thin-Section CT Findings in 32 Immunocompromised Patients with Cytomegalovirus Pneumonia Who Do Not Have AIDS
 Tomás Franquet 1,2 Kyung S. Lee 3 Nestor L. Müller 1 Received January 27, 2003; accepted after revision April 21, 2003. 1 Department of Radiology, Vancouver Hospital and Health Sciences Center and University
Tomás Franquet 1,2 Kyung S. Lee 3 Nestor L. Müller 1 Received January 27, 2003; accepted after revision April 21, 2003. 1 Department of Radiology, Vancouver Hospital and Health Sciences Center and University
Imaging Spectrum of Allergic Lung Disease: Hypersensitivity Reactions on the Lung Parenchyma
 Imaging Spectrum of Allergic Lung Disease: Hypersensitivity Reactions on the Lung Parenchyma Moon Sung Kim 1, Ki-Nam Lee 1, Won Jin Choi 1, Bo Ra Kim 1, Eun-Ju Kang 1 1 Department of Radiology, Dong-A
Imaging Spectrum of Allergic Lung Disease: Hypersensitivity Reactions on the Lung Parenchyma Moon Sung Kim 1, Ki-Nam Lee 1, Won Jin Choi 1, Bo Ra Kim 1, Eun-Ju Kang 1 1 Department of Radiology, Dong-A
Radiological Aspects of Pulmonary Tuberculosis in Immunocompetent Hosts
 Nov 2003 Radiological Aspects of Pulmonary Tuberculosis in Immunocompetent Hosts Josh Rempell, Harvard Medical School Year III Tuberculosis: the captain of all (wo)men of death Overall, one third of the
Nov 2003 Radiological Aspects of Pulmonary Tuberculosis in Immunocompetent Hosts Josh Rempell, Harvard Medical School Year III Tuberculosis: the captain of all (wo)men of death Overall, one third of the
Radiation Pneumonitis Joseph Junewick, MD FACR
 Radiation Pneumonitis Joseph Junewick, MD FACR 03/19/2010 History 16 year old with history of relapsed stage IV-A Hodgkin disease. Prior pulmonary involvement was irradiated. Diagnosis Radiation Pneumonitis
Radiation Pneumonitis Joseph Junewick, MD FACR 03/19/2010 History 16 year old with history of relapsed stage IV-A Hodgkin disease. Prior pulmonary involvement was irradiated. Diagnosis Radiation Pneumonitis
Pulmonary Diseases. We Move A Lot of Air. Basic Categories. Alveolar Level. Developmental
 Pulmonary Diseases We Move A Lot of Air Alveolar Level Functions Oxygenation CO 2 & ph Basic defenses Nose hairs Cilia Mucus Cough reflex Immune system Basic Categories Congenital Infectious Neoplastic
Pulmonary Diseases We Move A Lot of Air Alveolar Level Functions Oxygenation CO 2 & ph Basic defenses Nose hairs Cilia Mucus Cough reflex Immune system Basic Categories Congenital Infectious Neoplastic
Radiology Pathology Conference
 Radiology Pathology Conference Sharlin Johnykutty,, MD, Cytopathology Fellow Sara Majewski, MD, Radiology Resident Friday, August 28, 2009 Presentation material is for education purposes only. All rights
Radiology Pathology Conference Sharlin Johnykutty,, MD, Cytopathology Fellow Sara Majewski, MD, Radiology Resident Friday, August 28, 2009 Presentation material is for education purposes only. All rights
4/17/2010 C ini n ca c l a Ev E a v l a ua u t a ion o n of o ILD U dat a e t e i n I LDs
 Update in ILDs Diagnosis 101: Clinical Evaluation April 17, 2010 Jay H. Ryu, MD Mayo Clinic, Rochester MN Clinical Evaluation of ILD Outline General aspects of ILDs Classification of ILDs Clinical evaluation
Update in ILDs Diagnosis 101: Clinical Evaluation April 17, 2010 Jay H. Ryu, MD Mayo Clinic, Rochester MN Clinical Evaluation of ILD Outline General aspects of ILDs Classification of ILDs Clinical evaluation
Thoracic Surgery; An Overview
