February EMS Training: Pulmonary Emergencies. Used with permission of Silver Cross EMS System
|
|
|
- Anastasia Wiggins
- 5 years ago
- Views:
Transcription


1 February EMS Training: Pulmonary Emergencies Used with permission of Silver Cross EMS System
2 Goals Review airway anatomy and physiology for adults and pediatrics Review issues and techniques in airway management Review prehospital management of: COPD, Asthma, Croup, and Pneumonia Review smoke inhalation injury patterns Review of oxygen delivery devices for prehospital providers 2

3 Anatomy Review 3

4 Anatomy of the Upper Airway Tongue Epiglottis Glottis Vocal chord Trachea Vallecula 4

5 Internal Anatomy of the Upper Airway Cricothyroid membrane 5
6 Anatomy of the Lower Airway Lung Sound Flyby You hear rhonchi in the bronchi 6

7 Anatomy of the Pediatric Airway 7

8 In the supine position, an infant s or child s larger head tips forward, causing airway obstruction. 8

9 Placing padding under the patient s back and shoulders will bring the airway to a neutral alignment. 9

10 Airway Assessment Abnormal upper airway sounds Snoring Crowing Gurgling Stridor Upper Airway 10

11 What is the most common airway obstruction? The tongue! 11




12 OXYGEN DELIVERY DEVICES 12

13 NASAL CANNULA 13

14 NON-REBREATHER MASK 14

15 HAND-HELD NEBULIZER (HHN) 15

16 IN-LINE NEBULIZER Depending on your agency or restock availability, In-Line Nebulizer set-ups can vary dramatically. Become familiar with your equipment Separate oxygen supplies are required for the BVM and the nebulizer 16


17 Bag-Valve Mask Devices 17

18 Pediatric bag-valve-mask device. 18
19 BVM Devices Self inflating and nonrebreathing valve Used with BLS or ALS airway maintenance device Use with apenic patient or diminished respiratory effort Provides blood/body fluid barrier Room air (21%) to 100% concentration Sense of lung compliance Difficult to master tidal volume dependent on mask seal Complications Inadequate tidal volume from poor technique, poor mask seal, and gastric distention 19
20 BVM Devices Method Rescuer at patient s head Clear airway Head tilt- chin lift BLS or ALS airway Tight seal on mouth with C-E positioning One and two rescuer options 20


21 C E Technique 21

22 Two-Person Technique 22

23 Side-by-Side Comparison 23
24 BVM Devices Method/Technique Observe for gastric distension, changes in bag compliance, color changes, improvement in level of consciousness, air leak around mask Trauma patients require in-line BVM 24

25 Pertrach More expensive than needle crichs, but really easy to use! 25

26 Pertrach Procedure Patient supine with head slightly extended if no cervical spine trauma suspected Locate the cricothyroid membrane Cleanse the overlying skin 26
27 Pertrach Use ADULT PERTRACH DIRECTIONS FOR USE Directions for Pertrach Disposable Emergency Cricothyrotomy or Emergency / Elective Tracheostomy Device 1. Remove dilator from the package and protective sheath and advance it into tracheostomy tube. 2. Landmark cricothyroid membrane. Either make an incision in the skin or simply insert Splitting Needle through skin directly over cricothyroid membrane, depending on local medical protocol. 3. While advancing Splitting Needle perpendicular to the skin, lightly pull back on the plunger of syringe. When air bubbles occur or you feel a break in resistance, cease advancement of Splitting Needle. 27
28 Pertrach Use Continued 4. Incline needle more than 45 degrees toward carina and complete insertion. Always maintain the tip of the needle in the midline of the airway. Remove syringe. 5. Insert tip of dilator into the hub of Splitting Needle. Squeeze wings of needle together, then open them out completely to split the needle. Remove needle, continuing to pull it apart in opposite directions, while leaving dilator in trachea. 6. Place thumb on dilator knob while first and second fingers are curved under flange of trachea tube. By exerting pressure, advance dilator and tracheostomy tube into position until flange is against skin. 7. Remove dilator. Inflate cuff until you have control of the airway. Attach resuscitator or ventilator to tracheostomy tube. Secure tracheostomy tube around patient s neck with twill tape. 28

29 Pertrach Insertion 29

30 CPAP Continuous positive airway pressure A form of noninvasive positive pressure ventilation Used in awake, spontaneously breathing patients who need ventilatory support 30
31 CPAP Positive pressure is measured in cmh 2 O. Positive pressure helps inflate collapsed alveoli and improve oxygenation. Helps displace fluid in alveoli in left ventricular failure 31
32 CPAP Indications Congestive heart failure Pulmonary edema COPD Asthma Pneumonia 32
33 CPAP Contraindications Apnea or agonal respirations Inability to follow commands Inability to maintain an airway Unresponsive Shock with cardiac insufficiency Cardiac arrest Vomiting Pneumothorax or chest trauma Tracheotomy Facial trauma 33
34 CPAP Procedure Inform and coach the patient. Minimize the patient's anxiety. Obtain vital signs and SpO 2. Have an adequate oxygen supply. Place the patient in seated or semi- Fowler's position. 34
35 CPAP Procedure Assemble and check the device. Secure the mask with straps. Provide pressure up to 10 cmh 2 O. Continue to coach the patient. 35
36 CPAP Procedure Do not discontinue CPAP unless contraindications arise or you are advised by medical direction. Notify the receiving facility so they can prepare to transfer CPAP. 36
37 CPAP Assess effectiveness with these measures: Respiratory rate Heart rate Systolic blood pressure Oxygen saturation End-tidal CO 2 Complaint of dyspnea Monitor for: Pneumothorax Gastric distention Vomiting Worsening of respiratory distress or failure Decreased mental status Intolerance of the device 37
38 Hazards of Overinflation Overinflation leads to serious complications. In cardiac arrest, perfusion is decreased. In spontaneously breathing patients, return to the left ventricle can be reduced. 38

39 Pulmonary Emergencies & SMO Review 39
40 COPD Obstructive pulmonary diseases Emphysema Chronic bronchitis Asthma 40
41 Emphysema Emphysema Destruction of alveolar walls and distention of alveoli Increased resistance to air flow Severe reduction in gas exchange Caused primarily by smoking 41



42 42
43 Emphysema Signs & Symptoms Anxious Dyspneic Accessory muscle use Thin, barrelchested appearance Coughing Prolonged exhalation Diminished breath sounds Wheezing and rhonchi Pursed-lip breathing Difficulty breathing with exertion Tripod position 43
44 Emphysema Clinical findings Tachypnea Tachycardia Diaphoresis Normal low pulse oximetry 90-94% could be normal On home oxygen 44
45 CODE 30 Acute Asthma/COPD With Wheezing Don t get lured by the Oxygen Demon COPD patients don t typically require high amounts of oxygen. In fact, two published studies concluded that prehospital administration of high flow oxygen may lead to increase mortality rates and poor clinical outcomes 45
46 CODE 30 Acute Asthma/COPD With Wheezing Don t get lured by the Oxygen Demon COPD patients are believed to breathe through a process called hypoxic drive. This means that they are adjusted to low oxygen levels in the blood. They typically retain a higher level of CO2 than non- COPD patients. 46

47 47
48 Treatment for COPD patients Per CODE 30 Initial Medical Care Oxygen at 2-6L/min If severe distress or cyanosis, 15L NRB DO NOT DELAY TRANSPORT These patients decompensate rapidly Delay may lead to respiratory failure, require intubation Treat wheezes with Albuterol May administer in-line if patient is intubated CPAP may be applied at the discretion of Medical Control 48
49 ASTHMA Symptoms present in a similar way as those of COPD Anxious Dominantly heard in the Dyspneic middle lungs Accessory muscle use Diminished breath sounds Wheezing and rhonchi Pursed-lip breathing Difficulty breathing with exertion Tripod position 49
50 Asthma Pathophysiology Bronchial walls are normally thicker and contain some mucous in an asthma patient Asthma attacks have triggers Temperature Humidity Allergens/Exposure to toxins in the air Acute respiratory infections During an asthma attack Bronchiale walls thicken even further Increase in bronchiale mucous secretions Air goes in easy but cannot be exhaled very well Alveolar sacs trap air, cannot push through bronchial swelling and mucous to exit the lungs 50


