Chronic Traumatic Encephalopathy
|
|
|
- Stella Poole
- 6 years ago
- Views:
Transcription
1 Chronic Traumatic Encephalopathy Sandeep Gupta MD PGY-4 Clinical Instructor House Staff, Department of Psychiatry The Ohio State Wexner Medical Center 01/09/13

2 Objectives 1. Examine history of disorder now referred to as CTE and previous nomenclature and descriptions. 2. Detail the stereotypic macroscopic and microscopic changes associated with CTE. 3. Discuss clinical manifestations of CTE, specifically in regards to mood and behavioral changes. 4. Describe more specific incidences of CTE in professional athletes and associated signs/symptoms. 5. Briefly

3 Jacked Up
4 History of Diagnosis The first known mention of neuropsychiatric deficits associated with head injuries seems to date back to the very late 1800 s. In 1893, a U.S. Navy football player (Joseph M. Reeves) was warned by a Navy doctor that another blow to the head could cause instant insanity or death. Reeves, instead of heeding the doctor s advice, paid a shoemaker to construct the first football helmet of leather in order to play in Army-Navy game. In 1912 Glenn Pop Warner stated Playing without helmets gives players more confidence, saves their heads many hard jolts, and keeps their ears from becoming torn or sore. I do not encourage their use. I have never seen an accident to the head which was serious, but I have many times seen cases when hard bumps on the head so dazed the player receiving them that he lost his memory for a time and had to be removed from the game. In the 1920 s there were the beginnings of reports of neurologic deterioration associated with repetitive brain trauma, specifically as it related to the sport of boxing- hence, the term dementia pugilistica.
5 History of Diagnosis The syndrome was first formally described in literature in 1928 by Dr. Harrison Stanford Martland with an article titled Punch Drunk 1. Some time fight fans and promoters have recognized a peculiar condition occurring among prize fighters which, in ring parlance, they speak of as "punch drunk." Fighters in whom the early symptoms are well recognized are said by the fans to be "cuckoo," "goofy," "cutting paper dolls," or "slug nutty." Frequently it takes a fighter from one to two hours to recover from a severe blow to the head or jaw. He outlined early symptoms as a mild tremor of the extremities, a slowing of all motor function, confusion, and speech problems (slurring of words).
6 History of Diagnosis A 1956 study examined the pathology of closed head injury patients who never regained full level of consciousness but lived for between five to fifteen months (defined as without skull fracture, intracranial hematoma, brain lacerations, or signs of elevated intracranial pressure) 2. Microscopic examination of brain tissue showed diffuse degeneration of white matter throughout cerebral hemispheres without fibrosis or destruction of remaining nerve fibers or myelin sheaths. There were noted to be specific areas of more severe volume loss including around ventricles, internal capsule, and thalamus. Important to study was fact that dementia-like states of these patients were differentiated from previously described loss of consciousness/comatose states with head injuries of various types along with histologic differentiation that this was not a result of damage to cerebral cortex, infarction, or laceration but rather a degeneration of white matter.
7 History of Diagnosis In 1969, A.H. Roberts studied the cognitive functioning of 224 former boxers and found that 17% of them suffered from significant memory loss, aggression, confusion, or depression (at that time termed just traumatic encephalopathy) and that there was direct correlation of incidence to number of fights and overall length of boxing career 3. In 1973, general term for syndrome changed from DP to CTE as a result of study by JA Corsellis et al which histologically analyzed the brains of 15 former boxers who had been diagnosed with Dementia Pugilistica and found that all showed some common characteristics: cavum septum (ranging from 1-8mm, strained thin dorsal attachment), scarring of cerebellum, degeneration of substantia nigra, and presence of neurofibrillary tangles (specifically in hippocampus and medial temporal gray matter).
8
9 History of Diagnosis In the early 1990 s, researchers used an antibody to the beta-protein known to be present in AD plaques and found similar levels of beta protein deposition in symptomatic retired boxers 5. Tokuda et al found that there were tau immunoreactive neurofibrillary tangles in addition to the beta-protein deposits 6. Dale et al proved histologically that there was ubiquitin present in the NF tangles of both boxers with clinical signs of dementia and patients with AD 7.


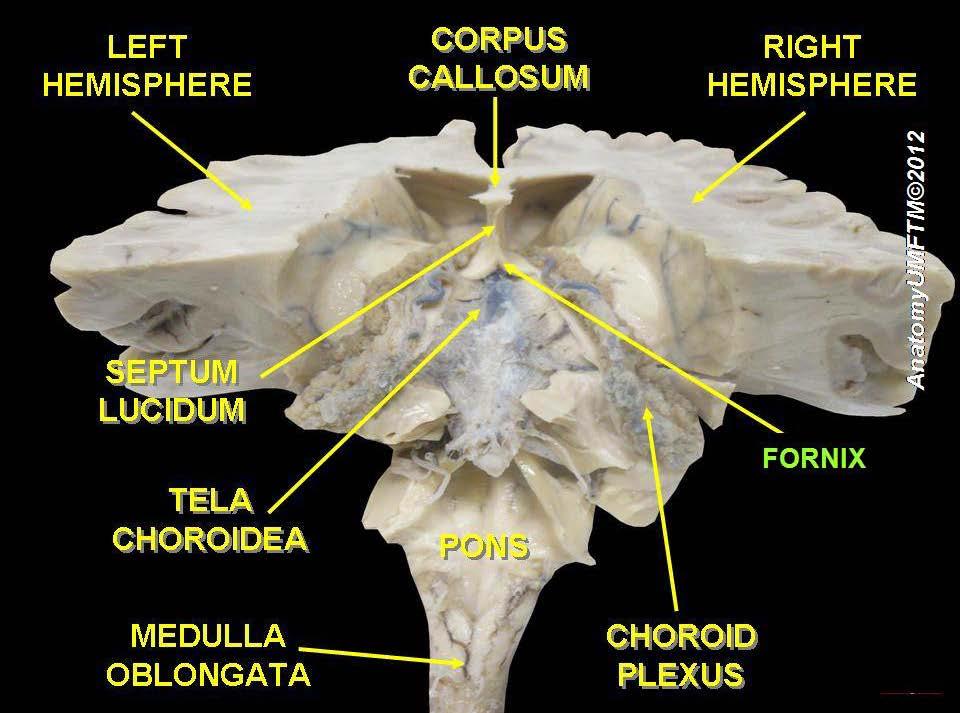
10 Macroscopic Pathology in CTE Overall reduction in brain weight- more specifically atrophy of the medial temporal lobe as well as temporal and frontal cortices

11 Stereotypic Pathology in CTE Enlargement of third and lateral ventricles Cavum septum pellucidum Atrophy of mammilary bodies, olfactory bulbs, thalamus Depigmentation or pallor of substantia nigra and locus ceruleus Scarring and decreased number of Purkinje cells in inferior region of cerebellum Atrophy of hippocampus, amygdala noted in severe cases

12 Stereotypic Pathology in CTE


13 Microscopic Pathology in CTE Tau immunoreactive neurofibrillary tangles in irregular pattern of deposition- most often closer to superficial cortex (as compared to AD) and concentrated in perivascular regions 7. Also a higher concentration of NFT s in basal region of brain, especially in depths of sulci.

14 Microscopic Pathology in CTE In advanced cases, these tau immunoreactive NFT s are also found in limbic areas, brainstem, and subcortical white matter. Unlike plaques in Alzheimer s dementia, there is much lower incidence of Beta-amyloid protein deposits in cases of CTE 10. In addition, higher levels of hyper-phosphorylated, ubiquinated TAR DNA binding protein 43(TDP-43) are found in brainstem, basal ganglia, medial temporal lobe, frontal, temporal, and insular cortices. TDP-43 binds to neurofilament mrna and plays a major role in stabilizing mrna transcription and mediating the response of neuronal cytoskeleton to axonal injury. Hyperphosphorylation of TDP-43 results in NFT s in a similar helical process to tau proteinopathy.
15 Microscopic Pathology in CTE Recent evidence shows that TDP-43 proteinopathy develops at a very early stage in the course, as revealed by presence in post-portem analyses of brains of 18 y/o high school student with history of multiple concussions who died suddenly of other causes but had experienced CTE symptoms 16, and 26 year old Chris Henry(former Cincinnati Bengals WR) who died after falling from the back of a truck but was still active in the NFL at the time of his death 17. If significant levels of pathologic TDP-43 accumulate in the anterior horns of spinal cord and motor cortex, the result is corticospinal tract degeneration which appears clinically similar to ALS- weakness, spasticity, fasciculations, and muscular atrophy 10.

