DSM-5 Has Arrived. page 5 in syllabus. David J. Kupfer, MD
|
|
|
- Ashlee Davidson
- 6 years ago
- Views:
Transcription






1 DSM-5 Has Arrived page 5 in syllabus David J. Kupfer, MD Professor, Department of Psychiatry Professor of Neuroscience and Clinical and Translational Science, Center for Neuroscience, University of Pittsburgh School of Medicine Chair, DSM-5 Task Force Sponsored by the Neuroscience Education Institute Additionally sponsored by Fairleigh Dickinson University School of Psychology This activity is supported solely by the sponsor, Neuroscience Education Institute, and participant registration fees. Copyright 2013 Neuroscience Education Institute. All rights reserved.
2 Individual Disclosure Statement Faculty Author / Presenter David J. Kupfer, MD, is a professor in the department of psychiatry and a professor of neuroscience and clinical and translational science in the center for neuroscience at the University of Pittsburgh School of Medicine, PA. Consultant/Advisor: Servier (spouse) Dr. Kupfer reports receiving consulting fees from the American Psychiatric Association for serving as the Chair of the DSM-5 Task Force. Copyright 2013 Neuroscience Education Institute. All rights reserved.
3 Learning Objectives Describe the major changes made to the DSM between DSM-IV and DSM-5, including manualwide changes and diagnosis-specific changes Explain the rationale for the changes to the chapter structure in DSM-5 Explain how changes made in DSM-5 might affect clinical practice Explain how changes made in DSM-5 might affect research outcomes Copyright 2013 Neuroscience Education Institute. All rights reserved.
4 Pretest Question 1 In DSM-5: 1. The DSM-IV multiaxial system was fully retained 2. The DSM-IV multiaxial system was modified 3. The DSM-IV multiaxial system was replaced with a new multiaxial system 4. The multiaxial system was removed
5 Pretest Question 2 The chapter organization of DSM-5 1. Retains that of DSM-IV 2. Replaces that of DSM-IV with an alphabetical one 3. Replaces that of DSM-IV with a developmentallyinformed one 4. Was entirely determined by the World Health Organization
6 DSM-5 The Future Arrived David J. Kupfer, MD Emily A. Kuhl, PhD Darrel A. Regier, MD, MPH JAMA 2013;309:
7 Strategies for Improving DSM Incorporate research into the revision and evolution of the classification Move beyond a process of clinical consensus and build diagnoses on a foundation of empirical findings from scientific disciplines Seek multidisciplinary, international, scientific participation in the task of planning the DSM-5 revision
8 APA/WHO/NIH Diagnosis Research Planning Conferences: Participant Distribution Eastern Mediterranean, 5 U.S.A., 194 Latin America, 16 Europe, 119 Canada, Participants - 39 Countries - 16 Developing Nations - 51% Non-US Participants - 10% Developing Nation Paticipants Africa, 9 South Asia, 10 Western Pacific, 32 Africa Kenya, 2 Nigeria, 3 South Africa, 4 Latin Am erica Argentina, 2 Brazil, 4 Chile, 3 Mexico, 5 Puerto Rico, 2 Eastern Mediterranean Bahrain, 1 Israel, 3 Lebanon, 1 Europe Belarus, 1 Belgium, 2 Denmark, 4 Estonia, 1 France, 3 Germany, 11 Europe (Cont) Greece, 1 Hungary, 1 Italy, 5 Luxembourg, 1 Netherlands, 12 Norw ay, 2 Russia, 4 Spain, 5 Sw eden, 4 Sw itzerland, 21 UK, 41 South Asia India, 5 Pakistan, 2 Sri Lanka, 1 Thailand, 2 Western Pacific Australia, 9 China, 9 Japan, 8 Korea, 3 New Zealand, 3
9 DSM-5 Conference Output 13 conferences ( ) 10 monographs published Dimensional Models of Personality Disorders Diagnostic Issues in Substance Use Disorders Diagnostic Issues in Dementia Dimensional Approaches in Diagnostic Classification Stress-Induced and Fear Circuitry Disorders Somatic Presentations of Mental Disorders Deconstructing Psychosis Depression and GAD Obsessive-Compulsive Behavior Spectrum Disorders Public Health Aspects of Psychiatric Diagnosis More than 200 journal articles published
10
11 DSM-5 Work Groups and Chairs ADHD and Disruptive Behavior Disorders (David Shaffer, MD) Anxiety, Obsessive-Compulsive Spectrum, Posttraumatic, and Dissociative Disorders (Katharine Phillips, MD) Disorders in Childhood and Adolescence (Daniel Pine, MD) Eating Disorders (Timothy Walsh, MD) Mood Disorders (Jan Fawcett, MD) Neurocognitive Disorders (Dilip Jeste, MD) Neurodevelopmental Disorders (Susan Swedo, MD) Personality Disorders (Andrew Skodol, MD) Psychotic Disorders (William Carpenter, MD) Sexual and Gender Identity Disorders (Kenneth Zucker, PhD) Sleep Wake Disorders (Charles Reynolds, MD) Somatic Distress Disorders (Joel Dimsdale, MD) Substance-Related Disorders (Charles O'Brien, MD, PhD)
12 DSM-5 Revisions: Rationales
13 DSM-5 Revisions: Rationales DSM-IV's organizational structure failed to reflect shared features or symptoms of related disorders and diagnostic groups (e.g., psychotic disorders and bipolar disorders; internalizing (depressive, anxiety, somatic) and externalizing (impulse control, conduct, substance use) disorders) DSM-5 restructuring better reflects these interrelationships within and across diagnostic chapters
14 DSM-5 Revisions: Rationales DSM-IV does not adequately address the lifespan perspective, including variations in symptom presentations across the developmental trajectory, or cultural perspectives DSM-5's chapter structure, criteria revisions, and text outline actively address age and development as part of diagnosis and classification Culture is discussed more explicitly to bring greater attention to cultural variations in symptom presentations
15 DSM-5 Revisions: Rationales DSM-5 represents an opportunity to better integrate neuroscience and the wealth of findings from neuroimaging, genetics, cognitive research, etc. that have emerged over the past several decades, all of which are vital to diagnosis and treatment development DSM-5 will be more amenable to updates in psychiatry and neuroscience, making it a living document and less susceptible to becoming outdated
16 DSM-5 Revisions: Rationales The multiaxial system in DSM-IV is not required to make a mental disorder diagnosis and has not been universally used DSM-5 has moved to a nonaxial documentation of diagnosis (formerly Axes I, II, and III), with separate notations for important psychosocial and contextual factors (formerly Axis IV) and disability (formerly Axis V) This approach is consistent with established WHO and ICD guidance to consider the individual's functional status separately from his or her diagnosis or symptom status
17 DSM-5 Revisions: Highlights of Changes

18 DSM-5 Structure Section I: DSM-5 Basics Section II: Essential Elements: Diagnostic Criteria and Codes Section III: Emerging Measures and Models Appendix Index
19 Section I Brief DSM-5 developmental history Guidance on use of the manual Definition of a mental disorder Cautionary forensic statement Brief DSM-5 classification summary
20 Use of the Manual Approach to Clinical Case Formulation Definition of a Mental Disorder Criterion for Clinical Significance Elements of a Diagnosis Diagnostic Criteria and Descriptors Subtypes and Specifiers

21 Section II Revised DSM-5 Chapter Structure
22 Clustering of Chapters Neurodevelopmental Disorders Emotional (Internalizing) Disorders Somatic Disorders Externalizing Disorders Neurocognitive Disorders Personality Disorders

23 Section II: Chapter Structure A. Neurodevelopmental Disorders B. Schizophrenia Spectrum and Other Psychotic Disorders C. Bipolar and Related Disorders D. Depressive Disorders E. Anxiety Disorders F. Obsessive-Compulsive and Related Disorders G. Trauma- and Stress-Related Disorders H. Dissociative Disorders
24 Section II: Chapter Structure I. Somatic Symptom and Related Disorders J. Feeding and Eating Disorders K. Elimination Disorders L. Sleep Wake Disorders M. Sexual Dysfunction N. Gender Dysphoria

25 Section II: Chapter Structure O. Disruptive, Impulse Control, and Conduct Disorders P. Substance-Related and Addictive Disorders Q. Neurocognitive Disorders R. Personality Disorders S. Paraphilic Disorders T. Other Disorders U. Medication-Induced Movement Disorders and Other Adverse Effects of Medication V. Other Conditions That May Be a Focus of Clinical Attention
")
 conditions are counted")
26 Changes in Specific DSM Disorder Numbers: Combination of New, Eliminated, and Combined Disorders (Net Difference = -15) DSM-IV DSM-5 Specific Mental Disorders* *NOS (DSM-IV) and Other Specified/Unspecified (DSM-5) conditions are counted separately
 4. Hoarding Disorder 5. Excoriation (Skin Picking) Disorder 6. Disinhibited Social Engagement Disorder (split from Reactive Attachment Disorder) 7.")
27 New and Eliminated Disorders in DSM-5 (Net Difference = +13) New Disorders 1. Social (Pragmatic) Communication Disorder 2. Disruptive Mood Dysregulation Disorder 3. Premenstrual Dysphoric Disorder (DSM IV appendix) 4. Hoarding Disorder 5. Excoriation (Skin Picking) Disorder 6. Disinhibited Social Engagement Disorder (split from Reactive Attachment Disorder) 7. Binge Eating Disorder (DSM IV appendix) 8. Central Sleep Apnea (split from Breathing-Related Sleep Disorder) 9. Sleep-Related Hypoventilation (split from Breathing-Related Sleep Disorder) 10. Rapid Eye Movement Sleep Behavior Disorder (Parasomnia NOS) 11. Restless Legs Syndrome (Dyssomnia NOS) 12. Caffeine Withdrawal (DSM IV Appendix) 13. Cannabis Withdrawal 14. Major Neurocognitive Disorder With Lewy Body Disease (Dementia Due to Other Medical Conditions) 15. Mild Neurocognitive Disorder (DSM IV Appendix) Eliminated Disorders 1. Sexual Aversion Disorder 2. Polysubstance-Related Disorder
 3.")