51 This is a normal asthmatic airway This is what happens during an asthma attack 51

52 52
53 Treating Acute Asthma Attacks Initial Medical Care Do not delay transport These patients decompensate rapidly when not responding to therapies Start oxygen delivery low and titrate upward to relief Quickly administer bronchodilators (Albuterol) If bronchodilators are not working, contact Medical Control for discretionary orders Epinephrine 1:1000, 0.01mg/kg (up to 0.3mg) SQ 53

54 CROUP 54
")
55 Croup Viral disease Affects children 6 months to 7 years old Most often caused by the parainfluenza virus Swollen tissue that narrows airway in the larynx (voicebox) 55
56 Signs and Symptoms The most common and obvious symptom of Croup is the seal bark cough Onset is usually in the evening to overnight hours Patient may appear short of breathe Pay attention to work of breathing Accessory muscle use Patient positioning SKIN PARAMETERS ARE A TELLTALE SIGN OF RESPIRATORY DISTRESS Inhalation often results in a high-pitched wheezing These patients do not typically present with a fever, drooling, or lethargy (this would represent Epiglottitis) 56
57 Treatment CODE 55 Pediatric Respiratory Distress Croup is rarely life threatening but very unnerving for parents! You may need to keep parent calm Reactive (Lower) Airway Disease Consider Blow-By treatments for agitated patients 57
58 Code 55 Pediatric Respiratory Distress Position of comfort Nebulized Albuterol (Ventolin) 2.5mg Pulse oximetry Cardiac monitor Support ABC s Observe Keep warm TRANSPORT 58
59 Albuterol and Croup Just saying A great majority of croup patients respond just as well to humidified oxygen, or nebulized 0.9% Normal Saline Ask any parent with a croupy child and they will tell you to bring them into a steamed up bathroom or even take them outside on a cold evening (cold temp will cause quick bronchoconstriction) Albuterol works GREAT on the bronchial tree but is hit-ormiss when it comes to dilation of the trachea For agitated children whose heart rate is already elevated, consider other options after discussion with Medical Control. LEAD THE CONVERSATION AND STATE YOUR CASE!!! A rationale explanation from a critically thinking paramedic goes a LONG way in advocating for your patient!!! 59


60 PNEUMONIA 60
61 What is it? Pneumonia is a common lung infection caused by bacteria, a virus or fungi. Treatment depends on the cause of your pneumonia, how severe your symptoms are, and your age and overall health. Most healthy people recover from pneumonia in one to three weeks, but pneumonia can be life-threatening. Pneumonia can be prevented by getting an annual flu shot (as flu often leads to pneumonia), frequently washing your hands, and for people at high risk, getting a vaccine for pneumococcal pneumonia. 61

62 Signs & Symptoms Cough (with some pneumonias you may cough up greenish or yellow mucus, or even bloody mucus) Fever, which may be mild or high Shaking chills Shortness of breath, which may only occur when you climb stairs Sharp or stabbing chest pain that gets worse when you breathe deeply or cough Headache Excessive sweating and clammy skin Loss of appetite, low energy, and fatigue Confusion, especially in older people 62
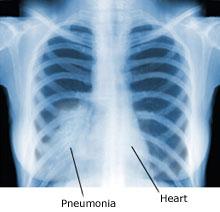
63 Diagnosis It is impossible to narrow down a pneumonia in the prehospital setting. We CAN get half way there though. Physicians use two tools to diagnose a pneumonia: Physical exam: In pneumonia, lungs may make crackling, bubbling, and rumbling sounds on inhalation. There may also be wheezing, and it may be hard to hear sounds of breathing in some areas of your chest. Chest x-ray 63
64 What can EMS do? Administer fluids for fever and dehydration Treat shortness of breathe The primary treatment of shortness of breath due to pneumonia in the prehospital setting is preventing hypoxia with the application of supplemental oxygen. These patients need early treatment with antibiotics for improvement of symptoms and disease resolution. Often, pneumonia can exacerbate COPD; thus, Albuterol may be helpful in decreasing wheezing and dyspnea. 64

65 SMOKE INHALATION INJURIES 65
66 SMOKE INHALATION INJURIES During fires, smoke inhalation victims are unable to efficiently breathe through the nose, thereby decreasing inspiratory air filtration and enabling a greater amount of particle distribution in the airway. This subsequently leads to severe lung injury. Inhalation injury from smoke in fires may account for as many as 60-80% of fire-related deaths in the United States, many of which are preventable. 66

