Customizing Contrast Injection for Body MDCT: Algorithmic Approach
|
|
|
- Russell Greene
- 6 years ago
- Views:
Transcription
1 Customizing Contrast Injection for Body MDCT: Algorithmic Approach Lincoln L. Berland, M.D., F.A.C.R. University of Alabama at Birmingham
2 Before Contrast
3 Prep and Hydration Hydration single most important factor: To get adequate collecting system filling To limit nephrotoxicity Don't keep patient NPO (clear liquids in am) Lots of water prior to scan
4 Intravenous Contrast Parameters Contrast or not? Route - IV arm, central line, hand, foot Concentration Volume Rate Saline chaser Fixed, bolus tracking, test bolus
5 Principles of Intravenous Contrast Dynamics
6 General - Iodine Dose If increase dose of Iodine, but inject within same duration: Increases peak enhancement Does not change time at which peak occurs How to achieve this: Increase contrast concentration, or Increase injection rate, maintain injection duration (more contrast volume)
7 Iodine Concentration Selection Higher concentration: can inject more Iodine for a specific volume/second Equivalent to increasing injection rate if you don t increase concentration With higher concentration, can decrease the volume injection rate for given Iodine injection rate Therefore, mg I/mL preferred over 300 mg I/mL
8 Aorta, Liver by Rate If increase injection rate, but keep Iodine dose constant: Aortic enhancement peak increases continuously with rate Liver enhancement peak levels off above 1.5 ml/sec
9 Aorta, Liver Enhancement MYTH: Can decrease contrast dose for liver scan by increasing injection rate TRUTH: Can decrease contrast dose for CTA by increasing injection rate
10 Injection Duration TIME to peak aortic and liver enhancement depends most strongly on injection duration Peak enhancement usually occurs shortly after injection completed
11 Injection Duration MYTH: For body scans, can use fixed scan delay regardless of injection rate TRUTH: Enhancement curves vary greatly by patient Use bolus tracking for arterial studies Fixed delay (by duration) usually OK for liver, etc.
12 Scan Delay MYTH: Faster scanner (e.g. 64 vs. 4- slice), shorter delay to scanning TRUTH: Faster scanner, longer delay to begin scanning Peak doesn t change, but more likely to finish scan before peak occurs Downslope of enhancement not as fast as upslope, so better to scan a little late rather than early
13 Patient-Specific Factors
14 Patient Weight - Enhancement Hepatic and arterial enhancement are proportional to Iodine dose administered and inversely proportional to weight Time to the enhancement peak is affected little by weight Therefore, Iodine dose should be increased proportional to weight
15 Cardiac Output - Aorta As cardiac output decreases, delay to peak increases MYTH: As cardiac output decreases, enhancement decreases TRUTH: Decreased cardiac output increases enhancement Therefore, decrease Iodine dose with decreased cardiac function
16 Cardiac Output - Hepatic As cardiac output decreases, delay to hepatic enhancement increases 60% decrease in cardiac output can delay peak from baseline 60 seconds to 150 seconds MYTH: Decreased cardiac output affects peak hepatic enhancement TRUTH: Hepatic enhancement won t change, but later peak
17 Phase by Application Consequence of these effects is that you must consider the target organ(s) to best design protocols, e.g.: Earlier scan for aorta Slower scan for runoff Later scan for liver
18 Contrast - From Theory to Practice
19 Iodine Dose Selection Patient weight Renal and cardiac function Brand and concentration of contrast available Organ and body region
20 Iodine Dose Selection Base dose varies from gm Iodine Should select based on Iodine dose, not volume We recommend standard dose based of 42 gm Iodine for average weight patient Select by patient weight, other factors
21 Iodine Dose Selection Some select: ml/kg If vary continuously by weight: Should be: gm I/kg We prefer weight categories for the average patient
22 Contrast Injection Rate Selection Route of injection Adequacy of line Injector - Dual Head with saline chaser better uses contrast injected Speed of scanner
23 Scan Timing Selection Specific application (e.g. 3-phase, routine, etc.) Speed of scanner
24 Algorithm Weight +concentration of agent + application: Volume Volume + application + adequacy of IV: Injection rate Injection rate + volume: Injection duration Injection duration + application + scanner: Scan timing
25 Contrast Dose Selection Select Contrast Dose Weight kg ( lb) kg ( lbs) kg ( lb) >110 kg (>240 lb) Body CT Based on 42 gi for average patient 350 mg/ml 350 mg/ml Š Renal insufficiency Contrast Volume 85 ml 120 ml 150 ml 180 ml Weight kg ( lb) kg ( lbs) kg ( lb) >110 kg (>240 lb) Body CT Select Contrast Dose Based on 42 gi for average patient 370 mg/ml 370 mg/ml Š Renal insufficiency Contrast Volume 85 ml 115 ml 140 ml 175 ml Weight kg ( lb) kg ( lbs) >90 kg (>200 lb) Contrast Volume 56 ml 80 ml 100 ml Weight kg ( lb) kg ( lbs) >90 kg (>200 lb) Contrast Volume 55 ml 75 ml 90 ml
26 Contrast Dose Selection Body CT Select Contrast Dose Based on 52 gi for average patient Weight kg ( lb) kg ( lbs) kg ( lb) >110 kg (>240 lb) 350 mg/ml 350 mg/ml Š Renal insufficiency Contrast Volume 104 ml 148 ml 185 ml 200 ml* Body CT Select Contrast Dose Based on 52 gi for average patient Weight kg ( lb) kg ( lbs) kg ( lb) >110 kg (>240 lb) 370 mg/ml 370 mg/ml Š Renal insufficiency Contrast Volume 98 ml 140 ml 175 ml 200 ml* Weight kg ( lb) kg ( lbs) >90 kg (>200 lb) Contrast Volume 56 ml 80 ml 100 ml Weight kg ( lb) kg ( lbs) >90 kg (>200 lb) Contrast Volume 55 ml 75 ml 90 ml Notes: *Calculated volume for high weight exceeds 200 ml capacity of injector. Renal insufficiency dose based on 42 gi chart rather than 52 gi chart. Notes: *Calculated volume for high weight exceeds 200 ml capacity of injector. Renal insufficiency dose based on 42 gi chart rather than 52 gi chart.
27 Contrast Injection Rate Body CT (excluding CTAs) Select Injection Rate All contrast agents Routine injection duration Injection Volume Injection Rate Injection Duration ml 1.6 ml/sec 30 seconds ml 1.8 ml/sec 30 seconds ml 2.0 ml/sec 30 seconds ml 2.1 ml/sec 30 seconds ml 2.3 ml/sec 30 seconds ml 2.5 ml/sec 30 seconds ml 2.6 ml/sec 30 seconds ml 2.8 ml/sec 30 seconds ml 3.0 ml/sec 30 seconds ml 3.1 ml/sec 30 seconds ml 3.3 ml/sec 30 seconds ml 3.5 ml/sec 30 seconds ml 3.6 ml/sec 30 seconds ml 3.8 ml/sec 30 seconds ml 4.0 ml/sec 35 seconds ml 4.6 ml/sec 30 seconds ml 4.8 ml/sec 30 seconds mL 5.0 ml/sec 30 seconds 175 ml 5.8 ml/sec 30 seconds 180 ml 6.0 ml/sec 30 seconds 185 ml 6.0 ml/sec 31 seconds 200 ml 6.0 ml/sec 33 seconds
28 Contrast Injection Rate Body CT (excluding CTAs) Select Injection Rate All contrast agents If IV cannot accept > 2.0 ml/sec Injection Volume Injection Rate Injection Duration ml 1.6 ml/sec 30 seconds ml 1.8 ml/sec 30 seconds ml 2.0 ml/sec 30 seconds ml 2.0 ml/sec 32 seconds ml 2.0 ml/sec 35 seconds ml 2.0 ml/sec 37 seconds ml 2.0 ml/sec 40 seconds ml 2.0 ml/sec 42 seconds ml 2.0 ml/sec 45 seconds ml 2.0 ml/sec 47 seconds ml 2.0 ml/sec 50 seconds ml 2.0 ml/sec 52 seconds ml 2.0 ml/sec 55 seconds ml 2.0 ml/sec 57 seconds ml 2.0 ml/sec 60 seconds ml 2.0 ml/sec 70 seconds ml 2.0 ml/sec 72 seconds mL 2.0 ml/sec 75 seconds 175 ml 2.0 ml/sec 87 seconds 180 ml 2.0 ml/sec 90 seconds 185 ml 2.0 ml/sec 92 seconds 200 ml 2.0 ml/sec 100 seconds
29 Body CT (excluding CTAs) Select Scanning Delay Routine Scans All scanners All delays from the beginning of injection Portal phase routine scan Injection Duration 30 seconds 31 seconds 32 seconds 33 seconds 35 seconds 37 seconds 40 seconds 42 seconds 45 seconds 47 seconds 50 seconds 52 seconds 55 seconds 57 seconds 60 seconds 70 seconds 72 seconds 75 seconds 87 seconds 90 seconds 92 seconds 100 seconds Delay 70 seconds 71 seconds 72 seconds 73 seconds 75 seconds 77 seconds 80 seconds 82 seconds 85 seconds 87 seconds 90 seconds 92 seconds 95 seconds 97 seconds 100 seconds 110 seconds 112 seconds 115 seconds 127 seconds 130 seconds 131 seconds 140 seconds
