Eun-Young Kang, M.D., Jae Wook Lee, M.D., Ji Yung Choo, M.D., Hwan Seok Yong, M.D., Ki Yeol Lee, M.D., Yu-Whan Oh, M.D.
|
|
|
- Buddy Nelson
- 5 years ago
- Views:
Transcription

1 Eun-Young Kang, M.D., Jae Wook Lee, M.D., Ji Yung Choo, M.D., Hwan Seok Yong, M.D., Ki Yeol Lee, M.D., Yu-Whan Oh, M.D. Department of Radiology, Korea University Guro Hospital, College of Medicine, Korea University, Seoul, Korea
2 No financial disclosures for all authors Presenting author contact information: Eun-Young Kang ) 2

3 Respiratory Tract Infection Upper respiratory tract infection: Sinusitis, Tonsillitis, Pharyngitis, Laryngitis,. Lower respiratory tract infection: Tracheobronchitis, Bronchiolitis, Pneumonia Upper respiratory tract Nasal cavity Pharynx Larynx Lower respiratory tract Trachea Bronchus Lung 3
4 Classification of Pneumonia Community-acquired pneumonia (CAP), Hospital-acquired pneumonia (HAP), Ventilator-associated pneumonia (VAP), Healthcare-associated pneumonia (HCAP) Pneumonia in normal host, Pneumonia in AIDS patients, Pneumonia in non-aids immune compromised host Acute vs Chronic, Typical vs Atypical pneumonia Bacteria, Mycoplasma, Mycobacteria, Virus, Rickettsia, Protozoa, Parasite, Fungi, Mixed pneumonia Lobar pneumonia, Bronchopneumonia, Interstitial pneumonia 4
5 CAP HAP VAP HCAP Pneumonia acquired in the community or within 48 hours of admission to a hospital Pneumonia that occurs 48 hours or more after admission, which was not incubating at the time of admission Pneumonia that arises more than hours after endotracheal intubation Pneumonia in any patient with one of the following features Hospitalized in an acute care hospital for 2 or more days within 90 days of the infection Resided in a nursing home or long-term care facility Received recent intravenous antibiotic therapy, chemotherapy, or wound care within the past 30 days of the current infection Attended a hospital or hemodialysis clinic ATS and IDSA, Am J Respir Crit Care Med 2005;171:388 5
6 Healthcare-associated Pneumonia A distinct clinical entity Between CAP and HAP Increased risk in the elderly Increased elderly populations receiving health care outside the hospital setting, including home wound care, infusion therapy, dialysis, nursing homes, and similar settings One of the most frequent causes of hospitalization and mortality in these patients is pneumonia. 6



7 Pathogens in HCAP A wide spectrum of bacterial pathogens, may be polymicrobial Viral or fungal pathogens, rare in immunocompetent hosts Multidrug-resistant pathogens Comorbidity in HCAP Respiratory Medicine 2010;104:1729 7
8 HCAP >> CAP Older patient More multiple and chronic comorbidities Less classic respiratory symptoms, more frequent extrapulmonary manifestations Increased risk for drug-resistant pathogens More severe disease Increased mortality Microbiologically different Common CAP Pathogens Streptococcus pneumoniae Haemophilus influenzae Mycoplasma pneumoniae Chlamydia pneumoniae Respiratory viruses Legionella species Gram-negative bacilli MRSA Common HCAP Pathogens MRSA Pseudomonas aeruginosa Klebsiella pneumoniae Acinetobacter species Legionella species Semin Respir Crit Care Med 2009;30:3 8
9 Pathogenesis of Pneumonia Pathogenesis Inhalation of airborne pathogens Aspiration of oropharyngeal or gastric flora An important mechanism for development of HCAP Hematogenous spread Invasion from infected adjacent structures Development and severity of pneumonia: balance between and 9
10 Aspiration-related Lung Diseases Aspiration: Accidental entrance of foreign matter into the lower respiratory tract Predominantly airway manifestation: Foreign body aspiration, Diffuse aspiration bronchiolitis Predominantly lung parenchymal manifestation: Acute diseases: Aspiration pneumonia, Aspiration pneumonitis, Near drowning Chronic diseases: Exogenous lipoid pneumonia, Interstitial lung disease Pathophysiology: Quantity and nature of the aspirated material, chronicity of aspiration, hosts defense mechanisms, hosts response to the aspirated material bronchiolitis, pneumonitis, acute pneumonia, organizing pneumonia, abscess formation, and interstitial fibrosis, 10

11 Infectious process caused by the aspiration of oropharyngeal secretions colonized by pathogenic bacteria. Aspiration pneumonia Risk factors Dysphagia: cerebrovascular diseases, Parkinson s disease, dementia, head and neck cancer,.. Poor oral hygiene - increased oropharyngeal colonization with pathogens Defects in host defenses 75% of the hospitalized patients with pneumonia were aged 70 and older 80.1% of pneumonia patients aged 70 and older were diagnosed with aspiration pneumonia. J Am Geriatr Soc. 2008;56:577 11


12 Aspiration pneumonia Imaging findings: Bronchopneumonia pattern Segmental or lobar airspace consolidation Abscess, cavitation Parapneumonic effusion, empyema Distribution: gravity dependence In supine patients, posterior segments of the upper lobes and superior segments of the lower lobes In upright patients, the posterior segments of the lower lobes 65/M, nursing home 12
13 Diffuse aspiration bronchiolitis Chronic bronchiolar inflammation secondary to recurrent occult aspiration First defined by Matsuse T et al. (Chest 1996;110:1289) Imaging findings: Chest radiographs: regional or disseminated small nodules and hyperlucency. Chest CT: diffuse centrilobular nodules with a tree-in-bud pattern. segmental and subsegmental air trapping Distribution: Unilateral or bilateral, regional or diffuse Lower lobes, dependent aspects of the lungs Associated findings: Esophageal mass, esophageal hiatal hernia, air-fluid level within the esophagus 13



14 68/M, Parkinson s disease, home-nursing care 14
15 Diagnosis of Pneumonia Combination of Clinical assessment, Microbiological tests, The presence of infiltrates on chest radiograph: the gold standard for diagnosing pneumonia when clinical and microbiologic features are supportive. 15
16 Difficulties in Diagnosis of Pneumonia in the Elderly Clinical presentation: Frequently unusual, Mild respiratory symptoms and frequent extrapulmonary manifestations in the elderly HCAP Microbiological tests: Low diagnostic rate Chest radiographs: Initially negative finding and nonspecific findings in the elderly HCAP. Biological markers: may have a greater role in the diagnosis of pneumonia. 16
17 Radiologic Assessment of Pneumonia Chest radiographs: Initial diagnostic imaging test, must be acquired in all patients with suspected pneumonia Chest CT: not routinely used, more sensitive and specific than chest radiographs Radiologic pattern approach Radiologic pattern recognition + Clinical setting such as epidemiology, patient s immune status, medical history, and laboratory data Basic radiologic patterns Airspace pneumonia Bronchopneumonia Interstitial pneumonia Nodules Cavity 17





18 Three Basic Patterns Interstitial pneumonia, Airspace pneumonia, Streptococcus pneumoniae Bronchopneumonia, Pseudomonas aeruginosa Mycoplasma pneumoniae 18






19 Nodules Nodule with GGO halo, Paragonimus westermani Micronodule, Miliary tuberculosis Small nodule, Varicella pneumonia Cavitary nodule, Septic lung, Staphylococcus aureus 19






20 Cavity Lung abscess Invasive aspergillosis Pulmonary gangrene, Necrotizing pneumonia, Pneumatocele, Aspergillus fumigatus Klebsiella pneumoniae Staphylococcus aureus 20
21 Great variations in radiologic pattern of pneumonia Same microorganism produces several patterns and radiologic patterns overlap in an individual patient Interpretation of a chest radiograph usually does not give useful clues about the causative pathogen. However, chest radiographs provide useful information about the location, extent of pneumonia, and the presence of pleural effusion. 21
22 Role of Radiologic Imaging Detecting pneumonia Determining extent and location of pneumonia Detecting complications Differentiating infection from noninfectious disease Evaluating underlying predisposing conditions Monitoring the radiologic progression and resolution Predicting infecting microorganism 22

23 Difficulties in Radiologic Assessment of Elderly HCAP Chest radiographs must be acquired initially in patients with suspected pneumonia. However, negative chest radiographs do not exclude pneumonia in patients with suspected HCAP. Problems to depict current pneumonia due to multiple comorbidities 23