 6. Dissociative Amnesia (Dissociative Fugue and Dissociative Amnesia) 7.")
28 Combined Specific Disorders in DSM-5 (Net Difference = -28) 1. Language Disorder (Expressive Language Disorder and Mixed Receptive-Expressive Language Disorder) 2. Autism Spectrum Disorder (Autistic Disorder, Asperger's Disorder, Childhood Disintegrative Disorder, and Rett's Disorder; PDD-NOS is in the NOS count) 3. Specific Learning Disorder (Reading Disorder, Math Disorder, and Disorder of Written Expression) 4. Delusional Disorder (Shared Psychotic Disorder and Delusional Disorder) 5. Panic Disorder (Panic Disorder Without Agoraphobia and Panic Disorder With Agoraphobia) 6. Dissociative Amnesia (Dissociative Fugue and Dissociative Amnesia) 7. Somatic Symptom Disorder (Somatization Disorder, Undifferentiated Somatoform Disorder, and Pain Disorder) 8. Insomnia Disorder (Primary Insomnia and Insomnia Related to Another Mental Disorder) 9. Hypersomnolence Disorder (Primary Hypersomnia and Hypersomnia Related to Another Mental Disorder) 10. Non-rapid Eye Movement Sleep Arousal Disorders (Sleepwalking Disorder and Sleep Terror Disorder)
 13. Cannabis Use Disorder (Cannabis Abuse and Cannabis Dependence) 14.")
29 Combined Specific Disorders in DSM-5 (cont.) (Net Difference = -28) 11. Genito Pelvic Pain/Penetration Disorder (Vaginismus and Dyspareunia) 12. Alcohol Use Disorder (Alcohol Abuse and Alcohol Dependence) 13. Cannabis Use Disorder (Cannabis Abuse and Cannabis Dependence) 14. Phencyclidine Use Disorder (Phencyclidine Abuse and Phencyclidine Dependence) 15. Other Hallucinogen Use Disorder (Hallucinogen Abuse and Hallucinogen Dependence) 16. Inhalant Use Disorder (Inhalant Abuse and Inhalant Dependence) 17. Opioid Use Disorder (Opioid Abuse and Opioid Dependence) 18. Sedative, Hypnotic, or Anxiolytic Use Disorder (Sedative, Hypnotic, or Anxiolytic Abuse and Sedative, Hypnotic, or Anxiolytic Dependence) 19. Stimulant Use Disorder (Amphetamine Abuse, Amphetamine Dependence, Cocaine Abuse, and Cocaine Dependence) 20. Stimulant Intoxication (Amphetamine Intoxication and Cocaine Intoxication) 21. Stimulant Withdrawal (Amphetamine Withdrawal and Cocaine Withdrawal) 22. Substance/Medication-Induced Disorders (aggregate of Mood (+1), Anxiety (+1), and Neurocognitive (-3) Disorders)
30 Changes From NOS to Other Specified/Unspecified (Net Difference = +24) DSM-IV DSM-5 NOS (DSM-IV) and Other Specified/Unspecified (DSM-5) Other Specified/Unspecified Disorders in DSM-5 replaced the Not Otherwise Specified (NOS) conditions in DSM-IV to maintain greater concordance with the official International Classification of Diseases (ICD) coding system. This statistical accounting change does not signify any new specific mental disorders.
31 Highlights of Specific Disorder Revisions and Rationales
32 Autism Spectrum Disorder (ASD) (Neurodevelopmental Disorders) ASD replaces DSM-IV's autistic disorder, Asperger's disorder, childhood disintegration disorder, and pervasive developmental disorder NOS Rationale: Clinicians had been applying the DSM-IV criteria for these disorders inconsistently and incorrectly. Subsequently, reliability data to support their continued separation was very poor. Specifiers can be used to describe variants of ASD (e.g., the former diagnosis of Asperger's can now be diagnosed as autism spectrum disorder, without intellectual impairment and without structural language impairment).
33 Autism Spectrum Disorder The criteria from DSM-IV's autistic disorder, Asperger's disorder, childhood disintegrative disorder, and pervasive developmental disorder NOS have been combined into a single diagnosis of autism spectrum disorder The aim is to more accurately characterize children with social communication and interaction deficits as well as restrictive, repetitive behaviors, activities, or interests
34 Autism Spectrum Disorder (2) This revision is not expected to significantly alter prevalence rates The criteria were developed with enough sensitivity and specificity that most children (91%) previously diagnosed with a pervasive developmental disorder under DSM-IV will meet criteria for autism spectrum disorder, allowing them to retain a diagnosis and continue receiving treatment and educational services
35 Intellectual Disability (Intellectual Developmental Disorder) Mental retardation was renamed intellectual disability (intellectual developmental disorder) Rationale: The term intellectual disability reflects the wording adopted into US law in 2010 (Rosa's Law), in use in professional journals, and endorsed by certain patient advocacy groups. The term intellectual developmental disorder is consistent with the language proposed for ICD-11. Greater emphasis on adaptive functioning deficits rather than IQ scores alone Rationale: Standardized IQ test scores were overemphasized as the determining factor of abilities in DSM-IV. Consideration of functioning provides a more comprehensive assessment of the individual.
36 Attention-Deficit/Hyperactivity Disorder Age of onset was raised from 7 to 12 years Rationale: Numerous large-scale studies indicate that in many cases, onset is not identified until after age 7, when a child is challenged by school requirements. Recall of onset is more accurate at 12 years. The symptom threshold for adults aged 17 years and older was reduced to 5 Rationale: The reduction in symptom threshold was for adults only and was made based on longitudinal studies showing that patients tend to have fewer symptoms in adulthood than in childhood. This should result in a minimal increase in the prevalence of adult ADHD.
37 Specific Learning Disorder Now presented as a single disorder with coded specifiers for specific deficits in reading, writing, and mathematics Rationale: There was widespread concern among clinicians and researchers that clinical reality did not support DSM-IV's 3 independent learning disorders. This is particularly important given that most children with specific learning disorder manifest deficits in more than 1 area. By reclassifying these as a single disorder, separate specifiers can be used to code the level of deficits present in each of the 3 areas for any person.
38 Schizophrenia (Schizophrenia Spectrum and Other Psychotic Disorders) Elimination of special treatment of bizarre delusions and "special" hallucinations in Criterion A (characteristic symptoms) Rationale: This was removed due to poor reliability in distinguishing bizarre from non-bizarre delusions. At least 1 of the 2 symptoms required to meet Criterion A must be delusions, hallucinations, or disorganized speech Rationale: This will improve reliability and prevent individuals with only negative symptoms and catatonia from being diagnosed with schizophrenia.
39 Schizophrenia (cont.) Deletion of specific subtypes Rationale: DSM-IV's subtypes were shown to have very poor reliability and validity. They also failed to differentiate from one another based on treatment response and course.
40 Schizoaffective Disorder Now based on lifetime (rather than episodic) duration of illness in which the mood and psychotic symptoms described in Criterion A occur Rationale: The criteria in DSM-IV have demonstrated poor reliability and clinical utility, in part because the language in DSM-IV regarding the duration of illness is ambiguous. This revision is consistent with the schizophrenia and mood episodes language, which explicitly describes a longitudinal rather than an episodic course. Applying a longitudinal course to schizoaffective disorder will aid in its differential diagnosis from these related disorders.
41 Catatonia Now exists as a specifier for neurodevelopmental, psychotic, mood, and other mental disorders as well as other medical disorders (catatonia due to another medical condition) Rationale: As represented in DSM-IV, catatonia was underrecognized, particularly in psychiatric disorders other than schizophrenia and psychotic mood disorders as well as in other medical disorders. It was also apparent that the inclusion of catatonia as a specific condition that can apply more broadly across the manual may help address gaps in the treatment of catatonia.
42 Anxiety Disorders Relocated to own chapter, separate from other anxiety-related disorders "With panic attacks": specifier for any mental disorder Panic disorder and agoraphobia unlinked Inclusion of separation anxiety disorder and selective mutism in this chapter rather than in a chapter on child/adolescent disorders
43 Obsessive-Compulsive and Related Disorders Relocated to own chapter, separate from other anxiety disorders New or renamed disorders Hoarding disorder Excoriation (skin-picking) disorder Trichotillomania (hair-pulling disorder) Expansion of insight specifiers for OCD and BDD (i.e., "good or fair," "poor," "absent/delusional")
44 Trauma- and Stress-Related Disorders Relocated to own chapter, separate from other anxiety disorders PTSD criteria revised Stressor criterion (Criterion A) more explicit; elimination of subjective reaction (Criterion A2) Expansion to 4 symptom clusters, with avoidance/numbing cluster divided into 2 distinct clusters: avoidance and persistent negative alterations in cognitions and mood
45 Trauma- and Stress-Related Disorders (2) By including an additional criteria set focused solely on symptoms in children aged 6 and younger, diagnosis will be more developmentally sensitive and will call attention to differences in presentation among young children vs. adults (e.g., the re-experiencing of traumatic events through play or storytelling)
46 Trauma- and Stress-Related Disorders (3) Subtypes of reactive attachment disorder are now 2 distinct disorders Reactive attachment disorder Disinhibited social engagement disorder
47 Feeding and Eating Disorders Binge eating disorder elevated to the main body of the manual Inclusion of pica and rumination disorder in this chapter rather than in a chapter on child/adolescent disorders Anorexia nervosa: elimination of amenorrhea requirement Feeding disorder of infancy or early childhood has been renamed avoidant/restrictive food intake disorder

48 Sleep Wake Disorders Primary insomnia renamed insomnia disorder Subtypes of circadian rhythm sleep disorders expanded to include advanced sleep phase syndrome, irregular sleep wake type, and freerunning type Rapid eye movement sleep behavior disorder and restless legs syndrome both elevated to the main body of the manual Age and development more explicitly addressed in criteria and text
49 Gender Dysphoria New diagnostic class to reflect a change in the conceptualization of the disorder's defining features by emphasizing the phenomenon of "gender incongruence" rather than cross-gender identification, as in DSM-IV Gender identity disorder now named gender dysphoria Includes 2 separate sets of criteria for children and adults and adolescents Subtyping on the basis of sexual orientation is eliminated
50 Disruptive, Impulse Control, and Conduct Disorders Conduct disorder Addition of specifier: "with limited prosocial emotions" Lack of remorse Callous or lack of empathy Unconcerned about performance in school/work Shallow or deficient affect Cross-listing of antisocial personality disorder here and in personality disorders
51 Substance-Related and Addictive Disorders Consolidate substance abuse and substance dependence into a single disorder called substance use disorder Create a continuum that includes mild, moderate, and severe substance use Removal of one of the DSM-IV abuse criteria; addition of a new criterion to the new substance use disorder diagnosis Removal of legal consequences (e.g., multiple arrests) Addition of craving
52 Neurocognitive Disorders (NCD) Use of the term major neurocognitive disorder rather than dementia Rationale: The term dementia is usually associated with neurodegenerative conditions occurring in older populations, as in Alzheimer's disease and Lewy Body dementia. However, DSM-5's major NCD refers to a broad range of possible etiologies that can occur even in young adults, such as major NCD due to traumatic brain injury or HIV infection.
