PAEDIATRIC RESPIRATORY FAILURE. Tang Swee Fong Department of Paediatrics University Kebangsaan Malaysia Medical Centre
|
|
|
- Molly Golden
- 5 years ago
- Views:
Transcription
1 PAEDIATRIC RESPIRATORY FAILURE Tang Swee Fong Department of Paediatrics University Kebangsaan Malaysia Medical Centre


2 Outline of lecture Bronchiolitis Bronchopulmonary dysplasia Asthma ARDS


3 Bronchiolitis
 Hospitalisations (57,000-172,00")




4 Bronchiolitis - Epidemiology Deaths (100) Hospitalisations (57, ,00 2-3% of children <12 months) Hospital charges: >$1.7 billion in ,000 to 199,000 deaths in children <5 years of age (mainly in resourcelimited countries) Outpatient care (800,00 children - 20% of birth cohort) Hall CB, et al. New Engl J Med 2009;360: Nair H, et al. Lancet 2010;375:
 to infants and children with diagnosis of bronchiolitis AAP Guidelines 2014")
5 Bronchiolitis - Management Lack of curative therapy Bronchodilators Corticosteroids Wheeze Clinicians should not administer albuterol (or salbutamol) to infants and children with diagnosis of bronchiolitis AAP Guidelines 2014

6 Hypertonic saline Draw fluid from submucosal and adventitial spaces replenishes air liquid surface and improve clearance of airway
7 Double-blind RCT 3%HS vs 0.9%NS 68 patients (HS: 33; NS:35) Mild to moderate acute viral bronchiolitis
 1 5.8 + 2.1 6.3 + 1.7 0.286 Severity score D2 (33, 34) 1 5.9 + 2.3 6.8 + 2.4 0.099 Severity score D3 (29, 31) 1 5.5 + 3.2 5.6 + 2.7 0.865 Severity score when fit to 1.")
8 Major outcomes Hypertonic saline Group 1 (HS) N=33 Normal saline Group II (NS) N=35 p value Days until fit to discharge (mean + SD) Days until discharge (mean + SD) Severity score D1 (33, 35) Severity score D2 (33, 34) Severity score D3 (29, 31) Severity score when fit to discharge (33, 35) 1 1 (N Group I, N Group II) Flores P, et al. Pediatr Pulmonology 2016;51:418-25
9 Major outcomes Hypertonic saline Group 1 (HS) N=33 Normal saline Group II (NS) N=35 p value Days until fit to discharge (mean + SD) Days until discharge (mean + SD) Severity score D1 (33, 35) Severity score D2 (33, 34) Severity score D3 (29, 31) Severity score when fit to discharge (33, 35) 1 1 (N Group I, N Group II) Flores P, et al. Pediatr Pulmonology 2016;51:418-25
10 Minor outcomes Hypertonic saline Group 1 (HS) N=33 Normal saline Group II (NS) N=35 p value Supplemental oxygen, duration (h) Further doses of salbutamol 17 (51.5) 23 (65.7) Nebulised epinephrine 9 (27.3) 23 (14.3) Systemic corticosteroids 8 (24.2) 10 (28.6) Antibiotics 18 (54.5) 13 (37.1) Patients in HS group had significantly more Cough (46% vs 20%, p=0.025) Rhinorrhoea infants with bronchiolitis (58% vs 31%, p=0.03) Our results do not support the use of HS in Flores P, et al. Pediatr Pulmonology 2016;51:418-25

11 10 hospitals in UK 317 infants (HS: 158; NS: 159) 3% HS vs standard therapy Thorax 2014;69:
 Hazard ratio: 0.97, (95%CI: 0.76-1.")

12 SABRE (hypertonic Saline in Acute Bronchiolitis Rct and Economic evaluation Hazard ratio: 0.95, (95%CI: ) Hazard ratio: 0.97, (95%CI: ) This study does not support the use of nebulised HS in the treatment of acute bronchiolitis over usual care with minimal handlings Everard M, et al. Thorax 2014;69:
13 Retrospective, cohort study Single centre 135 patients Pediatr Crit Care Med 2017;18:e106-e111
14 Cumulative fluid balance (ml/kg) Early fluid overload prolongs mechanical ventilation *p<0.05 *p<0.01 * ** * * 92.6% had a positive cumulative fluid balance starting on day of admission Duration of mechanical ventilation positively correlated with mean cumulative fluid balance Study day No association between fluid status and OSI Ingelse SA, et al. Pediatr Crit Care Med 2017;18:e108-e111

15 (Pediatr Crit Care Med 2017;18:e106-e111) Early fluid overload independent predictor of prolonged mechanical ventilation

16 New Engl J Med 2006;354: Crit Care Med 2012;40:2883-9
 p<0.")
 p<0.02, 95%CI -0.")
17 (Crit Care Res Pract 2011;854142) p<0.02, 95%CI 1.09 (1.00, 1.18) p<0.02, 95%CI (-0.42, -0.01)

18 Judicious fluid management

19 Lancet 2017;369:930-9 Aim HFWHO provided enhanced respiratory support Shorter time to weaning off oxygen Treatment arm HFWHO (1L/kg to maximum of 20 L, maximum FiO 2 of 0.6) Control arm standard therapy (cold wall oxygen 100% via nasal cannulae at low flow to a maximum of 2L/min)
20
21 HFWHO treatment failure and care escalation (ITT) Treatment failure Standard therapy N (%) HFWHO N (%) p value Difference (95%CI) 33 (33) 14 (14) % (8-30) Crossover 32 (32) 1 (1) < % (17-44) Rescued 20 (20) ICU transfer 17 (12) 14 (14) % (-7 to 16) Kepreotes E, et al. Lancet 2017;369:930-9
22 HFWHO HFWHO - summary and standard therapy were both effective early use did not alter overall course of bronchiolitis prevented deterioration in significantly more infants able to reverse deterioration in 63% This study provides evidence for the use of HFWHO at a maximum of 1L/kg per min (FIO 2 0.6) in the management of children with bronchiolitis of moderate severity for whom standard therapy with oxygen at 2L/min has failed or have used HFWHO from the outset Kepreotes E, et al. Lancet 2017;369:930-9

23 Bronchiolitis management in 2017 Supplemental oxygen Minimal handling Provision and judicious use of fluids

24 Chronic lung disease of infancy (Bronchopulmonary dysplasia) BPD complicated with pulmonary hypertension associated with increased morbidity and mortality
25 18 patients with BPD Pulmonary pressure assessment: Echocardiography and cardiac catheterisation PH medication: Sildenafil alone - 12, Sildenafil + Bosentan 5, Bosentan alone 1
26 Clinical improvement A decrease in Ross functional class by at least one degree Haemodynamic improvement A decrease in pulmonary hypertension severity by one level
27 Ross functional class over time Echocardiographic score over time vs , p< Moderate or severe PH 72% vs 17% moderate PH, p<0.001
 Circulation")
28 PAH-targeted therapy can be useful for infants with BPD and PH on optimal treatment of underlying respiratory and cardiac disease (Class IIa; Level ofevidence C) Circulation 2015;132

29 Asthma Magnesium sulphate infusion

30 Pediatr Crit Care Med 2016;17:e29-33 Prospective randomised open-label trial 6-16 year old with severe asthma Emergency department iv MgSO 4 50mg/kg bolus vs high dose infusion 50mg/kg/hr for 4 hours
31 Outcomes Main outcomes Bolus High dose infusion p value LOS < 24 hrs, n (%) 2 (10.5) 9 (47.4) Absolute risk reduction 37%; 95% CI, 10-63; NNT, 3 LOS (hr) (mean + SD) Cost (US$) (mean + SD) Irazuzta et al. Pediatr Crit Care Med 2016;17:e29-33
32 Outcomes Main outcomes Bolus High dose infusion p value Early utilisation of high-dose prolonged MgSO 4 infusion expedites discharge from emergency department with significant reduction in healthcare cost LOS < 24 hrs, n (%) 2 (10.5) 9 (47.4) Absolute risk reduction 37%; 95% CI, 10-63; NNT, 3 LOS (hr) (mean + SD) Cost (US$) (mean + SD) Irazuzta et al. Pediatr Crit Care Med 2016;17:e29-33

33 ..if a little is good, more is even better? Comparatively easy to use Relatively good side effect profile Inexpensive? Higher dose short term infusion useful adjunct