24 Detection failure of chest radiography J Infect Chemother 2015;21:492 24
25 CT is superior to chest radiographs 162 patients with suspected NHCAP 147/162 (90.6%): pneumonic infiltration diagnosed by CT 10.2% (15/147): no pneumonic infiltration on CXR For diagnosing and evaluating the severity of elderly CAP 142 patients with 65 years of age or older and hospital admission for suspected CAP. 127/142 (89.4%): diagnosed by CT 9.4% (12/127): no pneumonic infiltration on CXR In 127 CAP, bilateral pneumonic infiltration are more frequently detected by CT in non-survivors than survivors (79.0% vs. 53.7%; p <0.05) Geriatr Gerontol Int 2017;17:41 Intern Med 2016;55:437 25



26 86/F, nursing home Negative chest radiographs do not exclude pneumonia. Early chest CT can provide more valuable information for elderly HCAP. 26



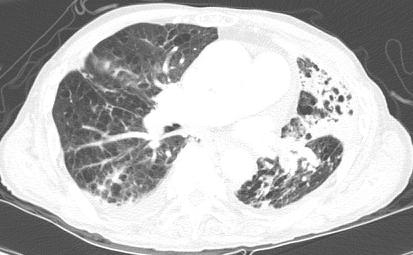
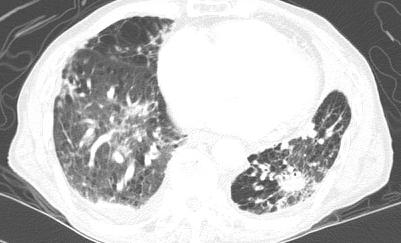

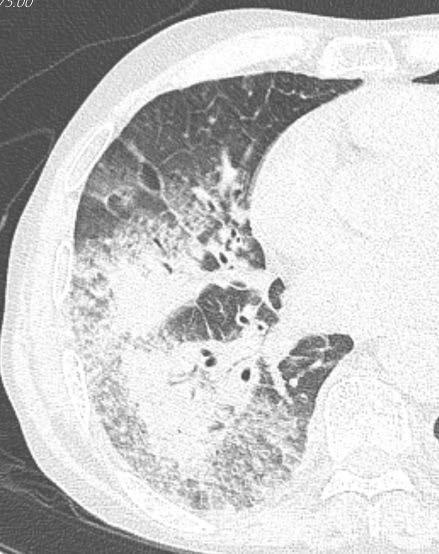
27 89/M, nursing home, Pneumonia + Previous TB + Centrilobular emphysema + Pulmonary edema + Pleural effusion Problems to depict current pneumonia due to multiple comorbidities

28 Radiologic Differential Diagnosis Pneumonia vs / and Atelectasis Pulmonary edema Tuberculosis Neoplasm Drug-induced lung disease Organizing pneumonia ARDS Not all opacity in the lung is pneumonia. Diagnosis of pneumonia can be complicated by other diseases showing lung opacities. In patients with suspected HCAP, radiologists will try to depict current pneumonia among other different diseases. 28


29 Atelectasis vs/and Pneumonia 65/M, Pneumonia: Heterogeneous, less enhanced consolidation 72/F, Atelectasis: Homogeneous, highly enhanced consolidation Atelectasis >> Pneumonia Volume loss Vessel or airway crowding Homogeneous enhancement of nonaerated lung on CT 29




30 Pulmonary edema vs/and Pneumonia Pulmonary edema >> Pneumonia Bilateral and symmetric, interstitial or airspace opacities Cardiomegaly Pleural effusion 82/M CKD and IPF, Pulmonary edema 81/M Sepsis, Pneumonia Pulmonary edema can mimic pneumonia and coexist with pneumonia. 30
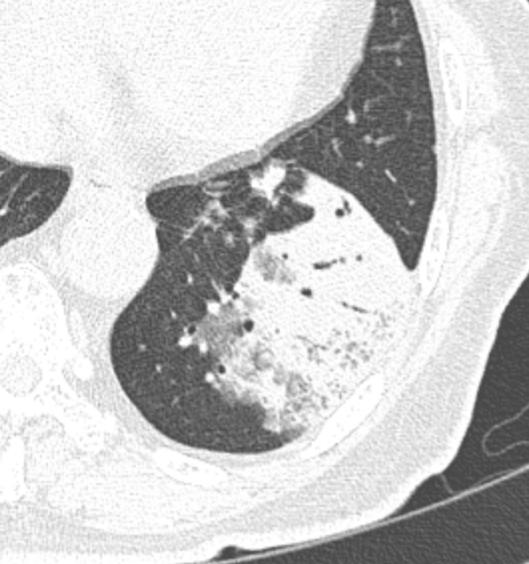
31 Pulmonary tuberculosis vs/and HCAP Concomitant TB and HCAP higher PSI scores more acute respiratory failure higher in-hospital mortality 21/701 (3%) of hospitalized HCAP patients have concomitant TB PLoS ONE 2012;7:e36832 Elderly patients with pulmonary TB TB In the elderly become an increasingly important problem More likely to present with negative sputum smears cavity negative lesions lower lung field involvement pleural effusion Infection 2008;36:335 31



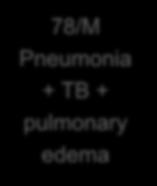
32 73/M TB 78/M Pneumonia + TB + pulmonary edema 32
33 Lung cancer vs/and Pneumonia Invasive mucinous adenocarcinoma (mucinous BAC) >> Pneumonia Stretching and sweeping of branching air-filled bronchi within consolidation Bulging contour CT angiogram sign Eur Radiol 2006;16:




34 82/F, Pneumonia with parapneumonic effusion 76/F, Mucinous adenocarcinoma with lepidic pattern 34

35 Summary Along with the rapid rise in the elderly population, the need for healthcare in the elderly population will rise quickly. The elderly are vulnerable to pneumonia. Elderly HCAP show more severe pneumonia, more drug-resistant pathogens, and worse clinical outcomes. Aspiration pneumonia is an important pathogenesis of elderly HCAP Bronchopneumonia pattern with gravity dependent distribution is common in elderly HCAP. Difficulties in radiologic assessment of elderly HCAP are due to false negative findings on initial chest radiographs and clinical overlapping pathology with multiple comorbidities. Early chest CT can provide more valuable information for elderly HCAP 35

