Respiratory Diseases
|
|
|
- Natalie Nelson
- 5 years ago
- Views:
Transcription
1 8-year system Curriculum 6nd Week Theme Respiratory Diseases ZHANG WEI ( 张伟 ) Associate Professor, Ph.D. Institute of Pathology & Forensic Medicine Department of Pathology & Patho-physiology Zhejiang University School of Medicine zwei72@zju.edu.cn
2 Diseases Chronic obstructive pulmonary disease, COPD Chronic bronchitis Pulmonary emphysema Bronchiectasis Bronchial asthma Pneumoconiosis:Silicosis Chronic cor pulmonale Pulmonary infections: Pneumonia Lobar pneumonia Lobular pneumonia Interstitial pneumonia Pulmonary tuberculosis Tumors of lung
3 Pneumonia Broadly defined:any infection in the lung. Pathologically Defined: any inflammation of lung due to infection affecting distal airways, especially alveoli, with the formation of an inflammatory exudate.
4 Classification of pneumonia 1. Etiological classification: bacterial pneumonia viral pneumonia fungal pneumonia mycoplasma pneumonia etc.
5 2. Anatomical classification: lobar pneumonia lobular pneumonia interstitial pneumonia

6
7 The anatomical classification may give a great help to the etiological diagnosis some times. > 90% lobar pneumonia: caused by Streptococcus pneumoniae (pneumococcus) ; interstitial pneumonia are caused by virus or mycoplasm.
8 Bacterial Pneumonia Lobar pneumonia Def. an acute bacterial infection resulting in fibrinosuppurative consolidation of a large portion of a lobe or of an entire lobe. often seen in previously healthy young adults. Symptoms: abrupt onset, high fever, shaking chills, pleuritic chest pain, a productive mucopurulent cough ( rusty sputum )


9

10
11 Etiology pathogens: streptococcus-pneumoniae, pneumobacillus inducing factors: cold, excessive tired, anethesia Pathogenesis bacteria---alveoli---proliferate, capillary dilate, serious exudates---kohn s pores---spreading entire lobe
12 Morphology For purposes of description, it is convenient to divide the process into four phases: (1) Congestion (1st-2nd day) (2) Red hepatization (consolidation) (3rd-4th day) (3) Gray hepatization (5th-6th day) (4) Resolution (1 week)

13
14 1. Congestion stage (1st-2nd days) the outpouring of a protein-rich exudate into alveolar spaces and rapid proliferation of bacteria. grossly: LM: heavy, red, boggy A frothy blood-stained fluid can be squeezed from the cut surface. alveolar wall: cap. dilate, congestion alveolar space: proteinaceous edema fluid, few neutrophils, RBC, and numerous bacteria. Clinically: the onset is sudden with fever and rigors.

15
16 2. Red hepatization stage (3rd-4th day) grossly: the lobe distinctly red, firm, and airless with a liver-like consistency LM: Septal capillaries are congested markedly Alveolar spaces are packed with many red cells, and several neutrophils, fibrin the pleura usually demonstrates a fibrinous or fibrinopurulent exudates.


17


18
19 3. Gray hepatization stage (5th 6th day) grossly: gray-brown and more solid, liver like consistency Pleural surface is covered with a confluent fibrinous exudates. The cut surface is dry and granular but of a grayish-white color. LM: Congestion of septal capillaries lightens. The fibrinous exudate persists within the alveoli and a fibrin net forms. There are many neutrophils but is relatively depleted of red cells in the alveoli.


20

21


22
23 4. Resolution stage (7th-9th day) the resorption of exudate and enzymatic digestion of inflammatory debris, with preservation of the underlying alveolar wall architecture Gross: softening, volume LM: WBC fibrin absorbed

24
25 Complication 1. pulmonary carnification: hypoexudation of neutrophils---proteinase defficiency/ over-exudation of fibrin---organization of the intra-alveolar exudate convert areas of the lung into solid fibrous tissue. 2. Tissue destruction and necrosis may lead to abscess formation. 3. Suppurative material may accumulate in the pleural cavity, producing purulent pleurisy and empyema. 4. Septicemia or pyemia: Bacteremic dissemination may lead to meningitis, arthritis, or infective endocarditis. 5. Infective shock: Failure of terminal circulation and appearance of toxic symptoms.

26 Pulmonary carnification

27 Lobar pneumonia(carnification)
28 Lobular pneumonia (Bronchopneumonia) Conception: Defined as an acute purulent inflammation characterized by diffuse patchy pneumonic consolidation often with bronchiolitis in its center. clinic: infants, the aged, and those suffering from chronic debilitating illness or immunosuppression. children: Whooping cough and measles are important antecedents adult: influenza, chronic bronchitis, alcoholism, malnutrition, and carcinomatosis are all predisposing conditions. patchy distribution, a purulent inflammation that centered bronchioles.
29 Etiology and pathogenesis Pathogens: staphylococci, pneumococci, streptococci, influenzae haemophilus Induce factors: cold, heart failure Infection ways: respiratory tract, blood
30 Morphology gross: patchy consolidation through one lobe, more often multilobar and frequently bilateral and basal 0.5-1cm,gray-red to yellow, slightly elevated, poorly delimited at the margins Severe: confluent bronchopneumonia


31


32


33
 walls of bronchioles and")
the abscesses are marked by necrosis of the")
34 LM: (1) a suppurative, neutrophil-rich exudates centered the bronchi, bronchioles, adjacent alveolar spaces (2) walls of bronchioles and alveoli: congestion,edema (3)surrounding: hyperemic edematous compensative emphysema (4)the abscesses are marked by necrosis of the underlying architecture


35


36
pyemia (4)abscess")
37 complication (1)respiratory failure (2)heart failure (3)pyemia (4)abscess (5)bronchiectasis
38 Hypostatic pneumonia The patient with pulmonary edema from cardiac failure or heavy uremia, et al, is particularly vulnerable. Aspiration pneumonia The patient in coma or apoplexy, heavy anesthesia and so on is particularly vulnerable.
39 Viral pneumonia and mycoplasmal pneumonia They both belong to interstitial pneumonia Def. an inflammatory process involving the interstitial tissue of the lungs.
40 Etiology and pathogenesis pathogens: Most common: influenza virus A/B Less common: parainfluenza, respiratory syncytial virus ( especially in infants and children) Adenovirus common in army recruits Mycoplasmal pneumonia common among children and young adults Others: measles, chickenbox
41 Attachment of the organisms to the respiratory epithelium is followed by necrosis of the cells and an inflammatory response. Then, the inflammation extends to the interstitial tissue including peribronchial connective tissue and interalveolar septa.
42 Morphology Macroscopically: red-blue, congested, volume slightly enlarge and subcrepitant. little inflammatory exudates escapes on sectioning of the lung Histologically: the inflammatory process is largely confined within the walls of the alveoli. The septa are widened and edematous with a mononuclear infiltrate of lymphocytes, histiocytes and occasionally plasma cells. alveolar spaces are remarkably free of cellular exudate

43
44 In virus infection, inclusion bodies may be formed within cytoplasm or nucleus of the epithelial cells of bronchioles and alveoli. In severe cases alveolar damage with hyaline membranes may develop.


45 viral inclusion body is round or oval shape, erythrocyte-like in size, eosinophilic cytoplasmic or nuclear
46 TYPES of PNEUMONIA LOBAR BRONCHO- PNEUMONIA Interstitial Distribution One or two lobes Scattered Scattered Cause Strept.Pneumoniae Multiple Bacteria Influenza/Mycoplasma Pathology Inflammation in alveolar wall cause consolidation. Pleuritis Inflam & purulent exudate in alveoli. Often from previous process Interstitial inflam. Around alveoli. Necrosis of bronchial epithelium Onset Sudden and acute Insidious Variable Signs High fever & chills Productive cough with rusty sputum. Progressive Rales to absence of sounds in affected lobe Mild fever. Productive cough with yellow-green sputum. Dyspnea Variable fever, headache. Aching muscles. Nonproductive hacking cough


47 TYPES of PNEUMONIA BRONCHOPNEUMONIA LOBAR PNEUMONIA
48
49 Tuberculosis a communicable chronic granulomatous disease caused by Mycobacterium tuberculosis. After HIV, tuberculosis is the leading infectious cause of death in the world. Infection with HIV makes people susceptible to rapidly progressive tuberculosis; over 50 million people are infected with both HIV and M. tuberculosis. The lung is the most often affected organ.

