Five Consecutive cases of Bronchial Thermoplasty
|
|
|
- Rodger Weaver
- 5 years ago
- Views:
Transcription
1 Five Consecutive cases of Bronchial Thermoplasty -Hiren J. Mehta MD Assistant Professor of Medicine Interventional Pulmonology University of Florida
2 none Disclosures
3 Asthma Overview: Prevalence, Morbidity and Mortality 24.6 million People diagnosed with asthma 12.8 million People experience asthma attacks 1.8 million Emergency room visits 456,000 Hospitalizations 3,447 Asthma-related deaths Approximately 9 People Die From Asthma Each Day in the U.S. Annual incidence, based on 2007 data Centers for Disease Control and Prevention National Center for Health Statistics, National Health Statistics Report: Asthma Prevalence, Health Care Use, and Mortality: United States, :
4 Stepwise Approach for Managing Asthma 6 High-dose ICS + LABA + Oral Corticosteroids and Consider Omalizumab Alternatives Needed 5 High-dose ICS + LABA and Consider Omalizumab 4 Medium-dose ICS + LABA 3 Low-dose ICS + Long-acting Beta 2 -agonists (LABA) or Medium-dose ICS 2 Low-dose Inhaled Corticosteroids (ICS) 1 Short-acting Beta 2 -agonists Adapted from National Asthma Education and Prevention Program (NAEPP) Guidelines. Expert Panel Report 3: Guidelines for the Diagnosis and Management of Asthma. National Heart, Lung, and Blood Institute, NIH Publication No , Revised August 2007.
5 Challenges in Managing Severe Asthma Prevalence of severe asthma (NAEPP) = 5-10% Many patients remain symptomatic despite standard of care medications Medications are limited, require adherence, and can have serious side effects High economic costs and resource utilization associated with medications, hospitalizations, physician visits and lost days of work/school ~ $20.7B Additional therapeutic treatment options are needed
6 What is Bronchial Thermoplasty? A procedure that delivers thermal energy to the airways via a bronchoscope to reduce excess airway smooth muscle and limit its ability to constrict the airways Outpatient hospital procedure performed over 3 treatment sessions, routinely under moderate sedation Complementary treatment, and not a replacement, to current asthma reliever and controller medications
7 Bronchial Thermoplasty Rationale Reduced Excessive Airway Smooth Muscle (ASM) Reduced Ability for Bronchoconstriction Reduced Asthma Symptoms and Exacerbations Improved Asthma Control and Quality of Life


8 Reduced ASM 12 Days Post-Treatment Ciliated Epithelium ASM ASM Reduced Ciliated Epithelium Untreated Treated Miller et al. CHEST 2005; 127:1999


9 The Alair Bronchial Thermoplasty System Alair Catheter a flexible tube with an expandable wire array at the tip (introduced into the lungs through a standard bronchoscope) Alair Radiofrequency (RF) Controller supplies energy via the Catheter to heat the airway wall
10 Case # 1 44 year old female referred for difficult to treat Asthma. History of asthma since childhood. Worse in the last 5-7 years. Current symptoms include wheezing and chest tightness 2-3 times a day requiring rescue inhaler.
11 Case # 1 She usually has 4-5 exacerbations a year requiring steroids and or hospitalizations. Last hospitalization in 2004 and last ER visit in Dec Never been intubated. Patient has been seen by multiple pulmonologist in the past
12 Case # 1 Spent 3 month in the national Jewish center and weeks at Duke for Asthma management. Symptoms persisted and as a teenager she was on steroids for 11 years.
13 Case # 1 Past Medical History: Asthma GERD Esophageal stricture Surgical History: Esophageal dilatation Sinus polyps removed 3 C sections Plastic surgery
14 Case# 1 Social History: She is a nonsmoker. Marital Status: married Children:3 Education: Bachelor Occupation(s): Ultrasound technician full time job Pets:dog. Pets are indoor.
15 Case # 1 Medications: Advair HFA Puffs BID Nasonex nasal spray Zafirlukast 20 mg PO BID Albuterol 90 mcg 2 puffs q 4hrs PRN Theophylline 300 mg CR BID Protonix 40 mg PO BID
16 Case # 1 PHYSICAL EXAM: BP 140/63 Pulse 70 Temp(Src) 36.3 C (97.4 F) (Oral) Resp 20 Ht m (5' 1") Wt 65 kg (143 lb 4.8 oz) BMI kg/m2 SpO2 97%Body mass index is kg/(m^2).
17 Case # 1 Pulmonary: clear to auscultation bilaterally with no wheezes, rhonchi, or crackles Cardiovascular: S1, S2 normal, no murmur, rub or gallop, regular rate and rhythm Abdomen: soft, non-tender, nondistended and active bowel sounds.
18
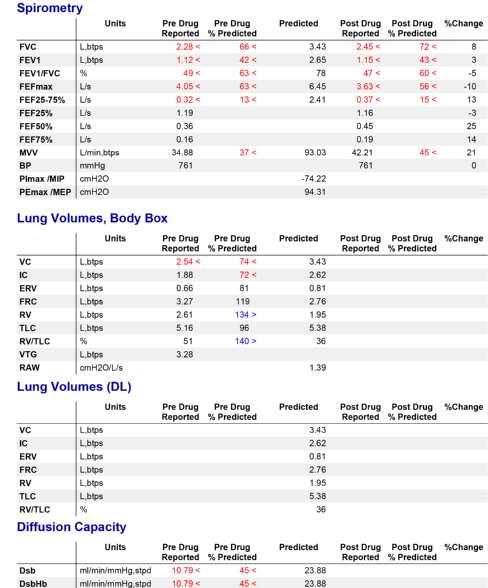
19 Case # 1
20 Case # 1 Spiriva 18 mcg once daily Sleep study ordered Inhaler use assessed Xolair tried in past.. Follow up in 3 months
21 Case # 1 3 months later. 1 more exacerbation requiring oral steroids. Continues to have frequent bronchodilator use. Sleep study: negative
22 Case # 1 Bronchial Thermoplasty was performed. 1 st Session >>> LLL >>> 95 activations 2 nd Session >>> RLL >>> 108 activations 3rd Session >>> LUL and RUL >>> 178 activations
23 Case # 1 Follow up at 1 year Improved QOL including better effort tolerance Decreased frequency of rescue inhaler to once weekly. No exacerbations requiring prednisone or ER visit
24 AIR1 Study
25 AIR1 Study Randomized, nonblinded study BT vs usual medical care Inclusion criteria Moderate or severe persistent asthma, defined according to the guidelines of the Global Initiative for Asthma Requiring daily therapy with ICS equivalent to a dose > 200 μg or more of beclomethasone and LABA at a dose of >100 μg salmeterol or the equivalent Airflow obstruction: prebronchodilator FEV % predicted value and airway hyperresponsiveness, defined by a methacholine challenge PC20 < 8 mg/ml Cox et al. NEJM 2007; 356:1327
26 AIR1 Study 11 centers in four countries Randomly assigned 112 subjects treated with ICS and LABAs and in whom asthma control was impaired when the LABA were withdrawn to either bronchial thermoplasty (n=56) or a control group (n=56) Therapy with ICS and LABA was resumed for the treatment period At 3 months asked to refrain from using LABA after this point unless they had a severe exacerbation or poor asthma control Cox et al. NEJM 2007; 356:1327
27 AIR1 Study For subjects whose asthma could be controlled without LABA, evaluations were performed after 6 and 12 months of treatment with ICS alone Subjects who needed to resume LABA therapy before 6 and 12 months visits were evaluated at those assessment points after withdrawal from LABA therapy for 2 weeks Adverse events Increase in cough and dyspnea in some patients day after procedure, majority resolved by 7 days 3% of events were listed as severe 6 hospitalizations in BT group, 2 in control group Similar during the period from 6 weeks to 12 months after treatment Cox et al. NEJM 2007; 356:1327
28 AIR1 Study Results at 12 months significantly greater improvements in the BT group vs control group for: Morning peak expiratory flow (39.3±48.7 vs 8.5±44.2 liters per minute) Scores on the AQLQ (1.3±1.0 vs 0.6±1.1) ACQ scores (reduction, 1.2±1.0 vs 0.5±1.0) Percentage of symptom-free days (40.6±39.7 vs17.0±37.9) Symptom scores (reduction, 1.9±2.1 vs 0.7±2.5) Fewer puffs of rescue medication were required Cox et al. NEJM 2007; 356:1327
29 AIR1 Study

30 AIR1 Study
31 Case # 2 60 y F with history of severe asthma x 30yrs Intubation leading to tracheotomy in 2003 Annual admissions for asthma exacerbations Albuterol 6 x a day and her duonebs 2 x daily Currently still taking 20mg of prednisone daily
32 Case # 2 Unable to tolerate ICS/LABA and or Spiriva due to: - Increased SOB - Recurrent URTI - Increased cough Could not tolerate Singulair due to gastric side effects. Theophylline did not benefit
33 Case # 2 Work up so far has included: - normal IgE levels - Sinus surgeries several years ago with no more episodes of sinusitis - negative sleep study - negative allergy and autoimmune tests - normal gastric ph testing
34 Case # 2 Past Medical History: asthma & bronchitis sinusitis Surgical History: C section Tracheotomy
35 Case # 2 Social History: She reports that she has never smoked. Children:4 Passive Smoking Exposure: yes, exposed for 18 years Pets: cat and dog. Pets are indoor. Functional Capacity: Class 2
36 Case # 2 Medications: Albuterol HFA 90 2 puffs q 4 hrs PRN Duonebs (0.5/2.5) 3 mls q 6 hrs PRN Prednisone 20 mg PO daily Allegra 180 mg PO daily
37 Case # 2 PHYSICAL EXAM: BP: 130/75 mmhg Temp: 36.8 C (98.2 F) Pulse: 112 Resp: 24 SpO2: 96 % Height: 160 cm (5' 3") Weight: kg (122 lb) Body mass index is kg/(m2).
38 Case # 2 Pulmonary: Wheezing bilaterally Cardiovascular: S1, S2 normal, no murmur, rub or gallop, regular rate and rhythm Abdomen: soft, non-tender, nondistended.