 Thoracic Surgery What we see Thoracic Surgery; An Overview James P. Locher, Jr, MD Methodist Cardiovascular and Thoracic Surgery Lung cancer Mets Fungus and TB Lung abcess and empyema Pleural based disease
Thoracic Surgery What we see Thoracic Surgery; An Overview James P. Locher, Jr, MD Methodist Cardiovascular and Thoracic Surgery Lung cancer Mets Fungus and TB Lung abcess and empyema Pleural based disease
LUNG NODULES: MODERN MANAGEMENT STRATEGIES
 Department of Radiology LUNG NODULES: MODERN MANAGEMENT STRATEGIES Christian J. Herold M.D. Department of Biomedical Imaging and Image-guided Therapy Medical University of Vienna Vienna, Austria Pulmonary
Department of Radiology LUNG NODULES: MODERN MANAGEMENT STRATEGIES Christian J. Herold M.D. Department of Biomedical Imaging and Image-guided Therapy Medical University of Vienna Vienna, Austria Pulmonary
The Spectrum of Management of Pulmonary Ground Glass Nodules
 The Spectrum of Management of Pulmonary Ground Glass Nodules Stanley S Siegelman CT Society 10/26/2011 No financial disclosures. Noguchi M et al. Cancer 75: 2844-2852, 1995. 236 surgically resected peripheral
The Spectrum of Management of Pulmonary Ground Glass Nodules Stanley S Siegelman CT Society 10/26/2011 No financial disclosures. Noguchi M et al. Cancer 75: 2844-2852, 1995. 236 surgically resected peripheral
Unit II Problem 2 Pathology: Pneumonia
 Unit II Problem 2 Pathology: Pneumonia - Definition: pneumonia is the infection of lung parenchyma which occurs especially when normal defenses are impaired such as: Cough reflex. Damage of cilia in respiratory
Unit II Problem 2 Pathology: Pneumonia - Definition: pneumonia is the infection of lung parenchyma which occurs especially when normal defenses are impaired such as: Cough reflex. Damage of cilia in respiratory
PULMONARY TUBERCULOSIS RADIOLOGY
 PULMONARY TUBERCULOSIS RADIOLOGY RADIOLOGICAL MODALITIES Medical radiophotography Radiography Fluoroscopy Linear (conventional) tomography Computed tomography Pulmonary angiography, bronchography Ultrasonography,
PULMONARY TUBERCULOSIS RADIOLOGY RADIOLOGICAL MODALITIES Medical radiophotography Radiography Fluoroscopy Linear (conventional) tomography Computed tomography Pulmonary angiography, bronchography Ultrasonography,
Pneumonia. Definition of pneumonia Infection of the lung parenchyma Usually bacterial
 Pneumonia Definition of pneumonia Infection of the lung parenchyma Usually bacterial Epidemiology of pneumonia Commonest infectious cause of death in the UK and USA Incidence - 5-11 per 1000 per year Worse
Pneumonia Definition of pneumonia Infection of the lung parenchyma Usually bacterial Epidemiology of pneumonia Commonest infectious cause of death in the UK and USA Incidence - 5-11 per 1000 per year Worse
Case Study #2. Case Study #1 cont 9/28/2011. CAPA 2011 Christy Wilson PA C. LH is 78 yowf with PMHx of metz breast CA presents
 Case Study #1 CAPA 2011 Christy Wilson PA C 46 yo female presents with community acquired PNA (CAP). Her condition worsened and she was transferred to the ICU and placed on mechanical ventilation. Describe
Case Study #1 CAPA 2011 Christy Wilson PA C 46 yo female presents with community acquired PNA (CAP). Her condition worsened and she was transferred to the ICU and placed on mechanical ventilation. Describe
Atopic Pulmonary Disease: Findings on Thoracic Imaging
 July 2003 Atopic Pulmonary Disease: Findings on Thoracic Imaging Rebecca G. Breslow Harvard Medical School Year IV Churg-Strauss Syndrome Hypersensitivity Pneumonitis Asthma Atopic Pulmonary Disease Allergic
