Respiratory infection what works Professor Terence Stephenson President Royal College of Paediatrics & Child Health
|
|
|
- Jonas Rice
- 5 years ago
- Views:
Transcription

1 Respiratory infection what works Professor Terence Stephenson President Royal College of Paediatrics & Child Health Nuffield Professor, Institute of Child Health, University College London & Great Ormond Street Hospital, London
2 Community Acquired in Previously Well Children: Pneumonia Bronchiolitis (RSV) Swine Flu (H1N1 Influenza)



3 Local microbiology
4 Right middle lobe pneumonia 36/1000/year < 5 years 16/1000/year children 5-14 years
5 Definition of pneumonia respiratory symptoms / signs absence of wheeze abnormal chest x-ray

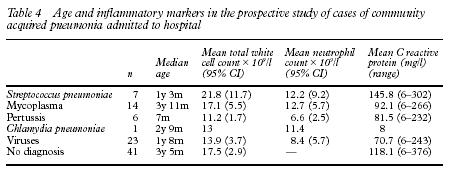
6 89 children recruited 51 positive aetiological diagnoses in 48 children S.pneumoniae 7 M.pneumoniae 14 B.pertussis 6 C.pneumoniae 1 Viruses 23
7
8
9 iv antibiotic use before and after introduction of a written guideline Benzylpenicillin (%) (%) Erythromycin 2 7 Cefotaxime Ampicillin 21 3 Flucloxacillin 7 2 Metronidazole 0 2


10 ATKINSON M, LAKHANPAUL M, SMYTH A, VYAS H, WESTON V, STIHOLE J, OWEN V, HALLIDAY K, SAMMONS H, CRANE J, GUNTUPALLI N, WALTON L, NINAN T, MORJARIA A, STEPHENSON T. A multicentre randomised controlled equivalence trial comparing oral amoxicillin and intravenous benzyl penicillin for community acquired pneumonia in children: PIVOT Trial. Thorax 62, , 2007
11 DEFINITION OF PNEUMONIA - ENTRY CRITERIA All 3 must be present: Respiratory symptoms or signs but no wheeze Documented fever of 37.5 deg C or a history of fever at home CXR reviewed by 2 masked radiologists independently confirms radiological pneumonia Excluded: children younger than 6 months; SaO2 < 85%; shocked despite 20 ml/kg fluid; chronic lung disease; immunodeficiency; penicillin allergy NOT excluded: asthma; already receiving antibiotics
12 Treatment - all ages randomised to either: Oral amoxycillin versus IV benzyl penicillin [8 mg/kg 8 hrly versus 25 mg/kg 6 hrly] Rescue Treatment Oral erythromycin or IV clarithromycin At 48 hours if no improvement or before if deemed appropriate by the clinician in charge
13 HOW ILL WERE THE CASES? Admission observations: - (mean and 95% CI) Temperature Pulse Respiratory rate < 1 year > 1 year SaO2 (in air) Neutrophil count x10 9 /l C-reactive protein mg/l 38.6 deg ( ) 151 ( ) 50 (45-61) 40 (37-43) 95% (94-96) 14 ( ) 159 ( ) 38.4 deg ( ) 149 ( ) 50 (45-61) 43 (40-46) 95% (95-96) 13.4 ( ) 172 ( )
14 Probability that the child meets the primary outcome measure after time t Time for temperature to settle in the oral and IV groups (PP) =IV treatment = oral treatment.6.4 Wellek log rank test for equivalence P= Time for temperature to be less than 38 0 C for 24 continuous hours (days)
15 Number of children Number of children Time to resolution of symptoms IV group PP Time to resolution of symptoms oral group PP Time to resolution of symptoms in days Time to resolution of symptoms in days Median of 9 days to full recovery in both arms of the study
16 REPEAT CHEST X-RAY? Gibson NA. Hollman AS. Paton JY. Value of radiological follow up of childhood pneumonia. BMJ. 307(6912):1117, 1993 Oct 30
17 Pleural effusion If a child remains pyrexial or unwell 48 hours after admission for pneumonia, effusion/empyema must be excluded. If a child has significant pleural infection, a drain should be inserted at the outset and repeated taps are not recommended. Ultrasound should be used to guide thoracocentesis or drain placement. Since there is no evidence that large bore chest drains confer any advantage, small drains (including pigtail catheters) should be used Intrapleural fibrinolytics for thick fluid with loculations or empyema (overt pus). Urokinase has been studied in an RCT in children: recommended twice daily for 3 days (6 doses in total) using units in 40 ml 0.9% saline for children weighing 10 kg or above, and units in 10 ml 0.9% saline for children weighing under 10 kg.
18 CONCLUSION Oral and IV treatment are equivalent for Community Acquired Pneumonia Oral group spent significantly less time in hospital and required less oxygen Complications are not increased in the oral group Time to resolution of symptoms is the same in both groups Yield from blood culture is low and did not predict complications (previous studies have not shown CRP and FBC are reliably predictive of bacterial or viral pneumonia) Treatment with oral antibiotics is cheaper
19
 Post-CXR: ED doctor diagnosed 40 pneumonias which were not confirmed. This interpretation resulted in a fivefold increase in the rate of antibiotic therapy after radiography, from 2.")
20 Omitting radiography in diagnosis of acute bronchiolitis 265 infants, 2 23 months old, presenting to Toronto Sick Childrens Hospital Emergency Department with typical clinical bronchiolitis (wheeze + crepitations) Post-CXR: ED doctor diagnosed 40 pneumonias which were not confirmed. This interpretation resulted in a fivefold increase in the rate of antibiotic therapy after radiography, from 2.6% to 14.7%. J Yong. Pediatric Pulmonology Volume 44, Issue 2, pages , February 2009
21 Steroids for bronchiolitis systemic & inhaled 17 trials (2596 participants): only two had low overall risk of bias. Highest dose = 6 doses of oral dexamethasone (1 mg/kg followed by 0.6 mg/kg for five days) Outpatients: No significant reduction in outpatient admissions by days 1 and 7 when compared to placebo (pooled risk ratios (RRs) 0.92; 95% CI 0.78 to 1.08; and 0.86; 95% CI 0.7 to 1.06, respectively). Inpatients: There was no benefit in Length of Stay for inpatients (mean difference days; 95% CI to 0.04).
22 Bronchodilators 28 trials (1912 infants) with bronchiolitis. In 10 inpatient and 10 outpatient studies, oxygen saturation did not improve with bronchodilators (mean difference (MD) -0.45, 95% confidence interval (CI) to 0.05, n = 1182). Outpatient bronchodilator treatment did not reduce the rate of hospitalization (12% in bronchodilator group versus 16% in placebo, odds ratio (OR) 0.78, 95% CI 0.47 to 1.29, n = 650). Inpatient bronchodilator treatment did not reduce the duration of hospitalization (MD 0.06, 95% CI to 0.39, n = 349).
23 Epinephrine Epinephrine versus Placebo Five inpatient studies: Only one out of ten inpatient outcomes demonstrated a significant difference between treatment groups: change in clinical score at 60 minutes showed a SMD of favouring epinephrine (95% CI -1.00,-0.03).
24 Epinephrine Epinephrine versus Salbutamol Four inpatient studies: Only one of the seven outcomes evaluated was statistically significant: respiratory rate at 30 minutes favoured epinephrine over salbutamol (WMD -5.12; 95% CI -6.83,- 3.41). Changes in clinical score, oxygen saturation, heart rate, and length of stay were not significantly different between the treatment groups.
25 Heliox four trials involving 84 infants under two years of age with respiratory distress secondary to bronchiolitis caused by respiratory syncytial virus (RSV) and requiring PICU when compared to those treated with air or oxygen, there was no clinically significant reduction in the rate of intubation (risk ratio (RR) 1.38, 95% CI 0.41 to 4.56, P = 0.60, n = 58), in the need for mechanical ventilation (RR 1.11, 95% CI 0.36 to 3.38, P = 0.86, n = 58), or in the length of stay in a PICU (MD = days, 95% CI to 0.61, P = 0.69, n = 58).