39 Case # 2
40 Case # 2
41 Case # 2 Bronchial Thermoplasty was performed. 1st Session >>> RLL >>> 76 activations 2nd Session >>> LLL >>> 65 activations 3rd Session >>> LUL and RUL >>> 98 activations
42 Case # 2 Follow up after 3 Months Improved QOL including better effort tolerance No exacerbations requiring prednisone or ER visit Patient weaned off oral prednisone
43 Case # 2

44 RISA Study
45 RISA Study 32 patients with severe, symptomatic asthma randomized to BT vs usual care Inclusion criteria High-dose ICS (750 mcg fluticasone/day or equivalent) and LABA (> 100 mcg salmeterol per day or equivalent) With or without oral prednisone (<30 mg/d), LTA, or theophylline Prebronchodilator FEV1 > 50% of predicted Demonstrable airway hyperresponsiveness by methacholine challenge with methacholine or increase in FEV1 of at least 12% with SABA Uncontrolled symptoms despite taking maintenance medication Use of rescue medication on at least 8 of the 14 days before enrollment Daytime symptoms on at least 10 of the 14 days before enrollment) Abstinence from smoking for 1 year or greater and past smoking history of less than 10 pack-years Pavord et al. Am J Respir Crit Care Med 2007; 176:1185
46 RISA Study After the treatment period Subjects entered a 16-week steroid stable phase (Weeks 6 22) Followed by a 14-week steroid wean phase (Weeks 22 36) A 16-week reduced steroid phase (Weeks 36 52) During the steroid wean phase Attempted to wean subjects, following a prospectively defined protocol, from oral corticosteroids (OCS) or ICS OCS dose was reduced by 20 to 25% of the baseline dose in steps of 2 weeks each For subjects successfully weaned to OCS daily doses of mg, further attempts to reduce the OCS dose were per investigator discretion For subjects taking only ICS/LABA, the ICS dose was tapered in three stages by 20 to 25% of the baseline dose every 4 weeks to a minimal dose of mcg/day of fluticasone or equivalent Pavord et al. Am J Respir Crit Care Med 2007; 176:1185

47 RISA Study Change in rescue inhaler: puffs/7 days Change in pre- BD FEV1: % predicted Change in AQLQ scores Change in ACQ scores Black bars-bt group; White bars-control group
48 RISA Study BT subjects had significant improvements vs control subjects in: Rescue medication use (-26.6 vs 1.5 puffs/7 d, P<0.05) Prebronchodilator FEV1% predicted (14.9 vs 0.94, P=0.04) ACQ scores ( vs , P=0.02) 4/8 BT patients vs 1/7 controls weaned off OCS Reduction in OCS dose 63% vs 26% 7 hospitalizations for respiratory symptoms in 4/15 BT subjects during the treatment period 5 hospitalizations were within 3 days of treatment 2 subjects had segmental collapse involving the most recently treated lobe; 1 required bronchoscopy and aspiration of a mucus plug Pavord et al. Am J Respir Crit Care Med 2007; 176:1185
49 Case # 3 44 y F with refractory Asthma. Diagnosed with Asthma at the age of 31 after her last pregnancy. Multiple ER and unscheduled office visits for asthma exacerbations. Several courses of oral prednisone in the last 2 years.
50 Case # 3 Work up so far has included: - Positive GERD w/u s/p fundoplication - Chronic sinusitis s/p sinus surgeries - Negative sleep study - Normal IgE levels and RAST panel.
51 Case # 3 Past Medical History: Asthma; GERD; and Obesity. Surgical History: sinus surgery; partial hysterectomy; Cholecystectomy; Gastric fundoplication; Carpal tunnel release (2011); Bunionectomy;
52 Case # 3 Social History: She reports that she has never smoked. Marital Status: married Children:3 Education: high school Occupation(s): administrative assistant in medical office full time job Pets:dog. Pets are indoor.
53 Case # 3 Medications: Albuterol 90 mcg 2 puffs bid q 4 hrs PRN Albuterol 2.5 mg nebulizer q 6 hrs PRN Montelukast 10 mg nightly QVAR 80 mcg 1 puff bid Advair (50/500) 1 puff bid Nasonex Prilosec 20 mg Po bid
54 Case # 3 PHYSICAL EXAM: BP 106/72 Pulse 86 Temp(Src) 36.8 C (98.2 F) Resp 20 Ht m (5') Wt kg (192 lb 8 oz) BMI kg/m2 SpO2 98% BMI is kg/(m2).
55 Case # 3 Physical Exam: Pulmonary: clear to auscultation bilaterally wheezes present L base Cardiovascular: S1, S2 normal, no murmur, rub or gallop, regular rate and rhythm Abdomen: soft, non-tender, nondistended and active bowel sounds.


56 Case # 3

57 Case # 3
58 Case # 3 Bronchial Thermoplasty was performed. 1st Session >>> LLL >>> 127 activations 2nd Session >>> RLL >>> 102 activations 3rd Session >>> LUL and RUL >>> 197 activations
59 Case # 3 Pt had Chest pains and tightness after each treatment. Required unscheduled office visit 3 days after last treatment. Received 7 days of Prednisone and antibiotics.
60 Case # 3 On 3 months follow up: - No more exacerbations - Improved QOL and ability to perform ADL s - Decreased use of rescue medications.
61 Case # 3

62 AIR2 Study
 Other medications allowed: LTAs, omalizumab (if used for at least 1 year prior), and oral corticosteroids (10 mg/d or less) Key inclusion criteria were")
63 AIR2 study Multicenter, international, randomized trial BT vs usual medical care with sham control group Inclusion criteria Maintenance medications of ICS (>1,000 mcg/d beclomethasone or equivalent) and LABA (>100 mcg/d salmeterol or equivalent) Other medications allowed: LTAs, omalizumab (if used for at least 1 year prior), and oral corticosteroids (10 mg/d or less) Key inclusion criteria were Subjects on stable medication regimen Baseline Asthma Quality of Life Questionnaire (AQLQ) score 6.25 or lower Prebronchodilator FEV1 >60% of predicted Airway hyperresponsiveness (methacholine PC20 <8 mg/ml) At least 2 days of asthma symptoms during the 4-week baseline period Nonsmoker for at least 1 year with less than 10 pack-years smoking history Castro et al. Am J Respir Crit Care Med 2010; 181:116
64 Percentage of Subjects Changes in AQLQ Scores Percentage of Subjects Achieving AQLQ Score > 0.5 (MID) Treated Per Protocol < -0.5 > to < 0.5 > 0.5 Change in Baseline from Average AQLQ Score ** Posterior Probability of Superiority = 99.6% ** Sham BT
65 Events / Subject/ Year Health Care Utilization for Respiratory Symptoms During Post-Treatment Period 6 weeks after the last bronchoscopy procedure to 12 month follow-up 0.9 * Posterior Probability of Superiority = 95.6% ** Posterior Probability of Superiority = 99.9% * 32% decrease over Sham ** Sham BT % decrease over Sham Severe Exacerbations (Steroid) Unscheduled Physician Office Visits 84% decrease over Sham 0.07 Emergency Room Visits Hospitalizations 73% decrease over Sham
66 Respiratory Symptoms Resulting in Hospitalization Following Procedure BT (N=190) 19 Hospitalizations in 16 Subjects No. of Events (Incident Rate %) Sham (N=98) 2 Hospitalizations in 2 Subjects No. of Events (Incident Rate %) Asthma Aggravated 12 (6.3%) Asthma Aggravated 2 (2.0%) Atelectasis 3 (1.6%) Lower Resp. Tract Infect. 1 (0.5%) Hemoptysis 1 (0.5%) Low FEV 1 1 (0.5%) Aspirated prosthetic tooth in airway 1 (0.5%) Castro et al. Am J Respir Crit Care Med 2010; 181:116
67 Case # 4 57-year-old white male with history of asthma since childhood. Worsening symptoms in the last few years. Several asthma hospitalizations. No intubations. Symptoms include: daily tightness and almost daily nighttime awakenings
68 Case # 4 Rescue inhaler use from 5 times/day to 5 times a week. Impaired effort tolerance: Police officer pulled off from field to desk. On Xolair for the last 3 years and multiple bouts of Prednisone.
69 Case # 4 Past Medical History: Asthma, hypertension, sinus polyps/allergies. Past Surgical History: Polypectomy years ago. Social History: He has never smoked. Occasional use of alcohol. He works as a major in the police department.
70 Case # 4 Medications: Advair 500/50 1 puff bid Spiriva 18 mcg 1 puff daily Albuterol 80 mcg 2 puffs q 4 hrs PRN Albuterol 2.5 mg nebulizer PRN Xolair once every 4 weeks
71 Case # 4 Physical Exam: Height 182 cm, weight 92.5 kg, temperature 98.2, pulse 87, respiratory rate 20, oxygen saturation 93% on room air, blood pressure 134/73.
72 Case # 4 HEENT: PERRLA. EOMI. Conjunctivae nonicteric. Intraoral nasopharynx normal. Cardiovascular: Regular rate and rhythm. No murmurs, rubs, or gallops. Respiratory: Bilateral inspiratory and expiratory wheezes. Abdomen: Soft, nontender, nondistended. No hepatosplenomegaly.