July 2003 Atopic Pulmonary Disease: Findings on Thoracic Imaging Rebecca G. Breslow Harvard Medical School Year IV Churg-Strauss Syndrome Hypersensitivity Pneumonitis Asthma Atopic Pulmonary Disease Allergic
Hospital-acquired Pneumonia
 Hospital-acquired Pneumonia Hospital-acquired pneumonia (HAP) Pneumonia that occurs at least 2 days after hospital admission. The second most common and the leading cause of death due to hospital-acquired
Hospital-acquired Pneumonia Hospital-acquired pneumonia (HAP) Pneumonia that occurs at least 2 days after hospital admission. The second most common and the leading cause of death due to hospital-acquired
Imaging Small Airways Diseases: Not Just Air trapping. Eric J. Stern MD University of Washington
 Imaging Small Airways Diseases: Not Just Air trapping Eric J. Stern MD University of Washington What we are discussing SAD classification SAD imaging with MDCT emphasis What is a small airway? Airway with
Imaging Small Airways Diseases: Not Just Air trapping Eric J. Stern MD University of Washington What we are discussing SAD classification SAD imaging with MDCT emphasis What is a small airway? Airway with
Pathologic Assessment of Interstitial Lung Disease
 Pathologic Assessment of Interstitial Lung Disease Dry and itchy? It could be eczema or fungal infection. We don t need to worry, the drugs aren t that dangerous. Kirk D. Jones, MD UCSF Dept. of Pathology
Pathologic Assessment of Interstitial Lung Disease Dry and itchy? It could be eczema or fungal infection. We don t need to worry, the drugs aren t that dangerous. Kirk D. Jones, MD UCSF Dept. of Pathology
Clinical syndromes: experience from the bedside. Professor Rob Miller University College Hospital, London
 Clinical syndromes: experience from the bedside Professor Rob Miller University College Hospital, London Presented at ECCMID Berlin April 30 th 2013 Pneumocystis jirovecii pneumonia http://commons.wikimedia.org/wiki/file
Clinical syndromes: experience from the bedside Professor Rob Miller University College Hospital, London Presented at ECCMID Berlin April 30 th 2013 Pneumocystis jirovecii pneumonia http://commons.wikimedia.org/wiki/file
10/17/2016. Nuts and Bolts of Thoracic Radiology. Objectives. Techniques
 Nuts and Bolts of Thoracic Radiology October 20, 2016 Carleen Risaliti Objectives Understand the basics of chest radiograph Develop a system for interpreting chest radiographs Correctly identify thoracic
Nuts and Bolts of Thoracic Radiology October 20, 2016 Carleen Risaliti Objectives Understand the basics of chest radiograph Develop a system for interpreting chest radiographs Correctly identify thoracic
Bronchial syndrome. Atelectasis Draining bronchus Bronchiectasis
 Bronchial syndrome Atelectasis Draining bronchus Bronchiectasis Etienne Leroy Terquem Pierre L Her SPI / ISP Soutien Pneumologique International / International Support for Pulmonology Atelectasis Consequence
Bronchial syndrome Atelectasis Draining bronchus Bronchiectasis Etienne Leroy Terquem Pierre L Her SPI / ISP Soutien Pneumologique International / International Support for Pulmonology Atelectasis Consequence
Diagnosis of TB: Radiology David Finlay, MD
 TB Intensive Tyler, Texas June 2-4, 2010 Diagnosis of TB: Radiology David Finlay, MD June 3, 2010 2stages stages- Tuberculosis 1. primary infection 2. reactivation, or post primary disease 2 1 Primary
TB Intensive Tyler, Texas June 2-4, 2010 Diagnosis of TB: Radiology David Finlay, MD June 3, 2010 2stages stages- Tuberculosis 1. primary infection 2. reactivation, or post primary disease 2 1 Primary