26 Physiotherapy Based on the results of three RCTs in infants with acute bronchiolitis, chest physiotherapy using vibration and percussion techniques does not: reduce length of hospital stay oxygen requirements or improve the severity clinical score. These were infants who were not on mechanical ventilation and who did not have any other comorbidity.
27 3% nebulised saline Four trials involving 254 infants with acute viral bronchiolitis (189 inpatients and 65 outpatients) Patients treated with nebulized 3% saline had a significantly shorter mean length of hospital stay compared to those treated with nebulized 0.9% saline (mean difference (MD) days, 95% CI to -0.40, P = ) Length of Stay reduced from 3.5 to 2.5 days
28

29
30
 children who died were previously healthy. 45 (64%) had severe pre-existing disorders especially chronic neurological disease (1536 per million population).")
31 70 paediatric deaths related to H1N1 were reported. Childhood mortality rate was 6 per million population. The rate was highest for children aged less than 1 year. 15 (21%) children who died were previously healthy. 45 (64%) had severe pre-existing disorders especially chronic neurological disease (1536 per million population). Overall, 45 (64%) children had received oseltamivir (seven within 48 h of symptom onset).

32 Catch it, bin it, kill it

33
34 Treatment Fluids Paracetamol Ibuprofen No Aspirin

35 Antivirals and Vaccines
36 Evidence that Neuraminidase blockers treat children? 2 randomised trials of Tamiflu and 2 of Relenza 1766 children aged less than 12 years Illness shortened by 36 hours on average Otitis media reduced from 30% to 15% in children 1-5 years old No reduction in asthma episodes in children with asthma
37 Side-effects of Tamiflu in large Randomised Controlled Trials In untreated Winter flu, 1 in 20 children vomit In Winter flu treated with Tamiflu, 1 in 10 children vomit

38 Antibiotics?
39
40

41 Evidence that winter flu vaccine protects children? 51 trials of winter flu vaccine in children 294,159 children Inactivated vaccines 59% efficacy in children over 2 years but no better than placebo under 2 years Live vaccines 82% efficacy in children over 2 years
42 PRIORITY GROUPS FOR H1N1 VACCINE 1. Individuals aged six months to 65 years with underlying health problems and the immuno-supressed including chemotherapy patients 2. Pregnant women 3. Household contacts of people with compromised immune systems 4. Individuals aged over 65 with health problems
43
44 Straus W et al Co-trimoxazole versus amoxycillin for pneumonia in children in Pakistan an RCT Lancet 1998; 352: Oral amoxil 45 mg/kg/day successful in 82% of children with severe pneumonia severe pneumonia defined as lower chest indrawing with or without tachypnoea Wheeze was not an exclusion All 600 children had CXR but only 150/600 had radiological confirmation of pneumonia
45 MASCOT pneumonia study group 3 days versus 5 days amoxycillin for pneumonia in children in Pakistan an RCT Lancet 2002; 360: Oral amoxil 45 mg/kg/day successful in 80% of children with pneumonia, irrespective of 3 or 5 days Rx Only non-severe pneumonia by WHO criteria Wheeze was not an exclusion only 14% had radiological confirmation of pneumonia
46 ISCAP pneumonia study group 3 days versus 5 days amoxycillin for pneumonia in children in India an RCT BMJ 2004; 360: Oral amoxil mg/kg/day successful in 90% of children with pneumonia, irrespective of 3 or 5 days Rx Only non-severe pneumonia by WHO criteria Wheeze was not an exclusion (24% had RSV) No CXR performed
47 Addo-Yobo E et al Oral amoxycillin versus injectable penicillin for severe pneumonia in children in Africa, Asia and S. America an RCT Lancet 1998; 352: Oral amoxil 45 mg/kg/day versus parenteral penicillin 200,000 iu/kg/day [120 mg/kg/day] successful in 82% of children with severe pneumonia severe pneumonia defined as lower chest indrawing with or without tachypnoea Wheeze at presentation was an exclusion but 46% heard to wheeze subsequently CXR not required
48 3% nebulised saline + salbutamol Luo Z. Liu E. Luo J. Li S. Zeng F. Yang X. Fu Z. Pediatrics International. 52(2): , 2010 Apr randomized controlled trial, 93 infants with mild to moderate bronchiolitis the infants received inhalation of 2.5 mg (0.5 ml) salbutamol dissolved in either 4.0 ml normal (0.9%) saline (control group, n= 43) or 4.0 ml hypertonic (3%) saline (treatment group, n= 50). The therapy was repeated three times daily until discharge. Wheezing remission time was or days in the control group and or days in the treatment group (P < 0.01). Cough remission time was or days in the control group and or days in the treatment group (P < 0.01). Length of hospital stay decreased from or days in the control group to or days in the treatment group (P < 0.01). CONCLUSIONS: Inhalation of nebulized 3% hypertonic saline solution and salbutamol is a safe and effective therapy for patients with mild to moderate bronchiolitis.
49 GSK H1N1 Vaccine (Pandremix) yrs one dose Including pregnant women 6 months -18 years two doses Winter: UK government did NOT recommend seasonal flu vaccine (H1N1 and Flu B) for healthy children
50 Neonates Vaccination in pregnancy protects Breast feeding OK with Anti-Virals for mother
51 246 Randomised to oral treatment 126 Received study treatment 121 Did not receive study treatment 5 Randomised to IV treatment 120 Received study treatment 116 Did not receive study treatment 4 Did not meet radiological criteria (21) Eligible for per protocol analysis 100 Did not meet radiological criteria (13) Eligible for per protocol analysis 103 Unable to contact for telephone FU (3) Unable to contact for telephone FU (2)
52 Cumulative weekly number of reports of Invasive Pneumococcal Disease due to any of the serotypes in Prevenar7 : Persons aged over 5 Years in England and Wales
53 Cumulative weekly number of reports of Invasive Pneumococcal Disease due to any of the serotypes not in Prevenar7 : Persons aged over 5 Years in England and Wales
54
55
The McMaster at night Pediatric Curriculum
 The McMaster at night Pediatric Curriculum Community Acquired Pneumonia Based on CPS Practice Point Pneumonia in healthy Canadian children and youth and the British Thoracic Society Guidelines on CAP Objectives
The McMaster at night Pediatric Curriculum Community Acquired Pneumonia Based on CPS Practice Point Pneumonia in healthy Canadian children and youth and the British Thoracic Society Guidelines on CAP Objectives
NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE SCOPE
 NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE 1 Guideline title SCOPE Bronchiolitis: diagnosis and management of bronchiolitis in children. 1.1 Short title Bronchiolitis in children 2 The remit The
NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE 1 Guideline title SCOPE Bronchiolitis: diagnosis and management of bronchiolitis in children. 1.1 Short title Bronchiolitis in children 2 The remit The
Setting The setting was outpatient departments of referral hospitals. The economic analysis was conducted in India.