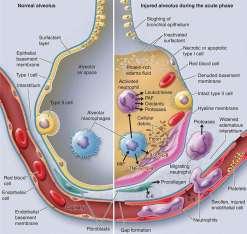
34 Acute Respiratory Distress Syndrome
 / PaCO")
35 Pediatr Crit Care Med 2016;17:101-9 Alveolar dead space fraction = (PaCo 2 PetCO 2 ) / PaCO 2
36 AVDSf
37 AVDSf AUROC 0.76; (95% CI, ; p<0.001) Better than OI or PaO 2 /FiO 2 Yehya N, et al. Pediatr Crit Care Med 2016;17:101-9

38 Pediatr Crit Care Med 2017;18:e229-e234 Oxygenation

39 Pediatr Crit Care Med 2017;18:e229-e mechanically ventilated patients Responders: >10% increase in OI
40 Changes in oxygenation and regional ventilation Responders (n=4) Non-responders (n=8) Baseline 60 min Baseline 60 min OI % change in OI N/A N/A PaO 2 /FiO SpO 2 /FiO Responders proportion of ventilation increased in dorsal lung (49% to 57%) Improvement in ventilation homogeneity Lupton-Smith A, et al.. Pediatr Crit Care Med 2017;18:e229-e234
41 Novel insights on ventilation distribution on turning prone Not all infants and children respond positively Degree of response variable Ventilation becomes more homogenous with time improving V/Q matching Highlights clinical utility of electrical impedance tomography to aid in identifying those more likely to respond
42 JPEN J Parentr Enteral Nutr 2016? Nutrition delivery to children pards? Provision of adequate nutrition improved clinical outcomes
43 Caloric intake Protein intake ICU mortality with adequate caloric intake, 34.6% vs 60.5%, p=.025 ICU mortality with adequate protein intake, 14.3% vs 60.2%, p=.002 Significantly associated with ventilator-free days
44 JPEN J Parentr Enteral Nutr 2016 Adequate nutrition delivery improves clinical outcome Protein delivery may have potentially more impact than caloric intake

45 Pediatri Crit Care Med 2017;18:
46 Guidelines for provision and assessment of nutrition support therapy Reiterates importance of nutritional assessment Need for renewed focus on Accurate estimation of energy needs Attention to optimising protein intake Optimal route and timing of nutrient delivery still debated and investigated enteral nutrition preferred route of delivery
47 Open-labelled RCT Expected length of stay > 72 hours JAMA, 2016;316: JAMA 2016;316: PaO 2 (mmhg) SpO 2 (%) Conservative Conventional Up to Unplanned early termination
48 Oxygen-ICU: ICU mortality Conservative PaO2 70 to 100 mmhg SpO2 94%-98% Conventional PaO2 up to 150 mmhg SpO2 97%-100% Girardis M, et al. JAMA 2015;316:1583-9
 Secondary outcome Shock Liver failure Bacteraemia 8 (3.7) 4 (1.9) 11 (5.1) 23 (10.6) 14 (6.4) 22 (10.1) 0.086 (0.017-0.150) NNT 12 0.068 (0.020-0.120) 0.046 (0.008-0.088) 0.050 (0.000-0.")
49 Oxygen therapy, No. (%) Conservative (n=216) Conventional (n=218) Absolute risk JAMA 2016;316: p value reduction (95%CI) Primary outcome Mortality 25 (11.6) 44 (20.2) Secondary outcome Shock Liver failure Bacteraemia 8 (3.7) 4 (1.9) 11 (5.1) 23 (10.6) 14 (6.4) 22 (10.1) ( ) NNT ( ) ( ) ( )

50 Potential impact to current practice Mindful of the potential harms of hyperoxia in critically ill patients Judicious use of supplemental oxygen titrating to maintain normoxia

51 Am J Respir Crit Care Med 2017;195:331-8
52 Clinical outcome by ARDS Subphenotype Subphenotype 1 (n=727) Subphenotype 2 (n=273) p value 60-d mortality, % < d mortality, % <0.001 Ventilator-free days, median 19 3 <0.001
53 Clinical outcome by ARDS Subphenotype Subphenotype 1 (n=727) Subphenotype 2 (n=273) p value 60-d mortality, % < d mortality, % <0.001 Ventilator-free days, median 19 3 <0.001 Interaction between ARDS Subphenotype and Fluid Management Strategy Fluid management strategy Subphenotype 1 Subphenotype 2 p value Conservative (n=349) Liberal (n=367) Conservative (n=142) Liberal (n=131) 60-d mortality, % d mortality, % Ventilator-free days, median


54 Lancet Respir Med 2014
55 Association between phenotype assignment and clinical outcome ARMA cohort ALVEOLI cohort Phenotype 1 (n=308) Phenotype 2 (n=155) p value Phenotype 1 (n=404) Phenotype 2 (n=145) p value 90-d mortality 23% 44% % 51% <0.001 Ventilator-free days Organ-failure free days < < < <0.001 Differences in response to PEEP strategy (ALVEOLI cohort only) Phenotype 1 (n=404) Phenotype 2 (n=145) Low PEEP (n=202) High PEEP (n=202) Low PEEP (n=71) High PEEP (n=74) p value 90-d mortality 33 (16%) 48 (24%) 36 (51%) 31 (42%) Ventilator-free days 20 (10-25) 21 (3-24) 2 (0-21) 4.5 (0-20) Organ-failure free days 22 (11-26) 22 (9-26) 4 (0-18) 6.5 (0-21) 0.003


