Bone and Joint Infections Oh, My
|
|
|
- Amelia McCormick
- 5 years ago
- Views:
Transcription





1 Bone and Joint Infections Oh, My Dale Jarka, MD,CM, FRCSC The Children s Mercy Hospitals & Clinics The Children's Mercy Hospital
2 Disclosures A: I have no relevant financial relationships with the manufacturer(s) of any commercial product(s) and/or provider(s) of commercial services discussed in this CME activity B: I do not intend to discuss an unapproved/investigative use of a commercial product/device in my presentation

3 Objectives Compare and contrast the bacterial causes of osteomyelitis and septic arthritis in children 3

4 Gap New information on bone and joint infections has been published 4
5 Practice Change In addition to local cultures, the learner will obtain a blood culture in any child suspected of having a bone and joint infection 5
6 Bone & Joint Infections Objectives: Compare and contrast the bacterial causes of osteomyelitis & septic arthritis in children 6
7 Bone & Joint Infections Objectives: Compare and contrast the bacterial causes of osteomyelitis & septic arthritis in children Identify the importance of diagnosing pediatric MSK infections 7
8 Bone & Joint Infections Objectives: Compare and contrast the bacterial causes of osteomyelitis & septic arthritis in children Identify the importance of diagnosing pediatric MSK infections Review appropriate diagnostic work-up 8
9 Bone & Joint Infections Rationale: 9
10 Bone & Joint Infections Rationale: Increasing number & virulence 10
11 Bone & Joint Infections Rationale: Increasing number & virulence Challenging to recognize & treat 11
12 Bone & Joint Infections Rationale: Increasing number & virulence Challenging to recognize & treat High morbidity & mortality 12

13 MSK Work Up Consider: Age & history Physical exam Radiology Lab 13
14 14

15 2 yo male Limping yesterday Case 1 Today refuses to bear weight
16 Case 1 No recent illness No trauma Febrile to 102º F in ER
17 Case 1 Exam: Doesn t move RLE Pain, crying with attempts at motion
18 Case 1 Lab results WBC 10 ESR 48 CRP 18 Blood cultures pending (remember to obtain!)


19 xrays Imaging
20 Ultrasound
21 Ultrasound
22 Ultrasound
23 Ultrasound
24 Diagnosis? Presumptive septic hip: Fevers, elevated ESR/CRP Refusal to bear weight +hip joint effusion 24
25 Diagnosis? Next step?? Aspiration by I.R.? Surgery? MRI first? 25

26 Gm stain = Gm + cocci Aspiration Septic arthritis > 50,000 WBC 20,000-50,000 WBC? (Cut-off for septic arthritis is gray) WBC = 78,000 (92% neutrophils)

27 Arthrotomy & Irrigation Obtain cultures Drain the hip joint decreases hydrostatic pressure & reduce risk of AVN evacuates debris and bacterial products decrease inflammatory response
28 Antibiotic management Timing of antibiotics JBJS 2015 Antibiotic use (pre hospital or within institution) not associated with lower rate of positive surgical site cultures.
29 Antibiotic management Choice and duration of antibiotics: Presumptive organism (staph. vs strep.) Now more likely to start w/ clinda (rather than Ancef) MSSA vs. MRSA: The former beginning to behave like the latter
30 Case 2 3 yo female limp 6 days now won t bear weight on R leg Recent URI Afebrile Hip irritable w/ ROM WBC 18 ESR 15 CRP


31 Case 2 Fluid analysis Cloudy 28,000 cells 68% neut. Gram stain no organism
32 Multivariate analysis Transient synovitis vs. septic arthritis Kocher MS, et al JBJS 81A, independent clinical predictors differentiate septic arthritis & transient synovitis: History of fever >/= 38.5 degrees Celsius Non-weightbearing ESR > 40 mm/hr WBC > 12,000/mm3
33 Multivariate analysis Transient synovitis vs. septic arthritis Kocher MS, et al JBJS 81A, 1999 Score Likelihood of septic arthritis 1 3% 2 40% 3 93% 4 99%
34 Case 1 Fever(+), NWB (+), ESR 48 (+), WBC 10 (-) Fever NWB ESR>40 WBC>12 Probability SA yes yes yes yes 99.8% yes yes yes no 97.3% yes yes no yes 95.2% ye s ye s no no 57.8% yes no yes yes 95.5% ye s no ye s no 62.2% ye s no no ye s 44.8% ye s no no no 5.3% no yes yes yes 93.0% no ye s ye s no 48.0% no ye s no ye s 33.8% no ye s no no 3.4% no no ye s ye s 35.3% no no ye s no 3.7% no no no ye s 2.1% no no no no 1 in 700
35 Case 2 Fever(-), NWB (+), ESR 15(-), WBC 18(+) Fever NWB ESR>40 WBC>12 Probability SA yes yes yes yes 99.8% yes yes yes no 97.3% yes yes no yes 95.2% ye s ye s no no 57.8% yes no yes yes 95.5% ye s no ye s no 62.2% ye s no no ye s 44.8% ye s no no no 5.3% no yes yes yes 93.0% no ye s ye s no 48.0% no ye s no ye s 33.8% no ye s no no 3.4% no no ye s ye s 35.3% no no ye s no 3.7% no no no ye s 2.1% no no no no 1 in 700
36 Septic hip vs. Transient Synovitis Other studies of same criteria: lower predictive value in other populations Luhmann et al. 59% predictive w/ all 4 variables Caird et al. JBJS 2006 Evaluated Kocher criteria + CRP Fever (oral temp > 38.5 ) CRP found to be strong independent risk factor
37 Importance of identifying infection Poor results of delayed diagnosis/treatment of septic hip Osteomyelitis Septic dislocation Avascular necrosis of femoral head Femoral head deformity Long term: leg length discrepancy
38 Importance of identifying infection If neglected Sepsis Death
39 MRI: work up for infection JPO 2014, Gottschalk Improved diagnostic efficiency with MRI as part of work up Decrease rate of reoperation
40 MRI: work up for infection Indications for MRI Negative hip aspiration Location and severity of infection Age of patient Availability of MRI

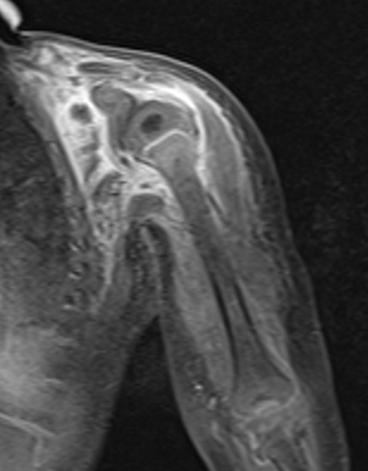
41 12 month old male Won t move arm Case 3 Nursemaid s elbow one week ago Recent fevers, runny nose


42
43 Other imaging?


44 Other imaging?
45 Additional studies Labs WBC 18.3 ESR 60 CRP 8.4 Blood cultures pending


46 Next step?

47 Surgery Arthrotomy & irrigation of shoulder

48 6 months postop
49 Septic arthritis & osteomyelitis Shoulder, hip, ankle, elbow have metaphyseal bone within the joint capsule.
50 Septic arthritis & osteomyelitis 20% of infants with septic arthritis of hip have adjacent osteomyelitis > 50% of neonates may have concomitant osteomyelitis High incidence of concomitant osteo and septic arthritis in adolescents Shoulder most at risk (Montgomery et al. JPO 2013) Related to duration of symptoms


51 Follow up 17 months 12 years Saisu et al. JBJS 2007 Humeral shortening and inferior shoulder subluxation as sequelae of septic shoulder arthritis in neonates and infants.
52 Case 4 20 mo F Developed pain, refusal to bear weight at daycare Parents report temp 101º F Rhinorrhea prior week Otherwise healthy
53 Exam Afebrile, VS WNL Left leg flexed and externally rotated Pain and resistance with any movement of LLE Will allow manipulation of RLE No erythema or warmth on exam

54 Labs: Work up WBC 17 ESR 29 CRP 3.5 Blood cultures pending

55
56 Diagnosis?? fever, refusal to WB WBC 17, ESR 29, CRP 3.5 Septic arthritis vs transient synovitis Admitted overnight Started on NSAIDS MRI ordered for following morning


57
58 Exam after MRI Hospital course Receiving Motrin overnight (no antibiotics) Afebrile Full passive range of motion of left hip without any visible discomfort. Able to bear weight with limp Plan?? Continue to observe.
59 Hospital day 2 Afebrile overnight. Patient with active and passive range of motion of LLE. No erythema or swelling. Infectious Disease, Pediatrics, Orthopedics ok with D/C home.