 Three day versus five day treatment with amoxicillin for non-severe pneumonia in young children: a multicentre randomised controlled trial ISCAP study group Record Status This is a critical abstract of
Three day versus five day treatment with amoxicillin for non-severe pneumonia in young children: a multicentre randomised controlled trial ISCAP study group Record Status This is a critical abstract of
NOVEL INFLUENZA A (H1N1) Swine Flu
 Swine Flu") Introduction Definitions Influenza-like Illness Emergency Department Assessment Anitiviral Medication Oseltamivir (Tamiflu) Dosing Infection Control Issues Staff Exposure References Introduction This guideline
Introduction Definitions Influenza-like Illness Emergency Department Assessment Anitiviral Medication Oseltamivir (Tamiflu) Dosing Infection Control Issues Staff Exposure References Introduction This guideline
Guideline for the Management of Acute Chest Syndrome in Children with Sickle Cell Disease
 Guideline for the Management of Acute Chest Syndrome in Children with Sickle Cell Disease Definition Acute chest syndrome (ACS) is defined as an acute illness characterized by fever and/or respiratory
Guideline for the Management of Acute Chest Syndrome in Children with Sickle Cell Disease Definition Acute chest syndrome (ACS) is defined as an acute illness characterized by fever and/or respiratory
Quick Literature Searches
 Quick Literature Searches National Pediatric Nighttime Curriculum Written by Leticia Shanley, MD, FAAP Institution: University of Texas Southwestern Medical Center Case 1 It s 1:00am and you have just
Quick Literature Searches National Pediatric Nighttime Curriculum Written by Leticia Shanley, MD, FAAP Institution: University of Texas Southwestern Medical Center Case 1 It s 1:00am and you have just
British Thoracic Society Paediatric Pneumonia Audit National Audit Period: 1 November January 2017 Dr Julian Legg and Dr Charlotte Rampton
 British Thoracic Society Paediatric Pneumonia Audit National Audit Period: 1 November 2016 31 January 2017 Dr Julian Legg and Dr Charlotte Rampton Number of records submitted: 7302 Number of participants:
British Thoracic Society Paediatric Pneumonia Audit National Audit Period: 1 November 2016 31 January 2017 Dr Julian Legg and Dr Charlotte Rampton Number of records submitted: 7302 Number of participants:
BRONCHIOLITIS. See also the PSNZ guideline - Wheeze & Chest Infections in infants under 1 year (www.paediatrics.org.nz)
") Definition What is Bronchiolitis? Assessment Management Flow Chart Admission Guidelines Investigations Management Use of Bronchodilators Other treatments Discharge Planning Bronchiolitis & Asthma References
Definition What is Bronchiolitis? Assessment Management Flow Chart Admission Guidelines Investigations Management Use of Bronchodilators Other treatments Discharge Planning Bronchiolitis & Asthma References
Supplementary appendix
 Supplementary appendix This appendix formed part of the original submission and has been peer reviewed. We post it as supplied by the authors. Supplement to: Blum CA, Nigro N, Briel M, et al. Adjunct prednisone
Supplementary appendix This appendix formed part of the original submission and has been peer reviewed. We post it as supplied by the authors. Supplement to: Blum CA, Nigro N, Briel M, et al. Adjunct prednisone
Guideline for management of children & adolescents with pleural empyema
 CHILD AND ADOLESCENT HEALTH SERVICE PRINCESS MARGARET HOSPITAL FOR CHILDREN Guideline for management of children & adolescents with pleural empyema This guideline provides an evidence-based framework for
CHILD AND ADOLESCENT HEALTH SERVICE PRINCESS MARGARET HOSPITAL FOR CHILDREN Guideline for management of children & adolescents with pleural empyema This guideline provides an evidence-based framework for
Dr. Rai Muhammad Asghar Associate Professor of Pediatrics Benazir Bhutto Hospital Rawalpindi
 Dr. Rai Muhammad Asghar Associate Professor of Pediatrics Benazir Bhutto Hospital Rawalpindi MANAGEMENT OF THE CHILD WITH COUGH OR DIFFICULT BREATHING Global Burden * Commonest cause of death * 2 million
Dr. Rai Muhammad Asghar Associate Professor of Pediatrics Benazir Bhutto Hospital Rawalpindi MANAGEMENT OF THE CHILD WITH COUGH OR DIFFICULT BREATHING Global Burden * Commonest cause of death * 2 million
Department of Pediatrics RGH Rawalpindi Medical College
 Department of Pediatrics RGH Rawalpindi Medical College COUGH OR DIFFICULT BREATING Dr. Rai Muhammad Asghar Associate Professor of Pediatrics department RGH Rawalpindi MANAGEMENT OF THE CHILD WITH COUGH
Department of Pediatrics RGH Rawalpindi Medical College COUGH OR DIFFICULT BREATING Dr. Rai Muhammad Asghar Associate Professor of Pediatrics department RGH Rawalpindi MANAGEMENT OF THE CHILD WITH COUGH
Safety, feasibility and efficacy of outpatient management of moderate pneumonia at Port Moresby General Hospital: a prospective study
 Safety, feasibility and efficacy of outpatient management of moderate pneumonia at Port Moresby General Hospital: a prospective study Dr Rose Morre Master of Medicine research project, 2017 Aim To trial
Safety, feasibility and efficacy of outpatient management of moderate pneumonia at Port Moresby General Hospital: a prospective study Dr Rose Morre Master of Medicine research project, 2017 Aim To trial
Supplementary Appendix
 Supplementary Appendix This appendix has been provided by the authors to give readers additional information about their work. Supplement to: Jain S, Kamimoto L, Bramley AM, et al. Hospitalized patients
Supplementary Appendix This appendix has been provided by the authors to give readers additional information about their work. Supplement to: Jain S, Kamimoto L, Bramley AM, et al. Hospitalized patients
The Management of Acute Chest Syndrome in Children with Sickle Cell Disease
 The Management of Acute Chest Syndrome in Children with Sickle Cell Disease Document Information Version: 4 Date: Dec 2013 Authors (incl. job title): Professor David Rees and Dr Sue Height, consultant
The Management of Acute Chest Syndrome in Children with Sickle Cell Disease Document Information Version: 4 Date: Dec 2013 Authors (incl. job title): Professor David Rees and Dr Sue Height, consultant
Management of URTI s in Children
 Management of URTI s in Children Robin J Green PhD Antibiotics - Dilemmas for General Practitioners Antibiotic overuse = Resistance Delay in antibiotic use = Mortality Patient expectation Employer expectation
Management of URTI s in Children Robin J Green PhD Antibiotics - Dilemmas for General Practitioners Antibiotic overuse = Resistance Delay in antibiotic use = Mortality Patient expectation Employer expectation
Swine Influenza Update #3. Triage, Assessment, and Care of Patients Presenting with Respiratory Symptoms
 Updated 12:00 p.m. April 30, 2009 Swine Influenza Update #3 Introduction: This document revises our last update which was sent April 28 th, 2009. The most important revisions include the following: 1.
Updated 12:00 p.m. April 30, 2009 Swine Influenza Update #3 Introduction: This document revises our last update which was sent April 28 th, 2009. The most important revisions include the following: 1.
