Musculoskeletal Management of A Limping Child
|
|
|
- Byron Goodman
- 5 years ago
- Views:
Transcription



1 Musculoskeletal Management of A Limping Child Julieanne P. Sees, DO, FAOAO Pediatric Neuro-Orthopaedic Surgeon Medical Director, Neuro-Orthopaedic Rehabilitation Unit Wilmington, DE

2 Objectives Identify common disorders: Age is helpful What to order Labs: CBC, ESR, CRP X-rays, Bone scan, CT, MRI When to refer Let s Start What to do for the child with a Limp?
3 No Disclosures



4 Introduction Important approach systematic and orderly manner Thorough H&P Inspect joints: swelling, effusion, erythema, warmth muscle atrophy, deformity, symmetry Note range of motion & pain Observe gait
5 Limping in Various Age Groups Toddler (1-3 years) Child (4-10 years) Adolescent (11+ years) Transient synovitis Transient synovitis Slipped capital femoral epiphysis Septic arthritis Septic arthritis Hip dysplasia Diskitis Legg-Calve- Perthes Chondrolysis Toddler s fracture Discoid meniscus Overuse syndromes Cerebral Palsy Limb length discrepancy Osteochondritis dissecans Muscle dystrophy Developmental Dysplasia Juvenile arthritis RARE: Leukemia Osteoid osteoma
6 Infant and Toddler Occult fx Septic Arthritis Osteomyelitis Toxic Synovitis Leukemia Child Abuse Cerebral Palsy Muscular dystrophy DDH Coxa vara Pauciarticular JA Diskitis
7 School-Aged Children Fracture Septic arthritis / Osteomyelitis Toxic synovitis Leukemia LLD Legg-Calve-Perthes disease Tumor: Ewing s sarcoma
8 Adolescent Fracture Sprain, strain, overuse syndromes Hip dysplasia Osteochondritis disecans Gonococcal arthritis Slipped Capital Femoral Epiphysis (SCFE) Tumor: Osteosarcoma
9 Abnormal Gait Patterns Antalgic gait Trendelenburg gait Proximal muscle weakness gait Spastic gait Short-limb gait
10 Antalgic Gait Caused by pain in LE or back (most common) Child takes quick, soft steps on the leg ( short-stepping ) Reduces time of extremity in stance phase Normal limb longer in stance phase If source is hip = lean toward affected side decreasing abductor force across the hip
11 Trendelenburg Gait Functionally weak hip abductors During stance: hip abductors function ineffectively pelvis tilts away from affected side Child compensates leaning over affected hip
12 Proximal Muscle Weakness Gait Lack of hip extensor strength causes increased lordosis of the lumbar spine in order to remain upright Gower s sign Usually seen in muscular dystrophy
13 Short-limb Gait Gait asymmetry: LLD > 3.7 to 5.5 cm Toe-walking: keeps pelvis level idiopathic neurologic Hip and knee flexion of longer extremity in stance

14 Inflammatory and Infectious Disorders Transient (Toxic) Synovitis Septic Arthritis Osteomyelitis Diskitis Pauciarticular Juvenile Arthritis
 Often hx of antecedent viral illness Rare fever, normal WBC, CRP, ESR <30 U/S shows")
15 Transient (Toxic) Synovitis Most common cause of LE pain Inflammation of synovial membrane Age: 18 months 10 years Rapid onset of hip pain, limited joint ROM, limping (or inability to walk) Often hx of antecedent viral illness Rare fever, normal WBC, CRP, ESR <30 U/S shows effusion


16 Transient (Toxic) Synovitis Aspiration may be necessary to r/o septic arthritis WBC 5,000-15,000, > 25% polys Tx: Brief period non weightbearing NSAIDs Most resolve within 2 weeks Recurrence 4-17% within 6 months
 Acute onset of joint")

17 Septic Arthritis Microbial invasion of joint spaces Hematogenous spread Urgent medical management (differentiate from transient synovitis) Acute onset of joint pain limp or refusal to walk hx of mild trauma or concurrent infx/illness Progresses to febrile systemic illness Age < 10 years Approx. 90% lower extremity Monoarticular

 Blood Cx positive in 50% X-ray changes 7-10 days Definitive DX: synovial fluid Staph")
18 Septic Arthritis Physical exam Holds affected extremity immobile Joint swelling, erythema, warmth, tenderness to palpation Pain with passive ROM WBC, ESR elevated (Kocher. JBJS 2004) CRP > 2mg/dL (Jung. JPO 2003) Blood Cx positive in 50% X-ray changes 7-10 days Definitive DX: synovial fluid Staph Aureus most common R/O group B strep in toddler CALL Ortho: Treatment is Surgical I&D

 Rx:")
19 Osteomyelitis Antalgic gait Toddlers and children localized swelling, pain, pseudoparalysis, fever/toxic Adolescents may be more indolent Xrays and MRI are helpful Hematogenous spread S. aureus most common (also GBS, Diplococcus pneumoniae) Rx: antibiotics +/- surgery I&D
 Not appear ill, ESR")

20 Diskitis (Infectious Spondylitis) Back pain interferes with normal walking / bending forward (refuses to pick up object from floor) Not appear ill, ESR elevated in 80% S. aureus most common With time: XRs show narrow disk space & bone irregularity Bone scan may help localize Rx: systemic abx, +/- bracing

21 Pauciarticular Juvenile Arthritis Most common type of juvenile arthritis Mild limp in children 2 y of age Girls:boys 4:1 Lab values normal, 50% with normal ANA Most commonly involved joints Subtalar, ankle, knee with limited ROM Refer to rheumatologist
")
22 Neurologic Disorders Cerebral Palsy Muscular Dystrophy Consider if child has always had an abnormal gait Delayed start to ambulation (>18 months)

23 Cerebral Palsy Spastic gait Diagnostic challenge in mild CP Hx: premature, develop delays Limited ROM in ankle/knee Hyperreflexia, clonus Refer to orthopaedist
24 Muscular Dystrophy Proximal muscle weakness gait Usually first noted in boys 2-5 y Hx: delayed ambulation, frequent stumbles, falls, difficult climbing stairs Gower s sign, toe-walking +/- pseudohypertrophy of calf Elevated serum CPK Refer to neurology

25 Anatomic Disorders Developmental Dysplasia of Hip (DDH) Legg-Calve-Perthes Disease Slipped Capital Femoral Epiphysis (SCFE) Toddler s Fx Growth plate fracture Overuse syndromes Limb length discrepancy Femoral Torsion Tibial Torsion Foot deformities: clubfoot
26 DDH Painless limp in toddler (trendelenburg gait) Femoral head partially or completely displaced from acetabulum Slight delay in ambulation (14-15 mo) Shortened lower extremity with restricted abduction of affected hip If bilateral, waddling gait with swayback (excessive lumbar lordosis)


27 DDH Radiographs at 6 mo or older Hip pain and limp may not present until adolescence

28 Legg-Calve-Perthes Disease AVN of proximal femoral epiphysis in children 4-12 yo Boys:girls 4:1 Antalgic gait exacerbated by physical activity, alleviated by rest, worse later in day +/- night pain Exam depends on severity greater loss of abduction and internal rotation with more severe disease

29 Legg-Calve-Perthes Initial radiographs Slight lateralization with slightly smaller FH nucleus 1/3 of cases = subchondral lucency in femoral head on lateral As disease progresses: collapse and fragmentation of femoral epiphysis Refer to Ortho MRI and bone scan: early before radiographic changes
 > girls (10-13 y) Younger: metabolic / endocrinopathy Age < 10 or >16, non-obese (hypothyroid, low GH, pituitary tumor, renal")
30 Slipped Capital Femoral Epiphysis (SCFE) Antalgic gait in adolescent Capital femoral epiphysis displaces posterior & medial on femoral neck Slippage acute or gradual Boys (12-15 y) > girls (10-13 y) Younger: metabolic / endocrinopathy Age < 10 or >16, non-obese (hypothyroid, low GH, pituitary tumor, renal osteodystrophy)


31 SCFE Constant, mild pain in hip, groin, thigh or KNEE in overweight kid Pain with passive ROM, decreased internal rotation/abduction Hip is flexed, LE rotates externally Acute slippage has increased incidence of AVN Dx with AP/lateral radiograph Bilateral in 1/3

