Tuberculosis Chronic infectious disease caused by Mycobacterium Tuberculosis D A P UNIBA
|
|
|
- Muriel Stanley
- 5 years ago
- Views:
Transcription
1 Chronic infectious disease caused by Mycobacterium Tuberculosis
2 Trasmission Airborne Airways- Lympha6c Inges6on (M. Bovis) Mycobacteria : aerobic bacteria forming single or branched chains Cell wall: mycolic acid (acid- alcohol fast) Reservoir for M. Tuberculosis Subjects with ac6ve tuberculosis Tuberculosis caused by M. Bovis (intes6nal) s6ll detected in countries with: Infected cows Non pasteurised milk
3 Epidemiology: spread worldwide 1,7 billion people affected by TB 8-10 million new cases every year 1,7 million deaths each year. Second most frequent infec6ous disease (1 HIV) HIV infec6on makes pa6ents prone to TB 50 millions people worldwide have HIV+TB In the U.S. from 1985 to 1992 >> than 20% of cases (>HIV) among homeless, immigrants, prisoners AYer 1993 < of cases, cases of TBC + among immigrants
4 TBC endemic in poor, overcrowded countries hit by chronic debilita6ng diseases In the U.S. typically affects the elderly, homeless and HIV pa6ents Some diseases > the risk of TBC: diabetes mellitus, Hodgkin lymphoma, chronic lung diseases (silicosis), chronic renal failure, malnutri6on, alcohol addic6on and immune suppression.
5 Mycobacterium Tuberculosis (hominis / bovis) Presence of micro- organisms Acquired through transmissions of droplets of saliva from subjects with ac6ve TB Presence of a small calcified nodule at the site of infec6on indicates previous infec6on only (micro- organisms may be quiescent, but can become ac6ve in case of immune suppression) It causes delayed hypersensi6vity to M.T. an6gens (basis for the Mantoux test)
6 Tuberculin skin test (Mantoux) Intradermal injec6on of purified protein deriva6ves (PPD) of M.T hours later: appearance of palpable nodule Posi6vity = Cell- mediated hypersensi6vity to M.T. an6gens It doesn t dis6nguish between previous infec6on and ac6ve disease False nega6ves: Viral infec6ons, sarcoidosis, malnutri6on, Hodgkin disease, immune suppression and hyperacute tubercolosis (immune system hasn t reacted to the infec6on) False posi6ves: Infec6on by atypical mycobacteria
7 Pathogenesis: Immunocompetent subject with no previous exposure depends on: Cell- mediated immunity, which allows resistance to mycobacteria and hypersensi6vity against mycobacterial an6gens Clinical manifesta6ons like caseous granulomas and forma6on of cavi6es inside the lung = hypersensi6vity of the host, aquired immunity against the microorganism

8
9 Immunocompetent subject with previous exposure to M.T. results in: Rapid ac6va6on of immune response Increased 6ssue necrosis Hypersensi6vity and resistance appear at the same 6me Loss of hypersensi6vity (PPD- ) = loss of resistance to mycroorganisms

10
11 Primary infection: focus or primary complex (pulmonary or intes6nal): - Most ven6lated areas, subpleural - Exuda6ve alveoli6s (epithelioid) - Produc6ve alveoli6s (granulomatous) - Lymphangi6s - Granulomatous lymphadeni6s Anatomic healing Clinical healing with sclerosis / calcifica6on Spread into lungs / other viscera - Lympha6c - Haematogenous - Canalicular
12 Clinical characteris6cs of TB infec6on: Primary tubercolosis occurs in subjects with no previous exposure Exogenous source Elderly people and immune- compromised pa6ents can lose their specific immunity against M.T. and so develop primary tubercolosis more than once Clinical history Latent infec6on (>>>) Progressive infec6on
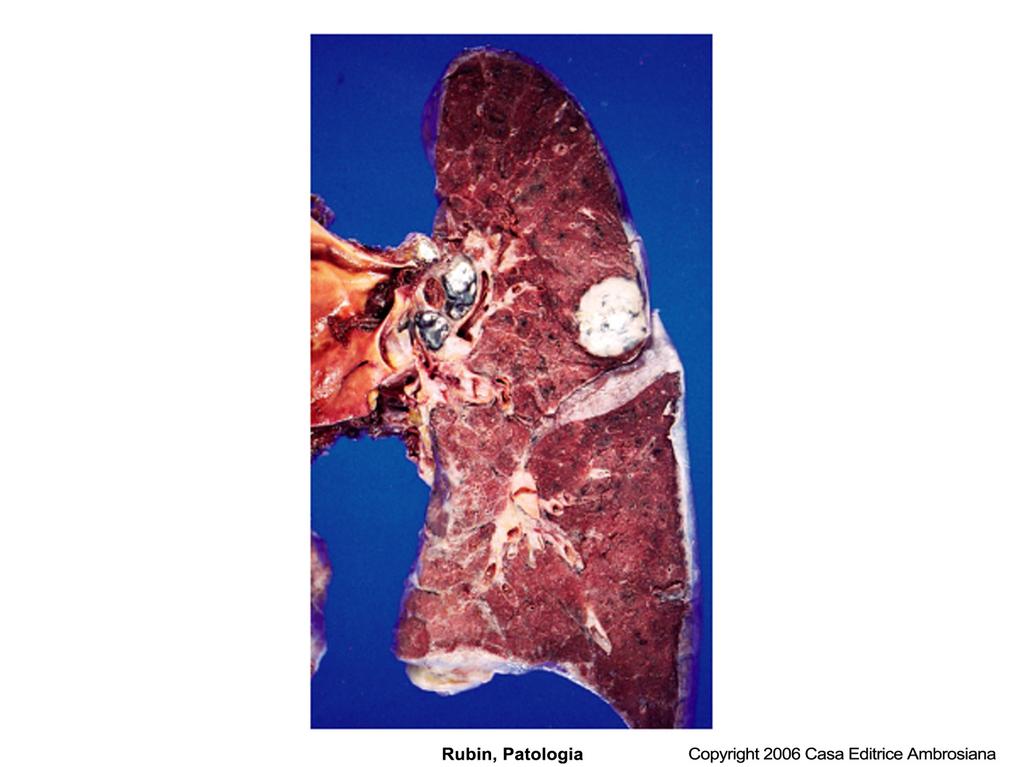
13 Morphology Primary tuberculosis: Starts in the lungs Upper lobe (lower part) Lower lobe (upper part) Peripheral (close to the pleura) Hypersensi6vity develops Primary tubercle Nodule cm 1-1,5 Grey- whi6sh Caseous necrosis = primary complex (Ghon focus) Bacilli are drained - Regional lymphonodes (caseous necrosis) = Ranke s complex Cell- mediated immunity controls the infec6on
14
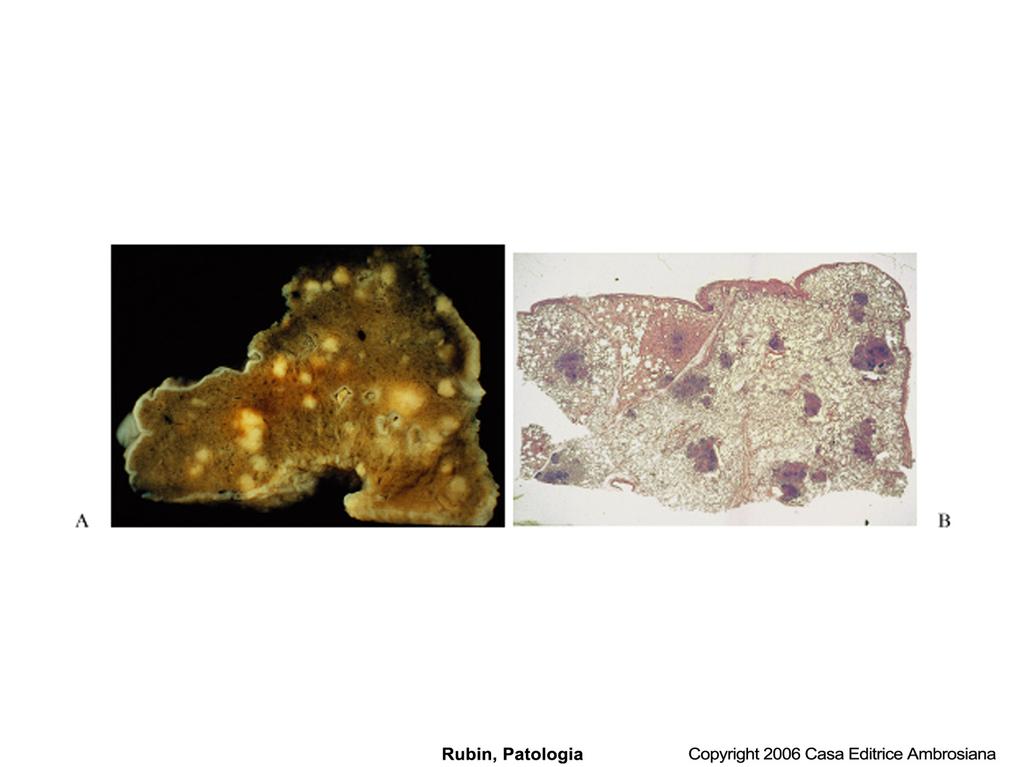
15 Histology: Granulomatous reac6on with tubercles (casea6ng or not) Single tubercles are microscopic Confluent tubercles become macroscopically evident Surrounded by fibroblast reac6on Presence of lymphocytes and mul6nucleated giant cells (Langhans cells)



16


17
18 Immediate POST-PRIMARY TB (JUVENILE) Bronchopneumonia Caseous Pneumonia Miliary TB (hematogenous or lympho- hematogenous) Chronic apical tubercolosis of Aschoff- Puhl Fibro- sclerosis of the apex
19 Secondary (post-primary) TB Pulmonary - Early subclavicular infiltrate Assmann- Redeker type (epithelioid alveoli6s of the apex) - Tubercular lobi6s - Secondary bronchopneumonia - Caseous pulmoni6s (lobi6s) - Secondary Haematogenous Miliary Renal Uterine- salpingeal Cerebro- meningeal Lymph nodal
20 Secondary tuberculosis occurs in subjects with previous sensiczacon : AYer primary tubercolosis Reac6va6on of quiescent primary lesions (even ayer many years + lower resistance of host) External re- infec6on (virulent strains or immunosuppression) Reac6va6on: frequent in areas with low prevalence Reinfec6on: important in endemic areas
21 Morphology Secondary tuberculosis Ini6al Lesion: Small focus of consolida6on (< 2 cm) Within 1-2 cm from the apical pleura Small, hard, grey- whi6sh focuses, variable caseous necrosis, peripheral fibrosis Parenchymal focus develops a fibrous capsule eventually calcified scar Histology: confluent tubercles with caseous necrosis Secondary tubercolosis of the lung can: Heal spontaneously / ayer therapy Progress

22



23
24 Complications (tertiary TB) Fibro- caseous tuberculosis Ulcero- cavernous tuberculosis - Necro6c layer - Granulomatous layer - Fibro6clayer Tubercle Pleuri6s Tb Pyo- pneumothorax TB Meningi6dis

25
26 Progressive pulmonary TB - Occurs in the elderly and immunocompromised pa6ents - Enlargement of the apical lesion with >> caseous necrosis - Bronchial erosion with draining of caseous material - Irregular cavity with indented borders, small amounts of fibro6c 6ssue - Haemoptysis (erosion of blood vessels) Adequate treatment: Fibrosis with bronchial distor6on Inadequate treatment: Infec6on spreads through airways, lympha6cs, blood
27 Miliary pulmonary TB Microrganisms are drained by lympha6c ducts Systemic veins > Right heart > Pulmonary artery Small lesions (2mm), yellow- whi6sh Spread throughout lungs Pleural cavity is involved Serous pleural effusions, tuberculous empyema, obliteracng fibrinous pleurics If infec6ous material spreads via lympha6cs or sputum Endobronchial, endotracheal or laryngeal tubercolosis

28