56 Amer J Respir Crit Care Med 2017;195:3:280-1


57

58 2026/2027 PAEDIATRIC RESPIRATORY FAILURE

59
60 Thank you
Steroids for ARDS. Clinical Problem. Management
 Steroids for ARDS James Beck Clinical Problem A 60 year old lady re-presented to ICU with respiratory failure. She had previously been admitted for fluid management and electrolyte correction having presented
Steroids for ARDS James Beck Clinical Problem A 60 year old lady re-presented to ICU with respiratory failure. She had previously been admitted for fluid management and electrolyte correction having presented
Landmark articles on ventilation
 Landmark articles on ventilation Dr Shrikanth Srinivasan MD,DNB,FNB,EDIC Consultant, Critical Care Medicine Medanta, The Medicity ARDS AECC DEFINITION-1994 ALI Acute onset Bilateral chest infiltrates PCWP
Landmark articles on ventilation Dr Shrikanth Srinivasan MD,DNB,FNB,EDIC Consultant, Critical Care Medicine Medanta, The Medicity ARDS AECC DEFINITION-1994 ALI Acute onset Bilateral chest infiltrates PCWP
Pediatric Respiratory Disease: A Model for the Future of Emergency Medicine Research
 Pediatric Respiratory Disease: A Model for the Future of Emergency Medicine Research Joseph J. Zorc, MD, MSCE Mark Fishman Professor, Department of Pediatrics Perelman School of Medicine, University of
Pediatric Respiratory Disease: A Model for the Future of Emergency Medicine Research Joseph J. Zorc, MD, MSCE Mark Fishman Professor, Department of Pediatrics Perelman School of Medicine, University of
NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE SCOPE
 NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE 1 Guideline title SCOPE Bronchiolitis: diagnosis and management of bronchiolitis in children. 1.1 Short title Bronchiolitis in children 2 The remit The
NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE 1 Guideline title SCOPE Bronchiolitis: diagnosis and management of bronchiolitis in children. 1.1 Short title Bronchiolitis in children 2 The remit The
Management of Acute Asthma Exacerbations in Children 2012 Update. Sharon Kling Dept Paediatrics & Child Health University of Stellenbosch
 Management of Acute Asthma Exacerbations in Children 2012 Update Sharon Kling Dept Paediatrics & Child Health University of Stellenbosch Acknowledgements BTS/SIGN guidelines GINA guidelines NAEPP guidelines
Management of Acute Asthma Exacerbations in Children 2012 Update Sharon Kling Dept Paediatrics & Child Health University of Stellenbosch Acknowledgements BTS/SIGN guidelines GINA guidelines NAEPP guidelines
Hazards and Benefits of Postnatal Steroids. David J. Burchfield, MD Professor and Chief, Neonatology University of Florida
 Hazards and Benefits of Postnatal Steroids David J. Burchfield, MD Professor and Chief, Neonatology University of Florida Disclosures I have no financial affiliations or relationships to disclose. I will
Hazards and Benefits of Postnatal Steroids David J. Burchfield, MD Professor and Chief, Neonatology University of Florida Disclosures I have no financial affiliations or relationships to disclose. I will
Early Studies. Then, the Meta-analysis. Recent Studies Al-Ansari. Recent Studies Luo University of Texas Health Science Center at San Antonio
 Pediatrics Grand Rounds Objectives Review the available literature on the use of nebulized hypertonic saline in the treatment of acute viral bronchiolitis Review proposed mechanism(s) of action and safety
Pediatrics Grand Rounds Objectives Review the available literature on the use of nebulized hypertonic saline in the treatment of acute viral bronchiolitis Review proposed mechanism(s) of action and safety
Oxygenation Failure. Increase FiO2. Titrate end-expiratory pressure. Adjust duty cycle to increase MAP. Patient Positioning. Inhaled Vasodilators
 Oxygenation Failure Increase FiO2 Titrate end-expiratory pressure Adjust duty cycle to increase MAP Patient Positioning Inhaled Vasodilators Extracorporeal Circulation ARDS Radiology Increasing Intensity
Oxygenation Failure Increase FiO2 Titrate end-expiratory pressure Adjust duty cycle to increase MAP Patient Positioning Inhaled Vasodilators Extracorporeal Circulation ARDS Radiology Increasing Intensity
Emergency Medicine High Velocity Nasal Insufflation (Hi-VNI) VAPOTHERM POCKET GUIDE
 VAPOTHERM POCKET GUIDE") Emergency Medicine High Velocity Nasal Insufflation (Hi-VNI) VAPOTHERM POCKET GUIDE Indications for Vapotherm High Velocity Nasal Insufflation (Hi-VNI ) administration, the patient should be: Spontaneously
Emergency Medicine High Velocity Nasal Insufflation (Hi-VNI) VAPOTHERM POCKET GUIDE Indications for Vapotherm High Velocity Nasal Insufflation (Hi-VNI ) administration, the patient should be: Spontaneously
USE OF INHALED NITRIC OXIDE IN THE NICU East Bay Newborn Specialists Guideline Prepared by P Joe, G Dudell, A D Harlingue Revised 7/9/2014
 USE OF INHALED NITRIC OXIDE IN THE NICU East Bay Newborn Specialists Guideline Prepared by P Joe, G Dudell, A D Harlingue Revised 7/9/2014 ino for Late Preterm and Term Infants with Severe PPHN Background:
USE OF INHALED NITRIC OXIDE IN THE NICU East Bay Newborn Specialists Guideline Prepared by P Joe, G Dudell, A D Harlingue Revised 7/9/2014 ino for Late Preterm and Term Infants with Severe PPHN Background:
ARDS: an update 6 th March A. Hakeem Al Hashim, MD, FRCP SQUH
 ARDS: an update 6 th March 2017 A. Hakeem Al Hashim, MD, FRCP SQUH 30M, previously healthy Hx: 1 week dry cough Gradually worsening SOB No travel Hx Case BP 130/70, HR 100/min ph 7.29 pco2 35 po2 50 HCO3
ARDS: an update 6 th March 2017 A. Hakeem Al Hashim, MD, FRCP SQUH 30M, previously healthy Hx: 1 week dry cough Gradually worsening SOB No travel Hx Case BP 130/70, HR 100/min ph 7.29 pco2 35 po2 50 HCO3
Year in Review Intensive Care Training Program Radboud University Medical Centre Nijmegen
 Year in Review 2013 Intensive Care Training Program Radboud University Medical Centre Nijmegen Contents ARDS Ventilator associated pneumonia Tracheostomy and endotracheal intubation Enteral feeding Fluid
Year in Review 2013 Intensive Care Training Program Radboud University Medical Centre Nijmegen Contents ARDS Ventilator associated pneumonia Tracheostomy and endotracheal intubation Enteral feeding Fluid
An Overview of Bronchopulmonary Dysplasia and Chronic Lung Disease in Infancy
 An Overview of Bronchopulmonary Dysplasia and Chronic Lung Disease in Infancy Housekeeping: I have no financial disclosures Learning objectives: Develop an understanding of bronchopulmonary dysplasia (BPD)
An Overview of Bronchopulmonary Dysplasia and Chronic Lung Disease in Infancy Housekeeping: I have no financial disclosures Learning objectives: Develop an understanding of bronchopulmonary dysplasia (BPD)
The use of proning in the management of Acute Respiratory Distress Syndrome
 Case 3 The use of proning in the management of Acute Respiratory Distress Syndrome Clinical Problem This expanded case summary has been chosen to explore the rationale and evidence behind the use of proning
Case 3 The use of proning in the management of Acute Respiratory Distress Syndrome Clinical Problem This expanded case summary has been chosen to explore the rationale and evidence behind the use of proning
Inhaled nitric oxide: clinical evidence for use in adults
 Inhaled nitric oxide: clinical evidence for use in adults Neill Adhikari Critical Care Medicine Sunnybrook Health Sciences Centre and University of Toronto 31 October 2014 Conflict of interest Ikaria provided
Inhaled nitric oxide: clinical evidence for use in adults Neill Adhikari Critical Care Medicine Sunnybrook Health Sciences Centre and University of Toronto 31 October 2014 Conflict of interest Ikaria provided
The new ARDS definitions: what does it mean?
 The new ARDS definitions: what does it mean? Richard Beale 7 th September 2012 METHODS ESICM convened an international panel of experts, with representation of ATS and SCCM The objectives were to update
The new ARDS definitions: what does it mean? Richard Beale 7 th September 2012 METHODS ESICM convened an international panel of experts, with representation of ATS and SCCM The objectives were to update
Management of Severe ARDS: Current Canadian Practice