30 Implementing Algorithm Loose leaf handbooks (cookbooks) created One customized cookbook placed at each scanner Each cookbook is specific for scanner type and concentration of contrast material used Master reference cookbooks placed in radiology reading room
31 Liver Four-Phase (Abdomen or Abdomen/Pelvis): 40-slice, 64-slice Indications: Cirrhosis: evaluating for HCC and portal hypertension. Pre-Intervention planning: for TIPS, chemoembolization, embolization, ablation. Cholangiocarcinoma. Characterize unknown liver lesion. Notes, modifications: Should be done on 40 or 64-slice scanners, if possible, because 3D rendering is usually needed and these provide better image quality Pelvis should be performed if concern about pelvic metastasis or if known prior important pelvic abnormality If following up vascular metastases that are known to be seen best on portal venous phase, perform routine abdomen protocol. Contrast Unenhanced Phase (UP) Hepatic Arterial Phase (HAP) Portal Venous Phase (PVP) Delayed Phase (DP) Comments Oral contrast No No Rectal contrast No No IV contrast Š iodine conc. (mgi/ml) Iodine dose (gi), Volume and Flow Rate 52 gi for kg patient. Adjust proportionally for weight. See "Contrast Cookbook" This is a higher dose than routine protocols to optimize postprocessing and segmentation Saline flush - volume (ml) 50 If no dual injector, increase contrast dose by 10 ml Saline flush - flow rate (ml/s) Same as contrast injection rate Scan delay Trigger at 150 HU in aorta plus 15 seconds 45 seconds post-trigger 3 minutes post-trigger HAP slightly later than routine AP. Change delay to 10 minute for cholangiocarcinoma Acquisition Parameters Scout PA Lateral scanogram can help see spinal compressions; post-scan scanogram serves as a one-shot IVP Patient position Supine, feet first Supine, feet first Supine, feet first Supine, feet first Scan range Diaphragm to iliac crest Diaphragm to iliac crest Diaphragm to iliac crest or greater trochanter Liver Scanning direction Out Out Out Out Acquisition field of view Full patient width Full patient width Full patient width Full patient width Tube voltage (kvp) Can use 140 kvp for large patients Tube load (mas) 170 to to to to 200 Consider automated dose modulation Gantry rotation time (s) Consider 0.75 for obese patients Detector configuration (mm) 40 x or 64 x x or 64 x x or 64 x x 1.25 or 64 x Pitch Reconstruction Parameters Axial reconstruction (mm) 5.0 x x x x 5.0 Thin section axial for 3D/MPR (mm) 1.3 x 0.7 up to 2.0 x x 0.7 up to 2.0 x 1.0 Coronal reconstruction (mm) 3.0 Š 4.0 x Š 4.0 x 3.0 Recon filter kernel B or C B or C B or C Recon field of view Evolving Evolving Evolving Scanner automatically assigns optimal pitch based on approximate selection. Coronal and sagittal reconstructions should be performed routinely on HAP and PVP. Thick slab MIPs and/or sagittal MIPs may replace coronal and sagittal MPRs. Filter A helpful for very obese patients (less noisy images). Filter B if lower mas chosen (more noise than Filter A, but appropriate for average patient). Filter C increases spatial resolution, but also increases noise.
32 Pancreas (Abdomen or Abdomen/Pelvis): 40-slice, 64-slice Indications: Pancreatic mass known or suspected. Pancreatic carcinoma follow-up after treatment (surgery, XRT, chemotherapy) if pancreatic phase needed (see Exclusions, Notes below). Painless jaundice. Chronic pancreatitis vs. pancreatic mass. Acute pancreatitis > age 50 to rule out mass as etiology of pancreatitis. Exclusions: Acute pancreatitis < age 50 (Routine protocol). Known chronic pancreatitis to evaluate complications (Routine protocol). Known pancreatic adenocarcinoma recurrence or metastasis if well seen on PVP (Routine protocol). Pancreatic neuroendocrine tumor follow-up after treatment (RCC, Vascular Cancer FU protocol). Notes, modifications: Should be done on 40 or 64-slice scanners, if possible, because 3D rendering is usually needed and these provide better image quality. Pelvis should be performed if concern about pelvic metastasis or if known prior important pelvic abnormality. If following known unresectable pancreatic carcinoma, including with metastases, a routine abdomen or abdomen/pelvis may suffice. Routine examination may also be done for chronic pancreatitis to evaluate complications, acute pancreatitis < age 50, or pancreatitis reassessment. Contrast Unenhanced Phase (UP) Pancreatic Phase (PP) Portal Venous Phase (PVP) Comments Water or Volumen TM 500 ml to tolerance plus 250 ml Oral contrast water on table Rectal contrast No IV contrast Š iodine conc. (mgi/ml) Iodine dose (gi), Volume and Flow Rate 52 gi for kg patient. Adjust proportionally for weight. See "Contrast Cookbook" Saline flush - volume (ml) 30 Saline flush - flow rate (ml/s) Same as contrast injection rate Trigger at 150 HU in aorta plus 15 Scan delay seconds Acquisition Parameters 50 seconds post-trigger Scout PA Patient position Supine, feet first Supine, feet first Supine, feet first Diaphragm to iliac crest or greater Scan range Diaphragm to iliac crest Diaphragm to iliac crest trochanter Scanning direction Out Out Out Acquisition field of view Full patient width Full patient width Full patient width This is a higher dose than routine protocols to optimize post-processing and segmentation. Prefer higher injection rate, if possible, up to 5 ml/sec. If no dual injector, increase contrast dose by 10 ml Lateral scanogram can help see spinal compressions; post-scan scanogram serves as a one-shot IVP Tube voltage (kvp) Can use 140 kvp for large patients Tube load (mas) 170 to to to 300 Consider automated dose modulation Gantry rotation time (s) Consider 0.75 for obese patients Detector configuration (mm) 40 x or 64 x x or 64 x x or 64 x Pitch Reconstruction Parameters Axial reconstruction (mm) 5.0 x x x 3.0 Thin section axial for 3D/MPR (mm) 1.3 x 0.7 up to 2.0 x x 0.7 up to 2.0 x 1.0 Coronal reconstruction (mm) 3.0 Š 4.0 x Š 4.0 x 3.0 Recon filter kernel B or C B or C Recon field of view Evolving Evolving Scanner automatically assigns optimal pitch based on approximate selection. Perform 3D volume and curved planar reformatting. Note: qualifies for additional postprocessing coding Coronal reconstructions should be performed on both the Pancreatic and Portal Venous phases. Thick slab MIPs and/or sagittal MIPs may be considered as a replacement for coronal and sagittal MPRs. Filter A helpful for very obese patients. Filter B if lower mas chosen
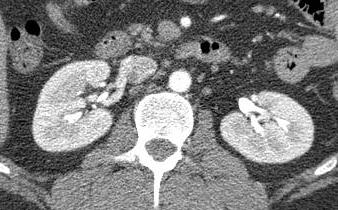
33 Renal Mass Pre-Intervention
34 Renal Mass Pre-intervention Indications: Prepare for nephron-sparing surgery or ablation Objectives: Define detailed vascular supply Localization Staging
35 Scan Phases Non-contrast May delete if have had recent non-contrast Arterial Through mid-pelvis to assure ID of anomalous arteries Nephrographic/excretory Entire abdomen-pelvis Split-dose
36 Split-Dose Injection Permits multiple purposes in single series, e.g. Late corticomedullary-early nephrographic Nephrographic-excretory
37 Split-Dose Injection Purpose Combine advantages of excretory, nephrographic and portal venous phases Use for both renal mass pre-intervention and CT urography protocols Renal mass includes arterial phase CT urography does not
38 Split-Dose Protocol Example Example: 115 ml Isovue 370 selected for 70 kg patient Inject about 1/4 of usual dose (30 ml) by hand Wait 10 minutes for excretion 300 ml saline IV during pause Inject additional complete dose (115 4 ml/sec) Arterial phase Scan delay of 100 sec (for nephrographic phase)

39 Split-Dose Injection Nephrographic-Excretory Late CM-Arterial-Excretory

40 Renal Mass Visualization Lesion margins seen better on nephrographic phase


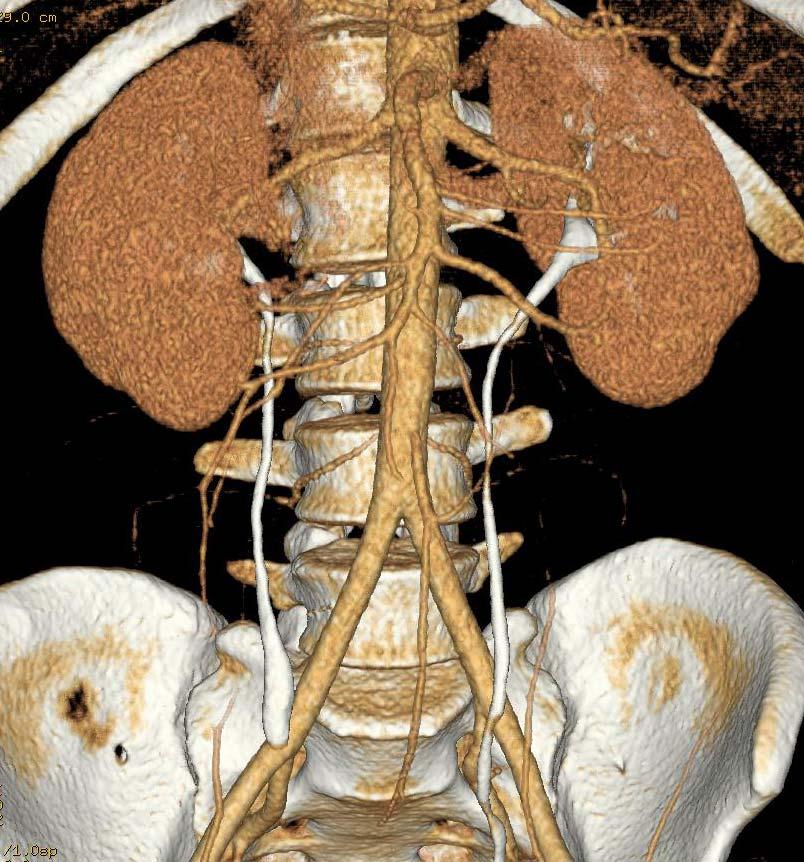
41 Post-Processing - MIPS Nephrographic/Excretory depicts vascular-collecting system to lesion relationships

42 Split-Dose Injection Arterial-Nephrographic Nephrographic-Excretory

43 Summary CT technology and protocol design is extremely complex. First step to tailoring exams is to understand basic principles of contrast dynamics and CT technology.
