Joachim M. Baehring, MD, DSc Associate Professor of Neurology, Medicine and Neurosurgery Director, Yale Brain Tumor Center Yale University School of
|
|
|
- Barbra Riley
- 6 years ago
- Views:
Transcription

1 Joachim M. Baehring, MD, DSc Associate Professor of Neurology, Medicine and Neurosurgery Director, Yale Brain Tumor Center Yale University School of Medicine New Haven, Connecticut 1
2 Disclosure of Conflicts of Interest Joachim M. Baehring, MD, DSc Joachim M. Baehring, MD, DSc, has affiliations with Sigma Tau Pharmaceuticals, Inc. (Speakers Bureau) Learning Objectives Summarize the strengths and limitations of current treatments for newly diagnosed and recurrent glioblastoma Describe prognostic factors in the survival of adults with glioblastoma Identify molecular and genetic biomarkers associated with response to treatment Identify emerging targeted treatment alternatives that have demonstrated favorable results in glioblastoma 2
3 Milestones in Neuro-Oncology Approvals Radiotherapy Lomustine Carmustine Carmustineimpegnated wafers TMZ for relapsed AA accelerated approval TMZ up front for GBM Bevacizumab for recurrent GBM First US commercial CT Levin criteria CT scans First US commercial MRI Macdonald criteria WHO Pathology criteria Brain Tumor Clinical Trial Endpoints Workshop RANO criteria Technology Advances AA=anaplastic astrocytoma; CT=computed tomography; GBM=glioblastoma multiforme; MRI=magnetic resonance imaging; RANO=Response Assessment in Neuro-Oncology. Epidemiology ~66,290 new patients are estimated to be diagnosed with primary brain tumors in the United States in ~33% tumors of neuroepithelial tissue (NET) ~50% of all NET are glioblastoma multiforme (GBM) Among patients with GBM 1,2 Median overall survival: 8 to 15 months 2-year survival rates: 13% to 27% Central Brain Tumor Registry of the United States (CBTRUS) Report. 2. Stupp R, et al. Lancet Oncol. 2009;10:
4 Incidence Distribution of All Primary Brain and CNS Tumors by Histology Lymphoma 2.3% All Other 12.2% Glioblastoma 20.3% Nerve Sheath 8.5% Craniopharyngioma 0.7% Pituitary 13.5% Astrocytomas 6.8% Ependymomas 1.8% Oligodendrogliomas 1.9% Embryonal, including medulloblastoma 1.1% 2012 CBTRUS Report. Meningioma 34.7% Incidence Distribution of All Gliomas by Histology Subtypes Ependymomas 5.8% All Other Gliomas 11.4% Oligodendrogliomas 6.4% Pilocytic Astrocytoma 5.2% Glioblastoma 53.9% Diffuse Astrocytoma 1.8% Anaplastic Astrocytoma 6.7% 2012 CBTRUS Report. All Other Astrocytomas 8.8% 4
5 Classification and Grading World Health Organization (WHO) Classification System Released in 1993; updated in 2007 Tumors classified by cell origin and level of aggression (Grades I IV) 1 Grade Histology Proportion of All Gliomas 2 Median Survival (y) 2 I Pilocytic astrocytoma 5.2% >10 II Well-differentiated astrocytoma 1.8% >4 III Anaplastic astrocytoma 13.8% , 3 IV Glioblastoma multiforme 53.9% <1 1. Kleihues, et al. Brain Pathol. 1993;3(3): CBTRUS Report. 3. Wick, et al. J Clin Oncol. 2009;27: Risk Factors for Malignant Glioma Family history of cancer in 19% of patients 1 Genetically inherited syndromes in 5% of patients with primary brain tumors 1 Neurofibromatosis types 1 and 2 Li-Fraumeni syndrome von Hippel-Lindau syndrome Turcot syndrome Tuberous sclerosis Brain irradiation in childhood 2 1. Grossman SA, et al. Cancer Invest. 1999;17: Neglia JP, et al. J Natl Cancer Inst. 2006;98:

6 Gliomagenesis DCC=deleted in colon cancer; LOH=loss of heterozygosity; RB=retinoblastoma. Courtesy of Marc C. Chamberlain; with permission. Frequent Genetic Alterations in Three Critical Signaling Pathways The Cancer Genome Atlas Research Network. Nature. 2008;455: ; with permission. 6
7 Symptoms Incidence of Symptoms in Patients With Glioma Patients with Symptoms (Median %) Low-grade glioma Malignant glioma Data modified from DeAngelis LM. N Engl J Med. 2001;344: Wen PY, Kesari S. N Engl J Med. 2008;359: Symptom Etiology Direct infiltration and destruction of neuronal networks Local pressure from Edema Hemorrhage Tumor mass Cyst formation Intracranial hypertension Mass effect CSF flow obstruction 7
 Perfusion MRI Positron emission tomography (PET) Tissue sample Confirm diagnosis Determine tumor type and grade Molecular genetic analysis Current Treatment: Surgery Rationale for extensive")
8 Diagnostic Assessment Gold standard Magnetic resonance imaging (MRI) with contrast Computed tomography (CT) scan when MRI is contraindicated Adjunctive techniques Magnetic resonance spectroscopy (MRS) Perfusion MRI Positron emission tomography (PET) Tissue sample Confirm diagnosis Determine tumor type and grade Molecular genetic analysis Current Treatment: Surgery Rationale for extensive resection Provides adequate tissue for diagnosis Palliates mass effect Allows for improvements in tumor-related signs and symptoms May increase survival Helps halt disease progression by eliminating resistance clones National Comprehensive Cancer Network. Practice Guidelines in Oncology: Central Nervous System Cancers;



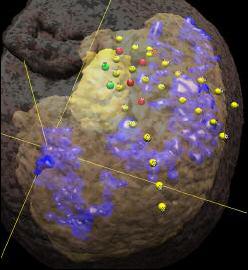
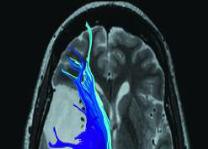
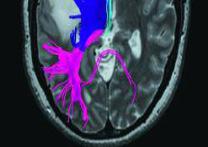
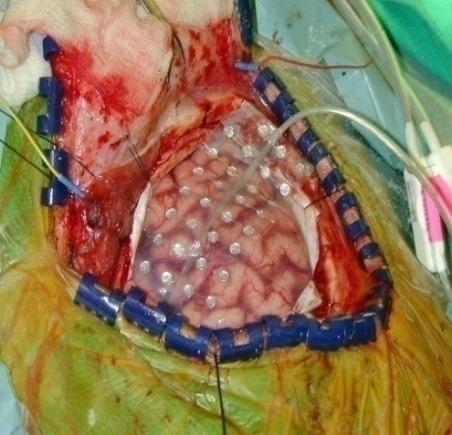
9 Surgery Challenges Biopsy vs. resection Tumor location Patient factors Co-administration of local therapy Treatment toxicity Clinical trial exclusion Surgery Maximal Safe Resection Wilson A. Available at: 2. Courtesy of Michael A. Vogelbaum, MD; with permission. 3. Brigham and Women s Hospital. Available at: 9
10 Benefit of Complete Surgical Resection Study EORTC Extent of Resection Complete Subtotal Biopsy Median OS with RT alone 14.2 months 11.7 months 7.8 months 2-year survival with RT alone Median OS with RT + temozolomide 2-year survival with RT + temozolomide 5-ALA % 9.4% 4.6% 18.8 months 13.5 months 9.4 months 38.4% 23.7% 10.4% Median OS 16.9 months 11.8 months 2-year survival 26% 7% OS=overall survival; RT=radiotherapy; 5-ALA=5-aminolevulinic acid induced tumor fluorescence. 1. Stupp R, et al. Lancet Oncol. 2009;10: Stummer W, et al. Neurosurgery. 2008;62: Surgery Plus Local Therapy Carmustine (BCNU) wafers Polyanhydride wafers, 7.7 mg carmustine (BCNU) 1 Carmustine released over 2 to 3 weeks >70% degradation by Week 3 Approval 1996 for recurrent GBM as adjunct to surgery expanded for all high-grade gliomas, including newly diagnosed 3 Local delivery obviates the blood brain barrier Lower toxicity than systemic chemotherapy 1. Gliadel wafer prescribing information. Accessed March 30, Brem H, et al. Lancet. 1995;345: Westphal M, et al. Neuro Oncol. 2003;5:
11 Surgery Plus Local Therapy BCNU Wafer Improves Survival vs. Placebo 1.00 Salvage 1.00 Adjuvant Probability of survival Placebo Hazard Ratio: 0.67 P=0.02 BCNU wafer Probability of survival Placebo Hazard Ratio: % CI: Risk Reduction: 29% P=0.018 BCNU wafer Time (weeks) Months from implant surgery Brem H, et al. Lancet. 1995;345: Westphal M, et al. Acta Neurochir (Wien). 2006;148: Westphal M, et al. Neuro Oncol. 2003;5: Current Treatment: Radiation Therapy (RT) Challenges Recurrence is the major source of therapeutic failure Surgery and radiation therapy often fail to prevent recurrence Most recurrent gliomas occur at close proximity to initial tumor Distance from Edge of Initial Tumor (cm) Incidence (% of All Recurrent Gliomas) < >3 3 Hochberg FH, Pruitt A. Neurology. 1980;30: Wallner KE, et al. Int J Radiat Oncol Biol Phys. 1989;16:
12 Radiation Therapy RTOG trial analyses Improved outcomes with involved-field vs. whole-brain RT Dose-response relationship: best response with 60 to 65 Gy conventional external beam RT (cebrt) No apparent survival benefit with: >65 Gy cebrt Conformal RT Accelerated or hyperfractionated schedules Boost gamma knife RT Brachytherapy boost Cardinale R, et al. Int J Radiat Oncol Biol Phys. 2006;65: Tsao MN, et al. Int J Radiat Oncol Biol Phys. 2005;63: Chang JE, et al. Clin Adv Hematol Oncol. 2007;5: , Radiation Therapy RT +/- SRS RT +/- SRS Survival rate (%) RT SRS+RT Median n Survival Time mo mo P=0.64 Survival probability RT SRS+RT Median n Survival Time mo mo P= Months Months to death since surgery SRS=stereotactic radiosurgery. Souhami L, et al. Int J Radiat Oncol Biol Phys. 2004;60: ; with permission. Laperriere NJ, et al. Int J Radiat Oncol Biol Phys. 1998;41: ; with permission. 12