 Management of Severe ARDS: Current Canadian Practice Erick Duan MD FRCPC Clinical Scholar, Department of Medicine, Division of Critical Care, McMaster University Intensivist, St. Joseph's Healthcare Hamilton
Management of Severe ARDS: Current Canadian Practice Erick Duan MD FRCPC Clinical Scholar, Department of Medicine, Division of Critical Care, McMaster University Intensivist, St. Joseph's Healthcare Hamilton
Acute Wheezing Emergencies: From Young to Old! Little Wheezers in the ED: Managing Acute Pediatric Asthma
 Acute Wheezing Emergencies: From Young to Old! Little Wheezers in the ED: Managing Acute Pediatric Asthma Talk Outline Case Delivery of bronchodilators Meter-dose inhalers and spacers Continuous nebulization
Acute Wheezing Emergencies: From Young to Old! Little Wheezers in the ED: Managing Acute Pediatric Asthma Talk Outline Case Delivery of bronchodilators Meter-dose inhalers and spacers Continuous nebulization
Best of Pulmonary Jennifer R. Hucks, MD University of South Carolina School of Medicine
 Best of Pulmonary 2012-2013 Jennifer R. Hucks, MD University of South Carolina School of Medicine Topics ARDS- Berlin Definition Prone Positioning For ARDS Lung Protective Ventilation In Patients Without
Best of Pulmonary 2012-2013 Jennifer R. Hucks, MD University of South Carolina School of Medicine Topics ARDS- Berlin Definition Prone Positioning For ARDS Lung Protective Ventilation In Patients Without
UPDATE IN HOSPITAL MEDICINE
 UPDATE IN HOSPITAL MEDICINE FLORIDA CHAPTER ACP MEETING 2016 Himangi Kaushal, M.D., F.A.C.P. Program Director Memorial Healthcare System Internal Medicine Residency DISCLOSURES None OBJECTIVES Review some
UPDATE IN HOSPITAL MEDICINE FLORIDA CHAPTER ACP MEETING 2016 Himangi Kaushal, M.D., F.A.C.P. Program Director Memorial Healthcare System Internal Medicine Residency DISCLOSURES None OBJECTIVES Review some
The Art and Science of Weaning from Mechanical Ventilation
 The Art and Science of Weaning from Mechanical Ventilation Shekhar T. Venkataraman M.D. Professor Departments of Critical Care Medicine and Pediatrics University of Pittsburgh School of Medicine Some definitions
The Art and Science of Weaning from Mechanical Ventilation Shekhar T. Venkataraman M.D. Professor Departments of Critical Care Medicine and Pediatrics University of Pittsburgh School of Medicine Some definitions
DAYTON CHILDREN S HOSPITAL CLINICAL PRACTICE GUIDELINES
 DAYTON CHILDREN S HOSPITAL CLINICAL PRACTICE GUIDELINES DISCLAIMER: This Clinical Practice Guideline (CPG) generally describes a recommended course of treatment for patients with the identified health
DAYTON CHILDREN S HOSPITAL CLINICAL PRACTICE GUIDELINES DISCLAIMER: This Clinical Practice Guideline (CPG) generally describes a recommended course of treatment for patients with the identified health
Case discussion Acute severe asthma during pregnancy. J.G. van der Hoeven
 Case discussion Acute severe asthma during pregnancy J.G. van der Hoeven Case (1) 32-year-old female - gravida 3 - para 2 Previous medical history - asthma Pregnant (33 w) Acute onset fever with wheezing
Case discussion Acute severe asthma during pregnancy J.G. van der Hoeven Case (1) 32-year-old female - gravida 3 - para 2 Previous medical history - asthma Pregnant (33 w) Acute onset fever with wheezing
High-flow nasal cannula use in a paediatric intensive care unit over 3 years
 High-flow nasal cannula use in a paediatric intensive care unit over 3 years Tracey I Wraight and Subodh S Ganu Respiratory illness and/or distress is the commonest reason for non-elective paediatric intensive
High-flow nasal cannula use in a paediatric intensive care unit over 3 years Tracey I Wraight and Subodh S Ganu Respiratory illness and/or distress is the commonest reason for non-elective paediatric intensive
Kugelman A, Riskin A, Said W, Shoris I, Mor F, Bader D.
 Heated, Humidified High-Flow Nasal Cannula (HHHFNC) vs. Nasal Intermittent Positive Pressure Ventilation (NIPPV) for the Primary Treatment of RDS, A Randomized, Controlled, Prospective, Pilot Study Kugelman
Heated, Humidified High-Flow Nasal Cannula (HHHFNC) vs. Nasal Intermittent Positive Pressure Ventilation (NIPPV) for the Primary Treatment of RDS, A Randomized, Controlled, Prospective, Pilot Study Kugelman
DAYTON CHILDREN S HOSPITAL CLINICAL PRACTICE GUIDELINES
 DAYTON CHILDREN S HOSPITAL CLINICAL PRACTICE GUIDELINES DISCLAIMER: This Clinical Practice Guideline (CPG) generally describes a recommended course of treatment for patients with the identified health
DAYTON CHILDREN S HOSPITAL CLINICAL PRACTICE GUIDELINES DISCLAIMER: This Clinical Practice Guideline (CPG) generally describes a recommended course of treatment for patients with the identified health
ECMO FOR PEDIATRIC RESPIRATORY FAILURE. Novik Budiwardhana * PCICU Harapan Kita National Cardiovascular Center Jakarta
 ECMO FOR PEDIATRIC RESPIRATORY FAILURE Novik Budiwardhana * PCICU Harapan Kita National Cardiovascular Center Jakarta Introduction Case D 8 month old baby with severe ARDS with fungal sepsis. He was on
ECMO FOR PEDIATRIC RESPIRATORY FAILURE Novik Budiwardhana * PCICU Harapan Kita National Cardiovascular Center Jakarta Introduction Case D 8 month old baby with severe ARDS with fungal sepsis. He was on
Wanchai Wongkornrat Cardiovascular Thoracic Surgery Siriraj Hospital Mahidol University
 Wanchai Wongkornrat Cardiovascular Thoracic Surgery Siriraj Hospital Mahidol University Assess adequacy of ventilation and oxygenation Aids in establishing a diagnosis and severity of respiratory failure
Wanchai Wongkornrat Cardiovascular Thoracic Surgery Siriraj Hospital Mahidol University Assess adequacy of ventilation and oxygenation Aids in establishing a diagnosis and severity of respiratory failure
Supplementary appendix
 Supplementary appendix This appendix formed part of the original submission and has been peer reviewed. We post it as supplied by the authors. Supplement to: Blum CA, Nigro N, Briel M, et al. Adjunct prednisone
Supplementary appendix This appendix formed part of the original submission and has been peer reviewed. We post it as supplied by the authors. Supplement to: Blum CA, Nigro N, Briel M, et al. Adjunct prednisone
Weaning and extubation in PICU An evidence-based approach
 Weaning and extubation in PICU An evidence-based approach Suchada Sritippayawan, MD. Div. Pulmonology & Crit Care Dept. Pediatrics Faculty of Medicine Chulalongkorn University Kanokporn Udomittipong, MD.
Weaning and extubation in PICU An evidence-based approach Suchada Sritippayawan, MD. Div. Pulmonology & Crit Care Dept. Pediatrics Faculty of Medicine Chulalongkorn University Kanokporn Udomittipong, MD.
BRONCHIOLITIS. See also the PSNZ guideline - Wheeze & Chest Infections in infants under 1 year (www.paediatrics.org.nz)
") Definition What is Bronchiolitis? Assessment Management Flow Chart Admission Guidelines Investigations Management Use of Bronchodilators Other treatments Discharge Planning Bronchiolitis & Asthma References
Definition What is Bronchiolitis? Assessment Management Flow Chart Admission Guidelines Investigations Management Use of Bronchodilators Other treatments Discharge Planning Bronchiolitis & Asthma References
Adjunct Therapies for Pediatric ARDS: Where are the Data?
 Adjunct Therapies for Pediatric ARDS: Where are the Data? Alexandre T. Rotta, MD, FCCM Professor of Pediatrics, Linsalata Family Endowed Chair in Pediatric Critical Care and Emergency Medicine Rainbow
Adjunct Therapies for Pediatric ARDS: Where are the Data? Alexandre T. Rotta, MD, FCCM Professor of Pediatrics, Linsalata Family Endowed Chair in Pediatric Critical Care and Emergency Medicine Rainbow
Difficult Ventilation in ARDS Patients
 Thank you for viewing this presentation. We would like to remind you that this material is the property of the author. It is provided to you by the ERS for your personal use only, as submitted by the author.
Thank you for viewing this presentation. We would like to remind you that this material is the property of the author. It is provided to you by the ERS for your personal use only, as submitted by the author.
Fluid Resuscitation in Critically Ill Patients with Acute Kidney Injury (AKI)