INFLUENZA. Rob Young (James. J. Reid) Faculty of Medicine University of Auckland (Otago)
 Faculty of Medicine University of Auckland (Otago)") INFLUENZA Rob Young (James. J. Reid) Faculty of Medicine University of Auckland (Otago) INFLUENZA Don t confuse with the common cold Symptoms may be similar BUT those with influenza are sick those with
INFLUENZA Rob Young (James. J. Reid) Faculty of Medicine University of Auckland (Otago) INFLUENZA Don t confuse with the common cold Symptoms may be similar BUT those with influenza are sick those with
TREAMENT OF RECURRENT VIRUS-INDUCED WHEEZING IN YOUNG CHILDREN. Dr Lại Lê Hưng Respiratory Department
 TREAMENT OF RECURRENT VIRUS-INDUCED WHEEZING IN YOUNG CHILDREN Dr Lại Lê Hưng Respiratory Department Literature review current through: Feb 2013. This topic last updated: Aug 14, 2012 INTRODUCTION Wheezing
TREAMENT OF RECURRENT VIRUS-INDUCED WHEEZING IN YOUNG CHILDREN Dr Lại Lê Hưng Respiratory Department Literature review current through: Feb 2013. This topic last updated: Aug 14, 2012 INTRODUCTION Wheezing
Shally Awasthi Professor of Pediatrics Chhatrapati Shahuji Maharaj Medical University, Lucknow
 Shally Awasthi Professor of Pediatrics Chhatrapati Shahuji Maharaj Medical University, Lucknow Magnitude of problem Misclassification of pneumonia Inappropriate use of antibiotics Inadequate Surveillance
Shally Awasthi Professor of Pediatrics Chhatrapati Shahuji Maharaj Medical University, Lucknow Magnitude of problem Misclassification of pneumonia Inappropriate use of antibiotics Inadequate Surveillance
PAEDIATRIC RESPIRATORY FAILURE. Tang Swee Fong Department of Paediatrics University Kebangsaan Malaysia Medical Centre
 PAEDIATRIC RESPIRATORY FAILURE Tang Swee Fong Department of Paediatrics University Kebangsaan Malaysia Medical Centre Outline of lecture Bronchiolitis Bronchopulmonary dysplasia Asthma ARDS Bronchiolitis
PAEDIATRIC RESPIRATORY FAILURE Tang Swee Fong Department of Paediatrics University Kebangsaan Malaysia Medical Centre Outline of lecture Bronchiolitis Bronchopulmonary dysplasia Asthma ARDS Bronchiolitis
Guidelines/Guidance/CAP/ Hospitalized Child. PHM Boot Camp 2014 Jay Tureen, MD June 19, 2014
 Guidelines/Guidance/CAP/ Hospitalized Child PHM Boot Camp 2014 Jay Tureen, MD June 19, 2014 CAP in Children: Epi Greatest cause of death in children worldwide Estimated > 2 M deaths in children In developed
Guidelines/Guidance/CAP/ Hospitalized Child PHM Boot Camp 2014 Jay Tureen, MD June 19, 2014 CAP in Children: Epi Greatest cause of death in children worldwide Estimated > 2 M deaths in children In developed
A Trust Guideline for the Management of. Bronchiolitis in Infants and Children under the age of 24 months
 A Clinical Guideline recommended Children s Assessment Unit (CAU), Buxton Ward, For use in: Children s Day Ward, Jenny Lind Out-patients Department, Accident and Emergency Department By: Medical and Nursing
A Clinical Guideline recommended Children s Assessment Unit (CAU), Buxton Ward, For use in: Children s Day Ward, Jenny Lind Out-patients Department, Accident and Emergency Department By: Medical and Nursing
Novel H1N1 Influenza A Update. William Muth MD 2 Oct 2009
 Novel H1N1 Influenza A Update William Muth MD 2 Oct 2009 Novel H1N1 Influenza A Update Epidemiology Treatment Chemoprophylaxis Vaccine Infection Prevention Novel H1N1 Influenza A International Epidemiology
Novel H1N1 Influenza A Update William Muth MD 2 Oct 2009 Novel H1N1 Influenza A Update Epidemiology Treatment Chemoprophylaxis Vaccine Infection Prevention Novel H1N1 Influenza A International Epidemiology
Objectives. Pneumonia. Pneumonia. Epidemiology. Prevalence 1/7/2012. Community-Acquired Pneumonia in infants and children
 Objectives Community-Acquired in infants and children Review of Clinical Practice Guidelines by the Pediatric Infectious Diseases Society and the Infectious Diseases Society of America - 2011 Sabah Charania,
Objectives Community-Acquired in infants and children Review of Clinical Practice Guidelines by the Pediatric Infectious Diseases Society and the Infectious Diseases Society of America - 2011 Sabah Charania,
BRONCHIOLITIS. Introduction
 BRONCHIOLITIS Introduction Bronchiolitis is the most common lower respiratory infection in infants and a leading cause of hospital admission in this age group. It is a viral infection and is most commonly
BRONCHIOLITIS Introduction Bronchiolitis is the most common lower respiratory infection in infants and a leading cause of hospital admission in this age group. It is a viral infection and is most commonly
Reducing unnecessary antibiotic use in respiratory tract infections in children
 Reducing unnecessary antibiotic use in respiratory tract infections in children -a secondary care perspective Dr Conor Doherty (Consultant in paediatric infectious diseases and immunology GGC) Current
Reducing unnecessary antibiotic use in respiratory tract infections in children -a secondary care perspective Dr Conor Doherty (Consultant in paediatric infectious diseases and immunology GGC) Current
Swine Flu Update and FAQ
 Swine Flu Update and FAQ There have now been almost 6000 laboratory proven cases of A/H1N1 in the UK and the numbers are increasing rapidly on a daily basis. The published figure will significantly underestimate
Swine Flu Update and FAQ There have now been almost 6000 laboratory proven cases of A/H1N1 in the UK and the numbers are increasing rapidly on a daily basis. The published figure will significantly underestimate
Flu is a more severe form of what people generally associate with as Cough, Cold and Fever and symptoms are usually incapacitating.
 SEASONAL HUMAN INFLUENZA (THE FLU) What is Seasonal Human Influenza? Seasonal Influenza is a viral infection that affects millions of people worldwide. It is transmitted from person to person through direct
SEASONAL HUMAN INFLUENZA (THE FLU) What is Seasonal Human Influenza? Seasonal Influenza is a viral infection that affects millions of people worldwide. It is transmitted from person to person through direct
Clinical Guidance for 2009 H1N1 Influenza and Seasonal Influenza. Barbara Wallace, MD New York State Department of Health (Updated 10/8/09)
") Clinical Guidance for 2009 H1N1 Influenza and Seasonal Influenza Barbara Wallace, MD New York State Department of Health (Updated 10/8/09) 1 Outline Clinical assessment Diagnostic testing Antiviral medications
Clinical Guidance for 2009 H1N1 Influenza and Seasonal Influenza Barbara Wallace, MD New York State Department of Health (Updated 10/8/09) 1 Outline Clinical assessment Diagnostic testing Antiviral medications
Swine flu - information prescription
 Swine flu - information prescription Introduction Swine flu is a relatively new strain of influenza (flu) that was responsible for a flu pandemic during 2009-2010. It is sometimes known as H1N1 influenza
Swine flu - information prescription Introduction Swine flu is a relatively new strain of influenza (flu) that was responsible for a flu pandemic during 2009-2010. It is sometimes known as H1N1 influenza
Objectives. Case Presentation. Respiratory Emergencies
 Respiratory Emergencies Objectives Describe how to assess airway and breathing, including interpreting information from the PAT and ABCDEs. Differentiate between respiratory distress, respiratory failure,
Respiratory Emergencies Objectives Describe how to assess airway and breathing, including interpreting information from the PAT and ABCDEs. Differentiate between respiratory distress, respiratory failure,
AT TRIAGE. Alberta Acute Childhood Asthma Pathway: Evidence based* recommendations For Emergency / Urgent Care
 1 1 Should the child be placed into the Pathway? Asthma Clinical Score (PRAM) Inclusion Children 1 year and 18 years of age who present with wheezing and respiratory distress, and have been diagnosed by
1 1 Should the child be placed into the Pathway? Asthma Clinical Score (PRAM) Inclusion Children 1 year and 18 years of age who present with wheezing and respiratory distress, and have been diagnosed by
Revised Recommendations for the Use of Influenza Antiviral Drugs
 QUESTIONS & ANSWERS Revised Recommendations for the Use of Influenza Antiviral Drugs Background On September 8, 2009 CDC updated its recommendations for the use of influenza antiviral medicines to provide
