Clinical Study Stereotactic Body Radiotherapy as an Alternative to Brachytherapy in Gynecologic Cancer
|
|
|
- Moses Cole
- 5 years ago
- Views:
Transcription
1 BioMed Research International Volume 2013, Article ID , 6 pages Clinical Study Stereotactic Body Radiotherapy as an Alternative to Brachytherapy in Gynecologic Cancer Gregory J. Kubicek, 1 Jinyu Xue, 1 Qianyi Xu, 1 Sucha O. Asbell, 1 Leslie Hughes, 1 Noel Kramer, 1 Ashraf Youssef, 1 Yan Chen, 1 James Aikens, 2 Howard Saul, 3 Niraj Pahlajani, 1 and Tamara LaCouture 1 1 Department of Radiation Oncology, Cooper University Hospital, One Cooper Plaza, Camden, NJ 08103, USA 2 Department of Gynecology, Cooper University Hospital, One Cooper Plaza, Camden, NJ 08103, USA 3 Department of Gynecology, Center for Cancer and Hematologic Disease, Marlton, NJ 08003, USA Correspondence should be addressed to Gregory J. Kubicek; greg.kubicek@gmail.com Received 18 April 2013; Accepted 12 July 2013 Academic Editor: Eng-Yen Huang Copyright 2013 Gregory J. Kubicek et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. Introduction. Brachytherapy plays a key role in the treatment of many gynecologic cancers. However, some patients are unable to tolerate brachytherapy for medical or other reasons. For these patients, stereotactic body radiotherapy (SBRT) offers an alternative form of treatment. Methods. Retrospective review of patients prospectively collected on SBRT database is conducted. A total of 11 gynecologic patients who could not have brachytherapy received SBRT for treatment of their malignancies. Five patients have been candidates for interstitial brachytherapy, and six have required tandem and brachytherapy. Median SBRT dose was 25 Gy in five fractions. Results. At last followup, eight patients were alive, and three patients had died of progressive disease. One patient had a local recurrence. Median followup for surviving patients was 420 days (median followup for all patients was 120 days). Two patients had acute toxicity (G2 dysuria and G2 GI), and one patient had late toxicity (G3 GI, rectal bleeding requiring cauterization). Conclusions. Our data show acceptable toxicity and outcome for gynecologic patients treated with SBRT who were unable to receive a brachytherapy boost. This treatment modality should be further evaluated in a phase II study. 1. Introduction Gynecologic malignancies, mostly consisting of endometrial and cervical cancers, remain common cancers in the United States. For locally advanced cervical cancer, the standard treatment combines chemotherapy (CTX) along with conventional external-beam radiation therapy (EBRT) and a brachytherapy boost (BB) [1 5]. BB is also used in endometrial cancer, in early-stage disease as the sole treatment, and in unresectable and recurrent disease in combination with EBRT [6]. BB is a valuable treatment option because it allows forahighdosetothetumorwhilesparingthenearbynormal structures. To treat to a tumoricidal dose using EBRT alone wouldleadtosignificantdosetonearbynormalstructures (mainly rectum, small bowel, and bladder), which would entail a high likelihood of acute and late toxicity. BB is ideal for treatment of gynecologic cancers because it allows the radioactivesourcetobeplacedveryclosetothetargetwhich receives full dose, but because of the inverse-square law (the radiation dose decreases exponentially with distance; so as distance goes from x to 2x, the radiation dose decreases from y to 0.25y), the nearby normal tissues receive a much lower dose; thus, BB allows for maximal tumor dose and maximal normal tissue sparing [5, 6]. WhileBBremainsthestandardtreatmentoptionfor many gynecologic cancers, there are some patients who are not candidates for this treatment. Patients with comorbid conditions may not be able to tolerate BB, especially an interstitial implant. Also, for patients with unfavorable anatomy, it may not be possible to place BB even with assistance from gynecology oncologists. One possible alternative to BB is stereotactic body radiotherapy (SBRT), which entails high doses of external radiation delivered in a very conformal
2 2 BioMed Research International fashion. While SBRT is commonly used in medically unresectable early-stage lung cancer and has a growing use in other pathologies, there are very little data regarding the role of SBRT used in place of BB. Several retrospective clinical reports [7 12] and retrospective dosimetric reports [13] haveshownthatsbrt appears to be a reasonable treatment option for patients unabletoreceiveabb.haasetal.[7] reported on six cervical cancer patients who had anatomic or medical conditions that precluded BB using tandems and s. The patients received an SBRT boost to the cervix instead, using the doses of 20 Gy in five fractions (five patients) and 19.5 Gy in three fractions (one patient). With a median followup of 14 months, there were no reported local failures and no toxicities from thesbrtboost.mollaetal.[8]reportedon16patients(nine endometrial and seven cervical) who had an SBRT boost to high-risk areas (14 Gy in two fractions for operated patients and 20 Gy in five fractions for nonoperated ones). With a median followup of 12.6 months, there was one patient with a central pelvic recurrence and one patient with late grade- 3 rectal toxicity. A retrospective comparative analysis [12] of BB and SBRT plans found that SBRT plans had better target coverage and better dose distributions to normal structures except for bone marrow. In order to increase the knowledge pool regarding SBRT as an alternate to BB in certain patients, we are reporting our institution s experience of this treatment modality. 2. Methods Patients in this study were collected using an IRB-approved prospective radiosurgery database. Clinical information not contained in the database was retrospectively acquired. Eligibility criteria for the review included gynecologic patients whoreceivedsbrtbuthadbeenreferredandhadclinical indications for BB. All patients were initially evaluated and had been recommended to undergo a BB, and for medical or other reasons, they were unable to complete the BB and were thus treated with SBRT (Table 1). All patients were evaluated by both gynecology-oncology and radiation oncology; for patients that needed Smit s Sleeve placement, this was performed by the gynecology-oncologist. A total of 11 patients met the eligibility criteria for this review. Median age was 62 years (range: years). Seven patients had cervical cancer, two patients had endometrial cancer, and two patients had vaginal cancer. Histology was squamous-cell carcinoma in eight patients, adenocarcinoma in two patients, and carcinosarcoma in one patient. Patients had locally advanced (seven) or recurrent cancers (four patients) but were not metastatic. All patients had conventional externalbeam radiation to the pelvis prior to SBRT, three in the form of IMRT and eight in the form of 3D-CRT; dose range for previous EBRT was 45 to 50.4 Gy. Three patients had both EBRT and BB prior to SBRT, two patients had completed EBRT and BB and had local recurrence 1.4 and 1.1 years later, and the other patient had two HDR treatments, but the patient s Smit s Sleeve became misplaced after the second treatment, and when it was not able to be replaced, the patient went on to have SBRT for the remaining treatments. Three patients had surgery (hysterectomy) in addition to previous EBRT; indication for surgery in these patients was for recurrent disease. The initial consult note and progress notes were reviewed for the treatment recommendations; in all patients, a BB was recommended. The types of BB that were indicated included tandem and BB in six patients and interstitial BB in five patients. Reasons for not being able to treat with BB are listed in Table 1. Prior to SBRT, all patients had gold fiducial markers implanted for SBRT tracking. It was recommended that four gold-seed fiducial markers be placed, either into the cervix orintothegrosstumorifvisualized.ctscanfortreatment planning was performed without contrast using 1.25 mm slices. Patients were instructed to have a low-residue meal prior to simulation and were coached to have a consistent fluid intake on the day of simulation and the daily treatments to maintain a regular bladder filling rate throughout the treatment. An MRI of the pelvis with contrast was obtained andfusedtotheplanningctscanforbettervisualization of the cervix and gross disease; MRI series included T2 weighting with contrast, with and without fat saturation. Prior to SBRT, 7 patients had gross disease present visible on MRI or physical exam. SBRT target consisted of the gross tumor volume (GTV) in patients with gross disease present prior to SBRT and also a clinical target volume (CTV) for areas thought to be at high risk for residual disease. GTV consisted of gross disease noted on the MRI and physical exam. The CTV would include any extracervical disease at the time of the MRI and physical exam. CTV would also include the entire cervix for patients with cervical cancer with an intact uterus. The CTV was uniformly expanded by 5 mm to create a planning targetvolume(ptv)toaccountforaset-uperrorincluding rotation. In patients with small intestine or other critical structures adjacent to targets, the PTV was subtracted from theorgansatrisktodecreasedosetotheorgansatrisk.see Table 2. SBRT was delivered in five fractions using CyberKnife (Accuray Incorporated, Sunnyvale, CA, USA) with multiplan planning system version Numerous noncoplanar beams using 6 MV photons were used for each treatment. Target tracking was performed via the CyberKnife s realtime tracking algorithm; synchrony (respiratory motion software) was not used. CyberKnife tracking, has the ability to track movements (with aid of gold fiducials), and this ability is critical since the cervix is prone to movement [14]. Treatments were delivered every other day, and we feel that normal tissues such as small bowel would tolerate everyother-day better than every-day treatments; every-other-day treatments are also similar to what is used in BB using HDR. Patients were instructed to use Simethicone (Himalaya Drug Company, Bangalore, India) during every day of treatment to reduce bowel distension. None of the patients received chemotherapy concurrent with SBRT, although chemotherapy was typically delivered with EBRT. Treatments were delivered to an isodose line that was aimed for a compromise of target coverage and sparing of the organs at risk.