") Fluid Resuscitation in Critically Ill Patients with Acute Kidney Injury (AKI) Robert W. Schrier, MD University of Colorado School of Medicine Denver, Colorado USA Prevalence of acute renal failure in Intensive
Fluid Resuscitation in Critically Ill Patients with Acute Kidney Injury (AKI) Robert W. Schrier, MD University of Colorado School of Medicine Denver, Colorado USA Prevalence of acute renal failure in Intensive
Timing of Parenteral Nutrition
 Timing of Parenteral Nutrition Arun Bansal; MD, FCCM, MRCPCH Professor Pediatric Critical Care PGIMER, Chandigarh, INDIA drarunbansal@gmail.com Malnutrition in Critically Ill Incidence: from 19 32% Associated
Timing of Parenteral Nutrition Arun Bansal; MD, FCCM, MRCPCH Professor Pediatric Critical Care PGIMER, Chandigarh, INDIA drarunbansal@gmail.com Malnutrition in Critically Ill Incidence: from 19 32% Associated
Wheezy? Easy Peasy! The Emergent Management of Asthma & Bronchiolitis. Maneesha Agarwal MD Assistant Professor of Pediatrics & Emergency Medicine
 Wheezy? Easy Peasy! The Emergent Management of Asthma & Bronchiolitis Maneesha Agarwal MD Assistant Professor of Pediatrics & Emergency Medicine Asthma Defined National Asthma Education and Prevention
Wheezy? Easy Peasy! The Emergent Management of Asthma & Bronchiolitis Maneesha Agarwal MD Assistant Professor of Pediatrics & Emergency Medicine Asthma Defined National Asthma Education and Prevention
Steroids in ARDS: if, when, how much? John Fowler, MD, FACEP Dept. of Emergency Medicine Kent Hospital, İzmir, Türkiye
 Steroids in ARDS: if, when, how much? John Fowler, MD, FACEP Dept. of Emergency Medicine Kent Hospital, İzmir, Türkiye Steroids in ARDS: conclusion Give low-dose steroids if indicated for another problem
Steroids in ARDS: if, when, how much? John Fowler, MD, FACEP Dept. of Emergency Medicine Kent Hospital, İzmir, Türkiye Steroids in ARDS: conclusion Give low-dose steroids if indicated for another problem
Recurrent wheezing illnesses 24.9% Similar to Australia Above global averages
 Prof Mike South Department of General Medicine Royal Children s Hospital Melbourne Australia www.mikesouth.org.au Asthma is very common in Australia Approx 25% children have recurrent wheezing illnesses
Prof Mike South Department of General Medicine Royal Children s Hospital Melbourne Australia www.mikesouth.org.au Asthma is very common in Australia Approx 25% children have recurrent wheezing illnesses
Guidelines and Best Practices for High Flow Nasal Cannula (HFNC) Pediatric Pocket Guide
 Pediatric Pocket Guide") Guidelines Best Practices for High Flow Nasal Cannula (HFNC) Pediatric Pocket Guide Patient Selection Diagnoses Patient presents with one or more of the following signs or symptoms of respiratory distress:
Guidelines Best Practices for High Flow Nasal Cannula (HFNC) Pediatric Pocket Guide Patient Selection Diagnoses Patient presents with one or more of the following signs or symptoms of respiratory distress:
Ventilatory Management of ARDS. Alexei Ortiz Milan; MD, MSc
 Ventilatory Management of ARDS Alexei Ortiz Milan; MD, MSc 2017 Outline Ventilatory management of ARDS Protected Ventilatory Strategy Use of NMB Selection of PEEP Driving pressure Lung Recruitment Prone
Ventilatory Management of ARDS Alexei Ortiz Milan; MD, MSc 2017 Outline Ventilatory management of ARDS Protected Ventilatory Strategy Use of NMB Selection of PEEP Driving pressure Lung Recruitment Prone
Sub-category: Intensive Care for Respiratory Distress
 Course n : Course 3 Title: RESPIRATORY PHYSIOLOGY, PHYSICS AND PATHOLOGY IN RELATION TO ANAESTHESIA AND INTENSIVE CARE Sub-category: Intensive Care for Respiratory Distress Topic: Acute Respiratory Distress
Course n : Course 3 Title: RESPIRATORY PHYSIOLOGY, PHYSICS AND PATHOLOGY IN RELATION TO ANAESTHESIA AND INTENSIVE CARE Sub-category: Intensive Care for Respiratory Distress Topic: Acute Respiratory Distress
ARDS and Lung Protection
 ARDS and Lung Protection Kristina Sullivan, MD Associate Professor University of California, San Francisco Department of Anesthesia and Perioperative Care Division of Critical Care Medicine Overview Low
ARDS and Lung Protection Kristina Sullivan, MD Associate Professor University of California, San Francisco Department of Anesthesia and Perioperative Care Division of Critical Care Medicine Overview Low
Provide guidelines for the management of mechanical ventilation in infants <34 weeks gestation.
 Page 1 of 5 PURPOSE: Provide guidelines for the management of mechanical ventilation in infants
Page 1 of 5 PURPOSE: Provide guidelines for the management of mechanical ventilation in infants
Bronchoalveolar lavage (BAL) with surfactant in pediatric ARDS
 with surfactant in pediatric ARDS") Bronchoalveolar lavage (BAL) with surfactant in pediatric ARDS M. Luchetti, E. M. Galassini, A. Galbiati, C. Pagani,, F. Silla and G. A. Marraro gmarraro@picu.it www.picu.it Anesthesia and Intensive Care
Bronchoalveolar lavage (BAL) with surfactant in pediatric ARDS M. Luchetti, E. M. Galassini, A. Galbiati, C. Pagani,, F. Silla and G. A. Marraro gmarraro@picu.it www.picu.it Anesthesia and Intensive Care
Top Papers in Cri-cal Care Janna Landsperger, ACNP- BC
 Top Papers in Cri-cal Care 2016 Janna Landsperger, ACNP- BC Objec-ves Review journal articles regarding delivery of critical care published over the past twelve months Provide evidence in support of current
Top Papers in Cri-cal Care 2016 Janna Landsperger, ACNP- BC Objec-ves Review journal articles regarding delivery of critical care published over the past twelve months Provide evidence in support of current
Late pulmonary hypertension in preterm infants How to sort things out? V.Gournay, FCPC, La Martinique, Nov 23,2015
 Late pulmonary hypertension in preterm infants How to sort things out? V.Gournay, FCPC, La Martinique, Nov 23,2015 Epidemiology Incidence of extreme prematurity (
Late pulmonary hypertension in preterm infants How to sort things out? V.Gournay, FCPC, La Martinique, Nov 23,2015 Epidemiology Incidence of extreme prematurity (
Keeping Patients Off the Vent: Bilevel, HFNC, Neither?
 Keeping Patients Off the Vent: Bilevel, HFNC, Neither? Robert Kempainen, MD Pulmonary and Critical Care Medicine Hennepin County Medical Center University of Minnesota School of Medicine Objectives Summarize
Keeping Patients Off the Vent: Bilevel, HFNC, Neither? Robert Kempainen, MD Pulmonary and Critical Care Medicine Hennepin County Medical Center University of Minnesota School of Medicine Objectives Summarize
Noah Hillman M.D. IPOKRaTES Conference Guadalajaira, Mexico August 23, 2018
 Postnatal Steroids Use for Bronchopulmonary Dysplasia in 2018 + = Noah Hillman M.D. IPOKRaTES Conference Guadalajaira, Mexico August 23, 2018 AAP Policy Statement - 2002 This statement is intended for
Postnatal Steroids Use for Bronchopulmonary Dysplasia in 2018 + = Noah Hillman M.D. IPOKRaTES Conference Guadalajaira, Mexico August 23, 2018 AAP Policy Statement - 2002 This statement is intended for
PEDIATRIC ACUTE ASTHMA SCORE (P.A.A.S.) GUIDELINES. >97% 94% to 96% 91%-93% <90% Moderate to severe expiratory wheeze
 GUIDELINES. >97% 94% to 96% 91%-93% <90% Moderate to severe expiratory wheeze") Inclusion: Children experiencing acute asthma exacerbation 24 months to 18 years of age with a diagnosis of asthma Patients with a previous history of asthma (Consider differential diagnosis for infants
Inclusion: Children experiencing acute asthma exacerbation 24 months to 18 years of age with a diagnosis of asthma Patients with a previous history of asthma (Consider differential diagnosis for infants
Disclosures. Learning Objectives. Mechanical Ventilation of Infants with Severe BPD: An Interdisciplinary Approach 3/10/2017
 Mechanical Ventilation of Infants with Severe BPD: An Interdisciplinary Approach Steven H. Abman, MD Professor, Department of Pediatrics Director, Pediatric Heart Lung Center University of Colorado School
Mechanical Ventilation of Infants with Severe BPD: An Interdisciplinary Approach Steven H. Abman, MD Professor, Department of Pediatrics Director, Pediatric Heart Lung Center University of Colorado School
Bronchiolitis in children