32 Toddler s Fracture Torsion injury produces spiral fx of tibia without fibular fx Initial XR may appear normal F/U XR in 1-2 wks show new bone Treat with short term immobilization 3-4 weeks



33 Anatomy Unique to Skeletally Immature Bones Epiphysis, physis, metaphysis, diaphysis Periosteum - thicker, osteogenic, attaches firmly at periphery of physis Bone - more porous, ductile


34 Fractures Common only in Skeletally Immature Physeal injuries - weak link = physis Buckle or Torus Plastic Deformation Greenstick Fracture
35 Salter - Harris Classification Type I - through physis Type II - through physis & metaphysis Type III - through physis & epiphysis Type IV - through metaphysis, physis & epiphysis Type V - crush injury to entire physis

 Gentle reduction of physeal injuries (traction first,")
36 Treatment Principles Closed Methods Vast majority of pediatric fractures treated by closed methods Except - open, Salter III & IV, multi-trauma Attempt to restore alignment (do not always rely on remodeling) Gentle reduction of physeal injuries (traction first, adequate relaxation)


37 Remodeling of Children s Fractures Occurs by physeal & periosteal growth changes Remodel best in younger children & if near a rapidly growing physis Has to be reduced to remodel Cast most fractures, no worry for stiffness

38 Growth Arrest Secondary to Growth Plate Injury Complete cessation of longitudinal growth = limb length discrepancy Partial cessation angular deformity if peripheral progressive shortening if central

39 Limb Length Discrepancy Apparent in children 4-10 yo Toe-walk to keep pelvis level To accurately measure: child stands with shorter extremity on blocks until the pelvis is level Need standing film of entire lower extremities



40 Overuse Syndromes Apophysitis (Osgood-Schlatter) Point tenderness at tibial tubercle Apophysitis: (Sever) Point tenderness at calcaneus growth plate Stress Fx s Bone scan

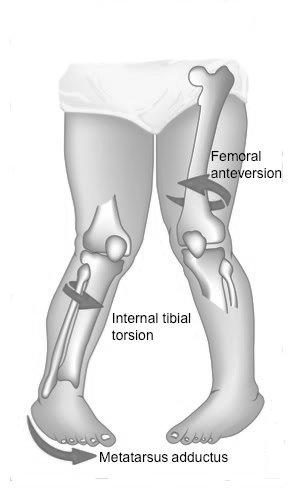
41 Normal Torsion


42 Clubfoot: congenital malalignment of the foot and ankle If left untreated, clubfoot persists as rigid deformity Weightbearing surface is dorsolateral midfoot Treat: early Serial manipulation and casting Ponseti technique

43 Neoplasms Leukemia Most common cancer in children < 16 y Peak incidence 2-5 y 20% with musculoskeletal c/o = Joint symptoms & bone PAIN causing limp Fatigue, skin bruising, & bleeding, hepatosplenomegaly should alert clinician Initial XRs unremarkable, or transverse zones of lucent metaphyseal bands adjacent to physis Dx: Labs, Bone marrow aspiration & biopsy


44 BONE LESIONS Size Location Description Sclerotic Blastic Lytic Expansile Single vs multiple


45 BONE LESIONS


46 Final Thoughts Remember pediatric skeletal differences Diagnose common conditions Listen the kid will give you the answer!



47 Take Home Points Differential of common conditions Age, history, PE Know what to order & what to look for Fractures, deformities, disorders If you are unsure, ask for help - Phone an friend Repetition is key: the more you see, the more you review, the more comfortable you will feel


48 Thank you for your kind attention
49 REFERENCES Herring, W. Learning Radiology: Recognizing the Basics Mettler. Essentials of Radiology, 2nd ed Google Images
The Limping Child: Differential Diagnosis
 The Limping Child: Differential Diagnosis Kathryn A Keeler, MD Assistant Professor University of Missouri-Kansas City School of Medicine, Department of Orthopaedic Surgery and Department of Pediatrics
The Limping Child: Differential Diagnosis Kathryn A Keeler, MD Assistant Professor University of Missouri-Kansas City School of Medicine, Department of Orthopaedic Surgery and Department of Pediatrics
Effects of Immobilization. N24 Pedi Musculoskeletal Spring 2012, Week 14. Cabrillo ADN/C. Madsen RN, MSN 1. Physical effects on other systems
 Common Orthopedic Problems of Children Congenital Acquired Bones Neuromuscular Physical effects on other systems Pulmonary Cardiac Skin integrity Elimination GI GU 1 4 General Nursing Considerations any
Common Orthopedic Problems of Children Congenital Acquired Bones Neuromuscular Physical effects on other systems Pulmonary Cardiac Skin integrity Elimination GI GU 1 4 General Nursing Considerations any
The Child With a Limp
 KID WITH A LIMP Common in ED, common in Exams Differential diagnosis is very wide Most causes benign, but mustn't miss Septic arthritis Osteomyelitis Fractures / NAI SUFE (older, heavier children) The
KID WITH A LIMP Common in ED, common in Exams Differential diagnosis is very wide Most causes benign, but mustn't miss Septic arthritis Osteomyelitis Fractures / NAI SUFE (older, heavier children) The
An understanding of the components of the normal gait cycle will aid in describing abnormalities of gait.
 Approach to the Child with a Limp: Student writer: Brian Mayson Resident editor: Elmine Statham Background The child with a limp is a common problem seen in pediatrics. A limp is defined as any deviation
Approach to the Child with a Limp: Student writer: Brian Mayson Resident editor: Elmine Statham Background The child with a limp is a common problem seen in pediatrics. A limp is defined as any deviation
I have no financial relationships related to disclose
 Evaluation of a child with a limp / Slipped Capital Femoral Epiphysis (SCFE) Lee S. Segal, MD Chief, Division of Pediatric Orthopedics American Family Children s Hospital Department of Orthopedics and
Evaluation of a child with a limp / Slipped Capital Femoral Epiphysis (SCFE) Lee S. Segal, MD Chief, Division of Pediatric Orthopedics American Family Children s Hospital Department of Orthopedics and
7/1/2012. Repetitive valgus stresses cause microfractures in the apophyseal cartilage (weak link) Common in year olds
 Common in year olds") 1 2 3 4 5 6 7 When growing pains are not growing pains David W. Gray,M.D. Medical Director Orthopedics Differential Diagnosis Fracture Ligament Injury Disloclation Cartilage Injury Apophysitis Inflammation
1 2 3 4 5 6 7 When growing pains are not growing pains David W. Gray,M.D. Medical Director Orthopedics Differential Diagnosis Fracture Ligament Injury Disloclation Cartilage Injury Apophysitis Inflammation
The Limping Child. Todd Milbrandt, MD Division Chair Pediatric Orthopaedics Mayo Clinic Rochester
 The Limping Child Todd Milbrandt, MD Division Chair Pediatric Orthopaedics Mayo Clinic Rochester Faculty Disclosure No disclosures relevant to this talk Practice Gap Primary Care Providers are faced with
The Limping Child Todd Milbrandt, MD Division Chair Pediatric Orthopaedics Mayo Clinic Rochester Faculty Disclosure No disclosures relevant to this talk Practice Gap Primary Care Providers are faced with
Non-inflammatory joint pain
 Non-inflammatory joint pain Lawrence Owino Okong o, Mmed (UoN); Mphil. (UCT). Lecturer, Department of Paediatrics and Child Health, University of Nairobi. Paediatrician/ Rheumatologist. INTRODUCTION Musculoskeletal
Non-inflammatory joint pain Lawrence Owino Okong o, Mmed (UoN); Mphil. (UCT). Lecturer, Department of Paediatrics and Child Health, University of Nairobi. Paediatrician/ Rheumatologist. INTRODUCTION Musculoskeletal
THE HIP. Cooler than cool, the pinnacle of what is "it". Beyond all trends and conventional coolness.
 THE HIP Cooler than cool, the pinnacle of what is "it". Beyond all trends and conventional coolness. Objectives Hip anatomy Causes of hip pain Hip exam Anatomy Bones Ilium Anterior Superior Iliac Spine
THE HIP Cooler than cool, the pinnacle of what is "it". Beyond all trends and conventional coolness. Objectives Hip anatomy Causes of hip pain Hip exam Anatomy Bones Ilium Anterior Superior Iliac Spine
A Patient s Guide to Limping in Children
 A Patient s Guide to Limping in Children 651 Old Country Road Plainview, NY 11803 Phone: 5166818822 Fax: 5166813332 p.lettieri@aol.com DISCLAIMER: The information in this booklet is compiled from a variety
A Patient s Guide to Limping in Children 651 Old Country Road Plainview, NY 11803 Phone: 5166818822 Fax: 5166813332 p.lettieri@aol.com DISCLAIMER: The information in this booklet is compiled from a variety
PEM GUIDE CHILDHOOD FRACTURES
 PEM GUIDE CHILDHOOD FRACTURES INTRODUCTION Skeletal injuries account for 10-15% of all injuries in children; 20% of those are fractures, 3 out of 4 fractures affect the physis or growth plate. Always consider
PEM GUIDE CHILDHOOD FRACTURES INTRODUCTION Skeletal injuries account for 10-15% of all injuries in children; 20% of those are fractures, 3 out of 4 fractures affect the physis or growth plate. Always consider
Pediatric Orthopedic Pathology Pathology 2 Dr. Gary Mumaugh
 Pediatric Orthopedic Pathology Pathology 2 Dr. Gary Mumaugh Congenital Defects - Clubfoot (congenital equinovarus) Forefoot is adducted and supinated o Positional equinovarus o Idiopathic congenital equinovarus
Pediatric Orthopedic Pathology Pathology 2 Dr. Gary Mumaugh Congenital Defects - Clubfoot (congenital equinovarus) Forefoot is adducted and supinated o Positional equinovarus o Idiopathic congenital equinovarus
Pediatric Orthopedics: ``To Refer or Not to Refer``
 Pediatric Orthopedics: ``To Refer or Not to Refer`` Thierry E. Benaroch, MD, FRCS(C) McGill University Health Centre Intoeing Knock knees Bowlegs Flatfeet Toe walking Knee pain Hip click Intoeing Objectives
Pediatric Orthopedics: ``To Refer or Not to Refer`` Thierry E. Benaroch, MD, FRCS(C) McGill University Health Centre Intoeing Knock knees Bowlegs Flatfeet Toe walking Knee pain Hip click Intoeing Objectives
A Patient s Guide to Transient Synovitis of the Hip in Children
 A Patient s Guide to Transient Synovitis of the Hip in Children 651 Old Country Road Plainview, NY 11803 Phone: 5166818822 Fax: 5166813332 p.lettieri@aol.com DISCLAIMER: The information in this booklet
A Patient s Guide to Transient Synovitis of the Hip in Children 651 Old Country Road Plainview, NY 11803 Phone: 5166818822 Fax: 5166813332 p.lettieri@aol.com DISCLAIMER: The information in this booklet
1. Discuss some common pediatric problems seen in the clinic. Diagnosis Clinical examination (at birth and subsequent well-baby examinations)
") 1 Pediatric Orthopaedics for Primary Care Providers 2 Disclosure Statement No conflicts related to this presentation 3 4 Goals 1. Discuss some common pediatric problems seen in the clinic 2. Examination
1 Pediatric Orthopaedics for Primary Care Providers 2 Disclosure Statement No conflicts related to this presentation 3 4 Goals 1. Discuss some common pediatric problems seen in the clinic 2. Examination
General Concepts. Growth Around the Knee. Topics. Evaluation
 General Concepts Knee Injuries in Skeletally Immature Athletes Zachary Stinson, M.D. Increased rate and ability of healing Higher strength of ligaments compared to growth plates Continued growth Children
General Concepts Knee Injuries in Skeletally Immature Athletes Zachary Stinson, M.D. Increased rate and ability of healing Higher strength of ligaments compared to growth plates Continued growth Children
1/10/2017 PEDIATRIC LIMP: BOARD REVIEW GOALS & OBJECTIVES RELEVANCE DAVID POHL, D.O. PGY-3 ST. JOHN MACOMB-OAKLAND JANUARY 21, 2017
