Using Task Group 137 to Prescribe and Report Dose. Vrinda Narayana. Department of Radiation Oncology University of Michigan. The
|
|
|
- Corey Dixon
- 5 years ago
- Views:
Transcription

1 Using Task Group 137 to Prescribe and Report Dose Vrinda Narayana The Department of Radiation Oncology University of Michigan
2 TG137 AAPM Recommendations on Dose Prescription and Reporting Methods for Permanent Interstitial Brachytherapy for Prostate Cancer R. Nath W. S. Bice W. M. Butler Z. Chen A. Meigooni V. Narayana M. J. Rivard Y. Yu 2016 AAPM Spring 2
3 TG 137 Charge Review Prescription Reporting Radiobiological models Consensus Min requirements for prescription and reporting Pre implant Post implant Recommend Optimal requirements for prescription and reporting Pre implant Post implant 2016 AAPM Spring 3
4 Outline Permanent Prostate Implants Impact of dose reporting based upon Imaging modalities Timing of imaging study Treatment planning approaches Interoperative planning strategies Biophysical models BED EUD TCP 2016 AAPM Spring 4
5 History Dose Prescription Bladde r Prostate Rectum Nomogram based on a modified peripheral loading Zheng et al., Medical Dosimetry, 28, (2003) AAPM Spring 5
6 History Dose Reporting D 99 Dose to 99% of target mpd minimum Peripheral Dose Bladde r Prostate Rectum Volume % US PROSTATE DVH Isodose Surface Implant too deep Implant too shallow Best Fit 0.5 cm superior 1.0 cm superior 0.5 cm inferior 1.0 cm inferior Dose Gy 2016 AAPM Spring 6
7 Plan evaluation today V100 Vol that receives 100% of dose 90 % excellent implant D90 Dose to 90 % of the volume Prescribed dose 2016 AAPM Spring 7

8 Today D 90 Dose to 90% of target V Volume that receives Rx dose V 100 Rx D AAPM Spring 8
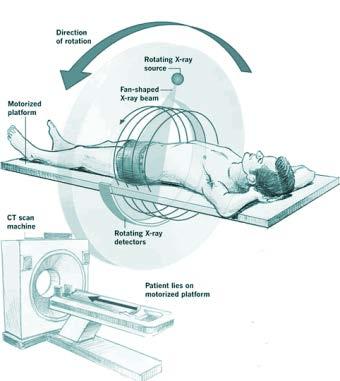
9 Dose calculation Imaging 2016 AAPM Spring 9
10 Today D 90 Dose to 90% of target V Volume that receives Rx dose V 100 Rx IDS V 100 D 90 Rx D AAPM Spring 10
11 D90 issue False Decrease D90 False Increase D90 CT Prostate MR prostate 2016 AAPM Spring 11
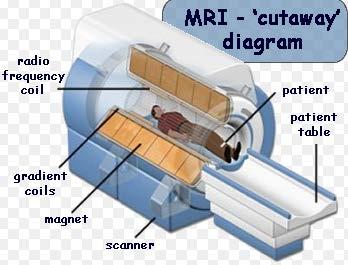
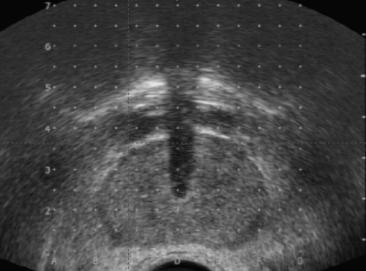
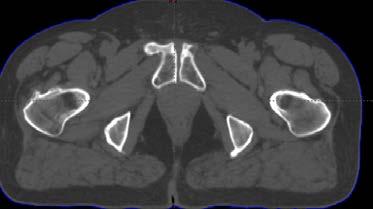
12 Impact of Imaging Modality on Dose Reporting Ultrasound Imaging CT Imaging MR Imaging Recommendations on Imaging modality 2016 AAPM Spring 12




13 Imaging modalities Target delineation www 2016 AAPM Spring 13

14 Prostate Anatomy 2016 AAPM Spring 14

15 2016 AAPM Spring 15
16 Imaging Modalities Plane CT MRI TRUS films * Identification * Localization Prostate Delineation Critical St Delineation Comfort Cost & Convenience AAPM Spring 16

17 Ultrasound Prostate Urethra Rectal wall 2016 AAPM Spring 17



18 Ultrasound Apex / GUD Transition Prostate Apex GUD external sphincter Bulbourethral Gland H shaped External sphincter 2016 AAPM Spring 18


19 MRI Coronal vs. CT Coronal 2016 AAPM Spring 19

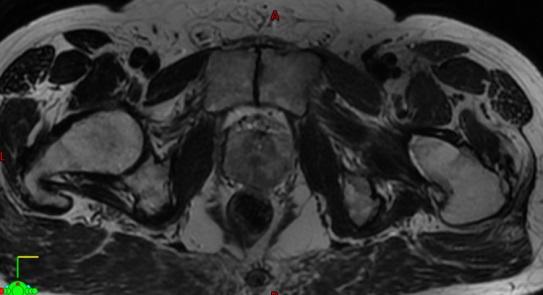
20 MR Anatomy Prostate Urethra Rectal wall Corpus Cavernosum Pudendal Arteries Sphincter Neurovascular bundle 2016 AAPM Spring 20
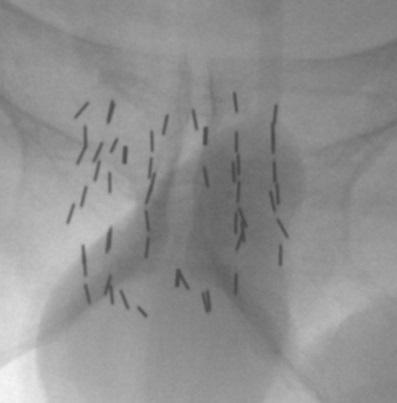
21 CT Prostate Apex when do you stop Base bladder neck oblitaration 2016 AAPM Spring 21


22 2016 AAPM Spring 22

23 Intra - lumen bladder density-small gland 2016 AAPM Spring 23

24 Figure AAPM Spring 24

25 Bladder Neck Obliteration 2016 AAPM Spring 25

26 MRI Coronal vs. CT Coronal 2016 AAPM Spring 26


27 MRI Coronal vs. CT Coronal 2016 AAPM Spring 27
28 CT Prostate post implant Apex when do you stop Base bladder neck obliteration Seminal vesicles Rectal surface 2016 AAPM Spring 28
29 Axial CT without Contour Axial MRI without Contour Axial CT with Contour Axial MRI with Contour 2016 AAPM Spring 29
30 Variations without a Standard (Lee) Observer 1 Observer 2 Observer 3 Vol 39 cc 48 cc 32 cc D Gy 123 Gy 155 Gy V100 93% 86% 99% 2016 AAPM Spring 30
31 Perils of CT contouring Bladder Anterior CT base Prostate Rectum CT apex Saggital McLaughlin et. al AAPM Spring 31

32 CT Prostate Outer Rectum Inner Rectum de-expansion 5 mm Urethra Foley Penile Bulb Urethra Prostate Rectum Axial 2016 AAPM Spring 32

33 Why MR? EXPECT VARIATION 2016 AAPM Spring 33


34 CT contouring / 6 national experts McLaughlin 2016 AAPM Spring et. 34 al.
35 CT contouring 3.00 Wide margin implants Observer/Std Volume Study Observer/Std V Observer/Std D Study Narayana et. al Study AAPM Spring
36 Deviation from a Standard (6 experts) MRI Observer 1 Observer 2 36cc 34cc 38cc Prostate Volume Agreement 2016 AAPM Spring 36
37 Deviation from a Standard (6 experts) MRI Observer 1 Observer Gy 153 Gy 143 Gy D90 Agreement 2016 AAPM Spring 37
38 Deviation from a Standard (6 experts) MRI Observer 1 Observer 2 95% 98% 92% V100 Agreement 2016 AAPM Spring 38


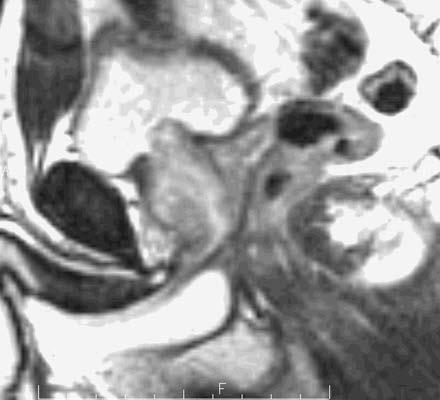
39 bladder seminal vesicle bone prostate rectum external sphincter Proximal penis Prostate side view: Note labels on right. Prostate is not enlarged and does not extend into the bladder. Urethra opening from the bladder is open (yellow arrow). Sphincter is normal length and there is no bony restriction note space between the bone and prostate (purple arrows) 2016 AAPM Spring 39

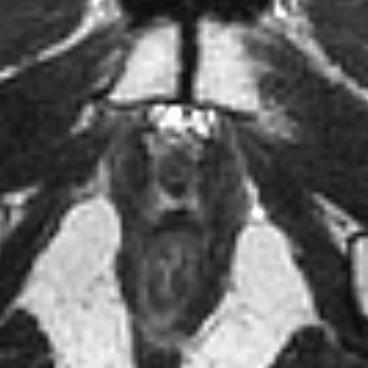
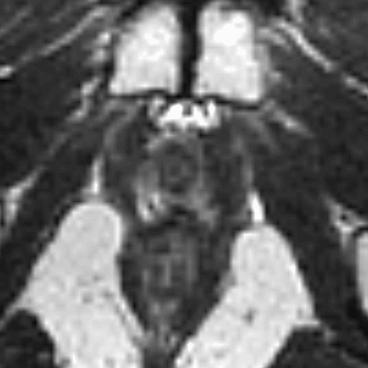
40 Central = transition zone (TZ) = dark Peripheral zone (PZ) = light normal prostate - normal appearance with light peripheral zone where tumors form and the dark central area called the transition zone this enlarges with age 2016 AAPM Spring 40
41 Multiparameter Imaging T2 DCE DWI 2016 AAPM Spring 41


