RCPath Cancer datasets guiding care for the individual and the wider population. Reporting of lung cancer
|
|
|
- Cory Watkins
- 5 years ago
- Views:
Transcription
1 RCPath Cancer datasets guiding care for the individual and the wider population Reporting of lung cancer Thursday 30 th March 2017 Coin Street Conference Centre London Professor Andrew G Nicholson, DM, FRCPath Consultant Histopathologist, Royal Brompton and Harefield NHS Foundation Trust, and Honorary Professor of Respiratory Pathology National Heart and Lung Division Imperial College, London, United Kingdom



2 Purpose of the dataset.
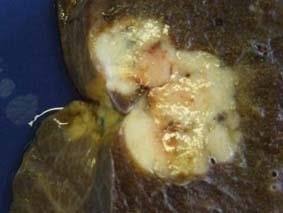
3 CLINICAL DETAILS Adenocarcinoma in right lower lobe. Specimen: A Right upper lobe MACROSCOPIC DESCRIPTION A piece of lung measuring 15x10x8mm. Cut surface shows an ill-defined firm area measuring 7x5x5mm. Bisected & all embedded in A1 (2 pieces). MICROSCOPIC EXAMINATION Sections show a localised area of fibrosis and inflammation within which are several epithelioid granulomas with very focal central necrosis. Acid fast bacilli (AFB) are noted on ZN stain. Special stain for fungi (Grocott) is negative. The features are of granulomatous inflammation due to mycobacterial infection. There is no evidence of malignancy. B 10i C 11i; D 7; E 9 MACROSCOPIC DESCRIPTION Lymph nodes All embedded in B1 (3 pieces); B2 (3 pieces); C1 (1 piece); D1 (2 pieces); E1 (2 pieces) and E2 (3 pieces.) MICROSCOPIC EXAMINATION All lymph nodes showing no granuloma formation or evidence of malignancy. F Right lower lobe of lung MACROSCOPIC DESCRIPTION Right lower lobe measuring 160x160x75mm in the inflated state. At the base of the lobe, there is a circumscribed tumour measuring 42x28mm x approximately 35mm, which abuts the visceral pleura. The tumour lies 75mm from the bronchial resection margin. The remaining lung is unremarkable. F1: bronchial & vascular resection margin (3 pieces); F2-F3: hilar lymph nodes (2 pieces in each); F4-F6: tumour (1 piece in each); F6- F8: random lung (1 piece in each). Tissue remains. MICROSCOPIC EXAMINATION Sections show a non-mucinous adenocaricnoma with mainly acinar (90%) pattern other than an occasional microscopic focus of micropapillary change (10%). The tumour breaches the visceral pleura, confirmed on EVG stain., but does not reach the surface The resection margins are free of atypia and malignancy. The adjacent lung is unremarkable. The hilar lymph node shows no granuloma formation or evidence of malignancy. The adjacent lung is unremarkable. G 11s; H right 2; J 12m; K Highest L 12L; M 10s N Right 4 MACROSCOPIC DESCRIPTION Lymph nodes. G1 (2 pieces); H1 (4 pieces); J1 (4 pieces); K1 (4 pieces); L1: (2 pieces); M1 (1 piece); N1 (2 pieces); N2 (1 piece) & N3 (1 piece). All tissue embedded. MICROSCOPIC EXAMINATION All lymph nodes showing no granuloma formation or evidence of malignancy. Right lower lobe of lung Non-mucinous adenocarcinoma, acinar pattern, predominant. (pt2a N0 PL1, R0) Right uppler lobe of lung - Granulomatous inflammation due to mycobacterial infection.
4 Provides data points for Pathology diagnosis Clinical practice Cancer registration Epidemiologic studies Clinical trials Cancer research
5 AIMS OF PRESENTATION Updated staging Discuss changes to T, N, M staging categories in the 8 th TNM Discuss handling of multiple pulmonary tumour nodules Dealing with in-situ components/subsolid nodules Present correct terminology for small biopsies and cytology specimens (2015 WHO classification) Discuss the lung dataset in relation to molecular testing
6 AIMS OF PRESENTATION Updated staging Discuss changes to T, N, M staging categories in the 8 th TNM Discuss handling of multiple pulmonary tumour nodules Dealing with in-situ components/subsolid nodules Present correct terminology for small biopsies and cytology specimens (2015 WHO classification) Discuss the lung dataset in relation to molecular testing

