Partial Nephrectomy Planning: Everybody s s doing it, you can to
|
|
|
- Nicholas Owen
- 5 years ago
- Views:
Transcription


1 Partial Nephrectomy Planning: Everybody s s doing it, you can to Brian R. Herts, MD Associate Professor of Radiology Head, Abdominal Imaging, Imaging Institute & Staff, The Glickman Urological and Kidney Inst. Cleveland Clinic
2 Objectives Review the current recommendations for treating small renal tumors and the indications for partial nephrectomy Review the surgical planning needs for nephron sparing surgery Learn imaging techniques and tips to provide surgical planning information Nephron sparing surgery includes Open and laparoscopic partial nephrectomy Laparoscopic and percutaneous ablation techniques
3 RCC Facts 3% of all visceral malignancies Risk factors - smoking, obesity ,000 new cases 4% bilateral 13,000 deaths/yr 33% present with locally advanced or metastatic disease 10-yr survival rate (2000) T1-91%, T2-70% T3a - 53% T3b,c % 43%
4 RCC treatment Treatment Surgery remains best curative treatment option Medical therapies and radiation therapy poor IFN-α,, IL2, vaccines all have had limited success Response rates < 30% Recent advances Surgical options have expanded - NSS, cryoablation,, RF Cellular receptor targeted therapy for metastatic disease VEG-F F & PDGF-α inhibitors showing promise Sutent (sunitinib malate) ) & Sorafenib
5 Trend towards MIS and NSS (Part 1: Everybody s s doing it ) More institutions and more Urologists are performing open and laparoscopic NSS More radiologists performing percutaneous NSS Washington University study showed an increase in NSS - 33/yr to 91/yr Laparoscopic pnx went from 3% to 56% of all pnx Bhayani et al, Urology 2006;68:732


6 CC Urologic Surgical Procedures Cleveland Clinic Glickman Urological Institute data NSS procedures more than doubled in an 8-year 8 period Laparoscopic procedures have had the biggest growth
7 Revised Staging Criteria 1997 / 2003 Tumor (T) T1 7 cm,, confined to the kidney (previously 2.5 cm) T1a 4 cm T1b > 4 cm T2 > 7 cm,, confined to the kidney T3 - Venous invasion, adrenal or perinephric fat T3a - adrenal gland, w/i Gerota s fascia T3b - renal vein / vena cava below diaphragm T3c - vena cava or wall above diaphragm (former T4b) T4 - Beyond Gerota s fascia (no a or b) Note: changes in 1997 highlighted in yellow
8 Renal central sinus invasion and urothelial invasion Occurs in less than 10% of patients but Invasion of the central sinus fat may have significant prognostic indications similar to extension outside the renal capsule Patients with T2 tumors with urothelial invasion did worse than those without urothelial invasion suggested as an added criterion for staging Patients with central tumors more likely to need collecting system repair at surgery
9 Imperative indications for NSS for Renal Neoplasms Bilateral renal tumors (approx 4% at diagnosis) Solitary kidney (prior Nx, renal agenesis) Functionally solitary kidney chronic obstruction, infection, renal vascular disease Underlying disease predisposing to CKD Calculus, infection, diabetes mellitus, SLE, HTN Why? - avoid dialysis whenever possible.
10 Treatment recommendations for ct1 tumors Open partial nephrectomy is considered the standard of care by the AUA for clinical T1 renal mass - particularly if renal function is compromised or potentially compromised regardless of the presence of a normal contralateral kidney Despite dissemination of pnx techniques, radical nephrectomy remains over utilized. Estimated that less than 50% of T1 tumors are treated by partial nephrectomy therefore the number of partial nephrectomies for small renal tumors will be increasing
11 Why nephron sparing surgery? #1 - Success with imperative indications #2 - Increase in incidentally detected renal masses #3 - More benign tumors are resected as smaller tumors discovered and treated #4 - Better outcomes for patients, particularly with better long-term renal function
12 Reason #1 - Good treatment success First and foremost this is a cancer operation No. of patients in study* Recurrence rate Local tumor survival % 90% % 89% % 93% % 2.7% 92% 93% *Table adapted from Novick AC. Ann Rev Med 2002
13 Reason #2 - the incidental renal mass Approximately 60-65% 65% of RCC are incidentally detected Classic triad of fever, flank pain, hematuria is rare Abdominal imaging trends (all modalities) per 1000 Medicare patients per 1000 Medicare patients 25% increase CT/CTA: +141% increase 99.4 to 239.3/1000 MR/MRA: +365% increase 2 to 9.3/1000
14 Reason #2 - the incidental renal mass More incidental renal masses are low stage 64% - 78% incidental RCC are stage T1 or T2 36% - 57% symptomatic RCC are stage T1 or T2 Incidental tumors are smaller 5.9 cm v cm Smaller tumors are less aggressive (Remzi et al J Urol 2006) 4/168 (2.4%) of 3 cm or less v. 10/119 (8.4%) of cm with distant metastases therefore they are more suitable for NSS!
15 Reason #3 - Benign Findings at Surgery Frank et al J Urol tumors in 2770 adults all specimens < 1.0 cm cm cm cm cm cm cm % benign 46.3% 22.4% 22.0% 19.9% 9.9% 13% 4.5% % malignant 53.8% 77.7% 78.0% 80.1% 90.1% 87.0% 95.5% Kutikov et al Urol tumors in 143 adults with suspected RCC < 2.0 cm cm > 4.0 cm % benign 15.9% 16.5% 14.3% % malignant 84.1% 83.5% 85.7%
16 Reason #4 - Outcomes Radical versus partial nephrectomy 50% more Rad Nx pts with proteinuria (55% v. 34.5%) Nearly 2x as many Rad NX pts with CKD (22.4% v. 11.6%) 3-yr probability of CKD 65% after RNx v. 20% after PNx Survival in patients with pt1a tumors Radical Nx (290) versus partial Nx (358) Higher relative risk of death w/ Rad Nx (age < 65)



17 Complications Hemorrhage Renal infarction / loss Urinary leak or fistula Abscess Rates Lap PNx - 9% Open PNx - 6.3% RFA - 6% Lap RNx - 3.4% Open RNx - 1.3% Planning for NSS (Part 2: You can do it to )
18 Planning info for NSS - avoid complications! Renal arterial and venous anatomy Vena Cava variants Kidney position Tumor location and depth Collecting system involvement Number, course of ureter(s)
19 1) Unenhanced Three-phase MDCT scan 20 cc timing bolus (scan q1 sec from s) or contrast preload wait 2 minutes to opacify the collecting system 2) Vascular or corticomedullary phase Timing bolus or automated tracking (abd( aorta trigger) Add + 5 seconds or auto-tracking tracking Aim for both arterial and venous enhancement 3) Nephrographic or parenchymal phase 120 seconds from start of contrast injection Earlier for younger patients, later for older, fast scans Ensures nephrographic phase








20 Three-phase renal CT 16 slice / detector MDCT & up 0.6, or 0.75 mm slice collimation 3-55 mm slice thickness / 3 mm interval for diagnostic interpretation 1 mm slice thickness x 0.8 mm for MPR, VR reconstructions Obese patients Use thicker collimator - 1.2, 1.25, 1.5 We use dose modulation algorithms (both x-y and z directions) NC CMP NP

21 MR protocols Coils 1.5 T & 3T phased array body coils Pre contrast Axial T1 in/out mm slices. Axial & Coronal HASTE - No fat sat - 5-6mm slices Axial VIBE 1.5 mm effective slice thickness Coronal 3D FLASH - Try to get effective thickness 2mm
 Timing Run - axial thru kidneys contrast")


22 Post contrast MR protocols (cont.) Timing Run - axial thru kidneys contrast at 2cc/sec followed by 20 cc saline at 2cc/sec Standard timing formula TP + inject-time/2 time/2 time-to to-center Coronal 3D FLASH Axial & coronal VIBEs 0, 30, 60, 90, 180 secs Subtraction



23 MIPs and MPRs Image creation Coronal oblique MIPs of arterial system aorta MPRs oblique coronal and sagittal MPRs long axis of the kidney