73 Case # 4

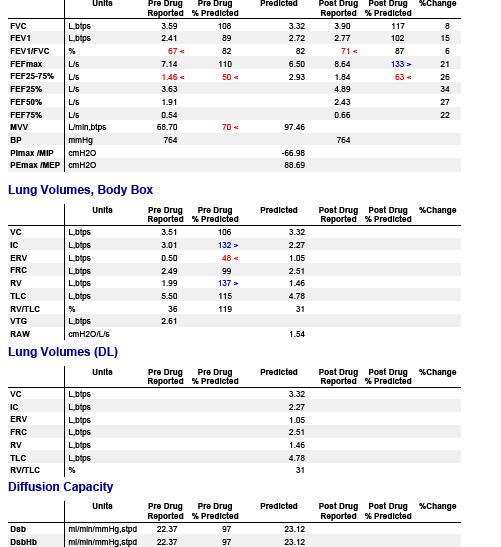
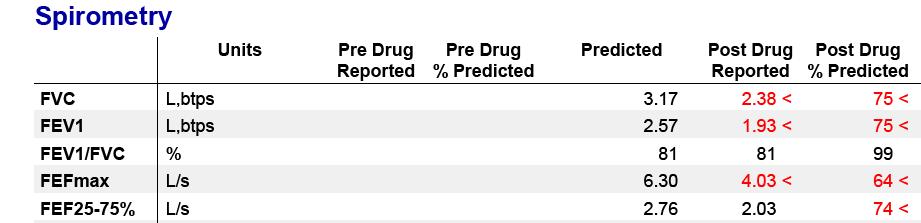
74 Case # 4 FVC of 4.36 liters or 90% predicted FEV1 of 2.33 liters or 61% predicted FEV1/FVC ratio of 53% FEF 25/75 was 1.26 liters or 35% predicted. DLCO 76% of predicted
75 Case # 4 Bronchial Thermoplasty was performed. 1st Session >>> RLL >>> 79 activations 2nd Session >>> LLL >>> 111 activations 3rd Session >>> LUL and RUL >>> 129 activations
76 Case # 4 6 months follow up: - Patient had no more flares. - No use of PO Prednisone. - Back to field work with no DOE. - Patient stopped using ICS as he did not feel the need for it.
77 Case # 4
78 AIR1 Follow-Up
79 AIR1 5 Year Follow-up Rate of respiratory adverse events (AEs/subject) was stable in years 2 to 5 following BT (1.2,1.3, 1.2, and 1.1, respectively,) No increase in hospitalizations or emergency room visits for respiratory symptoms in Years 2, 3, 4, and 5 compared to Year 1 FVC and FEV1 values showed no deterioration over the 5 year period in the BT group Mean reduction from baseline in ICS dose for BT subjects was 182 μg/day, 135 μg/day, 150, 151 μg/day, and 194 μg/day at Years 1, 2, 3, 4, and 5 respectively 57% of BT subjects reported a decrease in LABA use, 40% of subjects reported no change in LABA use, and 3% reported an increase in LABA use Sustained improvement over baseline in the methacholine PC20 doubling in the BT group compared to the control group in each year out to Year 3 Thomson et al. BMC Pulmonary Medicine 2011; 11:8



80 RISA 5 Year Extension Study Overall hospitalization rate 0.23 per patient per year vs 0.71 prior to BT ED visits 0.12 per patient per year vs 0.36 prior to BT FEV1 remained stable over 5 years Pavord et al. Ann Allergy Asthma Immunol 2013; 111:402

81 AIR2 Follow-Up
82 AIR2 Follow-up Long-term safety follow-up phase of the Asthma Intervention Research 2 (AIR2) Trial Evaluated proportion of subjects who experienced exacerbations, adverse events, or healthcare utilization during the first 2 years after treatment Pre- and post-bronchodilator FEV1 values remained stable between year 1 and year 2 after BT Castro et al. Ann Allergy Asthma Immunol 2011; 107:65
83 AIR2 Follow-Up Severe exacerbations Respiratory adverse events Baseline Sham Year 1 Sham Percentage of Subjects Baseline BT Year 1 BT Year 2 BT ER visits Hospitalizations Respiratory adverse events: wheezing, dyspnea, cough, chest discomfort, nocturnal awakenings, URI, chest congestion, nasal congestion, throat irritation Castro et al. Ann Allergy Asthma Immunol 2011; 107:65

84 AIR2 5 Year Follow-Up Data Severe exacerbations decreased by 44% ED visits decreased by 78% Weschler et al. J Allergy Clin Immunol 2013; 132:1295
85 AIR2 5 Year Follow-Up Data Weschler et al. J Allergy Clin Immunol 2013; 132:1295
86 AIR2 5 Year Follow-Up Data HRCT evaluation 3 patients noted to have bronchiectasis 1 with worsened pre-existing bronchiectasis 1 had bronchiectasis in 2 lobes including untreated RML 1 had new bronchiectasis No evidence of bronchial stenosis or bronchiolitis obliterans in any patient Medication changes 28% had a > 50% decrease in ICS dose 12% weaned off LABA 9% weaned off LABA and ICS 7% required no maintenance asthma medications Weschler et al. J Allergy Clin Immunol 2013; 132:1295
87 Case # 5 60 year old female with dyspnea and cough. Symptoms since the last 18 months. Cough associated with greenish expectoration. DOE with ADL s Multiple courses of antibiotics and steroids in the last 18 months. Lower extremity edema.
88 Case # 5 Past Medical History: Asthma COPD CAD Social History: 50 pack year. Quit a year ago. Owner of a tile company. Denies any exposures. No pets.
89 Case # 5 Medications: Aclidinium 400 mcg 2 puffs bid Asmanex 80 mcg 2 puffs bid Albuterol MDI 2 puffs q 4 hrs PRN Prednisone 20 mg PO daily Daliresp 500 mcg PO daily
90 Case # 5 Physical Examination: BP: 111/78 mmhg Temp: 37.1 C (98.8 F) Pulse: 92 Resp: 20 SpO2: 93 % (2 lit/min) Height: cm (5' 5") Weight: kg Body mass index is kg/(m^2).
91 Case # 5 Pulmonary: clear to auscultation bilaterally with no wheezes, rhonchi, or crackles Cardiovascular: S1, S2 normal, no murmur, rub or gallop, regular rate and rhythm Abdomen: soft, non-tender, nondistended.
92 Case # 5 ( )

93 Case # 5
94 Case # 5
95 Case # 5 Other investigations to date: - Normal IgE levels. - Sleep study was normal. - Normal AAT levels. - ECHO shows diastolic dysunction.
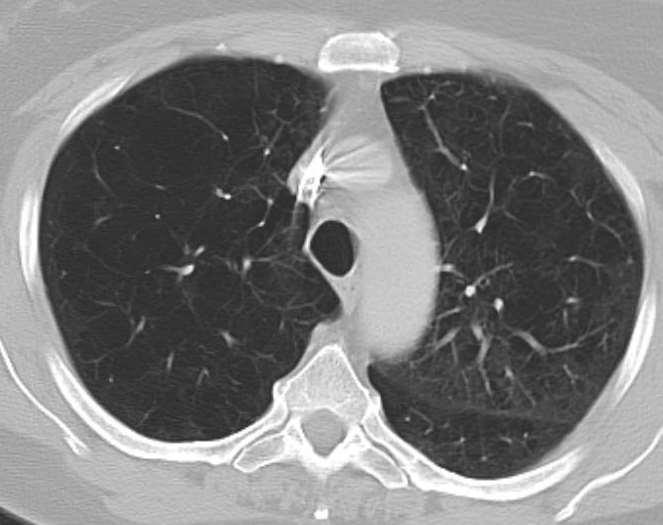
96 Case # 5 Assessment: Patient has significant emphysema. Unlikely that patient has pure asthma. Patient will not benefit from BT since emphysema appears to be the predominant pathology.
97 Case # 5 Following Medications adjustments were made: Asmanex switched to Dulera Azithromycin 250 mg PO qod Theophylline SR 400 md nightly Lasix 20 mg PO bid
98 Who is Appropriate for Bronchial Thermoplasty? FDA Indication: The Alair Bronchial Thermoplasty System has been approved by the FDA for the treatment of severe persistent asthma in patients 18 years and older whose asthma is not well controlled with inhaled corticosteroids and long-acting beta-agonists. Adult severe, persistent asthmatics ( 18 years old) Inadequate control despite combination of inhaled high dose corticosteroids (ICS) and a long-acting beta-agonists (LABA) Estimated 5% of asthma patients are severe persistent and not well controlled, therefore may be BT candidates Able to safely undergo bronchoscopy per hospital guidelines
99 Who is Not Appropriate for Bronchial Thermoplasty? Contraindications: Patients that have a pacemaker, internal defibrillator, or other implantable electronic device Patients that have a known sensitivity to medications required to perform bronchoscopy, including lidocaine, atropine, and benzodiazepines Patients that have previously been treated with the Alair System