53 Mild NCD Newly added to DSM-5 Rationale: Patients with mild NCD are frequently seen in clinics and research settings, and there is widespread consensus throughout the field that this population can benefit from diagnosis and treatment. The clinical utility of such a diagnosis is also highly supported in the literature.
54 Select Changes in Diagnoses: Personality Disorders All 10 DSM-IV personality disorders will remain intact and located in Section II of DSM-5 Section III contains an alternative, trait-based diagnostic approach to personality disorders that separates functional impairment (A Criteria) and the expression of characteristic traits (B Criteria) for 6 personality disorders Personality disorder trait specified A direct mapping to existing criteria for DSM-IV personality disorders will assist clinicians in learning the new approach
55 Section III: Purpose Section III serves as a designated location, separate from diagnostic criteria, text, and clinical codes, for items that appear to have initial support in terms of clinical use but require further research before being officially recommended as part of the main body of the manual This separation clearly conveys to readers that the content may be clinically useful and warrants review but is not a part of an official diagnosis of a mental disorder and cannot be used as such
56 Section III: Content Section III: Emerging Measures and Models Assessment Measures Cultural Formulation Alternative DSM-5 Model for Personality Disorders Conditions for Further Study


57 Optional Section III: Measures Recommended for Further Study and Evaluation
58 Optional Measurements in DSM-5 Assess patient characteristics not necessarily included in diagnostic criteria but of high relevance to prognosis, treatment planning, and outcome for most patients In DSM-5, these include: Level 1 and Level 2 Cross-Cutting Symptom assessments Diagnosis-specific severity ratings Disability assessment May be patient, informant, or clinician completed, depending on the measure
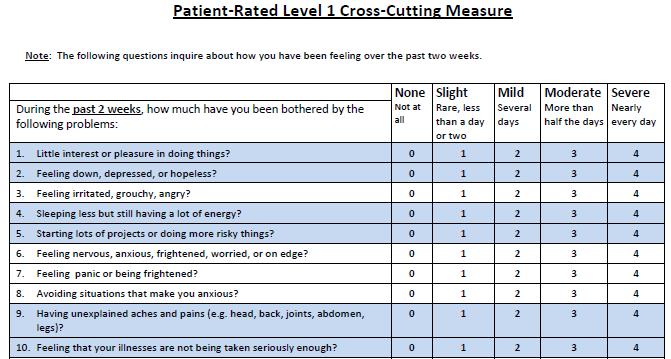
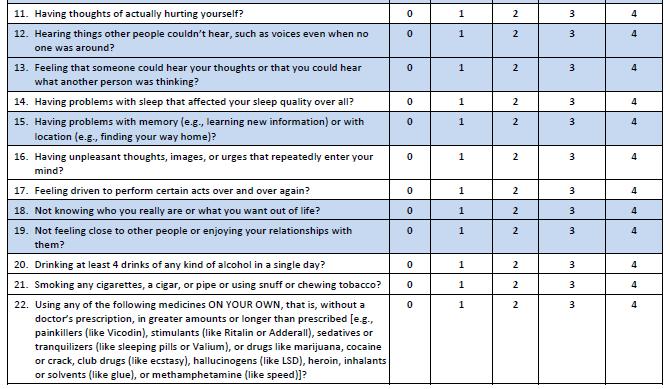
59 Level 1 Cross-Cutting Symptom Measure Referred to as "cross-cutting" because it calls attention to symptoms relevant to most if not all psychiatric disorders (e.g., mood, anxiety, sleep disturbance, substance use, suicide) Self-administered by patient 13 symptom domains for adults 12 symptom domains for children 11+ and parents of children 6+ Brief; 1-3 questions per symptom domain Screen for important symptoms, not for specific diagnoses (i.e., "cross-cutting")
60
61
62 Level 2 Cross-Cutting Measure Completed when the corresponding Level 1 item is endorsed at the level of "mild" or greater (for most but not all items; e.g., psychosis, inattention) Gives a more detailed assessment of the symptom domain Largely based on pre-existing, well-validated measures, including the SNAP-IV (inattention); NIDAmodified ASSIST (substance use); and PROMIS forms (anger, sleep disturbance, emotional distress)
63 Example of a Level 2 Cross-Cutting Assessment: Sleep Please respond to each item by choosing one option per question. Not at all A little Somewhat Quite a Very In the past SEVEN (7) DAYS... bit bit much My sleep was restless I was satisfied with my sleep My sleep was refreshing I had difficulty falling asleep In the past SEVEN (7) DAYS... Never Rarely Sometime Often Always s I had trouble staying asleep I had trouble sleeping I got enough sleep In the past SEVEN (7) DAYS Very Poor Poor Fair Good Very good My sleep quality was
64 Diagnosis-Specific Severity Measures For documenting the severity of a specific disorder using, for example, the frequency and intensity of its component symptoms Can be administered to individuals with: A diagnosis meeting full criteria An "other specified" diagnosis, especially a clinically significant syndrome that does not meet diagnostic threshold Some clinician rated, some patient rated
 Impaired Cognition Depression Mania 0 = Not Present 1 = Equivocal 2 = Present, but mild 3 = Present and moderate 4 = Present")
65 Diagnosis-Specific Severity Assessment: Symptom Domains for Schizophrenia Hallucinations Delusions Disorganized Speech Abnormal Psychomotor Behavior Negative Symptoms (Restricted Emotional Expression or Avolition) Impaired Cognition Depression Mania 0 = Not Present 1 = Equivocal 2 = Present, but mild 3 = Present and moderate 4 = Present and severe
66 World Health Organization Disability Assessment Schedule (WHODAS 2.0) WHODAS 2.0 is the recommended but not required assessment for disability Corresponds to disability domains of ICF Developed for use in all clinical and general population groups Tested worldwide and in DSM-5 Field Trials 36 questions, self-administered with clinician review For adult patients Child version developed by DSM-5, not yet approved by WHO
67 Section III: Content Section III: Conditions for Further Study Attenuated Psychosis Syndrome Depressive Episodes With Short-Duration Hypomania Persistent Complex Bereavement Disorder Caffeine Use Disorder Internet Gaming Disorder Neurobehavioral Disorder Due to Prenatal Alcohol Exposure Suicidal Behavior Disorder Non-suicidal Self-Injury
68 Appendix: Content Separate from Section III will be an Appendix including: Highlights of Changes From DSM-IV to DSM-5 Glossary of Technical Terms Glossary of Cultural Concepts of Distress Alphabetical Listing of DSM-5 Diagnoses and Codes (ICD-9-CM and ICD-10-CM) Numerical Listing of DSM-5 Diagnoses and Codes (ICD-9-CM) Numerical Listing of DSM-5 Diagnoses and Codes (ICD-10-CM) DSM-5 Advisors and Other Contributors

69
70
71 Posttest Question 1 In DSM-5: 1. The DSM-IV multiaxial system was fully retained 2. The DSM-IV multiaxial system was modified 3. The DSM-IV multiaxial system was replaced with a new multiaxial system 4. The multiaxial system was removed
72 Posttest Question 2 The chapter organization of DSM-5 1. Retains that of DSM-IV 2. Replaces that of DSM-IV with an alphabetical one 3. Replaces that of DSM-IV with a developmentallyinformed one 4. Was entirely determined by the World Health Organization
DSM-5 Has Arrived Copyright 2013 Neuroscience Education Institute. All rights reserved.
 Handout for the Neuroscience Education Institute (NEI) online activity: DSM-5 Has Arrived Learning Objectives Describe the major changes made to the DSM between DSM-IV and DSM-5, including manualwide changes
Handout for the Neuroscience Education Institute (NEI) online activity: DSM-5 Has Arrived Learning Objectives Describe the major changes made to the DSM between DSM-IV and DSM-5, including manualwide changes
DSM-5 Table of Contents
 DSM-5 Table of Contents DSM-5 Classification Preface Section I: DSM-5 Basics Introduction Use of DSM-5 Cautionary Statement for Forensic Use of DSM-5 Section II: Essential Elements: Diagnostic Criteria
DSM-5 Table of Contents DSM-5 Classification Preface Section I: DSM-5 Basics Introduction Use of DSM-5 Cautionary Statement for Forensic Use of DSM-5 Section II: Essential Elements: Diagnostic Criteria
What is the DSM. Diagnostic and Statistical Manual of Mental Disorders Purpose
 DSM 5 The Basics What is the DSM Diagnostic and Statistical Manual of Mental Disorders Purpose Standardize diagnosis criteria (objectivity) Assist in research Provide common terminology Public health statistics
DSM 5 The Basics What is the DSM Diagnostic and Statistical Manual of Mental Disorders Purpose Standardize diagnosis criteria (objectivity) Assist in research Provide common terminology Public health statistics
DSM-5 UPDATE FOR THOSE WORKING WITH OLDER ADULTS
 DSM-5 UPDATE FOR THOSE WORKING WITH OLDER ADULTS Ole J. Thienhaus, MD Professor and Chair Department of Psychiatry College of Medicine The University of Arizona, Tucson Learning Objectives: Discuss the
DSM-5 UPDATE FOR THOSE WORKING WITH OLDER ADULTS Ole J. Thienhaus, MD Professor and Chair Department of Psychiatry College of Medicine The University of Arizona, Tucson Learning Objectives: Discuss the
*Many of these DSM 5 Diagnoses might also be used to argue for eligibility using Other Health Impaired Criteria
 Handout 2: DSM 5 Diagnoses that May be Associated with One or More of the Five ED Characteristics* 1. An inability to learn that cannot be explained by intellectual, sensory, or health factors. a) Selective
Handout 2: DSM 5 Diagnoses that May be Associated with One or More of the Five ED Characteristics* 1. An inability to learn that cannot be explained by intellectual, sensory, or health factors. a) Selective
Navigating changes for Practitioners. Mehul Mankad, M.D.