67 67
68 Smoke Inhalation Injuries Smoke inhalation may produce injury through several mechanisms. Heated air from a fire can cause significant thermal injury to the upper airway. Particulate matter produced during combustion (soot) can mechanically obstruct and irritate the airways, causing reflex bronchoconstriction. Noxious gases released from burning materials include carbon monoxide (CO) and hydrogen cyanide. 68
69 Smoke Inhalation Treatment DO NOT DELAY TRANSPORT Secure the airway as needed, deliver high-flow oxygen by mask, and obtain IV access. Cardiac monitoring also is important for any patient with respiratory distress. Albuterol may be given as a treatment for wheezing If respiratory failure is present, the patient should have assisted ventilation and/or endotracheal intubation. Perform cricothyrotomy if airway obstruction is present or impending and an airway cannot be secured orally. Obtain a CO level at the scene if possible. 69
Airway and Ventilation. Emergency Medical Response
 Airway and Ventilation Lesson 14: Airway and Ventilation You Are the Emergency Medical Responder Your medical emergency response team has been called to the fitness center by building security on a report
Airway and Ventilation Lesson 14: Airway and Ventilation You Are the Emergency Medical Responder Your medical emergency response team has been called to the fitness center by building security on a report
Objectives. Case Presentation. Respiratory Emergencies
 Respiratory Emergencies Objectives Describe how to assess airway and breathing, including interpreting information from the PAT and ABCDEs. Differentiate between respiratory distress, respiratory failure,
Respiratory Emergencies Objectives Describe how to assess airway and breathing, including interpreting information from the PAT and ABCDEs. Differentiate between respiratory distress, respiratory failure,
Respiratory Emergencies. Chapter 11
 Respiratory Emergencies Chapter 11 Respiratory System Anatomy and Function of the Lung Characteristics of Adequate Breathing Normal rate and depth Regular breathing pattern Good breath sounds on both sides
Respiratory Emergencies Chapter 11 Respiratory System Anatomy and Function of the Lung Characteristics of Adequate Breathing Normal rate and depth Regular breathing pattern Good breath sounds on both sides
Paramedic Rounds. Pre-Hospital Continuous Positive Airway Pressure (CPAP)
") Paramedic Rounds Pre-Hospital Continuous Positive Airway Pressure (CPAP) Morgan Hillier MD Class of 2011 Dr. Mike Peddle Assistant Medical Director SWORBHP Objectives Outline evidence for pre-hospital
Paramedic Rounds Pre-Hospital Continuous Positive Airway Pressure (CPAP) Morgan Hillier MD Class of 2011 Dr. Mike Peddle Assistant Medical Director SWORBHP Objectives Outline evidence for pre-hospital
1 Chapter 13 Respiratory Emergencies 2 Respiratory Distress Patients often complain about. Shortness of breath Symptom of many different Cause can be
 1 Chapter 13 Respiratory Emergencies 2 Respiratory Distress Patients often complain about. Shortness of breath Symptom of many different Cause can be difficult to determine. Even for physician in hospital
1 Chapter 13 Respiratory Emergencies 2 Respiratory Distress Patients often complain about. Shortness of breath Symptom of many different Cause can be difficult to determine. Even for physician in hospital
Respiratory Emergencies. Lesson Goal. Lesson Objectives 9/10/2012
 Respiratory Emergencies Lesson Goal Assess and provide timely treatment & transport to patients experiencing respiratory emergencies Lesson Objectives List parts of respiratory system and how they work
Respiratory Emergencies Lesson Goal Assess and provide timely treatment & transport to patients experiencing respiratory emergencies Lesson Objectives List parts of respiratory system and how they work
Chapter 16. Objectives. Objectives. Respiratory Emergencies
 Chapter 16 Respiratory Emergencies Prehospital Emergency Care, Ninth Edition Joseph J. Mistovich Keith J. Karren Copyright 2010 by Pearson Education, Inc. All rights reserved. Objectives 1. Define key
Chapter 16 Respiratory Emergencies Prehospital Emergency Care, Ninth Edition Joseph J. Mistovich Keith J. Karren Copyright 2010 by Pearson Education, Inc. All rights reserved. Objectives 1. Define key
Unconscious exchange of air between lungs and the external environment Breathing
 Respiration Unconscious exchange of air between lungs and the external environment Breathing Two types External Exchange of carbon dioxide and oxygen between the environment and the organism Internal Exchange
Respiration Unconscious exchange of air between lungs and the external environment Breathing Two types External Exchange of carbon dioxide and oxygen between the environment and the organism Internal Exchange
Chapter 13. Respiratory Emergencies
 Chapter 13 Respiratory Emergencies Introduction Patients often complain about dyspnea. Shortness of breath Symptom of many different conditions Cause can be difficult to determine. Even for physician in
Chapter 13 Respiratory Emergencies Introduction Patients often complain about dyspnea. Shortness of breath Symptom of many different conditions Cause can be difficult to determine. Even for physician in
Chapter 19 - Respiratory_Emergencies
 Introduction to Emergency Medical Care 1 OBJECTIVES 19.1 Define key terms introduced in this chapter. Slides 14 15, 41, 54 19.2 Describe the anatomy and physiology of respiration. Slides 13 15 19.3 Differentiate
Introduction to Emergency Medical Care 1 OBJECTIVES 19.1 Define key terms introduced in this chapter. Slides 14 15, 41, 54 19.2 Describe the anatomy and physiology of respiration. Slides 13 15 19.3 Differentiate
Respiratory Emergencies
 CHAPTER 16 Respiratory Emergencies Anatomy Review Anatomy Review Pediatric Anatomy Airway structure differences Proportionally larger tongue Smaller, more flexible trachea Abdominal breathers Reasons for
CHAPTER 16 Respiratory Emergencies Anatomy Review Anatomy Review Pediatric Anatomy Airway structure differences Proportionally larger tongue Smaller, more flexible trachea Abdominal breathers Reasons for
Anatomy Review. Anatomy Review. Respiratory Emergencies CHAPTER 16
 CHAPTER 16 Respiratory Emergencies Anatomy Review Anatomy Review 1 Pediatric Anatomy Airway structure differences Proportionally larger tongue Smaller, more flexible trachea Abdominal breathers Reasons
CHAPTER 16 Respiratory Emergencies Anatomy Review Anatomy Review 1 Pediatric Anatomy Airway structure differences Proportionally larger tongue Smaller, more flexible trachea Abdominal breathers Reasons
Firefighter Pre-Hospital Care Program Recruit Presentation. Respiratory Emergencies
 Firefighter Pre-Hospital Care Program Recruit Presentation Respiratory Emergencies The Respiratory System Anatomy Pharynx Nasopharynx Oropharynx Epiglottis Larynx Trachea Right main bronchus Left main
Firefighter Pre-Hospital Care Program Recruit Presentation Respiratory Emergencies The Respiratory System Anatomy Pharynx Nasopharynx Oropharynx Epiglottis Larynx Trachea Right main bronchus Left main
CPAP. Pre-Hospital Treatment Using The Respironics Whisperflow CPAP Device. Charlottesville Albemarle Rescue Squad - CPAP
 CPAP Pre-Hospital Treatment Using The Respironics Whisperflow CPAP Device CPAP What Is It? C ontinuous P ositive A irway P ressure Anatomy Review Anatomy Review Anatomy Review Alveoli Anatomy Review Chest
CPAP Pre-Hospital Treatment Using The Respironics Whisperflow CPAP Device CPAP What Is It? C ontinuous P ositive A irway P ressure Anatomy Review Anatomy Review Anatomy Review Alveoli Anatomy Review Chest
Respiratory Management in Pediatrics
 Respiratory Management in Pediatrics Children s Hospital Omaha Critical Care Transport Sue Holmer RN, C-NPT Objectives Examine the differences between the pediatric and adults airways. Recognize respiratory
Respiratory Management in Pediatrics Children s Hospital Omaha Critical Care Transport Sue Holmer RN, C-NPT Objectives Examine the differences between the pediatric and adults airways. Recognize respiratory