100
Bronchial Thermoplasty For Severe Persistent Asthma
 Bronchial Thermoplasty For Severe Persistent Asthma Faisal Khan MD Center For Respiratory and Sleep Medicine Indiana Internal Medicine Consultants Franciscan Saint Francis hospital Agenda Burden of Severe
Bronchial Thermoplasty For Severe Persistent Asthma Faisal Khan MD Center For Respiratory and Sleep Medicine Indiana Internal Medicine Consultants Franciscan Saint Francis hospital Agenda Burden of Severe
Endobronchial Thermoplasty
 Endobronchial Thermoplasty Asthma Education Day Thursday, October 30, 2014 Cynthia Ray, MD, FCCP Senior Staff Physician Interventional Pulmonology Pulmonary and Critical Care Medicine Henry Ford Hospital
Endobronchial Thermoplasty Asthma Education Day Thursday, October 30, 2014 Cynthia Ray, MD, FCCP Senior Staff Physician Interventional Pulmonology Pulmonary and Critical Care Medicine Henry Ford Hospital
Endobronchial Thermoplasty
 Endobronchial Thermoplasty Michigan Society for Respiratory Care Monday, October 5, 2015 Cynthia Ray, MD, FCCP Senior Staff Physician Interventional Pulmonology Pulmonary and Critical Care Medicine Henry
Endobronchial Thermoplasty Michigan Society for Respiratory Care Monday, October 5, 2015 Cynthia Ray, MD, FCCP Senior Staff Physician Interventional Pulmonology Pulmonary and Critical Care Medicine Henry
Complements asthma therapy NOT a CURE for Severe. Non pharmacologic treatment of asthma. limits the ability of the airways to constrict.
 Bronchial Thermoplasty Karla Provost Pulmonary and Critical Care Medicine 2015 What is Bronchial Thermoplasty Non pharmacologic treatment of asthma Outpatient procedure performed over 3 treatment sessions
Bronchial Thermoplasty Karla Provost Pulmonary and Critical Care Medicine 2015 What is Bronchial Thermoplasty Non pharmacologic treatment of asthma Outpatient procedure performed over 3 treatment sessions
What is Severe Persistent Asthma? What is Bronchial Thermoplasty Non pharmacologic treatment of asthma
 Objectives BT defined What is Severe Persistent Asthma Case Study introduction How is BT performed Pre-op, PACU and Discharge care Who does it work for the criteria for BT Brief overview of BT results
Objectives BT defined What is Severe Persistent Asthma Case Study introduction How is BT performed Pre-op, PACU and Discharge care Who does it work for the criteria for BT Brief overview of BT results
Robert Kruklitis, MD, PhD Chief, Pulmonary Medicine Lehigh Valley Health Network
 Robert Kruklitis, MD, PhD Chief, Pulmonary Medicine Lehigh Valley Health Network Robert.kruklitis@lvh.com Correlation of a Asthma pathophyisology with basic science Asthma (Physiology) Bronchodilators
Robert Kruklitis, MD, PhD Chief, Pulmonary Medicine Lehigh Valley Health Network Robert.kruklitis@lvh.com Correlation of a Asthma pathophyisology with basic science Asthma (Physiology) Bronchodilators
Smooth Muscle & Asthma: Bronchial Thermoplasty - A Smooth Muscle Modifier
 Smooth Muscle & Asthma: Bronchial Thermoplasty - A Smooth Muscle Modifier Mario Castro, MD, MPH Professor of Medicine and Pediatrics Director, The Asthma and Airway Translational Research Unit, Washington
Smooth Muscle & Asthma: Bronchial Thermoplasty - A Smooth Muscle Modifier Mario Castro, MD, MPH Professor of Medicine and Pediatrics Director, The Asthma and Airway Translational Research Unit, Washington
Corporate Medical Policy
 Corporate Medical Policy File Name: Origination: Last CAP Review: Next CAP Review: Last Review: bronchial_thermoplasty 10/2010 3/2018 3/2019 3/2018 Description of Procedure or Service Bronchial thermoplasty
Corporate Medical Policy File Name: Origination: Last CAP Review: Next CAP Review: Last Review: bronchial_thermoplasty 10/2010 3/2018 3/2019 3/2018 Description of Procedure or Service Bronchial thermoplasty
Bronchial Thermoplasty
 Bronchial Thermoplasty Policy Number: 7.01.127 Last Review: 9/2014 Origination: 11/2010 Next Review: 3/2015 Policy Blue Cross and Blue Shield of Kansas City (Blue KC) will not provide coverage for bronchial
Bronchial Thermoplasty Policy Number: 7.01.127 Last Review: 9/2014 Origination: 11/2010 Next Review: 3/2015 Policy Blue Cross and Blue Shield of Kansas City (Blue KC) will not provide coverage for bronchial
BRONCHIAL THERMOPLASTY
 Review Article 155 BRONCHIAL THERMOPLASTY Prince James* and Richa Gupta* (Received on 4.5.2010; Accepted after revision on 5.9.2011) Summary: Even with the use of maximum pharmacological treatment, asthma
Review Article 155 BRONCHIAL THERMOPLASTY Prince James* and Richa Gupta* (Received on 4.5.2010; Accepted after revision on 5.9.2011) Summary: Even with the use of maximum pharmacological treatment, asthma
THE PROMISE OF NEW AND NOVEL DRUGS. Pyng Lee Respiratory & Critical Care Medicine National University Hospital
 THE PROMISE OF NEW AND NOVEL DRUGS Pyng Lee Respiratory & Critical Care Medicine National University Hospital Pyng_lee@nuhs.edu.sg Asthma Prevalence, Morbidity, Mortality 235 million suffer from asthma
THE PROMISE OF NEW AND NOVEL DRUGS Pyng Lee Respiratory & Critical Care Medicine National University Hospital Pyng_lee@nuhs.edu.sg Asthma Prevalence, Morbidity, Mortality 235 million suffer from asthma
Learning the Asthma Guidelines by Case Studies
 Learning the Asthma Guidelines by Case Studies Timothy Craig, DO Professor of Medicine and Pediatrics Distinguished Educator Penn State University Hershey Medical Center Objectives 1. Learn the Asthma
Learning the Asthma Guidelines by Case Studies Timothy Craig, DO Professor of Medicine and Pediatrics Distinguished Educator Penn State University Hershey Medical Center Objectives 1. Learn the Asthma
Bronchial Thermoplasty
 Medical Policy Manual Surgery, Policy No. 178 Bronchial Thermoplasty Next Review: September 2018 Last Review: October 2017 Effective: November 1, 2017 IMPORTANT REMINDER Medical Policies are developed
Medical Policy Manual Surgery, Policy No. 178 Bronchial Thermoplasty Next Review: September 2018 Last Review: October 2017 Effective: November 1, 2017 IMPORTANT REMINDER Medical Policies are developed
HCT Medical Policy. Bronchial Thermoplasty. Policy # HCT113 Current Effective Date: 05/24/2016. Policy Statement. Overview
 HCT Medical Policy Bronchial Thermoplasty Policy # HCT113 Current Effective Date: 05/24/2016 Medical Policies are developed by HealthyCT to assist in administering plan benefits and constitute neither
HCT Medical Policy Bronchial Thermoplasty Policy # HCT113 Current Effective Date: 05/24/2016 Medical Policies are developed by HealthyCT to assist in administering plan benefits and constitute neither
Asthma Management Updates: A Focus on Long-acting Muscarinic Antagonists and Intermittent Inhaled Corticosteroid Dosing
 Asthma Management Updates: A Focus on Long-acting Muscarinic Antagonists and Intermittent Inhaled Corticosteroid Dosing Diana M. Sobieraj, PharmD, BCPS Assistant Professor University of Connecticut School
Asthma Management Updates: A Focus on Long-acting Muscarinic Antagonists and Intermittent Inhaled Corticosteroid Dosing Diana M. Sobieraj, PharmD, BCPS Assistant Professor University of Connecticut School
COPD and Asthma Update. April 29 th, 2017 Rachel M Taliercio, DO Staff, Respiratory Institute
 COPD and Asthma Update April 29 th, 2017 Rachel M Taliercio, DO Staff, Respiratory Institute What we ll be talking about COPD: diagnosis, management of stable COPD, COPD exacerbations Asthma: diagnosis,
COPD and Asthma Update April 29 th, 2017 Rachel M Taliercio, DO Staff, Respiratory Institute What we ll be talking about COPD: diagnosis, management of stable COPD, COPD exacerbations Asthma: diagnosis,
12/18/2017. Disclosures. Asthma Management Updates: A Focus on Long-acting Muscarinic Antagonists and Intermittent Inhaled Corticosteroid Dosing
 Asthma Management Updates: A Focus on Long-acting Muscarinic Antagonists and Intermittent Inhaled Corticosteroid Dosing Diana M. Sobieraj, PharmD, BCPS Assistant Professor University of Connecticut School
Asthma Management Updates: A Focus on Long-acting Muscarinic Antagonists and Intermittent Inhaled Corticosteroid Dosing Diana M. Sobieraj, PharmD, BCPS Assistant Professor University of Connecticut School
West of Scotland Difficult Asthma Group Statement of Practice
 West of Scotland Difficult Asthma Group Statement of Practice Member Health Boards: Ayrshire and Arran Dumfries and Galloway Forth Valley Lanarkshire Glasgow INFORMATION ON THE USE OF BRONCHIAL THERMOPLASTY
West of Scotland Difficult Asthma Group Statement of Practice Member Health Boards: Ayrshire and Arran Dumfries and Galloway Forth Valley Lanarkshire Glasgow INFORMATION ON THE USE OF BRONCHIAL THERMOPLASTY
Subject: Bronchial Thermoplasty
 Subject: Bronchial Thermoplasty Guidance Number: MCG-171 Revision Date(s): Original Effective Date: 6/12/14 Medical Coverage Guidance Approval Date: 6/12/14 PREFACE This Medical Guidance is intended to
Subject: Bronchial Thermoplasty Guidance Number: MCG-171 Revision Date(s): Original Effective Date: 6/12/14 Medical Coverage Guidance Approval Date: 6/12/14 PREFACE This Medical Guidance is intended to
Endobronchial thermoplasty for asthma
 Review Article on Aerodigestive Endoscopy Endobronchial thermoplasty for asthma Felix Zamora 1, Roy Cho 1, Madhuri Rao 2, Heidi Gibson 3, H. Erhan Dincer 1 1 Division of Pulmonary, Allergy, Critical Care
Review Article on Aerodigestive Endoscopy Endobronchial thermoplasty for asthma Felix Zamora 1, Roy Cho 1, Madhuri Rao 2, Heidi Gibson 3, H. Erhan Dincer 1 1 Division of Pulmonary, Allergy, Critical Care
Improving the Management of Asthma to Improve Patient Adherence and Outcomes