 Wake AHEC & UNC Chapel Hill School of Social Work Clinical Lecture Series Transition to DSM-5: Navigating changes for Practitioners webinar presented by Mehul Mankad, M.D. mehul.mankad@duke.edu September
Wake AHEC & UNC Chapel Hill School of Social Work Clinical Lecture Series Transition to DSM-5: Navigating changes for Practitioners webinar presented by Mehul Mankad, M.D. mehul.mankad@duke.edu September
A HELPFUL WALK THROUGH DSM-5
 A HELPFUL WALK THROUGH DSM-5 ROGER SHAFER, MD UNITY POINT-FINLEY SUMMIT CENTER FOR OLDER ADULTS DUBUQUE, IA OBJECTIVES The learner will identify the foundational differences between the DSM-5 and the previous
A HELPFUL WALK THROUGH DSM-5 ROGER SHAFER, MD UNITY POINT-FINLEY SUMMIT CENTER FOR OLDER ADULTS DUBUQUE, IA OBJECTIVES The learner will identify the foundational differences between the DSM-5 and the previous
DSM Comparison Chart DSM-5 (Revisions in bold)
") 317.0-318.2 DSM Comparison Chart DSM-IV-TR DSM-5 (Revisions in bold) Multi-axial system s Usually First Diagnosed in Infancy, Childhood and Adolescence Single line diagnosis with specifiers Neurodevelopmental
317.0-318.2 DSM Comparison Chart DSM-IV-TR DSM-5 (Revisions in bold) Multi-axial system s Usually First Diagnosed in Infancy, Childhood and Adolescence Single line diagnosis with specifiers Neurodevelopmental
Mastering DSM-5: Diagnosing Disorders in Children, Adolescents, and Adults
 Mastering DSM-5: Diagnosing Disorders in Children, Adolescents, and Adults 1. The original DSM was published in: a. 1942 b. 1952 c. 1962 d. 1972 2. The first attempt to gather information about mental
Mastering DSM-5: Diagnosing Disorders in Children, Adolescents, and Adults 1. The original DSM was published in: a. 1942 b. 1952 c. 1962 d. 1972 2. The first attempt to gather information about mental
HIBBING COMMUNITY COLLEGE COURSE OUTLINE
 HIBBING COMMUNITY COLLEGE COURSE OUTLINE COURSE NUMBER & TITLE: PSYC 1400: Abnormal Psychology CREDITS: 3 (3Lec 0 / Lab) PREREQUISITES: PSYC 1205: General Psychology CATALOG DESCRIPTION: Abnormal Psychology
HIBBING COMMUNITY COLLEGE COURSE OUTLINE COURSE NUMBER & TITLE: PSYC 1400: Abnormal Psychology CREDITS: 3 (3Lec 0 / Lab) PREREQUISITES: PSYC 1205: General Psychology CATALOG DESCRIPTION: Abnormal Psychology
The New DSM- 5: A Clinical Discussion Through A Developmental Lens. Marit E. Appeldoorn, MSW, LICSW
 The New DSM- 5: A Clinical Discussion Through A Developmental Lens Marit E. Appeldoorn, MSW, LICSW 612-412- 1159 mappeldoornlicsw@gmail.com Introductions and My (Not- So- Bad) Dilemma What We Already Know
The New DSM- 5: A Clinical Discussion Through A Developmental Lens Marit E. Appeldoorn, MSW, LICSW 612-412- 1159 mappeldoornlicsw@gmail.com Introductions and My (Not- So- Bad) Dilemma What We Already Know
DSM-5 UPDATE. Supplement to DIAGNOSTIC AND STATISTICAL MANUAL OF MENTAL DISORDERS, FIFTH EDITION
 DSM-5 UPDATE Supplement to DIAGNOSTIC AND STATISTICAL MANUAL OF MENTAL DISORDERS, FIFTH EDITION October 2017 DSM-5 Update October 2017 Supplement to Diagnostic and Statistical Manual of Mental Disorders,
DSM-5 UPDATE Supplement to DIAGNOSTIC AND STATISTICAL MANUAL OF MENTAL DISORDERS, FIFTH EDITION October 2017 DSM-5 Update October 2017 Supplement to Diagnostic and Statistical Manual of Mental Disorders,
Introduction to DSM-5
 Changes in the Diagnostic and Statistical Manual of Mental s that Impact Forensic Psychology Kristine M. Jacquin, Ph.D. Fielding Graduate University Presented at ACFP Symposium 2014 Overview of Presentation
Changes in the Diagnostic and Statistical Manual of Mental s that Impact Forensic Psychology Kristine M. Jacquin, Ph.D. Fielding Graduate University Presented at ACFP Symposium 2014 Overview of Presentation
DSM 5 in Practice 9/16/2013. Susan Marie, PMHNP, PhD, BC. Focus on primary care usage. Relationship to ICD 9/10. Conceptual changes
 DSM 5 in Practice Susan Marie, PMHNP, PhD, BC Focus on primary care usage Relationship to ICD 9/10 Conceptual changes No multiaxial system No onset in childhood section Substance Induced/Medication Induced
DSM 5 in Practice Susan Marie, PMHNP, PhD, BC Focus on primary care usage Relationship to ICD 9/10 Conceptual changes No multiaxial system No onset in childhood section Substance Induced/Medication Induced
Changes to the Organization and Diagnostic Coverage of the SCID-5-RV
 Changes to the Organization and Diagnostic Coverage of the SCID-5-RV Core vs. Enhanced SCID configuration A number of new disorders have been added to the SCID-5-RV. To try to reduce the length and complexity
Changes to the Organization and Diagnostic Coverage of the SCID-5-RV Core vs. Enhanced SCID configuration A number of new disorders have been added to the SCID-5-RV. To try to reduce the length and complexity
Disclosure Information. Preparing for DSM-5. Program Outline. Rajiv Tandon, M.D. Professor Of Psychiatry University of Florida.
 Preparing for DSM-5 Disclosure Information Rajiv Tandon, M.D. Professor Of Psychiatry University of Florida NO RELEVANT FINANCIAL CONFLICTS OF INTEREST MEMBER OF THE DSM-5 WORKGROUP ON PSYCHOTIC DISORDERS
Preparing for DSM-5 Disclosure Information Rajiv Tandon, M.D. Professor Of Psychiatry University of Florida NO RELEVANT FINANCIAL CONFLICTS OF INTEREST MEMBER OF THE DSM-5 WORKGROUP ON PSYCHOTIC DISORDERS
INPATIENT INCLUDED ICD-10 CODES
 INPATIENT INCLUDED ICD-10 CODES MHSUDS IN 18-053 ICD-10 F01.51 Vascular Dementia With Behavioral Disturbance F10.14 Alcohol Abuse With Alcohol-Induced Mood Disorder F10.150 Alcohol Abuse With Alcohol-Induced
INPATIENT INCLUDED ICD-10 CODES MHSUDS IN 18-053 ICD-10 F01.51 Vascular Dementia With Behavioral Disturbance F10.14 Alcohol Abuse With Alcohol-Induced Mood Disorder F10.150 Alcohol Abuse With Alcohol-Induced
The Virtual En-psych-lopedia by Dr. Bob. DSM-IV Diagnoses and Codes, Alphabetical Listing
 The Virtual En-psych-lopedia by Dr. Bob DSM-IV Diagnoses and Codes, Alphabetical Listing DSM-5 listings: alphabetical, by diagnosis numerical, by ICD-9-CM and ICD-10-CM code This is just an alphabetical
The Virtual En-psych-lopedia by Dr. Bob DSM-IV Diagnoses and Codes, Alphabetical Listing DSM-5 listings: alphabetical, by diagnosis numerical, by ICD-9-CM and ICD-10-CM code This is just an alphabetical
DSM-5 Task Force 13 workgroups led by task force member Scientific Review Committee 6 committee members, chair and vicechair
 Nancy M. Birtley, DNP, APRN, PMHCNS-BC, PMHNP-BC Owner, Psychiatric Consultation Services Assistant Teaching Professor, University of Missouri, Columbia DSM-5 Task Force 13 workgroups led by task force
Nancy M. Birtley, DNP, APRN, PMHCNS-BC, PMHNP-BC Owner, Psychiatric Consultation Services Assistant Teaching Professor, University of Missouri, Columbia DSM-5 Task Force 13 workgroups led by task force
ICD 10 CM Codes for Evaluation & Management October 1, 2017
 ICD 10 CM Codes for Evaluation & Management October 1, 2017 Code Description Comments F01.50 Vascular dementia without behavioral disturbance F01.51 Vascular dementia with behavioral disturbance F02.80
ICD 10 CM Codes for Evaluation & Management October 1, 2017 Code Description Comments F01.50 Vascular dementia without behavioral disturbance F01.51 Vascular dementia with behavioral disturbance F02.80
A PRACTICAL INTRODUCTION TO THE DSM-5: IMPLEMENTING THE CHANGES IN CLINICAL PRACTICE
 A PRACTICAL INTRODUCTION TO THE DSM-5: IMPLEMENTING THE CHANGES IN CLINICAL PRACTICE Diane R. Gehart, Ph.D. California State University, Northridge Acknowledgements Sections of this chapter were developed
A PRACTICAL INTRODUCTION TO THE DSM-5: IMPLEMENTING THE CHANGES IN CLINICAL PRACTICE Diane R. Gehart, Ph.D. California State University, Northridge Acknowledgements Sections of this chapter were developed
CMASA 2016 Stellenbosch. Dr David Swingler 02 June Acknowledgements
 CMASA 2016 Stellenbosch Dr David Swingler 02 June 2016 Acknowledgements DSM-5 History & development What s new Concepts Overview A speed-dating surf through the disorders With particular reference to conditions
CMASA 2016 Stellenbosch Dr David Swingler 02 June 2016 Acknowledgements DSM-5 History & development What s new Concepts Overview A speed-dating surf through the disorders With particular reference to conditions
Highlights of Changes from DSM-IV-TR to DSM-5
 Highlights of Changes from DSM-IV-TR to DSM-5 Changes made to the DSM-5 diagnostic criteria and texts are outlined in this chapter in the same order in which they appear in the DSM-5 classification. This
Highlights of Changes from DSM-IV-TR to DSM-5 Changes made to the DSM-5 diagnostic criteria and texts are outlined in this chapter in the same order in which they appear in the DSM-5 classification. This
DSM-5: research informed changes?