CT angiography techniques. Boot camp
 CT angiography techniques Boot camp Overview Basic concepts Contrast administration arterial opacification Time scan acquisition during the arterial phase Protocol examples Helical non-gated CTA Pulmonary
CT angiography techniques Boot camp Overview Basic concepts Contrast administration arterial opacification Time scan acquisition during the arterial phase Protocol examples Helical non-gated CTA Pulmonary
Liver 4 Phase CT Abdomen WO W - NC.A.V.D
 Liver 4 Phase CT Abdomen WO W - NC.A.V.D Reviewed By: Rachael Edwards, MD; Anna Ellermeier, MD; Brett Mollard, MD Last Reviewed: January 2019 Contact: (866) 761-4200, Option 1 In accordance with the ALARA
Liver 4 Phase CT Abdomen WO W - NC.A.V.D Reviewed By: Rachael Edwards, MD; Anna Ellermeier, MD; Brett Mollard, MD Last Reviewed: January 2019 Contact: (866) 761-4200, Option 1 In accordance with the ALARA
CTA Chest Pulmonary Embolism & Routine CT Abdomen + Pelvis W CTA Chest W (arterial) & CT Abdomen + Pelvis W (venous)
 & CT Abdomen + Pelvis W (venous)") CTA Chest Pulmonary Embolism & Routine CT Abdomen + Pelvis W CTA Chest W (arterial) & CT Abdomen + Pelvis W (venous) Reviewed By: Anna Ellermeier, MD; Brett Mollard, MD Last Reviewed: August 2018 Contact:
CTA Chest Pulmonary Embolism & Routine CT Abdomen + Pelvis W CTA Chest W (arterial) & CT Abdomen + Pelvis W (venous) Reviewed By: Anna Ellermeier, MD; Brett Mollard, MD Last Reviewed: August 2018 Contact:
CT Renal 3 Phase + Pelvis CT Abdomen Pelvis WO W - NC.A.V, Pelvis during V
 CT Renal 3 Phase + Pelvis CT Abdomen Pelvis WO W - NC.A.V, Pelvis during V Reviewed By: Anna Ellermeier, MD; Brett Mollard, MD Last Reviewed: August 2018 Contact: (866) 761-4200, Option 1 In accordance
CT Renal 3 Phase + Pelvis CT Abdomen Pelvis WO W - NC.A.V, Pelvis during V Reviewed By: Anna Ellermeier, MD; Brett Mollard, MD Last Reviewed: August 2018 Contact: (866) 761-4200, Option 1 In accordance
CT Pancreas 3 Phase CT Abdomen WO W - NC.A.V
 CT Pancreas 3 Phase CT Abdomen WO W - NC.A.V Reviewed By: Rachael Edwards, MD; Anna Ellermeier, MD; Brett Mollard, MD Last Reviewed: January 2019 Contact: (866) 761-4200, Option 1 In accordance with the
CT Pancreas 3 Phase CT Abdomen WO W - NC.A.V Reviewed By: Rachael Edwards, MD; Anna Ellermeier, MD; Brett Mollard, MD Last Reviewed: January 2019 Contact: (866) 761-4200, Option 1 In accordance with the
Vascular CT Protocols
 Vascular CT Protocols V 1D: Chest and abdominal CT angiogram (aortic dissection protocol) V 1T: Chest CT angiogram (aortic trauma protocol) V 2: Abdominal and pelvis CT angiogram (aortic aneurysm protocol)
Vascular CT Protocols V 1D: Chest and abdominal CT angiogram (aortic dissection protocol) V 1T: Chest CT angiogram (aortic trauma protocol) V 2: Abdominal and pelvis CT angiogram (aortic aneurysm protocol)
CTA Pulmonary Embolism CTA Chest W (arterial)
") CTA Pulmonary Embolism CTA Chest W (arterial) Reviewed By: Rachael Edwards, MD; Anna Ellermeier, MD; Brett Mollard, MD Last Reviewed: January 2019 Contact: (866) 761-4200, Option 1 In accordance with the
CTA Pulmonary Embolism CTA Chest W (arterial) Reviewed By: Rachael Edwards, MD; Anna Ellermeier, MD; Brett Mollard, MD Last Reviewed: January 2019 Contact: (866) 761-4200, Option 1 In accordance with the
(Non-EKG Gated) CTA Thoracic Aorta = CTA Chest
 CTA Thoracic Aorta = CTA Chest") (Non-EKG Gated) CTA Thoracic Aorta = CTA Chest Reviewed By: Dan Verdini, MD, Rachael Edwards, MD Last Reviewed: January 2019 Contact: (866) 761-4200, Option 1 In accordance with the ALARA principle, TRA
(Non-EKG Gated) CTA Thoracic Aorta = CTA Chest Reviewed By: Dan Verdini, MD, Rachael Edwards, MD Last Reviewed: January 2019 Contact: (866) 761-4200, Option 1 In accordance with the ALARA principle, TRA
Routine CT Chest + Abdomen WO
 Routine CT Chest + Abdomen WO Reviewed By: Anna Ellermeier, MD; Brett Mollard, MD Last Reviewed: August 2018 Contact: (866) 761-4200, Option 1 In accordance with the ALARA principle, TRA policies and protocols
Routine CT Chest + Abdomen WO Reviewed By: Anna Ellermeier, MD; Brett Mollard, MD Last Reviewed: August 2018 Contact: (866) 761-4200, Option 1 In accordance with the ALARA principle, TRA policies and protocols
CT Chest HRCT CT Chest WO
 CT Chest HRCT CT Chest WO Reviewed By: Anna Ellermeier, MD; Brett Mollard, MD Last Reviewed: August 2018 Contact: (866) 761-4200, Option 1 In accordance with the ALARA principle, TRA policies and protocols
CT Chest HRCT CT Chest WO Reviewed By: Anna Ellermeier, MD; Brett Mollard, MD Last Reviewed: August 2018 Contact: (866) 761-4200, Option 1 In accordance with the ALARA principle, TRA policies and protocols
Hi RES Extremity - (04/18/2011) CTDI: ~13 mgy per acquisition Used for evaluation of: Ankle Elbow Hand Wrist Foot /Calcaneous Toes Fingers
 CTDI: ~13 mgy per acquisition Used for evaluation of: Ankle Elbow Hand Wrist Foot /Calcaneous Toes Fingers") P a g e 1 Hi RES Extremity - (04/18/2011) CTDI: ~13 mgy per acquisition Used for evaluation of: Ankle Elbow Hand Wrist Foot /Calcaneous Toes Fingers Billing: 1. CT Upper/Lower Extremity of concern without
P a g e 1 Hi RES Extremity - (04/18/2011) CTDI: ~13 mgy per acquisition Used for evaluation of: Ankle Elbow Hand Wrist Foot /Calcaneous Toes Fingers Billing: 1. CT Upper/Lower Extremity of concern without
HI-Res Extremity Sensation 16
 Page 1 Routine Extremity - (2/14/2013) CTDI: ~20 mgy per acquisition Used for evaluation of: Humerus Forearm Femur Knee Tib/Fib Billing: 1. CT Upper/Lower Extremity of concern without contrast, with contrast,
Page 1 Routine Extremity - (2/14/2013) CTDI: ~20 mgy per acquisition Used for evaluation of: Humerus Forearm Femur Knee Tib/Fib Billing: 1. CT Upper/Lower Extremity of concern without contrast, with contrast,
Handzettel 1. CT Contrast Media. Agenda. Contrast Media Definition. Agenda. Why we need contrast media? Agenda
 Agenda CT Contrast Media Weena Swatdiswanee Factorinvolvein contrast enchancement Senior Application Specialist, CT Regional Headquarter Asia Australia weena.swat@siemens.com Page 1 Page 2 Agenda Contrast
Agenda CT Contrast Media Weena Swatdiswanee Factorinvolvein contrast enchancement Senior Application Specialist, CT Regional Headquarter Asia Australia weena.swat@siemens.com Page 1 Page 2 Agenda Contrast
W/ (2) (3) (4) (5) (5) (6) (6) CTA
 (3) (4) (5) (5) (6) (6) CTA") Index Abdomen W/ and W/Out (2) Abdomen Pelvis W/Out (3) Abdomen Pelvis W/ (4) Pelvis W/ (5) Chest W/Out (5) Chest/Abdomen/Pelvis W/ (6) Chest W/ (6) CTA ( 7-8) Neuro (8-9) Musculoskeletal (10) Trauma (11)