60 Follow up Return visit to ED one day later: Temp 101º F at home Refusing to bear weight or move LLE Exam in ED PE - Afebrile, VS WNL Irritable with decreased active and passive ROM of LLE. WBC ESR 40 CRP 4.2 US - left hip effusion 2.4 cm x 5 mm Admitted - NPO, OR
61 OR septic arthritis To OR for aspiration and possible arthrotomy Aspiration - frank pus, sent for cultures Frank pus upon arthrotomy Started on Clindamycin q6h
62 Post op course POD1 - afebrile, active ROM LLE Cultures: Kingella Kingae Changed to Ancef with transition to Keflex (3 weeks)

63 Follow up 3 weeks postop ID clinic Doing well, labs normalized Final visit with ortho at 3 months Asymptomatic


64 Kingella Kingae Gram negative aerobe Patients 6-48 months, often in daycare Labs may only show mild elevations Specimen in blood culture bottle increases probability of identifying PCR most sensitive method
65 Case 5 8 year old female CC: L knee pain ( fall during basketball ) PMH Asthma Recurrent UTIs

66 T 39º C Knee exam: Exam No swelling, ecchymosis, erythema TTP proximal tibia Xrays negative for fracture

67 ED Plan Diagnosed with contusion vs sprain Urinalysis performed to work up fever Positive for UTI Discharge home on Bactrim, Ibuprofen Follow-up PCP
68 Follow up Returned to ED 4 days later with persistent knee pain Unable to ambulate, Temp at home 102º F T 37.3 HR 88 RR24 BP 110/60 Urine cultures from prior visit E coli resistant to bactrim Rocephen administered
69 Orthopaedic consult obtained for knee pain Swelling and TTP proximal tibia, no erythema Minimal pain with ROM of knee Unable to weight bear, NVI
70 Work up? Labs WBC 16 ESR 73 CRP 18.2 Blood cultures pending
71 Diagnosis? Musculoskeletal infection vs untreated UTI with knee injury?
72 Plan? Patient admitted to peds team MRI ordered Infectious disease team consulted Positive Blood culture Gram positive cocci in clusters



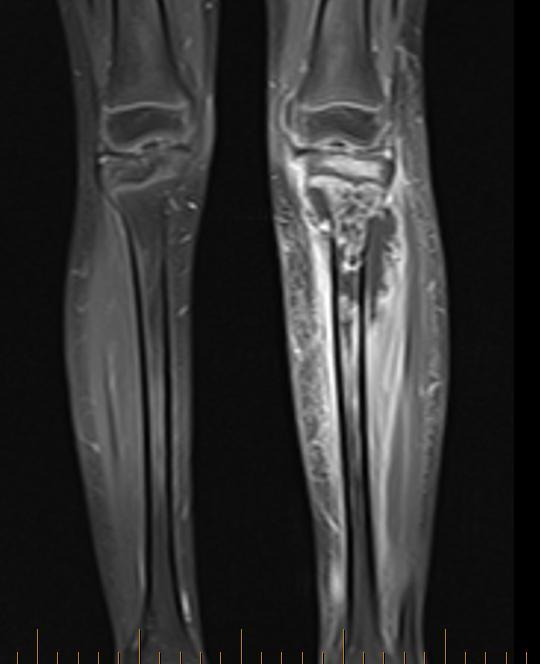
73 MRI
74 Surgical Treatment Irrigation and debridement left proximal tibial subperiosteal abscess Extensive purulent material Cultures
75 Surgical Treatment Procedure repeated 2 days later 2º to severity of infection Persistent post-operative fevers

76 Disposition Discharge home 3 days post initial surgery Culture MSSA Cephalexin for 6 weeks Follow-up with ID and Ortho post-operatively TTWB with crutches


77 2 Months Post-op

78


79
80 Case 5 7 yo presents with inability to weight bear Knee swelling 4-5 days Noted after playing in bounce house Minimal symptoms Now more swelling, over last 24 hours decreased ability to weight bear
81 Exam T 38.6º C Knee + large effusion Minimal tenderness over knee ROM 0º-110º, pain with flexion

82

83 Work up? ESR 44 CRP 2.3 WBC 8 Aspiration 55 ml fluid 24,000 WBC
84 Next step? Admitted Exam after aspiration: Painless knee Full ROM Able to weight bear
85 Differential diagnosis Septic knee Transient synovitis: Not aware this exists outside of the hip ID consulted, discussed History: travel across US,? Tick bite in Colorado

86 Diagnosis Went to OR for repeat aspirate & arthrotomy Fluid slightly cloudy + Lyme PCR Completed course of amoxicillin
87
88 15 yo male Case 6 3 week h/o worsening right thigh/back pain Fell x2 playing volleyball 3 weeks prior Visited PCP twice NSAIDs, Oral Steroid Taper, Flexeril Two episodes of emesis the week Denies fevers, chills, recent illness
89 Exam General: Afebrile, vitals stable In obvious discomfort MSK exam Right hip is flexed, externally rotated Will not allow ROM of RLE Will not bear weight



90 Work up WBC 14.7 ESR 66 CRP 11.8 Blood cultures + Ultrasound moderate right hip effusion with synovial hypertrophy
91 Work up Diagnosis? Additional tests? Right hip aspirate: positive for gram (+) cocci in clusters Admitted to PICU for septicemia
92 Work up Diagnosis? Additional tests?
93 Work up Diagnosis? Additional tests? Right hip aspirate: positive for gram (+) cocci in clusters
94 Work up Diagnosis? Additional tests? Right hip aspirate: positive for gram (+) cocci in clusters Admitted to PICU for septicemia

95 Osteomyelitis & Abscess

96 Osteomyelitis
97 Clinical Course Admitted to PICU for resuscitation Started on clindamycin and ceftriaxone Switched to vancomycin after ID consult Surgery next day with IR and Orthopedics IR percutanous drainage of right thigh abscess Arthrotomy & irrigation right septic hip
98 Clinical Course Stable after surgery Cultures positive for MSSA Treated in hospital with Cefazolin, discharged home on Cephalexin
99 Clinical Course Discharged from ID and Orthopedic clinic after completing 8 week course of Cephalexin 1 month later presented to ED with left lower quadrant pain, nausea, vomiting, fever. WBC 8, CRP 31.7, ESR 54 US showed trace left hip effusion.

100 Osteomyelitis MRI: Pelvic osteomyelitis, deep pelvic abscess
101 Recurrence Left pelvic osteomyelitis with associated abscess. Treatment drainage by IR Cultures grew MSSA Abx 8 weeks of Linezolid. Doing well at last follow-up visit.


102 Follow-up
 Toddlers may have K. kingae (mild presentation) Adolescents can have infections too!")
103 Take-home Messages Consider MSK infection with limb disuse Obtain blood cultures with labs Image early (U/S, MRI) Toddlers may have K. kingae (mild presentation) Adolescents can have infections too! 103
104 Practice Change In addition to local cultures, the learner will obtain a blood culture in any child suspected of having a bone and joint infection 104