 Edition of the TNM Classification of Lung Cancer.")
7 # of Countries/Centers # of Patients Countries Centers Patients st 5th 6th 7th 8th Stage Classification Edition 0 Courtesy of Frank Detterbeck: The IASLC Lung Cancer Staging Project: Methodology and Validation Used in the Development of Proposals for Revision of the Stage Classification of Non-Small Cell Lung Cancer in the Forthcoming (Eighth) Edition of the TNM Classification of Lung Cancer. Submitted for publication
8 T stage Recommendations for changes to subclassify T1 into T1a ( 1 cm), T1b (>1 to 2 cm), and T1c (>2 to 3 cm); to subclassify T2 into T2a (>3 to 4 cm) and T2b (>4 to 5 cm); to reclassify tumors greater than 5 to less than or equal to 7 cm as T3; to reclassify tumors greater than 7 cm as T4; to group involvement of main bronchus as T2 regardless of distance from carina; to group partial and total atelectasis/pneumonitis as T2; to reclassify diaphragm invasion as T4; to delete mediastinal pleura invasion as a T descriptor Rami-Porta R et al. The IASLC Lung Cancer Staging Project: Proposals for the Revisions of the T Descriptors in the Forthcoming Eighth Edition of the TNM Classification for Lung Cancer. J Thorac Oncol Jul;10(7):
9 FIGURE 1 A, Survival of pathologically staged T1 T2 N0R0 tumours according to size only, at 1-cm intervals. B, Survival of clinically staged T1 T2 N0 tumours according to size only, at 1-cm intervals. Rami-Porta R et al. The IASLC Lung Cancer Staging Project: Proposals for the Revisions of the T Descriptors in the Forthcoming Eighth Edition of the TNM Classification for Lung Cancer. J Thorac Oncol Jul;10(7): Journal of Thoracic Oncology , DOI: ( /JTO )

