Paediatric CNS Tumours
|
|
|
- Emma Fields
- 5 years ago
- Views:
Transcription
1 Paediatric CNS Tumours Challenges and research NBCNS meeting Sweden 2009 Dr Antony Michalski Great Ormond Street Hospital, London
2 Structure of Presentation The scale of the problem of CNS tumours History of evolution of studies How improved tools facilitate research New solutions lead to new problems Potential strategies for the future Discussion lots of discussion!
3 Malignant Brain Tumours in Children <15 years: Distributed by tumour type Medulloblastoma/PNET 23% Low Grade Supratentorial Acstrocytoma 25% Cerebellar Astrocytoma High Grade Astrocytoma 12% 11% Brain Stem Glioma Ependymoma 8% 9% Germ Cell Tumours 4% Choroid Plexus Tumours 0.5% Other 7.5%
4 Survival According to Tumour Type Cerebellar astrocytoma (109) Low grade astrocytoma (220) % Survival All types (887) Medulloblastoma (204) High grade astrocytoma (95) Ependymoma (73) 20 Brainstem Glioma (80) Years since diagnosis
5 Percent by Age (distribution of all types) % < Age
6 Survival According to Age at Diagnosis % Survival yrs (286) 5-9 yrs (313) 2-4 yrs (176) <2 yrs (112) Years since diagnosis 5
7 Brain Tumours <15 years: Treatment Approaches None 5% Surgery 19% Radiation 17% S + RT 33% S + RT + CT 15% S + CT 3% RT + CT 5% CT 1% Unknown 1%
8 Why was neuro-oncology the Cinderella of cancer therapy? Fragmentation of service delivery Difficulties in tissue collection Problems with histological classification Inability to judge response of therapy accurately and non-invasively
9 Neuro-oncology research c1970s Intracranial tumours: response and resistance to therapeutic endeavors, Bloom et al, IJROBP
10 >2 decades of improved ability to perform clinical trials Improved surgical and anaesthetic technique allowed tissue to be obtained operating microscope and beyond Agreed histopathological classification (we all agreed what we were treating.well almost all of us did) Improved neuroimaging allowed us to stage disease and measure response to therapy other than clinical response and survival More collaboration (we all agreed what the problems were) Increased recognition and improved measurement of late effects of therapy
11 How does neuroradiology help an oncologist? Helps make a diagnosis Stages disease neuraxis spread Allows assessment of response to treatment internationally agreed response criteria Helps diagnose a recurrence


12 Astonishing progress..




13 CT scan MRI scan PET scanner Angiography suite


14 Making a diagnosis sometimes without histological confirmation
15 Collaboration- how data set was obtained is important - don t do your best! Care delivered on risk-adapted protocols The radiological diagnosis changes the treatment group Treatment groups need to be homogeneous Therefore, techniques should be reproducible and consistent between participating hospitals Risk of stage migration Role of central radiological review

16 More usually a diagnosis is made using radiology and pathology
17 Agreed and updated classification The WHO Classification of Tumors of the Nervous System Kleihues P, Louis D, Scheithauer B et al Journal of Neuropathology & Experimental Neurology: Volume 61 - Issue 3 - p

18 Names are important
19 What is a diagnosis? Not just a label The data set necessary to do a job: - planning therapy - giving a prognosis - entry on to a scientific or clinical research protocol The data varies with the job to be done
20 Diagnostic labels not static New histopathological entities identified ATRT from what was called PNET Subclassification within entities Desmoplasia in PNET Massive impact of molecular biology What defines a tumour? Need for collaboration between biologists and neuropathologists
21 So, problem solved? All the major tools in place Just use the same tools in different disease types Just continue to develop the technology
22 Really good trials HIT/SIOP PNET 4 Randomised comparison of two different radiation techniques in standard risk medulloblastoma Tightly defined population, central review of key data, multinational, biological and late effects questions Run from Sweden
23 Technological development Further development of current tools Interaction with technological developers It is all very exciting but how does it help us?
24 Technological development in neurosurgical issues Knowing where you are in the brain Open surgery direct vision Operating microscope Stereotaxy and neuronavigation

25 Finding you way in neurosurgery - traditional Stereotaxy Frame based

26 Finding you way in neurosurgery Stereotaxy Frame based


27 Finding you way in neurosurgery contemporary Image guided surgery


28 Frameless stereotaxy
29 Don t cut that; it s important Neuronavigation is largely based on the anatomy doing what it normally does Plasticity of nervous system means that other areas can take over function How do you resect as much as possible safely?
30 Functional imaging Functional MRI Tractography (Dr Chris Clark, ICH, London)

31 Neurosurgical planning


32 Recurrent meningioma No hemiparesis Anaplastic Astrocytoma Left Hemiparesis Chris Clarke, ICH
33 Problems with studies Better defined subsets result in small numbers of patients to study the story of Baby brains
34 Baby-Brain Studies Duffner: VCR, cyclo, cisplat, etoposide Baram: MOPP Geyer: 8 in 1 NEJM Cancer Cancer , JCO Jeng: VBL, cisplat, etoposide IT triples Child s Nerv Syst UKCCSG: VCR, carbo, MTX, cyclo, cisplat
35 Different groups different philosophies POG delay radiotherapy for all reduce dose for those responding to chemotherapy UKCCSG - defer or avoid radiotherapy by using intensive (but not dose intensive) chemotherapy SFOP treat gently no RT - salvage recurrences with myeloablative chemotherapy and focal irradiation HIT defer (and eventually avoid) radiotherapy by using chemotherapy and intraventricular chemotherapy No agreement over age or diagnosis as entry criteria
36 UKCCSG trials Evolution of understanding of PNET
37 UKCCSG Baby Brain Study Aimed to: Delay Radiation for all Withdraw radiation for patients in CR at end of chemotherapy
38 UKCCSG CNS results EFS M0/R0 ependymoma Medulloblastoma Non-Medullo PNET years

39 Cure-alls don t work: Specific therapy for specific diseases. The end of the baby-brain era.
40 Infant PNET study Aimed to investigate maximum tolerated dose of cyclophosphamide when given with G-CSF and stem cell rich blood. Dose intensive induction Focal radiotherapy for focal disease post induction Continuation therapy post radiotherapy


41 Response to chemotherapy
42 Survival by diagnosis Medulloblastoma 20/29 alive (70%) Supratentorial PNET 1/6 alive (17%) Pineoblastoma 1/8 alive (12.5%) Choroid plexus carcinoma 0/3 alive ATRT 0/2 alive Other 2/4 alive
43 The end of the PNET era?
44 Results of HIT/SKK EFS M0/R0 M0/R+ 20 M2/3 P= years NEJM 2005
45 The end of the infant medulloblastoma era?
46 In >3y olds biology predicts bad actors Survival No 17p13.3 loss 17p13.3 loss P= years Clinical Cancer Res 2004
47 More biological prognosticators.. CGH Expression profiling TrkC expression Survival MYC amplification Epigenetic events (RASSF1A, CASP8) β-catenin PTCH
48 Does that mean we need to split M0 infant medulloblastoma group any more?
49 Role of desmoplasia in <3year olds EFS % Desmoplastic % Classic 20 P= years NEJM 2005
50 Evolution of baby-brain trials All diagnoses PNET Medullo S/T PNET M0 M+ Desmoplasia Resection? Biology?
51 Future studies in infant medulloblastoma Small groups with different outcomes Small numbers No chance of running randomised studies with decent power How do we run small studies? First past the post, pick a winner, Baysian stats? Do we believe results?
52 Lots of problems persist Survival of UKCCSG Patients Diagnosed , by Calendar Period High-Grade Astrocytoma 100 % still alive Years since diagnosis
53 Novel molecular therapies in neuro-oncology Blocking tumour angiogenesis Blocking signal transduction from overactive oncogenes Blocking tumour invasion Promoting apoptosis Decreasing DNA transcription - histone de-acetylation Response my not result in immediate shrinkage in size Do we have the tools to measure what we are doing? Herrington and Kieran 2009 Pediatr Blood and Cancer
54 Rational molecular therapy Confirm target is present in a given tumour Show drug gets to target Show drug blocks target Show that this has desired effect on molecular pathway (no escape) Investigate clinical response to blockade Is this practical?
55 Surrogates for response Measuring tumour vascularity Measuring tumour metabolism (MRS, PET) Changes in tumour aggressiveness Molecular neuro-imaging: From conventional to emerging techniques Hammoud et al 2007 Radiology