42 Right side of the gland panel is normal prostate with clear PZ and TZ. On the left side (red) note the dark area that extends into the TZ and from front to back. This is tumor 2016 AAPM Spring 42
43 with contrast the area of concern on the left side of the panel is clearly seen, with a suggestion of extension beyond the gland (arrow) AAPM Spring 43
44 Note the tumor on the left side of the panel (red) and possible extension beyond the capsule 2016 AAPM Spring 44
45 Imaging Recommendations CT 2/3 mm cuts Prostate mindful of pitfalls Rectum outer 1 cm sup and inf Rectal wall cm contraction Urethra Foley Day 0 Foley Optional later scans Penial Bulb 2016 AAPM Spring 45
46 Imaging Guidelines MR T2 3 mm cuts (no rectal coil) immediately before or after CT Axial, coronal, sagittal Rectum 1 cm above & below Bladder axial MR Urethra axial and Sag MR Register CT-MR around prostate only CT seed positions 2016 AAPM Spring 46
47 Impact of timing of imaging on dose reporting Prostate edema Source displacement with time Optimal timing for post implant dosimetry Recommendations on timing of imaging 2016 AAPM Spring 47
48 Edema? Needle insertion? Bleeding needle pentration? General inflamation 2016 AAPM Spring 48
49 Edema Model Volume V max V T V 0 T 0 T max T Time 2016 AAPM Spring 49
50 Edema Model? T max? Different imaging modalities? Prostate Volumes 2016 AAPM Spring 50
51 Edema US 80% 1m CT1 14d CT2 150% CT3 120% Narayana et. al AAPM Spring 51


52 Edema CT 130% US 14 d MR 101% McLaughlin et. al 2016 AAPM Spring 52

53 MR edema 3 w MR 130% MR Implant 3 w Chung et. al 2016 AAPM Spring 53
54 Edema Model Max 1 day Longer to resolve than initial swelling Quick resolution - 2 weeks Slow resolution 2 to 4 weeks T1/2 ~ 10 d (4 to 25 days) 2016 AAPM Spring 54
55 Effect on post implant dosimetry Day 1 edema large underestimate dose Day 100 edema resolved overestimate dose 2016 AAPM Spring 55
56 Edema Model Assumes seeds move with the prostate Seeds inside the prostate? Stranded seeds 2016 AAPM Spring 56
57 McLaughlin et. al AAPM Spring 57

58 2016 AAPM Spring 58
59 2016 AAPM Spring 59

60 2016 AAPM Spring 60

61 2016 AAPM Spring 61
62 By how much? Timing of imaging Magnitude of prostate swelling Rate of resolution Radioactive T 1/2 Short T1/2 & low energy 2016 AAPM Spring 62

63 Optimal time 131 Cs 10+2 days 103 Pd 16+2 days 125 I 42+2 days 2016 AAPM Spring 63
64 Recommendation Timing of imaging Pre-Implant prostate volume Implant day dosimetry US immediate CT/MR 2 to 4 h Post-Implant dosimetry 131 Cs 10+2 days 103 Pd 16+2 days 125 I 1month+1week 2016 AAPM Spring 64
65 The optimal timing for post implant dosimetry is 20% 1. Immediately following the implant 20% 20% 20% 20% 2. 2 weeks after the implant 3. 1 month after the implant 4. 10, 16 and 42 days for 131 Cs, 103 Pd, 125 I respectively 5. No post implant dosimetry is required 10
66 The optimal timing for post implant dosimetry is 20% 1. Immediately following the implant 20% 20% 20% 20% 2. 2 weeks after the implant 3. 1 month after the implant 4. 10, 16 and 42 days for 131 Cs, 103 Pd, 125 I respectively 5. No post implant dosimetry is required Answer: 4 Reference: AAPM TG137, Nath et. al
67 Post implant prostate volume under- or overestimation is a result of 20% 1. The timing of dosimetry 20% 20% 20% 20% 2. Magnitude of preimplant prostate swelling 3. The rate of edema resolution 4. The radioactive decay half-life 5. All of the above 10
68 Post implant prostate volume under- or overestimation is a result of 20% 1. The timing of dosimetry 20% 20% 20% 20% 2. Magnitude of preimplant prostate swelling 3. The rate of edema resolution 4. The radioactive decay half-life 5. All of the above Answer: 5 Reference: AAPM TG137, Nath et. al
69 Impact of treatment planning approaches on dose reporting Planning techniques Choice of isotope Choice of source strength Calculation Algorithm Dose indices for target and normal tissue Recommendations for planning and dose reporting 2016 AAPM Spring 69


70 Peripheral loading? Volume % Prostate, with error Nomogram Differential Periphery Spike Volume % Prostate cm margin, with error Nomogram Differential Periphery Spike Dose (Gy) Narayana et. al Dose (Gy) 2016 AAPM Spring 70
71 Loose seeds vs strands Loose Seeds Expand with the prostate Migrate to the lung Strands No migration May not track with the prostate 2016 AAPM Spring 71
72 Seed Drop off Stranded preloaded Mick applicator Thin stranded seeds Preloaded cartridge 2016 AAPM Spring 72
73 Seed Drop off Prostate V100 % Prostate D90 Gy Rec wall D1cc Gy Rec wall D2cc Gy Urethra D10 Gy Rapid Strand Mick applicator Thin strand Preloaded cartridge AAPM Spring 73
74 Choice of Isotope 131 Cs 103 Pd 125 I 2016 AAPM Spring 74
75 I125 I-125 vs. Pd Vol + Error Ideal I Vol + Error Error Pd-103 Volume % Volume % Ideal Error Relative Prescription Dose Relative Prescription Dose Narayana et. al 2016 AAPM Spring 75
76 Seed Drop off Prostate V100 % Prostate D90 Gy Rec wall D1cc Gy Rec wall D2cc Gy Urethra D10 Gy Rapid Strand Mick applicator Thin strand Preloaded cartridge AAPM Spring 76
77 Source strength? Prospective Randomized Trial high vs. low mci No sig diff Transition Zone 2mm exp Prostate Narayana et. al Rectum Axial 2016 AAPM Spring 77
78 Calculation Algorithm 2016 AAPM Spring 78
79 GTV Recommendations CTV no posterior expansion PTV=CTV OAR Urethra Rectum Penile bulb 2016 AAPM Spring 79
80 Recommendations Dose clinical decision 131 Cs 115 Gy? ( Gy) 103 Pd 125 Gy 125 I 145 Gy 2016 AAPM Spring 80
81 CTV Recommendations Planning criteria V100> 95% of CTV D90 > 100 % of Rx V150 < 50% of CTV Rectum D2cc < Rx dose Urethra D10 < 150% Rx dose D30< 130% of Rx dose Penile bulb - investigational 2016 AAPM Spring 81
82 Recommendations Dose Reporting DVH for target Primary, D90,V100, V150 Secondary V200, V90,D100 Urethra D10 Secondary: D0.4cc, D30, D5 Rectum D2cc, Secondary: D0.1 cc, V AAPM Spring 82
83 Primary dose parameters for prostate implant that should always be 20% 1. D 90 reported are 20% 20% 20% 20% 2. V D 90 & V D 90 V 100 & V D 90 D 100 V 90 V 100 & V
84 Primary dose parameters for prostate implant that should always be 20% 1. D 90 reported are 20% 20% 20% 20% 2. V D 90 & V D 90 V 100 & V D 90 D 100 V 90 V 100 & V 150 Answer: 4 Reference: AAPM TG137, Nath et. al
85 Intraoperative treatment planning strategies Intraoperative preplanning Interactive planning Dynamic dose calculations Recommendations on Intraoperative planning and evaluation 2016 AAPM Spring 85
86 Pre vs. OR planning Pre 2 procedures Reproducible setup OR Target Volume Stress Time pressure # of seeds ordered 2016 AAPM Spring 86
87 Techniques Intraoperative Creation of plan in OR just before the implant Immediate execution Interactive Stepwise refinement Computerized dose calculations based on image feedback Dynamic Calculations constantly updated using continuous deposited-seed-position feed back 2016 AAPM Spring 87
88 Recommendations Enhanced implant quality Post implant dosimetry Edema Seed migration 2016 AAPM Spring 88
89 Sector anaylsis Research setting 2016 AAPM Spring 89
90 Biophysical Models BED for prostate implants EUD calculations TCP Recommendations for reporting radiobiological response 2016 AAPM Spring 90
91 . BED BED = D[ 1+ D /( α / β )] BED = D( T ) RE( T ) eff eff ln 2 T α eff T p RE( T ) = 1+ D 1 ( ) α ( µ λ) 1 e β 2λT ( µ + λ ) T {1 e 2λ (1 e µ + λ 0 eff eff λt eff )} T eff = T ln[ α D avg T p T 1/ 2 ] 2016 AAPM Spring 91
92 BED for inhomogeneous dose BED 1 = ln( α i ν e i α BED i ) Teff 1 D( T ) ( ) ln 2 = ln( eff RE T ν eff ie αt α p i α BED i ) 2016 AAPM Spring 92
93 Equivalent uniform EBRT dose EUD d = α + ln( β d i γ ν i e α BED ln 2 /( d i ) T p ) 2016 AAPM Spring 93
94 TCP TCP( D) = ( TCD / D) k 50 TCP = exp[ N exp( α BED)] AAPM Spring 94
 235.3 93.9 60.8 Calculated with: α = 0.15 Gy -1, β = 0.05 Gy -2, α/β = 3.0 Gy, T p = 42 days, repair half-life of 0.")
95 Example Indices Radionuclide 125 I 103 Pd 131 Cs Dose (Gy) BED (Gy) EUD (Gy) TCP (%) T eff (day) Calculated with: α = 0.15 Gy -1, β = 0.05 Gy -2, α/β = 3.0 Gy, T p = 42 days, repair half-life of 0.27 hour, and N 0 = 5x AAPM Spring 95
96 Linear Quadratic Model ERD Nd 1 + N= # fx D = dose/fx α/β = 3Gy d = α β 2016 AAPM Spring 96
97 Linear Quadratic Model ERD NRt 1 + R = dose rate t = time Rt = G α β 2016 AAPM Spring 97
98 Linear Quadratic Model G LDR = 2 µ t 1 ( ) 1 e µ t µ t µ = repair rate const Rt ERD = NRt 1 + G α β 2016 AAPM Spring 98
99 Linear Quadratic Model ERD = R / λ IMP 1 + R ( ) µ + λ α β R = dose rate λ = decay constant µ = repair rate constant α/β = tissue specific parameter 2016 AAPM Spring 99