QUESTIONS & ANSWERS Revised Recommendations for the Use of Influenza Antiviral Drugs Background On September 8, 2009 CDC updated its recommendations for the use of influenza antiviral medicines to provide
Antibiotic Protocols for Paediatrics Steve Biko Academic Hospital
 Antibiotic Protocols for Paediatrics Steve Biko Academic Hospital Respiratory tract infections in children Uncomplicated URTI A child with a cold should not receive an antibiotic Paracetamol (15 mg/kg/dose
Antibiotic Protocols for Paediatrics Steve Biko Academic Hospital Respiratory tract infections in children Uncomplicated URTI A child with a cold should not receive an antibiotic Paracetamol (15 mg/kg/dose
Pediatric Respiratory Disease: A Model for the Future of Emergency Medicine Research
 Pediatric Respiratory Disease: A Model for the Future of Emergency Medicine Research Joseph J. Zorc, MD, MSCE Mark Fishman Professor, Department of Pediatrics Perelman School of Medicine, University of
Pediatric Respiratory Disease: A Model for the Future of Emergency Medicine Research Joseph J. Zorc, MD, MSCE Mark Fishman Professor, Department of Pediatrics Perelman School of Medicine, University of
Avian Influenza Clinical Picture, Risk profile & Treatment
 Avian Influenza Clinical Picture, Risk profile & Treatment Jantjie Taljaard Adult ID Unit Tygerberg Academic Hospital University of Stellenbosch jjt@sun.ac.za 083 419 1452 CLINICAL PICTURE The clinical
Avian Influenza Clinical Picture, Risk profile & Treatment Jantjie Taljaard Adult ID Unit Tygerberg Academic Hospital University of Stellenbosch jjt@sun.ac.za 083 419 1452 CLINICAL PICTURE The clinical
Emergency Department Guideline. Asthma
 Emergency Department Guideline Inclusion criteria: Patients 2 years old with: o Known history of asthma or wheezing responsive to bronchodilators presenting to the ED with cough, wheeze, shortness of breath,
Emergency Department Guideline Inclusion criteria: Patients 2 years old with: o Known history of asthma or wheezing responsive to bronchodilators presenting to the ED with cough, wheeze, shortness of breath,
Pediatric Respiratory Infections
 Pediatric Respiratory Infections Brenda Kelly PharmD BCPS Residency Program Director Virginia Mason Memorial, Yakima, Washington brendakelly@yvmh.org Disclosure The presenter has no actual or potential
Pediatric Respiratory Infections Brenda Kelly PharmD BCPS Residency Program Director Virginia Mason Memorial, Yakima, Washington brendakelly@yvmh.org Disclosure The presenter has no actual or potential
Advances in the Management of Empyema
 Advances in the Management of Empyema RCP Update in Respiratory Medicine 26 th January 2017 Najib M Rahman Associate Professor of Respiratory Medicine University of Oxford najib.rahman@ndm.ox.ac.uk Financial
Advances in the Management of Empyema RCP Update in Respiratory Medicine 26 th January 2017 Najib M Rahman Associate Professor of Respiratory Medicine University of Oxford najib.rahman@ndm.ox.ac.uk Financial
Management of Bronchiolitis in Infants
 Co-issued by Paediatric Medicine and the Division of Paediatric Emergency Medicine. 1.0 Introduction Bronchiolitis is an acute inflammatory disease of the lower respiratory tract, resulting from obstruction
Co-issued by Paediatric Medicine and the Division of Paediatric Emergency Medicine. 1.0 Introduction Bronchiolitis is an acute inflammatory disease of the lower respiratory tract, resulting from obstruction
Acute Respiratory Infection. Dr Anthony Gibson
 Acute Respiratory Infection Dr Anthony Gibson Range of Conditions Upper tract Common Cold coryza Sore Throat- Pharyngitis Sinusitis Epiglottitis Range of Conditions Lower Acute Bronchitis Acute Exacerbation
Acute Respiratory Infection Dr Anthony Gibson Range of Conditions Upper tract Common Cold coryza Sore Throat- Pharyngitis Sinusitis Epiglottitis Range of Conditions Lower Acute Bronchitis Acute Exacerbation
Management of Common Respiratory Disorders in Children. Whitney Pressler, MD Pediatric Brown Bag Series Webinar June 14, 2016
 Management of Common Respiratory Disorders in Children Whitney Pressler, MD Pediatric Brown Bag Series Webinar June 14, 2016 Disclosures I have no financial relationships to disclose I will not be discussing
Management of Common Respiratory Disorders in Children Whitney Pressler, MD Pediatric Brown Bag Series Webinar June 14, 2016 Disclosures I have no financial relationships to disclose I will not be discussing
Management of Common Respiratory Disorders in Children. Disclosures. Roadmap 6/10/2016
 Management of Common Respiratory Disorders in Children Whitney Pressler, MD Pediatric Brown Bag Series Webinar June 14, 2016 Disclosures I have no financial relationships to disclose I will not be discussing
Management of Common Respiratory Disorders in Children Whitney Pressler, MD Pediatric Brown Bag Series Webinar June 14, 2016 Disclosures I have no financial relationships to disclose I will not be discussing
Infant and Pediatric Influenza. Mike Czervinske RRT-NPS University of Kansas Medical Center
 Infant and Pediatric Influenza Mike Czervinske RRT-NPS University of Kansas Medical Center Influenza Infants and Influenza Acute infection of the respiratory tract Nose Throat Possibly lungs Pathophysiology
Infant and Pediatric Influenza Mike Czervinske RRT-NPS University of Kansas Medical Center Influenza Infants and Influenza Acute infection of the respiratory tract Nose Throat Possibly lungs Pathophysiology
Community Acquired Pneumonia
 April 2014 References: 1. Bradley JS, Byington CL, Shah SS, Alverson B, Carter ER, Harrison C, Kaplan SL Mace SE, McCracken Jr. GH, Moor MR, St. Peter SD, Stockwell JA, and Swanson JT. The Management of
April 2014 References: 1. Bradley JS, Byington CL, Shah SS, Alverson B, Carter ER, Harrison C, Kaplan SL Mace SE, McCracken Jr. GH, Moor MR, St. Peter SD, Stockwell JA, and Swanson JT. The Management of
Acute Wheezing Emergencies: From Young to Old! Little Wheezers in the ED: Managing Acute Pediatric Asthma
 Acute Wheezing Emergencies: From Young to Old! Little Wheezers in the ED: Managing Acute Pediatric Asthma Talk Outline Case Delivery of bronchodilators Meter-dose inhalers and spacers Continuous nebulization
Acute Wheezing Emergencies: From Young to Old! Little Wheezers in the ED: Managing Acute Pediatric Asthma Talk Outline Case Delivery of bronchodilators Meter-dose inhalers and spacers Continuous nebulization
ESCMID Online Lecture Library. by author
 INFLUENZA IN CHILDREN Cristian Launes Infectious Diseases Unit. Department of Paediatrics. Hospital Sant Joan de Déu (Universitat de Barcelona) Innovation in Severe Acute Respiratory Infections (SARI),
INFLUENZA IN CHILDREN Cristian Launes Infectious Diseases Unit. Department of Paediatrics. Hospital Sant Joan de Déu (Universitat de Barcelona) Innovation in Severe Acute Respiratory Infections (SARI),
Seasonal Influenza in Pregnancy and Puerperium Guideline (GL1086)
") Seasonal Influenza in Pregnancy and Puerperium Guideline (GL1086) Approval Approval Group Job Title, Chair of Committee Date Maternity & Children s Services Clinical Governance Committee Chair, Maternity
Seasonal Influenza in Pregnancy and Puerperium Guideline (GL1086) Approval Approval Group Job Title, Chair of Committee Date Maternity & Children s Services Clinical Governance Committee Chair, Maternity
Wheezing is associated with or
 S P E C I A L A R T I C L E Pertinent Issues in Diagnosis and Management of Wheezing in Under-five Children at Community Level DHEERAJ SHAH AND PIYUSH GUPTA From the Department of Pediatrics, University
S P E C I A L A R T I C L E Pertinent Issues in Diagnosis and Management of Wheezing in Under-five Children at Community Level DHEERAJ SHAH AND PIYUSH GUPTA From the Department of Pediatrics, University
SIB Chart Review Tool
 SIB Chart Review Tool Month/Year Chart Number (number sequentially 1-20) The first three questions are the same for BOTH the Inpatient and ED chart review tools. Inclusion Criteria Exclusion Criteria Age
SIB Chart Review Tool Month/Year Chart Number (number sequentially 1-20) The first three questions are the same for BOTH the Inpatient and ED chart review tools. Inclusion Criteria Exclusion Criteria Age
Viruses, bacteria, fungus, parasites (in rare cases) or other organisms can cause pneumonia.