36
Immunocompromised patients. Immunocompromised patients. Immunocompromised patients
 Value of CT in Early Pneumonia in Immunocompromised Patients Nantaka Kiranantawat, PSU Preventative Factors Phagocyts Cellular immunity Humoral immunity Predisposing Factors Infection, Stress, Poor nutrition,
Value of CT in Early Pneumonia in Immunocompromised Patients Nantaka Kiranantawat, PSU Preventative Factors Phagocyts Cellular immunity Humoral immunity Predisposing Factors Infection, Stress, Poor nutrition,
Chapter 22. Pulmonary Infections
 Chapter 22 Pulmonary Infections Objectives State the incidence of pneumonia in the United States and its economic impact. Discuss the current classification scheme for pneumonia and be able to define hospital-acquired
Chapter 22 Pulmonary Infections Objectives State the incidence of pneumonia in the United States and its economic impact. Discuss the current classification scheme for pneumonia and be able to define hospital-acquired
Hospital-acquired Pneumonia
 Hospital-acquired Pneumonia Hospital-acquired pneumonia (HAP) Pneumonia that occurs at least 2 days after hospital admission. The second most common and the leading cause of death due to hospital-acquired
Hospital-acquired Pneumonia Hospital-acquired pneumonia (HAP) Pneumonia that occurs at least 2 days after hospital admission. The second most common and the leading cause of death due to hospital-acquired
Pathology of Pneumonia
 Pathology of Pneumonia Dr. Atif Ali Bashir Assistant Professor of Pathology College of Medicine Majma ah University Introduction: 5000 sq meters of area.! (olympic track) Filters >10,000 L of air / day!
Pathology of Pneumonia Dr. Atif Ali Bashir Assistant Professor of Pathology College of Medicine Majma ah University Introduction: 5000 sq meters of area.! (olympic track) Filters >10,000 L of air / day!
Critical Care Nursing Theory. Pneumonia. - Pneumonia is an acute infection of the pulmonary parenchyma
 - is an acute infection of the pulmonary parenchyma - is a common infection encountered by critical care nurses when it complicates the course of a serious illness or leads to acute respiratory distress.
- is an acute infection of the pulmonary parenchyma - is a common infection encountered by critical care nurses when it complicates the course of a serious illness or leads to acute respiratory distress.
Unit II Problem 2 Pathology: Pneumonia
 Unit II Problem 2 Pathology: Pneumonia - Definition: pneumonia is the infection of lung parenchyma which occurs especially when normal defenses are impaired such as: Cough reflex. Damage of cilia in respiratory
Unit II Problem 2 Pathology: Pneumonia - Definition: pneumonia is the infection of lung parenchyma which occurs especially when normal defenses are impaired such as: Cough reflex. Damage of cilia in respiratory
PULMONARY TUBERCULOSIS RADIOLOGY
 PULMONARY TUBERCULOSIS RADIOLOGY RADIOLOGICAL MODALITIES Medical radiophotography Radiography Fluoroscopy Linear (conventional) tomography Computed tomography Pulmonary angiography, bronchography Ultrasonography,
PULMONARY TUBERCULOSIS RADIOLOGY RADIOLOGICAL MODALITIES Medical radiophotography Radiography Fluoroscopy Linear (conventional) tomography Computed tomography Pulmonary angiography, bronchography Ultrasonography,
Community Acquired Pneumonia. Abdullah Alharbi, MD, FCCP
 Community Acquired Pneumonia Abdullah Alharbi, MD, FCCP A 68 y/ male presented to the ED with SOB and productive coughing for 2 days. Reports poor oral intake since onset due to nausea and intermittent
Community Acquired Pneumonia Abdullah Alharbi, MD, FCCP A 68 y/ male presented to the ED with SOB and productive coughing for 2 days. Reports poor oral intake since onset due to nausea and intermittent
TB Intensive Houston, Texas
 TB Intensive Houston, Texas October 15-17, 17 2013 Diagnosis of TB: Radiology Rosa M Estrada-Y-Martin, MD MSc FCCP October 16, 2013 Rosa M Estrada-Y-Martin, MD MSc FCCP, has the following disclosures to
TB Intensive Houston, Texas October 15-17, 17 2013 Diagnosis of TB: Radiology Rosa M Estrada-Y-Martin, MD MSc FCCP October 16, 2013 Rosa M Estrada-Y-Martin, MD MSc FCCP, has the following disclosures to
HEALTHCARE-ASSOCIATED PNEUMONIA: EPIDEMIOLOGY, MICROBIOLOGY & PATHOPHYSIOLOGY
 HEALTHCARE-ASSOCIATED PNEUMONIA: EPIDEMIOLOGY, MICROBIOLOGY & PATHOPHYSIOLOGY David Jay Weber, M.D., M.P.H. Professor of Medicine, Pediatrics, & Epidemiology Associate Chief Medical Officer, UNC Health
HEALTHCARE-ASSOCIATED PNEUMONIA: EPIDEMIOLOGY, MICROBIOLOGY & PATHOPHYSIOLOGY David Jay Weber, M.D., M.P.H. Professor of Medicine, Pediatrics, & Epidemiology Associate Chief Medical Officer, UNC Health
Respiratory Diseases and Disorders
 Chapter 9 Respiratory Diseases and Disorders Anatomy and Physiology Chest, lungs, and conducting airways Two parts: Upper respiratory system consists of nose, mouth, sinuses, pharynx, and larynx Lower
Chapter 9 Respiratory Diseases and Disorders Anatomy and Physiology Chest, lungs, and conducting airways Two parts: Upper respiratory system consists of nose, mouth, sinuses, pharynx, and larynx Lower
Radiological Imaging in pneumonia and its complications
 Radiological Imaging in pneumonia and its complications Cornelia Schaefer-Prokop Meander Medical Center Amersfoort Radboud University Nijmegen Netherlands Outline Radiographic patterns Infections in immunocompromised
Radiological Imaging in pneumonia and its complications Cornelia Schaefer-Prokop Meander Medical Center Amersfoort Radboud University Nijmegen Netherlands Outline Radiographic patterns Infections in immunocompromised
an inflammation of the bronchial tubes
 BRONCHITIS DEFINITION Bronchitis is an inflammation of the bronchial tubes (or bronchi), which are the air passages that extend from the trachea into the small airways and alveoli. Triggers may be infectious
BRONCHITIS DEFINITION Bronchitis is an inflammation of the bronchial tubes (or bronchi), which are the air passages that extend from the trachea into the small airways and alveoli. Triggers may be infectious
Diagnosis of TB: Radiology David Finlay, MD
 TB Intensive Tyler, Texas June 2-4, 2010 Diagnosis of TB: Radiology David Finlay, MD June 3, 2010 2stages stages- Tuberculosis 1. primary infection 2. reactivation, or post primary disease 2 1 Primary
TB Intensive Tyler, Texas June 2-4, 2010 Diagnosis of TB: Radiology David Finlay, MD June 3, 2010 2stages stages- Tuberculosis 1. primary infection 2. reactivation, or post primary disease 2 1 Primary
Eun-Young Kang, M.D., Jae Wook Lee, M.D., Ji Yung Choo, M.D., Hwan Seok Yong, M.D., Ki Yeol Lee, M.D., Yu-Whan Oh, M.D.
 Eun-Young Kang, M.D., Jae Wook Lee, M.D., Ji Yung Choo, M.D., Hwan Seok Yong, M.D., Ki Yeol Lee, M.D., Yu-Whan Oh, M.D. Department of Radiology, Korea University Guro Hospital, College of Medicine, Korea
Eun-Young Kang, M.D., Jae Wook Lee, M.D., Ji Yung Choo, M.D., Hwan Seok Yong, M.D., Ki Yeol Lee, M.D., Yu-Whan Oh, M.D. Department of Radiology, Korea University Guro Hospital, College of Medicine, Korea
Pneumonia. Dr. Rami M Adil Al-Hayali Assistant professor in medicine
 Pneumonia Dr. Rami M Adil Al-Hayali Assistant professor in medicine Definition Pneumonia is an acute respiratory illness caused by an infection of the lung parenchyma, associated with recently developed
Pneumonia Dr. Rami M Adil Al-Hayali Assistant professor in medicine Definition Pneumonia is an acute respiratory illness caused by an infection of the lung parenchyma, associated with recently developed
POLICY FOR TREATMENT OF LOWER RESPIRATORY TRACT INFECTIONS
 POLICY F TREATMENT OF LOWER RESPIRATY TRACT INFECTIONS Written by: Dr M Milupi, Consultant Microbiologist Date: June 2018 Approved by: The Drugs & Therapeutics Committee Date: July 2018 Implementation