3 BioMed Research International 3 Patient # Diagnosis Stage Histology Table 1: Patient characteristics. Recommended implant Reasonthatimplantcouldnotbeperformed 1 Cervical Recurrent Scc Interstitial Size and location 2 Cervical Recurrent Carcinosarcoma Interstitial Bleeding 3 Endometrial Recurrent Adenocarcinoma Interstitial Difficulty with interstitial, short endocervix makes tandem difficult 4 Vaginal T2 Scc Interstitial Proximity to bladder and bowel 5 Vaginal T2 Scc Interstitial Difficulty w visualization of tumor 6 Cervical IIIb Scc Comorbid conditions 7 Cervical IIIb Scc Unable to place Smits Sleeve 8 Cervical IIIb Scc Unable to place sleeve 9 Cervical IIIb Scc SmitsSleevebecamemisplaced 10 Cervical Recurrent Scc Unable to place sleeve 11 Endometrial T2N1 Adenocarcinoma Smits Sleeve perforation through uterus Scc: squamous cell carcinoma. Structure GTV CTV PTV Rectum Bladder Smallbowel Table 2: Target and OAR definitions. Definition Gross tumor as visualized on MRI (T2) and physical exam Entire cervix for most patients, including extracervical disease if present on pre-sbrt MRI CTV plus expansion of 5 mm (using less of an expansion if adjacent to organs at risk) Entire rectum, superior limit will be rectosigmoid junction Entire bladder and contents Bowelloopsupto2cmabovetarget Normal tissues were contoured including large bowel, small bowel, femoral heads, sigmoid colon, rectum, bladder, and skin. See Table 2 for more information regarding contouring specifics. Note that the entire organ was contoured asopposedtojusttheorganwall.forpatientsthathavehad previous pelvic radiation to 45 to 50.4 Gy, the point dose limit to the sigmoid colon, rectum, and small bowel was 21 Gy; and the bladder dose limit was 24 Gy. A small volume was allowed to exceed this dose if the normal structures abutted the tumor, in which case 1-2 cc were allowed higher doses up to the target dose. After completion of treatment, patients were followed by gynecology oncology as well as radiation oncology, and patients were typically seen 4 weeks after completion of treatment and then every 2 months for the first year; followup visit would include pelvic exam. Imaging (typically MRI) was done at 3 months posttreatment. Toxicity was physicianscored based on CTCAE 4.0. Oncologic outcomes at followup were based on combination of both the physical exam and the followup imaging. 3. Results 3.1. Radiotherapy Treatment. Ten patients had five prescribed fractions. One patient who had completed two fractions of HDR BB and then had Smit s Sleeve malposition received three fractions of SBRT. SBRT boost was completed in 10 patients. One patient suffered a stroke after the first fraction and had a subsequent decline in performance status, necessitating the treatment to be discontinued. The stroke was not felt to be related to SBRT. This patient s dosimetric information was not included in the analysis. Median SBRT dose for patients completing the treatment was 25 Gy (range: Gy); the median dose per fraction was 5.0 Gy (range: Gy). Treatments were prescribed to themedian61%isodoseline(range:51% 81%).Mediantreatment volume was 9,163 cc (range: 1,665 35,740 cc). Median PTV coverage was 88% (range: 71% 94%), and median GTV coverage was 96.5% (range: 90% 97.6%). Median PTV conformality index was 1.5 (range: ), where conformality index is defined as treated volume divided by PTV. Maximum rectal point dose ranged from 20.8 to 32.6 Gy (median: 23.8 Gy), median rectal dose to 1 cc was 19.6 Gy (range: 18.2 to27.5gy),andmedianrectaldoseto2ccwas19.3gy(range: Gy). Maximum bladder point dose ranged from Gy (median: 25.7 Gy), median bladder dose to 1 cc was 20.7 Gy (range: Gy), and median bladder dose to 2 cc was 19 Gy (range: Gy); see Table 3. A typical SBRT plan is seen in Figure 1. Onepatient had SBRT after two HDR BB (Smit s Sleeve shifted out of position after the second BB). On comparing her BB and
 alpha/beta 10 SBRT dose equivalent (2 Gy/fx) alphabeta3 1 45 + 30 Gy HDR 254485.7 27.5/5 35.52083 46.75 2 45 9893.03 25/5 31.25 40 3 50.4 34818.04 25/5 31.")
4 4 BioMed Research International Patient Previous RT (EBRT and HDR) CTV volume (mm 3 ) Table 3: Treatment characteristics. SBRT dose/fx SBRT dose equivalent (2 Gy/fx) alpha/beta 10 SBRT dose equivalent (2 Gy/fx) alphabeta Gy HDR / / / / / / / / HDR / HDR / / cancer and died of progressive disease; the other had locally advanced cervical cancer and had a stroke during therapy and subsequently went on to hospice care without completing the entire course of treatment. Of the eight surviving patients, one (patient no. 2) had a local recurrence 3.5 years after completion of SBRT (recurrence took place in cervical stump in the region of the previous SBRT). This patient was treated with surgical exoneration and was disease-free after salvage surgery. All of the other patients were disease-free (both local and distant) at last followup. Figure 1: Sample SBRT plan. Typical SBRT plan, patient treated to 25 Gy in five fractions. Bladder, CTV, and rectal contours are shown. Isodose lines include prescription isodose line (75%), pink (50%), and light blue (20%). SBRT treatments, maximum normal-tissue point doses were lower for the BB. For this patient, maximum dose per fraction to bladder was 5.8 Gy with SBRT versus 4.45 Gy with BB; for rectum, 5.6 Gy with SBRT versus 5.0 with BB; and for small bowel, 5.3 Gy with SBRT versus 2.8 Gy with BB. Doses to 1 and 2 cc of bladder were 5.2 and 4.9 Gy with SBRT and 5.3 and4.7withbb,respectively.dosesto1and2ccofrectum were 4.9 and 4.5 Gy with SBRT and 4.7 and 4.2 Gy with BB, respectively. Comparison between SBRT and HDR plans is shown in Figure 2. The biologically equivalent dose (BED) in terms of equivalent doses given at 2 Gy per day (EQ2) was calculated using the linear quadratic (LQ) equation [15]. The α/β ratio was taken to be 10 Gy for tumor effects and 3 Gy for late effects. Median EQ2 for the tumor was 31.3 Gy (range: Gy) for the entire group, and median EQ2 for late effects on normal tissues was 40 Gy (range: Gy), Table Oncologic Outcome. At last followup, eight patients were alive. Median followup for all patients was 120 days, and median followup for surviving patients was 14 months. Of the three patients who died, two had recurrent cervical 3.3. Toxicity. DuringtheSBRTboost,twopatientswerenoted to have acute toxicity (grade-2 GU and grade-2 GI, resp.). There was no grade-3 or greater toxicities during the SBRT or within 90 days after SBRT. One patient (patient no. 8) was noted to have late toxicity one year from the completion of SBRT, in the form of mild GI bleeding, and underwent cauterization of the rectal vessels, which resolved the bleeding (GI grade-3 toxicity). The patient who had GI Grade 3 toxicity had a maximum point dose to rectum of 24 Gy, 1 cc dose of 19.4, 2 cc dose of 18.6, and a mean rectal dose of 6.7 Gy, all of which were around the median for all patients treated. There were no other reported late toxicities. 4. Discussion Inthetreatmentoflocallyadvancedandrecurrentgynecologic cancers, chemoradiotherapy and brachytherapy boost (either ring and tandem or interstitial) remain the standard ofcare.thisresultsingooddiseasecontrolandacceptable toxicity. Gynecologic Oncology Group (GOG) Trial 120 [1] reported 60% overall survival at 5 years, 22% local progression,andalatetoxicityrate(grade3or4)of1.7%forpatients treated with chemoradiotherapy (including intracavity BB) with a median followup of 35 months. With regard to patients treated with interstitial BB, Pinn-Bingham et al. [16] have reported on 116 patients with locally advanced cervical cancer who were not candidates for intracavity BB. Following treatment with external-beam radiation and interstitial BB,

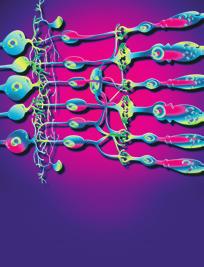
![For gynecologic patientss both intracavity and interstitial BB have good outcomes and are important components of the standard treatment for these patients [1 6, 16, 17].](/docs-images/89/99999887/images/5-1.jpg "However, some patients are unable to receive BB, because of either unfavorable anatomy or comorbid conditions. For these patients, treatment options become more limited.")
5 BioMed Research International 5 (a) (b) Figure 2: Comparison of SBRT (a) and BB (b). Comparison of target dose using BB and SBRT for the same patient. they found 85.3% locoregional control and 13% late toxicity rates. For gynecologic patientss both intracavity and interstitial BB have good outcomes and are important components of the standard treatment for these patients [1 6, 16, 17]. However, some patients are unable to receive BB, because of either unfavorable anatomy or comorbid conditions. For these patients, treatment options become more limited. Conventional EBRT has been tried in place of BB with overall poor results. Barraclough et al. [18] have reported on 44 patients treated with external-beam boost instead of BB ( technical limitations was listed as the reason for not providing BB in 73% of patients) and found a 48% recurrence rate with a median followup of 2.3 years. While this treatment is likely better than no boost at all, the importance of a high recurrence rate of the disease is secondary to dose limitations of normal pelvic tissue with conventional EBRT. Another possible option for patients who are not BB candidates is SBRT. SBRT has advantages over conventional radiotherapy in being able to deliver higher doses while minimizing normal tissue radiation exposure. This allows the tumor to receive a higher biologically equivalent dose than with conventional radiation. Our results for SBRT showed good local control and a medically acceptable toxicity. Among the surviving patients (nine patients), only one had a local recurrence. Two patients with recurrent disease had persistent disease after SBRT, and they continued to have disease progression despite SBRT, and they subsequently died from the disease. Our toxicity results were also determined as tolerable with only one grade-3 toxicity (grade-3 GI) reported. The data on this topic are limited to a few retrospective series, and our results mirror the available literature on SBRT in place of BB. Haas et al. [7] havereportedonsix cervical cancer patients treated with SBRT boost (median of 20 Gy in five fractions) after CRT. Their series did not find any local recurrences and did not report any toxicity with a median followup of 14 months. Molla et al. [8] have reported on 16 patients (nine endometrial and seven cervical cancers, while 15 patients had a hysterectomy) treated with SBRT (14 Gy in two fractions for postoperative and 20 Gy in five fractions for nonoperated patients) instead of BB. This report found one patient with late rectal bleeding (GI grade-3 toxicity) and 1 recurrence with a median followup of 12.6 months. Guckenberger et al. [12] have reported on 19 patients with recurrent cervical or endometrial cancer, who had pelvic sidewall involvement or large tumors not amenable to BB. SBRT consisted of 15 Gy in three fractions, withamedianfollowupof22months.three-yearoverall survival was 34%, and local control was 81%; two patients had grade-4 intestinovaginal fistulae, and one had a grade-4 small bowel ileus. Kemmerer et al. [10] reported on 11 patients with stage unresectable I-III endometrial cancer treated with SBRTboostof30Gyin5fractions;theyfoundnolatetoxicity and 55% local-regional control. Higginson et al. [11] reported on a heterogeneous group of 5 with a range of SBRT doses, one of whom had late grade-3 rectal bleeding after receiving 20 Gy in 5 fractions. All of the data to date are retrospective and heterogeneous butsometrendsdoemerge.firstofall,thereappearstobe good local control with this treatment modality. Secondly, the majorlatetoxicityseeninourseriesandthatofseveralothers [8, 11]havebeenlateGItoxicity,whilethedatathusfardonot allow a precise calculation of dose tolerance for the rectum; it is important that this toxicity be discussed with patients and that there be attempts to constrain dose to the rectum. At this point, it is not standard of practice to replace BB with SBRT in patients who are BB candidates. However, we have shown that, when BB is not an option, SBRT can be a safe and effective treatment modality. Further work in this area can be used to better define SBRT dose and to prospectively collect toxicity and outcome information on this patient subset. Our current treatment protocol is to treat to 25 Gy in five fractions using dose constraints as described previously. 5. Conclusions Brachytherapy implants remain the standard of care as a method to deliver radiation boost for gynecological cancers.