105 Thank you! 105
The Limping Child: Differential Diagnosis
 The Limping Child: Differential Diagnosis Kathryn A Keeler, MD Assistant Professor University of Missouri-Kansas City School of Medicine, Department of Orthopaedic Surgery and Department of Pediatrics
The Limping Child: Differential Diagnosis Kathryn A Keeler, MD Assistant Professor University of Missouri-Kansas City School of Medicine, Department of Orthopaedic Surgery and Department of Pediatrics
Osteomyelitis and Septic Joints; Practical Considerations. Coleen K. Cunningham
 Osteomyelitis and Septic Joints; Practical Considerations Coleen K. Cunningham Goals/objectives To improve understanding of the diagnosis, treatment, and follow-up of pediatric bone and joint infections
Osteomyelitis and Septic Joints; Practical Considerations Coleen K. Cunningham Goals/objectives To improve understanding of the diagnosis, treatment, and follow-up of pediatric bone and joint infections
The Child with a Limp
 The Child with a Limp DR S Rajapaksa RCH CHIld with a limp Case: An 11 year old presents to ED with a 4 days history of a painful limp. He had been playing footie over the weekend and had fallen but then
The Child with a Limp DR S Rajapaksa RCH CHIld with a limp Case: An 11 year old presents to ED with a 4 days history of a painful limp. He had been playing footie over the weekend and had fallen but then
Andrea Marmor, MD Associate Clinical Professor, Pediatrics UCSF San Francisco General Hospital
 Andrea Marmor, MD Associate Clinical Professor, Pediatrics UCSF San Francisco General Hospital Carambola is a 16 mo old girl brought to the ED for crying nonstop She has been not herself for about a week,
Andrea Marmor, MD Associate Clinical Professor, Pediatrics UCSF San Francisco General Hospital Carambola is a 16 mo old girl brought to the ED for crying nonstop She has been not herself for about a week,
Osteomyelitis Samir S. Shah, MD, MSCE
 Osteomyelitis Samir S. Shah, MD, MSCE Professor, Department of Pediatrics University of Cincinnati College of Medicine Director, Division of Hospital Medicine Attending Physician in Infectious Diseases
Osteomyelitis Samir S. Shah, MD, MSCE Professor, Department of Pediatrics University of Cincinnati College of Medicine Director, Division of Hospital Medicine Attending Physician in Infectious Diseases
Bone and Joint Infections Case Presentations Pediatric MSK Bootcamp Sept 29, 2019 American Academy of Pediatrics/ Penn State
 Bone and Joint Infections Case Presentations Pediatric MSK Bootcamp Sept 29, 2019 American Academy of Pediatrics/ Penn State Douglas Armstrong MD Darmstrong@hmc.psu.edu Penn State College of Medicine Disclosures
Bone and Joint Infections Case Presentations Pediatric MSK Bootcamp Sept 29, 2019 American Academy of Pediatrics/ Penn State Douglas Armstrong MD Darmstrong@hmc.psu.edu Penn State College of Medicine Disclosures
Assessment of limping child (beware the child who does not weight bear at all):
:") Department of Paediatrics Clinical Guideline Acutely Limping Child and Septic Arthritis Assessment of limping child (beware the child who does not weight bear at all): History Careful history of any significant
Department of Paediatrics Clinical Guideline Acutely Limping Child and Septic Arthritis Assessment of limping child (beware the child who does not weight bear at all): History Careful history of any significant
Pediatric Case Studies. Case 1
 Pediatric Case Studies James Naprawa, MD Assistant Clinical Professor Pediatric Emergency Medicine Children s Hospital, Columbus Case 1 Almost 4 year old AA girl PMH UTI x 2 with abdominal pain and fever
Pediatric Case Studies James Naprawa, MD Assistant Clinical Professor Pediatric Emergency Medicine Children s Hospital, Columbus Case 1 Almost 4 year old AA girl PMH UTI x 2 with abdominal pain and fever
SEPTIC ARTHRITIS. Dr Ahmed Husam Al Ahmed Rheumatologist SYRIA. University of Science and technology Hospital Sanaa Yemen 18/Dec/2014
 SEPTIC ARTHRITIS Dr Ahmed Husam Al Ahmed Rheumatologist SYRIA University of Science and technology Hospital Sanaa Yemen 18/Dec/2014 Objectives be able to define Septic Arthritis know what factors predispose
SEPTIC ARTHRITIS Dr Ahmed Husam Al Ahmed Rheumatologist SYRIA University of Science and technology Hospital Sanaa Yemen 18/Dec/2014 Objectives be able to define Septic Arthritis know what factors predispose
Prof Oluwadiya KS FMCS (Orthop) Consultant Orthopaedic Surgeon / Associate Professor Division of Orthopaedics and Traumatology Department of Surgery
 Consultant Orthopaedic Surgeon / Associate Professor Division of Orthopaedics and Traumatology Department of Surgery") Prof Oluwadiya KS FMCS (Orthop) Consultant Orthopaedic Surgeon / Associate Professor Division of Orthopaedics and Traumatology Department of Surgery College of Health Sciences Ladoke Akintola University
Prof Oluwadiya KS FMCS (Orthop) Consultant Orthopaedic Surgeon / Associate Professor Division of Orthopaedics and Traumatology Department of Surgery College of Health Sciences Ladoke Akintola University
ESPID New Bone and Joint Infection Guidelines
 ESPID New Bone and Joint Infection Guidelines Theoklis Zaoutis, MD, MSCE Professor of Pediatrics and Epidemiology Perelman School of Medicine at the University of Pennsylvania Chief, Division of Infectious
ESPID New Bone and Joint Infection Guidelines Theoklis Zaoutis, MD, MSCE Professor of Pediatrics and Epidemiology Perelman School of Medicine at the University of Pennsylvania Chief, Division of Infectious
Case. 5 year old with 2 weeks leg pain and now refusing to walk + Fevers, lower leg swelling, warmth Denies and history of trauma or wounds
 Case 5 year old with 2 weeks leg pain and now refusing to walk + Fevers, lower leg swelling, warmth Denies and history of trauma or wounds Exam I: Swelling over entire tibia extending to foot P: Tenderness
Case 5 year old with 2 weeks leg pain and now refusing to walk + Fevers, lower leg swelling, warmth Denies and history of trauma or wounds Exam I: Swelling over entire tibia extending to foot P: Tenderness
Management of Acute Haematogenous Osteomyelitis. SAPOS ICL 2017 Anthony Robertson
 Management of Acute Haematogenous Osteomyelitis SAPOS ICL 2017 Anthony Robertson Diagnosis Diagnosis RED FLAGS: Nunn, Rollinson;; SAMJ 2007 Acute hip pain in a child Infant with loss of movement in a limb
Management of Acute Haematogenous Osteomyelitis SAPOS ICL 2017 Anthony Robertson Diagnosis Diagnosis RED FLAGS: Nunn, Rollinson;; SAMJ 2007 Acute hip pain in a child Infant with loss of movement in a limb
The Child With a Limp
 KID WITH A LIMP Common in ED, common in Exams Differential diagnosis is very wide Most causes benign, but mustn't miss Septic arthritis Osteomyelitis Fractures / NAI SUFE (older, heavier children) The
KID WITH A LIMP Common in ED, common in Exams Differential diagnosis is very wide Most causes benign, but mustn't miss Septic arthritis Osteomyelitis Fractures / NAI SUFE (older, heavier children) The
SMF PCP Treatment & Referral Guideline Orthopedics Developed February 1, 2003 Revised: October, 2011
 SUTTER MEDICAL FOUNDATION (SMF) 2800 L Street, 7 th Floor Sacramento, CA 95816 SMF PCP Treatment & Referral Guideline Orthopedics Developed February 1, 2003 Revised: October, 2011 I. Shoulder Pain...Page
SUTTER MEDICAL FOUNDATION (SMF) 2800 L Street, 7 th Floor Sacramento, CA 95816 SMF PCP Treatment & Referral Guideline Orthopedics Developed February 1, 2003 Revised: October, 2011 I. Shoulder Pain...Page
Acute Osteomyelitis: similar to septic arthritis but up to 40% may be afebrile swelling overlying the bone & tenderness
 Osteomyelitis / Bone and Joint Infections Bone infections in children are usually from haematogenous bacterial seeding to a single joint, usually the lower limbs, but may be multifocal. Approximately 10%
Osteomyelitis / Bone and Joint Infections Bone infections in children are usually from haematogenous bacterial seeding to a single joint, usually the lower limbs, but may be multifocal. Approximately 10%
AAP Boot Camp KNEE AND ANKLE EXAM
