IORT State of the Art and Beyond
|
|
|
- Bethany Nichols
- 5 years ago
- Views:
Transcription




1 IORT State of the Art and Beyond Marco Krengli Dept. of Radiotherapy University of Piemonte Orientale A. Avogadro University Hospital Maggiore della Carità Novara, Italy
2 No conflicts of interest


3 IORT Definition IORT (Intra-Operative Radiation Therapy) is a Radiotherapy Technique allowing to deliver a relevant dose during the surgical procedure while sparing the surrounding healthy tissues Dose intensification Normal tissue protection Better tumor control Less side effects

4 IORT Historical Notes March : first IORT treatment (with orthovoltage) of cervical carcinoma in a 33 y/o woman operated by hysterectomy, pelvic node dissection, and partial cystectomy. The treatment was performed by Comas and Prio in Barcelona.





5 IORT Historical Notes (courtesy of F. Calvo)


6 IORT Technical Aspects






7 IORT Organizational Aspects Conventional Linac with patient s transportation Conventionl Linac in operating room Dedicated mobile Linac mobile operating room Targit Brachiterapia (peri-operatoria)

8 IORT Organizational Aspects Guidelines for Quality Assurance in IORT Istituto Superiore di Sanità, Rome - Structural aspects - Machines - Professionals - Organization of clinical activity WEBSITE: - Analysis of costs
9 IORT Biological Aspects Effect of Single High Dose (Fuks, Cancer Cell, 2005)
 Dose >10 Gy causes endothelial cell apoptosis (max effect 25 Gy) (Garcia-Barros")
10 IORT Biological Aspects Effect of Single High Dose Target = membrane of endothelial cells Dose >8 Gy kills cript stem cells (Potten 1990) Dose >10 Gy causes endothelial cell apoptosis (max effect 25 Gy) (Garcia-Barros 2003)
11 IORT - Biological Aspects Normal Tissue Tolerance (animal models) Vessels (aorta and vena cava) Peripheral nerves Surgical anastomosis

12 IORT - Clinical Indications Breast cancer Rectal cancer Gastric cancer Pancreatic cancer Biliary tract cancer Esophageal cancer Lung cancer Soft tissue sarcoma Head & Neck cancers Brain glioma Gynecological cancer Bladder cancer Renal cancer Prostate cancer Pediatric cancers
13 IORT - Clinical Indications IORT as a boost (dose escalation) IORT as a single treatment (dose de-escalation)
14 IORT - Clinical Indications Breast Cancer (Ruano-Ravina, Cancer Letters, 2011)
15 IORT - Clinical Indications Breast Cancer (Ruano-Ravina, Cancer Letters, 2011)


16 Vaidya S. et al. Intrabeam - low energy x-rays - 50 kv maximum IORT dose: 20 Gy in single fraction Inclusione criteria: Age 45, T2-T3 tumour, N0-N1 nodal status 28 centres in 9 countries (UK, USA, Germany, Italy, Poland, Switzerland, Denmark, Canada, Australia)

17 Vaidya S. et al. The local recurrence rate in the targeted intraoperative radiotherapy group was not significantly different from that in the external beam radiotherapy group (1.2% vs 0.95%, p=0.41 at 4 years). This large, international randomised trial provides robust and mature evidence that targeted intraoperative radiotherapy is safe.


18 IORT - Clinical Indications Rectal Cancer
19 Preop. EBRT: 40 Gy + IORT: 18 Gy Preop. EBRT: 40 Gy
radiotherapy, intended radical surgery, IORT and elective adjuvant chemotherapy (act).")
20 Pts: 605 with local advanced rectal cancer (LARC) who underwent multimodality treatment up to The basic treatment principle was preoperative (chemo)radiotherapy, intended radical surgery, IORT and elective adjuvant chemotherapy (act). Results: Chemoradiotherapy lead to more downstaging and complete remissions than radiotherapy alone (P < 0.001). It is difficult to study the quantitative effect of IORT, but 5-year LR rate of 12% is very low in this high-risk group of patients. Further, 55% of the patients with positive surgical margins did not develop LR, suggesting that these residual tumor cells were sterilized.
21 IORT - Recurrent Rectal Cancer Series Pts IORT EBRT *OS *Local year (Gy) (Gy) 5 yrs Control Haddock (42pts) % 60% 2001 (5-FU) Lindel % 47% 2001 (5-FU) Alektiar (HDR) +/ % 43% 2000 (5-FU) Mannaerts % (3ys) 73% (3 y) 2001 Valentini % 79% 1999 (5-FU) * microscopic positive margins
22 IORT - Clinical Indications Gastric Cancer Randomized Trials: Surgery vs S+IORT (28-35Gy) Takahashi M and Abe M, 86 Surg +RT (50 Gy) vs p= (Local Control) Surg +IORT (20 Gy) Sindelar WF et al Surgery vs p=ns (OS) p=0.04 in N+ Preop 20Gy+S+IORT(20Gy) Skoropad VY et al. 2000

23 IORT - Clinical Indications Gastric Cancer

24 IORT as a single modality or in combination with low dose of preoperative radiotherapyfailed to show a statistically significant benefit.studies without IORT showed a statistically significant improvement in survival at both 3 and 5 years of follow-up.



25 IORT - Pancreatic Cancer (Ruano-Ravina, Radiother Oncol, 2008)



26 IORT - Pancreatic Cancer (Ruano-Ravina, Radiother Oncol, 2008)
 or >2 years")

. The 5-year local control of 23.")
27 Local Control Overall Survival Overall survival stratified on the basis of the freedom from local recurrence <2 years (blue line) or >2 years (red line). From this joint analysis emerges the fact that preoperative radiotherapy increases the effects of IORT in terms of local control and overall survival (theory of filter-induction ). The 5-year local control of 23.3% confirms the beneficial sterilizing effect of IORT on the tumor bed.




28
29 IORT - Clinical Indications Biliary Tract Cancer CENTER TUMOR CHARACTERISTICS TREATMENT SURVIVAL Todoroki, Tsukuba University Japan, pts IVA Klatskin tumours 47 pts micr. res. tumour S+/-IORT+/- EBRT vs 33.9% 5y (39.6% 5y IORT+EBRT) 13.5% 5y Surgery alone Lindell, 20 pts S+IORT+EBRT 47% 5y Lund Hospital, Sweden, 2003 Locally advanced (10 IORT) vs Surgery alone 13% 5y
30 Author Tot. Pts IORT - Esophageal Cancer Site of IORT Surgery Toxicity of IORT Loco-regional rec. (%) Survival (%) 2 aa 3 aa 5 aa FEASIBILITY STUDIES WITH VARIOUS IORT DOSE Arimoto et al N MEDIAST. IORT: 25Gy o 20 Gy o 15 Gy o 18 Gy Tracheal ulcer in 6 pts with 25Gy none Hosokawa et al N MEDIAST. IORT :20-25 Gy o Gy o 12 Gy Tracheal ulcer with 25 Gy none Miller et al N ABDOMINAL IORT: 10-25Gy nv CT-RT + SURGERY AND IORT VS CT-RT EXCLUSIVE Murakami et al (T1-T2) N ABDOMINAL IORT : Gy none nv - 90% CT-RT+ S + IORT vs 80% CT-RT excl. - Murakami et al (T3-T4) N ABDOMINAL IORT : Gy none nv - 30% CT-RT+ S + IORT vs 48% CT-RT excl. - SURGERY+IORT VS SURGERY ALONE Murakami et al N ABDOMINAL IORT : Gy none N abdominal : 8% S + IORT vs 24% S alone 46% CT- RT+ S + IORT vs 56% CT-RT excl. - -


31 IORT - Esophageal Cancer mediastinum Limit: subclavian artery Field about 8 x 4 cm Lower to the tracheal biforcation Anteriorly to trachea and posteriorly to vertebrae
32 IORT - Esophageal Cancer
33 IORT Lung Cancer (NSCLC) Series Pts IORT EBRT OS Local year (Gy) (Gy) 5 yrs Control Martinez-M* % (4ys) 91% (4ys) 1994 Aristu % (IIIA) DDP-based CT Van Geel* % (2ys) 85% (2ys) Jaske % (3ys) 68% (3ys) 2007 * Superior sulcus tumor Phase II Study Preop CT-Surg/IORT-Postop RT
34 IORT Retroperitoneal STS Series Pts EBRT IORT OS Local year (Gy) (Gy) 5 yrs Control Sindelar % 60% % 40% Petersen % 59% 2002 Alektiar* (HDR) 45% 62% 2000 Gieschen** % 59% 2001 Azinovic % 53% 2001 Krempien % 40% 2006 Randomised study (P<0.001) *IORT-HDR; **Pre-op RT
35 IORT Extremity STS Series Pts year EBRT IORT OS Local (Gy) (Gy) 5 yrs Control Rochbauer (HDR) - 100%(2ys) 2003 Azinovic *75% 88% 2003 Kretzler % 84% 2004 Krempien % 78% 2006 *Primary tumors
36 IORT Head & Neck Cancer Advanced T-stage Nag 1997 (Ohio University) (40 pts) Larynx 32%, oral cavity 26%, oropharynx 8%, hypopharynx 8%, paranasal sinus 8% 20 pts IORT (6-9 MeV e-), Dose Gy 20 pts HDR-IORT, Dose Gy EBRT 50 Gy was added in 28 pts LC and OS 50% and 33% vs. 79% and 88% with EBRT No stat. difference between IORT by e- and by HDR Pinheiro 2002, Mayo Clinic (34 pts, 56% skull base, 44% neck) Dose IORT Gy, (6-15 MeV) SCC vs. non-scc : LC 46% vs. 52%; OS 32% vs. 50%, DFS 21% vs. 40% IORT safe with dose of 20 Gy or less (one neuropathy in pt treated with 22.5 Gy)
37 IORT Recurrent H&N Cancer after RT Chen (UCSF) 2007 (137 pts) Sites: oropharynx 24%, oral cavity 23%, 12% paranasal sinuses, 7% hypopharynx, 6% salivary glands, 6% skin, 3% nasopharynx, 3% larynx, 2% ear, 2% others IORT dose Gy (median 15 Gy), e- 6 MeV LC In-field IORT at 1,2,3 anni: 70, 64, 61% Positive margins are predictive for recurrence in IORT field (p=0.002) OS correlates with site of recurrence (44% T 19% N, p=0.001) Loco-regional control, DMFS and OS at 3 yrs: 51, 46, 36% No perioperatory mortality Complications in 7% (infections, fistolae, necrosis, trismus, neuropathy)