100 Linear Quadratic Model Beam? d = 2 Gy/fx α/β = 3Gy Brachy R = 4.4 cgy/h λ = 0.693/59.4 d -1 α/β = 3Gy µ =.4 h -1 d = D + α β ERD 1 R ERD = R / λ 1+ eq ( ) µ + λ α β 2016 AAPM Spring 100
101 Recommendations Adequate information BED EUD TCP Other 2016 AAPM Spring 101
102 Recommendation Model parameters should be specified All parameters required to calculate the biodose should be specified Encourage vendors to provide models 2016 AAPM Spring 102
103 What is the cause of most inconsistencies in dose reporting? 20% 1. Identification of source positions 20% 20% 20% 20% 2. Dose calculations 3. Target delineation 4. Timing of the imaging study 5. Type of isotope used 10
104 What is the cause of most inconsistencies in dose reporting? 20% 1. Identification of source positions 20% 20% 20% 20% 2. Dose calculations 3. Target delineation 4. Timing of the imaging study 5. Type of isotope used Answer: 3 Reference: AAPM TG137, Nath et. al
Patient Safety Focused QA. LDR Brachytherapy Vrinda Narayana
 Patient Safety Focused QA LDR Brachytherapy Vrinda Narayana D < 2 Gy/h Old LDR Brachytherapy? Ra-226; Cs-137; Ir-192 New Gynecological; interstitial Pd-103; I-125; Cs-131 Prostate implants Eye plaques
Patient Safety Focused QA LDR Brachytherapy Vrinda Narayana D < 2 Gy/h Old LDR Brachytherapy? Ra-226; Cs-137; Ir-192 New Gynecological; interstitial Pd-103; I-125; Cs-131 Prostate implants Eye plaques
Trina Lynd, M.S. Medical Physicist Lifefirst Imaging & Oncology Cullman, AL Tri-State Alabama, Louisiana and Mississippi Spring 2016 Meeting April
 Trina Lynd, M.S. Medical Physicist Lifefirst Imaging & Oncology Cullman, AL Tri-State Alabama, Louisiana and Mississippi Spring 2016 Meeting April 17, 2016 Discuss permanent prostate brachytherapy and
Trina Lynd, M.S. Medical Physicist Lifefirst Imaging & Oncology Cullman, AL Tri-State Alabama, Louisiana and Mississippi Spring 2016 Meeting April 17, 2016 Discuss permanent prostate brachytherapy and
DOSIMETRIC OPTIONS AND POSSIBILITIES OF PROSTATE LDR BRACHYTHERAPY WITH PERMANENT I-125 IMPLANTS
 DOSIMETRIC OPTIONS AND POSSIBILITIES OF PROSTATE LDR BRACHYTHERAPY WITH PERMANENT I-125 IMPLANTS Andrius IVANAUSKAS*, Eduardas ALEKNAVIČIUS*, Arvydas BURNECKIS*, Albert MILLER *Institute of Oncology Vilnius
DOSIMETRIC OPTIONS AND POSSIBILITIES OF PROSTATE LDR BRACHYTHERAPY WITH PERMANENT I-125 IMPLANTS Andrius IVANAUSKAS*, Eduardas ALEKNAVIČIUS*, Arvydas BURNECKIS*, Albert MILLER *Institute of Oncology Vilnius
Content. Acknowledgments. Prostate brachy LDR Prostate brachy HDR. Use of permanent seeds and HDR in prostate: Current practice and advances
 IRIMED Use of permanent seeds and HDR in prostate: Current practice and advances Content Prostate brachy LDR Prostate brachy HDR Jose Perez-Calatayud Hospital Universitario y Politecnico La Fe. Valencia.
IRIMED Use of permanent seeds and HDR in prostate: Current practice and advances Content Prostate brachy LDR Prostate brachy HDR Jose Perez-Calatayud Hospital Universitario y Politecnico La Fe. Valencia.
HDR vs. LDR Is One Better Than The Other?
 HDR vs. LDR Is One Better Than The Other? Daniel Fernandez, MD, PhD 11/3/2017 New Frontiers in Urologic Oncology Learning Objectives Indications for prostate brachytherapy Identify pros/cons of HDR vs
HDR vs. LDR Is One Better Than The Other? Daniel Fernandez, MD, PhD 11/3/2017 New Frontiers in Urologic Oncology Learning Objectives Indications for prostate brachytherapy Identify pros/cons of HDR vs
Permanent Prostate Brachytherapy Post Procedure Evaluation
 Permanent Prostate Brachytherapy Post Procedure Evaluation William S. Bice, Jr., Ph.D. UTHSCSA, San Antonio, Texas IMPS, San Antonio, Texas Texas Cancer Clinic, San Antonio, Texas Implant Evaluation for
Permanent Prostate Brachytherapy Post Procedure Evaluation William S. Bice, Jr., Ph.D. UTHSCSA, San Antonio, Texas IMPS, San Antonio, Texas Texas Cancer Clinic, San Antonio, Texas Implant Evaluation for
Definitions. Brachytherapy in treatment of cancer. Implantation Techniques and Methods of Dose Specifications. Importance of Brachytherapy in GYN
 Implantation Techniques and Methods of Dose Specifications Brachytherapy Course Lecture V Krishna Reddy, MD, PhD Assistant Professor, Radiation Oncology Brachytherapy in treatment of cancer GYN Cervical
Implantation Techniques and Methods of Dose Specifications Brachytherapy Course Lecture V Krishna Reddy, MD, PhD Assistant Professor, Radiation Oncology Brachytherapy in treatment of cancer GYN Cervical
Transperineal Interstitial Permanent Prostate Brachytherapy (TIPPB) Quality Assurance Guidelines
 Quality Assurance Guidelines") Prostate Brachytherapy QA Page 1 of 1 Transperineal Interstitial Permanent Prostate Brachytherapy (TIPPB) Quality Assurance Guidelines I. Purpose Table of Contents II. III. IV. Background Credentialing
Prostate Brachytherapy QA Page 1 of 1 Transperineal Interstitial Permanent Prostate Brachytherapy (TIPPB) Quality Assurance Guidelines I. Purpose Table of Contents II. III. IV. Background Credentialing
Brachytherapy Planning and Quality Assurance w Classical implant systems and modern computerized dosimetry w Most common clinical applications w
 Brachytherapy Planning and Quality Assurance w Classical implant systems and modern computerized dosimetry w Most common clinical applications w Quality assurance Classical implant systems w Manchester
Brachytherapy Planning and Quality Assurance w Classical implant systems and modern computerized dosimetry w Most common clinical applications w Quality assurance Classical implant systems w Manchester
Brachytherapy Planning and Quality Assurance
 Brachytherapy Planning and Quality Assurance Classical implant systems Most common clinical applications and modern dosimetry methods Quality assurance Classical implant systems Manchester (Paterson-Parker)
Brachytherapy Planning and Quality Assurance Classical implant systems Most common clinical applications and modern dosimetry methods Quality assurance Classical implant systems Manchester (Paterson-Parker)
Radiobiological Models in Brachytherapy Planning and Evaluation
 Therapy Educational Course (TH-C-108, 10:30-11:25 am): Radiobiological Models in Brachytherapy Planning and Evaluation Zhe (Jay) Chen, PhD & David J. Carlson, PhD Department of Therapeutic Radiology S
Therapy Educational Course (TH-C-108, 10:30-11:25 am): Radiobiological Models in Brachytherapy Planning and Evaluation Zhe (Jay) Chen, PhD & David J. Carlson, PhD Department of Therapeutic Radiology S
Feasibility of 4D IMRT Delivery for Hypofractionated High Dose Partial Prostate Treatments
 Feasibility of 4D IMRT Delivery for Hypofractionated High Dose Partial Prostate Treatments R.A. Price Jr., Ph.D., J. Li, Ph.D., A. Pollack, M.D., Ph.D.*, L. Jin, Ph.D., E. Horwitz, M.D., M. Buyyounouski,
Feasibility of 4D IMRT Delivery for Hypofractionated High Dose Partial Prostate Treatments R.A. Price Jr., Ph.D., J. Li, Ph.D., A. Pollack, M.D., Ph.D.*, L. Jin, Ph.D., E. Horwitz, M.D., M. Buyyounouski,
CONFLICTS OF INTEREST FOR THIS SESSION
 LDR PROSTATE 2 CONFLICTS OF INTEREST FOR THIS SESSION Zhe (Jay) Chen: Reports an NIH research grant Zoubir Ouhib: is a member of the Elekta Speakers Bureau The following speakers have no conflicts to declare
LDR PROSTATE 2 CONFLICTS OF INTEREST FOR THIS SESSION Zhe (Jay) Chen: Reports an NIH research grant Zoubir Ouhib: is a member of the Elekta Speakers Bureau The following speakers have no conflicts to declare
IMRT - the physician s eye-view. Cinzia Iotti Department of Radiation Oncology S.Maria Nuova Hospital Reggio Emilia
 IMRT - the physician s eye-view Cinzia Iotti Department of Radiation Oncology S.Maria Nuova Hospital Reggio Emilia The goals of cancer therapy Local control Survival Functional status Quality of life Causes
IMRT - the physician s eye-view Cinzia Iotti Department of Radiation Oncology S.Maria Nuova Hospital Reggio Emilia The goals of cancer therapy Local control Survival Functional status Quality of life Causes
CT Guided Contouring: Challenges and Pitfalls
 CT Guided Contouring: Challenges and Pitfalls Dr Umesh Mahantshetty, Associate Professor, GYN & Urology Disease Management Group (DMG) Member Tata Memorial Hospital, Mumbai, India GYN GEC ESTRO NETWORK
CT Guided Contouring: Challenges and Pitfalls Dr Umesh Mahantshetty, Associate Professor, GYN & Urology Disease Management Group (DMG) Member Tata Memorial Hospital, Mumbai, India GYN GEC ESTRO NETWORK