16 Microscopic Pathology in CTE TDP-43 proteinopathy has previously been found in patients with ALS and FTLD, indicating that CTE may share similar pathogenic mechanisms 15. Other recent studies have shown that brains of patients with a single TBIboth in acute and long-term recovery phase- do not show evidence of TDP-43 proteinopathy 14. Figure 7. TDP-43 in FTLD-U and ALS. This figure shows the different cellular distribution of TDP-43 in normal cells (top) as opposed to neuronal cells from patients affected by FTLD-U or ALS (bottom). In these patients, no wild type TDP-43 protein can be found within the nucleus and all the pool of intracellular TDP-43 can be found accumulating in the cytoplasm. The modifications to which this cytoplasmic TDP-43 has been subjected include hyperphosphorylation, ubiquitination, and cleavage to generate C-terminal fragments 18.
17 The four histologic stages of CTE Stage 1- pathology restricted to discrete foci in cerebral cortex, most commonly in the dorsolateral and lateral prefrontal cortices and specifically around small blood vessels at depths of sulci Stage 2- multiple pathologic sites in similar distribution but with associated spread of pathology to adjacent superficial cortex but, by definition, with no involvement of medial temporal lobe Stage 3- Widespread pathology with highest concentration of neurofibrillary degeneration in frontal, temporal, insular, and parietal cortices along with NFT s in hippocampus and amygdala Stage 4- Severe pathology affecting the majority of cerebral cortex


18
19 Lack of clear clinical stages/criteria Mckee et al proposed in 2009 a three tier model of staging CTE 10 -Stage 1 involved affective changes and psychotic symptoms -Stage 2 described also social instability, erratic behavior, memory loss, and motor symptoms similar to early Parkinson s -Stage 3 was progressive deterioration into dementia-like clinical picture along with Parkinsonian symptoms of dysarthria, dysphagia, shuffling gait, and ptosis However, still no accepted consensus among providers as to consistent method
20 Clinical Progression of CTE Earliest features tend to be deficits in attention and concentration, memory, mild disorientation and confusion, as well as headaches and dizziness. Progression involves worsening hypofrontality and degeneration of prefrontal cortex influencing mood regulation, poor decision-making, planning, and impulsivity/aggression as well as worsening dementia(global cognition) More severe cases show slowing of motor function, shuffling gait, masked facies, dysarthria, tremor, and deafness
21 Mood and Behavioral Symptoms Most commonly described associated symptoms have been depression(thought to be more refractory to treatment), apathy, mood instability, impulsivity, as well as a significantly higher incidence of substance abuse and suicidality. 11 A review was done in 2009 of the cases of 51 patients with confirmed neuropathologic changes associated with CTE to assess correlation with clinical features. It was found that in fourteen(30%) of the cases, there was documentation of concern for mood illness, with large majority being depression and one case with description of euphoric dementia. Two of the cases of depression also involved manic symptoms and these patients were described as either manic-depressive or bipolar. 10,12,13 Motor abnormalities were described in cases of 21(42%) of these patients including Parkinsonism, staggered, slowed or shuffling gait, slowed or slurred speech, ataxia, dysphagia, and ocular abnormalities and in no cases was there described any clinical course other than progressive worsening of symptoms.
22 Mood and Behavioral Symptoms Pathologic mechanism of mood and behavioral symptoms most likely related to significant degeneration of dorsolateral prefrontal cortex(dlpfc), amygdala, and hippocampus. DLPC is highest cortical area involved in planning, organization, regulation/inhibition, integration of sensory information, regulation of attention and action, as well as working memory. Involvement of dorsal frontal cortex as opposed to more ventral areas helps explain more specific deficits with processing of memorized material as opposed to direct deficits of storage/recall of factual information.

23 Mood and Behavioral Symptoms Amygdala specifically involved in emotional and social awareness and processing- specifically as they pertain to fear and pleasure responses. Abnormal functioning of the amygdala has been correlated with autism, PTSD, all anxiety conditions, violent behavior, antisocial personality disorder, and unipolar depression. Interestingly, there has been evidence of hyperactive amygdalae in patients with bipolar I disorder- high incidence of paranoia.
, 1 professional wrestler, and 1 soccer player.")
 with average age of 43 years old.")
24 Post-mortem study of 51 patients with neuropathologic CTE Of the 51 confirmed cases of CTE studied, 46(90%) were athletes- more specifically, there were 39 boxers(amateur or professional), 5 football players(average involvement time of 18 years), 1 professional wrestler, and 1 soccer player. Interestingly, one of non-athletes worked as a circus clown and others were either victims of physical abuse or patients with epilepsy 10. There was a wide range in reported age of initial onset of symptoms(25-78) with average age of 43 years old. At the time that these athletes retired from their playing careers, one-third already demonstrated clinical features of CTE and within four years after stopping, one-half of the sample group was experiencing symptoms.
25 Focus on Football Sport Science: Concussions
26 Five cases of former football players Extremely small sample size but limited available data Sample group of football players died at a younger age(range of years old at death with mean of 44) as compared to the group of former boxers(range of with mean of 60) 10. All five football players played positions which, by nature, involve a high volume of repetitive impacts including three offensive linemen, one defensive lineman, and one linebacker 10. 4/5 players had symptoms of depression, memory loss, paranoia, and poor insight/judgment noted. 3/5 had outbursts of anger or aggression, irritability, and apathy. 2/5 had confusion, hyperreligiosity, reduced concentration
27 Five cases of former football players Out of the five players, only one experienced a death that could easily be deemed unrelated to CTE(had severe CAD) as two committed suicide, one died during a high speed police chase, and the fifth described below died from what was deemed as an accidental gunshot wound to the chest while cleaning a gun 10. Example is case of a 45 year old retired NFL linebacker who was described by his wife to have had at least three concussions during college career and at least eight concussions during NFL career(only one documented in medical chart review) but without any instances of losing consciousness for more than 1-2 seconds, being carried off the field, seeking treatment or requiring hospitalization for cognitive or behavioral deficits 10. Around age 40, family noticed impairments in his short-term memory, attention, concentration, organization, planning, problem-solving, judgment, and multi-tasking ability. Language skills were unaffected and he continued to work as a hunting/fishing guide until time of death. However, towards the end of his life, family describes anger, verbal aggression, emotional lability, and alcohol abuse 10.
28 Football and Closed Head Trauma It has been estimated that, during a course of a college football season, linemen in particular can experience up to 1500 subconcussive head impacts while some high school players(who play both offense and defense) may experience upwards of 2000 of these collisions 19. A research study recorded data about 300,000 head impacts by implanting a sensor in helmets. It showed that while quarterbacks and running backs suffered the most severe blows to the head, linebackers as well as offensive and defensive linemen experience a significantly higher volume of head impacts than any other position. Data indicated that hits to the top of the head carried greater risk of concussion than hits to back front, or lateral areas.


29 Dr. Bennet Omalu Forensic pathologist who happened to be working in Pittsburgh when bodies of former Steelers Mike Webster and Terry Long came in for autopsy. After discovering similar anatomic abnormalities, he sought out brain tissue from other athletes including former NFL players and professional wrestler Chris Benoit and found these same brain changes. He authored recent book titled Play Hard, Die Young: Football, Dementia, Depression, and Death.

30 Mike Webster( ) NFL Hall of Fame Center(played ) Nicknamed Iron Mike for never missing plays Experienced severe decline of cognitive functioning as well as behavioral and personality changes after retirement from football. His son described an incident during a family dinner when his father got up from eating the meal, walked around in a confused fashion, opened up the oven door and urinated in the oven. His son also describes the family having to always a have a specific flag on the porch outside their home so Mike would recognize the house. In his last years of life, he exhibited extreme paranoia, resulting in the ending of his marriage and him living homeless for periods of time, refusing the help of friends and family 22. He eventually passed away as a direct result of a heart attack.




31 Dave Duerson( ) NFL safety from Dave Duerson Video After retirement, he built a very successful food services company before he began experiencing symptoms of CTE per family. Per family members, Duerson experienced severe memory loss, poor impulse control, and displayed abusive behavior towards family and employees, leading to the collapse of the business, declaration of bankruptcy, ending of his marriage. He later completed suicide by gunshot wound to the chest. This case was particularly prominent in media due to Duerson s role on NFL s six- person committee which decided disability claims filed by former NFL players, his growing concern that his own struggles may have been a result of football-related injuries, and text message to family that his brain be studied by Boston University s Center for the Study of Traumatic Encephalopathy, which, after biopsy, confirmed diagnosis of CTE.

32 Chris Henry( ) Chris Henry John Lynch NFL WR from when he passed away in tragic accident after he fell from back of a pickup truck driven by his fiancee as she attempted to drive away following a domestic dispute. In the last four years of his life, Henry was arrested more than five times on a variety of charges including aggravated assault with a firearm, driving while intoxicated, supplying alcohol to underage females at a hotel, and multiple assault and battery charges. His brain was studied by the Brain Injury Research Institute at West Virginia University and he was found to have CTE. He was the first still-active NFL player to be diagnosed with CTE. He had never been formally been diagnosed with concussion throughout college and NFL playing career.