38

39 IORT Brain Glioma (recurrent) Author # IOERT dose Shibamoto 1994 Histology Median survival (months) Gy AA / GBM 12 Matsutani 1994 Willich 1997 Ortiz de Urbina 1999 Schueller Gy GBM Gy AA / GBM Gy AA / GBM Gy AA / GBM 12.5
40 IORT Gynecological Cancer CENTRE # pts TUMOUR CHARACTERISTICS TREATMENT LOCAL CONTROL SURVIVAL Mahe, 70 Recurrent cervix S+IORT 75% 3y 8% 3y French Intraop.Gr., 1995 (10-25 Gy) +/- EBRT+/-CT No sign. diff. with IORT No sign. diff. with IORT Martinez- Monge, Univ.Navarra Cervix: 31 primary 36 recurrent EBRT+CT (primary)+ S+IOERT (12-15 Gy) 69% 10y 93% prim. 46% rec. 15% tox. pain and neuropathy Liu, Xi an Jiaotong University (China), Cervix, stage IIB EBRT +S + IORT (18-20 Gy) RT only EBRT+BRT - 95% 5y (91% adenoca) 88% 5y (33% adenoca) Dowdy, Mayo Clinic, Recurrent endometrial S+IORT (10-25 Gy) +EBRT(84%) - 47% 5y Tran, Stanford, CA Recurrent S+IORT ( Gy) +EBRT(53%) 44% 5y 47% 5y (DSS)
41 HDR-IORT Gynecological Cancer CENTRE # pts TUMOUR CHARACTERISTICS TREATMENT LOCAL CONTROL SURVIVAL Gemignani, MSKCC, Recurrent Cervix 53% Uterus 41% Vagina 6% S+HDR- IORT (mean 14Gy) 67% 3y (83% gross resection, 25% partial resection) 54% 3y (OS) Orr, Ft.Myers,FL Persistent/Recurrent S+HDR- IORT (mean 20Gy) 86% mos (mean OS)
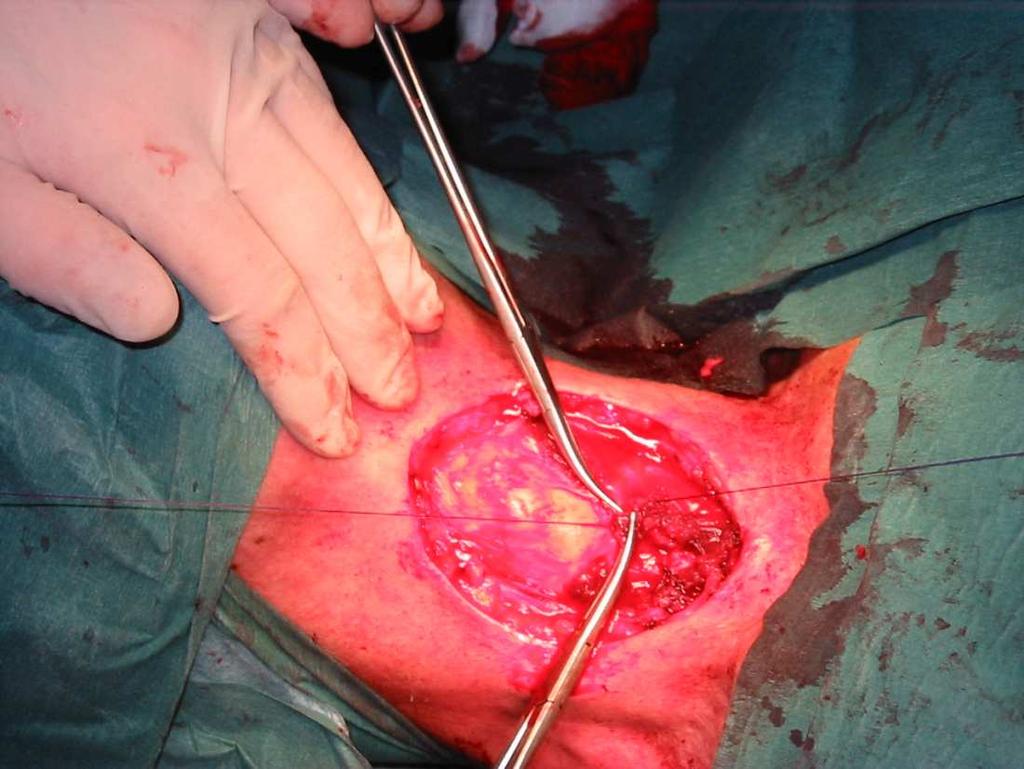
42 IORT Bladder Cancer Bladder-preservation protocol Radiotherapy + cystotomy and IOERT The bladder has been opened superiorly and the treatment cylinder is angled laterally to avoid irradiating the right ureteral orifice and the rectum. Electron beams of 15 to 18 MeV, that penetrate 4 to 5.5 cm are necessary to treat the extra-vesical extensions of these advanced tumors. The treatment cylinder is angled latero-inferiorly so that the anus, rectum, and prostate or lower vagina are not in the path of the exit beam. (Shipley WU, Cancer 1987)
43 IORT Bladder Cancer Brachytherapy or IOERT Author # Clinical stage Treatment 5 year Local Control 5 year Survival van der Werf-Messing et al 328 T2 EBRT, Ra % 56% Batterman et al 85 T2 EBRT, Ra % 55% Mazeron et al 24 T2 Resection, Ir-192, EBRT 92% 58% Matsumoto et al 28 T2 IOERT, EBRT 82% 62% Nieuwenhuijzen et al 108 T1-T2 EBRT, Ir % 62% van Onna et al 111 T1-T2 EBRT, Ir % van der Steen-Banasik et al 76 T1-T2 EBRT, Cs-137, Ir % 57% Blank et al 122 T1-T2-T3 EBRT, Ir % 73% Rostom et al 27 T2-T3 IOERT, EBRT 81% 53% Preservation of bladder function in more than 75% of patients with solitary tumors that invade into but not beyond the bladder muscle
 and in Belgium (Soete 1997, Van Poppel 2000). (Courtesy of J.P. Gerard)")
44 IORT Bladder Cancer Intra/Peri-Operative Brachytherapy This technique was introduced and developed in the Netherlands by Brigit Van der Werf- Messing and has been employed mainly in France (Hoffstetter 1998, Mazeron 1988, Pernot 1996, Rozan 1992) and in Belgium (Soete 1997, Van Poppel 2000). (Courtesy of J.P. Gerard)

45 122 pts; pathologic stage distribution was: 30 pt1, 81 pt2, and 11 pt3 Tx: EBRT SURGERY BRT (99 LDR, 23 PDR) 5-yr local was 76% and distant relapse-free survival 83% 5 and 10-yr relapse-free survival were 69% and 66%, respectively 5 and 10-yr OS were 73% and 49%, respectively Toxicity was low. No differences were found between the LDR and PDR groups. In the Netherlands, a nationwide evaluation of bladder-saving techniques is underway.
46 IORT - Clinical Indications Renal Cancer Institution # pts Dx Tx Local control Survival Comment Santos 1989 Univ. Navarra 11 Stage III- IV S+IOERT (10-20 Gy)+EBRT 5/11 long survivors 3/11 long survivors No toxicity Eble 1998 Univ. Heidelberg 11 3 primary 8 recurrent S + IOERT(15-20 Gy) + EBRT 100% 4y No toxicity Master 2005 UCSF 14 Locally advanced S +/- IOERT - 5y No difference for IOERT Hallemaier 2012 Mayo Clinic 22 3 primary 19 recurrent S + IOERT (10-20 Gy) + EBRT 73% 5y 10y 23% grade III-V toxicity In patients with LR recurrent or LR advanced primary RCC, a multimodality approach of perioperative EBRT, maximal surgical resection, and IOERT yielded encouraging results. This regimen warrants further investigation (Hallemaier, 2012).
47 IORT - Clinical Indications Prostate Cancer High risk, locally advanced Conventional approaches (S/EBRT/HT): 37-62% Relapse-Free 5 yrs 40% Local Failure after radical prostatectomy
48 IORT - Clinical Indications Prostate Cancer Low α/β value for prostate cancer Analysis of 5,969 pts: α/β = 1.4 (95% CI = ) Gy (Miralbell, IJROBP, 2011) High sensitivity to dose/fraction (rationale for single dose and hypofractionated protocols) The administration of high doses per fraction may represent a potential advantage for local control for prostate cancer.
49 IORT - Prostate Cancer Author # Patients selection Takahashi Stage B2-D2 Surgical approach IORT Energy / Dose EBRT Perineal No RP MeV / Gy (single dose) Gy combined with EBRT 50 Gy to pelvic lymph nodes Abe Stage B2-D2 Perineal No RP 8-14 MeV / Gy (single dose) or Gy combined with EBRT 50 Gy to pelvic lymph nodes Higashi Stage B-C Perineal/retropubic No RP Gy 30 Gy, 2 Gy/fx Kato Stage B2-D1 Perineal/retropubic No RP Gy 30 Gy, 2 Gy/fx Orecchia Interm.- high risk Retropubic IORT-RP 8-10 MeV / 12 Gy 45 Gy, 1.8 Gy/fx Saracino Interm. risk Retropubic RP-IORT 7-9 MeV / Gy (dose escalation) no Rocco Interm.- high risk Retropubic IORT-RP 8-10 MeV / 12 Gy 45 Gy, 1.8 Gy/fx Krengli Interm.- high risk Retropubic IORT-RP 9-12 MeV / Gy Gy, 2 Gy/fx
50 IORT - Prostate Cancer High risk, locally advanced No prostatectomy - Japanese series: (Takahashi, 1985) - Kyoto University (first report by Abe in 1975) - Saitama Cancer Center
 (courtesy of")
 - EIO, Milan;")
51 IORT - Prostate Cancer Intermediate and High risk, locally advanced - Italian series : (Saracino, 2008) (courtesy of R. Orecchia) - Inst. Regina Elena, Rome (after prostate removal) - EIO, Milan; UH of Novara (before prostate removal)
52 Author Local control and F/U Takahashi % (4-140 mos) Abe yrs IORT - Prostate Cancer Survival Higashi % (stage B), 87% (stage C) 5 years Toxicity - Delayed wound healing of perineal incision No severe IORT related 72% 5 years 100% early hematuria 10% early pollakiuria 1 chronic cystitis, 1 late urethral stricture No critical cystitis, proctitis, anal bleeding Kato yrs 89% DSS, 74% 5 yrs 20% early rectal G3-G4 (without rectal spacer) 7% early rectal G3 (with rectal spacer) Orecchia Peri-operative: 1 lymphocele, 3 anastomotic leakage Saracino % (19-59 mos) Rocco % 2 yrs, 100% OS (3-24 months) Krengli % (6-46 mos) 77% 3 years No urinary or rectal toxicity G1 82% BRFS, 100% OS (6-46 months) GU: 17% G 2 (early), 7% G 2 (late) GI: 10% G 2 (early), 0% G 2 (late) Peri-operative: lymphocele 16%, hematoma 6%; After EBRT: 11% G2 early rectal G2 11%, early urinary G2 4%; bladder neck stricture 7%
 0.04 ng/ml 9 44/70 (62.8%) 19/70 (27.1%) Inclusion Criteria (at least 2 of the following) PSA tot.")
53 CLINICAL SERIES From September 2005 to February 2011: 70 pts with prostate ca., high-risk Median ipsa (IQR, min-max), ng/ml Mean post-op. PSA Pathological GS (median) Positive surgical margins pn ( , ) 0.04 ng/ml 9 44/70 (62.8%) 19/70 (27.1%) Inclusion Criteria (at least 2 of the following) PSA tot. > 10 ng/ml Gleason Score 7 Stadio Clinico ct2c 24% Stadio Patologico pt2c 30% Clinical Stage ct2c > 2/3 positive biopsies Probability of organ confined disease < 25% (Kattan nomogram MSKCC) > ct2c 76% Basato su DRE, TRUS o TC > pt2c 70%