POLICY F TREATMENT OF LOWER RESPIRATY TRACT INFECTIONS Written by: Dr M Milupi, Consultant Microbiologist Date: June 2018 Approved by: The Drugs & Therapeutics Committee Date: July 2018 Implementation
Chapter 10 Respiratory System J00-J99. Presented by: Jesicca Andrews
 Chapter 10 Respiratory System J00-J99 Presented by: Jesicca Andrews 1 Respiratory System 2 Respiratory Infections A respiratory infection cannot be assumed from a laboratory report alone; physician concurrence
Chapter 10 Respiratory System J00-J99 Presented by: Jesicca Andrews 1 Respiratory System 2 Respiratory Infections A respiratory infection cannot be assumed from a laboratory report alone; physician concurrence
Chapter 16. Lung Abscess. Mosby items and derived items 2011, 2006 by Mosby, Inc., an affiliate of Elsevier Inc.
 Chapter 16 Lung Abscess 1 EDA PM C AFC RB A B Figure 16-1. Lung abscess. A, Cross-sectional view of lung abscess. B, Consolidation and (C) excessive bronchial secretions are common secondary anatomic alterations
Chapter 16 Lung Abscess 1 EDA PM C AFC RB A B Figure 16-1. Lung abscess. A, Cross-sectional view of lung abscess. B, Consolidation and (C) excessive bronchial secretions are common secondary anatomic alterations
Nosocomial Pneumonia. <5 Days: Non-Multidrug-Resistant Bacteria
 Nosocomial Pneumonia Meredith Deutscher, MD Troy Schaffernocker, MD Ohio State University Burden of Hospital-Acquired Pneumonia Second most common nosocomial infection in the U.S. 5-10 episodes per 1000
Nosocomial Pneumonia Meredith Deutscher, MD Troy Schaffernocker, MD Ohio State University Burden of Hospital-Acquired Pneumonia Second most common nosocomial infection in the U.S. 5-10 episodes per 1000
Community-Acquired Acinetobacter baumannii Pneumonia: Initial Chest Radiographic Findings and Follow-up CT Findings in Helping Predict Patient Outcome
 Community-Acquired Acinetobacter baumannii Pneumonia: Initial Chest Radiographic Findings and Follow-up CT Findings in Helping Predict Patient Outcome Jeong Joo Woo, Dong Hyun Lee, Jin Kyung An Department
Community-Acquired Acinetobacter baumannii Pneumonia: Initial Chest Radiographic Findings and Follow-up CT Findings in Helping Predict Patient Outcome Jeong Joo Woo, Dong Hyun Lee, Jin Kyung An Department
Lecture Notes. Chapter 16: Bacterial Pneumonia
 Lecture Notes Chapter 16: Bacterial Pneumonia Objectives Explain the epidemiology Identify the common causes Explain the pathological changes in the lung Identify clinical features Explain the treatment
Lecture Notes Chapter 16: Bacterial Pneumonia Objectives Explain the epidemiology Identify the common causes Explain the pathological changes in the lung Identify clinical features Explain the treatment
PULMONARY EMERGENCIES
 EMERGENCIES I. Pneumonia A. Bacterial Pneumonia (most common cause of a focal infiltrate) 1. Epidemiology a. Accounts for up to 10% of hospital admissions in the U.S. b. Most pneumonias are the result
EMERGENCIES I. Pneumonia A. Bacterial Pneumonia (most common cause of a focal infiltrate) 1. Epidemiology a. Accounts for up to 10% of hospital admissions in the U.S. b. Most pneumonias are the result
Pneumonia Community-Acquired Healthcare-Associated
 Pneumonia Community-Acquired Healthcare-Associated Edwin Yu Clin Infect Dis 2007;44(S2):27-72 Am J Respir Crit Care Med 2005; 171:388-416 IDSA / ATS Guidelines Microbiology Principles and Practice of Infectious
Pneumonia Community-Acquired Healthcare-Associated Edwin Yu Clin Infect Dis 2007;44(S2):27-72 Am J Respir Crit Care Med 2005; 171:388-416 IDSA / ATS Guidelines Microbiology Principles and Practice of Infectious
Radiological Aspects of Pulmonary Tuberculosis in Immunocompetent Hosts
 Nov 2003 Radiological Aspects of Pulmonary Tuberculosis in Immunocompetent Hosts Josh Rempell, Harvard Medical School Year III Tuberculosis: the captain of all (wo)men of death Overall, one third of the
Nov 2003 Radiological Aspects of Pulmonary Tuberculosis in Immunocompetent Hosts Josh Rempell, Harvard Medical School Year III Tuberculosis: the captain of all (wo)men of death Overall, one third of the
Upper...and Lower Respiratory Tract Infections
 Upper...and Lower Respiratory Tract Infections Robin Jump, MD, PhD Cleveland Geriatric Research Education and Clinical Center (GRECC) Louis Stokes Cleveland VA Medical Center Case Western Reserve University
Upper...and Lower Respiratory Tract Infections Robin Jump, MD, PhD Cleveland Geriatric Research Education and Clinical Center (GRECC) Louis Stokes Cleveland VA Medical Center Case Western Reserve University
An Introduction to Radiology for TB Nurses
 An Introduction to Radiology for TB Nurses Garold O. Minns, MD September 14, 2017 TB Nurse Case Management September 12 14, 2017 EXCELLENCE EXPERTISE INNOVATION Garold O. Minns, MD has the following disclosures
An Introduction to Radiology for TB Nurses Garold O. Minns, MD September 14, 2017 TB Nurse Case Management September 12 14, 2017 EXCELLENCE EXPERTISE INNOVATION Garold O. Minns, MD has the following disclosures
HIV related pulmonary infections. A radiologic pictorial review.
 HIV related pulmonary infections. A radiologic pictorial review. Poster No.: C-0836 Congress: ECR 2013 Type: Educational Exhibit Authors: N. Arcalis, P. Trallero, L. Berrocal Morales, S. Medrano, S. 1
HIV related pulmonary infections. A radiologic pictorial review. Poster No.: C-0836 Congress: ECR 2013 Type: Educational Exhibit Authors: N. Arcalis, P. Trallero, L. Berrocal Morales, S. Medrano, S. 1
Pathology of pulmonary tuberculosis. Dr: Salah Ahmed
 Pathology of pulmonary tuberculosis Dr: Salah Ahmed Is a chronic granulomatous disease, caused by Mycobacterium tuberculosis (hominis) Usually it involves lungs but may affect any organ or tissue Transmission:
Pathology of pulmonary tuberculosis Dr: Salah Ahmed Is a chronic granulomatous disease, caused by Mycobacterium tuberculosis (hominis) Usually it involves lungs but may affect any organ or tissue Transmission:
Sheet: Patho-Pulmonary infections Done by: Maen Faoury
 Sheet: Patho-Pulmonary infections Done by: Maen Faoury Pneumonitis : might be an infection or not. Chemical Pneumonitis : not an infection. Parenchyma : an infection.( تندرج تحت ال pneumonitis) Lung Parenchyma
Sheet: Patho-Pulmonary infections Done by: Maen Faoury Pneumonitis : might be an infection or not. Chemical Pneumonitis : not an infection. Parenchyma : an infection.( تندرج تحت ال pneumonitis) Lung Parenchyma
PNEUMONIA. I. Background 6 th most common cause of death in U.S. Most common cause of infection related mortality
 Page 1 of 8 September 4, 2001 Donald P. Levine, M.D. University Health Center Suite 5C Office: 577-0348 dlevine@intmed.wayne.edu Assigned reading: pages 153-160; 553-563 PNEUMONIA the most widespread and
Page 1 of 8 September 4, 2001 Donald P. Levine, M.D. University Health Center Suite 5C Office: 577-0348 dlevine@intmed.wayne.edu Assigned reading: pages 153-160; 553-563 PNEUMONIA the most widespread and
Chest Radiology Interpretation: Findings of Tuberculosis
 Chest Radiology Interpretation: Findings of Tuberculosis Get out your laptops, smart phones or other devices pollev.com/chestradiology Case #1 1 Plombage Pneumonia Cancer 2 Reading the TB CXR Be systematic!
Chest Radiology Interpretation: Findings of Tuberculosis Get out your laptops, smart phones or other devices pollev.com/chestradiology Case #1 1 Plombage Pneumonia Cancer 2 Reading the TB CXR Be systematic!
How to Analyse Difficult Chest CT
 How to Analyse Difficult Chest CT Complex diseases are:- - Large lesion - Unusual or atypical pattern - Multiple discordant findings Diffuse diseases are:- - Numerous findings in both sides 3 basic steps
How to Analyse Difficult Chest CT Complex diseases are:- - Large lesion - Unusual or atypical pattern - Multiple discordant findings Diffuse diseases are:- - Numerous findings in both sides 3 basic steps
INTRODUCTION TO UPPER RESPIRATORY TRACT DISEASES