33 Relevant stories of other Professional Athletes Chris Benoit( )- Professional wrestler who placed copies of Bible alongside bodies of wife and son after strangling them and then hanging himself. His brain was tested and showed signs of CTE. Neurosurgeon Julian Bailes commented Benoit s brain was so severely damaged it resembled the brain of an 85 year old Alzheimer s patient. 23 Bob Probert( )- NHL player infamous for fighting and being an enforcer. He was arrested in 2004 after getting into physical altercation over drugs but police had to use tasers and stun guns to subdue him. In 2005, he was arrested for breach of peace, resisting arrest, and assaulting a police officer. After death from cardiac arrest in 2010, his brain was studied at Boston University and showed evidence of CTE.
34 Future of Research With similarities in protein deposition between CTE, AD, FTD, and ALS, what role does head trauma play in the development of all of these disorders?- Similarities/differences What can be done to prevent damage associated with repetitive head trauma(helmets, banning of certain types of impact, age limits on certain sports, rules on return to sport after known head injury)? Is there a way to design studies of at-risk persons currently in regards to specific symptoms and follow them longitudinally to better be able to identify odds ratios to help provide guidance with risk analysis regarding retirement?
35 References 1, Martland HS. Punch Drunk. JAMA. 1928;91(15): Strich, Sabina J. Diffuse Degeneration of the Cerebral White Matter in Severe Dementia Following Head Injury. Journal of Neurology, Neurosurgery, and Psychiatry, 1956, 19, Roberts, Anthony Herbers. Brain Damage in Boxers: A study of the prevalence of traumatic encephalopathy among ex-professional boxers. London: Pitman Medical & Scientific Publishing Co., Ltd., Corsellis JA, Bruton CJ, Freeman-Browne D. "The Aftermath of Boxing." Psychology Medicine (1973) Aug;3(3): Roberts GW, Allsop D. Bruton C. The occult aftermath of boxing. J Neurol Neurosurg Psychiatry 1990;53: Tokuda T, Ikeda S, Yanugesa N, et al. Re-examination of ex-boxer's brain using immunohistochemistry with antibodies to amyloid beta protein and tau protein. Acta Neuropathol 1991;82: Dale GE, Leigh PN, Luthert P, et al. Neurofibrillary tangles in dementia pugilistica are ubiquitinated. J Neurol Neurosurg Psychiatry 1991;54: Geddes JF, Vowles GH, Nicoll JA, et al. Neuronal cytoskeletal changes are an early consequence of repetitive head injury. Acta Neuropathol. 1999;98: Lakhan S, Kirchgessner A.Chronic traumatic encephalopathy: the dangers of getting dinged. SpringerPlus 2012, 1:2 doi: / McKee AC, Cantu RC, Nowinski CJ, et al. Chronic traumatic encephalopathy in athletes: Progressive tauopathy after repetitive head injury. J Neuropathol Exp Neurol 2009;68:
36 References 11. Stern RA, Riley DO, Daneshvar DH, Nowinski CJ, Cantu RC, McKee AC. Long-term consequences of repetitive brain trauma: chronic traumatic encephalopathy PM R 3:S460-S Payne EE. Brains of boxers. Neurochirurgia (Stuttg) 1968;11: Schwarz A. Lineman, dead at 36, exposes brain injuries [New York Times Web site] June Johnson VE, Stewart W, Trojanowski JQ, Smith DH. Acute and chronically increased immunoreactivity to phosphorylationindependent but not pathological TDP-43 after a single traumatic brain injury in humans. ActaNeuropathol 201;122: Geser F, Lee VM, Trojanowski JQ Amylotrophic lateral sclerosis and frontotemporal lobar degeneration: a spectrum of TDP-43 proteinopathies. Neuropathology 2010;30(103-12). 16. Omalu B. Emerging histomorphologic phenotypes of chronic traumatic encephalopathy (CTE) in American athletes- Case 15. Neurosurgery (1): Schwarz, Alan (June 28, 2010). "Former Bengal Henry Found to Have Had Brain Damage". New York Times. 18. Buratti E, Baralle F. Multiple roles of TDP-43 in gene expression, splicing regulation, and human disease. Frontiers in Bioscience 13, , January 1, Owen AM. "The functional organization of working memory processes within human lateral frontal cortex: the contribution of functional neuroimaging". The European Journal of Neuroscience July 1997; 9 (7): Crisco JJ, Fiore R, Beckwith JG, Chu JJ, Brolinson PG, Duma S, McAllister TW, Duhaime AC, Greenwald RM. Frequency and location of head impact exposures in individual collegiate football players. J Athl Train 2010;45:
37 References 21. Guskiewicz KM, Mihalik JP, Shankar V, Marshall SW, Crowell DH, Oliaro SM, Ciocca MF, Hooker DN. Measurement of head impacts in collegiate football players: relationship between head impact biomechanics and acute clinical outcome after concussion. Neurosurgery 2007; 61: Krieger D. Paying heavy price for glory on Sundays. Rocky Mountain News. January 22, Benoit's Brain Showed Severe Damage From Multiple Concussions, Doctor and Dad Say". ABCNEWS. Retrieved
the injured brain, the injured mind.
 the injured brain, the injured mind. mary et boyle, ph.d. department of cognitive science ucsd Traumatic Brain Injury (TBI) is caused by a bump, blow or jolt to the head or a penetrating head injury the
the injured brain, the injured mind. mary et boyle, ph.d. department of cognitive science ucsd Traumatic Brain Injury (TBI) is caused by a bump, blow or jolt to the head or a penetrating head injury the
A Critical Review of Chronic Traumatic Encephalopathy
 A Critical Review of Chronic Traumatic Encephalopathy Grant L. Iverson, Ph.D. Professor, Department of Physical Medicine and Rehabilitation, Harvard Medical School; Director, MassGeneral Hospital for Children
A Critical Review of Chronic Traumatic Encephalopathy Grant L. Iverson, Ph.D. Professor, Department of Physical Medicine and Rehabilitation, Harvard Medical School; Director, MassGeneral Hospital for Children
Chronic Traumatic Encephalopathy Provider and Parent Essentials
 Chronic Traumatic Encephalopathy Provider and Parent Essentials Concussion Global Cast July 30, 2014 John Lockhart, MD Seattle Children s Hospital Chronic Traumatic Encephaly (CTE) Working Definition Chronic
Chronic Traumatic Encephalopathy Provider and Parent Essentials Concussion Global Cast July 30, 2014 John Lockhart, MD Seattle Children s Hospital Chronic Traumatic Encephaly (CTE) Working Definition Chronic
Sports Concussion: What Do We Really Know?
 Sports Concussion: What Do We Really Know? Anthony G. Alessi MD, FAAN Director, UConn NeuroSport October 17, 2018 Overview Significance Diagnosis Sideline diagnosis v Management Concussion Tools Return-to-Play
Sports Concussion: What Do We Really Know? Anthony G. Alessi MD, FAAN Director, UConn NeuroSport October 17, 2018 Overview Significance Diagnosis Sideline diagnosis v Management Concussion Tools Return-to-Play
DVHIP. TBI: Clinical Issues, Controversies, and Learning from Patients. Defense and Veterans Head Injury Program. What is Neuropsychology?
 TBI: Clinical Issues, Controversies, and Learning from Patients DVHIP Defense and Veterans Head Injury Program Richard A. Lanham, Jr., Ph.D. Assistant Professor Division of Medical Psychology Psychiatry
TBI: Clinical Issues, Controversies, and Learning from Patients DVHIP Defense and Veterans Head Injury Program Richard A. Lanham, Jr., Ph.D. Assistant Professor Division of Medical Psychology Psychiatry
Plan for Today. Brain Injury: 8/4/2017. Effective Services for People Living with Brain Injury. What is it & what causes it?
 Effective Services for People Living with Brain Injury Jean Capler, MSW, LSW Local Support Network Leader The Rehabilitation Hospital of Indiana Department of Resource Facilitation Plan for Today Brain
Effective Services for People Living with Brain Injury Jean Capler, MSW, LSW Local Support Network Leader The Rehabilitation Hospital of Indiana Department of Resource Facilitation Plan for Today Brain
The Changing Landscape of Sports Concussions
 The Changing Landscape of Sports Concussions Anthony G. Alessi MD, FAAN Director, UConn NeuroSport Sports Medicine Symposium August 2, 2016 Overview Significance Diagnosis Sideline diagnosis v Management
The Changing Landscape of Sports Concussions Anthony G. Alessi MD, FAAN Director, UConn NeuroSport Sports Medicine Symposium August 2, 2016 Overview Significance Diagnosis Sideline diagnosis v Management
Chronic traumatic encephalopathy: Emerging Concepts
 Chronic traumatic encephalopathy: Emerging Concepts Ann C. McKee M.D. Professor of Neurology and Pathology VA Boston Healthcare System Boston University School of Medicine Director of the CTE Center Boston
Chronic traumatic encephalopathy: Emerging Concepts Ann C. McKee M.D. Professor of Neurology and Pathology VA Boston Healthcare System Boston University School of Medicine Director of the CTE Center Boston
Mild Traumatic Brain Injury
 Mild Traumatic Brain Injury Concussions This presentation is for information purposes only, not for any commercial purpose, and may not be sold or redistributed. David Wesley, M.D. Outline Epidemiology