13 Chemotherapy Challenges Issues of efficacy Intrinsic resistance Pharmacologic (tumor delivery) Concurrent medications Anticonvulsants Steroids Systemic toxicity Response measurements Current Treatment: Chemotherapy Three Major Meta-Analyses Fine et al. 1 Stewart 2 Spiegel et al. 3 Date of meta-analysis Trials analyzed, n Patients analyzed, n >3,000 3,004 >3,000 Agent(s) used Various Various Various Absolute increase in survival, % 1 year * 2 year * * TMZ treatment group only. 1. Fine HA, et al. Cancer. 1993;71: Stewart LA. Lancet. 2002;359: Spiegel BM, et al. CNS Drugs. 2007;21:
14 Current Treatment: Temozolomide (TMZ) Methylating agent Cytotoxic product is O 6 -methylguanine DNA adducts Initiates mismatch repair pathway recycling, resulting in apoptotic cell death Efficacy Activity in newly diagnosed anaplastic glioma 1 Activity in recurrent anaplastic astrocytoma 2 Activity in recurrent GBM 3 Activity in adjuvant treatment of GBM 4,5 1. Wick W, et al. J Clin Oncol. 2009;27: Yung WK, et al. J Clin Oncol. 1999;17: Yung WK, et al. Br J Cancer. 2000;83: Stupp R, et al. N Engl J Med. 2005;352: Stupp R, et al. J Clin Oncol. 2002;20: Temozolomide European Organization for the Research and Treatment of Cancer (EORTC)/National Cancer Institute of Canada (NCIC) Treatment Platform PCP Prophylaxis RT 30 2 Gy PCP Prophylaxis TMZ daily 42d 4 wks RT 30 2 Gy Radiotherapy (RT): Focal, 60 Gy in 6 wk to tumor volume plus 2- to 3-cm margin TMZ: During RT: 75 mg/m 2 /d (including weekends) for up to 49 d; administered 1 2 h before RT in AM on days without RT Maintenance: mg/m 2 /d 5d, for up to 6 cycles; antiemetic prophylaxis PCP=Pneumocystis carinii pneumonia. Stupp R, et al. N Engl J Med. 2005;352: Control Arm 5d 4 5d 5d wks Experimental Arm 6 cycles 14
15 Temozolomide EORTC/NCIC trial 1 RT alone vs. RT plus TMZ Primary endpoint: overall survival Secondary endpoints: progression-free survival, quality of life (QOL), safety No negative impact on QOL 5-year follow-up data 2 A benefit of combined therapy was recorded in all subgroups EORTC/NCIC Trial Survival RT RT + TMZ 2-year 10.4% 26.5% 5-Year Follow-Up Survival RT RT + TMZ 2-year 10.9% 27.3% 3-year 4.4% 16.0% 4-year 3.0% 12.1% 5-year 1.9% 9.8% 1. Stupp R, et al. N Engl J Med. 2005;352: Stupp R, et al. Lancet Oncol. 2009;10: Temozolomide DNA repair O 6 -methylguanine-dna-methyltransferase (MGMT) 1 Also known as hepatic O 6 -alkylguanine-dna alkyltransferase (AGT, AGAT) Reverses alkylation at O 6 position of guanine, prevents cell death High tumor levels cause resistance to alkylating agents Low tumor levels cause susceptibility to alkylating drugs MGMT and TMZ 2 Retrospective analysis of MGMT tumor content and TMZ sensitivity in EORTC/NCIC trial data Low levels of MGMT in glioblastoma tumors correspond with improved response to TMZ 1. Esteller M, et al. N Engl J Med. 2000;343: Hegi ME, et al. N Engl J Med. 2005;352:
16 MGMT Promoter Methylation and GBM: Outcomes MGMT unmethylated TMZ EORTC/NCIC Trial 1 Median 2-yr 3-yr 4-yr 5-yr 12.6 months 14.8% 11/1% 11.1% 8.3% RT only 11.8 months 1.8% 0% 0% 0% MGMT methylated TMZ 23.4 months 48.9% 23.1% 23.1% 13.8% RT only 15.3 months 23.9% 7.8% 7.8% 5.2% Methylation of MGMT promoter is a strong predictor for outcome and benefit from temozolomide chemotherapy 1,2 1. Stupp R, et al. Lancet Oncol. 2009;10: Hegi ME, et al. N Engl J Med. 2005;352: Current Treatment Remaining Questions Which aspect of the EORTC regimen has influenced survival? Which new treatments can be added to the EORTC regimen? How much TMZ should be given following radiation therapy (dose and duration)? Pseudoprogression? May appear as progression either clinically or by imaging May result in erroneous treatment modification Consider continuation of treatment despite early progressive changes 16

 in 32 patients and early disease progression in 18")
 of 23 methylated MGMT promoter and 11 (41%) of 27 unmethylated MGMT")

17 Pseudoprogression Pre-op Post-XRT/TMZ Post-op After 2 cycles TMZ After 4 cycles TMZ d Avella D, et al. Acta Neurochir Suppl. 1998;71: Pseudoprogression Lesion enlargement, evidenced at the first MRI scan in 50 of 103 patients, was subsequently classified as pseudoprogression (pspd) in 32 patients and early disease progression in 18 patients. PsPD was recorded in 21 (91%) of 23 methylated MGMT promoter and 11 (41%) of 27 unmethylated MGMT promoter (P=.0002) patients. MGMT status (P=.001) and pspd detection (P=.045) significantly influenced survival. Improvement in the early recognition of pspd patterns and knowledge of mechanisms underlying this phenomenon are crucial to eliminating biases in evaluating the results of clinical trials and guaranteeing effective treatment. Brandes AA, et al. J Clin Oncol. 2008;26:
18 Best Initial Treatment Strategies: Summary Maximum safe resection Conventional fractionated EBRT (as defined by RTOG and EORTC studies) RT and concomitant TMZ (EORTC/NCIC study) Post-RT TMZ chemotherapy for 6 months (EORTC/NCIC study) National Comprehensive Cancer Network. Practice Guidelines in Oncology: Central Nervous System Cancers; Considerations for Challenging Patient Groups Elderly (age 70 and up): 20% or more of all GBM No standard of therapy; no consensus Usually excluded from trials 1 Compromised patients: 10% or more of all GBM Defined as moderate to severe impairment in performance (Karnofsky Performance Status <70) and inability to perform activities of daily living No standard of therapy; no consensus Usually excluded from trials 2 MGMT-expressing: >50% of all GBM Prospective evaluation is ongoing 1,3 1. Roa W, et al. J Clin Oncol. 2004;22: Keime-Guibert F, et al. N Engl J Med. 2007;356: Hegi ME, et al. N Engl J Med. 2005;352:
19 Genotype-Guided Therapy in High-Grade Gliomas MGMT methylation 1p19q co-deletion Isocitrate dehydrogenase 1/2 mutation (2q33) PTEN mutation EGFR overexpression/amplification/variant (EGFRvIII) VEGF expression Prognostic Classification RTOG Recursive Partitioning Classification System Patients with high-grade gliomas identified in the Radiation Therapy Oncology Group (RTOG) database Stratification into groups (Class 1 6) based on Age Performance status Histology Neurological function Duration of symptoms Extent of resection Prognostic variables may be used to compare trial data Class *GBM. Median Survival (mo) 2-Year Survival (%) * * * 9 6 6* Curran WJ Jr, et al. J Natl Cancer Inst. 1993;85: ; with permission. 19
20 Current Treatment Challenges Biologically aggressive tumors Brain localization Pharmacologic delivery Blood brain barrier Limited therapeutic response Intrinsic resistance to conventional therapies Microenvironment (hypoxia, interstitial pressure, angiogenesis) Neurotoxicity of glioma-directed treatments Susceptibility of normal brain to therapy-related injury Spread of malignant cells into brain parenchyma Chamberlain MC. Neurosurg Focus. 2006;20(4):E2. Options for Salvage Therapy Re-operation (if possible and clinically appropriate) Re-irradiation (if no other options or small-volume recurrence) Local therapy (in conjunction with re-operation or investigational therapy) Chemotherapy Bevacizumab Investigational therapy 20
21 Treatment of GBM at First Recurrence National Analysts Worldwide Survey, January 2009 (Question1b): Of your firstline GBM patients who progressed in the last 6 months, what percent fall into the following category? 10% 15% 9% 13% 1% Died before 2L diagnosis Not appropriate for/cannot tolerate further treatment Refused further treatment Progressed and will receive or have/is receiving a subsequent surgery or radiation but no systemic therapy Other Progressed and will receive subsequent systemic therapy 52% 1L Patients who progress, Q Prospective Trials of Bevacizumab for Recurrent GBM 21