 Bronchiolitis in children NICE guideline Draft for consultation, November 2014 If you wish to comment on this version of the guideline, please be aware that all the supporting information and evidence
Bronchiolitis in children NICE guideline Draft for consultation, November 2014 If you wish to comment on this version of the guideline, please be aware that all the supporting information and evidence
Does proning patients with refractory hypoxaemia improve mortality?
 Does proning patients with refractory hypoxaemia improve mortality? Clinical problem and domain I selected this case because although this was the second patient we had proned in our unit within a week,
Does proning patients with refractory hypoxaemia improve mortality? Clinical problem and domain I selected this case because although this was the second patient we had proned in our unit within a week,
Supplementary Medications during asthma attack. Prof. Dr Finn Rasmussen PhD. DrMedSc. Near East University Hospital North Cyprus
 Supplementary Medications during asthma attack Prof. Dr Finn Rasmussen PhD. DrMedSc. Near East University Hospital North Cyprus Conflicts of Interest None Definition of Asthma Airway narrowing that is
Supplementary Medications during asthma attack Prof. Dr Finn Rasmussen PhD. DrMedSc. Near East University Hospital North Cyprus Conflicts of Interest None Definition of Asthma Airway narrowing that is
15 Years Of Clinical Trials In ARDS: What Progress Have We Made?
 15 Years Of Clinical Trials In ARDS: What Progress Have We Made? Niall D. Ferguson, MD, FRCPC, MSc Head of Critical Care Medicine University Health Network & Mount Sinai Hospital Senior Scientist, Toronto
15 Years Of Clinical Trials In ARDS: What Progress Have We Made? Niall D. Ferguson, MD, FRCPC, MSc Head of Critical Care Medicine University Health Network & Mount Sinai Hospital Senior Scientist, Toronto
Beyond the Golden Hour: Caring for the ICU Boarder
 Beyond the Golden Hour: Caring for the ICU Boarder Kami M. Hu, MD Dept. of Emergency Medicine Dept. of Pulmonology & Critical Care University of Maryland SOM I have no relevant financial relationships
Beyond the Golden Hour: Caring for the ICU Boarder Kami M. Hu, MD Dept. of Emergency Medicine Dept. of Pulmonology & Critical Care University of Maryland SOM I have no relevant financial relationships
Reverse (fluid) resuscitation Should we be doing it? NAHLA IRTIZA ISMAIL
 resuscitation Should we be doing it? NAHLA IRTIZA ISMAIL") Reverse (fluid) resuscitation Should we be doing it? NAHLA IRTIZA ISMAIL 65 Male, 60 kg D1 in ICU Admitted from OT intubated Diagnosis : septic shock secondary to necrotising fasciitis of the R lower limb
Reverse (fluid) resuscitation Should we be doing it? NAHLA IRTIZA ISMAIL 65 Male, 60 kg D1 in ICU Admitted from OT intubated Diagnosis : septic shock secondary to necrotising fasciitis of the R lower limb
1. What is delayed sequence intubation? Can it be used for severe Asthma exacerbation? 2. What about pregnancy and Asthma is so important?
 Chapter 073 Asthma Episode Overview 1. 10 different causes of a wheeze. 2. List 8 risk factors for death from asthma 3. List 6 objective findings of severe asthma 4. 10 therapies for an acute severe asthma
Chapter 073 Asthma Episode Overview 1. 10 different causes of a wheeze. 2. List 8 risk factors for death from asthma 3. List 6 objective findings of severe asthma 4. 10 therapies for an acute severe asthma
Facilitating EndotracheaL Intubation by Laryngoscopy technique and Apneic Oxygenation Within the Intensive Care Unit (FELLOW)
") Facilitating EndotracheaL Intubation by Laryngoscopy technique and Apneic Oxygenation Within the Intensive Data Analysis Plan: Apneic Oxygenation vs. No Apneic Oxygenation Background Critically ill patients
Facilitating EndotracheaL Intubation by Laryngoscopy technique and Apneic Oxygenation Within the Intensive Data Analysis Plan: Apneic Oxygenation vs. No Apneic Oxygenation Background Critically ill patients
Neuromuscular Blockade in ARDS
 Neuromuscular Blockade in ARDS Maureen O. Meade, MD, FRCPC Critical care consultant, Hamilton Health Sciences Professor of Medicine, McMaster University www.oscillatetrial.com Disclosures None Possible
Neuromuscular Blockade in ARDS Maureen O. Meade, MD, FRCPC Critical care consultant, Hamilton Health Sciences Professor of Medicine, McMaster University www.oscillatetrial.com Disclosures None Possible
ARDS and Ventilators PG26 Update in Surgical Critical Care October 9, 2013
 ARDS and Ventilators PG26 Update in Surgical Critical Care October 9, 2013 Pauline K. Park MD, FACS, FCCM University of Michigan School of Medicine Ann Arbor, MI OVERVIEW New Berlin definition of ARDS
ARDS and Ventilators PG26 Update in Surgical Critical Care October 9, 2013 Pauline K. Park MD, FACS, FCCM University of Michigan School of Medicine Ann Arbor, MI OVERVIEW New Berlin definition of ARDS
Post Arrest Ventilation/Oxygenation Management
 Post Arrest Ventilation/Oxygenation Management Richard Branson MSc RRT Professor of Surgery University of Cincinnati Editor-In-Chief Respiratory Care 0 Presenter Disclosure Information Richard Branson
Post Arrest Ventilation/Oxygenation Management Richard Branson MSc RRT Professor of Surgery University of Cincinnati Editor-In-Chief Respiratory Care 0 Presenter Disclosure Information Richard Branson
OSCAR & OSCILLATE. & the Future of High Frequency Oscillatory Ventilation (HFOV)
") & & the Future of High Frequency Oscillatory Ventilation (HFOV) www.philippelefevre.com What do we know already? Sud S et al. BMJ 2010 & Multi-centre randomised controlled trials of HFOV verses current
& & the Future of High Frequency Oscillatory Ventilation (HFOV) www.philippelefevre.com What do we know already? Sud S et al. BMJ 2010 & Multi-centre randomised controlled trials of HFOV verses current
Protein Supplementation in the Pediatric Intensive Care Unit. Jan Hau Lee, MBBS, MRCPCH, MCI Children s Intensive Care Unit 28 th July 2017
 Protein Supplementation in the Pediatric Intensive Care Unit Jan Hau Lee, MBBS, MRCPCH, MCI Children s Intensive Care Unit 28 th July 2017 1 Objectives Basis for protein supplementation Challenges in monitoring
Protein Supplementation in the Pediatric Intensive Care Unit Jan Hau Lee, MBBS, MRCPCH, MCI Children s Intensive Care Unit 28 th July 2017 1 Objectives Basis for protein supplementation Challenges in monitoring
Management of acute asthma in children in emergency department. Moderate asthma
 152 Moderate asthma SpO2 92% No clinical features of severe asthma NB: If a patient has signs and symptoms across categories, always treat according to their most severe features agonist 2-10 puffs via
152 Moderate asthma SpO2 92% No clinical features of severe asthma NB: If a patient has signs and symptoms across categories, always treat according to their most severe features agonist 2-10 puffs via
AEROSURF Phase 2 Program Update Investor Conference Call
 AEROSURF Phase 2 Program Update Investor Conference Call November 12, 2015 Forward Looking Statement To the extent that statements in this presentation are not strictly historical, including statements
AEROSURF Phase 2 Program Update Investor Conference Call November 12, 2015 Forward Looking Statement To the extent that statements in this presentation are not strictly historical, including statements
Asthma Care in the Emergency Department Clinical Practice Guideline
 Asthma Care in the Emergency Department Clinical Practice Guideline Inclusion: 1) Children 2 years of age or older with a prior history of wheezing, and 2) Children less than 2 years of age with likely
Asthma Care in the Emergency Department Clinical Practice Guideline Inclusion: 1) Children 2 years of age or older with a prior history of wheezing, and 2) Children less than 2 years of age with likely
1
 1 2 3 RIFAI 5 6 Dublin cohort, retrospective review. Milrinone was commenced at an initial dose of 0.50 μg/kg/minute up to 0.75 μg/kg/minute and was continued depending on clinical response. No loading
1 2 3 RIFAI 5 6 Dublin cohort, retrospective review. Milrinone was commenced at an initial dose of 0.50 μg/kg/minute up to 0.75 μg/kg/minute and was continued depending on clinical response. No loading