 or other organisms can cause pneumonia.") 1 Pneumonia Pneumonia is an infection which inflames the air sacs either in one or both of the lungs. The air sacs are generally filled with fluid or pus, causing cough along with phlegm or pus, fever,
1 Pneumonia Pneumonia is an infection which inflames the air sacs either in one or both of the lungs. The air sacs are generally filled with fluid or pus, causing cough along with phlegm or pus, fever,
THIS ACTIVITY HAS EXPIRED. CME CREDIT IS NO LONGER AVAILABLE
 THIS ACTIVITY HAS EXPIRED. CME CREDIT IS NO LONGER AVAILABLE The following content is provided for informational purposes only. PREVENTION AND CONTROL OF INFLUENZA Lisa McHugh, MPH Influenza can be a serious
THIS ACTIVITY HAS EXPIRED. CME CREDIT IS NO LONGER AVAILABLE The following content is provided for informational purposes only. PREVENTION AND CONTROL OF INFLUENZA Lisa McHugh, MPH Influenza can be a serious
Dr Conroy Wong. Professor Richard Beasley. Dr Sarah Mooney. Professor Innes Asher
 Professor Richard Beasley University of Otago Director Medical Research Institute of New Zealand Wellington Dr Sarah Mooney Physiotherapy Advanced Clinician Counties Manukau Health NZ Respiratory and Sleep
Professor Richard Beasley University of Otago Director Medical Research Institute of New Zealand Wellington Dr Sarah Mooney Physiotherapy Advanced Clinician Counties Manukau Health NZ Respiratory and Sleep
Table 2: Outcomes measured. Table 1: Intrapleural alteplase instillation therapy protocol
 ORIGINAL RESEARCH ARTICLE Intrapleural F brinolytic Therapy with Alteplase in Empyema Thoracis in Children conducted in the Department of Pediatric critical care and Pulmonology unit at our institution
ORIGINAL RESEARCH ARTICLE Intrapleural F brinolytic Therapy with Alteplase in Empyema Thoracis in Children conducted in the Department of Pediatric critical care and Pulmonology unit at our institution
Trust Guideline for the management of Parapneumonic Effusion in children
 A clinical guideline recommended for use For Use in: By: For: Division responsible for document: Buxton ward, Children s Assessment Unit (CAU) All staff Children with parapneumonic effusion Women and Children
A clinical guideline recommended for use For Use in: By: For: Division responsible for document: Buxton ward, Children s Assessment Unit (CAU) All staff Children with parapneumonic effusion Women and Children
PAEDIATRIC ACUTE CARE GUIDELINE. Croup. This document should be read in conjunction with this DISCLAIMER
 Princess Margaret Hospital for Children PAEDIATRIC ACUTE CARE GUIDELINE Croup Scope (Staff): Scope (Area): All Emergency Department Clinicians Emergency Department This document should be read in conjunction
Princess Margaret Hospital for Children PAEDIATRIC ACUTE CARE GUIDELINE Croup Scope (Staff): Scope (Area): All Emergency Department Clinicians Emergency Department This document should be read in conjunction
Bronchiolitis Update. Key reviewer: Dr Philip Pattemore, Associate Professor of Paediatrics, University of Otago, Christchurch.
 www.bpac.org.nz keyword: bronchiolitis Bronchiolitis Update Key reviewer: Dr Philip Pattemore, Associate Professor of Paediatrics, University of Otago, Christchurch Key Points: Bronchiolitis is the most
www.bpac.org.nz keyword: bronchiolitis Bronchiolitis Update Key reviewer: Dr Philip Pattemore, Associate Professor of Paediatrics, University of Otago, Christchurch Key Points: Bronchiolitis is the most
INFLUENZA AND OTHER RESPIRATORY VIRUSES
 INFLUENZA AND OTHER RESPIRATORY VIRUSES Lung Foundation Australia Patient Seminar 21 st October 2017 Lynette Reid Respiratory Clinical Nurse Specialist, RHH What is influenza (the flu )? Influenza (flu)
INFLUENZA AND OTHER RESPIRATORY VIRUSES Lung Foundation Australia Patient Seminar 21 st October 2017 Lynette Reid Respiratory Clinical Nurse Specialist, RHH What is influenza (the flu )? Influenza (flu)
Paediatric Wheeze and pneumonia. RCH Asthma RCH bronchiolitis RCH pneumonia Dr S Rajapaksa
 Paediatric Wheeze and pneumonia RCH Asthma RCH bronchiolitis RCH pneumonia Dr S Rajapaksa Case Charlotte is a 2 ½ year old who presents to ED with shortness of breath and wheeze. She had been picked up
Paediatric Wheeze and pneumonia RCH Asthma RCH bronchiolitis RCH pneumonia Dr S Rajapaksa Case Charlotte is a 2 ½ year old who presents to ED with shortness of breath and wheeze. She had been picked up
Hot Topic: H1N1 Flu (Swine Flu)
") Hot Topic: H1N1 Flu (Swine Flu) For additional information go to: http://www.cdc.gov/ swineflu/general_info.htm Note: The information in this document is based on information from the CDC. The CDC site
Hot Topic: H1N1 Flu (Swine Flu) For additional information go to: http://www.cdc.gov/ swineflu/general_info.htm Note: The information in this document is based on information from the CDC. The CDC site
Turkish Thoracic Society
 Türk Toraks Derneği Turkish Thoracic Society Pocket Books Series Diagnosis and Treatment of Community Acquired Pneumonia in Children Short Version (Handbook) in English www.toraks.org.tr This report was
Türk Toraks Derneği Turkish Thoracic Society Pocket Books Series Diagnosis and Treatment of Community Acquired Pneumonia in Children Short Version (Handbook) in English www.toraks.org.tr This report was
Serum Institute of India Ltd. The Nasal-Spray Flu Vaccine (Live Attenuated Influenza Vaccine [LAIV])
![Serum Institute of India Ltd. The Nasal-Spray Flu Vaccine (Live Attenuated Influenza Vaccine [LAIV])](/thumbs/89/100792695.jpg "Serum Institute of India Ltd. The Nasal-Spray Flu Vaccine (Live Attenuated Influenza Vaccine [LAIV])") Nasovac The Nasal-Spray Flu Vaccine (Live Attenuated Influenza Vaccine [LAIV]) Questions & Answers Who can be vaccinated with the nasal-spray flu vaccine LAIV (Nasovac )? LAIV (Nasovac ) is approved for
Nasovac The Nasal-Spray Flu Vaccine (Live Attenuated Influenza Vaccine [LAIV]) Questions & Answers Who can be vaccinated with the nasal-spray flu vaccine LAIV (Nasovac )? LAIV (Nasovac ) is approved for
BEST PRACTICE COMMUNITY ACQUIRED PNEUMONIA IN CHILDREN: A CLINICAL UPDATE
 COMMUNITY ACQUIRED PNEUMONIA IN CHILDREN: A CLINICAL UPDATE See end of article for authors affiliations Correspondence to: Dr Monica Lakhanpaul, Academic Division of Child Health, Department of Medical
COMMUNITY ACQUIRED PNEUMONIA IN CHILDREN: A CLINICAL UPDATE See end of article for authors affiliations Correspondence to: Dr Monica Lakhanpaul, Academic Division of Child Health, Department of Medical
1/30/2016 RESPIRATORY INFECTIONS AND ASTHMA NO DISCLOSURES NO FINANCIAL INTEREST INFORMATION OBTAINED JACI AJRCCM
 RESPIRATORY INFECTIONS AND ASTHMA NO DISCLOSURES NO FINANCIAL INTEREST INFORMATION OBTAINED JACI AJRCCM 1 2 year old male HISTORY -Daycare since 9 months of age -Recurrent symptoms since 10 months of age:
RESPIRATORY INFECTIONS AND ASTHMA NO DISCLOSURES NO FINANCIAL INTEREST INFORMATION OBTAINED JACI AJRCCM 1 2 year old male HISTORY -Daycare since 9 months of age -Recurrent symptoms since 10 months of age:
MCH-Immunization Conference. September 2012
 MCH-Immunization Conference September 2012 Rosalyn Singleton MD Arctic Investigations Program-CDC Alaska Native Tribal Health Consortium, Anchorage, AK DISCLAIMER: The results and conclusions presented
MCH-Immunization Conference September 2012 Rosalyn Singleton MD Arctic Investigations Program-CDC Alaska Native Tribal Health Consortium, Anchorage, AK DISCLAIMER: The results and conclusions presented
Antiviral Treatment and Prophylaxis for seasonal Influenza QRG 2017/18
 Antiviral Treatment and Prophylaxis for seasonal Influenza QRG 2017/18 Selection of antiviral therapy for treatment of influenza (definitions + doses on p.2) When indicated, treatment should be started
Antiviral Treatment and Prophylaxis for seasonal Influenza QRG 2017/18 Selection of antiviral therapy for treatment of influenza (definitions + doses on p.2) When indicated, treatment should be started