29 Systemic miliary TB Infec6ous lung foci spread through pulmonary veins > heart > arterial circula6on > any organ Granulomatous Tubercles Liver, Bone Marrow, Spleen, Adrenal glands, Meninges, oviducts, epididymis


30
31 Isolated organ TB Can appear in any organ or Cssue infected via blood and it can be the only manifestacon of the disease Meninges, Kidneys, Adrenal glands, Bones (osteomyelics) Oviducts, Vertebrae (PoN s disease) Lymphadeni6s Extra- pulmonary TB Tuberculous cervical adeni6s (scrofula) HIV neg. = unifocal HIV pos. = mul6focal, systemic symptoms, lungs or other organs involved Intes6nal TB Intes6nal tuberculosis nowadays appears as secondary tuberculosis due to inges6on of infected sputum
32 Oral tuberculosis Primary lesions are rare Secondary lesions are frequent, due to coughing of infected material from pulmonary lesions Chronic ulcer, painless, undermined edge, covered by yellow- greyish eschar, tongue localisacon Gingival granular lesions Cervical lymphadenics, intra- ed extra- parocdeal Diagnosis - - Biopsy Detec6on of tubercular bacilli (specific stains or special cultural methods)
Pathology of pulmonary tuberculosis. Dr: Salah Ahmed
 Pathology of pulmonary tuberculosis Dr: Salah Ahmed Is a chronic granulomatous disease, caused by Mycobacterium tuberculosis (hominis) Usually it involves lungs but may affect any organ or tissue Transmission:
Pathology of pulmonary tuberculosis Dr: Salah Ahmed Is a chronic granulomatous disease, caused by Mycobacterium tuberculosis (hominis) Usually it involves lungs but may affect any organ or tissue Transmission:
Tuberculosis. By: Shefaa Q aqa
 Tuberculosis By: Shefaa Q aqa Tuberculosis is a communicable chronic granulomatous disease caused by Mycobacterium tuberculosis. It usually involves the lungs but may affect any organ or tissue in the
Tuberculosis By: Shefaa Q aqa Tuberculosis is a communicable chronic granulomatous disease caused by Mycobacterium tuberculosis. It usually involves the lungs but may affect any organ or tissue in the
Respiratory System الفريق الطبي االكاديمي
 Respiratory System الفريق الطبي االكاديمي Pathology sheet 5 Tuberculosis Done by: Ahmad Al-Sahele Introduction: as we know TB is caused by mycobacterium tubercolosis; now keep in your mind another microorganism
Respiratory System الفريق الطبي االكاديمي Pathology sheet 5 Tuberculosis Done by: Ahmad Al-Sahele Introduction: as we know TB is caused by mycobacterium tubercolosis; now keep in your mind another microorganism
CHRONIC INFLAMMATION
 CHRONIC INFLAMMATION Chronic inflammation is an inflammatory response of prolonged duration often for months, years or even indefinitely. Its prolonged course is proved by persistence of the causative
CHRONIC INFLAMMATION Chronic inflammation is an inflammatory response of prolonged duration often for months, years or even indefinitely. Its prolonged course is proved by persistence of the causative
Mycobacterium tuberculosis. Lecture (14) Dr.Baha, AL-Amiedi Ph. D.Microbiology
 Dr.Baha, AL-Amiedi Ph. D.Microbiology") Mycobacterium tuberculosis Lecture (14) Dr.Baha, AL-Amiedi Ph. D.Microbiology Robert Koch 1843-1910 German physician Became famous for isolating the anthrax bacillus (1877), tuberculosis bacillus (1882)
Mycobacterium tuberculosis Lecture (14) Dr.Baha, AL-Amiedi Ph. D.Microbiology Robert Koch 1843-1910 German physician Became famous for isolating the anthrax bacillus (1877), tuberculosis bacillus (1882)
TB Intensive Houston, Texas
 TB Intensive Houston, Texas October 15-17, 17 2013 Diagnosis of TB: Radiology Rosa M Estrada-Y-Martin, MD MSc FCCP October 16, 2013 Rosa M Estrada-Y-Martin, MD MSc FCCP, has the following disclosures to
TB Intensive Houston, Texas October 15-17, 17 2013 Diagnosis of TB: Radiology Rosa M Estrada-Y-Martin, MD MSc FCCP October 16, 2013 Rosa M Estrada-Y-Martin, MD MSc FCCP, has the following disclosures to
Tuberculosis: The Essentials
 Tuberculosis: The Essentials Kendra L. Fisher, MD, PhD THORACIC TUBERCULOSIS: THE BARE ESSENTIALS Kendra Fisher MD, FRCP (C) Department of Radiology Loma Linda University Medical Center TUBERCULOSIS ()
Tuberculosis: The Essentials Kendra L. Fisher, MD, PhD THORACIC TUBERCULOSIS: THE BARE ESSENTIALS Kendra Fisher MD, FRCP (C) Department of Radiology Loma Linda University Medical Center TUBERCULOSIS ()
Diagnosis of TB: Radiology David Finlay, MD
 TB Intensive Tyler, Texas June 2-4, 2010 Diagnosis of TB: Radiology David Finlay, MD June 3, 2010 2stages stages- Tuberculosis 1. primary infection 2. reactivation, or post primary disease 2 1 Primary
TB Intensive Tyler, Texas June 2-4, 2010 Diagnosis of TB: Radiology David Finlay, MD June 3, 2010 2stages stages- Tuberculosis 1. primary infection 2. reactivation, or post primary disease 2 1 Primary
TUBERCULOSIS. By Dr. Najaf Masood Assistant Prof Pediatrics Benazir Bhutto Hospital Rawalpindi
 TUBERCULOSIS By Dr. Najaf Masood Assistant Prof Pediatrics Benazir Bhutto Hospital Rawalpindi Tuberculosis Infectious, Systemic, Chronic granulomatous disease caused by mycobacterium tuberculosis DEFINITION
TUBERCULOSIS By Dr. Najaf Masood Assistant Prof Pediatrics Benazir Bhutto Hospital Rawalpindi Tuberculosis Infectious, Systemic, Chronic granulomatous disease caused by mycobacterium tuberculosis DEFINITION
Tuberculosis Pathogenesis
 Tuberculosis Pathogenesis Renuka Khurana, MD, MPH May 12, 2015 TB for Community Providers May 12, 2015 Phoenix, Arizona EXCELLENCE EXPERTISE INNOVATION Renuka Khurana, MD, MPH has the following disclosures
Tuberculosis Pathogenesis Renuka Khurana, MD, MPH May 12, 2015 TB for Community Providers May 12, 2015 Phoenix, Arizona EXCELLENCE EXPERTISE INNOVATION Renuka Khurana, MD, MPH has the following disclosures
Tuberculosis Intensive
 Tuberculosis Intensive San Antonio, Texas April 3 6, 2012 Tuberculosis Pathogenesis Lynn Horvath, MD April 3, 2012 Lynn Horvath, MD has the following disclosures to make: No conflict of interests No relevant
Tuberculosis Intensive San Antonio, Texas April 3 6, 2012 Tuberculosis Pathogenesis Lynn Horvath, MD April 3, 2012 Lynn Horvath, MD has the following disclosures to make: No conflict of interests No relevant
Currently, there are about 15 million TB patients including 11 million of working age.
 Currently, there are about 15 million TB patients including 11 million of working age. The vast majority of infected people (90%) the disease does not progress. Predicted by WHO in the next twenty years
Currently, there are about 15 million TB patients including 11 million of working age. The vast majority of infected people (90%) the disease does not progress. Predicted by WHO in the next twenty years
CHAPTER 3: DEFINITION OF TERMS