3. Identify the importance in the prehospital setting for the administration of nebulized bronchodilator.
 TERMINAL OBJECTIVE At the end of this lesson, the EMT-Basic will be able to utilize the assessment findings to formulate a field impression of bronchospasm and understand the administration of nebulized
TERMINAL OBJECTIVE At the end of this lesson, the EMT-Basic will be able to utilize the assessment findings to formulate a field impression of bronchospasm and understand the administration of nebulized
Chapter 10. Objectives. Objectives 01/09/2013. Airway Management, Artificial Ventilation, and Oxygenation
 Chapter 10 Airway Management, Artificial Ventilation, and Oxygenation Prehospital Emergency Care, Ninth Edition Joseph J. Mistovich Keith J. Karren Copyright 2010 by Pearson Education, Inc. All rights
Chapter 10 Airway Management, Artificial Ventilation, and Oxygenation Prehospital Emergency Care, Ninth Edition Joseph J. Mistovich Keith J. Karren Copyright 2010 by Pearson Education, Inc. All rights
Overview of COPD INTRODUCTION
 Overview of COPD INTRODUCTION Chronic obstructive pulmonary disease (COPD) is a common lung disease that affects millions of people, and it is the fourth leading cause of death in the United States. It
Overview of COPD INTRODUCTION Chronic obstructive pulmonary disease (COPD) is a common lung disease that affects millions of people, and it is the fourth leading cause of death in the United States. It
Overview. The Respiratory System. Chapter 18. Respiratory Emergencies 9/11/2012
 Chapter 18 Respiratory Emergencies Slide 1 Overview Respiratory System Review Anatomy Physiology Breathing Assessment Adequate Breathing Breathing Difficulty Focused History and Physical Examination Emergency
Chapter 18 Respiratory Emergencies Slide 1 Overview Respiratory System Review Anatomy Physiology Breathing Assessment Adequate Breathing Breathing Difficulty Focused History and Physical Examination Emergency
Pediatric Patients. BCFPD Paramedic Education Program. EMS Education Paramedic Level
 Pediatric Patients BCFPD Program Basic Considerations Much of the initial patient assessment can be done during visual examination of the scene. Involve the caregiver or parent as much as possible. Allow
Pediatric Patients BCFPD Program Basic Considerations Much of the initial patient assessment can be done during visual examination of the scene. Involve the caregiver or parent as much as possible. Allow
Training. Continuous Positive Airway Pressure (CPAP)
") Training The training module will follow the national standard curriculum as it relates to the application and use of CPAP. The proposed curriculum will closely resemble the following algorithm utilizing
Training The training module will follow the national standard curriculum as it relates to the application and use of CPAP. The proposed curriculum will closely resemble the following algorithm utilizing
The Respiratory System
 130 20 The Respiratory System 1. Define important words in this chapter 2. Explain the structure and function of the respiratory system 3. Discuss changes in the respiratory system due to aging 4. Discuss
130 20 The Respiratory System 1. Define important words in this chapter 2. Explain the structure and function of the respiratory system 3. Discuss changes in the respiratory system due to aging 4. Discuss
Epiglottitis. Bronchitis. Bronchiolitis. Pneumonia. Croup syndrome. Miss. kamlah 2
 Miss. kamlah 1 Epiglottitis. Bronchitis. Bronchiolitis. Pneumonia. Croup syndrome. Miss. kamlah 2 Acute Epiglottitis Is an infection of the epiglottis, the long narrow structure that closes off the glottis
Miss. kamlah 1 Epiglottitis. Bronchitis. Bronchiolitis. Pneumonia. Croup syndrome. Miss. kamlah 2 Acute Epiglottitis Is an infection of the epiglottis, the long narrow structure that closes off the glottis
Pediatric Shock. Hypovolemia. Sepsis. Most common cause of pediatric shock Small blood volumes (80cc/kg)
") Critical Concepts: Shock Inadequate peripheral perfusion where oxygen delivery does not meet metabolic demand Adult vs Pediatric Shock - Same causes/different frequencies Pediatric Shock Hypovolemia Most
Critical Concepts: Shock Inadequate peripheral perfusion where oxygen delivery does not meet metabolic demand Adult vs Pediatric Shock - Same causes/different frequencies Pediatric Shock Hypovolemia Most
County of Santa Clara Emergency Medical Services System
 County of Santa Clara Emergency Medical Services System Policy #700-M12: Continuous Positive Airway Pressure CONTINUOUS POSITIVE AIRWAY PRESSURE Effective: February 8, 2013TBD Replaces: NewFebruary 8,
County of Santa Clara Emergency Medical Services System Policy #700-M12: Continuous Positive Airway Pressure CONTINUOUS POSITIVE AIRWAY PRESSURE Effective: February 8, 2013TBD Replaces: NewFebruary 8,
Bronchoconstriction is also treated with medications that inhibit bronchiolar constriction such as: Ipratropium (Atrovent)
") Patients with difficulty breathing (dyspnea) may have problems with: Oxygenation due to alveolar problems Ventilation due to bronchiolar problems Oxygenation due to lung perfusion problems Combinations
Patients with difficulty breathing (dyspnea) may have problems with: Oxygenation due to alveolar problems Ventilation due to bronchiolar problems Oxygenation due to lung perfusion problems Combinations
Airway Management From Brady s First Responder (8th Edition) 82 Questions
 82 Questions") Airway Management From Brady s First Responder (8th Edition) 82 Questions 1. What color will cyanotic skin be? p. 119 *A.) Blue B.) Red C.) Yellow D.) Green 2. Which is the primary path for air to enter
Airway Management From Brady s First Responder (8th Edition) 82 Questions 1. What color will cyanotic skin be? p. 119 *A.) Blue B.) Red C.) Yellow D.) Green 2. Which is the primary path for air to enter
yregion I EMERGENCY MEDICAL SERVICES STANDING MEDICAL ORDERS EMT Basic SMO: Airway Management
 yregion I EMERGENCY MEDICAL SERVICES STANDING MEDICAL ORDERS EMT Basic SMO: Airway Management Overview: Managing a patient s airway may be necessitated due to upper or lower airway obstruction, inadequate
yregion I EMERGENCY MEDICAL SERVICES STANDING MEDICAL ORDERS EMT Basic SMO: Airway Management Overview: Managing a patient s airway may be necessitated due to upper or lower airway obstruction, inadequate
McHenry Western Lake County EMS System Optional CE for Paramedics, EMT-B and PHRN s Croup vs. Epiglottitis. Optional #2 2017
 McHenry Western Lake County EMS System Optional CE for Paramedics, EMT-B and PHRN s Croup vs. Epiglottitis Optional #2 2017 The tones go out at 3 am for a child with difficulty breathing. As it is a kid
McHenry Western Lake County EMS System Optional CE for Paramedics, EMT-B and PHRN s Croup vs. Epiglottitis Optional #2 2017 The tones go out at 3 am for a child with difficulty breathing. As it is a kid
Pneumonia. Trachea , The Patient Education Institute, Inc. id Last reviewed: 11/11/2017 1
 Pneumonia Introduction Pneumonia is an inflammation and infection of the lungs. Pneumonia causes millions of deaths every year. It can affect anybody, but is more dangerous to older adults, babies and
Pneumonia Introduction Pneumonia is an inflammation and infection of the lungs. Pneumonia causes millions of deaths every year. It can affect anybody, but is more dangerous to older adults, babies and
Respiratory System Anatomy Respiratory system: all the structures that contribute to
 1 2 3 4 5 6 7 8 Chapter 15 Respiratory Emergencies Respiratory Distress Patients often complain about dyspnea. Shortness of breath Symptom of many different conditions Cause can be difficult to determine.
1 2 3 4 5 6 7 8 Chapter 15 Respiratory Emergencies Respiratory Distress Patients often complain about dyspnea. Shortness of breath Symptom of many different conditions Cause can be difficult to determine.
Chapter 15 - Respiratory Emergencies
 1 2 3 4 5 6 7 National EMS Education Standard Competencies (1 of 5) Medicine Applies fundamental knowledge to provide basic emergency care and transportation based on assessment findings for an acutely