50

51
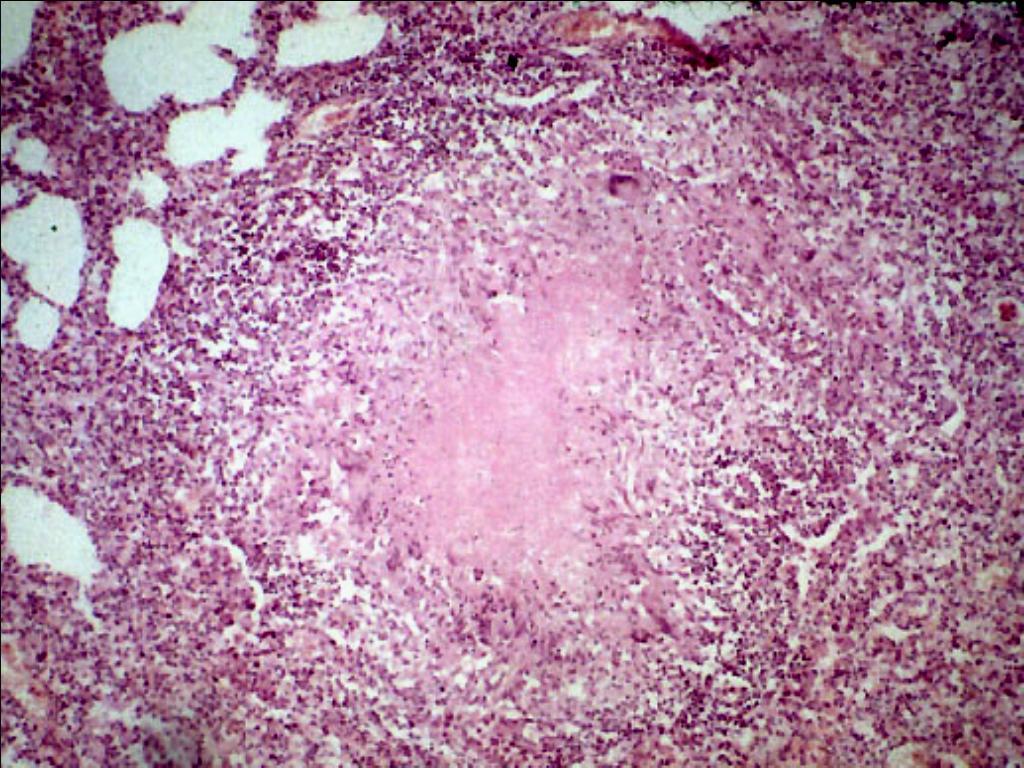
52 Basic pathological changes TB is a special type of inflammation. Alteration Exudation Proliferation

53 Alteration Grossly : gray- yellowish, massive caseation, consolidated Microscopically : red strained homogeneous amorphic material with cell debris sometimes or slightly granular material.

54 Caseous necrosis

55 Caseous necrosis
56 Exudative changes Early infections, numerous mycobecteria, high bacteria virulence, low host immunity and pronouned hypersensitivity. Sero-fibrinous inflammation, neutrophil cells, macrophages Location: lung, pleurea,
57 Proliferation Few organisms, low virulence and high host immunity. tubercle the most characteristic changes in tuberculosis
58 Tubercle (tuberculous granuloma) Typical tubercle consists of caseous necrosis in the center, surrounding it by the epithelioid and some Langhan s giant cells, with a peripheral aggregation of small lymphocytes and fibroblasts. The tubercle can be isolated or fuse to a large one. the epithelioid cells show a pale pink granular cytoplasm with indistinct cell boundaries, often appearing to merge into one another. The nucleus is less dense than that of a lymphocyte (vesicular), is oval or elongated and may show folding of the nuclear membrane.

59 Epithelioid cells

60 Tubercle nodules surrounding fibrosis

61

62 Langhans giant cell
63
64 Fate of the tuberculosis Healing of tuberculosis lesion Absorption and resolution. Fibrosis, fibrous encapsulation and calcification. Exacerbation of tuberculous lesions Infiltration and progression. Dissolution and dissemination.
65 primary tuberculosis secondary tuberculosis
66 Primary pulmonary tuberculosis the first infection TB more frequent in children, so called the childhood type TB, but primary lesion may also occurs in adult at a low rate of the tuberculosis.
67 Pathology Characteristic : Primary complex (the Ghon complex). Primary lesion (Ghon focus) Tuberculous lymphangitis Tuberculous lymphadenitis (in the hilar lymph nodes) X-ray : dumbbell-like

68

69 Swelling of lymph nodes with caseous necrosis Primary focus with Caseous necrosis


70

71
72 Clinical features Primary pulmonary tuberculosis is usually asymptomatic or manifested as a mild flu-like illness.
73 The fate of primary pulmonary TB In 95% of cases, immunity stops disease progression and healing occurs. small focus: resolution, fibrosis large focus: fibrous capsulation, calcification In 5% of cases, rapidly progressive pulmonary disease causing extensive caseous consolidation of the lung, usually occurs only in malnourished or immunodeficient children.
74 Three routes of dissemination 1.Bronchial dissemination----multiple foci 2.Lymphatic dissemination---hilar peribronchial cervical even distant lymph nodes 3.Hematogenous dissemination----miliary disease in lung or generalized military tuberculosis
75 Blood-borne dissemination: miliary tuberculosis Acute systematic/pulmonary miliary tuberculosis Numerous pale, translucent nodules in millet size are seen in lungs, kidneys, liver etc. Chronic systematic/pulmonary miliary tuberculosis

76


77

78

79

80
81 Secondary pulmonary tuberculosis
82 Characteristic second infection adults bronchial dissemination infection from the apex downwards the course is usually protracted combination of old and fresh lesions proliferation is main lesions
83 Six types Focal pulmonary tuberculosis Infiltrative pulmonary tuberculosis Chronic fibro-cavernous pulmonary TB Caseous pneumonia Tuberculoma Tuberculous pleuritis
84 1. Focal tuberculosis The earliest lesions. most common site: lung apex number: one or more size: 0.5-1cm shape: well circumscribed, grayish white, yellow nature: mostly proliferative with central caseous necrosis and peripheral fibrosis Usually asymptomatic may calcify or quiescent form of infection or change into other types

85
86 2. Infiltrative pulmonary tuberculosis (subclavicular lesion): most common type, Sputum infection-open TB (1)site: upper part of the lungs (subclavicular infiltration) (2)serofibrinous exudative lesions with central caseous necrosis (3) X-ray : cloudiness (4) tuberculous toxic symptoms and chronic cough, frequently with hemoptysis easily cured and short clinical course

87

88
89 outcome a: healing b: progressive: enlargement, liquefaction, cavitation bronchogenic spread caseous pneumonia breaks through pleura-pneumothorax,tuberculosis pyopneumothoraxtransform into chronic fibro-cavernous TB
90 3. Chronic fibro-cavernous pulmonary TB (1) The upper lobes of lung contains multiple variant sizes, thick-walled chronic cavities. (2) Thicked cavity wall -- three components a. caseous necrosis b. tuberculous granulation tissue c. fibrous tissue (3) coexisting bronchial disseminated many tuberculous lesions and diffuse fibrosis in the pulmonary tissues. Later period, the lung becomes small, indurated,with pleural extensive adhesion, the function of the lung may be severely damaged.

91

92 Tubercle cavity Old foci of TB New foci of TB

93

94
95 Clinical feature Toxic:fever, night-sweat Respirator:cough, expectoration, hemoptysis, dyspnea, asphyxia breaks through pleura-pneumothorax, pyopneumothorax fibrosis -Cor Pulmonale
96 4. Caseous pneumonia May occur in debilitated immunodeficient or highly sensitized patients. Dissemination of large numbers of organisms in the focus via the bronchial tree, and spreading rapidly throughout large areas of lung parenchyma and producing a diffuse bronchopneumonia or lobar exudative consolidation ( galloping consumption ).
97 Pathological feature 1. Rapid serious condition of TB progression 2. One lobe or an entire lung affected and become consolidation 3. Severe exudation and severe necrosis 4. Serous exudate contain monocytes and lymphocytes in the alveoli 5. Young patients are more frequently affected

98

99
100

101

102

103 5. Tuberculoma Definition: solitary globular caseous lesion surrounded by fibrosis Size: 2-5cm in diameter. Site: well delineated upper lobe X-ray: it is easily mistaken for tumor Tuberculomas represent quiescent disease.

104

105 tuberculoma
106 6.Tuberculosis pleuritis According affected feature divide into: Moist tuberculous pleuritis (exudative tuberculous pleuritis) exudative inflammation (serious or serofibrinous). Heavy serious liquid hydrothorax. heavy fibrin formation thoracalgia. Dry tuberculous pleuritis (proliferative tuberculous pleuritis) This is a proliferative lesion dominate. Localized tubercles may form in the visceral pleura, and this may be followed by an tuberculous focus beneath pleura.