 PEDIATRIC LIMP: BOARD REVIEW DAVID POHL, D.O. PGY-3 ST. JOHN MACOMB-OAKLAND JANUARY 21, 2017 RELEVANCE AOBFP EXAM BLUEPRINT: ORTHO 5% PEDS 4% ADOLESCENTS 4% SPORTS 3 % http://static3.businessinsider.com/image/52545f89eab8ea62534aa515-1200-375/brain%20golfing.jpg
PEDIATRIC LIMP: BOARD REVIEW DAVID POHL, D.O. PGY-3 ST. JOHN MACOMB-OAKLAND JANUARY 21, 2017 RELEVANCE AOBFP EXAM BLUEPRINT: ORTHO 5% PEDS 4% ADOLESCENTS 4% SPORTS 3 % http://static3.businessinsider.com/image/52545f89eab8ea62534aa515-1200-375/brain%20golfing.jpg
Other Hip Disorders: Congenital (Developmental) & Idiopathic 이대목동병원 윤여헌
 & Idiopathic 이대목동병원 윤여헌") Other Hip Disorders: Congenital (Developmental) & Idiopathic 이대목동병원 윤여헌 Children s hip disorders Congenital & developmental disorders Developmental hip dysplasia (dislocation) of the hip Developmental
Other Hip Disorders: Congenital (Developmental) & Idiopathic 이대목동병원 윤여헌 Children s hip disorders Congenital & developmental disorders Developmental hip dysplasia (dislocation) of the hip Developmental
Musculoskeletal Concerns in the Pediatric Athlete. John Hatzenbuehler, MD FACSM ACSM TPC Course 2015
 Musculoskeletal Concerns in the Pediatric Athlete John Hatzenbuehler, MD FACSM ACSM TPC Course 2015 Dislclosures Neither I, John Hatzenbuehler nor any family member(s), have any relevant financial relationships
Musculoskeletal Concerns in the Pediatric Athlete John Hatzenbuehler, MD FACSM ACSM TPC Course 2015 Dislclosures Neither I, John Hatzenbuehler nor any family member(s), have any relevant financial relationships
Pediatric Fractures. Objectives. Epiphyseal Complex. Anatomy and Physiology. Ligaments. Bony matrix
 1 Pediatric Fractures Nicholas White, MD Assistant Professor of Pediatrics Eastern Virginia Medical School Attending, Pediatric Emergency Department Children s Hospital of The King s Daughters Objectives
1 Pediatric Fractures Nicholas White, MD Assistant Professor of Pediatrics Eastern Virginia Medical School Attending, Pediatric Emergency Department Children s Hospital of The King s Daughters Objectives
Disclosures Head to Toe: Common Sports Injuries in Kids
 Disclosures Head to Toe: Common Sports Injuries in Kids None R. Jay Lee MD Director Pediatric Orthopaedic Fellowship Assistant Professor Pediatric Orthopaedics Johns Hopkins / Bloomberg Children s Objectives
Disclosures Head to Toe: Common Sports Injuries in Kids None R. Jay Lee MD Director Pediatric Orthopaedic Fellowship Assistant Professor Pediatric Orthopaedics Johns Hopkins / Bloomberg Children s Objectives
OBJECTIVES: Define basic assessments skills needed to identify orthopedic injuries. Differentiate when an orthopedic injury is a medical emergency
 1 2 How to Triage Orthopaedic Care David W. Gray, M.D. OBJECTIVES: Define basic assessments skills needed to identify orthopedic injuries Differentiate when an orthopedic injury is a medical emergency
1 2 How to Triage Orthopaedic Care David W. Gray, M.D. OBJECTIVES: Define basic assessments skills needed to identify orthopedic injuries Differentiate when an orthopedic injury is a medical emergency
Friday Teaching. Bones
 Friday Teaching Bones Regarding slipped femoral capital epiphysis It represents Salter Harris type V injury 20% are bilateral There is slight widening of the joint space Slip is typically posteromedial
Friday Teaching Bones Regarding slipped femoral capital epiphysis It represents Salter Harris type V injury 20% are bilateral There is slight widening of the joint space Slip is typically posteromedial
Assessment of limping child (beware the child who does not weight bear at all):
:") Department of Paediatrics Clinical Guideline Acutely Limping Child and Septic Arthritis Assessment of limping child (beware the child who does not weight bear at all): History Careful history of any significant
Department of Paediatrics Clinical Guideline Acutely Limping Child and Septic Arthritis Assessment of limping child (beware the child who does not weight bear at all): History Careful history of any significant
The Child with a Limp
 The Child with a Limp DR S Rajapaksa RCH CHIld with a limp Case: An 11 year old presents to ED with a 4 days history of a painful limp. He had been playing footie over the weekend and had fallen but then
The Child with a Limp DR S Rajapaksa RCH CHIld with a limp Case: An 11 year old presents to ED with a 4 days history of a painful limp. He had been playing footie over the weekend and had fallen but then
A free online interactive information resource for clinicians.
 A free online interactive information resource for clinicians www.pmmonline.org The limping child Helen Foster Professor of Paediatric Rheumatology Newcastle University Honorary Consultant Great North
A free online interactive information resource for clinicians www.pmmonline.org The limping child Helen Foster Professor of Paediatric Rheumatology Newcastle University Honorary Consultant Great North
AAP Boot Camp KNEE AND ANKLE EXAM
 AAP Boot Camp KNEE AND ANKLE EXAM Disclosures I have no relevant financial relationships with the manufacturers of any commercial products and or providers of commercial services discussed in this CME
AAP Boot Camp KNEE AND ANKLE EXAM Disclosures I have no relevant financial relationships with the manufacturers of any commercial products and or providers of commercial services discussed in this CME
Andrea Marmor, MD Associate Clinical Professor, Pediatrics UCSF San Francisco General Hospital
 Andrea Marmor, MD Associate Clinical Professor, Pediatrics UCSF San Francisco General Hospital Carambola is a 16 mo old girl brought to the ED for crying nonstop She has been not herself for about a week,
Andrea Marmor, MD Associate Clinical Professor, Pediatrics UCSF San Francisco General Hospital Carambola is a 16 mo old girl brought to the ED for crying nonstop She has been not herself for about a week,
Upper Extremity Fractures
 Upper Extremity Fractures Ranie Whatley, RN,FNP-C David W. Gray, MD Skeletal Trauma 10 to 15 % of all Childhood Injuries Physeal (Growth Plate) Injuries are ~ 15% of all Skeletal Injuries Orthopaedic Assessment
Upper Extremity Fractures Ranie Whatley, RN,FNP-C David W. Gray, MD Skeletal Trauma 10 to 15 % of all Childhood Injuries Physeal (Growth Plate) Injuries are ~ 15% of all Skeletal Injuries Orthopaedic Assessment
Common Orthopaedic Injuries in Children
 Common Orthopaedic Injuries in Children Rakesh P. Mashru, M.D. Division of Orthopaedic Trauma Cooper University Hospital Cooper Medical School of Rowan University December 1, 2017 1 Learning Objectives
Common Orthopaedic Injuries in Children Rakesh P. Mashru, M.D. Division of Orthopaedic Trauma Cooper University Hospital Cooper Medical School of Rowan University December 1, 2017 1 Learning Objectives
Orthopedics. 1. GOAL: Understand the pediatrician's role in preventing and screening for
 The University of Arizona Pediatric Residency Program Primary Goals for Rotation Orthopedics 1. GOAL: Understand the pediatrician's role in preventing and screening for orthopedic injury, disease and dysfunction.
The University of Arizona Pediatric Residency Program Primary Goals for Rotation Orthopedics 1. GOAL: Understand the pediatrician's role in preventing and screening for orthopedic injury, disease and dysfunction.
6/23/2017. What do you see? skull fracture
 What do you see? skull fracture 1 Head CT On soft tissue windows, posterior soft tissues swelling and hemorrhage, no definite evidence of fracture Head CT On bone windows, fracture now seen subjacent to
What do you see? skull fracture 1 Head CT On soft tissue windows, posterior soft tissues swelling and hemorrhage, no definite evidence of fracture Head CT On bone windows, fracture now seen subjacent to
On the Field Management of Pediatric Trauma
 On the Field Management of Pediatric Trauma Kyle Nagle, MD MPH University of Colorado Department of Orthopedics Children s Hospital Colorado Orthopedics Institute Disclosures I have no conflicts of interest
On the Field Management of Pediatric Trauma Kyle Nagle, MD MPH University of Colorado Department of Orthopedics Children s Hospital Colorado Orthopedics Institute Disclosures I have no conflicts of interest
University of South Florida