A Review of Interstitial Lung Diseases
 Outline A Review of Interstitial Lung Diseases Paul J. Wolters, MD Associate Professor Department of Medicine University of California San Francisco Overview of diagnosis in ILD Why it is important Definition/Classification
Outline A Review of Interstitial Lung Diseases Paul J. Wolters, MD Associate Professor Department of Medicine University of California San Francisco Overview of diagnosis in ILD Why it is important Definition/Classification
A Review of Interstitial Lung Diseases. Paul J. Wolters, MD Associate Professor Department of Medicine University of California San Francisco
 A Review of Interstitial Lung Diseases Paul J. Wolters, MD Associate Professor Department of Medicine University of California San Francisco Outline Overview of diagnosis in ILD Why it is important Definition/Classification
A Review of Interstitial Lung Diseases Paul J. Wolters, MD Associate Professor Department of Medicine University of California San Francisco Outline Overview of diagnosis in ILD Why it is important Definition/Classification
Tuberculosis: The Essentials
 Tuberculosis: The Essentials Kendra L. Fisher, MD, PhD THORACIC TUBERCULOSIS: THE BARE ESSENTIALS Kendra Fisher MD, FRCP (C) Department of Radiology Loma Linda University Medical Center TUBERCULOSIS ()
Tuberculosis: The Essentials Kendra L. Fisher, MD, PhD THORACIC TUBERCULOSIS: THE BARE ESSENTIALS Kendra Fisher MD, FRCP (C) Department of Radiology Loma Linda University Medical Center TUBERCULOSIS ()
Diagnostic Evaluation of NTM and Bronchiectasis
 Division of Pulmonary, Critical Care and Sleep Medicine Diagnostic Evaluation of NTM and Bronchiectasis Ashwin Basavaraj, MD, FCCP NTM patient education program November 9, 2016 Involves a combination
Division of Pulmonary, Critical Care and Sleep Medicine Diagnostic Evaluation of NTM and Bronchiectasis Ashwin Basavaraj, MD, FCCP NTM patient education program November 9, 2016 Involves a combination
Diagnostic Procedures for Pulmonary Infiltrates in the Compromised Host
 Diagnostic Procedures for Pulmonary Infiltrates in the Compromised Host Michael Douvas, MD Heme/Onc Gerald Donowitz, MD - ID Eric Davis, MD - Pulmonary Disclosure Drs. Davis, Donowitz, and Douvas do not
Diagnostic Procedures for Pulmonary Infiltrates in the Compromised Host Michael Douvas, MD Heme/Onc Gerald Donowitz, MD - ID Eric Davis, MD - Pulmonary Disclosure Drs. Davis, Donowitz, and Douvas do not
Imaging of cardio-pulmonary treatment related damage. Radiotheraphy and Lung
 Imaging of cardio-pulmonary treatment related damage Dr. Andrea Borghesi Dr. Emanuele Gavazzi Department of Radiology 2 University of Brescia Radiotheraphy and Lung The goal of radiation therapy (RT) is
Imaging of cardio-pulmonary treatment related damage Dr. Andrea Borghesi Dr. Emanuele Gavazzi Department of Radiology 2 University of Brescia Radiotheraphy and Lung The goal of radiation therapy (RT) is
Mimics in chest disease: interstitial opacities
 Insights Imaging (2013) 4:9 27 DOI 10.1007/s13244-012-0207-7 PICTORIAL REVIEW Mimics in chest disease: interstitial opacities Anastasia Oikonomou & Panos Prassopoulos Received: 19 June 2012 / Revised:
Insights Imaging (2013) 4:9 27 DOI 10.1007/s13244-012-0207-7 PICTORIAL REVIEW Mimics in chest disease: interstitial opacities Anastasia Oikonomou & Panos Prassopoulos Received: 19 June 2012 / Revised:
Interpretation of Chest Radiographs Paul Christensen, MD 10/21/09. Diagnostic Evaluation. Medical Evaluation & CXR Interpretation.