22 Prospective Trials of Bevacizumab for Recurrent GBM Forty-eight heavily pretreated patients with recurrent glioblastoma were treated with bevacizumab 10 mg/kg every 2 weeks. 17 patients (35%) achieved radiographic response based on Macdonald criteria (one CR, 16 PR). Median PFS was 16 weeks (95% CI, 12 to 26 weeks). The 6-month PFS was 29% (95% CI, 18% to 48%). The 6-month OS was 57% (95% CI, 44% to 75%). Median OS was 31 weeks (95% CI, 21 to 54 weeks). Early magnetic resonance imaging response (first 96 hours and 4 weeks) was predictive of long-term PFS. Thromboembolic events (12.5%), hypertension (12.5%), hypophosphatemia (6%), and thrombocytopenia (6%) were the most common drug-associated adverse events. Six patients (12.5%) were removed from study for drug-associated toxicity (five thromboembolic events, one bowel perforation). Kreisl, et al. J Clin Oncol. 2009;27(5): Prospective Trials of Bevacizumab for Recurrent GBM Phase II, multicenter, open-label, noncomparative trial 167 patients; bevacizumab 10 mg/kg alone or in combination with irinotecan 340 mg/m 2 or 125 mg/m 2 (with or without concomitant enzymeinducing antiepileptic drugs, respectively) once every 2 weeks Primary end points: 6-month progression-free survival (42.6% (bev), 50.3% (bev + iri)) and objective response rate (28.2% (bev), 37.8% (bev+iri)) Secondary end points: safety and overall survival (median 9.2 months (bev), 8.7 months (bev+iri)) Grade 3 adverse events: 46.4% (bev; hypertension, convulsion), 65.8% (bev+iri; convulsion, neutropenia, and fatigue). Intracranial hemorrhage was noted in two patients (2.4%; bev) and three patients (3.8%; bev+iri) Bevacizumab, alone or in combination with irinotecan, was well tolerated and active in recurrent glioblastoma. The BRAIN Study. Friedman HS, et al. J Clin Oncol. 2009;27:
23 Response Rate and 6-Month PFS in Pooled Analyses of Trials for Relapsed Glioblastoma Publication Sample Size Response Rate 6-Month PFS Overall Survival 1-Year Survival 8 MD Anderson trials % 15% 5.7 months 21% 16 NCCTG trials NA 9% 5.1 months 14% 12 NABTC trials % 16% 6.9 months 25% Lomustine control arm, phase III study of % 19% 7.1 months 24% enzastaurin 4 PFS=progression-free survival. 1. Wong ET, et al. J Clin Oncol. 1999;17: Ballman KV, et al. Neuro Oncol. 2007;9: Lamborn KR, et al. Neuro Oncol. 2008;10: Wick W, et al. J Clin Oncol. 2010;28: Radiation Sensitizers Radiosensitizers Motexafin gadolinium (MGd) 1 Putative radiation enhancer Phase I trial (safety, tolerability) 2- to 6-week course of MGd 1 case-matched analysis: MGd patients: median OS 16.1 months matched RTOG database patients: median OS 11.8 months Phase II trial completed accrual (RTOG 0513) Temozolomide (TMZ) 2,3 Pre-clinical activity 1. Ford JM, et al. Int J Radiat Oncol Biol Phys. 2007;69: Kil WJ, et al. Clin Cancer Res. 2008;14: Chakravarti A, et al. Clin Cancer Res. 2006;12:
24 Temozolomide RTOG 0525 Completed Phase III trial comparing conventional adjuvant TMZ with dose-intensive TMZ in newly diagnosed GBM Radiation (60 Gy in 2-Gy fractions) + Concurrent daily TMZ ( 49d max) n=1154 Standard Arm TMZ days 1 5 of 28-day cycle for 6 cycles* Experimental Arm TMZ days 1 21 of 28-day cycle for 6 cycles* * Up to 12 cycles may be given if continued improvement shown by MRI scan, decreasing corticosteroid requirement, improvement in performance status, or improvement in neurologic function. Radiation Therapy Oncology Group (RTOG) Summaries. Brain. Available at: Accessed March 30, No statistical difference was observed between Arms 1 and 2 for median OS (16.6, 14.9 mo, p= 0.63), or median PFS (5.5, 6.7 mo, p= 0.06), or by methylation status. MGMT methylation was associated with improved OS (21.2, 14 mo, p<0.0001), PFS (8.7, 5.7 mo, p<0.0001) and response (p = 0.012). Cox modeling showed that MGMT status and RPA class were significant predictors of OS while the treatment arm and radiation technique (EORTC vs. RTOG) were not. There was increased grade 3 toxicity in Arm 2 (19%, 27%, p= 0.008); mostly lymphopenia and fatigue. Gilbert,et al. J Clin Oncol. 229:2011 (suppl; abstr 2006). Up-Front Clinical Trials for GBM (completed or near completion) Bevacizumab - UCLA study (phase II) overall survival 19.6 months, progression-free survival 13.6 months - RTOG 0825 (phase III): completed accrual - AVAGLIO (phase III): ongoing 2 Cilengitide - CENTRIC (phase III) - CORE (phase II) Cediranib - RTOG 0837 (phase II) 3 : Randomized, Phase II, Double-Blind, Placebo- Controlled Trial of Conventional Chemoradiation and Adjuvant Temozolomide Plus Cediranib versus Conventional Chemoradiation and Adjuvant Temozolomide Plus Placebo in Patients with Newly Diagnosed Glioblastoma 1. Lai, et al. J Clin Oncol. 2011;29: J Clin Oncol. 29:2011 (suppl; abstr TPS136)
 1 Platelet-derived growth factor receptor (PDGFR) 2 Vascular endothelial growth factor receptor")
25 Major Signaling Pathways in Glioma Wen PY, Kesari S. N Engl J Med. 2008;359: ; with permission. Treatment Strategies Targeted Biological Therapy Target Epidermal growth factor receptor (EGFR) 1 Platelet-derived growth factor receptor (PDGFR) 2 Vascular endothelial growth factor receptor (VEGF-R) 3 Integrin 4 Akt Pathway 5 Mammalian target of rapamycin 6 (mtor) Farnesyl transferase 7 Agent(s) Erlotinib Imatinib Cediranib, sunitinib, CEP-5214, CEP-7055 Cilengitide Perifosin (PI3K) Temsirolimus Tipifarnib 1. Rich JN, et al. J Clin Oncol. 2004;22: Akhavan, et al. Neuro Oncol. 2010;12(8): Reardon, et al. Br J Cancer. 2009;101(12): Galanis, et al. J Clin Oncol. 2005;23(23): Batchelor, et al. Cancer Cell. 2007;11: Cloughesy TF, et al. J Clin Oncol. 2006;24: Nabors, et al. Cancer. 2012; Epub ahead of print. 25
26 Treatment Strategies Targeted Biological Therapy Target Histone deacetylase (HDAC) inhibitors 1 Ras-Raf-MAPK inhibitors 2 Multiple kinase inhibitors 3 Protein Kinase C 4 Proteasome 1 STAT3 5 C-Met/Hepatic growth factor 6 Agent(s) Suberoylanilide hydroxamic acid (SAHA), valproic acid Sorafenib Vandetanib (EGFR, VEGFR), vatalanib (VEGFR2, PDGFR, c-kit), AEE788 (EGFR, VEGFR2), XL184 (Met, VEGFR2) Enzastaurin Bortezomib WP1066 AMG Friday, et al. Neuro Oncol. 2012;14(2): Hainsworth JD, et al. Cancer. 2010;116(15): Drappatz, et al. Int J Radiat Oncol Biol Phys. 2010;78(1): Wick W, et al. J Clin Oncol. 2010;28(7): Heimberger AB, et al. Recent Pat CNS Drug Discov. 2008;3(3): Wen PY, et al. Neuro Oncol. 2011;13(4): Other Emerging Treatment Concepts Vaccines Dendritic cell-based vaccines 1 Rindopepimut 2 Immunomodulatory therapy (ipilimumab; anti PD1/PD1 ligand directed therapies) 3 Cancer stem cell targeted therapy Inhibition of base excision repair strategies PARP inhibitors 4 Methoxamine 5 Novel delivery strategies Nanoparticles 6 Convection-enhanced delivery 7 PRECISE: IL-13 (Cintredekin besudotox) linked to Pseudomonas exotoxin Efficacy comparable to BCNU wafer 8 1. Knutson KL. Curr Opin Mol Ther. 2002;4: Liu L, et al. Clin Cancer Res. 2006;12: Heimberger AB, et al. Expert Opin Biol Ther. 2009;9: Patel T, et al. Adv Drug Deliv Rev. 2012;64(7): Chen, et al. Nat Rev Immunol May;4(5): Ratliff JK, Oldfield EH. J Neurosurg. 2001;95: Tentori L, et al. Pharmacol Res. 2002;45: Kunwar S, et al. Presented at SNO 2007, Abstract MA
27 Thank You 27
Contemporary Management of Glioblastoma
 Contemporary Management of Glioblastoma Incidence Rates of Primary Brain Tumors Central Brain Tumor Registry of the United States, 1992-1997 100 Number of Cases per 100,000 Population 10 1 0.1 x I x I
Contemporary Management of Glioblastoma Incidence Rates of Primary Brain Tumors Central Brain Tumor Registry of the United States, 1992-1997 100 Number of Cases per 100,000 Population 10 1 0.1 x I x I
Collection of Recorded Radiotherapy Seminars
 IAEA Human Health Campus Collection of Recorded Radiotherapy Seminars http://humanhealth.iaea.org The Role of Radiosurgery in the Treatment of Gliomas Luis Souhami, MD Professor Department of Radiation
IAEA Human Health Campus Collection of Recorded Radiotherapy Seminars http://humanhealth.iaea.org The Role of Radiosurgery in the Treatment of Gliomas Luis Souhami, MD Professor Department of Radiation
CNS Tumors: The Med Onc Perspective. Ronald J. Scheff, MD Associate Clinical Professor Weill Medical College of Cornell U.