 Improving the Management of Asthma to Improve Patient Adherence and Outcomes Robert Sussman, MD Atlantic Health System Overlook Medical Center Asthma Remains a Serious Health Risk in the US Every day in
Improving the Management of Asthma to Improve Patient Adherence and Outcomes Robert Sussman, MD Atlantic Health System Overlook Medical Center Asthma Remains a Serious Health Risk in the US Every day in
Bronchial Thermoplasty
 Bronchial Thermoplasty Policy Number: 7.01.127 Last Review: 4/2018 Origination: 11/2010 Next Review: 9/2018 Policy Blue Cross and Blue Shield of Kansas City (Blue KC) will not provide coverage for bronchial
Bronchial Thermoplasty Policy Number: 7.01.127 Last Review: 4/2018 Origination: 11/2010 Next Review: 9/2018 Policy Blue Cross and Blue Shield of Kansas City (Blue KC) will not provide coverage for bronchial
Asthma 2015: Establishing and Maintaining Control
 Asthma 2015: Establishing and Maintaining Control Webinar for Michigan Center for Clinical Systems Improvement (Mi-CCSI) Karen Meyerson, MSN, APRN, NP-C, AE-C June 16, 2015 Asthma Prevalence Approx. 26
Asthma 2015: Establishing and Maintaining Control Webinar for Michigan Center for Clinical Systems Improvement (Mi-CCSI) Karen Meyerson, MSN, APRN, NP-C, AE-C June 16, 2015 Asthma Prevalence Approx. 26
Allwin Mercer Dr Andrew Zurek
 Allwin Mercer Dr Andrew Zurek 1 in 11 people are currently receiving treatment for asthma (5.4 million people in the UK) Every 10 seconds, someone is having a potentially life-threatening asthma attack
Allwin Mercer Dr Andrew Zurek 1 in 11 people are currently receiving treatment for asthma (5.4 million people in the UK) Every 10 seconds, someone is having a potentially life-threatening asthma attack
Meeting the Challenges of Asthma
 Presenter Disclosure Information 11:05 11:45am Meeting the Challenge of Asthma SPEAKER Christopher Fanta, MD The following relationships exist related to this presentation: Christopher Fanta, MD: No financial
Presenter Disclosure Information 11:05 11:45am Meeting the Challenge of Asthma SPEAKER Christopher Fanta, MD The following relationships exist related to this presentation: Christopher Fanta, MD: No financial
GINA. At-A-Glance Asthma Management Reference. for adults, adolescents and children 6 11 years. Updated 2017
 GINA At-A-Glance Asthma Management Reference for adults, adolescents and children 6 11 years Updated 2017 This resource should be used in conjunction with the Global Strategy for Asthma Management and
GINA At-A-Glance Asthma Management Reference for adults, adolescents and children 6 11 years Updated 2017 This resource should be used in conjunction with the Global Strategy for Asthma Management and
Bronchial Thermoplasty for the Treatment of Severe Asthma
 TITLE: Bronchial Thermoplasty for the Treatment of Severe Asthma AUTHOR: Jeffrey A. Tice, MD Assistant Professor of Medicine Division of General Internal Medicine Department of Medicine University of California
TITLE: Bronchial Thermoplasty for the Treatment of Severe Asthma AUTHOR: Jeffrey A. Tice, MD Assistant Professor of Medicine Division of General Internal Medicine Department of Medicine University of California
BRONCHIAL THERMOPLASTY
 BRONCHIAL THERMOPLASTY UnitedHealthcare Community Plan Medical Policy Policy Number: CS014.E Effective Date: July 1, 2017 Table of Contents Page INSTRUCTIONS FOR USE... 1 BENEFIT CONSIDERATIONS... 1 COVERAGE
BRONCHIAL THERMOPLASTY UnitedHealthcare Community Plan Medical Policy Policy Number: CS014.E Effective Date: July 1, 2017 Table of Contents Page INSTRUCTIONS FOR USE... 1 BENEFIT CONSIDERATIONS... 1 COVERAGE
Tips on managing asthma in children
 Tips on managing asthma in children Dr Ranjan Suri Consultant in Respiratory Paediatrics Bupa Cromwell Hospital Clinics: Friday (pm) Asthma in Children Making the diagnosis Patterns of childhood asthma
Tips on managing asthma in children Dr Ranjan Suri Consultant in Respiratory Paediatrics Bupa Cromwell Hospital Clinics: Friday (pm) Asthma in Children Making the diagnosis Patterns of childhood asthma
Provider Respiratory Inservice
 Provider Respiratory Inservice 2 Welcome Opening Remarks We will cover: Definition of Asthma & COPD Evidence based guidelines for diagnosis, evaluation, and management of asthma Evidence based guidelines
Provider Respiratory Inservice 2 Welcome Opening Remarks We will cover: Definition of Asthma & COPD Evidence based guidelines for diagnosis, evaluation, and management of asthma Evidence based guidelines
Asthma Update A/Prof. John Abisheganaden. Senior Consultant, Dept Of Respiratory & Crit Care Medicine Tan Tock Seng Hospital
 Asthma Update - 2013 A/Prof. John Abisheganaden Senior Consultant, Dept Of Respiratory & Crit Care Medicine Tan Tock Seng Hospital Asthma A complex syndrome Multifaceted disease Heterogeneous Genetic and
Asthma Update - 2013 A/Prof. John Abisheganaden Senior Consultant, Dept Of Respiratory & Crit Care Medicine Tan Tock Seng Hospital Asthma A complex syndrome Multifaceted disease Heterogeneous Genetic and
COPD: Current Medical Therapy
 COPD: Current Medical Therapy Angela Golden, DNP, FNP-C, FAANP Owner, NP from Home, LLC Outcomes As a result of this activity, learners will be able to: 1. List the appropriate classes of medications for
COPD: Current Medical Therapy Angela Golden, DNP, FNP-C, FAANP Owner, NP from Home, LLC Outcomes As a result of this activity, learners will be able to: 1. List the appropriate classes of medications for
Difficult Asthma Assessment: A systematic approach
 Difficult Asthma Assessment: A systematic approach Dr Naghmeh Radhakrishna Respiratory, Sleep & Allergy Physician Allergy, Asthma & Clinical Immunology Service The Alfred Hospital Melbourne, Australia
Difficult Asthma Assessment: A systematic approach Dr Naghmeh Radhakrishna Respiratory, Sleep & Allergy Physician Allergy, Asthma & Clinical Immunology Service The Alfred Hospital Melbourne, Australia
Key features and changes to these four components of asthma care include:
 Guidelines for the Diagnosis and Management of Asthma in Adults Clinical Practice Guideline MedStar Health These guidelines are provided to assist physicians and other clinicians in making decisions regarding
Guidelines for the Diagnosis and Management of Asthma in Adults Clinical Practice Guideline MedStar Health These guidelines are provided to assist physicians and other clinicians in making decisions regarding
Bronchial Thermoplasty
 Bronchial Thermoplasty Policy Number: 7.01.127 Last Review: 9/2018 Origination: 11/2010 Next Review: 3/2019 Policy Blue Cross and Blue Shield of Kansas City (Blue KC) will not provide coverage for bronchial
Bronchial Thermoplasty Policy Number: 7.01.127 Last Review: 9/2018 Origination: 11/2010 Next Review: 3/2019 Policy Blue Cross and Blue Shield of Kansas City (Blue KC) will not provide coverage for bronchial
Asthma Management in Pregnancy HEATHER HOWE, MD UNIVERSITY OF UTAH PULMONARY DIVISION
 Asthma Management in Pregnancy HEATHER HOWE, MD UNIVERSITY OF UTAH PULMONARY DIVISION Asthma Management in Pregnancy Effects of asthma on pregnancy outcomes Effects of pregnancy on asthma control Management
Asthma Management in Pregnancy HEATHER HOWE, MD UNIVERSITY OF UTAH PULMONARY DIVISION Asthma Management in Pregnancy Effects of asthma on pregnancy outcomes Effects of pregnancy on asthma control Management
Pediatric Asthma: Pharmacotherapy. Joseph Spahn, MD Children s Hospital Colorado & University of Colorado Medical School Aurora, Colorado
 Pediatric Asthma: Pharmacotherapy Joseph Spahn, MD Children s Hospital Colorado & University of Colorado Medical School Aurora, Colorado Pediatric Asthma: Pharmacotherapy Disclosures/Conflicts of Interest:
Pediatric Asthma: Pharmacotherapy Joseph Spahn, MD Children s Hospital Colorado & University of Colorado Medical School Aurora, Colorado Pediatric Asthma: Pharmacotherapy Disclosures/Conflicts of Interest:
Asthma Management for the Athlete
 Asthma Management for the Athlete Khanh Lai, MD Assistant Professor Division of Pediatric Pulmonary and Sleep Medicine University of Utah School of Medicine 2 nd Annual Sports Medicine Symposium: The Pediatric
Asthma Management for the Athlete Khanh Lai, MD Assistant Professor Division of Pediatric Pulmonary and Sleep Medicine University of Utah School of Medicine 2 nd Annual Sports Medicine Symposium: The Pediatric
Peak Expiratory Flow Rate (PEFR) for ED Management of Acute Asthma Exacerbation
 for ED Management of Acute Asthma Exacerbation") Peak Expiratory Flow Rate (PEFR) for ED Management of Acute Asthma Exacerbation PI: Brian Driver, MD Checklist Reviewed Inclusion and Exclusion Criteria Confirm pertinent exclusion criteria with PMP Engage
Peak Expiratory Flow Rate (PEFR) for ED Management of Acute Asthma Exacerbation PI: Brian Driver, MD Checklist Reviewed Inclusion and Exclusion Criteria Confirm pertinent exclusion criteria with PMP Engage
Dual-Controller Asthma Therapy: Rationale and Clinical Benefits
 B/1 Dual-Controller Asthma Therapy: Rationale and Clinical Benefits MODULE B The 1997 National Heart, Lung, and Blood Institute (NHLBI) Expert Panel guidelines on asthma management recommend a 4-step approach
B/1 Dual-Controller Asthma Therapy: Rationale and Clinical Benefits MODULE B The 1997 National Heart, Lung, and Blood Institute (NHLBI) Expert Panel guidelines on asthma management recommend a 4-step approach
The Asthma Guidelines: Diagnosis and Assessment of Asthma
 The Asthma Guidelines: Diagnosis and Assessment of Asthma Christopher H. Fanta, M.D. Partners Asthma Center Brigham and Women s Hospital Harvard Medical School Objectives Know how the diagnosis of asthma
The Asthma Guidelines: Diagnosis and Assessment of Asthma Christopher H. Fanta, M.D. Partners Asthma Center Brigham and Women s Hospital Harvard Medical School Objectives Know how the diagnosis of asthma