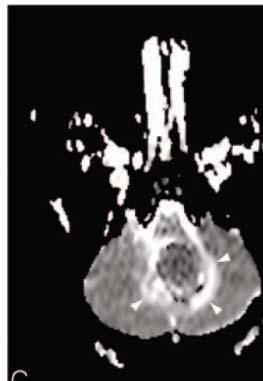
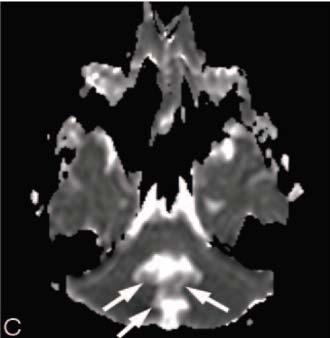
56 MR diffusion JPA Medullo Epend Rumbolt et al., 2005

57 MR Spectroscopy NAA Lipids & lactate tcr tcho tcr mi Glx MM tcho NAA
58 Average spectra of human brain tumours Meningioma Glx mi tcho tcho Glx/MM Ala Lac Lipid tcr Astrocytoma II Glx/MM Lac Lipid Astrocytoma III Lac/Lipid Glioblastoma tcho tcr MM Lipid Franklyn Howe, St George s Hospital Medical School
59 Immunotherapy Example of getting used to new response criteria

 TNF-R CD40 TNF Nature Reviews, Immunology, Drew Pardoll")
60 STRATEGIES: Ex Vivo GENERATION OF Ag PULSED DCs Leukapheresis monocytes /CD14 isolation 6 days GM-CSF + IL-4 CD14 Immature DCs Tumour Lysate Pulsing (Day7) + KLH PGP2 Vaccine Administration (Day 8) TNF-R CD40 TNF Nature Reviews, Immunology, Drew Pardoll Activated DCs
61 Primary Study endpoints of osteosarcoma trial (immunological) Specific IFNγ / IL2/ Granzyme B release in vitro following addition of autologous tumour cells to PBMC collected pre and post vaccines Flow cytometric charcterisation of IFNγ secreting cells Local skin reaction to sequential vaccinations Secondary immunological endpoints Immunological environment of osteosarcoma (Treg, NK, NKT cells) Isolation of tumour reactive T cell clones for identification of target antigens
62 Early clinical trial data IFN-γ ELISPOT PBMC + Autologous tumour cells PBMC+ TL or Irr TL + Autologous tumour cells 250 Prevacc + TL Prevacc Patient 2 Patient 3 Post vacc2 + TL Post vacc2 200 Post vacc4 + TL Post vacc4 150 Prevacc + Irr TL Post vacc2 + Irr TL Post Vacc4 + Irr TL Number of spots Number of spots 0 0 Prevacc Post vacc2 Post vacc4 Prevacc Post vacc2 Post vacc4 Prevacc + Irr TL Post vacc2 Irr TL Post Vacc4 Irr TL Patient 4 Pre vaccination Post vaccine 2 Post vaccine 4 Spots per 10>5 cells PBMC + tumour PBMC + lysate PBMC + irrel lysate PBMC + DC/lysate 0
63 What are the clinical outcomes for immunotherapy? Early increase in tumour size Signs of inflammation Later stabilisation and shrinkage of disease in some patients How do we define success? Immunology or clinical studies or survival?
64 Research that changes understanding of disease and therapy Traditional outcomes: Treatment makes tumour smaller Treatment prolongs life

65 A success of radical craniopharyngioma surgery? 8 years old Wt > 99 th percentile Hyperphagia VA 6/60 bilaterally Hypothalmic and chiasmatic damage

66 GOS Experience De Vile et al J Neurosurg 85:
67 Craniopharyngioma diagnosd Good Risk Factors Age <7years Age >7years Attempted radical removal Limited surgery Complete removal Incomplete removal Radiotherapy Surveillance Surveillance Progression Repeat procedures Cyst aspirations/instillations >7 years
68 Craniopharyngioma diagnosed Poor Risk Factors Limited Surgery Age < 7 years Age > 7years Surveillance Radiotherapy Progression Surveillance Repeat procedures Progression Subtotal Surgery Repeat procedures
69 Late Effects and Quality of life Moving from descriptive, single institution studies to collaborative studies on homogeneously treated patients. Broad agreement on methodologies Translation and validation for national norms
70 QOL studies challenges to accepted truths Radiotherapy is always bad? excellent results of conformal RT in ependymoma (JCO ) Chemotherapy is always good? neuropsychological late effects of HD salvage (SFOP), leukencephalopathy post IV and IT MTX (HIT), chemo group worse in PNET3 Complete surgery always good? increased awareness of incidence and severity of posterior fossa syndrome.
71 Late Effects studies - future So far studies parallel clinical study results How do we use results to alter therapy? Is there a metric for what % decrease in EFS we would accept for a given % better QOL outcome? Who decides this medics, families, funders?

72 Palliative Care >30% of children still die of their disease Move to palliative care accepted part of journey What do we understand about what families want?
73 Great progress but still loads to do

74 Great progress but still loads to do Just because you have a protocol it doesn t mean you know what you are doing

75 Collaborative trials are key
76 Thanks Dr Lannering for invitation Drs Clark, Saunders, Anderson, Mr Thompson for slides and data You all for your attention
Update on Pediatric Brain Tumors
 Update on Pediatric Brain Tumors David I. Sandberg, M.D. Director of Pediatric Neurosurgery & Associate Professor Dr. Marnie Rose Professorship in Pediatric Neurosurgery Pre-talk Questions for Audience
Update on Pediatric Brain Tumors David I. Sandberg, M.D. Director of Pediatric Neurosurgery & Associate Professor Dr. Marnie Rose Professorship in Pediatric Neurosurgery Pre-talk Questions for Audience
Pediatric Oncology. Vlad Radulescu, MD
 Pediatric Oncology Vlad Radulescu, MD Objectives Review the epidemiology of childhood cancer Discuss the presenting signs and symptoms, general treatment principles and overall prognosis of the most common
Pediatric Oncology Vlad Radulescu, MD Objectives Review the epidemiology of childhood cancer Discuss the presenting signs and symptoms, general treatment principles and overall prognosis of the most common
SCIENTIFIC PROGRAMME SNOLA THE STATE OF THE ART ON NEURO-ONCOLOGY th March
 SCIENTIFIC PROGRAMME SNOLA THE STATE OF THE ART ON NEURO-ONCOLOGY 2018 15th March 13h 13h45 ROOM 1 ROOM 2 ROOM 3 Imaging and pathology case discussion Lymphomas case discussion- Meningeomas Moderator:
SCIENTIFIC PROGRAMME SNOLA THE STATE OF THE ART ON NEURO-ONCOLOGY 2018 15th March 13h 13h45 ROOM 1 ROOM 2 ROOM 3 Imaging and pathology case discussion Lymphomas case discussion- Meningeomas Moderator:
Translating MRS into clinical benefit for children with brain tumours
 Translating MRS into clinical benefit for children with brain tumours Andrew Peet NIHR Research Professor Childhood Cancer The Facts Cancer is the most common cause of death from disease in childhood Brain
Translating MRS into clinical benefit for children with brain tumours Andrew Peet NIHR Research Professor Childhood Cancer The Facts Cancer is the most common cause of death from disease in childhood Brain
Pediatric Brain Tumors Pre, Intra & Post Op Evaluation and Management. Timothy M. George, MD, FACS, FAAP
 Pediatric Brain Tumors Pre, Intra & Post Op Evaluation and Management Timothy M. George, MD, FACS, FAAP PEDIATRIC BRAIN TUMORS BACKGROUND: Incidence: Third most common pediatric tumor type (leukemia, neuroblastoma,
Pediatric Brain Tumors Pre, Intra & Post Op Evaluation and Management Timothy M. George, MD, FACS, FAAP PEDIATRIC BRAIN TUMORS BACKGROUND: Incidence: Third most common pediatric tumor type (leukemia, neuroblastoma,
CHAPTER 11 Tumors Originating in the Brain Medulloblastomas, PNETs and Ependymomas
 Tumors Originating in the Brain Medulloblastomas, PNETs and Ependymomas Foolishly, I waited 7 months before I joined this (or any) group. By that time, my son had radiation, chemo, and a recurrence of
Tumors Originating in the Brain Medulloblastomas, PNETs and Ependymomas Foolishly, I waited 7 months before I joined this (or any) group. By that time, my son had radiation, chemo, and a recurrence of
Pediatric Brain Tumors: Updates in Treatment and Care
 Pediatric Brain Tumors: Updates in Treatment and Care Writer Classroom Rishi R. Lulla, MD MS Objectives Introduce the common pediatric brain tumors Discuss current treatment strategies for pediatric brain
Pediatric Brain Tumors: Updates in Treatment and Care Writer Classroom Rishi R. Lulla, MD MS Objectives Introduce the common pediatric brain tumors Discuss current treatment strategies for pediatric brain
BRAIN TUMORS IN INFANTS
 BRAIN TUMORS IN INFANTS Dr Sergio Valenzuela M.D-( ISPN-ESPN-FLANC)&cols. Head Pediatric Neurosurgery Unit I Instituto de NeurocirugiaAsenjo Santiago CHILE RATE OF MENINGEAL,BRAIN AND OTHER CNS MALIGNANT
BRAIN TUMORS IN INFANTS Dr Sergio Valenzuela M.D-( ISPN-ESPN-FLANC)&cols. Head Pediatric Neurosurgery Unit I Instituto de NeurocirugiaAsenjo Santiago CHILE RATE OF MENINGEAL,BRAIN AND OTHER CNS MALIGNANT
SURGICAL MANAGEMENT OF BRAIN TUMORS
 SURGICAL MANAGEMENT OF BRAIN TUMORS LIGIA TATARANU, MD, Ph D NEUROSURGICAL CLINIC, BAGDASAR ARSENI CLINICAL HOSPITAL BUCHAREST, ROMANIA SURGICAL INDICATIONS CONFIRMING HISTOLOGIC DIAGNOSIS REDUCING TUMOR
SURGICAL MANAGEMENT OF BRAIN TUMORS LIGIA TATARANU, MD, Ph D NEUROSURGICAL CLINIC, BAGDASAR ARSENI CLINICAL HOSPITAL BUCHAREST, ROMANIA SURGICAL INDICATIONS CONFIRMING HISTOLOGIC DIAGNOSIS REDUCING TUMOR
PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES
 PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES CENTRAL NERVOUS SYSTEM MEDULLOBLASTOMA AND PNET CNS Site Group Medulloblastoma and PNET Author: Dr. Norm Laperriere 1. INTRODUCTION 3 2. PREVENTION
PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES CENTRAL NERVOUS SYSTEM MEDULLOBLASTOMA AND PNET CNS Site Group Medulloblastoma and PNET Author: Dr. Norm Laperriere 1. INTRODUCTION 3 2. PREVENTION
Key Words. Infants Brain tumors Chemotherapy Radiation therapy
 The Oncologist The Oncologist CME Program is located online at http://cme.theoncologist.com/. To take the CME activity related to this article, you must be a registered user. Pediatric Oncology Current
The Oncologist The Oncologist CME Program is located online at http://cme.theoncologist.com/. To take the CME activity related to this article, you must be a registered user. Pediatric Oncology Current
Treatment of Recurrent. Central Nervous System. Primitive Neuroectodermal Tumours (PNETs) in Children and Young People. Version 1.
 in Children and Young People. Version 1.") Treatment of Recurrent Central Nervous System Primitive Neuroectodermal Tumours (PNETs) in Children and Young People Version 1.0 September 2011 Barry Pizer on behalf of the CCLG CNS Interest Group Guidance
Treatment of Recurrent Central Nervous System Primitive Neuroectodermal Tumours (PNETs) in Children and Young People Version 1.0 September 2011 Barry Pizer on behalf of the CCLG CNS Interest Group Guidance
Protocol for management of patients with pineal region tumours v1
 Protocol for management of patients with pineal region tumours v1 West Midlands Cancer Alliance Coversheet for Cancer Alliance Expert Advisory Group Agreed Documentation This sheet is to accompany all
Protocol for management of patients with pineal region tumours v1 West Midlands Cancer Alliance Coversheet for Cancer Alliance Expert Advisory Group Agreed Documentation This sheet is to accompany all
PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES
 PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES CENTRAL NERVOUS SYSTEM LOW GRADE GLIOMAS CNS Site Group Low Grade Gliomas Author: Dr. Norm Laperriere 1. INTRODUCTION 3 2. PREVENTION 3 3. SCREENING
PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES CENTRAL NERVOUS SYSTEM LOW GRADE GLIOMAS CNS Site Group Low Grade Gliomas Author: Dr. Norm Laperriere 1. INTRODUCTION 3 2. PREVENTION 3 3. SCREENING
CNS pathology Third year medical students. Dr Heyam Awad 2018 Lecture 12: CNS tumours 2/3
 CNS pathology Third year medical students Dr Heyam Awad 2018 Lecture 12: CNS tumours 2/3 Pilocytic astrocytoma Relatively benign ( WHO grade 1) Occurs in children and young adults Mostly: in the cerebellum
CNS pathology Third year medical students Dr Heyam Awad 2018 Lecture 12: CNS tumours 2/3 Pilocytic astrocytoma Relatively benign ( WHO grade 1) Occurs in children and young adults Mostly: in the cerebellum
SCIENTIFIC PROGRAMME SNOLA UPDATE ON NEURO- ONCOLOGY th March
 SCIENTIFIC PROGRAMME SNOLA UPDATE ON NEURO- ONCOLOGY 2016 24th March 13h 13h45 pathology case case parasellar meningeoma case : posterior fossa pediatric tumor 13h45 16h Imaging for CNS lymphomas Parasellar
SCIENTIFIC PROGRAMME SNOLA UPDATE ON NEURO- ONCOLOGY 2016 24th March 13h 13h45 pathology case case parasellar meningeoma case : posterior fossa pediatric tumor 13h45 16h Imaging for CNS lymphomas Parasellar
Neuroblastoma. Elizabeth Roberts. Data Coordinator CIBMTR Data Managers Mentor. Tandem Meeting February 18
 Neuroblastoma Elizabeth Roberts Data Coordinator CIBMTR Data Managers Mentor Tandem Meeting February 18 Objectives Know what neuroblastoma is, how it is diagnosed, and how it is treated Complete form 2026:
Neuroblastoma Elizabeth Roberts Data Coordinator CIBMTR Data Managers Mentor Tandem Meeting February 18 Objectives Know what neuroblastoma is, how it is diagnosed, and how it is treated Complete form 2026:
Collection of Recorded Radiotherapy Seminars
 IAEA Human Health Campus Collection of Recorded Radiotherapy Seminars http://humanhealth.iaea.org The Role of Radiosurgery in the Treatment of Gliomas Luis Souhami, MD Professor Department of Radiation
IAEA Human Health Campus Collection of Recorded Radiotherapy Seminars http://humanhealth.iaea.org The Role of Radiosurgery in the Treatment of Gliomas Luis Souhami, MD Professor Department of Radiation
MALIGNANT GLIOMAS: TREATMENT AND CHALLENGES
 MALIGNANT GLIOMAS: TREATMENT AND CHALLENGES DISCLOSURE No conflicts of interest to disclose Patricia Bruns APRN, CNS Givens Brain Tumor Center Abbott Northwestern Hospital October 12, 2018 OBJECTIVES THEN
MALIGNANT GLIOMAS: TREATMENT AND CHALLENGES DISCLOSURE No conflicts of interest to disclose Patricia Bruns APRN, CNS Givens Brain Tumor Center Abbott Northwestern Hospital October 12, 2018 OBJECTIVES THEN
Shared Care & Survival CTYA SSCRG (Childhood Cancer Research Group)
") Shared Care & Survival CTYA SSCRG (Childhood Cancer Research Group) January 2013 The NCIN is a UK-wide initiative, working to drive improvements in standards of cancer care and clinical outcomes by improving
Shared Care & Survival CTYA SSCRG (Childhood Cancer Research Group) January 2013 The NCIN is a UK-wide initiative, working to drive improvements in standards of cancer care and clinical outcomes by improving
7/1/2015. Radiotherapy in Infant Brain Tumors. Goals and Objectives. Primary Brain and CNS Tumors (0-14 years) Brain Tumors (1 to 4 years)
 Brain Tumors (1 to 4 years)") Radiotherapy in Infant Brain Tumors ARNOLD C. PAULINO, M.D. PROFESSOR OF RADIATION ONCOLOGY MD ANDERSON CANCER CENTER AND TEXAS CHILDREN S HOSPITAL Radiotherapy in Infant Brain Tumors 1. Try to Avoid Irradiation
Radiotherapy in Infant Brain Tumors ARNOLD C. PAULINO, M.D. PROFESSOR OF RADIATION ONCOLOGY MD ANDERSON CANCER CENTER AND TEXAS CHILDREN S HOSPITAL Radiotherapy in Infant Brain Tumors 1. Try to Avoid Irradiation
CNS TUMORS. D r. Ali Eltayb ( U. of Omdurman. I ). M. Path (U. of Alexandria)
. M. Path (U. of Alexandria)") CNS TUMORS D r. Ali Eltayb ( U. of Omdurman. I ). M. Path (U. of Alexandria) CNS TUMORS The annual incidence of intracranial tumors of the CNS ISmore than intraspinal tumors May be Primary or Secondary
CNS TUMORS D r. Ali Eltayb ( U. of Omdurman. I ). M. Path (U. of Alexandria) CNS TUMORS The annual incidence of intracranial tumors of the CNS ISmore than intraspinal tumors May be Primary or Secondary
Clinical, radiological, and histopathological features and prognostic factors of brain tumors in children
 Journal of Physics: Conference Series PAPER OPEN ACCESS Clinical, radiological, and histopathological features and prognostic factors of brain tumors in children To cite this article: M H Siregar et al
Journal of Physics: Conference Series PAPER OPEN ACCESS Clinical, radiological, and histopathological features and prognostic factors of brain tumors in children To cite this article: M H Siregar et al
Brain Tumors in Children
 Brain Tumors in Children Michael A. Grotzer University Children s Hospital of Zurich, Switzerland Incidence of Childhood Cancer CNS Tumors Acute lymphoblastic Leukemia Neuroblastoma Non-Hodgkin Lymphoma
Brain Tumors in Children Michael A. Grotzer University Children s Hospital of Zurich, Switzerland Incidence of Childhood Cancer CNS Tumors Acute lymphoblastic Leukemia Neuroblastoma Non-Hodgkin Lymphoma
Challenging Paediatric Brain Tumours. ASP Belfast March 2017 Dr Jane Pears Consultant Paediatric Oncologist, Dublin
 Challenging Paediatric Brain Tumours ASP Belfast March 2017 Dr Jane Pears Consultant Paediatric Oncologist, Dublin Overview (i) Paediatric malignancy (ii) Central nervous system tumours (iii) Diffuse Intrinsic
Challenging Paediatric Brain Tumours ASP Belfast March 2017 Dr Jane Pears Consultant Paediatric Oncologist, Dublin Overview (i) Paediatric malignancy (ii) Central nervous system tumours (iii) Diffuse Intrinsic
Supra- and infratentorial brain tumors from childhood to maternity
 Supra- and infratentorial brain tumors from childhood to maternity What to expect? I am going to show you the characteristic imaging findings of following tumors: Thierry A.G.M. Huisman, MD, FICIS, EQNR
Supra- and infratentorial brain tumors from childhood to maternity What to expect? I am going to show you the characteristic imaging findings of following tumors: Thierry A.G.M. Huisman, MD, FICIS, EQNR
Small and Big Operations: New Tools of the Trade for Brain Tumors. Disclosure. Incidence of Childhood Cancer
 Small and Big Operations: New Tools of the Trade for Brain Tumors Nalin Gupta MD PhD Chief, Division of Pediatric Neurosurgery Departments of Neurosurgery and Pediatrics University of California San Francisco
Small and Big Operations: New Tools of the Trade for Brain Tumors Nalin Gupta MD PhD Chief, Division of Pediatric Neurosurgery Departments of Neurosurgery and Pediatrics University of California San Francisco
PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES
 PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES CENTRAL NERVOUS SYSTEM EPENDYMOMA Last Revision Date July 2015 1 CNS Site Group Ependymoma Author: Dr. Norm Laperriere 1. INTRODUCTION 3 2.
PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES CENTRAL NERVOUS SYSTEM EPENDYMOMA Last Revision Date July 2015 1 CNS Site Group Ependymoma Author: Dr. Norm Laperriere 1. INTRODUCTION 3 2.
Pediatric CNS Tumors. Disclosures. Acknowledgements. Introduction. Introduction. Posterior Fossa Tumors. Whitney Finke, MD
 Pediatric CNS Tumors Disclosures Whitney Finke, MD Neuroradiology Fellow PGY-6 University of Utah Health Sciences Center Salt Lake City, Utah None Acknowledgements Introduction Nicholas A. Koontz, MD Luke
Pediatric CNS Tumors Disclosures Whitney Finke, MD Neuroradiology Fellow PGY-6 University of Utah Health Sciences Center Salt Lake City, Utah None Acknowledgements Introduction Nicholas A. Koontz, MD Luke
available at journal homepage:
 E U R O P E A N J O U R NA L O F CA N C E R46 (21) 12 133 available at www.sciencedirect.com journal homepage: www.ejconline.com Primary postoperative chemotherapy without radiotherapy for treatment of
E U R O P E A N J O U R NA L O F CA N C E R46 (21) 12 133 available at www.sciencedirect.com journal homepage: www.ejconline.com Primary postoperative chemotherapy without radiotherapy for treatment of
Off-Label Treatments. Clinical Trials for Recurrent GBM UCSF Radiation Oncology Course: Management of Recurrent Disease. Outline
 Off-Label Treatments Clinical Trials for Recurrent GBM UCSF Radiation Oncology Course: Management of Recurrent Disease Jennifer Clarke, MD, MPH Assistant Professor Division of Neuro-Oncology Depts of Neurological
Off-Label Treatments Clinical Trials for Recurrent GBM UCSF Radiation Oncology Course: Management of Recurrent Disease Jennifer Clarke, MD, MPH Assistant Professor Division of Neuro-Oncology Depts of Neurological
Optic Pathway Gliomas, Germinomas, Spinal Cord Tumours. Colin Kennedy March 2015
 Optic Pathway Gliomas, Germinomas, Spinal Cord Tumours Colin Kennedy March 2015 Glioma of the optic chiasm. T1-weighted MRI with gadolinium enhancement, showing intense irregular uptake of contrast. The
Optic Pathway Gliomas, Germinomas, Spinal Cord Tumours Colin Kennedy March 2015 Glioma of the optic chiasm. T1-weighted MRI with gadolinium enhancement, showing intense irregular uptake of contrast. The
WHY BIOPSY? Diagnosis and Research
 WHY BIOPSY? Diagnosis and Research 9 2 4 1 3 1 1. Diagnosis only by Imaging (like no other tumor) The issue of Typical versus Atypical DIPG T1 FLAIR Gad. T2 Tractography Functional MRI Diffusion/Perfusion