 CNS Tumors: The Med Onc Perspective Ronald J. Scheff, MD Associate Clinical Professor Weill Medical College of Cornell U. Disclosure Speakers Bureau, Merck Basic Oncology Concepts Tissue Diagnosis Stage
CNS Tumors: The Med Onc Perspective Ronald J. Scheff, MD Associate Clinical Professor Weill Medical College of Cornell U. Disclosure Speakers Bureau, Merck Basic Oncology Concepts Tissue Diagnosis Stage
Hypofractionated radiation therapy for glioblastoma
 Hypofractionated radiation therapy for glioblastoma Luis Souhami, MD, FASTRO Professor McGill University Department of Oncology, Division of Radiation Oncology Montreal Canada McGill University Health
Hypofractionated radiation therapy for glioblastoma Luis Souhami, MD, FASTRO Professor McGill University Department of Oncology, Division of Radiation Oncology Montreal Canada McGill University Health
Concomitant (without adjuvant) temozolomide and radiation to treat glioblastoma: A retrospective study
 temozolomide and radiation to treat glioblastoma: A retrospective study") Concomitant (without adjuvant) temozolomide and radiation to treat glioblastoma: A retrospective study T Sridhar 1, A Gore 1, I Boiangiu 1, D Machin 2, R P Symonds 3 1. Department of Oncology, Leicester
Concomitant (without adjuvant) temozolomide and radiation to treat glioblastoma: A retrospective study T Sridhar 1, A Gore 1, I Boiangiu 1, D Machin 2, R P Symonds 3 1. Department of Oncology, Leicester
Carmustine implants and Temozolomide for the treatment of newly diagnosed high grade glioma
 National Institute for Health and Clinical Excellence Health Technology Appraisal Carmustine implants and Temozolomide for the treatment of newly diagnosed high grade glioma Personal statement Conventional
National Institute for Health and Clinical Excellence Health Technology Appraisal Carmustine implants and Temozolomide for the treatment of newly diagnosed high grade glioma Personal statement Conventional
Neuro-Oncology Program
 Neuro-Oncology Program The goals of the Neuro-oncology Committee are: 1) to improve duration and quality of life of brain tumor patients; 2) to assess disease and treatment-related effects on neurocognitive
Neuro-Oncology Program The goals of the Neuro-oncology Committee are: 1) to improve duration and quality of life of brain tumor patients; 2) to assess disease and treatment-related effects on neurocognitive
Antiangiogenic drugs in unresectable glioblastoma. Dra. Carmen Balañá. /
 Antiangiogenic drugs in unresectable glioblastoma Dra. Carmen Balañá. / Outcome for unresectable GBM Overall survival for unresectable GBM without further treatment is: 3 months at most. Radiotherapy increases
Antiangiogenic drugs in unresectable glioblastoma Dra. Carmen Balañá. / Outcome for unresectable GBM Overall survival for unresectable GBM without further treatment is: 3 months at most. Radiotherapy increases
UPDATES ON CHEMOTHERAPY FOR LOW GRADE GLIOMAS
 UPDATES ON CHEMOTHERAPY FOR LOW GRADE GLIOMAS Antonio M. Omuro Department of Neurology Memorial Sloan-Kettering Cancer Center II International Neuro-Oncology Congress Sao Paulo, 08/17/12 CHALLENGES IN
UPDATES ON CHEMOTHERAPY FOR LOW GRADE GLIOMAS Antonio M. Omuro Department of Neurology Memorial Sloan-Kettering Cancer Center II International Neuro-Oncology Congress Sao Paulo, 08/17/12 CHALLENGES IN
Scottish Medicines Consortium
 Scottish Medicines Consortium temozolomide 5, 20, 100 and 250mg capsules (Temodal ) Schering Plough UK Ltd No. (244/06) New indication: for the treatment of newly diagnosed glioblastoma multiforme concomitantly
Scottish Medicines Consortium temozolomide 5, 20, 100 and 250mg capsules (Temodal ) Schering Plough UK Ltd No. (244/06) New indication: for the treatment of newly diagnosed glioblastoma multiforme concomitantly
Precision medicine for gliomas
 Precision medicine for YAZMIN ODIA, MD MS LEAD PHYSICIAN OF MEDICAL NEURO-ONCOLOGY DISCLOSURES Novocure: Advisory Board for Optune in No other financial conflicts of interest Glioma OVERVIEW INFILTRATIVE,
Precision medicine for YAZMIN ODIA, MD MS LEAD PHYSICIAN OF MEDICAL NEURO-ONCOLOGY DISCLOSURES Novocure: Advisory Board for Optune in No other financial conflicts of interest Glioma OVERVIEW INFILTRATIVE,
Innovative Multimodal Imaging Techniques in Brain Tumor Clinical Trials
 Innovative Multimodal Imaging Techniques in Brain Tumor Clinical Trials Benjamin M. Ellingson, Ph.D. Assistant Professor of Radiology, Biomedical Physics, and Bioengineering Brain Tumor Imaging Laboratory
Innovative Multimodal Imaging Techniques in Brain Tumor Clinical Trials Benjamin M. Ellingson, Ph.D. Assistant Professor of Radiology, Biomedical Physics, and Bioengineering Brain Tumor Imaging Laboratory
Bevacizumab rescue therapy extends the survival in patients with recurrent malignant glioma
 Original Article Bevacizumab rescue therapy extends the survival in patients with recurrent malignant glioma Lin-Bo Cai, Juan Li, Ming-Yao Lai, Chang-Guo Shan, Zong-De Lian, Wei-Ping Hong, Jun-Jie Zhen,
Original Article Bevacizumab rescue therapy extends the survival in patients with recurrent malignant glioma Lin-Bo Cai, Juan Li, Ming-Yao Lai, Chang-Guo Shan, Zong-De Lian, Wei-Ping Hong, Jun-Jie Zhen,
MALIGNANT GLIOMAS: TREATMENT AND CHALLENGES
 MALIGNANT GLIOMAS: TREATMENT AND CHALLENGES DISCLOSURE No conflicts of interest to disclose Patricia Bruns APRN, CNS Givens Brain Tumor Center Abbott Northwestern Hospital October 12, 2018 OBJECTIVES THEN
MALIGNANT GLIOMAS: TREATMENT AND CHALLENGES DISCLOSURE No conflicts of interest to disclose Patricia Bruns APRN, CNS Givens Brain Tumor Center Abbott Northwestern Hospital October 12, 2018 OBJECTIVES THEN
It s s Always Something!
 It s s Always Something! New Approaches in Brain Tumor Treatment Virginia Stark-Vance, M.D. When Something Is a Brain Tumor Brain tumors aren t rare: there are over 100,000/yr Most originate as other cancers
It s s Always Something! New Approaches in Brain Tumor Treatment Virginia Stark-Vance, M.D. When Something Is a Brain Tumor Brain tumors aren t rare: there are over 100,000/yr Most originate as other cancers
Clinical Trials for Adult Brain Tumors - the Imaging Perspective
 Clinical Trials for Adult Brain Tumors - the Imaging Perspective Whitney B. Pope, M.D., Ph.D. Department of Radiology David Geffen School of Medicine at UCLA August 22, 2015 1 Disclosure of Financial Relationships
Clinical Trials for Adult Brain Tumors - the Imaging Perspective Whitney B. Pope, M.D., Ph.D. Department of Radiology David Geffen School of Medicine at UCLA August 22, 2015 1 Disclosure of Financial Relationships
Off-Label Treatments. Clinical Trials for Recurrent GBM UCSF Radiation Oncology Course: Management of Recurrent Disease. Outline
 Off-Label Treatments Clinical Trials for Recurrent GBM UCSF Radiation Oncology Course: Management of Recurrent Disease Jennifer Clarke, MD, MPH Assistant Professor Division of Neuro-Oncology Depts of Neurological
Off-Label Treatments Clinical Trials for Recurrent GBM UCSF Radiation Oncology Course: Management of Recurrent Disease Jennifer Clarke, MD, MPH Assistant Professor Division of Neuro-Oncology Depts of Neurological
Incidence of Early Pseudo-progression in a Cohort of Malignant Glioma Patients Treated With Chemoirradiation With Temozolomide
 405 Incidence of Early Pseudo-progression in a Cohort of Malignant Glioma Patients Treated With Chemoirradiation With Temozolomide Walter Taal, MD 1 Dieta Brandsma, MD, PhD 1 Hein G. de Bruin, MD, PhD
405 Incidence of Early Pseudo-progression in a Cohort of Malignant Glioma Patients Treated With Chemoirradiation With Temozolomide Walter Taal, MD 1 Dieta Brandsma, MD, PhD 1 Hein G. de Bruin, MD, PhD
Glioblastoma: Current Treatment Approach 8/20/2018
 Glioblastoma: Current Treatment Approach 8/20/2018 Overview What is Glioblastoma? How is it diagnosed How is it treated? Principles of Treatment Surgery, Radiation, Chemotherapy Current Standard of care
Glioblastoma: Current Treatment Approach 8/20/2018 Overview What is Glioblastoma? How is it diagnosed How is it treated? Principles of Treatment Surgery, Radiation, Chemotherapy Current Standard of care
Corporate Medical Policy
 Corporate Medical Policy Analysis of MGMT Promoter Methylation in Malignant Gliomas File Name: Origination: Last CAP Review: Next CAP Review: Last Review: analysis_of_mgmt_promoter_methylation_in_malignant_gliomas
Corporate Medical Policy Analysis of MGMT Promoter Methylation in Malignant Gliomas File Name: Origination: Last CAP Review: Next CAP Review: Last Review: analysis_of_mgmt_promoter_methylation_in_malignant_gliomas
A Single Institution s Experience with Bevacizumab in Combination with Cytotoxic Chemotherapy in Progressive Malignant Glioma
 REVIEW A Single Institution s Experience with Bevacizumab in Combination with Cytotoxic Chemotherapy in Progressive Malignant Glioma Tina Mayer, Jill Lacy and Joachim Baehring Medical Oncology, Yale University
REVIEW A Single Institution s Experience with Bevacizumab in Combination with Cytotoxic Chemotherapy in Progressive Malignant Glioma Tina Mayer, Jill Lacy and Joachim Baehring Medical Oncology, Yale University
Cilengitide (Impetreve) for glioblastoma multiforme. February 2012
 for glioblastoma multiforme. February 2012") Cilengitide (Impetreve) for glioblastoma multiforme February 2012 This technology summary is based on information available at the time of research and a limited literature search. It is not intended to
Cilengitide (Impetreve) for glioblastoma multiforme February 2012 This technology summary is based on information available at the time of research and a limited literature search. It is not intended to
Survival of High Grade Glioma Patients Treated by Three Radiation Schedules with Chemotherapy: A Retrospective Comparative Study
 Original Article Research in Oncology June 2017; Vol. 13, No. 1: 18-22. DOI: 10.21608/resoncol.2017.552.1022 Survival of High Grade Glioma Patients Treated by Three Radiation Schedules with Chemotherapy:
Original Article Research in Oncology June 2017; Vol. 13, No. 1: 18-22. DOI: 10.21608/resoncol.2017.552.1022 Survival of High Grade Glioma Patients Treated by Three Radiation Schedules with Chemotherapy:
Oncological Management of Brain Tumours. Anna Maria Shiarli SpR in Clinical Oncology 15 th July 2013
 Oncological Management of Brain Tumours Anna Maria Shiarli SpR in Clinical Oncology 15 th July 2013 Outline General considerations of Primary Brain Tumours: epidemiology, pathology, presentation. Diagnosis
Oncological Management of Brain Tumours Anna Maria Shiarli SpR in Clinical Oncology 15 th July 2013 Outline General considerations of Primary Brain Tumours: epidemiology, pathology, presentation. Diagnosis
CURRENT CONTROVERSIES IN THE MANAGEMENT OF HIGH GRADE GLIOMAS: AN INTERACTIVE CASE DISCUSSION *
 CURRENT CONTROVERSIES IN THE MANAGEMENT OF HIGH GRADE GLIOMAS: AN INTERACTIVE CASE DISCUSSION * Alessandro Olivi, MD, Jaishri Blakeley, MD, and Allen K. Sills, MD, FACS ABSTRACT The management of glioma
CURRENT CONTROVERSIES IN THE MANAGEMENT OF HIGH GRADE GLIOMAS: AN INTERACTIVE CASE DISCUSSION * Alessandro Olivi, MD, Jaishri Blakeley, MD, and Allen K. Sills, MD, FACS ABSTRACT The management of glioma
Clinical Management Protocol Chemotherapy [Glioblastoma Multiforme (CNS)] Protocol for Planning and Treatment
![Clinical Management Protocol Chemotherapy [Glioblastoma Multiforme (CNS)] Protocol for Planning and Treatment](/thumbs/87/96032554.jpg "Clinical Management Protocol Chemotherapy [Glioblastoma Multiforme (CNS)] Protocol for Planning and Treatment") Protocol for Planning and Treatment The process to be followed when a course of chemotherapy is required to treat: GLIOBLASTOMA MULTIFORME (CNS) Patient information given at each stage following agreed