6 6 BioMed Research International However,forpatientsunabletohaveabrachytherapyprocedure, we found acceptable toxicity and outcome with SBRT. This treatment modality should be further evaluated in a phaseiistudy,withdoseandfractionationof25gyin5 fractions, and close adherence to organ at risk limits. Conflict of Interests The authors declare that they have no conflict of interests. References [1] M. Morris, P. J. Eifel, J. Lu et al., Pelvic radiation with concurrent chemotherapy compared with pelvic and paraaortic radiation for high-risk cervical cancer, The New England Medicine, vol. 340, no. 15, pp , [2]P.G.Rose,B.N.Bundy,E.B.Watkinsetal., Concurrent cisplatin-based radiotherapy and chemotherapy for locally advanced cervical cancer, The New England Medicine, vol.340,no.15,pp ,1999. [3] P. J. Eifel, K. Winter, M. Morris et al., Pelvic irradiation with concurrent chemotherapy versus pelvic and para-aortic irradiation for high-risk cervical cancer: an update of radiation therapyoncologygrouptrial(rtog)90-01, Clinical Oncology,vol.22,no.5,pp ,2004. [4] T. E. Schefter, K. Winter, J. S. Kwon et al., A phase II study of Bevacizumab in combination with definitive radiotherapy and cisplatin chemotherapy in untreated patients with locally advanced cervical carcinoma: preliminary results of RTOG 0417, International Radiation Oncology, Biology, Physics,vol.83,no.4,pp ,2012. [5] A.N.Viswanathan,B.Thomadsen,andAmericanBrachytherapy Society Cervical Cancer Recommendations Committee, American brachytherapy society consensus guidelines for locally advanced carcinoma of the cervix part I: general principles, Brachytherapy, vol. 11,no. 1, pp , [6] W. Small Jr., S. Beriwal, D. J. Demanes et al., American brachytherapy society consensus guidelines for adjuvant vaginal cuff brachytherapy after hysterectomy, Brachytherapy, vol. 11,no.1,pp.58 67,2012. [7] J.A.Haas,M.R.Witten,O.Clancey,K.Episcopia,D.Accordino, and E. Chalas, CyberKnife boost for patients with cervical cancer unable to undergo brachytherapy, Frontiers in Oncology, vol. 2, article 25, [8] M.Molla,L.Escude,P.Nouetetal., Fractionatedstereotactic radiotherapy boost for gynecologic tumors: an alternative to brachytherapy? International Radiation Oncology, Biology, Physics, vol. 62, no. 1, pp , [9] C. H. Hsieh, M. C. Wei, Y. P. Hsu et al., Should helical tomotherapy replace brachy therapy for cervical cancer? Case report, BMC Cancer, vol. 10, article 637, [10] E. Kemmerer, E. Hernandez, J. S. Ferriss et al., Use of imageguided stereotactic body radiation therapy in Lieu of intracavitary brachytherapy for the treatment of inoperable endometrial neoplasia, International Radiation Oncology, Biology, Physics,vol.85,no.1,pp ,2013. [11] D. S. Higginson, D. E. Morris, E. L. Jones, D. Clarke-Pearson, and M. A. Varia, Stereotactic body radiotherapy (SBRT): technological innovation and application in gynecologic oncology, Gynecologic Oncology,vol.120,no.3,pp ,2011. [12] M. Guckenberger, J. Bachmann, J. Wulf et al., Stereotactic body radiotherapy for local boost irradiation in unfavourable locally recurrent gynaecological cancer, Radiotherapy and Oncology, vol.94,no.1,pp.53 59,2010. [13] M. Cengiz, A. Dogan, G. Ozyigit et al., Comparison of intracavitary brachytherapy and stereotactic body radiotherapy dose distribution for cervical cancer, Brachytherapy,vol.11,no. 2, pp , [14] N. H. Haripotepornkul, S. K. Nath, D. Scanderbeg, C. Saenz, and C. M. Yashar, Evaluation of intra- and inter-fraction movement of the cervix during intensity modulated radiation therapy, Radiotherapy and Oncology, vol. 98, no. 3, pp , [15] S. Nag and N. Gupta, A simple method of obtaining equivalent doses for use in HDR brachytherapy, International Radiation Oncology, Biology, Physics,vol.46,no.2,pp , [16] M. Pinn-Bingham, A. A. Puthawala, A. M. Syed et al., Outcomes of high-dose-rate interstitial brachytherapy in the treatment of locally advanced cervical cancer: long-term results, International Radiation Oncology, Biology, Physics, vol.85,no.3,pp ,2013. [17] S. Beriwal, A. Bhatnagar, D. E. Heron et al., High-doserate interstitial brachytherapy for gynecologic malignancies, Brachytherapy,vol.5,no.4,pp ,2006. [18] L. H. Barraclough, R. Swindell, J. E. Livsey, R. D. Hunter, and S. E. Davidson, External beam boost for cancer of the cervix uteri when intracavitary therapy cannot be performed, International JournalofRadiationOncology,Biology,Physics,vol.71,no.3,pp , 2008.
















7 MEDIATORS of INFLAMMATION The Scientific World Journal Gastroenterology Research and Practice Diabetes Research International Endocrinology Immunology Research Disease Markers Submit your manuscripts at BioMed Research International PPAR Research Obesity Ophthalmology Evidence-Based Complementary and Alternative Medicine Stem Cells International Oncology Parkinson s Disease Computational and Mathematical Methods in Medicine AIDS Behavioural Neurology Research and Treatment Oxidative Medicine and Cellular Longevity
Dosimetric Analysis of 3DCRT or IMRT with Vaginal-cuff Brachytherapy (VCB) for Gynaecological Cancer
 for Gynaecological Cancer") Dosimetric Analysis of 3DCRT or IMRT with Vaginal-cuff Brachytherapy (VCB) for Gynaecological Cancer Tan Chek Wee 15 06 2016 National University Cancer Institute, Singapore Clinical Care Education Research
Dosimetric Analysis of 3DCRT or IMRT with Vaginal-cuff Brachytherapy (VCB) for Gynaecological Cancer Tan Chek Wee 15 06 2016 National University Cancer Institute, Singapore Clinical Care Education Research
PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES GYNECOLOGIC CANCER CERVIX
 PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES GYNECOLOGIC CANCER CERVIX Site Group: Gynecology Cervix Author: Dr. Stephane Laframboise 1. INTRODUCTION 3 2. PREVENTION 3 3. SCREENING AND
PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES GYNECOLOGIC CANCER CERVIX Site Group: Gynecology Cervix Author: Dr. Stephane Laframboise 1. INTRODUCTION 3 2. PREVENTION 3 3. SCREENING AND
IMRT - the physician s eye-view. Cinzia Iotti Department of Radiation Oncology S.Maria Nuova Hospital Reggio Emilia
 IMRT - the physician s eye-view Cinzia Iotti Department of Radiation Oncology S.Maria Nuova Hospital Reggio Emilia The goals of cancer therapy Local control Survival Functional status Quality of life Causes
IMRT - the physician s eye-view Cinzia Iotti Department of Radiation Oncology S.Maria Nuova Hospital Reggio Emilia The goals of cancer therapy Local control Survival Functional status Quality of life Causes
A Comparison of IMRT and VMAT Technique for the Treatment of Rectal Cancer
 A Comparison of IMRT and VMAT Technique for the Treatment of Rectal Cancer Tony Kin Ming Lam Radiation Planner Dr Patricia Lindsay, Radiation Physicist Dr John Kim, Radiation Oncologist Dr Kim Ann Ung,
A Comparison of IMRT and VMAT Technique for the Treatment of Rectal Cancer Tony Kin Ming Lam Radiation Planner Dr Patricia Lindsay, Radiation Physicist Dr John Kim, Radiation Oncologist Dr Kim Ann Ung,
INTRODUCTION PATIENT. J. Radiat. Res., 52, (2011)
") J. Radiat. Res., 52, 54 58 (2011) Regular Paper Intracavitary Combined with CT-guided Interstitial Brachytherapy for Locally Advanced Uterine Cervical Cancer: Introduction of the Technique and a Case Presentation
J. Radiat. Res., 52, 54 58 (2011) Regular Paper Intracavitary Combined with CT-guided Interstitial Brachytherapy for Locally Advanced Uterine Cervical Cancer: Introduction of the Technique and a Case Presentation
3D ANATOMY-BASED PLANNING OPTIMIZATION FOR HDR BRACHYTHERAPY OF CERVIX CANCER
 SAUDI JOURNAL OF OBSTETRICS AND GYNECOLOGY VOLUME 11 NO. 2 1430 H - 2009 G 3D ANATOMY-BASED PLANNING OPTIMIZATION FOR HDR BRACHYTHERAPY OF CERVIX CANCER DR YASIR BAHADUR 1, DR CAMELIA CONSTANTINESCU 2,
SAUDI JOURNAL OF OBSTETRICS AND GYNECOLOGY VOLUME 11 NO. 2 1430 H - 2009 G 3D ANATOMY-BASED PLANNING OPTIMIZATION FOR HDR BRACHYTHERAPY OF CERVIX CANCER DR YASIR BAHADUR 1, DR CAMELIA CONSTANTINESCU 2,
Enterprise Interest None
 Enterprise Interest None Cervical Cancer -Management of late stages ESP meeting Bilbao Spain 2018 Dr Mary McCormack PhD FRCR Consultant Clinical Oncologist University College Hospital London On behalf
Enterprise Interest None Cervical Cancer -Management of late stages ESP meeting Bilbao Spain 2018 Dr Mary McCormack PhD FRCR Consultant Clinical Oncologist University College Hospital London On behalf
Challenging Cases in Cervical Cancer: Parametrial Boosting. Beth Erickson, MD, FACR, FASTRO Medical College Wisconsin
 Challenging Cases in Cervical Cancer: Parametrial Boosting Beth Erickson, MD, FACR, FASTRO Medical College Wisconsin Disclosure Chart Rounds participant No COI Learning Objectives Discuss the challenges
Challenging Cases in Cervical Cancer: Parametrial Boosting Beth Erickson, MD, FACR, FASTRO Medical College Wisconsin Disclosure Chart Rounds participant No COI Learning Objectives Discuss the challenges
Jean Pouliot, PhD Professor and Vice Chair, Department of Radiation Oncology, Director of Physics Division
 IMRT / Tomo / VMAT / Cyberknife / HDR Brachytherapy: Jean Pouliot, PhD Professor and Vice Chair, Department of Radiation Oncology, Director of Physics Division Should Choices be Based on Dosimetric and
IMRT / Tomo / VMAT / Cyberknife / HDR Brachytherapy: Jean Pouliot, PhD Professor and Vice Chair, Department of Radiation Oncology, Director of Physics Division Should Choices be Based on Dosimetric and
Definitions. Brachytherapy in treatment of cancer. Implantation Techniques and Methods of Dose Specifications. Importance of Brachytherapy in GYN
 Implantation Techniques and Methods of Dose Specifications Brachytherapy Course Lecture V Krishna Reddy, MD, PhD Assistant Professor, Radiation Oncology Brachytherapy in treatment of cancer GYN Cervical
Implantation Techniques and Methods of Dose Specifications Brachytherapy Course Lecture V Krishna Reddy, MD, PhD Assistant Professor, Radiation Oncology Brachytherapy in treatment of cancer GYN Cervical
La Pianificazione e I Volumi di Trattamento
 TRATTAMENTI INTEGRATI NEL CARCINOMA DELLA VULVA La Pianificazione e I Volumi di Trattamento PAOLO MUTO Direttore UOC Radioterapia ISTITUTO NAZIONALE TUMORI IRCCS Fondazione Pascale di Napoli Minimize collateral
TRATTAMENTI INTEGRATI NEL CARCINOMA DELLA VULVA La Pianificazione e I Volumi di Trattamento PAOLO MUTO Direttore UOC Radioterapia ISTITUTO NAZIONALE TUMORI IRCCS Fondazione Pascale di Napoli Minimize collateral
Comparison of rectal and bladder ICRU point doses to the GEC ESTRO volumetric doses in Cervix cancer
 Comparison of rectal and bladder ICRU point doses to the GEC ESTRO volumetric doses in Cervix cancer Poster No.: RO-0049 Congress: RANZCR FRO 202 Type: Authors: Scientific Exhibit G. Govindarajulu, A.