Limitations. General Clinical Applications of Brachytherapy Physics. Learning Objectives. Conflicts of Interest. University of Wisconsin - Madison
 General Clinical Applications of Brachytherapy Physics Bruce Thomadsen Limitations Due to file size limitations for this handout, many of the figures have had to be removed. I apologize for the lack of
General Clinical Applications of Brachytherapy Physics Bruce Thomadsen Limitations Due to file size limitations for this handout, many of the figures have had to be removed. I apologize for the lack of
Graduate Theses and Dissertations
 University of South Florida Scholar Commons Graduate Theses and Dissertations Graduate School 2011 Biological Effective Dose (BED) Distribution Matching for Obtaining Brachytherapy Prescription Doses &
University of South Florida Scholar Commons Graduate Theses and Dissertations Graduate School 2011 Biological Effective Dose (BED) Distribution Matching for Obtaining Brachytherapy Prescription Doses &
Outline - MRI - CT - US. - Combinations of imaging modalities for treatment planning
 Imaging Outline - MRI - CT - US - Combinations of imaging modalities for treatment planning Imaging Part 1: MRI MRI for cervical cancer high soft tissue contrast multiplanar imaging MRI anatomy: the normal
Imaging Outline - MRI - CT - US - Combinations of imaging modalities for treatment planning Imaging Part 1: MRI MRI for cervical cancer high soft tissue contrast multiplanar imaging MRI anatomy: the normal
MRI Based treatment planning for with focus on prostate cancer. Xinglei Shen, MD Department of Radiation Oncology KUMC
 MRI Based treatment planning for with focus on prostate cancer Xinglei Shen, MD Department of Radiation Oncology KUMC Overview How magnetic resonance imaging works (very simple version) Indications for
MRI Based treatment planning for with focus on prostate cancer Xinglei Shen, MD Department of Radiation Oncology KUMC Overview How magnetic resonance imaging works (very simple version) Indications for
IMRT for Prostate Cancer
 IMRT for Cancer All patients are simulated in the supine position. Reproducibility is achieved using a custom alpha cradle cast that extends from the mid-back to mid-thigh. The feet are positioned in a
IMRT for Cancer All patients are simulated in the supine position. Reproducibility is achieved using a custom alpha cradle cast that extends from the mid-back to mid-thigh. The feet are positioned in a
MR-Guided Brachytherapy
 MR-Guided Brachytherapy Joann I. Prisciandaro, Ph.D. The Department of Radiation Oncology University of Michigan Outline Traditional 2D technique for brachytherapy treatment planning Transition to MR-guided
MR-Guided Brachytherapy Joann I. Prisciandaro, Ph.D. The Department of Radiation Oncology University of Michigan Outline Traditional 2D technique for brachytherapy treatment planning Transition to MR-guided
Outline. Contour quality control. Dosimetric impact of contouring errors and variability in Intensity Modulated Radiation Therapy (IMRT)
") Dosimetric impact of contouring errors and variability in Intensity Modulated Radiation Therapy (IMRT) James Kavanaugh, MS DABR Department of Radiation Oncology Division of Medical Physics Outline Importance
Dosimetric impact of contouring errors and variability in Intensity Modulated Radiation Therapy (IMRT) James Kavanaugh, MS DABR Department of Radiation Oncology Division of Medical Physics Outline Importance
A Comparison of IMRT and VMAT Technique for the Treatment of Rectal Cancer
 A Comparison of IMRT and VMAT Technique for the Treatment of Rectal Cancer Tony Kin Ming Lam Radiation Planner Dr Patricia Lindsay, Radiation Physicist Dr John Kim, Radiation Oncologist Dr Kim Ann Ung,
A Comparison of IMRT and VMAT Technique for the Treatment of Rectal Cancer Tony Kin Ming Lam Radiation Planner Dr Patricia Lindsay, Radiation Physicist Dr John Kim, Radiation Oncologist Dr Kim Ann Ung,
Dose escalation in permanent brachytherapy for prostate cancer: dosimetric and biological considerations*
 INSTITUTE OF PHYSICS PUBLISHING Phys. Med. Biol. 48 (2003) 2753 2765 PHYSICS IN MEDICINE AND BIOLOGY PII: S0031-9155(03)62377-8 Dose escalation in permanent brachytherapy for prostate cancer: dosimetric
INSTITUTE OF PHYSICS PUBLISHING Phys. Med. Biol. 48 (2003) 2753 2765 PHYSICS IN MEDICINE AND BIOLOGY PII: S0031-9155(03)62377-8 Dose escalation in permanent brachytherapy for prostate cancer: dosimetric
Radiobiological principles of brachytherapy
 Radiobiological principles of brachytherapy Low dose rate (LDR) Medium dose rate (MDR) High dose rate (HDR) The effect of dose rate As the dose rate is decreased, there is more time during irradiation
Radiobiological principles of brachytherapy Low dose rate (LDR) Medium dose rate (MDR) High dose rate (HDR) The effect of dose rate As the dose rate is decreased, there is more time during irradiation
CT Guided Contouring: Challenges and Pitfalls
 CT Guided Contouring: Challenges and Pitfalls Dr Umesh Mahantshetty, Associate Professor, GYN & Urology Disease Management Group (DMG) Member Tata Memorial Hospital, Mumbai, India GYN GEC ESTRO NETWORK
CT Guided Contouring: Challenges and Pitfalls Dr Umesh Mahantshetty, Associate Professor, GYN & Urology Disease Management Group (DMG) Member Tata Memorial Hospital, Mumbai, India GYN GEC ESTRO NETWORK
Can we deliver the dose distribution we plan in HDR-Brachytherapy of Prostate Cancer?
 Can we deliver the dose distribution we plan in HDR-Brachytherapy of Prostate Cancer? Dimos Baltas Dept. of Medical Physics & Engineering, Strahlenklinik, Klinikum Offenbach GmbH 63069 Offenbach, Germany
Can we deliver the dose distribution we plan in HDR-Brachytherapy of Prostate Cancer? Dimos Baltas Dept. of Medical Physics & Engineering, Strahlenklinik, Klinikum Offenbach GmbH 63069 Offenbach, Germany
2
 1 2 3 4 5 6 7 The RTOG contouring recommendations state the femurs are to be contourned to the bottom of the ischial tuberosity. 8 This slide shows the hourglass configuration. It is only present in about
1 2 3 4 5 6 7 The RTOG contouring recommendations state the femurs are to be contourned to the bottom of the ischial tuberosity. 8 This slide shows the hourglass configuration. It is only present in about
CyberKnife Monotherapy for Prostate Cancer
 C H A P T E R 29 CyberKnife Monotherapy for Prostate Cancer Clinton A. Medbery Marianne M. Young Astrid E. Morrison J. Stephen Archer Maximian F. D Souza Cindy Parry Abstract The purpose of our planned
C H A P T E R 29 CyberKnife Monotherapy for Prostate Cancer Clinton A. Medbery Marianne M. Young Astrid E. Morrison J. Stephen Archer Maximian F. D Souza Cindy Parry Abstract The purpose of our planned
MRI Guided GYN Brachytherapy: Clinical Considerations
 MRI Guided GYN Brachytherapy: Clinical Considerations AAPM Junzo Chino MD Duke Radiation Oncology 8/8/2013 Disclosures none Learning Objectives Historical Context: Film based Brachytherapy Advantages of
MRI Guided GYN Brachytherapy: Clinical Considerations AAPM Junzo Chino MD Duke Radiation Oncology 8/8/2013 Disclosures none Learning Objectives Historical Context: Film based Brachytherapy Advantages of
20 Prostate Cancer Dan Ash
 20 Prostate Cancer Dan Ash 1 Introduction Prostate cancer is a disease of ageing men for which the aetiology remains unknown. The incidence rises up to 30 to 40% in men over 80. The symptoms of localised
20 Prostate Cancer Dan Ash 1 Introduction Prostate cancer is a disease of ageing men for which the aetiology remains unknown. The incidence rises up to 30 to 40% in men over 80. The symptoms of localised
Post Prostatectomy Radia/on. Bill McLaughlin MD University of Michigan
 Post Prostatectomy Radia/on Bill McLaughlin MD University of Michigan No disclosures COI Important Disclosure I am the most pro-surgery radia/on oncologist in the universe Example: If a 45 year old man
Post Prostatectomy Radia/on Bill McLaughlin MD University of Michigan No disclosures COI Important Disclosure I am the most pro-surgery radia/on oncologist in the universe Example: If a 45 year old man
Index. B Biologically effective dose (BED), 158
, 158") Index B Biologically effective dose (BED), 158 C Catheter displacement, 113, 114 rectal probe, 114 self-anchoring catheters, 113 Catheter fixation, HDR, 106 107 Catheter insertion, HDR sagittal ultrasound