 University of South Florida Pediatric Orthopaedics PGY 4 Competency Based Goals & Objectives Competency 1- Patient Care: Provide family centered patient care that is developmentally and age appropriate,
University of South Florida Pediatric Orthopaedics PGY 4 Competency Based Goals & Objectives Competency 1- Patient Care: Provide family centered patient care that is developmentally and age appropriate,
Hip Biomechanics and Osteotomies
 Hip Biomechanics and Osteotomies Organization Introduction Hip Biomechanics Principles of Osteotomy Femoral Osteotomies Pelvic Osteotomies Summary Inroduction Osteoarthritis is very prevalent Primary OA
Hip Biomechanics and Osteotomies Organization Introduction Hip Biomechanics Principles of Osteotomy Femoral Osteotomies Pelvic Osteotomies Summary Inroduction Osteoarthritis is very prevalent Primary OA
Exam of the Knee and Ankle I HAVE NO FINANCIAL DISCLOSURES RELEVANT TO THIS PRESENTATION
 Exam of the Knee and Ankle I HAVE NO FINANCIAL DISCLOSURES RELEVANT TO THIS PRESENTATION Disclosures I have no relevant financial relationships with the manufacturers of any commercial products and or
Exam of the Knee and Ankle I HAVE NO FINANCIAL DISCLOSURES RELEVANT TO THIS PRESENTATION Disclosures I have no relevant financial relationships with the manufacturers of any commercial products and or
Evaluation of the Hip and Knee
 Evaluation of the Hip and Knee Causes of hip pain RA Osteoarthritis Psoriatic arthritis Septic arthritis Bursitis Hip fx Labral tear Tendinitis Referred back pain Cancer AVN Legg-Calve-Perthes Paget's
Evaluation of the Hip and Knee Causes of hip pain RA Osteoarthritis Psoriatic arthritis Septic arthritis Bursitis Hip fx Labral tear Tendinitis Referred back pain Cancer AVN Legg-Calve-Perthes Paget's
Case Presentations The Child with a Limp
 Case Presentations The Child with a Limp Douglas G. Armstrong, M.D. Professor, PennState Hershey College of Medicine Division Head, Pediatric Orthopaedics Dept. of Orthopaedics and Rehabilitation PennState
Case Presentations The Child with a Limp Douglas G. Armstrong, M.D. Professor, PennState Hershey College of Medicine Division Head, Pediatric Orthopaedics Dept. of Orthopaedics and Rehabilitation PennState
Lower Extremity Fracture Management. Fractures of the Hip. Lower Extremity Fractures. Vascular Anatomy. Lower Extremity Fractures in Children
 Lower Extremity Fracture Management Brian Brighton, MD, MPH Levine Children s s Hospital Carolinas Medical Center Charlotte, NC Oscar Miller Day October 16, 2009 Lower Extremity Fractures in Children Anatomic
Lower Extremity Fracture Management Brian Brighton, MD, MPH Levine Children s s Hospital Carolinas Medical Center Charlotte, NC Oscar Miller Day October 16, 2009 Lower Extremity Fractures in Children Anatomic
Ankle Sprains and Their Imitators
 Ankle Sprains and Their Imitators Mark Halstead, MD Dr. Mark Halstead is the Associate Professor of the Departments of Orthopedics and Pediatrics at Washington University School of Medicine; Director of
Ankle Sprains and Their Imitators Mark Halstead, MD Dr. Mark Halstead is the Associate Professor of the Departments of Orthopedics and Pediatrics at Washington University School of Medicine; Director of
Case. 5 year old with 2 weeks leg pain and now refusing to walk + Fevers, lower leg swelling, warmth Denies and history of trauma or wounds
 Case 5 year old with 2 weeks leg pain and now refusing to walk + Fevers, lower leg swelling, warmth Denies and history of trauma or wounds Exam I: Swelling over entire tibia extending to foot P: Tenderness
Case 5 year old with 2 weeks leg pain and now refusing to walk + Fevers, lower leg swelling, warmth Denies and history of trauma or wounds Exam I: Swelling over entire tibia extending to foot P: Tenderness
DR. (PROF.) ANIL ARORA MS
 ANIL ARORA MS") Hip Examination DR. (PROF.) ANIL ARORA MS (Ortho) DNB (Ortho) Dip SIROT (USA) FAPOA (Korea), FIGOF (Germany), FJOA (Japan) Commonwealth Fellow Joint Replacement (Royal National Orthopaedic Hospital, London,
Hip Examination DR. (PROF.) ANIL ARORA MS (Ortho) DNB (Ortho) Dip SIROT (USA) FAPOA (Korea), FIGOF (Germany), FJOA (Japan) Commonwealth Fellow Joint Replacement (Royal National Orthopaedic Hospital, London,
Identify signs/symptoms/risk factors for: Understand issues of overtraining and signs of pediatric burnout
 Identify signs/symptoms/risk factors for: Little League Elbow Apophysitis including Osgood-Schlatter and Sever s Slipped Capital Femoral Epiphysis Understand issues of overtraining and signs of pediatric
Identify signs/symptoms/risk factors for: Little League Elbow Apophysitis including Osgood-Schlatter and Sever s Slipped Capital Femoral Epiphysis Understand issues of overtraining and signs of pediatric
PAEDIATRIC ORTHOPAEDICS BRENT WEATHERHEAD, MD, FRCSC PAEDIATRIC ORTHOPAEDIC SURGEON MEDICAL DIRECTOR, REBALANCE
 PAEDIATRIC ORTHOPAEDICS BRENT WEATHERHEAD, MD, FRCSC PAEDIATRIC ORTHOPAEDIC SURGEON MEDICAL DIRECTOR, REBALANCE DISCLOSURES I HAVE NO INDUSTRY CONFLICTS TO DECLARE I AM AN ORTHOPAEDIC SURGEON TRAINED IN
PAEDIATRIC ORTHOPAEDICS BRENT WEATHERHEAD, MD, FRCSC PAEDIATRIC ORTHOPAEDIC SURGEON MEDICAL DIRECTOR, REBALANCE DISCLOSURES I HAVE NO INDUSTRY CONFLICTS TO DECLARE I AM AN ORTHOPAEDIC SURGEON TRAINED IN
42 nd Annual Symposium on Sports Medicine. Knee Injuries In The Pediatric Athlete. Disclosure
 42 nd Annual Symposium on Sports Medicine Travis Murray, MD Assistant Professor University of Texas Health Science Center San Antonio January 23, 2015 Knee Injuries In The Pediatric Athlete Disclosure
42 nd Annual Symposium on Sports Medicine Travis Murray, MD Assistant Professor University of Texas Health Science Center San Antonio January 23, 2015 Knee Injuries In The Pediatric Athlete Disclosure
Childhood Fractures. Incomplete fractures more common. Ligaments stronger than bone. Tendons stronger than bone. Fractures may be pathologic
 Childhood Fractures Incomplete fractures more common Plastic bowing Torus / Buckle Greenstick Ligaments stronger than bone Fracture patterns different Physeal injury, not dislocation Tendons stronger than
Childhood Fractures Incomplete fractures more common Plastic bowing Torus / Buckle Greenstick Ligaments stronger than bone Fracture patterns different Physeal injury, not dislocation Tendons stronger than
Hip Pain in Adults: Evaluation 67th Annual McGill Refresher Course for Family Physicians Dec6/2016
 Hip Pain in Adults: Evaluation 67th Annual McGill Refresher Course for Family Physicians Dec6/2016 David J Zukor MD FRCSC Chief Department of Orthopedic Surgery SMBD-Jewish General Hospital Associate Professor
Hip Pain in Adults: Evaluation 67th Annual McGill Refresher Course for Family Physicians Dec6/2016 David J Zukor MD FRCSC Chief Department of Orthopedic Surgery SMBD-Jewish General Hospital Associate Professor
Bone and Joint Infections Oh, My
 Bone and Joint Infections Oh, My Dale Jarka, MD,CM, FRCSC The Children s Mercy Hospitals & Clinics The Children's Mercy Hospital 2016 1 Disclosures A: I have no relevant financial relationships with the
Bone and Joint Infections Oh, My Dale Jarka, MD,CM, FRCSC The Children s Mercy Hospitals & Clinics The Children's Mercy Hospital 2016 1 Disclosures A: I have no relevant financial relationships with the
Slipped Capital Femoral Epiphysis
 Slipped Capital Femoral Epiphysis Nicholas D. Fletcher, MD Assistant Professor of Orthopaedics and Scoliosis Emory University Orthopaedics Emory Orthopaedics Center for Hip Preservation What is it? Misnomer
Slipped Capital Femoral Epiphysis Nicholas D. Fletcher, MD Assistant Professor of Orthopaedics and Scoliosis Emory University Orthopaedics Emory Orthopaedics Center for Hip Preservation What is it? Misnomer
Broadening the Differential: Spine and Lower Extremity Injuries in the Young Athlete. Disclosures. Goals. Dr. Nirav K. Pandya
 Broadening the Differential: Spine and Lower Extremity Injuries in the Young Athlete Disclosures - Consultant - Orthopediatrics - Committee Member POSNA Dr. Nirav K. Pandya Assistant Professor of Orthopaedic
Broadening the Differential: Spine and Lower Extremity Injuries in the Young Athlete Disclosures - Consultant - Orthopediatrics - Committee Member POSNA Dr. Nirav K. Pandya Assistant Professor of Orthopaedic