107

108

109
110
111 Respiratory tumors Nasopharyngeal carcinoma Laryngocarcinoma Pulmonary carcinoma
112 Pulmonary carcinoma (Bronchogenic carcinoma) 95% of primary lung tumors arise from the bronchial epithelium. Undoubtedly, the bronchogenic carcinoma is the number one cause of cancer related deaths in industrialized cities.
113 Etiopathogenisis Smoking Air pollution Vocational factor Molecular genetic change
114 Morphology Types of gross: central type periphery type diffuse type

115


116

117

118
119 Early stage pulmonary carcinoma: tumor mass <2cm, limited intrabronchi or infiltrated the bronchial wall and surrounding tissue, no metastasis in LN. Occult (concealed) carcinoama: cytologic smeares of sputum :tumor cells(+), clinic and X-ray(-), biopsy showed carcinoma in situ or early infiltrative carcinoma no metastasis in LN
120 Histologic classification (2003 WHO): squamous cell carcinoma small cell carcinoma adenocarcinoma large cell carcinoma adeno-squamous carcinoma sarcomatoid carcinoma carcinoid tumor salivary gland type carcinoma
121 Squamous cell carcinoma More common in men than women Tend to arise centrally in major bronchi and eventually spread to local hilar nodes Disseminate outside the thorax later than other histologic types Undergo central necrosis, cavitation Often preceded for years by squamous metaplasia/ dysplasia in the bronchial epithelium carcinoma in situ Atypical cells may be identified in cytologic smears of sputum or in bronchial lavage fluids or brushings, although asymptomatic and undetectable on radiographs

122

123 squamous carcinoma
124 Small cell lung carcinoma(sclc) The five-year survival rate is only 1 to 2%. Derived from neuroendocrine cells of the lung, express a variety of neuroendocrine markers.

125

126

127 Nests and cords of round to polygonal cell with scant cytoplasm, granular chromatin, and inconspicuous nucleoli.
128 Adenocarcinoma More common in women, and the association with smoking is weaker than for squamous cell carcinoma. usually peripherally located. grow slowly and form smaller masses than do other subtypes, but metastasize widely at an early stage.
 A special type of")
129 Bronchioloalveolar carcinoma (BAC) A special type of adenocarcinoma.
130 BAC has a better prognosis than other bronchogenic carcinoma, the localized single mass has a 50 to 70% five-year survival rate, and the multifocal variant has a 20 to 25% five-year survival rate.
131 Large cell carcinoma A group of neoplasm that lack cytological differentiation and probably represent squamous carcinoma or glandular neoplasms that are too undifferentiated to permit categorization. Have a poor prognosis because of their tendency to spread to distant sites early. five-year survival rate is 2 to 3%.