 DSM-5: research informed changes? Dr. Danai Dima 26.09.2014, University of Malta The history that led to the Diagnostic and Statistical Manual ofmental Disorders -5 History of DSMs The initial impetus
DSM-5: research informed changes? Dr. Danai Dima 26.09.2014, University of Malta The history that led to the Diagnostic and Statistical Manual ofmental Disorders -5 History of DSMs The initial impetus
Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5 TM) - Overview What You Need to Know
 - Overview What You Need to Know") Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5 TM) - Overview What You Need to Know 2 CE Hours By: Kathryn Brohl, MA, LMFT Reviewed and edited by: Wade T. Lijewski, Ph.D. Learning
Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5 TM) - Overview What You Need to Know 2 CE Hours By: Kathryn Brohl, MA, LMFT Reviewed and edited by: Wade T. Lijewski, Ph.D. Learning
Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5 TM) Overview. (2 CEU s)
 Overview. (2 CEU s)") Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5 TM) Overview Course Objectives: (2 CEU s) At the completion of this course, participants will be able to: Explain the importance
Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5 TM) Overview Course Objectives: (2 CEU s) At the completion of this course, participants will be able to: Explain the importance
DSM-5: Update presented by Dr. Risby
 DSM-5: Update presented by Dr. Risby Purpose Update on some of the key diagnostic changes from DSM-IV-TR to DSM-5. This is not intended to be a basic course on DSM-5. New and Eliminated Disorders in DSM-5
DSM-5: Update presented by Dr. Risby Purpose Update on some of the key diagnostic changes from DSM-IV-TR to DSM-5. This is not intended to be a basic course on DSM-5. New and Eliminated Disorders in DSM-5
EVOLUTION OF THE DSM 8/23/2013. The New DSM-5 : What Administrators Need to Know. American Psychiatric Association Copyright Statement
 The New DSM-5 : What Administrators Need to Know Jason J. Washburn, PhD., ABPP Director, Center for Evidence-Based Practice American Psychiatric Association Copyright Statement DSM and DSM-5 are registered
The New DSM-5 : What Administrators Need to Know Jason J. Washburn, PhD., ABPP Director, Center for Evidence-Based Practice American Psychiatric Association Copyright Statement DSM and DSM-5 are registered
ACBHCS Outpatient Included List DHCS ICD-10
 12-19-17 ACBHCS Mental Health Outpatient (includes PES/CSU) Crosswalk Medi-Cal Included Dx List Numeric by Code (Crossed out diagnoses are not allowed. Always use the code) Instructions: Crossed out diagnoses
12-19-17 ACBHCS Mental Health Outpatient (includes PES/CSU) Crosswalk Medi-Cal Included Dx List Numeric by Code (Crossed out diagnoses are not allowed. Always use the code) Instructions: Crossed out diagnoses
ACBHCS Mental Health Outpatient (includes PES/CSU) Medi-Cal Included Diagnosis List - Alpha by Name
 Medi-Cal Included Diagnosis List - Alpha by Name") Instructions: DHCS publishes the list of diagnoses covered by Medi-Cal in format. The DSM is used because does not provide specific diagnostic criteria. Providers must always use DSM-5 first and whenever
Instructions: DHCS publishes the list of diagnoses covered by Medi-Cal in format. The DSM is used because does not provide specific diagnostic criteria. Providers must always use DSM-5 first and whenever
ACBHCS Outpatient Included List DHCS ICD-10
 12-19-17 ACBHCS Mental Health Outpatient (includes PES/CSU) Crosswalk Medi-Cal Included Dx List-Alpha by Name (Crossed out diagnoses are not allowed. Always use the code) Instructions: Crossed out diagnoses
12-19-17 ACBHCS Mental Health Outpatient (includes PES/CSU) Crosswalk Medi-Cal Included Dx List-Alpha by Name (Crossed out diagnoses are not allowed. Always use the code) Instructions: Crossed out diagnoses
True/False Quiz questions on the DSM 5
 True/False Quiz questions on the DSM 5 These questions were designed to guide your learning about changes and important points in the DSM 5. You can get 15 CE credits for only $69 by taking this quiz at
True/False Quiz questions on the DSM 5 These questions were designed to guide your learning about changes and important points in the DSM 5. You can get 15 CE credits for only $69 by taking this quiz at
ACBHCS Mental Health Outpatient (includes PES/CSU) Medi-Cal Included Diagnosis List by ICD-10 Code
 Medi-Cal Included Diagnosis List by ICD-10 Code") Instructions: DHCS publishes the list of diagnoses covered by Medi-Cal in format. The DSM is used because does not provide specific diagnostic criteria. Providers must always use DSM-5 first and whenever
Instructions: DHCS publishes the list of diagnoses covered by Medi-Cal in format. The DSM is used because does not provide specific diagnostic criteria. Providers must always use DSM-5 first and whenever
Serious Mental Illness (SMI) CRITERIA CHECKLIST
 CRITERIA CHECKLIST") Serious Mental Illness (SMI) CRITERIA CHECKLIST BEHAVIORAL HEALTH COLLABORATIVE NEW MEXICO SMI determination is based on the age of the individual, functional impairment, duration of the disorder and the
Serious Mental Illness (SMI) CRITERIA CHECKLIST BEHAVIORAL HEALTH COLLABORATIVE NEW MEXICO SMI determination is based on the age of the individual, functional impairment, duration of the disorder and the
Journal of Research and Practice in K-20 Education 29 Volume 1, 2015
 Journal of Research and Practice in K-20 Education 29 Changes in DSM-5: A Counselor Educator s Review By: Debra Leggett, Ph.D. and Dr. Beverly Mustaine, Ed.D. Abstract The purpose of this study is to provide
Journal of Research and Practice in K-20 Education 29 Changes in DSM-5: A Counselor Educator s Review By: Debra Leggett, Ph.D. and Dr. Beverly Mustaine, Ed.D. Abstract The purpose of this study is to provide
9/17/2013 EVOLUTION OF THE DSM. The Future is Now: DSM-5. The American Psychiatric Association is not. Copyright Statement
 The Future is Now: DSM-5 Jason J. Washburn, PhD., ABPP Center for Evidence-Based Practice American Psychiatric Association Copyright Statement DSM and DSM-5 are registered trademarks of the American Psychiatric
The Future is Now: DSM-5 Jason J. Washburn, PhD., ABPP Center for Evidence-Based Practice American Psychiatric Association Copyright Statement DSM and DSM-5 are registered trademarks of the American Psychiatric
ICD-10 and DSM-5: Making Sense in the Clinical Environment. Mehul Mankad, MD Assistant Professor Duke University Medical Center
 ICD-10 and DSM-5: Making Sense in the Clinical Environment Mehul Mankad, MD Assistant Professor Duke University Medical Center 1 GSK Foundation Disclosures 2 Specific Aims Review of pertinent differences
ICD-10 and DSM-5: Making Sense in the Clinical Environment Mehul Mankad, MD Assistant Professor Duke University Medical Center 1 GSK Foundation Disclosures 2 Specific Aims Review of pertinent differences
7 DSM Codes. CARE System April 2013 DSM Codes 7-1
 7 DSM Codes This section contains codes and decode values used in CARE from the current edition of the and Statistical Manual of Mental Disorders. There is also an Axis (Axis 1, Axis 2, or Blank for both)
7 DSM Codes This section contains codes and decode values used in CARE from the current edition of the and Statistical Manual of Mental Disorders. There is also an Axis (Axis 1, Axis 2, or Blank for both)
OUTPATIENT INCLUDED ICD-10 CODES
 MHSUDS IN 18-053 ICD-10 OUTPATIENT INCLUDED ICD-10 CODES F20.0 Paranoid Schizophrenia F20.1 Disorganized Schizophrenia F20.2 Catatonic Schizophrenia F20.3 Undifferentiated Schizophrenia F20.5 Residual
MHSUDS IN 18-053 ICD-10 OUTPATIENT INCLUDED ICD-10 CODES F20.0 Paranoid Schizophrenia F20.1 Disorganized Schizophrenia F20.2 Catatonic Schizophrenia F20.3 Undifferentiated Schizophrenia F20.5 Residual
A DSM By Any Other Name? 6/18/2013
 A DSM By Any Other Name? Disclosures Financial Conflicts PrairieCare Medical Group (co-owner) PrairieCare (CEO & Chief Medical Officer) CATCH, LLC (co-owner) A University of Minnesota Medical School Affiliate
A DSM By Any Other Name? Disclosures Financial Conflicts PrairieCare Medical Group (co-owner) PrairieCare (CEO & Chief Medical Officer) CATCH, LLC (co-owner) A University of Minnesota Medical School Affiliate
Profile of PAES Recipients and Factors That Influence PAES Outcomes
 ` San Francisco Department of Human Services County Adult Assistance Programs Personal Assisted Employment Services Program Profile of PAES Recipients and Factors That Influence PAES Outcomes Analysis
` San Francisco Department of Human Services County Adult Assistance Programs Personal Assisted Employment Services Program Profile of PAES Recipients and Factors That Influence PAES Outcomes Analysis
INDIANA HEALTH COVERAGE PROGRAMS
 INDIANA HEALTH COVERAGE PROGRAMS PROVIDER CODE TABLES Medicaid Rehabilitation Option (MRO) Services Codes Note: Due to possible changes in Indiana Health Coverage Programs (IHCP) policy or national coding
INDIANA HEALTH COVERAGE PROGRAMS PROVIDER CODE TABLES Medicaid Rehabilitation Option (MRO) Services Codes Note: Due to possible changes in Indiana Health Coverage Programs (IHCP) policy or national coding
What We ll Cover. Why Do We Have a DSM? 10/6/2013
 1 Aaron Norton, LMHC, CAP, CRC President Elect, Suncoast Mental Health Counselors Association Licensed Mental Health Counselor www.anorton.com Henry Tenenbaum, Ph.D. Licensed Psychologist Licensed School
1 Aaron Norton, LMHC, CAP, CRC President Elect, Suncoast Mental Health Counselors Association Licensed Mental Health Counselor www.anorton.com Henry Tenenbaum, Ph.D. Licensed Psychologist Licensed School
Health Care Agency, Behavioral Health Service, AQIS CYBH Support
 Health Care Agency, Behavioral Health Service, AQIS CYBH Support DX Code F20.0 Paranoid schizophrenia F20.1 Disorganized schizophrenia F20.2 Catatonic schizophrenia F20.3 Undifferentiated schizophrenia
Health Care Agency, Behavioral Health Service, AQIS CYBH Support DX Code F20.0 Paranoid schizophrenia F20.1 Disorganized schizophrenia F20.2 Catatonic schizophrenia F20.3 Undifferentiated schizophrenia
Psych Grand Rounds. Disclosure. My books
 for Asperger Syndrome and Other Related Disorders Practical Strategies for Assessment Practical Strategies and for Treatment Assessment and Treatment Illustrated by Laura S. Kowalski A Simple Technique
for Asperger Syndrome and Other Related Disorders Practical Strategies for Assessment Practical Strategies and for Treatment Assessment and Treatment Illustrated by Laura S. Kowalski A Simple Technique
Provider Bulletin Philadelphia Department of Behavioral Health Community Behavioral Health State Allowable ICD-9-CM Codes.