 - 12")



54 METHOD Prostate exposure ANTERIOR CAUDAL APEX Intra-op. US RECTUM Diameter of collimator: cm Energy of electrons: 9 (47%) - 12 (53%) MeV TARGET VOLUME: Prostate with 5-10 mm margin Mobetron, Intraop Dose (12 Gy, isodose 90%) as anticipated boost




55 Rectal Dosimetry Mean dose to the anterior rectal wall was 4.8 Gy (range: Gy) Rectal probe (diameter: 2.5 cm) Anterior Posterior 4 radio-chromic films positioned on the surface Laterals



56 Results after S + IORT + EBRT (pts with more that 12 mos F/U) G3 2% Tossicità GE Acuta G2 15% G1 15% Acute GI toxicity G0 68% G3 2% Tossicità GU acuta G2 17% G1 24% Acute GU toxicity G0 57% Late GI toxicity 1,0 G1 2% G2 2% G2 9% G4 G3 4% 9% Tossicità tardiva GU G3 4% Late GU toxicity Biochemical Recurrence Free Survival 0,8 0,6 0,4 0,2 0,0 5 yrs follow-up (months) 60 G0 85%

57 IORT Pediatric Cancer : 44 consecutive patients IORT after gross total resection of recurrent/persistent tumor. IORT after re-resection of locally recurrent/persistent neuroblastoma results in a reasonable rate of local control with acceptable morbidity and survival. This approach should be considered in this high-risk population.
58 Future Perspectives Treatment Planning Coordination of multicenter prospective clinical trials Biological Research in IORT



59 Future Perspectives Treatment Planning Multiplanar reconstruction in pancreatic cancer





60 Future Perspectives Treatment Planning Multiplanar reconstruction in solitary fibrous tumor



61 Future Perspectives Treatment Planning Multiplanar reconstruction and volume rendering Simulation Previsional dosimetry (courtesy of Radiance )




62 HOW IS IT DONE? FIX THE APPLICATOR IN THE OR TRANSPORT TO THE SCAN SCAN OF THE PATIENT INTRA IMAG
 Clinical Tumor Volume (CTV)")
 Surgical frame Patient orientation Cone diameter")


63 WORKFLOW SEGMENTATION SIMULATION DOSE COMPUTATION Gross Tumot Volume (GTV) Clinical Tumor Volume (CTV) Organs to protect Resected Volume (surgery) Tumor bed (PTV) Surgical frame Patient orientation Cone diameter and bevel Cone position and orientation Select enery which covers the target volume Use the DVH and 2D/3D images to confirm that the dose at the selected percentage covers the target area protecting the risky healthy areas

64 Future Perspectives Coordination of Clinical Trails by ISIORT? ISIORT EUROPE Registry Joint analysis of data from centers within the ISIORT- Europe program to investigate the role of intraoperative radiotherapy (IORT) by collecting information on tumour presentation and treatment modalities.

:")
65 ISIORT EUROPE Registry Available data ( ): 3,754 cases

:")
66 ISIORT EUROPE Registry Available data ( ): 3,754 cases



67 Future Perspectives Biological Research in IORT
68 Conclusion Available data show a favourable impact on local control and, in selected tumour sites, in OS when IORT is used as dose-intensification treatment The use of IORT as a single radiation treatment requires specific validation by prospective controlled clinical trials as in breast cancer Technological and biological advances may allow a development of IORT clinical activity in the frame of customized protocols based on biological knowledge of tumour cell characteristics