Comparison of rectal and bladder ICRU point doses to the GEC ESTRO volumetric doses in Cervix cancer Poster No.: RO-0049 Congress: RANZCR FRO 202 Type: Authors: Scientific Exhibit G. Govindarajulu, A.
Interstitial Brachytherapy. Low dose rate brachytherapy. Brachytherapy alone cures some cervical cancer. Learning Objectives
 Interstitial Learning Objectives To discuss practical aspects of selection and insertion techniques for interstitial brachytherapy and their relation to clinical trials Akila Viswanathan, MD MPH Johns
Interstitial Learning Objectives To discuss practical aspects of selection and insertion techniques for interstitial brachytherapy and their relation to clinical trials Akila Viswanathan, MD MPH Johns
The Evolution of RT Techniques for Gynaecological Cancers in a developing country context
 The Evolution of RT Techniques for Gynaecological Cancers in a developing country context Hannah Simonds Stellenbosch University/ Tygerberg Academic Hospital ESMO Africa 2017 I have no disclosures External
The Evolution of RT Techniques for Gynaecological Cancers in a developing country context Hannah Simonds Stellenbosch University/ Tygerberg Academic Hospital ESMO Africa 2017 I have no disclosures External
ARROCase: Locally Advanced Endometrial Cancer
 ARROCase: Locally Advanced Endometrial Cancer Charles Vu, MD (PGY-3) Faculty Advisor: Peter Y. Chen, MD, FACR Beaumont Health (Royal Oak, MI) November 2016 Case 62yo female with a 3yr history of vaginal
ARROCase: Locally Advanced Endometrial Cancer Charles Vu, MD (PGY-3) Faculty Advisor: Peter Y. Chen, MD, FACR Beaumont Health (Royal Oak, MI) November 2016 Case 62yo female with a 3yr history of vaginal
 https://patient.varian.com/sit es/default/files/videos/origin al/imrt.mp4 brachy- from Greek brakhys "short" Historically LDR has been used. Cs-137 at 0.4-0.8 Gy/h With optimally placed device, dose
https://patient.varian.com/sit es/default/files/videos/origin al/imrt.mp4 brachy- from Greek brakhys "short" Historically LDR has been used. Cs-137 at 0.4-0.8 Gy/h With optimally placed device, dose
The Role of Radiation in the Management of Gynecologic Cancers. Scott Glaser, MD
 The Role of Radiation in the Management of Gynecologic Cancers Scott Glaser, MD Nothing to disclose DISCLOSURE Outline The role of radiation in: Endometrial Cancer Adjuvant Medically inoperable Cervical
The Role of Radiation in the Management of Gynecologic Cancers Scott Glaser, MD Nothing to disclose DISCLOSURE Outline The role of radiation in: Endometrial Cancer Adjuvant Medically inoperable Cervical
PORTEC-4. Patient seqnr. Age at inclusion (years) Hospital:
 Hospital:") May 2016 Randomisation Checklist Form 1, page 1 of 2 Patient seqnr. Age at inclusion (years) Hospital: Eligible patients should be registered and randomised via the Internet at : https://prod.tenalea.net/fs4/dm/delogin.aspx?refererpath=dehome.aspx
May 2016 Randomisation Checklist Form 1, page 1 of 2 Patient seqnr. Age at inclusion (years) Hospital: Eligible patients should be registered and randomised via the Internet at : https://prod.tenalea.net/fs4/dm/delogin.aspx?refererpath=dehome.aspx
Role of IMRT in the Treatment of Gynecologic Malignancies. John C. Roeske, PhD Associate Professor The University of Chicago
 Role of IMRT in the Treatment of Gynecologic Malignancies John C. Roeske, PhD Associate Professor The University of Chicago Acknowledgements B Aydogan, PhD Univ of Chicago P Chan, MD Princess Margaret
Role of IMRT in the Treatment of Gynecologic Malignancies John C. Roeske, PhD Associate Professor The University of Chicago Acknowledgements B Aydogan, PhD Univ of Chicago P Chan, MD Princess Margaret
ART for Cervical Cancer: Dosimetry and Technical Aspects
 ART for Cervical Cancer: Dosimetry and Technical Aspects D.A. Jaffray, Ph.D. Radiation Therapy Physics Princess Margaret Cancer Centre/Techna/Ontario Cancer Institute Professor Departments of Radiation
ART for Cervical Cancer: Dosimetry and Technical Aspects D.A. Jaffray, Ph.D. Radiation Therapy Physics Princess Margaret Cancer Centre/Techna/Ontario Cancer Institute Professor Departments of Radiation
Nordic Society for Gynecological Oncology Advisory Board of Radiotherapy
 Nordic Society for Gynecological Oncology Advisory Board of Radiotherapy Guidelines for postoperative irradiation of cervical cancer Contents: 1. Treatment planning for EBRT. 2 2. Target definition for
Nordic Society for Gynecological Oncology Advisory Board of Radiotherapy Guidelines for postoperative irradiation of cervical cancer Contents: 1. Treatment planning for EBRT. 2 2. Target definition for
It s All About Margins. Maaike Milder, Ph.D. Accuray Symposium April 21 st 2018
 It s All About Margins Maaike Milder, Ph.D. Accuray Symposium April 21 st 2018 Why margins? The smaller the better! Short Introduction Erasmus MC has been using the CyberKnife Robotic Radiosurgery System
It s All About Margins Maaike Milder, Ph.D. Accuray Symposium April 21 st 2018 Why margins? The smaller the better! Short Introduction Erasmus MC has been using the CyberKnife Robotic Radiosurgery System
NEWER RADIATION (3 D -CRT, IMRT, IGRT) TECHNIQUES FOR CERVICAL CANCERS (COMMON PELVIC TUMORS)
 TECHNIQUES FOR CERVICAL CANCERS (COMMON PELVIC TUMORS)") NEWER RADIATION (3 D -CRT, IMRT, IGRT) TECHNIQUES FOR CERVICAL CANCERS (COMMON PELVIC TUMORS) Umesh Mahantshetty, DMRT, MD, DNBR Associate Professor, Radiation Oncology Convener: Urology Disease Management
NEWER RADIATION (3 D -CRT, IMRT, IGRT) TECHNIQUES FOR CERVICAL CANCERS (COMMON PELVIC TUMORS) Umesh Mahantshetty, DMRT, MD, DNBR Associate Professor, Radiation Oncology Convener: Urology Disease Management
Research Article Implant R100 Predicts Rectal Bleeding in Prostate Cancer Patients Treated with IG-IMRT to 45 Gy and Pd-103 Implant
 Radiotherapy, Article ID 130652, 6 pages http://dx.doi.org/10.1155/2014/130652 Research Article Implant R100 Predicts Rectal Bleeding in Prostate Cancer Patients Treated with IG-IMRT to 45 Gy and Pd-103
Radiotherapy, Article ID 130652, 6 pages http://dx.doi.org/10.1155/2014/130652 Research Article Implant R100 Predicts Rectal Bleeding in Prostate Cancer Patients Treated with IG-IMRT to 45 Gy and Pd-103
Brachytherapy-emulating robotic radiosurgery in patients with cervical carcinoma
 Marnitz et al. Radiation Oncology 2013, 8:109 SHORT REPORT Open Access Brachytherapy-emulating robotic radiosurgery in patients with cervical carcinoma Simone Marnitz 1*, Christhardt Köhler 2, Volker Budach
Marnitz et al. Radiation Oncology 2013, 8:109 SHORT REPORT Open Access Brachytherapy-emulating robotic radiosurgery in patients with cervical carcinoma Simone Marnitz 1*, Christhardt Köhler 2, Volker Budach
GYNECOLOGIC CANCER and RADIATION THERAPY. Jon Anders M.D. Radiation Oncology
 GYNECOLOGIC CANCER and RADIATION THERAPY Jon Anders M.D. Radiation Oncology Brachytherapy Comes from the Greek brakhus meaning short Brachytherapy is treatment at short distance Intracavitary vs interstitial
GYNECOLOGIC CANCER and RADIATION THERAPY Jon Anders M.D. Radiation Oncology Brachytherapy Comes from the Greek brakhus meaning short Brachytherapy is treatment at short distance Intracavitary vs interstitial
Basic Concepts in Image Based Brachytherapy (GEC-ESTRO Target Concept & Contouring)
") Basic Concepts in Image Based Brachytherapy (GEC-ESTRO Target Concept & Contouring) Dr Umesh Mahantshetty, Professor, Radiation Oncology GYN & Urology Disease Management Group (DMG) Member Tata Memorial
Basic Concepts in Image Based Brachytherapy (GEC-ESTRO Target Concept & Contouring) Dr Umesh Mahantshetty, Professor, Radiation Oncology GYN & Urology Disease Management Group (DMG) Member Tata Memorial
Changing Paradigms in Radiotherapy
 Changing Paradigms in Radiotherapy Marco van Vulpen, MD, PhD Mouldroomdag-2015 Towards the elimination of invasion 1 NIH opinion on the future of oncology Twenty-five years from now,i hope that we won
Changing Paradigms in Radiotherapy Marco van Vulpen, MD, PhD Mouldroomdag-2015 Towards the elimination of invasion 1 NIH opinion on the future of oncology Twenty-five years from now,i hope that we won
External Beam Radiotherapy for Prostate Cancer
 External Beam Radiotherapy for Prostate Cancer Chomporn Sitathanee, Radiation Oncology Unit Ramathibodi Hospital, Mahidol University Roles of RT in prostate cancer Definitive RT; intact prostate Post radical
External Beam Radiotherapy for Prostate Cancer Chomporn Sitathanee, Radiation Oncology Unit Ramathibodi Hospital, Mahidol University Roles of RT in prostate cancer Definitive RT; intact prostate Post radical