Index Abdomen W/ and W/Out (2) Abdomen Pelvis W/Out (3) Abdomen Pelvis W/ (4) Pelvis W/ (5) Chest W/Out (5) Chest/Abdomen/Pelvis W/ (6) Chest W/ (6) CTA ( 7-8) Neuro (8-9) Musculoskeletal (10) Trauma (11)
Fundamentals, Techniques, Pitfalls, and Limitations of MDCT Interpretation and Measurement
 Fundamentals, Techniques, Pitfalls, and Limitations of MDCT Interpretation and Measurement 3 rd Annual Imaging & Physiology Summit November 20-21, 21, 2009 Seoul, Korea Wm. Guy Weigold, MD, FACC Cardiovascular
Fundamentals, Techniques, Pitfalls, and Limitations of MDCT Interpretation and Measurement 3 rd Annual Imaging & Physiology Summit November 20-21, 21, 2009 Seoul, Korea Wm. Guy Weigold, MD, FACC Cardiovascular
Cardiac CTA Prospective Gating Broad Beam
 Cardiac CTA Prospective Gating Broad Beam ACQUISITION- Broad Beam Gating: Prospective Non Contrast Scan-Calcium Score Patient Position Supine Feet First into Gantry Heart Isocenter Scanogram AP and Lateral
Cardiac CTA Prospective Gating Broad Beam ACQUISITION- Broad Beam Gating: Prospective Non Contrast Scan-Calcium Score Patient Position Supine Feet First into Gantry Heart Isocenter Scanogram AP and Lateral
Cardiac CT - Coronary Calcium Basics Workshop II (Basic)
") Cardiac CT - Coronary Calcium Basics Workshop II (Basic) J. Jeffrey Carr, MD, MSCE Dept. of Radiology & Public Health Sciences Wake Forest University School of Medicine Winston-Salem, NC USA No significant
Cardiac CT - Coronary Calcium Basics Workshop II (Basic) J. Jeffrey Carr, MD, MSCE Dept. of Radiology & Public Health Sciences Wake Forest University School of Medicine Winston-Salem, NC USA No significant
Gemstone Spectral Imaging quantifies lesion characteristics for a confident diagnosis
 GE Healthcare Gemstone Spectral Imaging quantifies lesion characteristics for a confident diagnosis CT clinical case study lesion characterization Desiree Morgan, MD Vice Chair of Clinical Research Professor
GE Healthcare Gemstone Spectral Imaging quantifies lesion characteristics for a confident diagnosis CT clinical case study lesion characterization Desiree Morgan, MD Vice Chair of Clinical Research Professor
Whole Body CT Protocol Update 2018
 Whole Body CT Protocol Update 2018 10 th Nordic Course in Trauma Radiology Gothenburg, Sweden K.SHANMUGANATHAN M.D. Disclosure of Commercial Interest Neither I nor my immediate family members have a financial
Whole Body CT Protocol Update 2018 10 th Nordic Course in Trauma Radiology Gothenburg, Sweden K.SHANMUGANATHAN M.D. Disclosure of Commercial Interest Neither I nor my immediate family members have a financial
CT: Common Protocols. Michael Steigner, M.D. Director, Vascular CT/MR Assistant Professor of Radiology
 CT: Common Protocols BRIGHAM AND WOMEN S HOSPITAL Heart & Vascular Center Harvard Medical School Teaching Hospital Michael Steigner, M.D. Director, Vascular CT/MR Assistant Professor of Radiology msteigner@bwh.harvard.edu
CT: Common Protocols BRIGHAM AND WOMEN S HOSPITAL Heart & Vascular Center Harvard Medical School Teaching Hospital Michael Steigner, M.D. Director, Vascular CT/MR Assistant Professor of Radiology msteigner@bwh.harvard.edu
How do the Parameters affect Image Quality and Dose for Abdominal CT? Image Review
 How do the Parameters affect Image Quality and Dose for Abdominal CT? Image Review Mannudeep K. Kalra, MD, DNB Massachusetts General Hospital Harvard Medical School Financial Disclosure This presentation
How do the Parameters affect Image Quality and Dose for Abdominal CT? Image Review Mannudeep K. Kalra, MD, DNB Massachusetts General Hospital Harvard Medical School Financial Disclosure This presentation
Dual Energy CT Aortography: Can We Reduce Iodine Dose??
 Dual Energy CT Aortography: Can We Reduce Iodine Dose?? William P. Shuman MD, FACR FSCBTMR Department of Radiology University of Washington SCBTMR Annual Course Boston, October 10, 2012 Conflict of Interest
Dual Energy CT Aortography: Can We Reduce Iodine Dose?? William P. Shuman MD, FACR FSCBTMR Department of Radiology University of Washington SCBTMR Annual Course Boston, October 10, 2012 Conflict of Interest
Anterior Spinal Artery and Artery of Adamkiewicz Detected by Using Multi-Detector Row CT
 AJNR Am J Neuroradiol 24:13 17, January 2003 Anterior Spinal Artery and Artery of Adamkiewicz Detected by Using Multi-Detector Row CT Kohsuke Kudo, Satoshi Terae, Takeshi Asano, Masaki Oka, Kenshi Kaneko,
AJNR Am J Neuroradiol 24:13 17, January 2003 Anterior Spinal Artery and Artery of Adamkiewicz Detected by Using Multi-Detector Row CT Kohsuke Kudo, Satoshi Terae, Takeshi Asano, Masaki Oka, Kenshi Kaneko,
Patient preparation and coronary CTA techniques. Gregory Kicska, M.D. Ph.D. University of Washington, Thoracic Imaging
 Patient preparation and coronary CTA techniques Gregory Kicska, M.D. Ph.D. University of Washington, Thoracic Imaging Overview 1. Patient preparation 2. Scanning techniques Patient preparation Preparation
Patient preparation and coronary CTA techniques Gregory Kicska, M.D. Ph.D. University of Washington, Thoracic Imaging Overview 1. Patient preparation 2. Scanning techniques Patient preparation Preparation
Recommendations for cross-sectional imaging in cancer management, Second edition
 www.rcr.ac.uk Recommendations for cross-sectional imaging in cancer management, Second edition Renal and adrenal tumours Faculty of Clinical Radiology www.rcr.ac.uk Contents Renal cell carcinoma 3 Clinical
www.rcr.ac.uk Recommendations for cross-sectional imaging in cancer management, Second edition Renal and adrenal tumours Faculty of Clinical Radiology www.rcr.ac.uk Contents Renal cell carcinoma 3 Clinical
Translating Protocols Across Patient Size: Babies to Bariatric
 Translating Protocols Across Patient Size: Babies to Bariatric Cynthia H. McCollough, PhD, FACR, FAAPM Professor of Radiologic Physics Director, CT Clinical Innovation Center Department of Radiology Mayo
Translating Protocols Across Patient Size: Babies to Bariatric Cynthia H. McCollough, PhD, FACR, FAAPM Professor of Radiologic Physics Director, CT Clinical Innovation Center Department of Radiology Mayo
MRI Abdomen Protocol Pancreas/MRCP with Contrast
 MRI Abdomen Protocol Pancreas/MRCP with Contrast Reviewed By: Brett Mollard, MD; Anna Ellermeier, MD Last Reviewed: July 2018 Contact: (866) 761-4200 Standard uses: 1. Characterization of cystic and solid
MRI Abdomen Protocol Pancreas/MRCP with Contrast Reviewed By: Brett Mollard, MD; Anna Ellermeier, MD Last Reviewed: July 2018 Contact: (866) 761-4200 Standard uses: 1. Characterization of cystic and solid
Liver Perfusion Analysis New Frontiers in Dynamic Volume Imaging. Case Study Brochure Chang Gung Memorial Hospital.