24 Volume rendering Image creation Opacity settings to preference Mine approx 50% Or use presets



25 Tumor position Four renal segments, based on vascular territories anterior apical posterior basilar
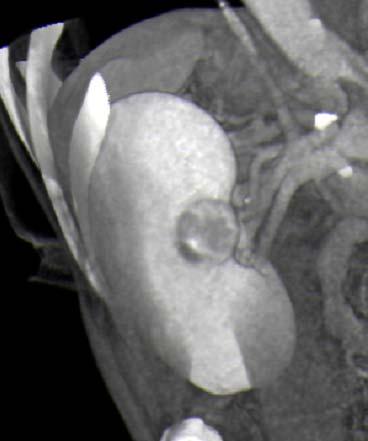
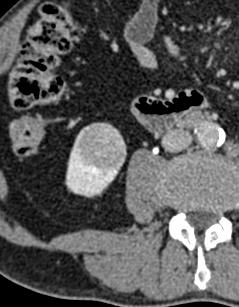
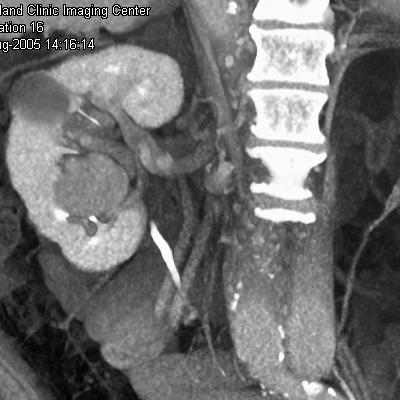
26 Tumor depth of extension - terminology Central extends into the central sinus fat or abuts the central sinus Higher likelihood of collecting system entry Peripheral no central extension Surgically simpler Exophytic identifiable on surface Intrarenal may require IOUS