Back to the Future: Updated Guidelines for Evaluation and Management of Adrenal Insufficiency in the Critically Ill
 Back to the Future: Updated Guidelines for Evaluation and Management of Adrenal Insufficiency in the Critically Ill Joe Palumbo PGY-2 Critical Care Pharmacy Resident Buffalo General Medical Center Disclosures
Back to the Future: Updated Guidelines for Evaluation and Management of Adrenal Insufficiency in the Critically Ill Joe Palumbo PGY-2 Critical Care Pharmacy Resident Buffalo General Medical Center Disclosures
Protocol Update 2019
 Protocol Update 2019 There have been several questions revolving around protocol updates and how they are to be conducted. As many of you are aware there is a protocol submission process in the appendix
Protocol Update 2019 There have been several questions revolving around protocol updates and how they are to be conducted. As many of you are aware there is a protocol submission process in the appendix
Is There a Treatment for BPD?
 Is There a Treatment for BPD? Amir Kugelman, Pediatric Pulmonary Unit and Department of Neonatology Bnai Zion Medical Center, Rappaport Faculty of Medicine Haifa, Israel Conflict of Interest Our study
Is There a Treatment for BPD? Amir Kugelman, Pediatric Pulmonary Unit and Department of Neonatology Bnai Zion Medical Center, Rappaport Faculty of Medicine Haifa, Israel Conflict of Interest Our study
ARDS and treatment strategies
 ARDS and treatment strategies Geoff Bellingan Medical Director University College Hospital ARDS: Definitions History of predisposing condition Refractory hypoxaemia of acute onset PaO 2 /FiO 2 ratio:
ARDS and treatment strategies Geoff Bellingan Medical Director University College Hospital ARDS: Definitions History of predisposing condition Refractory hypoxaemia of acute onset PaO 2 /FiO 2 ratio:
Acute NIV in COPD and what happens next. Dr Rachael Evans PhD Associate Professor, Respiratory Medicine, Glenfield Hospital
 Acute NIV in COPD and what happens next Dr Rachael Evans PhD Associate Professor, Respiratory Medicine, Glenfield Hospital Content Scenarios Evidence based medicine for the first 24 hrs Who should we refer
Acute NIV in COPD and what happens next Dr Rachael Evans PhD Associate Professor, Respiratory Medicine, Glenfield Hospital Content Scenarios Evidence based medicine for the first 24 hrs Who should we refer
Respiratory Medicine. Some pet peeves and other random topics. Kyle Perrin
 Respiratory Medicine Some pet peeves and other random topics Kyle Perrin Overview 1. Acute asthma Severity assessment and management 2. Acute COPD NIV and other management 3. Respiratory problems in the
Respiratory Medicine Some pet peeves and other random topics Kyle Perrin Overview 1. Acute asthma Severity assessment and management 2. Acute COPD NIV and other management 3. Respiratory problems in the
Caring For the ICU Boarder. Kami M. Hu, MD Depts of Emergency & Internal Medicine University of Maryland SOM
 Caring For the ICU Boarder Kami M. Hu, MD Depts of Emergency & Internal Medicine University of Maryland SOM I have no relevant financial relationships with the manufacturer(s) of any commercial product(s)and/or
Caring For the ICU Boarder Kami M. Hu, MD Depts of Emergency & Internal Medicine University of Maryland SOM I have no relevant financial relationships with the manufacturer(s) of any commercial product(s)and/or
Respiratory insufficiency in bariatric patients
 Respiratory insufficiency in bariatric patients Special considerations or just more of the same? Weaning and rehabilation conference 6th November 2015 Definition of obesity Underweight BMI< 18 Normal weight
Respiratory insufficiency in bariatric patients Special considerations or just more of the same? Weaning and rehabilation conference 6th November 2015 Definition of obesity Underweight BMI< 18 Normal weight
Chronic Lung Disease Of Prematurity. Dr Jo Harrison
 Chronic Lung Disease Of Prematurity Dr Jo Harrison 9.9.14 Chronic Neonatal Lung Disease Bronchopulmonary dysplasia (BPD) first described in 1967 by Northway Defined as O 2 dependence at 28 days post birth
Chronic Lung Disease Of Prematurity Dr Jo Harrison 9.9.14 Chronic Neonatal Lung Disease Bronchopulmonary dysplasia (BPD) first described in 1967 by Northway Defined as O 2 dependence at 28 days post birth
Part 2 of park s Ventilator and ARDS slides for syllabus
 Part 2 of park s Ventilator and ARDS slides for syllabus Early Neuromuscular Blockade Question 4 The early use of cis-atracurium in severe ARDS is: A. Contraindicated in patients with diabetes B. Associated
Part 2 of park s Ventilator and ARDS slides for syllabus Early Neuromuscular Blockade Question 4 The early use of cis-atracurium in severe ARDS is: A. Contraindicated in patients with diabetes B. Associated
ARDS: The Evidence. Topics. New definition Breaths: Little or Big? Wet or Dry? Moving or Still? Upside down or Right side up?
 ARDS: The Evidence Todd M Bull MD Professor of Medicine Division of Pulmonary Sciences and Critical Care Division of Cardiology Director Pulmonary Vascular Disease Center Director Center for Lungs and
ARDS: The Evidence Todd M Bull MD Professor of Medicine Division of Pulmonary Sciences and Critical Care Division of Cardiology Director Pulmonary Vascular Disease Center Director Center for Lungs and
ECMO for Severe Hypoxemic Respiratory Failure: Pro-Con Debate. Carolyn Calfee, MD MAS Mark Eisner, MD MPH
 ECMO for Severe Hypoxemic Respiratory Failure: Pro-Con Debate Carolyn Calfee, MD MAS Mark Eisner, MD MPH June 3, 2010 Case Presentation Setting: Community hospital, November 2009 29 year old woman with
ECMO for Severe Hypoxemic Respiratory Failure: Pro-Con Debate Carolyn Calfee, MD MAS Mark Eisner, MD MPH June 3, 2010 Case Presentation Setting: Community hospital, November 2009 29 year old woman with
DAILY SCREENING FORM
 DAILY SCREENING FORM Patient s initials: Date of admission: Time of admission: Gender: M F Year of Birth: Type of admission: Medical/Surgical/Postoperative (elective) Days Date Mechanical ventilation Lung
DAILY SCREENING FORM Patient s initials: Date of admission: Time of admission: Gender: M F Year of Birth: Type of admission: Medical/Surgical/Postoperative (elective) Days Date Mechanical ventilation Lung
ACUTE RESPIRATORY DISTRESS SYNDROME
 ACUTE RESPIRATORY DISTRESS SYNDROME Angel Coz MD, FCCP, DCE Assistant Professor of Medicine UCSF Fresno November 4, 2017 No disclosures OBJECTIVES Identify current trends and risk factors of ARDS Describe
ACUTE RESPIRATORY DISTRESS SYNDROME Angel Coz MD, FCCP, DCE Assistant Professor of Medicine UCSF Fresno November 4, 2017 No disclosures OBJECTIVES Identify current trends and risk factors of ARDS Describe
Staging Sepsis for the Emergency Department: Physician
 Staging Sepsis for the Emergency Department: Physician Sepsis Continuum 1 Sepsis Continuum SIRS = 2 or more clinical criteria, resulting in Systemic Inflammatory Response Syndrome Sepsis = SIRS + proven/suspected
Staging Sepsis for the Emergency Department: Physician Sepsis Continuum 1 Sepsis Continuum SIRS = 2 or more clinical criteria, resulting in Systemic Inflammatory Response Syndrome Sepsis = SIRS + proven/suspected
Analyzing Lung protective ventilation F Javier Belda MD, PhD Sº de Anestesiología y Reanimación. Hospital Clinico Universitario Valencia (Spain)
") Analyzing Lung protective ventilation F Javier Belda MD, PhD Sº de Anestesiología y Reanimación Hospital Clinico Universitario Valencia (Spain) ALI/ARDS Report of the American-European consensus conference
Analyzing Lung protective ventilation F Javier Belda MD, PhD Sº de Anestesiología y Reanimación Hospital Clinico Universitario Valencia (Spain) ALI/ARDS Report of the American-European consensus conference
PEEP recruitment maneuver
 Robert M. Rodriguez, MD FAAEM Clinical Professor of Medicine and Emergency Medicine, UCSF Case 1: 40 yo Male restrained driver high speed MVA P 140, RR 40 labored, BP 100/70, O 2 sat 70 Chest wheeze, crackles
Robert M. Rodriguez, MD FAAEM Clinical Professor of Medicine and Emergency Medicine, UCSF Case 1: 40 yo Male restrained driver high speed MVA P 140, RR 40 labored, BP 100/70, O 2 sat 70 Chest wheeze, crackles