 AAP Boot Camp KNEE AND ANKLE EXAM Disclosures I have no relevant financial relationships with the manufacturers of any commercial products and or providers of commercial services discussed in this CME
AAP Boot Camp KNEE AND ANKLE EXAM Disclosures I have no relevant financial relationships with the manufacturers of any commercial products and or providers of commercial services discussed in this CME
Osteomieliti STEOMIE
 OsteomielitiSTEOMIE Osteomyelitis is the inflammation of bone caused by pyogenic organisms. Major sources of infection: - haematogenous spread - tracking from adjacent foci of infection - direct inoculation
OsteomielitiSTEOMIE Osteomyelitis is the inflammation of bone caused by pyogenic organisms. Major sources of infection: - haematogenous spread - tracking from adjacent foci of infection - direct inoculation
P-1 (Former P-1) Are pediatric patients on oral or intravenous steroids at an increased risk of developing septic arthritis?
 Are pediatric patients on oral or intravenous steroids at an increased risk of developing septic arthritis?") Pediatrics Prevention P-1 (Former P-1) Are pediatric patients on oral or intravenous steroids at an increased risk of developing septic arthritis? RESEARCHED BY: Muhammad Amin Chinoy MD, Pakistan Literature:
Pediatrics Prevention P-1 (Former P-1) Are pediatric patients on oral or intravenous steroids at an increased risk of developing septic arthritis? RESEARCHED BY: Muhammad Amin Chinoy MD, Pakistan Literature:
Bone and Joint Infections in Diabetics: Diagnosis and Management of Diabetic Foot and Other Common Lower Extremity Infections
 Bone and Joint Infections in Diabetics: Diagnosis and Management of Diabetic Foot and Other Common Lower Extremity Infections Objectives How do you to diagnose, classify and manage DFI? How do you diagnose
Bone and Joint Infections in Diabetics: Diagnosis and Management of Diabetic Foot and Other Common Lower Extremity Infections Objectives How do you to diagnose, classify and manage DFI? How do you diagnose
Research Article Septic Arthritis of the Pediatric Shoulder: From Infancy to Adolescence
 International Pediatrics Volume 2016, Article ID 3086019, 4 pages http://dx.doi.org/10.1155/2016/3086019 Research Article Septic Arthritis of the Pediatric Shoulder: From Infancy to Adolescence Justin
International Pediatrics Volume 2016, Article ID 3086019, 4 pages http://dx.doi.org/10.1155/2016/3086019 Research Article Septic Arthritis of the Pediatric Shoulder: From Infancy to Adolescence Justin
Pediatric Potpourri: What do we now?
 Pediatric Potpourri: What do we now? April 19, 2013 Robert Wittler, MD 1 Disclosure I have no relevant financial relationships with the manufacturer(s) of any commercial products(s) and/or provider of
Pediatric Potpourri: What do we now? April 19, 2013 Robert Wittler, MD 1 Disclosure I have no relevant financial relationships with the manufacturer(s) of any commercial products(s) and/or provider of
I have no financial relationships related to disclose
 Evaluation of a child with a limp / Slipped Capital Femoral Epiphysis (SCFE) Lee S. Segal, MD Chief, Division of Pediatric Orthopedics American Family Children s Hospital Department of Orthopedics and
Evaluation of a child with a limp / Slipped Capital Femoral Epiphysis (SCFE) Lee S. Segal, MD Chief, Division of Pediatric Orthopedics American Family Children s Hospital Department of Orthopedics and
A Patient s Guide to Transient Synovitis of the Hip in Children
 A Patient s Guide to Transient Synovitis of the Hip in Children 651 Old Country Road Plainview, NY 11803 Phone: 5166818822 Fax: 5166813332 p.lettieri@aol.com DISCLAIMER: The information in this booklet
A Patient s Guide to Transient Synovitis of the Hip in Children 651 Old Country Road Plainview, NY 11803 Phone: 5166818822 Fax: 5166813332 p.lettieri@aol.com DISCLAIMER: The information in this booklet
Top 10 Ortho Urgent Care Injuries. J.C. Clark, M.D. ORA Orthopedics
 Top 10 Ortho Urgent Care Injuries J.C. Clark, M.D. ORA Orthopedics 10. Proximal Humerus Fractures Treatment Simple sling ICE, pain meds Button-down shirts Recliner to sleep in It will be up to the surgeon
Top 10 Ortho Urgent Care Injuries J.C. Clark, M.D. ORA Orthopedics 10. Proximal Humerus Fractures Treatment Simple sling ICE, pain meds Button-down shirts Recliner to sleep in It will be up to the surgeon
Musculoskeletal Management of A Limping Child
 Musculoskeletal Management of A Limping Child Julieanne P. Sees, DO, FAOAO Pediatric Neuro-Orthopaedic Surgeon Medical Director, Neuro-Orthopaedic Rehabilitation Unit Wilmington, DE Objectives Identify
Musculoskeletal Management of A Limping Child Julieanne P. Sees, DO, FAOAO Pediatric Neuro-Orthopaedic Surgeon Medical Director, Neuro-Orthopaedic Rehabilitation Unit Wilmington, DE Objectives Identify
Infectious Diseases Society of America Emerging Infections Network. Comments for Query: Osteomyelitis in Children
 Infectious Diseases Society of America Emerging Infections Network Comments for Query: Osteomyelitis in Children Choice of antimicrobial At our institution, we typically start with clindamycin (unless
Infectious Diseases Society of America Emerging Infections Network Comments for Query: Osteomyelitis in Children Choice of antimicrobial At our institution, we typically start with clindamycin (unless
ID Emergencies. BGSMC Internal Medicine Edwin Yu
 ID Emergencies BGSMC Internal Medicine Edwin Yu Learning Objectives Bacterial meningitis IDSA guidelines: Clin Infect Dis 2004; 39:1267-84 HSV encephalitis IDSA guidelines: Clin Infect Dis 2008; 47:303-27
ID Emergencies BGSMC Internal Medicine Edwin Yu Learning Objectives Bacterial meningitis IDSA guidelines: Clin Infect Dis 2004; 39:1267-84 HSV encephalitis IDSA guidelines: Clin Infect Dis 2008; 47:303-27
Case Report Sequential MR Images and Radiographs of Epiphyseal Osteomyelitis in the Distal Femur of an Infant
 Case Reports in Radiology Volume 2013, Article ID 672815, 4 pages http://dx.doi.org/10.1155/2013/672815 Case Report Sequential MR Images and Radiographs of Epiphyseal Osteomyelitis in the Distal Femur
Case Reports in Radiology Volume 2013, Article ID 672815, 4 pages http://dx.doi.org/10.1155/2013/672815 Case Report Sequential MR Images and Radiographs of Epiphyseal Osteomyelitis in the Distal Femur
OBJECTIVE INFECTION OF BONE AND JOINT CONTENT. Case. Case. Make diagnosis and treatment in bone and joint sepsis
 INFECTION OF BONE AND JOINT ธนพจน จ นทร น ม ภาคว ชาออร โธป ด กส โรงพยาบาลรามาธ บด OBJECTIVE Make diagnosis and treatment in bone and joint sepsis Prevent complications i from disease and treatment Use
INFECTION OF BONE AND JOINT ธนพจน จ นทร น ม ภาคว ชาออร โธป ด กส โรงพยาบาลรามาธ บด OBJECTIVE Make diagnosis and treatment in bone and joint sepsis Prevent complications i from disease and treatment Use
Forty-Eighth Annual Teaching Conference Pediatrics for the Practitioner -UT Health Science Center San Antonio School of Medicine June 10-12, 2011
 The 48 th Annual Pediatrics for the Practitioner Symposium June 11, 2011 James H. Brien, DO James H. Brien, DO has no relevant financial relationships with commercial interests to disclose. Case #1 4½-month-old
The 48 th Annual Pediatrics for the Practitioner Symposium June 11, 2011 James H. Brien, DO James H. Brien, DO has no relevant financial relationships with commercial interests to disclose. Case #1 4½-month-old
Good Morning! Welcome Applicants! FRIDAY, N OVEMBER, 7 TH 2014
 Good Morning! Welcome Applicants! FRIDAY, N OVEMBER, 7 TH 2014 Prep Question You are camping with a group of boys at a rural campground in the southeastern Unites States when one of the campers is bitten
Good Morning! Welcome Applicants! FRIDAY, N OVEMBER, 7 TH 2014 Prep Question You are camping with a group of boys at a rural campground in the southeastern Unites States when one of the campers is bitten
THE HIP. Cooler than cool, the pinnacle of what is "it". Beyond all trends and conventional coolness.
 THE HIP Cooler than cool, the pinnacle of what is "it". Beyond all trends and conventional coolness. Objectives Hip anatomy Causes of hip pain Hip exam Anatomy Bones Ilium Anterior Superior Iliac Spine