10 Survival Comparisons of Pathologically Staged Tumours According to the T Categories of the 7 th Edition and to the Proposed T Categories for the 8 th Edition 7 th Edition Categories Proposed Categories Contrast Estimate Lower Limit Upper Limit P Value Contrast Estimate Lower Limit Upper Limit P Value T1a vs. T1b < T1a vs. T1b < T1b vs. T2a < T1b vs. T1c < T2a vs. T2b < T1c vs. T2a < T2b vs. T < T2a vs. T2b T3 vs. T T2b vs. T < T3 vs. T < Rami-Porta R et al. The IASLC Lung Cancer Staging Project: Proposals for the Revisions of the T Descriptors in the Forthcoming Eighth Edition of the TNM Classification for Lung Cancer. J Thorac Oncol Jul;10(7):
11 T stage Recommendations for changes to subclassify T1 into T1a ( 1 cm), T1b (>1 to 2 cm), and T1c (>2 to 3 cm); to subclassify T2 into T2a (>3 to 4 cm) and T2b (>4 to 5 cm); to reclassify tumors greater than 5 to less than or equal to 7 cm as T3; to reclassify tumors greater than 7 cm as T4; to group involvement of main bronchus as T2 regardless of distance from carina; to group partial and total atelectasis/pneumonitis as T2; to reclassify diaphragm invasion as T4; to delete mediastinal pleura invasion as a T descriptor Rami-Porta R et al. The IASLC Lung Cancer Staging Project: Proposals for the Revisions of the T Descriptors in the Forthcoming Eighth Edition of the TNM Classification for Lung Cancer. J Thorac Oncol Jul;10(7):
12 Survival of pathologically staged T2-T3 main bronchus N0 R0 tumors vs. others by Main Bronchus (PT2 or PT3) pt3 N0 M0 R0 NSCLC 100% 80% 60% 40% 20% 0% Deaths / N pt2 M.Bronchus >=2cm 21 / 75 pt2 Size/Other 2202 / 7660 pt3 M.Bronchus <2cm 8 / 28 pt3 Multiple Other 48 / 77 pt3 Single Other 355 / Year Estimate 66% 70% 69% 33% 49% Years After Surgery Rami-Porta R et al. The IASLC Lung Cancer Staging Project: Proposals for the Revisions of the T Descriptors in the Forthcoming Eighth Edition of the TNM Classification for Lung Cancer. J Thorac Oncol Jul;10(7):
13 Visceral pleural invasion Visceral pleural invasion is well positioned as a T2 descriptor and confers a worse prognosis even after adjusting for the current tumor size cutpoints. The extent of the visceral pleura invasion as currently defined (PL0: tumor within the subpleural lung parenchyma or invades superficially into the pleural connective tissue beneath the elastic layer; PL1: tumor invades beyond the elastic layer; and PL2: tumor invades to the pleural surface) appropriately distinguishes between risk groups and, while the prognosis PL1 and PL2 is worse than that of PL0. There are also significant differences between PL1 and PL2, the latter having a worse prognosis. Further analyses in pathologically and clinically staged tumors show that pathologically staged tumor of >3-4 cm with visceral pleura invasion have similar prognosis than those >4-5 cm; and that those of >4-5 cm with visceral pleura invasion have similar prognosis than those >5-7 cm. Impact on VPI remains the same in 8 th TNM
14 Recommendations for N and M changes N STAGING Current N descriptors adequately predict the prognosis and therefore should be maintained in the forthcoming staging system. Furthermore, we recommend that physicians record the number of metastatic lymph nodes (or stations) and to further classify the N category using new descriptors, such as N1a (single station), N1b (multi station), N2a1 (single/n1- (skip)), N2a2 (single/n1+) N2b (multi), and N3, for further testing M STAGING Cases with pleural/pericardial effusions, contralateral/bilateral lung nodules, contralateral/bilateral pleural nodules, or a combination of multiple of these parameters should continue to be grouped as M1a category. Single metastatic lesions in a single distant organ should be newly designated to the M1b category. Multiple lesions in a single organ or multiple lesions in multiple organs should be reclassified as M1c category. This new division can serve as a first step into providing rational definitions for an oligometastatic disease stage in non-small-cell lung cancer in the future. Asamura H et al. The International Association for the Study of Lung Cancer Lung Cancer Staging Project: Proposals for the Revision of the N Descriptors in the Forthcoming 8th Edition of the TNM Classification for Lung Cancer. J Thorac Oncol. 2015;10: Eberhardt WE et al. The IASLC Lung Cancer Staging Project: Proposals for the Revision of the M Descriptors in the Forthcoming Eighth Edition of the TNM Classification of Lung Cancer. J Thorac Oncol Nov;10(11):
15 AIMS OF PRESENTATION Updated staging Discuss changes to T, N, M staging categories in the 8 th TNM Discuss handling of multiple pulmonary tumour nodules Dealing with in-situ components/subsolid nodules Present correct terminology for small biopsies and cytology specimens (2015 WHO classification) Discuss the lung dataset in relation to molecular testing
16 DISEASE FREE SURVIVAL COMPARING MARTINI MELAMED VS MOLECULAR VS SURGICAL PATHOLOGY Martini Melamed P=0.052 Molecular P=0.013 Surgical Pathology P=0.001 different histology, different lobe time period of >2 yrs favoured second primary. Girard, N, et al: Clin Ca Res 2009:15: Courtesy of WD Travis