40 th Annual Symposium on Sports Medicine. Knee Injuries In The Pediatric Athlete. Disclosure
 40 th Annual Symposium on Sports Medicine Travis Murray, MD Assistant Professor University of Texas Health Science Center San Antonio Knee Injuries In The Pediatric Athlete Disclosure Dr. Travis Murray
40 th Annual Symposium on Sports Medicine Travis Murray, MD Assistant Professor University of Texas Health Science Center San Antonio Knee Injuries In The Pediatric Athlete Disclosure Dr. Travis Murray
Will She Still Make the WNBA? Sports Injuries & Fractures
 Will She Still Make the WNBA? Sports Injuries & Fractures Aharon Z. Gladstein MD Pediatric Orthopaedic Surgery Pediatric Sports Medicine Sports Injuries Chronic (overuse) Acute Who can be treated in PCP
Will She Still Make the WNBA? Sports Injuries & Fractures Aharon Z. Gladstein MD Pediatric Orthopaedic Surgery Pediatric Sports Medicine Sports Injuries Chronic (overuse) Acute Who can be treated in PCP
No Disclosures. Topics. Pediatric ACL Tears
 Knee Injuries in Skeletally Immature Athletes No Disclosures Zachary Stinson, M.D. 2 Topics ACL Tears and Tibial Eminence Fractures Meniscus Injuries Discoid Meniscus Osteochondritis Dessicans Patellar
Knee Injuries in Skeletally Immature Athletes No Disclosures Zachary Stinson, M.D. 2 Topics ACL Tears and Tibial Eminence Fractures Meniscus Injuries Discoid Meniscus Osteochondritis Dessicans Patellar
What a Pain! Radiology Evaluation of Leg Complaints and Limping. I have nothing to disclose. Leg Complaints. Leg Complaints
 What a Pain! Radiology Evaluation of Leg Complaints and Limping I have nothing to disclose Maria-Gisela Mercado-Deane, MD FAAP Christus Santa Rosa Children Hospital San Antonio, TX Age groups Infant and
What a Pain! Radiology Evaluation of Leg Complaints and Limping I have nothing to disclose Maria-Gisela Mercado-Deane, MD FAAP Christus Santa Rosa Children Hospital San Antonio, TX Age groups Infant and
Apply this knowledge into proper management strategies and referrals
 1 2 3 Lower Extremity Injuries Jason Kennedy, M.D. Disclosures I have no financial/ industry disclosures. Objectives Identify common lower extremity injury patterns in the child and adolescent Apply this
1 2 3 Lower Extremity Injuries Jason Kennedy, M.D. Disclosures I have no financial/ industry disclosures. Objectives Identify common lower extremity injury patterns in the child and adolescent Apply this
Non Surgical Management Of Hip And Knee Osteoarthritis Toolkit. Evaluation and Diagnosis of Osteoarthritis in Primary Care
 Non Surgical Management Of Hip And Knee Osteoarthritis Toolkit Evaluation and Diagnosis of Osteoarthritis in Primary Care OA-HxPE-716.indd 1 TABLE OF CONTENTS HISTORY TAKING... 3 EVALUATION OF SUSPECTED
Non Surgical Management Of Hip And Knee Osteoarthritis Toolkit Evaluation and Diagnosis of Osteoarthritis in Primary Care OA-HxPE-716.indd 1 TABLE OF CONTENTS HISTORY TAKING... 3 EVALUATION OF SUSPECTED
Index. Note: Page numbers of article titles are in boldface type.
 Note: Page numbers of article titles are in boldface type. A Abductor hallucis tendon procedures, for hallux varus, 536 537 Acetabular disorders, intoeing in, 551 553 Akron dome osteotomy, for cavus deformities,
Note: Page numbers of article titles are in boldface type. A Abductor hallucis tendon procedures, for hallux varus, 536 537 Acetabular disorders, intoeing in, 551 553 Akron dome osteotomy, for cavus deformities,
Pediatric Rounds Topics and Objectives
 Pediatric Rounds Topics and Objectives Development Dysplasia Hip... 4... 4... 4... 5 Communicator... 5 Scholar... 5 Slipped Capital Femoral Epiphysis... 5... 5... 5... 6 Communicator... 6 Health Advocate...
Pediatric Rounds Topics and Objectives Development Dysplasia Hip... 4... 4... 4... 5 Communicator... 5 Scholar... 5 Slipped Capital Femoral Epiphysis... 5... 5... 5... 6 Communicator... 6 Health Advocate...
Outline. Ankle/Foot Anatomy Ankle Sprains Ottawa Ankle Rules DDx: The Sprain That Wasn t
 Ankle Injuries Outline Ankle/Foot Anatomy Ankle Sprains Ottawa Ankle Rules DDx: The Sprain That Wasn t Anatomy: Ankle Mortise Bony Anatomy Lateral Ligament Complex Medial Ligament Complex Ankle Sprains
Ankle Injuries Outline Ankle/Foot Anatomy Ankle Sprains Ottawa Ankle Rules DDx: The Sprain That Wasn t Anatomy: Ankle Mortise Bony Anatomy Lateral Ligament Complex Medial Ligament Complex Ankle Sprains
Orthopedic Emergencies. Peter Gutierrez, MD Pediatric Emergency Medicine Children s Healthcare of Atlanta
 Orthopedic Emergencies Peter Gutierrez, MD Pediatric Emergency Medicine Children s Healthcare of Atlanta Disclosures I have no relevant financial relationships to disclose I do not intend to discuss unapproved
Orthopedic Emergencies Peter Gutierrez, MD Pediatric Emergency Medicine Children s Healthcare of Atlanta Disclosures I have no relevant financial relationships to disclose I do not intend to discuss unapproved
EXAMINATION OF HIP. A. Inspection Examination
 EXAMINATION OF HIP History: What is your trouble? Pain, stiffness, limp Please tell me more about your problem?.listen Listen for at least one minute: Let patient do the talking Do not ask leading question
EXAMINATION OF HIP History: What is your trouble? Pain, stiffness, limp Please tell me more about your problem?.listen Listen for at least one minute: Let patient do the talking Do not ask leading question
Sports Medicine in your office: What not to miss!
 Sports Medicine in your office: What not to miss! 2018 Primary Care Approach to Treating the Injured Athlete May 4, 2018 John H. Wilckens, MD Associate Professor, Dept of Orthopaedic Surgery Disclosures
Sports Medicine in your office: What not to miss! 2018 Primary Care Approach to Treating the Injured Athlete May 4, 2018 John H. Wilckens, MD Associate Professor, Dept of Orthopaedic Surgery Disclosures
Topics and Cases in Pediatric Orthopaedics (Tuesday 6:30am 4 th Floor Orthopaedic Conference Room at Hamot)
") 2015-2016 Topics and Cases in Pediatric Orthopaedics (Tuesday 6:30am 4 th Floor Orthopaedic Conference Room at Hamot) 1. Considerations in the Management of Pediatric Patients Kerry Armet 7 July 2015 Fluid
2015-2016 Topics and Cases in Pediatric Orthopaedics (Tuesday 6:30am 4 th Floor Orthopaedic Conference Room at Hamot) 1. Considerations in the Management of Pediatric Patients Kerry Armet 7 July 2015 Fluid
Tibial Shaft Fractures
 Tibial Shaft Fractures Mr Krishna Vemulapalli Consultant Orthopaedics Surgeon Queens & King George Hospitals Queens Hospital 14/03/2018 Google Maps Map data 2018 Google 10 km Orthopaedics Department Covers
Tibial Shaft Fractures Mr Krishna Vemulapalli Consultant Orthopaedics Surgeon Queens & King George Hospitals Queens Hospital 14/03/2018 Google Maps Map data 2018 Google 10 km Orthopaedics Department Covers
3/18/18. Adolescent Hip Injuries. Adolescents with Hip Injuries DISCLOSURES
 Adolescent Hip Injuries Henry Bone Ellis, Jr., MD DFW Sports Medicine Symposium March 24, 2018 DISCLOSURES Royalties and stock options Consulting income Smith and Nephew Other support Research on Osteochondritis
Adolescent Hip Injuries Henry Bone Ellis, Jr., MD DFW Sports Medicine Symposium March 24, 2018 DISCLOSURES Royalties and stock options Consulting income Smith and Nephew Other support Research on Osteochondritis
Surgery-Ortho. Fractures of the tibia and fibula. Management. Treatment of low energy fractures. Fifth stage. Lec-6 د.
 Fifth stage Lec-6 د. مثنى Surgery-Ortho 28/4/2016 Indirect force: (low energy) Fractures of the tibia and fibula Twisting: spiral fractures of both bones Angulatory: oblique fractures with butterfly segment.
Fifth stage Lec-6 د. مثنى Surgery-Ortho 28/4/2016 Indirect force: (low energy) Fractures of the tibia and fibula Twisting: spiral fractures of both bones Angulatory: oblique fractures with butterfly segment.
Intoeing: When to Worry? Sukhdeep K. Dulai SPORC 2018
 Intoeing: When to Worry? Sukhdeep K. Dulai SPORC 2018 What is it? Intoeing: When to worry? Why isn t it always cause for worry? What are the benign causes of intoeing? What are the pathologic causes of