2/12/2015. ASTHMA & COPD The Yin &Yang. Asthma General Information. Asthma General Information
 ASTHMA & COPD The Yin &Yang Arizona State Association of Physician Assistants March 6, 2015 Sedona, Arizona Randy D. Danielsen, PhD, PA-C, DFAAPA Dean & Professor A.T. Still University Asthma General Information
ASTHMA & COPD The Yin &Yang Arizona State Association of Physician Assistants March 6, 2015 Sedona, Arizona Randy D. Danielsen, PhD, PA-C, DFAAPA Dean & Professor A.T. Still University Asthma General Information
Nancy Davis, RRT, AE-C
 Nancy Davis, RRT, AE-C Asthma Statistics 25.6 million Americans diagnosed with asthma 6.8 million are children 10.5 million missed school days per year 14.2 lost work days for adults Approximately 10%
Nancy Davis, RRT, AE-C Asthma Statistics 25.6 million Americans diagnosed with asthma 6.8 million are children 10.5 million missed school days per year 14.2 lost work days for adults Approximately 10%
Asthma in Pregnancy. Asthma. Chronic Airway Inflammation. Objective Measures of Airflow. Peak exp. flow rate (PEFR)
") Chronic Airway Inflammation Asthma in Pregnancy Robin Field, MD Maternal Fetal Medicine Kaiser Permanente San Francisco Asthma Chronic airway inflammation increased airway responsiveness to a variety of
Chronic Airway Inflammation Asthma in Pregnancy Robin Field, MD Maternal Fetal Medicine Kaiser Permanente San Francisco Asthma Chronic airway inflammation increased airway responsiveness to a variety of
Update in Pulmonology Update in Medicine and Primary Care November 11, 2017
 Update in Pulmonology Update in Medicine and Primary Care November 11, 2017 Denitza P. Blagev, MD Pulmonary & Critical Care Medicine Director, Schmidt Chest Clinic Director, Lung Cancer Screening Program
Update in Pulmonology Update in Medicine and Primary Care November 11, 2017 Denitza P. Blagev, MD Pulmonary & Critical Care Medicine Director, Schmidt Chest Clinic Director, Lung Cancer Screening Program
Adult asthma management: focus on control
 Adult asthma management: focus on control Jennifer W. McCallister, MD Associate Professor Pulmonary, Allergy, Critical Care & Sleep Medicine The Ohio State University Wexner Medical Center Objectives Apply
Adult asthma management: focus on control Jennifer W. McCallister, MD Associate Professor Pulmonary, Allergy, Critical Care & Sleep Medicine The Ohio State University Wexner Medical Center Objectives Apply
Diagnosis, Assessment, Monitoring and Pharmacological Treatment of Asthma
 Diagnosis, Assessment, Monitoring and Pharmacological Treatment of Asthma Magnitude of Asthma - India Delhi Childhood asthma: 10.9% Adults: 8% Other Cities 3 to 18% Chhabra SK et al Ann Allergy Asthma
Diagnosis, Assessment, Monitoring and Pharmacological Treatment of Asthma Magnitude of Asthma - India Delhi Childhood asthma: 10.9% Adults: 8% Other Cities 3 to 18% Chhabra SK et al Ann Allergy Asthma
COPD: A Renewed Focus. Disclosures
 COPD: A Renewed Focus Heath Latham, MD Assistant Professor Division of Pulmonary and Critical Care Medicine Disclosures No Business Interests No Consulting No Speakers Bureau No Off Label Use to Discuss
COPD: A Renewed Focus Heath Latham, MD Assistant Professor Division of Pulmonary and Critical Care Medicine Disclosures No Business Interests No Consulting No Speakers Bureau No Off Label Use to Discuss
Pulmonary Function Testing: Concepts and Clinical Applications. Potential Conflict Of Interest. Objectives. Rationale: Why Test?
 Pulmonary Function Testing: Concepts and Clinical Applications David M Systrom, MD Potential Conflict Of Interest Nothing to disclose pertinent to this presentation BRIGHAM AND WOMEN S HOSPITAL Harvard
Pulmonary Function Testing: Concepts and Clinical Applications David M Systrom, MD Potential Conflict Of Interest Nothing to disclose pertinent to this presentation BRIGHAM AND WOMEN S HOSPITAL Harvard
Asthma - Chronic. Presentations of asthma Cough Wheeze Breathlessness Chest tightness
 Asthma - Chronic Definition of asthma Chronic inflammatory disease of the airways 3 components: o Reversible and variable airflow obstruction o Airway hyper-responsiveness to stimuli o Inflammation of
Asthma - Chronic Definition of asthma Chronic inflammatory disease of the airways 3 components: o Reversible and variable airflow obstruction o Airway hyper-responsiveness to stimuli o Inflammation of
7/7/2015. Somboon Chansakulporn, MD. History of variable respiratory symptoms. 1. Documented excessive variability in PFT ( 1 test)
") Definition of Asthma GINA 2010: Chronic inflammatory disorder of the airways Airway hyper-responsiveness Recurrent wheezing, breathlessness, chest tightness, coughing Variable, reversible airflow obstruction
Definition of Asthma GINA 2010: Chronic inflammatory disorder of the airways Airway hyper-responsiveness Recurrent wheezing, breathlessness, chest tightness, coughing Variable, reversible airflow obstruction
Study No.: Title: Rationale: Phase: Study Period: Study Design: Centres: Indication: Treatment: Objectives: Primary Outcome/Efficacy Variable:
 The study listed may include approved and non-approved uses, formulations or treatment regimens. The results reported in any single study may not reflect the overall results obtained on studies of a product.
The study listed may include approved and non-approved uses, formulations or treatment regimens. The results reported in any single study may not reflect the overall results obtained on studies of a product.
Asthma in Day to Day Practice
 Asthma in Day to Day Practice VIJAY.K.VANAM Financial relationships: Disclosures Employed at Mercy Medical Center, Mason City. Nonfinancial relationships: I receive no financial gain from any pharmaceutical
Asthma in Day to Day Practice VIJAY.K.VANAM Financial relationships: Disclosures Employed at Mercy Medical Center, Mason City. Nonfinancial relationships: I receive no financial gain from any pharmaceutical
New Therapies for Asthma
 New Therapies for Asthma Tracy Bridges, MD Speaker Disclosure: Dr. Bridges participates in speaker bureaus for Teva, Genetech & Astra Zeneca. Objectives: Discuss the use of LAMA s for Asthma Detail the
New Therapies for Asthma Tracy Bridges, MD Speaker Disclosure: Dr. Bridges participates in speaker bureaus for Teva, Genetech & Astra Zeneca. Objectives: Discuss the use of LAMA s for Asthma Detail the
RESPIRATORY CARE IN GENERAL PRACTICE
 RESPIRATORY CARE IN GENERAL PRACTICE Definitions of Asthma and COPD Asthma is due to inflammation of the air passages in the lungs and affects the sensitivity of the nerve endings in the airways so they
RESPIRATORY CARE IN GENERAL PRACTICE Definitions of Asthma and COPD Asthma is due to inflammation of the air passages in the lungs and affects the sensitivity of the nerve endings in the airways so they
Outline FEF Reduced FEF25-75 in asthma. What does it mean and what are the clinical implications?
 Reduced FEF25-75 in asthma. What does it mean and what are the clinical implications? Fernando Holguin MD MPH Director, Asthma Clinical & Research Program Center for lungs and Breathing University of Colorado
Reduced FEF25-75 in asthma. What does it mean and what are the clinical implications? Fernando Holguin MD MPH Director, Asthma Clinical & Research Program Center for lungs and Breathing University of Colorado
Controversial Issues in the Management of Childhood Asthma: Insights from NIH Asthma Network Studies
 Controversial Issues in the Management of Childhood Asthma: Insights from NIH Asthma Network Studies Stanley J. Szefler, MD Helen Wohlberg and Herman Lambert Chair in Pharmacokinetics, Head, Pediatric
Controversial Issues in the Management of Childhood Asthma: Insights from NIH Asthma Network Studies Stanley J. Szefler, MD Helen Wohlberg and Herman Lambert Chair in Pharmacokinetics, Head, Pediatric
Primary Care Medicine: Concepts and Controversies Wed., February 17, 2010 Fiesta Americana Puerto Vallarta, Mexico Update on Asthma and COPD
 Primary Care Medicine: Concepts and Controversies Wed., February 17, 2010 Fiesta Americana Puerto Vallarta, Mexico Update on Asthma and COPD Talmadge E. King, Jr., M.D. Krevins Distinguished Professor
Primary Care Medicine: Concepts and Controversies Wed., February 17, 2010 Fiesta Americana Puerto Vallarta, Mexico Update on Asthma and COPD Talmadge E. King, Jr., M.D. Krevins Distinguished Professor
The New Medtech Economic Reality MassMEDIC Annual Meeting
 The New Medtech Economic Reality MassMEDIC Annual Meeting Susan Posner Vice President sposner@healthadvances.com May 1, 2012 The New Medtech Reality The economic downturn coupled with the focus on health
The New Medtech Economic Reality MassMEDIC Annual Meeting Susan Posner Vice President sposner@healthadvances.com May 1, 2012 The New Medtech Reality The economic downturn coupled with the focus on health
Asthma Care in the Emergency Department Clinical Practice Guideline
 Asthma Care in the Emergency Department Clinical Practice Guideline Inclusion: 1) Children 2 years of age or older with a prior history of wheezing, and 2) Children less than 2 years of age with likely
Asthma Care in the Emergency Department Clinical Practice Guideline Inclusion: 1) Children 2 years of age or older with a prior history of wheezing, and 2) Children less than 2 years of age with likely
COPD. Breathing Made Easier
 COPD Breathing Made Easier Catherine E. Cooke, PharmD, BCPS, PAHM Independent Consultant, PosiHleath Clinical Associate Professor, University of Maryland School of Pharmacy This program has been brought
COPD Breathing Made Easier Catherine E. Cooke, PharmD, BCPS, PAHM Independent Consultant, PosiHleath Clinical Associate Professor, University of Maryland School of Pharmacy This program has been brought