1 2 3 4 5 6 7 National EMS Education Standard Competencies (1 of 5) Medicine Applies fundamental knowledge to provide basic emergency care and transportation based on assessment findings for an acutely
Chapter 11: Respiratory Emergencies
 29698_CH11_ANS_p001_005 4/12/05 2:02 PM Page 1 Answer Key Chapter 11 1 Chapter 11: Respiratory Emergencies Matching 1. B (page 373) 8. E (page 370) 2. D (page 369) 9. M(page 389) 3. H (page 370) 10. A
29698_CH11_ANS_p001_005 4/12/05 2:02 PM Page 1 Answer Key Chapter 11 1 Chapter 11: Respiratory Emergencies Matching 1. B (page 373) 8. E (page 370) 2. D (page 369) 9. M(page 389) 3. H (page 370) 10. A
Other methods for maintaining the airway (not definitive airway as still unprotected):
:") Page 56 Where anaesthetic skills and drugs are available, endotracheal intubation is the preferred method of securing a definitive airway. This technique comprises: rapid sequence induction of anaesthesia
Page 56 Where anaesthetic skills and drugs are available, endotracheal intubation is the preferred method of securing a definitive airway. This technique comprises: rapid sequence induction of anaesthesia
Basic Airway Management
 Basic Airway Management Dr. Madhurita Singh, Assoc. Professor, Dept. of Critical Care, CMC Vellore. This is the first module in a series on management of airway and ventilation in critically ill patients.
Basic Airway Management Dr. Madhurita Singh, Assoc. Professor, Dept. of Critical Care, CMC Vellore. This is the first module in a series on management of airway and ventilation in critically ill patients.
Lecture Notes. Chapter 3: Asthma
 Lecture Notes Chapter 3: Asthma Objectives Define asthma and status asthmaticus List the potential causes of asthma attacks Describe the effect of asthma attacks on lung function List the clinical features
Lecture Notes Chapter 3: Asthma Objectives Define asthma and status asthmaticus List the potential causes of asthma attacks Describe the effect of asthma attacks on lung function List the clinical features
Respiratory Emergencies
 29698_CH11_Q_p001_012 4/12/05 2:03 PM Page 1 MEDICAL EMERGENCIES S E C T I O N 4 C H A P T E R Respiratory Emergencies 11 Workbook Activities The following activities have been designed to help you. Your
29698_CH11_Q_p001_012 4/12/05 2:03 PM Page 1 MEDICAL EMERGENCIES S E C T I O N 4 C H A P T E R Respiratory Emergencies 11 Workbook Activities The following activities have been designed to help you. Your
PEDIATRIC EMERGENCIES Sandra Horning, MD Sacred Heart Medical Center Emergency Department
 PEDIATRIC EMERGENCIES Sandra Horning, MD Sacred Heart Medical Center Emergency Department Overview Roles of the EMS in Pediatric Care Growth and Development Assessment Airway Adjuncts and Intravenous Access
PEDIATRIC EMERGENCIES Sandra Horning, MD Sacred Heart Medical Center Emergency Department Overview Roles of the EMS in Pediatric Care Growth and Development Assessment Airway Adjuncts and Intravenous Access
Glossary of Asthma Terms
 HealthyKidsExpress@bjc.org Asthma Words to Know Developed in partnership with Health Literacy Missouri Airways (Bronchi, Bronchial Tubes): The tubes in the lungs that let air in and out of the body. Airway
HealthyKidsExpress@bjc.org Asthma Words to Know Developed in partnership with Health Literacy Missouri Airways (Bronchi, Bronchial Tubes): The tubes in the lungs that let air in and out of the body. Airway
Respiratory Distress/Failure - General
 Respiratory Distress/Failure - General Criteria: Dyspnea WITHOUT a clear etiology O 2 V/S and SpO 2 (with and without Oxygen therapy if possible) Blood glucose analysis: if less than 80 mg/dl, refer to
Respiratory Distress/Failure - General Criteria: Dyspnea WITHOUT a clear etiology O 2 V/S and SpO 2 (with and without Oxygen therapy if possible) Blood glucose analysis: if less than 80 mg/dl, refer to
AIRWAY & HEART ANOTOMY
 Objectives I CAN T BREATH Respiratory Emergencies Review of anatomical structures related to heart & lungs Differentiate differences between adult and pediatric airways Identify the need for airway assistance
Objectives I CAN T BREATH Respiratory Emergencies Review of anatomical structures related to heart & lungs Differentiate differences between adult and pediatric airways Identify the need for airway assistance
Function of the Respiratory System. Exchange CO2 (on expiration) for O2 (on inspiration)
 for O2 (on inspiration)") Function of the Respiratory System Exchange CO2 (on expiration) for O2 (on inspiration) Upper Respiratory Tract Includes: Nose Mouth Pharynx Larynx Function: Warms and humidifies the inspired air Filters
Function of the Respiratory System Exchange CO2 (on expiration) for O2 (on inspiration) Upper Respiratory Tract Includes: Nose Mouth Pharynx Larynx Function: Warms and humidifies the inspired air Filters
Competency Title: Continuous Positive Airway Pressure
 Competency Title: Continuous Positive Airway Pressure Trainee Name: ------------------------------------------------------------- Title: ---------------------------------------------------------------
Competency Title: Continuous Positive Airway Pressure Trainee Name: ------------------------------------------------------------- Title: ---------------------------------------------------------------
PEPP Course: PEPP BLS Pretest
 PEPP Course: PEPP BLS Pretest 1. What is the best way to administer oxygen to a child in moderate respiratory distress? Nasal cannula Simple mask Nonrebreathing mask Bag-valve-mask device 2. A 2-year-old
PEPP Course: PEPP BLS Pretest 1. What is the best way to administer oxygen to a child in moderate respiratory distress? Nasal cannula Simple mask Nonrebreathing mask Bag-valve-mask device 2. A 2-year-old
CONTINUOUS POSITIVE AIRWAY PRESSURE (CPAP)
") CONTINUOUS POSITIVE AIRWAY PRESSURE (CPAP) Continuous Positive Airway Pressure (CPAP) may be used as an adjunctive therapy for the treatment of patients with suspected Acute Pulmonary Edema, Chronic Obstructive
CONTINUOUS POSITIVE AIRWAY PRESSURE (CPAP) Continuous Positive Airway Pressure (CPAP) may be used as an adjunctive therapy for the treatment of patients with suspected Acute Pulmonary Edema, Chronic Obstructive
General Medical Procedure. Emergency Airway Techniques (General Airway Protocol)
") General Medical Procedure Appropriate airway management is often the most important intervention a prehospital care provider makes, as ensuring adequate oxygenation and ventilation is crucial to the survival
General Medical Procedure Appropriate airway management is often the most important intervention a prehospital care provider makes, as ensuring adequate oxygenation and ventilation is crucial to the survival
10/17/2016 OXYGEN DELIVERY: INDICATIONS AND USE OF EQUIPMENT COURSE OBJECTIVES COMMON CAUSES OF RESPIRATORY FAILURE
 OXYGEN DELIVERY: INDICATIONS AND USE OF EQUIPMENT J U L I E Z I M M E R M A N, R N, M S N C L I N I C A L N U R S E S P E C I A L I S T E L O I S A C U T L E R, R R T, B S R C C L I N I C A L / E D U C
OXYGEN DELIVERY: INDICATIONS AND USE OF EQUIPMENT J U L I E Z I M M E R M A N, R N, M S N C L I N I C A L N U R S E S P E C I A L I S T E L O I S A C U T L E R, R R T, B S R C C L I N I C A L / E D U C
PEMSS PROTOCOLS INVASIVE PROCEDURES
 PEMSS PROTOCOLS INVASIVE PROCEDURES Panhandle Emergency Medical Services System SURGICAL AND NEEDLE CRICOTHYROTOMY Inability to intubate is the primary indication for creating an artificial airway. Care
PEMSS PROTOCOLS INVASIVE PROCEDURES Panhandle Emergency Medical Services System SURGICAL AND NEEDLE CRICOTHYROTOMY Inability to intubate is the primary indication for creating an artificial airway. Care
Introduction to Emergency Medical Care 1
 Introduction to Emergency Medical Care 1 OBJECTIVES 8.1 Define key terms introduced in this chapter. Slides 12 15, 21, 24, 31-34, 39, 40, 54 8.2 Describe the anatomy and physiology of the upper and lower
Introduction to Emergency Medical Care 1 OBJECTIVES 8.1 Define key terms introduced in this chapter. Slides 12 15, 21, 24, 31-34, 39, 40, 54 8.2 Describe the anatomy and physiology of the upper and lower
Using an Inhaler and Nebulizer