Index B Biologically effective dose (BED), 158 C Catheter displacement, 113, 114 rectal probe, 114 self-anchoring catheters, 113 Catheter fixation, HDR, 106 107 Catheter insertion, HDR sagittal ultrasound
New Technologies for the Radiotherapy of Prostate Cancer
 Prostate Cancer Meyer JL (ed): IMRT, IGRT, SBRT Advances in the Treatment Planning and Delivery of Radiotherapy. Front Radiat Ther Oncol. Basel, Karger, 27, vol. 4, pp 315 337 New Technologies for the
Prostate Cancer Meyer JL (ed): IMRT, IGRT, SBRT Advances in the Treatment Planning and Delivery of Radiotherapy. Front Radiat Ther Oncol. Basel, Karger, 27, vol. 4, pp 315 337 New Technologies for the
Basic Concepts in Image Based Brachytherapy (GEC-ESTRO Target Concept & Contouring)
") Basic Concepts in Image Based Brachytherapy (GEC-ESTRO Target Concept & Contouring) Dr Umesh Mahantshetty, Professor, Radiation Oncology GYN & Urology Disease Management Group (DMG) Member Tata Memorial
Basic Concepts in Image Based Brachytherapy (GEC-ESTRO Target Concept & Contouring) Dr Umesh Mahantshetty, Professor, Radiation Oncology GYN & Urology Disease Management Group (DMG) Member Tata Memorial
Radiation Therapy for Prostate Cancer. Resident Dept of Urology General Surgery Grand Round November 24, 2008
 Radiation Therapy for Prostate Cancer Amy Hou,, MD Resident Dept of Urology General Surgery Grand Round November 24, 2008 External Beam Radiation Advances Improving Therapy Generation of linear accelerators
Radiation Therapy for Prostate Cancer Amy Hou,, MD Resident Dept of Urology General Surgery Grand Round November 24, 2008 External Beam Radiation Advances Improving Therapy Generation of linear accelerators
ADVANCED TECHNOLOGY CONSORTIUM (ATC) CREDENTIALING PROCEDURES FOR LUNG BRACHYTHERAPY IMPLANT PROTOCOLS
 CREDENTIALING PROCEDURES FOR LUNG BRACHYTHERAPY IMPLANT PROTOCOLS") ACOSOG-RTOG Lung Brachytherapy QA Page 1 of 8 ADVANCED TECHNOLOGY CONSORTIUM (ATC) CREDENTIALING PROCEDURES FOR LUNG BRACHYTHERAPY IMPLANT PROTOCOLS FACILITY QUESTIONNAIRE Institutions wishing to enter
ACOSOG-RTOG Lung Brachytherapy QA Page 1 of 8 ADVANCED TECHNOLOGY CONSORTIUM (ATC) CREDENTIALING PROCEDURES FOR LUNG BRACHYTHERAPY IMPLANT PROTOCOLS FACILITY QUESTIONNAIRE Institutions wishing to enter
Quality Assurance of Ultrasound Imaging in Radiation Therapy. Zuofeng Li, D.Sc. Murty S. Goddu, Ph.D. Washington University St.
 Quality Assurance of Ultrasound Imaging in Radiation Therapy Zuofeng Li, D.Sc. Murty S. Goddu, Ph.D. Washington University St. Louis, Missouri Typical Applications of Ultrasound Imaging in Radiation Therapy
Quality Assurance of Ultrasound Imaging in Radiation Therapy Zuofeng Li, D.Sc. Murty S. Goddu, Ph.D. Washington University St. Louis, Missouri Typical Applications of Ultrasound Imaging in Radiation Therapy
Can we deliver the dose distribution we plan in HDR-Brachytherapy of Prostate Cancer?
 Can we deliver the dose distribution we plan in HDR-Brachytherapy of Prostate Cancer? Dimos Baltas 1,3, Natasa Milickovic 1, Nikolaos Zamboglou 2 1 Dept. of Medical Physics & Engineering, 2 Strahlenklinik,
Can we deliver the dose distribution we plan in HDR-Brachytherapy of Prostate Cancer? Dimos Baltas 1,3, Natasa Milickovic 1, Nikolaos Zamboglou 2 1 Dept. of Medical Physics & Engineering, 2 Strahlenklinik,
BASIC CLINICAL RADIOBIOLOGY
 INT6062: Strengthening Capacity for Cervical Cancer Control through Improvement of Diagnosis and Treatment BASIC CLINICAL RADIOBIOLOGY Alfredo Polo MD, PhD Applied Radiation Biology and Radiotherapy Section
INT6062: Strengthening Capacity for Cervical Cancer Control through Improvement of Diagnosis and Treatment BASIC CLINICAL RADIOBIOLOGY Alfredo Polo MD, PhD Applied Radiation Biology and Radiotherapy Section
Acknowledgements. QA Concerns in MR Brachytherapy. Learning Objectives. Traditional T&O. Traditional Summary. Dose calculation 3/7/2015
 Acknowledgements QA Concerns in MR Brachytherapy Robert A. Cormack Dana Farber Cancer Institute & Brigham and Women s Hospital No financial conflicts of interest I may mention use of devices in ways that
Acknowledgements QA Concerns in MR Brachytherapy Robert A. Cormack Dana Farber Cancer Institute & Brigham and Women s Hospital No financial conflicts of interest I may mention use of devices in ways that
Predicting (and avoiding) Morbidity in LDR Prostate Brachytherapy
 Morbidity in LDR Prostate Brachytherapy") Predicting (and avoiding) Morbidity in LDR Prostate Brachytherapy Juanita Crook Professor Radiation Oncology University of Toronto University of British Columbia BCCA CSI 1 Categories of Morbidity Urinary
Predicting (and avoiding) Morbidity in LDR Prostate Brachytherapy Juanita Crook Professor Radiation Oncology University of Toronto University of British Columbia BCCA CSI 1 Categories of Morbidity Urinary
Optimal Imaging and Technical Aspects of Prostate SRT
 Optimal Imaging and Technical Aspects of Prostate SRT Maris Mezeckis Dr., MBA, Vladislav Buryk Dr., PhD Sigulda Hospital Stereotactic Radiosurgery centre Homogeneous planning: PTV=prostate + 5 mm, 3 mm
Optimal Imaging and Technical Aspects of Prostate SRT Maris Mezeckis Dr., MBA, Vladislav Buryk Dr., PhD Sigulda Hospital Stereotactic Radiosurgery centre Homogeneous planning: PTV=prostate + 5 mm, 3 mm
Regulatory Guidelines and Computational Methods for Safe Release of Radioactive Patients II. Brachytherapy
 Regulatory Guidelines and Computational Methods for Safe Release of Radioactive Patients II. Brachytherapy Firas Mourtada, Ph.D., DABR Chief of Clinical Physics Helen F. Graham Cancer Center Christiana
Regulatory Guidelines and Computational Methods for Safe Release of Radioactive Patients II. Brachytherapy Firas Mourtada, Ph.D., DABR Chief of Clinical Physics Helen F. Graham Cancer Center Christiana
Evaluation of Normal Tissue Complication Probability and Risk of Second Primary Cancer in Prostate Radiotherapy
 Evaluation of Normal Tissue Complication Probability and Risk of Second Primary Cancer in Prostate Radiotherapy Rungdham Takam Thesis submitted for the degree of Doctor of Philosophy in The School of Chemistry
Evaluation of Normal Tissue Complication Probability and Risk of Second Primary Cancer in Prostate Radiotherapy Rungdham Takam Thesis submitted for the degree of Doctor of Philosophy in The School of Chemistry
3D ANATOMY-BASED PLANNING OPTIMIZATION FOR HDR BRACHYTHERAPY OF CERVIX CANCER
 SAUDI JOURNAL OF OBSTETRICS AND GYNECOLOGY VOLUME 11 NO. 2 1430 H - 2009 G 3D ANATOMY-BASED PLANNING OPTIMIZATION FOR HDR BRACHYTHERAPY OF CERVIX CANCER DR YASIR BAHADUR 1, DR CAMELIA CONSTANTINESCU 2,
SAUDI JOURNAL OF OBSTETRICS AND GYNECOLOGY VOLUME 11 NO. 2 1430 H - 2009 G 3D ANATOMY-BASED PLANNING OPTIMIZATION FOR HDR BRACHYTHERAPY OF CERVIX CANCER DR YASIR BAHADUR 1, DR CAMELIA CONSTANTINESCU 2,
HDR Applicators and Dosimetry*
 HDR Applicators and Dosimetry* Jason Rownd, MS Medical College of Wisconsin *with a too much radiobiology Objectives Review the radiobiology of brachytherapy-linear quadratic model. Understand how to convert
HDR Applicators and Dosimetry* Jason Rownd, MS Medical College of Wisconsin *with a too much radiobiology Objectives Review the radiobiology of brachytherapy-linear quadratic model. Understand how to convert
UltrasoundeCT fusion compared with MReCT fusion for postimplant dosimetry in permanent prostate brachytherapy
 Brachytherapy 12 (2013) 38e43 UltrasoundeCT fusion compared with MReCT fusion for postimplant dosimetry in permanent prostate brachytherapy David Bowes 1, Juanita M. Crook 2, *, Cynthia Araujo 3, Deidre
Brachytherapy 12 (2013) 38e43 UltrasoundeCT fusion compared with MReCT fusion for postimplant dosimetry in permanent prostate brachytherapy David Bowes 1, Juanita M. Crook 2, *, Cynthia Araujo 3, Deidre
HDR Brachytherapy: Results and Future Studies in Monotherapy
 HDR Brachytherapy: Results and Future Studies in Monotherapy Nikolaos Zamboglou and Nikolaos Tselis Strahlenklinik Klinikum Offenbach - Germany Prostate Brachytherapy UK & Ireland Conference 2013 Comparison
HDR Brachytherapy: Results and Future Studies in Monotherapy Nikolaos Zamboglou and Nikolaos Tselis Strahlenklinik Klinikum Offenbach - Germany Prostate Brachytherapy UK & Ireland Conference 2013 Comparison
JOURNAL OF APPLIED CLINICAL MEDICAL PHYSICS, VOLUME 6, NUMBER 2, SPRING 2005