THE HIP Cooler than cool, the pinnacle of what is "it". Beyond all trends and conventional coolness. Objectives Hip anatomy Causes of hip pain Hip exam Anatomy Bones Ilium Anterior Superior Iliac Spine
OUTLINE FRACTURES OUTLINE. PÆDIATRIC ORTHOPÆDIC CHALLENGES in the EMERGENCY DEPARTMENT. Mohammad Diab M.D. UCSF FRACTURE
 PÆDIATRIC ORTHOPÆDIC CHALLENGES in the EMERGENCY DEPARTMENT FRACTURE Mohammad Diab M.D. UCSF FRACTURE articular displacement < 2 mm. accept FRACTURES routine imaging S-H 3 S-H 4 displacement > 2 mm. ORIF
PÆDIATRIC ORTHOPÆDIC CHALLENGES in the EMERGENCY DEPARTMENT FRACTURE Mohammad Diab M.D. UCSF FRACTURE articular displacement < 2 mm. accept FRACTURES routine imaging S-H 3 S-H 4 displacement > 2 mm. ORIF
A Patient s Guide to Limping in Children
 A Patient s Guide to Limping in Children 651 Old Country Road Plainview, NY 11803 Phone: 5166818822 Fax: 5166813332 p.lettieri@aol.com DISCLAIMER: The information in this booklet is compiled from a variety
A Patient s Guide to Limping in Children 651 Old Country Road Plainview, NY 11803 Phone: 5166818822 Fax: 5166813332 p.lettieri@aol.com DISCLAIMER: The information in this booklet is compiled from a variety
A RARE CASE OF SEPTIC SHOCK SECONDARY TO PRIMARY STERNOCLAVICULAR JOINT SEPTIC ARTHRITIS
 A RARE CASE OF SEPTIC SHOCK SECONDARY TO PRIMARY STERNOCLAVICULAR JOINT SEPTIC ARTHRITIS Dr Ehab F. Girgis & Dr Daniel S.Z.M. Boctor National Health Service, UK TAKE HOME MESSAGES 1. SCJ Septic Arthritis
A RARE CASE OF SEPTIC SHOCK SECONDARY TO PRIMARY STERNOCLAVICULAR JOINT SEPTIC ARTHRITIS Dr Ehab F. Girgis & Dr Daniel S.Z.M. Boctor National Health Service, UK TAKE HOME MESSAGES 1. SCJ Septic Arthritis
BONE AND JOINT INFECTION. Dr.Jónás Zoltán Dept.of Orthopaedics
 BONE AND JOINT INFECTION Dr.Jónás Zoltán Dept.of Orthopaedics www.ortopedia.dote.hu Order of verbal exams: The students are able to register for the exam on the Neptun system. The students pick two titles,
BONE AND JOINT INFECTION Dr.Jónás Zoltán Dept.of Orthopaedics www.ortopedia.dote.hu Order of verbal exams: The students are able to register for the exam on the Neptun system. The students pick two titles,
Sports Medicine in your office: What not to miss!
 Sports Medicine in your office: What not to miss! 2018 Primary Care Approach to Treating the Injured Athlete May 4, 2018 John H. Wilckens, MD Associate Professor, Dept of Orthopaedic Surgery Disclosures
Sports Medicine in your office: What not to miss! 2018 Primary Care Approach to Treating the Injured Athlete May 4, 2018 John H. Wilckens, MD Associate Professor, Dept of Orthopaedic Surgery Disclosures
National Healthcare Safety Network: Central Line-associated Bloodstream Case Studies Teresa C. Horan, MPH
 National Healthcare Safety Network: Central Line-associated Bloodstream Case Studies Teresa C. Horan, MPH National Center for Emerging and Zoonotic Infectious Diseases Division of Healthcare Quality Promotion
National Healthcare Safety Network: Central Line-associated Bloodstream Case Studies Teresa C. Horan, MPH National Center for Emerging and Zoonotic Infectious Diseases Division of Healthcare Quality Promotion
7/1/2012. Repetitive valgus stresses cause microfractures in the apophyseal cartilage (weak link) Common in year olds
 Common in year olds") 1 2 3 4 5 6 7 When growing pains are not growing pains David W. Gray,M.D. Medical Director Orthopedics Differential Diagnosis Fracture Ligament Injury Disloclation Cartilage Injury Apophysitis Inflammation
1 2 3 4 5 6 7 When growing pains are not growing pains David W. Gray,M.D. Medical Director Orthopedics Differential Diagnosis Fracture Ligament Injury Disloclation Cartilage Injury Apophysitis Inflammation
ID Emergencies. BUMC-P Internal Medicine Edwin Yu
 ID Emergencies BUMC-P Internal Medicine Edwin Yu Learning Objectives Bacterial meningitis IDSA guidelines: Clin Infect Dis 2004; 39:1267-84 HSV encephalitis IDSA guidelines: Clin Infect Dis 2008; 47:303-27
ID Emergencies BUMC-P Internal Medicine Edwin Yu Learning Objectives Bacterial meningitis IDSA guidelines: Clin Infect Dis 2004; 39:1267-84 HSV encephalitis IDSA guidelines: Clin Infect Dis 2008; 47:303-27
BONES & JOINTS INFECTION BONE TUMOURS
 BONES & JOINTS INFECTION BONE TUMOURS IMPORTANT SERIOUS CONSEQUENCE PLEASE DON T MISS!! EARLY DIAGNOSIS & PROPER TREATMENT HOW?? AWARE of THEIR EXISTENCE (Knowledge) PREPARE for THEIR OCCURRENCE A HIGH
BONES & JOINTS INFECTION BONE TUMOURS IMPORTANT SERIOUS CONSEQUENCE PLEASE DON T MISS!! EARLY DIAGNOSIS & PROPER TREATMENT HOW?? AWARE of THEIR EXISTENCE (Knowledge) PREPARE for THEIR OCCURRENCE A HIGH
Exam of the Knee and Ankle I HAVE NO FINANCIAL DISCLOSURES RELEVANT TO THIS PRESENTATION
 Exam of the Knee and Ankle I HAVE NO FINANCIAL DISCLOSURES RELEVANT TO THIS PRESENTATION Disclosures I have no relevant financial relationships with the manufacturers of any commercial products and or
Exam of the Knee and Ankle I HAVE NO FINANCIAL DISCLOSURES RELEVANT TO THIS PRESENTATION Disclosures I have no relevant financial relationships with the manufacturers of any commercial products and or
The Hip from Cradle to Grave. Haemish Crawford Ascot Hospital Starship Children s Hospital
 The Hip from Cradle to Grave Haemish Crawford Ascot Hospital Starship Children s Hospital Developmental dysplasia hip DDH Irritable vs. septic hip Perthes disease Slipped Upper Femoral Epiphysis (SUFE)
The Hip from Cradle to Grave Haemish Crawford Ascot Hospital Starship Children s Hospital Developmental dysplasia hip DDH Irritable vs. septic hip Perthes disease Slipped Upper Femoral Epiphysis (SUFE)
Red Stick ID Visual Diagnosis Questions August 22, 2014
 Red Stick ID Visual Diagnosis Questions August 22, 2014 James H. Brien, DO Case #1 The setting is a Pediatric Clinic in San Antonio, Texas on a Saturday in 1989. However, it could have been yesterday in
Red Stick ID Visual Diagnosis Questions August 22, 2014 James H. Brien, DO Case #1 The setting is a Pediatric Clinic in San Antonio, Texas on a Saturday in 1989. However, it could have been yesterday in
1/10/2017 PEDIATRIC LIMP: BOARD REVIEW GOALS & OBJECTIVES RELEVANCE DAVID POHL, D.O. PGY-3 ST. JOHN MACOMB-OAKLAND JANUARY 21, 2017
 PEDIATRIC LIMP: BOARD REVIEW DAVID POHL, D.O. PGY-3 ST. JOHN MACOMB-OAKLAND JANUARY 21, 2017 RELEVANCE AOBFP EXAM BLUEPRINT: ORTHO 5% PEDS 4% ADOLESCENTS 4% SPORTS 3 % http://static3.businessinsider.com/image/52545f89eab8ea62534aa515-1200-375/brain%20golfing.jpg
PEDIATRIC LIMP: BOARD REVIEW DAVID POHL, D.O. PGY-3 ST. JOHN MACOMB-OAKLAND JANUARY 21, 2017 RELEVANCE AOBFP EXAM BLUEPRINT: ORTHO 5% PEDS 4% ADOLESCENTS 4% SPORTS 3 % http://static3.businessinsider.com/image/52545f89eab8ea62534aa515-1200-375/brain%20golfing.jpg
Evaluation of the Knee and Shoulder
 Evaluation of the Knee and Shoulder Karen J. Boselli, MD Northeast Regional Nurse Practitioner Conference May 2018 Knee Overview History Examination Top 5 diagnoses When to image When to refer Pain most
Evaluation of the Knee and Shoulder Karen J. Boselli, MD Northeast Regional Nurse Practitioner Conference May 2018 Knee Overview History Examination Top 5 diagnoses When to image When to refer Pain most
TOTAL SHOULDER REPLACEMENT The following is designed to present an overview of shoulder replacement surgery options
 SHOULDER SERVICE TOTAL SHOULDER REPLACEMENT The following is designed to present an overview of shoulder replacement surgery options SHOULDER PAIN Chronic shoulder pain can limit your activities, keep
SHOULDER SERVICE TOTAL SHOULDER REPLACEMENT The following is designed to present an overview of shoulder replacement surgery options SHOULDER PAIN Chronic shoulder pain can limit your activities, keep
Case Presentation. The Failure to Diagnose Sepsis. chills. pain out of proportion to mechanism. low-grade fever. tachycardia that does not make sense
 Case Presentation The Failure to Diagnose Sepsis Sepsis is a regular visitor in the news as cases of flesh-eating bacteria and the dramatic speed with which victims deteriorate hit the headlines. The failure