 CHAPTER 3: DEFINITION OF TERMS NOTE: TB bacteria is used in place of Mycobacterium tuberculosis and Mycobacterium tuberculosis complex in most of the definitions presented here. 3.1 Acid-fast bacteria
CHAPTER 3: DEFINITION OF TERMS NOTE: TB bacteria is used in place of Mycobacterium tuberculosis and Mycobacterium tuberculosis complex in most of the definitions presented here. 3.1 Acid-fast bacteria
TUBERCULOSIS. Famous victims in their intellectual prime: Chopin, Paganini, Thoreau, Keats, Elizabeth Browning, Brontës
 TUBERCULOSIS GENERAL Tuberculosis (TB) kills 1,700,000 annually worldwide. "The Captain of all the men of death that came to take him away was the consumption, for it was that which brought him down to
TUBERCULOSIS GENERAL Tuberculosis (TB) kills 1,700,000 annually worldwide. "The Captain of all the men of death that came to take him away was the consumption, for it was that which brought him down to
Fundamentals of Tuberculosis (TB)
") TB in the United States Fundamentals of Tuberculosis (TB) From 1953 to 1984, reported cases decreased by approximately 5.6% each year From 1985 to 1992, reported cases increased by 20% 25,313 cases reported
TB in the United States Fundamentals of Tuberculosis (TB) From 1953 to 1984, reported cases decreased by approximately 5.6% each year From 1985 to 1992, reported cases increased by 20% 25,313 cases reported
PULMONARY TUBERCULOSIS RADIOLOGY
 PULMONARY TUBERCULOSIS RADIOLOGY RADIOLOGICAL MODALITIES Medical radiophotography Radiography Fluoroscopy Linear (conventional) tomography Computed tomography Pulmonary angiography, bronchography Ultrasonography,
PULMONARY TUBERCULOSIS RADIOLOGY RADIOLOGICAL MODALITIES Medical radiophotography Radiography Fluoroscopy Linear (conventional) tomography Computed tomography Pulmonary angiography, bronchography Ultrasonography,
Tuberculosis - clinical forms. Dr. A.Torossian,, M.D., Ph. D. Department of Respiratory Diseases
 Tuberculosis - clinical forms Dr. A.Torossian,, M.D., Ph. D. Department of Respiratory Diseases 1 TB DISEASE Primary Post-primary (Secondary) Common primary forms Primary complex Tuberculosis of the intrathoracic
Tuberculosis - clinical forms Dr. A.Torossian,, M.D., Ph. D. Department of Respiratory Diseases 1 TB DISEASE Primary Post-primary (Secondary) Common primary forms Primary complex Tuberculosis of the intrathoracic
CLINICAL FEATURES IN PULMONARY TUBERCULOSIS
 CLINICAL FEATURES IN PULMONARY TUBERCULOSIS Dr. Amitesh Aggarwal Department of Medicine Tuberculosis Captain of all the Men of Death Great White Plague devastating effect on society 100 years ago one in
CLINICAL FEATURES IN PULMONARY TUBERCULOSIS Dr. Amitesh Aggarwal Department of Medicine Tuberculosis Captain of all the Men of Death Great White Plague devastating effect on society 100 years ago one in
Tuberculosis and Johne s Disease
 Tuberculosis and Johne s Disease Prof. R. S. Chauhan Joint Director, Indian Veterinary Research Institute Izatnagar 243 122 (India) TUBERCULOSIS Tuberculosis is a chronic bacterial disease of animals caused
Tuberculosis and Johne s Disease Prof. R. S. Chauhan Joint Director, Indian Veterinary Research Institute Izatnagar 243 122 (India) TUBERCULOSIS Tuberculosis is a chronic bacterial disease of animals caused
Mycobacteria & Tuberculosis PROF.HANAN HABIB & PROF ALI SOMILY DEPRTMENT OF PATHOLOGY, MICROBIOLOGY UNIT COLLEGE OF MEDICINE
 Mycobacteria & Tuberculosis PROF.HANAN HABIB & PROF ALI SOMILY DEPRTMENT OF PATHOLOGY, MICROBIOLOGY UNIT COLLEGE OF MEDICINE Objectives l Recognize that tuberculosis as a chronic disease mainly affecting
Mycobacteria & Tuberculosis PROF.HANAN HABIB & PROF ALI SOMILY DEPRTMENT OF PATHOLOGY, MICROBIOLOGY UNIT COLLEGE OF MEDICINE Objectives l Recognize that tuberculosis as a chronic disease mainly affecting
David E. Griffith, MD has the following disclosures to make:
 Diagnosis of TB: Radiology David E. Griffith, MD March 13, 2015 TB for Pulmonologist March 13, 2015 Phoenix, AZ EXCELLENCE EXPERTISE INNOVATION David E. Griffith, MD has the following disclosures to make:
Diagnosis of TB: Radiology David E. Griffith, MD March 13, 2015 TB for Pulmonologist March 13, 2015 Phoenix, AZ EXCELLENCE EXPERTISE INNOVATION David E. Griffith, MD has the following disclosures to make:
Pathology of TB OBJECTIVES:
 Pathology of TB OBJECTIVES: Define tuberculosis. List the diseases caused by Mycobacteria. Know the epidemiology of tuberculosis (TB). List conditions associated with increased risk of Tuberculosis. List
Pathology of TB OBJECTIVES: Define tuberculosis. List the diseases caused by Mycobacteria. Know the epidemiology of tuberculosis (TB). List conditions associated with increased risk of Tuberculosis. List
An Introduction to Radiology for TB Nurses
 An Introduction to Radiology for TB Nurses Garold O. Minns, MD September 14, 2017 TB Nurse Case Management September 12 14, 2017 EXCELLENCE EXPERTISE INNOVATION Garold O. Minns, MD has the following disclosures
An Introduction to Radiology for TB Nurses Garold O. Minns, MD September 14, 2017 TB Nurse Case Management September 12 14, 2017 EXCELLENCE EXPERTISE INNOVATION Garold O. Minns, MD has the following disclosures
TB Intensive San Antonio, Texas December 1-3, 2010
 TB Intensive San Antonio, Texas December 1-3, 2010 TB Pathogenesis and Transmission Lynn Horvath, MD; TCID December 1, 2010 Tuberculosis Pathogenesis Lynn L. Horvath, MD, FACP, FIDSA Associate Professor
TB Intensive San Antonio, Texas December 1-3, 2010 TB Pathogenesis and Transmission Lynn Horvath, MD; TCID December 1, 2010 Tuberculosis Pathogenesis Lynn L. Horvath, MD, FACP, FIDSA Associate Professor
Radiological Aspects of Pulmonary Tuberculosis in Immunocompetent Hosts
 Nov 2003 Radiological Aspects of Pulmonary Tuberculosis in Immunocompetent Hosts Josh Rempell, Harvard Medical School Year III Tuberculosis: the captain of all (wo)men of death Overall, one third of the
Nov 2003 Radiological Aspects of Pulmonary Tuberculosis in Immunocompetent Hosts Josh Rempell, Harvard Medical School Year III Tuberculosis: the captain of all (wo)men of death Overall, one third of the
Tuberculosis. TB is an ancient disease. Tuberculosis. Tuberculosis (TB) today. 18th Century Hungarian Mummies
 today. 18th Century Hungarian Mummies") Tuberculosis TB is an ancient disease The human TB appears to be significantly older than 10 000 years : a recent study from Turkey reported a 500 000 year old fossil of Homo erectus, which shows lesions
Tuberculosis TB is an ancient disease The human TB appears to be significantly older than 10 000 years : a recent study from Turkey reported a 500 000 year old fossil of Homo erectus, which shows lesions