 JOURNAL OF APPLIED CLINICAL MEDICAL PHYSICS, VOLUME 6, NUMBER 2, SPRING 2005 Advantages of inflatable multichannel endorectal applicator in the neo-adjuvant treatment of patients with locally advanced
JOURNAL OF APPLIED CLINICAL MEDICAL PHYSICS, VOLUME 6, NUMBER 2, SPRING 2005 Advantages of inflatable multichannel endorectal applicator in the neo-adjuvant treatment of patients with locally advanced
Stereotactic ablative body radiation for prostate cancer SABR
 Stereotactic ablative body radiation for prostate cancer SABR John Armstrong. Sinead Callinan. Luke Rock. Beacon Hospital, Dublin, Ireland Low- Intermediate Risk Prostate Comparing treatment choices IMRT
Stereotactic ablative body radiation for prostate cancer SABR John Armstrong. Sinead Callinan. Luke Rock. Beacon Hospital, Dublin, Ireland Low- Intermediate Risk Prostate Comparing treatment choices IMRT
Jean Pouliot, PhD Professor and Vice Chair, Department of Radiation Oncology, Director of Physics Division
 IMRT / Tomo / VMAT / Cyberknife / HDR Brachytherapy: Jean Pouliot, PhD Professor and Vice Chair, Department of Radiation Oncology, Director of Physics Division Should Choices be Based on Dosimetric and
IMRT / Tomo / VMAT / Cyberknife / HDR Brachytherapy: Jean Pouliot, PhD Professor and Vice Chair, Department of Radiation Oncology, Director of Physics Division Should Choices be Based on Dosimetric and
Prostate Cancer: Low Dose Rate (Seed) Brachytherapy. Information for patients, families and friends
 Brachytherapy. Information for patients, families and friends") Prostate Cancer: Low Dose Rate (Seed) Brachytherapy Information for patients, families and friends About this booklet This booklet is designed to give you information about low dose-rate (seed) brachytherapy
Prostate Cancer: Low Dose Rate (Seed) Brachytherapy Information for patients, families and friends About this booklet This booklet is designed to give you information about low dose-rate (seed) brachytherapy
The Physics of Oesophageal Cancer Radiotherapy
 The Physics of Oesophageal Cancer Radiotherapy Dr. Philip Wai Radiotherapy Physics Royal Marsden Hospital 1 Contents Brief clinical introduction Imaging and Target definition Dose prescription & patient
The Physics of Oesophageal Cancer Radiotherapy Dr. Philip Wai Radiotherapy Physics Royal Marsden Hospital 1 Contents Brief clinical introduction Imaging and Target definition Dose prescription & patient
Long Term Clinical Experience Using Ultrasound Alignment. Overview. Ultrasound Alignment Experience at Fox Chase
 Long Term Clinical Experience Using Ultrasound Alignment Shawn McNeeley M.S.. Fox Chase Cancer Center Department of Radiation Oncology Philadelphia, PA Overview Discuss various technique, and patient related,
Long Term Clinical Experience Using Ultrasound Alignment Shawn McNeeley M.S.. Fox Chase Cancer Center Department of Radiation Oncology Philadelphia, PA Overview Discuss various technique, and patient related,
Radiation Damage Comparison between Intensity Modulated Radiotherapy (IMRT) and Field-in-field (FIF) Technique In Breast Cancer Treatments
 and Field-in-field (FIF) Technique In Breast Cancer Treatments") Radiation Damage Comparison between Intensity Modulated Radiotherapy () and Field-in-field (FIF) Technique In Breast Cancer Treatments Huisi Ai 1 and Hualin Zhang 2 1. Department of Radiation Oncology,
Radiation Damage Comparison between Intensity Modulated Radiotherapy () and Field-in-field (FIF) Technique In Breast Cancer Treatments Huisi Ai 1 and Hualin Zhang 2 1. Department of Radiation Oncology,
CyberKnife SBRT for Prostate Cancer
 CyberKnife SBRT for Prostate Cancer Robert Meier, MD Swedish Radiosurgery Center Swedish Cancer Institute Seattle, WA 2017 ESTRO Meeting, Vienna Austria 5-year safety, efficacy & quality of life outcomes
CyberKnife SBRT for Prostate Cancer Robert Meier, MD Swedish Radiosurgery Center Swedish Cancer Institute Seattle, WA 2017 ESTRO Meeting, Vienna Austria 5-year safety, efficacy & quality of life outcomes
Pelvic Angiogram - Male
 Pelvic Angiogram - Male Common iliac artery Internal iliac artery Lateral sacral artery Iliolumbar artery Posterior trunk of internal iliac artery Superior gluteal artery Internal pudendal artery External
Pelvic Angiogram - Male Common iliac artery Internal iliac artery Lateral sacral artery Iliolumbar artery Posterior trunk of internal iliac artery Superior gluteal artery Internal pudendal artery External
Recent proceedings in Brachytherapy Physics
 Recent proceedings in Brachytherapy Physics Frank-André Siebert UKSH, Campus Kiel, Germany Clinic of Radiotherapy Dept. Medical Physics Physical characteristics of brachytherapy (Courtesy Luc Beaulieu,
Recent proceedings in Brachytherapy Physics Frank-André Siebert UKSH, Campus Kiel, Germany Clinic of Radiotherapy Dept. Medical Physics Physical characteristics of brachytherapy (Courtesy Luc Beaulieu,
MRI Applications in Radiation Oncology:
 MRI Applications in Radiation Oncology: Physician s Perspective Jeff Olsen, MD Department of Radiation Oncology Washington University, St. Louis, MO Disclosures Washington University has research and service
MRI Applications in Radiation Oncology: Physician s Perspective Jeff Olsen, MD Department of Radiation Oncology Washington University, St. Louis, MO Disclosures Washington University has research and service
Rectal dose and toxicity dosimetric evaluation for various beam arrangements using pencil beam scanning protons with and without rectal spacers
 Rectal dose and toxicity dosimetric evaluation for various beam arrangements using pencil beam scanning protons with and without rectal spacers 2015 MAC-AAPM Annual Meeting, Baltimore, MD Heeteak Chung,
Rectal dose and toxicity dosimetric evaluation for various beam arrangements using pencil beam scanning protons with and without rectal spacers 2015 MAC-AAPM Annual Meeting, Baltimore, MD Heeteak Chung,
Practical considerations in the selection of seed strength for prostate implants
 JOURNAL OF APPLIED CLINICAL MEDICAL PHYSICS, VOLUME 16, NUMBER 5, 2015 Practical considerations in the selection of seed strength for prostate implants Sarah L Elliott, 1a Catherine L. Beaufort, 1 Jeremy
JOURNAL OF APPLIED CLINICAL MEDICAL PHYSICS, VOLUME 16, NUMBER 5, 2015 Practical considerations in the selection of seed strength for prostate implants Sarah L Elliott, 1a Catherine L. Beaufort, 1 Jeremy
Transition to Heterogeneity Corrections. Why have accurate dose algorithms?
 Transition to Heterogeneity Corrections Eric E. Klein, M.S., Washington University, St. Louis, MO Craig Stevens, M.D., Ph.D., MD Anderson Cancer Center, Houston, TX Nikos Papinikolou, Ph.D., University
Transition to Heterogeneity Corrections Eric E. Klein, M.S., Washington University, St. Louis, MO Craig Stevens, M.D., Ph.D., MD Anderson Cancer Center, Houston, TX Nikos Papinikolou, Ph.D., University
8/2/2017. Improving Dose Prescriptions for Safety, Reporting, and Clinical Guideline Consistency. Part III
 Improving Dose Prescriptions for Safety, Reporting, and Clinical Guideline Consistency Part III I Das, J Moran, M Langer Keeping Guidelines On Track: The Effect On Clinical Practice of Neglecting Guidelines
Improving Dose Prescriptions for Safety, Reporting, and Clinical Guideline Consistency Part III I Das, J Moran, M Langer Keeping Guidelines On Track: The Effect On Clinical Practice of Neglecting Guidelines
PROSTATE CANCER BRACHYTHERAPY. Kazi S. Manir MD,DNB,PDCR RMO cum Clinical Tutor Department of Radiotherapy R. G. Kar Medical College
 PROSTATE CANCER BRACHYTHERAPY Kazi S. Manir MD,DNB,PDCR RMO cum Clinical Tutor Department of Radiotherapy R. G. Kar Medical College Risk categorization Very Low Risk Low Risk Intermediate Risk High Risk
PROSTATE CANCER BRACHYTHERAPY Kazi S. Manir MD,DNB,PDCR RMO cum Clinical Tutor Department of Radiotherapy R. G. Kar Medical College Risk categorization Very Low Risk Low Risk Intermediate Risk High Risk
Comprehensive and Practical Brachytherapy March 04-8 March 2018, Ljubljana, Slovenia Day 1 Sunday 4 March 2018
 Day 1 Sunday 4 March 2018 Welcome and Summary of the course 13:00-13:20 15 introduction 13:20-13:50 30 Radioactivity Radioactivity: What we need to know Characteristics of LDR-PDR-HDR, radiobiological
Day 1 Sunday 4 March 2018 Welcome and Summary of the course 13:00-13:20 15 introduction 13:20-13:50 30 Radioactivity Radioactivity: What we need to know Characteristics of LDR-PDR-HDR, radiobiological