WHY BIOPSY? Diagnosis and Research 9 2 4 1 3 1 1. Diagnosis only by Imaging (like no other tumor) The issue of Typical versus Atypical DIPG T1 FLAIR Gad. T2 Tractography Functional MRI Diffusion/Perfusion
PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES
 PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES CENTRAL NERVOUS SYSTEM ANAPLASTIC GLIOMAS CNS Site Group Anaplastic Gliomas Author: Dr. Norm Laperriere Date: February 20, 2018 1. INTRODUCTION
PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES CENTRAL NERVOUS SYSTEM ANAPLASTIC GLIOMAS CNS Site Group Anaplastic Gliomas Author: Dr. Norm Laperriere Date: February 20, 2018 1. INTRODUCTION
Tumors of the Nervous System
 Tumors of the Nervous System Peter Canoll MD. PhD. What I want to cover What are the most common types of brain tumors? Who gets them? How do they present? What do they look like? How do they behave? 1
Tumors of the Nervous System Peter Canoll MD. PhD. What I want to cover What are the most common types of brain tumors? Who gets them? How do they present? What do they look like? How do they behave? 1
Case Report Atypical Presentation of Atypical Teratoid Rhabdoid Tumor in a Child
 Case Reports in Oncological Medicine Volume 2013, Article ID 815923, 4 pages http://dx.doi.org/10.1155/2013/815923 Case Report Atypical Presentation of Atypical Teratoid Rhabdoid Tumor in a Child Y. T.
Case Reports in Oncological Medicine Volume 2013, Article ID 815923, 4 pages http://dx.doi.org/10.1155/2013/815923 Case Report Atypical Presentation of Atypical Teratoid Rhabdoid Tumor in a Child Y. T.
A PROSPECTIVE RANDOMISED CONTROLLED TRIAL OF HYPERFRACTIONATED VERSUS CONVENTIONALLY FRACTIONATED RADIOTHERAPY IN STANDARD RISK MEDULLOBLASTOMA
 A PROSPECTIVE RANDOMISED CONTROLLED TRIAL OF HYPERFRACTIONATED VERSUS CONVENTIONALLY FRACTIONATED RADIOTHERAPY IN STANDARD RISK MEDULLOBLASTOMA HIT SIOP PNET 4 A SIOP and GPOH TRIAL START DATE 1 st September
A PROSPECTIVE RANDOMISED CONTROLLED TRIAL OF HYPERFRACTIONATED VERSUS CONVENTIONALLY FRACTIONATED RADIOTHERAPY IN STANDARD RISK MEDULLOBLASTOMA HIT SIOP PNET 4 A SIOP and GPOH TRIAL START DATE 1 st September
Case Report Tackling a Recurrent Pinealoblastoma
 Case Reports in Oncological Medicine, Article ID 135435, 4 pages http://dx.doi.org/10.1155/2014/135435 Case Report Tackling a Recurrent Pinealoblastoma Siddanna Palled, 1 Sruthi Kalavagunta, 1 Jaipal Beerappa
Case Reports in Oncological Medicine, Article ID 135435, 4 pages http://dx.doi.org/10.1155/2014/135435 Case Report Tackling a Recurrent Pinealoblastoma Siddanna Palled, 1 Sruthi Kalavagunta, 1 Jaipal Beerappa
New Imaging Concepts in Central Nervous System Neoplasms
 New Imaging Concepts in Central Nervous System Neoplasms Maarten Lequin Department of Pediatric Radiology Wilhelmina Children s Hospital/University Medical Center Utrecht New Imaging Concepts in Central
New Imaging Concepts in Central Nervous System Neoplasms Maarten Lequin Department of Pediatric Radiology Wilhelmina Children s Hospital/University Medical Center Utrecht New Imaging Concepts in Central
Case 7391 Intraventricular Lesion
 Case 7391 Intraventricular Lesion Bastos Lima P1, Marques C1, Cabrita F2, Barbosa M2, Rebelo O3, Rio F1. 1Neuroradiology, 2Neurosurgery, 3Neuropathology, Coimbra University Hospitals, Portugal. University
Case 7391 Intraventricular Lesion Bastos Lima P1, Marques C1, Cabrita F2, Barbosa M2, Rebelo O3, Rio F1. 1Neuroradiology, 2Neurosurgery, 3Neuropathology, Coimbra University Hospitals, Portugal. University
Management of pediatric brain tumors, strategies and long term outcome
 Management of pediatric brain tumors, strategies and long term outcome SAN The Sudanese association of neurosurgeons By Dr. Abubakr Darrag Salim Ahmed Dr. Mohammed Awad Elzain Khartoum Sudan Pediatric
Management of pediatric brain tumors, strategies and long term outcome SAN The Sudanese association of neurosurgeons By Dr. Abubakr Darrag Salim Ahmed Dr. Mohammed Awad Elzain Khartoum Sudan Pediatric
WHAT ARE PAEDIATRIC CANCERS
 WHAT ARE PAEDIATRIC CANCERS INTRODUCTION Childhood cancers are RARE 0.5% of all cancers in the West Overall risk that a child will develop cancer during first 15 years of life is 1 in 450 and 1 in 600
WHAT ARE PAEDIATRIC CANCERS INTRODUCTION Childhood cancers are RARE 0.5% of all cancers in the West Overall risk that a child will develop cancer during first 15 years of life is 1 in 450 and 1 in 600
Ependymoma Programme Synopsis
 Ependymoma Programme Synopsis TITLE SPONSOR PROTOCOL NUMBER EUDRACT NUMBER NATIONAL INVESTIGATOR- COORDINATOR SIOP Ependymoma program II: An International Clinical Program for the diagnosis and treatment
Ependymoma Programme Synopsis TITLE SPONSOR PROTOCOL NUMBER EUDRACT NUMBER NATIONAL INVESTIGATOR- COORDINATOR SIOP Ependymoma program II: An International Clinical Program for the diagnosis and treatment
Protocol Abstract and Schema
 Protocol Abstract and Schema A Phase I Trial of p28 (NSC745104), a Non-HDM2 mediated peptide inhibitor of p53 ubiquitination in pediatric patients with recurrent or progressive CNS tumors Description and
Protocol Abstract and Schema A Phase I Trial of p28 (NSC745104), a Non-HDM2 mediated peptide inhibitor of p53 ubiquitination in pediatric patients with recurrent or progressive CNS tumors Description and
Table 7: PBTC Protocols [ ] Protocol Title Strata Status Neuroimaging Objective/Test
![Table 7: PBTC Protocols [ ] Protocol Title Strata Status Neuroimaging Objective/Test](/thumbs/82/85455518.jpg "Table 7: PBTC Protocols [ ] Protocol Title Strata Status Neuroimaging Objective/Test") Table 7: PBTC Protocols [001 009] Protocol Title Strata Status Neuroimaging Objective/Test PBTC-001 PBTC-002 PBTC-003 PBTC-004 PBTC-005 PBTC-006 PBTC-007 PBTC-009 A Pilot of Systemic and Intrathecal Chemotherapy
Table 7: PBTC Protocols [001 009] Protocol Title Strata Status Neuroimaging Objective/Test PBTC-001 PBTC-002 PBTC-003 PBTC-004 PBTC-005 PBTC-006 PBTC-007 PBTC-009 A Pilot of Systemic and Intrathecal Chemotherapy
Adjuvant therapy for thyroid cancer
 Carcinoma of the thyroid Adjuvant therapy for thyroid cancer John Hay Department of Radiation Oncology Vancouver Cancer Centre Department of Surgery UBC 1% of all new malignancies 0.5% in men 1.5% in women
Carcinoma of the thyroid Adjuvant therapy for thyroid cancer John Hay Department of Radiation Oncology Vancouver Cancer Centre Department of Surgery UBC 1% of all new malignancies 0.5% in men 1.5% in women
Imaging for suspected glioma
 Imaging for suspected glioma 1.1.1 Offer standard structural MRI (defined as T2 weighted, FLAIR, DWI series and T1 pre- and post-contrast volume) as the initial diagnostic test for suspected glioma, unless
Imaging for suspected glioma 1.1.1 Offer standard structural MRI (defined as T2 weighted, FLAIR, DWI series and T1 pre- and post-contrast volume) as the initial diagnostic test for suspected glioma, unless
Oncological Management of Brain Tumours. Anna Maria Shiarli SpR in Clinical Oncology 15 th July 2013
 Oncological Management of Brain Tumours Anna Maria Shiarli SpR in Clinical Oncology 15 th July 2013 Outline General considerations of Primary Brain Tumours: epidemiology, pathology, presentation. Diagnosis
Oncological Management of Brain Tumours Anna Maria Shiarli SpR in Clinical Oncology 15 th July 2013 Outline General considerations of Primary Brain Tumours: epidemiology, pathology, presentation. Diagnosis
LOW GRADE ASTROCYTOMAS
 LOW GRADE ASTROCYTOMAS This article was provided to us by David Schiff, MD, Associate Professor of Neurology, Neurosurgery, and Medicine at University of Virginia, Charlottesville. We appreciate his generous
LOW GRADE ASTROCYTOMAS This article was provided to us by David Schiff, MD, Associate Professor of Neurology, Neurosurgery, and Medicine at University of Virginia, Charlottesville. We appreciate his generous
STUDY OFPAEDIATRIC CNS TUMORS IN TERTIARY CARE CENTER