 Diagnostic Evaluation Medical Evaluation & CXR Interpretation University of Michigan TB Consultant Washtenaw County Medical history Physical examination Testing for TB exposure (previously covered) Radiologic
Diagnostic Evaluation Medical Evaluation & CXR Interpretation University of Michigan TB Consultant Washtenaw County Medical history Physical examination Testing for TB exposure (previously covered) Radiologic
Respiratory Diseases and Disorders
 Chapter 9 Respiratory Diseases and Disorders Anatomy and Physiology Chest, lungs, and conducting airways Two parts: Upper respiratory system consists of nose, mouth, sinuses, pharynx, and larynx Lower
Chapter 9 Respiratory Diseases and Disorders Anatomy and Physiology Chest, lungs, and conducting airways Two parts: Upper respiratory system consists of nose, mouth, sinuses, pharynx, and larynx Lower
Systemic lupus erythematosus (SLE): Pleuropulmonary Manifestations
: Pleuropulmonary Manifestations") 08/30/10 09/26/10 Systemic lupus erythematosus (SLE): Pleuropulmonary Manifestations Camila Downey S. Universidad de Chile, School of Medicine, Year VII Harvard University, School of Medicine Sept 17,
08/30/10 09/26/10 Systemic lupus erythematosus (SLE): Pleuropulmonary Manifestations Camila Downey S. Universidad de Chile, School of Medicine, Year VII Harvard University, School of Medicine Sept 17,
TB Intensive San Antonio, Texas November 29-December 2, 2011
 TB Intensive San Antonio, Texas November 29-December 2, 2011 Diagnosis of TB: Radiology Michael McCarthy, MD, FACR November 30, 2011 Michael McCarthy, MD, FACR has the following disclosures to make: No
TB Intensive San Antonio, Texas November 29-December 2, 2011 Diagnosis of TB: Radiology Michael McCarthy, MD, FACR November 30, 2011 Michael McCarthy, MD, FACR has the following disclosures to make: No
Judith A. Aberg, MD; Linda M. Mundy, MD; and William G. Powderly, MD
 Pulmonary Cryptococcosis in Patients Without HIV Infection* Judith A. Aberg, MD; Linda M. Mundy, MD; and William G. Powderly, MD Purpose: To further elucidate the diagnostic and therapeutic approaches
Pulmonary Cryptococcosis in Patients Without HIV Infection* Judith A. Aberg, MD; Linda M. Mundy, MD; and William G. Powderly, MD Purpose: To further elucidate the diagnostic and therapeutic approaches
Evaluation of Neck Mass. Disclosure. Learning Objectives 3/24/2014. Karen T. Pitman MD, FACS Banner MDACC, Gilbert AZ. Nothing to disclose
 Evaluation of Neck Mass Karen T. Pitman MD, FACS Banner MDACC, Gilbert AZ Nothing to disclose Disclosure Learning Objectives 1. Describe a systematic method to evaluate a patient with a neck mass 2. Select
Evaluation of Neck Mass Karen T. Pitman MD, FACS Banner MDACC, Gilbert AZ Nothing to disclose Disclosure Learning Objectives 1. Describe a systematic method to evaluate a patient with a neck mass 2. Select
HIV-associated Pulmonary Disease. Classic and Challenging Cases from the HIV/AIDS Clinic and Beyond QUESTION: HIV-associated Pulmonary Diseases
 Classic and Challenging Cases from the HIV/AIDS Clinic and Beyond Laurence Huang, MD Professor of Medicine University of California San Francisco Chief, HIV/AIDS Chest Clinic Zuckerberg San Francisco General
Classic and Challenging Cases from the HIV/AIDS Clinic and Beyond Laurence Huang, MD Professor of Medicine University of California San Francisco Chief, HIV/AIDS Chest Clinic Zuckerberg San Francisco General
How to identify interstitial pneumonias.