Case Presentation The Failure to Diagnose Sepsis Sepsis is a regular visitor in the news as cases of flesh-eating bacteria and the dramatic speed with which victims deteriorate hit the headlines. The failure
Case Report Arthroscopic Treatment of Septic Arthritis of the Elbow in a 4-Year-Old Girl
 Case Reports in Orthopedics Volume 2015, Article ID 853974, 4 pages http://dx.doi.org/10.1155/2015/853974 Case Report Arthroscopic Treatment of Septic Arthritis of the Elbow in a 4-Year-Old Girl Masashi
Case Reports in Orthopedics Volume 2015, Article ID 853974, 4 pages http://dx.doi.org/10.1155/2015/853974 Case Report Arthroscopic Treatment of Septic Arthritis of the Elbow in a 4-Year-Old Girl Masashi
Septic Arthritis and Concern for Osteomyelitis in a Child with Rat Bite Fever. Dustin D Flannery DO
 JCM Accepts, published online ahead of print on 3 April 2013 J. Clin. Microbiol. doi:10.1128/jcm.03139-12 Copyright 2013, American Society for Microbiology. All Rights Reserved. 1 1 Septic Arthritis and
JCM Accepts, published online ahead of print on 3 April 2013 J. Clin. Microbiol. doi:10.1128/jcm.03139-12 Copyright 2013, American Society for Microbiology. All Rights Reserved. 1 1 Septic Arthritis and
OSTEOMYELITIS AND SEPTIC ARTHRITIS IN CHILDREN: REVIEW
 OSTEOMYELITIS AND SEPTIC ARTHRITIS IN CHILDREN: REVIEW Dr. Roshan Sah* and Prof. Lui Ke bin Department of Orthopaedics, The First Affiliated Peoples Hospital of Yangtze University, Jingzhou, Hubei, PR.
OSTEOMYELITIS AND SEPTIC ARTHRITIS IN CHILDREN: REVIEW Dr. Roshan Sah* and Prof. Lui Ke bin Department of Orthopaedics, The First Affiliated Peoples Hospital of Yangtze University, Jingzhou, Hubei, PR.
Limping Kids. SJRHEM Rounds - Dr David Lewis
 Limping Kids SJRHEM Rounds - Dr David Lewis October 11th 2014 Limping Kids A Case Base Rounds Interactive Links to further reading Posted to the website www.sjrhem.ca Case 1 - Age of Child An 18 month
Limping Kids SJRHEM Rounds - Dr David Lewis October 11th 2014 Limping Kids A Case Base Rounds Interactive Links to further reading Posted to the website www.sjrhem.ca Case 1 - Age of Child An 18 month
MRI Non-Joint Extremity Questionnaire
 MRI n-joint Extremity Questionnaire INSTRUCTIONS FOR COMPLETING QUESTIONNAIRE: Answer all of the initial questions (Pages 1 and 2) Select the reason for imaging by answering question #6. Based on your
MRI n-joint Extremity Questionnaire INSTRUCTIONS FOR COMPLETING QUESTIONNAIRE: Answer all of the initial questions (Pages 1 and 2) Select the reason for imaging by answering question #6. Based on your
Joint Trust Guidelines for the Limping Child with No History of Trauma
 A Clinical Guideline For Use in: Children s Assessment Unit By: Medical and Nursing staff Children (0-16) presenting with a limp or acute For: lower limb pain but with no history of trauma Division responsible
A Clinical Guideline For Use in: Children s Assessment Unit By: Medical and Nursing staff Children (0-16) presenting with a limp or acute For: lower limb pain but with no history of trauma Division responsible
A free online interactive information resource for clinicians.
 A free online interactive information resource for clinicians www.pmmonline.org The limping child Helen Foster Professor of Paediatric Rheumatology Newcastle University Honorary Consultant Great North
A free online interactive information resource for clinicians www.pmmonline.org The limping child Helen Foster Professor of Paediatric Rheumatology Newcastle University Honorary Consultant Great North
Non-inflammatory joint pain
 Non-inflammatory joint pain Lawrence Owino Okong o, Mmed (UoN); Mphil. (UCT). Lecturer, Department of Paediatrics and Child Health, University of Nairobi. Paediatrician/ Rheumatologist. INTRODUCTION Musculoskeletal
Non-inflammatory joint pain Lawrence Owino Okong o, Mmed (UoN); Mphil. (UCT). Lecturer, Department of Paediatrics and Child Health, University of Nairobi. Paediatrician/ Rheumatologist. INTRODUCTION Musculoskeletal
The use of CRP within a clinical prediction algorithm for the differentiation of septic arthritis and transient synovitis in children
 CHILDREN S ORTHOPAEDICS The use of CRP within a clinical prediction algorithm for the differentiation of septic arthritis and transient synovitis in children R. Singhal, D. C. Perry, F. N. Khan, D. Cohen,
CHILDREN S ORTHOPAEDICS The use of CRP within a clinical prediction algorithm for the differentiation of septic arthritis and transient synovitis in children R. Singhal, D. C. Perry, F. N. Khan, D. Cohen,
Diagnosis and Management of Shoulder PJI
 Diagnosis and Management of Shoulder PJI Surena Namdari MD, MSc Associate Professor of Orthopaedic Surgery The Rothman Institute Thomas Jefferson University Health System Philadelphia, PA Disclosures Research
Diagnosis and Management of Shoulder PJI Surena Namdari MD, MSc Associate Professor of Orthopaedic Surgery The Rothman Institute Thomas Jefferson University Health System Philadelphia, PA Disclosures Research
Tibial Nonunions: Should I Tackle and How
 Tibial Nonunions: Should I Tackle and How Frank R. Avilucea, MD Assistant Professor Department of Orthopaedic Surgery University of Cincinnati Medical Center Disclosures Journal Reviewer Journal of Bone
Tibial Nonunions: Should I Tackle and How Frank R. Avilucea, MD Assistant Professor Department of Orthopaedic Surgery University of Cincinnati Medical Center Disclosures Journal Reviewer Journal of Bone
BONE & JOINT INFECTIONS
 BONE & JOINT INFECTIONS Henry F. Chambers, MD Disclosures AstraZeneca advisory board Cubist research grant, advisory panel Genentech advisory board Merck stock Pfizer advisory board Theravance advisory
BONE & JOINT INFECTIONS Henry F. Chambers, MD Disclosures AstraZeneca advisory board Cubist research grant, advisory panel Genentech advisory board Merck stock Pfizer advisory board Theravance advisory
Knee Case Studies. You might KNEED to know some of this stuff
 Knee Case Studies You might KNEED to know some of this stuff Mark Mildren, MD Specializing in Adult Reconstruction Slocum Center for Orthopedics & Sports Medicine 25 th Annual Orthopedic & Sports Medicine
Knee Case Studies You might KNEED to know some of this stuff Mark Mildren, MD Specializing in Adult Reconstruction Slocum Center for Orthopedics & Sports Medicine 25 th Annual Orthopedic & Sports Medicine
 Fever Phobia and the ED Doc Ran Goldman, MD (rgoldman@cw.bc.ca) BC Children s Hospital, Professor, University of British Columbia SLIDES ON : www.clinicalpeds.com/whistler Define Fever 38.0 o Doesn t
Fever Phobia and the ED Doc Ran Goldman, MD (rgoldman@cw.bc.ca) BC Children s Hospital, Professor, University of British Columbia SLIDES ON : www.clinicalpeds.com/whistler Define Fever 38.0 o Doesn t
6/23/2017. What do you see? skull fracture
 What do you see? skull fracture 1 Head CT On soft tissue windows, posterior soft tissues swelling and hemorrhage, no definite evidence of fracture Head CT On bone windows, fracture now seen subjacent to
What do you see? skull fracture 1 Head CT On soft tissue windows, posterior soft tissues swelling and hemorrhage, no definite evidence of fracture Head CT On bone windows, fracture now seen subjacent to
Evaluation of the Hip and Knee
 Evaluation of the Hip and Knee Causes of hip pain RA Osteoarthritis Psoriatic arthritis Septic arthritis Bursitis Hip fx Labral tear Tendinitis Referred back pain Cancer AVN Legg-Calve-Perthes Paget's
Evaluation of the Hip and Knee Causes of hip pain RA Osteoarthritis Psoriatic arthritis Septic arthritis Bursitis Hip fx Labral tear Tendinitis Referred back pain Cancer AVN Legg-Calve-Perthes Paget's
Advanced Management of Patients with Tuberculosis Little Rock, Arkansas August 13 14, 2014
 Advanced Management of Patients with Tuberculosis Little Rock, Arkansas August 13 14, 2014 TB Case Presentation Andrea Cruz, MD, MPH August 14, 2014 Andrea Cruz, MD, MPH has the following disclosures to
Advanced Management of Patients with Tuberculosis Little Rock, Arkansas August 13 14, 2014 TB Case Presentation Andrea Cruz, MD, MPH August 14, 2014 Andrea Cruz, MD, MPH has the following disclosures to