69 7 th International Conference June 22-24, 2012 Grand Hotel Dino, Baveno, Italy
ISIORT Conference September 25-27, 2014 Cologne/Germany Cologne Marriott Hotel
 8th International ISIORT Conference September 25-27, 2014 Cologne/Germany Cologne Marriott Hotel IORT for genitourinary malignancies Marco Krengli Dept. of Radiotherapy University of Piemonte Orientale
8th International ISIORT Conference September 25-27, 2014 Cologne/Germany Cologne Marriott Hotel IORT for genitourinary malignancies Marco Krengli Dept. of Radiotherapy University of Piemonte Orientale
Original Policy Date
 MP 8.01.06 Intraoperative Radiation Therapy Medical Policy Section Therapy Issue 12/2013 Original Policy Date 12/2013 Last Review Status/Date Reviewed with literature search/12/2013 Return to Medical Policy
MP 8.01.06 Intraoperative Radiation Therapy Medical Policy Section Therapy Issue 12/2013 Original Policy Date 12/2013 Last Review Status/Date Reviewed with literature search/12/2013 Return to Medical Policy
Intraoperative Radiotherapy
 Intraoperative Radiotherapy Policy Number: 8.01.08 Last Review: 10/2018 Origination: 10/1988 Next Review: 10/2019 Policy Blue Cross and Blue Shield of Kansas City (Blue KC) will provide coverage for radiation
Intraoperative Radiotherapy Policy Number: 8.01.08 Last Review: 10/2018 Origination: 10/1988 Next Review: 10/2019 Policy Blue Cross and Blue Shield of Kansas City (Blue KC) will provide coverage for radiation
INTRAOPERATIVE RADIATION THERAPY FOR RETROPERITONEAL SARCOMA
 INTRAOPERATIVE RADIATION THERAPY FOR RETROPERITONEAL SARCOMA ISIORT 2014 Ivy A Petersen, MD Mayo Clinic Rochester, MN NOTHING TO DISCLOSE SOFT TISSUE SARCOMAS 2014 Estimated cases in the USA 12,020 diagnosed
INTRAOPERATIVE RADIATION THERAPY FOR RETROPERITONEAL SARCOMA ISIORT 2014 Ivy A Petersen, MD Mayo Clinic Rochester, MN NOTHING TO DISCLOSE SOFT TISSUE SARCOMAS 2014 Estimated cases in the USA 12,020 diagnosed
Linac Based SBRT for Low-intermediate Risk Prostate Cancer in 5 Fractions: Preliminary Report of a Phase II Study with FFF Delivery
 Linac Based SBRT for Low-intermediate Risk Prostate Cancer in 5 Fractions: Preliminary Report of a Phase II Study with FFF Delivery FILIPPO ALONGI MD Radiation Oncology & Radiosurgery Istituto Clinico
Linac Based SBRT for Low-intermediate Risk Prostate Cancer in 5 Fractions: Preliminary Report of a Phase II Study with FFF Delivery FILIPPO ALONGI MD Radiation Oncology & Radiosurgery Istituto Clinico
Radiation Therapy for Soft Tissue Sarcomas
 Radiation Therapy for Soft Tissue Sarcomas Alexander R. Gottschalk, MD, PhD Assistant Professor, Radiation Oncology University of California, San Francisco 1/25/08 NCI: limb salvage vs. amputation 43 patients
Radiation Therapy for Soft Tissue Sarcomas Alexander R. Gottschalk, MD, PhD Assistant Professor, Radiation Oncology University of California, San Francisco 1/25/08 NCI: limb salvage vs. amputation 43 patients
Pediatric electron intraoperative radiotherapy: results and innovations
 Pediatric electron intraoperative radiotherapy: results and innovations Felipe A. Calvo ESTRO Hospital General Universitario Gregorio Marañon Madrid, Spain 2017 IOeRT in pediatric cancer: results and innovations
Pediatric electron intraoperative radiotherapy: results and innovations Felipe A. Calvo ESTRO Hospital General Universitario Gregorio Marañon Madrid, Spain 2017 IOeRT in pediatric cancer: results and innovations
This policy does not address the use of IORT for breast cancer, for that indication, see related policy
 Subject: Intraoperative Radiotherapy Page: 1 of 16 Last Review Status/Date: December 2015 Intraoperative Radiotherapy Description Intraoperative radiation therapy is delivered directly to exposed tissues
Subject: Intraoperative Radiotherapy Page: 1 of 16 Last Review Status/Date: December 2015 Intraoperative Radiotherapy Description Intraoperative radiation therapy is delivered directly to exposed tissues
2/14/09. Why Discuss this topic? Managing Local Recurrences after Radiation Failure. PROSTATE CANCER Second Treatment
 Why Discuss this topic? Mack Roach III, MD Professor and Chair Radiation Oncology UCSF Managing Local Recurrences after Radiation Failure 1. ~15 to 75% of CaP pts recur after definitive RT. 2. Heterogeneous
Why Discuss this topic? Mack Roach III, MD Professor and Chair Radiation Oncology UCSF Managing Local Recurrences after Radiation Failure 1. ~15 to 75% of CaP pts recur after definitive RT. 2. Heterogeneous
External Beam Radiotherapy for Prostate Cancer
 External Beam Radiotherapy for Prostate Cancer Chomporn Sitathanee, Radiation Oncology Unit Ramathibodi Hospital, Mahidol University Roles of RT in prostate cancer Definitive RT; intact prostate Post radical
External Beam Radiotherapy for Prostate Cancer Chomporn Sitathanee, Radiation Oncology Unit Ramathibodi Hospital, Mahidol University Roles of RT in prostate cancer Definitive RT; intact prostate Post radical
Salvage HDR Brachytherapy. Amit Bahl Consultant Clinical Oncologist The Bristol Cancer Institute, UK
 Salvage HDR Brachytherapy Amit Bahl Consultant Clinical Oncologist The Bristol Cancer Institute, UK Disclosures Still No financial disclosures! Limited personal experience of HDR Brachy as salvage option
Salvage HDR Brachytherapy Amit Bahl Consultant Clinical Oncologist The Bristol Cancer Institute, UK Disclosures Still No financial disclosures! Limited personal experience of HDR Brachy as salvage option
Overview of Radiotherapy for Clinically Localized Prostate Cancer
 Session 16A Invited lectures: Prostate - H&N. Overview of Radiotherapy for Clinically Localized Prostate Cancer Mack Roach III, MD Department of Radiation Oncology UCSF Helen Diller Family Comprehensive
Session 16A Invited lectures: Prostate - H&N. Overview of Radiotherapy for Clinically Localized Prostate Cancer Mack Roach III, MD Department of Radiation Oncology UCSF Helen Diller Family Comprehensive
Effective on or after May 1, 2015, refer to: Blue Cross and Blue Shield of Alabama Radiation Therapy Management RTM Policies
 Effective on or after May 1, 2015, refer to: Blue Cross and Blue Shield of Alabama Radiation Therapy Management RTM Policies Name of Policy: Intraoperative Radiation Therapy (IORT) Policy #: 220 Latest
Effective on or after May 1, 2015, refer to: Blue Cross and Blue Shield of Alabama Radiation Therapy Management RTM Policies Name of Policy: Intraoperative Radiation Therapy (IORT) Policy #: 220 Latest
Collection of Recorded Radiotherapy Seminars
 IAEA Human Health Campus Collection of Recorded Radiotherapy Seminars http://humanhealth.iaea.org Conservative Treatment of Invasive Bladder Cancer Luis Souhami, MD Professor Department of Radiation Oncology
IAEA Human Health Campus Collection of Recorded Radiotherapy Seminars http://humanhealth.iaea.org Conservative Treatment of Invasive Bladder Cancer Luis Souhami, MD Professor Department of Radiation Oncology
Radiation Therapy for Prostate Cancer. Resident Dept of Urology General Surgery Grand Round November 24, 2008
 Radiation Therapy for Prostate Cancer Amy Hou,, MD Resident Dept of Urology General Surgery Grand Round November 24, 2008 External Beam Radiation Advances Improving Therapy Generation of linear accelerators
Radiation Therapy for Prostate Cancer Amy Hou,, MD Resident Dept of Urology General Surgery Grand Round November 24, 2008 External Beam Radiation Advances Improving Therapy Generation of linear accelerators
Nordic Society for Gynecological Oncology Advisory Board of Radiotherapy
 Nordic Society for Gynecological Oncology Advisory Board of Radiotherapy Guidelines for postoperative irradiation of cervical cancer Contents: 1. Treatment planning for EBRT. 2 2. Target definition for
Nordic Society for Gynecological Oncology Advisory Board of Radiotherapy Guidelines for postoperative irradiation of cervical cancer Contents: 1. Treatment planning for EBRT. 2 2. Target definition for
Modern Dose Fractionation and Treatment Techniques for Definitive Prostate RT
 Modern Dose Fractionation and Treatment Techniques for Definitive Prostate RT Daniel J Bourgeois, III MD, MPH Board Certified Radiation Oncologist Southeast Louisiana Radiation Oncology Group (SLROG) Disclosures
Modern Dose Fractionation and Treatment Techniques for Definitive Prostate RT Daniel J Bourgeois, III MD, MPH Board Certified Radiation Oncologist Southeast Louisiana Radiation Oncology Group (SLROG) Disclosures
INTRAOPERATIVE ELECTRON-BEAM THERAPY FOR PRIMARY AND RECURRENT RETROPERITONEAL SOFT-TISSUE SARCOMA
 doi:10.1016/j.ijrobp.2006.01.028 Int. J. Radiation Oncology Biol. Phys., Vol. 65, No. 3, pp. 773 779, 2006 Copyright 2006 Elsevier Inc. Printed in the USA. All rights reserved 0360-3016/06/$ see front
doi:10.1016/j.ijrobp.2006.01.028 Int. J. Radiation Oncology Biol. Phys., Vol. 65, No. 3, pp. 773 779, 2006 Copyright 2006 Elsevier Inc. Printed in the USA. All rights reserved 0360-3016/06/$ see front
Prostate Cancer. 3DCRT vs IMRT : Hasan Murshed
 Prostate Cancer 3DCRT vs IMRT : the second debate Hasan Murshed Take home message IMRT allows dose escalation. Preliminary data shows IMRT technique improves cancer control while keeping acceptable morbidity
Prostate Cancer 3DCRT vs IMRT : the second debate Hasan Murshed Take home message IMRT allows dose escalation. Preliminary data shows IMRT technique improves cancer control while keeping acceptable morbidity
Protons for Head and Neck Cancer. William M Mendenhall, M.D.
 Protons for Head and Neck Cancer William M Mendenhall, M.D. Protons for Head and Neck Cancer Potential Advantages: Reduce late complications via more conformal dose distributions Likely to be the major
Protons for Head and Neck Cancer William M Mendenhall, M.D. Protons for Head and Neck Cancer Potential Advantages: Reduce late complications via more conformal dose distributions Likely to be the major
Curie - davinci connection
 Organ sparing treatment in MIBC: Robot assisted laparoscopy & Interstitial Radiotherapy brachytherapy Curie - davinci connection Geert Smits MD PhD FEBU Rijnstate Hospital, Arnhem, NL 010 Geert Smits Intuitive:
Organ sparing treatment in MIBC: Robot assisted laparoscopy & Interstitial Radiotherapy brachytherapy Curie - davinci connection Geert Smits MD PhD FEBU Rijnstate Hospital, Arnhem, NL 010 Geert Smits Intuitive:
IORT: clinical indications
 IORT: clinical indications M. Krengli, L. Masini, D. Beldì Introduction The concept of using ionizing radiation to treat the tumour bed or the tumour itself during a surgical procedure was envisaged for
IORT: clinical indications M. Krengli, L. Masini, D. Beldì Introduction The concept of using ionizing radiation to treat the tumour bed or the tumour itself during a surgical procedure was envisaged for
BENEFIT APPLICATION BLUECARD/NATIONAL ACCOUNT ISSUES
 Medical Policy MP 8.01.08 BCBSA Ref. Policy: 8.01.08 Last Review: 07/25/2018 Effective Date: 07/25/2018 Section: Therapy Related Policies 8.01.13 Accelerated Breast Irradiation After Breast- Conserving
Medical Policy MP 8.01.08 BCBSA Ref. Policy: 8.01.08 Last Review: 07/25/2018 Effective Date: 07/25/2018 Section: Therapy Related Policies 8.01.13 Accelerated Breast Irradiation After Breast- Conserving
IORT im multimodalen. Salzburg, Austria
 Stellenwert der IORT im multimodalen Behandlungskonzept Felix Sedlmayer Salzburg, Austria Definition IORT refers e to the delivery e of irradiation at at surgery. A large single dose of irradiation is
Stellenwert der IORT im multimodalen Behandlungskonzept Felix Sedlmayer Salzburg, Austria Definition IORT refers e to the delivery e of irradiation at at surgery. A large single dose of irradiation is
Intraoperative Radiation Therapy for
 Frontiers ofradiation Therapy and Oncology Reprint Editors: J.M. Vaeth, J.L. Meyer, San Francisco, Calif. ~' Publishers: S.Karger, Basel Printed in Switzerland Vaeth JM, Meyer JL (eds): The Role of High
Frontiers ofradiation Therapy and Oncology Reprint Editors: J.M. Vaeth, J.L. Meyer, San Francisco, Calif. ~' Publishers: S.Karger, Basel Printed in Switzerland Vaeth JM, Meyer JL (eds): The Role of High
DEPARTMENT OF ONCOLOGY ELECTIVE
 DEPARTMENT OF ONCOLOGY ELECTIVE 2015-2016 www.uwo.ca/oncology Oncology Elective Program Administrator: Ms. Kimberly Trudgeon Room A4-901C (Admin) LHSC London Regional Cancer Centre (Victoria Campus) Phone:
DEPARTMENT OF ONCOLOGY ELECTIVE 2015-2016 www.uwo.ca/oncology Oncology Elective Program Administrator: Ms. Kimberly Trudgeon Room A4-901C (Admin) LHSC London Regional Cancer Centre (Victoria Campus) Phone:
LA TOMOTERAPIA IN ITALIA: ESPERIENZE A CONFRONTO
 LA TOMOTERAPIA IN ITALIA: ESPERIENZE A CONFRONTO BARD 20 NOVEMBRE 2010 DI MUZIO NADIA H. S. RAFFAELE MILANO PHASE I-II STUDY OF HYPOFRACTIONATED SIMULTANEOUS INTEGRATED BOOST WITH TOMOTHERAPY FOR PROSTATE
LA TOMOTERAPIA IN ITALIA: ESPERIENZE A CONFRONTO BARD 20 NOVEMBRE 2010 DI MUZIO NADIA H. S. RAFFAELE MILANO PHASE I-II STUDY OF HYPOFRACTIONATED SIMULTANEOUS INTEGRATED BOOST WITH TOMOTHERAPY FOR PROSTATE
BRACHYTHERAPY FOR PROSTATE CANCER. Dr Brandon Nguyen MBBS(Hons), FRANZCR Radiation Oncologist, The Canberra Hospital
, FRANZCR Radiation Oncologist, The Canberra Hospital") BRACHYTHERAPY FOR PROSTATE CANCER Dr Brandon Nguyen MBBS(Hons), FRANZCR Radiation Oncologist, The Canberra Hospital PROSTATE BRACHYTHERAPY Why brachytherapy? How do we do it? What are the results? Questions?
BRACHYTHERAPY FOR PROSTATE CANCER Dr Brandon Nguyen MBBS(Hons), FRANZCR Radiation Oncologist, The Canberra Hospital PROSTATE BRACHYTHERAPY Why brachytherapy? How do we do it? What are the results? Questions?
LDR Monotherapy vs. HDR Monotherapy
 Abstract No. 1234 LDR Monotherapy vs. HDR Monotherapy Is it time for LDR to retire? Gerard Morton 2 LDR Seed Brachytherapy First 2000 LDR patients from BCCA Low and Intermediate Risk LDR Implant Morris
Abstract No. 1234 LDR Monotherapy vs. HDR Monotherapy Is it time for LDR to retire? Gerard Morton 2 LDR Seed Brachytherapy First 2000 LDR patients from BCCA Low and Intermediate Risk LDR Implant Morris
Interstitial Brachytherapy. Low dose rate brachytherapy. Brachytherapy alone cures some cervical cancer. Learning Objectives
 Interstitial Learning Objectives To discuss practical aspects of selection and insertion techniques for interstitial brachytherapy and their relation to clinical trials Akila Viswanathan, MD MPH Johns
Interstitial Learning Objectives To discuss practical aspects of selection and insertion techniques for interstitial brachytherapy and their relation to clinical trials Akila Viswanathan, MD MPH Johns
Locally advanced disease & challenges in management
 Gynecologic Cancer InterGroup Cervix Cancer Research Network Cervix Cancer Education Symposium, February 2018 Locally advanced disease & challenges in management Carien Creutzberg Radiation Oncology, Leiden
Gynecologic Cancer InterGroup Cervix Cancer Research Network Cervix Cancer Education Symposium, February 2018 Locally advanced disease & challenges in management Carien Creutzberg Radiation Oncology, Leiden
Surgery for Breast Cancer
 Surgery for Breast Cancer 1750 Mastectomy - Petit 1894 Radical mastectomy Halsted Extended, Super radical mastectomy 1948 Modified radical mastectomy Patey 1950-60 WLE & RT Baclesse, Mustakallio 1981-85
Surgery for Breast Cancer 1750 Mastectomy - Petit 1894 Radical mastectomy Halsted Extended, Super radical mastectomy 1948 Modified radical mastectomy Patey 1950-60 WLE & RT Baclesse, Mustakallio 1981-85
What s New in Radiotherapy For STS of The Extremity? Kaled M. Alektiar, MD, FASTRO Dept of Rad Onc Memorial Sloan Kettering Cancer Center
 What s New in Radiotherapy For STS of The Extremity? Kaled M. Alektiar, MD, FASTRO Dept of Rad Onc Memorial Sloan Kettering Cancer Center Topics Predictive tools for risk assessment Reassessment of dose/volume
What s New in Radiotherapy For STS of The Extremity? Kaled M. Alektiar, MD, FASTRO Dept of Rad Onc Memorial Sloan Kettering Cancer Center Topics Predictive tools for risk assessment Reassessment of dose/volume
Trimodality Therapy for Muscle Invasive Bladder Cancer
 Trimodality Therapy for Muscle Invasive Bladder Cancer Brita Danielson, MD, FRCPC Radiation Oncologist, Cross Cancer Institute Assistant Professor, Department of Oncology University of Alberta Edmonton,
Trimodality Therapy for Muscle Invasive Bladder Cancer Brita Danielson, MD, FRCPC Radiation Oncologist, Cross Cancer Institute Assistant Professor, Department of Oncology University of Alberta Edmonton,
FEP Medical Policy Manual
 FEP Medical Policy Manual Effective Date: October 15, 2018 Related Policies: None Intraoperative Radiotherapy Description Intraoperative radiotherapy (IORT) is delivered directly to exposed tissues during
FEP Medical Policy Manual Effective Date: October 15, 2018 Related Policies: None Intraoperative Radiotherapy Description Intraoperative radiotherapy (IORT) is delivered directly to exposed tissues during
State of the Art Radiotherapy for Pediatric Tumors. Suzanne L. Wolden, MD Memorial Sloan-Kettering Cancer Center
 State of the Art Radiotherapy for Pediatric Tumors Suzanne L. Wolden, MD Memorial Sloan-Kettering Cancer Center Introduction Progress and success in pediatric oncology Examples of low-tech and high-tech
State of the Art Radiotherapy for Pediatric Tumors Suzanne L. Wolden, MD Memorial Sloan-Kettering Cancer Center Introduction Progress and success in pediatric oncology Examples of low-tech and high-tech
PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES GYNECOLOGIC CANCER CERVIX
 PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES GYNECOLOGIC CANCER CERVIX Site Group: Gynecology Cervix Author: Dr. Stephane Laframboise 1. INTRODUCTION 3 2. PREVENTION 3 3. SCREENING AND
PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES GYNECOLOGIC CANCER CERVIX Site Group: Gynecology Cervix Author: Dr. Stephane Laframboise 1. INTRODUCTION 3 2. PREVENTION 3 3. SCREENING AND
Definitions. Brachytherapy in treatment of cancer. Implantation Techniques and Methods of Dose Specifications. Importance of Brachytherapy in GYN
 Implantation Techniques and Methods of Dose Specifications Brachytherapy Course Lecture V Krishna Reddy, MD, PhD Assistant Professor, Radiation Oncology Brachytherapy in treatment of cancer GYN Cervical
Implantation Techniques and Methods of Dose Specifications Brachytherapy Course Lecture V Krishna Reddy, MD, PhD Assistant Professor, Radiation Oncology Brachytherapy in treatment of cancer GYN Cervical
Rola brachyterapii w leczeniu wznów nowotworów języka i dna jamy ustnej. The role of brachytherapy in recurrent. oral cavity
 Rola brachyterapii w leczeniu wznów nowotworów języka i dna jamy ustnej The role of brachytherapy in recurrent tumours of the tongue and fundus of the oral cavity Janusz Skowronek, MD, PhD, Ass. Prof.
Rola brachyterapii w leczeniu wznów nowotworów języka i dna jamy ustnej The role of brachytherapy in recurrent tumours of the tongue and fundus of the oral cavity Janusz Skowronek, MD, PhD, Ass. Prof.
RADIOTHERAPY IN THE MANAGEMENT OF CANCERS OF THE URINARY BLADDER
 RADIOTHERAPY IN THE MANAGEMENT OF CANCERS OF THE URINARY BLADDER INTRODUCTION Incidence: Mortality: 20/100000/year (Europe) 8-9/100000/year Worldwide fourth most common cancer in men Incidence: 31.1 mortality:
RADIOTHERAPY IN THE MANAGEMENT OF CANCERS OF THE URINARY BLADDER INTRODUCTION Incidence: Mortality: 20/100000/year (Europe) 8-9/100000/year Worldwide fourth most common cancer in men Incidence: 31.1 mortality:
UCL. Rectum Adenocarcinoma. Quality of conformal radiotherapy Impact for the surgeon P. Scalliet & K. Haustermans
 Rectum Adenocarcinoma Quality of conformal radiotherapy Impact for the surgeon P. Scalliet & K. Haustermans Fifth Belgian Surgical Week May 6th, 2004, Oostende SOR rectum adenocarcinoma Indication of radiotherapy
Rectum Adenocarcinoma Quality of conformal radiotherapy Impact for the surgeon P. Scalliet & K. Haustermans Fifth Belgian Surgical Week May 6th, 2004, Oostende SOR rectum adenocarcinoma Indication of radiotherapy
Dr. Tareq Salah Ahmed,MD,ESMO. Lecturer of clinical oncology, Assiut faculty of medicine ESMO accreditation certificate
 Dr. Tareq Salah Ahmed,MD,ESMO Lecturer of clinical oncology, Assiut faculty of medicine ESMO accreditation certificate 1 st Assiut Urology department conference,marsa Alam 3 rd February 2015 Bladder cancer
Dr. Tareq Salah Ahmed,MD,ESMO Lecturer of clinical oncology, Assiut faculty of medicine ESMO accreditation certificate 1 st Assiut Urology department conference,marsa Alam 3 rd February 2015 Bladder cancer
Radiotherapy for Rectal Cancer. Kevin Palumbo Adelaide Radiotherapy Centre
 Radiotherapy for Rectal Cancer Kevin Palumbo Adelaide Radiotherapy Centre Overview CRC are common (3 rd commonest cancer) rectal Ca approx 25-30% of all CRC. Presentation PR bleeding: beware attributing
Radiotherapy for Rectal Cancer Kevin Palumbo Adelaide Radiotherapy Centre Overview CRC are common (3 rd commonest cancer) rectal Ca approx 25-30% of all CRC. Presentation PR bleeding: beware attributing
Would SBRT Hypofractionated Approach Be as Good? Then Why Bother With Brachytherapy?
 Would SBRT Hypofractionated Approach Be as Good? Then Why Bother With Brachytherapy? Yasuo Yoshioka, MD Department of Radiation Oncology Osaka University Graduate School of Medicine Osaka, Japan Disclosure
Would SBRT Hypofractionated Approach Be as Good? Then Why Bother With Brachytherapy? Yasuo Yoshioka, MD Department of Radiation Oncology Osaka University Graduate School of Medicine Osaka, Japan Disclosure
Radiation Therapy: From Fallacy to Science
 27 th Annual Management of Colon and Rectal Diseases 2.23.2019 Radiation Therapy: From Fallacy to Science Hadi Zahra, MD, DABR Radiation Oncologist CHI Health Henry Lynch Cancer Center Assistant Clinical
27 th Annual Management of Colon and Rectal Diseases 2.23.2019 Radiation Therapy: From Fallacy to Science Hadi Zahra, MD, DABR Radiation Oncologist CHI Health Henry Lynch Cancer Center Assistant Clinical
PORTEC-4. Patient seqnr. Age at inclusion (years) Hospital:
 Hospital:") May 2016 Randomisation Checklist Form 1, page 1 of 2 Patient seqnr. Age at inclusion (years) Hospital: Eligible patients should be registered and randomised via the Internet at : https://prod.tenalea.net/fs4/dm/delogin.aspx?refererpath=dehome.aspx
May 2016 Randomisation Checklist Form 1, page 1 of 2 Patient seqnr. Age at inclusion (years) Hospital: Eligible patients should be registered and randomised via the Internet at : https://prod.tenalea.net/fs4/dm/delogin.aspx?refererpath=dehome.aspx
Gynecologic Cancer InterGroup Cervix Cancer Research Network. Management of Cervical Cancer in Resource Limited Settings.
 Management of Cervical Cancer in Resource Limited Settings Linus Chuang MD Conflict of Interests None Cervical cancer is the fourth most common malignancy in women worldwide 530,000 new cases per year
Management of Cervical Cancer in Resource Limited Settings Linus Chuang MD Conflict of Interests None Cervical cancer is the fourth most common malignancy in women worldwide 530,000 new cases per year
A Comparison of IMRT and VMAT Technique for the Treatment of Rectal Cancer
 A Comparison of IMRT and VMAT Technique for the Treatment of Rectal Cancer Tony Kin Ming Lam Radiation Planner Dr Patricia Lindsay, Radiation Physicist Dr John Kim, Radiation Oncologist Dr Kim Ann Ung,
A Comparison of IMRT and VMAT Technique for the Treatment of Rectal Cancer Tony Kin Ming Lam Radiation Planner Dr Patricia Lindsay, Radiation Physicist Dr John Kim, Radiation Oncologist Dr Kim Ann Ung,
CPT Codes: 77424, Last Review Date: July 2017 Guideline Number: NIA_CG_226 Last Revised Date: July 2017 Responsible Department:
 Magellan Healthcare Clinical guideline: INTRAOPERATIVE RADIATION THERAPY (IORT) Original Date: November 2013 Page 1 of 5 CPT Codes: 77424, 77425 Last Review Date: July 2017 Guideline Number: NIA_CG_226
Magellan Healthcare Clinical guideline: INTRAOPERATIVE RADIATION THERAPY (IORT) Original Date: November 2013 Page 1 of 5 CPT Codes: 77424, 77425 Last Review Date: July 2017 Guideline Number: NIA_CG_226
Index. Surg Oncol Clin N Am 14 (2005) Note: Page numbers of article titles are in boldface type.
 Note: Page numbers of article titles are in boldface type.") Surg Oncol Clin N Am 14 (2005) 433 439 Index Note: Page numbers of article titles are in boldface type. A Abdominosacral resection, of recurrent rectal cancer, 202 215 Ablative techniques, image-guided,
Surg Oncol Clin N Am 14 (2005) 433 439 Index Note: Page numbers of article titles are in boldface type. A Abdominosacral resection, of recurrent rectal cancer, 202 215 Ablative techniques, image-guided,
Radiation Oncology MOC Study Guide
 Radiation Oncology MOC Study Guide The following study guide is intended to give a general overview of the type of material that will be covered on the Radiation Oncology Maintenance of Certification (MOC)
Radiation Oncology MOC Study Guide The following study guide is intended to give a general overview of the type of material that will be covered on the Radiation Oncology Maintenance of Certification (MOC)
Bladder Sparing Treatment of Muscle Invasive Bladder Cancer
 Bladder Sparing Treatment of Muscle Invasive Bladder Cancer Pr Alexandre de la Taille CHU Mondor, Créteil INSERMU955Eq07 adelataille@hotmail.com High-Risk Invasive and Muscle-Invasive BCa Radical cystectomy
Bladder Sparing Treatment of Muscle Invasive Bladder Cancer Pr Alexandre de la Taille CHU Mondor, Créteil INSERMU955Eq07 adelataille@hotmail.com High-Risk Invasive and Muscle-Invasive BCa Radical cystectomy
New Technologies in Radiation Oncology. Catherine Park, MD, MPH Advocate Good Shepherd Hospital
 New Technologies in Radiation Oncology Catherine Park, MD, MPH Advocate Good Shepherd Hospital Breast Radiation Early Stage Breast Cancer Whole Breast Radiation Delivered to the whole breast Boost to the
New Technologies in Radiation Oncology Catherine Park, MD, MPH Advocate Good Shepherd Hospital Breast Radiation Early Stage Breast Cancer Whole Breast Radiation Delivered to the whole breast Boost to the
Questions may be submitted anytime during the presentation.
 Understanding Radiation Therapy and its Role in Treating Patients with Pancreatic Cancer Presented by Pancreatic Cancer Action Network www.pancan.org August 18, 2014 If you experience technical difficulty
Understanding Radiation Therapy and its Role in Treating Patients with Pancreatic Cancer Presented by Pancreatic Cancer Action Network www.pancan.org August 18, 2014 If you experience technical difficulty
Intraoperative. Radiotherapy
 Intraoperative Radiotherapy ROBERTO ORECCHIA UNIVERSITY of MILAN & EUROPEAN INSTITUTE of ONCOLOGY & CNAO FOUNDATION Breast Cancer Brescia, 30th September 2011 IORT, very selective technique to intensify
Intraoperative Radiotherapy ROBERTO ORECCHIA UNIVERSITY of MILAN & EUROPEAN INSTITUTE of ONCOLOGY & CNAO FOUNDATION Breast Cancer Brescia, 30th September 2011 IORT, very selective technique to intensify
RADIO- AND RADIOCHEMOTHERAPY OF HEAD AND NECK TUMORS. Zoltán Takácsi-Nagy PhD Department of Radiotherapy National Institute of Oncology, Budapest 1.
 RADIO- AND RADIOCHEMOTHERAPY OF HEAD AND NECK TUMORS Zoltán Takácsi-Nagy PhD Department of Radiotherapy National Institute of Oncology, Budapest 1. 550 000 NEW PATIENTS/YEAR WITH HEAD AND NECK CANCER ALL
RADIO- AND RADIOCHEMOTHERAPY OF HEAD AND NECK TUMORS Zoltán Takácsi-Nagy PhD Department of Radiotherapy National Institute of Oncology, Budapest 1. 550 000 NEW PATIENTS/YEAR WITH HEAD AND NECK CANCER ALL
Multidisciplinary management of retroperitoneal sarcomas
 Multidisciplinary management of retroperitoneal sarcomas Eric K. Nakakura, MD UCSF Department of Surgery UCSF Comprehensive Cancer Center San Francisco, CA 7 th Annual Clinical Cancer Update North Lake
Multidisciplinary management of retroperitoneal sarcomas Eric K. Nakakura, MD UCSF Department of Surgery UCSF Comprehensive Cancer Center San Francisco, CA 7 th Annual Clinical Cancer Update North Lake
Basic Concepts in Image Based Brachytherapy (GEC-ESTRO Target Concept & Contouring)
") Basic Concepts in Image Based Brachytherapy (GEC-ESTRO Target Concept & Contouring) Dr Umesh Mahantshetty, Professor, Radiation Oncology GYN & Urology Disease Management Group (DMG) Member Tata Memorial
Basic Concepts in Image Based Brachytherapy (GEC-ESTRO Target Concept & Contouring) Dr Umesh Mahantshetty, Professor, Radiation Oncology GYN & Urology Disease Management Group (DMG) Member Tata Memorial
INTRAOPERATIVE IRRADIATION: A PRIMER FOR THE COMMUNITY ONCOLOGY TEAM
 INTRAOPERATIVE IRRADIATION: A PRIMER FOR THE COMMUNITY ONCOLOGY TEAM Conflicts of Interest Yes, we did have a latte; don t own stock Acknowledgements Jonathan Ashman (Mayo Scottsdale) Rodney Ellis (Case
INTRAOPERATIVE IRRADIATION: A PRIMER FOR THE COMMUNITY ONCOLOGY TEAM Conflicts of Interest Yes, we did have a latte; don t own stock Acknowledgements Jonathan Ashman (Mayo Scottsdale) Rodney Ellis (Case
New Technologies for the Radiotherapy of Prostate Cancer
 Prostate Cancer Meyer JL (ed): IMRT, IGRT, SBRT Advances in the Treatment Planning and Delivery of Radiotherapy. Front Radiat Ther Oncol. Basel, Karger, 27, vol. 4, pp 315 337 New Technologies for the
Prostate Cancer Meyer JL (ed): IMRT, IGRT, SBRT Advances in the Treatment Planning and Delivery of Radiotherapy. Front Radiat Ther Oncol. Basel, Karger, 27, vol. 4, pp 315 337 New Technologies for the
Pavel ŠLAMPA, Jana RUZICKOVA, Barbora ONDROVA, Hana TICHA, Hana DOLEZELOVA
 Sole conformal perioperative interstitial brachytherapy of early stage breast carcinoma using high-dose rate afterloading: longer-term results and toxicity Received: 0.09.2007 Accepted: 7.02.2008 Subject:
Sole conformal perioperative interstitial brachytherapy of early stage breast carcinoma using high-dose rate afterloading: longer-term results and toxicity Received: 0.09.2007 Accepted: 7.02.2008 Subject:
Feasibility of 4D IMRT Delivery for Hypofractionated High Dose Partial Prostate Treatments
 Feasibility of 4D IMRT Delivery for Hypofractionated High Dose Partial Prostate Treatments R.A. Price Jr., Ph.D., J. Li, Ph.D., A. Pollack, M.D., Ph.D.*, L. Jin, Ph.D., E. Horwitz, M.D., M. Buyyounouski,
Feasibility of 4D IMRT Delivery for Hypofractionated High Dose Partial Prostate Treatments R.A. Price Jr., Ph.D., J. Li, Ph.D., A. Pollack, M.D., Ph.D.*, L. Jin, Ph.D., E. Horwitz, M.D., M. Buyyounouski,
DOES RADIOTHERAPY TECHNIQUE / DOSE / FRACTIONATION REALLY MATTER? YES
 DOES RADIOTHERAPY TECHNIQUE / DOSE / FRACTIONATION REALLY MATTER? YES Marco Krengli Radiotherapy, Department of Translational Medicine, University of Piemonte Orientale A. Avogadro THE STANDARD OF CARE
DOES RADIOTHERAPY TECHNIQUE / DOSE / FRACTIONATION REALLY MATTER? YES Marco Krengli Radiotherapy, Department of Translational Medicine, University of Piemonte Orientale A. Avogadro THE STANDARD OF CARE
Intraoperative radiotherapy in gynaecological and genito-urinary malignancies: focus on endometrial, cervical, renal, bladder and prostate cancers
 Krengli et al. Radiation Oncology (2017) 12:18 DOI 10.1186/s13014-016-0748-x REVIEW Intraoperative radiotherapy in gynaecological and genito-urinary malignancies: focus on endometrial, cervical, renal,
Krengli et al. Radiation Oncology (2017) 12:18 DOI 10.1186/s13014-016-0748-x REVIEW Intraoperative radiotherapy in gynaecological and genito-urinary malignancies: focus on endometrial, cervical, renal,
Hypofractionated RT in Cervix Cancer. Anuja Jhingran, MD
 Hypofractionated RT in Cervix Cancer Anuja Jhingran, MD Hypofractionated RT in Cervix Cancer: Clinicaltrials.gov 919 cervix trials 134 hypofractionated RT trials Prostate, breast, NSCLC, GBM 0 cervix trials
Hypofractionated RT in Cervix Cancer Anuja Jhingran, MD Hypofractionated RT in Cervix Cancer: Clinicaltrials.gov 919 cervix trials 134 hypofractionated RT trials Prostate, breast, NSCLC, GBM 0 cervix trials
PORT after RP. Adjuvant. Salvage
 PORT after RP Adjuvant Or Salvage RT after RP 40-50% PSA relapse after RP in HR Definition: PSA should be undetectable within 6 weeks of RP Initial PSA is measured 6-12 weeks after RP AUA defines biochemical
PORT after RP Adjuvant Or Salvage RT after RP 40-50% PSA relapse after RP in HR Definition: PSA should be undetectable within 6 weeks of RP Initial PSA is measured 6-12 weeks after RP AUA defines biochemical
Does RT favor RP in long term Quality of Life? Juanita Crook MD FRCPC Professor of Radiation Oncology University of British Columbia
 Does RT favor RP in long term Quality of Life? Juanita Crook MD FRCPC Professor of Radiation Oncology University of British Columbia Disclosures Advisory Board/honoraria: Varian Advisory Board: Breast
Does RT favor RP in long term Quality of Life? Juanita Crook MD FRCPC Professor of Radiation Oncology University of British Columbia Disclosures Advisory Board/honoraria: Varian Advisory Board: Breast
3/8/2014. Case Presentation. Primary Treatment of Anal Cancer. Anatomy. Overview. March 6, 2014
 Case Presentation Primary Treatment of Anal Cancer 65 year old female presents with perianal pain, lower GI bleeding, and anemia with Hb of 7. On exam 6 cm mass protruding through the anus with bulky R
Case Presentation Primary Treatment of Anal Cancer 65 year old female presents with perianal pain, lower GI bleeding, and anemia with Hb of 7. On exam 6 cm mass protruding through the anus with bulky R
CLINICAL TRIALS Open clinical uro-oncology trials in Canada George Rodrigues, MD, Eric Winquist, MD
 Open clinical uro-oncology trials in Canada George Rodrigues, MD, Eric Winquist, MD London Health Sciences Centre, London, Ontario, Canada bladder cancer AN OPEN-LABEL, MULTICENTER, RANDOMIZED PHASE II
Open clinical uro-oncology trials in Canada George Rodrigues, MD, Eric Winquist, MD London Health Sciences Centre, London, Ontario, Canada bladder cancer AN OPEN-LABEL, MULTICENTER, RANDOMIZED PHASE II
Proposed All Wales Vulval Cancer Guidelines. Dr Amanda Tristram
 Proposed All Wales Vulval Cancer Guidelines Dr Amanda Tristram Previous FIGO staging FIGO Stage Features TNM Ia Lesion confined to vulva with
Proposed All Wales Vulval Cancer Guidelines Dr Amanda Tristram Previous FIGO staging FIGO Stage Features TNM Ia Lesion confined to vulva with
Mini J.Elnaggar M.D. Radiation Oncology Ochsner Medical Center 9/23/2016. Background
 Mini J.Elnaggar M.D. Radiation Oncology Ochsner Medical Center 9/23/2016 Background Mostly adenocarcinoma (scc possible, but treated like anal cancer) 39, 220 cases annually Primary treatment: surgery
Mini J.Elnaggar M.D. Radiation Oncology Ochsner Medical Center 9/23/2016 Background Mostly adenocarcinoma (scc possible, but treated like anal cancer) 39, 220 cases annually Primary treatment: surgery
GYNECOLOGIC CANCER and RADIATION THERAPY. Jon Anders M.D. Radiation Oncology
 GYNECOLOGIC CANCER and RADIATION THERAPY Jon Anders M.D. Radiation Oncology Brachytherapy Comes from the Greek brakhus meaning short Brachytherapy is treatment at short distance Intracavitary vs interstitial
GYNECOLOGIC CANCER and RADIATION THERAPY Jon Anders M.D. Radiation Oncology Brachytherapy Comes from the Greek brakhus meaning short Brachytherapy is treatment at short distance Intracavitary vs interstitial
High Risk Localized Prostate Cancer Treatment Should Start with RT
 High Risk Localized Prostate Cancer Treatment Should Start with RT Jason A. Efstathiou, M.D., D.Phil. Assistant Professor of Radiation Oncology Massachusetts General Hospital Harvard Medical School 10
High Risk Localized Prostate Cancer Treatment Should Start with RT Jason A. Efstathiou, M.D., D.Phil. Assistant Professor of Radiation Oncology Massachusetts General Hospital Harvard Medical School 10
Pre- Versus Post-operative Radiotherapy
 Postoperative Radiation and Chemoradiation: Indications and Optimization of Practice Dislosures Clinical trial support from Genentech Inc. Sue S. Yom, MD, PhD Associate Professor UCSF Radiation Oncology
Postoperative Radiation and Chemoradiation: Indications and Optimization of Practice Dislosures Clinical trial support from Genentech Inc. Sue S. Yom, MD, PhD Associate Professor UCSF Radiation Oncology
HDR Brachytherapy: Results and Future Studies in Monotherapy
 HDR Brachytherapy: Results and Future Studies in Monotherapy Nikolaos Zamboglou and Nikolaos Tselis Strahlenklinik Klinikum Offenbach - Germany Prostate Brachytherapy UK & Ireland Conference 2013 Comparison
HDR Brachytherapy: Results and Future Studies in Monotherapy Nikolaos Zamboglou and Nikolaos Tselis Strahlenklinik Klinikum Offenbach - Germany Prostate Brachytherapy UK & Ireland Conference 2013 Comparison
Radiotherapy for rectal cancer. Karin Haustermans Department of Radiation Oncology
 Radiotherapy for rectal cancer Karin Haustermans Department of Radiation Oncology O U T L I N E RT with TME surgery? Neoadjuvant or adjuvant RT? 5 x 5 Gy or long-course CRT? RT with new drugs? Selection
Radiotherapy for rectal cancer Karin Haustermans Department of Radiation Oncology O U T L I N E RT with TME surgery? Neoadjuvant or adjuvant RT? 5 x 5 Gy or long-course CRT? RT with new drugs? Selection
Outline - MRI - CT - US. - Combinations of imaging modalities for treatment planning
 Imaging Outline - MRI - CT - US - Combinations of imaging modalities for treatment planning Imaging Part 1: MRI MRI for cervical cancer high soft tissue contrast multiplanar imaging MRI anatomy: the normal
Imaging Outline - MRI - CT - US - Combinations of imaging modalities for treatment planning Imaging Part 1: MRI MRI for cervical cancer high soft tissue contrast multiplanar imaging MRI anatomy: the normal
Radiotherapy Considerations in Extremity Sarcoma
 Radiotherapy Considerations in Extremity Sarcoma Peter Chung Department of Radiation Oncology Princess Margaret Hospital University of Toronto Role of RT in STS Local tumour eradication while allowing
Radiotherapy Considerations in Extremity Sarcoma Peter Chung Department of Radiation Oncology Princess Margaret Hospital University of Toronto Role of RT in STS Local tumour eradication while allowing
Gynecologic Vaginal Brachytherapy (Mostly Post-Op Endometrial)
") Gynecologic Vaginal Brachytherapy (Mostly Post-Op Endometrial) D. Jeffrey Demanes M.D. FACRO, FACR, FASTRO Director Brachytherapy UCLA David Geffen School of Medicine Brachytherapy 11 (2012) 58-67 1 Manual
Gynecologic Vaginal Brachytherapy (Mostly Post-Op Endometrial) D. Jeffrey Demanes M.D. FACRO, FACR, FASTRO Director Brachytherapy UCLA David Geffen School of Medicine Brachytherapy 11 (2012) 58-67 1 Manual
PROSTATE CANCER BRACHYTHERAPY. Kazi S. Manir MD,DNB,PDCR RMO cum Clinical Tutor Department of Radiotherapy R. G. Kar Medical College
 PROSTATE CANCER BRACHYTHERAPY Kazi S. Manir MD,DNB,PDCR RMO cum Clinical Tutor Department of Radiotherapy R. G. Kar Medical College Risk categorization Very Low Risk Low Risk Intermediate Risk High Risk
PROSTATE CANCER BRACHYTHERAPY Kazi S. Manir MD,DNB,PDCR RMO cum Clinical Tutor Department of Radiotherapy R. G. Kar Medical College Risk categorization Very Low Risk Low Risk Intermediate Risk High Risk