Wheezy? Easy Peasy! The Emergent Management of Asthma & Bronchiolitis. Maneesha Agarwal MD Assistant Professor of Pediatrics & Emergency Medicine
 Wheezy? Easy Peasy! The Emergent Management of Asthma & Bronchiolitis Maneesha Agarwal MD Assistant Professor of Pediatrics & Emergency Medicine Asthma Defined National Asthma Education and Prevention
Wheezy? Easy Peasy! The Emergent Management of Asthma & Bronchiolitis Maneesha Agarwal MD Assistant Professor of Pediatrics & Emergency Medicine Asthma Defined National Asthma Education and Prevention
URIs and Pneumonia. Elena Bissell, MD 10/16/2013
 URIs and Pneumonia Elena Bissell, MD 10/16/2013 Objectives Recognize and treat community acquired PNA in children/adults Discern between inpatient and outpatient treatment of PNA Recognize special populations/cases
URIs and Pneumonia Elena Bissell, MD 10/16/2013 Objectives Recognize and treat community acquired PNA in children/adults Discern between inpatient and outpatient treatment of PNA Recognize special populations/cases
Early Studies. Then, the Meta-analysis. Recent Studies Al-Ansari. Recent Studies Luo University of Texas Health Science Center at San Antonio
 Pediatrics Grand Rounds Objectives Review the available literature on the use of nebulized hypertonic saline in the treatment of acute viral bronchiolitis Review proposed mechanism(s) of action and safety
Pediatrics Grand Rounds Objectives Review the available literature on the use of nebulized hypertonic saline in the treatment of acute viral bronchiolitis Review proposed mechanism(s) of action and safety
Influenza in the pediatric population
 Influenza in the pediatric population Annual attack rates 10%-40% in children Hospitalization Increased risk in children
Influenza in the pediatric population Annual attack rates 10%-40% in children Hospitalization Increased risk in children
Potential public health impact of RSV vaccines. R. Karron December 2016
 Potential public health impact of RSV vaccines R. Karron December 2016 1. RSV is The leading cause of hospitalization in infants and in many high-income countries; >2 million medical visits annually in
Potential public health impact of RSV vaccines R. Karron December 2016 1. RSV is The leading cause of hospitalization in infants and in many high-income countries; >2 million medical visits annually in
PEDIATRIC INFLUENZA CLINICAL PRACTICE GUIDELINES
 PEDIATRIC INFLUENZA CLINICAL PRACTICE GUIDELINES DEFINITIONS AND BACKGROUND Uncomplicated influenza illness is characterized by the abrupt onset of constitutional and respiratory signs and symptoms. Signs
PEDIATRIC INFLUENZA CLINICAL PRACTICE GUIDELINES DEFINITIONS AND BACKGROUND Uncomplicated influenza illness is characterized by the abrupt onset of constitutional and respiratory signs and symptoms. Signs
An overview on paediatric community-acquir ed pneumonia
 An overview on paediatric community-acquir ed pneumonia Ping LAM Department of Paediatrics, Caritas Medical Center, Hong Kong Introduction Community-acquired pneumonia (CAP) refers to pneumonia that is
An overview on paediatric community-acquir ed pneumonia Ping LAM Department of Paediatrics, Caritas Medical Center, Hong Kong Introduction Community-acquired pneumonia (CAP) refers to pneumonia that is
Outline. Seasonal Influenza & Pneumonia National & State Statistics Novel Influenza A H1N1
 Outline Seasonal Influenza & Pneumonia National & State Statistics Novel Influenza A H1N1 National & State Statistics Lessons from Past Pandemics Vaccination & Treatment Strategies Influenza Virus Influenza
Outline Seasonal Influenza & Pneumonia National & State Statistics Novel Influenza A H1N1 National & State Statistics Lessons from Past Pandemics Vaccination & Treatment Strategies Influenza Virus Influenza
Croup (Laryngo-tracheo-bronchitis)
") Croup (Laryngo-tracheo-bronchitis) 1a 2a 2b Title of Guideline (must include the word Guideline (not protocol, policy, procedure etc) Contact Name and Job Title (author) Directorate & Speciality Date of
Croup (Laryngo-tracheo-bronchitis) 1a 2a 2b Title of Guideline (must include the word Guideline (not protocol, policy, procedure etc) Contact Name and Job Title (author) Directorate & Speciality Date of
Epiglottitis. Bronchitis. Bronchiolitis. Pneumonia. Croup syndrome. Miss. kamlah 2
 Miss. kamlah 1 Epiglottitis. Bronchitis. Bronchiolitis. Pneumonia. Croup syndrome. Miss. kamlah 2 Acute Epiglottitis Is an infection of the epiglottis, the long narrow structure that closes off the glottis
Miss. kamlah 1 Epiglottitis. Bronchitis. Bronchiolitis. Pneumonia. Croup syndrome. Miss. kamlah 2 Acute Epiglottitis Is an infection of the epiglottis, the long narrow structure that closes off the glottis
Flu Vaccination. John Hann, MD UC Irvine Health
 Flu Vaccination John Hann, MD UC Irvine Health So you got the flu. What to do about. Influenza spread in US https://www.cdc.gov/flu/weekly/ Influenza spread world wide http://apps.who.int/flumart/default?reportno=6
Flu Vaccination John Hann, MD UC Irvine Health So you got the flu. What to do about. Influenza spread in US https://www.cdc.gov/flu/weekly/ Influenza spread world wide http://apps.who.int/flumart/default?reportno=6
Community school Influenza like illness In season HPZ : February 2019
 rd Public Health England South West T +44 (0)300 303 8162 3 Floor, 2 Rivergate F +44 (0)117 930 0205 Temple Quay, Bristol, BS1 6EH Follaton House, Plymouth Road F: +44 (0)1392 367356 Totnes, Devon TQ9
rd Public Health England South West T +44 (0)300 303 8162 3 Floor, 2 Rivergate F +44 (0)117 930 0205 Temple Quay, Bristol, BS1 6EH Follaton House, Plymouth Road F: +44 (0)1392 367356 Totnes, Devon TQ9
Fever in children aged less than 5 years
 Fever in children aged less than 5 years A fever is defined as a temperature greater than 38 degrees celsius Height and duration of fever do not identify serious illness. However fever in children younger
Fever in children aged less than 5 years A fever is defined as a temperature greater than 38 degrees celsius Height and duration of fever do not identify serious illness. However fever in children younger
Printed copies of this document may not be up to date, obtain the most recent version from
 Children s Acute Transport Service Clinical Guidelines Acute Severe Asthma Document Control Information Author E Randle Author Position CATS Consultant Document Owner E Polke Document Owner Position Co-ordinator
Children s Acute Transport Service Clinical Guidelines Acute Severe Asthma Document Control Information Author E Randle Author Position CATS Consultant Document Owner E Polke Document Owner Position Co-ordinator
Pandemic H1N1 2009: The Public Health Perspective. Massachusetts Department of Public Health November, 2009
 Pandemic H1N1 2009: The Public Health Perspective Massachusetts Department of Public Health November, 2009 Training Objectives Describe and distinguish between seasonal and pandemic influenza. Provide
Pandemic H1N1 2009: The Public Health Perspective Massachusetts Department of Public Health November, 2009 Training Objectives Describe and distinguish between seasonal and pandemic influenza. Provide
PEDIATRIC ACUTE ASTHMA SCORE (P.A.A.S.) GUIDELINES. >97% 94% to 96% 91%-93% <90% Moderate to severe expiratory wheeze
 GUIDELINES. >97% 94% to 96% 91%-93% <90% Moderate to severe expiratory wheeze") Inclusion: Children experiencing acute asthma exacerbation 24 months to 18 years of age with a diagnosis of asthma Patients with a previous history of asthma (Consider differential diagnosis for infants
Inclusion: Children experiencing acute asthma exacerbation 24 months to 18 years of age with a diagnosis of asthma Patients with a previous history of asthma (Consider differential diagnosis for infants
FLU VACCINE INFORMATION The FLU JAB
 FLU VACCINE INFORMATION 2018 In the UK the flu vaccine is available each year from late September or early October onwards. It is recommended to get the flu vaccine in the autumn, before outbreaks of flu