17 Genomic profiling: similar profile = metastases Genomic profiling: different profile = multiple primary 42 tumors from 20 patients - 22 tumor pairs were evaluable by CGH. Classification based on genomic profiling contradicted the clinicopathologic diagnosis in 18% of cases Conclusion: Genomic analysis can help distinguish clonal tumors from independent primaries. The development of rapid, inexpensive, and reliable molecular tools may allow for refinement of clinicopathologic criteria currently used in this setting Girard, N, et al: Clin Ca Res 2009:15: ,
18 DISEASE FREE SURVIVAL COMPARING MARTINI MELAMED VS MOLECULAR VS SURGICAL PATHOLOGY Martini Melamed P=0.052 Molecular P=0.013 Surgical Pathology P=0.001 different histology, different lobe time period of >2 yrs favoured second primary. Girard, N, et al: AJSP 33: , 2009 Courtesy of WD Travis
19 Comprehensive histologic assessment methodology for multiple nonsmall cell lung cancer. P value Feature Fisher Exact Nuclear pleomorphism Cell size Gland Formation Nucleolar size Mitotic Rate Nuclear inclusions 0.59 Intra-aveolar Clusters Necrosis pattern Lymphocytosis 0.07 Mucin content 1 Lepidic Growth Vascular invasion 0.83 Macrophage response Clear cell change 0.23 Acute inflammation 0.39 Keratinization 1 Emperipolesis NA Cytoplasmic granules NA Comprehensive Histologic Assessment Helps to Differentiate Multiple Lung Primary Nonsmall Cell Carcinomas From Metastases. Girard, Ni et al. American Journal of Surgical Pathology. 33(12): , 2009 Lippincott Williams & Wilkins, Inc. Published by Lippincott Williams & Wilkins, Inc. 2

")








20 Interobserver variation study on multiple nodules (separate primary tumour versus intrapulmonary metastasis) Undertaken by the IASLC Pathology Committee, Denver, PATHOLOGIST INTEROBSERVER AGREEMENT Kappa is 0.60 This is on H&E only. IHC would likely increase this,? molecular/mdt also. PATHOLOGY-IMAGING INTEROBSERVER AGREEMENT Of 12 cases where there was disagreement, only 3 were SPT and the majority were cases classified on pathology as IM. Kappa value of Unpublished data presented at World IASLC meeting, Denver 2015 IM IM IM IM IM IM IM IM IM IM IM IM IM 0 IM IM IM IM sqcc sqcc SPT SPT SPT SPT SPT SPT SPT SPT SPT SPT SPT SPT SPT SPT SPT SPT SPT SPT LCC MIA
21 Imaging Features Second Primary Lung Cancer Two or more distinct masses with imaging characteristic of lung cancer (e.g. spiculated) Multifocal GG/L Nodules Multiple ground glass or part-solid nodules Pneumonic-Type of Lung Cancer Patchy areas of ground glass and consolidation Separate Tumor Nodule/ Intrapulmonary metastasis Typical lung cancer (e.g. solid, spiculated) with separate solid nodule Pathologic Features TNM Classification Conceptual View Different histotype or different morphology by comprehensive histologic assessment Separate ctnm and ptnm for each cancer Unrelated tumors Adenocarcinomas with prominent lepidic component (typically varying degrees of AIS, MIA, LPA) T based on highest T lesion with (#/m) indicating multiplicity; single N and M Separate tumors, albeit with similarities Same histology throughout (most often invasive mucinous adenocarcinoma) T based on size or T3 if in single lobe, T4 or M1a if in different ipsi- or contralateral lobes; single N and M Single tumor, diffuse pulmonary involvement Distinct masses with the same morphology by comprehensive histologic assessment Location of separate nodule relative to primary site determines if T3, T4 or M1a; single N and M Single tumor with intrapulmonary metastasis The IASLC Lung Cancer Staging Project: Proposals for Revisions of the Classification of Lung Cancers with Multiple Pulmonary Sites of Involvement in the Forthcoming Eighth Edition of the TNM Classification. Frank C. Detterbeck FC, Nicholson AG, Franklin WA, Marom EM et al. Journal of Thoracic Oncology, in press
22 AIMS OF PRESENTATION Updated staging Discuss changes to T, N, M staging categories in the 8 th TNM Discuss handling of multiple pulmonary tumour nodules Dealing with in-situ components/subsolid nodules Present correct terminology for small biopsies and cytology specimens (2015 WHO classification) Discuss the lung dataset in relation to molecular testing
23 Should we only be measuring the invasive area? Disease-free survival (DFS) comparing T1a ( 2 cm) versus T1b (>2 cm or 3 cm). (a) T1a and T1b defined according to gross tumor size (P=0.04). (b) T1a and T1b defined according to invasive size (P<0.001). Yoshizawa A, et al Mod Pathol May;24(5):
24 116 (40%) T1b (>2-3 cm) T1a ( 2 cm) 45 (25%) T2a (>3-5 cm) T1b (>2-3 cm) Kadota K et al, Am J Surg Path 38:448-60, 2014
25 Prognostic Significance of Solid vs Whole Tumor Size by HRCT 502 Stage IA Adenoca DFS by HRCT A: 3 yr DFS 92.5% 2 cm and 86.7 >2cm B: 3 yr DFS 93.2% 2 cm and 78.9 >2cm Solid size independent predictor in multivariate analysis (HR 2.30; 95% CI ) Tsutani et al JTCVS 143:607-12, 2012
 If multiple OK to use")


