Dr.Sivaramakrishnan PICU KKCTH
|
|
|
- Jonas Harris
- 5 years ago
- Views:
Transcription
1 Dr.Sivaramakrishnan PICU KKCTH
2 CASE 1 11/2 year old female child Known wheezer on intermittent bronchodilators Admitted with h/o cough for 2 days Increased work of breathing for 1 day
3 Afebrile/sick looking Severe respiratory distress (RR=80/min) Bilateral wheeze/scr/icr/ssr INVESTIGATIONS Mild anaemia / leucocytosis / negative CRP Normal RFT

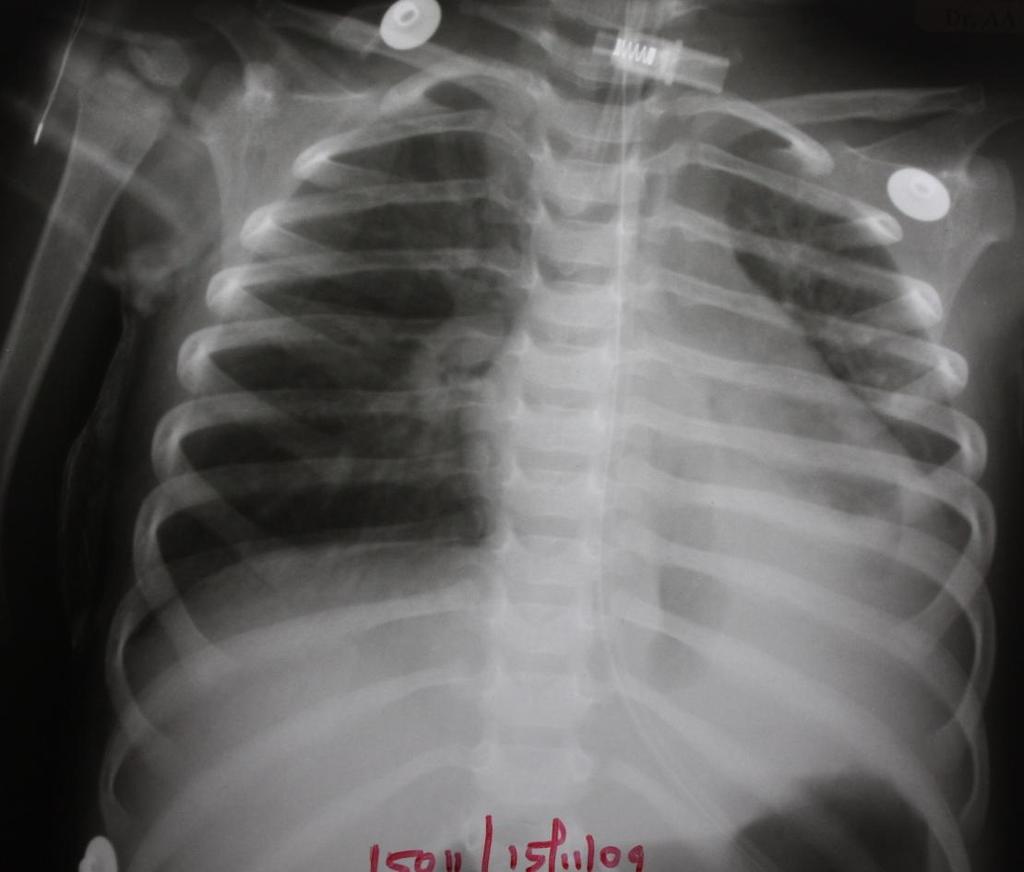
4 IN ER CXRay showed bilateral increased BVM With haziness in left lower zone
5 Child continuously nebulised IV hydrocort/mgso4/sc terbutaline given Wheeze persisted Distress worsened shifted to PICU
6 Nebulization's continued Child worsened further - intubated ABG PH-7.16/PCO2-86/PO2-179/HCO3-30/SPO2-99% Terbutaline & MgSO4 infusions started Did not improve despite various ventilator manipulations

7 CX-RAY Child worsened further

8 ICD placed

9 Repeat X-Ray: No improvement PH-6.8 /PCO2-199 /PO2-51 /HCO3-34 /SPO2-54%
10 FOREIGN BODY versus recalcitrant asthma BRONCHOSCOPY PLANNED


11 BINGO BRONCHOSCOPY FOREIGN BODY in rt. Main bronchus CULPRIT-thoor dal Edema of bronchial mucosa seen & purulent secretions suctioned out
12 Dramatic improvement ABG-PH-7.4/PO2-84/PCO2-48/HCO3-29/SPO2-97% Infusions gradually tapered off Nebulisations frequency decreased Extubated on 5 th day of ICU stay Unremarkable post extubation ICU stay
13 Post extubation


14 Post ICU stay

15 2 yr old male child Known wheezer since early infancy Admitted with h/o cough 4 days Increased work of breathing & fever 2 days No H/S/O FB aspiration On intermittent nebulisations
16 Irritable/sick looking Tachypnoeic (RR-54/min) Febrile/haemodynamically stable B/L extensive wheeze
17 continuosly nebulised IV hydrocort/mgso4/sc terbutaline given INVESTIGATIONS N counts with mild anemia/positive CRP Normal liver enzymes & RFT

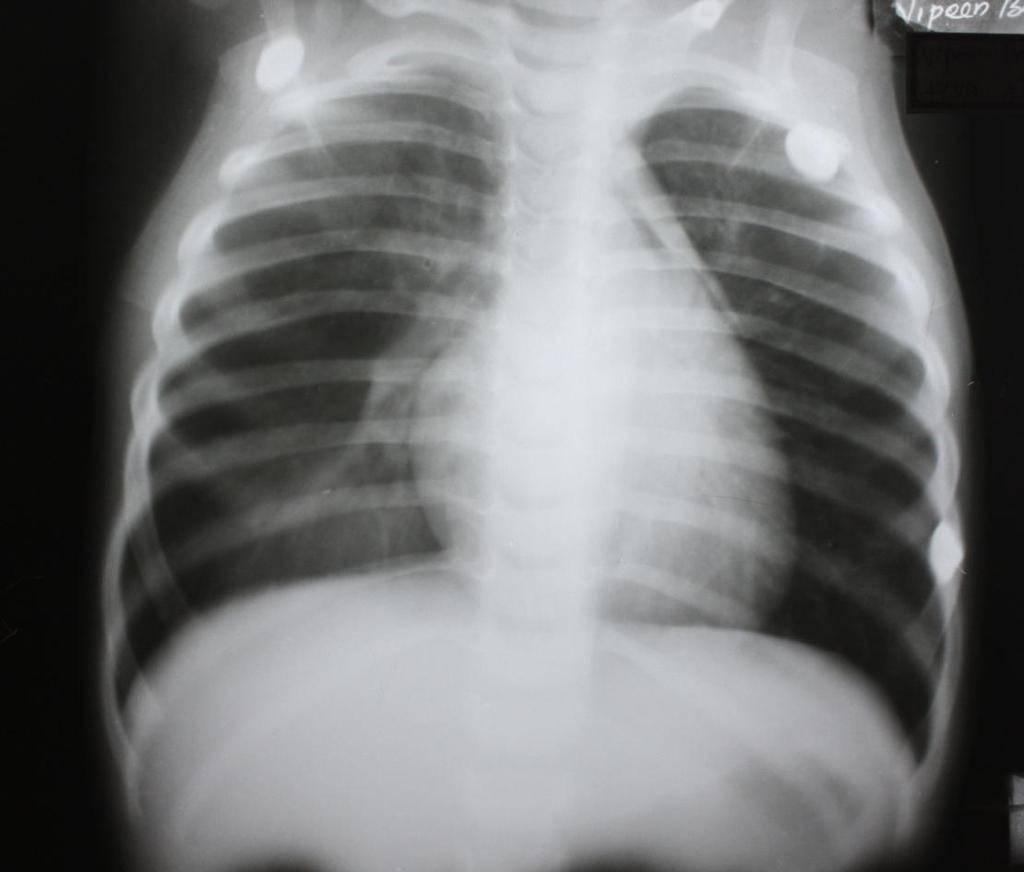
18 CX-RAY IN ER Due to worsening distress shifted to PICU
19 Child had persistent wheezing O/E: sick,very irritable, tachypnoeic ICR/SCR/SSR Decreased breath sounds in LT B/L crackles & wheeze Nebulisations continued Hydrocortisone continued


20 Following day Marginal improvement Cont to be tachypneic Cxray rpt
21 BRONCHOSCOPY LT bronchial system:both lingula & UL bronchi are filled with mucus cast suggesting PLASTIC BRONCHITIS RT bronchial system normal Thorough bronchial lavage done Cast removed by repeated saline wash

22 BRONCHIAL CAST
23 Child improved dramatically Nebulisations decreased N acetyl cysteine nebulisations added Steroids continued Wheezing settled Child shifted out next day for further care
24 POST BRONCHOSCOPY

25 In HDU had resp distress again, urgent bronchoscopy done again revealed a cast similar to the first one - removed intoto and thorough lavage given. Improved and shifted to ward.
26 Child discharged on inhaled bronchodilators Reviewed 1 week later No symptoms of recurrence Doing well
27 Formation of obstructive bronchial plugs or casts of thick, tenacious mucus associated with involvement of one or more lobes or even associated entire lung may collapse. FIBRINOUS/PSEUDOMEMBRANOUS/HOFFMAN S BRONCHIAL CROUP First described as early as 1902
28 AGE affects all ages Youngest reported being 3 wks PRECIPITATING FACTORS commonly associated with hyper reactive airway disease (asthma, pneumonia), cystic fibrosis, bronchiectasis, chronic bronchitis, inhalation of aeroallergens, CHD, bronchopulmonary aspergillosis or may sometimes be IDIOPATHIC
29 MODERATE INFLAMMATORY CHANGES in bronchial wall most constantly associated. May include congestion and edema of bronchial wall or sometimes haemorrage and infiltration by polymorphonuclear leukocytes, eosinophils or lymphocytes
30 Signs of infection (fever, cough, dyspnea etc) h/s/o underlying disease often present wheeze localised or bilateral Decreased air entry in collapsed side Resp distress Adults sometimes cough out cast Mimics FB/status asthmaticus
31 CX-RAY one or more areas of collapse No predilection to any part of lung Recurrent attacks may lead to fibrosis & bronchiectasis BRONCHOSCOPY diagnostic and therapeutic
32 Cylindrical / adherent to bronchial wall Pale grayish or greenish white Peculiarly tough & viscid with smooth surface 2 types of cast INFLAMMATORY : made up of fibrin & esonophil infiltrates. Usually in underlying bronchial disease ACELLULAR : mainly mucin with little fibrin, no inflammatory infiltrates. Usually in CHD SEER ET AL.
33 MUCUS PLUG Small plugs Causes segmental collapse Not very tight Can be expectorated PLASTIC BRONCHITIS Large plugs Collapse of entire lobe/lung Tightly adherent Retained rather than expectorated
34 Beta agonists Steroids beneficial but yet uncertain NAC (breaks disulfide bonds in mucin thus lowering their viscosity) Aerosolised urokinase / heparin have been tried Aerosolised tpa (fibrin enhanced conversion of plasminogen to plasmin which initiates local fibrinolysis. Used in casts with high fibrin content. No definitive data, so can be tried in refractory cases) Chest physiotherapy BRONCHOSCOPY
35 FOLLOW UP Recurrence very common No strict pattern of recurrence No preventive therapy Bronchoscopy immediately if child comes with recurrence PROGNOSIS good
36 ALL THAT WHEEZES IS NOT ASTHMA High index of suspicion to any child presenting with acute respiratory distress with wheeze refractory to conventional medical therapy with unusual radiographic picture consider BRONCH SCOPY
37 sleigh johnson & E.G sita lumsden THORAX 1960 J.Y park,a.a elshemi EUR.RESPIR J,1996 John m.costeldo,david steinhom,pediatrics 2002 D.Vijayasekaran,N.G.gowrishankar IP 2004

38 THANK YOU
Shifting Atelectasis: A sign of foreign body aspiration in a pediatric patient
 Shifting Atelectasis: A sign of foreign body aspiration in a pediatric patient Diana L Mark, RRT Pediatric Clinical Specialist Respiratory Care Wesley Children s Hospital Discuss when foreign body aspiration
Shifting Atelectasis: A sign of foreign body aspiration in a pediatric patient Diana L Mark, RRT Pediatric Clinical Specialist Respiratory Care Wesley Children s Hospital Discuss when foreign body aspiration
ASTHMA. Epidemiology. Pathophysiology. Diagnosis. IAP UG Teaching slides
 BRONCHIAL ASTHMA ASTHMA Epidemiology Pathophysiology Diagnosis 2 CHILDHOOD ASTHMA Childhood bronchial asthma is characterized by Airway obstruction which is reversible Airway inflammation Airway hyper
BRONCHIAL ASTHMA ASTHMA Epidemiology Pathophysiology Diagnosis 2 CHILDHOOD ASTHMA Childhood bronchial asthma is characterized by Airway obstruction which is reversible Airway inflammation Airway hyper
PULMONARY MEDICINE BOARD REVIEW. Financial Conflicts of Interest. Question #1: Question #1 (Cont.): None. Christopher H. Fanta, M.D.
: None. Christopher H. Fanta, M.D.") PULMONARY MEDICINE BOARD REVIEW Christopher H. Fanta, M.D. Pulmonary and Critical Care Division Brigham and Women s Hospital Partners Asthma Center Harvard Medical School Financial Conflicts of Interest
PULMONARY MEDICINE BOARD REVIEW Christopher H. Fanta, M.D. Pulmonary and Critical Care Division Brigham and Women s Hospital Partners Asthma Center Harvard Medical School Financial Conflicts of Interest
Quality Care Innovation lead clinician for integrated respiratory service georges ng* man kwong
 Working in partnership Quality Care Innovation lead clinician for integrated respiratory service georges ng* man kwong chest physician pronounced ning qualified 1990 chief clinical information officer
Working in partnership Quality Care Innovation lead clinician for integrated respiratory service georges ng* man kwong chest physician pronounced ning qualified 1990 chief clinical information officer
Objectives. Case Presentation. Respiratory Emergencies
 Respiratory Emergencies Objectives Describe how to assess airway and breathing, including interpreting information from the PAT and ABCDEs. Differentiate between respiratory distress, respiratory failure,
Respiratory Emergencies Objectives Describe how to assess airway and breathing, including interpreting information from the PAT and ABCDEs. Differentiate between respiratory distress, respiratory failure,
MAYA RAMAGOPAL M.D. DIVISION OF PULMONOLOGY & CYSTIC FIBROSIS CENTER
 MAYA RAMAGOPAL M.D. DIVISION OF PULMONOLOGY & CYSTIC FIBROSIS CENTER 16 year old female with h/o moderate persistent asthma presents to the ED after 6 hours of difficulty breathing, cough, and wheezing
MAYA RAMAGOPAL M.D. DIVISION OF PULMONOLOGY & CYSTIC FIBROSIS CENTER 16 year old female with h/o moderate persistent asthma presents to the ED after 6 hours of difficulty breathing, cough, and wheezing
62 year old man with a cough! Dr. Aflah Sadikeen Consultant Respiratory Physician Colombo
 62 year old man with a cough! Dr. Aflah Sadikeen Consultant Respiratory Physician Colombo History Mr.KS, a 62 year-old, has been feeling unwell - Worsening cough for the last 5 days - Feels out of breath
62 year old man with a cough! Dr. Aflah Sadikeen Consultant Respiratory Physician Colombo History Mr.KS, a 62 year-old, has been feeling unwell - Worsening cough for the last 5 days - Feels out of breath
A 31-year-old female with a rare cause of recurrent lower lobar collapses
 Radhika Banka, Dayle Terrington, Ajay V. Kamath radhika.banka@gmail.com Dept of Respiratory Medicine, Norfolk and Norwich University Hospital, Norwich, UK. A 31-year-old female with a rare cause of recurrent
Radhika Banka, Dayle Terrington, Ajay V. Kamath radhika.banka@gmail.com Dept of Respiratory Medicine, Norfolk and Norwich University Hospital, Norwich, UK. A 31-year-old female with a rare cause of recurrent
Total collapse of the lung in aspergillosis
 Thorax (1965), 20, 118. Total collapse of the lung in aspergillosis R. H. ELLIS From the Gloucestershire Royal Hospital, Pulmonary aspergillosis can be divided conveniently into two main types, allergic
Thorax (1965), 20, 118. Total collapse of the lung in aspergillosis R. H. ELLIS From the Gloucestershire Royal Hospital, Pulmonary aspergillosis can be divided conveniently into two main types, allergic
RESPIRATORY BLOCK. Bronchial Asthma. Dr. Maha Arafah Department of Pathology KSU
 RESPIRATORY BLOCK Bronchial Asthma Dr. Maha Arafah Department of Pathology KSU marafah@ksu.edu.sa Jan 2018 Objectives Define asthma (BA) Know the two types of asthma 1. Extrinsic or atopic allergic 2.
RESPIRATORY BLOCK Bronchial Asthma Dr. Maha Arafah Department of Pathology KSU marafah@ksu.edu.sa Jan 2018 Objectives Define asthma (BA) Know the two types of asthma 1. Extrinsic or atopic allergic 2.
GOALS AND INSTRUCTIONAL OBJECTIVES
 October 4-7, 2004 Respiratory GOALS: GOALS AND INSTRUCTIONAL OBJECTIVES By the end of the week, the first quarter student will have an in-depth understanding of the diagnoses listed under Primary Diagnoses
October 4-7, 2004 Respiratory GOALS: GOALS AND INSTRUCTIONAL OBJECTIVES By the end of the week, the first quarter student will have an in-depth understanding of the diagnoses listed under Primary Diagnoses
Chronic Cough An Unusual Presentation. Dr Sourabh Jain Department of Respiratory Medicine
 Chronic Cough An Unusual Presentation Dr Sourabh Jain Department of Respiratory Medicine A 72 years old male from Pune, non smoker, with no co-morbidities Chief Complaints : Chronic cough with scanty mucoid
Chronic Cough An Unusual Presentation Dr Sourabh Jain Department of Respiratory Medicine A 72 years old male from Pune, non smoker, with no co-morbidities Chief Complaints : Chronic cough with scanty mucoid
an inflammation of the bronchial tubes
 BRONCHITIS DEFINITION Bronchitis is an inflammation of the bronchial tubes (or bronchi), which are the air passages that extend from the trachea into the small airways and alveoli. Triggers may be infectious
BRONCHITIS DEFINITION Bronchitis is an inflammation of the bronchial tubes (or bronchi), which are the air passages that extend from the trachea into the small airways and alveoli. Triggers may be infectious
Transient pulmonary infiltrations in cystic fibrosis due to allergic aspergillosis
 Thorax (1965), 20, 385 Transient pulmonary infiltrations in cystic fibrosis due to allergic aspergillosis MARGARET MEARNS, WINIFRED YOUNG, AND JOHN BATTEN From the Queen Elizabeth Hospital, Hackney, and
Thorax (1965), 20, 385 Transient pulmonary infiltrations in cystic fibrosis due to allergic aspergillosis MARGARET MEARNS, WINIFRED YOUNG, AND JOHN BATTEN From the Queen Elizabeth Hospital, Hackney, and
MRSA pneumonia mucus plug burden and the difficult airway
 Case report Crit Care Shock (2016) 19:54-58 MRSA pneumonia mucus plug burden and the difficult airway Ann Tsung, Brian T. Wessman An 80-year-old female with a past medical history of chronic obstructive
Case report Crit Care Shock (2016) 19:54-58 MRSA pneumonia mucus plug burden and the difficult airway Ann Tsung, Brian T. Wessman An 80-year-old female with a past medical history of chronic obstructive
RESPIRATORY EMERGENCIES. Michael Waters MD April 2004
 RESPIRATORY EMERGENCIES Michael Waters MD April 2004 ASTHMA Asthma is a chronic inflammatory disease of the airways with variable or reversible airway obstruction Characterized by increased sensitivity
RESPIRATORY EMERGENCIES Michael Waters MD April 2004 ASTHMA Asthma is a chronic inflammatory disease of the airways with variable or reversible airway obstruction Characterized by increased sensitivity
A Place For Airway Clearance Therapy In Today s Healthcare Environment
 A Place For Airway Clearance Therapy In Today s Healthcare Environment Michigan Society for Respiratory Care 2015 Fall Conference K. James Ehlen, MD October 6, 2015 Objectives Describe patients who will
A Place For Airway Clearance Therapy In Today s Healthcare Environment Michigan Society for Respiratory Care 2015 Fall Conference K. James Ehlen, MD October 6, 2015 Objectives Describe patients who will
Lecture Notes. Chapter 3: Asthma
 Lecture Notes Chapter 3: Asthma Objectives Define asthma and status asthmaticus List the potential causes of asthma attacks Describe the effect of asthma attacks on lung function List the clinical features
Lecture Notes Chapter 3: Asthma Objectives Define asthma and status asthmaticus List the potential causes of asthma attacks Describe the effect of asthma attacks on lung function List the clinical features
Asthma - Chronic. Presentations of asthma Cough Wheeze Breathlessness Chest tightness
 Asthma - Chronic Definition of asthma Chronic inflammatory disease of the airways 3 components: o Reversible and variable airflow obstruction o Airway hyper-responsiveness to stimuli o Inflammation of
Asthma - Chronic Definition of asthma Chronic inflammatory disease of the airways 3 components: o Reversible and variable airflow obstruction o Airway hyper-responsiveness to stimuli o Inflammation of
Pulmonary Pearls. Medical Pearls. Case 1: Case 1 (cont.): Case 1: What is the Most Likely Diagnosis? Case 1 (cont.):
: Case 1: What is the Most Likely Diagnosis? Case 1 (cont.):") Pulmonary Pearls Christopher H. Fanta, MD Pulmonary and Critical Care Division Brigham and Women s Hospital Partners Asthma Center Harvard Medical School Medical Pearls Definition: Medical fact that is
Pulmonary Pearls Christopher H. Fanta, MD Pulmonary and Critical Care Division Brigham and Women s Hospital Partners Asthma Center Harvard Medical School Medical Pearls Definition: Medical fact that is
2/12/2015. ASTHMA & COPD The Yin &Yang. Asthma General Information. Asthma General Information
 ASTHMA & COPD The Yin &Yang Arizona State Association of Physician Assistants March 6, 2015 Sedona, Arizona Randy D. Danielsen, PhD, PA-C, DFAAPA Dean & Professor A.T. Still University Asthma General Information
ASTHMA & COPD The Yin &Yang Arizona State Association of Physician Assistants March 6, 2015 Sedona, Arizona Randy D. Danielsen, PhD, PA-C, DFAAPA Dean & Professor A.T. Still University Asthma General Information
Basic mechanisms disturbing lung function and gas exchange
 Basic mechanisms disturbing lung function and gas exchange Blagoi Marinov, MD, PhD Pathophysiology Department, Medical University of Plovdiv Respiratory system 1 Control of breathing Structure of the lungs
Basic mechanisms disturbing lung function and gas exchange Blagoi Marinov, MD, PhD Pathophysiology Department, Medical University of Plovdiv Respiratory system 1 Control of breathing Structure of the lungs
Paramedic Rounds. Pre-Hospital Continuous Positive Airway Pressure (CPAP)
") Paramedic Rounds Pre-Hospital Continuous Positive Airway Pressure (CPAP) Morgan Hillier MD Class of 2011 Dr. Mike Peddle Assistant Medical Director SWORBHP Objectives Outline evidence for pre-hospital
Paramedic Rounds Pre-Hospital Continuous Positive Airway Pressure (CPAP) Morgan Hillier MD Class of 2011 Dr. Mike Peddle Assistant Medical Director SWORBHP Objectives Outline evidence for pre-hospital
DIFFICULT ASTHMA. Dr. Prathyusha Dr. S.Balasubramanian KKCTH
 DIFFICULT ASTHMA Dr. Prathyusha Dr. S.Balasubramanian KKCTH CASE SUMMARY 11 yr old girl, Neyveli Treated as moderate persistent asthma x 5 years On Seroflo [ LABA + steroid ] 250 2 puffs BD and intermittent
DIFFICULT ASTHMA Dr. Prathyusha Dr. S.Balasubramanian KKCTH CASE SUMMARY 11 yr old girl, Neyveli Treated as moderate persistent asthma x 5 years On Seroflo [ LABA + steroid ] 250 2 puffs BD and intermittent
Chronic obstructive pulmonary disease
 Chronic obstructive pulmonary disease By: Dr. Fatima Makee AL-Hakak () University of kerbala College of nursing Out lines What is the? Overview Causes of Symptoms of What's the difference between and asthma?
Chronic obstructive pulmonary disease By: Dr. Fatima Makee AL-Hakak () University of kerbala College of nursing Out lines What is the? Overview Causes of Symptoms of What's the difference between and asthma?
Bronchospasm & SOB. Kim Kilmurray Senior Clinical Teaching Fellow
 Bronchospasm & SOB Kim Kilmurray Senior Clinical Teaching Fellow LEARNING OBJECTIVES Perform a comprehensive respiratory examination & link clinical signs to underlying pathology Identify the spectrum
Bronchospasm & SOB Kim Kilmurray Senior Clinical Teaching Fellow LEARNING OBJECTIVES Perform a comprehensive respiratory examination & link clinical signs to underlying pathology Identify the spectrum
Respiratory Medicine. Some pet peeves and other random topics. Kyle Perrin
 Respiratory Medicine Some pet peeves and other random topics Kyle Perrin Overview 1. Acute asthma Severity assessment and management 2. Acute COPD NIV and other management 3. Respiratory problems in the
Respiratory Medicine Some pet peeves and other random topics Kyle Perrin Overview 1. Acute asthma Severity assessment and management 2. Acute COPD NIV and other management 3. Respiratory problems in the
Respiratory Medicine
 Respiratory Medicine This document is based on the handout from the Medicine for Finals course. The notes provided here summarise key aspects, focusing on areas that are popular in clinical examinations.
Respiratory Medicine This document is based on the handout from the Medicine for Finals course. The notes provided here summarise key aspects, focusing on areas that are popular in clinical examinations.
Diagnosis, Treatment and Management of Asthma
 Diagnosis, Treatment and Management of Asthma Asthma is a complex disorder characterized by variable and recurring symptoms, airflow obstruction, bronchial hyperresponsiveness, and an underlying inflammation.
Diagnosis, Treatment and Management of Asthma Asthma is a complex disorder characterized by variable and recurring symptoms, airflow obstruction, bronchial hyperresponsiveness, and an underlying inflammation.
CONGENITAL TRACHEAL STENOSIS PRESENTING IN THE NEONATAL PERIOD
 CONGENITAL TRACHEAL STENOSIS PRESENTING IN THE NEONATAL PERIOD J Reiter, C Springer, E Erez Israel Society of Pediatric Pulmonolgy Jerusalem, September 2 nd, 2015 Topics Case Presentation Surgical Intervention
CONGENITAL TRACHEAL STENOSIS PRESENTING IN THE NEONATAL PERIOD J Reiter, C Springer, E Erez Israel Society of Pediatric Pulmonolgy Jerusalem, September 2 nd, 2015 Topics Case Presentation Surgical Intervention
1. What is delayed sequence intubation? Can it be used for severe Asthma exacerbation? 2. What about pregnancy and Asthma is so important?
 Chapter 073 Asthma Episode Overview 1. 10 different causes of a wheeze. 2. List 8 risk factors for death from asthma 3. List 6 objective findings of severe asthma 4. 10 therapies for an acute severe asthma
Chapter 073 Asthma Episode Overview 1. 10 different causes of a wheeze. 2. List 8 risk factors for death from asthma 3. List 6 objective findings of severe asthma 4. 10 therapies for an acute severe asthma
Epiglottitis. Bronchitis. Bronchiolitis. Pneumonia. Croup syndrome. Miss. kamlah 2
 Miss. kamlah 1 Epiglottitis. Bronchitis. Bronchiolitis. Pneumonia. Croup syndrome. Miss. kamlah 2 Acute Epiglottitis Is an infection of the epiglottis, the long narrow structure that closes off the glottis
Miss. kamlah 1 Epiglottitis. Bronchitis. Bronchiolitis. Pneumonia. Croup syndrome. Miss. kamlah 2 Acute Epiglottitis Is an infection of the epiglottis, the long narrow structure that closes off the glottis
CPAP. Pre-Hospital Treatment Using The Respironics Whisperflow CPAP Device. Charlottesville Albemarle Rescue Squad - CPAP
 CPAP Pre-Hospital Treatment Using The Respironics Whisperflow CPAP Device CPAP What Is It? C ontinuous P ositive A irway P ressure Anatomy Review Anatomy Review Anatomy Review Alveoli Anatomy Review Chest
CPAP Pre-Hospital Treatment Using The Respironics Whisperflow CPAP Device CPAP What Is It? C ontinuous P ositive A irway P ressure Anatomy Review Anatomy Review Anatomy Review Alveoli Anatomy Review Chest
Outpatient Guideline for the Diagnosis and Management of Asthma
 Outpatient Guideline for the Diagnosis and Management of Asthma Initial Visit Follow-Up Visits See page 2 Asthma Diagnosis See page 3 Classifying Asthma Severity and Initiating Treatment See pages 2 and
Outpatient Guideline for the Diagnosis and Management of Asthma Initial Visit Follow-Up Visits See page 2 Asthma Diagnosis See page 3 Classifying Asthma Severity and Initiating Treatment See pages 2 and
Exacerbations. Ronald Dahl, Aarhus University Hospital, Denmark
 1st WAO Allied Health Session - Asthma: Diagnosi Exacerbations Ronald Dahl, Aarhus University Hospital, Denmark The health professional that care for patients with asthma exacerbation must be able to Identificafy
1st WAO Allied Health Session - Asthma: Diagnosi Exacerbations Ronald Dahl, Aarhus University Hospital, Denmark The health professional that care for patients with asthma exacerbation must be able to Identificafy
Asthma. - A chronic inflammatory disorder which causes recurrent episodes of wheezing, breathlessness, cough and chest tightness.
 Obstructive diseases Asthma - A chronic inflammatory disorder which causes recurrent episodes of wheezing, breathlessness, cough and chest tightness. - Characterized by Intermittent and reversible (the
Obstructive diseases Asthma - A chronic inflammatory disorder which causes recurrent episodes of wheezing, breathlessness, cough and chest tightness. - Characterized by Intermittent and reversible (the
Respiratory Diseases and Disorders
 Chapter 9 Respiratory Diseases and Disorders Anatomy and Physiology Chest, lungs, and conducting airways Two parts: Upper respiratory system consists of nose, mouth, sinuses, pharynx, and larynx Lower
Chapter 9 Respiratory Diseases and Disorders Anatomy and Physiology Chest, lungs, and conducting airways Two parts: Upper respiratory system consists of nose, mouth, sinuses, pharynx, and larynx Lower
OSAMA A. ABDULMAJID, ABDELMOMEN M. EBEID, MOHAMED M. MOTAWEH, and IBRAHIM S. KLEIBO
 Aspirated foreign bodies in the tracheobronchial tree: report of 250 cases Thorax (1976), 31, 635. OSAMA A. ABDULMAJID, ABDELMOMEN M. EBEID, MOHAMED M. MOTAWEH, and IBRAHIM S. KLEIBO Thoracic Surgical
Aspirated foreign bodies in the tracheobronchial tree: report of 250 cases Thorax (1976), 31, 635. OSAMA A. ABDULMAJID, ABDELMOMEN M. EBEID, MOHAMED M. MOTAWEH, and IBRAHIM S. KLEIBO Thoracic Surgical
Acute respiratory failure
 Rita Williams, NP-C, PA PeaceHealth Medical Group Pulmonary & Critical Care Acute respiratory failure Ventilation/perfusion mismatching Most common cause of hypoxemia Normal is 1:1 ratio or 1 Ventilation
Rita Williams, NP-C, PA PeaceHealth Medical Group Pulmonary & Critical Care Acute respiratory failure Ventilation/perfusion mismatching Most common cause of hypoxemia Normal is 1:1 ratio or 1 Ventilation
HealthPartners Care Coordination Clinical Care Planning and Resource Guide ASTHMA
 The following evidence based guideline was used in developing this clinical care guide: National Institute of Health (NIH National Heart, Lung, and Blood Institute (NHLBI) and American Academy of Allergy,
The following evidence based guideline was used in developing this clinical care guide: National Institute of Health (NIH National Heart, Lung, and Blood Institute (NHLBI) and American Academy of Allergy,
Problem Based Learning Session. Mr Robinson is a 67 year old man. He visits the GP as he has had a cough and fever for 5 days.
 Problem Based Learning Session Mr Robinson is a 67 year old man. He visits the GP as he has had a cough and fever for 5 days. The GP takes a history from him and examines his chest. Over the left base
Problem Based Learning Session Mr Robinson is a 67 year old man. He visits the GP as he has had a cough and fever for 5 days. The GP takes a history from him and examines his chest. Over the left base
Significance. Asthma Definition. Focus on Asthma
 Focus on Asthma (Relates to Chapter 29, Nursing Management: Obstructive Pulmonary Diseases, in the textbook) Asthma Definition Chronic inflammatory disorder of airways Causes airway hyperresponsiveness
Focus on Asthma (Relates to Chapter 29, Nursing Management: Obstructive Pulmonary Diseases, in the textbook) Asthma Definition Chronic inflammatory disorder of airways Causes airway hyperresponsiveness
Session Guidelines. This is a 15 minute webinar session for CNC physicians and staff
 Respiratory Disease Session Guidelines This is a 15 minute webinar session for CNC physicians and staff CNC holds webinars monthly to address topics related to risk adjustment documentation and coding
Respiratory Disease Session Guidelines This is a 15 minute webinar session for CNC physicians and staff CNC holds webinars monthly to address topics related to risk adjustment documentation and coding
COUGH. Jim Reid University of Otago Medical School Dunedin, New Zealand
 COUGH Jim Reid University of Otago Medical School Dunedin, New Zealand COUGH One of five most common presentations in general practice Remember the law of probability Common things occur commonly But
COUGH Jim Reid University of Otago Medical School Dunedin, New Zealand COUGH One of five most common presentations in general practice Remember the law of probability Common things occur commonly But
MUCINAC 600 Tablets (Acetylcysteine)
") Published on: 10 Jul 2014 MUCINAC 600 Tablets (Acetylcysteine) Composition MUCINAC 600 Tablets Each effervescent tablet contains: Acetylcysteine 600 mg Dosage Form Oral Tablet Pharmacology Pharmacodynamics
Published on: 10 Jul 2014 MUCINAC 600 Tablets (Acetylcysteine) Composition MUCINAC 600 Tablets Each effervescent tablet contains: Acetylcysteine 600 mg Dosage Form Oral Tablet Pharmacology Pharmacodynamics
RESPIRATORY REHABILITATION
 RESPIRATORY REHABILITATION By: Dr. Fatima Makee AL-Hakak University of kerbala College of nursing CHEST PHYSIOTHERAPY Chest physiotherapy (CPT) includes: 1.Postural drainage. 2.Chest percussion and vibration.
RESPIRATORY REHABILITATION By: Dr. Fatima Makee AL-Hakak University of kerbala College of nursing CHEST PHYSIOTHERAPY Chest physiotherapy (CPT) includes: 1.Postural drainage. 2.Chest percussion and vibration.
Printed copies of this document may not be up to date, obtain the most recent version from
 Children s Acute Transport Service Clinical Guidelines Acute Severe Asthma Document Control Information Author E Randle Author Position CATS Consultant Document Owner E Polke Document Owner Position Co-ordinator
Children s Acute Transport Service Clinical Guidelines Acute Severe Asthma Document Control Information Author E Randle Author Position CATS Consultant Document Owner E Polke Document Owner Position Co-ordinator
Simulation 1: Two Year-Old Child in Respiratory Distress
 Simulation 1: Two Year-Old Child in Respiratory Distress Opening Scenario (Links to Section 1) You are the respiratory therapist in a 300 bed community hospital working the evening shift. At 8:30 PM you
Simulation 1: Two Year-Old Child in Respiratory Distress Opening Scenario (Links to Section 1) You are the respiratory therapist in a 300 bed community hospital working the evening shift. At 8:30 PM you
Chronic obstructive lung disease. Dr/Rehab F.Gwada
 Chronic obstructive lung disease Dr/Rehab F.Gwada Obstructive lung diseases Problem is in the expiratory phase Lung disease Restrictive lung disease Restriction may be with, or within the chest wall Problem
Chronic obstructive lung disease Dr/Rehab F.Gwada Obstructive lung diseases Problem is in the expiratory phase Lung disease Restrictive lung disease Restriction may be with, or within the chest wall Problem
Chapter 10 Respiratory System J00-J99. Presented by: Jesicca Andrews
 Chapter 10 Respiratory System J00-J99 Presented by: Jesicca Andrews 1 Respiratory System 2 Respiratory Infections A respiratory infection cannot be assumed from a laboratory report alone; physician concurrence
Chapter 10 Respiratory System J00-J99 Presented by: Jesicca Andrews 1 Respiratory System 2 Respiratory Infections A respiratory infection cannot be assumed from a laboratory report alone; physician concurrence
1 Chapter 13 Respiratory Emergencies 2 Respiratory Distress Patients often complain about. Shortness of breath Symptom of many different Cause can be
 1 Chapter 13 Respiratory Emergencies 2 Respiratory Distress Patients often complain about. Shortness of breath Symptom of many different Cause can be difficult to determine. Even for physician in hospital
1 Chapter 13 Respiratory Emergencies 2 Respiratory Distress Patients often complain about. Shortness of breath Symptom of many different Cause can be difficult to determine. Even for physician in hospital
11.3 RESPIRATORY SYSTEM DISORDERS
 11.3 RESPIRATORY SYSTEM DISORDERS TONSILLITIS Infection of the tonsils Bacterial or viral Symptoms: red and swollen tonsils, sore throat, fever, swollen glands Treatment: surgically removed Tonsils: in
11.3 RESPIRATORY SYSTEM DISORDERS TONSILLITIS Infection of the tonsils Bacterial or viral Symptoms: red and swollen tonsils, sore throat, fever, swollen glands Treatment: surgically removed Tonsils: in
AFCH NEUROMUSCULAR DISORDERS (NMD) PROTOCOL
 PROTOCOL") AFCH NEUROMUSCULAR DISORDERS (NMD) PROTOCOL A. Definition of Therapy: 1. Cough machine: 4 sets of 5 breaths with a goal of I:E pressures approximately the same of 30-40. Inhale time = 1 second, exhale
AFCH NEUROMUSCULAR DISORDERS (NMD) PROTOCOL A. Definition of Therapy: 1. Cough machine: 4 sets of 5 breaths with a goal of I:E pressures approximately the same of 30-40. Inhale time = 1 second, exhale
Unconscious exchange of air between lungs and the external environment Breathing
 Respiration Unconscious exchange of air between lungs and the external environment Breathing Two types External Exchange of carbon dioxide and oxygen between the environment and the organism Internal Exchange
Respiration Unconscious exchange of air between lungs and the external environment Breathing Two types External Exchange of carbon dioxide and oxygen between the environment and the organism Internal Exchange
Asthma Care in the Emergency Department Clinical Practice Guideline
 Asthma Care in the Emergency Department Clinical Practice Guideline Inclusion: 1) Children 2 years of age or older with a prior history of wheezing, and 2) Children less than 2 years of age with likely
Asthma Care in the Emergency Department Clinical Practice Guideline Inclusion: 1) Children 2 years of age or older with a prior history of wheezing, and 2) Children less than 2 years of age with likely
Paediatric Wheeze and pneumonia. RCH Asthma RCH bronchiolitis RCH pneumonia Dr S Rajapaksa
 Paediatric Wheeze and pneumonia RCH Asthma RCH bronchiolitis RCH pneumonia Dr S Rajapaksa Case Charlotte is a 2 ½ year old who presents to ED with shortness of breath and wheeze. She had been picked up
Paediatric Wheeze and pneumonia RCH Asthma RCH bronchiolitis RCH pneumonia Dr S Rajapaksa Case Charlotte is a 2 ½ year old who presents to ED with shortness of breath and wheeze. She had been picked up
Knowledge Translation and Emergency Medicine. Eddy Lang Jeremy Grimshaw Michael Brown
 Knowledge Translation and Emergency Medicine Eddy Lang Jeremy Grimshaw Michael Brown Knowledge Translation The exchange, synthesis and application of research evidence within a complex system of relationships
Knowledge Translation and Emergency Medicine Eddy Lang Jeremy Grimshaw Michael Brown Knowledge Translation The exchange, synthesis and application of research evidence within a complex system of relationships
5/26/10. Upper Airway Emergencies Identify life threatening upper airway infections Recognize and treat anaphylaxis and airway burns in children
 Andi Marmor, MD Assistant Clinical Professor, Pediatrics University of California, San Francisco Upper Airway Emergencies Identify life threatening upper airway infections Recognize and treat anaphylaxis
Andi Marmor, MD Assistant Clinical Professor, Pediatrics University of California, San Francisco Upper Airway Emergencies Identify life threatening upper airway infections Recognize and treat anaphylaxis
FOREIGN BODY ASPIRATION in children. Dr. Xayyavong Bouathongthip, M.D Emergency department, children s hospital
 FOREIGN BODY ASPIRATION in children Dr. Xayyavong Bouathongthip, M.D Emergency department, children s hospital How common is choking? About 3,000 people die/year from choking Figure remained unchanged
FOREIGN BODY ASPIRATION in children Dr. Xayyavong Bouathongthip, M.D Emergency department, children s hospital How common is choking? About 3,000 people die/year from choking Figure remained unchanged
Pulmonary Pathophysiology
 Pulmonary Pathophysiology 1 Reduction of Pulmonary Function 1. Inadequate blood flow to the lungs hypoperfusion 2. Inadequate air flow to the alveoli - hypoventilation 2 Signs and Symptoms of Pulmonary
Pulmonary Pathophysiology 1 Reduction of Pulmonary Function 1. Inadequate blood flow to the lungs hypoperfusion 2. Inadequate air flow to the alveoli - hypoventilation 2 Signs and Symptoms of Pulmonary
Respiratory Management in Pediatrics
 Respiratory Management in Pediatrics Children s Hospital Omaha Critical Care Transport Sue Holmer RN, C-NPT Objectives Examine the differences between the pediatric and adults airways. Recognize respiratory
Respiratory Management in Pediatrics Children s Hospital Omaha Critical Care Transport Sue Holmer RN, C-NPT Objectives Examine the differences between the pediatric and adults airways. Recognize respiratory
COPD COPD. C - Chronic O - Obstructive P - Pulmonary D - Disease OBJECTIVES
 COPD C - Chronic O - Obstructive P - Pulmonary D - Disease 1 OBJECTIVES Following this presentation the participant should be able to demonstrate understanding of chronic lung disease by successful completion
COPD C - Chronic O - Obstructive P - Pulmonary D - Disease 1 OBJECTIVES Following this presentation the participant should be able to demonstrate understanding of chronic lung disease by successful completion
June 2013 Pulmonary Case of the Month: Diagnosis Makes a Difference. Lewis J. Wesselius, MD 1 Henry D. Tazelaar, MD 2
 June 2013 Pulmonary Case of the Month: Diagnosis Makes a Difference Lewis J. Wesselius, MD 1 Henry D. Tazelaar, MD 2 Departments of Pulmonary Medicine 1 and Laboratory Medicine and Pathology 2 Mayo Clinic
June 2013 Pulmonary Case of the Month: Diagnosis Makes a Difference Lewis J. Wesselius, MD 1 Henry D. Tazelaar, MD 2 Departments of Pulmonary Medicine 1 and Laboratory Medicine and Pathology 2 Mayo Clinic
Bronchitis. Anatomy of the Lungs The lungs allow us to fill our blood with oxygen. The oxygen we breathe is absorbed into our blood in the lungs.
 Bronchitis Introduction Bronchitis is an inflammation of the bronchial tubes, the airways that carry air to the lungs. It causes shortness of breath, wheezing and chest tightness as well as a cough that
Bronchitis Introduction Bronchitis is an inflammation of the bronchial tubes, the airways that carry air to the lungs. It causes shortness of breath, wheezing and chest tightness as well as a cough that
Hospital-acquired Pneumonia
 Hospital-acquired Pneumonia Hospital-acquired pneumonia (HAP) Pneumonia that occurs at least 2 days after hospital admission. The second most common and the leading cause of death due to hospital-acquired
Hospital-acquired Pneumonia Hospital-acquired pneumonia (HAP) Pneumonia that occurs at least 2 days after hospital admission. The second most common and the leading cause of death due to hospital-acquired
Chronic lung diseases in children Simple choice 1. Finger clubbing is not characteristic for: a) Diffuse bronchiectasis b) Cystic fibrosis c)
 Diffuse bronchiectasis b) Cystic fibrosis c)") Chronic lung diseases in children Simple choice 1. Finger clubbing is not characteristic for: a) Diffuse bronchiectasis b) Cystic fibrosis c) Bronchiolitis obliterans d) Complicated acute pneumonia e)
Chronic lung diseases in children Simple choice 1. Finger clubbing is not characteristic for: a) Diffuse bronchiectasis b) Cystic fibrosis c) Bronchiolitis obliterans d) Complicated acute pneumonia e)
Wheezy? Easy Peasy! The Emergent Management of Asthma & Bronchiolitis. Maneesha Agarwal MD Assistant Professor of Pediatrics & Emergency Medicine
 Wheezy? Easy Peasy! The Emergent Management of Asthma & Bronchiolitis Maneesha Agarwal MD Assistant Professor of Pediatrics & Emergency Medicine Asthma Defined National Asthma Education and Prevention
Wheezy? Easy Peasy! The Emergent Management of Asthma & Bronchiolitis Maneesha Agarwal MD Assistant Professor of Pediatrics & Emergency Medicine Asthma Defined National Asthma Education and Prevention
Eosinophilic lung diseases
 Eosinophilic lung diseases Chai Gin Tsen Department of Respiratory and Critical Care Medicine Tan Tock Seng Hospital The eyes do not see what the mind does not know Not very common A high index of suspicion
Eosinophilic lung diseases Chai Gin Tsen Department of Respiratory and Critical Care Medicine Tan Tock Seng Hospital The eyes do not see what the mind does not know Not very common A high index of suspicion
Case Scenarios. Dr Shrikanth Srinivasan MD,DNB,FNB,EDIC. Consultant, Critical Care Medicine Medanta, The Medicity
 Case Scenarios Dr Shrikanth Srinivasan MD,DNB,FNB,EDIC Consultant, Critical Care Medicine Medanta, The Medicity Case 1 A 36 year male with cirrhosis and active GI bleeding is intubated to protect his airway,
Case Scenarios Dr Shrikanth Srinivasan MD,DNB,FNB,EDIC Consultant, Critical Care Medicine Medanta, The Medicity Case 1 A 36 year male with cirrhosis and active GI bleeding is intubated to protect his airway,
Simulation 01: Two Year-Old Child in Respiratory Distress (Croup)
") Simulation 01: Two Year-Old Child in Respiratory Distress (Croup) Flow Chart Opening Scenario 2 year-old child in respiratory distress - assess Section 1 Type: IG audible stridor with insp + exp wheezing;
Simulation 01: Two Year-Old Child in Respiratory Distress (Croup) Flow Chart Opening Scenario 2 year-old child in respiratory distress - assess Section 1 Type: IG audible stridor with insp + exp wheezing;
Asthma Management in ICU. by DrGary Au From KWH
 Asthma Management in ICU by DrGary Au From KWH Overview of Asthma Pathophysiology Therapeutic options Medical treatment NPPV Mechanical ventilation Salvage therapy ~ 235 million people worldwide were affected
Asthma Management in ICU by DrGary Au From KWH Overview of Asthma Pathophysiology Therapeutic options Medical treatment NPPV Mechanical ventilation Salvage therapy ~ 235 million people worldwide were affected
Cystic Fibrosis Complications ANDRES ZIRLINGER, MD STANFORD UNIVERSITY MEDICAL CENTER MARCH 3, 2012
 Cystic Fibrosis Complications ANDRES ZIRLINGER, MD STANFORD UNIVERSITY MEDICAL CENTER MARCH 3, 2012 INTRODUCTION PNEUMOTHORAX HEMOPTYSIS RESPIRATORY FAILURE Cystic Fibrosis Autosomal Recessive Genetically
Cystic Fibrosis Complications ANDRES ZIRLINGER, MD STANFORD UNIVERSITY MEDICAL CENTER MARCH 3, 2012 INTRODUCTION PNEUMOTHORAX HEMOPTYSIS RESPIRATORY FAILURE Cystic Fibrosis Autosomal Recessive Genetically
COPD: A Renewed Focus. Disclosures
 COPD: A Renewed Focus Heath Latham, MD Assistant Professor Division of Pulmonary and Critical Care Medicine Disclosures No Business Interests No Consulting No Speakers Bureau No Off Label Use to Discuss
COPD: A Renewed Focus Heath Latham, MD Assistant Professor Division of Pulmonary and Critical Care Medicine Disclosures No Business Interests No Consulting No Speakers Bureau No Off Label Use to Discuss
PIDS AND RESPIRATORY DISORDERS
 PRIMARY IMMUNODEFICIENCIES PIDS AND RESPIRATORY DISORDERS PIDS AND RESPIRATORY DISORDERS 1 PRIMARY IMMUNODEFICIENCIES ABBREVIATIONS COPD CT MRI IG PID Chronic obstructive pulmonary disease Computed tomography
PRIMARY IMMUNODEFICIENCIES PIDS AND RESPIRATORY DISORDERS PIDS AND RESPIRATORY DISORDERS 1 PRIMARY IMMUNODEFICIENCIES ABBREVIATIONS COPD CT MRI IG PID Chronic obstructive pulmonary disease Computed tomography
Emergency Department Guideline. Asthma
 Emergency Department Guideline Inclusion criteria: Patients 2 years old with: o Known history of asthma or wheezing responsive to bronchodilators presenting to the ED with cough, wheeze, shortness of breath,
Emergency Department Guideline Inclusion criteria: Patients 2 years old with: o Known history of asthma or wheezing responsive to bronchodilators presenting to the ED with cough, wheeze, shortness of breath,
Sample Case Study. The patient was a 77-year-old female who arrived to the emergency room on
 Sample Case Study The patient was a 77-year-old female who arrived to the emergency room on February 25 th with a chief complaint of shortness of breath and a deteriorating pulmonary status along with
Sample Case Study The patient was a 77-year-old female who arrived to the emergency room on February 25 th with a chief complaint of shortness of breath and a deteriorating pulmonary status along with
Bronchiectasis in Adults - Suspected
 Bronchiectasis in Adults - Suspected Clinical symptoms which may indicate bronchiectasis for patients Take full respiratory history including presenting symptoms, past medical & family history Factors
Bronchiectasis in Adults - Suspected Clinical symptoms which may indicate bronchiectasis for patients Take full respiratory history including presenting symptoms, past medical & family history Factors
a. Will not suppress respiratory drive in acute asthma
 Status Asthmaticus & COPD with Respiratory Failure - Key Points M.J. Betzner MD FRCPc - NYEMU Toronto 2018 Overview This talk is about the sickest of the sick patients presenting with severe or near death
Status Asthmaticus & COPD with Respiratory Failure - Key Points M.J. Betzner MD FRCPc - NYEMU Toronto 2018 Overview This talk is about the sickest of the sick patients presenting with severe or near death
Disease spectrum. IPA Invasive pulmonary aspergillosis
 Aspergillus & ABPA Disease spectrum IPA Invasive pulmonary aspergillosis ABPA ABPA pathophysiology conidia of Aspergillus trapped in mucous and narrowed airways of asthmatics/cf germinate to form hyphae
Aspergillus & ABPA Disease spectrum IPA Invasive pulmonary aspergillosis ABPA ABPA pathophysiology conidia of Aspergillus trapped in mucous and narrowed airways of asthmatics/cf germinate to form hyphae
Case Study #2. Case Study #1 cont 9/28/2011. CAPA 2011 Christy Wilson PA C. LH is 78 yowf with PMHx of metz breast CA presents
 Case Study #1 CAPA 2011 Christy Wilson PA C 46 yo female presents with community acquired PNA (CAP). Her condition worsened and she was transferred to the ICU and placed on mechanical ventilation. Describe
Case Study #1 CAPA 2011 Christy Wilson PA C 46 yo female presents with community acquired PNA (CAP). Her condition worsened and she was transferred to the ICU and placed on mechanical ventilation. Describe
ADULT ASTHMA GUIDE SUMMARY. This summary provides busy health professionals with key guidance for assessing and treating adult asthma.
 ADULT ASTHMA GUIDE SUMMARY This summary provides busy health professionals with key guidance for assessing and treating adult asthma. Its source document Asthma and Respiratory Foundation NZ Adult Asthma
ADULT ASTHMA GUIDE SUMMARY This summary provides busy health professionals with key guidance for assessing and treating adult asthma. Its source document Asthma and Respiratory Foundation NZ Adult Asthma
Respiratory Disease. Dr Amal Damrah consultant Neonatologist and Paediatrician
 Respiratory Disease Dr Amal Damrah consultant Neonatologist and Paediatrician Signs and Symptoms of Respiratory Diseases Cardinal Symptoms Cough Sputum Hemoptysis Dyspnea Wheezes Chest pain Signs and Symptoms
Respiratory Disease Dr Amal Damrah consultant Neonatologist and Paediatrician Signs and Symptoms of Respiratory Diseases Cardinal Symptoms Cough Sputum Hemoptysis Dyspnea Wheezes Chest pain Signs and Symptoms
PEDIATRIC ACUTE ASTHMA SCORE (P.A.A.S.) GUIDELINES. >97% 94% to 96% 91%-93% <90% Moderate to severe expiratory wheeze
 GUIDELINES. >97% 94% to 96% 91%-93% <90% Moderate to severe expiratory wheeze") Inclusion: Children experiencing acute asthma exacerbation 24 months to 18 years of age with a diagnosis of asthma Patients with a previous history of asthma (Consider differential diagnosis for infants
Inclusion: Children experiencing acute asthma exacerbation 24 months to 18 years of age with a diagnosis of asthma Patients with a previous history of asthma (Consider differential diagnosis for infants
PEDIATRIC RESPIRATORY ILLNESS MADE SIMPLE
 Copyright 2012 Joel Berezow, MD and The Pediatrics for Emergency Physicians Network All rights reserved. Duplication in whole or in part, or electronic transmission in any form, is prohibited THE PEDIATRICS
Copyright 2012 Joel Berezow, MD and The Pediatrics for Emergency Physicians Network All rights reserved. Duplication in whole or in part, or electronic transmission in any form, is prohibited THE PEDIATRICS
Community Acquired Pneumonia. Abdullah Alharbi, MD, FCCP
 Community Acquired Pneumonia Abdullah Alharbi, MD, FCCP A 68 y/ male presented to the ED with SOB and productive coughing for 2 days. Reports poor oral intake since onset due to nausea and intermittent
Community Acquired Pneumonia Abdullah Alharbi, MD, FCCP A 68 y/ male presented to the ED with SOB and productive coughing for 2 days. Reports poor oral intake since onset due to nausea and intermittent
Pulmonary Emergencies. Emergency Medicine Clerkship Lecture Series Primary Author: David Gordon, MD Edited: Darren Manthey, MD 4/2012
 Pulmonary Emergencies Emergency Medicine Clerkship Lecture Series Primary Author: David Gordon, MD Edited: Darren Manthey, MD 4/2012 Learning Objectives Review commonly encountered pulmonary emergencies
Pulmonary Emergencies Emergency Medicine Clerkship Lecture Series Primary Author: David Gordon, MD Edited: Darren Manthey, MD 4/2012 Learning Objectives Review commonly encountered pulmonary emergencies
The Respiratory System
 130 20 The Respiratory System 1. Define important words in this chapter 2. Explain the structure and function of the respiratory system 3. Discuss changes in the respiratory system due to aging 4. Discuss
130 20 The Respiratory System 1. Define important words in this chapter 2. Explain the structure and function of the respiratory system 3. Discuss changes in the respiratory system due to aging 4. Discuss
Mucomist Respirator Solution, Acetylcysteine USP 200 mg/ ml Solution for inhalation (not for injection)
") Mucomist Respirator Solution, Acetylcysteine USP 200 mg/ ml Solution for inhalation (not for injection) DESCRIPTION Mucomist Respirator Solution is a derivative of the amino acid, cysteine. It acts mostly
Mucomist Respirator Solution, Acetylcysteine USP 200 mg/ ml Solution for inhalation (not for injection) DESCRIPTION Mucomist Respirator Solution is a derivative of the amino acid, cysteine. It acts mostly
Acute Respiratory Infections
 T e c h n i c a l S e m i n a r s Acute Respiratory Infections Sensivity & specificity Definition Pneumonia Recognition Fast breathing Antibiotics Severe Pneumonia or Very Severe Disease Lower chest wall
T e c h n i c a l S e m i n a r s Acute Respiratory Infections Sensivity & specificity Definition Pneumonia Recognition Fast breathing Antibiotics Severe Pneumonia or Very Severe Disease Lower chest wall
Allergic Bronchopulmonary Aspergillosis: An Unusual Complication of Bronchial Asthma
 Allergic Bronchopulmonary Aspergillosis: An Unusual Complication of Bronchial Asthma Pages with reference to book, From 329 To 331 S. Fayyaz Hussain, Javaid A. Khan ( Department of Medicine, The Aga Khan
Allergic Bronchopulmonary Aspergillosis: An Unusual Complication of Bronchial Asthma Pages with reference to book, From 329 To 331 S. Fayyaz Hussain, Javaid A. Khan ( Department of Medicine, The Aga Khan
OBSERVATION UNIT ASTHMA PATHWAY OUTLINE Westmoreland Hospital PAGE 1 OF 5
 PAGE 1 OF 5 Exclusion Criteria: (Reason to admit to hospital) A. New EKG changes except sinus tachycardia B. Respiratory Rate > 40 C. Signs/symptoms of Heart Failure D. Impending respiratory failure or
PAGE 1 OF 5 Exclusion Criteria: (Reason to admit to hospital) A. New EKG changes except sinus tachycardia B. Respiratory Rate > 40 C. Signs/symptoms of Heart Failure D. Impending respiratory failure or
Some Facts About Asthma
 Some Facts About Asthma Contents What is asthma? Diagnosing asthma Asthma symptoms Asthma triggers Thanks What is asthma?? Asthma is a chronic lung-disease that inflames and narrows the airways (tubes
Some Facts About Asthma Contents What is asthma? Diagnosing asthma Asthma symptoms Asthma triggers Thanks What is asthma?? Asthma is a chronic lung-disease that inflames and narrows the airways (tubes
BPD. Neonatal/Pediatric Cardiopulmonary Care. Disease. Bronchopulmonary Dysplasia. Baby Jane
 1 Neonatal/Pediatric Cardiopulmonary Care Disease 2 Bronchopulmonary Dysplasia 3 is a 33-day-old prematurely born girl who weighs 1420 g. At birth, her estimated gestational age was 28 weeks. Her initial
1 Neonatal/Pediatric Cardiopulmonary Care Disease 2 Bronchopulmonary Dysplasia 3 is a 33-day-old prematurely born girl who weighs 1420 g. At birth, her estimated gestational age was 28 weeks. Her initial
PLASTIC BRONCHITIS BY R. SLEIGH JOHNSON AND E. G. SITA-LUMSDEN From Southend-on-Sea Hospital, Essex
 Thorax (1960), 15, 325. PLASTIC BRONCHITIS BY R. SLEIGH JOHNSON AND E. G. SITA-LUMSDEN From Southend-on-Sea Hospital, Essex The specific feature of plastic bronchitis is the formation of obstructive bronchial
Thorax (1960), 15, 325. PLASTIC BRONCHITIS BY R. SLEIGH JOHNSON AND E. G. SITA-LUMSDEN From Southend-on-Sea Hospital, Essex The specific feature of plastic bronchitis is the formation of obstructive bronchial
ACUTE PULMNARY INFECTIONS: UNDERSTANDING THE CHEST RADIOGRAPH. Leonard E. Swischuk, M.D. University of Texas Medical Branch
 ACUTE PULMNARY INFECTIONS: UNDERSTANDING THE CHEST RADIOGRAPH Leonard E. Swischuk, M.D. University of Texas Medical Branch AUTHOR HAS NOTHING TO DECLARE LEARNING OBJETIVES Understand the pathophysiology
ACUTE PULMNARY INFECTIONS: UNDERSTANDING THE CHEST RADIOGRAPH Leonard E. Swischuk, M.D. University of Texas Medical Branch AUTHOR HAS NOTHING TO DECLARE LEARNING OBJETIVES Understand the pathophysiology
NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE SCOPE
 NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE 1 Guideline title SCOPE Bronchiolitis: diagnosis and management of bronchiolitis in children. 1.1 Short title Bronchiolitis in children 2 The remit The
NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE 1 Guideline title SCOPE Bronchiolitis: diagnosis and management of bronchiolitis in children. 1.1 Short title Bronchiolitis in children 2 The remit The
Semiology of respiratory system in children Simple choice 1. Mark the intrauterine age of lung development onset from the gut: a) 1 week b) 24 days
 1 week b) 24 days") Semiology of respiratory system in children Simple choice 1. Mark the intrauterine age of lung development onset from the gut: a) 1 week b) 24 days c) 6 weeks d) 12 weeks e) 35 weeks 2. Stridor is not
Semiology of respiratory system in children Simple choice 1. Mark the intrauterine age of lung development onset from the gut: a) 1 week b) 24 days c) 6 weeks d) 12 weeks e) 35 weeks 2. Stridor is not
Chapter 15 - Respiratory Emergencies
 1 2 3 4 5 6 7 National EMS Education Standard Competencies (1 of 5) Medicine Applies fundamental knowledge to provide basic emergency care and transportation based on assessment findings for an acutely
1 2 3 4 5 6 7 National EMS Education Standard Competencies (1 of 5) Medicine Applies fundamental knowledge to provide basic emergency care and transportation based on assessment findings for an acutely
Chapter 16. Objectives. Objectives. Respiratory Emergencies
 Chapter 16 Respiratory Emergencies Prehospital Emergency Care, Ninth Edition Joseph J. Mistovich Keith J. Karren Copyright 2010 by Pearson Education, Inc. All rights reserved. Objectives 1. Define key
Chapter 16 Respiratory Emergencies Prehospital Emergency Care, Ninth Edition Joseph J. Mistovich Keith J. Karren Copyright 2010 by Pearson Education, Inc. All rights reserved. Objectives 1. Define key
Contents. In this lecture, we will discuss: Tuberculosis. Asthma. Cystic fibrosis. Bronchopulmonary dysplasia. Miss.kamlah
 1 Contents In this lecture, we will discuss: Tuberculosis. Asthma. Cystic fibrosis. Bronchopulmonary dysplasia. 2 Tuberculosis (TB) is caused by organism Mycobacterium tuberculosis, which is transmitted
1 Contents In this lecture, we will discuss: Tuberculosis. Asthma. Cystic fibrosis. Bronchopulmonary dysplasia. 2 Tuberculosis (TB) is caused by organism Mycobacterium tuberculosis, which is transmitted