 Upper Respiratory Tract Infections Return to Syllabus INTRODUCTION TO UPPER RESPIRATORY TRACT DISEASES General Goal: To know the major mechanisms of defense in the URT, the major mechanisms invaders use
Upper Respiratory Tract Infections Return to Syllabus INTRODUCTION TO UPPER RESPIRATORY TRACT DISEASES General Goal: To know the major mechanisms of defense in the URT, the major mechanisms invaders use
11/19/2012. The spectrum of pulmonary diseases in HIV-infected persons is broad.
 The spectrum of pulmonary diseases in HIV-infected persons is broad. HIV-associated Opportunistic infections Neoplasms Miscellaneous conditions Non HIV-associated Antiretroviral therapy (ART)-associated
The spectrum of pulmonary diseases in HIV-infected persons is broad. HIV-associated Opportunistic infections Neoplasms Miscellaneous conditions Non HIV-associated Antiretroviral therapy (ART)-associated
ACUTE PULMNARY INFECTIONS: UNDERSTANDING THE CHEST RADIOGRAPH. Leonard E. Swischuk, M.D. University of Texas Medical Branch
 ACUTE PULMNARY INFECTIONS: UNDERSTANDING THE CHEST RADIOGRAPH Leonard E. Swischuk, M.D. University of Texas Medical Branch AUTHOR HAS NOTHING TO DECLARE LEARNING OBJETIVES Understand the pathophysiology
ACUTE PULMNARY INFECTIONS: UNDERSTANDING THE CHEST RADIOGRAPH Leonard E. Swischuk, M.D. University of Texas Medical Branch AUTHOR HAS NOTHING TO DECLARE LEARNING OBJETIVES Understand the pathophysiology
11/10/2014. Multi-disciplinary Approach to Diffuse Lung Disease: The Imager s Perspective. Radiology
 Multi-disciplinary Approach to Diffuse Lung Disease: The Imager s Perspective Radiology Pathology Clinical 1 Role of HRCT Diagnosis Fibrosis vs. inflammation Next step in management Response to treatment
Multi-disciplinary Approach to Diffuse Lung Disease: The Imager s Perspective Radiology Pathology Clinical 1 Role of HRCT Diagnosis Fibrosis vs. inflammation Next step in management Response to treatment
TB Radiology for Nurses Garold O. Minns, MD
 TB Nurse Case Management Salina, Kansas March 31-April 1, 2010 TB Radiology for Nurses Garold O. Minns, MD April 1, 2010 TB Radiology for Nurses Highway Patrol Training Center Salina, KS April 1, 2010
TB Nurse Case Management Salina, Kansas March 31-April 1, 2010 TB Radiology for Nurses Garold O. Minns, MD April 1, 2010 TB Radiology for Nurses Highway Patrol Training Center Salina, KS April 1, 2010
Slide 120, Lobar Pneumonia. Slide 120, Lobar Pneumonia. Slide 172, Interstitial Pneumonia. Slide 172, Interstitial Pneumonia. 53 Year-Old Smoker
 Slide 120, Lobar Pneumonia Slide 120, Lobar Pneumonia Slide 172, Interstitial Pneumonia Slide 172, Interstitial Pneumonia 53 Year-Old Smoker Emphysema Pink puffer Barrel chest Hyperinflation Trapped air
Slide 120, Lobar Pneumonia Slide 120, Lobar Pneumonia Slide 172, Interstitial Pneumonia Slide 172, Interstitial Pneumonia 53 Year-Old Smoker Emphysema Pink puffer Barrel chest Hyperinflation Trapped air
Excavated pulmonary nodule: steps to diagnosis?
 Excavated pulmonary nodule: steps to diagnosis? Poster No.: C-1044 Congress: ECR 2014 Type: Authors: Keywords: DOI: Educational Exhibit W. Mnari, M. MAATOUK, A. Zrig, B. Hmida, M. GOLLI; Monastir/ TN Metastases,
Excavated pulmonary nodule: steps to diagnosis? Poster No.: C-1044 Congress: ECR 2014 Type: Authors: Keywords: DOI: Educational Exhibit W. Mnari, M. MAATOUK, A. Zrig, B. Hmida, M. GOLLI; Monastir/ TN Metastases,
RSV infection and lung ultrasound
 RSV infection and lung ultrasound Neonatology Clinic, University Hospital, Krakow Joanna Hurkała Joanna Pietras Agnieszka Ochoda-Mazur Poznań, 28.09.2018 1 Disclosure In relations to this presentation,
RSV infection and lung ultrasound Neonatology Clinic, University Hospital, Krakow Joanna Hurkała Joanna Pietras Agnieszka Ochoda-Mazur Poznań, 28.09.2018 1 Disclosure In relations to this presentation,
The RESPIRATORY System. Unit 3 Transportation Systems
 The RESPIRATORY System Unit 3 Transportation Systems The Respiratory System Functions of the Respiratory System Warms, moistens, and filters incoming air Nasal cavity Resonating chambers for speech and
The RESPIRATORY System Unit 3 Transportation Systems The Respiratory System Functions of the Respiratory System Warms, moistens, and filters incoming air Nasal cavity Resonating chambers for speech and
Respiratory Pathology. Kristine Krafts, M.D.
 Respiratory Pathology Kristine Krafts, M.D. Normal lung: alveolar spaces Respiratory Pathology Outline Acute respiratory distress syndrome Obstructive lung diseases Restrictive lung diseases Vascular
Respiratory Pathology Kristine Krafts, M.D. Normal lung: alveolar spaces Respiratory Pathology Outline Acute respiratory distress syndrome Obstructive lung diseases Restrictive lung diseases Vascular
PBL RESPIRATORY SYSTEM DR. NATHEER OBAIDAT
 PBL RESPIRATORY SYSTEM DR. NATHEER OBAIDAT Dr started to talk about his specialty at the hospital which is (ICU-Pulmonary-Internal Medicine). Pulmonary medical branch is a subspecialty of internal medicine.
PBL RESPIRATORY SYSTEM DR. NATHEER OBAIDAT Dr started to talk about his specialty at the hospital which is (ICU-Pulmonary-Internal Medicine). Pulmonary medical branch is a subspecialty of internal medicine.
Pneumonia. Definition of pneumonia Infection of the lung parenchyma Usually bacterial
 Pneumonia Definition of pneumonia Infection of the lung parenchyma Usually bacterial Epidemiology of pneumonia Commonest infectious cause of death in the UK and USA Incidence - 5-11 per 1000 per year Worse
Pneumonia Definition of pneumonia Infection of the lung parenchyma Usually bacterial Epidemiology of pneumonia Commonest infectious cause of death in the UK and USA Incidence - 5-11 per 1000 per year Worse
Pneumonia Aetiology Why is it so difficult to distinguish pathogens from innocent bystanders?
 Pneumonia Aetiology Why is it so difficult to distinguish pathogens from innocent bystanders? David Murdoch Department of Pathology University of Otago, Christchurch Outline Background Diagnostic challenges
Pneumonia Aetiology Why is it so difficult to distinguish pathogens from innocent bystanders? David Murdoch Department of Pathology University of Otago, Christchurch Outline Background Diagnostic challenges
The Respiratory System
 The Respiratory System Respiratory Anatomy Upper respiratory tract Nose Nasal passages Pharynx Larynx Respiratory Anatomy Functions of the upper respiratory tract: Provide entry for inhaled air Respiratory
The Respiratory System Respiratory Anatomy Upper respiratory tract Nose Nasal passages Pharynx Larynx Respiratory Anatomy Functions of the upper respiratory tract: Provide entry for inhaled air Respiratory
Hospital Acquired Pneumonias
 Hospital Acquired Pneumonias Hospital Acquired Pneumonia ( HAP ) Hospital acquired pneumonia ( HAP ) is defined as an infection of the lung parenchyma developing during hospitalization and not present
Hospital Acquired Pneumonias Hospital Acquired Pneumonia ( HAP ) Hospital acquired pneumonia ( HAP ) is defined as an infection of the lung parenchyma developing during hospitalization and not present
Disclosure. What are pneumonitis and pneumonia? J. Coyle, Ph.D. April 2016; WVSHA Conference 04/06/2016
 Pneumonia & Common Pulmonary Diseases in Adults West Virginia Speech Language and Hearing Association Annual Conference, Bridgeport WV April, 2016 James L. Coyle, Ph.D., CCC SLP, BCS S University of Pittsburgh
Pneumonia & Common Pulmonary Diseases in Adults West Virginia Speech Language and Hearing Association Annual Conference, Bridgeport WV April, 2016 James L. Coyle, Ph.D., CCC SLP, BCS S University of Pittsburgh
X-Rays. Prepared by Prof.Dr. Magda Hassab Allah Assist.lecturer Marwa Al Hady
 X-Rays Prepared by Prof.Dr. Magda Hassab Allah Assist.lecturer Marwa Al Hady CHEST X-RAYS Normal Chest X-ray Comments on chest X ray includes examination of 1- Bony cage (ribs,clavicles &vertebral column