 New Frontiers in Dynamic Volume Imaging dynamic volume CT Case Study Brochure Chang Gung Memorial Hospital http://www.toshibamedicalsystems.com Toshiba Medical Systems Corporation 2010-2011. All rights
New Frontiers in Dynamic Volume Imaging dynamic volume CT Case Study Brochure Chang Gung Memorial Hospital http://www.toshibamedicalsystems.com Toshiba Medical Systems Corporation 2010-2011. All rights
Cardiac CT Techniques in Neonates (and infants)
") Cardiac CT Techniques in Neonates (and infants) Siddharth P. Jadhav, MD Director, Body CT and MRI Edward B. Singleton Department of Pediatric Radiology Texas Children s Hospital Disclosures None Objectives
Cardiac CT Techniques in Neonates (and infants) Siddharth P. Jadhav, MD Director, Body CT and MRI Edward B. Singleton Department of Pediatric Radiology Texas Children s Hospital Disclosures None Objectives
Pediatric CT Protocols (18 years old or less)
") Pediatric CT Protocols (18 years old or less) Ped1: Head CT Ped2: Cervical spine CT Ped3: Sinus CT Ped4: Neck CT Ped5: Chest CT Ped6: Abdomen and pelvis CT Ped7: Thoracic or lumbar spine CT Ped8: Extremity
Pediatric CT Protocols (18 years old or less) Ped1: Head CT Ped2: Cervical spine CT Ped3: Sinus CT Ped4: Neck CT Ped5: Chest CT Ped6: Abdomen and pelvis CT Ped7: Thoracic or lumbar spine CT Ped8: Extremity
CT SCAN PROTOCOL. Shoulder
 CT SCAN PROTOCOL Shoulder Purpose and Summary CT images made with this protocol are used to provide the orthopedic surgeon with a detailed 3D anatomical reconstruction of the patient s scapula and proximal
CT SCAN PROTOCOL Shoulder Purpose and Summary CT images made with this protocol are used to provide the orthopedic surgeon with a detailed 3D anatomical reconstruction of the patient s scapula and proximal
Liver imaging takes a step forward with Ingenia
 Publication for the Philips MRI Community ISSUE 49 2013 / 2 Liver imaging takes a step forward with Ingenia Lyon South Hospital strives to move from several studies first CT, then MR or PET to using just
Publication for the Philips MRI Community ISSUE 49 2013 / 2 Liver imaging takes a step forward with Ingenia Lyon South Hospital strives to move from several studies first CT, then MR or PET to using just
03/01/17. Table of Contents GENERAL CT GUIDELINES... 3 ORAL CONTRAST... 3 RECTAL CONTRAST... 5 VAGINAL CONTRAST... 5
 03/01/17 Table of Contents GENERAL CT GUIDELINES... 3 ORAL CONTRAST... 3 RECTAL CONTRAST... 5 VAGINAL CONTRAST... 5 ROUTINE ABDOMEN/PELVIS... 6 ABDOMEN/PELVIS with DELAY... 7 NON CONTRAST ABDOMEN/PELVIS...
03/01/17 Table of Contents GENERAL CT GUIDELINES... 3 ORAL CONTRAST... 3 RECTAL CONTRAST... 5 VAGINAL CONTRAST... 5 ROUTINE ABDOMEN/PELVIS... 6 ABDOMEN/PELVIS with DELAY... 7 NON CONTRAST ABDOMEN/PELVIS...
FieldStrength. Tips for abdomen/pelvis oncology imaging. SPECIAL ISSUE MR in oncology. Publication for the Philips MRI Community
 FieldStrength Publication for the Philips MRI Community Issue 41 September 2010 Tips for abdomen/pelvis oncology imaging SPECIAL ISSUE MR in oncology This article is part of Field Strength issue 41, September
FieldStrength Publication for the Philips MRI Community Issue 41 September 2010 Tips for abdomen/pelvis oncology imaging SPECIAL ISSUE MR in oncology This article is part of Field Strength issue 41, September
CT Contrast Protocols for Different Organ Imaging
 CT Contrast Protocols for Different Organ Imaging g Paul Shreve, M.D. Advanced Radiology Services, P.C. & Spectrum Health Grand Rapids, MI, USA Correlative Imaging Council Society of Nuclear Medicine 56
CT Contrast Protocols for Different Organ Imaging g Paul Shreve, M.D. Advanced Radiology Services, P.C. & Spectrum Health Grand Rapids, MI, USA Correlative Imaging Council Society of Nuclear Medicine 56
CHEST CT PROTOCOL FOR MULTIPLE DETECTOR ROW SCANNERS
 1. Standard ed 2. Standard ed & Abdomen 3. Standard ed, Abdomen, & Pelvis 4. Aortic Dissection arch dome thru adrenals apex arch + 2 arch dome thru abdomen apex arch + 2 arch dome to crests apex arch +
1. Standard ed 2. Standard ed & Abdomen 3. Standard ed, Abdomen, & Pelvis 4. Aortic Dissection arch dome thru adrenals apex arch + 2 arch dome thru abdomen apex arch + 2 arch dome to crests apex arch +
Abdomen and Pelvis CT (1) By the end of the lecture students should be able to:
 By the end of the lecture students should be able to:") RAD 451 Abdomen and Pelvis CT (1) By the end of the lecture students should be able to: State the common indications for Abdomen and pelvis CT exams Identify possible contra indications for Abdomen and
RAD 451 Abdomen and Pelvis CT (1) By the end of the lecture students should be able to: State the common indications for Abdomen and pelvis CT exams Identify possible contra indications for Abdomen and
CT of the Head, Spine, and Cerebral Vessels
 CT of the Head, Spine, and Cerebral Vessels Objectives Determine specific imaging plane used to acquire or reformat CT scan, i.e. sagittal, coronal, transverse, and offaxis or oblique. Assess and evaluate
CT of the Head, Spine, and Cerebral Vessels Objectives Determine specific imaging plane used to acquire or reformat CT scan, i.e. sagittal, coronal, transverse, and offaxis or oblique. Assess and evaluate
Ask EuroSafe Imaging. Tips & Tricks. CT Working Group
 Ask EuroSafe Imaging Tips & Tricks CT Working Group The use of bi-phase injection protocols to reduce the number of acquisition phases and radiation dose Alban Gervaise (Medical Imaging Department, HIA
Ask EuroSafe Imaging Tips & Tricks CT Working Group The use of bi-phase injection protocols to reduce the number of acquisition phases and radiation dose Alban Gervaise (Medical Imaging Department, HIA
The Computed Tomography Examination
 CONTENT SPECIFICATIONS The Computed Tomography Examination The purpose of The American Registry of Radiologic Technologists (ARRT ) Computed Tomography Examination is to assess the knowledge and cognitive
CONTENT SPECIFICATIONS The Computed Tomography Examination The purpose of The American Registry of Radiologic Technologists (ARRT ) Computed Tomography Examination is to assess the knowledge and cognitive
PICTORIAL ESSAY. Experiences of using a single post-contrast CT scan of the urinary tract after triphasic contrast injection
 Experiences of using a single post-contrast CT scan of the urinary tract after triphasic contrast injection P C Pretorius, FCRad (Diag) SA Drs Visser, Erasmus, Vawda & Partners, Port Elizabeth Corresponding
Experiences of using a single post-contrast CT scan of the urinary tract after triphasic contrast injection P C Pretorius, FCRad (Diag) SA Drs Visser, Erasmus, Vawda & Partners, Port Elizabeth Corresponding
ROUTINE MRI PROTOCOLS: I. Abdomen Plus Post Gadolinium Screening Pelvis
 ROUTINE MRI PROTOCOLS: I. Abdomen Plus Post Gadolinium Screening Pelvis Sequence Coverage Slice/Gap Notes COR T2 ssfse 32-40 6/-1 Coverage from all sequences is above the liver dome, through the kidneys.
ROUTINE MRI PROTOCOLS: I. Abdomen Plus Post Gadolinium Screening Pelvis Sequence Coverage Slice/Gap Notes COR T2 ssfse 32-40 6/-1 Coverage from all sequences is above the liver dome, through the kidneys.