 Provider Bulletin 07-01 Philadelphia Department of Behavioral Health Community Behavioral Health State Allowable ICD-9-CM Codes. February 12, 2007 The Commonwealth of Pennsylvania lists the allowable ICD-9-CM
Provider Bulletin 07-01 Philadelphia Department of Behavioral Health Community Behavioral Health State Allowable ICD-9-CM Codes. February 12, 2007 The Commonwealth of Pennsylvania lists the allowable ICD-9-CM
Introduction to the DSM-5 for APRNs. Presenters. Disclosures. Continuing Education Subcommittee APNA Education Council. Co-Chairs of CE subcommittee:
 Introduction to the DSM-5 for APRNs Continuing Education Subcommittee APNA Education Council Presenters Co-Chairs of CE subcommittee: Barbara J. Limandri, PhD, PMHCNS-BC Joyce M. Shea, DNSc, APRN, BC Presenters:
Introduction to the DSM-5 for APRNs Continuing Education Subcommittee APNA Education Council Presenters Co-Chairs of CE subcommittee: Barbara J. Limandri, PhD, PMHCNS-BC Joyce M. Shea, DNSc, APRN, BC Presenters:
Minnesota DC:0-3R Crosswalk to ICD codes
 DC 0-3R 0 Post-Traumatic Stress (this diagnosis must be considered first according to the DC:0-3R decision tree) 150 Deprivation/Maltreatment 200 of Affect 2 Prolonged Bereavement/Grief Reaction 220 Anxiety
DC 0-3R 0 Post-Traumatic Stress (this diagnosis must be considered first according to the DC:0-3R decision tree) 150 Deprivation/Maltreatment 200 of Affect 2 Prolonged Bereavement/Grief Reaction 220 Anxiety
INDIANA HEALTH COVERAGE PROGRAMS
 INDIANA HEALTH COVERAGE PROGRAMS PROVIDER CODE TABLES Division of Mental Health and Addiction (DMHA) Behavioral and Primary Healthcare Coordination (BPHC) Codes Note: Due to possible changes in Indiana
INDIANA HEALTH COVERAGE PROGRAMS PROVIDER CODE TABLES Division of Mental Health and Addiction (DMHA) Behavioral and Primary Healthcare Coordination (BPHC) Codes Note: Due to possible changes in Indiana
Psychological Disorders. Schizophrenia Spectrum & Other Psychotic Disorders. Schizophrenia. Neurodevelopmental Disorders 4/12/2018
 Psychological s Schizophrenia Spectrum & Other Psychotic s Schizophrenia Spectrum & Other Psychotic s 0Presence of delusions, hallucinations, disorganized thinking/speech, disorganized or abnormal motor
Psychological s Schizophrenia Spectrum & Other Psychotic s Schizophrenia Spectrum & Other Psychotic s 0Presence of delusions, hallucinations, disorganized thinking/speech, disorganized or abnormal motor
FOLLOW-UP CARE FOR CHILDREN PRESCRIBED ADHD MEDICATION (ADD) To ensure child members who are newly prescribed attentiondeficit/hyperactivity
 To ensure child members who are newly prescribed attentiondeficit/hyperactivity") FOLLOW-UP CARE FOR CHILDREN PRESCRIBED ADHD MEDICATION (ADD) APPLICATIONS OBJECTIVE Purpose of Measure: ELIGIBLE POPULATION Which members are included? STANDARD OF CARE NCQA ACCEPTED CODES DOCUMENTATION
FOLLOW-UP CARE FOR CHILDREN PRESCRIBED ADHD MEDICATION (ADD) APPLICATIONS OBJECTIVE Purpose of Measure: ELIGIBLE POPULATION Which members are included? STANDARD OF CARE NCQA ACCEPTED CODES DOCUMENTATION
Rutgers University Course Syllabus Abnormal Psychology 01: 830: 340H7 Summer 3 rd Session 2014
 Rutgers University Course Syllabus Abnormal Psychology 01: 830: 340H7 Summer 3 rd Session 2014 Date & Time: Monday and Wednesday 6:00PM- 9:40PM Location: LSB rm B115 Livingston Campus Instructor: Stevie
Rutgers University Course Syllabus Abnormal Psychology 01: 830: 340H7 Summer 3 rd Session 2014 Date & Time: Monday and Wednesday 6:00PM- 9:40PM Location: LSB rm B115 Livingston Campus Instructor: Stevie
Oklahoma Psychological Association DSM-5 Panel November 8-9, 2013 Jennifer L. Morris, Ph.D.
 Oklahoma Psychological Association DSM-5 Panel November 8-9, 2013 Jennifer L. Morris, Ph.D. DSM-5 continues developmental progression, starting with disorders that are observed in early life. Disorders
Oklahoma Psychological Association DSM-5 Panel November 8-9, 2013 Jennifer L. Morris, Ph.D. DSM-5 continues developmental progression, starting with disorders that are observed in early life. Disorders
Table of substance use disorder diagnoses:
 Table of substance use disorder diagnoses: ICD-9 Codes Description 291 Alcohol withdrawal delirium 291.3 Alcohol-induced psychotic disorder with hallucinations 291.4 Idiosyncratic alcohol intoxication
Table of substance use disorder diagnoses: ICD-9 Codes Description 291 Alcohol withdrawal delirium 291.3 Alcohol-induced psychotic disorder with hallucinations 291.4 Idiosyncratic alcohol intoxication
Agoraphobia. An anxiety disorder marked by fear of being in situations in which escape may be difficult or impossible.
 Agoraphobia An anxiety disorder marked by fear of being in situations in which escape may be difficult or impossible. (See page 634) Antisocial personality disorder (APD) A personality disorder marked
Agoraphobia An anxiety disorder marked by fear of being in situations in which escape may be difficult or impossible. (See page 634) Antisocial personality disorder (APD) A personality disorder marked
Five Changes in DSM 5 Principles for Primary Care. Tom Janzen, M.D. STEGH Mental Health May 14, 2014
 Five Changes in DSM 5 Principles for Primary Care Tom Janzen, M.D. STEGH Mental Health May 14, 2014 Overall Learning Objectives Review 5 changes to DSM 5 which have significance for Family Physicians Examine
Five Changes in DSM 5 Principles for Primary Care Tom Janzen, M.D. STEGH Mental Health May 14, 2014 Overall Learning Objectives Review 5 changes to DSM 5 which have significance for Family Physicians Examine
FOLLOW-UP AFTER HOSPITALIZATION FOR MENTAL ILLNESS (FUH)
") FOLLOW-UP AFTER HOSPITALIZATION FOR MENTAL ILLNESS (FUH) APPLICATIONS OBJECTIVE Purpose of Measure: ELIGIBLE POPULATION Which members are included? STANDARD OF CARE NCQA ACCPETED CODES HEDIS (Administrative)
FOLLOW-UP AFTER HOSPITALIZATION FOR MENTAL ILLNESS (FUH) APPLICATIONS OBJECTIVE Purpose of Measure: ELIGIBLE POPULATION Which members are included? STANDARD OF CARE NCQA ACCPETED CODES HEDIS (Administrative)
Psychological Disorders
 Chapter 12 Psychological 12-1 Abnormal Behavior The most commonly used criteria for distinguishing between normal and abnormal behaviors are: 12-2 Abnormal Behavior We can define behaviors as abnormal
Chapter 12 Psychological 12-1 Abnormal Behavior The most commonly used criteria for distinguishing between normal and abnormal behaviors are: 12-2 Abnormal Behavior We can define behaviors as abnormal
SPECIALTY MENTAL HEALTH OUTPATIENT SERVICES ICD-10 COVERED DIAGNOSIS TABLE Diagnosis Code
 SPECIALTY MENTAL HEALTH OUTPATIENT SERVICES F20.0 Paranoid schizophrenia F20.1 Disorganized schizophrenia F20.2 Catatonic schizophrenia F20.3 Undifferentiated schizophrenia F20.5 Residual schizophrenia
SPECIALTY MENTAL HEALTH OUTPATIENT SERVICES F20.0 Paranoid schizophrenia F20.1 Disorganized schizophrenia F20.2 Catatonic schizophrenia F20.3 Undifferentiated schizophrenia F20.5 Residual schizophrenia
Rutgers University Course Syllabus Abnormal Psychology 01: 830: 340H6 Summer 3 rd Session 2015
 Rutgers University Course Syllabus Abnormal Psychology 01: 830: 340H6 Summer 3 rd Session 2015 Date & Time: Monday and Wednesday 6:00PM- 9:40PM Location: Tillett bldg. room 253 Livingston Campus Instructor:
Rutgers University Course Syllabus Abnormal Psychology 01: 830: 340H6 Summer 3 rd Session 2015 Date & Time: Monday and Wednesday 6:00PM- 9:40PM Location: Tillett bldg. room 253 Livingston Campus Instructor:
Specialty Mental Health Services ICD-10 Outpatient Diagnosis Table
 Specialty Mental Health Services ICD-10 Table Enclosure 3 295.10 Schizophrenia, Disorganized Type F20.1 Disorganized schizophrenia 295.20 Schizophrenia, Catatonic Type F20.2 Catatonic schizophrenia 295.30
Specialty Mental Health Services ICD-10 Table Enclosure 3 295.10 Schizophrenia, Disorganized Type F20.1 Disorganized schizophrenia 295.20 Schizophrenia, Catatonic Type F20.2 Catatonic schizophrenia 295.30
DSM-5. Jon E. Grant, JD, MD, MPH Professor University of Chicago Pritzker School of Medicine Chicago, IL
 DSM-5 Jon E. Grant, JD, MD, MPH Professor University of Chicago Pritzker School of Medicine Chicago, IL Disclosure Information Financial relationships: Grant/Research support from: NIDA, NCRG, Forest Pharmaceuticals
DSM-5 Jon E. Grant, JD, MD, MPH Professor University of Chicago Pritzker School of Medicine Chicago, IL Disclosure Information Financial relationships: Grant/Research support from: NIDA, NCRG, Forest Pharmaceuticals
VALID AXIS DSM 5 CODICD 10 DESCRIPTOR BOTH R69 Diagnosis deferred BOTH Z0389 Encounter for observation for other suspected diseases and conditions
 VALID AXIS DSM 5 CODICD 10 DESCRIPTOR BOTH R69 Diagnosis deferred BOTH Z0389 Encounter for observation for other suspected diseases and conditions ruled out 1 E669 Obesity, unspecified 1 F0150 Vascular
VALID AXIS DSM 5 CODICD 10 DESCRIPTOR BOTH R69 Diagnosis deferred BOTH Z0389 Encounter for observation for other suspected diseases and conditions ruled out 1 E669 Obesity, unspecified 1 F0150 Vascular