PEDIATRIC TB. Modified PPT from group A seminar (F)
") PEDIATRIC TB Modified PPT from group A seminar (F) objectives the epidemiology of pediatric TB. TB Mycobacteriology. pediatric TB presentations compared to adults TB. Know the differences between, and
PEDIATRIC TB Modified PPT from group A seminar (F) objectives the epidemiology of pediatric TB. TB Mycobacteriology. pediatric TB presentations compared to adults TB. Know the differences between, and
TB Radiology for Nurses Garold O. Minns, MD
 TB Nurse Case Management Salina, Kansas March 31-April 1, 2010 TB Radiology for Nurses Garold O. Minns, MD April 1, 2010 TB Radiology for Nurses Highway Patrol Training Center Salina, KS April 1, 2010
TB Nurse Case Management Salina, Kansas March 31-April 1, 2010 TB Radiology for Nurses Garold O. Minns, MD April 1, 2010 TB Radiology for Nurses Highway Patrol Training Center Salina, KS April 1, 2010
Medical Bacteriology- Lecture 10. Mycobacterium. Actinomycetes. Nocardia
 Medical Bacteriology- Lecture 10 Mycobacterium Actinomycetes Nocardia 1 Mycobacterium Characteristics - Large, very weakly gram positive rods - Obligate aerobes, related to Actinomycetes - Catalase positive
Medical Bacteriology- Lecture 10 Mycobacterium Actinomycetes Nocardia 1 Mycobacterium Characteristics - Large, very weakly gram positive rods - Obligate aerobes, related to Actinomycetes - Catalase positive
Communicable Disease Control Manual Chapter 4: Tuberculosis
 Provincial TB Services 655 West 12th Avenue Vancouver, BC V5Z 4R4 www.bccdc.ca Communicable Disease Control Manual Definitions Page 1 2.0 DEFINITIONS Many of the definitions that follow are taken from
Provincial TB Services 655 West 12th Avenue Vancouver, BC V5Z 4R4 www.bccdc.ca Communicable Disease Control Manual Definitions Page 1 2.0 DEFINITIONS Many of the definitions that follow are taken from
TB Intensive San Antonio, Texas November 29-December 2, 2011
 TB Intensive San Antonio, Texas November 29-December 2, 2011 Diagnosis of TB: Radiology Michael McCarthy, MD, FACR November 30, 2011 Michael McCarthy, MD, FACR has the following disclosures to make: No
TB Intensive San Antonio, Texas November 29-December 2, 2011 Diagnosis of TB: Radiology Michael McCarthy, MD, FACR November 30, 2011 Michael McCarthy, MD, FACR has the following disclosures to make: No
Tuberculosis Part 1. Some useful truths
 Tuberculosis Part 1 Some useful truths Tuberculosis will be dealt with in detail in chapter 9 in a few week s time when we deal with the air borne bacterial diseases and the diseases of the lower respiratory
Tuberculosis Part 1 Some useful truths Tuberculosis will be dealt with in detail in chapter 9 in a few week s time when we deal with the air borne bacterial diseases and the diseases of the lower respiratory
2015/4/14. Pneumonia. Diseases of Respiratory System Infection in the lung (distal airways, esp. alveoli) Lobar pneumonia.
 Lobar pneumonia.") Pneumonia Diseases of Respiratory System Infection in the lung (distal airways, esp. alveoli) 邓红浙江大学医学院病理学系 LUNG(reformed)5y-DH 1 hongdeng@zju.edu.cn Pathology (DH) 2 Pneumonia Bacteria pneumonia Viral
Pneumonia Diseases of Respiratory System Infection in the lung (distal airways, esp. alveoli) 邓红浙江大学医学院病理学系 LUNG(reformed)5y-DH 1 hongdeng@zju.edu.cn Pathology (DH) 2 Pneumonia Bacteria pneumonia Viral
MYCOBACTERIUM. Mycobacterium Tuberculosis (Mtb) nontuberculous mycobacteria (NTM) Mycobacterium lepray
 nontuberculous mycobacteria (NTM) Mycobacterium lepray") MYCOBACTERIUM nontuberculous mycobacteria (NTM) Mycobacterium Tuberculosis (Mtb) Mycobacterium lepray 1-tubercle bacilli are thin 2- straight rods 3- obligate aerobes 4- derive energy from the oxidation
MYCOBACTERIUM nontuberculous mycobacteria (NTM) Mycobacterium Tuberculosis (Mtb) Mycobacterium lepray 1-tubercle bacilli are thin 2- straight rods 3- obligate aerobes 4- derive energy from the oxidation
Pathology lab 4 DONE BY : MORAD ABU QAMAR
 Pathology lab 4 DONE BY : MORAD ABU QAMAR Chronic interstitial inflammation, lung Certain etiologic agents such as viruses are more likely to lead to chronic inflammation, as seen here in the lung of a
Pathology lab 4 DONE BY : MORAD ABU QAMAR Chronic interstitial inflammation, lung Certain etiologic agents such as viruses are more likely to lead to chronic inflammation, as seen here in the lung of a
Diagnosis & Medical Case Management of TB Disease. Lisa Armitige, MD, PhD October 22, 2015
 Diagnosis & Medical Case Management of TB Disease Lisa Armitige, MD, PhD October 22, 2015 Comprehensive Care of Patients with Tuberculosis and Their Contacts October 19 22, 2015 Wichita, KS EXCELLENCE
Diagnosis & Medical Case Management of TB Disease Lisa Armitige, MD, PhD October 22, 2015 Comprehensive Care of Patients with Tuberculosis and Their Contacts October 19 22, 2015 Wichita, KS EXCELLENCE
Chapter 22. Pulmonary Infections
 Chapter 22 Pulmonary Infections Objectives State the incidence of pneumonia in the United States and its economic impact. Discuss the current classification scheme for pneumonia and be able to define hospital-acquired
Chapter 22 Pulmonary Infections Objectives State the incidence of pneumonia in the United States and its economic impact. Discuss the current classification scheme for pneumonia and be able to define hospital-acquired
HISTORY TB = 25% ADULT DEATHS EGYPTIAN MUMMIES: SPINAL TB. 17 th -18th CENTURIES- URBANIZATION MID 24
 HISTORY EGYPTIAN MUMMIES: SPINAL TB 17 th -18th CENTURIES- URBANIZATION 19th CENTURY INDUSTRIALIZATION TB = 25% ADULT DEATHS GERM THEORY OF DISEASE KOCH S BACILLUS-1883 PRE-ANTIBIOTIC ERA SANATORIUM REGIMENS
HISTORY EGYPTIAN MUMMIES: SPINAL TB 17 th -18th CENTURIES- URBANIZATION 19th CENTURY INDUSTRIALIZATION TB = 25% ADULT DEATHS GERM THEORY OF DISEASE KOCH S BACILLUS-1883 PRE-ANTIBIOTIC ERA SANATORIUM REGIMENS
HISTORY TB = 25% ADULT DEATHS MID 24 PRE-ANTIBIOTIC ERA
 PRE-ANTIBIOTIC ERA SANATORIUM REGIMENS & REST CAVITARY DISEASE & COLLAPSE THERAPY FRESH AIR, SUNSHINE-ROOFTOPS SOLARIA HISTORY EGYPTIAN MUMMIES: SPINAL TB 17 th -18th CENTURIES- URBANIZATION 19th CENTURY
PRE-ANTIBIOTIC ERA SANATORIUM REGIMENS & REST CAVITARY DISEASE & COLLAPSE THERAPY FRESH AIR, SUNSHINE-ROOFTOPS SOLARIA HISTORY EGYPTIAN MUMMIES: SPINAL TB 17 th -18th CENTURIES- URBANIZATION 19th CENTURY
Chest Radiology Interpretation: Findings of Tuberculosis
 Chest Radiology Interpretation: Findings of Tuberculosis Get out your laptops, smart phones or other devices pollev.com/chestradiology Case #1 1 Plombage Pneumonia Cancer 2 Reading the TB CXR Be systematic!