Infection. Arthrocentesis: Cell count Differential Culture. Infection and associated microorganism(s) confirmed
 confirmed") Painful joint History and examination Radiograph of affected joint Erythrocyte sedimentation rate C-reactive protein Infection No infection suspected Arthrocentesis: Cell count Differential Culture Stop
Painful joint History and examination Radiograph of affected joint Erythrocyte sedimentation rate C-reactive protein Infection No infection suspected Arthrocentesis: Cell count Differential Culture Stop
Yi-Wei Tang, MD, PhD, F(AAM), FIDSA Professor of Pathology and Medicine Director, Molecular Infectious Diseases Laboratory
, FIDSA Professor of Pathology and Medicine Director, Molecular Infectious Diseases Laboratory") Yi-Wei Tang, MD, PhD, F(AAM), FIDSA Professor of Pathology and Medicine Director, Molecular Infectious Diseases Laboratory Start with a case presentation Background and techniques PCR mass spectrometry
Yi-Wei Tang, MD, PhD, F(AAM), FIDSA Professor of Pathology and Medicine Director, Molecular Infectious Diseases Laboratory Start with a case presentation Background and techniques PCR mass spectrometry
Case Report Haematogenous Spread of Staphylococcus aureus from an Iliacus Abscess to an ACL Reconstructed Knee
 Case Reports in Orthopedics Volume 2013, Article ID 914329, 4 pages http://dx.doi.org/10.1155/2013/914329 Case Report Haematogenous Spread of Staphylococcus aureus from an Iliacus Abscess to an ACL Reconstructed
Case Reports in Orthopedics Volume 2013, Article ID 914329, 4 pages http://dx.doi.org/10.1155/2013/914329 Case Report Haematogenous Spread of Staphylococcus aureus from an Iliacus Abscess to an ACL Reconstructed
Osteomyelitis in infancy and childhood: A clinical and diagnostic overview M. Mearadji
 Osteomyelitis in infancy and childhood: A clinical and diagnostic overview M. Mearadji International Foundation for Pediatric Imaging Aid Introduction Osteomyelitis is a relative common disease in infancy
Osteomyelitis in infancy and childhood: A clinical and diagnostic overview M. Mearadji International Foundation for Pediatric Imaging Aid Introduction Osteomyelitis is a relative common disease in infancy
Musculoskeletal Concerns in the Pediatric Athlete. John Hatzenbuehler, MD FACSM ACSM TPC Course 2015
 Musculoskeletal Concerns in the Pediatric Athlete John Hatzenbuehler, MD FACSM ACSM TPC Course 2015 Dislclosures Neither I, John Hatzenbuehler nor any family member(s), have any relevant financial relationships
Musculoskeletal Concerns in the Pediatric Athlete John Hatzenbuehler, MD FACSM ACSM TPC Course 2015 Dislclosures Neither I, John Hatzenbuehler nor any family member(s), have any relevant financial relationships
Right Iliac Fossa Pain
 Princess Margaret Hospital for Children PAEDIATRIC ACUTE CARE GUIDELINE Right Iliac Fossa Pain Scope (Staff): Scope (Area): All Emergency Department Clinicians Emergency Department This document should
Princess Margaret Hospital for Children PAEDIATRIC ACUTE CARE GUIDELINE Right Iliac Fossa Pain Scope (Staff): Scope (Area): All Emergency Department Clinicians Emergency Department This document should
DDH. Abnormal hip development Traditionally CDH (congenital dysplasia of the hip) Today DDH(developmental dysplasia of the hip)
 Today DDH(developmental dysplasia of the hip)") DDH Update on Screening Kathryn A Keeler, MD Assistant Professor University of Missouri-Kansas City School of Medicine, Department of Orthopaedic Surgery and Department of Pediatrics Children s Mercy Kansas
DDH Update on Screening Kathryn A Keeler, MD Assistant Professor University of Missouri-Kansas City School of Medicine, Department of Orthopaedic Surgery and Department of Pediatrics Children s Mercy Kansas
SKIN AND SOFT TISSUE INFECTIONS
 SKIN AND SOFT TISSUE INFECTIONS ZAIN CHAGLA SEA COURSES - PATAGONIA COPYRIGHT 2017 BY SEA COURSES INC. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in
SKIN AND SOFT TISSUE INFECTIONS ZAIN CHAGLA SEA COURSES - PATAGONIA COPYRIGHT 2017 BY SEA COURSES INC. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in
Objectives. Define classes of uncomplicated skin and soft tissue infection (SSTI) that drive empiric antimicrobial selection
 that drive empiric antimicrobial selection") Objectives Define classes of uncomplicated skin and soft tissue infection (SSTI) that drive empiric antimicrobial selection Purulent SSTI Non-purulent SSTI Recognize conditions that suggest complications
Objectives Define classes of uncomplicated skin and soft tissue infection (SSTI) that drive empiric antimicrobial selection Purulent SSTI Non-purulent SSTI Recognize conditions that suggest complications
TUBERCULOSIS OF HIP AND KNEE JOINT
 TUBERCULOSIS OF HIP AND KNEE JOINT TUBERCULOSIS OF HIP JOINT Occurrence-15% of all osteo articular tuber culosis Next common after spinal TB AETIO PATHOGENESIS Most common cause Mycobacterium tuberculosis
TUBERCULOSIS OF HIP AND KNEE JOINT TUBERCULOSIS OF HIP JOINT Occurrence-15% of all osteo articular tuber culosis Next common after spinal TB AETIO PATHOGENESIS Most common cause Mycobacterium tuberculosis
Case Report Pseudoseptic Arthritis: A Case Series and Review of the Literature
 Case Reports in Infectious Diseases Volume 2011, Article ID 942023, 4 pages doi:10.1155/2011/942023 Case Report Pseudoseptic Arthritis: A Case Series and Review of the Literature Brian P. Oppermann, 1
Case Reports in Infectious Diseases Volume 2011, Article ID 942023, 4 pages doi:10.1155/2011/942023 Case Report Pseudoseptic Arthritis: A Case Series and Review of the Literature Brian P. Oppermann, 1
Goals &Objectives. 1. Review the anatomy of the knee 2. Practice your hands-on skills 3. By the end of the workshop:
 Clinical Knee Exam Goals &Objectives 1. Review the anatomy of the knee 2. Practice your hands-on skills 3. By the end of the workshop: Be able to categorize knee injuries Understand the significance of
Clinical Knee Exam Goals &Objectives 1. Review the anatomy of the knee 2. Practice your hands-on skills 3. By the end of the workshop: Be able to categorize knee injuries Understand the significance of
9/22/2017. I am a local. Born at Desert Samaritan
 I am a local Born at Desert Samaritan 1 MOUNTAIN VIEW HIGH SCHOOL ASU U OF IOWA MED SCHOOL PHOENIX FOR RESIDENCY 2 Discuss the 5 most controversial topics in foot and ankle Injuries that are routinely
I am a local Born at Desert Samaritan 1 MOUNTAIN VIEW HIGH SCHOOL ASU U OF IOWA MED SCHOOL PHOENIX FOR RESIDENCY 2 Discuss the 5 most controversial topics in foot and ankle Injuries that are routinely
Clinical Pearls Infectious Diseases. Pritish K. Tosh, MD MN ACP Nov 7, [Answers and discussion slides will be posted after the meeting]
![Clinical Pearls Infectious Diseases. Pritish K. Tosh, MD MN ACP Nov 7, [Answers and discussion slides will be posted after the meeting]](/thumbs/83/87318178.jpg "Clinical Pearls Infectious Diseases. Pritish K. Tosh, MD MN ACP Nov 7, [Answers and discussion slides will be posted after the meeting]") Clinical Pearls Infectious Diseases Pritish K. Tosh, MD MN ACP Nov 7, 2014 [Answers and discussion slides will be posted after the meeting] Case 1 A 33-year-old male with diffuse large B-cell lymphoma
Clinical Pearls Infectious Diseases Pritish K. Tosh, MD MN ACP Nov 7, 2014 [Answers and discussion slides will be posted after the meeting] Case 1 A 33-year-old male with diffuse large B-cell lymphoma
Periprosthetic Infection
 Periprosthetic Infection Donald W Hohman MD Greater Dallas Orthopaedics Dallas, TX Presented by Jay Pond, M.D. Common Scenarios Acute Infection (Less than 2 weeks of symptoms) Well Fixed Components 2 Stage
Periprosthetic Infection Donald W Hohman MD Greater Dallas Orthopaedics Dallas, TX Presented by Jay Pond, M.D. Common Scenarios Acute Infection (Less than 2 weeks of symptoms) Well Fixed Components 2 Stage
Differential Diagnosis
 Case 31yo M who sustained an injury to L knee while playing Basketball approximately 2 weeks ago. He describes pivoting and hyperextending his knee, which swelled over the next few days. He now presents