JMSCR Vol 06 Issue 12 Page December 2018
 www.jmscr.igmpublication.org Impact Factor (SJIF): 6.379 Index Copernicus Value: 79.54 ISSN (e)-2347-176x ISSN (p) 2455-0450 DOI: https://dx.doi.org/10.18535/jmscr/v6i12.129 Research Paper Establishing
www.jmscr.igmpublication.org Impact Factor (SJIF): 6.379 Index Copernicus Value: 79.54 ISSN (e)-2347-176x ISSN (p) 2455-0450 DOI: https://dx.doi.org/10.18535/jmscr/v6i12.129 Research Paper Establishing
Corporate Medical Policy
 Corporate Medical Policy Intensity Modulated Radiation Therapy (IMRT) of Abdomen and File Name: Origination: Last CAP Review: Next CAP Review: Last Review: intensity_modulated_radiation_therapy_imrt_of_abdomen_and_pelvis
Corporate Medical Policy Intensity Modulated Radiation Therapy (IMRT) of Abdomen and File Name: Origination: Last CAP Review: Next CAP Review: Last Review: intensity_modulated_radiation_therapy_imrt_of_abdomen_and_pelvis
Role of Belly Board Device in the Age of Intensity Modulated Radiotherapy for Pelvic Irradiation
 Role of Belly Board Device in the Age of Intensity Modulated Radiotherapy for Pelvic Irradiation 2017 AAMD 42 nd Annual Meeting Neil C. Estabrook, MD 6 / 14 / 2017 7/5/2017 1 Conflicts of Interest None
Role of Belly Board Device in the Age of Intensity Modulated Radiotherapy for Pelvic Irradiation 2017 AAMD 42 nd Annual Meeting Neil C. Estabrook, MD 6 / 14 / 2017 7/5/2017 1 Conflicts of Interest None
Case Scenario 1. History
 History Case Scenario 1 A 53 year old white female presented to her primary care physician with post-menopausal vaginal bleeding. The patient is not a smoker and does not use alcohol. She has no family
History Case Scenario 1 A 53 year old white female presented to her primary care physician with post-menopausal vaginal bleeding. The patient is not a smoker and does not use alcohol. She has no family
Evaluation of Whole-Field and Split-Field Intensity Modulation Radiation Therapy (IMRT) Techniques in Head and Neck Cancer
 Techniques in Head and Neck Cancer") 1 Charles Poole April Case Study April 30, 2012 Evaluation of Whole-Field and Split-Field Intensity Modulation Radiation Therapy (IMRT) Techniques in Head and Neck Cancer Abstract: Introduction: This study
1 Charles Poole April Case Study April 30, 2012 Evaluation of Whole-Field and Split-Field Intensity Modulation Radiation Therapy (IMRT) Techniques in Head and Neck Cancer Abstract: Introduction: This study
Locally advanced disease & challenges in management
 Gynecologic Cancer InterGroup Cervix Cancer Research Network Cervix Cancer Education Symposium, February 2018 Locally advanced disease & challenges in management Carien Creutzberg Radiation Oncology, Leiden
Gynecologic Cancer InterGroup Cervix Cancer Research Network Cervix Cancer Education Symposium, February 2018 Locally advanced disease & challenges in management Carien Creutzberg Radiation Oncology, Leiden
Chemoradiation (CRT) Safety Analysis of ACOSOG Z6041: A Phase II Trial of Neoadjuvant CRT followed by Local Excision in ut2 Rectal Cancer
 Safety Analysis of ACOSOG Z6041: A Phase II Trial of Neoadjuvant CRT followed by Local Excision in ut2 Rectal Cancer") Chemoradiation (CRT) Safety Analysis of ACOSOG Z6041: A Phase II Trial of Neoadjuvant CRT followed by Local Excision in ut2 Rectal Cancer Emily Chan, Qian Shi, Julio Garcia-Aguilar, Peter Cataldo, Jorge
Chemoradiation (CRT) Safety Analysis of ACOSOG Z6041: A Phase II Trial of Neoadjuvant CRT followed by Local Excision in ut2 Rectal Cancer Emily Chan, Qian Shi, Julio Garcia-Aguilar, Peter Cataldo, Jorge
CyberKnife SBRT for Prostate Cancer
 CyberKnife SBRT for Prostate Cancer Robert Meier, MD Swedish Radiosurgery Center Swedish Cancer Institute Seattle, WA 2017 ESTRO Meeting, Vienna Austria 5-year safety, efficacy & quality of life outcomes
CyberKnife SBRT for Prostate Cancer Robert Meier, MD Swedish Radiosurgery Center Swedish Cancer Institute Seattle, WA 2017 ESTRO Meeting, Vienna Austria 5-year safety, efficacy & quality of life outcomes
NCCN GUIDELINES ON PROTON THERAPY (AS OF 4/23/18) BONE (Version , 03/28/18)
 BONE (Version , 03/28/18)") BONE (Version 2.2018, 03/28/18) NCCN GUIDELINES ON PROTON THERAPY (AS OF 4/23/18) Radiation Therapy Specialized techniques such as intensity-modulated RT (IMRT); particle beam RT with protons, carbon ions,
BONE (Version 2.2018, 03/28/18) NCCN GUIDELINES ON PROTON THERAPY (AS OF 4/23/18) Radiation Therapy Specialized techniques such as intensity-modulated RT (IMRT); particle beam RT with protons, carbon ions,
Treatment Planning for Lung. Kristi Hendrickson, PhD, DABR University of Washington Dept. of Radiation Oncology
 Treatment Planning for Lung Kristi Hendrickson, PhD, DABR University of Washington Dept. of Radiation Oncology Outline of Presentation Dosimetric planning strategies for SBRT lung Delivery techniques Examples
Treatment Planning for Lung Kristi Hendrickson, PhD, DABR University of Washington Dept. of Radiation Oncology Outline of Presentation Dosimetric planning strategies for SBRT lung Delivery techniques Examples
INTRODUCTION. J. Radiat. Res., 53, (2012)
") J. Radiat. Res., 53, 281 287 (2012) The Effects of Two HDR Brachytherapy Schedules in Locally Advanced Cervical Cancer Treated with Concurrent Chemoradiation: A Study from Chiang Mai, Thailand Ekkasit
J. Radiat. Res., 53, 281 287 (2012) The Effects of Two HDR Brachytherapy Schedules in Locally Advanced Cervical Cancer Treated with Concurrent Chemoradiation: A Study from Chiang Mai, Thailand Ekkasit
Trimodality Therapy for Muscle Invasive Bladder Cancer
 Trimodality Therapy for Muscle Invasive Bladder Cancer Brita Danielson, MD, FRCPC Radiation Oncologist, Cross Cancer Institute Assistant Professor, Department of Oncology University of Alberta Edmonton,
Trimodality Therapy for Muscle Invasive Bladder Cancer Brita Danielson, MD, FRCPC Radiation Oncologist, Cross Cancer Institute Assistant Professor, Department of Oncology University of Alberta Edmonton,
Implementation of Gynaecological IMRT Planning Technique Clinical Guidelines and Constraints. Chloe Pandeli
 Implementation of Gynaecological IMRT Planning Technique Clinical Guidelines and Constraints Chloe Pandeli 1 Session Name: Proffered papers - Gastrointestinal / Gynaecological In accordance with the policy
Implementation of Gynaecological IMRT Planning Technique Clinical Guidelines and Constraints Chloe Pandeli 1 Session Name: Proffered papers - Gastrointestinal / Gynaecological In accordance with the policy
HDR vs. LDR Is One Better Than The Other?
 HDR vs. LDR Is One Better Than The Other? Daniel Fernandez, MD, PhD 11/3/2017 New Frontiers in Urologic Oncology Learning Objectives Indications for prostate brachytherapy Identify pros/cons of HDR vs
HDR vs. LDR Is One Better Than The Other? Daniel Fernandez, MD, PhD 11/3/2017 New Frontiers in Urologic Oncology Learning Objectives Indications for prostate brachytherapy Identify pros/cons of HDR vs
Linac Based SBRT for Low-intermediate Risk Prostate Cancer in 5 Fractions: Preliminary Report of a Phase II Study with FFF Delivery
 Linac Based SBRT for Low-intermediate Risk Prostate Cancer in 5 Fractions: Preliminary Report of a Phase II Study with FFF Delivery FILIPPO ALONGI MD Radiation Oncology & Radiosurgery Istituto Clinico
Linac Based SBRT for Low-intermediate Risk Prostate Cancer in 5 Fractions: Preliminary Report of a Phase II Study with FFF Delivery FILIPPO ALONGI MD Radiation Oncology & Radiosurgery Istituto Clinico
High dose-rate tandem and ovoid brachytherapy in cervical cancer: dosimetric predictors of adverse events
 Romano et al. Radiation Oncology (2018) 13:129 https://doi.org/10.1186/s13014-018-1074-2 RESEARCH Open Access High dose-rate tandem and ovoid brachytherapy in cervical cancer: dosimetric predictors of
Romano et al. Radiation Oncology (2018) 13:129 https://doi.org/10.1186/s13014-018-1074-2 RESEARCH Open Access High dose-rate tandem and ovoid brachytherapy in cervical cancer: dosimetric predictors of
Image based Brachytherapy- HDR applications in Gynecological Tumors
 Image based Brachytherapy- HDR applications in Gynecological Tumors Yakov Pipman, D. Sc. North Shore LIJ Health System Sites amenable to treatment with HDR Brachytherapy GYN Breast Prostate Head and Neck
Image based Brachytherapy- HDR applications in Gynecological Tumors Yakov Pipman, D. Sc. North Shore LIJ Health System Sites amenable to treatment with HDR Brachytherapy GYN Breast Prostate Head and Neck
Would SBRT Hypofractionated Approach Be as Good? Then Why Bother With Brachytherapy?