Mild Traumatic Brain Injury Concussions This presentation is for information purposes only, not for any commercial purpose, and may not be sold or redistributed. David Wesley, M.D. Outline Epidemiology
TRAUMATIC BRAIN INJURY: CHRONIC TRAUMATIC ENCEPHALOPATHY
 TRAUMATIC BRAIN INJURY: CHRONIC TRAUMATIC ENCEPHALOPATHY Lasting Impacts of mtbi Global EOD Symposium and Exposition 2018 Alexandra M Bradley, MALS, MCHES, ATC Client Informatics Consultant Veterans CRG
TRAUMATIC BRAIN INJURY: CHRONIC TRAUMATIC ENCEPHALOPATHY Lasting Impacts of mtbi Global EOD Symposium and Exposition 2018 Alexandra M Bradley, MALS, MCHES, ATC Client Informatics Consultant Veterans CRG
REVIEW. Montenigro et al. Alzheimer's Research & Therapy 2014, 6:68
 Montenigro et al. Alzheimer's Research & Therapy 2014, 6:68 REVIEW Clinical subtypes of chronic traumatic encephalopathy: literature review and proposed research diagnostic criteria for traumatic encephalopathy
Montenigro et al. Alzheimer's Research & Therapy 2014, 6:68 REVIEW Clinical subtypes of chronic traumatic encephalopathy: literature review and proposed research diagnostic criteria for traumatic encephalopathy
The ABCs of Dementia Diagnosis
 The ABCs of Dementia Diagnosis Dr. Robin Heinrichs, Ph.D., ABPP Board Certified Clinical Neuropsychologist Associate Professor, Psychiatry & Behavioral Sciences Director of Neuropsychology Training What
The ABCs of Dementia Diagnosis Dr. Robin Heinrichs, Ph.D., ABPP Board Certified Clinical Neuropsychologist Associate Professor, Psychiatry & Behavioral Sciences Director of Neuropsychology Training What
IT S ALL IN YOUR HEAD!
 IT S ALL IN YOUR HEAD! CARING FOR CONCUSSIONS IN YOUR COMMUNITY Stephen K Stacey, DO CPT, MC, USA OUTLINE Definition Epidemiology Diagnosis Evaluation Recovery Sequelae Prevention Resources for providers
IT S ALL IN YOUR HEAD! CARING FOR CONCUSSIONS IN YOUR COMMUNITY Stephen K Stacey, DO CPT, MC, USA OUTLINE Definition Epidemiology Diagnosis Evaluation Recovery Sequelae Prevention Resources for providers
The Dangers of CTE. James Ryan Cox. Skylar Spriggs. Sawyer Solfest. Team THS131
 The Dangers of CTE James Ryan Cox Skylar Spriggs Sawyer Solfest Team THS131 Dec 10th, 2017 The human body works alike to a well-oiled machine, each vital organ working as a valuable gear or cog. Yet if
The Dangers of CTE James Ryan Cox Skylar Spriggs Sawyer Solfest Team THS131 Dec 10th, 2017 The human body works alike to a well-oiled machine, each vital organ working as a valuable gear or cog. Yet if
The Person: Dementia Basics
 The Person: Dementia Basics Objectives 1. Discuss how expected age related changes in the brain might affect an individual's cognition and functioning 2. Discuss how changes in the brain due to Alzheimer
The Person: Dementia Basics Objectives 1. Discuss how expected age related changes in the brain might affect an individual's cognition and functioning 2. Discuss how changes in the brain due to Alzheimer
Lecture 13. The Nervous System. Lecture 13
 Lecture 13 The Nervous System Lecture 13 1. Introduction 2. Functions of the Nervous System 3. Neurons 4. CNS Brain and Spinal Cord 5. Peripheral Nervous System 6. Nervous System Health Concerns 1 The
Lecture 13 The Nervous System Lecture 13 1. Introduction 2. Functions of the Nervous System 3. Neurons 4. CNS Brain and Spinal Cord 5. Peripheral Nervous System 6. Nervous System Health Concerns 1 The
Concussion Update and Case Presentations
 Concussion Update and Case Presentations Cayce Onks, DO, MS, ATC Associate Professor Primary Care Sports Medicine Penn State Concussion Program Departments of Family Medicine and Orthopaedics I have no
Concussion Update and Case Presentations Cayce Onks, DO, MS, ATC Associate Professor Primary Care Sports Medicine Penn State Concussion Program Departments of Family Medicine and Orthopaedics I have no
8/24/18. Dementia. Risk of Dementia Following Traumatic Brain Injury: A Review of the Literature. Media Presence. Media Presence
 Risk of Dementia Following Traumatic Brain Injury: A Review of the Literature Media Presence Carlos Marquez de la Plata, Ph.D. & Jeff Schaffert, M.S. Media Presence Dementia What is dementia? Dementia
Risk of Dementia Following Traumatic Brain Injury: A Review of the Literature Media Presence Carlos Marquez de la Plata, Ph.D. & Jeff Schaffert, M.S. Media Presence Dementia What is dementia? Dementia
Pathogenesis of Degenerative Diseases and Dementias. D r. Ali Eltayb ( U. of Omdurman. I ). M. Path (U. of Alexandria)
. M. Path (U. of Alexandria)") Pathogenesis of Degenerative Diseases and Dementias D r. Ali Eltayb ( U. of Omdurman. I ). M. Path (U. of Alexandria) Dementias Defined: as the development of memory impairment and other cognitive deficits
Pathogenesis of Degenerative Diseases and Dementias D r. Ali Eltayb ( U. of Omdurman. I ). M. Path (U. of Alexandria) Dementias Defined: as the development of memory impairment and other cognitive deficits
Dhiren J. Naidu MD FRCPC Dip. Sport Med.
 Dhiren J. Naidu MD FRCPC Dip. Sport Med. Associate Professor, Division of Physical Medicine & Rehabilitation Faculty of Medicine & Dentistry Varsity Health, University of Alberta Team Physician - Oilers,
Dhiren J. Naidu MD FRCPC Dip. Sport Med. Associate Professor, Division of Physical Medicine & Rehabilitation Faculty of Medicine & Dentistry Varsity Health, University of Alberta Team Physician - Oilers,
It s better to miss one game than the whole season. What should I do if I think I have a concussion? Concussion facts:
 Concussion facts: A concussion is a brain injury that affects how your brain works. A concussion is caused by a bump, blow, or jolt to the head or body. A concussion can happen even if you haven t been
Concussion facts: A concussion is a brain injury that affects how your brain works. A concussion is caused by a bump, blow, or jolt to the head or body. A concussion can happen even if you haven t been
Role of TDP-43 in Non-Alzheimer s and Alzheimer s Neurodegenerative Diseases
 Role of TDP-43 in Non-Alzheimer s and Alzheimer s Neurodegenerative Diseases Keith A. Josephs, MD, MST, MSc Professor of Neurology 13th Annual Mild Cognitive Impairment (MCI) Symposium: Alzheimer and Non-Alzheimer
Role of TDP-43 in Non-Alzheimer s and Alzheimer s Neurodegenerative Diseases Keith A. Josephs, MD, MST, MSc Professor of Neurology 13th Annual Mild Cognitive Impairment (MCI) Symposium: Alzheimer and Non-Alzheimer
Amyotrophic lateral sclerosis (ALS) is a progressive neurodegenerative
 is a progressive neurodegenerative") ORIGINAL RESEARCH E. Matsusue S. Sugihara S. Fujii T. Kinoshita T. Nakano E. Ohama T. Ogawa Cerebral Cortical and White Matter Lesions in Amyotrophic Lateral Sclerosis with Dementia: Correlation with MR
ORIGINAL RESEARCH E. Matsusue S. Sugihara S. Fujii T. Kinoshita T. Nakano E. Ohama T. Ogawa Cerebral Cortical and White Matter Lesions in Amyotrophic Lateral Sclerosis with Dementia: Correlation with MR
An Autopsy Proven Child Onset Chronic Traumatic Encephalopathy
 https://doi.org/10.5607/en.2017.26.3.172 Exp Neurobiol. 2017 Jun;26(3):172-177. pissn 1226-2560 eissn 2093-8144 Case Report An Autopsy Proven Child Onset Chronic Traumatic Encephalopathy Kyuho Lee 1, Seong-Ik
https://doi.org/10.5607/en.2017.26.3.172 Exp Neurobiol. 2017 Jun;26(3):172-177. pissn 1226-2560 eissn 2093-8144 Case Report An Autopsy Proven Child Onset Chronic Traumatic Encephalopathy Kyuho Lee 1, Seong-Ik
Concussion Information
 What is a Concussion? Concussion Information Information taken from the Sports Concussion Institute http://www.concussiontreatment.com A concussion is defined as a complex pathophysiological process that
What is a Concussion? Concussion Information Information taken from the Sports Concussion Institute http://www.concussiontreatment.com A concussion is defined as a complex pathophysiological process that
Functional Neuroanatomy and Traumatic Brain Injury The Frontal Lobes
 Functional Neuroanatomy and Traumatic Brain Injury The Frontal Lobes Jessica Matthes, Ph.D., ABN Barrow TBI Symposium March 23, 2019 jessica.matthes@dignityhealth.org Outline TBI Mechanisms of Injury Types
Functional Neuroanatomy and Traumatic Brain Injury The Frontal Lobes Jessica Matthes, Ph.D., ABN Barrow TBI Symposium March 23, 2019 jessica.matthes@dignityhealth.org Outline TBI Mechanisms of Injury Types
Neuropathology of Neurodegenerative Disorders Prof. Jillian Kril
 Neurodegenerative disorders to be discussed Alzheimer s disease Lewy body diseases Frontotemporal dementia and other tauopathies Huntington s disease Motor Neuron Disease 2 Neuropathology of neurodegeneration
Neurodegenerative disorders to be discussed Alzheimer s disease Lewy body diseases Frontotemporal dementia and other tauopathies Huntington s disease Motor Neuron Disease 2 Neuropathology of neurodegeneration
Concussion Management