26 PROPOSAL FOR 8 TH EDITION TNM In situ carcinoma Tis (AIS) Tis (SCIS) Minimally invasive adenocarcinoma T1a(mi) If multiple OK to use T1a(mi)(m) 21mm T1b (7 th TNM) 4mm T1a(mi) (8 th TNM) The IASLC Lung Cancer Staging Project: Proposals for Coding T Categories for Subsolid Nodules and Assessment of Tumor Size in Part-Solid Tumors in the Forthcoming Eighth Edition of the TNM Classification of Lung Cancer. Travis WD et al. JTO, 2016



27 Part solid nodules with small solid component Small solid component within a subsolid nodule may indicate invasive adenocarcinoma.but not always Adenocarcinoma in situ (Noguchi type B) c/o Professor K Kerr
28 AIMS OF PRESENTATION Updated staging Discuss changes to T, N, M staging categories in the 8 th TNM Discuss handling of multiple pulmonary tumour nodules Dealing with in-situ components/subsolid nodules Present correct terminology for small biopsies and cytology specimens (2015 WHO classification) Discuss the lung dataset in relation to molecular testing
29 2015 WHO CLASSIFICATION 1-2: Adenocarcinoma 1-2A Invasive adenocarcinoma 1-2B Variants of invasive adenocarcinoma 1-2C Minimally invasive adenocarcinoma 1-2D Preinvasive lesions 1-2D-i: Atypical adenomatous hyperplasia 1-2D-ii: Adenocarcinoma in situ 1-3: Squamous cell carcinoma 1-3A: Keratinizing and nonkeratinizing squamous cell carcinoma 1-3B: Basaloid carcinoma 1-3C: Preinvasive lesion: Squamous carcinoma in situ 1-4: Neuroendocrine Tumours 1-4A: Small cell carcinoma 1-4B: Large cell neuroendocrine carcinoma 1-4C: Carcinoid tumors 1-4D: Preinvasive lesion: Diffuse idiopathic pulmonary neuroendocrine cell hyperplasia 1-5: Large cell carcinoma 1-6: Adenosquamous carcinoma 1-1: Introduction 1-1A Lung cancer staging and grading 1-1B Rationale for classification in small biopsies and cytology 1-1C Terminology and criteria in non-resection specimens 1-1D Molecular testing for treatment selection in lung cancer 1-7: Sarcomatoid carcinoma 1-7A: Pleomorphic, spindle cell and giant cell carcinoma 1-7B: Carcinosarcoma 1-7C: Pulmonary blastoma 1-8: Other carcinomas 1-8A: Lymphoepithelioma-like carcinoma 1-8B: NUT-carcinoma

")
 Invasive mucinous adenocarcinoma Invasive mucinous adenocarcinoma (describe patterns present; use")