X-Rays Prepared by Prof.Dr. Magda Hassab Allah Assist.lecturer Marwa Al Hady CHEST X-RAYS Normal Chest X-ray Comments on chest X ray includes examination of 1- Bony cage (ribs,clavicles &vertebral column
심사사례 성균관의대강북삼성병원감염내과 염준섭
 폐렴및호흡기질환의치료와 심사사례 성균관의대강북삼성병원감염내과 염준섭 서 론 미국 : 매년 560만명의환자발생 -- 20% 입원 사망률 - 외래에서치료가능한환자 : 1-5% - 입원치료가필요한환자 : 25% - 국내 ( 사망원인통계결과 ) : 2001년 ; 6.1명 /10만명, 1991년 ; 5.1명 /10만명 50-90% 가외래에서치료 30-40% 는원인을밝혀내지못함
폐렴및호흡기질환의치료와 심사사례 성균관의대강북삼성병원감염내과 염준섭 서 론 미국 : 매년 560만명의환자발생 -- 20% 입원 사망률 - 외래에서치료가능한환자 : 1-5% - 입원치료가필요한환자 : 25% - 국내 ( 사망원인통계결과 ) : 2001년 ; 6.1명 /10만명, 1991년 ; 5.1명 /10만명 50-90% 가외래에서치료 30-40% 는원인을밝혀내지못함
Tuberculosis: The Essentials
 Tuberculosis: The Essentials Kendra L. Fisher, MD, PhD THORACIC TUBERCULOSIS: THE BARE ESSENTIALS Kendra Fisher MD, FRCP (C) Department of Radiology Loma Linda University Medical Center TUBERCULOSIS ()
Tuberculosis: The Essentials Kendra L. Fisher, MD, PhD THORACIC TUBERCULOSIS: THE BARE ESSENTIALS Kendra Fisher MD, FRCP (C) Department of Radiology Loma Linda University Medical Center TUBERCULOSIS ()
Resident Case Review CHEST. Daria Manos CAR 2016
 Resident Case Review CHEST CAR 2016 Daria Manos Disclosure Speakers bureau, Roche CAR 2016 Daria Manos 1. Recognize common and critical chest radiograph and computed tomography signs and use these clues
Resident Case Review CHEST CAR 2016 Daria Manos Disclosure Speakers bureau, Roche CAR 2016 Daria Manos 1. Recognize common and critical chest radiograph and computed tomography signs and use these clues
Lung Cancer - Suspected
 Lung Cancer - Suspected Shared Decision Making Lung Cancer: http://www.enhertsccg.nhs.uk/ Patient presents with abnormal CXR Lung cancer - clinical presentation History and Examination Incidental finding
Lung Cancer - Suspected Shared Decision Making Lung Cancer: http://www.enhertsccg.nhs.uk/ Patient presents with abnormal CXR Lung cancer - clinical presentation History and Examination Incidental finding
Community Acquired & Nosocomial Pneumonias
 Community Acquired & Nosocomial Pneumonias IDSA/ATS 2007 & 2016 Guidelines José Luis González, MD Clinical Assistant Professor of Medicine Outline Intro - Definitions & Diagnosing CAP treatment VAP & HAP
Community Acquired & Nosocomial Pneumonias IDSA/ATS 2007 & 2016 Guidelines José Luis González, MD Clinical Assistant Professor of Medicine Outline Intro - Definitions & Diagnosing CAP treatment VAP & HAP
Surgical indications: Non-malignant pulmonary diseases. Punnarerk Thongcharoen
 Surgical indications: Non-malignant pulmonary diseases Punnarerk Thongcharoen Non-malignant Malignant as a pathological term: Cancer Non-malignant = not cancer Malignant as an adjective: Disposed to cause
Surgical indications: Non-malignant pulmonary diseases Punnarerk Thongcharoen Non-malignant Malignant as a pathological term: Cancer Non-malignant = not cancer Malignant as an adjective: Disposed to cause
and localized ground glass opacities, or bronchiolar focal or multifocal micronodules;
 E1 Chest CT scan and Pneumoniae_YE Claessens et al- Supplementary methods Level of CAP probability according to CT scan - definite CAP: systematic alveolar condensation, or alveolar condensation with peripheral
E1 Chest CT scan and Pneumoniae_YE Claessens et al- Supplementary methods Level of CAP probability according to CT scan - definite CAP: systematic alveolar condensation, or alveolar condensation with peripheral
David E. Griffith, MD has the following disclosures to make:
 Diagnosis of TB: Radiology David E. Griffith, MD March 13, 2015 TB for Pulmonologist March 13, 2015 Phoenix, AZ EXCELLENCE EXPERTISE INNOVATION David E. Griffith, MD has the following disclosures to make:
Diagnosis of TB: Radiology David E. Griffith, MD March 13, 2015 TB for Pulmonologist March 13, 2015 Phoenix, AZ EXCELLENCE EXPERTISE INNOVATION David E. Griffith, MD has the following disclosures to make:
5/9/2015. Multi-disciplinary Approach to Diffuse Lung Disease: The Imager s Perspective. No, I am not a pulmonologist! Radiology
 Multi-disciplinary Approach to Diffuse Lung Disease: The Imager s Perspective No, I am not a pulmonologist! Radiology Pathology Clinical 1 Everyone needs a CT Confidence in diagnosis Definitive HRCT +
Multi-disciplinary Approach to Diffuse Lung Disease: The Imager s Perspective No, I am not a pulmonologist! Radiology Pathology Clinical 1 Everyone needs a CT Confidence in diagnosis Definitive HRCT +
May. Pathology #2. part. Rahaf Al-yousef. Mohammad Al-Qudah
 8 th May Pathology #2 nd Pneumonias 2 part Mohammad Al-Qudah Rahaf Al-yousef In the first part of our lectures today, we will define pneumonia clinically and pathologically(which is an infection of the
8 th May Pathology #2 nd Pneumonias 2 part Mohammad Al-Qudah Rahaf Al-yousef In the first part of our lectures today, we will define pneumonia clinically and pathologically(which is an infection of the
Tuberculosis - clinical forms. Dr. A.Torossian,, M.D., Ph. D. Department of Respiratory Diseases
 Tuberculosis - clinical forms Dr. A.Torossian,, M.D., Ph. D. Department of Respiratory Diseases 1 TB DISEASE Primary Post-primary (Secondary) Common primary forms Primary complex Tuberculosis of the intrathoracic
Tuberculosis - clinical forms Dr. A.Torossian,, M.D., Ph. D. Department of Respiratory Diseases 1 TB DISEASE Primary Post-primary (Secondary) Common primary forms Primary complex Tuberculosis of the intrathoracic
The Respiratory System. Dr. Ali Ebneshahidi
 The Respiratory System Dr. Ali Ebneshahidi Functions of The Respiratory System To allow gases from the environment to enter the bronchial tree through inspiration by expanding the thoracic volume. To allow
The Respiratory System Dr. Ali Ebneshahidi Functions of The Respiratory System To allow gases from the environment to enter the bronchial tree through inspiration by expanding the thoracic volume. To allow
Patient information: Pneumonia in adults (Beyond the Basics)
") Page 1 of 8 Official reprint from UpToDate www.uptodate.com 2014 UpToDate Patient information: Pneumonia in adults (Beyond the Basics) Authors Thomas J Marrie, MD Thomas M File, Jr, MD Section Editor John
Page 1 of 8 Official reprint from UpToDate www.uptodate.com 2014 UpToDate Patient information: Pneumonia in adults (Beyond the Basics) Authors Thomas J Marrie, MD Thomas M File, Jr, MD Section Editor John
Types of infections & Mode of transmission of diseases
 Types of infections & Mode of transmission of diseases Badil dass Karachi King s College of Nursing Types of Infection Community acquired infection: Patient may acquire infection before admission to the
Types of infections & Mode of transmission of diseases Badil dass Karachi King s College of Nursing Types of Infection Community acquired infection: Patient may acquire infection before admission to the
Epiglottitis. Bronchitis. Bronchiolitis. Pneumonia. Croup syndrome. Miss. kamlah 2
 Miss. kamlah 1 Epiglottitis. Bronchitis. Bronchiolitis. Pneumonia. Croup syndrome. Miss. kamlah 2 Acute Epiglottitis Is an infection of the epiglottis, the long narrow structure that closes off the glottis
Miss. kamlah 1 Epiglottitis. Bronchitis. Bronchiolitis. Pneumonia. Croup syndrome. Miss. kamlah 2 Acute Epiglottitis Is an infection of the epiglottis, the long narrow structure that closes off the glottis
Let s Talk TB A Series on Tuberculosis, A Disease That Affects Over 2 Million Indians Every Year
 A Series on Tuberculosis, A Disease That Affects Over 2 Million Indians Every Year Barry Rabinovitch, MD, FRCP(C) Author Madhukar Pai, MD, PhD co-author and Series Editor Barry Rabinovitch is an assistant
A Series on Tuberculosis, A Disease That Affects Over 2 Million Indians Every Year Barry Rabinovitch, MD, FRCP(C) Author Madhukar Pai, MD, PhD co-author and Series Editor Barry Rabinovitch is an assistant
Invasive Pulmonary Aspergillosis in
 Infection & Sepsis Symposium Porto, April 1-3, 2009 Invasive Pulmonary Aspergillosis in Non-Immunocompromised Patients Stijn BLOT, PhD General Internal Medicine & Infectious Diseases Ghent University Hospital,
Infection & Sepsis Symposium Porto, April 1-3, 2009 Invasive Pulmonary Aspergillosis in Non-Immunocompromised Patients Stijn BLOT, PhD General Internal Medicine & Infectious Diseases Ghent University Hospital,
MDR AGENTS: RISK FACTORS AND THERAPEUTIC STRATEGIES
 MDR AGENTS: RISK FACTORS AND THERAPEUTIC STRATEGIES 1 Marin H. Kollef, MD Professor of Medicine Virginia E. and Sam J. Golman Chair in Respiratory Intensive Care Medicine Washington University School of
MDR AGENTS: RISK FACTORS AND THERAPEUTIC STRATEGIES 1 Marin H. Kollef, MD Professor of Medicine Virginia E. and Sam J. Golman Chair in Respiratory Intensive Care Medicine Washington University School of
Uses, limitations and interpretation of CT in pulmonary infections: A practical approach
 Uses, limitations and interpretation of CT in pulmonary infections: A practical approach Canadian Association of Radiologists 2013 DISCLOSURES Speakers honorarium, Siemens Canada Objectives 1. Recognize
Uses, limitations and interpretation of CT in pulmonary infections: A practical approach Canadian Association of Radiologists 2013 DISCLOSURES Speakers honorarium, Siemens Canada Objectives 1. Recognize
CAP, HCAP, HAP, VAP. 1. In 1898, William Osler described community-acquired pneumonia as:
 1. In 1898, William Osler described community-acquired pneumonia as: Brad Sharpe, M.D. Professor of Clinical Medicine Department of Medicine UCSF sharpeb@medicine.ucsf.edu I have no relevant financial
1. In 1898, William Osler described community-acquired pneumonia as: Brad Sharpe, M.D. Professor of Clinical Medicine Department of Medicine UCSF sharpeb@medicine.ucsf.edu I have no relevant financial
Acute and Chronic Lung Disease
 KATHOLIEKE UNIVERSITEIT LEUVEN Faculty of Medicine Acute and Chronic Lung Disease W De Wever, JA Verschakelen Department of Radiology, University Hospitals Leuven, Belgium Clinical utility of HRCT To detect
KATHOLIEKE UNIVERSITEIT LEUVEN Faculty of Medicine Acute and Chronic Lung Disease W De Wever, JA Verschakelen Department of Radiology, University Hospitals Leuven, Belgium Clinical utility of HRCT To detect
Epidemiology of Infectious Complications of H1N1 Influenza Virus Infection
 Epidemiology of Infectious Complications of H1N1 Influenza Virus Infection Lyn Finelli, DrPH, MS Lead, Influenza Surveillance and Outbreak Response Epidemiology and Prevention Branch Influenza Division
Epidemiology of Infectious Complications of H1N1 Influenza Virus Infection Lyn Finelli, DrPH, MS Lead, Influenza Surveillance and Outbreak Response Epidemiology and Prevention Branch Influenza Division
Key Difference - Pleural Effusion vs Pneumonia
 Difference Between Pleural Effusion and Pneumonia www.differencebetween.com Key Difference - Pleural Effusion vs Pneumonia Pleural effusion and pneumonia are two conditions that affect our respiratory
Difference Between Pleural Effusion and Pneumonia www.differencebetween.com Key Difference - Pleural Effusion vs Pneumonia Pleural effusion and pneumonia are two conditions that affect our respiratory
TB Intensive San Antonio, Texas November 29-December 2, 2011
 TB Intensive San Antonio, Texas November 29-December 2, 2011 Diagnosis of TB: Radiology Michael McCarthy, MD, FACR November 30, 2011 Michael McCarthy, MD, FACR has the following disclosures to make: No
TB Intensive San Antonio, Texas November 29-December 2, 2011 Diagnosis of TB: Radiology Michael McCarthy, MD, FACR November 30, 2011 Michael McCarthy, MD, FACR has the following disclosures to make: No
Residents Section Pattern of the Month
 Residents Section Pattern of the Month Gosset et al. Tree-In-Bud Pattern Residents Section Pattern of the Month Residents inradiology Natacha Gosset 1 Alexander A. Bankier Ronald L. Eisenberg Gosset N,
Residents Section Pattern of the Month Gosset et al. Tree-In-Bud Pattern Residents Section Pattern of the Month Residents inradiology Natacha Gosset 1 Alexander A. Bankier Ronald L. Eisenberg Gosset N,
Brice Taylor Assistant Professor Division of Pulmonary and Critical Care Medicine
 Brice Taylor Assistant Professor Division of Pulmonary and Critical Care Medicine Discuss advances in predicting prognosis Understand dwhat we know (and don t know) about the Microbiology Recognize important
Brice Taylor Assistant Professor Division of Pulmonary and Critical Care Medicine Discuss advances in predicting prognosis Understand dwhat we know (and don t know) about the Microbiology Recognize important
RADIOLOGIC EVALUATION OF PULMONARY NTM INFECTION. Tilman Koelsch, MD National Jewish Health - Department of Radiology
 Pr N op ot er fo ty r R of ep Pr ro es du en ct te io r n RADIOLOGIC EVALUATION OF PULMONARY NTM INFECTION Tilman Koelsch, MD National Jewish Health - Department of Radiology Disclosures No relevant financial
Pr N op ot er fo ty r R of ep Pr ro es du en ct te io r n RADIOLOGIC EVALUATION OF PULMONARY NTM INFECTION Tilman Koelsch, MD National Jewish Health - Department of Radiology Disclosures No relevant financial
Radiological Features of Mycobacterium tuberculosis TUBERCULE BACILLUS TUBERCULE BACILLUS DIAGNOSIS. Guy Richards. PATHOGENESIS of TUBERCULOSIS
 Radiological Features of Guy Richards Department of critical care Charlotte Maxeke Johannesburg Academic Hospital University of the Witwatersrand, Johannesburg, South Africa TUBERCULE BACILLUS Discovery
Radiological Features of Guy Richards Department of critical care Charlotte Maxeke Johannesburg Academic Hospital University of the Witwatersrand, Johannesburg, South Africa TUBERCULE BACILLUS Discovery
Anatomy & Physiology 2 Canale. Respiratory System: Exchange of Gases
 Anatomy & Physiology 2 Canale Respiratory System: Exchange of Gases Why is it so hard to hold your breath for Discuss! : ) a long time? Every year carbon monoxide poisoning kills 500 people and sends another
Anatomy & Physiology 2 Canale Respiratory System: Exchange of Gases Why is it so hard to hold your breath for Discuss! : ) a long time? Every year carbon monoxide poisoning kills 500 people and sends another
ARDS - a must know. Page 1 of 14
 ARDS - a must know Poster No.: C-1683 Congress: ECR 2016 Type: Authors: Keywords: DOI: Educational Exhibit M. Cristian; Turda/RO Education and training, Edema, Acute, Localisation, Education, Digital radiography,
ARDS - a must know Poster No.: C-1683 Congress: ECR 2016 Type: Authors: Keywords: DOI: Educational Exhibit M. Cristian; Turda/RO Education and training, Edema, Acute, Localisation, Education, Digital radiography,
WF RESPIRATORY SYSTEM. RESPIRATORY MEDICINE
 WF RESPIRATORY SYSTEM. RESPIRATORY MEDICINE 1 Societies 11 History 13 Dictionaries. Encyclopaedias. Bibliographies Use for general works only. Classify with specific aspect where possible 15 Classification.
WF RESPIRATORY SYSTEM. RESPIRATORY MEDICINE 1 Societies 11 History 13 Dictionaries. Encyclopaedias. Bibliographies Use for general works only. Classify with specific aspect where possible 15 Classification.
Respiratory System Disorders 3
 Respiratory System Disorders 3 Lecture 25 Pathology and Clinical Science 1 (BIOC211) Department of Bioscience Text Reference: Porth s Pathophysiology: Concepts of Altered Health States Sheila C. Grossman
Respiratory System Disorders 3 Lecture 25 Pathology and Clinical Science 1 (BIOC211) Department of Bioscience Text Reference: Porth s Pathophysiology: Concepts of Altered Health States Sheila C. Grossman
Systemic lupus erythematosus (SLE): Pleuropulmonary Manifestations