 Concussion Management Bill Meehan, MD Director, Micheli Center for Sports Injury Prevention Co-Director, Football Players Health Study at Harvard Division of Sports Medicine, Boston Children s Hospital
Concussion Management Bill Meehan, MD Director, Micheli Center for Sports Injury Prevention Co-Director, Football Players Health Study at Harvard Division of Sports Medicine, Boston Children s Hospital
Seth Smith MD, PharmD. Thank You!
 Seth Smith MD, PharmD Thank You! Concussion Headlines!!! Concussion Headlines!!! Concussion rules put kids health before winning games The Miami Herald 8/21/12 FHSAA's implementation of legislation goes
Seth Smith MD, PharmD Thank You! Concussion Headlines!!! Concussion Headlines!!! Concussion rules put kids health before winning games The Miami Herald 8/21/12 FHSAA's implementation of legislation goes
CONCUSSION and SUDDEN CARDIAC ARREST ACKNOWLEDGEMENT AND SIGNATURE FORM FOR PARENTS AND STUDENT ATHLETES. Sport Participating In (If Known):
:") Student Athlete s Name (Please Print): CONCUSSION and SUDDEN CARDIAC ARREST ACKNOWLEDGEMENT AND SIGNATURE FORM FOR PARENTS AND STUDENT ATHLETES Sport Participating In (If Known): Date: IC 20-34-7 and IC
Student Athlete s Name (Please Print): CONCUSSION and SUDDEN CARDIAC ARREST ACKNOWLEDGEMENT AND SIGNATURE FORM FOR PARENTS AND STUDENT ATHLETES Sport Participating In (If Known): Date: IC 20-34-7 and IC
DOC // HOW STROKES AFFECT THE BRAIN EBOOK
 17 February, 2018 DOC // HOW STROKES AFFECT THE BRAIN EBOOK Document Filetype: PDF 503.33 KB 0 DOC // HOW STROKES AFFECT THE BRAIN EBOOK They occur when the blood supply to the brain becomes. This phenomenon
17 February, 2018 DOC // HOW STROKES AFFECT THE BRAIN EBOOK Document Filetype: PDF 503.33 KB 0 DOC // HOW STROKES AFFECT THE BRAIN EBOOK They occur when the blood supply to the brain becomes. This phenomenon
International Brain Bee Syllabus 2012 Department of Neurosciences, Universiti Sains Malaysia
 BRAIN DEVELOPMENT The cells of the nervous system connect with one another in trillions of remarkably specific patterns that form and change over the course of an organism s life. These connections develop
BRAIN DEVELOPMENT The cells of the nervous system connect with one another in trillions of remarkably specific patterns that form and change over the course of an organism s life. These connections develop
V. CENTRAL NERVOUS SYSTEM TRAUMA
 V. CENTRAL NERVOUS SYSTEM TRAUMA I. Concussion - Is a clinical syndrome of altered consiousness secondary to head injury - Brought by a change in the momentum of the head when a moving head suddenly arrested
V. CENTRAL NERVOUS SYSTEM TRAUMA I. Concussion - Is a clinical syndrome of altered consiousness secondary to head injury - Brought by a change in the momentum of the head when a moving head suddenly arrested
What About Dementia? Module 8, Part B (With Dr Allison Lamont)
") What About Dementia? Module 8, Part B (With Dr Allison Lamont) Slide 1 Module 8 Part B will address the question What about dementia? Several surveys of older people both in the UK and USA have shown that
What About Dementia? Module 8, Part B (With Dr Allison Lamont) Slide 1 Module 8 Part B will address the question What about dementia? Several surveys of older people both in the UK and USA have shown that
Measuring Head Impact Exposure and Mild Traumatic Brain Injury in Humans
 Measuring Head Impact Exposure and Mild Traumatic Brain Injury in Humans Bryan Cobb Wake Forest University Center for Injury Biomechanics ABSTRACT Helmeted sports such as football offer a unique opportunity
Measuring Head Impact Exposure and Mild Traumatic Brain Injury in Humans Bryan Cobb Wake Forest University Center for Injury Biomechanics ABSTRACT Helmeted sports such as football offer a unique opportunity
! slow, progressive, permanent loss of neurologic function.
 UBC ! slow, progressive, permanent loss of neurologic function.! cause unknown.! sporadic, familial or inherited.! degeneration of specific brain region! clinical syndrome.! pathology: abnormal accumulation
UBC ! slow, progressive, permanent loss of neurologic function.! cause unknown.! sporadic, familial or inherited.! degeneration of specific brain region! clinical syndrome.! pathology: abnormal accumulation
Overview of Brain Structures
 First Overview of Brain Structures Psychology 470 Introduction to Chemical Additions Steven E. Meier, Ph.D. All parts are interrelated. You need all parts to function normally. Neurons = Nerve cells Listen
First Overview of Brain Structures Psychology 470 Introduction to Chemical Additions Steven E. Meier, Ph.D. All parts are interrelated. You need all parts to function normally. Neurons = Nerve cells Listen
Mild traumatic brain injury in contact sport athletes and the development of neurodegenerative disease
 Boston University OpenBU Theses & Dissertations http://open.bu.edu Boston University Theses & Dissertations 2016 Mild traumatic brain injury in contact sport athletes and the development of neurodegenerative
Boston University OpenBU Theses & Dissertations http://open.bu.edu Boston University Theses & Dissertations 2016 Mild traumatic brain injury in contact sport athletes and the development of neurodegenerative
Chapter 15: Late Life and Psychological Disorders
 \ Chapter 15: Late Life and Psychological Disorders 1. Ageism refers to a. the physical deterioration that accompanies old age. b. the intellectual deterioration that frequently occurs as a person ages.
\ Chapter 15: Late Life and Psychological Disorders 1. Ageism refers to a. the physical deterioration that accompanies old age. b. the intellectual deterioration that frequently occurs as a person ages.
PET Scanning of Brain Tau in Retired National Football League Players: Preliminary Findings
 PET Scanning of Brain Tau in Retired National Football League Players: Preliminary Findings Gary W. Small, M.D., Vladimir Kepe, Ph.D., Prabha Siddarth, Ph.D., Linda M. Ercoli, Ph.D., David A. Merrill,
PET Scanning of Brain Tau in Retired National Football League Players: Preliminary Findings Gary W. Small, M.D., Vladimir Kepe, Ph.D., Prabha Siddarth, Ph.D., Linda M. Ercoli, Ph.D., David A. Merrill,
MULTIPLE CONCUSSIONS LEAD TO CHRONIC TRAUMATIC ENCEPHALOPATHY (CTE)
") MULTIPLE CONCUSSIONS LEAD TO CHRONIC TRAUMATIC ENCEPHALOPATHY (CTE) CTE may develop within a short time of trauma but usually years intervene Symptoms Cognitive: depression, dementia Movement disorders:
MULTIPLE CONCUSSIONS LEAD TO CHRONIC TRAUMATIC ENCEPHALOPATHY (CTE) CTE may develop within a short time of trauma but usually years intervene Symptoms Cognitive: depression, dementia Movement disorders:
2. Subarachnoid Hemorrhage
 Causes: 2. Subarachnoid Hemorrhage A. Saccular (berry) aneurysm - Is the most frequent cause of clinically significant subarachnoid hemorrhage is rupture of a saccular (berry) aneurysm. B. Vascular malformation
Causes: 2. Subarachnoid Hemorrhage A. Saccular (berry) aneurysm - Is the most frequent cause of clinically significant subarachnoid hemorrhage is rupture of a saccular (berry) aneurysm. B. Vascular malformation
Dementia Update. October 1, 2013 Dylan Wint, M.D. Cleveland Clinic Lou Ruvo Center for Brain Health Las Vegas, Nevada
 Dementia Update October 1, 2013 Dylan Wint, M.D. Cleveland Clinic Lou Ruvo Center for Brain Health Las Vegas, Nevada Outline New concepts in Alzheimer disease Biomarkers and in vivo diagnosis Future trends
Dementia Update October 1, 2013 Dylan Wint, M.D. Cleveland Clinic Lou Ruvo Center for Brain Health Las Vegas, Nevada Outline New concepts in Alzheimer disease Biomarkers and in vivo diagnosis Future trends
Chronic Traumatic Encephalopathy in Athletes: Progressive Tauopathy After Repetitive Head Injury
 Chronic Traumatic Encephalopathy in Athletes: Progressive Tauopathy After Repetitive Head Injury The Harvard community has made this article openly available. Please share how this access benefits you.
Chronic Traumatic Encephalopathy in Athletes: Progressive Tauopathy After Repetitive Head Injury The Harvard community has made this article openly available. Please share how this access benefits you.
THE ASSOCIATIONS BETWEEN FOOTBALL EXPOSURE, CONCUSSION HISTORY AND PLAYING POSITION ON CEREBRAL WHITE MATTER INTEGRITY AND NEUROCOGNITIVE PERFORMANCE
 THE ASSOCIATIONS BETWEEN FOOTBALL EXPOSURE, CONCUSSION HISTORY AND PLAYING POSITION ON CEREBRAL WHITE MATTER INTEGRITY AND NEUROCOGNITIVE PERFORMANCE By Allen Anthony Champagne Senior Honors Thesis Department
THE ASSOCIATIONS BETWEEN FOOTBALL EXPOSURE, CONCUSSION HISTORY AND PLAYING POSITION ON CEREBRAL WHITE MATTER INTEGRITY AND NEUROCOGNITIVE PERFORMANCE By Allen Anthony Champagne Senior Honors Thesis Department
Director of Athletics
 3341-8-1 Concussion Management Policy. Applicability Intercollegiate Athletics Responsible Unit Policy Administrator Intercollegiate Athletics/Director of Athletics Director of Athletics (A) Policy Purpose
3341-8-1 Concussion Management Policy. Applicability Intercollegiate Athletics Responsible Unit Policy Administrator Intercollegiate Athletics/Director of Athletics Director of Athletics (A) Policy Purpose
Delirium & Dementia. Nicholas J. Silvestri, MD
 Delirium & Dementia Nicholas J. Silvestri, MD Outline Delirium vs. Dementia Neural pathways relating to consciousness Encephalopathy Stupor Coma Dementia Delirium vs. Dementia Delirium Abrupt onset Lasts
Delirium & Dementia Nicholas J. Silvestri, MD Outline Delirium vs. Dementia Neural pathways relating to consciousness Encephalopathy Stupor Coma Dementia Delirium vs. Dementia Delirium Abrupt onset Lasts
Nervous System. 1. What N.S. division controls skeletal muscles? 3. What kind of neuroglia myelinates axons in the PNS?
 . What N.S. division controls skeletal muscles? Nervous System SRS Review %. Central nervous system %. Peripheral nervous system %. Afferent division %. Somatic division %. Autonomic division %. Sympathetic
. What N.S. division controls skeletal muscles? Nervous System SRS Review %. Central nervous system %. Peripheral nervous system %. Afferent division %. Somatic division %. Autonomic division %. Sympathetic
Common Causes of Brain Damage Cerebrovascular Disorders = Stroke Arteriosclerosis Ischemia and Excitotoxicity
 1 2 Common Causes of Brain Damage Cerebrovascular Disorders = Stroke Tumors Closed-head injuries Infections Neurotoxins Genetic Factors Cerebrovascular Disorders = Stroke May result from: Cerebral hemorrhage
1 2 Common Causes of Brain Damage Cerebrovascular Disorders = Stroke Tumors Closed-head injuries Infections Neurotoxins Genetic Factors Cerebrovascular Disorders = Stroke May result from: Cerebral hemorrhage
Concussions in Sport Definitions, Mechanisms, and Current Issues
 Concussions in Sport Definitions, Mechanisms, and Current Issues Concussions are Everyone s Responsibility! If you do not LOOK FOR IT you will not FIND IT! Paul Echlin MD CCFP, Dip. ABFM, Dip. SM, CAQSM
Concussions in Sport Definitions, Mechanisms, and Current Issues Concussions are Everyone s Responsibility! If you do not LOOK FOR IT you will not FIND IT! Paul Echlin MD CCFP, Dip. ABFM, Dip. SM, CAQSM
SECTION 1: as each other, or as me. THE BRAIN AND DEMENTIA. C. Boden *
 I read all the available books by other [people with] Alzheimer s disease but they never had quite the same problems as each other, or as me. I t s not like other diseases, where there is a standard set
I read all the available books by other [people with] Alzheimer s disease but they never had quite the same problems as each other, or as me. I t s not like other diseases, where there is a standard set
The Biological Basis of Chronic Traumatic Encephalopathy following Blast Injury: A Literature Review
 JOURNAL OF NEUROTRAUMA 34:S-26 S-43 (Supplement 1, 2017) ª Mary Ann Liebert, Inc. DOI: 10.1089/neu.2017.5218 The Biological Basis of Chronic Traumatic Encephalopathy following Blast Injury: A Literature
JOURNAL OF NEUROTRAUMA 34:S-26 S-43 (Supplement 1, 2017) ª Mary Ann Liebert, Inc. DOI: 10.1089/neu.2017.5218 The Biological Basis of Chronic Traumatic Encephalopathy following Blast Injury: A Literature
Lecture 42: Final Review. Martin Wessendorf, Ph.D.
 Lecture 42: Final Review Martin Wessendorf, Ph.D. Lecture 33 cortex Heilbronner 5 lobes of the cortex Lateral view (left side) Mid-saggital view (right side) Cellular organization of cortex White matter
Lecture 42: Final Review Martin Wessendorf, Ph.D. Lecture 33 cortex Heilbronner 5 lobes of the cortex Lateral view (left side) Mid-saggital view (right side) Cellular organization of cortex White matter
Richard C. Stabb, D.O. Memorial Symposium. Concussion: A Gray Matter, Understanding Concussion
 Richard C. Stabb, D.O. Memorial Symposium Concussion: A Gray Matter, Understanding Concussion Objectives To review current, traumatic brain injury (TBI), concussion terminology, evaluation and management.
Richard C. Stabb, D.O. Memorial Symposium Concussion: A Gray Matter, Understanding Concussion Objectives To review current, traumatic brain injury (TBI), concussion terminology, evaluation and management.
Mark J. Harary, MD Primary Care Sports Medicine St Charles Orthopedics, LLP
 Mark J. Harary, MD Primary Care Sports Medicine St Charles Orthopedics, LLP Facts, Definitions, etc Appropriate Recognition Comprehensive Management Treatment Consequences of Concussions Neurocognitive
Mark J. Harary, MD Primary Care Sports Medicine St Charles Orthopedics, LLP Facts, Definitions, etc Appropriate Recognition Comprehensive Management Treatment Consequences of Concussions Neurocognitive
Language After Traumatic Brain Injury
 Chapter 7 Language After Traumatic Brain Injury 10/24/05 COMD 326, Chpt. 7 1 1 10/24/05 COMD 326, Chpt. 7 2 http://www.californiaspinalinjurylawyer.com/images/tbi.jpg 2 TBI http://www.conleygriggs.com/traumatic_brain_injury.shtml
Chapter 7 Language After Traumatic Brain Injury 10/24/05 COMD 326, Chpt. 7 1 1 10/24/05 COMD 326, Chpt. 7 2 http://www.californiaspinalinjurylawyer.com/images/tbi.jpg 2 TBI http://www.conleygriggs.com/traumatic_brain_injury.shtml
The Spectrum of Age-Associated Astroglial Tauopathies. Dennis W. Dickson MD Department of Neuroscience Mayo Clinic, Jacksonville, FL
 The Spectrum of Age-Associated Astroglial Tauopathies Dennis W. Dickson MD Mayo Clinic, Jacksonville, FL Thorn-shaped astrocytes TSA were first reported by Ikeda (1995), as tau-positive astrocytes in various
The Spectrum of Age-Associated Astroglial Tauopathies Dennis W. Dickson MD Mayo Clinic, Jacksonville, FL Thorn-shaped astrocytes TSA were first reported by Ikeda (1995), as tau-positive astrocytes in various
The Central Nervous System I. Chapter 12
 The Central Nervous System I Chapter 12 The Central Nervous System The Brain and Spinal Cord Contained within the Axial Skeleton Brain Regions and Organization Medical Scheme (4 regions) 1. Cerebral Hemispheres
The Central Nervous System I Chapter 12 The Central Nervous System The Brain and Spinal Cord Contained within the Axial Skeleton Brain Regions and Organization Medical Scheme (4 regions) 1. Cerebral Hemispheres
Brain Concussion: A Stealth Injury. Christine Schulman, RN, MS, CNS, CCRN Trauma & Critical Care CNS Legacy Health, Portland, Oregon Director, AACN
 Brain Concussion: A Stealth Injury Christine Schulman, RN, MS, CNS, CCRN Trauma & Critical Care CNS Legacy Health, Portland, Oregon Director, AACN Legacy Emanuel Medical Center Portland, Oregon Disclosures
Brain Concussion: A Stealth Injury Christine Schulman, RN, MS, CNS, CCRN Trauma & Critical Care CNS Legacy Health, Portland, Oregon Director, AACN Legacy Emanuel Medical Center Portland, Oregon Disclosures
NEBRASKA SCHOOL ACTIVITIES ASSOCIATION Member of the National Federation of State High School Associations
 NEBRASKA SCHOOL ACTIVITIES ASSOCIATION Member of the National Federation of State High School Associations 500 Charleston P.O. Box 85448 Lincoln, Nebraska 68501 Phone: 402-489-0386 Fax: 402-489-0934 E-mail:
NEBRASKA SCHOOL ACTIVITIES ASSOCIATION Member of the National Federation of State High School Associations 500 Charleston P.O. Box 85448 Lincoln, Nebraska 68501 Phone: 402-489-0386 Fax: 402-489-0934 E-mail:
Dementia. Stephen S. Flitman, MD Medical Director 21st Century Neurology
 Dementia Stephen S. Flitman, MD Medical Director 21st Century Neurology www.neurozone.org Dementia is a syndrome Progressive memory loss, plus Progressive loss of one or more cognitive functions: Language
Dementia Stephen S. Flitman, MD Medical Director 21st Century Neurology www.neurozone.org Dementia is a syndrome Progressive memory loss, plus Progressive loss of one or more cognitive functions: Language
CASE 49. What type of memory is available for conscious retrieval? Which part of the brain stores semantic (factual) memories?
 memories?") CASE 49 A 43-year-old woman is brought to her primary care physician by her family because of concerns about her forgetfulness. The patient has a history of Down syndrome but no other medical problems.
CASE 49 A 43-year-old woman is brought to her primary care physician by her family because of concerns about her forgetfulness. The patient has a history of Down syndrome but no other medical problems.
Concussion is the most common type of
 CMAJ Early release, published at www.cmaj.ca on July 22, 2013. Subject to revision. Practice Primer Concussions and their consequences: current diagnosis, management and prevention Charles H. Tator MD
CMAJ Early release, published at www.cmaj.ca on July 22, 2013. Subject to revision. Practice Primer Concussions and their consequences: current diagnosis, management and prevention Charles H. Tator MD
Conflicts. Objectives. You can t hide. Epidemiology 4/16/2018. I have no relevant financial relationships to disclose.