Individualized dosimetry treatment planning for liver irradiation
 Individualized dosimetry treatment planning for liver irradiation A. Tai, B. Erickson, K. A. Khater,, X. A. Li Medical College of Wisconsin, Milwaukee Waukesha, Wisconsin 1 Outline Introduction Materials
Individualized dosimetry treatment planning for liver irradiation A. Tai, B. Erickson, K. A. Khater,, X. A. Li Medical College of Wisconsin, Milwaukee Waukesha, Wisconsin 1 Outline Introduction Materials
Johannes C. Athanasios Dimopoulos
 BrachyNext Symposium Miami Beach, USA, May 30 31, 2014 Imaging Modalities: Current Challenges and Future Directions Johannes C. Athanasios Dimopoulos Imaging Modalities: Current Challenges and Future Directions
BrachyNext Symposium Miami Beach, USA, May 30 31, 2014 Imaging Modalities: Current Challenges and Future Directions Johannes C. Athanasios Dimopoulos Imaging Modalities: Current Challenges and Future Directions
Pitfalls in SBRT Treatment Planning for a Moving Target
 Pitfalls in SBRT Treatment Planning for a Moving Target Cynthia F. Chuang, Ph.D. Department of Radiation Oncology University of California-San Francisco I have no conflicts of interests to disclose In
Pitfalls in SBRT Treatment Planning for a Moving Target Cynthia F. Chuang, Ph.D. Department of Radiation Oncology University of California-San Francisco I have no conflicts of interests to disclose In
Developments in Directional Brachytherapy William Y. Song, PhD, DABR
 Developments in Directional Brachytherapy William Y. Song, PhD, DABR Medical Physicist Dept. Radiation Oncology Massey Cancer Center Director CAMPEP Graduate Program Virginia Commonwealth University Associate
Developments in Directional Brachytherapy William Y. Song, PhD, DABR Medical Physicist Dept. Radiation Oncology Massey Cancer Center Director CAMPEP Graduate Program Virginia Commonwealth University Associate
Isoeffective Dose Specification of Normal Liver in Yttrium-90 Microsphere Radioembolization*
 Isoeffective Dose Specification of Normal Liver in Yttrium-90 Microsphere Radioembolization* Barry W. Wessels, Ph.D 1 ; Amilia G. Di Dia, PhD 2 ;Yiran Zheng, PhD 1 Marta Cremonesi, PhD 2 1 University Hospitals
Isoeffective Dose Specification of Normal Liver in Yttrium-90 Microsphere Radioembolization* Barry W. Wessels, Ph.D 1 ; Amilia G. Di Dia, PhD 2 ;Yiran Zheng, PhD 1 Marta Cremonesi, PhD 2 1 University Hospitals
Abstract Purpose: Material and methods: Results: Conclusions: Key words: Purpose Address for correspondence:
 Original paper Physics Contributions The impact of activating source dwell positions outside the CTV on the dose to treated normal tissue volumes in TRUS guided 3D conformal interstitial HDR brachytherapy
Original paper Physics Contributions The impact of activating source dwell positions outside the CTV on the dose to treated normal tissue volumes in TRUS guided 3D conformal interstitial HDR brachytherapy
TRANSRECTAL ULTRASOUND-GUIDED PROSTATE BRACHYTHERAPY
 TRANSRECTAL ULTRASOUND-GUIDED PROSTATE BRACHYTHERAPY 1 TRANSRECTAL ULTRASOUND-GUIDED PROSTATE BRACHYTHERAPY BRENDAN CAREY, MD TRANSRECTAL ULTRASOUND-GUIDED PROSTATE BRACHYTHERAPY 2 TRANSRECTAL ULTRASOUND-GUIDED
TRANSRECTAL ULTRASOUND-GUIDED PROSTATE BRACHYTHERAPY 1 TRANSRECTAL ULTRASOUND-GUIDED PROSTATE BRACHYTHERAPY BRENDAN CAREY, MD TRANSRECTAL ULTRASOUND-GUIDED PROSTATE BRACHYTHERAPY 2 TRANSRECTAL ULTRASOUND-GUIDED
The New ICRU/GEC ESTRO Report in Clinical Practice. Disclosures
 The New ICRU/GEC ESTRO Report in Clinical Practice Christian Kirisits, MSc, PhD; Richard Pötter, MD Medical University of Vienna, Vienna, Austria On behalf of the Committee: B. Erickson, C. Haie Meder,
The New ICRU/GEC ESTRO Report in Clinical Practice Christian Kirisits, MSc, PhD; Richard Pötter, MD Medical University of Vienna, Vienna, Austria On behalf of the Committee: B. Erickson, C. Haie Meder,
Real-time brachytherapy for prostate cancer implant analysis
 Rep Pract Oncol Radiother, 2008; 13(1): 9-14 Original Paper Received: 2007.04.17 Accepted: 2008.02.07 Published: 2008.02.29 Authors Contribution: A Study Design B Data Collection C Statistical Analysis
Rep Pract Oncol Radiother, 2008; 13(1): 9-14 Original Paper Received: 2007.04.17 Accepted: 2008.02.07 Published: 2008.02.29 Authors Contribution: A Study Design B Data Collection C Statistical Analysis
Will CyberKnife M6 Multileaf collimator offer advantages over IRIS collimator in prostate SBRT?
 Will CyberKnife M6 Multileaf collimator offer advantages over collimator in prostate SBRT? Vindu Kathriarachchi Professional Science Master in Medical Physics Department of Physics, Florida Atlantic University,
Will CyberKnife M6 Multileaf collimator offer advantages over collimator in prostate SBRT? Vindu Kathriarachchi Professional Science Master in Medical Physics Department of Physics, Florida Atlantic University,
Clinical Implementation of a New Ultrasound Guidance System. Vikren Sarkar Bill Salter Martin Szegedi
 Clinical Implementation of a New Ultrasound Guidance System Vikren Sarkar Bill Salter Martin Szegedi Disclosure The University of Utah has research agreements with Elekta Agenda Historical Review Trans-Abdominal
Clinical Implementation of a New Ultrasound Guidance System Vikren Sarkar Bill Salter Martin Szegedi Disclosure The University of Utah has research agreements with Elekta Agenda Historical Review Trans-Abdominal
Prostate MRI: Not So Difficult. Neil M. Rofsky, MD, FACR, FSCBTMR, FISMRM Dallas, TX
 Prostate MRI: Not So Difficult Neil M. Rofsky, MD, FACR, FSCBTMR, FISMRM Dallas, TX What is the biggest barrier to your practice incorporating prostate MRI? 1) I don t know how to read the cases 2) I don
Prostate MRI: Not So Difficult Neil M. Rofsky, MD, FACR, FSCBTMR, FISMRM Dallas, TX What is the biggest barrier to your practice incorporating prostate MRI? 1) I don t know how to read the cases 2) I don
From position verification and correction to adaptive RT Adaptive RT and dose accumulation
 From position verification and correction to adaptive RT Adaptive RT and dose accumulation Hans de Boer Move away from Single pre-treatment scan Single treatment plan Treatment corrections by couch shifts
From position verification and correction to adaptive RT Adaptive RT and dose accumulation Hans de Boer Move away from Single pre-treatment scan Single treatment plan Treatment corrections by couch shifts
Radiotherapy physics & Equipments
 Radiotherapy physics & Equipments RAD 481 Lecture s Title: An Overview of Radiation Therapy for Health Care Professionals Dr. Mohammed Emam Vision :IMC aspires to be a leader in applied medical sciences,
Radiotherapy physics & Equipments RAD 481 Lecture s Title: An Overview of Radiation Therapy for Health Care Professionals Dr. Mohammed Emam Vision :IMC aspires to be a leader in applied medical sciences,
11/10/2015. Prostate cancer in the U.S. Multi-parametric MRI of Prostate Diagnosis and Treatment Planning. NIH estimates for 2015.
 Multi-parametric MRI of Prostate Diagnosis and Treatment Planning Temel Tirkes, M.D. Associate Professor of Radiology Director, Genitourinary Radiology Indiana University School of Medicine Department
Multi-parametric MRI of Prostate Diagnosis and Treatment Planning Temel Tirkes, M.D. Associate Professor of Radiology Director, Genitourinary Radiology Indiana University School of Medicine Department
Prostate Fossa Contouring Guide. Jill Gunther, MD Modified by the econtour Team
 Prostate Fossa Contouring Guide Jill Gunther, MD Modified by the econtour Team You want to contour: Post-op Prostate What now? Find your references RTOG Prostate Fossa Contouring Atlas hdps://www.rtog.org/corelab/contouringatlases/
Prostate Fossa Contouring Guide Jill Gunther, MD Modified by the econtour Team You want to contour: Post-op Prostate What now? Find your references RTOG Prostate Fossa Contouring Atlas hdps://www.rtog.org/corelab/contouringatlases/
SASCRO Prostate Brachytherapy Guidelines Task Group
 SASCRO Prostate Brachytherapy Guidelines Task Group Anderson D 1, N Coetzee 2,Du Toit PD 3, Webb G 4 1Radiation Oncologist, Groote Schuur Hospital. 2Medical Physicist, Equra Health 3Medical Physicist,
SASCRO Prostate Brachytherapy Guidelines Task Group Anderson D 1, N Coetzee 2,Du Toit PD 3, Webb G 4 1Radiation Oncologist, Groote Schuur Hospital. 2Medical Physicist, Equra Health 3Medical Physicist,