 Using an Inhaler and Nebulizer Introduction An inhaler is a handheld device that is used to deliver medication directly to your airways. A nebulizer is an electric or battery powered machine that turns
Using an Inhaler and Nebulizer Introduction An inhaler is a handheld device that is used to deliver medication directly to your airways. A nebulizer is an electric or battery powered machine that turns
The Respiratory System Structures of the Respiratory System Structures of the Respiratory System Structures of the Respiratory System Nose Sinuses
 CH 14 D.E. Human Biology The Respiratory System The Respiratory System OUTLINE: Mechanism of Breathing Transport of Gases between the Lungs and the Cells Respiratory Centers in the Brain Function Provides
CH 14 D.E. Human Biology The Respiratory System The Respiratory System OUTLINE: Mechanism of Breathing Transport of Gases between the Lungs and the Cells Respiratory Centers in the Brain Function Provides
Respiratory Diseases and Disorders
 Chapter 9 Respiratory Diseases and Disorders Anatomy and Physiology Chest, lungs, and conducting airways Two parts: Upper respiratory system consists of nose, mouth, sinuses, pharynx, and larynx Lower
Chapter 9 Respiratory Diseases and Disorders Anatomy and Physiology Chest, lungs, and conducting airways Two parts: Upper respiratory system consists of nose, mouth, sinuses, pharynx, and larynx Lower
Cardiovascular and Respiratory Disorders
 Cardiovascular and Respiratory Disorders Blood Pressure Normal blood pressure is 120/80 mmhg (millimeters of mercury) Hypertension is when the resting blood pressure is too high Systolic BP is 140 mmhg
Cardiovascular and Respiratory Disorders Blood Pressure Normal blood pressure is 120/80 mmhg (millimeters of mercury) Hypertension is when the resting blood pressure is too high Systolic BP is 140 mmhg
Bronchitis. Anatomy of the Lungs The lungs allow us to fill our blood with oxygen. The oxygen we breathe is absorbed into our blood in the lungs.
 Bronchitis Introduction Bronchitis is an inflammation of the bronchial tubes, the airways that carry air to the lungs. It causes shortness of breath, wheezing and chest tightness as well as a cough that
Bronchitis Introduction Bronchitis is an inflammation of the bronchial tubes, the airways that carry air to the lungs. It causes shortness of breath, wheezing and chest tightness as well as a cough that
Review. 1. How does a child s anatomy differ from an adult s anatomy?
 Chapter 32 Review Review 1. How does a child s anatomy differ from an adult s anatomy? A. The child s trachea is more rigid B. The tongue is proportionately smaller C. The epiglottis is less floppy in
Chapter 32 Review Review 1. How does a child s anatomy differ from an adult s anatomy? A. The child s trachea is more rigid B. The tongue is proportionately smaller C. The epiglottis is less floppy in
Chapter 40 Advanced Airway Management
 1 2 3 4 5 Chapter 40 Advanced Airway Management Advanced Airway Management The advanced airway management techniques discussed in this chapter are to introduce the EMT-B student to these procedures only.
1 2 3 4 5 Chapter 40 Advanced Airway Management Advanced Airway Management The advanced airway management techniques discussed in this chapter are to introduce the EMT-B student to these procedures only.
I. Subject: Continuous Positive Airway Pressure CPAP by Continuous Flow Device
 I. Subject: Continuous Positive Airway Pressure CPAP by Continuous Flow Device II. Policy: Continuous Positive Airway Pressure CPAP by the Down's system will be instituted by Respiratory Therapy personnel
I. Subject: Continuous Positive Airway Pressure CPAP by Continuous Flow Device II. Policy: Continuous Positive Airway Pressure CPAP by the Down's system will be instituted by Respiratory Therapy personnel
LESSON ASSIGNMENT. After completing this lesson, you should be able to:
 LESSON ASSIGNMENT LESSON 3 Cricothyroidotomy LESSON ASSIGNMENT Paragraphs 3-1 through 3-7. LESSON OBJECTIVES After completing this lesson, you should be able to: 3-1. Define cricothyroidotomy. 3-2. Identify
LESSON ASSIGNMENT LESSON 3 Cricothyroidotomy LESSON ASSIGNMENT Paragraphs 3-1 through 3-7. LESSON OBJECTIVES After completing this lesson, you should be able to: 3-1. Define cricothyroidotomy. 3-2. Identify
Continuous Positive Airway Pressure (CPAP) Paramedic Learner Package
 Paramedic Learner Package") Continuous Positive Airway Pressure (CPAP) Paramedic Learner Package www.lhsc.on.ca/bhp 1 This page left blank intentionally. Table of Contents Introduction & Expectations... 4 Learning Objectives... 4
Continuous Positive Airway Pressure (CPAP) Paramedic Learner Package www.lhsc.on.ca/bhp 1 This page left blank intentionally. Table of Contents Introduction & Expectations... 4 Learning Objectives... 4
Evaluation of the Effect of Prehospital Application of Continuous Positive Airway Pressure Therapy in Acute Respiratory Distress
 BRIEF REPORT Evaluation of the Effect of Prehospital Application of Continuous Positive Airway Pressure Therapy in Acute Respiratory Distress G. Scott Warner, MD, FACP, FCCP Cullman Emergency Medical Services,
BRIEF REPORT Evaluation of the Effect of Prehospital Application of Continuous Positive Airway Pressure Therapy in Acute Respiratory Distress G. Scott Warner, MD, FACP, FCCP Cullman Emergency Medical Services,
NON INVASIVE LIFE SAVERS. Non Invasive Ventilation (NIV)
") Table 1. NIV: Mechanisms Of Action Decreases work of breathing Increases functional residual capacity Recruits collapsed alveoli Improves respiratory gas exchange Reverses hypoventilation Maintains upper
Table 1. NIV: Mechanisms Of Action Decreases work of breathing Increases functional residual capacity Recruits collapsed alveoli Improves respiratory gas exchange Reverses hypoventilation Maintains upper
1 Chapter 40 Advanced Airway Management 2 Advanced Airway Management The advanced airway management techniques discussed in this chapter are to
 1 Chapter 40 Advanced Airway Management 2 Advanced Airway Management The advanced airway management techniques discussed in this chapter are to introduce the EMT-B student to these procedures only. In
1 Chapter 40 Advanced Airway Management 2 Advanced Airway Management The advanced airway management techniques discussed in this chapter are to introduce the EMT-B student to these procedures only. In
Respiratory Anesthetic Emergencies in Oral and Maxillofacial Surgery. By: Lillian Han
 Respiratory Anesthetic Emergencies in Oral and Maxillofacial Surgery By: Lillian Han Background: Respiratory anesthetic emergencies are the most common complications during the administration of anesthesia
Respiratory Anesthetic Emergencies in Oral and Maxillofacial Surgery By: Lillian Han Background: Respiratory anesthetic emergencies are the most common complications during the administration of anesthesia
The RESPIRATORY System. Unit 3 Transportation Systems
 The RESPIRATORY System Unit 3 Transportation Systems The Respiratory System Functions of the Respiratory System Warms, moistens, and filters incoming air Nasal cavity Resonating chambers for speech and
The RESPIRATORY System Unit 3 Transportation Systems The Respiratory System Functions of the Respiratory System Warms, moistens, and filters incoming air Nasal cavity Resonating chambers for speech and
Lecture Notes. Chapter 9: Smoke Inhalation Injury and Burns
 Lecture Notes Chapter 9: Smoke Inhalation Injury and Burns Objectives List the factors that influence mortality rate Describe the nature of smoke inhalation and the fire environment Recognize the pulmonary
Lecture Notes Chapter 9: Smoke Inhalation Injury and Burns Objectives List the factors that influence mortality rate Describe the nature of smoke inhalation and the fire environment Recognize the pulmonary
Condensed version.
 I m Stu 3 Condensed version smcvicar@uwhealth.org Listen 1. Snoring 2. Gurgling 3. Hoarseness 4. Stridor (inspiratory/expiratory) 5. Wheezing 6. Grunting Listen Crackles Wheezing Stridor Absent Crackles
I m Stu 3 Condensed version smcvicar@uwhealth.org Listen 1. Snoring 2. Gurgling 3. Hoarseness 4. Stridor (inspiratory/expiratory) 5. Wheezing 6. Grunting Listen Crackles Wheezing Stridor Absent Crackles