Medications for Managing COPD in Hospice Patients. Jim Joyner, PharmD, CGP Director of Clinical Operations Outcome Resources
 Medications for Managing COPD in Hospice Patients Jim Joyner, PharmD, CGP Director of Clinical Operations Outcome Resources Goal of medications in COPD Decrease symptoms and/or complications Reduce frequency
Medications for Managing COPD in Hospice Patients Jim Joyner, PharmD, CGP Director of Clinical Operations Outcome Resources Goal of medications in COPD Decrease symptoms and/or complications Reduce frequency
TARGET POPULATION Eligibility Inclusion Criterion Exclusion Criterion RECOMMENDATIONS
 TARGET POPULATION Eligibility Inclusion Criterion Exclusion Criterion RECOMMENDATIONS Recommendation PULMONARY FUNCTION TESTING (SPIROMETRY) Conditional: The Expert Panel that spirometry measurements FEV1,
TARGET POPULATION Eligibility Inclusion Criterion Exclusion Criterion RECOMMENDATIONS Recommendation PULMONARY FUNCTION TESTING (SPIROMETRY) Conditional: The Expert Panel that spirometry measurements FEV1,
Clinical Policy Title: Bronchial thermoplasty for severe asthma
 Clinical Policy Title: Bronchial thermoplasty for severe asthma Clinical Policy Number: 07.03.01 Effective Date: March 1, 2013 Initial Review Date: October 16, 2013 Most Recent Review Date: October 19,
Clinical Policy Title: Bronchial thermoplasty for severe asthma Clinical Policy Number: 07.03.01 Effective Date: March 1, 2013 Initial Review Date: October 16, 2013 Most Recent Review Date: October 19,
BRONCHIAL THERMOPLASTY
 BRONCHIAL THERMOPLASTY UnitedHealthcare Oxford Clinical Policy Policy Number: RESPIRATORY 009.11 T2 Effective Date: August 1, 2017 Table of Contents Page BRONCHIAL THERMOPLASTY... 1 INSTRUCTIONS FOR USE...
BRONCHIAL THERMOPLASTY UnitedHealthcare Oxford Clinical Policy Policy Number: RESPIRATORY 009.11 T2 Effective Date: August 1, 2017 Table of Contents Page BRONCHIAL THERMOPLASTY... 1 INSTRUCTIONS FOR USE...
Biologic Agents in the treatment of Severe Asthma
 Biologic Agents in the treatment of Severe Asthma Daniel L Maxwell, D.O., FACOI, FAASM Clinical Assistant Professor of Medicine Michigan State University College of Osteopathic Medicine College of Human
Biologic Agents in the treatment of Severe Asthma Daniel L Maxwell, D.O., FACOI, FAASM Clinical Assistant Professor of Medicine Michigan State University College of Osteopathic Medicine College of Human
Improving Outcomes in the Management & Treatment of Asthma. April 21, Spring Managed Care Forum
 Improving Outcomes in the Management & Treatment of Asthma April 21, 2016 2016 Spring Managed Care Forum David M. Mannino, M.D. Professor Department of Preventive Medicine and Environmental Health University
Improving Outcomes in the Management & Treatment of Asthma April 21, 2016 2016 Spring Managed Care Forum David M. Mannino, M.D. Professor Department of Preventive Medicine and Environmental Health University
ADULT ASTHMA GUIDE SUMMARY. This summary provides busy health professionals with key guidance for assessing and treating adult asthma.
 ADULT ASTHMA GUIDE SUMMARY This summary provides busy health professionals with key guidance for assessing and treating adult asthma. Its source document Asthma and Respiratory Foundation NZ Adult Asthma
ADULT ASTHMA GUIDE SUMMARY This summary provides busy health professionals with key guidance for assessing and treating adult asthma. Its source document Asthma and Respiratory Foundation NZ Adult Asthma
Study No.: Title: Rationale: Phase: Study Period: Study Design: Centres: Indication: Treatment: Objectives: Primary Outcome/Efficacy Variable:
 The study listed may include approved and non-approved uses, formulations or treatment regimens. The results reported in any single study may not reflect the overall results obtained on studies of a product.
The study listed may include approved and non-approved uses, formulations or treatment regimens. The results reported in any single study may not reflect the overall results obtained on studies of a product.
Asthma. Definition. Symptoms
 Asthma Definition Asthma is a condition in which your airways narrow and swell and produce extra mucus. This can make breathing difficult and trigger coughing, wheezing and shortness of breath. For some
Asthma Definition Asthma is a condition in which your airways narrow and swell and produce extra mucus. This can make breathing difficult and trigger coughing, wheezing and shortness of breath. For some
Asthma ASTHMA. Current Strategies for Asthma and COPD
 Current Strategies for Asthma and COPD Talmadge E. King, Jr., M.D. Krevins Distinguished Professor of Medicine Chair, Department of Medicine University of California San Francisco (UCSF) San Francisco,
Current Strategies for Asthma and COPD Talmadge E. King, Jr., M.D. Krevins Distinguished Professor of Medicine Chair, Department of Medicine University of California San Francisco (UCSF) San Francisco,
MAYA RAMAGOPAL M.D. DIVISION OF PULMONOLOGY & CYSTIC FIBROSIS CENTER
 MAYA RAMAGOPAL M.D. DIVISION OF PULMONOLOGY & CYSTIC FIBROSIS CENTER 16 year old female with h/o moderate persistent asthma presents to the ED after 6 hours of difficulty breathing, cough, and wheezing
MAYA RAMAGOPAL M.D. DIVISION OF PULMONOLOGY & CYSTIC FIBROSIS CENTER 16 year old female with h/o moderate persistent asthma presents to the ED after 6 hours of difficulty breathing, cough, and wheezing
Asthma and Vocal Cord Dysfunction
 Asthma and Vocal Cord Dysfunction Amy L. Marks DO, FACOP Pediatric Allergy and Immunology Assistant Professor of Pediatrics Oakland University William Beaumont School of Medicine Objectives: Understanding
Asthma and Vocal Cord Dysfunction Amy L. Marks DO, FACOP Pediatric Allergy and Immunology Assistant Professor of Pediatrics Oakland University William Beaumont School of Medicine Objectives: Understanding
Chronic Obstructive Pulmonary Disease Guidelines and updates
 Chronic Obstructive Pulmonary Disease Guidelines and updates October 20, 2018 Saratoga Springs, NY COPD (Chronic obstructive pulmonary disease) is a major cause of mortality and morbidity in the United
Chronic Obstructive Pulmonary Disease Guidelines and updates October 20, 2018 Saratoga Springs, NY COPD (Chronic obstructive pulmonary disease) is a major cause of mortality and morbidity in the United
Predicting, Preventing and Managing Asthma Exacerbations. Heather Zar Department of Paediatrics & Child Health University of Cape Town South Africa
 Predicting, Preventing and Managing Asthma Exacerbations Heather Zar Department of Paediatrics & Child Health University of Cape Town South Africa Asthma exacerbations Predicting exacerbation recognising
Predicting, Preventing and Managing Asthma Exacerbations Heather Zar Department of Paediatrics & Child Health University of Cape Town South Africa Asthma exacerbations Predicting exacerbation recognising
Differential diagnosis
 Differential diagnosis The onset of COPD is insidious. Pathological changes may begin years before symptoms appear. The major differential diagnosis is asthma, and in some cases, a clear distinction between
Differential diagnosis The onset of COPD is insidious. Pathological changes may begin years before symptoms appear. The major differential diagnosis is asthma, and in some cases, a clear distinction between
Expert Panel Report 3: Guidelines for the Diagnosis and Management of Asthma Full Report 2007
 Expert Panel Report 3: Guidelines for the Diagnosis and Management of Asthma Full Report 2007 TARGET POPULATION Eligibility Inclusion Criterion Exclusion Criterion RECOMMENDATIONS Selecting Initial Therapy
Expert Panel Report 3: Guidelines for the Diagnosis and Management of Asthma Full Report 2007 TARGET POPULATION Eligibility Inclusion Criterion Exclusion Criterion RECOMMENDATIONS Selecting Initial Therapy
Pulmonary Pearls. Medical Pearls. Case 1: Case 1 (cont.): Case 1: What is the Most Likely Diagnosis? Case 1 (cont.):
: Case 1: What is the Most Likely Diagnosis? Case 1 (cont.):") Pulmonary Pearls Christopher H. Fanta, MD Pulmonary and Critical Care Division Brigham and Women s Hospital Partners Asthma Center Harvard Medical School Medical Pearls Definition: Medical fact that is
Pulmonary Pearls Christopher H. Fanta, MD Pulmonary and Critical Care Division Brigham and Women s Hospital Partners Asthma Center Harvard Medical School Medical Pearls Definition: Medical fact that is
MANAGING ASTHMA. Nancy Davis, RRT, AE-C
 MANAGING ASTHMA Nancy Davis, RRT, AE-C What is asthma? Asthma is a chronic respiratory disease characterized by episodes or attacks of inflammation and narrowing of small airways in response to asthma
MANAGING ASTHMA Nancy Davis, RRT, AE-C What is asthma? Asthma is a chronic respiratory disease characterized by episodes or attacks of inflammation and narrowing of small airways in response to asthma
Pediatric and Adult. Disclosure. Asthma. Learning Objectives. EPR-3: What s Changed? Asthma: Pediatric and Adult
 Asthma: Pediatric and Adult Americo D. Fraboni, MD, FAAFP Assistant Clinical Professor Department of Family Practice & Community Health University of Minnesota Medical School Minneapolis, Minnesota Disclosure
Asthma: Pediatric and Adult Americo D. Fraboni, MD, FAAFP Assistant Clinical Professor Department of Family Practice & Community Health University of Minnesota Medical School Minneapolis, Minnesota Disclosure
Lecture Notes. Chapter 3: Asthma
 Lecture Notes Chapter 3: Asthma Objectives Define asthma and status asthmaticus List the potential causes of asthma attacks Describe the effect of asthma attacks on lung function List the clinical features