Protocol for Planning and Treatment The process to be followed when a course of chemotherapy is required to treat: GLIOBLASTOMA MULTIFORME (CNS) Patient information given at each stage following agreed
PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES
 PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES CENTRAL NERVOUS SYSTEM ANAPLASTIC GLIOMAS CNS Site Group Anaplastic Gliomas Author: Dr. Norm Laperriere Date: February 20, 2018 1. INTRODUCTION
PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES CENTRAL NERVOUS SYSTEM ANAPLASTIC GLIOMAS CNS Site Group Anaplastic Gliomas Author: Dr. Norm Laperriere Date: February 20, 2018 1. INTRODUCTION
Department of Neurological Surgery, University of California, San Francisco, California
 Neurosurg Focus 37 (6):E15, 2014 AANS, 2014 Molecularly targeted therapies for recurrent glioblastoma: current and future targets Darryl Lau, M.D., Stephen T. Magill, M.D., Ph.D., and Manish K. Aghi, M.D.,
Neurosurg Focus 37 (6):E15, 2014 AANS, 2014 Molecularly targeted therapies for recurrent glioblastoma: current and future targets Darryl Lau, M.D., Stephen T. Magill, M.D., Ph.D., and Manish K. Aghi, M.D.,
21/03/2017. Disclosure. Practice Changing Articles in Neuro Oncology for 2016/17. Gliomas. Objectives. Gliomas. No conflicts to declare
 Practice Changing Articles in Neuro Oncology for 2016/17 Disclosure No conflicts to declare Frances Cusano, BScPharm, ACPR April 21, 2017 Objectives Gliomas To describe the patient selection, methodology
Practice Changing Articles in Neuro Oncology for 2016/17 Disclosure No conflicts to declare Frances Cusano, BScPharm, ACPR April 21, 2017 Objectives Gliomas To describe the patient selection, methodology
Management of Glioma: The Basics Glioma Update The clinical challenge. Glioma a malignant disease of the CNS
 Management of Glioma: The Basics Glioma Update 3 oger Stupp, MD Department of Oncology & Cancer Center University Hospital Zurich, Switzerland (roger.stupp@usz.ch) Bern, 3. August 3 The clinical challenge
Management of Glioma: The Basics Glioma Update 3 oger Stupp, MD Department of Oncology & Cancer Center University Hospital Zurich, Switzerland (roger.stupp@usz.ch) Bern, 3. August 3 The clinical challenge
Glioblastoma: Adjuvant Treatment Abdulrazag Ajlan, MD, MSc, FRCSC, UCNS(D)
") Glioblastoma: Adjuvant Treatment Abdulrazag Ajlan, MD, MSc, FRCSC, UCNS(D) *Neurosurgery Consultant, King Saud University, Riyadh, KSA *Adjunct Teaching Faculty, Neurosurgery, Stanford School Of Medicine,
Glioblastoma: Adjuvant Treatment Abdulrazag Ajlan, MD, MSc, FRCSC, UCNS(D) *Neurosurgery Consultant, King Saud University, Riyadh, KSA *Adjunct Teaching Faculty, Neurosurgery, Stanford School Of Medicine,
Bevacizumab in combination with temozolomide and regional radiation therapy for up-front treatment of patients with newly-diagnosed glioblastoma
 Bevacizumab in combination with temozolomide and regional radiation therapy for up-front treatment of patients with newly-diagnosed glioblastoma Design and analysis of single-arm Phase II clinical trial
Bevacizumab in combination with temozolomide and regional radiation therapy for up-front treatment of patients with newly-diagnosed glioblastoma Design and analysis of single-arm Phase II clinical trial
Treatment with Tumor-Treating Fields therapy and pulse dose bevacizumab in patients with bevacizumab-refractory recurrent glioblastoma: A case series.
 School of Medicine Digital Commons@Becker Open Access Publications 2016 Treatment with Tumor-Treating Fields therapy and pulse dose bevacizumab in patients with bevacizumab-refractory recurrent glioblastoma:
School of Medicine Digital Commons@Becker Open Access Publications 2016 Treatment with Tumor-Treating Fields therapy and pulse dose bevacizumab in patients with bevacizumab-refractory recurrent glioblastoma:
University of Zurich. Temozolomide and MGMT forever? Zurich Open Repository and Archive. Weller, M. Year: 2010
 University of Zurich Zurich Open Repository and Archive Winterthurerstr. 190 CH-8057 Zurich Year: 2010 Temozolomide and MGMT forever? Weller, M Weller, M (2010). Temozolomide and MGMT forever? Neuro-Oncology,
University of Zurich Zurich Open Repository and Archive Winterthurerstr. 190 CH-8057 Zurich Year: 2010 Temozolomide and MGMT forever? Weller, M Weller, M (2010). Temozolomide and MGMT forever? Neuro-Oncology,
PROCARBAZINE, lomustine, and vincristine (PCV) is
 is") RAPID PUBLICATION Procarbazine, Lomustine, and Vincristine () Chemotherapy for Anaplastic Astrocytoma: A Retrospective Review of Radiation Therapy Oncology Group Protocols Comparing Survival With Carmustine
RAPID PUBLICATION Procarbazine, Lomustine, and Vincristine () Chemotherapy for Anaplastic Astrocytoma: A Retrospective Review of Radiation Therapy Oncology Group Protocols Comparing Survival With Carmustine
Temozolomide with Radiotherapy for the Treatment of Malignant Gliomas, Center Experience
 Temozolomide with Radiotherapy for the Treatment of Malignant Gliomas, Center Experience *Ehab Abdou and **Mohamed Gaafar *Department of Radiation Oncology, Faculty of Medicine, Al-Azhar University, Cairo,
Temozolomide with Radiotherapy for the Treatment of Malignant Gliomas, Center Experience *Ehab Abdou and **Mohamed Gaafar *Department of Radiation Oncology, Faculty of Medicine, Al-Azhar University, Cairo,
THE EFFECTIVE OF BRAIN CANCER AND XAY BETWEEN THEORY AND IMPLEMENTATION. Mustafa Rashid Issa
 THE EFFECTIVE OF BRAIN CANCER AND XAY BETWEEN THEORY AND IMPLEMENTATION Mustafa Rashid Issa ABSTRACT: Illustrate malignant tumors that form either in the brain or in the nerves originating in the brain.
THE EFFECTIVE OF BRAIN CANCER AND XAY BETWEEN THEORY AND IMPLEMENTATION Mustafa Rashid Issa ABSTRACT: Illustrate malignant tumors that form either in the brain or in the nerves originating in the brain.
PRESURGICAL PLANNING. Strongly consider neuropsychological evaluation before functional imaging study Strongly consider functional imaging study
 NOTE: Consider Clinical Trials as treatment options for eligible patients. Page 1 of 6 RADIOLOGICAL PRESENTATION PRESURGICAL PLANNING TREATMENT Imaging study suggestive of glioma 1 Left hemisphere speech/motor
NOTE: Consider Clinical Trials as treatment options for eligible patients. Page 1 of 6 RADIOLOGICAL PRESENTATION PRESURGICAL PLANNING TREATMENT Imaging study suggestive of glioma 1 Left hemisphere speech/motor
Systemic Treatment. Third International Neuro-Oncology Course. 23 May 2014
 Low-Grade Astrocytoma of the CNS: Systemic Treatment Third International Neuro-Oncology Course São Paulo, Brazil 23 May 2014 John de Groot, MD Associate Professor, Neuro-Oncology UT MD Anderson Cancer
Low-Grade Astrocytoma of the CNS: Systemic Treatment Third International Neuro-Oncology Course São Paulo, Brazil 23 May 2014 John de Groot, MD Associate Professor, Neuro-Oncology UT MD Anderson Cancer
CILENT P Leblond, DIPG Meeting, Barcelone 2012
 CILENT-0902 Cilengitide (EMD121974) in combination with irradiation in children and adolescents with newly diagnosed diffuse intrinsic brainstem glioma : Phase I Study P Leblond, DIPG Meeting, Barcelone
CILENT-0902 Cilengitide (EMD121974) in combination with irradiation in children and adolescents with newly diagnosed diffuse intrinsic brainstem glioma : Phase I Study P Leblond, DIPG Meeting, Barcelone
National Horizon Scanning Centre. Bevacizumab (Avastin) for glioblastoma multiforme - relapsed. August 2008
 for glioblastoma multiforme - relapsed. August 2008") Bevacizumab (Avastin) for glioblastoma multiforme - relapsed August 2008 This technology summary is based on information available at the time of research and a limited literature search. It is not intended
Bevacizumab (Avastin) for glioblastoma multiforme - relapsed August 2008 This technology summary is based on information available at the time of research and a limited literature search. It is not intended
Radioterapia no Tratamento dos Gliomas de Baixo Grau
 Radioterapia no Tratamento dos Gliomas de Baixo Grau Dr. Luis Souhami University Montreal - Canada Low Grade Gliomas Relatively rare Heterogeneous, slow growing tumors WHO Classification Grade I Pilocytic
Radioterapia no Tratamento dos Gliomas de Baixo Grau Dr. Luis Souhami University Montreal - Canada Low Grade Gliomas Relatively rare Heterogeneous, slow growing tumors WHO Classification Grade I Pilocytic
University of Colorado Cancer Center Brain Disease Site Schema
 GBM FIRST LINE 18 0376/Kazia Phase 2a study (Part 1): A phase 2a study to evaluate the safety, pharmacokinetics and clinical activity of the PI3K/mTOR inhibitor GDC 0084 administered to patients with glioblastoma
GBM FIRST LINE 18 0376/Kazia Phase 2a study (Part 1): A phase 2a study to evaluate the safety, pharmacokinetics and clinical activity of the PI3K/mTOR inhibitor GDC 0084 administered to patients with glioblastoma
Optimal Management of Isolated HER2+ve Brain Metastases
 Optimal Management of Isolated HER2+ve Brain Metastases Eliot Sims November 2013 Background Her2+ve patients 15% of all breast cancer Even with adjuvant trastuzumab 10-15% relapse Trastuzumab does not
Optimal Management of Isolated HER2+ve Brain Metastases Eliot Sims November 2013 Background Her2+ve patients 15% of all breast cancer Even with adjuvant trastuzumab 10-15% relapse Trastuzumab does not
Lynn S. Ashby 1*, Kris A. Smith 2 and Baldassarre Stea 3
 Ashby et al. World Journal of Surgical Oncology (2016) 14:225 DOI 10.1186/s12957-016-0975-5 REVIEW Gliadel wafer implantation combined with standard radiotherapy and concurrent followed by adjuvant temozolomide
Ashby et al. World Journal of Surgical Oncology (2016) 14:225 DOI 10.1186/s12957-016-0975-5 REVIEW Gliadel wafer implantation combined with standard radiotherapy and concurrent followed by adjuvant temozolomide
Advances in Brain Tumor Research: Leveraging BIG data for BIG discoveries
 Advances in Brain Tumor Research: Leveraging BIG data for BIG discoveries Jill Barnholtz-Sloan, PhD Associate Professor & Associate Director for Bioinformatics and Translational Informatics jsb42@case.edu
Advances in Brain Tumor Research: Leveraging BIG data for BIG discoveries Jill Barnholtz-Sloan, PhD Associate Professor & Associate Director for Bioinformatics and Translational Informatics jsb42@case.edu
Zurich Open Repository and Archive. Long-term survival of glioblastoma patients treated with radiotherapy and lomustine plus temozolomide
 University of Zurich Zurich Open Repository and Archive Winterthurerstr. 190 CH-8057 Zurich http://www.zora.uzh.ch Year: 2009 Long-term survival of glioblastoma patients treated with radiotherapy and lomustine
University of Zurich Zurich Open Repository and Archive Winterthurerstr. 190 CH-8057 Zurich http://www.zora.uzh.ch Year: 2009 Long-term survival of glioblastoma patients treated with radiotherapy and lomustine
Marizomib (MRZ): Brain Penetrant Irreversible Pan-Proteasome Inhibitor
: Brain Penetrant Irreversible Pan-Proteasome Inhibitor") MARIZOMIB (MRZ) WITH BEVACIZUMAB (BEV) IN WHO GRADE IV MALIGNANT GLIOMA (G4 MG): FULL ENROLLMENT RESULTS FROM THE PHASE 1, MULTICENTER, OPEN-LABEL STUDY Daniela Bota, MD, PhD 1, Annick Desjardins, MD,
MARIZOMIB (MRZ) WITH BEVACIZUMAB (BEV) IN WHO GRADE IV MALIGNANT GLIOMA (G4 MG): FULL ENROLLMENT RESULTS FROM THE PHASE 1, MULTICENTER, OPEN-LABEL STUDY Daniela Bota, MD, PhD 1, Annick Desjardins, MD,
ORIGINAL PAPERS. The Impact of Surgery on the Efficacy of Adjuvant Therapy in Glioblastoma Multiforme
 ORIGINAL PAPERS Adv Clin Exp Med 2015, 24, 2, 279 287 DOI: 10.17219/acem/40456 Copyright by Wroclaw Medical University ISSN 1899 5276 Anna Brzozowska 1, 2, A D, Anna Toruń 3, G, Maria Mazurkiewicz1, 2,
ORIGINAL PAPERS Adv Clin Exp Med 2015, 24, 2, 279 287 DOI: 10.17219/acem/40456 Copyright by Wroclaw Medical University ISSN 1899 5276 Anna Brzozowska 1, 2, A D, Anna Toruń 3, G, Maria Mazurkiewicz1, 2,
New Approaches in Brain Tumor Treatment. Virginia Stark-Vance, M.D.
 New Approaches in Brain Tumor Treatment Virginia Stark-Vance, M.D. The Primary Brain Tumors es for PicturesMCD for 004.JPG 00 Meningioma 30% Glioblastoma 20% Astrocytoma 10% Nerve sheath 8% Pituitary 6%
New Approaches in Brain Tumor Treatment Virginia Stark-Vance, M.D. The Primary Brain Tumors es for PicturesMCD for 004.JPG 00 Meningioma 30% Glioblastoma 20% Astrocytoma 10% Nerve sheath 8% Pituitary 6%
2011 Oncology Highlights News from ASCO 2011:
 2011 Oncology Highlights News from ASCO 2011: Malignant Glioma David A. Reardon, M.D. Clinical Director Center for Neuro-Oncology Dana-Farber Cancer Institute 450 Brookline Avenue SW-430 Boston, MA 02215
2011 Oncology Highlights News from ASCO 2011: Malignant Glioma David A. Reardon, M.D. Clinical Director Center for Neuro-Oncology Dana-Farber Cancer Institute 450 Brookline Avenue SW-430 Boston, MA 02215
Low grade glioma: a journey towards a cure
 Editorial Page 1 of 5 Low grade glioma: a journey towards a cure Ali K. Choucair SIU School of Medicine, Springfield, IL, USA Correspondence to: Ali K. Choucair, MD. Professor of Neurology, Director of
Editorial Page 1 of 5 Low grade glioma: a journey towards a cure Ali K. Choucair SIU School of Medicine, Springfield, IL, USA Correspondence to: Ali K. Choucair, MD. Professor of Neurology, Director of
성균관대학교삼성창원병원신경외과학교실신경종양학 김영준. KNS-MT-03 (April 15, 2015)
") 성균관대학교삼성창원병원신경외과학교실신경종양학 김영준 INTRODUCTIONS Low grade gliomas (LGG) - heterogeneous group of tumors with astrocytic, oligodendroglial, ependymal, or mixed cellular histology - In adults diffuse, infiltrating
성균관대학교삼성창원병원신경외과학교실신경종양학 김영준 INTRODUCTIONS Low grade gliomas (LGG) - heterogeneous group of tumors with astrocytic, oligodendroglial, ependymal, or mixed cellular histology - In adults diffuse, infiltrating
Zurich Open Repository and Archive. Long-term survival of glioblastoma patients treated with radiotherapy and lomustine plus temozolomide
 University of Zurich Zurich Open Repository and Archive Winterthurerstr. 19 CH-857 Zurich http://www.zora.uzh.ch Year: 29 Long-term survival of glioblastoma patients treated with radiotherapy and lomustine
University of Zurich Zurich Open Repository and Archive Winterthurerstr. 19 CH-857 Zurich http://www.zora.uzh.ch Year: 29 Long-term survival of glioblastoma patients treated with radiotherapy and lomustine
Adjuvant treatment of high grade gliomas
 17 (Supplement 10): x186 x190, 2006 doi:10.1093/annonc/mdl258 Adjuvant treatment of high grade gliomas M. J. van den Bent Department of Neuro-Oncology, Erasmus University Hospital Rotterdam/Rotterdam Cancer
17 (Supplement 10): x186 x190, 2006 doi:10.1093/annonc/mdl258 Adjuvant treatment of high grade gliomas M. J. van den Bent Department of Neuro-Oncology, Erasmus University Hospital Rotterdam/Rotterdam Cancer
Brain Schema March 2018
 Breast Cancer w/brain Mets 14 2283 / Lilly Abemaciclib PO Breast Ca or Melanoma mets allowed Leptomeningeal mets excluded Want brain met tissue Melanoma w/brain Mets 14 2209 / Bristol Myers Squibb Nivolumab
Breast Cancer w/brain Mets 14 2283 / Lilly Abemaciclib PO Breast Ca or Melanoma mets allowed Leptomeningeal mets excluded Want brain met tissue Melanoma w/brain Mets 14 2209 / Bristol Myers Squibb Nivolumab
VAL-083: Validated DNA-targeting Agent for Underserved Cancer Patients. September 2018
 VAL-083: Validated DNA-targeting Agent for Underserved Cancer Patients September 2018 Forward-Looking Statements Any statements contained in this presentation that do not describe historical facts may
VAL-083: Validated DNA-targeting Agent for Underserved Cancer Patients September 2018 Forward-Looking Statements Any statements contained in this presentation that do not describe historical facts may
Protocol Abstract and Schema
 Protocol Abstract and Schema Phase II study of Bevacizumab plus Irinotecan (Camptosar ) in Children with Recurrent, Progressive, or Refractory Malignant Gliomas, Diffuse/Intrinsic Brain Stem Gliomas, Medulloblastomas,
Protocol Abstract and Schema Phase II study of Bevacizumab plus Irinotecan (Camptosar ) in Children with Recurrent, Progressive, or Refractory Malignant Gliomas, Diffuse/Intrinsic Brain Stem Gliomas, Medulloblastomas,
RT +/- Surgery. Concurrent ChemoRT +/- Surgery
 Molecular targeted approaches to head and neck cancer Lillian L. Siu Department of Medical Oncology & Hematology Princess Margaret Hospital, University of Toronto Locally Advanced HNSCC Locally Advanced
Molecular targeted approaches to head and neck cancer Lillian L. Siu Department of Medical Oncology & Hematology Princess Margaret Hospital, University of Toronto Locally Advanced HNSCC Locally Advanced
Radiation and concomitant chemotherapy for patients with glioblastoma multiforme
 Chinese Journal of Cancer Review Radiation and concomitant chemotherapy for patients with glioblastoma multiforme Salvador Villà 1, Carme Balañà 2 and Sílvia Comas 1 Abstract Postoperative external beam
Chinese Journal of Cancer Review Radiation and concomitant chemotherapy for patients with glioblastoma multiforme Salvador Villà 1, Carme Balañà 2 and Sílvia Comas 1 Abstract Postoperative external beam
Table 7: PBTC Protocols [ ] Protocol Title Strata Status Neuroimaging Objective/Test
![Table 7: PBTC Protocols [ ] Protocol Title Strata Status Neuroimaging Objective/Test](/thumbs/82/85455518.jpg "Table 7: PBTC Protocols [ ] Protocol Title Strata Status Neuroimaging Objective/Test") Table 7: PBTC Protocols [001 009] Protocol Title Strata Status Neuroimaging Objective/Test PBTC-001 PBTC-002 PBTC-003 PBTC-004 PBTC-005 PBTC-006 PBTC-007 PBTC-009 A Pilot of Systemic and Intrathecal Chemotherapy
Table 7: PBTC Protocols [001 009] Protocol Title Strata Status Neuroimaging Objective/Test PBTC-001 PBTC-002 PBTC-003 PBTC-004 PBTC-005 PBTC-006 PBTC-007 PBTC-009 A Pilot of Systemic and Intrathecal Chemotherapy
Dose dense 1 week on/1 week off temozolomide in recurrent glioma: a retrospective study
 J Neurooncol (2012) 108:195 200 DOI 10.1007/s11060-012-0832-5 CLINICAL STUDY Dose dense 1 week on/1 week off temozolomide in recurrent glioma: a retrospective study Walter Taal Joyce M. W. Segers-van Rijn
J Neurooncol (2012) 108:195 200 DOI 10.1007/s11060-012-0832-5 CLINICAL STUDY Dose dense 1 week on/1 week off temozolomide in recurrent glioma: a retrospective study Walter Taal Joyce M. W. Segers-van Rijn
Going Past the Data for Temozolomide. J. Lee Villano, M.D., Ph.D., Nathalie Letarte, B.Pharm, M.Sc, Linda R. Bressler, Pharm. D.
 Going Past the Data for Temozolomide J. Lee Villano, M.D., Ph.D., Nathalie Letarte, B.Pharm, M.Sc, Linda R. Bressler, Pharm. D. Departments of Medicine (JLV), Neurosurgery (JLV) and Pharmacy Practice (LRB)
Going Past the Data for Temozolomide J. Lee Villano, M.D., Ph.D., Nathalie Letarte, B.Pharm, M.Sc, Linda R. Bressler, Pharm. D. Departments of Medicine (JLV), Neurosurgery (JLV) and Pharmacy Practice (LRB)
10/16/2012. Neuro-Oncology The Beginnings. Neuro-Oncology The Beginnings. Primary Brain Tumors. Types of Primary Brain Tumors
 Neuro Oncology From Old to New Maciej M Mrugala, MD, PhD, MPH Associate Professor Department of Neurology and Neurosurgery University of Washington Medical Center Neuro-Oncology The Beginnings Galen (129
Neuro Oncology From Old to New Maciej M Mrugala, MD, PhD, MPH Associate Professor Department of Neurology and Neurosurgery University of Washington Medical Center Neuro-Oncology The Beginnings Galen (129
Imaging for suspected glioma
 Imaging for suspected glioma 1.1.1 Offer standard structural MRI (defined as T2 weighted, FLAIR, DWI series and T1 pre- and post-contrast volume) as the initial diagnostic test for suspected glioma, unless
Imaging for suspected glioma 1.1.1 Offer standard structural MRI (defined as T2 weighted, FLAIR, DWI series and T1 pre- and post-contrast volume) as the initial diagnostic test for suspected glioma, unless
NON-SURGICAL STRATEGY FOR ADULT EPENDYMOMA
 NON-SURGICAL STRATEGY FOR ADULT EPENDYMOMA Roberta Rudà Department of Neuro-Oncology University and City of Health and Science Hospital of Turin, Italy EORTC EANO ESMO Conference 2015 Istanbul, March 27-28
NON-SURGICAL STRATEGY FOR ADULT EPENDYMOMA Roberta Rudà Department of Neuro-Oncology University and City of Health and Science Hospital of Turin, Italy EORTC EANO ESMO Conference 2015 Istanbul, March 27-28
RINDOPEPIMUT (CDX-110) IN GLIOBLASTOMA
 IN GLIOBLASTOMA") RINDOPEPIMUT (CDX-110) IN GLIOBLASTOMA MULTIFORM GEINO 2014 Dra Estela Pineda Madrid Hospital Clínic Barcelona EGFRvIII in glioblastoma multiform The most common mutation of EGFR in GBM Expressed in 30%
RINDOPEPIMUT (CDX-110) IN GLIOBLASTOMA MULTIFORM GEINO 2014 Dra Estela Pineda Madrid Hospital Clínic Barcelona EGFRvIII in glioblastoma multiform The most common mutation of EGFR in GBM Expressed in 30%
PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES
 PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES CENTRAL NERVOUS SYSTEM LOW GRADE GLIOMAS CNS Site Group Low Grade Gliomas Author: Dr. Norm Laperriere 1. INTRODUCTION 3 2. PREVENTION 3 3. SCREENING
PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES CENTRAL NERVOUS SYSTEM LOW GRADE GLIOMAS CNS Site Group Low Grade Gliomas Author: Dr. Norm Laperriere 1. INTRODUCTION 3 2. PREVENTION 3 3. SCREENING
CNS SESSION 3/8/ th Multidisciplinary Management of Cancers: A Case based Approach
 CNS SESSION Chair: Ruben Fragoso, MD/PhD UC Davis Fellow: Michael Cardenas, MD UC Davis Panel: Gordon Li, MD Stanford Seema Nagpal, MD Stanford Jennie Taylor, MD UCSF HPI: 46 yo right handed woman who
CNS SESSION Chair: Ruben Fragoso, MD/PhD UC Davis Fellow: Michael Cardenas, MD UC Davis Panel: Gordon Li, MD Stanford Seema Nagpal, MD Stanford Jennie Taylor, MD UCSF HPI: 46 yo right handed woman who
3-D conformal radiotherapy with concomitant and adjuvant temozolomide for patients with glioblastoma multiforme and evaluation of prognostic factors
 research article 213 3-D conformal radiotherapy with concomitant and adjuvant temozolomide for patients with glioblastoma multiforme and evaluation of prognostic factors Yilmaz Tezcan and Mehmet Koc Department
research article 213 3-D conformal radiotherapy with concomitant and adjuvant temozolomide for patients with glioblastoma multiforme and evaluation of prognostic factors Yilmaz Tezcan and Mehmet Koc Department
Predictive Biomarkers in GBM
 Predictive Biomarkers in GBM C. David James, Ph.D. Professor & Associate Director, Brain Tumor Research Center Dept. Neurological Surgery and Helen Diller Comprehensive Cancer Center, University of California
Predictive Biomarkers in GBM C. David James, Ph.D. Professor & Associate Director, Brain Tumor Research Center Dept. Neurological Surgery and Helen Diller Comprehensive Cancer Center, University of California
Interferon β and temozolomide combination therapy for temozolomide monotherapy refractory malignant gliomas
 MOLECULAR AND CLINICAL ONCOLOGY 3: 909-913, 2015 Interferon β and temozolomide combination therapy for temozolomide monotherapy refractory malignant gliomas HIROSHI KAWAJI, TSUTOMU TOKUYAMA, TOMOHIRO YAMASAKI,
MOLECULAR AND CLINICAL ONCOLOGY 3: 909-913, 2015 Interferon β and temozolomide combination therapy for temozolomide monotherapy refractory malignant gliomas HIROSHI KAWAJI, TSUTOMU TOKUYAMA, TOMOHIRO YAMASAKI,
Elderly Patients with Glioblastoma Multiforme Treated with Concurrent Temozolomide and Standard- versus Abbreviated-Course Radiotherapy
 Elderly Patients with Glioblastoma Multiforme Treated with Concurrent Temozolomide and Standard- versus Abbreviated-Course Radiotherapy Christine N Chang-Halpenny, MD; Jekwon Yeh, MD; Winston W Lien, MD
Elderly Patients with Glioblastoma Multiforme Treated with Concurrent Temozolomide and Standard- versus Abbreviated-Course Radiotherapy Christine N Chang-Halpenny, MD; Jekwon Yeh, MD; Winston W Lien, MD
NOTE: PODCAST/MP3 PROGRAM 1
 PODCAST/MP3 PROGRAM 1 I N S T R U C T I O N S This program consists of a podcast/mp3 audio file and a printable PDF of the post-test that can be submitted for credit and/or used to assist learning. You
PODCAST/MP3 PROGRAM 1 I N S T R U C T I O N S This program consists of a podcast/mp3 audio file and a printable PDF of the post-test that can be submitted for credit and/or used to assist learning. You
J Clin Oncol 27: by American Society of Clinical Oncology INTRODUCTION
 VOLUME 27 NUMBER 8 MARCH 10 2009 JOURNAL OF CLINICAL ONCOLOGY O R I G I N A L R E P O R T Recurrence Pattern After Temozolomide Concomitant With and Adjuvant to Radiotherapy in Newly Diagnosed Patients
VOLUME 27 NUMBER 8 MARCH 10 2009 JOURNAL OF CLINICAL ONCOLOGY O R I G I N A L R E P O R T Recurrence Pattern After Temozolomide Concomitant With and Adjuvant to Radiotherapy in Newly Diagnosed Patients
Temozolomide Concomitant and Adjuvant to Radiotherapy in Elderly Patients With Glioblastoma
 Temozolomide Concomitant and Adjuvant to Radiotherapy in Elderly Patients With Glioblastoma Correlation With MGMT Promoter Methylation Status Alba A. Brandes, MD 1 ; Enrico Franceschi, MD 1 ; Alicia Tosoni,
Temozolomide Concomitant and Adjuvant to Radiotherapy in Elderly Patients With Glioblastoma Correlation With MGMT Promoter Methylation Status Alba A. Brandes, MD 1 ; Enrico Franceschi, MD 1 ; Alicia Tosoni,
Glioblastoma and CNS tumors
 Glioblastoma and CNS tumors PRECEPTORSHIP PROGRAMME IMMUNO-ONCOLOGY Amsterdam, 27 May 2017 Patrick Roth Department of Neurology and Brain Tumor Center University Hospital Zurich Challenges in immunooncology
Glioblastoma and CNS tumors PRECEPTORSHIP PROGRAMME IMMUNO-ONCOLOGY Amsterdam, 27 May 2017 Patrick Roth Department of Neurology and Brain Tumor Center University Hospital Zurich Challenges in immunooncology
Brain Tumors: Radiologic Perspective
 Brain Tumors: Radiologic Perspective Alberto Bizzi, M.D. Neuroradiology Humanitas Research Hospital Milan, Italy The job of the neuroradiologist in the work-up of brain tumors has quite changed in the
Brain Tumors: Radiologic Perspective Alberto Bizzi, M.D. Neuroradiology Humanitas Research Hospital Milan, Italy The job of the neuroradiologist in the work-up of brain tumors has quite changed in the
High-Grade Gliomas. Andrew B. Lassman, Diana Matceyevsky, and Benjamin W. Corn ETIOLOGY AND EPIDEMIOLOGY PREVENTION AND EARLY DETECTION
 C H A P T E R 27 High-Grade Gliomas Andrew B. Lassman, Diana Matceyevsky, and Benjamin W. Corn INCIDENCE There are approximately 68,000 new cases of brain tumors diagnosed in the United States each year.
C H A P T E R 27 High-Grade Gliomas Andrew B. Lassman, Diana Matceyevsky, and Benjamin W. Corn INCIDENCE There are approximately 68,000 new cases of brain tumors diagnosed in the United States each year.