 The Concussion Epidemic What the EM provider needs to know Conflicts I have no relevant financial relationships to disclose. Certified ImPACT consultant NFL/KSI grant reviewer Paid consultant for Weber-Shandwick
The Concussion Epidemic What the EM provider needs to know Conflicts I have no relevant financial relationships to disclose. Certified ImPACT consultant NFL/KSI grant reviewer Paid consultant for Weber-Shandwick
Neocortex. Hemispheres 9/22/2010. Psychology 472 Pharmacology of Psychoactive Drugs. Structures are divided into several section or lobes.
 Neocortex Psychology 472 Pharmacology of Psychoactive Drugs 1 Is the most developed in Humans Has many folds and fissures The folds of tissue are called gyri or a gyrus (single) The fissures or valleys
Neocortex Psychology 472 Pharmacology of Psychoactive Drugs 1 Is the most developed in Humans Has many folds and fissures The folds of tissue are called gyri or a gyrus (single) The fissures or valleys
Caring Sheet #11: Alzheimer s Disease:
 CARING SHEETS: Caring Sheet #11: Alzheimer s Disease: A Summary of Information and Intervention Suggestions with an Emphasis on Cognition By Shelly E. Weaverdyck, PhD Introduction This caring sheet focuses
CARING SHEETS: Caring Sheet #11: Alzheimer s Disease: A Summary of Information and Intervention Suggestions with an Emphasis on Cognition By Shelly E. Weaverdyck, PhD Introduction This caring sheet focuses
Name: Period: Test Review: Chapter 2
 Name: Period: Test Review: Chapter 2 1. The function of dendrites is to A) receive incoming signals from other neurons. B) release neurotransmitters into the spatial junctions between neurons. C) coordinate
Name: Period: Test Review: Chapter 2 1. The function of dendrites is to A) receive incoming signals from other neurons. B) release neurotransmitters into the spatial junctions between neurons. C) coordinate
FTD basics! Etienne de Villers-Sidani, MD!
 FTD basics! Etienne de Villers-Sidani, MD! Frontotemporal lobar degeneration (FTLD) comprises 3 clinical syndromes! Frontotemporal dementia (behavioral variant FTD)! Semantic dementia (temporal variant
FTD basics! Etienne de Villers-Sidani, MD! Frontotemporal lobar degeneration (FTLD) comprises 3 clinical syndromes! Frontotemporal dementia (behavioral variant FTD)! Semantic dementia (temporal variant
Concussions in High School Athletics. John F. Kosowicz Jr., ATC
 Concussions in High School Athletics John F. Kosowicz Jr., ATC What is an Athletic Trainer - Directly responsible for all phases of health care in an athletic environment - Six performance domains established
Concussions in High School Athletics John F. Kosowicz Jr., ATC What is an Athletic Trainer - Directly responsible for all phases of health care in an athletic environment - Six performance domains established
FRONTOTEMPORAL DEGENERATION: OVERVIEW, TRENDS AND DEVELOPMENTS
 FRONTOTEMPORAL DEGENERATION: OVERVIEW, TRENDS AND DEVELOPMENTS Norman L. Foster, M.D. Director, Center for Alzheimer s Care, Imaging and Research Chief, Division of Cognitive Neurology, Department of Neurology
FRONTOTEMPORAL DEGENERATION: OVERVIEW, TRENDS AND DEVELOPMENTS Norman L. Foster, M.D. Director, Center for Alzheimer s Care, Imaging and Research Chief, Division of Cognitive Neurology, Department of Neurology
NCFE Level 2 Certificate in The Principles of Dementia Care
 The Principles of Dementia Care S A M P LE NCFE Level 2 Certificate in The Principles of Dementia Care Part A 1 These learning resources and assessment questions have been approved and endorsed by ncfe
The Principles of Dementia Care S A M P LE NCFE Level 2 Certificate in The Principles of Dementia Care Part A 1 These learning resources and assessment questions have been approved and endorsed by ncfe
What APS Workers Need to Know about Frontotemporal, Lewy Body and Vascular Dementias
 What APS Workers Need to Know about Frontotemporal, Lewy Body and Vascular Dementias Presenter: Kim Bailey, MS Gerontology, Program & Education Specialist, Alzheimer s Orange County 1 1 Facts About Our
What APS Workers Need to Know about Frontotemporal, Lewy Body and Vascular Dementias Presenter: Kim Bailey, MS Gerontology, Program & Education Specialist, Alzheimer s Orange County 1 1 Facts About Our
CONCUSSION INFORMATION AND SIGNATURE FORM FOR COACHES (Adapted from CDC Heads Up Concussion in Youth Sports )
") CONCUSSION INFORMATION AND SIGNATURE FORM FOR COACHES (Adapted from CDC Heads Up Concussion in Youth Sports ) Read and keep this page. Sign and return the signature page. THE FACTS A concussion is a brain
CONCUSSION INFORMATION AND SIGNATURE FORM FOR COACHES (Adapted from CDC Heads Up Concussion in Youth Sports ) Read and keep this page. Sign and return the signature page. THE FACTS A concussion is a brain
CONCUSSION INFORMATION AND SIGNATURE FORM FOR COACHES (Adapted from CDC Heads Up Concussion in Youth Sports )
") CONCUSSION INFORMATION AND SIGNATURE FORM FOR COACHES (Adapted from CDC Heads Up Concussion in Youth Sports ) Read and keep this page. Sign and return the signature page. THE FACTS A concussion is a brain
CONCUSSION INFORMATION AND SIGNATURE FORM FOR COACHES (Adapted from CDC Heads Up Concussion in Youth Sports ) Read and keep this page. Sign and return the signature page. THE FACTS A concussion is a brain
Brain Structures. Some scientists divide the brain up into three parts. Hindbrain Midbrain Forebrain
 The Brain Phineas Gage Play The Frontal Lobes and Behavior: The Story of Phineas Gage (12:03) Module #25 from The Brain: Teaching Modules (2 nd edition). http://www.learner.org/resources/series1 42.html
The Brain Phineas Gage Play The Frontal Lobes and Behavior: The Story of Phineas Gage (12:03) Module #25 from The Brain: Teaching Modules (2 nd edition). http://www.learner.org/resources/series1 42.html
Biological Psychology. Unit Two AB Mr. Cline Marshall High School Psychology
 Biological Psychology Unit Two AB Mr. Cline Marshall High School Psychology What happens in your nervous system when you react to stimuli? Did you know that the brain is sometimes uninvolved with reflexes?
Biological Psychology Unit Two AB Mr. Cline Marshall High School Psychology What happens in your nervous system when you react to stimuli? Did you know that the brain is sometimes uninvolved with reflexes?
Dementia. Assessing Brain Damage. Mental Status Examination
 Dementia Assessing Brain Damage Mental status examination Information about current behavior and thought including orientation to reality, memory, and ability to follow instructions Neuropsychological
Dementia Assessing Brain Damage Mental status examination Information about current behavior and thought including orientation to reality, memory, and ability to follow instructions Neuropsychological
Sports Related Concussions. The King-Devick Test: the Science & Implementation
 Sports Related Concussions The King-Devick Test: the Science & Implementation King-Devick Test: the Today Show CLICK HERE for Video: King-Devick Test on the Today Show Concussion by the Numbers Highest
Sports Related Concussions The King-Devick Test: the Science & Implementation King-Devick Test: the Today Show CLICK HERE for Video: King-Devick Test on the Today Show Concussion by the Numbers Highest
The human brain. of cognition need to make sense gives the structure of the brain (duh). ! What is the basic physiology of this organ?
. ! What is the basic physiology of this organ?") The human brain The human brain! What is the basic physiology of this organ?! Understanding the parts of this organ provides a hypothesis space for its function perhaps different parts perform different
The human brain The human brain! What is the basic physiology of this organ?! Understanding the parts of this organ provides a hypothesis space for its function perhaps different parts perform different
Alzheimer's disease (AD), also known as Senile Dementia of the Alzheimer Type (SDAT) or simply Alzheimer s is the most common form of dementia.
, also known as Senile Dementia of the Alzheimer Type (SDAT) or simply Alzheimer s is the most common form of dementia.") CHAPTER 3 Alzheimer's disease (AD), also known as Senile Dementia of the Alzheimer Type (SDAT) or simply Alzheimer s is the most common form of dementia. This incurable, degenerative, terminal disease
CHAPTER 3 Alzheimer's disease (AD), also known as Senile Dementia of the Alzheimer Type (SDAT) or simply Alzheimer s is the most common form of dementia. This incurable, degenerative, terminal disease
CNS Tour (Lecture 12)
") A. Introduction CNS Tour (Lecture 12) There are to a chemical pathways in the nervous system. These pathways also form different neurological structures B. Spinal Cord Receives sensory neurons from skin
A. Introduction CNS Tour (Lecture 12) There are to a chemical pathways in the nervous system. These pathways also form different neurological structures B. Spinal Cord Receives sensory neurons from skin