132 Large cell carcinoma

133 Thanks!
2015/4/14. Pneumonia. Diseases of Respiratory System Infection in the lung (distal airways, esp. alveoli) Lobar pneumonia.
 Lobar pneumonia.") Pneumonia Diseases of Respiratory System Infection in the lung (distal airways, esp. alveoli) 邓红浙江大学医学院病理学系 LUNG(reformed)5y-DH 1 hongdeng@zju.edu.cn Pathology (DH) 2 Pneumonia Bacteria pneumonia Viral
Pneumonia Diseases of Respiratory System Infection in the lung (distal airways, esp. alveoli) 邓红浙江大学医学院病理学系 LUNG(reformed)5y-DH 1 hongdeng@zju.edu.cn Pathology (DH) 2 Pneumonia Bacteria pneumonia Viral
Pathology of Pneumonia
 Pathology of Pneumonia Dr. Atif Ali Bashir Assistant Professor of Pathology College of Medicine Majma ah University Introduction: 5000 sq meters of area.! (olympic track) Filters >10,000 L of air / day!
Pathology of Pneumonia Dr. Atif Ali Bashir Assistant Professor of Pathology College of Medicine Majma ah University Introduction: 5000 sq meters of area.! (olympic track) Filters >10,000 L of air / day!
Key Difference - Pleural Effusion vs Pneumonia
 Difference Between Pleural Effusion and Pneumonia www.differencebetween.com Key Difference - Pleural Effusion vs Pneumonia Pleural effusion and pneumonia are two conditions that affect our respiratory
Difference Between Pleural Effusion and Pneumonia www.differencebetween.com Key Difference - Pleural Effusion vs Pneumonia Pleural effusion and pneumonia are two conditions that affect our respiratory
Unit II Problem 2 Pathology: Pneumonia
 Unit II Problem 2 Pathology: Pneumonia - Definition: pneumonia is the infection of lung parenchyma which occurs especially when normal defenses are impaired such as: Cough reflex. Damage of cilia in respiratory
Unit II Problem 2 Pathology: Pneumonia - Definition: pneumonia is the infection of lung parenchyma which occurs especially when normal defenses are impaired such as: Cough reflex. Damage of cilia in respiratory
Pathology of pulmonary tuberculosis. Dr: Salah Ahmed
 Pathology of pulmonary tuberculosis Dr: Salah Ahmed Is a chronic granulomatous disease, caused by Mycobacterium tuberculosis (hominis) Usually it involves lungs but may affect any organ or tissue Transmission:
Pathology of pulmonary tuberculosis Dr: Salah Ahmed Is a chronic granulomatous disease, caused by Mycobacterium tuberculosis (hominis) Usually it involves lungs but may affect any organ or tissue Transmission:
Respiratory Pathology. Kristine Krafts, M.D.
 Respiratory Pathology Kristine Krafts, M.D. Normal lung: alveolar spaces Respiratory Pathology Outline Acute respiratory distress syndrome Obstructive lung diseases Restrictive lung diseases Vascular
Respiratory Pathology Kristine Krafts, M.D. Normal lung: alveolar spaces Respiratory Pathology Outline Acute respiratory distress syndrome Obstructive lung diseases Restrictive lung diseases Vascular
Sheet: Patho-Pulmonary infections Done by: Maen Faoury
 Sheet: Patho-Pulmonary infections Done by: Maen Faoury Pneumonitis : might be an infection or not. Chemical Pneumonitis : not an infection. Parenchyma : an infection.( تندرج تحت ال pneumonitis) Lung Parenchyma
Sheet: Patho-Pulmonary infections Done by: Maen Faoury Pneumonitis : might be an infection or not. Chemical Pneumonitis : not an infection. Parenchyma : an infection.( تندرج تحت ال pneumonitis) Lung Parenchyma
09-Mar-15 PNEUMONIA RESPIRATORY SYSTEM L-3
 RESPIRATORY SYSTEM L-3 Professor Department of Pathology, University of Agriculture, Faisalabad. Email: mtjaved@uaf.edu.pk Web: https://sites.geocities.ws/mtjaved PNEUMONIA The pulmonary inflammatory response
RESPIRATORY SYSTEM L-3 Professor Department of Pathology, University of Agriculture, Faisalabad. Email: mtjaved@uaf.edu.pk Web: https://sites.geocities.ws/mtjaved PNEUMONIA The pulmonary inflammatory response
Histopathology: pulmonary pathology
 Histopathology: pulmonary pathology These presentations are to help you identify basic histopathological features. They do not contain the additional factual information that you need to learn about these
Histopathology: pulmonary pathology These presentations are to help you identify basic histopathological features. They do not contain the additional factual information that you need to learn about these
Pathology lab 4 DONE BY : MORAD ABU QAMAR
 Pathology lab 4 DONE BY : MORAD ABU QAMAR Chronic interstitial inflammation, lung Certain etiologic agents such as viruses are more likely to lead to chronic inflammation, as seen here in the lung of a
Pathology lab 4 DONE BY : MORAD ABU QAMAR Chronic interstitial inflammation, lung Certain etiologic agents such as viruses are more likely to lead to chronic inflammation, as seen here in the lung of a
Tuberculosis. By: Shefaa Q aqa
 Tuberculosis By: Shefaa Q aqa Tuberculosis is a communicable chronic granulomatous disease caused by Mycobacterium tuberculosis. It usually involves the lungs but may affect any organ or tissue in the
Tuberculosis By: Shefaa Q aqa Tuberculosis is a communicable chronic granulomatous disease caused by Mycobacterium tuberculosis. It usually involves the lungs but may affect any organ or tissue in the
an inflammation of the bronchial tubes
 BRONCHITIS DEFINITION Bronchitis is an inflammation of the bronchial tubes (or bronchi), which are the air passages that extend from the trachea into the small airways and alveoli. Triggers may be infectious
BRONCHITIS DEFINITION Bronchitis is an inflammation of the bronchial tubes (or bronchi), which are the air passages that extend from the trachea into the small airways and alveoli. Triggers may be infectious
TB Intensive Houston, Texas
 TB Intensive Houston, Texas October 15-17, 17 2013 Diagnosis of TB: Radiology Rosa M Estrada-Y-Martin, MD MSc FCCP October 16, 2013 Rosa M Estrada-Y-Martin, MD MSc FCCP, has the following disclosures to
TB Intensive Houston, Texas October 15-17, 17 2013 Diagnosis of TB: Radiology Rosa M Estrada-Y-Martin, MD MSc FCCP October 16, 2013 Rosa M Estrada-Y-Martin, MD MSc FCCP, has the following disclosures to
Currently, there are about 15 million TB patients including 11 million of working age.
 Currently, there are about 15 million TB patients including 11 million of working age. The vast majority of infected people (90%) the disease does not progress. Predicted by WHO in the next twenty years
Currently, there are about 15 million TB patients including 11 million of working age. The vast majority of infected people (90%) the disease does not progress. Predicted by WHO in the next twenty years
CLINICAL FEATURES IN PULMONARY TUBERCULOSIS
 CLINICAL FEATURES IN PULMONARY TUBERCULOSIS Dr. Amitesh Aggarwal Department of Medicine Tuberculosis Captain of all the Men of Death Great White Plague devastating effect on society 100 years ago one in
CLINICAL FEATURES IN PULMONARY TUBERCULOSIS Dr. Amitesh Aggarwal Department of Medicine Tuberculosis Captain of all the Men of Death Great White Plague devastating effect on society 100 years ago one in
Tuberculosis - clinical forms. Dr. A.Torossian,, M.D., Ph. D. Department of Respiratory Diseases
 Tuberculosis - clinical forms Dr. A.Torossian,, M.D., Ph. D. Department of Respiratory Diseases 1 TB DISEASE Primary Post-primary (Secondary) Common primary forms Primary complex Tuberculosis of the intrathoracic
Tuberculosis - clinical forms Dr. A.Torossian,, M.D., Ph. D. Department of Respiratory Diseases 1 TB DISEASE Primary Post-primary (Secondary) Common primary forms Primary complex Tuberculosis of the intrathoracic
PULMONARY TUBERCULOSIS RADIOLOGY
 PULMONARY TUBERCULOSIS RADIOLOGY RADIOLOGICAL MODALITIES Medical radiophotography Radiography Fluoroscopy Linear (conventional) tomography Computed tomography Pulmonary angiography, bronchography Ultrasonography,
PULMONARY TUBERCULOSIS RADIOLOGY RADIOLOGICAL MODALITIES Medical radiophotography Radiography Fluoroscopy Linear (conventional) tomography Computed tomography Pulmonary angiography, bronchography Ultrasonography,
Slide 120, Lobar Pneumonia. Slide 120, Lobar Pneumonia. Slide 172, Interstitial Pneumonia. Slide 172, Interstitial Pneumonia. 53 Year-Old Smoker
 Slide 120, Lobar Pneumonia Slide 120, Lobar Pneumonia Slide 172, Interstitial Pneumonia Slide 172, Interstitial Pneumonia 53 Year-Old Smoker Emphysema Pink puffer Barrel chest Hyperinflation Trapped air
Slide 120, Lobar Pneumonia Slide 120, Lobar Pneumonia Slide 172, Interstitial Pneumonia Slide 172, Interstitial Pneumonia 53 Year-Old Smoker Emphysema Pink puffer Barrel chest Hyperinflation Trapped air
TUBERCULOSIS. By Dr. Najaf Masood Assistant Prof Pediatrics Benazir Bhutto Hospital Rawalpindi
 TUBERCULOSIS By Dr. Najaf Masood Assistant Prof Pediatrics Benazir Bhutto Hospital Rawalpindi Tuberculosis Infectious, Systemic, Chronic granulomatous disease caused by mycobacterium tuberculosis DEFINITION
TUBERCULOSIS By Dr. Najaf Masood Assistant Prof Pediatrics Benazir Bhutto Hospital Rawalpindi Tuberculosis Infectious, Systemic, Chronic granulomatous disease caused by mycobacterium tuberculosis DEFINITION
Exam 2 Respiratory Disorders
 Exam 2 Respiratory Disorders Common Cold Common Cold Pathology Common Cold Consequences Rhinosinusitis Rhinosinusitis Pathology Rhinosinusitis ostia can close due to Influenza (Flu) Influenza Pathology