27 Anterior, central, exophytic axial MPR VR
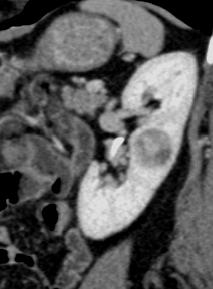

28 Posterior, central, exophytic



29 Apical, peripheral, exophytic


30 Basilar, exophytic, central

31 Central, intrarenal


32 Tumor position



33 Arterial anatomy


34 Venous anatomy Retroaortic left renal vein Circumaortic left renal vein

35 Billing 2007 reimbursement rates (from the web)

36 What s s next? Segmentation and tumor volume Studies looking at relationship of tumor and renal parenchymal volume to NSS and outcome Segmentation results from software Volume Mean density & std. dev. Recist diameters
37 Summary Open pnx is now recommended treatment for small renal mass More Urologists will be doing more NSS for SRM Least experienced will need the most operative guidance! Images to provide Arterial / Venous anatomy Number, location, branching Anomalies Tumor Location anterior/posterior/apical/basilar Location - exophytic / depth / involvement of calices Ureter(s) Bill as 3D when requested by the surgeon
38 References Remzi M, et al. J Urol 2006;176: Frank I, et al. J Urol 2003;170: Kutikov A, et al Urol 2006;68: Bhayani et al. Urology 2006;68:732 Novick AC. Ann Rev Med 2002;53: Levin DC et al, J Am Coll Radiol 2008;5: Lau et al, Mayo Clinic Proceedings, 2000;75: Thompson et al J Urol 2008;179:
GUIDELINES ON RENAL CELL CARCINOMA
 GUIDELINES ON RENAL CELL CARCINOMA B. Ljungberg (chairman), D.C. Hanbury, M.A. Kuczyk, A.S. Merseburger, P.F.A. Mulders, J-J. Patard, I.C. Sinescu Introduction This EAU guideline was prepared to help urologists
GUIDELINES ON RENAL CELL CARCINOMA B. Ljungberg (chairman), D.C. Hanbury, M.A. Kuczyk, A.S. Merseburger, P.F.A. Mulders, J-J. Patard, I.C. Sinescu Introduction This EAU guideline was prepared to help urologists
Guidelines on Renal Cell
 Guidelines on Renal Cell Carcinoma (Text update March 2009) B. Ljungberg (Chairman), D.C. Hanbury, M.A. Kuczyk, A.S. Merseburger, P.F.A. Mulders, J-J. Patard, I.C. Sinescu Introduction Renal cell carcinoma
Guidelines on Renal Cell Carcinoma (Text update March 2009) B. Ljungberg (Chairman), D.C. Hanbury, M.A. Kuczyk, A.S. Merseburger, P.F.A. Mulders, J-J. Patard, I.C. Sinescu Introduction Renal cell carcinoma
Guidelines for the Management of Renal Cancer West Midlands Expert Advisory Group for Urological Cancer
 Guidelines for the Management of Renal Cancer West Midlands Expert Advisory Group for Urological Cancer West Midlands Clinical Networks and Clinical Senate Coversheet for Network Expert Advisory Group
Guidelines for the Management of Renal Cancer West Midlands Expert Advisory Group for Urological Cancer West Midlands Clinical Networks and Clinical Senate Coversheet for Network Expert Advisory Group
Recommendations for cross-sectional imaging in cancer management, Second edition
 www.rcr.ac.uk Recommendations for cross-sectional imaging in cancer management, Second edition Renal and adrenal tumours Faculty of Clinical Radiology www.rcr.ac.uk Contents Renal cell carcinoma 3 Clinical
www.rcr.ac.uk Recommendations for cross-sectional imaging in cancer management, Second edition Renal and adrenal tumours Faculty of Clinical Radiology www.rcr.ac.uk Contents Renal cell carcinoma 3 Clinical
GUIDELINES ON RENAL CELL CANCER
 20 G. Mickisch (chairman), J. Carballido, S. Hellsten, H. Schulze, H. Mensink Eur Urol 2001;40(3):252-255 Introduction is characterised by a constant rise in incidence over the last 50 years, with a predominance
20 G. Mickisch (chairman), J. Carballido, S. Hellsten, H. Schulze, H. Mensink Eur Urol 2001;40(3):252-255 Introduction is characterised by a constant rise in incidence over the last 50 years, with a predominance
Patient Selection for Ablative Therapies. Adrian D Joyce Leeds UK
 Patient Selection for Ablative Adrian D Joyce Leeds UK Therapy Renal Cell Ca USA: 30,000 new cases annually >12,000 deaths RCC accounts for 3% of all adult malignancy 40% of patients will die from their
Patient Selection for Ablative Adrian D Joyce Leeds UK Therapy Renal Cell Ca USA: 30,000 new cases annually >12,000 deaths RCC accounts for 3% of all adult malignancy 40% of patients will die from their
Partial Nephrectomy Techniques for Renal Preservation: Historical and Modern Approaches
 Partial Nephrectomy Techniques for Renal Preservation: Historical and Modern Approaches Cary N Robertson MD FACS Associate Professor Division of Urology Associate Director Urologic Oncology Duke Cancer
Partial Nephrectomy Techniques for Renal Preservation: Historical and Modern Approaches Cary N Robertson MD FACS Associate Professor Division of Urology Associate Director Urologic Oncology Duke Cancer
Manchester Cancer. Guidelines for the management of renal cancer
 Guidelines for the management of renal cancer Approved by the urology pathway board September 2014 To be reviewed September 2016 Renal Cancer Guidelines 1. Introduction 1.1 Kidney cancer accounts for 3%
Guidelines for the management of renal cancer Approved by the urology pathway board September 2014 To be reviewed September 2016 Renal Cancer Guidelines 1. Introduction 1.1 Kidney cancer accounts for 3%
1/25/13 Right partial nephrectomy followed by completion right radical nephrectomy.
 History and Physical Case Scenario 1 45 year old white male presents with complaints of nausea, weight loss, and back pain. A CT of the chest, abdomen and pelvis was done on 12/8/12 that revealed a 12
History and Physical Case Scenario 1 45 year old white male presents with complaints of nausea, weight loss, and back pain. A CT of the chest, abdomen and pelvis was done on 12/8/12 that revealed a 12
WHAT IS THE ROLE OF ACTIVE SURVEILLANCE
 WHAT IS THE ROLE OF ACTIVE SURVEILLANCE IN THE CONTEXT OF RENAL ABLATION AND PARTIAL NEPHRECTOMY? Alessandro Volpe University of Eastern Piedmont Novara, Italy RCC INCIDENCE SEER DATABASE (1975-2006) RCC
WHAT IS THE ROLE OF ACTIVE SURVEILLANCE IN THE CONTEXT OF RENAL ABLATION AND PARTIAL NEPHRECTOMY? Alessandro Volpe University of Eastern Piedmont Novara, Italy RCC INCIDENCE SEER DATABASE (1975-2006) RCC
St. Dominic s Annual Cancer Report Outcomes
 St. Dominic s 2017 Annual Cancer Report Outcomes Cancer Program Practice Profile Reports (CP3R) St. Dominic s Cancer Committee monitors and ensures that patients treated at St. Dominic Hospital receive
St. Dominic s 2017 Annual Cancer Report Outcomes Cancer Program Practice Profile Reports (CP3R) St. Dominic s Cancer Committee monitors and ensures that patients treated at St. Dominic Hospital receive
The new TNM staging for renal cell carcinoma: what and why the urologists want to know.
 The new TNM staging for renal cell carcinoma: what and why the urologists want to know. Poster No.: C-1132 Congress: ECR 2011 Type: Educational Exhibit Authors: Y. Y. Lim, A. Hattab, A. Bradley ; Manchester/UK,
The new TNM staging for renal cell carcinoma: what and why the urologists want to know. Poster No.: C-1132 Congress: ECR 2011 Type: Educational Exhibit Authors: Y. Y. Lim, A. Hattab, A. Bradley ; Manchester/UK,
Kidney Case 1 SURGICAL PATHOLOGY REPORT
 Kidney Case 1 Surgical Pathology Report February 9, 2007 Clinical History: This 45 year old woman was found to have a left renal mass. CT urography with reconstruction revealed a 2 cm medial mass which
Kidney Case 1 Surgical Pathology Report February 9, 2007 Clinical History: This 45 year old woman was found to have a left renal mass. CT urography with reconstruction revealed a 2 cm medial mass which
Renal vascular evaluation with 64 Multislice Computerized Tomography Daniela Stoisa, Fabrizzio E. Galiano, Andrés Quaranta, Roberto L.
 Renal vascular evaluation with 64 Multislice Computerized Tomography Daniela Stoisa, Fabrizzio E. Galiano, Andrés Quaranta, Roberto L. Villavicencio Footnote Diagnóstico Médico Oroño. Bv. Oroño 1515. 2000.
Renal vascular evaluation with 64 Multislice Computerized Tomography Daniela Stoisa, Fabrizzio E. Galiano, Andrés Quaranta, Roberto L. Villavicencio Footnote Diagnóstico Médico Oroño. Bv. Oroño 1515. 2000.
Who are Candidates for Laparoscopic or Open Radical Nephrectomy. Arieh Shalhav
 Who are Candidates for Laparoscopic or Open Radical Nephrectomy Arieh Shalhav Fritz Duda Chair of Urologic Surgery Professor of Surgery and the Comprehensive Cancer Research Center Who are Candidates for