Case 31yo M who sustained an injury to L knee while playing Basketball approximately 2 weeks ago. He describes pivoting and hyperextending his knee, which swelled over the next few days. He now presents
Hip Preservation Timothy J Sauber MD Orthopaedic Update March 22, 2015 Nemacolin Woodlands Resort
 Hip Preservation Timothy J Sauber MD Orthopaedic Update March 22, 2015 Nemacolin Woodlands Resort Disclosures No disclosures relevant to this topic Objectives Evaluate and recognize common hip pathology
Hip Preservation Timothy J Sauber MD Orthopaedic Update March 22, 2015 Nemacolin Woodlands Resort Disclosures No disclosures relevant to this topic Objectives Evaluate and recognize common hip pathology
Evaluation and Management of Knee Pain. Michael Cassat, MD University of Arkansas for Medical Sciences
 Evaluation and Management of Knee Pain Michael Cassat, MD University of Arkansas for Medical Sciences Disclosure I have no actual or potential conflict of interest in relation to this program/presentation.
Evaluation and Management of Knee Pain Michael Cassat, MD University of Arkansas for Medical Sciences Disclosure I have no actual or potential conflict of interest in relation to this program/presentation.
An understanding of the components of the normal gait cycle will aid in describing abnormalities of gait.
 Approach to the Child with a Limp: Student writer: Brian Mayson Resident editor: Elmine Statham Background The child with a limp is a common problem seen in pediatrics. A limp is defined as any deviation
Approach to the Child with a Limp: Student writer: Brian Mayson Resident editor: Elmine Statham Background The child with a limp is a common problem seen in pediatrics. A limp is defined as any deviation
Objectives. The ability to demonstrate knowledge of the following:
 Objectives The ability to demonstrate knowledge of the following: Bone and joints infections presentation Assessment and work up for bone and joint infections Differential diagnosis for bone and joint
Objectives The ability to demonstrate knowledge of the following: Bone and joints infections presentation Assessment and work up for bone and joint infections Differential diagnosis for bone and joint
Nursing Management: Musculoskeletal Trauma and Orthopedic Surgery. By: Aun Lauriz E. Macuja SAC_SN4
 Nursing Management: Musculoskeletal Trauma and Orthopedic Surgery By: Aun Lauriz E. Macuja SAC_SN4 The most common cause of musculoskeletal injuries is a traumatic event resulting in fracture, dislocation,
Nursing Management: Musculoskeletal Trauma and Orthopedic Surgery By: Aun Lauriz E. Macuja SAC_SN4 The most common cause of musculoskeletal injuries is a traumatic event resulting in fracture, dislocation,
Pediatric Injuries/Fractures. Rena Heathcote
 Pediatric Injuries/Fractures Rena Heathcote INTRODUCTION Incidence Anatomy of the Growing Bone Injury Patterns What can we X-ray PEDIATRIC FRACTURES INCIDENCE What makes children susceptible to fractures?
Pediatric Injuries/Fractures Rena Heathcote INTRODUCTION Incidence Anatomy of the Growing Bone Injury Patterns What can we X-ray PEDIATRIC FRACTURES INCIDENCE What makes children susceptible to fractures?
The McMaster at night Pediatric Curriculum
 The McMaster at night Pediatric Curriculum Robinson, J, et al. and the Canadian Pediatric Society. Urinary tract infection in infants and children: Diagnosis and management. Pediatr Child Health 2014;
The McMaster at night Pediatric Curriculum Robinson, J, et al. and the Canadian Pediatric Society. Urinary tract infection in infants and children: Diagnosis and management. Pediatr Child Health 2014;
Practice Changes I Hope You Make
 Is that Bad? What PCPs (& Parents) Need to Know about Fractures Aharon Z. Gladstein, MD Pediatric Orthopaedics & Sports Medicine Texas Children s Hospital Assistant Professor, Orthopaedics Baylor College
Is that Bad? What PCPs (& Parents) Need to Know about Fractures Aharon Z. Gladstein, MD Pediatric Orthopaedics & Sports Medicine Texas Children s Hospital Assistant Professor, Orthopaedics Baylor College
Nuclear medicine and Prosthetic Joint Infections
 Nuclear medicine and Prosthetic Joint Infections Christophe Van de Wiele, M.D., Ph.D. Department of Nuclear Medicine, University Hospital Ghent, Belgium Orthopedic prostheses: world market 1996 Prosthetic
Nuclear medicine and Prosthetic Joint Infections Christophe Van de Wiele, M.D., Ph.D. Department of Nuclear Medicine, University Hospital Ghent, Belgium Orthopedic prostheses: world market 1996 Prosthetic
The Painful Hip. Jennifer R Marks, MD
 The Painful Hip Jennifer R Marks, MD The Painful Hip A 64 yo F presents to clinic complaining of a sore hip What further questions do you have for this patient? What is on your differential diagnosis?
The Painful Hip Jennifer R Marks, MD The Painful Hip A 64 yo F presents to clinic complaining of a sore hip What further questions do you have for this patient? What is on your differential diagnosis?
Lower Extremity Sports Injuries
 Lower Extremity Sports Injuries AAP Musculoskeletal Boot Camp Sigrid F. Wolf, MD Pediatric Sports Medicine Fellow Northwestern University Lurie Children s Hospital Disclosure I have no relevant financial
Lower Extremity Sports Injuries AAP Musculoskeletal Boot Camp Sigrid F. Wolf, MD Pediatric Sports Medicine Fellow Northwestern University Lurie Children s Hospital Disclosure I have no relevant financial
Orthopedics. 1. GOAL: Understand the pediatrician's role in preventing and screening for
 The University of Arizona Pediatric Residency Program Primary Goals for Rotation Orthopedics 1. GOAL: Understand the pediatrician's role in preventing and screening for orthopedic injury, disease and dysfunction.
The University of Arizona Pediatric Residency Program Primary Goals for Rotation Orthopedics 1. GOAL: Understand the pediatrician's role in preventing and screening for orthopedic injury, disease and dysfunction.
The Limping Child. Todd Milbrandt, MD Division Chair Pediatric Orthopaedics Mayo Clinic Rochester
 The Limping Child Todd Milbrandt, MD Division Chair Pediatric Orthopaedics Mayo Clinic Rochester Faculty Disclosure No disclosures relevant to this talk Practice Gap Primary Care Providers are faced with
The Limping Child Todd Milbrandt, MD Division Chair Pediatric Orthopaedics Mayo Clinic Rochester Faculty Disclosure No disclosures relevant to this talk Practice Gap Primary Care Providers are faced with
Goals. Initial management skeletal trauma. Physical Exam ABC OF PRIMARY CARE MEDICINE FRACTURE MANAGEMENT 12/4/2010
 ABC OF PRIMARY CARE MEDICINE FRACTURE MANAGEMENT Brian Feeley, MD UCSF Sports Medicine and Shoulder Surgery Goals Discuss common fractures and initial management, treatment guidelines Let your patients
ABC OF PRIMARY CARE MEDICINE FRACTURE MANAGEMENT Brian Feeley, MD UCSF Sports Medicine and Shoulder Surgery Goals Discuss common fractures and initial management, treatment guidelines Let your patients
APPROACH TO PATIENTS WITH POLYARTHRALGIA
 APPROACH TO PATIENTS WITH POLYARTHRALGIA Scott Vogelgesang, MD Division of Immunology University of Iowa No conflicts of interest DEFINITIONS Arthralgia joint pain with no evidence of inflammation Arthritis
APPROACH TO PATIENTS WITH POLYARTHRALGIA Scott Vogelgesang, MD Division of Immunology University of Iowa No conflicts of interest DEFINITIONS Arthralgia joint pain with no evidence of inflammation Arthritis
Types of bone/joint infections. Bone and Joint Infections. Septic Arthritis. Pathogenesis. Pathogenesis. Bacterial arthritis: predisposing factors
 Bone and Joint Infections Types of bone/joint infections Arthritis (infective/septic) Osteomyelitis Prosthetic bone and joint infections Septic Arthritis Common destructive athroplasty Mono-articular Poly-articular
Bone and Joint Infections Types of bone/joint infections Arthritis (infective/septic) Osteomyelitis Prosthetic bone and joint infections Septic Arthritis Common destructive athroplasty Mono-articular Poly-articular