D. Jeffrey Demanes M.D. FACRO, FACR, FASTRO Director UCLA Brachytherapy combined HDR + EBRT 574 HDR monotherapy Total Patients
 Salvage Prostate Brachytherapy D. Jeffrey Demanes M.D. FACRO, FACR, FASTRO Director UCLA Brachytherapy 1996-2013 1515 combined HDR + EBRT 574 HDR monotherapy 36 Salvage 2125 Total Patients No Disclosure
Salvage Prostate Brachytherapy D. Jeffrey Demanes M.D. FACRO, FACR, FASTRO Director UCLA Brachytherapy 1996-2013 1515 combined HDR + EBRT 574 HDR monotherapy 36 Salvage 2125 Total Patients No Disclosure
Current Status and Future Medical Perspectives at MedAustron. U. Mock EBG MedAustron GmbH
 Current Status and Future Medical Perspectives at MedAustron U. Mock EBG MedAustron GmbH Cancer treatment facility Ion beam therapy with protons and carbon ions Research facility Medical physics Radiobiology
Current Status and Future Medical Perspectives at MedAustron U. Mock EBG MedAustron GmbH Cancer treatment facility Ion beam therapy with protons and carbon ions Research facility Medical physics Radiobiology
External Beam Radiation Therapy for Low/Intermediate Risk Prostate Cancer
 External Beam Therapy for Low/Intermediate Risk Prostate Cancer Jeff Michalski, M.D. The Carlos A. Perez Distinguished Professor of Department of and Siteman Cancer Center Learning Objectives Understand
External Beam Therapy for Low/Intermediate Risk Prostate Cancer Jeff Michalski, M.D. The Carlos A. Perez Distinguished Professor of Department of and Siteman Cancer Center Learning Objectives Understand
A schematic of the rectal probe in contact with the prostate is show in this diagram.
 Hello. My name is William Osai. I am a nurse practitioner in the GU Medical Oncology Department at The University of Texas MD Anderson Cancer Center in Houston. Today s presentation is Part 2 of the Overview
Hello. My name is William Osai. I am a nurse practitioner in the GU Medical Oncology Department at The University of Texas MD Anderson Cancer Center in Houston. Today s presentation is Part 2 of the Overview
Intensity Modulated Radiation Therapy (IMRT)
") Intensity Modulated Radiation Therapy (IMRT) Policy Number: Original Effective Date: MM.05.006 03/09/2004 Line(s) of Business: Current Effective Date: HMO; PPO; QUEST Integration 05/01/2017 Section: Radiology
Intensity Modulated Radiation Therapy (IMRT) Policy Number: Original Effective Date: MM.05.006 03/09/2004 Line(s) of Business: Current Effective Date: HMO; PPO; QUEST Integration 05/01/2017 Section: Radiology
New research in prostate brachytherapy
 New research in prostate brachytherapy Dr Ann Henry Associate Professor in Clinical Oncology University of Leeds and Leeds Cancer Centre PIVOTAL boost opening 2017 To evaluate - The benefits of pelvic
New research in prostate brachytherapy Dr Ann Henry Associate Professor in Clinical Oncology University of Leeds and Leeds Cancer Centre PIVOTAL boost opening 2017 To evaluate - The benefits of pelvic
Staging and Treatment Update for Gynecologic Malignancies
 Staging and Treatment Update for Gynecologic Malignancies Bunja Rungruang, MD Medical College of Georgia No disclosures 4 th most common new cases of cancer in women 5 th and 6 th leading cancer deaths
Staging and Treatment Update for Gynecologic Malignancies Bunja Rungruang, MD Medical College of Georgia No disclosures 4 th most common new cases of cancer in women 5 th and 6 th leading cancer deaths
Case Scenario 1. 7/13/12 Anterior floor of mouth biopsy: Infiltrating squamous cell carcinoma, not completely excised.
 Case Scenario 1 7/5/12 History A 51 year old white female presents with a sore area on the floor of her mouth. She claims the area has been sore for several months. She is a current smoker and user of
Case Scenario 1 7/5/12 History A 51 year old white female presents with a sore area on the floor of her mouth. She claims the area has been sore for several months. She is a current smoker and user of
HDR vs. LDR Is One Better Than The Other?
 HDR vs. LDR Is One Better Than The Other? Daniel Fernandez, MD, PhD 11/3/2017 New Frontiers in Urologic Oncology Learning Objectives Indications for prostate brachytherapy Identify pros/cons of HDR vs
HDR vs. LDR Is One Better Than The Other? Daniel Fernandez, MD, PhD 11/3/2017 New Frontiers in Urologic Oncology Learning Objectives Indications for prostate brachytherapy Identify pros/cons of HDR vs
Stereotactic radiotherapy
 Stereotactic radiotherapy Influence of patient positioning and fixation on treatment planning - clinical results Frank Zimmermann Institut für Radioonkologie Universitätsspital Basel Petersgraben 4 CH
Stereotactic radiotherapy Influence of patient positioning and fixation on treatment planning - clinical results Frank Zimmermann Institut für Radioonkologie Universitätsspital Basel Petersgraben 4 CH
CyberKnife SBRT for Prostate Cancer
 CyberKnife SBRT for Prostate Cancer Robert Meier, MD Swedish Radiosurgery Center Swedish Cancer Institute Seattle, WA 2017 ESTRO Meeting, Vienna Austria 5-year safety, efficacy & quality of life outcomes
CyberKnife SBRT for Prostate Cancer Robert Meier, MD Swedish Radiosurgery Center Swedish Cancer Institute Seattle, WA 2017 ESTRO Meeting, Vienna Austria 5-year safety, efficacy & quality of life outcomes
Collection of Recorded Radiotherapy Seminars
 IAEA Human Health Campus Collection of Recorded Radiotherapy Seminars http://humanhealth.iaea.org The Role of Radiosurgery in the Treatment of Gliomas Luis Souhami, MD Professor Department of Radiation
IAEA Human Health Campus Collection of Recorded Radiotherapy Seminars http://humanhealth.iaea.org The Role of Radiosurgery in the Treatment of Gliomas Luis Souhami, MD Professor Department of Radiation
The objective of this lecture is to integrate our knowledge of the differences between 2D and 3D planning and apply the same to various clinical
 The objective of this lecture is to integrate our knowledge of the differences between 2D and 3D planning and apply the same to various clinical sites. The final aim will be to be able to make out these
The objective of this lecture is to integrate our knowledge of the differences between 2D and 3D planning and apply the same to various clinical sites. The final aim will be to be able to make out these
The Paul Evans Memorial Lecture Functional radiotherapy targeting using focused dose escalation. Roberto Alonzi Mount Vernon Cancer Centre
 The Paul Evans Memorial Lecture Functional radiotherapy targeting using focused dose escalation Roberto Alonzi Mount Vernon Cancer Centre Overview Introduction and rationale for focused dose escalation
The Paul Evans Memorial Lecture Functional radiotherapy targeting using focused dose escalation Roberto Alonzi Mount Vernon Cancer Centre Overview Introduction and rationale for focused dose escalation
 https://patient.varian.com/sit es/default/files/videos/origin al/imrt.mp4 brachy- from Greek brakhys "short" Historically LDR has been used. Cs-137 at 0.4-0.8 Gy/h With optimally placed device, dose
https://patient.varian.com/sit es/default/files/videos/origin al/imrt.mp4 brachy- from Greek brakhys "short" Historically LDR has been used. Cs-137 at 0.4-0.8 Gy/h With optimally placed device, dose
HYPERTHERMIA in CERVIX and VAGINA CANCER. J. van der Zee
 HYPERTHERMIA in CERVIX and VAGINA CANCER J. van der Zee ESTRO 2006 Deep hyperthermia in Rotterdam HYPERTHERMIA in CERVIX and VAGINA CANCER ESTRO 2006 Hyperthermia and radiotherapy in primary advanced cervix
HYPERTHERMIA in CERVIX and VAGINA CANCER J. van der Zee ESTRO 2006 Deep hyperthermia in Rotterdam HYPERTHERMIA in CERVIX and VAGINA CANCER ESTRO 2006 Hyperthermia and radiotherapy in primary advanced cervix
In the United States, approximately 38,000 patients were
 ORIGINAL ARTICLE Multimodality Therapy Including Surgical Resection and Intraoperative Electron Radiotherapy for Recurrent or Advanced Primary Carcinoma of the Urinary Bladder or Ureter Christopher L.
ORIGINAL ARTICLE Multimodality Therapy Including Surgical Resection and Intraoperative Electron Radiotherapy for Recurrent or Advanced Primary Carcinoma of the Urinary Bladder or Ureter Christopher L.
Clinically Proven Metabolically-Guided TomoTherapy SM Treatments Advancing Cancer Care
 Clinically Proven Metabolically-Guided TomoTherapy SM Treatments Advancing Cancer Care Institution: San Raffaele Hospital Milan, Italy By Nadia Di Muzio, M.D., Radiotherapy Department (collaborators: Berardi
Clinically Proven Metabolically-Guided TomoTherapy SM Treatments Advancing Cancer Care Institution: San Raffaele Hospital Milan, Italy By Nadia Di Muzio, M.D., Radiotherapy Department (collaborators: Berardi
University of Washington, Radiation Oncology Physics Residency Program. Medical Physics Site Specific Clinical Rotation
 Physics Faculty Mentor: Start date: End Date: Duration: Medical Physics Site Specific Clinical Rotation Meet with mentor(s) every week on?? to review work including readings, journal entries, project development,
Physics Faculty Mentor: Start date: End Date: Duration: Medical Physics Site Specific Clinical Rotation Meet with mentor(s) every week on?? to review work including readings, journal entries, project development,
The role of chemoradiotherapy in GE junction and gastric cancer. Karin Haustermans
 The role of chemoradiotherapy in GE junction and gastric cancer Karin Haustermans Overview Postoperative chemoradiotherapy Preoperative chemoradiotherapy Palliative radiation Technical aspects Overview
The role of chemoradiotherapy in GE junction and gastric cancer Karin Haustermans Overview Postoperative chemoradiotherapy Preoperative chemoradiotherapy Palliative radiation Technical aspects Overview