Who are Candidates for Laparoscopic or Open Radical Nephrectomy Arieh Shalhav Fritz Duda Chair of Urologic Surgery Professor of Surgery and the Comprehensive Cancer Research Center Who are Candidates for
Sex: 女 Age: 51 Occupation: 無 Admission date:92/07/22
 Sex: 女 Age: 51 Occupation: 無 Admission date:92/07/22 Chief complaint Unknown fever for one month Hand tremor and left huge renal tumor was noted Present illness Suffered from fever for one month, hand
Sex: 女 Age: 51 Occupation: 無 Admission date:92/07/22 Chief complaint Unknown fever for one month Hand tremor and left huge renal tumor was noted Present illness Suffered from fever for one month, hand
Customizing Contrast Injection for Body MDCT: Algorithmic Approach
 Customizing Contrast Injection for Body MDCT: Algorithmic Approach Lincoln L. Berland, M.D., F.A.C.R. University of Alabama at Birmingham Before Contrast Prep and Hydration Hydration single most important
Customizing Contrast Injection for Body MDCT: Algorithmic Approach Lincoln L. Berland, M.D., F.A.C.R. University of Alabama at Birmingham Before Contrast Prep and Hydration Hydration single most important
AUA Guidelines Renal Mass and Localized Kidney Cancer
 AUA Guidelines Renal Mass and Localized Kidney Cancer Steven C. Campbell, MD, PhD Chair AUA Guidelines Panel Professor Surgery, Vice Chair, Program Director Department of Urology Glickman Urological and
AUA Guidelines Renal Mass and Localized Kidney Cancer Steven C. Campbell, MD, PhD Chair AUA Guidelines Panel Professor Surgery, Vice Chair, Program Director Department of Urology Glickman Urological and
Vincenzo Ficarra 1,2,3. Associate Editor BJU International
 Partial Nephrectomy for RCC Vincenzo Ficarra 1,2,3 1 Director Department of Urology University of Udine, Italy 2 Associate Editor BJU International 3 Scientific Director OLV Robotic Surgery Institute,
Partial Nephrectomy for RCC Vincenzo Ficarra 1,2,3 1 Director Department of Urology University of Udine, Italy 2 Associate Editor BJU International 3 Scientific Director OLV Robotic Surgery Institute,
Presentation of Cases /Audience Voting/Panel/Discussion
 Presentation of Cases /Audience Voting/Panel/Discussion JJ Patard Tim O Brien Ninth European International Kidney Cancer Symposium Dublin 25-26 April 2014 Clinical case 1 63 years old women Medical past
Presentation of Cases /Audience Voting/Panel/Discussion JJ Patard Tim O Brien Ninth European International Kidney Cancer Symposium Dublin 25-26 April 2014 Clinical case 1 63 years old women Medical past
Renal Parenchymal Neoplasms
 Renal Parenchymal Neoplasms د. BENIGN TUMORS : Benign renal tumors include adenoma, oncocytoma, angiomyolipoma, leiomyoma, lipoma, hemangioma, and juxtaglomerular tumors. Renal Adenomas : The adenoma is
Renal Parenchymal Neoplasms د. BENIGN TUMORS : Benign renal tumors include adenoma, oncocytoma, angiomyolipoma, leiomyoma, lipoma, hemangioma, and juxtaglomerular tumors. Renal Adenomas : The adenoma is
CT Renal 3 Phase + Pelvis CT Abdomen Pelvis WO W - NC.A.V, Pelvis during V
 CT Renal 3 Phase + Pelvis CT Abdomen Pelvis WO W - NC.A.V, Pelvis during V Reviewed By: Anna Ellermeier, MD; Brett Mollard, MD Last Reviewed: August 2018 Contact: (866) 761-4200, Option 1 In accordance
CT Renal 3 Phase + Pelvis CT Abdomen Pelvis WO W - NC.A.V, Pelvis during V Reviewed By: Anna Ellermeier, MD; Brett Mollard, MD Last Reviewed: August 2018 Contact: (866) 761-4200, Option 1 In accordance
Optimal Treatment of ct1b Renal Mass in Patient with Normal GFR: a Role for Radical Nephrectomy?
 Optimal Treatment of ct1b Renal Mass in Patient with Normal GFR: a Role for Radical Nephrectomy? Steven C. Campbell, MD, PhD Program Director, Vice Chairman Department of Urology Center for Urologic Oncology
Optimal Treatment of ct1b Renal Mass in Patient with Normal GFR: a Role for Radical Nephrectomy? Steven C. Campbell, MD, PhD Program Director, Vice Chairman Department of Urology Center for Urologic Oncology
The Surgical Management of RCC
 The Surgical Management of RCC From Robson to Radiofrequency Ablation Tony Finelli, MD, MSc, FRCSC University Health Network University of Toronto Background Renal cell carcinoma (RCC) is 9 th most common
The Surgical Management of RCC From Robson to Radiofrequency Ablation Tony Finelli, MD, MSc, FRCSC University Health Network University of Toronto Background Renal cell carcinoma (RCC) is 9 th most common
PICTORIAL ESSAY. Experiences of using a single post-contrast CT scan of the urinary tract after triphasic contrast injection
 Experiences of using a single post-contrast CT scan of the urinary tract after triphasic contrast injection P C Pretorius, FCRad (Diag) SA Drs Visser, Erasmus, Vawda & Partners, Port Elizabeth Corresponding
Experiences of using a single post-contrast CT scan of the urinary tract after triphasic contrast injection P C Pretorius, FCRad (Diag) SA Drs Visser, Erasmus, Vawda & Partners, Port Elizabeth Corresponding
Indications For Partial
 Indications For Partial Nephrectomy Christopher G. Wood, M. D., FACS Professor and Deputy Chairman Douglas E. Johnson, M. D. Endowed Professorship in Urology Department of Urology The University of Texas
Indications For Partial Nephrectomy Christopher G. Wood, M. D., FACS Professor and Deputy Chairman Douglas E. Johnson, M. D. Endowed Professorship in Urology Department of Urology The University of Texas
Renal cell carcinoma (RCC)
") Renal cell carcinoma (RCC) Introduction The most common solid renal tumor. Accounts for 2 3% of all adult malignancies. It is the 3 rd most common urological tumor in men and the 2 nd in women. It is th
Renal cell carcinoma (RCC) Introduction The most common solid renal tumor. Accounts for 2 3% of all adult malignancies. It is the 3 rd most common urological tumor in men and the 2 nd in women. It is th
Ureteropelvic Junction Obstruction (UPJO) syndrome: imaging with Multidetector CT (MDCT) prior to minimally invasive treatment
 syndrome: imaging with Multidetector CT (MDCT) prior to minimally invasive treatment") Ureteropelvic Junction Obstruction (UPJO) syndrome: imaging with Multidetector CT (MDCT) prior to minimally invasive treatment Poster No.: C-1753 Congress: ECR 2011 Type: Scientific Exhibit Authors: E.
Ureteropelvic Junction Obstruction (UPJO) syndrome: imaging with Multidetector CT (MDCT) prior to minimally invasive treatment Poster No.: C-1753 Congress: ECR 2011 Type: Scientific Exhibit Authors: E.
Naif H. Alsaikhan, MD Noushin Vahdat, MD. University of California in San Diego VA San Diego Healthcare System
 Naif H. Alsaikhan, MD Noushin Vahdat, MD University of California in San Diego VA San Diego Healthcare System Goals Describe the morphologic parameters that urologists and interventional radiologists need
Naif H. Alsaikhan, MD Noushin Vahdat, MD University of California in San Diego VA San Diego Healthcare System Goals Describe the morphologic parameters that urologists and interventional radiologists need
The Incidental Renal Mass in the Primary Care Setting
 The Incidental Renal Mass in the Primary Care Setting Adele M. Caruso, MSN, CRNP Adult Nurse Practitioner The Perelman School of Medicine at the University of Pennsylvania Abstract There are approximately
The Incidental Renal Mass in the Primary Care Setting Adele M. Caruso, MSN, CRNP Adult Nurse Practitioner The Perelman School of Medicine at the University of Pennsylvania Abstract There are approximately
CT Urography. Bladder. Stuart G. Silverman, M.D.
 CT Urography Stuart G. Silverman, M.D. Professor of Radiology Harvard Medical School Director, Abdominal Imaging and Intervention Brigham and Women s Hospital Bladder Boston, MA CT Urography Stuart G.
CT Urography Stuart G. Silverman, M.D. Professor of Radiology Harvard Medical School Director, Abdominal Imaging and Intervention Brigham and Women s Hospital Bladder Boston, MA CT Urography Stuart G.
What is the role of partial nephrectomy in the context of active surveillance and renal ablation?
 What is the role of partial nephrectomy in the context of active surveillance and renal ablation? Dogu Teber Department of Urology University Hospital Heidelberg Coming from Heidelberg obligates to speak