Intoeing: When to Worry? Sukhdeep K. Dulai SPORC 2018 What is it? Intoeing: When to worry? Why isn t it always cause for worry? What are the benign causes of intoeing? What are the pathologic causes of
Physical Examination of the Knee
 History: Pain Traumatic vs. atraumatic Acute vs Chronic Mechanism of injury Swelling, catching, instability Previous evaluation and treatment General Setup Examine standing, sitting and supine Evaluate
History: Pain Traumatic vs. atraumatic Acute vs Chronic Mechanism of injury Swelling, catching, instability Previous evaluation and treatment General Setup Examine standing, sitting and supine Evaluate
Acquired Hip Disorders in Children and Adolescents. Sarah D. Bixby Department of Radiology Boston Children s Hospital Boston, MA
 Acquired Hip Disorders in Children and Adolescents Sarah D. Bixby Department of Radiology Boston Children s Hospital Boston, MA Don t Miss Acquired Hip Disorders SCFE Posterior Hip Dislocation Osteoid
Acquired Hip Disorders in Children and Adolescents Sarah D. Bixby Department of Radiology Boston Children s Hospital Boston, MA Don t Miss Acquired Hip Disorders SCFE Posterior Hip Dislocation Osteoid
Ankle Ligament Injury: Don t Worry- It s Only a Sprain Wes Jackson MD Orthopaedic Foot & Ankle
 Ankle Ligament Injury: Don t Worry- It s Only a Sprain Wes Jackson MD Orthopaedic Foot & Ankle Outline I. Epidemiology II. Classification and Types of Sprains III. Anatomy IV. Clinical Assessment and Imaging
Ankle Ligament Injury: Don t Worry- It s Only a Sprain Wes Jackson MD Orthopaedic Foot & Ankle Outline I. Epidemiology II. Classification and Types of Sprains III. Anatomy IV. Clinical Assessment and Imaging
Running Injuries in Children and Adolescents
 Running Injuries in Children and Adolescents Cook Children s SPORTS Symposium July 2, 2014 Running Injuries Overuse injuries Acute injuries Anatomic conditions 1 Overuse Injuries Pain that cannot be tied
Running Injuries in Children and Adolescents Cook Children s SPORTS Symposium July 2, 2014 Running Injuries Overuse injuries Acute injuries Anatomic conditions 1 Overuse Injuries Pain that cannot be tied
The Hip from Cradle to Grave. Haemish Crawford Ascot Hospital Starship Children s Hospital
 The Hip from Cradle to Grave Haemish Crawford Ascot Hospital Starship Children s Hospital Developmental dysplasia hip DDH Irritable vs. septic hip Perthes disease Slipped Upper Femoral Epiphysis (SUFE)
The Hip from Cradle to Grave Haemish Crawford Ascot Hospital Starship Children s Hospital Developmental dysplasia hip DDH Irritable vs. septic hip Perthes disease Slipped Upper Femoral Epiphysis (SUFE)
Pediatric Orthopedics in Your Office. Laurel Saliman, MD Pediatric Orthopedic Surgeon Swedish Pediatric Specialty Care
 Pediatric Orthopedics in Your Office Laurel Saliman, MD Pediatric Orthopedic Surgeon Swedish Pediatric Specialty Care Overview for 20 minute whirlwind Clavicle Distal radius fractures Finger fractures
Pediatric Orthopedics in Your Office Laurel Saliman, MD Pediatric Orthopedic Surgeon Swedish Pediatric Specialty Care Overview for 20 minute whirlwind Clavicle Distal radius fractures Finger fractures
Common Apophyseal Problems in the Athlete
 Disclosure Common Apophyseal Problems in the Athlete Mark Halstead, MD November 19, 2009 Faculty Disclosure Information In the past 12 months, I have no relevant financial relationships with the manufacturer
Disclosure Common Apophyseal Problems in the Athlete Mark Halstead, MD November 19, 2009 Faculty Disclosure Information In the past 12 months, I have no relevant financial relationships with the manufacturer
LECTURE 8: DEVELOPMENTAL ORTHOPAEDICS. Paediatric MS History o Reason for referral o Past history
 LECTURE 8: DEVELOPMENTAL ORTHOPAEDICS Paediatric MS History o Reason for referral o Past history Antenatal history Birth history (term? Premmy? Breech? Complications?). Medical history/investigations/tests
LECTURE 8: DEVELOPMENTAL ORTHOPAEDICS Paediatric MS History o Reason for referral o Past history Antenatal history Birth history (term? Premmy? Breech? Complications?). Medical history/investigations/tests
PEDIATRIC AND CONGENITAL IMAGING GUIDELINES MUSCULOSKELETAL 2009 MedSolutions, Inc
 MedSolutions, Inc. This tool addresses common symptoms and symptom complexes. Imaging requests for patients with atypical Clinical Decision Support Tool symptoms or clinical presentations that are not
MedSolutions, Inc. This tool addresses common symptoms and symptom complexes. Imaging requests for patients with atypical Clinical Decision Support Tool symptoms or clinical presentations that are not
The Painful Hip. Jennifer R Marks, MD
 The Painful Hip Jennifer R Marks, MD The Painful Hip A 64 yo F presents to clinic complaining of a sore hip What further questions do you have for this patient? What is on your differential diagnosis?
The Painful Hip Jennifer R Marks, MD The Painful Hip A 64 yo F presents to clinic complaining of a sore hip What further questions do you have for this patient? What is on your differential diagnosis?
Bilateral hip pain with right proximal femoral lesion
 Bilateral hip pain with right proximal femoral lesion Legg-Calve-Perthes Idiopathic osteonecrosis of the femoral head epiphysis during childhood First described by Arthur Thorton Legg in 1909 and published
Bilateral hip pain with right proximal femoral lesion Legg-Calve-Perthes Idiopathic osteonecrosis of the femoral head epiphysis during childhood First described by Arthur Thorton Legg in 1909 and published
Hths 2231 Laboratory 13 Alterations in Musculoskeletal
 Watch Movie: Osteoporosis Answer the movie questions on the worksheet. Complete activities 1-4. Activity #1: Click on the website link in activity 1 to review the structure and function of bone. Activity
Watch Movie: Osteoporosis Answer the movie questions on the worksheet. Complete activities 1-4. Activity #1: Click on the website link in activity 1 to review the structure and function of bone. Activity
4/28/2010. Fractures. Normal Bone and Normal Ossification Bone Terms. Epiphysis Epiphyseal Plate (physis) Metaphysis
 Metaphysis") Fractures Normal Bone and Normal Ossification Bone Terms Epiphysis Epiphyseal Plate (physis) Metaphysis Diaphysis 1 Fracture Classifications A. Longitudinal B. Transverse C. Oblique D. Spiral E. Incomplete
Fractures Normal Bone and Normal Ossification Bone Terms Epiphysis Epiphyseal Plate (physis) Metaphysis Diaphysis 1 Fracture Classifications A. Longitudinal B. Transverse C. Oblique D. Spiral E. Incomplete
Foot and Ankle Natalie Stork, MD
 Foot and Ankle Natalie Stork, MD Assistant Professor University of Missouri-Kansas City School of Medicine, Department of Orthopaedic Surgery and Department of Pediatrics Children s Mercy Kansas City,
Foot and Ankle Natalie Stork, MD Assistant Professor University of Missouri-Kansas City School of Medicine, Department of Orthopaedic Surgery and Department of Pediatrics Children s Mercy Kansas City,
Physeal Fractures and Growth Arrest
 Physeal Fractures and Growth Arrest Raymond W. Liu, M.D. Victor M. Goldberg Master Clinician-Scientist in Orthopaedics Rainbow Babies and Children s Hospital Case Western Reserve University Outline General
Physeal Fractures and Growth Arrest Raymond W. Liu, M.D. Victor M. Goldberg Master Clinician-Scientist in Orthopaedics Rainbow Babies and Children s Hospital Case Western Reserve University Outline General
July 2011 Case of the Month. By Matt Grady, MD
 July 2011 Case of the Month By Matt Grady, MD CC: Knee Pain - Osteochondritis Dissecans or not? A Case Comparison HPI: The first patient is a 12 year old female swimmer with right knee pain. The pain started
July 2011 Case of the Month By Matt Grady, MD CC: Knee Pain - Osteochondritis Dissecans or not? A Case Comparison HPI: The first patient is a 12 year old female swimmer with right knee pain. The pain started
BATES VISUAL GUIDE TO PHYSICAL EXAMINATION. OSCE 4: Knee Pain
 BATES VISUAL GUIDE TO PHYSICAL EXAMINATION OSCE 4: Knee Pain This video format is designed to help you prepare for objective structured clinical examinations, or OSCEs. You are going to observe and participate