Austin Radiological Association Nuclear Medicine Procedure PET SODIUM FLUORIDE BONE SCAN (F-18 NaF)
") Austin Radiological Association Nuclear Medicine Procedure PET SODIUM FLUORIDE BONE SCAN (F-18 NaF) Overview Indication Sodium Fluoride F18 injection is a radioactive diagnostic agent for positron emission
Austin Radiological Association Nuclear Medicine Procedure PET SODIUM FLUORIDE BONE SCAN (F-18 NaF) Overview Indication Sodium Fluoride F18 injection is a radioactive diagnostic agent for positron emission
SPECIFIC PRINCIPLES FOR DOSE REDUCTION IN HEAD CT IMAGING. Rajiv Gupta, MD, PhD Neuroradiology, Massachusetts General Hospital Harvard Medical School
 SPECIFIC PRINCIPLES FOR DOSE REDUCTION IN HEAD CT IMAGING Rajiv Gupta, MD, PhD Neuroradiology, Massachusetts General Hospital Harvard Medical School OUTLINE 1 st Presentation: Dose optimization strategies
SPECIFIC PRINCIPLES FOR DOSE REDUCTION IN HEAD CT IMAGING Rajiv Gupta, MD, PhD Neuroradiology, Massachusetts General Hospital Harvard Medical School OUTLINE 1 st Presentation: Dose optimization strategies
Body CT Protocols General tips:
 Body CT Protocols General tips: -Check the list of protocol types on Intrad -Look at prior studies for help -Look up clinical info in Epic or Powerchart -Call ordering clinician if you have unanswered
Body CT Protocols General tips: -Check the list of protocol types on Intrad -Look at prior studies for help -Look up clinical info in Epic or Powerchart -Call ordering clinician if you have unanswered
Newcastle HPB MDM updated radiology imaging protocol recommendations. Author Dr John Scott. Consultant Radiologist Freeman Hospital
 Newcastle HPB MDM updated radiology imaging protocol recommendations Author Dr John Scott. Consultant Radiologist Freeman Hospital This document is intended as a guide to aid radiologists and clinicians
Newcastle HPB MDM updated radiology imaging protocol recommendations Author Dr John Scott. Consultant Radiologist Freeman Hospital This document is intended as a guide to aid radiologists and clinicians
X-Ray & CT Physics / Clinical CT
 Computed Tomography-Basic Principles and Good Practice X-Ray & CT Physics / Clinical CT INSTRUCTORS: Dane Franklin, MBA, RT (R) (CT) Office hours will be Tuesdays from 5pm to 6pm CLASSROOM: TIME: REQUIRED
Computed Tomography-Basic Principles and Good Practice X-Ray & CT Physics / Clinical CT INSTRUCTORS: Dane Franklin, MBA, RT (R) (CT) Office hours will be Tuesdays from 5pm to 6pm CLASSROOM: TIME: REQUIRED
PULMONARY EMBOLISM ANGIOCT (CTA) ASSESSMENT OF VASCULAR OCCLUSION EXTENT AND LOCALIZATION OF EMBOLI 1. BACKGROUND
 ASSESSMENT OF VASCULAR OCCLUSION EXTENT AND LOCALIZATION OF EMBOLI 1. BACKGROUND") JOURNAL OF MEDICAL INFORMATICS & TECHNOLOGIES Vol. 11/2007, ISSN 1642-6037 Damian PTAK * pulmonary embolism, AngioCT, postprocessing techniques, Mastora score PULMONARY EMBOLISM ANGIOCT (CTA) ASSESSMENT
JOURNAL OF MEDICAL INFORMATICS & TECHNOLOGIES Vol. 11/2007, ISSN 1642-6037 Damian PTAK * pulmonary embolism, AngioCT, postprocessing techniques, Mastora score PULMONARY EMBOLISM ANGIOCT (CTA) ASSESSMENT
Shoulder Position: Supine arm in the neutral position. Collateral arm above head Indication: fracture humerus, fracture scapula
 Shoulder Position: Supine arm in the neutral position. Collateral arm above head Indication: fracture humerus, fracture scapula No instrumentation With metal or cast KV/ Effective mas/rotation time 140/300/1.0
Shoulder Position: Supine arm in the neutral position. Collateral arm above head Indication: fracture humerus, fracture scapula No instrumentation With metal or cast KV/ Effective mas/rotation time 140/300/1.0
Utility of Variable Helical Pitch CT Scanning Technique for CT Angiography of Aortoiliac and Lower Extremity Arteries
 Utility of Variable Helical Pitch CT Scanning Technique for CT Angiography of Aortoiliac and Lower Extremity Arteries Poster No.: C-0863 Congress: ECR 2015 Type: Scientific Exhibit Authors: A. Nakamoto,
Utility of Variable Helical Pitch CT Scanning Technique for CT Angiography of Aortoiliac and Lower Extremity Arteries Poster No.: C-0863 Congress: ECR 2015 Type: Scientific Exhibit Authors: A. Nakamoto,
North American Society of Cardiovascular Imaging Annual Meeting, Baltimore MD, October 15-18, Tips and Tricks in Vascular Imaging
 North American Society of Cardiovascular Imaging Annual Meeting, Baltimore MD, October 15-18, 2016 Tips and Tricks in Vascular Imaging Lower Extremity CTA Dominik Fleischmann, Richard Hallett Division
North American Society of Cardiovascular Imaging Annual Meeting, Baltimore MD, October 15-18, 2016 Tips and Tricks in Vascular Imaging Lower Extremity CTA Dominik Fleischmann, Richard Hallett Division
PERIPHERAL CTA. Richard L. Hallett, MD
 RC 812B Lakeside E351 1 December 2017 0830 1000 Richard L. Hallett, MD Chief, Cardiovascular Imaging Northwest Radiology Network Indianapolis, IN Adjunct Assistant Professor Radiology Cardiovascular Imaging
RC 812B Lakeside E351 1 December 2017 0830 1000 Richard L. Hallett, MD Chief, Cardiovascular Imaging Northwest Radiology Network Indianapolis, IN Adjunct Assistant Professor Radiology Cardiovascular Imaging
Cardiac Computed Tomography
 Cardiac Computed Tomography Authored and approved by Koen Nieman Stephan Achenbach Francesca Pugliese Bernard Cosyns Patrizio Lancellotti Anastasia Kitsiou Contents CARDIAC COMPUTED TOMOGRAPHY Page 1.
Cardiac Computed Tomography Authored and approved by Koen Nieman Stephan Achenbach Francesca Pugliese Bernard Cosyns Patrizio Lancellotti Anastasia Kitsiou Contents CARDIAC COMPUTED TOMOGRAPHY Page 1.
Managing Radiation Risk in Pediatric CT Imaging
 Managing Radiation Risk in Pediatric CT Imaging Mahadevappa Mahesh, MS, PhD, FAAPM, FACR, FACMP, FSCCT. Professor of Radiology and Cardiology Johns Hopkins University School of Medicine Chief Physicist
Managing Radiation Risk in Pediatric CT Imaging Mahadevappa Mahesh, MS, PhD, FAAPM, FACR, FACMP, FSCCT. Professor of Radiology and Cardiology Johns Hopkins University School of Medicine Chief Physicist
Lung Perfusion Analysis New Pathways in Lung Imaging. Case Study Brochure PLA 309 Hospital
 Lung Perfusion Analysis New Pathways in Lung Imaging Case Study Brochure PLA 309 Hospital http://www.toshibamedicalsystems.com Toshiba Medical Systems Corporation 2012 all rights reserved. Design and specifications
Lung Perfusion Analysis New Pathways in Lung Imaging Case Study Brochure PLA 309 Hospital http://www.toshibamedicalsystems.com Toshiba Medical Systems Corporation 2012 all rights reserved. Design and specifications
Genitourinary. Common Clinical Scenarios Protocoling Module. Patty Ojeda & Mariam Shehata
 The following training module was developed as a quality improvement project to serve as an educational tool for junior radiology residents. The following diagnostic radiology protocoling modules were
The following training module was developed as a quality improvement project to serve as an educational tool for junior radiology residents. The following diagnostic radiology protocoling modules were
STRUCTURED EDUCATION REQUIREMENTS EFFECTIVE: JANUARY 1, 2016
 Computed Tomography The purpose of structured education is to provide the opportunity for individuals to develop mastery of discipline-specific knowledge that, when coupled with selected clinical experiences,
Computed Tomography The purpose of structured education is to provide the opportunity for individuals to develop mastery of discipline-specific knowledge that, when coupled with selected clinical experiences,
Upper GI Malignancies Imaging Guidelines for the Management of Gastric, Oesophageal & Pancreatic Cancers 2012
 Upper GI Malignancies Imaging Guidelines for the Management of Gastric, Oesophageal & Pancreatic Cancers 2012 Version Control This is a controlled document please destroy all previous versions on receipt
Upper GI Malignancies Imaging Guidelines for the Management of Gastric, Oesophageal & Pancreatic Cancers 2012 Version Control This is a controlled document please destroy all previous versions on receipt
Radiation Dose Reduction: Should You Use a Bismuth Breast Shield?
 Radiation Dose Reduction: Should You Use a Bismuth Breast Shield? Lincoln L. Berland, M.D., F.A.C.R. Michael V. Yester, Ph.D. University of Alabama at Birmingham Breast Radiation on CT Use of chest CT
Radiation Dose Reduction: Should You Use a Bismuth Breast Shield? Lincoln L. Berland, M.D., F.A.C.R. Michael V. Yester, Ph.D. University of Alabama at Birmingham Breast Radiation on CT Use of chest CT
Protocols in Cardiac CT Dr. Bruce Precious Dalhousie University Friday, April 15, 2016
 Protocols in Cardiac CT Dr. Bruce Precious Dalhousie University Friday, April 15, 2016 Disclosure Statement: No Conflict of Interest I do not have an affiliation, financial or otherwise, with a pharmaceutical
Protocols in Cardiac CT Dr. Bruce Precious Dalhousie University Friday, April 15, 2016 Disclosure Statement: No Conflict of Interest I do not have an affiliation, financial or otherwise, with a pharmaceutical
Partial Nephrectomy Planning: Everybody s s doing it, you can to
 Partial Nephrectomy Planning: Everybody s s doing it, you can to Brian R. Herts, MD Associate Professor of Radiology Head, Abdominal Imaging, Imaging Institute & Staff, The Glickman Urological and Kidney
Partial Nephrectomy Planning: Everybody s s doing it, you can to Brian R. Herts, MD Associate Professor of Radiology Head, Abdominal Imaging, Imaging Institute & Staff, The Glickman Urological and Kidney
CT Guided Procedures And Interesting Cases. Stephen Kim, MD Diagnostic and Interventional Radiology
 CT Guided Procedures And Interesting Cases Stephen Kim, MD Diagnostic and Interventional Radiology CT guided procedure benefits Precise lesion targeting Clear image guidance for needle placement Immediate
CT Guided Procedures And Interesting Cases Stephen Kim, MD Diagnostic and Interventional Radiology CT guided procedure benefits Precise lesion targeting Clear image guidance for needle placement Immediate
CT abdomen and pelvis
 CT abdomen and pelvis General indications: Assessment of vague abdominal symptoms (pain, colics,distenstion,...) Varifecation of a lesion discovered by other diagnostic modalities as US, barium,ivp, Staging
CT abdomen and pelvis General indications: Assessment of vague abdominal symptoms (pain, colics,distenstion,...) Varifecation of a lesion discovered by other diagnostic modalities as US, barium,ivp, Staging
Ultrasound. Computed tomography. Case studies. Utility of IQon Spectral CT in. cardiac imaging
 Ultrasound Computed tomography Case studies Utility of IQon Spectral CT in cardiac imaging Cardiac imaging is a challenging procedure where it is necessary to image a motion-free heart. This requires a
Ultrasound Computed tomography Case studies Utility of IQon Spectral CT in cardiac imaging Cardiac imaging is a challenging procedure where it is necessary to image a motion-free heart. This requires a
Dual-Energy CT: The Technological Approaches
 Dual-Energy CT: The Technological Approaches Dushyant Sahani, M.D Director of CT Associate Professor of Radiology Massachusetts General Hospital Harvard Medical School Email-dsahani@partners.org Disclosure
Dual-Energy CT: The Technological Approaches Dushyant Sahani, M.D Director of CT Associate Professor of Radiology Massachusetts General Hospital Harvard Medical School Email-dsahani@partners.org Disclosure
Combined Anatomical and Functional Imaging with Revolution * CT
 GE Healthcare Case studies Combined Anatomical and Functional Imaging with Revolution * CT Jean-Louis Sablayrolles, M.D. Centre Cardiologique du Nord, Saint-Denis, France Case 1 Whole Brain Perfusion and
GE Healthcare Case studies Combined Anatomical and Functional Imaging with Revolution * CT Jean-Louis Sablayrolles, M.D. Centre Cardiologique du Nord, Saint-Denis, France Case 1 Whole Brain Perfusion and
Appendix Sample CT Protocols
 Appendix Sample CT Protocols The protocols in the following Appendix are designed to serve as a general guide to setting up comprehensive CT protocols on your scanner. The protocols are independent of
Appendix Sample CT Protocols The protocols in the following Appendix are designed to serve as a general guide to setting up comprehensive CT protocols on your scanner. The protocols are independent of
RC 612B 3 December Richard L. Hallett, MD
 RC 612B 3 December 2015 0830 1000 Richard L. Hallett, MD Chief, Cardiovascular Imaging Northwest Radiology Network Indianapolis, IN Adjunct Assistant Professor Radiology Stanford University Stanford, CA
RC 612B 3 December 2015 0830 1000 Richard L. Hallett, MD Chief, Cardiovascular Imaging Northwest Radiology Network Indianapolis, IN Adjunct Assistant Professor Radiology Stanford University Stanford, CA
Scientific Exhibit. Authors: D. Takenaka, Y. Ohno, Y. Onishi, K. Matsumoto, T.
 The feasibility of biphasic contrast-media-injection-protocol for chest imaging on 320-slice volume MDCT: Direct comparison of biphasic and bolus contrast-media injection protocols on 320-slice volume
The feasibility of biphasic contrast-media-injection-protocol for chest imaging on 320-slice volume MDCT: Direct comparison of biphasic and bolus contrast-media injection protocols on 320-slice volume
Reducing Radiation Dose in Body CT: A Practical Approach to Optimizing CT Protocols
 Medical Physics and Informatics Review Goldman and Maldjian Reducing Radiation Dose in ody CT Medical Physics and Informatics Review Downloaded from www.ajronline.org by lice Goldman on 03/26/13 from IP
Medical Physics and Informatics Review Goldman and Maldjian Reducing Radiation Dose in ody CT Medical Physics and Informatics Review Downloaded from www.ajronline.org by lice Goldman on 03/26/13 from IP
MDCT PROTOCOLS FOR POLYTRAUMA PATIENTS
 András Palkó Department of Radiology, University of Szeged, Hungary MDCT PROTOCOLS FOR POLYTRAUMA PATIENTS Agenda Definition and significance Clinical implications Roleof imaging Examination protocols
András Palkó Department of Radiology, University of Szeged, Hungary MDCT PROTOCOLS FOR POLYTRAUMA PATIENTS Agenda Definition and significance Clinical implications Roleof imaging Examination protocols
Assignable revenue codes: Explanation of services:
 computed tomography Chest/Cardiac Assignable revenue codes: Explanation of services: 0350 CT Scan General Classification 0351 CT Scan Head Scan 0352 CT Scan Body Scan 0359 CT Scan Other CT Scans Known
computed tomography Chest/Cardiac Assignable revenue codes: Explanation of services: 0350 CT Scan General Classification 0351 CT Scan Head Scan 0352 CT Scan Body Scan 0359 CT Scan Other CT Scans Known
Liver MRI in 30 minutes
 X Liver MRI in 30 minutes SCBT/MR Annual Meeting Salt Lake City September 18, 2016 Scott B. Reeder, MD, PhD Department of Radiology University of Wisconsin Madison, WI Disclosures University of Wisconsin-Madison
X Liver MRI in 30 minutes SCBT/MR Annual Meeting Salt Lake City September 18, 2016 Scott B. Reeder, MD, PhD Department of Radiology University of Wisconsin Madison, WI Disclosures University of Wisconsin-Madison
Cardiac CTA without and with IV Contrast
 Cardiac CTA without and with IV Contrast IMG 12122 Cardiac Prospective 12123 Cardiac Retrospective 12119 Cardiac ED Chest Pain 12150 Calcium Score A B A B Toshiba AquilionONE Toshiba AquilionPRIME Calcium
Cardiac CTA without and with IV Contrast IMG 12122 Cardiac Prospective 12123 Cardiac Retrospective 12119 Cardiac ED Chest Pain 12150 Calcium Score A B A B Toshiba AquilionONE Toshiba AquilionPRIME Calcium
CT PROCEDURE REFERENCE GUIDE 2017
 Head CT PROCEDURE REFERENCE GUIDE 2017 Procedure Contrast Scan Field Preparatio n Base of Skull to Vertex Sinuses Orbits Mastoids/IAC/ Temporal Bones Facial Bones ST Neck Low Dose Lung Screening Routine
Head CT PROCEDURE REFERENCE GUIDE 2017 Procedure Contrast Scan Field Preparatio n Base of Skull to Vertex Sinuses Orbits Mastoids/IAC/ Temporal Bones Facial Bones ST Neck Low Dose Lung Screening Routine
Imaging of liver and pancreas
 Imaging of liver and pancreas.. Disease of the liver Focal liver disease Diffusion liver disease Focal liver disease Benign Cyst Abscess Hemangioma FNH Hepatic adenoma HCC Malignant Fibrolamellar carcinoma
Imaging of liver and pancreas.. Disease of the liver Focal liver disease Diffusion liver disease Focal liver disease Benign Cyst Abscess Hemangioma FNH Hepatic adenoma HCC Malignant Fibrolamellar carcinoma
Evaluation and treatment of intracranial aneurysms using Dual Energy CT Angiography (DECTA) and rotational Digital Subtraction Angiography (DSA).
 and rotational Digital Subtraction Angiography (DSA).") Evaluation and treatment of intracranial aneurysms using Dual Energy CT Angiography (DECTA) and rotational Digital Subtraction Angiography (DSA). L. Testaverde, G. Pelle, A. Saltarelli, P. Rabuffi, M.
Evaluation and treatment of intracranial aneurysms using Dual Energy CT Angiography (DECTA) and rotational Digital Subtraction Angiography (DSA). L. Testaverde, G. Pelle, A. Saltarelli, P. Rabuffi, M.
Abdominal Solid Organ Injury
 Abdominal Solid Organ Injury 9th Nordic Trauma Radiology Course Aarhus, Denmark May 23-26, 2016 K.SHANMUGANATHAN M.D. ABDOMINAL TRAUMA OBJECTIVES Splenic injury Late arterial / early p-v phase imaging
Abdominal Solid Organ Injury 9th Nordic Trauma Radiology Course Aarhus, Denmark May 23-26, 2016 K.SHANMUGANATHAN M.D. ABDOMINAL TRAUMA OBJECTIVES Splenic injury Late arterial / early p-v phase imaging
Innovations in HCC Imaging: MDCT/MRI
 Innovations in HCC Imaging: MDCT/MRI Anthony E. Cheng, M.D. Cardinal MRI Center Cardinal Santos Medical Center, Wilson Street, San Juan Innovations in HCC Imaging: Goals/Objectives MDCT/MRI Learn the diagnostic
Innovations in HCC Imaging: MDCT/MRI Anthony E. Cheng, M.D. Cardinal MRI Center Cardinal Santos Medical Center, Wilson Street, San Juan Innovations in HCC Imaging: Goals/Objectives MDCT/MRI Learn the diagnostic
Computed tomographic pulmonary angiography procedures: Contrast media dilution from the venous to the systemic circulation
 Computed tomographic pulmonary angiography procedures: Contrast media dilution from the venous to the systemic circulation Petter Bugge Askeland Project thesis at the Faculty of Medicine UNIVERSITETET
Computed tomographic pulmonary angiography procedures: Contrast media dilution from the venous to the systemic circulation Petter Bugge Askeland Project thesis at the Faculty of Medicine UNIVERSITETET
Abdominal Solid Organ Injury
 Abdominal Solid Organ Injury 8 th Nordic Course Stockholm, Sweden May 19-22, 2014 K.SHANMUGANATHAN M.D. ABDOMINAL TRAUMA OBJECTIVES Splenic injury Late arterial / early p-v phase imaging Liver injury Blunt
Abdominal Solid Organ Injury 8 th Nordic Course Stockholm, Sweden May 19-22, 2014 K.SHANMUGANATHAN M.D. ABDOMINAL TRAUMA OBJECTIVES Splenic injury Late arterial / early p-v phase imaging Liver injury Blunt
Comparison of multidetector-row computed tomography findings of IgG4-related sclerosing cholangitis and cholangiocarcinoma
 Comparison of multidetector-row computed tomography findings of IgG4-related sclerosing cholangitis and cholangiocarcinoma Poster No.: C-0245 Congress: ECR 2014 Type: Scientific Exhibit Authors: M. Yata,
Comparison of multidetector-row computed tomography findings of IgG4-related sclerosing cholangitis and cholangiocarcinoma Poster No.: C-0245 Congress: ECR 2014 Type: Scientific Exhibit Authors: M. Yata,
Ultralow Dose Chest CT with MBIR
 Ultralow Dose Chest CT with MBIR Ella A. Kazerooni, M.D. Professor & Director Cardiothoracic Radiology Associate Chair for Clinical Affairs University of Michigan Disclosures Consultant: GE Healthcare
Ultralow Dose Chest CT with MBIR Ella A. Kazerooni, M.D. Professor & Director Cardiothoracic Radiology Associate Chair for Clinical Affairs University of Michigan Disclosures Consultant: GE Healthcare
CT Urography. Bladder. Stuart G. Silverman, M.D.