About the Respiratory System. Respiratory System. Human Respiratory System. Cellular Respiration. Nostrils. Label diagram
 Respiratory System Human Respiratory System A system to deliver oxygen (O2) to body cells & get rid of carbon dioxide (CO2) as a waste through cellular respiration. Two systems involved: Respiratory &
Respiratory System Human Respiratory System A system to deliver oxygen (O2) to body cells & get rid of carbon dioxide (CO2) as a waste through cellular respiration. Two systems involved: Respiratory &
Airway management. Dr. Dóra Ujvárosy Medical Unversity of Debrecen Emergency Department
 Airway management Dr. Dóra Ujvárosy Medical Unversity of Debrecen Emergency Department Airway management Airway management is the medical process of ensuring there is an open pathway between a patient
Airway management Dr. Dóra Ujvárosy Medical Unversity of Debrecen Emergency Department Airway management Airway management is the medical process of ensuring there is an open pathway between a patient
Protocol Update 2019
 Protocol Update 2019 There have been several questions revolving around protocol updates and how they are to be conducted. As many of you are aware there is a protocol submission process in the appendix
Protocol Update 2019 There have been several questions revolving around protocol updates and how they are to be conducted. As many of you are aware there is a protocol submission process in the appendix
Medical First Responder Program Protocols
 Medical Scene Safety Protocol Verify Scene Safety with Police or Dispatch UNKWN Scene Safe? Enter Continue to Appropriate Protocol Possible to Make Safe Make Safe Then Continue Exit Area and Stage Outside
Medical Scene Safety Protocol Verify Scene Safety with Police or Dispatch UNKWN Scene Safe? Enter Continue to Appropriate Protocol Possible to Make Safe Make Safe Then Continue Exit Area and Stage Outside
Prior to applying a nonrebreathing mask on a patient with difficulty breathing, you should:!
 An elderly woman with COPD presents with a decreased level of consciousness, cyanosis to her face and neck, and labored respirations. Her pulse is rapid and weak and her oxygen saturation is 76%. You should:
An elderly woman with COPD presents with a decreased level of consciousness, cyanosis to her face and neck, and labored respirations. Her pulse is rapid and weak and her oxygen saturation is 76%. You should:
9/25/2014. Medical Issues (Restrictive processes) Medical Issues (Obstructive processes) Respiratory Emergencies (Class 10)
 Medical Issues (Obstructive processes) Respiratory Emergencies (Class 10)") 1 2 3 Respiratory Emergencies (Class 10) Respiratory distress accounts for approximately 60% of all ambulance calls There are greater than 300,000 deaths annually due to respiratory emergencies All respiratory
1 2 3 Respiratory Emergencies (Class 10) Respiratory distress accounts for approximately 60% of all ambulance calls There are greater than 300,000 deaths annually due to respiratory emergencies All respiratory
Lesson 4-3: Cardiac Emergencies. CARDIAC EMERGENCIES Angina, AMI, CHF and AED
 Lesson 4-3: Cardiac Emergencies CARDIAC EMERGENCIES Angina, AMI, CHF and AED THREE FAMILIAR CARDIAC CONDITIONS Angina Pectoris Acute Myocardial Infarction Congestive Heart Failure ANGINA PECTORIS Chest
Lesson 4-3: Cardiac Emergencies CARDIAC EMERGENCIES Angina, AMI, CHF and AED THREE FAMILIAR CARDIAC CONDITIONS Angina Pectoris Acute Myocardial Infarction Congestive Heart Failure ANGINA PECTORIS Chest
STRIDOR. Respiratory system. Lecture
 STRIDOR Stridor is a continuous inspiratory harsh sound produced by partial obstruction in the region of the larynx or trachea. Total obstruction cyanosis & death. Etiology Acute stridor Infectious croup
STRIDOR Stridor is a continuous inspiratory harsh sound produced by partial obstruction in the region of the larynx or trachea. Total obstruction cyanosis & death. Etiology Acute stridor Infectious croup
What is the next best step?
 Noninvasive Ventilation William Janssen, M.D. Assistant Professor of Medicine National Jewish Health University of Colorado Denver Health Sciences Center What is the next best step? 65 year old female
Noninvasive Ventilation William Janssen, M.D. Assistant Professor of Medicine National Jewish Health University of Colorado Denver Health Sciences Center What is the next best step? 65 year old female
Chronic obstructive pulmonary disease
 Chronic obstructive pulmonary disease By: Dr. Fatima Makee AL-Hakak () University of kerbala College of nursing Out lines What is the? Overview Causes of Symptoms of What's the difference between and asthma?
Chronic obstructive pulmonary disease By: Dr. Fatima Makee AL-Hakak () University of kerbala College of nursing Out lines What is the? Overview Causes of Symptoms of What's the difference between and asthma?
Pulmonary Pathophysiology
 Pulmonary Pathophysiology 1 Reduction of Pulmonary Function 1. Inadequate blood flow to the lungs hypoperfusion 2. Inadequate air flow to the alveoli - hypoventilation 2 Signs and Symptoms of Pulmonary
Pulmonary Pathophysiology 1 Reduction of Pulmonary Function 1. Inadequate blood flow to the lungs hypoperfusion 2. Inadequate air flow to the alveoli - hypoventilation 2 Signs and Symptoms of Pulmonary
HASPI Medical Anatomy & Physiology 14b Lab Activity
 HASPI Medical Anatomy & Physiology 14b Lab Activity Name(s): Period: Date: Respiratory Distress Respiratory distress is a broad medical term that applies to any type of breathing difficulty and the associated
HASPI Medical Anatomy & Physiology 14b Lab Activity Name(s): Period: Date: Respiratory Distress Respiratory distress is a broad medical term that applies to any type of breathing difficulty and the associated
Chapter 11. Learning Objectives. Learning Objectives 9/18/2012. Respiratory Emergencies
 Chapter 11 Respiratory Learning Objectives List structures & functions of the respiratory system State signs/symptoms of patient with breathing difficulty Describe emergency medical care of patient with
Chapter 11 Respiratory Learning Objectives List structures & functions of the respiratory system State signs/symptoms of patient with breathing difficulty Describe emergency medical care of patient with
CHANHASSEN FIRE DEPARTMENT MEDICAL / RESCUE SKILLS
 CHANHASSEN FIRE DEPARTMENT MEDICAL / RESCUE SKILLS PRACTICAL STATIONS CHANHASSEN FIRE DEPARTMENT MEDICAL / RESCUE SKILLS 1. CARDIAC ARREST MANAGEMENT 2. AIRWAY & RESPIRATORY MANAGEMENT 3. SPINAL IMMOBILIZATION
CHANHASSEN FIRE DEPARTMENT MEDICAL / RESCUE SKILLS PRACTICAL STATIONS CHANHASSEN FIRE DEPARTMENT MEDICAL / RESCUE SKILLS 1. CARDIAC ARREST MANAGEMENT 2. AIRWAY & RESPIRATORY MANAGEMENT 3. SPINAL IMMOBILIZATION
ITLS Pediatric Provider Course Basic Pre-Test
 ITLS Pediatric Provider Course Basic Pre-Test 1. You arrive at the scene of a motor vehicle collision and are directed to evaluate a child who was in one of the vehicles. The patient appears to be a child
ITLS Pediatric Provider Course Basic Pre-Test 1. You arrive at the scene of a motor vehicle collision and are directed to evaluate a child who was in one of the vehicles. The patient appears to be a child
Anatomy & Physiology 2 Canale. Respiratory System: Exchange of Gases
 Anatomy & Physiology 2 Canale Respiratory System: Exchange of Gases Why is it so hard to hold your breath for Discuss! : ) a long time? Every year carbon monoxide poisoning kills 500 people and sends another
Anatomy & Physiology 2 Canale Respiratory System: Exchange of Gases Why is it so hard to hold your breath for Discuss! : ) a long time? Every year carbon monoxide poisoning kills 500 people and sends another
EMT OPTIONAL SKILL. Cell Phones and Pagers. Epinephrine Auto-injector. Course Outline 9/2017
 EMT OPTIONAL SKILL Epinephrine Auto-injector Cell Phones and Pagers Be courteous to your classmates! Please set your cell phones and/or pagers to silent or turn them off. Course Outline Introduction and
EMT OPTIONAL SKILL Epinephrine Auto-injector Cell Phones and Pagers Be courteous to your classmates! Please set your cell phones and/or pagers to silent or turn them off. Course Outline Introduction and
Interfacility Protocol Protocol Title:
 Interfacility Protocol Protocol Title: Mechanical Ventilator Monitoring & Management Original Adoption Date: 05/2009 Past Protocol Updates 05/2009, 12/2013 Date of Most Recent Update: March 23, 2015 Medical
Interfacility Protocol Protocol Title: Mechanical Ventilator Monitoring & Management Original Adoption Date: 05/2009 Past Protocol Updates 05/2009, 12/2013 Date of Most Recent Update: March 23, 2015 Medical
Waitin In The Wings. Esophageal/Tracheal Double Lumen Airway (Combitube ) Indications and Use for the Pre-Hospital Provider
 Indications and Use for the Pre-Hospital Provider") Waitin In The Wings Esophageal/Tracheal Double Lumen Airway (Combitube ) Indications and Use for the Pre-Hospital Provider 1 CombiTube Kit General Description The CombiTube is A double-lumen tube with
Waitin In The Wings Esophageal/Tracheal Double Lumen Airway (Combitube ) Indications and Use for the Pre-Hospital Provider 1 CombiTube Kit General Description The CombiTube is A double-lumen tube with
COPD. Helen Suen & Lexi Smith
 COPD Helen Suen & Lexi Smith What is COPD? Chronic obstructive pulmonary disease: a non reversible, long term lung disease Characterized by progressively limited airflow and an inability to perform full
COPD Helen Suen & Lexi Smith What is COPD? Chronic obstructive pulmonary disease: a non reversible, long term lung disease Characterized by progressively limited airflow and an inability to perform full
Chronic obstructive lung disease. Dr/Rehab F.Gwada
 Chronic obstructive lung disease Dr/Rehab F.Gwada Obstructive lung diseases Problem is in the expiratory phase Lung disease Restrictive lung disease Restriction may be with, or within the chest wall Problem
Chronic obstructive lung disease Dr/Rehab F.Gwada Obstructive lung diseases Problem is in the expiratory phase Lung disease Restrictive lung disease Restriction may be with, or within the chest wall Problem
The Respiratory System
 BIOLOGY OF HUMANS Concepts, Applications, and Issues Fifth Edition Judith Goodenough Betty McGuire 14 The Respiratory System Lecture Presentation Anne Gasc Hawaii Pacific University and University of Hawaii
BIOLOGY OF HUMANS Concepts, Applications, and Issues Fifth Edition Judith Goodenough Betty McGuire 14 The Respiratory System Lecture Presentation Anne Gasc Hawaii Pacific University and University of Hawaii
CHAPTER 7.1 STRUCTURES OF THE RESPIRATORY SYSTEM
 CHAPTER 7.1 STRUCTURES OF THE RESPIRATORY SYSTEM Pages 244-247 DO NOW What structures, do you think, are active participating in the breathing process? 2 WHAT ARE WE DOING IN TODAY S CLASS Finishing Digestion
CHAPTER 7.1 STRUCTURES OF THE RESPIRATORY SYSTEM Pages 244-247 DO NOW What structures, do you think, are active participating in the breathing process? 2 WHAT ARE WE DOING IN TODAY S CLASS Finishing Digestion
San Benito County EMS Agency Section 700: Patient Care Procedures
 Purpose: To outline the steps EMTs & paramedics will take to manage possible life threats in any child or adult patient they encounter. This policy is in effect for all treatment protocols & is to be referred
Purpose: To outline the steps EMTs & paramedics will take to manage possible life threats in any child or adult patient they encounter. This policy is in effect for all treatment protocols & is to be referred
Advanced Airway Management. University of Colorado Medical School Rural Track
 Advanced Airway Management University of Colorado Medical School Rural Track Advanced Airway Management Basic Airway Management Airway Suctioning Oxygen Delivery Methods Laryngeal Mask Airway ET Intubation
Advanced Airway Management University of Colorado Medical School Rural Track Advanced Airway Management Basic Airway Management Airway Suctioning Oxygen Delivery Methods Laryngeal Mask Airway ET Intubation
NIV - BI-LEVEL POSITIVE AIRWAY PRESSURE (BIPAP)
") Introduction NIV - BI-LEVEL POSITIVE AIRWAY PRESSURE (BIPAP) Noninvasive ventilation (NIV) is a method of delivering oxygen by positive pressure mask that allows for the prevention or postponement of invasive
Introduction NIV - BI-LEVEL POSITIVE AIRWAY PRESSURE (BIPAP) Noninvasive ventilation (NIV) is a method of delivering oxygen by positive pressure mask that allows for the prevention or postponement of invasive
Chapter 13. Respiratory Emergencies
 Student Notes Chapter 13: Respiratory Emergencies 1 Chapter 13 Respiratory Emergencies Unit Summary After students complete this chapter and the related course work, they will understand the significance
Student Notes Chapter 13: Respiratory Emergencies 1 Chapter 13 Respiratory Emergencies Unit Summary After students complete this chapter and the related course work, they will understand the significance
Introduction. Topics. Seattle/King County EMT-B Class. EMS Online. Class schedule Message board Lecture presentations
 Seattle/King County EMT-B Class Introduction EMS Online http://www.emsonline.net/emtb Class schedule Message board Lecture presentations Topics Airway Management: Chapter 7 Patient Assessment: Chapter
Seattle/King County EMT-B Class Introduction EMS Online http://www.emsonline.net/emtb Class schedule Message board Lecture presentations Topics Airway Management: Chapter 7 Patient Assessment: Chapter
student handbook BARS handbook September 2012.indd Front Cover 27/11/12 12:08 PM
 student handbook BARS handbook September 2012.indd Front Cover 27/11/12 12:08 PM All materials regarding the Basic Airway Resuscitation Strategy Course were written and developed by Dr. Richard Morris
student handbook BARS handbook September 2012.indd Front Cover 27/11/12 12:08 PM All materials regarding the Basic Airway Resuscitation Strategy Course were written and developed by Dr. Richard Morris
Anatomy and Physiology. The airways can be divided in to parts namely: The upper airway. The lower airway.
 Airway management Anatomy and Physiology The airways can be divided in to parts namely: The upper airway. The lower airway. Non-instrumental airway management Head Tilt and Chin Lift Jaw Thrust Advanced
Airway management Anatomy and Physiology The airways can be divided in to parts namely: The upper airway. The lower airway. Non-instrumental airway management Head Tilt and Chin Lift Jaw Thrust Advanced
an inflammation of the bronchial tubes
 BRONCHITIS DEFINITION Bronchitis is an inflammation of the bronchial tubes (or bronchi), which are the air passages that extend from the trachea into the small airways and alveoli. Triggers may be infectious
BRONCHITIS DEFINITION Bronchitis is an inflammation of the bronchial tubes (or bronchi), which are the air passages that extend from the trachea into the small airways and alveoli. Triggers may be infectious
Appendix (i) The ABCDE approach to the sick patient
 The ABCDE approach to the sick patient") Appendix (i) The ABCDE approach to the sick patient This appendix and the one following provide guidance on the initial approach and management of common medical emergencies which may arise in general
Appendix (i) The ABCDE approach to the sick patient This appendix and the one following provide guidance on the initial approach and management of common medical emergencies which may arise in general
BiLevel Pressure Device
 PROCEDURE - Page 1 of 7 Purpose Scope Classes/ Goals Define indications and care settings for acute and chronic initiation of Noninvasive Positive Pressure Ventilation. Identify the role of Respiratory
PROCEDURE - Page 1 of 7 Purpose Scope Classes/ Goals Define indications and care settings for acute and chronic initiation of Noninvasive Positive Pressure Ventilation. Identify the role of Respiratory
Nassau Regional Emergency Medical Services. Advanced Life Support Pediatric Protocol Manual
 Nassau Regional Emergency Medical Services Advanced Life Support Pediatric Protocol Manual 2014 PEDIATRIC ADVANCED LIFE SUPPORT PROTOCOLS TABLE OF CONTENTS Approved Effective Newborn Resuscitation P 1
Nassau Regional Emergency Medical Services Advanced Life Support Pediatric Protocol Manual 2014 PEDIATRIC ADVANCED LIFE SUPPORT PROTOCOLS TABLE OF CONTENTS Approved Effective Newborn Resuscitation P 1