 IJCRR Section: Healthcare Sci. Journal Impact Factor 4.016 Original Article STUDY OFPAEDIATRIC CNS TUMORS IN TERTIARY CARE CENTER Grishma P. Jobanputra Tutor, Department of Pathology, B.J. Medical College,
IJCRR Section: Healthcare Sci. Journal Impact Factor 4.016 Original Article STUDY OFPAEDIATRIC CNS TUMORS IN TERTIARY CARE CENTER Grishma P. Jobanputra Tutor, Department of Pathology, B.J. Medical College,
Chemotherapy for Childhood Medulloblastoma and Primitive Neuroectodermal Tumors
 Chemotherapy for Childhood and Primitive Neuroectodermal Tumors ROGER J. PACKER, a JONATHAN L. FINLAY b a Department of Neurology, Children s National Medical Center, Washington DC, USA; b Departments
Chemotherapy for Childhood and Primitive Neuroectodermal Tumors ROGER J. PACKER, a JONATHAN L. FINLAY b a Department of Neurology, Children s National Medical Center, Washington DC, USA; b Departments
Brain tumors: tumor types
 Brain tumors: tumor types Tumor types There are more than 120 types of brain tumors. Today, most medical institutions use the World Health Organization (WHO) classification system to identify brain tumors.
Brain tumors: tumor types Tumor types There are more than 120 types of brain tumors. Today, most medical institutions use the World Health Organization (WHO) classification system to identify brain tumors.
Adult Brain and Spinal Cord Tumors
 Adult Brain and Spinal Cord Tumors An adult central nervous system (CNS) tumor is a disease in which abnormal cells form in the tissues of the brain and or the spinal cord. Major Parts of the Brain Anatomy
Adult Brain and Spinal Cord Tumors An adult central nervous system (CNS) tumor is a disease in which abnormal cells form in the tissues of the brain and or the spinal cord. Major Parts of the Brain Anatomy
Building a Neuro-Oncology Program and Epidemiological Profiling of Pediatric Brain Tumors in a Tertiary Cancer Care Center in India
 Original Article Middle East Journal of Cancer; July 2018; 9(3): 228-234 Building a Neuro-Oncology Program and Epidemiological Profiling of Pediatric Brain Tumors in a Tertiary Cancer Care Center in India
Original Article Middle East Journal of Cancer; July 2018; 9(3): 228-234 Building a Neuro-Oncology Program and Epidemiological Profiling of Pediatric Brain Tumors in a Tertiary Cancer Care Center in India
Corporate Medical Policy
 Corporate Medical Policy Hematopoietic Stem-Cell Transplantation for CNS Embryonal Tumors File Name: Origination: Last CAP Review: Next CAP Review: Last Review: hematopoietic_stem-cell_transplantation_for_cns_embryonal_tumors
Corporate Medical Policy Hematopoietic Stem-Cell Transplantation for CNS Embryonal Tumors File Name: Origination: Last CAP Review: Next CAP Review: Last Review: hematopoietic_stem-cell_transplantation_for_cns_embryonal_tumors
Doppler ultrasound of the abdomen and pelvis, and color Doppler
 - - - - - - - - - - - - - Testicular tumors are rare in children. They account for only 1% of all pediatric solid tumors and 3% of all testicular tumors [1,2]. The annual incidence of testicular tumors
- - - - - - - - - - - - - Testicular tumors are rare in children. They account for only 1% of all pediatric solid tumors and 3% of all testicular tumors [1,2]. The annual incidence of testicular tumors
Brain cancer survival rate mayo clinic
 Brain cancer survival rate mayo clinic Ed' s Guide to Alternative Therapies. Contents: Acai Berries Acupuncture Artemisinin for cancer Beta-mannan to reverse dysplasia of the cervix Anti-Malignin antibody.
Brain cancer survival rate mayo clinic Ed' s Guide to Alternative Therapies. Contents: Acai Berries Acupuncture Artemisinin for cancer Beta-mannan to reverse dysplasia of the cervix Anti-Malignin antibody.
IAP XXVI International Congress Slide Seminar 07 (SS07)
") IAP XXVI International Congress Slide Seminar 07 (SS07) Pitfalls in Surgical Neuropathology Case 6 Richard A. Prayson, M.D. Cleveland Clinic Foundation Clinical History 64M S/P resection of pituitary adenoma
IAP XXVI International Congress Slide Seminar 07 (SS07) Pitfalls in Surgical Neuropathology Case 6 Richard A. Prayson, M.D. Cleveland Clinic Foundation Clinical History 64M S/P resection of pituitary adenoma
Brain Tumor Treatment
 Scan for mobile link. Brain Tumor Treatment Brain Tumors Overview A brain tumor is a group of abnormal cells that grows in or around the brain. Tumors can directly destroy healthy brain cells. They can
Scan for mobile link. Brain Tumor Treatment Brain Tumors Overview A brain tumor is a group of abnormal cells that grows in or around the brain. Tumors can directly destroy healthy brain cells. They can
Protocol Abstract and Schema
 Protocol Abstract and Schema Phase II study of Bevacizumab plus Irinotecan (Camptosar ) in Children with Recurrent, Progressive, or Refractory Malignant Gliomas, Diffuse/Intrinsic Brain Stem Gliomas, Medulloblastomas,
Protocol Abstract and Schema Phase II study of Bevacizumab plus Irinotecan (Camptosar ) in Children with Recurrent, Progressive, or Refractory Malignant Gliomas, Diffuse/Intrinsic Brain Stem Gliomas, Medulloblastomas,
PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES
 PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES CENTRAL NERVOUS SYSTEM MENINGIOMA CNS Site Group Meningioma Author: Dr. Norm Laperriere Date: February 20, 2018 1. INTRODUCTION 3 2. PREVENTION
PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES CENTRAL NERVOUS SYSTEM MENINGIOMA CNS Site Group Meningioma Author: Dr. Norm Laperriere Date: February 20, 2018 1. INTRODUCTION 3 2. PREVENTION
Case 1. Maysa Al-Hussaini MD FRCPath
 Case 1 Maysa Al-Hussaini MD FRCPath MAYSA King AL-HUSSAINI Hussein Cancer MD Center MRCPATH KING HUSSEIN Amman CANCER Jordan CENTER Clinical history 4 year old boy History of frontal headache, sleepiness.
Case 1 Maysa Al-Hussaini MD FRCPath MAYSA King AL-HUSSAINI Hussein Cancer MD Center MRCPATH KING HUSSEIN Amman CANCER Jordan CENTER Clinical history 4 year old boy History of frontal headache, sleepiness.
Pathologic Characteristics and Treatment Outcome of Patients with Malignant Brain Tumors: A Single Institutional Experience from Iran
 Middle East Special Report Middle East Journal of Cancer; April 2014; 5(2): 91-96 Pathologic Characteristics and Treatment Outcome of Patients with Malignant Brain Tumors: A Single Institutional Experience
Middle East Special Report Middle East Journal of Cancer; April 2014; 5(2): 91-96 Pathologic Characteristics and Treatment Outcome of Patients with Malignant Brain Tumors: A Single Institutional Experience
Pediatrics -Proton Beam Therapy in Children -
 Pediatrics -Proton Beam Therapy in Children - Beate Timmermann, M.D. West German Proton Therapy Centre Essen Germany Preview Survival Toxicity Why protons? (theoretically) Experiences so far (clinically)
Pediatrics -Proton Beam Therapy in Children - Beate Timmermann, M.D. West German Proton Therapy Centre Essen Germany Preview Survival Toxicity Why protons? (theoretically) Experiences so far (clinically)
CURRENTLY ENROLLING ONCOLOGY TREATMENT STUDIES (as of 4/27/2017)
") CURRENTLY ENROLLING ONCOLOGY TREATMENT STUDIES (as of 4/27/2017) Leukemia AALL0932 closed after Induction Treatment of Patients with Newly Diagnosed Standard Risk B-Lymphoblastic Leukemia (B-ALL) or Localized
CURRENTLY ENROLLING ONCOLOGY TREATMENT STUDIES (as of 4/27/2017) Leukemia AALL0932 closed after Induction Treatment of Patients with Newly Diagnosed Standard Risk B-Lymphoblastic Leukemia (B-ALL) or Localized
UPDATES ON CHEMOTHERAPY FOR LOW GRADE GLIOMAS
 UPDATES ON CHEMOTHERAPY FOR LOW GRADE GLIOMAS Antonio M. Omuro Department of Neurology Memorial Sloan-Kettering Cancer Center II International Neuro-Oncology Congress Sao Paulo, 08/17/12 CHALLENGES IN
UPDATES ON CHEMOTHERAPY FOR LOW GRADE GLIOMAS Antonio M. Omuro Department of Neurology Memorial Sloan-Kettering Cancer Center II International Neuro-Oncology Congress Sao Paulo, 08/17/12 CHALLENGES IN
NON-SURGICAL STRATEGY FOR ADULT EPENDYMOMA