Exam 2 Respiratory Disorders Common Cold Common Cold Pathology Common Cold Consequences Rhinosinusitis Rhinosinusitis Pathology Rhinosinusitis ostia can close due to Influenza (Flu) Influenza Pathology
Pulmonary Pathology II. William Bligh-Glover M.D. Department of Anatomy, CWRU
 Pulmonary Pathology II William Bligh-Glover M.D. Department of Anatomy, CWRU Goals and Objectives Comprehend the etiology, pathogenesis/pathopysiology and consequences of pulmonary hypertension Distinguish
Pulmonary Pathology II William Bligh-Glover M.D. Department of Anatomy, CWRU Goals and Objectives Comprehend the etiology, pathogenesis/pathopysiology and consequences of pulmonary hypertension Distinguish
Tuberculosis: The Essentials
 Tuberculosis: The Essentials Kendra L. Fisher, MD, PhD THORACIC TUBERCULOSIS: THE BARE ESSENTIALS Kendra Fisher MD, FRCP (C) Department of Radiology Loma Linda University Medical Center TUBERCULOSIS ()
Tuberculosis: The Essentials Kendra L. Fisher, MD, PhD THORACIC TUBERCULOSIS: THE BARE ESSENTIALS Kendra Fisher MD, FRCP (C) Department of Radiology Loma Linda University Medical Center TUBERCULOSIS ()
Respiratory Diseases and Disorders
 Chapter 9 Respiratory Diseases and Disorders Anatomy and Physiology Chest, lungs, and conducting airways Two parts: Upper respiratory system consists of nose, mouth, sinuses, pharynx, and larynx Lower
Chapter 9 Respiratory Diseases and Disorders Anatomy and Physiology Chest, lungs, and conducting airways Two parts: Upper respiratory system consists of nose, mouth, sinuses, pharynx, and larynx Lower
An Introduction to Radiology for TB Nurses
 An Introduction to Radiology for TB Nurses Garold O. Minns, MD September 14, 2017 TB Nurse Case Management September 12 14, 2017 EXCELLENCE EXPERTISE INNOVATION Garold O. Minns, MD has the following disclosures
An Introduction to Radiology for TB Nurses Garold O. Minns, MD September 14, 2017 TB Nurse Case Management September 12 14, 2017 EXCELLENCE EXPERTISE INNOVATION Garold O. Minns, MD has the following disclosures
Diagnosis of TB: Radiology David Finlay, MD
 TB Intensive Tyler, Texas June 2-4, 2010 Diagnosis of TB: Radiology David Finlay, MD June 3, 2010 2stages stages- Tuberculosis 1. primary infection 2. reactivation, or post primary disease 2 1 Primary
TB Intensive Tyler, Texas June 2-4, 2010 Diagnosis of TB: Radiology David Finlay, MD June 3, 2010 2stages stages- Tuberculosis 1. primary infection 2. reactivation, or post primary disease 2 1 Primary
PATHOLOGY OF RESPIRATORY SYSTEM
 PATHOLOGY OF RESPIRATORY SYSTEM PEERAYUT SITTHICHAIYAKUL, M.D. Upper respiratory tract Nose Pharynx (Throat) Larynx Trachea Lower respiratory tract Lung - Bronchi - Bronchiole - Alveoli 1 CONTENT Upper
PATHOLOGY OF RESPIRATORY SYSTEM PEERAYUT SITTHICHAIYAKUL, M.D. Upper respiratory tract Nose Pharynx (Throat) Larynx Trachea Lower respiratory tract Lung - Bronchi - Bronchiole - Alveoli 1 CONTENT Upper
PATHOLOGY OF RESPIRATORY SYSTEM
 PATHOLOGY OF RESPIRATORY SYSTEM Upper respiratory tract Lower respiratory tract Nose Lung Pharynx (Throat) - Bronchi Larynx - Bronchiole Trachea - Alveoli PEERAYUT SITTHICHAIYAKUL, M.D. CONTENT Upper respiratory
PATHOLOGY OF RESPIRATORY SYSTEM Upper respiratory tract Lower respiratory tract Nose Lung Pharynx (Throat) - Bronchi Larynx - Bronchiole Trachea - Alveoli PEERAYUT SITTHICHAIYAKUL, M.D. CONTENT Upper respiratory
TB Radiology for Nurses Garold O. Minns, MD
 TB Nurse Case Management Salina, Kansas March 31-April 1, 2010 TB Radiology for Nurses Garold O. Minns, MD April 1, 2010 TB Radiology for Nurses Highway Patrol Training Center Salina, KS April 1, 2010
TB Nurse Case Management Salina, Kansas March 31-April 1, 2010 TB Radiology for Nurses Garold O. Minns, MD April 1, 2010 TB Radiology for Nurses Highway Patrol Training Center Salina, KS April 1, 2010
How to Analyse Difficult Chest CT
 How to Analyse Difficult Chest CT Complex diseases are:- - Large lesion - Unusual or atypical pattern - Multiple discordant findings Diffuse diseases are:- - Numerous findings in both sides 3 basic steps
How to Analyse Difficult Chest CT Complex diseases are:- - Large lesion - Unusual or atypical pattern - Multiple discordant findings Diffuse diseases are:- - Numerous findings in both sides 3 basic steps
CHRONIC INFLAMMATION
 CHRONIC INFLAMMATION Chronic inflammation is an inflammatory response of prolonged duration often for months, years or even indefinitely. Its prolonged course is proved by persistence of the causative
CHRONIC INFLAMMATION Chronic inflammation is an inflammatory response of prolonged duration often for months, years or even indefinitely. Its prolonged course is proved by persistence of the causative
The Respiratory System
 The Respiratory System Respiratory Anatomy Upper respiratory tract Nose Nasal passages Pharynx Larynx Respiratory Anatomy Functions of the upper respiratory tract: Provide entry for inhaled air Respiratory
The Respiratory System Respiratory Anatomy Upper respiratory tract Nose Nasal passages Pharynx Larynx Respiratory Anatomy Functions of the upper respiratory tract: Provide entry for inhaled air Respiratory
Radiological Aspects of Pulmonary Tuberculosis in Immunocompetent Hosts
 Nov 2003 Radiological Aspects of Pulmonary Tuberculosis in Immunocompetent Hosts Josh Rempell, Harvard Medical School Year III Tuberculosis: the captain of all (wo)men of death Overall, one third of the
Nov 2003 Radiological Aspects of Pulmonary Tuberculosis in Immunocompetent Hosts Josh Rempell, Harvard Medical School Year III Tuberculosis: the captain of all (wo)men of death Overall, one third of the
INFLAMMATION & REPAIR
 INFLAMMATION & REPAIR Histopath Laboratory 1 Winter 2013 Chelsea Martin Special thanks to Drs. Hanna and Forzan Goals: Examine Tissue and Identify the Organ Describe the lesion, grossly and histologically
INFLAMMATION & REPAIR Histopath Laboratory 1 Winter 2013 Chelsea Martin Special thanks to Drs. Hanna and Forzan Goals: Examine Tissue and Identify the Organ Describe the lesion, grossly and histologically
Chapter 22. Pulmonary Infections
 Chapter 22 Pulmonary Infections Objectives State the incidence of pneumonia in the United States and its economic impact. Discuss the current classification scheme for pneumonia and be able to define hospital-acquired
Chapter 22 Pulmonary Infections Objectives State the incidence of pneumonia in the United States and its economic impact. Discuss the current classification scheme for pneumonia and be able to define hospital-acquired
Streptococcus pneumonia
 Streptococcus pneumonia The pneumococci (S. pneumoniae) are gram-positive diplococci. Often lancet shaped or arranged in chains, possessing a capsule of polysaccharide that permits typing with specific
Streptococcus pneumonia The pneumococci (S. pneumoniae) are gram-positive diplococci. Often lancet shaped or arranged in chains, possessing a capsule of polysaccharide that permits typing with specific
Characteristic. Course of disease:short Days--one month Changes : Alteration, exudation Tissue destruction Inflammation cells: major neutrophils
 ACUTE INFLAMMATION Characteristic Course of disease:short Days--one month Changes : Alteration, exudation Tissue destruction Inflammation cells: major neutrophils TYPES Serous Inflammation Fibrinous Inflammation
ACUTE INFLAMMATION Characteristic Course of disease:short Days--one month Changes : Alteration, exudation Tissue destruction Inflammation cells: major neutrophils TYPES Serous Inflammation Fibrinous Inflammation
Respiratory System الفريق الطبي االكاديمي
 Respiratory System الفريق الطبي االكاديمي Pathology sheet 5 Tuberculosis Done by: Ahmad Al-Sahele Introduction: as we know TB is caused by mycobacterium tubercolosis; now keep in your mind another microorganism
Respiratory System الفريق الطبي االكاديمي Pathology sheet 5 Tuberculosis Done by: Ahmad Al-Sahele Introduction: as we know TB is caused by mycobacterium tubercolosis; now keep in your mind another microorganism
DISEASES OF THE RESPIRATORY SYSTEM 2018 DR HEYAM AWAD LECTURE 3: CHRONIC BRNCHITIS AND BRONCHIECTASIS
 DISEASES OF THE RESPIRATORY SYSTEM 2018 DR HEYAM AWAD LECTURE 3: CHRONIC BRNCHITIS AND BRONCHIECTASIS INTRDUCTION In the last lecture we discussed the difference between restrictive and obstructive lung
DISEASES OF THE RESPIRATORY SYSTEM 2018 DR HEYAM AWAD LECTURE 3: CHRONIC BRNCHITIS AND BRONCHIECTASIS INTRDUCTION In the last lecture we discussed the difference between restrictive and obstructive lung
CELL AND TISSUE INJURY COURSE-II PATHOLOGY LABORATORY
 CELL AND TISSUE INJURY COURSE-II PATHOLOGY LABORATORY PATHOLOGY of INFECTIOUS DISEASES MICROSCOPY Rengin Ahıskalı Macroscopy samples are shown in the macroscopy presentations of the first two courses.
CELL AND TISSUE INJURY COURSE-II PATHOLOGY LABORATORY PATHOLOGY of INFECTIOUS DISEASES MICROSCOPY Rengin Ahıskalı Macroscopy samples are shown in the macroscopy presentations of the first two courses.
PULMONARY EMERGENCIES
 EMERGENCIES I. Pneumonia A. Bacterial Pneumonia (most common cause of a focal infiltrate) 1. Epidemiology a. Accounts for up to 10% of hospital admissions in the U.S. b. Most pneumonias are the result