Chest Radiology Interpretation: Findings of Tuberculosis Get out your laptops, smart phones or other devices pollev.com/chestradiology Case #1 1 Plombage Pneumonia Cancer 2 Reading the TB CXR Be systematic!
PREVENTION OF TUBERCULOSIS. Dr Amitesh Aggarwal
 PREVENTION OF TUBERCULOSIS Dr Amitesh Aggarwal 25 to 50 % of persons exposed to intimate contact with active PTB - latent infection with TB. Exposure to index case for 12 hours - high risk of infection.
PREVENTION OF TUBERCULOSIS Dr Amitesh Aggarwal 25 to 50 % of persons exposed to intimate contact with active PTB - latent infection with TB. Exposure to index case for 12 hours - high risk of infection.
Medical Bacteriology- lecture 13. Mycobacterium Actinomycetes
 Medical Bacteriology- lecture 13 Mycobacterium Actinomycetes Mycobacterium tuberculosis Large, very weakly gram positive rods, Obligate aerobes, related to Actinomycetes, non spore forming, non motile
Medical Bacteriology- lecture 13 Mycobacterium Actinomycetes Mycobacterium tuberculosis Large, very weakly gram positive rods, Obligate aerobes, related to Actinomycetes, non spore forming, non motile
Histopathology: granulomatous inflammation, including tuberculosis
 Histopathology: granulomatous inflammation, including tuberculosis These presentations are to help you identify basic histopathological features. They do not contain the additional factual information
Histopathology: granulomatous inflammation, including tuberculosis These presentations are to help you identify basic histopathological features. They do not contain the additional factual information
TB in Children. Rene De Gama Block 10 Lectures 2012
 TB in Children Rene De Gama Block 10 Lectures 2012 Contents Epidemiology Transmission and pathogenesis Diagnosis of TB TB and HIV Management Epidemiology The year 2000 8.3 million new TB cases diagnosed
TB in Children Rene De Gama Block 10 Lectures 2012 Contents Epidemiology Transmission and pathogenesis Diagnosis of TB TB and HIV Management Epidemiology The year 2000 8.3 million new TB cases diagnosed
Tuberculosis Elimination: The Role of the Infection Preventionist
 Tuberculosis Elimination: The Role of the Infection Preventionist Preface: What Happens when Health Care Professionals are not familiar with TB? A 15 year old student was diagnosed with highly infectious
Tuberculosis Elimination: The Role of the Infection Preventionist Preface: What Happens when Health Care Professionals are not familiar with TB? A 15 year old student was diagnosed with highly infectious
DIAGNOSIS AND MEDICAL MANAGEMENT OF TB DISEASE
 DIAGNOSIS AND MEDICAL MANAGEMENT OF TB DISEASE Annie Kizilbash MD, MPH Assistant Professor University of Texas Health Science Center Staff Physician, Texas Center for Infectious Diseases TB Nurse Case
DIAGNOSIS AND MEDICAL MANAGEMENT OF TB DISEASE Annie Kizilbash MD, MPH Assistant Professor University of Texas Health Science Center Staff Physician, Texas Center for Infectious Diseases TB Nurse Case
Tuberculosis. Impact of TB. Infectious Disease Epidemiology BMTRY 713 (A. Selassie, DrPH)
") Infectious Disease Epidemiology BMTRY 713 (A. Selassie, DrPH) Lecture 20 Tuberculosis Learning Objectives 1. Describe the biologic characteristics of the agent 2. Determine the epidemiologic characteristics
Infectious Disease Epidemiology BMTRY 713 (A. Selassie, DrPH) Lecture 20 Tuberculosis Learning Objectives 1. Describe the biologic characteristics of the agent 2. Determine the epidemiologic characteristics
NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE SCOPE
 TB Partial Update Appendix 1 - Scope NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE 1 Guideline title SCOPE Tuberculosis: interferon gamma tests for the diagnosis of latent tuberculosis (partial
TB Partial Update Appendix 1 - Scope NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE 1 Guideline title SCOPE Tuberculosis: interferon gamma tests for the diagnosis of latent tuberculosis (partial
Contracts Carla Chee, MHS May 8, 2012
 Moving Past the Basics of Tuberculosis Phoenix, Arizona May 8-10, 2012 Contracts Carla Chee, MHS May 8, 2012 Carla Chee, MHS has the following disclosures to make: No conflict of interests No relevant
Moving Past the Basics of Tuberculosis Phoenix, Arizona May 8-10, 2012 Contracts Carla Chee, MHS May 8, 2012 Carla Chee, MHS has the following disclosures to make: No conflict of interests No relevant
Latent Tuberculosis Infections Controversies in Diagnosis and Management Update 2016
 Latent Tuberculosis Infections Controversies in Diagnosis and Management Update 2016 Randy Culpepper, MD, MPH Deputy Heath Officer/Medical Director Frederick County Health Department March 16, 2016 2 No
Latent Tuberculosis Infections Controversies in Diagnosis and Management Update 2016 Randy Culpepper, MD, MPH Deputy Heath Officer/Medical Director Frederick County Health Department March 16, 2016 2 No
Radiological Features of Mycobacterium tuberculosis TUBERCULE BACILLUS TUBERCULE BACILLUS DIAGNOSIS. Guy Richards. PATHOGENESIS of TUBERCULOSIS
 Radiological Features of Guy Richards Department of critical care Charlotte Maxeke Johannesburg Academic Hospital University of the Witwatersrand, Johannesburg, South Africa TUBERCULE BACILLUS Discovery
Radiological Features of Guy Richards Department of critical care Charlotte Maxeke Johannesburg Academic Hospital University of the Witwatersrand, Johannesburg, South Africa TUBERCULE BACILLUS Discovery
NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE SCOPE
 NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE 1 Guideline title SCOPE Tuberculosis: interferon gamma tests for the diagnosis of latent tuberculosis (partial update) 1.1 Short title Tuberculosis
NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE 1 Guideline title SCOPE Tuberculosis: interferon gamma tests for the diagnosis of latent tuberculosis (partial update) 1.1 Short title Tuberculosis
Tuberculosis Tools: A Clinical Update
 Tuberculosis Tools: A Clinical Update CAPA Conference 2014 JoAnn Deasy, PA-C. MPH, DFAAPA jadeasy@sbcglobal.net Adjunct Faculty Touro PA Program Learning Objectives Outline the pathogenesis of active pulmonary
Tuberculosis Tools: A Clinical Update CAPA Conference 2014 JoAnn Deasy, PA-C. MPH, DFAAPA jadeasy@sbcglobal.net Adjunct Faculty Touro PA Program Learning Objectives Outline the pathogenesis of active pulmonary
What Drug Treatment Centers Can do to Prevent Tuberculosis
 What Drug Treatment Centers Can do to Prevent Tuberculosis Tuberculosis (TB) is alive and well Learn what you can do to prevent TB among your clients and protect yourself! Transmission TB is spread through
What Drug Treatment Centers Can do to Prevent Tuberculosis Tuberculosis (TB) is alive and well Learn what you can do to prevent TB among your clients and protect yourself! Transmission TB is spread through
has the following disclosures to make:
 CLINICAL DIAGNOSIS AND MANAGEMENT OF TB DISEASE Annie Kizilbash MD, MPH September 22, 2015 TB Nurse Case Management September 22 24, 2015 San Antonio. TX EXCELLENCE EXPERTISE INNOVATION Annie Kizilbash
CLINICAL DIAGNOSIS AND MANAGEMENT OF TB DISEASE Annie Kizilbash MD, MPH September 22, 2015 TB Nurse Case Management September 22 24, 2015 San Antonio. TX EXCELLENCE EXPERTISE INNOVATION Annie Kizilbash
Self-Study Modules on Tuberculosis
 Self-Study Modules on Tuberculosis Transmission and Pathogenesis of Tube rc ulos is U.S. DEPARTMENT OF HEALTH AND HUMAN SERVICES Centers for Disease Control and Prevention National Center for HIV/AIDS,
Self-Study Modules on Tuberculosis Transmission and Pathogenesis of Tube rc ulos is U.S. DEPARTMENT OF HEALTH AND HUMAN SERVICES Centers for Disease Control and Prevention National Center for HIV/AIDS,
56% of these were in south east Asia and west pacific region.