 NON-SURGICAL STRATEGY FOR ADULT EPENDYMOMA Roberta Rudà Department of Neuro-Oncology University and City of Health and Science Hospital of Turin, Italy EORTC EANO ESMO Conference 2015 Istanbul, March 27-28
NON-SURGICAL STRATEGY FOR ADULT EPENDYMOMA Roberta Rudà Department of Neuro-Oncology University and City of Health and Science Hospital of Turin, Italy EORTC EANO ESMO Conference 2015 Istanbul, March 27-28
Neuro-Oncology Resident Rotation
 Neuro-Oncology Resident Rotation Background. The past decade has witnessed significant strides in our ability to manage breast, lung, colon, and prostate cancer. These advances are a direct result of our
Neuro-Oncology Resident Rotation Background. The past decade has witnessed significant strides in our ability to manage breast, lung, colon, and prostate cancer. These advances are a direct result of our
Precision medicine for gliomas
 Precision medicine for YAZMIN ODIA, MD MS LEAD PHYSICIAN OF MEDICAL NEURO-ONCOLOGY DISCLOSURES Novocure: Advisory Board for Optune in No other financial conflicts of interest Glioma OVERVIEW INFILTRATIVE,
Precision medicine for YAZMIN ODIA, MD MS LEAD PHYSICIAN OF MEDICAL NEURO-ONCOLOGY DISCLOSURES Novocure: Advisory Board for Optune in No other financial conflicts of interest Glioma OVERVIEW INFILTRATIVE,
State of the Art Radiotherapy for Pediatric Tumors. Suzanne L. Wolden, MD Memorial Sloan-Kettering Cancer Center
 State of the Art Radiotherapy for Pediatric Tumors Suzanne L. Wolden, MD Memorial Sloan-Kettering Cancer Center Introduction Progress and success in pediatric oncology Examples of low-tech and high-tech
State of the Art Radiotherapy for Pediatric Tumors Suzanne L. Wolden, MD Memorial Sloan-Kettering Cancer Center Introduction Progress and success in pediatric oncology Examples of low-tech and high-tech
Understanding general brain tumor pathology, Part I: The basics. Craig Horbinski, M.D., Ph.D. Department of Pathology University of Kentucky
 Understanding general brain tumor pathology, Part I: The basics Craig Horbinski, M.D., Ph.D. Department of Pathology University of Kentucky plan of attack what IS a pathologist, anyway? what s so special
Understanding general brain tumor pathology, Part I: The basics Craig Horbinski, M.D., Ph.D. Department of Pathology University of Kentucky plan of attack what IS a pathologist, anyway? what s so special
Peter Canoll MD. PhD.
 Tumors of the Nervous System Peter Canoll MD. PhD. What I want to cover What are the most common types of brain tumors? Who gets them? How do they ypresent? What do they look like? How do they behave?
Tumors of the Nervous System Peter Canoll MD. PhD. What I want to cover What are the most common types of brain tumors? Who gets them? How do they ypresent? What do they look like? How do they behave?
Feasibility Trial of Optune for Children with Recurrent or Progressive Supratentorial High-Grade Glioma and Ependymoma
 Feasibility Trial of Optune for Children with Recurrent or Progressive Supratentorial High-Grade Glioma and Ependymoma ABSTRACT Recurrent or progressive pediatric CNS tumors generally have a poor prognosis
Feasibility Trial of Optune for Children with Recurrent or Progressive Supratentorial High-Grade Glioma and Ependymoma ABSTRACT Recurrent or progressive pediatric CNS tumors generally have a poor prognosis
UPDATE ON RADIOTHERAPY
 1 Miriam Kleiter UPDATE ON RADIOTHERAPY Department for Companion Animals and Horses, Plattform Radiooncology and Nuclear Medicine, University of Veterinary Medicine Vienna Introduction Radiotherapy has
1 Miriam Kleiter UPDATE ON RADIOTHERAPY Department for Companion Animals and Horses, Plattform Radiooncology and Nuclear Medicine, University of Veterinary Medicine Vienna Introduction Radiotherapy has
Histopathological Study and Categorisation of Brain Tumors
 Histopathological Study and Categorisation of Brain Tumors Ruchira Wadhwa 1*, Purvi Patel 2, Hansa Goswami 3 1 Third Year Resident, 2 Assistant Professor, 3 Professor and Head, Department of Pathology,
Histopathological Study and Categorisation of Brain Tumors Ruchira Wadhwa 1*, Purvi Patel 2, Hansa Goswami 3 1 Third Year Resident, 2 Assistant Professor, 3 Professor and Head, Department of Pathology,
Systemic Treatment. Third International Neuro-Oncology Course. 23 May 2014
 Low-Grade Astrocytoma of the CNS: Systemic Treatment Third International Neuro-Oncology Course São Paulo, Brazil 23 May 2014 John de Groot, MD Associate Professor, Neuro-Oncology UT MD Anderson Cancer
Low-Grade Astrocytoma of the CNS: Systemic Treatment Third International Neuro-Oncology Course São Paulo, Brazil 23 May 2014 John de Groot, MD Associate Professor, Neuro-Oncology UT MD Anderson Cancer
Brain tumors are, as a group, the most common
 See the corresponding editorial in this issue, pp 133 134. J Neurosurg Pediatrics 8:000 000, 8:135 148, 2011 Multidisciplinary management of childhood brain tumors: a review of outcomes, recent advances,
See the corresponding editorial in this issue, pp 133 134. J Neurosurg Pediatrics 8:000 000, 8:135 148, 2011 Multidisciplinary management of childhood brain tumors: a review of outcomes, recent advances,
Pathologic Analysis of CNS Surgical Specimens
 2015 Kenneth M. Earle Memorial Neuropathology Review Pathologic Analysis of CNS Surgical Specimens Peter C. Burger, MD Interdisciplinary Quality Control Familiarity with entities Use of diagnostic algorithm
2015 Kenneth M. Earle Memorial Neuropathology Review Pathologic Analysis of CNS Surgical Specimens Peter C. Burger, MD Interdisciplinary Quality Control Familiarity with entities Use of diagnostic algorithm
EVIDENCE BASED MANAGEMENT FOR Paediatric Brain tumours
 EVIDENCE BASED MANAGEMENT FOR Paediatric Brain tumours In children, tumours of the central nervous system comprise 20% of all tumours and are second most common after leukaemia. Unlike adults, almost half
EVIDENCE BASED MANAGEMENT FOR Paediatric Brain tumours In children, tumours of the central nervous system comprise 20% of all tumours and are second most common after leukaemia. Unlike adults, almost half
CT & MRI Evaluation of Brain Tumour & Tumour like Conditions
 CT & MRI Evaluation of Brain Tumour & Tumour like Conditions Dr. Anjana Trivedi 1, Dr. Jay Thakkar 2, Dr. Maulik Jethva 3, Dr. Ishita Virda 4 1 M.D. Radiology, Professor and Head, P.D.U. Medical College
CT & MRI Evaluation of Brain Tumour & Tumour like Conditions Dr. Anjana Trivedi 1, Dr. Jay Thakkar 2, Dr. Maulik Jethva 3, Dr. Ishita Virda 4 1 M.D. Radiology, Professor and Head, P.D.U. Medical College
Day Welcome. Tumours general I. Chairman:
 Day 1-7 th of December 0815 Welcome Tumours general I L1 0830 0850 Brain tumors/overview L2 0850 0910 Imaging of brain tumours L3 0910 0930 Cortical anatomy/imaging L4 0930 0950 Intraoperative monitoring
Day 1-7 th of December 0815 Welcome Tumours general I L1 0830 0850 Brain tumors/overview L2 0850 0910 Imaging of brain tumours L3 0910 0930 Cortical anatomy/imaging L4 0930 0950 Intraoperative monitoring
Radioterapia no Tratamento dos Gliomas de Baixo Grau
 Radioterapia no Tratamento dos Gliomas de Baixo Grau Dr. Luis Souhami University Montreal - Canada Low Grade Gliomas Relatively rare Heterogeneous, slow growing tumors WHO Classification Grade I Pilocytic
Radioterapia no Tratamento dos Gliomas de Baixo Grau Dr. Luis Souhami University Montreal - Canada Low Grade Gliomas Relatively rare Heterogeneous, slow growing tumors WHO Classification Grade I Pilocytic
Pediatr Blood Cancer 2014
 Low grade Glioma! 40% of pediatric brain tumors Pathologically, anatomically, clinically and biologically heterogeneous Leptomeningeal metastases in 5% Frequently protracted clinical course Long-Term Outcome
Low grade Glioma! 40% of pediatric brain tumors Pathologically, anatomically, clinically and biologically heterogeneous Leptomeningeal metastases in 5% Frequently protracted clinical course Long-Term Outcome
Childhood brain tumours
 Childhood brain tumours Our bodies are made up of billions of cells. Normally, these cells reproduce and repair themselves in a controlled way and do not cause us any problems. If for some reason this