EMERGENCIES I. Pneumonia A. Bacterial Pneumonia (most common cause of a focal infiltrate) 1. Epidemiology a. Accounts for up to 10% of hospital admissions in the U.S. b. Most pneumonias are the result
Pulmonary Diseases. We Move A Lot of Air. Basic Categories. Alveolar Level. Developmental
 Pulmonary Diseases We Move A Lot of Air Alveolar Level Functions Oxygenation CO 2 & ph Basic defenses Nose hairs Cilia Mucus Cough reflex Immune system Basic Categories Congenital Infectious Neoplastic
Pulmonary Diseases We Move A Lot of Air Alveolar Level Functions Oxygenation CO 2 & ph Basic defenses Nose hairs Cilia Mucus Cough reflex Immune system Basic Categories Congenital Infectious Neoplastic
Lung tumors & pleural lesions
 Lung tumors & pleural lesions A brief introduction 95% of lung tumors are carcinomas Among the remaining 5%, we will discuss: -Hamartoma the most common benign lung tumor spherical, coin lesion on x-rays
Lung tumors & pleural lesions A brief introduction 95% of lung tumors are carcinomas Among the remaining 5%, we will discuss: -Hamartoma the most common benign lung tumor spherical, coin lesion on x-rays
Destructive pulmonary disease due to mixed anaerobic infection
 Thorax (1970), 25, 41. Destructive pulmonary disease due to mixed anaerobic infection 0. SERIKI, A. ADEYOKUNNU, T. 0. DE LA CRUZ Departments of Paediatrics and Surgery, University College Hospital, Ibadan,
Thorax (1970), 25, 41. Destructive pulmonary disease due to mixed anaerobic infection 0. SERIKI, A. ADEYOKUNNU, T. 0. DE LA CRUZ Departments of Paediatrics and Surgery, University College Hospital, Ibadan,
SESSION IV: MECHANISMS OF HUMAN DISEASE: LABORATORY SESSIONS PULMONARY PATHOLOGY I. December 5, 2012
 SESSION IV: MECHANISMS OF HUMAN DISEASE: LABORATORY SESSIONS PULMONARY PATHOLOGY I December 5, 2012 FACULTY COPY GOAL: Describe the basic morphologic and pathophysiologic changes in various conditions
SESSION IV: MECHANISMS OF HUMAN DISEASE: LABORATORY SESSIONS PULMONARY PATHOLOGY I December 5, 2012 FACULTY COPY GOAL: Describe the basic morphologic and pathophysiologic changes in various conditions
May. Pathology #2. part. Rahaf Al-yousef. Mohammad Al-Qudah
 8 th May Pathology #2 nd Pneumonias 2 part Mohammad Al-Qudah Rahaf Al-yousef In the first part of our lectures today, we will define pneumonia clinically and pathologically(which is an infection of the
8 th May Pathology #2 nd Pneumonias 2 part Mohammad Al-Qudah Rahaf Al-yousef In the first part of our lectures today, we will define pneumonia clinically and pathologically(which is an infection of the
The Respiratory System. Dr. Ali Ebneshahidi
 The Respiratory System Dr. Ali Ebneshahidi Functions of The Respiratory System To allow gases from the environment to enter the bronchial tree through inspiration by expanding the thoracic volume. To allow
The Respiratory System Dr. Ali Ebneshahidi Functions of The Respiratory System To allow gases from the environment to enter the bronchial tree through inspiration by expanding the thoracic volume. To allow
Menigitidis. Dr Rodney Itaki Lecturer Anatomical Pathology Discipline
 Menigitidis Dr Rodney Itaki Lecturer Anatomical Pathology Discipline University of Papua New Guinea Division of Pathology School of Medicine & Health Sciences Review Normal Microanatomy Image Ref: www.histology-world.com
Menigitidis Dr Rodney Itaki Lecturer Anatomical Pathology Discipline University of Papua New Guinea Division of Pathology School of Medicine & Health Sciences Review Normal Microanatomy Image Ref: www.histology-world.com
(JPC ) Caprine lungs
 Caprine lungs") 2011-7-2 (JPC 3133973) Caprine lungs Bat Otgontugs Bovine Pathology Contributor: Natoinal Institute Animal Health, Tsukuba, Japan Signalment: 5-year 3-month old female Japanese native breed goat, (Capra
2011-7-2 (JPC 3133973) Caprine lungs Bat Otgontugs Bovine Pathology Contributor: Natoinal Institute Animal Health, Tsukuba, Japan Signalment: 5-year 3-month old female Japanese native breed goat, (Capra
New lung lesion in a 55 year-old male treated with chemoradiation for non-small cell lung carcinoma
 July 2016 New lung lesion in a 55 year-old male treated with chemoradiation for non-small cell lung carcinoma Contributed by: Laurel Rose, MD, Resident Physician, Indiana University School of Medicine,
July 2016 New lung lesion in a 55 year-old male treated with chemoradiation for non-small cell lung carcinoma Contributed by: Laurel Rose, MD, Resident Physician, Indiana University School of Medicine,
Acute pneumonia Simple complement
 Acute pneumonia Simple complement 1. Clinical variants of acute pneumonia in children are, except: A. Bronchopneumonia B. Lobar confluent pneumonia C. Viral pneumonia D. Interstitial pneumonia E. Chronic
Acute pneumonia Simple complement 1. Clinical variants of acute pneumonia in children are, except: A. Bronchopneumonia B. Lobar confluent pneumonia C. Viral pneumonia D. Interstitial pneumonia E. Chronic
Bronchogenic Carcinoma
 A 55-year-old construction worker has smoked 2 packs of ciggarettes daily for the past 25 years. He notes swelling in his upper extremity & face, along with dilated veins in this region. What is the most
A 55-year-old construction worker has smoked 2 packs of ciggarettes daily for the past 25 years. He notes swelling in his upper extremity & face, along with dilated veins in this region. What is the most
Inflammation. First Lab.
 Inflammation First Lab. The cardinal signs of inflammation are rubor (redness), calor (heat), tumor (swelling), dolor (pain), and loss of function. Seen here is skin with erythema, compared to the more
Inflammation First Lab. The cardinal signs of inflammation are rubor (redness), calor (heat), tumor (swelling), dolor (pain), and loss of function. Seen here is skin with erythema, compared to the more
Lung pathology. Acute pneumonias, acute viral respiratory infection. Ivan Sakharau, assist. lect.
 1 Lung pathology Acute pneumonias, acute viral respiratory infection Ivan Sakharau, assist. lect. Acute pneumonia is an inflammatory lung disease affecting alveoli with accumulation of exudate in the alveoli
1 Lung pathology Acute pneumonias, acute viral respiratory infection Ivan Sakharau, assist. lect. Acute pneumonia is an inflammatory lung disease affecting alveoli with accumulation of exudate in the alveoli
Firm Texture. (chronic) Cut surface: purulent exudate in bronchi Sequels: Abscesses,
 Cut surface: purulent exudate in bronchi Sequels: Abscesses,") 2008 Classification of Pneumonias in Domestic Animals There is no universal classification! Based on texture, distribution of lesions and type of exudate, pneumonias in domestic animals are currently classified
2008 Classification of Pneumonias in Domestic Animals There is no universal classification! Based on texture, distribution of lesions and type of exudate, pneumonias in domestic animals are currently classified
SESSION 1: GENERAL (BASIC) PATHOLOGY CONCEPTS Thursday, October 16, :30am - 11:30am FACULTY COPY
 PATHOLOGY CONCEPTS Thursday, October 16, :30am - 11:30am FACULTY COPY") SESSION 1: GENERAL (BASIC) PATHOLOGY CONCEPTS Thursday, October 16, 2008 9:30am - 11:30am FACULTY COPY GOAL: Describe the basic morphologic (structural) changes which occur in various pathologic conditions.
SESSION 1: GENERAL (BASIC) PATHOLOGY CONCEPTS Thursday, October 16, 2008 9:30am - 11:30am FACULTY COPY GOAL: Describe the basic morphologic (structural) changes which occur in various pathologic conditions.
Zhejiang University School of Medicine. Basic PATHOLOGY ZHOU REN. Prof., M.D., Ph.D.
 Zhejiang University School of Medicine Basic PATHOLOGY 周 韧 ZHOU REN Prof., M.D., Ph.D. Department of Pathology & Patho-physiology Institute of Pathology & Forensic Medicine Zhejiang University Judicial
Zhejiang University School of Medicine Basic PATHOLOGY 周 韧 ZHOU REN Prof., M.D., Ph.D. Department of Pathology & Patho-physiology Institute of Pathology & Forensic Medicine Zhejiang University Judicial
Cellular Pathology. Histopathology Lab #2 (web) Paul Hanna Jan 2018
 Paul Hanna Jan 2018") Cellular Pathology Histopathology Lab #2 (web) Paul Hanna Jan 2018 Slide #91 Clinical History: a necropsy was performed on an aged cat the gross pathological changes included: widespread subcutaneous edema
Cellular Pathology Histopathology Lab #2 (web) Paul Hanna Jan 2018 Slide #91 Clinical History: a necropsy was performed on an aged cat the gross pathological changes included: widespread subcutaneous edema
Pulmonary Pathophysiology
 Pulmonary Pathophysiology 1 Reduction of Pulmonary Function 1. Inadequate blood flow to the lungs hypoperfusion 2. Inadequate air flow to the alveoli - hypoventilation 2 Signs and Symptoms of Pulmonary
Pulmonary Pathophysiology 1 Reduction of Pulmonary Function 1. Inadequate blood flow to the lungs hypoperfusion 2. Inadequate air flow to the alveoli - hypoventilation 2 Signs and Symptoms of Pulmonary
Replacement of air with fluid, inflammatory. cells or cellular debris. Parenchymal, Interstitial (Restrictive) and Vascular Diseases.
 and Vascular Diseases.") Parenchymal, Interstitial (Restrictive) and Vascular Diseases Alain C. Borczuk, M.D. Dept of Pathology Replacement of air with fluid, inflammatory cells Pulmonary Edema Pneumonia Hemorrhage Diffuse alveolar