 Tuberc ulosis Dr. ASAAD FARHAN ASSIST. PROF.PEDS. Learning objectives epidemiology Tuberculosis remains worlds deadliest communicable disease. TB is present in all regions of the world. WHO estimates that
Tuberc ulosis Dr. ASAAD FARHAN ASSIST. PROF.PEDS. Learning objectives epidemiology Tuberculosis remains worlds deadliest communicable disease. TB is present in all regions of the world. WHO estimates that
Tanya Van, M.D. has the following disclosures to make:
 Imaging of Pulmonary Mycobacterial TB Infection Tanya Van, M.D. April6, 2016 TB Intensive April 5 8, 2016 San Antonio, TX EXCELLENCE EXPERTISE INNOVATION Tanya Van, M.D. has the following disclosures to
Imaging of Pulmonary Mycobacterial TB Infection Tanya Van, M.D. April6, 2016 TB Intensive April 5 8, 2016 San Antonio, TX EXCELLENCE EXPERTISE INNOVATION Tanya Van, M.D. has the following disclosures to
however, Continental and American workers have thrown some light
 THE ORIGIN AND SIGNIFICANCE OF TUBERCULOSIS OF THE TRACHEO-BRONCHIAL LYMPH NODES OF THE LUNG.* BY L. R. Jordan. Introduction. The frequency of latent tuberculosis has been recognized since the latter part
THE ORIGIN AND SIGNIFICANCE OF TUBERCULOSIS OF THE TRACHEO-BRONCHIAL LYMPH NODES OF THE LUNG.* BY L. R. Jordan. Introduction. The frequency of latent tuberculosis has been recognized since the latter part
Respiratory Diseases
 8-year system Curriculum 6nd Week Theme Respiratory Diseases ZHANG WEI ( 张伟 ) Associate Professor, Ph.D. Institute of Pathology & Forensic Medicine Department of Pathology & Patho-physiology Zhejiang University
8-year system Curriculum 6nd Week Theme Respiratory Diseases ZHANG WEI ( 张伟 ) Associate Professor, Ph.D. Institute of Pathology & Forensic Medicine Department of Pathology & Patho-physiology Zhejiang University
Mycobacteriology William H. Benjamin, Jr.
 Mycobacteriology William H. Benjamin, Jr. William H. Benjamin, PhD Department of Pathology UAB 1 Mycobacteria sp. Acid Fast Bacilli (AFB) Mycolic acids (C78-91) Waxes Obligate aerobes Slow growing days
Mycobacteriology William H. Benjamin, Jr. William H. Benjamin, PhD Department of Pathology UAB 1 Mycobacteria sp. Acid Fast Bacilli (AFB) Mycolic acids (C78-91) Waxes Obligate aerobes Slow growing days
Latent Tuberculosis in Adults: From Testing TO Treatment
 Latent Tuberculosis in Adults: From Testing TO Treatment Sergio M. Borgia, MD, MSc., FRCP(C) Infectious Diseases Consultant, WOHS Medical Director, WOHS Tuberculosis Clinic Assistant Clinical Professor,
Latent Tuberculosis in Adults: From Testing TO Treatment Sergio M. Borgia, MD, MSc., FRCP(C) Infectious Diseases Consultant, WOHS Medical Director, WOHS Tuberculosis Clinic Assistant Clinical Professor,
Understanding and Managing Latent TB Infection Arnold, Missouri October 5, 2010
 Understanding and Managing Latent TB Infection Arnold, Missouri October 5, 2010 What is Latent TB Infection (LTBI)? Traci Hadley, RN October 5, 2010 LTBI or TB Disease? Presented by : Traci Hadley, RN
Understanding and Managing Latent TB Infection Arnold, Missouri October 5, 2010 What is Latent TB Infection (LTBI)? Traci Hadley, RN October 5, 2010 LTBI or TB Disease? Presented by : Traci Hadley, RN
MODULE ONE" TB Basic Science" Treatment Action Group TB/HIV Advocacy Toolkit
 MODULE ONE" TB Basic Science" Treatment Action Group TB/HIV Advocacy Toolkit Topics to be covered What is Tuberculosis? TB bacteria and what is unique about it. How is TB different from HIV? How is TB
MODULE ONE" TB Basic Science" Treatment Action Group TB/HIV Advocacy Toolkit Topics to be covered What is Tuberculosis? TB bacteria and what is unique about it. How is TB different from HIV? How is TB
How to Analyse Difficult Chest CT
 How to Analyse Difficult Chest CT Complex diseases are:- - Large lesion - Unusual or atypical pattern - Multiple discordant findings Diffuse diseases are:- - Numerous findings in both sides 3 basic steps
How to Analyse Difficult Chest CT Complex diseases are:- - Large lesion - Unusual or atypical pattern - Multiple discordant findings Diffuse diseases are:- - Numerous findings in both sides 3 basic steps
CHAPTER:1 TUBERCULOSIS. BY Mrs. K.SHAILAJA., M. PHARM., LECTURER DEPT OF PHARMACY PRACTICE, SRM COLLEGE OF PHARMACY
 CHAPTER:1 TUBERCULOSIS BY Mrs. K.SHAILAJA., M. PHARM., LECTURER DEPT OF PHARMACY PRACTICE, SRM COLLEGE OF PHARMACY GLOBAL EMERGENCY: * Tuberculosis kills 5,000 people a day! * 2.3 million die each year!
CHAPTER:1 TUBERCULOSIS BY Mrs. K.SHAILAJA., M. PHARM., LECTURER DEPT OF PHARMACY PRACTICE, SRM COLLEGE OF PHARMACY GLOBAL EMERGENCY: * Tuberculosis kills 5,000 people a day! * 2.3 million die each year!