 Would SBRT Hypofractionated Approach Be as Good? Then Why Bother With Brachytherapy? Yasuo Yoshioka, MD Department of Radiation Oncology Osaka University Graduate School of Medicine Osaka, Japan Disclosure
Would SBRT Hypofractionated Approach Be as Good? Then Why Bother With Brachytherapy? Yasuo Yoshioka, MD Department of Radiation Oncology Osaka University Graduate School of Medicine Osaka, Japan Disclosure
MRI in Cervix and Endometrial Cancer
 28th Congress of the Hungarian Society of Radiologists RCR Session Budapest June 2016 MRI in Cervix and Endometrial Cancer DrSarah Swift St James s University Hospital Leeds, UK Objectives Cervix and endometrial
28th Congress of the Hungarian Society of Radiologists RCR Session Budapest June 2016 MRI in Cervix and Endometrial Cancer DrSarah Swift St James s University Hospital Leeds, UK Objectives Cervix and endometrial
MRI Guided GYN Brachytherapy: Clinical Considerations
 MRI Guided GYN Brachytherapy: Clinical Considerations AAPM Junzo Chino MD Duke Radiation Oncology 8/8/2013 Disclosures none Learning Objectives Historical Context: Film based Brachytherapy Advantages of
MRI Guided GYN Brachytherapy: Clinical Considerations AAPM Junzo Chino MD Duke Radiation Oncology 8/8/2013 Disclosures none Learning Objectives Historical Context: Film based Brachytherapy Advantages of
Prostate Cancer Appraisal Addendum: Stereotactic Body Radiation Therapy (SBRT)
") Prostate Cancer Appraisal Addendum: Stereotactic Body Radiation Therapy (SBRT) The Institute for Clinical and Economic Review (ICER) has published appraisals on multiple management options for clinically-localized,
Prostate Cancer Appraisal Addendum: Stereotactic Body Radiation Therapy (SBRT) The Institute for Clinical and Economic Review (ICER) has published appraisals on multiple management options for clinically-localized,
Outline. Contour quality control. Dosimetric impact of contouring errors and variability in Intensity Modulated Radiation Therapy (IMRT)
") Dosimetric impact of contouring errors and variability in Intensity Modulated Radiation Therapy (IMRT) James Kavanaugh, MS DABR Department of Radiation Oncology Division of Medical Physics Outline Importance
Dosimetric impact of contouring errors and variability in Intensity Modulated Radiation Therapy (IMRT) James Kavanaugh, MS DABR Department of Radiation Oncology Division of Medical Physics Outline Importance
Version A European study on MRI-guided brachytherapy in locally advanced cervical cancer EMBRACE (ENDORSED BY GEC ESTRO)
") A European study on MRI-guided brachytherapy in locally advanced cervical cancer EMBRACE (ENDORSED BY GEC ESTRO) 1 Contents: 1. ABBREVIATIONS... 4 2. SUMMARY... 5 3. INTRODUCTION AND PRINCIPLES OF IMAGE
A European study on MRI-guided brachytherapy in locally advanced cervical cancer EMBRACE (ENDORSED BY GEC ESTRO) 1 Contents: 1. ABBREVIATIONS... 4 2. SUMMARY... 5 3. INTRODUCTION AND PRINCIPLES OF IMAGE
Dose-Volume Histogram Analysis in Point A-based Dose Prescription of High-dose-rate Brachytherapy for Cervical Carcinoma
 Showa Univ J Med Sci 30 2, 227 235, June 2018 Original Dose-Volume Histogram Analysis in Point A-based Dose Prescription of High-dose-rate Brachytherapy for Cervical Carcinoma Rei KOBAYASHI 1, Yoshikazu
Showa Univ J Med Sci 30 2, 227 235, June 2018 Original Dose-Volume Histogram Analysis in Point A-based Dose Prescription of High-dose-rate Brachytherapy for Cervical Carcinoma Rei KOBAYASHI 1, Yoshikazu
Gynecologic Cancer InterGroup Cervix Cancer Research Network. Management of Cervical Cancer in Resource Limited Settings.
 Management of Cervical Cancer in Resource Limited Settings Linus Chuang MD Conflict of Interests None Cervical cancer is the fourth most common malignancy in women worldwide 530,000 new cases per year
Management of Cervical Cancer in Resource Limited Settings Linus Chuang MD Conflict of Interests None Cervical cancer is the fourth most common malignancy in women worldwide 530,000 new cases per year
Page 1. Helical (Spiral) Tomotherapy. UW Helical Tomotherapy Unit. Helical (Spiral) Tomotherapy. MVCT of an Anesthetized Dog with a Sinus Tumor
 Tomotherapy. UW Helical Tomotherapy Unit. Helical (Spiral) Tomotherapy. MVCT of an Anesthetized Dog with a Sinus Tumor") Helical (Spiral) Tomotherapy Novel Clinical Applications of IMRT Linac Ring Gantry CT Detector X-Ray Fan Beam Binary Multileaf Collimator Binary MLC Leaves James S Welsh, MS, MD Department of Human Oncology
Helical (Spiral) Tomotherapy Novel Clinical Applications of IMRT Linac Ring Gantry CT Detector X-Ray Fan Beam Binary Multileaf Collimator Binary MLC Leaves James S Welsh, MS, MD Department of Human Oncology
Stereotactic MR-guided adaptive radiation therapy (SMART) for locally advanced pancreatic tumors
 for locally advanced pancreatic tumors") Stereotactic MR-guided adaptive radiation therapy (SMART) for locally advanced pancreatic tumors Anna Bruynzeel, Radiation Oncologist VU University Medical Center, Amsterdam, The Netherlands Current standard
Stereotactic MR-guided adaptive radiation therapy (SMART) for locally advanced pancreatic tumors Anna Bruynzeel, Radiation Oncologist VU University Medical Center, Amsterdam, The Netherlands Current standard
Stereotactic ablative body radiation for prostate cancer SABR
 Stereotactic ablative body radiation for prostate cancer SABR John Armstrong. Sinead Callinan. Luke Rock. Beacon Hospital, Dublin, Ireland Low- Intermediate Risk Prostate Comparing treatment choices IMRT
Stereotactic ablative body radiation for prostate cancer SABR John Armstrong. Sinead Callinan. Luke Rock. Beacon Hospital, Dublin, Ireland Low- Intermediate Risk Prostate Comparing treatment choices IMRT
Vaginal Sparing with Volumetric Modulated Arc Therapy (VMAT) for Rectal Cancer. Scott Boulet BSc, RT(T)
 for Rectal Cancer. Scott Boulet BSc, RT(T)") Vaginal Sparing with Volumetric Modulated Arc Therapy (VMAT) for Rectal Cancer Scott Boulet BSc, RT(T) Outline Background Objectives Design Results Discussion Conclusion Acknowledgements Questions Background
Vaginal Sparing with Volumetric Modulated Arc Therapy (VMAT) for Rectal Cancer Scott Boulet BSc, RT(T) Outline Background Objectives Design Results Discussion Conclusion Acknowledgements Questions Background
W J R. World Journal of Radiology. Use of stereotactic radiosurgery in the treatment of gynecologic malignancies: A review. Abstract INTRODUCTION
 W J R World Journal of Radiology Submit a Manuscript: http://www.wjgnet.com/esps/ Help Desk: http://www.wjgnet.com/esps/helpdesk.aspx DOI: 10.4329/wjr.v6.i6.366 World J Radiol 2014 June 28; 6(6): 366-373
W J R World Journal of Radiology Submit a Manuscript: http://www.wjgnet.com/esps/ Help Desk: http://www.wjgnet.com/esps/helpdesk.aspx DOI: 10.4329/wjr.v6.i6.366 World J Radiol 2014 June 28; 6(6): 366-373
Bone Marrow Dosimetric Parameters and Hematological Toxicity In Cervical Cancer Patients Undergoing Concurrent Chemoradiation.
 IOSR Journal of Dental and Medical Sciences (IOSR-JDMS) e-issn: 2279-0853, p-issn: 2279-0861.Volume 17, Issue 4 Ver. 18 (April. 2018), PP 28-32 www.iosrjournals.org Bone Marrow Dosimetric Parameters and
IOSR Journal of Dental and Medical Sciences (IOSR-JDMS) e-issn: 2279-0853, p-issn: 2279-0861.Volume 17, Issue 4 Ver. 18 (April. 2018), PP 28-32 www.iosrjournals.org Bone Marrow Dosimetric Parameters and
High-Dose-Rate Orthogonal Intracavitary Brachytherapy with 9 Gy/Fraction in Locally Advanced Cervical Cancer: Is it Feasible??