The Nervous System and the Endocrine System
 The Nervous System and the Endocrine System Neurons: The Building Blocks of the Nervous System Nervous System The electrochemical communication system of the body Sends messages from the brain to the
The Nervous System and the Endocrine System Neurons: The Building Blocks of the Nervous System Nervous System The electrochemical communication system of the body Sends messages from the brain to the
Concussions: Diagnosis, Management and the world of known unknowns
 Concussions: Diagnosis, Management and the world of known unknowns Alexander Rogers, MD Associate Professor Michigan Medicine 1 Disclosures I have no Financial Conflicts of Interest to Declare I will discuss
Concussions: Diagnosis, Management and the world of known unknowns Alexander Rogers, MD Associate Professor Michigan Medicine 1 Disclosures I have no Financial Conflicts of Interest to Declare I will discuss
Cognitive Ability (Decline) & Social Isolation
 & Social Isolation") Cognitive Ability (Decline) & Social Isolation May 5, 2018 Women s Health Council of RI Doreen C. Putnam, CDP, CIPG DCPutnam Consulting www.dcputnamconsulting.com *** DISCLAIMER *** The information provided
Cognitive Ability (Decline) & Social Isolation May 5, 2018 Women s Health Council of RI Doreen C. Putnam, CDP, CIPG DCPutnam Consulting www.dcputnamconsulting.com *** DISCLAIMER *** The information provided
Chapter 28 NERVOUS SYSTEM
 Chapter 28 NERVOUS SYSTEM Functions of Nervous Tissue 1. Sensory Input: Conduction of signals from sensory organs (eyes, ears, nose, skin, etc.) to information processing centers (brain and spinal cord).
Chapter 28 NERVOUS SYSTEM Functions of Nervous Tissue 1. Sensory Input: Conduction of signals from sensory organs (eyes, ears, nose, skin, etc.) to information processing centers (brain and spinal cord).
LANGUAGE AND PATHOLOGY IN FRONTOTEMPORAL DEGENERATION
 LANGUAGE AND PATHOLOGY IN FRONTOTEMPORAL DEGENERATION Murray Grossman University of Pennsylvania Support from NIH (AG17586, AG15116, NS44266, NS35867, AG32953, AG38490), IARPA, ALS Association, and the
LANGUAGE AND PATHOLOGY IN FRONTOTEMPORAL DEGENERATION Murray Grossman University of Pennsylvania Support from NIH (AG17586, AG15116, NS44266, NS35867, AG32953, AG38490), IARPA, ALS Association, and the
Neural Basis of Motor Control. Chapter 4
 Neural Basis of Motor Control Chapter 4 Neurological Perspective A basic understanding of the physiology underlying the control of voluntary movement establishes a more comprehensive appreciation and awareness
Neural Basis of Motor Control Chapter 4 Neurological Perspective A basic understanding of the physiology underlying the control of voluntary movement establishes a more comprehensive appreciation and awareness
DEMENTIA 101: WHAT IS HAPPENING IN THE BRAIN? Philip L. Rambo, PhD
 DEMENTIA 101: WHAT IS HAPPENING IN THE BRAIN? Philip L. Rambo, PhD OBJECTIVES Terminology/Dementia Basics Most Common Types Defining features Neuro-anatomical/pathological underpinnings Neuro-cognitive
DEMENTIA 101: WHAT IS HAPPENING IN THE BRAIN? Philip L. Rambo, PhD OBJECTIVES Terminology/Dementia Basics Most Common Types Defining features Neuro-anatomical/pathological underpinnings Neuro-cognitive
Davidson College Sports Medicine Concussion Management Policy
 Davidson College Sports Medicine Concussion Management Policy Davidson College practices concussion management care based on the most current research and consensus statements from noted concussion experts.
Davidson College Sports Medicine Concussion Management Policy Davidson College practices concussion management care based on the most current research and consensus statements from noted concussion experts.
The Human Brain. I Think Therefore I am
 The Human Brain I Think Therefore I am The Beginning The simplest creatures have very simple nervous systems made up of nothing but a bunch of nerve cells They have neural nets, individual neurons linked
The Human Brain I Think Therefore I am The Beginning The simplest creatures have very simple nervous systems made up of nothing but a bunch of nerve cells They have neural nets, individual neurons linked
Movement Disorders. Psychology 372 Physiological Psychology. Background. Myasthenia Gravis. Many Types
 Background Movement Disorders Psychology 372 Physiological Psychology Steven E. Meier, Ph.D. Listen to the audio lecture while viewing these slides Early Studies Found some patients with progressive weakness
Background Movement Disorders Psychology 372 Physiological Psychology Steven E. Meier, Ph.D. Listen to the audio lecture while viewing these slides Early Studies Found some patients with progressive weakness
P20.2. Characteristics of different types of dementia and challenges for the clinician
 P20.2. Characteristics of different types of dementia and challenges for the clinician, professor Danish Dementia Research Center Rigshospitalet, University of Copenhagen (Denmark) This project has received
P20.2. Characteristics of different types of dementia and challenges for the clinician, professor Danish Dementia Research Center Rigshospitalet, University of Copenhagen (Denmark) This project has received
Concussion 2013 A Program For Logan County
 Concussion 2013 A Program For Logan County Boyd C Hoddinott MD, MPH Logan County Health Commissioner ----------------------------------- Kristy Wisner PT, DPT Mary Rutan Physical Rehab Center Consensus
Concussion 2013 A Program For Logan County Boyd C Hoddinott MD, MPH Logan County Health Commissioner ----------------------------------- Kristy Wisner PT, DPT Mary Rutan Physical Rehab Center Consensus
Lesson 14. The Nervous System. Introduction to Life Processes - SCI 102 1
 Lesson 14 The Nervous System Introduction to Life Processes - SCI 102 1 Structures and Functions of Nerve Cells The nervous system has two principal cell types: Neurons (nerve cells) Glia The functions
Lesson 14 The Nervous System Introduction to Life Processes - SCI 102 1 Structures and Functions of Nerve Cells The nervous system has two principal cell types: Neurons (nerve cells) Glia The functions
Examination of the relationship between sport concussion and long term neurodegenerative and psychological disorders: a literature review
 University of Central Florida HIM 1990-2015 Open Access Examination of the relationship between sport concussion and long term neurodegenerative and psychological disorders: a literature review 2013 Vivian
University of Central Florida HIM 1990-2015 Open Access Examination of the relationship between sport concussion and long term neurodegenerative and psychological disorders: a literature review 2013 Vivian
 Johnson, V. E., and Stewart, W. (2015) Traumatic brain injury: Age at injury influences dementia risk after TBI. Nature Reviews Neurology, 11(3), pp. 128-130. (doi:10.1038/nrneurol.2014.241) There may
Johnson, V. E., and Stewart, W. (2015) Traumatic brain injury: Age at injury influences dementia risk after TBI. Nature Reviews Neurology, 11(3), pp. 128-130. (doi:10.1038/nrneurol.2014.241) There may
Clinicopathologic and genetic aspects of hippocampal sclerosis. Dennis W. Dickson, MD Mayo Clinic, Jacksonville, Florida USA
 Clinicopathologic and genetic aspects of hippocampal sclerosis Dennis W. Dickson, MD Mayo Clinic, Jacksonville, Florida USA The hippocampus in health & disease A major structure of the medial temporal
Clinicopathologic and genetic aspects of hippocampal sclerosis Dennis W. Dickson, MD Mayo Clinic, Jacksonville, Florida USA The hippocampus in health & disease A major structure of the medial temporal
Prof. Saeed Abuel Makarem & Dr.Sanaa Alshaarawy
 Prof. Saeed Abuel Makarem & Dr.Sanaa Alshaarawy 1 Objectives By the end of the lecture, you should be able to: Describe the anatomy and main functions of the thalamus. Name and identify different nuclei
Prof. Saeed Abuel Makarem & Dr.Sanaa Alshaarawy 1 Objectives By the end of the lecture, you should be able to: Describe the anatomy and main functions of the thalamus. Name and identify different nuclei
SCHOOL CITY OF HOBART
 SCHOOL CITY OF HOBART 32 East 7 TH Street, Hobart, IN 46342 Phone: 219-942-8885 Fax: 219-942-0081 http://www.hobart.k12.in.us Building College and Career Ready Brickies 5340.01 F1/page 1 of 5 CONCUSSION
SCHOOL CITY OF HOBART 32 East 7 TH Street, Hobart, IN 46342 Phone: 219-942-8885 Fax: 219-942-0081 http://www.hobart.k12.in.us Building College and Career Ready Brickies 5340.01 F1/page 1 of 5 CONCUSSION
Unit 2 Brain & Behavior
 Unit 2 Brain & Behavior Brain & Behavior Unit Guide REV 2017 Essential Questions: Why is studying biology important to understanding psychology? Which brain structures are necessary for survival? What
Unit 2 Brain & Behavior Brain & Behavior Unit Guide REV 2017 Essential Questions: Why is studying biology important to understanding psychology? Which brain structures are necessary for survival? What