Tuberculin Skin Testing
 Understanding and Managing Latent TB Infection Arnold, Missouri October 5, 2010 Testing to TB Infection Using the TST Presented by Debra Howenstine, MD for Debbie Onofre, RN October 5, 2010 Tuberculin
Understanding and Managing Latent TB Infection Arnold, Missouri October 5, 2010 Testing to TB Infection Using the TST Presented by Debra Howenstine, MD for Debbie Onofre, RN October 5, 2010 Tuberculin
Pulmonary Pathology II. William Bligh-Glover M.D. Department of Anatomy, CWRU
 Pulmonary Pathology II William Bligh-Glover M.D. Department of Anatomy, CWRU Goals and Objectives Comprehend the etiology, pathogenesis/pathopysiology and consequences of pulmonary hypertension Distinguish
Pulmonary Pathology II William Bligh-Glover M.D. Department of Anatomy, CWRU Goals and Objectives Comprehend the etiology, pathogenesis/pathopysiology and consequences of pulmonary hypertension Distinguish
HISTOPATHOLOGY. Shannon Martinson
 HISTOPATHOLOGY Shannon Martinson March 2013 Case #1 History: 8 year old beagle Neck pain for the past couple of weeks Paresis, followed by paralysis developed over the past few days Gross Description courtesy
HISTOPATHOLOGY Shannon Martinson March 2013 Case #1 History: 8 year old beagle Neck pain for the past couple of weeks Paresis, followed by paralysis developed over the past few days Gross Description courtesy
MO TASEM AJ Nader Alaridah
 22 MO TASEM AJ...... Nader Alaridah Mycobacterium ** Mycobacterium is a class of Actinobacteria, which are non-spore forming, non-motile and acid-fast bacilli ( they remain stained with the red dye carbofuchsin
22 MO TASEM AJ...... Nader Alaridah Mycobacterium ** Mycobacterium is a class of Actinobacteria, which are non-spore forming, non-motile and acid-fast bacilli ( they remain stained with the red dye carbofuchsin
A Rare case of Tubercular Gingivitis Case Report
 Case Report A Rare case of Tubercular Gingivitis Case Report *Dr. Ansh Chugh 1, Dr. Firoz A Hakkim 2, Dr. Rajesh. V 3, Dr. Raghava Sharma 4 1: JUNIOR RESIDENT IN GENERAL MEDICINE 2: SENIOR RESIDENT IN
Case Report A Rare case of Tubercular Gingivitis Case Report *Dr. Ansh Chugh 1, Dr. Firoz A Hakkim 2, Dr. Rajesh. V 3, Dr. Raghava Sharma 4 1: JUNIOR RESIDENT IN GENERAL MEDICINE 2: SENIOR RESIDENT IN
Summary of Key Points WHO Position Paper on BCG Vaccine, February 2018
 Summary of Key Points WHO Position Paper on BCG Vaccine, February 2018 1 Introduction This position paper replaces the 2004 WHO position paper on Bacille Calmette-Guérin (BCG) vaccine and the 2007 WHO
Summary of Key Points WHO Position Paper on BCG Vaccine, February 2018 1 Introduction This position paper replaces the 2004 WHO position paper on Bacille Calmette-Guérin (BCG) vaccine and the 2007 WHO
HISTORY TB = 25% ADULT DEATHS PRE-ANTIBIOTIC ERA SANATORIUM REGIMENS & REST CAVITARY DISEASE & COLLAPSE THERAPY FRESH AIR, SUNSHINE-ROOFTOPS SOLARIA
 PRE-ANTIBIOTIC ERA SANATORIUM REGIMENS & REST CAVITARY DISEASE & COLLAPSE THERAPY FRESH AIR, SUNSHINE-ROOFTOPS SOLARIA HISTORY EGYPTIAN MUMMIES: SPINAL TB 17 th -18th CENTURIES- URBANIZATION 19th CENTURY
PRE-ANTIBIOTIC ERA SANATORIUM REGIMENS & REST CAVITARY DISEASE & COLLAPSE THERAPY FRESH AIR, SUNSHINE-ROOFTOPS SOLARIA HISTORY EGYPTIAN MUMMIES: SPINAL TB 17 th -18th CENTURIES- URBANIZATION 19th CENTURY
INDUSTRIALIZATION TB = 25% ADULT DEATHS
 HISTORY EGYPTIAN MUMMIES: SPINAL TB 17 th -18th CENTURIES- URBANIZATION 19th CENTURY INDUSTRIALIZATION TB = 25% ADULT DEATHS 1 GERM THEORY OF DISEASE KOCH S BACILLUS-1883 PRE-ANTIBIOTIC ERA SANATORIUM
HISTORY EGYPTIAN MUMMIES: SPINAL TB 17 th -18th CENTURIES- URBANIZATION 19th CENTURY INDUSTRIALIZATION TB = 25% ADULT DEATHS 1 GERM THEORY OF DISEASE KOCH S BACILLUS-1883 PRE-ANTIBIOTIC ERA SANATORIUM
Peripheral mycobacterial lymphadenitis (TB, NTM and BCG)
") Peripheral mycobacterial lymphadenitis (TB, NTM and BCG) H Simon Schaaf Desmond Tutu TB Centre, Department of Paediatrics and Child Health, Stellenbosch University, Cape Town, South Africa Questions Peripheral
Peripheral mycobacterial lymphadenitis (TB, NTM and BCG) H Simon Schaaf Desmond Tutu TB Centre, Department of Paediatrics and Child Health, Stellenbosch University, Cape Town, South Africa Questions Peripheral
The Diagnosis of Active TB. Deborah McMahan, MD TB Intensive September 28, 2017
 The Diagnosis of Active TB Deborah McMahan, MD TB Intensive September 28, 2017 Agenda Epidemiology Big picture Conditions that Should Make You Suspicious Which test? Eeenie meenie miny mo Radiographic
The Diagnosis of Active TB Deborah McMahan, MD TB Intensive September 28, 2017 Agenda Epidemiology Big picture Conditions that Should Make You Suspicious Which test? Eeenie meenie miny mo Radiographic
7. BCG Vaccination HSE/HPSC. Guidelines on the Prevention and Control of Tuberculosis in Ireland IUATLD criteria
 7. BCG Vaccination The Bacillus Calmette-Guerin (BCG) vaccine was derived by in-vitro attenuation of the bovine tubercle bacillus between the years 1908 and 1918 in France. WHO encouraged widespread use
7. BCG Vaccination The Bacillus Calmette-Guerin (BCG) vaccine was derived by in-vitro attenuation of the bovine tubercle bacillus between the years 1908 and 1918 in France. WHO encouraged widespread use
Characteristics of Mycobacterium
 Mycobacterium Characteristics of Mycobacterium Very thin, rod shape. Culture: Aerobic, need high levels of oxygen to grow. Very slow in grow compared to other bacteria (colonies may be visible in up to
Mycobacterium Characteristics of Mycobacterium Very thin, rod shape. Culture: Aerobic, need high levels of oxygen to grow. Very slow in grow compared to other bacteria (colonies may be visible in up to
Pathology of Pneumonia
 Pathology of Pneumonia Dr. Atif Ali Bashir Assistant Professor of Pathology College of Medicine Majma ah University Introduction: 5000 sq meters of area.! (olympic track) Filters >10,000 L of air / day!
Pathology of Pneumonia Dr. Atif Ali Bashir Assistant Professor of Pathology College of Medicine Majma ah University Introduction: 5000 sq meters of area.! (olympic track) Filters >10,000 L of air / day!