 DOI 10.1007/s13224-015-0812-8 ORIGINAL ARTICLE High-Dose-Rate Orthogonal Intracavitary Brachytherapy with 9 Gy/Fraction in Locally Advanced Cervical Cancer: Is it Feasible?? Saptarshi Ghosh 1 Pamidimukalabramhananda
DOI 10.1007/s13224-015-0812-8 ORIGINAL ARTICLE High-Dose-Rate Orthogonal Intracavitary Brachytherapy with 9 Gy/Fraction in Locally Advanced Cervical Cancer: Is it Feasible?? Saptarshi Ghosh 1 Pamidimukalabramhananda
Radiation Oncology MOC Study Guide
 Radiation Oncology MOC Study Guide The following study guide is intended to give a general overview of the type of material that will be covered on the Radiation Oncology Maintenance of Certification (MOC)
Radiation Oncology MOC Study Guide The following study guide is intended to give a general overview of the type of material that will be covered on the Radiation Oncology Maintenance of Certification (MOC)
Dosimetric comparison of interstitial brachytherapy with multi-channel vaginal cylinder plans in patients with vaginal tumors
 Mendez et al. Radiation Oncology (2017) 12:84 DOI 10.1186/s13014-017-0821-0 RESEARCH Open Access Dosimetric comparison of interstitial brachytherapy with multi-channel vaginal cylinder plans in patients
Mendez et al. Radiation Oncology (2017) 12:84 DOI 10.1186/s13014-017-0821-0 RESEARCH Open Access Dosimetric comparison of interstitial brachytherapy with multi-channel vaginal cylinder plans in patients
Pelvic palliative radiotherapy for gynecological cancers present state of knowledge and pending research questions to answer
 Pelvic palliative radiotherapy for gynecological cancers present state of knowledge and pending research questions to answer Esten S. Nakken MD PhD Division of Cancer Medicine Oslo University Hospital
Pelvic palliative radiotherapy for gynecological cancers present state of knowledge and pending research questions to answer Esten S. Nakken MD PhD Division of Cancer Medicine Oslo University Hospital
4D Radiotherapy in early ca Lung. Prof. Manoj Gupta Dept of Radiotherapy & oncology I.G.Medical College Shimla
 4D Radiotherapy in early ca Lung Prof. Manoj Gupta Dept of Radiotherapy & oncology I.G.Medical College Shimla Presentation focus on ---- Limitation of Conventional RT Why Interest in early lung cancer
4D Radiotherapy in early ca Lung Prof. Manoj Gupta Dept of Radiotherapy & oncology I.G.Medical College Shimla Presentation focus on ---- Limitation of Conventional RT Why Interest in early lung cancer
Modern Dose Fractionation and Treatment Techniques for Definitive Prostate RT
 Modern Dose Fractionation and Treatment Techniques for Definitive Prostate RT Daniel J Bourgeois, III MD, MPH Board Certified Radiation Oncologist Southeast Louisiana Radiation Oncology Group (SLROG) Disclosures
Modern Dose Fractionation and Treatment Techniques for Definitive Prostate RT Daniel J Bourgeois, III MD, MPH Board Certified Radiation Oncologist Southeast Louisiana Radiation Oncology Group (SLROG) Disclosures
New Radiation Treatment Modalities in the Treatment of Lung Cancer
 New Radiation Treatment Modalities in the Treatment of Lung Cancer David Perry, M.D. Chief, Radiation Oncology Medical Director, CyberKnife Radiosurgery Center Medstar Franklin Square Medical Center Definitions
New Radiation Treatment Modalities in the Treatment of Lung Cancer David Perry, M.D. Chief, Radiation Oncology Medical Director, CyberKnife Radiosurgery Center Medstar Franklin Square Medical Center Definitions
Chapter 5 Stage III and IVa disease
 Page 55 Chapter 5 Stage III and IVa disease Overview Concurrent chemoradiotherapy (CCRT) is recommended for stage III and IVa disease. Recommended regimen for the chemotherapy portion generally include
Page 55 Chapter 5 Stage III and IVa disease Overview Concurrent chemoradiotherapy (CCRT) is recommended for stage III and IVa disease. Recommended regimen for the chemotherapy portion generally include
Original Date: June 2013 Page 1 of 7 Radiation Oncology Last Review Date: September Implementation Date: December 2014 Clinical Operations
 National Imaging Associates, Inc. Clinical guideline CERVICAL CANCER Original Date: June 2013 Page 1 of 7 Radiation Oncology Last Review Date: September 2014 Guideline Number: NIA_CG_223 Last Revised Date:
National Imaging Associates, Inc. Clinical guideline CERVICAL CANCER Original Date: June 2013 Page 1 of 7 Radiation Oncology Last Review Date: September 2014 Guideline Number: NIA_CG_223 Last Revised Date:
The Evolution of SBRT and Hypofractionation in Thoracic Radiation Oncology
 The Evolution of SBRT and Hypofractionation in Thoracic Radiation Oncology (specifically, lung cancer) 2/10/18 Jeffrey Kittel, MD Radiation Oncology, Aurora St. Luke s Medical Center Outline The history
The Evolution of SBRT and Hypofractionation in Thoracic Radiation Oncology (specifically, lung cancer) 2/10/18 Jeffrey Kittel, MD Radiation Oncology, Aurora St. Luke s Medical Center Outline The history
Correspondence should be addressed to Alicia McMaster;
 Cancer Research Volume 2013, Article ID 308236, 5 pages http://dx.doi.org/10.1155/2013/308236 Research Article Taxpas: Epidemiological and Survival Data in Breast Cancer Patients Treated with a Docetaxel-Based
Cancer Research Volume 2013, Article ID 308236, 5 pages http://dx.doi.org/10.1155/2013/308236 Research Article Taxpas: Epidemiological and Survival Data in Breast Cancer Patients Treated with a Docetaxel-Based
A TREATMENT PLANNING STUDY COMPARING VMAT WITH 3D CONFORMAL RADIOTHERAPY FOR PROSTATE CANCER USING PINNACLE PLANNING SYSTEM *
 Romanian Reports in Physics, Vol. 66, No. 2, P. 394 400, 2014 A TREATMENT PLANNING STUDY COMPARING VMAT WITH 3D CONFORMAL RADIOTHERAPY FOR PROSTATE CANCER USING PINNACLE PLANNING SYSTEM * D. ADAM 1,2,
Romanian Reports in Physics, Vol. 66, No. 2, P. 394 400, 2014 A TREATMENT PLANNING STUDY COMPARING VMAT WITH 3D CONFORMAL RADIOTHERAPY FOR PROSTATE CANCER USING PINNACLE PLANNING SYSTEM * D. ADAM 1,2,
New Technologies for the Radiotherapy of Prostate Cancer
 Prostate Cancer Meyer JL (ed): IMRT, IGRT, SBRT Advances in the Treatment Planning and Delivery of Radiotherapy. Front Radiat Ther Oncol. Basel, Karger, 27, vol. 4, pp 315 337 New Technologies for the
Prostate Cancer Meyer JL (ed): IMRT, IGRT, SBRT Advances in the Treatment Planning and Delivery of Radiotherapy. Front Radiat Ther Oncol. Basel, Karger, 27, vol. 4, pp 315 337 New Technologies for the
IMRT for Prostate Cancer
 IMRT for Cancer All patients are simulated in the supine position. Reproducibility is achieved using a custom alpha cradle cast that extends from the mid-back to mid-thigh. The feet are positioned in a
IMRT for Cancer All patients are simulated in the supine position. Reproducibility is achieved using a custom alpha cradle cast that extends from the mid-back to mid-thigh. The feet are positioned in a
Case Report Two Cases of Small Cell Cancer of the Maxillary Sinus Treated with Cisplatin plus Irinotecan and Radiotherapy
 Case Reports in Otolaryngology Volume 2013, Article ID 893638, 4 pages http://dx.doi.org/10.1155/2013/893638 Case Report Two Cases of Small Cell Cancer of the Maxillary Sinus Treated with Cisplatin plus
Case Reports in Otolaryngology Volume 2013, Article ID 893638, 4 pages http://dx.doi.org/10.1155/2013/893638 Case Report Two Cases of Small Cell Cancer of the Maxillary Sinus Treated with Cisplatin plus
The New ICRU/GEC ESTRO Report in Clinical Practice. Disclosures
 The New ICRU/GEC ESTRO Report in Clinical Practice Christian Kirisits, MSc, PhD; Richard Pötter, MD Medical University of Vienna, Vienna, Austria On behalf of the Committee: B. Erickson, C. Haie Meder,
The New ICRU/GEC ESTRO Report in Clinical Practice Christian Kirisits, MSc, PhD; Richard Pötter, MD Medical University of Vienna, Vienna, Austria On behalf of the Committee: B. Erickson, C. Haie Meder,
Partial Breast Irradiation using adaptive MRgRT
 Partial Breast Irradiation using adaptive MRgRT Shyama Tetar, radiation-oncologist VUmc Amsterdam 15-12-2017 5 th Vumc SBRT symposium 2017 Current practice Breast conserving treatment (BCT) Breast conserving
Partial Breast Irradiation using adaptive MRgRT Shyama Tetar, radiation-oncologist VUmc Amsterdam 15-12-2017 5 th Vumc SBRT symposium 2017 Current practice Breast conserving treatment (BCT) Breast conserving
Basics of Cervix Cancer Brachytherapy
 Gynecologic Cancer InterGroup Cervix Cancer Research Network Basics of Cervix Cancer Brachytherapy David Gaffney MDPhD, FASTRO, FACR University of Utah Huntsman Cancer Institute Incidence Cervix: 445,000
Gynecologic Cancer InterGroup Cervix Cancer Research Network Basics of Cervix Cancer Brachytherapy David Gaffney MDPhD, FASTRO, FACR University of Utah Huntsman Cancer Institute Incidence Cervix: 445,000
Radiotherapy physics & Equipments
 Radiotherapy physics & Equipments RAD 481 Lecture s Title: An Overview of Radiation Therapy for Health Care Professionals Dr. Mohammed Emam Vision :IMC aspires to be a leader in applied medical sciences,
Radiotherapy physics & Equipments RAD 481 Lecture s Title: An Overview of Radiation Therapy for Health Care Professionals Dr. Mohammed Emam Vision :IMC aspires to be a leader in applied medical sciences,
Course Directors: Teaching Staff: Guest Lecturers: Local Organiser: ESTRO coordinator: Melissa Vanderijst, project manager (BE)
") ESTRO Teaching Course on Image-guided radiotherapy & chemotherapy in gynaecological cancer - With a special focus on adaptive brachytherapy Prague, Czech Republic 22-26 October 2017 Course Directors: Richard
ESTRO Teaching Course on Image-guided radiotherapy & chemotherapy in gynaecological cancer - With a special focus on adaptive brachytherapy Prague, Czech Republic 22-26 October 2017 Course Directors: Richard
Radiation Therapy: From Fallacy to Science
 27 th Annual Management of Colon and Rectal Diseases 2.23.2019 Radiation Therapy: From Fallacy to Science Hadi Zahra, MD, DABR Radiation Oncologist CHI Health Henry Lynch Cancer Center Assistant Clinical