What is the role of partial nephrectomy in the context of active surveillance and renal ablation? Dogu Teber Department of Urology University Hospital Heidelberg Coming from Heidelberg obligates to speak
UICC TNM 8 th Edition Errata
 UICC TNM 8 th Edition Errata ions are in italics Page 28 Oropharynx p16 positive Pathological Stage II,T2 N2 M0 T3 N0,N1 M0 Stage II,T2 N2 M0 T3,T4 N0,N1 M0 Page 61 Oesophagus Adenocarcinoma Pathological
UICC TNM 8 th Edition Errata ions are in italics Page 28 Oropharynx p16 positive Pathological Stage II,T2 N2 M0 T3 N0,N1 M0 Stage II,T2 N2 M0 T3,T4 N0,N1 M0 Page 61 Oesophagus Adenocarcinoma Pathological
EVALUATION OF THE OUTCOME OF THE MANAGEMENT OF PATIENTS WITH RENAL CELL CARCINOMA
 International Invention Journal of Medicine and Medical Sciences (ISSN: 2408-7246) Vol. (9) pp. 99-204, November, 206 Available online http://internationalinventjournals.org/journals/iijmms Copyright 206
International Invention Journal of Medicine and Medical Sciences (ISSN: 2408-7246) Vol. (9) pp. 99-204, November, 206 Available online http://internationalinventjournals.org/journals/iijmms Copyright 206
RCC in ADPKD / CKD / ESRD
 RCC in ADPKD / CKD / ESRD FOIU 2018 David A. Goldfarb, MD,FACS Professor of Surgery, Cleveland Clinic Lerner College of Medicine Glickman Urological and Kidney Institute Cleveland Clinic, Cleveland, Ohio
RCC in ADPKD / CKD / ESRD FOIU 2018 David A. Goldfarb, MD,FACS Professor of Surgery, Cleveland Clinic Lerner College of Medicine Glickman Urological and Kidney Institute Cleveland Clinic, Cleveland, Ohio
RENAL Nephrometry Scoring System: The Radiologist s Perspective
 Genitourinary Imaging Clinical Perspective Parsons et al. Nephrometry Score Genitourinary Imaging Clinical Perspective Rosaleen B. Parsons 1 Daniel Canter 2 Alexander Kutikov 3 Robert G. Uzzo 3 Parsons
Genitourinary Imaging Clinical Perspective Parsons et al. Nephrometry Score Genitourinary Imaging Clinical Perspective Rosaleen B. Parsons 1 Daniel Canter 2 Alexander Kutikov 3 Robert G. Uzzo 3 Parsons
Challenges in RCC surgery. Treatment Goals. Surgical challenges. Management options in VHL associated RCCs
 Management options in VHL associated RCCs Challenges in RCC surgery JJ PATARD, MD, PhD Paris XI University Observation, Radical nephrectomy, Renal parenchymal sparing surgery, Open, laparoscopic, robotic
Management options in VHL associated RCCs Challenges in RCC surgery JJ PATARD, MD, PhD Paris XI University Observation, Radical nephrectomy, Renal parenchymal sparing surgery, Open, laparoscopic, robotic
UICC TNM 8 th Edition Errata
 UICC TNM 8 th Edition Errata ions are in italics Head and Neck Tumours Pages 20, p27, p34, p38, p41, and p49 ly pn2a Metastasis in a single ipsilateral lymph node, less than 3cm in greatest dimension with
UICC TNM 8 th Edition Errata ions are in italics Head and Neck Tumours Pages 20, p27, p34, p38, p41, and p49 ly pn2a Metastasis in a single ipsilateral lymph node, less than 3cm in greatest dimension with
Male genital tract tumors. SiCA. Division of Urology, Department of Surgery, Faculty of Medicine Siriraj Hospital.
 Male genital tract tumors Division of Urology, Department of Surgery, Faculty of Medicine Siriraj Hospital. adenocarcinoma Prostate Cancer most common male cancer in western countries more detected in
Male genital tract tumors Division of Urology, Department of Surgery, Faculty of Medicine Siriraj Hospital. adenocarcinoma Prostate Cancer most common male cancer in western countries more detected in
CTA Chest Pulmonary Embolism & Routine CT Abdomen + Pelvis W CTA Chest W (arterial) & CT Abdomen + Pelvis W (venous)
 & CT Abdomen + Pelvis W (venous)") CTA Chest Pulmonary Embolism & Routine CT Abdomen + Pelvis W CTA Chest W (arterial) & CT Abdomen + Pelvis W (venous) Reviewed By: Anna Ellermeier, MD; Brett Mollard, MD Last Reviewed: August 2018 Contact:
CTA Chest Pulmonary Embolism & Routine CT Abdomen + Pelvis W CTA Chest W (arterial) & CT Abdomen + Pelvis W (venous) Reviewed By: Anna Ellermeier, MD; Brett Mollard, MD Last Reviewed: August 2018 Contact:
Role of imaging in evaluation of genitourinary i trauma Spectrum of GU injuries Relevance of imaging findings in determining management Focus on MDCT
 Genitourinary Tract Injuries 6 th Nordic Course Scott D. Steenburg, MD Assistant Professor University of Maryland Department of Radiology Division of Trauma and Emergency Radiology R Adams Cowley Shock
Genitourinary Tract Injuries 6 th Nordic Course Scott D. Steenburg, MD Assistant Professor University of Maryland Department of Radiology Division of Trauma and Emergency Radiology R Adams Cowley Shock
MRI Abdomen Protocol Pancreas/MRCP with Contrast
 MRI Abdomen Protocol Pancreas/MRCP with Contrast Reviewed By: Brett Mollard, MD; Anna Ellermeier, MD Last Reviewed: July 2018 Contact: (866) 761-4200 Standard uses: 1. Characterization of cystic and solid
MRI Abdomen Protocol Pancreas/MRCP with Contrast Reviewed By: Brett Mollard, MD; Anna Ellermeier, MD Last Reviewed: July 2018 Contact: (866) 761-4200 Standard uses: 1. Characterization of cystic and solid
Surgically Discovered Xanthogranulomatous Pyelonephritis Invading Inferior Vena Cava with Coexisting Renal Cell Carcinoma
 Case Study TheScientificWorldJOURNAL (2009) 9, 5 9 TSW Urology ISSN 1537-744X; DOI 10.1100/tsw.2009.6 Surgically Discovered Xanthogranulomatous Pyelonephritis Invading Inferior Vena Cava with Coexisting
Case Study TheScientificWorldJOURNAL (2009) 9, 5 9 TSW Urology ISSN 1537-744X; DOI 10.1100/tsw.2009.6 Surgically Discovered Xanthogranulomatous Pyelonephritis Invading Inferior Vena Cava with Coexisting
Small Renal Mass Guidelines. Clif Vestal, MD USMD Arlington, Texas
 Small Renal Mass Guidelines Clif Vestal, MD USMD Arlington, Texas Evaluation/Diagnosis 1. Obtain high quality, multiphase, cross-sectional abdominal imaging to optimally characterize/stage the renal mass.
Small Renal Mass Guidelines Clif Vestal, MD USMD Arlington, Texas Evaluation/Diagnosis 1. Obtain high quality, multiphase, cross-sectional abdominal imaging to optimally characterize/stage the renal mass.
RAPN. in T1b Renal Masses? A. Mottrie. G. Denaeyer, P. Schatteman, G. Novara
 RAPN in T1b Renal Masses? A. Mottrie G. Denaeyer, P. Schatteman, G. Novara Department of Urology O.L.V. Clinic Aalst OLV Vattikuti Robotic Surgery Institute Aalst Belgium Guidelines on Renal Cell Carcinoma
RAPN in T1b Renal Masses? A. Mottrie G. Denaeyer, P. Schatteman, G. Novara Department of Urology O.L.V. Clinic Aalst OLV Vattikuti Robotic Surgery Institute Aalst Belgium Guidelines on Renal Cell Carcinoma
Oncourology COMPLICATIONS OF PARTIAL NEPHRECTOMY AT OPERATIVE TREATMENT OF RENAL CELL CARCINOMA
 1 Oncourology COMPLICATIONS OF PARTIAL NEPHRECTOMY AT OPERATIVE TREATMENT OF RENAL CELL CARCINOMA Address: Eduard Oleksandrovych Stakhovsky, 03022, Kyiv, Lomonosova Str., 33/43, National Cancer Institute
1 Oncourology COMPLICATIONS OF PARTIAL NEPHRECTOMY AT OPERATIVE TREATMENT OF RENAL CELL CARCINOMA Address: Eduard Oleksandrovych Stakhovsky, 03022, Kyiv, Lomonosova Str., 33/43, National Cancer Institute
Vascular CT Protocols
 Vascular CT Protocols V 1D: Chest and abdominal CT angiogram (aortic dissection protocol) V 1T: Chest CT angiogram (aortic trauma protocol) V 2: Abdominal and pelvis CT angiogram (aortic aneurysm protocol)
Vascular CT Protocols V 1D: Chest and abdominal CT angiogram (aortic dissection protocol) V 1T: Chest CT angiogram (aortic trauma protocol) V 2: Abdominal and pelvis CT angiogram (aortic aneurysm protocol)
Patient Selection for Surgery in RCC with Thrombus. E. Jason Abel, M.D.
 Patient Selection for Surgery in RCC with Thrombus E. Jason Abel, M.D. RCC with venous invasion Venous invasion occurs in ~10% of RCC Surgery more complex Increased risk for morbidity Thrombus may be confined
Patient Selection for Surgery in RCC with Thrombus E. Jason Abel, M.D. RCC with venous invasion Venous invasion occurs in ~10% of RCC Surgery more complex Increased risk for morbidity Thrombus may be confined
KIDNEY HEALTH. Kidney Masses and Localized Kidney Tumors: A Patient Guide
 KIDNEY HEALTH Kidney Masses and Localized Kidney Tumors: A Patient Guide Table of Contents Kidney & Adrenal Health Committee Renal Mass Committee.... 2 Patient Story.... 3 Introduction: I have a kidney