TUBERCULOSIS. Pathogenesis and Transmission
 TUBERCULOSIS Pathogenesis and Transmission TUBERCULOSIS Pathogenesis and Transmission Infection to Disease Diagnostic & Isolation Updates Treatment Updates Pathogenesis Droplet nuclei of 5µm or less are
TUBERCULOSIS Pathogenesis and Transmission TUBERCULOSIS Pathogenesis and Transmission Infection to Disease Diagnostic & Isolation Updates Treatment Updates Pathogenesis Droplet nuclei of 5µm or less are
Key Difference - Pleural Effusion vs Pneumonia
 Difference Between Pleural Effusion and Pneumonia www.differencebetween.com Key Difference - Pleural Effusion vs Pneumonia Pleural effusion and pneumonia are two conditions that affect our respiratory
Difference Between Pleural Effusion and Pneumonia www.differencebetween.com Key Difference - Pleural Effusion vs Pneumonia Pleural effusion and pneumonia are two conditions that affect our respiratory
number Done by Corrected by Doctor Hamid Al Zoubi
 number 15 Done by أبو عجمي ة مها Corrected by Waseem Abu Obeida Doctor Hamid Al Zoubi In case you don t know - (Bacillus = rod) and (bacilli = rods) - hypersensitivity tests can be either immediate (within
number 15 Done by أبو عجمي ة مها Corrected by Waseem Abu Obeida Doctor Hamid Al Zoubi In case you don t know - (Bacillus = rod) and (bacilli = rods) - hypersensitivity tests can be either immediate (within
TB the basics. (Dr) Margaret (DHA) and John (INZ)
 Margaret (DHA) and John (INZ)") TB the basics (Dr) Margaret (DHA) and John (INZ) Question 1 The scientist who discovered M. tuberculosis was: A: Louis Pasteur B: Robert Koch C: Jean-Antoine Villemin D: Calmette and Guerin Question 2
TB the basics (Dr) Margaret (DHA) and John (INZ) Question 1 The scientist who discovered M. tuberculosis was: A: Louis Pasteur B: Robert Koch C: Jean-Antoine Villemin D: Calmette and Guerin Question 2
MYCOBACTERIA. Pulmonary T.B. (infect bird)
") MYCOBACTERIA SPP. Reservoir Clinical Manifestation Mycobacterium tuberculosis Human Pulmonary and dissem. T.B. M. lepra Human Leprosy M. bovis Human & cattle T.B. like infection M. avium Soil, water, birds,
MYCOBACTERIA SPP. Reservoir Clinical Manifestation Mycobacterium tuberculosis Human Pulmonary and dissem. T.B. M. lepra Human Leprosy M. bovis Human & cattle T.B. like infection M. avium Soil, water, birds,
Diagnosis and Medical Management of TB Disease. Quratulian Annie Kizilbash, MD, MPH March 17, 2015
 Diagnosis and Medical Management of TB Disease Quratulian Annie Kizilbash, MD, MPH March 17, 2015 TB Nurse Case Management March 17 19, 2015 San Antonio, Texas EXCELLENCE EXPERTISE INNOVATION Quratulian
Diagnosis and Medical Management of TB Disease Quratulian Annie Kizilbash, MD, MPH March 17, 2015 TB Nurse Case Management March 17 19, 2015 San Antonio, Texas EXCELLENCE EXPERTISE INNOVATION Quratulian
TUBERCULOUS PERICARDIAL EFFUSION
 BY S. SUZMAN From the Cardiographic Department, Guy's Hospital Received June 22, 1942 Tuberculous pericardial effusion is not common; and so the case described is of interest on account of the patient's
BY S. SUZMAN From the Cardiographic Department, Guy's Hospital Received June 22, 1942 Tuberculous pericardial effusion is not common; and so the case described is of interest on account of the patient's
Inflammation Laboratory 3 Emphasis: Chronic inflammation and healing. Shannon Martinson: VPM 152: April 2013
 Inflammation Laboratory 3 Emphasis: Chronic inflammation and healing Shannon Martinson: http://people.upei.ca/smartinson VPM 152: April 2013 Example A Reproductive tract and colon/rectum from a sheep Previous
Inflammation Laboratory 3 Emphasis: Chronic inflammation and healing Shannon Martinson: http://people.upei.ca/smartinson VPM 152: April 2013 Example A Reproductive tract and colon/rectum from a sheep Previous
For more information about how to cite these materials visit
 Project: Ghana Emergency Medicine Collaborative Document Title: Pneumonia in the ED Author(s): Phil Bossart (University of Utah), MD 2012 License: Unless otherwise noted, this material is made available
Project: Ghana Emergency Medicine Collaborative Document Title: Pneumonia in the ED Author(s): Phil Bossart (University of Utah), MD 2012 License: Unless otherwise noted, this material is made available
Diagnosis and Medical Management of Latent TB Infection
 Diagnosis and Medical Management of Latent TB Infection Marsha Majors, RN September 7, 2017 TB Contact Investigation 101 September 6 7, 2017 Little Rock, AR EXCELLENCE EXPERTISE INNOVATION Marsha Majors,
Diagnosis and Medical Management of Latent TB Infection Marsha Majors, RN September 7, 2017 TB Contact Investigation 101 September 6 7, 2017 Little Rock, AR EXCELLENCE EXPERTISE INNOVATION Marsha Majors,
Collar stud abscess an interesting case report
 Volume 2 issue 2 2012 ISSN 2250-0359 Collar stud abscess an interesting case report Kameshwaran Kannappan Punniyakodi * Balasubramanian Thiagarajan* *Stanley Medical College Chennai, Tamilnadu Abstract
Volume 2 issue 2 2012 ISSN 2250-0359 Collar stud abscess an interesting case report Kameshwaran Kannappan Punniyakodi * Balasubramanian Thiagarajan* *Stanley Medical College Chennai, Tamilnadu Abstract
Diagnosis and Management of TB Disease Lisa Armitige, MD, PhD September 27, 2011
 TB Nurse Case Management Davenport, Iowa September 27 28, 2011 Diagnosis and Management of TB Disease Lisa Armitige, MD, PhD September 27, 2011 Lisa Armitige, MD, PhD has the following disclosures to make:
TB Nurse Case Management Davenport, Iowa September 27 28, 2011 Diagnosis and Management of TB Disease Lisa Armitige, MD, PhD September 27, 2011 Lisa Armitige, MD, PhD has the following disclosures to make:
Tuberculosis Populations at Risk
 Tuberculosis Populations at Risk One-third of the world is infected with TB, an average of one new infection per second Two million people died from tuberculosis in 2010, 1 every 20 seconds TB is the leading
Tuberculosis Populations at Risk One-third of the world is infected with TB, an average of one new infection per second Two million people died from tuberculosis in 2010, 1 every 20 seconds TB is the leading
Chapter 133 Tuberculosis
 Chapter 133 Tuberculosis Peter E. Sokolove and Robert W. Derlet PERSPECTIVE History and Epidemiology Tuberculosis (TB) has plagued humankind throughout recorded history. Clear evidence of tuberculous lesions
Chapter 133 Tuberculosis Peter E. Sokolove and Robert W. Derlet PERSPECTIVE History and Epidemiology Tuberculosis (TB) has plagued humankind throughout recorded history. Clear evidence of tuberculous lesions
Learning Objectives: Case 1 11/12/2015. Tuberculosis: Focus on Transmission and Pathogenesis. TB: Some Important Terms
 A 11/12/2015 Learning Objectives: Tuberculosis: Focus on Transmission and Pathogenesis Henry Fraimow, M ivision of Infectious iseases ooper School of Medicine at Rowan University Medical onsultant, Southern
A 11/12/2015 Learning Objectives: Tuberculosis: Focus on Transmission and Pathogenesis Henry Fraimow, M ivision of Infectious iseases ooper School of Medicine at Rowan University Medical onsultant, Southern
Pleural syndrome Tuberculous pleurisy
 Pleural syndrome Tuberculous pleurisy Etienne Leroy Terquem Pierre L Her SPI / ISP Soutien Pneumologique International / International Support for Pulmonology Pleural effusion: Findings of fluid between
Pleural syndrome Tuberculous pleurisy Etienne Leroy Terquem Pierre L Her SPI / ISP Soutien Pneumologique International / International Support for Pulmonology Pleural effusion: Findings of fluid between
Etiological Agent: Pulmonary Tuberculosis. Debra Mercer BSN, RN, RRT. Definition
 Pulmonary Tuberculosis Debra Mercer BSN, RN, RRT Definition Tuberculosis is a contagious bacterial infection of the lungs caused by Mycobacterium Tuberculosis (TB) Etiological Agent: Mycobacterium Tuberculosis
Pulmonary Tuberculosis Debra Mercer BSN, RN, RRT Definition Tuberculosis is a contagious bacterial infection of the lungs caused by Mycobacterium Tuberculosis (TB) Etiological Agent: Mycobacterium Tuberculosis
Core Curriculum on Tuberculosis: What the Clinician Should Know
 Core Curriculum on Tuberculosis: What the Clinician Should Know Sixth Edition 2013 National Center for HIV/AIDS, Viral Hepatitis, STD, and TB Prevention Division of Tuberculosis Elimination 1 Chapters
Core Curriculum on Tuberculosis: What the Clinician Should Know Sixth Edition 2013 National Center for HIV/AIDS, Viral Hepatitis, STD, and TB Prevention Division of Tuberculosis Elimination 1 Chapters