 CT Urography Stuart G. Silverman, M.D. Professor of Radiology Harvard Medical School Director, Abdominal Imaging and Intervention Brigham and Women s Hospital Bladder Boston, MA CT Urography Stuart G.
CT Urography Stuart G. Silverman, M.D. Professor of Radiology Harvard Medical School Director, Abdominal Imaging and Intervention Brigham and Women s Hospital Bladder Boston, MA CT Urography Stuart G.
ECG Gated CT Aorta in Transcatheter Aortic Valve Implantation
 ECG Gated CT Aorta in Transcatheter Aortic Valve Implantation Poster No.: C-2014 Congress: ECR 2014 Type: Educational Exhibit Authors: M. A. Ottesen; Oslo/NO Keywords: Cardiac, Arteries / Aorta, CT, CT-Angiography,
ECG Gated CT Aorta in Transcatheter Aortic Valve Implantation Poster No.: C-2014 Congress: ECR 2014 Type: Educational Exhibit Authors: M. A. Ottesen; Oslo/NO Keywords: Cardiac, Arteries / Aorta, CT, CT-Angiography,
Pictorial Essay. Multidetector CT of the Pancreas and Bile Duct System: Value of Curved Planar Reformations
 Downloaded from www.ajronline.org by 46.3.207.229 on 02/03/18 from IP address 46.3.207.229. Copyright RRS. For personal use only; all rights reserved n important feature distinguishing multidetector CT
Downloaded from www.ajronline.org by 46.3.207.229 on 02/03/18 from IP address 46.3.207.229. Copyright RRS. For personal use only; all rights reserved n important feature distinguishing multidetector CT
128-slice dual-source CT coronary angiography using highpitch scan protocols in 102 patients
 128-slice dual-source CT coronary angiography using highpitch scan protocols in 102 patients Poster No.: C-0634 Congress: ECR 2010 Type: Scientific Exhibit Topic: Cardiac Authors: Y. H. Choe, J. W. Lee,
128-slice dual-source CT coronary angiography using highpitch scan protocols in 102 patients Poster No.: C-0634 Congress: ECR 2010 Type: Scientific Exhibit Topic: Cardiac Authors: Y. H. Choe, J. W. Lee,
CT Low Dose Lung Cancer Screening. Part I. Journey to LDCT LCS Program
 CT Low Dose Lung Cancer Screening Part I Journey to LDCT LCS Program Paul Johnson, M.S., DABHP, DABR Cleveland Clinic September 26, 2015 Lung Caner is No. 1 In Cancer Related Death In The United States
CT Low Dose Lung Cancer Screening Part I Journey to LDCT LCS Program Paul Johnson, M.S., DABHP, DABR Cleveland Clinic September 26, 2015 Lung Caner is No. 1 In Cancer Related Death In The United States
Dual Energy CT of the Liver
 34th Annual Course October 2011 Washington, DC Dual Energy CT of the Liver Vassilios Raptopoulos, MD Beth Israel Deaconess Medical Center Harvard Medical School Dual Energy CT (DECT) Different materials
34th Annual Course October 2011 Washington, DC Dual Energy CT of the Liver Vassilios Raptopoulos, MD Beth Israel Deaconess Medical Center Harvard Medical School Dual Energy CT (DECT) Different materials
B-Flow, Power Doppler and Color Doppler Ultrasound in the Assessment of Carotid Stenosis: Comparison with 64-MD-CT Angiography
 Med. J. Cairo Univ., Vol. 85, No. 2, March: 805-809, 2017 www.medicaljournalofcairouniversity.net B-Flow, Power Doppler and Color Doppler Ultrasound in the Assessment of Carotid Stenosis: Comparison with
Med. J. Cairo Univ., Vol. 85, No. 2, March: 805-809, 2017 www.medicaljournalofcairouniversity.net B-Flow, Power Doppler and Color Doppler Ultrasound in the Assessment of Carotid Stenosis: Comparison with
Les Outils Cliniques de Demain en Scanner Cardiaque. Cardiaque Status en ECR 2018 From Diagnosis to Prognosis
 ECR 2018 From Diagnosis to Prognosis ECR 2018 From Diagnosis to Prognosis Thursday, March 1, 2018/08:30-10:00/Room N Les Outils Cliniques de Demain en Scanner Cardiaque Cardiaque Status en 2018 Rodrigo
ECR 2018 From Diagnosis to Prognosis ECR 2018 From Diagnosis to Prognosis Thursday, March 1, 2018/08:30-10:00/Room N Les Outils Cliniques de Demain en Scanner Cardiaque Cardiaque Status en 2018 Rodrigo
American College of Radiology CT Accreditation Program. Testing Instructions
 American College of Radiology CT Accreditation Program Testing Instructions (Revised January 6, 2017) This guide provides all of the instructions necessary for clinical tests, phantom tests and general
American College of Radiology CT Accreditation Program Testing Instructions (Revised January 6, 2017) This guide provides all of the instructions necessary for clinical tests, phantom tests and general
THE TUFFEST STUFF CT REGISTRY REVIEW Live Lecture Seminar SUNDAY CURRICULUM
 A. INJECTION TECHNIQUES a. Drug administration routes i. Oral ii. Buccal iii. Topical iv. Rectal v. Parenteral b. Injection techniques i. Hand ii. Mechanical injector c. Injection parameters i. Catheters
A. INJECTION TECHNIQUES a. Drug administration routes i. Oral ii. Buccal iii. Topical iv. Rectal v. Parenteral b. Injection techniques i. Hand ii. Mechanical injector c. Injection parameters i. Catheters
Pediatric chest HRCT using the idose 4 Hybrid Iterative Reconstruction Algorithm: Which idose level to choose?
 Journal of Physics: Conference Series PAPER OPEN ACCESS Pediatric chest HRCT using the idose 4 Hybrid Iterative Reconstruction Algorithm: Which idose level to choose? To cite this article: M Smarda et
Journal of Physics: Conference Series PAPER OPEN ACCESS Pediatric chest HRCT using the idose 4 Hybrid Iterative Reconstruction Algorithm: Which idose level to choose? To cite this article: M Smarda et
Alessandro Albonico Philips
 Alessandro Albonico Philips Alessandro.albonico@philips.com Noise (Standard Deviation in HU) Virtually noise-free Characteristic of a true knowledge-based IR 80 70 Standard Recon idose4 Level6 1 mm Slice
Alessandro Albonico Philips Alessandro.albonico@philips.com Noise (Standard Deviation in HU) Virtually noise-free Characteristic of a true knowledge-based IR 80 70 Standard Recon idose4 Level6 1 mm Slice
B. CT protocols for the spine
 B. CT protocols for the spine Poster No.: A-003 Congress: ECR 2010 Type: Invited Speaker Topic: Neuro Authors: B. Tins; Oswestry/UK Keywords: CT, spine, diagnostic imaging protocol DOI: 10.1594/ecr2010/A-003
B. CT protocols for the spine Poster No.: A-003 Congress: ECR 2010 Type: Invited Speaker Topic: Neuro Authors: B. Tins; Oswestry/UK Keywords: CT, spine, diagnostic imaging protocol DOI: 10.1594/ecr2010/A-003
Pulmonary Embolism. Thoracic radiologist Helena Lauri
 Pulmonary Embolism Thoracic radiologist Helena Lauri 8.5.2017 Statistics 1-2 out of 1000 adults annually are diagnosed with deep vein thrombosis (DVT) and/or pulmonary embolism (PE) About half of patients
Pulmonary Embolism Thoracic radiologist Helena Lauri 8.5.2017 Statistics 1-2 out of 1000 adults annually are diagnosed with deep vein thrombosis (DVT) and/or pulmonary embolism (PE) About half of patients
Three-dimensional CT angiography of the canine hepatic vasculature
 J. Vet. Sci. (2008), 9(4), 407 413 JOURNAL OF Veterinary Science Three-dimensional CT angiography of the canine hepatic vasculature Yucheol Jeong, Changyun Lim, Sunkyoung Oh, Joohyun Jung, Jinhwa Chang,
J. Vet. Sci. (2008), 9(4), 407 413 JOURNAL OF Veterinary Science Three-dimensional CT angiography of the canine hepatic vasculature Yucheol Jeong, Changyun Lim, Sunkyoung Oh, Joohyun Jung, Jinhwa Chang,