2015 EUROPEAN CANCER CONGRESS
 2015 EUROPEAN CANCER CONGRESS 25-29 September 2015 Vienna, Austria SUMMARY The European Cancer Congress (ECC 2015) combined the 40th European Society for Medical Oncology (ESMO) congress with the 18th
2015 EUROPEAN CANCER CONGRESS 25-29 September 2015 Vienna, Austria SUMMARY The European Cancer Congress (ECC 2015) combined the 40th European Society for Medical Oncology (ESMO) congress with the 18th
EORTC (RTOG 0834 Endorsed) Opened: July 22, 2009
 Opened: July 22, 2009") January 2011 0834-1 EORTC 26053 22054 (RTOG 0834 Endorsed) Protocol Status: Opened: July 22, 2009 Title: Phase III Trial on Concurrent and Adjuvant Temozolomide Chemotherapy in Non-1P/19Q Deleted Anaplastic
January 2011 0834-1 EORTC 26053 22054 (RTOG 0834 Endorsed) Protocol Status: Opened: July 22, 2009 Title: Phase III Trial on Concurrent and Adjuvant Temozolomide Chemotherapy in Non-1P/19Q Deleted Anaplastic
Chemotherapy in malignant brain tumors
 Chemotherapy in malignant brain tumors Frank Zimmermann Institut für Radioonkologie Universitätsspital Basel Petersgraben 4 CH 4031 Basel zimmermannf@uhbs.ch Tumor types Neuro-epithelial tumors - Glioblastoma
Chemotherapy in malignant brain tumors Frank Zimmermann Institut für Radioonkologie Universitätsspital Basel Petersgraben 4 CH 4031 Basel zimmermannf@uhbs.ch Tumor types Neuro-epithelial tumors - Glioblastoma
Bevacizumab and dose-intense temozolomide in recurrent high-grade glioma
 Annals of Oncology 21: 1723 1727, 2010 doi:10.1093/annonc/mdp591 Published online 11 January 2010 Bevacizumab and dose-intense temozolomide in recurrent high-grade glioma J. J. C. Verhoeff 1, C. Lavini
Annals of Oncology 21: 1723 1727, 2010 doi:10.1093/annonc/mdp591 Published online 11 January 2010 Bevacizumab and dose-intense temozolomide in recurrent high-grade glioma J. J. C. Verhoeff 1, C. Lavini
Northside Cancer Institute Oncology Nursing Symposium Perspectives on Glioma. Gena Volas-Redd, MD Georgia Cancer Specialists May 19, 2012
 Northside Cancer Institute Oncology Nursing Symposium Perspectives on Glioma Gena Volas-Redd, MD Georgia Cancer Specialists May 19, 2012 Incidence: Primary Brain Tumors An estimated 51,210 new cases of
Northside Cancer Institute Oncology Nursing Symposium Perspectives on Glioma Gena Volas-Redd, MD Georgia Cancer Specialists May 19, 2012 Incidence: Primary Brain Tumors An estimated 51,210 new cases of
Targeted/Immunotherapy & Molecular Profiling State-of-the-art in Cancer Care
 Targeted/Immunotherapy & Molecular Profiling State-of-the-art in Cancer Care Manmeet Ahluwalia, MD, FACP Miller Family Endowed Chair in Neuro-Oncology Director Brain Metastasis Research Program Cleveland
Targeted/Immunotherapy & Molecular Profiling State-of-the-art in Cancer Care Manmeet Ahluwalia, MD, FACP Miller Family Endowed Chair in Neuro-Oncology Director Brain Metastasis Research Program Cleveland
Goals for this Lecture. Case 1. Key Points MRI TECHNIQUES FOR DIFFERENTIAL DIAGNOSIS OF RECURRENT BRAIN LESIONS
 MRI TECHNIQUES FOR DIFFERENTIAL DIAGNOSIS OF RECURRENT BRAIN LESIONS Goals for this Lecture 1. Review common appearances for recurrent tumor and treatment effects on conventional MRI 2. Discuss current
MRI TECHNIQUES FOR DIFFERENTIAL DIAGNOSIS OF RECURRENT BRAIN LESIONS Goals for this Lecture 1. Review common appearances for recurrent tumor and treatment effects on conventional MRI 2. Discuss current
Management of Brain Metastases Sanjiv S. Agarwala, MD
 Management of Brain Metastases Sanjiv S. Agarwala, MD Professor of Medicine Temple University School of Medicine Chief, Oncology & Hematology St. Luke s Cancer Center, Bethlehem, PA, USA Incidence (US):
Management of Brain Metastases Sanjiv S. Agarwala, MD Professor of Medicine Temple University School of Medicine Chief, Oncology & Hematology St. Luke s Cancer Center, Bethlehem, PA, USA Incidence (US):
Jon Trent, MD, PhD. Associate Professor Dept. of Sarcoma Medical Oncology The University of Texas, M. D. Anderson Cancer Center
 Gastrointestinal Stromal Tumor GISTS 2010: After Standard of Care Jon Trent, MD, PhD Associate Professor Dept. of Sarcoma Medical Oncology The University of Texas, M. D. Anderson Cancer Center jtrent@mdanderson.org
Gastrointestinal Stromal Tumor GISTS 2010: After Standard of Care Jon Trent, MD, PhD Associate Professor Dept. of Sarcoma Medical Oncology The University of Texas, M. D. Anderson Cancer Center jtrent@mdanderson.org
Protocol Abstract and Schema
 Protocol Abstract and Schema This is a phase I/II study to determine: 1) the maximum tolerated dose (MTD) or recommended phase II dose of ABT-888 in combination with radiation therapy, and 2) the efficacy
Protocol Abstract and Schema This is a phase I/II study to determine: 1) the maximum tolerated dose (MTD) or recommended phase II dose of ABT-888 in combination with radiation therapy, and 2) the efficacy
Glioblastoma is the most common primary malignant brain tumor in adults and is a
 NEUROLOGICAL REVIEW Recent Advances in Therapy for Glioblastoma Jennifer Clarke, MD, MPH; Nicholas Butowski, MD; Susan Chang, MD Glioblastoma is the most common primary malignant brain tumor in adults
NEUROLOGICAL REVIEW Recent Advances in Therapy for Glioblastoma Jennifer Clarke, MD, MPH; Nicholas Butowski, MD; Susan Chang, MD Glioblastoma is the most common primary malignant brain tumor in adults
John D. Hainsworth, MD, Kent C. Shih, MD, Gregg C. Shepard, MD, Guy W. Tillinghast, MD, Brett T. Brinker, MD, and David R. Spigel, MD.
 Phase II Study of Concurrent Radiation Therapy, Temozolomide, and Bevacizumab Followed by Bevacizumab/Everolimus as First- Line Treatment for Patients With Glioblastoma John D. Hainsworth, MD, Kent C.
Phase II Study of Concurrent Radiation Therapy, Temozolomide, and Bevacizumab Followed by Bevacizumab/Everolimus as First- Line Treatment for Patients With Glioblastoma John D. Hainsworth, MD, Kent C.
Technology appraisal guidance Published: 27 June 2007 nice.org.uk/guidance/ta121
 Carmustine implants and temozolomide for the treatment of newly diagnosed high-grade glioma Technology appraisal guidance Published: 27 June 2007 nice.org.uk/guidance/ta121 NICE 2018. All rights reserved.
Carmustine implants and temozolomide for the treatment of newly diagnosed high-grade glioma Technology appraisal guidance Published: 27 June 2007 nice.org.uk/guidance/ta121 NICE 2018. All rights reserved.
Approximately half of the 18,000 new cases of central nervous system
 Radiotherapy and Radiosensitizers in the Treatment of Glioblastoma Multiforme Julie E. Chang, MD, Deepak Khuntia, MD, H. Ian Robins, MD, and Minesh P. Mehta, MD Dr. Chang is Assistant Professor in the
Radiotherapy and Radiosensitizers in the Treatment of Glioblastoma Multiforme Julie E. Chang, MD, Deepak Khuntia, MD, H. Ian Robins, MD, and Minesh P. Mehta, MD Dr. Chang is Assistant Professor in the
Brain Tumor Treatment
 Scan for mobile link. Brain Tumor Treatment Brain Tumors Overview A brain tumor is a group of abnormal cells that grows in or around the brain. Tumors can directly destroy healthy brain cells. They can
Scan for mobile link. Brain Tumor Treatment Brain Tumors Overview A brain tumor is a group of abnormal cells that grows in or around the brain. Tumors can directly destroy healthy brain cells. They can
Glioblastoma and CNS tumors
 Glioblastoma and CNS tumors PRECEPTORSHIP PROGRAMME IMMUNO-ONCOLOGY Amsterdam, 1 October 2016 Patrick Roth Department of Neurology and Brain Tumor Center University Hospital Zurich Immunology in the CNS
Glioblastoma and CNS tumors PRECEPTORSHIP PROGRAMME IMMUNO-ONCOLOGY Amsterdam, 1 October 2016 Patrick Roth Department of Neurology and Brain Tumor Center University Hospital Zurich Immunology in the CNS
Molecular Epidemiology. Financial Disclosures. Central Nervous System Tumors Neuro-Oncology Clinical Research
 Financial Disclosures Update on clinical trials for malignant glioma Susan M. Chang MD, Director of Division of Neuro-Oncology Brain Tumor Research Center Department of Neurological Surgery UCSF Research
Financial Disclosures Update on clinical trials for malignant glioma Susan M. Chang MD, Director of Division of Neuro-Oncology Brain Tumor Research Center Department of Neurological Surgery UCSF Research
Clinical Policy: Electric Tumor Treating Fields (Optune) Reference Number: PA.CP.MP.145
 Reference Number: PA.CP.MP.145") Clinical Policy: Electric Tumor Treating Fields (Optune) Reference Number: PA.CP.MP.145 Effective Date: 01/18 Last Review Date: 04/18 Coding Implications Revision Log Description Electric tumor treating
Clinical Policy: Electric Tumor Treating Fields (Optune) Reference Number: PA.CP.MP.145 Effective Date: 01/18 Last Review Date: 04/18 Coding Implications Revision Log Description Electric tumor treating
Survival Analysis of Glioblastoma Multiforme
 DOI:10.22034/APJCP.2018.19.9.2613 RESEARCH ARTICLE Editorial Process: Submission:04/24/2018 Acceptance:08/19/2018 Supapan Witthayanuwat, Montien Pesee*, Chunsri Supaadirek, Narudom Supakalin, Komsan Thamronganantasakul,
DOI:10.22034/APJCP.2018.19.9.2613 RESEARCH ARTICLE Editorial Process: Submission:04/24/2018 Acceptance:08/19/2018 Supapan Witthayanuwat, Montien Pesee*, Chunsri Supaadirek, Narudom Supakalin, Komsan Thamronganantasakul,
Minesh Mehta, Northwestern University. Chicago, IL
 * Minesh Mehta, Northwestern University Chicago, IL Consultant: Adnexus, Bayer, Merck, Tomotherapy Stock Options: Colby, Pharmacyclics, Procertus, Stemina, Tomotherapy Board of Directors: Pharmacyclics
* Minesh Mehta, Northwestern University Chicago, IL Consultant: Adnexus, Bayer, Merck, Tomotherapy Stock Options: Colby, Pharmacyclics, Procertus, Stemina, Tomotherapy Board of Directors: Pharmacyclics
Stereotactic Radiosurgery for Brain Metastasis: Changing Treatment Paradigms. Overall Clinical Significance 8/3/13
 Stereotactic Radiosurgery for Brain Metastasis: Changing Treatment Paradigms Jason Sheehan, MD, PhD Departments of Neurosurgery and Radiation Oncology University of Virginia, Charlottesville, VA USA Overall
Stereotactic Radiosurgery for Brain Metastasis: Changing Treatment Paradigms Jason Sheehan, MD, PhD Departments of Neurosurgery and Radiation Oncology University of Virginia, Charlottesville, VA USA Overall