 How to identify interstitial pneumonias. Poster No.: C-0804 Congress: ECR 2014 Type: Educational Exhibit Authors: S. claret loaiza, M. C. Cañete Moslero, R. Carreño Gonzalez, C. de la Torre; Malaga/ES
How to identify interstitial pneumonias. Poster No.: C-0804 Congress: ECR 2014 Type: Educational Exhibit Authors: S. claret loaiza, M. C. Cañete Moslero, R. Carreño Gonzalez, C. de la Torre; Malaga/ES
Chief Complain. For chemotherapy
 Chief Complain For chemotherapy Present Illness 93.12 Progressive weakness of R t arm for 1 year X-ray: peneative lesion over right proximal humorous Bone scan: multiple increased intake Biopsy of distal
Chief Complain For chemotherapy Present Illness 93.12 Progressive weakness of R t arm for 1 year X-ray: peneative lesion over right proximal humorous Bone scan: multiple increased intake Biopsy of distal
ACUTE PULMNARY INFECTIONS: UNDERSTANDING THE CHEST RADIOGRAPH. Leonard E. Swischuk, M.D. University of Texas Medical Branch
 ACUTE PULMNARY INFECTIONS: UNDERSTANDING THE CHEST RADIOGRAPH Leonard E. Swischuk, M.D. University of Texas Medical Branch AUTHOR HAS NOTHING TO DECLARE LEARNING OBJETIVES Understand the pathophysiology
ACUTE PULMNARY INFECTIONS: UNDERSTANDING THE CHEST RADIOGRAPH Leonard E. Swischuk, M.D. University of Texas Medical Branch AUTHOR HAS NOTHING TO DECLARE LEARNING OBJETIVES Understand the pathophysiology
Clinical Radiological Pathological Conference
 Clinical Radiological Pathological Conference CASE 1: A 59-year-old female Housekeeper Live in Phuket, Thailand Progressive dyspnea for 1 year Present illness 1 year PTA : She developed dyspnea on exertion
Clinical Radiological Pathological Conference CASE 1: A 59-year-old female Housekeeper Live in Phuket, Thailand Progressive dyspnea for 1 year Present illness 1 year PTA : She developed dyspnea on exertion
THE SPECTRUM OF RADIOLOGICAL APPEARANCES IN BRONCHOSCOPICALLY PROVEN PNEUMOCYSTIS PNEUMONIA IN HIV POSITIVE ADULTS: A
 THE SPECTRUM OF RADIOLOGICAL APPEARANCES IN BRONCHOSCOPICALLY PROVEN PNEUMOCYSTIS PNEUMONIA IN HIV POSITIVE ADULTS: A retrospective analysis from Helen Joseph Hospital Dr Grace Rubin A research report
THE SPECTRUM OF RADIOLOGICAL APPEARANCES IN BRONCHOSCOPICALLY PROVEN PNEUMOCYSTIS PNEUMONIA IN HIV POSITIVE ADULTS: A retrospective analysis from Helen Joseph Hospital Dr Grace Rubin A research report
Lung Allograft Dysfunction
 Lung Allograft Dysfunction Carlos S. Restrepo M.D. Ameya Baxi M.D. Department of Radiology University of Texas Health San Antonio Disclaimer: We do not have any conflict of interest or financial gain to
Lung Allograft Dysfunction Carlos S. Restrepo M.D. Ameya Baxi M.D. Department of Radiology University of Texas Health San Antonio Disclaimer: We do not have any conflict of interest or financial gain to
Radiologists toolbox to differentiate alveolar versus interstitial lung diseases
 Radiologists toolbox to differentiate alveolar versus interstitial lung diseases Dr Sumer Shikhare, Dr Trishna Shimpi, Dr Ashish Chawla Khoo Teck Puat Hospital Singapore. Relevant financial disclosures
Radiologists toolbox to differentiate alveolar versus interstitial lung diseases Dr Sumer Shikhare, Dr Trishna Shimpi, Dr Ashish Chawla Khoo Teck Puat Hospital Singapore. Relevant financial disclosures
1/13/2014. Proper Radiographs. Proper Radiographs. A Review of Pulmonary Patterns
 Live Webinar A Review of Pulmonary Patterns Sofija R. Liles, DVM, DACVR Proper Radiographs Which views? One lateral plus ventrodorsal (at least) Left lateral is best for thorax Three views for full metastatic
Live Webinar A Review of Pulmonary Patterns Sofija R. Liles, DVM, DACVR Proper Radiographs Which views? One lateral plus ventrodorsal (at least) Left lateral is best for thorax Three views for full metastatic