STATE OF WASHINGTON ACCESS TO CARE STANDARDS
 STATE OF WASHINGTON ACCESS TO CARE STANDARDS FOR BEHAVIORAL HEALTH ORGANIZATIONS Effective: 01 April 2016 NORTH SOUND BHO-THERAPEUTIC-MEDICAID-16-18 1 P a g e INTRODUCTION AND SCOPE The statewide Access
STATE OF WASHINGTON ACCESS TO CARE STANDARDS FOR BEHAVIORAL HEALTH ORGANIZATIONS Effective: 01 April 2016 NORTH SOUND BHO-THERAPEUTIC-MEDICAID-16-18 1 P a g e INTRODUCTION AND SCOPE The statewide Access
Brief Notes on the Mental Health of Children and Adolescents
 Brief Notes on the Mental Health of Children and Adolescents The future of our country depends on the mental health and strength of our young people. However, many children have mental health problems
Brief Notes on the Mental Health of Children and Adolescents The future of our country depends on the mental health and strength of our young people. However, many children have mental health problems
ASHA Comments* (ASHA Recommendations Compared to DSM-5 Criteria) Austism Spectrum Disorder (ASD)
 Austism Spectrum Disorder (ASD)") DSM-5 (Criteria and Major Changes for SLP-Related Conditions) Individuals meeting the criteria will be given a diagnosis of autism spectrum disorder with three levels of severity based on degree of support
DSM-5 (Criteria and Major Changes for SLP-Related Conditions) Individuals meeting the criteria will be given a diagnosis of autism spectrum disorder with three levels of severity based on degree of support
Unit 1. Behavioral Health Course. ICD-10-CM Specialized Coding Training. For Local Health Departments and Rural Health
 ICD-10-CM Specialized Coding Training http://publichealth.nc.gov/lhd/icd10/training.htm Behavioral Health Course For Local Health Departments and Rural Health Unit 1 1 Behavioral Health Training Objectives
ICD-10-CM Specialized Coding Training http://publichealth.nc.gov/lhd/icd10/training.htm Behavioral Health Course For Local Health Departments and Rural Health Unit 1 1 Behavioral Health Training Objectives
Rutgers University Course Syllabus Abnormal Psychology 01: 830: 340 H6 Summer3 rd Session 2018
 Rutgers University Course Syllabus Abnormal Psychology 01: 830: 340 H6 Summer3 rd Session 2018 Date & Time: Monday and Wednesday 6:00PM- 9:40PM Location: Lucy Stone Hall room B-112 Livingston Campus Instructor:
Rutgers University Course Syllabus Abnormal Psychology 01: 830: 340 H6 Summer3 rd Session 2018 Date & Time: Monday and Wednesday 6:00PM- 9:40PM Location: Lucy Stone Hall room B-112 Livingston Campus Instructor:
Psychosis, Mood, and Personality: A Clinical Perspective
 Psychosis, Mood, and Personality: A Clinical Perspective John R. Chamberlain, M.D. Assistant Director, Psychiatry and the Law Program Assistant Clinical Professor University of California San Francisco
Psychosis, Mood, and Personality: A Clinical Perspective John R. Chamberlain, M.D. Assistant Director, Psychiatry and the Law Program Assistant Clinical Professor University of California San Francisco
Announcements. The final Aplia gauntlet: Final Exam is May 14, 3:30 pm Still more experiments going up daily! Enhanced Grade-query Tool+
 The final Aplia gauntlet: Announcements Chapter 12 Aplia due tonight Chapter 13 Aplia due Wednesday Final Exam is May 14, 3:30 pm Still more experiments going up daily! Enhanced Grade-query Tool+ Now includes
The final Aplia gauntlet: Announcements Chapter 12 Aplia due tonight Chapter 13 Aplia due Wednesday Final Exam is May 14, 3:30 pm Still more experiments going up daily! Enhanced Grade-query Tool+ Now includes
Visualizing Psychology
 Visualizing Psychology by Siri Carpenter & Karen Huffman PowerPoint Lecture Notes Presentation Chapter 13: Psychological Disorders Siri Carpenter, Yale University Karen Huffman, Palomar College Lecture
Visualizing Psychology by Siri Carpenter & Karen Huffman PowerPoint Lecture Notes Presentation Chapter 13: Psychological Disorders Siri Carpenter, Yale University Karen Huffman, Palomar College Lecture
10. Psychological Disorders & Health
 10. Psychological Disorders & Health We will now study different psychological disorders and theories for treating psychopathology. We will also cover health, stress and how to cope with them. The sections
10. Psychological Disorders & Health We will now study different psychological disorders and theories for treating psychopathology. We will also cover health, stress and how to cope with them. The sections
When is a Psychological Disorder a Disability? Dr. Leigh Ann Ford, PhD, HSP Licensed Psychologist ABVE 2017 Annual Conference. Goals for presentation
 When is a Psychological Disorder a Disability? Dr. Leigh Ann Ford, PhD, HSP Licensed Psychologist ABVE 2017 Annual Conference Goals for presentation *To review DSM-V criteria for some of the most frequently
When is a Psychological Disorder a Disability? Dr. Leigh Ann Ford, PhD, HSP Licensed Psychologist ABVE 2017 Annual Conference Goals for presentation *To review DSM-V criteria for some of the most frequently
3/9/2017. Diagnostic Classification of Mental Health and Developmental Disorders of Infancy and Early Childhood: An Overview of DC:0-5
 Diagnostic Classification of Mental Health and Developmental Disorders of Infancy and Early Childhood: An Overview of DC:0-5 Presented by: Kathleen Mulrooney, MA, LPC, IMH-E IV ZERO TO THREE Copyright
Diagnostic Classification of Mental Health and Developmental Disorders of Infancy and Early Childhood: An Overview of DC:0-5 Presented by: Kathleen Mulrooney, MA, LPC, IMH-E IV ZERO TO THREE Copyright
Chapter 14. Psychological Disorders 8 th Edition
 Chapter 14 Psychological Disorders 8 th Edition Abnormal Behavior Historical aspects of mental disorders F 14.1 The medical model What is abnormal behavior? 3 criteria F 14.2 Deviant Maladaptive Causing
Chapter 14 Psychological Disorders 8 th Edition Abnormal Behavior Historical aspects of mental disorders F 14.1 The medical model What is abnormal behavior? 3 criteria F 14.2 Deviant Maladaptive Causing
Program Outline. DSM-5 Schizophrenia Spectrum and Psychotic Disorders: Knowing it Better and Improving Clinical Practice.
 DSM-5 Spectrum and Disorders: Knowing it Better and Improving Clinical Practice Rajiv Tandon, MD Professor of Psychiatry University of Florida College of Medicine Gainesville, Florida Program Outline Changes
DSM-5 Spectrum and Disorders: Knowing it Better and Improving Clinical Practice Rajiv Tandon, MD Professor of Psychiatry University of Florida College of Medicine Gainesville, Florida Program Outline Changes
Diagnosis. Shayna Sokol, LSW, CHC
 Diagnosis Shayna Sokol, LSW, CHC Diagnosis Across the Age Continuum 1 in 5 Children have a diagnosable MH condition I m an adult Service Coordinator, so why do I need to know about child and adolescent
Diagnosis Shayna Sokol, LSW, CHC Diagnosis Across the Age Continuum 1 in 5 Children have a diagnosable MH condition I m an adult Service Coordinator, so why do I need to know about child and adolescent
APNA 27th Annual Conference Session 1025: October 9, 2013
 Sandra J. Cadena, PhD, APRN CPT WorkGroup - APNA Representative DrSJCadena@gmail.com Review the DSM-5 changes & additions Describe the 2013 revisions to the Current Procedural Terminology (CPT) codes CPT
Sandra J. Cadena, PhD, APRN CPT WorkGroup - APNA Representative DrSJCadena@gmail.com Review the DSM-5 changes & additions Describe the 2013 revisions to the Current Procedural Terminology (CPT) codes CPT
AUTISM SPECTRUM DISORDER: DSM-5 DIAGNOSTIC CRITERIA. Lisa Joseph, Ph.D.
 AUTISM SPECTRUM DISORDER: DSM-5 DIAGNOSTIC CRITERIA Lisa Joseph, Ph.D. Autism Spectrum Disorder Neurodevelopmental disorder Reflects understanding of the etiology of disorder as related to alterations
AUTISM SPECTRUM DISORDER: DSM-5 DIAGNOSTIC CRITERIA Lisa Joseph, Ph.D. Autism Spectrum Disorder Neurodevelopmental disorder Reflects understanding of the etiology of disorder as related to alterations
6/22/2012. Co-morbidity - when two or more conditions occur together. The two conditions may or may not be causally related.
 Autism Spectrum Disorders and Co-existing Mental Health Issues By Dr. Karen Berkman Objective To present an overview of common psychiatric conditions that occur in persons with autism spectrum disorders
Autism Spectrum Disorders and Co-existing Mental Health Issues By Dr. Karen Berkman Objective To present an overview of common psychiatric conditions that occur in persons with autism spectrum disorders
GOALS FOR THE PSCYHIATRY CLERKSHIP
 GOALS FOR THE PSCYHIATRY CLERKSHIP GOALS - The aim of the core psychiatry clerkship is to expose students to patients with mental illness and to prepare them to provide psychiatric care at a basic level.
GOALS FOR THE PSCYHIATRY CLERKSHIP GOALS - The aim of the core psychiatry clerkship is to expose students to patients with mental illness and to prepare them to provide psychiatric care at a basic level.