Parenchymal, Interstitial (Restrictive) and Vascular Diseases Alain C. Borczuk, M.D. Dept of Pathology Replacement of air with fluid, inflammatory cells Pulmonary Edema Pneumonia Hemorrhage Diffuse alveolar
Case 1 : Question. 1.1 What is the intralobular distribution? 1. Centrilobular 2. Perilymphatic 3. Random
 Interesting case Case 1 Case 1 : Question 1.1 What is the intralobular distribution? 1. Centrilobular 2. Perilymphatic 3. Random Case 1: Answer 1.1 What is the intralobular distribution? 1. Centrilobular
Interesting case Case 1 Case 1 : Question 1.1 What is the intralobular distribution? 1. Centrilobular 2. Perilymphatic 3. Random Case 1: Answer 1.1 What is the intralobular distribution? 1. Centrilobular
Acute and Chronic Lung Disease
 KATHOLIEKE UNIVERSITEIT LEUVEN Faculty of Medicine Acute and Chronic Lung Disease W De Wever, JA Verschakelen Department of Radiology, University Hospitals Leuven, Belgium Clinical utility of HRCT To detect
KATHOLIEKE UNIVERSITEIT LEUVEN Faculty of Medicine Acute and Chronic Lung Disease W De Wever, JA Verschakelen Department of Radiology, University Hospitals Leuven, Belgium Clinical utility of HRCT To detect
Cell injury, adaptation and death. Unite one Second Lab.
 Cell injury, adaptation and death Unite one Second Lab. The two lung abscesses seen here are examples of liquefactive necrosis in which there is a liquid center in an area of tissue injury. One abscess
Cell injury, adaptation and death Unite one Second Lab. The two lung abscesses seen here are examples of liquefactive necrosis in which there is a liquid center in an area of tissue injury. One abscess
Lymphoid System: cells of the immune system. Answer Sheet
 Lymphoid System: cells of the immune system Answer Sheet Q1 Which areas of the lymph node have most CD3 staining? A1 Most CD3 staining is present in the paracortex (T cell areas). This is towards the outside
Lymphoid System: cells of the immune system Answer Sheet Q1 Which areas of the lymph node have most CD3 staining? A1 Most CD3 staining is present in the paracortex (T cell areas). This is towards the outside
Respiratory system. Applied Anatomy &Physiology
 Respiratory system Applied Anatomy &Physiology Anatomy The respiratory system consists of 1)The Upper airway : Nose, mouth and larynx 2)The Lower airways Trachea and the two lungs. Within the lungs,
Respiratory system Applied Anatomy &Physiology Anatomy The respiratory system consists of 1)The Upper airway : Nose, mouth and larynx 2)The Lower airways Trachea and the two lungs. Within the lungs,
Kidney Case 1 SURGICAL PATHOLOGY REPORT
 Kidney Case 1 Surgical Pathology Report February 9, 2007 Clinical History: This 45 year old woman was found to have a left renal mass. CT urography with reconstruction revealed a 2 cm medial mass which
Kidney Case 1 Surgical Pathology Report February 9, 2007 Clinical History: This 45 year old woman was found to have a left renal mass. CT urography with reconstruction revealed a 2 cm medial mass which
Pathology of Tumors of Lung Pathology of Tumors of Lung o Classify lung tumors.
 Pathology of Tumors of Lung Pathology of Tumors of Lung o Classify lung tumors. o Classify bronchogenic carcinoma. o Discuss etiopathogenesis of bronchogenic ca. o Discuss morphological features of squamous
Pathology of Tumors of Lung Pathology of Tumors of Lung o Classify lung tumors. o Classify bronchogenic carcinoma. o Discuss etiopathogenesis of bronchogenic ca. o Discuss morphological features of squamous
5/5/2013. The Respiratory System. Chapter 16 Notes. The Respiratory System. Nasal Cavity. Sinuses
 The Respiratory System Chapter 16 Notes The Respiratory System Objectives List the general functions of the respiratory system. Identify the organs of the respiratory system. Describe the functions of
The Respiratory System Chapter 16 Notes The Respiratory System Objectives List the general functions of the respiratory system. Identify the organs of the respiratory system. Describe the functions of
PATHOLOGY Intracellular Degeneration LAB 1
 PATHOLOGY Intracellular Degeneration LAB 1 Cellular swelling Liver Organ :- Liver Lesion :- 1. Narrowing of hepatic sinusoids due to the swelling of hepatocyte. 2. The cytoplasm of affected hepatocyte
PATHOLOGY Intracellular Degeneration LAB 1 Cellular swelling Liver Organ :- Liver Lesion :- 1. Narrowing of hepatic sinusoids due to the swelling of hepatocyte. 2. The cytoplasm of affected hepatocyte
BREAST PATHOLOGY. Fibrocystic Changes
 BREAST PATHOLOGY Lesions of the breast are very common, and they present as palpable, sometimes painful, nodules or masses. Most of these lesions are benign. Breast cancer is the 2 nd most common cause
BREAST PATHOLOGY Lesions of the breast are very common, and they present as palpable, sometimes painful, nodules or masses. Most of these lesions are benign. Breast cancer is the 2 nd most common cause
Diseases of the Lung and Respiratory Tract, Part I. William Bligh-Glover M.D. Department of Anatomy, CWRU
 Diseases of the Lung and Respiratory Tract, Part I William Bligh-Glover M.D. Department of Anatomy, CWRU Educational objectives: Distinguish the types of atelectasis and their etiologies Distinguish the
Diseases of the Lung and Respiratory Tract, Part I William Bligh-Glover M.D. Department of Anatomy, CWRU Educational objectives: Distinguish the types of atelectasis and their etiologies Distinguish the
Acute and Chronic Inflammation Pathology 1 - Dr. Gary Mumaugh
 Acute and Chronic Inflammation Pathology 1 - Dr. Gary Mumaugh Introduction Injurious stimuli cause a protective vascular connective tissue reaction called inflammation Acute and chronic forms o Inflame
Acute and Chronic Inflammation Pathology 1 - Dr. Gary Mumaugh Introduction Injurious stimuli cause a protective vascular connective tissue reaction called inflammation Acute and chronic forms o Inflame
Respiratory Pathology Lab 2: Lung. Shannon Martinson,
 Respiratory Pathology Lab 2: Lung Shannon Martinson, 2017 http://people.upei.ca/smartinson/ Case 1 Signalment: 9 month old DSH cat History: Poor doer with stunted growth One month of lethargy one day the
Respiratory Pathology Lab 2: Lung Shannon Martinson, 2017 http://people.upei.ca/smartinson/ Case 1 Signalment: 9 month old DSH cat History: Poor doer with stunted growth One month of lethargy one day the
Asthma. - A chronic inflammatory disorder which causes recurrent episodes of wheezing, breathlessness, cough and chest tightness.
 Obstructive diseases Asthma - A chronic inflammatory disorder which causes recurrent episodes of wheezing, breathlessness, cough and chest tightness. - Characterized by Intermittent and reversible (the
Obstructive diseases Asthma - A chronic inflammatory disorder which causes recurrent episodes of wheezing, breathlessness, cough and chest tightness. - Characterized by Intermittent and reversible (the
Community Acquired Pneumonia. Abdullah Alharbi, MD, FCCP
 Community Acquired Pneumonia Abdullah Alharbi, MD, FCCP A 68 y/ male presented to the ED with SOB and productive coughing for 2 days. Reports poor oral intake since onset due to nausea and intermittent
Community Acquired Pneumonia Abdullah Alharbi, MD, FCCP A 68 y/ male presented to the ED with SOB and productive coughing for 2 days. Reports poor oral intake since onset due to nausea and intermittent
Diseases of the breast (1 of 2)
") Diseases of the breast (1 of 2) Introduction A histology introduction Normal ducts and lobules of the breast are lined by two layers of cells a layer of luminal cells overlying a second layer of myoepithelial
Diseases of the breast (1 of 2) Introduction A histology introduction Normal ducts and lobules of the breast are lined by two layers of cells a layer of luminal cells overlying a second layer of myoepithelial
Lecture Notes. Chapter 16: Bacterial Pneumonia
 Lecture Notes Chapter 16: Bacterial Pneumonia Objectives Explain the epidemiology Identify the common causes Explain the pathological changes in the lung Identify clinical features Explain the treatment
Lecture Notes Chapter 16: Bacterial Pneumonia Objectives Explain the epidemiology Identify the common causes Explain the pathological changes in the lung Identify clinical features Explain the treatment
Necrosis is death of cells and tissues in the living animal. Focal/ Multifocal necrosis- terms used for one
 Necrosis Necrosis Necrosis is death of cells and tissues in the living animal. Focal/ Multifocal necrosis- terms used for one or more, small, clearly defined areas of necrosis. Diffuse necrosis- term used
Necrosis Necrosis Necrosis is death of cells and tissues in the living animal. Focal/ Multifocal necrosis- terms used for one or more, small, clearly defined areas of necrosis. Diffuse necrosis- term used
Chest Radiology Interpretation: Findings of Tuberculosis
 Chest Radiology Interpretation: Findings of Tuberculosis Get out your laptops, smart phones or other devices pollev.com/chestradiology Case #1 1 Plombage Pneumonia Cancer 2 Reading the TB CXR Be systematic!