Dosimetric Analysis of 3DCRT or IMRT with Vaginal-cuff Brachytherapy (VCB) for Gynaecological Cancer
 for Gynaecological Cancer") Dosimetric Analysis of 3DCRT or IMRT with Vaginal-cuff Brachytherapy (VCB) for Gynaecological Cancer Tan Chek Wee 15 06 2016 National University Cancer Institute, Singapore Clinical Care Education Research
Dosimetric Analysis of 3DCRT or IMRT with Vaginal-cuff Brachytherapy (VCB) for Gynaecological Cancer Tan Chek Wee 15 06 2016 National University Cancer Institute, Singapore Clinical Care Education Research
Linac Based SBRT for Low-intermediate Risk Prostate Cancer in 5 Fractions: Preliminary Report of a Phase II Study with FFF Delivery
 Linac Based SBRT for Low-intermediate Risk Prostate Cancer in 5 Fractions: Preliminary Report of a Phase II Study with FFF Delivery FILIPPO ALONGI MD Radiation Oncology & Radiosurgery Istituto Clinico
Linac Based SBRT for Low-intermediate Risk Prostate Cancer in 5 Fractions: Preliminary Report of a Phase II Study with FFF Delivery FILIPPO ALONGI MD Radiation Oncology & Radiosurgery Istituto Clinico
Image based Brachytherapy- HDR applications in Gynecological Tumors
 Image based Brachytherapy- HDR applications in Gynecological Tumors Yakov Pipman, D. Sc. North Shore LIJ Health System Sites amenable to treatment with HDR Brachytherapy GYN Breast Prostate Head and Neck
Image based Brachytherapy- HDR applications in Gynecological Tumors Yakov Pipman, D. Sc. North Shore LIJ Health System Sites amenable to treatment with HDR Brachytherapy GYN Breast Prostate Head and Neck
OPTIMIZATION OF COLLIMATOR PARAMETERS TO REDUCE RECTAL DOSE IN INTENSITY-MODULATED PROSTATE TREATMENT PLANNING
 Medical Dosimetry, Vol. 30, No. 4, pp. 205-212, 2005 Copyright 2005 American Association of Medical Dosimetrists Printed in the USA. All rights reserved 0958-3947/05/$ see front matter doi:10.1016/j.meddos.2005.06.002
Medical Dosimetry, Vol. 30, No. 4, pp. 205-212, 2005 Copyright 2005 American Association of Medical Dosimetrists Printed in the USA. All rights reserved 0958-3947/05/$ see front matter doi:10.1016/j.meddos.2005.06.002
Role of Belly Board Device in the Age of Intensity Modulated Radiotherapy for Pelvic Irradiation
 Role of Belly Board Device in the Age of Intensity Modulated Radiotherapy for Pelvic Irradiation 2017 AAMD 42 nd Annual Meeting Neil C. Estabrook, MD 6 / 14 / 2017 7/5/2017 1 Conflicts of Interest None
Role of Belly Board Device in the Age of Intensity Modulated Radiotherapy for Pelvic Irradiation 2017 AAMD 42 nd Annual Meeting Neil C. Estabrook, MD 6 / 14 / 2017 7/5/2017 1 Conflicts of Interest None
First, how does radiation work?
 Hello, I am Prajnan Das, Faculty Member in the Department of Radiation Oncology at The University of Texas MD Anderson Cancer Center. We are going to talk today about some of the basic principles regarding
Hello, I am Prajnan Das, Faculty Member in the Department of Radiation Oncology at The University of Texas MD Anderson Cancer Center. We are going to talk today about some of the basic principles regarding
Varian Acuity BrachyTherapy Suite One Room Integrated Image-Guided Brachytherapy
 Varian Acuity BrachyTherapy Suite One Room Integrated Image-Guided Brachytherapy The Acuity BrachyTherapy Suite Integrating Imaging, Planning, and Treatment in a Single Room Each component draws on the
Varian Acuity BrachyTherapy Suite One Room Integrated Image-Guided Brachytherapy The Acuity BrachyTherapy Suite Integrating Imaging, Planning, and Treatment in a Single Room Each component draws on the
Patient Information. Prostate Tissue Ablation. High Intensity Focused Ultrasound for
 High Intensity Focused Ultrasound for Prostate Tissue Ablation Patient Information CAUTION: Federal law restricts this device to sell by or on the order of a physician CONTENT Introduction... 3 The prostate...
High Intensity Focused Ultrasound for Prostate Tissue Ablation Patient Information CAUTION: Federal law restricts this device to sell by or on the order of a physician CONTENT Introduction... 3 The prostate...
Prostate MRI. Overview. Introduction 2/20/2015. Prostate cancer is most frequently diagnosed noncutaneous cancer in males (25%)
") Prostate MRI John Bell, MD Introduction Prostate Cancer Screening Staging Anatomy Prostate MRI overview Functional MRI Multiparametric Approach Indications Example Cases Overview Introduction Prostate
Prostate MRI John Bell, MD Introduction Prostate Cancer Screening Staging Anatomy Prostate MRI overview Functional MRI Multiparametric Approach Indications Example Cases Overview Introduction Prostate
Herlev radiation oncology team explains what MRI can bring
 Publication for the Philips MRI Community Issue 46 2012/2 Herlev radiation oncology team explains what MRI can bring The radiotherapy unit at Herlev University Hospital investigates use of MRI for radiotherapy
Publication for the Philips MRI Community Issue 46 2012/2 Herlev radiation oncology team explains what MRI can bring The radiotherapy unit at Herlev University Hospital investigates use of MRI for radiotherapy
A PRACTICAL METHOD TO ACHIEVE PROSTATE GLAND IMMOBILIZATION AND TARGET VERIFICATION FOR DAILY TREATMENT
 PII S0360-3016(01)02663-3 Int. J. Radiation Oncology Biol. Phys., Vol. 51, No. 5, pp. 1431 1436, 2001 Copyright 2001 Elsevier Science Inc. Printed in the USA. All rights reserved 0360-3016/01/$ see front
PII S0360-3016(01)02663-3 Int. J. Radiation Oncology Biol. Phys., Vol. 51, No. 5, pp. 1431 1436, 2001 Copyright 2001 Elsevier Science Inc. Printed in the USA. All rights reserved 0360-3016/01/$ see front
ART for Cervical Cancer: Dosimetry and Technical Aspects
 ART for Cervical Cancer: Dosimetry and Technical Aspects D.A. Jaffray, Ph.D. Radiation Therapy Physics Princess Margaret Cancer Centre/Techna/Ontario Cancer Institute Professor Departments of Radiation
ART for Cervical Cancer: Dosimetry and Technical Aspects D.A. Jaffray, Ph.D. Radiation Therapy Physics Princess Margaret Cancer Centre/Techna/Ontario Cancer Institute Professor Departments of Radiation
THE TRANSITION FROM 2D TO 3D AND TO IMRT - RATIONALE AND CRITICAL ELEMENTS
 THE TRANSITION FROM 2D TO 3D AND TO IMRT - RATIONALE AND CRITICAL ELEMENTS ICTP SCHOOL ON MEDICAL PHYSICS FOR RADIATION THERAPY DOSIMETRY AND TREATMENT PLANNING FOR BASIC AND ADVANCED APPLICATIONS March
THE TRANSITION FROM 2D TO 3D AND TO IMRT - RATIONALE AND CRITICAL ELEMENTS ICTP SCHOOL ON MEDICAL PHYSICS FOR RADIATION THERAPY DOSIMETRY AND TREATMENT PLANNING FOR BASIC AND ADVANCED APPLICATIONS March
BRACHYTHERAPY IN HORSES
 Vet Times The website for the veterinary profession https://www.vettimes.co.uk BRACHYTHERAPY IN HORSES Author : DAVID DONALDSON Categories : Vets Date : June 16, 2014 DAVID DONALDSON BVSc(Hons), DipECVO,
Vet Times The website for the veterinary profession https://www.vettimes.co.uk BRACHYTHERAPY IN HORSES Author : DAVID DONALDSON Categories : Vets Date : June 16, 2014 DAVID DONALDSON BVSc(Hons), DipECVO,
REVISITING ICRU VOLUME DEFINITIONS. Eduardo Rosenblatt Vienna, Austria
 REVISITING ICRU VOLUME DEFINITIONS Eduardo Rosenblatt Vienna, Austria Objective: To introduce target volumes and organ at risk concepts as defined by ICRU. 3D-CRT is the standard There was a need for a
REVISITING ICRU VOLUME DEFINITIONS Eduardo Rosenblatt Vienna, Austria Objective: To introduce target volumes and organ at risk concepts as defined by ICRU. 3D-CRT is the standard There was a need for a
ICRU Report 91 Was ist neu, was ändert sich?
 DEGRO Stereotaxie Meeting 21.10.2017 ICRU Report 91 Was ist neu, was ändert sich? Lotte Wilke, Stephanie Tanadini-Lang, Matthias Guckenberger Klinik für Radio-Onkologie, Universitätsspital Zürich History
DEGRO Stereotaxie Meeting 21.10.2017 ICRU Report 91 Was ist neu, was ändert sich? Lotte Wilke, Stephanie Tanadini-Lang, Matthias Guckenberger Klinik für Radio-Onkologie, Universitätsspital Zürich History
CBCT of the patient in the treatment position has gained wider applications for setup verification during radiotherapy.
 Gülcihan CÖDEL Introduction The aim of this study is to evaluate the changes in bladder doses during the volumetric modulated arc therapy (VMAT) treatment of prostate cancer patients using weekly cone
Gülcihan CÖDEL Introduction The aim of this study is to evaluate the changes in bladder doses during the volumetric modulated arc therapy (VMAT) treatment of prostate cancer patients using weekly cone