Respiratory infection what works Professor Terence Stephenson President Royal College of Paediatrics & Child Health
 Respiratory infection what works Professor Terence Stephenson President Royal College of Paediatrics & Child Health Nuffield Professor, Institute of Child Health, University College London & Great Ormond
Respiratory infection what works Professor Terence Stephenson President Royal College of Paediatrics & Child Health Nuffield Professor, Institute of Child Health, University College London & Great Ormond
In-hospital Care of the Post-Cardiac Arrest Patient. David A. Pearson, MD, FACEP, FAAEM Associate Program Director Department of Emergency Medicine
 In-hospital Care of the Post-Cardiac Arrest Patient David A. Pearson, MD, FACEP, FAAEM Associate Program Director Department of Emergency Medicine Disclosures I have no financial interest, arrangement,
In-hospital Care of the Post-Cardiac Arrest Patient David A. Pearson, MD, FACEP, FAAEM Associate Program Director Department of Emergency Medicine Disclosures I have no financial interest, arrangement,
Non-invasive Positive Pressure Mechanical Ventilation: NIPPV: CPAP BPAP IPAP EPAP. My Real Goals. What s new in 2018? OMG PAP?
 Non-invasive Positive Pressure Mechanical Ventilation: What s new in 2018? Geoffrey R. Connors, MD, FACP Associate Professor of Medicine University of Colorado School of Medicine Division of Pulmonary
Non-invasive Positive Pressure Mechanical Ventilation: What s new in 2018? Geoffrey R. Connors, MD, FACP Associate Professor of Medicine University of Colorado School of Medicine Division of Pulmonary
Concerns and Controversial Issues in NPPV. Concerns and Controversial Issues in Noninvasive Positive Pressure Ventilation
 : Common Therapy in Daily Practice Concerns and Controversial Issues in Noninvasive Positive Pressure Ventilation Rongchang Chen Guangzhou Institute of Respiratory Disease as the first choice of mechanical
: Common Therapy in Daily Practice Concerns and Controversial Issues in Noninvasive Positive Pressure Ventilation Rongchang Chen Guangzhou Institute of Respiratory Disease as the first choice of mechanical
EFFECT OF EARLY VASOPRESSIN VS NOREPINEPHRINE ON KIDNEY FAILURE IN PATIENTS WITH SEPTIC SHOCK. Alexandria Rydz
 EFFECT OF EARLY VASOPRESSIN VS NOREPINEPHRINE ON KIDNEY FAILURE IN PATIENTS WITH SEPTIC SHOCK Alexandria Rydz BACKGROUND- SEPSIS Sepsis is defined as life-threatening organ dysfunction caused by a dysregulated
EFFECT OF EARLY VASOPRESSIN VS NOREPINEPHRINE ON KIDNEY FAILURE IN PATIENTS WITH SEPTIC SHOCK Alexandria Rydz BACKGROUND- SEPSIS Sepsis is defined as life-threatening organ dysfunction caused by a dysregulated
Wet Lungs Dry lungs Impact on Outcome in ARDS. Charlie Phillips MD Division of PCCM OHSU 2009
 Wet Lungs Dry lungs Impact on Outcome in ARDS Charlie Phillips MD Division of PCCM OHSU 2009 Today s talk Pathophysiology of ARDS The case for dry Targeting EVLW Disclosures Advisor for Pulsion Medical
Wet Lungs Dry lungs Impact on Outcome in ARDS Charlie Phillips MD Division of PCCM OHSU 2009 Today s talk Pathophysiology of ARDS The case for dry Targeting EVLW Disclosures Advisor for Pulsion Medical
Bronchiolitis & Hypertonic Saline
 Bronchiolitis & Hypertonic Saline Andrea Scheid MD FAAP Director, Pediatric Hospitalist Service & Medical Unit Director, Pediatric Floor Beaumont Children s Hospital, Royal Oak Assistant Professor, Oakland
Bronchiolitis & Hypertonic Saline Andrea Scheid MD FAAP Director, Pediatric Hospitalist Service & Medical Unit Director, Pediatric Floor Beaumont Children s Hospital, Royal Oak Assistant Professor, Oakland
Approach to Severe Sepsis. Jan Hau Lee, MBBS, MRCPCH. MCI Children s Intensive Care Unit KK Women s and Children's Hospital, Singapore
 Approach to Severe Sepsis Jan Hau Lee, MBBS, MRCPCH. MCI Children s Intensive Care Unit KK Women s and Children's Hospital, Singapore 1 2 No conflict of interest Overview Epidemiology of Pediatric Severe
Approach to Severe Sepsis Jan Hau Lee, MBBS, MRCPCH. MCI Children s Intensive Care Unit KK Women s and Children's Hospital, Singapore 1 2 No conflict of interest Overview Epidemiology of Pediatric Severe
Surviving Sepsis Campaign. Guidelines for Management of Severe Sepsis/Septic Shock. An Overview
 Surviving Sepsis Campaign Guidelines for Management of Severe Sepsis/Septic Shock An Overview Mechanical Ventilation of Sepsis-Induced ALI/ARDS ARDSnet Mechanical Ventilation Protocol Results: Mortality
Surviving Sepsis Campaign Guidelines for Management of Severe Sepsis/Septic Shock An Overview Mechanical Ventilation of Sepsis-Induced ALI/ARDS ARDSnet Mechanical Ventilation Protocol Results: Mortality
Noninvasive Ventilation: Non-COPD Applications
 Noninvasive Ventilation: Non-COPD Applications NONINVASIVE MECHANICAL VENTILATION Why Noninvasive Ventilation? Avoids upper A respiratory airway trauma system lacerations, protective hemorrhage strategy
Noninvasive Ventilation: Non-COPD Applications NONINVASIVE MECHANICAL VENTILATION Why Noninvasive Ventilation? Avoids upper A respiratory airway trauma system lacerations, protective hemorrhage strategy
Objectives. Case Presentation. Respiratory Emergencies
 Respiratory Emergencies Objectives Describe how to assess airway and breathing, including interpreting information from the PAT and ABCDEs. Differentiate between respiratory distress, respiratory failure,
Respiratory Emergencies Objectives Describe how to assess airway and breathing, including interpreting information from the PAT and ABCDEs. Differentiate between respiratory distress, respiratory failure,
IDPH ESF-8 Plan: Pediatric and Neonatal Surge Annex Sample Pediatric Admission Orders 2015
 Purpose: To provide guidance to practitioners caring for pediatric patients who need inpatient hospital care during a disaster. Disclaimer: This guideline is not meant to be all inclusive, replace an existing
Purpose: To provide guidance to practitioners caring for pediatric patients who need inpatient hospital care during a disaster. Disclaimer: This guideline is not meant to be all inclusive, replace an existing
IV fluid administration in sepsis. Dr David Inwald Consultant in PICU St Mary s Hospital, London CATS, London
 IV fluid administration in sepsis Dr David Inwald Consultant in PICU St Mary s Hospital, London CATS, London The talk What is septic shock? What are the recommendations? What is the evidence? Do we follow
IV fluid administration in sepsis Dr David Inwald Consultant in PICU St Mary s Hospital, London CATS, London The talk What is septic shock? What are the recommendations? What is the evidence? Do we follow
Guidelines for the Provision and Assessment of Nutrition Support Therapy in the Pediatric Critically Ill Patient: ASPEN-SCCM 2017
 Number of Patients Guidelines for the Provision and Assessment of Nutrition Support Therapy in the Pediatric Critically Ill Patient: ASPEN-SCCM 2017 Jorge A. Coss-Bu, MD Associate Professor of Pediatrics
Number of Patients Guidelines for the Provision and Assessment of Nutrition Support Therapy in the Pediatric Critically Ill Patient: ASPEN-SCCM 2017 Jorge A. Coss-Bu, MD Associate Professor of Pediatrics
Oxygen:..Nothing is without poison.. the poison is in the dose..
 Interdepartmental Division of Critical Care Medicine Mount Sinai Hospital/University Health Network University of Toronto Toronto, Canada Oxygen:..Nothing is without poison.. the poison is in the dose..
Interdepartmental Division of Critical Care Medicine Mount Sinai Hospital/University Health Network University of Toronto Toronto, Canada Oxygen:..Nothing is without poison.. the poison is in the dose..
AT TRIAGE. Alberta Acute Childhood Asthma Pathway: Evidence based* recommendations For Emergency / Urgent Care
 1 1 Should the child be placed into the Pathway? Asthma Clinical Score (PRAM) Inclusion Children 1 year and 18 years of age who present with wheezing and respiratory distress, and have been diagnosed by
1 1 Should the child be placed into the Pathway? Asthma Clinical Score (PRAM) Inclusion Children 1 year and 18 years of age who present with wheezing and respiratory distress, and have been diagnosed by