Chest Radiology Interpretation: Findings of Tuberculosis Get out your laptops, smart phones or other devices pollev.com/chestradiology Case #1 1 Plombage Pneumonia Cancer 2 Reading the TB CXR Be systematic!
Anatomy. The respiratory system starts from the nose, mouth, larynx, trachea, and the two lungs.
 Respiratory System Anatomy The respiratory system starts from the nose, mouth, larynx, trachea, and the two lungs. Within the lungs, the bronchi transport air with oxygen to the alveoli on inspiration
Respiratory System Anatomy The respiratory system starts from the nose, mouth, larynx, trachea, and the two lungs. Within the lungs, the bronchi transport air with oxygen to the alveoli on inspiration
Case Scenario 1: Thyroid
 Case Scenario 1: Thyroid History and Physical Patient is an otherwise healthy 80 year old female with the complaint of a neck mass first noticed two weeks ago. The mass has increased in size and is palpable.
Case Scenario 1: Thyroid History and Physical Patient is an otherwise healthy 80 year old female with the complaint of a neck mass first noticed two weeks ago. The mass has increased in size and is palpable.
WSC , Conference 9, Case 1. Tissue from a nyala.
 WSC 2009-2010, Conference 9, Case 1. Tissue from a nyala. MICROSCOPIC DESCRIPTION: Heart, atrium (1 pt.): Approximately 40% of the atrial myocardium is replaced by areas of fibrous connective tissue (1
WSC 2009-2010, Conference 9, Case 1. Tissue from a nyala. MICROSCOPIC DESCRIPTION: Heart, atrium (1 pt.): Approximately 40% of the atrial myocardium is replaced by areas of fibrous connective tissue (1
number Done by Corrected by Doctor Mousa Al-Abbadi
 number 11 Done by Husam Abu-Awad Corrected by Muhammad Tarabieh Doctor Mousa Al-Abbadi The possible outcomes of an acute inflammation are the following: 1- A complete resolution in which the tissue returns
number 11 Done by Husam Abu-Awad Corrected by Muhammad Tarabieh Doctor Mousa Al-Abbadi The possible outcomes of an acute inflammation are the following: 1- A complete resolution in which the tissue returns
7. Respiratory cilial function is affected by all except a. Smoking b. Loss of cough reflex c. Haemaglutins d. Cystic fibrosis e.
 RESPIRATORY SYSTEM 1. All of the following are neoplastic syndromes associated with lung cancer except a. Cushing s b. SIADH c. Hypocalcaemia d. Carcinoid e. Hypertrophic osteoarthropathy 2. Most PEs a.
RESPIRATORY SYSTEM 1. All of the following are neoplastic syndromes associated with lung cancer except a. Cushing s b. SIADH c. Hypocalcaemia d. Carcinoid e. Hypertrophic osteoarthropathy 2. Most PEs a.
Respiratory Tract Cytology
 Respiratory Tract Cytology 40 th European Congress of Cytology Liverpool, UK Momin T. Siddiqui M.D. Professor of Pathology and Laboratory Medicine Director of Cytopathology Emory University Hospital, Atlanta,
Respiratory Tract Cytology 40 th European Congress of Cytology Liverpool, UK Momin T. Siddiqui M.D. Professor of Pathology and Laboratory Medicine Director of Cytopathology Emory University Hospital, Atlanta,
RESPIRATORY DISORDERS
 RESPIRATORY DISORDERS INTRODUCTION Respiratory disorders refers to the medical term that include different pathological conditions affecting the organs and tissues of respiratory system which make gas
RESPIRATORY DISORDERS INTRODUCTION Respiratory disorders refers to the medical term that include different pathological conditions affecting the organs and tissues of respiratory system which make gas
Chapter 10 Respiratory System J00-J99. Presented by: Jesicca Andrews
 Chapter 10 Respiratory System J00-J99 Presented by: Jesicca Andrews 1 Respiratory System 2 Respiratory Infections A respiratory infection cannot be assumed from a laboratory report alone; physician concurrence
Chapter 10 Respiratory System J00-J99 Presented by: Jesicca Andrews 1 Respiratory System 2 Respiratory Infections A respiratory infection cannot be assumed from a laboratory report alone; physician concurrence
HISTOPATHOLOGY. Shannon Martinson
 HISTOPATHOLOGY Shannon Martinson March 2013 Case #1 History: 8 year old beagle Neck pain for the past couple of weeks Paresis, followed by paralysis developed over the past few days Gross Description courtesy
HISTOPATHOLOGY Shannon Martinson March 2013 Case #1 History: 8 year old beagle Neck pain for the past couple of weeks Paresis, followed by paralysis developed over the past few days Gross Description courtesy
Pneumonia. Dr. Rami M Adil Al-Hayali Assistant professor in medicine
 Pneumonia Dr. Rami M Adil Al-Hayali Assistant professor in medicine Definition Pneumonia is an acute respiratory illness caused by an infection of the lung parenchyma, associated with recently developed
Pneumonia Dr. Rami M Adil Al-Hayali Assistant professor in medicine Definition Pneumonia is an acute respiratory illness caused by an infection of the lung parenchyma, associated with recently developed
Epiglottitis. Bronchitis. Bronchiolitis. Pneumonia. Croup syndrome. Miss. kamlah 2
 Miss. kamlah 1 Epiglottitis. Bronchitis. Bronchiolitis. Pneumonia. Croup syndrome. Miss. kamlah 2 Acute Epiglottitis Is an infection of the epiglottis, the long narrow structure that closes off the glottis
Miss. kamlah 1 Epiglottitis. Bronchitis. Bronchiolitis. Pneumonia. Croup syndrome. Miss. kamlah 2 Acute Epiglottitis Is an infection of the epiglottis, the long narrow structure that closes off the glottis
Index. B Biological factors, 2 Brain stem encephalitis, Burkitt s lymphoma, 83, 105
 Index A Acquired immunodeficiency syndrome (AIDS) abdomen gallbladder complications, 97, 107 109 gastrointestinal complications, 96, 105 106 liver complications, 97, 107 109 neoplasm, 99, 110 111 pancreas
Index A Acquired immunodeficiency syndrome (AIDS) abdomen gallbladder complications, 97, 107 109 gastrointestinal complications, 96, 105 106 liver complications, 97, 107 109 neoplasm, 99, 110 111 pancreas
Clinical Manifestations of HIV
 HIV Symptoms Diane Havlir, MD Professor of Medicine and Chief, HIV/AIDS Division University of California, San Francisco (UCSF) WorldMedSchool; July 2, 2013 1 Clinical Manifestations of HIV! Result from
HIV Symptoms Diane Havlir, MD Professor of Medicine and Chief, HIV/AIDS Division University of California, San Francisco (UCSF) WorldMedSchool; July 2, 2013 1 Clinical Manifestations of HIV! Result from
Lung Cancer Risks. Cancer in the United States, Cancer Death Rates, US The Scheme: From Nicotine Addiction to Lung Cancer
 Cancer in the United States, 2004 Lung Cancer Risks Cigarette Smoking Environmental Tobacco Smoke Other Carcinogens Asbestos, Arsenic, Radon, Bis(chloromethyl) ether, Chromium, Foundry fumes, nickel, mustard
Cancer in the United States, 2004 Lung Cancer Risks Cigarette Smoking Environmental Tobacco Smoke Other Carcinogens Asbestos, Arsenic, Radon, Bis(chloromethyl) ether, Chromium, Foundry fumes, nickel, mustard
TB Intensive San Antonio, Texas November 29-December 2, 2011
 TB Intensive San Antonio, Texas November 29-December 2, 2011 Diagnosis of TB: Radiology Michael McCarthy, MD, FACR November 30, 2011 Michael McCarthy, MD, FACR has the following disclosures to make: No
TB Intensive San Antonio, Texas November 29-December 2, 2011 Diagnosis of TB: Radiology Michael McCarthy, MD, FACR November 30, 2011 Michael McCarthy, MD, FACR has the following disclosures to make: No
Respiratory Pathophysiology
 Respiratory Pathophysiology Objectives: Respiratory infections and lung cancer. Pleural effusion & edema, pleuritis, pneumothorax and atelectasis. Obstructive airway disease and chronic interstitial lung
Respiratory Pathophysiology Objectives: Respiratory infections and lung cancer. Pleural effusion & edema, pleuritis, pneumothorax and atelectasis. Obstructive airway disease and chronic interstitial lung
General History. 林陳 珠 Female 69 years old 住院期間 : ~ Chief Complaint : sudden loss of conscious 5 minutes in the morning.
 General History 林陳 珠 Female 69 years old 住院期間 : 93.5.8~93.5.15 Chief Complaint : sudden loss of conscious for 2-52 5 minutes in the morning. General History DM under regular medical control for 10 years.
General History 林陳 珠 Female 69 years old 住院期間 : 93.5.8~93.5.15 Chief Complaint : sudden loss of conscious for 2-52 5 minutes in the morning. General History DM under regular medical control for 10 years.
Radiological syndroms. Alveolar syndrome Bronchial syndrome Interstitial syndrome Vascular syndrome Mediastinal Syndrome
 Radiological syndroms Alveolar syndrome Bronchial syndrome Interstitial syndrome Vascular syndrome Mediastinal Syndrome Alveolar syndrome Pulmonary architecture : Morphological unit is the lobule 15-25mm
Radiological syndroms Alveolar syndrome Bronchial syndrome Interstitial syndrome Vascular syndrome Mediastinal Syndrome Alveolar syndrome Pulmonary architecture : Morphological unit is the lobule 15-25mm
Normal thyroid tissue
 Thyroid Pathology Overview Normal thyroid tissue Normal thyroid tissue with follicles filled with colloid. Thyroid cells form follicles, spheres of epithelial cells (always single layered in health, usually
Thyroid Pathology Overview Normal thyroid tissue Normal thyroid tissue with follicles filled with colloid. Thyroid cells form follicles, spheres of epithelial cells (always single layered in health, usually