FAMILY AND ADOLESCENT MENTAL HEALTH: THE PEDIATRICIAN S ROLE
 FAMILY AND ADOLESCENT MENTAL HEALTH: THE PEDIATRICIAN S ROLE Mark Cavitt, M.D. Medical Director, Pediatric Psychiatry All Children s Hospital/Johns Hopkins Medicine OBJECTIVES Review the prevalence of
FAMILY AND ADOLESCENT MENTAL HEALTH: THE PEDIATRICIAN S ROLE Mark Cavitt, M.D. Medical Director, Pediatric Psychiatry All Children s Hospital/Johns Hopkins Medicine OBJECTIVES Review the prevalence of
By Jason H. King DECONSTRUCTING THE DSM-5 ASSESSMENT AND DIAGNOSIS OF SCHIZOPHRENIA SPECTRUM DISORDERS THE NEW LANDSCAPE
 DECONSTRUCTING THE DSM-5 By Jason H. King ASSESSMENT AND DIAGNOSIS OF SCHIZOPHRENIA SPECTRUM DISORDERS Happy New Year as you engage in your counseling, research, supervision or educational endeavors. I
DECONSTRUCTING THE DSM-5 By Jason H. King ASSESSMENT AND DIAGNOSIS OF SCHIZOPHRENIA SPECTRUM DISORDERS Happy New Year as you engage in your counseling, research, supervision or educational endeavors. I
Rutgers University Course Syllabus Atypical Child and Adolescent Development Spring 2017
 Rutgers University Course Syllabus Atypical Child and Adolescent Development Spring 2017 Date & Time: Mon and Wedn. 5:00 6:20 pm Location: Tillett bldg. rm 232 Livingston Campus Instructor: Stevie M. McKenna
Rutgers University Course Syllabus Atypical Child and Adolescent Development Spring 2017 Date & Time: Mon and Wedn. 5:00 6:20 pm Location: Tillett bldg. rm 232 Livingston Campus Instructor: Stevie M. McKenna
Psychological Disorders: More Than Everyday Problems 14 /
 Psychological Disorders: More Than Everyday Problems 14 / Psychological Disorder(p.630) The presence of a constellation of symptoms that create significant distress; impair work, school, family, relationships,
Psychological Disorders: More Than Everyday Problems 14 / Psychological Disorder(p.630) The presence of a constellation of symptoms that create significant distress; impair work, school, family, relationships,
Psychotic disorders Dr. Sarah DeLeon, MD PGYIV, Psychiatry ConceptsInPsychiatry.com
 Psychotic disorders Dr. Sarah DeLeon, MD PGYIV, Psychiatry ConceptsInPsychiatry.com Introduction Psychotic spectrum disorders include schizotypal personality disorder, delusional disorder, brief psychotic
Psychotic disorders Dr. Sarah DeLeon, MD PGYIV, Psychiatry ConceptsInPsychiatry.com Introduction Psychotic spectrum disorders include schizotypal personality disorder, delusional disorder, brief psychotic
Rutgers University Course Syllabus Abnormal Psychology 01: 830: Spring 2017
 Rutgers University Course Syllabus Abnormal Psychology 01: 830: 340 - Spring 2017 Date & Time: Tuesday and Friday 10:20 11:40 AM Location: Tillett bldg. room 254 Livingston Campus Instructor: Stevie M.
Rutgers University Course Syllabus Abnormal Psychology 01: 830: 340 - Spring 2017 Date & Time: Tuesday and Friday 10:20 11:40 AM Location: Tillett bldg. room 254 Livingston Campus Instructor: Stevie M.
Deconstructing the DSM-5 By Jason H. King
 Deconstructing the DSM-5 By Jason H. King Assessment and diagnosis of sleep-wake disorders According to Arline Kaplan s article Catching up on sleep: From comorbidity to pharmacotherapy that appeared in
Deconstructing the DSM-5 By Jason H. King Assessment and diagnosis of sleep-wake disorders According to Arline Kaplan s article Catching up on sleep: From comorbidity to pharmacotherapy that appeared in
How to Win Friends and Influence People Lesson 6 Psychological Patterns and Disorders
 How to Win Friends and Influence People Lesson 6 Psychological Patterns and Disorders What are psychological disorders? Mental health workers view psychological disorders as ongoing patterns of thoughts,
How to Win Friends and Influence People Lesson 6 Psychological Patterns and Disorders What are psychological disorders? Mental health workers view psychological disorders as ongoing patterns of thoughts,
substance use and mental disorders: one, the other, or both?
 substance use and mental disorders: one, the other, or both? Stephen Strobbe, PhD, RN, PMHCNS-BC, CARN-AP Dawn Farm Education Series St. Joe s Education Center, Ypsilanti, MI Tuesday, January 27, 2015
substance use and mental disorders: one, the other, or both? Stephen Strobbe, PhD, RN, PMHCNS-BC, CARN-AP Dawn Farm Education Series St. Joe s Education Center, Ypsilanti, MI Tuesday, January 27, 2015
Fall 2013 Upcoming Workshops:
 Fall 2013 Upcoming Workshops: September 4, 2013 Similarities and Differences between DSM IV TR and DSM V: Part 1 This workshop examines the major changes that have occurred from DSM IV TR to DSM V. The
Fall 2013 Upcoming Workshops: September 4, 2013 Similarities and Differences between DSM IV TR and DSM V: Part 1 This workshop examines the major changes that have occurred from DSM IV TR to DSM V. The
Accurate Diagnosis of Primary Psychotic Disorders
 Accurate Diagnosis of Primary Psychotic Disorders The Care Transitions Network National Council for Behavioral Health Montefiore Medical Center Northwell Health New York State Office of Mental Health Netsmart
Accurate Diagnosis of Primary Psychotic Disorders The Care Transitions Network National Council for Behavioral Health Montefiore Medical Center Northwell Health New York State Office of Mental Health Netsmart
DSM-5 UPDATE FOR COUNSELORS THE PROCRASTINATOR S GUIDE. Aaron Norton, LMHC, LMFT, MCAP, CRC, CFMHE
 1 DSM-5 UPDATE FOR COUNSELORS THE PROCRASTINATOR S GUIDE Aaron Norton, LMHC, LMFT, MCAP, CRC, CFMHE About the Presenter 2 Mr. Norton is a Licensed Mental Health Counselor, Licensed Marriage & Family Therapist,
1 DSM-5 UPDATE FOR COUNSELORS THE PROCRASTINATOR S GUIDE Aaron Norton, LMHC, LMFT, MCAP, CRC, CFMHE About the Presenter 2 Mr. Norton is a Licensed Mental Health Counselor, Licensed Marriage & Family Therapist,
WORKBOOK ANSWERS CHAPTER 14 MENTAL DISORDERS
 WORKBOOK ANSWERS CHAPTER 14 MENTAL DISORDERS 1. POSTTRAUMATIC STRESS DISORDER SHORT ANSWERS 2. ALZHEIMER DISEASE 3. STRESS IS CONSIDERED A CONTRIBUTING FACTOR CAUSING EXACERBATION OF MENTAL DISORDERS.
WORKBOOK ANSWERS CHAPTER 14 MENTAL DISORDERS 1. POSTTRAUMATIC STRESS DISORDER SHORT ANSWERS 2. ALZHEIMER DISEASE 3. STRESS IS CONSIDERED A CONTRIBUTING FACTOR CAUSING EXACERBATION OF MENTAL DISORDERS.
Rutgers University Course Syllabus Atypical Child and Adolescent Development Fall 2016
 Rutgers University Course Syllabus Atypical Child and Adolescent Development Fall 2016 Date & Time: Mon and Wedn. 1:40 3:00 pm Location: Pharm. Rm 111 Busch Campus Instructor: Stevie M. McKenna MA E-Mail:
Rutgers University Course Syllabus Atypical Child and Adolescent Development Fall 2016 Date & Time: Mon and Wedn. 1:40 3:00 pm Location: Pharm. Rm 111 Busch Campus Instructor: Stevie M. McKenna MA E-Mail:
True or False? Chapter 14 Psychological Disorders. What is Abnormal Behavior? 12/9/10. Characteristics of Abnormal Behavior
 Chapter 14 Psychological Disorders Defining Abnormality Classifying Psychological Disorders Origins of Psychological Disorders True or False? Abnormal behaviors are always bizarre. A clear distinction
Chapter 14 Psychological Disorders Defining Abnormality Classifying Psychological Disorders Origins of Psychological Disorders True or False? Abnormal behaviors are always bizarre. A clear distinction
Other Disorders Myers for AP Module 69
 1 Other s Myers for AP Module 69 Describe the general characteristics of somatic symptom disorders. How does culture influence people s expression of physical complaints? Compare the symptoms of conversion
1 Other s Myers for AP Module 69 Describe the general characteristics of somatic symptom disorders. How does culture influence people s expression of physical complaints? Compare the symptoms of conversion
CUA. THE CATHOLIC UNIVERSITY OF AMERICA National Catholic School of Social Service Shahan Hall Washington, DC Fax
 1 CUA THE CATHOLIC UNIVERSITY OF AMERICA National Catholic School of Social Service Shahan Hall Washington, DC 20064 202-319-5458 Fax 202-319-5093 SSS 572 Human Development and Psychopathology Spring 2009
1 CUA THE CATHOLIC UNIVERSITY OF AMERICA National Catholic School of Social Service Shahan Hall Washington, DC 20064 202-319-5458 Fax 202-319-5093 SSS 572 Human Development and Psychopathology Spring 2009
AMERICAN BOARD OF PSYCHIATRY AND NEUROLOGY, INC. PART I EXAMINATION IN PSYCHIATRY A AND B 2013 Content Outline
 253 questions Percent Part A: Basic Concepts in Psychiatry I. Development through the life cycle 9% A. Infancy through adolescence 1. Personality development (e.g., moral development) 2. Developmental
253 questions Percent Part A: Basic Concepts in Psychiatry I. Development through the life cycle 9% A. Infancy through adolescence 1. Personality development (e.g., moral development) 2. Developmental
 Psychopathology Psychopathy (con t) Psychopathy Characteristics High impulsivity Thrill seeking Low empathy Low anxiety What is the common factor? Callous Self-Centeredness N M P Dr. Robert Hare
Psychopathology Psychopathy (con t) Psychopathy Characteristics High impulsivity Thrill seeking Low empathy Low anxiety What is the common factor? Callous Self-Centeredness N M P Dr. Robert Hare