Childhood brain tumours Our bodies are made up of billions of cells. Normally, these cells reproduce and repair themselves in a controlled way and do not cause us any problems. If for some reason this
Dr.Dafalla Ahmed Babiker Jazan University
 Dr.Dafalla Ahmed Babiker Jazan University Brain tumors are the second commonest malignancy in children Infratentorial tumors are more common As a general rule they do not metastasize out of the CNS, but
Dr.Dafalla Ahmed Babiker Jazan University Brain tumors are the second commonest malignancy in children Infratentorial tumors are more common As a general rule they do not metastasize out of the CNS, but
Neurosurgical Management of Brain Tumours. Nicholas Little Neurosurgeon RNSH
 Neurosurgical Management of Brain Tumours Nicholas Little Neurosurgeon RNSH General Most common tumours are metastatic 10x more common than primary Incidence of primary neoplasms is 20 per 100000 per year
Neurosurgical Management of Brain Tumours Nicholas Little Neurosurgeon RNSH General Most common tumours are metastatic 10x more common than primary Incidence of primary neoplasms is 20 per 100000 per year
Effective local and systemic therapy is necessary for the cure of Ewing tumor Most chemotherapy regimens are a combination of cyclophosphamide,
 Ewing Tumor Perez Ewing tumor is the second most common primary tumor of bone in childhood, and also occurs in soft tissues Ewing tumor is uncommon before 8 years of age and after 25 years of age In the
Ewing Tumor Perez Ewing tumor is the second most common primary tumor of bone in childhood, and also occurs in soft tissues Ewing tumor is uncommon before 8 years of age and after 25 years of age In the
Case Report Intracranial Capillary Hemangioma in the Posterior Fossa of an Adult Male
 Case Reports in Radiology Volume 2016, Article ID 6434623, 4 pages http://dx.doi.org/10.1155/2016/6434623 Case Report Intracranial Capillary Hemangioma in the Posterior Fossa of an Adult Male Jordan Nepute,
Case Reports in Radiology Volume 2016, Article ID 6434623, 4 pages http://dx.doi.org/10.1155/2016/6434623 Case Report Intracranial Capillary Hemangioma in the Posterior Fossa of an Adult Male Jordan Nepute,
Radiotherapy in feline and canine head and neck cancer
 Bettina Kandel Like surgery radiotherapy is usually a localized type of treatment. Today it is more readily available for the treatment of cancer in companion animals and many clients are well informed
Bettina Kandel Like surgery radiotherapy is usually a localized type of treatment. Today it is more readily available for the treatment of cancer in companion animals and many clients are well informed
Chapter 5 Section 3.1
 Radiology Chapter 5 Section 3.1 Issue Date: March 27, 1991 Authority: 32 CFR 199.4(b)(2), (b)(2)(x), (c)(2)(viii), and (g)(15) 1.0 CPT 1 PROCEDURE CODES 37243, 61793, 61795, 77261-77421, 77427-77799, 0073T
Radiology Chapter 5 Section 3.1 Issue Date: March 27, 1991 Authority: 32 CFR 199.4(b)(2), (b)(2)(x), (c)(2)(viii), and (g)(15) 1.0 CPT 1 PROCEDURE CODES 37243, 61793, 61795, 77261-77421, 77427-77799, 0073T
Role of radiotherapy in the treatment of lymphoma in Lena Specht MD DMSc Professor of Oncology Rigshospitalet, University of Copenhagen Denmark
 Role of radiotherapy in the treatment of lymphoma in 2017 Lena Specht MD DMSc Professor of Oncology Rigshospitalet, University of Copenhagen Denmark Disclosures Member of Advisory Board and Principal Investigator,
Role of radiotherapy in the treatment of lymphoma in 2017 Lena Specht MD DMSc Professor of Oncology Rigshospitalet, University of Copenhagen Denmark Disclosures Member of Advisory Board and Principal Investigator,
How to fight a silent killer: Lessons learned from Ovarian Cancer. Stephen A. Cannistra, M.D.
 How to fight a silent killer: Lessons learned from Ovarian Cancer Stephen A. Cannistra, M.D. How to fight a silent killer: Lessons learned from Ovarian Cancer Ovarian cancer is not common but is highly
How to fight a silent killer: Lessons learned from Ovarian Cancer Stephen A. Cannistra, M.D. How to fight a silent killer: Lessons learned from Ovarian Cancer Ovarian cancer is not common but is highly
Ependymomas: Prognostic Factors and Outcome Analysis in a Retrospective Series of 33 Patients
 ORIGINAL ARTICLE Brain Tumor Res Treat 2017;5(2):70-76 / pissn 2288-2405 / eissn 2288-2413 https://doi.org/10.14791/btrt.2017.5.2.70 Ependymomas: Prognostic Factors and Outcome Analysis in a Retrospective
ORIGINAL ARTICLE Brain Tumor Res Treat 2017;5(2):70-76 / pissn 2288-2405 / eissn 2288-2413 https://doi.org/10.14791/btrt.2017.5.2.70 Ependymomas: Prognostic Factors and Outcome Analysis in a Retrospective
Childhood Brain and Spinal Cord Tumors Treatment Overview (PDQ )
") 1 di 14 27/11/2016 17.42 NCBI Bookshelf. A service of the National Library of Medicine, National Institutes of Health. PDQ Cancer Information Summaries [Internet]. Bethesda (MD): National Cancer Institute
1 di 14 27/11/2016 17.42 NCBI Bookshelf. A service of the National Library of Medicine, National Institutes of Health. PDQ Cancer Information Summaries [Internet]. Bethesda (MD): National Cancer Institute
Protocol Abstract and Schema
 Protocol Abstract and Schema A Molecular Biology and Phase II Study of Imetelstat (GRN163L) in Children with Recurrent High-Grade Glioma, Ependymoma, Medulloblastoma/Primitive Neuroectodermal Tumor and
Protocol Abstract and Schema A Molecular Biology and Phase II Study of Imetelstat (GRN163L) in Children with Recurrent High-Grade Glioma, Ependymoma, Medulloblastoma/Primitive Neuroectodermal Tumor and
Theodore S. Johnson, MD, PhD
 Front-line Therapy of DIPG Using IDO Pathway Inhibitor Indoximod in Combination with Radiation and Chemotherapy American Association of Cancer Research (AACR) 2018 Theodore S. Johnson, MD, PhD Georgia
Front-line Therapy of DIPG Using IDO Pathway Inhibitor Indoximod in Combination with Radiation and Chemotherapy American Association of Cancer Research (AACR) 2018 Theodore S. Johnson, MD, PhD Georgia
THE ROLE OF TARGETED THERAPY AND IMMUNOTHERAPY IN THE TREATMENT OF ADVANCED CERVIX CANCER
 Gynecologic Cancer InterGroup Cervix Cancer Research Network THE ROLE OF TARGETED THERAPY AND IMMUNOTHERAPY IN THE TREATMENT OF ADVANCED CERVIX CANCER Linda Mileshkin, Medical Oncologist Peter MacCallum
Gynecologic Cancer InterGroup Cervix Cancer Research Network THE ROLE OF TARGETED THERAPY AND IMMUNOTHERAPY IN THE TREATMENT OF ADVANCED CERVIX CANCER Linda Mileshkin, Medical Oncologist Peter MacCallum
NK/T cell lymphoma Recent advances. Y.L Kwong University Department of Medicine Queen Mary Hospital
 NK/T cell lymphoma Recent advances Y.L Kwong University Department of Medicine Queen Mary Hospital Natural killer cell lymphomas NK cell lymphomas are mainly extranodal lymphomas Clinical classification
NK/T cell lymphoma Recent advances Y.L Kwong University Department of Medicine Queen Mary Hospital Natural killer cell lymphomas NK cell lymphomas are mainly extranodal lymphomas Clinical classification
PEDIATRIC ORBITAL TUMORS RADIOTHERAPY PLANNING
 PEDIATRIC ORBITAL TUMORS RADIOTHERAPY PLANNING ANATOMY ANATOMY CONT ANATOMY CONT. ANATOMY CONT. EYE OF A CHILD Normal tissue tolerance doses (in conventional #) TD 5/5 TD 50/5 Endpoint Gy Gy Optic nerve
PEDIATRIC ORBITAL TUMORS RADIOTHERAPY PLANNING ANATOMY ANATOMY CONT ANATOMY CONT. ANATOMY CONT. EYE OF A CHILD Normal tissue tolerance doses (in conventional #) TD 5/5 TD 50/5 Endpoint Gy Gy Optic nerve
Specialist Referral Service Willows Information Sheets. Cancer in cats and dogs: Assessment of the patient
 Specialist Referral Service Willows Information Sheets Cancer in cats and dogs: Assessment of the patient Cancer in cats and dogs: Assessment of the patient Cancer is common in human and veterinary medicine.
Specialist Referral Service Willows Information Sheets Cancer in cats and dogs: Assessment of the patient Cancer in cats and dogs: Assessment of the patient Cancer is common in human and veterinary medicine.