KIDNEY HEALTH Kidney Masses and Localized Kidney Tumors: A Patient Guide Table of Contents Kidney & Adrenal Health Committee Renal Mass Committee.... 2 Patient Story.... 3 Introduction: I have a kidney
CT angiography techniques. Boot camp
 CT angiography techniques Boot camp Overview Basic concepts Contrast administration arterial opacification Time scan acquisition during the arterial phase Protocol examples Helical non-gated CTA Pulmonary
CT angiography techniques Boot camp Overview Basic concepts Contrast administration arterial opacification Time scan acquisition during the arterial phase Protocol examples Helical non-gated CTA Pulmonary
Surgical Management of Renal Cancer. David Nicol Consultant Urologist
 Surgical Management of Renal Cancer David Nicol Consultant Urologist Roles of Surgery 1. Curative intervention localised disease 2. Symptomatic control advanced disease 3. Augmentation of efficacy of systemic
Surgical Management of Renal Cancer David Nicol Consultant Urologist Roles of Surgery 1. Curative intervention localised disease 2. Symptomatic control advanced disease 3. Augmentation of efficacy of systemic
(Non-EKG Gated) CTA Thoracic Aorta = CTA Chest
 CTA Thoracic Aorta = CTA Chest") (Non-EKG Gated) CTA Thoracic Aorta = CTA Chest Reviewed By: Dan Verdini, MD, Rachael Edwards, MD Last Reviewed: January 2019 Contact: (866) 761-4200, Option 1 In accordance with the ALARA principle, TRA
(Non-EKG Gated) CTA Thoracic Aorta = CTA Chest Reviewed By: Dan Verdini, MD, Rachael Edwards, MD Last Reviewed: January 2019 Contact: (866) 761-4200, Option 1 In accordance with the ALARA principle, TRA
MDCT Findings of Renal Trauma
 MDT of Renal Trauma Genitourinary Imaging Pictorial Essay Downloaded from www.ajronline.org by 148.251.232.83 on 04/06/18 from IP address 148.251.232.83. opyright RRS. For personal use only; all rights
MDT of Renal Trauma Genitourinary Imaging Pictorial Essay Downloaded from www.ajronline.org by 148.251.232.83 on 04/06/18 from IP address 148.251.232.83. opyright RRS. For personal use only; all rights
Urinary tract embolization
 Beograd, 14.10.2012 Urinary tract embolization asist. Peter Popovič, MD, MSc Head of abdominal radiology department, Institute of Radiology, UMC Ljubljana Embolization Who and when procedure: local/general
Beograd, 14.10.2012 Urinary tract embolization asist. Peter Popovič, MD, MSc Head of abdominal radiology department, Institute of Radiology, UMC Ljubljana Embolization Who and when procedure: local/general
Renal Mass Biopsy: Needed Now More than Ever
 Renal Mass Biopsy: Needed Now More than Ever Stuart G. Silverman, MD, FACR Professor of Radiology Harvard Medical School Director, Abdominal Imaging and Intervention Brigham and Women s Hospital Boston,
Renal Mass Biopsy: Needed Now More than Ever Stuart G. Silverman, MD, FACR Professor of Radiology Harvard Medical School Director, Abdominal Imaging and Intervention Brigham and Women s Hospital Boston,
RENAL CANCER GUIDELINES
 Greater Manchester and Cheshire Cancer Network RENAL CANCER GUIDELINES Agreed by Urology CSG: July 2010 Review Date: July 2012 Renal Cancer Guidelines 1. Introduction 1.1 Kidney cancer accounts for 3%
Greater Manchester and Cheshire Cancer Network RENAL CANCER GUIDELINES Agreed by Urology CSG: July 2010 Review Date: July 2012 Renal Cancer Guidelines 1. Introduction 1.1 Kidney cancer accounts for 3%
Analysis of Changes in Attenuation of Proven Renal Cysts on Different Scanning Phases of Triphasic MDCT
 Eugene P. Chung 1 Brian R. Herts 1,2 Grant Linnell 1 Andrew C. Novick 2 Nancy Obuchowski 1,3 Deirdre M. Coll 1,4 Mark E. Baker 1 Received June 24, 2003; accepted after revision August 28, 2003. Presented
Eugene P. Chung 1 Brian R. Herts 1,2 Grant Linnell 1 Andrew C. Novick 2 Nancy Obuchowski 1,3 Deirdre M. Coll 1,4 Mark E. Baker 1 Received June 24, 2003; accepted after revision August 28, 2003. Presented
Management of Locally Reccurent Renal Cell Carcinoma. Jose A. Karam, MD, FACS Assistant Professor Department of Urology
 Management of Locally Reccurent Renal Cell Carcinoma Jose A. Karam, MD, FACS Assistant Professor Department of Urology DefiniAons Defini&ve treatment Aiming for cure Abla&on therapy Radiofrequency abla&on
Management of Locally Reccurent Renal Cell Carcinoma Jose A. Karam, MD, FACS Assistant Professor Department of Urology DefiniAons Defini&ve treatment Aiming for cure Abla&on therapy Radiofrequency abla&on
CTA Pulmonary Embolism CTA Chest W (arterial)
") CTA Pulmonary Embolism CTA Chest W (arterial) Reviewed By: Rachael Edwards, MD; Anna Ellermeier, MD; Brett Mollard, MD Last Reviewed: January 2019 Contact: (866) 761-4200, Option 1 In accordance with the
CTA Pulmonary Embolism CTA Chest W (arterial) Reviewed By: Rachael Edwards, MD; Anna Ellermeier, MD; Brett Mollard, MD Last Reviewed: January 2019 Contact: (866) 761-4200, Option 1 In accordance with the
6/5/2010. Renal vein invasion & Capsule Penetration (T3a) Adrenal Gland involvement (T4 vs. M1) Beyond Gerota s Fascia? (?T4).
 Adrenal Gland involvement (T4 vs. M1) Beyond Gerota s Fascia? (?T4).") GU Cancer Staging: Updates and Challenging Areas 13 th Current Issues in Surgical Pathology San Francisco, CA June 5, 2010 Jeffry P. Simko, PhD, MD Associate Professor Departments of Urology and Anatomic
GU Cancer Staging: Updates and Challenging Areas 13 th Current Issues in Surgical Pathology San Francisco, CA June 5, 2010 Jeffry P. Simko, PhD, MD Associate Professor Departments of Urology and Anatomic
Section Activity Activity Description Details Reference(s)
") Intended for use by Clinicians and Health Care Providers involved in the Management or Referral of adult patients with Renal Cell Carcinoma AA Cancer Centre Referrals Not routine pre-op referral indicated
Intended for use by Clinicians and Health Care Providers involved in the Management or Referral of adult patients with Renal Cell Carcinoma AA Cancer Centre Referrals Not routine pre-op referral indicated
Kidney Q&A 5/5/16 Q1: Can we please get that clarification sent with the presentation and Q&A? Also a start date for that clarification
 Kidney Q&A 5/5/16 Q1: Can we please get that clarification sent with the presentation and Q&A? Also a start date for that clarification A1: Yes. See below. I don't think it will have a start date. Clarification
Kidney Q&A 5/5/16 Q1: Can we please get that clarification sent with the presentation and Q&A? Also a start date for that clarification A1: Yes. See below. I don't think it will have a start date. Clarification
Five Views of Transitional Cell Carcinoma: One Man s Journey
 September 2006 Five Views of Transitional Cell Carcinoma: One Man s Journey Amsalu Dabela, Harvard Medical School III Outline Overview: Renal Anatomy Our Patient s Story Diagnostic Imaging Studies Appearance
September 2006 Five Views of Transitional Cell Carcinoma: One Man s Journey Amsalu Dabela, Harvard Medical School III Outline Overview: Renal Anatomy Our Patient s Story Diagnostic Imaging Studies Appearance
How To Approach Renal Masses? - Differential Diagnosis On Image
 How To Approach Renal Masses? - Differential Diagnosis On Image Poster No.: C-1646 Congress: ECR 2015 Type: Educational Exhibit Authors: A. E. A. G. Costa, A. Gomes, A. Duarte, I. Távora; Lisbon/PT Keywords:
How To Approach Renal Masses? - Differential Diagnosis On Image Poster No.: C-1646 Congress: ECR 2015 Type: Educational Exhibit Authors: A. E. A. G. Costa, A. Gomes, A. Duarte, I. Távora; Lisbon/PT Keywords:
Fundamentals, Techniques, Pitfalls, and Limitations of MDCT Interpretation and Measurement
 Fundamentals, Techniques, Pitfalls, and Limitations of MDCT Interpretation and Measurement 3 rd Annual Imaging & Physiology Summit November 20-21, 21, 2009 Seoul, Korea Wm. Guy Weigold, MD, FACC Cardiovascular
Fundamentals, Techniques, Pitfalls, and Limitations of MDCT Interpretation and Measurement 3 rd Annual Imaging & Physiology Summit November 20-21, 21, 2009 Seoul, Korea Wm. Guy Weigold, MD, FACC Cardiovascular
Bilateral Renal Angiomyolipomas with Invasion of the Renal Vein: A Case Report