BATES VISUAL GUIDE TO PHYSICAL EXAMINATION OSCE 4: Knee Pain This video format is designed to help you prepare for objective structured clinical examinations, or OSCEs. You are going to observe and participate
RELEVANT DISCLOSURES OR CONFLICTS OF INTEREST PATHOPHYSIOLOGY -MECHANICAL STRESS FRACTURES OF THE LOWER EXTREMITIES
 RELEVANT DISCLOSURES OR CONFLICTS OF INTEREST STRESS FRACTURES OF THE LOWER EXTREMITIES NONE Mark A Foreman M.D. Assistant Professor, UTHSCSA General Orthopedics and Trauma WHAT IS A STRESS FRACTURE? A
RELEVANT DISCLOSURES OR CONFLICTS OF INTEREST STRESS FRACTURES OF THE LOWER EXTREMITIES NONE Mark A Foreman M.D. Assistant Professor, UTHSCSA General Orthopedics and Trauma WHAT IS A STRESS FRACTURE? A
Lower Extremity Alignment: Genu Varum / Valgum
 Lower Extremity Alignment: Genu Varum / Valgum Arthur B Meyers, MD Nemours Children s Hospital & Health System Associate Professor of Radiology, University of Central Florida Clinical Associate Professor
Lower Extremity Alignment: Genu Varum / Valgum Arthur B Meyers, MD Nemours Children s Hospital & Health System Associate Professor of Radiology, University of Central Florida Clinical Associate Professor
Pediatric Case Studies. Case 1
 Pediatric Case Studies James Naprawa, MD Assistant Clinical Professor Pediatric Emergency Medicine Children s Hospital, Columbus Case 1 Almost 4 year old AA girl PMH UTI x 2 with abdominal pain and fever
Pediatric Case Studies James Naprawa, MD Assistant Clinical Professor Pediatric Emergency Medicine Children s Hospital, Columbus Case 1 Almost 4 year old AA girl PMH UTI x 2 with abdominal pain and fever
Toe walking gives rise to parental concern. Therefore, toe-walkers are often referred at the 3 years of age.
 IDIOPATHIC TOE WALKING Toe walking is a common feature in immature gait and is considered normal up to 3 years of age. As walking ability improves, initial contact is made with the heel. Toe walking gives
IDIOPATHIC TOE WALKING Toe walking is a common feature in immature gait and is considered normal up to 3 years of age. As walking ability improves, initial contact is made with the heel. Toe walking gives
Pediatric Athletic Overuse Injuries. Susan Haralabatos, MD OPSC Annual Meeting 2018
 Pediatric Athletic Overuse Injuries Susan Haralabatos, MD OPSC Annual Meeting 2018 Text I have no disclosures Overview Etiology, Physiology &Anatomy Common Physeal Overuse Injuries Stress Fractures Concussion
Pediatric Athletic Overuse Injuries Susan Haralabatos, MD OPSC Annual Meeting 2018 Text I have no disclosures Overview Etiology, Physiology &Anatomy Common Physeal Overuse Injuries Stress Fractures Concussion
Osteomyelitis in infancy and childhood: A clinical and diagnostic overview M. Mearadji
 Osteomyelitis in infancy and childhood: A clinical and diagnostic overview M. Mearadji International Foundation for Pediatric Imaging Aid Introduction Osteomyelitis is a relative common disease in infancy
Osteomyelitis in infancy and childhood: A clinical and diagnostic overview M. Mearadji International Foundation for Pediatric Imaging Aid Introduction Osteomyelitis is a relative common disease in infancy
Hip Impingement and Arthritis: Preservation vs. Total Hip Arthroplasty. Faculty Disclosures. Objectives 11/17/2017
 Hip Impingement and Arthritis: Preservation vs. Total Hip Arthroplasty Jonathan R. Schiller, MD Assistant Professor of Orthopedics Warren Alpert Medical School of Brown University Director, Adolescent
Hip Impingement and Arthritis: Preservation vs. Total Hip Arthroplasty Jonathan R. Schiller, MD Assistant Professor of Orthopedics Warren Alpert Medical School of Brown University Director, Adolescent
Practice Changes I Hope You Make
 Is that Bad? What PCPs (& Parents) Need to Know about Fractures Aharon Z. Gladstein, MD Pediatric Orthopaedics & Sports Medicine Texas Children s Hospital Assistant Professor, Orthopaedics Baylor College
Is that Bad? What PCPs (& Parents) Need to Know about Fractures Aharon Z. Gladstein, MD Pediatric Orthopaedics & Sports Medicine Texas Children s Hospital Assistant Professor, Orthopaedics Baylor College
Lower Extremity Dislocations: Management and Triage on the Field
 Lower Extremity Dislocations: Management and Triage on the Field Scott J Tarantino, MD Towson Orthopaedic Associates, Towson, MD None Disclsures Purpose To provide you with knowledge which may guide you
Lower Extremity Dislocations: Management and Triage on the Field Scott J Tarantino, MD Towson Orthopaedic Associates, Towson, MD None Disclsures Purpose To provide you with knowledge which may guide you
The Surgical Management of Rickets & Osteogenesis Imperfecta
 The Surgical Management of Rickets & Osteogenesis Imperfecta Dr Greg Firth Chris Hani Baragwanath Academic Hospital Department of Orthopaedics University of the Witwatersrand Rickets Inadequate mineralization
The Surgical Management of Rickets & Osteogenesis Imperfecta Dr Greg Firth Chris Hani Baragwanath Academic Hospital Department of Orthopaedics University of the Witwatersrand Rickets Inadequate mineralization
EMERGENCY PITFALLS IN ORTHOPAEDIC TRAUMA. Thierry E. Benaroch, MD, FRCS MCH Trauma Rounds February 9, 2009
 EMERGENCY PITFALLS IN ORTHOPAEDIC TRAUMA Thierry E. Benaroch, MD, FRCS MCH Trauma Rounds February 9, 2009 MORAL OF THE STORY Fracture distal radius and intact ulna W/O radius fracture will most likely
EMERGENCY PITFALLS IN ORTHOPAEDIC TRAUMA Thierry E. Benaroch, MD, FRCS MCH Trauma Rounds February 9, 2009 MORAL OF THE STORY Fracture distal radius and intact ulna W/O radius fracture will most likely
Ouch, That s Gotta Hurt! Pediatric Fractures & Injuries
 Ouch, That s Gotta Hurt! Pediatric Fractures & Injuries Greg Canty, MD Medical Director, Sports Medicine Center Attending Physician, Emergency Medicine Children s Mercy Kansas City 2011 Children s Mercy
Ouch, That s Gotta Hurt! Pediatric Fractures & Injuries Greg Canty, MD Medical Director, Sports Medicine Center Attending Physician, Emergency Medicine Children s Mercy Kansas City 2011 Children s Mercy
A Patient s Guide to Femoroacetabular Impingement (FAI) of the Hip
 of the Hip") A Patient s Guide to Femoroacetabular Impingement (FAI) of the Hip 651 Old Country Road Plainview, NY 11803 Phone: 5166818822 Fax: 5166813332 p.lettieri@aol.com DISCLAIMER: The information in this booklet
A Patient s Guide to Femoroacetabular Impingement (FAI) of the Hip 651 Old Country Road Plainview, NY 11803 Phone: 5166818822 Fax: 5166813332 p.lettieri@aol.com DISCLAIMER: The information in this booklet
Slipped Capital Femoral Epiphysis (SCFE)
") Slipped Capital Femoral Epiphysis (SCFE) DR MUMTAZ HUSSAIN Senior Registrar DR ABDUL LATIF SAMI (Associate Professor) Head of Department Pediatric Orthopedics Introduction and Definition Epidemiology and
Slipped Capital Femoral Epiphysis (SCFE) DR MUMTAZ HUSSAIN Senior Registrar DR ABDUL LATIF SAMI (Associate Professor) Head of Department Pediatric Orthopedics Introduction and Definition Epidemiology and
11/5/14. I will try to make this painless. Great, a Fracture, Now What? Objectives. Basics for Fracture Workup. Basics for Fracture Workup
 Great, a Fracture, Now What? I will try to make this painless Mary Greve MS, PA-C Department of Orthopedic Surgery Trauma Team University of Iowa Hospitals and Clinics Mary-Greve@uiowa.edu Pager 2121 Objectives
Great, a Fracture, Now What? I will try to make this painless Mary Greve MS, PA-C Department of Orthopedic Surgery Trauma Team University of Iowa Hospitals and Clinics Mary-Greve@uiowa.edu Pager 2121 Objectives
DDH. Abnormal hip development Traditionally CDH (congenital dysplasia of the hip) Today DDH(developmental dysplasia of the hip)
 Today DDH(developmental dysplasia of the hip)") DDH Update on Screening Kathryn A Keeler, MD Assistant Professor University of Missouri-Kansas City School of Medicine, Department of Orthopaedic Surgery and Department of Pediatrics Children s Mercy Kansas
DDH Update on Screening Kathryn A Keeler, MD Assistant Professor University of Missouri-Kansas City School of Medicine, Department of Orthopaedic Surgery and Department of Pediatrics Children s Mercy Kansas