: Pleuropulmonary Manifestations") 08/30/10 09/26/10 Systemic lupus erythematosus (SLE): Pleuropulmonary Manifestations Camila Downey S. Universidad de Chile, School of Medicine, Year VII Harvard University, School of Medicine Sept 17,
08/30/10 09/26/10 Systemic lupus erythematosus (SLE): Pleuropulmonary Manifestations Camila Downey S. Universidad de Chile, School of Medicine, Year VII Harvard University, School of Medicine Sept 17,
Acute pneumonia Simple complement
 Acute pneumonia Simple complement 1. Clinical variants of acute pneumonia in children are, except: A. Bronchopneumonia B. Lobar confluent pneumonia C. Viral pneumonia D. Interstitial pneumonia E. Chronic
Acute pneumonia Simple complement 1. Clinical variants of acute pneumonia in children are, except: A. Bronchopneumonia B. Lobar confluent pneumonia C. Viral pneumonia D. Interstitial pneumonia E. Chronic
PNEUMONIA IN CHILDREN. IAP UG Teaching slides
 PNEUMONIA IN CHILDREN 1 INTRODUCTION 156 million new episodes / yr. worldwide 151 million episodes developing world 95% in developing countries 19% of all deaths in children
PNEUMONIA IN CHILDREN 1 INTRODUCTION 156 million new episodes / yr. worldwide 151 million episodes developing world 95% in developing countries 19% of all deaths in children
Diagnosis and Medical Management of Latent TB Infection
 Diagnosis and Medical Management of Latent TB Infection Marsha Majors, RN September 7, 2017 TB Contact Investigation 101 September 6 7, 2017 Little Rock, AR EXCELLENCE EXPERTISE INNOVATION Marsha Majors,
Diagnosis and Medical Management of Latent TB Infection Marsha Majors, RN September 7, 2017 TB Contact Investigation 101 September 6 7, 2017 Little Rock, AR EXCELLENCE EXPERTISE INNOVATION Marsha Majors,
Viral Threat on Respiratory Failure
 Viral Threat on Respiratory Failure Younsuck Koh, MD, PhD, FCCM Department of Pulmonary and Critical Care Medicine Asan Medical Center University of Ulsan College of Medicine Seoul, Korea No Conflict of
Viral Threat on Respiratory Failure Younsuck Koh, MD, PhD, FCCM Department of Pulmonary and Critical Care Medicine Asan Medical Center University of Ulsan College of Medicine Seoul, Korea No Conflict of
Diagnosis of Ventilator- Associated Pneumonia: Where are we now?
 Diagnosis of Ventilator- Associated Pneumonia: Where are we now? Gary French Guy s & St. Thomas Hospital & King s College, London BSAC Guideline 2008 Masterton R, Galloway A, French G, Street M, Armstrong
Diagnosis of Ventilator- Associated Pneumonia: Where are we now? Gary French Guy s & St. Thomas Hospital & King s College, London BSAC Guideline 2008 Masterton R, Galloway A, French G, Street M, Armstrong
Clinical and Etiological Profile of Unresolving Pneumonia Cases Attending Government Chest Hospital, Visakhapatnam
 IOSR Journal of Dental and Medical Sciences (IOSR-JDMS) e-issn: 2279-0853, p-issn: 2279-0861.Volume 14, Issue 7 Ver. VII (July. 2015), PP 56-61 www.iosrjournals.org Clinical and Etiological Profile of
IOSR Journal of Dental and Medical Sciences (IOSR-JDMS) e-issn: 2279-0853, p-issn: 2279-0861.Volume 14, Issue 7 Ver. VII (July. 2015), PP 56-61 www.iosrjournals.org Clinical and Etiological Profile of
To Study The Cinico-Radiological Features And Associated Co-Morbid Conditions
 IOSR Journal of Dental and Medical Sciences (IOSR-JDMS) e-issn: 2279-0853, p-issn: 2279-0861.Volume 17, Issue 7 Ver. 16 (July. 2018), PP 58-62 www.iosrjournals.org To study the clinico-radiological features
IOSR Journal of Dental and Medical Sciences (IOSR-JDMS) e-issn: 2279-0853, p-issn: 2279-0861.Volume 17, Issue 7 Ver. 16 (July. 2018), PP 58-62 www.iosrjournals.org To study the clinico-radiological features
RESPIRATORY TRACT INFECTIONS. CLS 212: Medical Microbiology
 RESPIRATORY TRACT INFECTIONS CLS 212: Medical Microbiology Anatomy of the Respiratory System Respiratory Infections Respiratory tract can be divided into: Upper Respiratory Tract (URT): Sinuses Nasopharynx,.
RESPIRATORY TRACT INFECTIONS CLS 212: Medical Microbiology Anatomy of the Respiratory System Respiratory Infections Respiratory tract can be divided into: Upper Respiratory Tract (URT): Sinuses Nasopharynx,.
Turkish Thoracic Society
 Türk Toraks Derneği Turkish Thoracic Society Pocket Books Series Diagnosis and Treatment of Community Acquired Pneumonia in Children Short Version (Handbook) in English www.toraks.org.tr This report was
Türk Toraks Derneği Turkish Thoracic Society Pocket Books Series Diagnosis and Treatment of Community Acquired Pneumonia in Children Short Version (Handbook) in English www.toraks.org.tr This report was
Preventing & Controlling the Spread of Infection
 Preventing & Controlling the Spread of Infection Contributors: Alice Pong M.D., Hospital Epidemiologist Chris Abe, R.N., Senior Director Ancillary and Support Services Objectives Review the magnitude of
Preventing & Controlling the Spread of Infection Contributors: Alice Pong M.D., Hospital Epidemiologist Chris Abe, R.N., Senior Director Ancillary and Support Services Objectives Review the magnitude of
The McMaster at night Pediatric Curriculum
 The McMaster at night Pediatric Curriculum Community Acquired Pneumonia Based on CPS Practice Point Pneumonia in healthy Canadian children and youth and the British Thoracic Society Guidelines on CAP Objectives
The McMaster at night Pediatric Curriculum Community Acquired Pneumonia Based on CPS Practice Point Pneumonia in healthy Canadian children and youth and the British Thoracic Society Guidelines on CAP Objectives
PULMONARY MEDICINE BOARD REVIEW. Financial Conflicts of Interest. Question #1: Question #1 (Cont.): None. Christopher H. Fanta, M.D.
: None. Christopher H. Fanta, M.D.") PULMONARY MEDICINE BOARD REVIEW Christopher H. Fanta, M.D. Pulmonary and Critical Care Division Brigham and Women s Hospital Partners Asthma Center Harvard Medical School Financial Conflicts of Interest
PULMONARY MEDICINE BOARD REVIEW Christopher H. Fanta, M.D. Pulmonary and Critical Care Division Brigham and Women s Hospital Partners Asthma Center Harvard Medical School Financial Conflicts of Interest
Unit 1: Asepsis and Infection Control
 Unit 1: Asepsis and Infection Control Outlines - Type of microorganism causing infection. - Types of infection. - Nosocomial infection. - Chain of infection. - Body defenses against infection. - Factors
Unit 1: Asepsis and Infection Control Outlines - Type of microorganism causing infection. - Types of infection. - Nosocomial infection. - Chain of infection. - Body defenses against infection. - Factors
Pneumonia Severity Scores:
 Pneumonia Severity Scores: Are they Accurate Predictors of Mortality? JILL McEWEN, MD FRCPC Clinical Professor Department of Emergency Medicine University of British Columbia Vancouver, BC Canada President,
Pneumonia Severity Scores: Are they Accurate Predictors of Mortality? JILL McEWEN, MD FRCPC Clinical Professor Department of Emergency Medicine University of British Columbia Vancouver, BC Canada President,
Community Acquired Pneumonia
 April 2014 References: 1. Bradley JS, Byington CL, Shah SS, Alverson B, Carter ER, Harrison C, Kaplan SL Mace SE, McCracken Jr. GH, Moor MR, St. Peter SD, Stockwell JA, and Swanson JT. The Management of
April 2014 References: 1. Bradley JS, Byington CL, Shah SS, Alverson B, Carter ER, Harrison C, Kaplan SL Mace SE, McCracken Jr. GH, Moor MR, St. Peter SD, Stockwell JA, and Swanson JT. The Management of
Pictorial essay of unusual radiologic manifestations of pulmonary and airway metastasis at initial presentation of lung cancer
 Pictorial essay of unusual radiologic manifestations of pulmonary and airway metastasis at initial presentation of lung cancer Poster No.: C-2297 Congress: ECR 2012 Type: Educational Exhibit Authors: Y.
Pictorial essay of unusual radiologic manifestations of pulmonary and airway metastasis at initial presentation of lung cancer Poster No.: C-2297 Congress: ECR 2012 Type: Educational Exhibit Authors: Y.