27 th Annual Management of Colon and Rectal Diseases 2.23.2019 Radiation Therapy: From Fallacy to Science Hadi Zahra, MD, DABR Radiation Oncologist CHI Health Henry Lynch Cancer Center Assistant Clinical
Goals and Objectives: Head and Neck Cancer Service Department of Radiation Oncology
 Goals and Objectives: Head and Neck Cancer Service Department of Radiation Oncology The head and neck cancer service provides training in the diagnosis, management, treatment, and follow-up care of head
Goals and Objectives: Head and Neck Cancer Service Department of Radiation Oncology The head and neck cancer service provides training in the diagnosis, management, treatment, and follow-up care of head
Feasibility of 4D IMRT Delivery for Hypofractionated High Dose Partial Prostate Treatments
 Feasibility of 4D IMRT Delivery for Hypofractionated High Dose Partial Prostate Treatments R.A. Price Jr., Ph.D., J. Li, Ph.D., A. Pollack, M.D., Ph.D.*, L. Jin, Ph.D., E. Horwitz, M.D., M. Buyyounouski,
Feasibility of 4D IMRT Delivery for Hypofractionated High Dose Partial Prostate Treatments R.A. Price Jr., Ph.D., J. Li, Ph.D., A. Pollack, M.D., Ph.D.*, L. Jin, Ph.D., E. Horwitz, M.D., M. Buyyounouski,
8/1/2017. Clinical Indications and Applications of Realtime MRI-Guided Radiotherapy
 Clinical Indications and Applications of Realtime MRI-Guided Radiotherapy Michael F Bassetti MD PhD Assistant Professor, Department of Human Oncology University of Wisconsin, Madison. Carbone Cancer Center
Clinical Indications and Applications of Realtime MRI-Guided Radiotherapy Michael F Bassetti MD PhD Assistant Professor, Department of Human Oncology University of Wisconsin, Madison. Carbone Cancer Center
Case Report Stereotactic Body Radiotherapy for Localized Ureter Transitional Cell Carcinoma: Three Case Reports
 Case Reports in Urology Volume 2015, Article ID 519897, 4 pages http://dx.doi.org/10.1155/2015/519897 Case Report Stereotactic Body Radiotherapy for Localized Ureter Transitional Cell Carcinoma: Three
Case Reports in Urology Volume 2015, Article ID 519897, 4 pages http://dx.doi.org/10.1155/2015/519897 Case Report Stereotactic Body Radiotherapy for Localized Ureter Transitional Cell Carcinoma: Three
Clinical Study Mucosal Melanoma in the Head and Neck Region: Different Clinical Features and Same Outcome to Cutaneous Melanoma
 ISRN Dermatology Volume 2013, Article ID 586915, 5 pages http://dx.doi.org/10.1155/2013/586915 Clinical Study Mucosal Melanoma in the Head and Neck Region: Different Clinical Features and Same Outcome
ISRN Dermatology Volume 2013, Article ID 586915, 5 pages http://dx.doi.org/10.1155/2013/586915 Clinical Study Mucosal Melanoma in the Head and Neck Region: Different Clinical Features and Same Outcome
Stereotactic Body Radiotherapy for Lung Lesions using the CyberKnife of-the-art and New Innovations
 Stereotactic Body Radiotherapy for Lung Lesions using the CyberKnife State-of of-the-art and New Innovations Chad Lee, PhD CK Solutions, Inc. and CyberKnife Centers of San Diego Outline Basic overview
Stereotactic Body Radiotherapy for Lung Lesions using the CyberKnife State-of of-the-art and New Innovations Chad Lee, PhD CK Solutions, Inc. and CyberKnife Centers of San Diego Outline Basic overview
Therapy of Non-Operable early stage NSCLC
 SBRT Stage I NSCLC Therapy of Non-Operable early stage NSCLC Dr. Adnan Al-Hebshi MD, FRCR(UK), FRCP(C), ABR King Faisal Specialist Hospital & Research Centre This is our territory Early Stages NSCLC Surgical
SBRT Stage I NSCLC Therapy of Non-Operable early stage NSCLC Dr. Adnan Al-Hebshi MD, FRCR(UK), FRCP(C), ABR King Faisal Specialist Hospital & Research Centre This is our territory Early Stages NSCLC Surgical
ICRT รศ.พญ.เยาวล กษณ ชาญศ ลป
 ICRT รศ.พญ.เยาวล กษณ ชาญศ ลป Brachytherapy การร กษาด วยร งส ระยะใกล Insertion การสอดใส แร Implantation การฝ งแร Surface application การวางแร physical benefit of brachytherapy - very high dose of radiation
ICRT รศ.พญ.เยาวล กษณ ชาญศ ลป Brachytherapy การร กษาด วยร งส ระยะใกล Insertion การสอดใส แร Implantation การฝ งแร Surface application การวางแร physical benefit of brachytherapy - very high dose of radiation
Clinical experience with TomoDirect System Tangential Mode
 Breast Cancer Clinical experience with TomoDirect System Tangential Mode European Institute of Oncology Milan, Italy Disclosure & Disclaimer An honorarium is provided by Accuray for this presentation The
Breast Cancer Clinical experience with TomoDirect System Tangential Mode European Institute of Oncology Milan, Italy Disclosure & Disclaimer An honorarium is provided by Accuray for this presentation The
North of Scotland Cancer Network Clinical Management Guideline for Carcinoma of the Uterine Cervix
 THIS DOCUMENT North of Scotland Cancer Network Carcinoma of the Uterine Cervix UNCONTROLLED WHEN PRINTED DOCUMENT CONTROL Prepared by A Kennedy/AG Macdonald/Others Approved by NOT APPROVED Issue date April
THIS DOCUMENT North of Scotland Cancer Network Carcinoma of the Uterine Cervix UNCONTROLLED WHEN PRINTED DOCUMENT CONTROL Prepared by A Kennedy/AG Macdonald/Others Approved by NOT APPROVED Issue date April
Original Date: April 2016 Page 1 of 7 FOR CMS (MEDICARE) MEMBERS ONLY
 MEMBERS ONLY") National Imaging Associates, Inc. Clinical guidelines STEREOTACTIC RADIATION THERAPY: STEREO RADIOSURGERY (SRS) AND STEREOTACTIC BODY RADIATION THERAPY (SBRT) CPT4 Codes: Please refer to pages 5-6 LCD
National Imaging Associates, Inc. Clinical guidelines STEREOTACTIC RADIATION THERAPY: STEREO RADIOSURGERY (SRS) AND STEREOTACTIC BODY RADIATION THERAPY (SBRT) CPT4 Codes: Please refer to pages 5-6 LCD
Course Directors: Teaching Staff: Guest Lecturers: Local Organiser: ESTRO coordinator: Melissa Vanderijst, project manager (BE)
") ESTRO Teaching Course on Image-guided radiotherapy & chemotherapy in gynaecological cancer - With a special focus on adaptive brachytherapy Prague, Czech Republic 22-26 October 2016 Course Directors: Richard
ESTRO Teaching Course on Image-guided radiotherapy & chemotherapy in gynaecological cancer - With a special focus on adaptive brachytherapy Prague, Czech Republic 22-26 October 2016 Course Directors: Richard
Fiducial-Free Lung Tracking and Treatment with the CyberKnife System: A Non-Invasive Approach
 Fiducial-Free Lung Tracking and Treatment with the CyberKnife System: A Non-Invasive Approach Jesse McKay, MS, DABR Erlanger Health System Chattanooga, TN JASTRO 2014, Yokohama Japan Disclosure I have
Fiducial-Free Lung Tracking and Treatment with the CyberKnife System: A Non-Invasive Approach Jesse McKay, MS, DABR Erlanger Health System Chattanooga, TN JASTRO 2014, Yokohama Japan Disclosure I have
Intensity Modulated Radiotherapy (IMRT) of the Abdomen and Pelvis
 of the Abdomen and Pelvis") Medical Policy Manual Medicine, Policy No. 139 Intensity Modulated Radiotherapy (IMRT) of the Abdomen and Pelvis Next Review: August 2018 Last Review: November 2017 Effective: December 1, 2017 IMPORTANT
Medical Policy Manual Medicine, Policy No. 139 Intensity Modulated Radiotherapy (IMRT) of the Abdomen and Pelvis Next Review: August 2018 Last Review: November 2017 Effective: December 1, 2017 IMPORTANT
Disclosure SBRT. SBRT for Spinal Metastases 5/2/2010. No conflicts of interest. Overview
 Stereotactic Body Radiotherapy (SBRT) for Recurrent Spine Tumors Arjun Sahgal M.D., F.R.C.P.C. Assistant Professor Princess Margaret Hospital Sunnybrook Health Sciences Center University of Toronto Department
Stereotactic Body Radiotherapy (SBRT) for Recurrent Spine Tumors Arjun Sahgal M.D., F.R.C.P.C. Assistant Professor Princess Margaret Hospital Sunnybrook Health Sciences Center University of Toronto Department
OPTIMIZATION OF COLLIMATOR PARAMETERS TO REDUCE RECTAL DOSE IN INTENSITY-MODULATED PROSTATE TREATMENT PLANNING
 Medical Dosimetry, Vol. 30, No. 4, pp. 205-212, 2005 Copyright 2005 American Association of Medical Dosimetrists Printed in the USA. All rights reserved 0958-3947/05/$ see front matter doi:10.1016/j.meddos.2005.06.002
Medical Dosimetry, Vol. 30, No. 4, pp. 205-212, 2005 Copyright 2005 American Association of Medical Dosimetrists Printed in the USA. All rights reserved 0958-3947/05/$ see front matter doi:10.1016/j.meddos.2005.06.002
Protocol. Intensity-Modulated Radiation Therapy (IMRT): Abdomen and Pelvis
: Abdomen and Pelvis") Intensity-Modulated Radiation Therapy (IMRT): Abdomen and (80149) Medical Benefit Effective Date: 07/01/11 Next Review Date: 03/13 Preauthorization* No Review Dates: 09/09, 09/10, 03/11, 03/12 The following
Intensity-Modulated Radiation Therapy (IMRT): Abdomen and (80149) Medical Benefit Effective Date: 07/01/11 Next Review Date: 03/13 Preauthorization* No Review Dates: 09/09, 09/10, 03/11, 03/12 The following
TRANS-TASMAN RADIATION ONCOLOGY GROUP INC. Quality Assurance. Treatment Planning Benchmark
 TRANS-TASMAN RADIATION ONCOLOGY GROUP INC. Quality Assurance Treatment Planning Benchmark PORTEC-3/ TROG 08.04 Randomised Phase III Trial Comparing Concurrent Chemoradiation and Adjuvant Chemotherapy with
TRANS-TASMAN RADIATION ONCOLOGY GROUP INC. Quality Assurance Treatment Planning Benchmark PORTEC-3/ TROG 08.04 Randomised Phase III Trial Comparing Concurrent Chemoradiation and Adjuvant Chemotherapy with
Research Article Prognostic Factors in Advanced Non-Small-Cell Lung Cancer Patients: Patient Characteristics and Type of Chemotherapy
 SAGE-Hindawi Access to Research Lung Cancer International Volume 2011, Article ID 152125, 4 pages doi:10.4061/2011/152125 Research Article Prognostic Factors in Advanced Non-Small-Cell Lung Cancer Patients:
SAGE-Hindawi Access to Research Lung Cancer International Volume 2011, Article ID 152125, 4 pages doi:10.4061/2011/152125 Research Article Prognostic Factors in Advanced Non-Small-Cell Lung Cancer Patients: