PLASMA CELL DISORDERS. Dr Mere Kende MBBS, Mmed (Path),MACTM, MAACB, MACRRM Lecturer: SMHS
|
|
|
- Octavia Gregory
- 5 years ago
- Views:
Transcription
1 PLASMA CELL DISORDERS Dr Mere Kende MBBS, Mmed (Path),MACTM, MAACB, MACRRM Lecturer: SMHS
2 Terms/Antigenic Determinants Isotypes: Ig molecules that form antigenic determinants, and these are used to classify immunoglobulins E.g., five heavy chains (IgG, IgM, IgA, IgD, IgE) and two light chains (kappa & lambda). It is species specific and the same in one species. Allotypes are distinct determinants that reflect regular small differences between individuals of the same species in the amino acid sequences of otherwise similar immunoglobulins. These differences are determined by allelic genes; by definition, they are detected by antibodies made in the same species. E.g., IgG1-4 Idiotypes are the third category of antigenic determinants. They are unique to the molecules produced by a given clone of antibodyproducing cells. Idiotypes are formed by the unique structure of the antigen-binding portion of the molecule.
3 Composition of Ab Two heavy chains (IgG, M, D, A, E) (mol wt ~ 50,000) Two light chains (lamba & kappa)- (mol wt ~ 25,000). Each chain has a constant portion (limited amino acid sequence variability) and a variable region (extensive sequence variability). The light and heavy chains linked by disulfide bonds Variable regions (antigen recognition) are adjacent to one another. Each chain is specified by distinct genes, synthesized separately, and assembled into an intact antibody molecule after translation. In most cells, free light chains are synthesized in slight excess, and are cleared by the kidney, but <10 mg of such light chains is excreted per day.
4
5 Plasma cell disorders (monoclonal gammopathies, paraproteinemias, plasma cell dyscrasias, and dysproteinemias. are monoclonal neoplasms related to each other by virtue of their development common progenitors in the B lymphocyte lineage. Normal: Maturation to antibody-secreting plasma cells is stimulated by exposure to the antigen for which the surface immunoglobulin is specific; Plasma cell dyscrasias: the control over this process is lost.
6 Examples of plasma cell disorders Multiple Myeloma, Waldenström's macroglobulinemia (IgM), Primary amyloidosis & Heavy Chain diseases
7 Pathogenesis/Clinical Manifestation Expansion of the neoplastic cells Secretion of cell products (immunoglobulin molecules or subunits, lymphokines), To some extent to the host's response to the tumour Effects of Monoclonal protein (M protein)
8
9 M-protein Electrophoretic analysis- detected if >5glL) Reliable measure of the tumour burden M component is an excellent tumour marker, (lack specificity)
10 M components may be detected in other lymphoid neoplasms CML Lymphomas CML Breast/Colon CA Nonneoplastic conditions such as cirrhosis, sarcoidosis, parasitic diseases, Gaucher disease, and pyoderma gangrenosum; Autoimmune conditions, including rheumatoid arthritis, myasthenia gravis, and cold agglutinin disease.
11 Multiple Myeloma Definition Multiple myeloma represents a malignant proliferation of plasma cells derived from a single clone. The terms multiple myeloma and myeloma may be used interchangeably. The tumour, its products, and the host response to it result in a number of organ dysfunctions
12 Etiology Cause? Exposure to radiation (WW II) Chromosomal abnormalities (deletions/translocations) Deletions: 13q14 deletions, 17p13 deletions, and 11q abnormalities predominate. Translocation: t(11;14)(q13;q32) and t(4;14)(p16;q32), and evidence is strong that errors in switch recombination the genetic mechanism to change antibody heavy chain isotype participate in the transformation pathway. Overexpression of myc or ras genes has been noted in some cases. Mutations in p53 and Rb-1 have also been described, but no common molecular pathogenesis has yet emerged.
13 High incidences in farmers, wood workers, leather workers, and those exposed to petroleum products.? Role of interleukin 6 may play a role in driving myeloma cell proliferation; a large fraction of myeloma cells exposed to IL-6 in vitro respond by proliferating.
14 Characteristic morphologic features of plasma cells, round or oval cells with an eccentric nucleus composed of coarsely clumped chromatin, a densely basophilic cytoplasm, and a perinuclear clear zone (hof) containing the Golgi apparatus. Binucleate and multinucleate malignant plasma cells can be seen.
15 Incidence and Prevalence In USA 19,900 cases of myeloma were diagnosed in 2007 & 10,790 people died Incidences increases in incidence with age Median age -68 years; it is uncommon under age 40. The yearly incidence is around 4 per 100,000 and remarkably similar throughout the world. Males > females, Blacks > twice the incidence of whites.
16 Myeloma accounts for ~1% of all malignancies in whites and 2% in blacks; 13% of all hematologic cancers in whites and 33% in blacks. Incidence: highest in African-American and Pacific islanders; intermediate in Europeans and North American Caucasians; and lowest in developing countries including Asia The higher incidence in more developed countries may result from the combination of a longer life expectancy and more frequent medical surveillance.
17 Pathogenesis and Clinical Manifestations

18 Pathogenesis of multiple myeloma. Multiple myeloma cells interact with bone marrow stromal cells and extracellular matrix proteins via adhesion molecules, triggering adhesionmediated signalling as well as cytokine production. This triggers cytokine-mediated signalling that provides growth, survival, and anti-apoptotic effects as well as development of drug resistance. HSP, heparin sulfate proteoglycan.
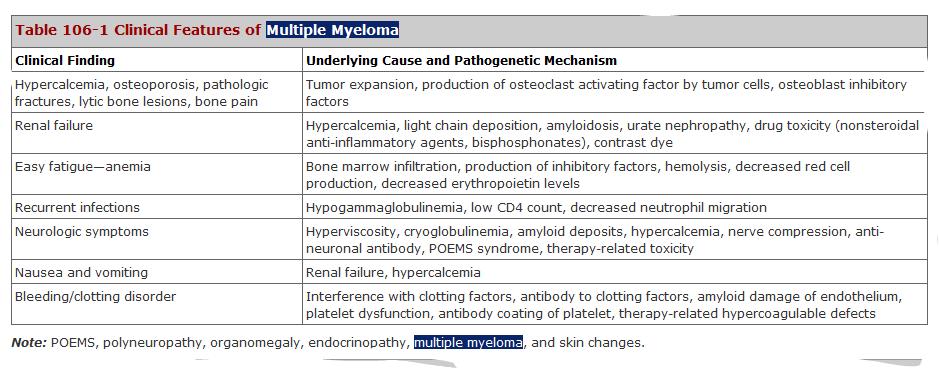
19 Clinical Features symptoms of bone pain or fracture, Renal failure Susceptibility to infection, Anaemia, Hypercalcemia, Occasionally clotting abnormalities, Neurologic symptoms, Manifestations of hyperviscosity (IgM).
20 Bone Pain back and ribs most common symptom in MM affecting nearly 70% of patients. Precipitated by movement Persistent localized pain ----pathologic fracture. Bone lesion- caused by the proliferation of tumor cells, activation of osteoclasts that destroy bone, and suppression of osteoblasts that form new bone.
21 Bony lesions in multiple myeloma. The skull demonstrates the typical "punched out" lesions characteristic of multiple myeloma. The lesion represents a purely osteolytic lesion with little or no osteoblastic activity. (Courtesy of Dr. Geraldine Schechter; with permission.)
22 Figure Cervical compression fracture. Lateral cervical x-ray showing an adequate image of the complete cervical spine from C1 to the top of T1. The arrows denote a compression fracture with loss of the vertebral body height of the fifth cervical vertebral body secondary to multiple myeloma. Note the sclerotic margins of the superior portion of the fifth vertebra, indicating this is a chronic lesion. There are other lesions in the third and fourth cervical vertebra as well.
23 Activation of Osteoclast by Osteoclast activating factors (OAF) OAF activity influenced by several cytokines, including IL-1, lymphotoxin, VEGF, receptor activator of NF-B (RANK) ligand, macrophage inhibitory factor (MIP)-1, and tumour necrosis factor (TNF)]. Glucocorticoids or interferon (IFN) decrease these cytokines. Result lytic bone lesion (No Bone Formation) Increased bone tissue resorption, lack of new bone formation, leaching of calcium ----increased serum levels & Normal ALP Localized bone lesions may expand to the point that mass lesions may be palpated, especially on the skull, clavicles, and sternum, and the collapse of vertebrae may lead to spinal cord compression.
24 Increased susceptibility to infection Pneumonias and pyelonephritis, and the most frequent pathogens are Streptococcus pneumoniae, Staphylococcus aureus, and Klebsiella pneumoniae in the lungs and Escherichia coli and other gram-negative organisms in the urinary tract. Decreased production and increased destruction of normal antibodies Impaired Neutrophil activity
25 Renal failure (~25%) Hypercalcemia Hyperuriceamia Increased light chain damage NSAID used to control pain Infections
26 Anaemia ~80% Normocytic and normochromic Replacement of normal marrow by expanding tumor cells and to the inhibition of hematopoiesis by factors made by the tumor. Mild hemolysis may contribute to the anemia. Associated megaloblastic anemia due to either folate or vitamin B 12 deficiency.
27 Clotting abnormalities may be seen due to the failure of antibody-coated platelets to function properly or to the interaction of the M component with clotting factors I, II, V, VII, or VIII. Deep venous thrombosis is also observed with use of thalidomide or lenalidomide in combination with dexamethasone.
28 Raynaud's phenomenon and impaired circulation may result if the M component forms cryoglobulins, and hyperviscosity syndromes may develop depending on the physical properties of the M component (most common with IgM, IgG3, and IgA paraproteins. Symptoms of hyperviscosity (normal 1.8) occur at a level of 5 6, a level usually reached at paraprotein concentrations of ~40 g/l (4 g/dl) for IgM, 50 g/l (5 g/dl) for IgG3, and 70 g/l (7 g/dl) for IgA.
29 Neurology Minority of patients, they may have many causes. Hypercalcemia may produce lethargy, weakness, depression, and confusion. Hyperviscosity may lead to headache, fatigue, visual disturbances, and retinopathy. Bony damage and collapse may lead to cord compression, radicular pain, and loss of bowel and bladder control. Infiltration of peripheral nerves by amyloid can be a cause of carpal tunnel syndrome and other sensorimotor mono- and polyneuropathies
30 Many of the clinical features of myeloma, e.g., cord compression, pathologic fractures, hyperviscosity, sepsis, and hypercalcemia, can present as medical emergencies. Despite the widespread distribution of plasma cells in the body, tumor expansion is dominantly within bone & marrow and, for reasons unknown, rarely causes enlargement of spleen, lymph nodes, or gut-associated lymphatic tissue.
31
32 Diagnosis and Staging MM classic Triad: Marrow plasmacytosis (>10%), Lytic bone lesions, & A serum and/or urine M component. (electrophoresis/immunoelectrophoresis)
33 Plasma Cells Large cells with eccentric nuclei, bi-nucleated/ multinucleated, clumped chromatin, mitotic figures
34
35

36
37 Differentials Monoclonal Gammopathy of Unknown Significance (MGUS) Solitary Plasmacytoma Extramedullary plasmacytoma
38 MGUS are vastly more common than myeloma, occurring in 1% of the population over age 50 and in up to 10% individuals over age 75. M protein <30g/L Require no therapy. Their survival is ~2 years shorter than age-matched controls without MGUS. Non-IgG subtype, abnormal kappa/lambda free light chain ratio, & serum M protein > 15 g/l (1.5 g/dl) are associated with higher incidence of progression to MM.
39 Solitary bone plasmacytoma & Extramedullary plasmacytoma Variants of MM Both are associated with an M component in <30% of the cases May affect younger individuals, Both are associated with median survivals of 10 years. Both tumors are highly responsive to local radiation therapy. If an M component is present, it should disappear after treatment.

40 Solitary bone plasmacytoma is a single lytic bone lesion without marrow plasmacytosis. May recur in other bony sites or evolve into myeloma.
41 Extramedullary plasmacytomas usually involve the submucosal lymphoid tissue of the nasopharynx or paranasal sinuses No Marrow plasmacytosis. No related organ or tissue impairment (no end organ damage other than solitary bone lesion) a Rarely recur or progress Normal skeletal survey (and MRI of spine and pelvis if done)
42 Diagnostic Criteria for MM Variants, and MGUS Monoclonal gammopathy of undetermined significance (MGUS) M protein in serum < 30 g/l Bone marrow clonal plasma cells < 10% No evidence of other B cell proliferative disorders No myeloma-related organ or tissue impairment (no end organ damage, including bone lesions) a Asymptomatic myeloma (smouldering myeloma) M protein in serum 30 g/l and/or Bone marrow clonal plasma cells 10% No myeloma-related organ or tissue impairment (no end organ damage, including bone lesions) a or symptoms
43 Symptomatic multiple myeloma M protein in serum and/or urine Bone marrow (clonal) plasma cells b or plasmacytoma Myeloma-related organ or tissue impairment (end organ damage, including bone lesions) Non-secretory myeloma No M protein in serum and/or urine with immunofixation Bone marrow clonal plasmacytosis 10% or plasmacytoma Myeloma-related organ or tissue impairment (end organ damage, including bone lesions) a
44 MM % IgG in 53% of patients, IgA in 25%, and IgD in 1%; 20% of patients will have only light chains in serum and urine. (50% BJP negative) Dipsticks for detecting proteinuria are not reliable at identifying light chains,
45 Other Laboratory features Normal ALP & hypercalcemia High ESR >20 Hyperuriceamia Azotaemia (increased urea/creat)
46 Treatment Systemic therapy to control the progression of myeloma Symptomatic supportive care to prevent serious morbidity from the complications of the disease. Therapy can significantly prolong survival and improve the quality of life for myeloma patients.
47 Cytotoxics/Dexamethasone Transplant Manage complications: hypercalcemia/hydration/renal failure/bone Pain/Fractures
48 References emedicine.medscape.com Harrison s Text Book of Medicine 17 th Edition
49 Myeloma Review Multiple Myeloma classic Triad: Marrow plasmacytosis (>10%), Lytic bone lesions, (x-ray) and A serum and/or urine M component. (electrophoresis/immunoelectrophoresis)
50 Clinical Features Mean Age: 65 Anaemia Hypercalcemia Renal failure Recurrent Infections Splenomegay/Lympadenopathy--RARE
51 Investigation Serum/Urine Electrophoresis (Monoclonal band) Bone Marrow Aspirate Skeletal X-ray
52
53 Bony lesions in multiple myeloma. The skull demonstrates the typical "punched out" lesions characteristic of multiple myeloma. The lesion represents a purely osteolytic lesion with little or no osteoblastic activity. (Courtesy of Dr. Geraldine Schechter; with permission.)
54 Characteristic morphologic features of plasma cells, round or oval cells with an eccentric nucleus composed of coarsely clumped chromatin, a densely basophilic cytoplasm, and a perinuclear clear zone (hof) containing the Golgi apparatus. Binucleate and multinucleate malignant plasma cells can be seen.
55 Brief Monoclonal Gammapathy of Unknown Significance (MGUS)-asymptomatic, no treatment required Solitary plasmacytopma-single bone lesion Extramedullary plasmacytomas -lympadenopathy, no BM plasmacytosis
56 Other Plasma Cell Dyscrasias Waldenstrom s Macroglobulinaemia Primary Amyloidosis Heavy Chain Diseases
57 Waldenström's Macroglobulinemia Essentials of Diagnosis Symptoms nonspecific; splenomegaly common on examination. Monoclonal IgM paraprotein. Infiltration of bone marrow by plasmacytic lymphocytes. Absence of lytic bone disease.
58 General Considerations Waldenström's macroglobulinemia is a malignant disease of B cells/plasma cells. Secrete IgM paraprotein, Clnical manifestations of the disease are related to this IgM macroglobulin.
59 Symptoms and Signs Age: 60s or 70s. Fatigue related to anemia. Hyperviscosity Syndrome Coagulation disorder -engorged vessels & PLT dysfunction (Mucosal and GIT bleeding) Neurological Symptoms: nausea, vertigo, and visual disturbances, stupor, coma or peripheral neuropathy (Demyelination)
60 Exam Findings hepatosplenomegaly or lymphadenopathy. Pallor Engorged retinal Veins +/-Purpura No Bone tenderness
61 Laboratory Findings Anemia is nearly universal (related in part to expansion of the plasma volume by % due to the presence of the paraprotein. Rouleaux formation is common. Other blood counts are usually normal.
62 Increased Plasma cells in BM Electrophoresis IgM monoclonal band Coomb s Test may be positive (cold agglutinin disease) Normal Bone x-rays No sign of Kidney Failure/hypercalcemia
63 Differential Diagnosis MGUS (no BM plasma cell increase) CLL & Multiple Myeloma (IgM spike/also on clinical grounds).
64 Treatment Plasmapheresis Drugs: fludarabine and rituximab BM transplant (younger patients with more aggressive disease).
65 Prognosis Median survival rate of 3 5 years. Patients may survive 10 years or longer.
66 Amyloidosis Deposition of abnormal insoluble protein (amyloid protein/fibrils) in various vascular beds and organ system
67 General Considerations Clinical Syndromes based on organ affected Can be primary or secondary to other chronic diseases In primary amyloidosis (AL), the protein fibrils are monoclonal immunoglobulin light chains, whereas in secondary amyloidosis (AA), protein deposits are derived from acute phase reactant apolipoprotein precursors. Familial forms have been reported Over 20 types of fibrils have been identified in amyloid deposits. Amyloidosis due to deposition of 2 -microglobulin in carpal ligaments occurs in long-term hemodialysis patients.
68 Symptoms and Signs Symptoms and signs of primary amyloidosis are due to amyloid infiltration. For example, nephritic syndrome and renal failure, cardiomyopathy and cardiac conduction defects Alzheimer's disease, intestinal malabsorption pseudo-obstruction,
69 carpal tunnel syndrome, macroglossia, peripheral neuropathy, end-organ insufficiency of endocrine glands, respiratory failure, capillary damage with ecchymosis).
70 Secondary amyloidosis is more often limited to the liver, spleen, and adrenals. Familial syndromes commonly cause infiltrative neuropathies.
71 Laboratory Tests Diagnosis of Primary amyloidosis clinical suspicion Serum electrophoresis Aspirate of abdominal fat pad or biopsy of rectal or gingival mucosa In systemic disease, rectal or gingival biopsies show a sensitivity of about 80%, bone-marrow biopsy about 50%, and abdominal fat aspiration between 70% and 80%.
72 Differential Diagnosis Multiple myeloma, Hemochromatosis, sarcoidosis, Waldenström's macroglobulinemia, Metastatic tumors, and Other cause of nephrotic syndrome, such as lupus nephritis.
73 Treatment Localised- surgical excision No effective treatment available for systemic amyloidosis Supportive treatment /hemodialysis Treat primary cause
74 Heavy Chain Diseases The clinical presentation is more typical of lymphoma than multiple myeloma, and there are no destructive bone lesions Rare lymphoplasmacytic malignancies. Clinical manifestations vary with the heavy chain isotype. Secretion of defective heavy chain that usually has an intact Fc fragment and a deletion in the Fd region. Gamma, alpha, and mu heavy chain diseases have been described, but no reports of delta or epsilon heavy chain diseases have appeared.
75 Gamma Heavy Chain Disease (Franklin's Disease) Characteristics :lymphadenopathy, fever, anemia, malaise, hepatosplenomegaly, and weakness. Its most distinctive symptom is palatal oedema, resulting from involvement of nodes in Waldeyer's ring, and this may progress to produce respiratory compromise. The diagnosis depends on the demonstration of an anomalous serum M component [often <20 g/l (<2 g/dl)] that reacts with anti-igg but not anti-light chain reagents. The M component is typically present in both serum and urine.
76 The patients may have thrombocytopenia, eosinophilia, and nondiagnostic bone marrow. Patients usually have a rapid downhill course and die of infection; however, some patients have survived 5 years with chemotherapy.
77 Alpha Heavy Chain Disease (Seligmann's Disease) This is the most common of the heavy chain diseases. Affects young persons in parts of the world where intestinal parasites are common, such as the Mediterranean, Asia, and South America. The disease is characterized by an infiltration of the lamina propria of the small intestine with lymphoplasmacytoid cells that secrete truncated alpha chains. Associated with GIT symptoms (Diarrhoea/ malabsorption)
78 Mu Heavy Chain Disease Occurs in a rare subset of patients with CLL. Presence of vacuoles in the malignant lymphocytes and the excretion of kappa light chains in the urine. Treatment is the same as other heavy chain disease

79 Figure Cervical compression fracture. Lateral cervical x-ray showing an adequate image of the complete cervical spine from C1 to the top of T1. The arrows denote a compression fracture with loss of the vertebral body height of the fifth cervical vertebral body secondary to multiple myeloma. Note the sclerotic margins of the superior portion of the fifth vertebra, indicating this is a chronic lesion. There are other lesions in the third and fourth cervical vertebra as well.
80 References emedicine.medscape.com Harrison s Text Book of Medicine 17 th Edition
Lec-14 د.خالد نافع. Medicine. Multiple Myeloma
 Fifth stage Lec-14 د.خالد نافع Medicine 24/4/2016 Multiple Myeloma Plasma cell myeloma Variants Non - secretory myeloma Indolent myeloma Smouldering myeloma Plasma cell leukaemia Plasmacytoma - Solitary
Fifth stage Lec-14 د.خالد نافع Medicine 24/4/2016 Multiple Myeloma Plasma cell myeloma Variants Non - secretory myeloma Indolent myeloma Smouldering myeloma Plasma cell leukaemia Plasmacytoma - Solitary
Osteosclerotic Myeloma (POEMS Syndrome)
") Osteosclerotic Myeloma (POEMS Syndrome) Osteosclerotic Myeloma (POEMS Syndrome) Synonyms Crow-Fukase syndrome Multicentric Castleman disease Takatsuki syndrome Acronym coined by Bardwick POEMS Scheinker,
Osteosclerotic Myeloma (POEMS Syndrome) Osteosclerotic Myeloma (POEMS Syndrome) Synonyms Crow-Fukase syndrome Multicentric Castleman disease Takatsuki syndrome Acronym coined by Bardwick POEMS Scheinker,
Hematology 101. Rachid Baz, M.D. 5/16/2014
 Hematology 101 Rachid Baz, M.D. 5/16/2014 Florida 101 Epidemiology Estimated prevalence 8,000 individuals in U.S (compare with 80,000 MM patients) Annual age adjusted incidence 3-8/million-year 1 More
Hematology 101 Rachid Baz, M.D. 5/16/2014 Florida 101 Epidemiology Estimated prevalence 8,000 individuals in U.S (compare with 80,000 MM patients) Annual age adjusted incidence 3-8/million-year 1 More
M-Protien, what to do next? Ismail A Sharif MD, FRCPc Internal Medicine Day 22 nd April 2016
 + M-Protien, what to do next? Ismail A Sharif MD, FRCPc Internal Medicine Day 22 nd April 2016 + Disclosures Advisory Boards: AMGEN, Lundbeck, NOVARTIS + Subtypes of Plasma Cell Disorders Increased Plasma
+ M-Protien, what to do next? Ismail A Sharif MD, FRCPc Internal Medicine Day 22 nd April 2016 + Disclosures Advisory Boards: AMGEN, Lundbeck, NOVARTIS + Subtypes of Plasma Cell Disorders Increased Plasma
Multiple myeloma Biological & Clinical Aspects Isabelle Vande Broek, MD, PhD
 Multiple myeloma Biological & Clinical Aspects Isabelle Vande Broek, MD, PhD Department of Oncology & Hematology AZ Nikolaas Iridium Kanker Netwerk Introduction Multiple myeloma = Kahler s disease Dr.
Multiple myeloma Biological & Clinical Aspects Isabelle Vande Broek, MD, PhD Department of Oncology & Hematology AZ Nikolaas Iridium Kanker Netwerk Introduction Multiple myeloma = Kahler s disease Dr.
Plasma cell myeloma (multiple myeloma)
") Plasma cell myeloma (multiple myeloma) Common lymphoid neoplasm, present at old age (70 years average) Remember: plasma cells are terminally differentiated B-lymphocytes that produces antibodies. B-cells
Plasma cell myeloma (multiple myeloma) Common lymphoid neoplasm, present at old age (70 years average) Remember: plasma cells are terminally differentiated B-lymphocytes that produces antibodies. B-cells
Tarek ElBaz, MD. Prof. Internal Medicine Chief, Division of Renal Medicine Al Azhar University President, ESNT
 The Kidney in Multiple Myeloma Tarek ElBaz, MD. Prof. Internal Medicine Chief, Division of Renal Medicine Al Azhar University President, ESNT Normal Cell Plasma cells produce antibodies that bind to antigens,
The Kidney in Multiple Myeloma Tarek ElBaz, MD. Prof. Internal Medicine Chief, Division of Renal Medicine Al Azhar University President, ESNT Normal Cell Plasma cells produce antibodies that bind to antigens,
Burkitt lymphoma. Sporadic Endemic in Africa associated with EBV Translocations involving MYC gene on chromosome 8
 Heme 8 Burkitt lymphoma Sporadic Endemic in Africa associated with EBV Translocations involving MYC gene on chromosome 8 Most common is t(8;14) Believed to be the fastest growing tumor in humans!!!! Morphology
Heme 8 Burkitt lymphoma Sporadic Endemic in Africa associated with EBV Translocations involving MYC gene on chromosome 8 Most common is t(8;14) Believed to be the fastest growing tumor in humans!!!! Morphology
Multiple Myeloma 101: Understanding Your Labs
 Multiple Myeloma 101: Understanding Your Labs Tim Wassenaar MD MS Hematologist, Director of Clinical Trials UW Cancer Center at ProHealth Care None Disclosures Outline Define hematopoiesis WBCs, RBCs,
Multiple Myeloma 101: Understanding Your Labs Tim Wassenaar MD MS Hematologist, Director of Clinical Trials UW Cancer Center at ProHealth Care None Disclosures Outline Define hematopoiesis WBCs, RBCs,
Expanding Spectrum of Diseases Associated with Plasma Cell Dyscrasias
 Expanding Spectrum of Diseases Associated with Plasma Cell Dyscrasias Eva Honsova Institute for Clinical and Experimental Medicine Prague, Czech Republic eva.honsova@ikem.cz Plasma cell dyscrasias Plasma
Expanding Spectrum of Diseases Associated with Plasma Cell Dyscrasias Eva Honsova Institute for Clinical and Experimental Medicine Prague, Czech Republic eva.honsova@ikem.cz Plasma cell dyscrasias Plasma
TYPE 1 GAUCHER DISEASE PRESENTING AS PERSISTENT THROMBOCYTOPENIA, ASSOCIATED FACTOR XI DEFICIENCY & EMERGENT MYELOMA
 TYPE 1 GAUCHER DISEASE PRESENTING AS PERSISTENT THROMBOCYTOPENIA, ASSOCIATED FACTOR XI DEFICIENCY & EMERGENT MYELOMA Trish Hyland, Medical Scientist, Department of Haematology, Cork University Hospital
TYPE 1 GAUCHER DISEASE PRESENTING AS PERSISTENT THROMBOCYTOPENIA, ASSOCIATED FACTOR XI DEFICIENCY & EMERGENT MYELOMA Trish Hyland, Medical Scientist, Department of Haematology, Cork University Hospital
Jo Abraham MD Division of Nephrology University of Utah
 Jo Abraham MD Division of Nephrology University of Utah 68 year old male presented 3 weeks ago with a 3 month history of increasing fatigue He reported a 1 week history of increasing dyspnea with a productive
Jo Abraham MD Division of Nephrology University of Utah 68 year old male presented 3 weeks ago with a 3 month history of increasing fatigue He reported a 1 week history of increasing dyspnea with a productive
Haematological Cancer Suspected (Adults & Children)
") Haematological Cancer Suspected (Adults & Children) Link to NICE guidelines: https://www.nice.org.uk/guidance/ng47 Patient of any age presents with symptoms of possible haematological cancer If 60 years
Haematological Cancer Suspected (Adults & Children) Link to NICE guidelines: https://www.nice.org.uk/guidance/ng47 Patient of any age presents with symptoms of possible haematological cancer If 60 years
Laboratory Examination
 Todd Zimmerman, M.D. 64 year old African American male presents to establish care with PCG. Meds: Norvasc 5 mg daily PMHx: HTN x 20 years, poorly controlled SHx: No tobacco, illicit; rare EtOH ROS: Negative
Todd Zimmerman, M.D. 64 year old African American male presents to establish care with PCG. Meds: Norvasc 5 mg daily PMHx: HTN x 20 years, poorly controlled SHx: No tobacco, illicit; rare EtOH ROS: Negative
Hematology Case Conference 8/5/03
 Hematology Case Conference 8/5/03 Bone Marrow Case Patient: Emmxxx Lylexxx 74 year old AA female S/P craniotomy for SDH. Pt has Hx of HTN, DM, Crohn s disease, (R) nephrectomy. Bone marrow for abnormal
Hematology Case Conference 8/5/03 Bone Marrow Case Patient: Emmxxx Lylexxx 74 year old AA female S/P craniotomy for SDH. Pt has Hx of HTN, DM, Crohn s disease, (R) nephrectomy. Bone marrow for abnormal
The ABCs of Waldenström s Macroglobulinemia (WM)
") The ABCs of Waldenström s Macroglobulinemia (WM) Jeffrey V. Matous MD Colorado Blood Cancer Institute IWMF Ed Forum May 2017 Objectives Describe the roots underneath WM Review incidence, possible risk
The ABCs of Waldenström s Macroglobulinemia (WM) Jeffrey V. Matous MD Colorado Blood Cancer Institute IWMF Ed Forum May 2017 Objectives Describe the roots underneath WM Review incidence, possible risk
HISTOPATHOLOGY. Shannon Martinson
 HISTOPATHOLOGY Shannon Martinson March 2013 Case #1 History: 8 year old beagle Neck pain for the past couple of weeks Paresis, followed by paralysis developed over the past few days Gross Description courtesy
HISTOPATHOLOGY Shannon Martinson March 2013 Case #1 History: 8 year old beagle Neck pain for the past couple of weeks Paresis, followed by paralysis developed over the past few days Gross Description courtesy
Sheena Surindran Grand Rounds 2/15/11
 Sheena Surindran Grand Rounds 2/15/11 Affects 5 12 person per million / year 5 10% associated with myeloma Median survival without treatment is 12 40 months Most commonly affected organs are kidney, heart
Sheena Surindran Grand Rounds 2/15/11 Affects 5 12 person per million / year 5 10% associated with myeloma Median survival without treatment is 12 40 months Most commonly affected organs are kidney, heart
Michael Joffe ST6 Haematology SpR
 Michael Joffe ST6 Haematology SpR Mrs SB 71 year old female on AMU Telephone referral to haematology by medicine with Hb 102 MCV 89, normal B12, Folate, Ferritin. PMH DM General decline over several weeks
Michael Joffe ST6 Haematology SpR Mrs SB 71 year old female on AMU Telephone referral to haematology by medicine with Hb 102 MCV 89, normal B12, Folate, Ferritin. PMH DM General decline over several weeks
Generation of post-germinal centre myeloma plasma B cell.
 Generation of post-germinal centre myeloma. DNA DAMAGE CXCR4 Homing to Lytic lesion activation CD38 CD138 CD56 Phenotypic markers Naive Secondary lymphoid organ Multiple myeloma is a malignancy of s caused
Generation of post-germinal centre myeloma. DNA DAMAGE CXCR4 Homing to Lytic lesion activation CD38 CD138 CD56 Phenotypic markers Naive Secondary lymphoid organ Multiple myeloma is a malignancy of s caused
Anaemias and other Pesky Haematology Questions
 Anaemias and other Pesky Haematology Questions 3 main topics How do I work out an anaemia.. That oh too common paraprotein patient. Those mildly raised lymphocyte count GP discussed patient with me over
Anaemias and other Pesky Haematology Questions 3 main topics How do I work out an anaemia.. That oh too common paraprotein patient. Those mildly raised lymphocyte count GP discussed patient with me over
The Lymphatic System and Body Defenses
 PowerPoint Lecture Slide Presentation by Patty Bostwick-Taylor, Florence-Darlington Technical College The Lymphatic System and Body Defenses 12PART B Adaptive Defense System: Third Line of Defense Immune
PowerPoint Lecture Slide Presentation by Patty Bostwick-Taylor, Florence-Darlington Technical College The Lymphatic System and Body Defenses 12PART B Adaptive Defense System: Third Line of Defense Immune
LYMPHOCYTES & IMMUNOGLOBULINS. Dr Mere Kende, Lecturer SMHS
 LYMPHOCYTES & IMMUNOGLOBULINS Dr Mere Kende, Lecturer SMHS Immunity Immune- protection against dangers of non-self/invader eg organism 3 components of immune system 1 st line: skin/mucosa/cilia/hair/saliva/fatty
LYMPHOCYTES & IMMUNOGLOBULINS Dr Mere Kende, Lecturer SMHS Immunity Immune- protection against dangers of non-self/invader eg organism 3 components of immune system 1 st line: skin/mucosa/cilia/hair/saliva/fatty
Pathology of Hematopoietic and Lymphoid tissue
 CONTENTS Pathology of Hematopoietic and Lymphoid tissue White blood cells and lymph nodes Quantitative disorder of white blood cells Reactive lymphadenopathies Infectious lymphadenitis Tumor metastasis
CONTENTS Pathology of Hematopoietic and Lymphoid tissue White blood cells and lymph nodes Quantitative disorder of white blood cells Reactive lymphadenopathies Infectious lymphadenitis Tumor metastasis
Lymphoma: What You Need to Know. Richard van der Jagt MD, FRCPC
 Lymphoma: What You Need to Know Richard van der Jagt MD, FRCPC Overview Concepts, classification, biology Epidemiology Clinical presentation Diagnosis Staging Three important types of lymphoma Conceptualizing
Lymphoma: What You Need to Know Richard van der Jagt MD, FRCPC Overview Concepts, classification, biology Epidemiology Clinical presentation Diagnosis Staging Three important types of lymphoma Conceptualizing
Suspecting Tumors, or Could it be cancer?
 Suspecting Tumors, or Could it be cancer? Donna E. Reece, M.D. Princess Margaret Cancer Centre University Health Network Toronto, ON CANADA 07 February 2018 Background Low back pain is common However,
Suspecting Tumors, or Could it be cancer? Donna E. Reece, M.D. Princess Margaret Cancer Centre University Health Network Toronto, ON CANADA 07 February 2018 Background Low back pain is common However,
Low grade High grade , immune suppression chronic persistent inflammation viruses B-symptoms
 We've one category for lymphoid neoplasm which is the lymphoma in contrast to that of myeloid which has three categories; acute myeloid leukemias, myeloproliferative & myelodysplastic disorders. Lymphoma
We've one category for lymphoid neoplasm which is the lymphoma in contrast to that of myeloid which has three categories; acute myeloid leukemias, myeloproliferative & myelodysplastic disorders. Lymphoma
Pathology of Hematopoietic and Lymphoid tissue
 Pathology of Hematopoietic and Lymphoid tissue Peerayut Sitthichaiyakul, M.D. Department of Pathology and Forensic Medicine Faculty of Medicine, Naresuan University CONTENTS White blood cells and lymph
Pathology of Hematopoietic and Lymphoid tissue Peerayut Sitthichaiyakul, M.D. Department of Pathology and Forensic Medicine Faculty of Medicine, Naresuan University CONTENTS White blood cells and lymph
University Journal of Surgery and Surgical Specialties
 University Journal of Surgery and Surgical Specialties ISSN 2455-2860 Volume 2 Issue 4 2016 A case of multiple myeloma with cranial nerve palsy SURESHBABU THIRUMAL Department of Neuro Surgery, MADRAS MEDICAL
University Journal of Surgery and Surgical Specialties ISSN 2455-2860 Volume 2 Issue 4 2016 A case of multiple myeloma with cranial nerve palsy SURESHBABU THIRUMAL Department of Neuro Surgery, MADRAS MEDICAL
Lymphoma/CLL 101: Know your Subtype. Dr. David Macdonald Hematologist, The Ottawa Hospital
 Lymphoma/CLL 101: Know your Subtype Dr. David Macdonald Hematologist, The Ottawa Hospital Function of the Lymph System Lymph Node Lymphocytes B-cells develop in the bone marrow and influence the immune
Lymphoma/CLL 101: Know your Subtype Dr. David Macdonald Hematologist, The Ottawa Hospital Function of the Lymph System Lymph Node Lymphocytes B-cells develop in the bone marrow and influence the immune
Pathology of the Hematopoietic System. Case studies
 Pathology of the Hematopoietic System Case studies Shannon Martinson, September 2015 Signalment: 9 yr-old MC cat Case Study 1 History: Cat had been anorexic and developed bleeding in the eyes Physical
Pathology of the Hematopoietic System Case studies Shannon Martinson, September 2015 Signalment: 9 yr-old MC cat Case Study 1 History: Cat had been anorexic and developed bleeding in the eyes Physical
Chapter 13 Lecture Outline
 Chapter 13 Lecture Outline See separate PowerPoint slides for all figures and tables preinserted into PowerPoint without notes. Copyright The McGraw-Hill Companies, Inc. Permission required for reproduction
Chapter 13 Lecture Outline See separate PowerPoint slides for all figures and tables preinserted into PowerPoint without notes. Copyright The McGraw-Hill Companies, Inc. Permission required for reproduction
Prepared by: Dr.Mansour Al-Yazji
 C L L CLL Prepared by: Abd El-Hakeem Abd El-Rahman Abu Naser Ahmed Khamis Abu Warda Ahmed Mohammed Abu Ghaben Bassel Ziad Abu Warda Nedal Mostafa El-Nahhal Dr.Mansour Al-Yazji LEUKEMIA Leukemia is a form
C L L CLL Prepared by: Abd El-Hakeem Abd El-Rahman Abu Naser Ahmed Khamis Abu Warda Ahmed Mohammed Abu Ghaben Bassel Ziad Abu Warda Nedal Mostafa El-Nahhal Dr.Mansour Al-Yazji LEUKEMIA Leukemia is a form
MULTIPLE MYELOMA AND RELATED DISORDERS
 SEVEN MULTIPLE MYELOMA AND RELATED DISORDERS Multiple myeloma Multiple myeloma or myelomatosis is a disease resulting from the proliferation in the bone marrow of a clone of neoplastic cells that are closely
SEVEN MULTIPLE MYELOMA AND RELATED DISORDERS Multiple myeloma Multiple myeloma or myelomatosis is a disease resulting from the proliferation in the bone marrow of a clone of neoplastic cells that are closely
Waldenstrom s Macroglobulinemia
 Waldenstrom s Macroglobulinemia : Introduction Waldenstrom s macroglobulinemia (WM) is a lymphoma, or cancer of the lymphatic system. It occurs in a type of white blood cell called a B-lymphocyte or B-cell,
Waldenstrom s Macroglobulinemia : Introduction Waldenstrom s macroglobulinemia (WM) is a lymphoma, or cancer of the lymphatic system. It occurs in a type of white blood cell called a B-lymphocyte or B-cell,
WBCs Disorders 1. Dr. Nabila Hamdi MD, PhD
 WBCs Disorders 1 Dr. Nabila Hamdi MD, PhD ILOs Compare and contrast ALL, AML, CLL, CML in terms of age distribution, cytogenetics, morphology, immunophenotyping, laboratory diagnosis clinical features
WBCs Disorders 1 Dr. Nabila Hamdi MD, PhD ILOs Compare and contrast ALL, AML, CLL, CML in terms of age distribution, cytogenetics, morphology, immunophenotyping, laboratory diagnosis clinical features
If unqualified, Complete remission is considered to be Haematological complete remission
 Scroll right to see the database codes for Disease status and Response Diagnosis it refers to Disease status or response to treatment AML ALL CML CLL MDS or MD/MPN or acute leukaemia secondary to previous
Scroll right to see the database codes for Disease status and Response Diagnosis it refers to Disease status or response to treatment AML ALL CML CLL MDS or MD/MPN or acute leukaemia secondary to previous
If unqualified, Complete remission is considered to be Haematological complete remission
 Scroll right to see the database codes for Disease status and Response Diagnosis it refers to Disease status or response to treatment AML ALL CML CLL MDS or MD/MPN or acute leukaemia secondary to previous
Scroll right to see the database codes for Disease status and Response Diagnosis it refers to Disease status or response to treatment AML ALL CML CLL MDS or MD/MPN or acute leukaemia secondary to previous
Physiology Unit 3. ADAPTIVE IMMUNITY The Specific Immune Response
 Physiology Unit 3 ADAPTIVE IMMUNITY The Specific Immune Response In Physiology Today The Adaptive Arm of the Immune System Specific Immune Response Internal defense against a specific pathogen Acquired
Physiology Unit 3 ADAPTIVE IMMUNITY The Specific Immune Response In Physiology Today The Adaptive Arm of the Immune System Specific Immune Response Internal defense against a specific pathogen Acquired
7 Omar Abu Reesh. Dr. Ahmad Mansour Dr. Ahmad Mansour
 7 Omar Abu Reesh Dr. Ahmad Mansour Dr. Ahmad Mansour -Leukemia: neoplastic leukocytes circulating in the peripheral bloodstream. -Lymphoma: a neoplastic process in the lymph nodes, spleen or other lymphatic
7 Omar Abu Reesh Dr. Ahmad Mansour Dr. Ahmad Mansour -Leukemia: neoplastic leukocytes circulating in the peripheral bloodstream. -Lymphoma: a neoplastic process in the lymph nodes, spleen or other lymphatic
Lymphatic System Disorders
 Lymphatic System Disorders Lymphomas Malignant neoplasms involving lymphocyte proliferation in lymph nodes Specific causes not identified // Higher risk in adults who received radiation during childhood
Lymphatic System Disorders Lymphomas Malignant neoplasms involving lymphocyte proliferation in lymph nodes Specific causes not identified // Higher risk in adults who received radiation during childhood
Primary Immunodeficiency
 Primary Immunodeficiency DiGeorge Syndrome Severe Combined Immunodeficiency SCID X-Linked Agammaglobulinemia Common variable immunodeficiency (CVID) IgA deficiency Hyper- IgM Syndrome Wiskott-Aldrich syndrome
Primary Immunodeficiency DiGeorge Syndrome Severe Combined Immunodeficiency SCID X-Linked Agammaglobulinemia Common variable immunodeficiency (CVID) IgA deficiency Hyper- IgM Syndrome Wiskott-Aldrich syndrome
Third line of Defense
 Chapter 15 Specific Immunity and Immunization Topics -3 rd of Defense - B cells - T cells - Specific Immunities Third line of Defense Specific immunity is a complex interaction of immune cells (leukocytes)
Chapter 15 Specific Immunity and Immunization Topics -3 rd of Defense - B cells - T cells - Specific Immunities Third line of Defense Specific immunity is a complex interaction of immune cells (leukocytes)
Non-Hodgkin lymphomas (NHLs) Hodgkin lymphoma )HL)
 Hodgkin lymphoma )HL)") Non-Hodgkin lymphomas (NHLs) Hodgkin lymphoma )HL) Lymphoid Neoplasms: 1- non-hodgkin lymphomas (NHLs) 2- Hodgkin lymphoma 3- plasma cell neoplasms Non-Hodgkin lymphomas (NHLs) Acute Lymphoblastic Leukemia/Lymphoma
Non-Hodgkin lymphomas (NHLs) Hodgkin lymphoma )HL) Lymphoid Neoplasms: 1- non-hodgkin lymphomas (NHLs) 2- Hodgkin lymphoma 3- plasma cell neoplasms Non-Hodgkin lymphomas (NHLs) Acute Lymphoblastic Leukemia/Lymphoma
Treatment of Waldenström s Macroglobulinemia Mayo Consensus
 Treatment of Waldenström s Macroglobulinemia Mayo Consensus Scottsdale, Arizona Rochester, Minnesota Jacksonville, Florida Mayo Clinic College of Medicine Mayo Clinic Comprehensive Cancer Center Mayo Clinic
Treatment of Waldenström s Macroglobulinemia Mayo Consensus Scottsdale, Arizona Rochester, Minnesota Jacksonville, Florida Mayo Clinic College of Medicine Mayo Clinic Comprehensive Cancer Center Mayo Clinic
MECHANISMS OF HUMAN DISEASE: LABORATORY SESSIONS LYMPHOMA. April 16, 2008
 MECHANISMS OF HUMAN DISEASE: LABORATORY SESSIONS LYMPHOMA April 16, 2008 FACULTY COPY GOAL: Learn the appearance of normal peripheral blood elements and lymph nodes. Recognize abnormal peripheral blood
MECHANISMS OF HUMAN DISEASE: LABORATORY SESSIONS LYMPHOMA April 16, 2008 FACULTY COPY GOAL: Learn the appearance of normal peripheral blood elements and lymph nodes. Recognize abnormal peripheral blood
Case 3. Ann T. Moriarty,MD
 Case 3 Ann T. Moriarty,MD Case 3 59 year old male with asymptomatic cervical lymphadenopathy. These images are from a fine needle biopsy of a left cervical lymph node. Image 1 Papanicolaou Stained smear,100x.
Case 3 Ann T. Moriarty,MD Case 3 59 year old male with asymptomatic cervical lymphadenopathy. These images are from a fine needle biopsy of a left cervical lymph node. Image 1 Papanicolaou Stained smear,100x.
Molecular Pathology of Lymphoma (Part 1) Rex K.H. Au-Yeung Department of Pathology, HKU
 Rex K.H. Au-Yeung Department of Pathology, HKU") Molecular Pathology of Lymphoma (Part 1) Rex K.H. Au-Yeung Department of Pathology, HKU Lecture outline Time 10:00 11:00 11:15 12:10 12:20 13:15 Content Introduction to lymphoma Review of lymphocyte biology
Molecular Pathology of Lymphoma (Part 1) Rex K.H. Au-Yeung Department of Pathology, HKU Lecture outline Time 10:00 11:00 11:15 12:10 12:20 13:15 Content Introduction to lymphoma Review of lymphocyte biology
2013 AAIM Pathology Workshop
 2013 AAIM Pathology Workshop John Schmieg, M.D., Ph.D. None Disclosures 1 Pathology Workshop Objectives Define the general philosophy of reviewing pathology reports Review the various components of Bone
2013 AAIM Pathology Workshop John Schmieg, M.D., Ph.D. None Disclosures 1 Pathology Workshop Objectives Define the general philosophy of reviewing pathology reports Review the various components of Bone
Instructions for Plasma Cell Disorders (PCD) Post-HCT Data (Form 2116 Revision 3)
 Post-HCT Data (Form 2116 Revision 3)") (Form 2116 Revision 3) This section of the CIBMTR Forms Instruction Manual is intended to be a resource for completing the Plasma Cell Disorders (PCD) Post-HCT Data Form. E-mail comments regarding the
(Form 2116 Revision 3) This section of the CIBMTR Forms Instruction Manual is intended to be a resource for completing the Plasma Cell Disorders (PCD) Post-HCT Data Form. E-mail comments regarding the
Third line of Defense. Topic 8 Specific Immunity (adaptive) (18) 3 rd Line = Prophylaxis via Immunization!
 (18) 3 rd Line = Prophylaxis via Immunization!") Topic 8 Specific Immunity (adaptive) (18) Topics - 3 rd Line of Defense - B cells - T cells - Specific Immunities 1 3 rd Line = Prophylaxis via Immunization! (a) A painting of Edward Jenner depicts a cow
Topic 8 Specific Immunity (adaptive) (18) Topics - 3 rd Line of Defense - B cells - T cells - Specific Immunities 1 3 rd Line = Prophylaxis via Immunization! (a) A painting of Edward Jenner depicts a cow
Laboratory diagnosis of plasma proteins and plasma enzymes
 Laboratory diagnosis of plasma proteins and plasma enzymes Functions of plasma proteins Function: transport humoral immunity enzymes protease inhibitors maintenance of oncotic pressure buffering Example:
Laboratory diagnosis of plasma proteins and plasma enzymes Functions of plasma proteins Function: transport humoral immunity enzymes protease inhibitors maintenance of oncotic pressure buffering Example:
Immunology - Lecture 2 Adaptive Immune System 1
 Immunology - Lecture 2 Adaptive Immune System 1 Book chapters: Molecules of the Adaptive Immunity 6 Adaptive Cells and Organs 7 Generation of Immune Diversity Lymphocyte Antigen Receptors - 8 CD markers
Immunology - Lecture 2 Adaptive Immune System 1 Book chapters: Molecules of the Adaptive Immunity 6 Adaptive Cells and Organs 7 Generation of Immune Diversity Lymphocyte Antigen Receptors - 8 CD markers
Acute Lymphoblastic Leukaemia
 Acute Lymphoblastic Leukaemia Terri Boyer 17 th October 2006 Overview Disease information: Aetiology of ALL proposed theory, contributing factors Symptoms Complications Diagnostic approaches - morphology
Acute Lymphoblastic Leukaemia Terri Boyer 17 th October 2006 Overview Disease information: Aetiology of ALL proposed theory, contributing factors Symptoms Complications Diagnostic approaches - morphology
Management Update: Multiple Myeloma. Presented by Prof. Dr. Khan Abul Kalam Azad Professor of Medicine Dhaka Medical College
 Management Update: Multiple Myeloma Presented by Prof. Dr. Khan Abul Kalam Azad Professor of Medicine Dhaka Medical College Introduction Multiple myeloma - clonal plasma cell neoplasm Monoclonal antibody
Management Update: Multiple Myeloma Presented by Prof. Dr. Khan Abul Kalam Azad Professor of Medicine Dhaka Medical College Introduction Multiple myeloma - clonal plasma cell neoplasm Monoclonal antibody
Multiple Myeloma Early Detection, Diagnosis, and Staging
 Multiple Myeloma Early Detection, Diagnosis, and Staging Detection and Diagnosis Catching cancer early often allows for more treatment options. Some early cancers may have signs and symptoms that can be
Multiple Myeloma Early Detection, Diagnosis, and Staging Detection and Diagnosis Catching cancer early often allows for more treatment options. Some early cancers may have signs and symptoms that can be
2016: Plasma Cell Disorders Pre-HCT Data
 2016: Plasma Cell Disorders Pre-HCT Data Registry Use Only Sequence Number: Date Received: Key Fields CIBMTR Center Number: Date of HCT for which this form is being completed: / / YYYY MM DD HCT type (check
2016: Plasma Cell Disorders Pre-HCT Data Registry Use Only Sequence Number: Date Received: Key Fields CIBMTR Center Number: Date of HCT for which this form is being completed: / / YYYY MM DD HCT type (check
Smoldering Multiple Myeloma. A Case Study
 Smoldering Multiple Myeloma A Case Study Case Presentation 53-Year-Old Male Patient presented for a routine exam No prior history of disease or family history of fhematologic disorders d or malignancies,
Smoldering Multiple Myeloma A Case Study Case Presentation 53-Year-Old Male Patient presented for a routine exam No prior history of disease or family history of fhematologic disorders d or malignancies,
*HSP is a common vasculitis of small vessels with cutaneous & systemic complications. Its etiology is unknown& often follows URTIs.
 BY Introduction The disease is eponymously named after Eduard heinrich Henoch (1820-1910), a German pediatrician, and his teacher Johann Lukas Schonlein (1793-1864), who described it in the 1860s. Cont
BY Introduction The disease is eponymously named after Eduard heinrich Henoch (1820-1910), a German pediatrician, and his teacher Johann Lukas Schonlein (1793-1864), who described it in the 1860s. Cont
What is a hematological malignancy? Hematology and Hematologic Malignancies. Etiology of hematological malignancies. Leukemias
 Hematology and Hematologic Malignancies Cancer of the formed elements of the blood What is a hematological malignancy? A hematologic malignancy is a malignancy (or cancer) of any of the formed elements
Hematology and Hematologic Malignancies Cancer of the formed elements of the blood What is a hematological malignancy? A hematologic malignancy is a malignancy (or cancer) of any of the formed elements
Unit 5 The Human Immune Response to Infection
 Unit 5 The Human Immune Response to Infection Unit 5-page 1 FOM Chapter 21 Resistance and the Immune System: Innate Immunity Preview: In Chapter 21, we will learn about the branch of the immune system
Unit 5 The Human Immune Response to Infection Unit 5-page 1 FOM Chapter 21 Resistance and the Immune System: Innate Immunity Preview: In Chapter 21, we will learn about the branch of the immune system
Extramedullary Presentation of Biclonal IgGk and IgAk Multiple Myeloma
 Extramedullary Presentation of Biclonal IgGk and IgAk * Department of Haematology, Ankara Hospital, ** Department of Haematology, Ankara Numune Hospital, *** Department of Haematology, Medical Faculty,
Extramedullary Presentation of Biclonal IgGk and IgAk * Department of Haematology, Ankara Hospital, ** Department of Haematology, Ankara Numune Hospital, *** Department of Haematology, Medical Faculty,
Plasma Cell Disorders (PCD) Pre-HCT Data
 Pre-HCT Data") Plasma Cell Disorders (PCD) Pre-HCT Data Registry Use Only Sequence Number: Date Received: CIBMTR Center Number: CIBMTR Recipient ID: Date of HCT for which this form is being completed: HCT type: (check
Plasma Cell Disorders (PCD) Pre-HCT Data Registry Use Only Sequence Number: Date Received: CIBMTR Center Number: CIBMTR Recipient ID: Date of HCT for which this form is being completed: HCT type: (check
Lymphatic System. Where s your immunity idol?
 Lymphatic System Where s your immunity idol? Functions of the Lymphatic System Fluid Balance Drains excess fluid from tissues Lymph contains solutes from plasma Fat Absorption Lymphatic system absorbs
Lymphatic System Where s your immunity idol? Functions of the Lymphatic System Fluid Balance Drains excess fluid from tissues Lymph contains solutes from plasma Fat Absorption Lymphatic system absorbs
3.Autoimmunity. a. Self-recognition of all body components. a. Auto-antibody directed against a self antigen.
 3.Autoimmunity I. Introduction A. Introduction 1. Normal individuals do not produce destructive immune responses to their own tissues due to immune tolerance. a. Self-recognition of all body components.
3.Autoimmunity I. Introduction A. Introduction 1. Normal individuals do not produce destructive immune responses to their own tissues due to immune tolerance. a. Self-recognition of all body components.
PLASMA CELL NEOPLASIA. Michael Miller, MD & Ajaz Shawl, MD
 PLASMA CELL NEOPLASIA Michael Miller, MD & Ajaz Shawl, MD Plasma Cell Neoplasia Board Questions Case Presentation Introduction Epidemiology Presentation Diagnosis Laboratory Tests Imaging Differentials
PLASMA CELL NEOPLASIA Michael Miller, MD & Ajaz Shawl, MD Plasma Cell Neoplasia Board Questions Case Presentation Introduction Epidemiology Presentation Diagnosis Laboratory Tests Imaging Differentials
Adaptive Immunity: Humoral Immune Responses
 MICR2209 Adaptive Immunity: Humoral Immune Responses Dr Allison Imrie 1 Synopsis: In this lecture we will review the different mechanisms which constitute the humoral immune response, and examine the antibody
MICR2209 Adaptive Immunity: Humoral Immune Responses Dr Allison Imrie 1 Synopsis: In this lecture we will review the different mechanisms which constitute the humoral immune response, and examine the antibody
Immune system. Aims. Immune system. Lymphatic organs. Inflammation. Natural immune system. Adaptive immune system
 Aims Immune system Lymphatic organs Inflammation Natural immune system Adaptive immune system Major histocompatibility complex (MHC) Disorders of the immune system 1 2 Immune system Lymphoid organs Immune
Aims Immune system Lymphatic organs Inflammation Natural immune system Adaptive immune system Major histocompatibility complex (MHC) Disorders of the immune system 1 2 Immune system Lymphoid organs Immune
Southern Derbyshire Shared Care Pathology Guidelines. MGUS (Monoclonal Gammopathy of Undetermined Significance)
") Southern Derbyshire Shared Care Pathology Guidelines MGUS (Monoclonal Gammopathy of Undetermined Significance) Purpose of guideline This guideline provides information about the risk stratification of
Southern Derbyshire Shared Care Pathology Guidelines MGUS (Monoclonal Gammopathy of Undetermined Significance) Purpose of guideline This guideline provides information about the risk stratification of
Malignant bone tumors. Incidence Myeloma 45% Osteosarcoma 24% Chondrosarcoma 12% Lyphoma 8% Ewing s Sarcoma 7%
 Malignant bone tumors Incidence Myeloma 45% Osteosarcoma 24% Chondrosarcoma 12% Lyphoma 8% Ewing s Sarcoma 7% Commonest primary bone sarcoma is osteosarcoma X ray Questions to ask 1. Solitary or Multiple
Malignant bone tumors Incidence Myeloma 45% Osteosarcoma 24% Chondrosarcoma 12% Lyphoma 8% Ewing s Sarcoma 7% Commonest primary bone sarcoma is osteosarcoma X ray Questions to ask 1. Solitary or Multiple
Corrigenda. WHO Classification of Tumours of Haematopoietic and Lymphoid Tissues (revised 4th edition): corrections made in second print run
: corrections made in second print run") Corrigenda WHO Classification of Tumours of Haematopoietic and Lymphoid Tissues (revised 4th edition): corrections made in second print run In addition to corrections of minor typographical errors, corrections
Corrigenda WHO Classification of Tumours of Haematopoietic and Lymphoid Tissues (revised 4th edition): corrections made in second print run In addition to corrections of minor typographical errors, corrections
The Paraprotein. Evaluating Paraproteinemia. Conditions Associated with PP. Paraprotein Structure
 Evaluating Paraproteinemia Jeffrey Wolf, MD, Director Thomas Martin, MD, Associate Director Myeloma Institute University of California, San Francisco The Paraprotein An abnormal immunoglobulin or part
Evaluating Paraproteinemia Jeffrey Wolf, MD, Director Thomas Martin, MD, Associate Director Myeloma Institute University of California, San Francisco The Paraprotein An abnormal immunoglobulin or part
Evaluating Paraproteinemia
 Evaluating Paraproteinemia Jeffrey Wolf, MD, Director Thomas Martin, MD, Associate Director Myeloma Institute University of California, San Francisco The Paraprotein An abnormal immunoglobulin or part
Evaluating Paraproteinemia Jeffrey Wolf, MD, Director Thomas Martin, MD, Associate Director Myeloma Institute University of California, San Francisco The Paraprotein An abnormal immunoglobulin or part
Done By : WESSEN ADNAN BUTHAINAH AL-MASAEED
 Done By : WESSEN ADNAN BUTHAINAH AL-MASAEED Acute Myeloid Leukemia Firstly we ll start with this introduction then enter the title of the lecture, so be ready and let s begin by the name of Allah : We
Done By : WESSEN ADNAN BUTHAINAH AL-MASAEED Acute Myeloid Leukemia Firstly we ll start with this introduction then enter the title of the lecture, so be ready and let s begin by the name of Allah : We
Pediatric Oncology. Vlad Radulescu, MD
 Pediatric Oncology Vlad Radulescu, MD Objectives Review the epidemiology of childhood cancer Discuss the presenting signs and symptoms, general treatment principles and overall prognosis of the most common
Pediatric Oncology Vlad Radulescu, MD Objectives Review the epidemiology of childhood cancer Discuss the presenting signs and symptoms, general treatment principles and overall prognosis of the most common
2014 Pearson Education, Inc. Exposure to pathogens naturally activates the immune system. Takes days to be effective Pearson Education, Inc.
 The innate immune interact with the adaptive immune system 1. Damage to skin causes bleeding = bradykinin activated, resulting in inflammation 2. Dendritic phagocytose pathogens Adaptive immunity 4. Dendritic
The innate immune interact with the adaptive immune system 1. Damage to skin causes bleeding = bradykinin activated, resulting in inflammation 2. Dendritic phagocytose pathogens Adaptive immunity 4. Dendritic
Myelodysplastic syndrome (MDS) & Myeloproliferative neoplasms
 & Myeloproliferative neoplasms") Myelodysplastic syndrome (MDS) & Myeloproliferative neoplasms Myelodysplastic syndrome (MDS) A multipotent stem cell that can differentiate into any of the myeloid lineage cells (RBCs, granulocytes, megakaryocytes)
Myelodysplastic syndrome (MDS) & Myeloproliferative neoplasms Myelodysplastic syndrome (MDS) A multipotent stem cell that can differentiate into any of the myeloid lineage cells (RBCs, granulocytes, megakaryocytes)
CHAPTER:4 LEUKEMIA. BY Mrs. K.SHAILAJA., M. PHARM., LECTURER DEPT OF PHARMACY PRACTICE, SRM COLLEGE OF PHARMACY 8/12/2009
 LEUKEMIA CHAPTER:4 1 BY Mrs. K.SHAILAJA., M. PHARM., LECTURER DEPT OF PHARMACY PRACTICE, SRM COLLEGE OF PHARMACY Leukemia A group of malignant disorders affecting the blood and blood-forming tissues of
LEUKEMIA CHAPTER:4 1 BY Mrs. K.SHAILAJA., M. PHARM., LECTURER DEPT OF PHARMACY PRACTICE, SRM COLLEGE OF PHARMACY Leukemia A group of malignant disorders affecting the blood and blood-forming tissues of
Amyloidosis and Waldenström s Macroglobulinemia
 Amyloidosis and Waldenström s Macroglobulinemia Morie A. Gertz, Giampaolo Merlini, and Steven P. Treon Primary systemic amyloidosis is an immunoglobulin light chain disorder that is 1/5th as common as
Amyloidosis and Waldenström s Macroglobulinemia Morie A. Gertz, Giampaolo Merlini, and Steven P. Treon Primary systemic amyloidosis is an immunoglobulin light chain disorder that is 1/5th as common as
What are bacteria? Microbes are microscopic(bacteria, viruses, prions, & some fungi etc.) How do the sizes of our cells, bacteria and viruses compare?
 How do the sizes of our cells, bacteria and viruses compare?") 7.1 Microbes, pathogens and you Chp. 7 Lymphatic System & Immunity The interaction between microbes and humans? Microbes are very abundant in the environment and as well as in and on our bodies GOOD: We
7.1 Microbes, pathogens and you Chp. 7 Lymphatic System & Immunity The interaction between microbes and humans? Microbes are very abundant in the environment and as well as in and on our bodies GOOD: We
WHY IS THIS IMPORTANT?
 CHAPTER 16 THE ADAPTIVE IMMUNE RESPONSE WHY IS THIS IMPORTANT? The adaptive immune system protects us from many infections The adaptive immune system has memory so we are not infected by the same pathogen
CHAPTER 16 THE ADAPTIVE IMMUNE RESPONSE WHY IS THIS IMPORTANT? The adaptive immune system protects us from many infections The adaptive immune system has memory so we are not infected by the same pathogen
Monoclonal Gammopathies and the Kidney. Tibor Nádasdy, MD The Ohio State University, Columbus, OH
 Monoclonal Gammopathies and the Kidney Tibor Nádasdy, MD The Ohio State University, Columbus, OH Monoclonal gammopathy of renal significance (MGRS) Biopsies at OSU (n=475) between 2007 and 2016 AL or AH
Monoclonal Gammopathies and the Kidney Tibor Nádasdy, MD The Ohio State University, Columbus, OH Monoclonal gammopathy of renal significance (MGRS) Biopsies at OSU (n=475) between 2007 and 2016 AL or AH
Lymphomas and multiple myeloma 12/23/2018 1
 60 Lymphomas and multiple myeloma 12/23/2018 1 Lymphomas Lymphoma is cancer of the lymphatic system. Lymphomas are subdivided into two main categories: Hodgkin's lymphoma (HL) and non- Hodgkin's lymphoma
60 Lymphomas and multiple myeloma 12/23/2018 1 Lymphomas Lymphoma is cancer of the lymphatic system. Lymphomas are subdivided into two main categories: Hodgkin's lymphoma (HL) and non- Hodgkin's lymphoma
Disease Morbidities 2; IgM related disorders, renal, hyperviscosity & Cryos
 Disease Morbidities 2; IgM related disorders, renal, hyperviscosity & Cryos Josephine MI Vos, MD St Antonius Ziekenhuis Utrecht/Nieuwegein Patientendag Waldenstrom workshop 2016 9th International Workshop
Disease Morbidities 2; IgM related disorders, renal, hyperviscosity & Cryos Josephine MI Vos, MD St Antonius Ziekenhuis Utrecht/Nieuwegein Patientendag Waldenstrom workshop 2016 9th International Workshop
POEMS syndrome. This Infosheet explains what POEMS syndrome is, how it is diagnosed and how it is treated and managed.
 POEMS syndrome This Infosheet explains what POEMS syndrome is, how it is diagnosed and how it is treated and managed. What is POEMS syndrome? POEMS syndrome is a rare type of plasma cell disorder that
POEMS syndrome This Infosheet explains what POEMS syndrome is, how it is diagnosed and how it is treated and managed. What is POEMS syndrome? POEMS syndrome is a rare type of plasma cell disorder that
Cell-mediated response (what type of cell is activated and what gets destroyed?)
") The Immune System Reading Guide (Chapter 43) Name Per 1. The immune response in animals can be divided into innate immunity and adaptive immunity. As an overview, complete this figure indicating the divisions
The Immune System Reading Guide (Chapter 43) Name Per 1. The immune response in animals can be divided into innate immunity and adaptive immunity. As an overview, complete this figure indicating the divisions
all of the above the ability to impart long term memory adaptive immunity all of the above bone marrow none of the above
 1. (3 points) Immediately after a pathogen enters the body, it faces the cells and soluble proteins of the innate immune system. Which of the following are characteristics of innate immunity? a. inflammation
1. (3 points) Immediately after a pathogen enters the body, it faces the cells and soluble proteins of the innate immune system. Which of the following are characteristics of innate immunity? a. inflammation
B. Environmental Factors. a. The major risk factor to papillary thyroid cancer is exposure to ionizing radiation, during the first 2 decades of life.
 B. Environmental Factors. a. The major risk factor to papillary thyroid cancer is exposure to ionizing radiation, during the first 2 decades of life. b. Deficiency of dietary iodine: - Is linked with a
B. Environmental Factors. a. The major risk factor to papillary thyroid cancer is exposure to ionizing radiation, during the first 2 decades of life. b. Deficiency of dietary iodine: - Is linked with a
Bisphosphonates in the Management of. Myeloma Bone Disease
 Bisphosphonates in the Management of Myeloma Bone Disease James R. Berenson, MD Medical & Scientific Director Institute for Myeloma & Bone Cancer Research Los Angeles, CA Myeloma Bone Disease Myeloma cells
Bisphosphonates in the Management of Myeloma Bone Disease James R. Berenson, MD Medical & Scientific Director Institute for Myeloma & Bone Cancer Research Los Angeles, CA Myeloma Bone Disease Myeloma cells
Successful Treatment of Immunoglobulin D Myeloma by Bortezomib and Dexamethasone Therapy
 CASE REPORT Successful Treatment of Immunoglobulin D Myeloma by Bortezomib and Dexamethasone Therapy Naohiro Sekiguchi 1, Naoki Takezako 1, Akihisa Nagata 1, Miyuki Wagatsuma 2, Satoshi Noto 1, Kazuaki
CASE REPORT Successful Treatment of Immunoglobulin D Myeloma by Bortezomib and Dexamethasone Therapy Naohiro Sekiguchi 1, Naoki Takezako 1, Akihisa Nagata 1, Miyuki Wagatsuma 2, Satoshi Noto 1, Kazuaki
Blood and Immune system Acquired Immunity
 Blood and Immune system Acquired Immunity Immunity Acquired (Adaptive) Immunity Defensive mechanisms include : 1) Innate immunity (Natural or Non specific) 2) Acquired immunity (Adaptive or Specific) Cell-mediated
Blood and Immune system Acquired Immunity Immunity Acquired (Adaptive) Immunity Defensive mechanisms include : 1) Innate immunity (Natural or Non specific) 2) Acquired immunity (Adaptive or Specific) Cell-mediated
Requirements in the Development of an Autoimmune Disease Amino Acids in the Shared Epitope
 + T cell MHC/self-peptide MHC/Vβ Induction of + T H 1 mediated autoimmunity: A paradigm for the pathogenesis of rheumatoid arthritis, multiple sclerosis and type I diabetes APC Activated autoreactive +
+ T cell MHC/self-peptide MHC/Vβ Induction of + T H 1 mediated autoimmunity: A paradigm for the pathogenesis of rheumatoid arthritis, multiple sclerosis and type I diabetes APC Activated autoreactive +
Hematology Unit Lab 1 Review Material
 Hematology Unit Lab 1 Review Material - 2018 Objectives Laboratory instructors: 1. Assist students during lab session Students: 1. Review the introductory material 2. Study the case histories provided
Hematology Unit Lab 1 Review Material - 2018 Objectives Laboratory instructors: 1. Assist students during lab session Students: 1. Review the introductory material 2. Study the case histories provided
A clinical syndrome, composed mainly of:
 Nephritic syndrome We will discuss: 1)Nephritic syndrome: -Acute postinfectious (poststreptococcal) GN -IgA nephropathy -Hereditary nephritis 2)Rapidly progressive GN (RPGN) A clinical syndrome, composed
Nephritic syndrome We will discuss: 1)Nephritic syndrome: -Acute postinfectious (poststreptococcal) GN -IgA nephropathy -Hereditary nephritis 2)Rapidly progressive GN (RPGN) A clinical syndrome, composed
Tracking Disease Status for Multiple Myeloma
 Tracking Disease Status for Multiple Myeloma This appendix is intended to provide additional resources when determining: Best response to line of therapy pre-transplant; Disease Status at the Last Evaluation
Tracking Disease Status for Multiple Myeloma This appendix is intended to provide additional resources when determining: Best response to line of therapy pre-transplant; Disease Status at the Last Evaluation
Rory McCulloch. Specialty Trainee Haematology Royal Devon & Exeter Hospital
 Rory McCulloch Specialty Trainee Haematology Royal Devon & Exeter Hospital Anaemia 1 Haematological disorders Anaemia 2 Non-haematological disorders Substrates: Iron, folate, vitamin B12 Red cell mass
Rory McCulloch Specialty Trainee Haematology Royal Devon & Exeter Hospital Anaemia 1 Haematological disorders Anaemia 2 Non-haematological disorders Substrates: Iron, folate, vitamin B12 Red cell mass
Chapter 24 The Immune System
 Chapter 24 The Immune System The Immune System Layered defense system The skin and chemical barriers The innate and adaptive immune systems Immunity The body s ability to recognize and destroy specific
Chapter 24 The Immune System The Immune System Layered defense system The skin and chemical barriers The innate and adaptive immune systems Immunity The body s ability to recognize and destroy specific
FBC CASES Vernon Louw Clinical Haematology 2010
 FBC CASES Vernon Louw Clinical Haematology 2010 FOR EACH OF THE FOLLOWING PATIENTS, SELECT THE MOST LIKELY FINDING FROM THE ANALYSIS OF THE PERIPHERAL BLOOD. A patient with infectious mononucleosis. A
FBC CASES Vernon Louw Clinical Haematology 2010 FOR EACH OF THE FOLLOWING PATIENTS, SELECT THE MOST LIKELY FINDING FROM THE ANALYSIS OF THE PERIPHERAL BLOOD. A patient with infectious mononucleosis. A
Pathology of Complement Mediated Renal Disease
 Pathology of Complement Mediated Renal Disease Mariam Priya Alexander, MD Associate Professor of Pathology GN Symposium Hong Kong Society of Nephrology July 8 th, 2017 2017 MFMER slide-1 The complement
Pathology of Complement Mediated Renal Disease Mariam Priya Alexander, MD Associate Professor of Pathology GN Symposium Hong Kong Society of Nephrology July 8 th, 2017 2017 MFMER slide-1 The complement
SWOG ONCOLOGY RESEARCH PROFESSIONAL (ORP) MANUAL RESPONSE ASSESSMENT MYELOMA CHAPTER 11C REVISED: SEPTEMBER 2016
 MANUAL RESPONSE ASSESSMENT MYELOMA CHAPTER 11C REVISED: SEPTEMBER 2016") MYELOMA Quantitative Markers-Myeloma Assessment Quantitative markers are biochemicals that are recorded in tests on body fluids such as serum and urine. Applicable Disease Sites The myeloma disease site
MYELOMA Quantitative Markers-Myeloma Assessment Quantitative markers are biochemicals that are recorded in tests on body fluids such as serum and urine. Applicable Disease Sites The myeloma disease site