 Case Study TheScientificWorldJOURNAL (2008) 8, 145 148 TSW Urology ISSN 1537-744X; DOI 10.1100/tsw.2008.29 Bilateral Renal Angiomyolipomas with Invasion of the Renal Vein: A Case Report C. Blick, N. Ravindranath,
Case Study TheScientificWorldJOURNAL (2008) 8, 145 148 TSW Urology ISSN 1537-744X; DOI 10.1100/tsw.2008.29 Bilateral Renal Angiomyolipomas with Invasion of the Renal Vein: A Case Report C. Blick, N. Ravindranath,
Normal morphology of renal vascularization and its related anatomic variations by use of imaging examinations in Albania
 ORIGINAL RESEARCH Normal morphology of renal vascularization and its related anatomic variations by use of imaging examinations in Albania Roland Hasa 1, Almir Skana 2 1 Orthodox Church Clinic & Hygeia
ORIGINAL RESEARCH Normal morphology of renal vascularization and its related anatomic variations by use of imaging examinations in Albania Roland Hasa 1, Almir Skana 2 1 Orthodox Church Clinic & Hygeia
Multidisciplinary approach for renal cell carcinoma Axel Bex, MD, PhD The Netherlands Cancer Institute
 Multidisciplinary approach for renal cell carcinoma Axel Bex, MD, PhD The Netherlands Cancer Institute 20 April, Antalya, Turkey RCC European Union 60.000 new diagnoses/year 26.000 Cancer related deaths
Multidisciplinary approach for renal cell carcinoma Axel Bex, MD, PhD The Netherlands Cancer Institute 20 April, Antalya, Turkey RCC European Union 60.000 new diagnoses/year 26.000 Cancer related deaths
Pediatric Retroperitoneal Masses Radiologic-Pathologic Correlation
 Acta Radiológica Portuguesa, Vol.XVIII, nº 70, pág. 61-70, Abr.-Jun., 2006 Pediatric Retroperitoneal Masses Radiologic-Pathologic Correlation Marilyn J. Siegel Mallinckrodt Institute of Radiology, Washington
Acta Radiológica Portuguesa, Vol.XVIII, nº 70, pág. 61-70, Abr.-Jun., 2006 Pediatric Retroperitoneal Masses Radiologic-Pathologic Correlation Marilyn J. Siegel Mallinckrodt Institute of Radiology, Washington
Role of imaging in RCC. Ultrasonography. Solid lesion. Cystic RCC. Solid RCC 31/08/60. From Diagnosis to Treatment: the Radiologist Perspective
 Role of imaging in RCC From Diagnosis to Treatment: the Radiologist Perspective Diagnosis Staging Follow up Imaging modalities Limitations and pitfalls Duangkamon Prapruttam, MD Department of Therapeutic
Role of imaging in RCC From Diagnosis to Treatment: the Radiologist Perspective Diagnosis Staging Follow up Imaging modalities Limitations and pitfalls Duangkamon Prapruttam, MD Department of Therapeutic
ROBOTIC SURGERY FOR RENAL CELL CANCER CLAYTON LAU, MD CHIEF OF UROLOGY AND UROLOGIC ONCOLOGY SEPT 2018
 ROBOTIC SURGERY FOR RENAL CELL CANCER CLAYTON LAU, MD CHIEF OF UROLOGY AND UROLOGIC ONCOLOGY SEPT 2018 Disclosures Consultant and Speaker for Intuitive Surgical and Covidien 2. Epidemiology 62K Estimated
ROBOTIC SURGERY FOR RENAL CELL CANCER CLAYTON LAU, MD CHIEF OF UROLOGY AND UROLOGIC ONCOLOGY SEPT 2018 Disclosures Consultant and Speaker for Intuitive Surgical and Covidien 2. Epidemiology 62K Estimated
My Patient Has Abdominal Pain PoCUS of the Biliary Tract and the Urinary Tract
 My Patient Has Abdominal Pain PoCUS of the Biliary Tract and the Urinary Tract Objectives PoCUS for Biliary Disease PoCUS for Renal Colic PoCUS for Urinary Retention Biliary Disease A patient presents
My Patient Has Abdominal Pain PoCUS of the Biliary Tract and the Urinary Tract Objectives PoCUS for Biliary Disease PoCUS for Renal Colic PoCUS for Urinary Retention Biliary Disease A patient presents
Index. Note: Page numbers of article titles are in boldface type.
 Magn Reson Imaging Clin N Am 12 (2004) 587 591 Index Note: Page numbers of article titles are in boldface type. A Adenoma(s), adrenal, gadolinium-enhanced MR imaging in, 533 534 hyperfunctioning versus
Magn Reson Imaging Clin N Am 12 (2004) 587 591 Index Note: Page numbers of article titles are in boldface type. A Adenoma(s), adrenal, gadolinium-enhanced MR imaging in, 533 534 hyperfunctioning versus
CT & MRI of Benign Liver Neoplasms Srinivasa R Prasad
 CT & MRI of Benign Liver Neoplasms Srinivasa R Prasad No financial disclosures Acknowledgements Many thanks to Drs. Heiken, Narra & Menias (MIR) Dr. Sahani (MGH) for sharing images Benign Liver Tumors:
CT & MRI of Benign Liver Neoplasms Srinivasa R Prasad No financial disclosures Acknowledgements Many thanks to Drs. Heiken, Narra & Menias (MIR) Dr. Sahani (MGH) for sharing images Benign Liver Tumors:
Killing Tumors with Scans Not Scalpels: Kidney Cancer Ablation. Basics. What is Percutaneous Ablation? Where are your kidneys?
 Killing Tumors with Scans Not Scalpels: Kidney Cancer Ablation Ronald J. Zagoria, M.D. UCSF Professor and Vice Chair Abdominal Imaging Section Chief Basics Where are your kidneys? What is ablation? Facts
Killing Tumors with Scans Not Scalpels: Kidney Cancer Ablation Ronald J. Zagoria, M.D. UCSF Professor and Vice Chair Abdominal Imaging Section Chief Basics Where are your kidneys? What is ablation? Facts
Wilms Tumor and Neuroblastoma
 Wilms Tumor and Neuroblastoma Wilm s Tumor AKA: Nephroblastoma the most common intra-abdominal cancer in children. peak incidence is 2 to 3 years of age Biology somatic mutations restricted to tumor tissue
Wilms Tumor and Neuroblastoma Wilm s Tumor AKA: Nephroblastoma the most common intra-abdominal cancer in children. peak incidence is 2 to 3 years of age Biology somatic mutations restricted to tumor tissue
Is renal cryoablation becoming an effective alternative to partial nephrectomy?
 Is renal cryoablation becoming an effective alternative to partial nephrectomy? J GARNON 1, G TSOUMAKIDOU 1, H LANG 2, A GANGI 1 1 department of interventional radiology 2 department of urology University
Is renal cryoablation becoming an effective alternative to partial nephrectomy? J GARNON 1, G TSOUMAKIDOU 1, H LANG 2, A GANGI 1 1 department of interventional radiology 2 department of urology University
Uroradiology For Medical Students
 Uroradiology For Medical Students Lesson 8 Computerized Tomography 2 American Urological Association Objectives In this lesson you will: Gain more experience reading CT images Learn how computer generated
Uroradiology For Medical Students Lesson 8 Computerized Tomography 2 American Urological Association Objectives In this lesson you will: Gain more experience reading CT images Learn how computer generated
Renal tumors of adults
 Renal tumors of adults Urinary Tract Tumors 2%-3% of all cancers in adults. The most common malignant tumor of the kidney is renal cell carcinoma. Tumors of the lower urinary tract are twice as common
Renal tumors of adults Urinary Tract Tumors 2%-3% of all cancers in adults. The most common malignant tumor of the kidney is renal cell carcinoma. Tumors of the lower urinary tract are twice as common
EAU GUIDELINES ON RENAL CELL CARCINOMA
 EAU GUIDELINES ON RENAL ELL ARINOMA (Limited text update March 2016) B. Ljungberg (hair), K. Bensalah, A. Bex (Vice-chair), S. anfield, R.H. Giles (Patient Organisation Representative), M. Hora, M.A. Kuczyk,
EAU GUIDELINES ON RENAL ELL ARINOMA (Limited text update March 2016) B. Ljungberg (hair), K. Bensalah, A. Bex (Vice-chair), S. anfield, R.H. Giles (Patient Organisation Representative), M. Hora, M.A. Kuczyk,
Ureteroscopy Is Indicated in every patient with suspected Upper Tract Urothelial Tumor
 Ureteroscopy Is Indicated in every patient with suspected Upper Tract Urothelial Tumor Scott G. Hubosky, MD The Demetrius H. Bagley Jr., MD Associate Professor of Urology Director of Endourology Vice Chair
Ureteroscopy Is Indicated in every patient with suspected Upper Tract Urothelial Tumor Scott G. Hubosky, MD The Demetrius H. Bagley Jr., MD Associate Professor of Urology Director of Endourology Vice Chair
Urology An introduction to cut up DR J R GOEPEL
 Urology An introduction to cut up DR J R GOEPEL Overview Principles Individual organs Small pieces Partial resections Whole organs Data recording and data sets Principles You are working for the patient
Urology An introduction to cut up DR J R GOEPEL Overview Principles Individual organs Small pieces Partial resections Whole organs Data recording and data sets Principles You are working for the patient
NAACCR Webinar Series 1