Lecture Notes Chapter 3: Asthma Objectives Define asthma and status asthmaticus List the potential causes of asthma attacks Describe the effect of asthma attacks on lung function List the clinical features
Asthma. UVM. University of Vermont. Alicia Jacobs MD Fletcher Allen Health Care and the University of Vermont
 University of Vermont ScholarWorks @ UVM Family Medicine Scholarly Works 6-14-2013 Asthma Alicia Jacobs MD Fletcher Allen Health Care and the University of Vermont Follow this and additional works at:
University of Vermont ScholarWorks @ UVM Family Medicine Scholarly Works 6-14-2013 Asthma Alicia Jacobs MD Fletcher Allen Health Care and the University of Vermont Follow this and additional works at:
Learning Objective. Asthma. Discuss the pathophysiology, clinical presentation, diagnosis, and treatment of Asthma 2/22/2017
 Marianne Curran, PA C 3/1/17 Learning Objective Discuss the pathophysiology, clinical presentation, diagnosis, and treatment of Definition many variations Chronic Disorder with Reversible (Intermittent
Marianne Curran, PA C 3/1/17 Learning Objective Discuss the pathophysiology, clinical presentation, diagnosis, and treatment of Definition many variations Chronic Disorder with Reversible (Intermittent
Asthma and Its Many Unmet Needs: Directions for Novel Therapeutic Approaches
 Asthma and Its Many Unmet Needs: Directions for Novel Therapeutic Approaches William W. Busse,, M.D. University of Wisconsin School of Medicine and Public Health Madison, WI, USA Disclosure Slide Employment
Asthma and Its Many Unmet Needs: Directions for Novel Therapeutic Approaches William W. Busse,, M.D. University of Wisconsin School of Medicine and Public Health Madison, WI, USA Disclosure Slide Employment
II: Moderate Worsening airflow limitations Dyspnea on exertion, cough, and sputum production; patient usually seeks medical
 Table 3.1. Classification of COPD Severity Stage Pulmonary Function Test Findings Symptoms I: Mild Mild airflow limitations +/ Chronic cough and sputum production; patient unaware of abnormal FEV 1 80%
Table 3.1. Classification of COPD Severity Stage Pulmonary Function Test Findings Symptoms I: Mild Mild airflow limitations +/ Chronic cough and sputum production; patient unaware of abnormal FEV 1 80%
Clinical Policy: Omalizumab (Xolair) Reference Number: ERX.SPA.141 Effective Date:
 Reference Number: ERX.SPA.141 Effective Date:") Clinical Policy: (Xolair) Reference Number: ERX.SPA.141 Effective Date: 03.01.14 Last Review Date: 02.18 Revision Log See Important Reminder at the end of this policy for important regulatory and legal
Clinical Policy: (Xolair) Reference Number: ERX.SPA.141 Effective Date: 03.01.14 Last Review Date: 02.18 Revision Log See Important Reminder at the end of this policy for important regulatory and legal
Inhaler Confusion. Today s Speaker Dr. Randall Brown. Director of Asthma Programs 6/7/2016. Dr. Randall Brown March 31, 2016
 + Inhaler Confusion Dr. Randall Brown March 31, 2016 + Today s Speaker Dr. Randall Brown Director of Asthma Programs Center for Managing Chronic Disease University of Michigan 1 ASTHMA ESSENTIALS IN PRIMARY
+ Inhaler Confusion Dr. Randall Brown March 31, 2016 + Today s Speaker Dr. Randall Brown Director of Asthma Programs Center for Managing Chronic Disease University of Michigan 1 ASTHMA ESSENTIALS IN PRIMARY
Treatment Options for Complicated/Severe Asthma. Henry J. Kanarek, MD Kanarek Allergy Asthma Immunology
 Treatment Options for Complicated/Severe Asthma Henry J. Kanarek, MD Kanarek Allergy Asthma Immunology www.kallergy.com 913-451-8555 Asthma Epidemiology World Health Organization, Asthma is one of the
Treatment Options for Complicated/Severe Asthma Henry J. Kanarek, MD Kanarek Allergy Asthma Immunology www.kallergy.com 913-451-8555 Asthma Epidemiology World Health Organization, Asthma is one of the
VA/DoD Clinical Practice Guideline Management of COPD Pocket Guide
 VA/DoD Clinical Practice Guideline Management of COPD Pocket Guide MODULE A: MAAGEMET OF COPD 1 2 Patient with suspected or confirmed COPD presents to primary care [ A ] See sidebar A Perform brief clinical
VA/DoD Clinical Practice Guideline Management of COPD Pocket Guide MODULE A: MAAGEMET OF COPD 1 2 Patient with suspected or confirmed COPD presents to primary care [ A ] See sidebar A Perform brief clinical
Asthma Pathophysiology and Treatment. John R. Holcomb, M.D.
 Asthma Pathophysiology and Treatment John R. Holcomb, M.D. Objectives Definition of Asthma Epidemiology and risk factors of Asthma Pathophysiology of Asthma Diagnostics test of Asthma Management of Asthma
Asthma Pathophysiology and Treatment John R. Holcomb, M.D. Objectives Definition of Asthma Epidemiology and risk factors of Asthma Pathophysiology of Asthma Diagnostics test of Asthma Management of Asthma
BRONCHIAL THERMOPLASTY
 BRONCHIAL THERMOPLASTY UnitedHealthcare of California (HMO) UnitedHealthcare Benefits Plan of California (IEX EPO, IEX PPO) UnitedHealthcare of Oklahoma, Inc. UnitedHealthcare of Oregon, Inc. UnitedHealthcare
BRONCHIAL THERMOPLASTY UnitedHealthcare of California (HMO) UnitedHealthcare Benefits Plan of California (IEX EPO, IEX PPO) UnitedHealthcare of Oklahoma, Inc. UnitedHealthcare of Oregon, Inc. UnitedHealthcare
ASTHMA IN THE PEDIATRIC POPULATION
 ASTHMA IN THE PEDIATRIC POPULATION SEARCH Rotation 2 August 23, 2010 Objectives Define asthma as a chronic disease Discuss the morbidity of asthma in pediatrics Discuss a few things that a health center
ASTHMA IN THE PEDIATRIC POPULATION SEARCH Rotation 2 August 23, 2010 Objectives Define asthma as a chronic disease Discuss the morbidity of asthma in pediatrics Discuss a few things that a health center
BRONCHIAL THERMOPLASTY AND OTHER ADVANCES IN NON- PHARMACOLOGICAL MANAGEMENT OF ASTHMA AND COPD. -Shailesh Agrawal
 BRONCHIAL THERMOPLASTY AND OTHER ADVANCES IN NON- PHARMACOLOGICAL MANAGEMENT OF ASTHMA AND COPD -Shailesh Agrawal Outline Introduction Patient selection Preparation for procedure Equipment and Technique
BRONCHIAL THERMOPLASTY AND OTHER ADVANCES IN NON- PHARMACOLOGICAL MANAGEMENT OF ASTHMA AND COPD -Shailesh Agrawal Outline Introduction Patient selection Preparation for procedure Equipment and Technique
Air Flow Limitation. In most serious respiratory disease, a key feature causing morbidity and functional disruption is air flow imitation.
 Asthma Air Flow Limitation In most serious respiratory disease, a key feature causing morbidity and functional disruption is air flow imitation. True whether reversible, asthma and exercise-induced bronchospasm,
Asthma Air Flow Limitation In most serious respiratory disease, a key feature causing morbidity and functional disruption is air flow imitation. True whether reversible, asthma and exercise-induced bronchospasm,
Asthma Upate 2018: What s New Since the 2007 Asthma Guidelines of NAEPP?
 10:50-11:50am Asthma Update 2018: What s New Since the 2007 National Asthma Guidelines? SPEAKER Christopher H. Fanta, MD Disclosures The following relationships exist related to this presentation: Christopher
10:50-11:50am Asthma Update 2018: What s New Since the 2007 National Asthma Guidelines? SPEAKER Christopher H. Fanta, MD Disclosures The following relationships exist related to this presentation: Christopher
SYNOPSIS A two-stage randomized, open-label, parallel group, phase III, multicenter, 7-month study to assess the efficacy and safety of SYMBICORT
 Drug product: Drug substance(s): Edition No.: Study code: SYMBICORT pmdi 160/4.5 g Budesonide/formoterol D5896C00005 Date: 8 May 2006 SYNOPSIS A two-stage randomized, open-label, parallel group, phase
Drug product: Drug substance(s): Edition No.: Study code: SYMBICORT pmdi 160/4.5 g Budesonide/formoterol D5896C00005 Date: 8 May 2006 SYNOPSIS A two-stage randomized, open-label, parallel group, phase
Update on Pulmonary Diseases. Jeffrey Lessar, MD
 Update on Pulmonary Diseases Jeffrey Lessar, MD 1 No disclosures to make No conflicts 2 Goals Update on key changes in Pulmonary Therapy 3 Spirometry Spirometry FEV1- forced expiratory Volume in 1 Sec
Update on Pulmonary Diseases Jeffrey Lessar, MD 1 No disclosures to make No conflicts 2 Goals Update on key changes in Pulmonary Therapy 3 Spirometry Spirometry FEV1- forced expiratory Volume in 1 Sec
Diagnosis, Treatment and Management of Asthma
 Diagnosis, Treatment and Management of Asthma Asthma is a complex disorder characterized by variable and recurring symptoms, airflow obstruction, bronchial hyperresponsiveness, and an underlying inflammation.
Diagnosis, Treatment and Management of Asthma Asthma is a complex disorder characterized by variable and recurring symptoms, airflow obstruction, bronchial hyperresponsiveness, and an underlying inflammation.
Medical Policy An independent licensee of the Blue Cross Blue Shield Association
 Xolair (omalizumab) Page 1 of 15 Medical Policy An independent licensee of the Blue Cross Blue Shield Association Title: Xolair (omalizumab) Prime Therapeutics will review Prior Authorization requests.
Xolair (omalizumab) Page 1 of 15 Medical Policy An independent licensee of the Blue Cross Blue Shield Association Title: Xolair (omalizumab) Prime Therapeutics will review Prior Authorization requests.
Omalizumab (Xolair ) ( Genentech, Inc., Novartis Pharmaceuticals Corp.) September Indication
 ( Genentech, Inc., Novartis Pharmaceuticals Corp.) September Indication") ( Genentech, Inc., Novartis Pharmaceuticals Corp.) September 2003 Indication The FDA recently approved Omalizumab on June 20, 2003 for adults and adolescents (12 years of age and above) with moderate to
( Genentech, Inc., Novartis Pharmaceuticals Corp.) September 2003 Indication The FDA recently approved Omalizumab on June 20, 2003 for adults and adolescents (12 years of age and above) with moderate to