FLU VACCINE INFORMATION 2018 In the UK the flu vaccine is available each year from late September or early October onwards. It is recommended to get the flu vaccine in the autumn, before outbreaks of flu
Deep discoveries: the ED. Brian H. Rowe, MD, MSc, CCFP(EM) Canada Research Chair in Emergency Airway Diseases Department of Emergency Medicine
 Canada Research Chair in Emergency Airway Diseases Department of Emergency Medicine") Deep discoveries: Treating respiratory infections in the ED. Brian H. Rowe, MD, MSc, CCFP(EM) Canada Research Chair in Emergency Airway Diseases Department of Emergency Medicine University of Alberta Respiratory
Deep discoveries: Treating respiratory infections in the ED. Brian H. Rowe, MD, MSc, CCFP(EM) Canada Research Chair in Emergency Airway Diseases Department of Emergency Medicine University of Alberta Respiratory
Watch out, flu season is here
 D. Gary Benfield, M.D. Talking to myself about this winter s flu season: I: Tell me, old swami, what do you think about this flu season so far? Me: You want the long answer or the short answer? I: Make
D. Gary Benfield, M.D. Talking to myself about this winter s flu season: I: Tell me, old swami, what do you think about this flu season so far? Me: You want the long answer or the short answer? I: Make
PNEUMONIA IN CHILDREN. IAP UG Teaching slides
 PNEUMONIA IN CHILDREN 1 INTRODUCTION 156 million new episodes / yr. worldwide 151 million episodes developing world 95% in developing countries 19% of all deaths in children
PNEUMONIA IN CHILDREN 1 INTRODUCTION 156 million new episodes / yr. worldwide 151 million episodes developing world 95% in developing countries 19% of all deaths in children
PNEUMONIA. Introduction
 PNEUMONIA Introduction While most respiratory infections in children are acute upper respiratory infections, children presenting to hospital emergency departments commonly have lower tract respiratory
PNEUMONIA Introduction While most respiratory infections in children are acute upper respiratory infections, children presenting to hospital emergency departments commonly have lower tract respiratory
Novel H1N1 Influenza. It s the flu after all! William Muth M.D. Samaritan Health Services 9 November 2009
 Novel H1N1 Influenza It s the flu after all! William Muth M.D. Samaritan Health Services 9 November 2009 Influenza A Primer.. What is the flu? How do you get it? What s a virus anyhow? Can the flu be prevented,
Novel H1N1 Influenza It s the flu after all! William Muth M.D. Samaritan Health Services 9 November 2009 Influenza A Primer.. What is the flu? How do you get it? What s a virus anyhow? Can the flu be prevented,
NEW PNEUMONIA CASE MANAGEMENT GUIDELINES. By Andolo Miheso,Christine Wambugu, Sophie Ngugi, Warfa Osman (NCAHU MOH) & Ambrose Agweyu (KWT)
 & Ambrose Agweyu (KWT)") NEW PNEUMONIA CASE MANAGEMENT GUIDELINES By Andolo Miheso,Christine Wambugu, Sophie Ngugi, Warfa Osman (NCAHU MOH) & Ambrose Agweyu (KWT) Outline of the presentation: Overview of Child Health situation
NEW PNEUMONIA CASE MANAGEMENT GUIDELINES By Andolo Miheso,Christine Wambugu, Sophie Ngugi, Warfa Osman (NCAHU MOH) & Ambrose Agweyu (KWT) Outline of the presentation: Overview of Child Health situation
Sorting the sheep from the goats
 Sorting the sheep from the goats How do we improve the diagnosis of pediatric respiratory diseases under low-resource conditions? Pediatric Grand Rounds February 27, 2015 It doesn t matter. refugee camp
Sorting the sheep from the goats How do we improve the diagnosis of pediatric respiratory diseases under low-resource conditions? Pediatric Grand Rounds February 27, 2015 It doesn t matter. refugee camp
Management of acute asthma in children in emergency department. Moderate asthma
 152 Moderate asthma SpO2 92% No clinical features of severe asthma NB: If a patient has signs and symptoms across categories, always treat according to their most severe features agonist 2-10 puffs via
152 Moderate asthma SpO2 92% No clinical features of severe asthma NB: If a patient has signs and symptoms across categories, always treat according to their most severe features agonist 2-10 puffs via
The University of Arizona Pediatric Residency Program. Primary Goals for Rotation. Pulmonary
 The University of Arizona Pediatric Residency Program Primary Goals for Rotation Pulmonary 1. GOAL: Diagnose and manage patients with asthma. 2. GOAL: Understand the role of the pediatrician in preventing
The University of Arizona Pediatric Residency Program Primary Goals for Rotation Pulmonary 1. GOAL: Diagnose and manage patients with asthma. 2. GOAL: Understand the role of the pediatrician in preventing
Pneumococcal Vaccine in Children: current situation
 Pneumococcal Vaccine in Children: current situation LAU Yu Lung Chair Professor of Paediatrics Doris Zimmern Professor in Community Child Health LKS Faculty of Medicine, The University of Hong Kong Chairman
Pneumococcal Vaccine in Children: current situation LAU Yu Lung Chair Professor of Paediatrics Doris Zimmern Professor in Community Child Health LKS Faculty of Medicine, The University of Hong Kong Chairman
Bronchiolitis in children
 Bronchiolitis in children NICE guideline Draft for consultation, November 2014 If you wish to comment on this version of the guideline, please be aware that all the supporting information and evidence
Bronchiolitis in children NICE guideline Draft for consultation, November 2014 If you wish to comment on this version of the guideline, please be aware that all the supporting information and evidence
Approach to Bronchiolitis
 PedsCases Podcast Scripts This is a text version of a podcast from Pedscases.com on Approach to Bronchiolitis. These podcasts are designed to give medical students an overview of key topics in pediatrics.
PedsCases Podcast Scripts This is a text version of a podcast from Pedscases.com on Approach to Bronchiolitis. These podcasts are designed to give medical students an overview of key topics in pediatrics.
USAID Health Care Improvement Project. pneumonia) respiratory infections through improved case management (amb/hosp)
 respiratory infections through improved case management (amb/hosp)") Improvement objective: : decrease morbidity and mortality due to acute upper (rhinitis, sinusitis, pharyngitis) and lower (bronchitis, pneumonia) respiratory infections through improved case management
Improvement objective: : decrease morbidity and mortality due to acute upper (rhinitis, sinusitis, pharyngitis) and lower (bronchitis, pneumonia) respiratory infections through improved case management
Community-acquired pneumonia is the leading
 S Y S T E M A T I C R E V I E W Oral Antibiotics for Community acquired Pneumonia with Chestindrawing in Children Aged Below Five Years: A Systematic Review RAKESH LODHA, SHIVANI RANDEV AND SUSHIL K KABRA
S Y S T E M A T I C R E V I E W Oral Antibiotics for Community acquired Pneumonia with Chestindrawing in Children Aged Below Five Years: A Systematic Review RAKESH LODHA, SHIVANI RANDEV AND SUSHIL K KABRA
Influenza Update for Iowa Long-Term Care Facilities. Iowa Department of Public Health Center for Acute Disease Epidemiology
 Influenza Update for Iowa Long-Term Care Facilities Iowa Department of Public Health Center for Acute Disease Epidemiology Webinar Information All participants will be muted during the presentation. Questions
Influenza Update for Iowa Long-Term Care Facilities Iowa Department of Public Health Center for Acute Disease Epidemiology Webinar Information All participants will be muted during the presentation. Questions
Community Acquired Pneumonia Pediatric Ages 3 month to 18 years Clinical Practice Guideline MedStar Health Antibiotic Stewardship
 Community Acquired Pneumonia Pediatric Ages 3 month to 18 years Clinical Practice Guideline MedStar Health Antibiotic Stewardship These guidelines are provided to assist physicians and other clinicians
Community Acquired Pneumonia Pediatric Ages 3 month to 18 years Clinical Practice Guideline MedStar Health Antibiotic Stewardship These guidelines are provided to assist physicians and other clinicians