 NAACCR 2009 2010 Webinar Series Collecting Cancer Data: Kidney 1 Questions Please use the Q&A panel to submit your questions Send questions to All Panelist 2 Fabulous Prizes 3 NAACCR 2009 2010 Webinar
NAACCR 2009 2010 Webinar Series Collecting Cancer Data: Kidney 1 Questions Please use the Q&A panel to submit your questions Send questions to All Panelist 2 Fabulous Prizes 3 NAACCR 2009 2010 Webinar
2 Adrenal Disease. Open Surgery. Andrew C. Novick SURGICAL ANATOMY
 Preface More than 125 years have passed since the basic contributions of John Hunter, Crawford Long, and Lord Lister transformed surgery into a sound science as well as a delicate art. Several great surgeons
Preface More than 125 years have passed since the basic contributions of John Hunter, Crawford Long, and Lord Lister transformed surgery into a sound science as well as a delicate art. Several great surgeons
ELECTIVE PARTIAL NEPHRECTOMY FOR T1B RCC. Vitaly Margulis MD. Associate Professor of Urology
 ELECTIVE PARTIAL NEPHRECTOMY FOR T1B RCC Vitaly Margulis MD Associate Professor of Urology NEPHRON SPARING SURGERY WHY? MAXIMIZING NEPHRON MASS SAVES LIVES ELECTIVE PARTIAL NEPHRECTOMY IF: TECHNICALLY
ELECTIVE PARTIAL NEPHRECTOMY FOR T1B RCC Vitaly Margulis MD Associate Professor of Urology NEPHRON SPARING SURGERY WHY? MAXIMIZING NEPHRON MASS SAVES LIVES ELECTIVE PARTIAL NEPHRECTOMY IF: TECHNICALLY
Liver 4 Phase CT Abdomen WO W - NC.A.V.D
 Liver 4 Phase CT Abdomen WO W - NC.A.V.D Reviewed By: Rachael Edwards, MD; Anna Ellermeier, MD; Brett Mollard, MD Last Reviewed: January 2019 Contact: (866) 761-4200, Option 1 In accordance with the ALARA
Liver 4 Phase CT Abdomen WO W - NC.A.V.D Reviewed By: Rachael Edwards, MD; Anna Ellermeier, MD; Brett Mollard, MD Last Reviewed: January 2019 Contact: (866) 761-4200, Option 1 In accordance with the ALARA
4,3,2,1...How Many Phases are Needed? Balancing Diagnostic Efficacy and Radiation Modulation for MDCT Imaging of Renal Cell Carcinoma
 4,3,2,1...How Many Phases are Needed? Balancing Diagnostic Efficacy and Radiation Modulation for MDCT Imaging of Renal Cell Carcinoma Jeremy Hackworth, MD, MS Steven P Rowe, MD, PhD Satomi Kawamoto, MD
4,3,2,1...How Many Phases are Needed? Balancing Diagnostic Efficacy and Radiation Modulation for MDCT Imaging of Renal Cell Carcinoma Jeremy Hackworth, MD, MS Steven P Rowe, MD, PhD Satomi Kawamoto, MD
Renal Tumors in Transplantation
 Renal Tumors in Transplantation Kevin Morrison Clinical-Pathological Correlation September 15 th, 2004 Overview Case reports Neoplasia in transplantation Renal allograft tumors Native kidney RCC Role of
Renal Tumors in Transplantation Kevin Morrison Clinical-Pathological Correlation September 15 th, 2004 Overview Case reports Neoplasia in transplantation Renal allograft tumors Native kidney RCC Role of
UnusalPresentationofMetastasisfromaRenalCellCarcinoma-A CaseReportwithReviewofLiterature
 Global Journal of Medical Research: K Interdisciplinary Volume 18 Issue 8 Version 1.0 Type: Double Blind Peer Reviewed International Research Journal Publisher: Global Journals Online ISSN: 2249-4618 &
Global Journal of Medical Research: K Interdisciplinary Volume 18 Issue 8 Version 1.0 Type: Double Blind Peer Reviewed International Research Journal Publisher: Global Journals Online ISSN: 2249-4618 &
THREE-DIMENSIONAL IMAGING AND DISPLAY OF RENAL TUMORS USING SPIRAL CT: A POTENTIAL AID TO PARTIAL NEPHRECTOMY
 PRELIMINARY COMMUNICATION THREE-DIMENSIONAL IMAGING AND DISPLAY OF RENAL TUMORS USING SPIRAL CT: A POTENTIAL AID TO PARTIAL NEPHRECTOMY DANIEL M. CHERNOFF, M.D., PH.D. STUART G. SILVERMAN, M.D. RON KIKINIS,
PRELIMINARY COMMUNICATION THREE-DIMENSIONAL IMAGING AND DISPLAY OF RENAL TUMORS USING SPIRAL CT: A POTENTIAL AID TO PARTIAL NEPHRECTOMY DANIEL M. CHERNOFF, M.D., PH.D. STUART G. SILVERMAN, M.D. RON KIKINIS,
MDCT signs differentiating retroperitoneal and intraperitoneal lesions- diagnostic pearls
 MDCT signs differentiating retroperitoneal and intraperitoneal lesions- diagnostic pearls Poster No.: C-0987 Congress: ECR 2015 Type: Educational Exhibit Authors: D. V. Bhargavi, R. Avantsa, P. Kala; Bangalore/IN
MDCT signs differentiating retroperitoneal and intraperitoneal lesions- diagnostic pearls Poster No.: C-0987 Congress: ECR 2015 Type: Educational Exhibit Authors: D. V. Bhargavi, R. Avantsa, P. Kala; Bangalore/IN
Chromophobe Renal Cell Carcinoma: Multiphase MDCT Enhancement Patterns and Morphologic Features
 Genitourinary Imaging Original Research Raman et al. Enhancement Patterns and Morphologic Features of Chromophobe Renal Cell Carcinoma Genitourinary Imaging Original Research Siva P. Raman 1 Pamela T.
Genitourinary Imaging Original Research Raman et al. Enhancement Patterns and Morphologic Features of Chromophobe Renal Cell Carcinoma Genitourinary Imaging Original Research Siva P. Raman 1 Pamela T.
John Fitzpatrick Memorial Lecture. John Fitzpatrick Memorial lecture
 John Fitzpatrick Memorial Lecture John Fitzpatrick Memorial Lecture John M Fitzpatrick, 1948 2014 Head of Research at the Irish Cancer Society Professor of Surgery and Consultant Urologist at the Mater
John Fitzpatrick Memorial Lecture John Fitzpatrick Memorial Lecture John M Fitzpatrick, 1948 2014 Head of Research at the Irish Cancer Society Professor of Surgery and Consultant Urologist at the Mater
CT Pancreas 3 Phase CT Abdomen WO W - NC.A.V
 CT Pancreas 3 Phase CT Abdomen WO W - NC.A.V Reviewed By: Rachael Edwards, MD; Anna Ellermeier, MD; Brett Mollard, MD Last Reviewed: January 2019 Contact: (866) 761-4200, Option 1 In accordance with the
CT Pancreas 3 Phase CT Abdomen WO W - NC.A.V Reviewed By: Rachael Edwards, MD; Anna Ellermeier, MD; Brett Mollard, MD Last Reviewed: January 2019 Contact: (866) 761-4200, Option 1 In accordance with the
Role of MDCT in Radiological evaluation of Renal Masses and its beneficial effects on patient management.
 International Journal of advances in health sciences (IJHS) ISSN 2349-7033 Vol2, Issue1, 2015, pp56-63 http://www.ijhsonline.com Research Article Role of MDCT in Radiological evaluation of Renal Masses
International Journal of advances in health sciences (IJHS) ISSN 2349-7033 Vol2, Issue1, 2015, pp56-63 http://www.ijhsonline.com Research Article Role of MDCT in Radiological evaluation of Renal Masses
Experimental Model of Upper-Pole Nephrectomy Using Human Tridimensional Endocasts: Analysis of Vascular Injuries
 JOURNAL OF ENDOUROLOGY Volume 25, Number 1, January 2011 ª Mary Ann Liebert, Inc. Pp. 113 118 DOI: 10.1089=end.2010.0214 Experimental Model of Upper-Pole Nephrectomy Using Human Tridimensional Endocasts:
JOURNAL OF ENDOUROLOGY Volume 25, Number 1, January 2011 ª Mary Ann Liebert, Inc. Pp. 113 118 DOI: 10.1089=end.2010.0214 Experimental Model of Upper-Pole Nephrectomy Using Human Tridimensional Endocasts:
Freeze, Fry or Cut. Jennifer A. Linehan, MD Associate Professor Urologic Oncology John Wayne Cancer Institute 2/9/2018
 Freeze, Fry or Cut Jennifer A. Linehan, MD Associate Professor Urologic Oncology John Wayne Cancer Institute 2/9/2018 Disclosures Consultant for UroGen Pharma. REDEFINING WHAT SURGEONS SEE Bay Area-based
Freeze, Fry or Cut Jennifer A. Linehan, MD Associate Professor Urologic Oncology John Wayne Cancer Institute 2/9/2018 Disclosures Consultant for UroGen Pharma. REDEFINING WHAT SURGEONS SEE Bay Area-based
Surgery of Renal Cell Carcinoma Axel Bex, MD, PhD The Netherlands Cancer Institute
 Surgery of Renal Cell Carcinoma Axel Bex, MD, PhD The Netherlands Cancer Institute 23 March 2012, Sao Paulo, Brazil Surgery of RCC Locally confined (small) renal tumours Locally advanced disease Metastatic
Surgery of Renal Cell Carcinoma Axel Bex, MD, PhD The Netherlands Cancer Institute 23 March 2012, Sao Paulo, Brazil Surgery of RCC Locally confined (small) renal tumours Locally advanced disease Metastatic
Traumatic and Non Traumatic Adrenal Emergencies
 Traumatic and Non Traumatic Adrenal Emergencies Michael N. Patlas, MD, FRCPC (1), Christine O. Menias, MD (2), Douglas S. Katz, MD, FACR (3), Ania Z. Kielar, MD, FRCPC (4), Alla M. Rozenblit, MD (5), Jorge
Traumatic and Non Traumatic Adrenal Emergencies Michael N. Patlas, MD, FRCPC (1), Christine O. Menias, MD (2), Douglas S. Katz, MD, FACR (3), Ania Z. Kielar, MD, FRCPC (4), Alla M. Rozenblit, MD (5), Jorge