30 SPECIFIC TERMINOLOGY AND CRITERIA FOR ADENOCARCINOMA, SQUAMOUS CELL CARCINOMA AND NON-SMALL CELL CARCINOMA-NOS IN SMALL BIOPSIES AND CYTOLOGY 2015 WHO Classification in resection specimens Morphology/Stains New Small Biopsy/Cytology Terminology ADENOCARCINOMA (Predominant pattern) Acinar Papillary Solid Micropapillary Morphologic adenocarcinoma patterns clearly present Adenocarcinoma (describe identifiable patterns present) Lepidic (nonmucinous) Adenocarcinoma with lepidic pattern (if pure, add note: an invasive component cannot be excluded) Invasive mucinous adenocarcinoma Invasive mucinous adenocarcinoma (describe patterns present; use term mucinous adenocarcinoma with lepidic pattern if pure lepidic pattern see text) Colloid adenocarcinoma Fetal adenocarcinoma Enteric adenocarcinoma Adenocarcinoma with mucinous features Adenocarcinoma with fetal features Adenocarcinoma with enteric features SQUAMOUS CELL CARCINOMA Morphologic squamous cell patterns clearly present Squamous cell carcinoma Adapted from: Travis WD et al. IASLC/ATS/ERS classification of ADCs J Thor Oncol 2011;6:
 Small")


 NSCC, NE marker +ve,?")
31 CLASSIFICATION FOR SMALL BIOPSIES/CYTOLOGY COMPARING 2015 WHO TERMS WITH NEW TERMS FOR SMALL CELL CARCINOMA, LARGE CELL NEUROENDOCRINE CARCINOMA, ADENOSQUAMOUS CARCINOMA AND SARCOMATOID CARCINOMA 2015 WHO Classification SMALL BIOPSY/CYTOLOGY: IASLC/ATS/ERS SMALL CELL CARCINOMA LARGE CELL NEUROENDOCRINE CARCINOMA (LCNEC) Small cell carcinoma Non-small cell carcinoma with neuroendocrine (NE) morphology and positive NE markers, possible LCNEC ADENOSQUAMOUS CARCINOMA No counterpart in 2015 WHO classification Pleomorphic, spindle and/or giant cell carcinoma Morphologic squamous cell and adenocarcinoma patterns present: Non-small cell carcinoma, NOS, (comment that adenocarcinoma and squamous components are present and this could represent adenosquamous carcinoma). Morphologic squamous cell or adenocarcinoma patterns not present but immunostains favor separate glandular and adenocarcinoma components Non-small cell carcinoma, NOS, (specify the results of the immunohistochemical stains and the interpretation) Comment: this could represent adenosquamous carcinoma. NSCC with spindle and/or giant cell carcinoma (mention if adenocarcinoma or squamous carcinoma are present) NSCC, NE marker +ve,?lcnec with pleomorphic features chromogranin Adapted from: Travis WD et al. IASLC/ATS/ERS classification of ADCs J Thor Oncol 2011;6:
 and 2 are highly expressed in pleomorphic")

32 MET exon 14 skipping mutations: responses to cabozantinib Paul K. Paik et al. Cancer Discovery 2015;5: Programmed death-1 Ligand 1 (PD-L1) and 2 are highly expressed in pleomorphic carcinomas of the lung: Comparison of sarcomatous and carcinomatous areas. Kim S et al. Eur J Cancer. 2015;51: High co-expression of PD-L1 and HIF-1α correlates with tumour necrosis in pulmonary pleomorphic carcinoma. Chang YL et al. Eur J Cancer epub
33 USE OF IMMUNOHISTOCHEMISTRY WHEN A TUMOUR SHOWS NON-SMALL CELL CARCINOMA- NOT OTHERWISE SPECIFIED (NOS) IN SMALL BIOPSIES AND CYTOLOGY SPECIFIC TERMINOLOGY AND CRITERIA FOR ADENOCARCINOMA, SQUAMOUS CELL CARCINOMA AND NON-SMALL CELL CARCINOMA-NOS IN SMALL BIOPSIES AND CYTOLOGY 2015 WHO Classification in resection specimens Morphology/Stains New Small Biopsy/Cytology Terminology Adenocarcinoma (solid pattern may be just one component of the tumor) Squamous cell carcinoma, (nonkeratinizing pattern may be just one component of the tumor) LARGE CELL CARCINOMA Morphologic adenocarcinoma patterns not present, but supported by special stains, i.e. +TTF-1 Morphologic squamous cell patterns not present, but supported by stains i.e. +p40 No clear adenocarcinoma, squamous or neuroendocrine morphology or staining pattern Non-small cell carcinoma, favour adenocarcinoma using IHC Non-small cell carcinoma, favour squamous cell carcinoma using IHC Non-small cell carcinoma, not otherwise specified NSCLC-NOS using IHC Adapted from: Travis WD et al. IASLC/ATS/ERS classification of ADCs J Thor Oncol 2011;6:





34 GENERAL PRINCIPLES NSCLC, favouring ADC TTF-1 P40 NSCLC, favouring SQCC TTF-1 Cut tissue block as sparingly as possible Obtain unstained slides for molecular at time of cutting block for IHC Minimize stains to maximize tissue for molecular testing by using a limited panel of IHC (i.e TTF-1 and P40) Further molecular testing, if clinically appropriate, can be performed on remaining tissue
35 LIGHT MICROSCOPY SQUAMOUS CELL CARCINOMA 20-30% NEW CLASSIFICATION NSCLC-NOS 20-40% TTF-1 and P40 GOAL = 5% ADENO- CARCINOMA 40-50%
 POSITIVE CYTOLOGY (effusion, aspirate, washings, brushings) NE morphology, large cells,")
36 Adapted from: Travis WD et al. IASLC/ATS/ERS classification of ADCs J Thor Oncol 2011;6: STEP 1 POSITIVE BIOPSY (FOB, TBBx, Core, SLBx) POSITIVE CYTOLOGY (effusion, aspirate, washings, brushings) NE morphology, large cells, NE IHC+ NE morphology, small cells, no nucleoli, NE IHC+, TTF-1 +/-, CK + Keratinization, pearls and/or intercellular bridges NSCLC,?LCNEC SCLC Classic Morphology: SQCC Histology: Lepidic, papillary, micropapillary and/or acinar architecture(s) Cytology: 3-D arrangements, delicate foamy/ vacuolated (translucent) cytoplasm, Fine nuclear chromatin and often prominent nucleoli Nuclei are often eccentrically situated No clear ADC or SQCC morphology: NSCLC-NOS NSCLC, favor SQCC ADC marker and/or Mucin +ve; SQCC marker ve (or weak in same cells) Classic morphology: ADC STEP 2 Apply ancillary panel of one SQCC and one ADC marker +/or Mucin SQCC marker +ve ADC marker -ve/or Mucin -ve NSCLC, favor ADC IHC ve and Mucin -ve NSCLC NOS ADC marker or Mucin +ve; as well as SQCC marker +ve in different cells Molecular analysis: e.g. EGFR mutation, ALK rearrangement NSCLC, NOS, possible adenosquamous ca STEP 3 If tumor tissue inadequate for molecular testing, discuss need for further sampling - back to Step 1
 POSITIVE CYTOLOGY (effusion, aspirate, washings, brushings) NE morphology, large cells,")
37 Adapted from: Travis WD et al. IASLC/ATS/ERS classification of ADCs J Thor Oncol 2011;6: STEP 1 POSITIVE BIOPSY (FOB, TBBx, Core, SLBx) POSITIVE CYTOLOGY (effusion, aspirate, washings, brushings) NE morphology, large cells, NE IHC+ NE morphology, small cells, no nucleoli, NE IHC+, TTF-1 +/-, CK + Keratinization, pearls and/or intercellular bridges NSCLC,?LCNEC SCLC Classic Morphology: SQCC Histology: Lepidic, papillary, micropapillary and/or acinar architecture(s) Cytology: 3-D arrangements, delicate foamy/ vacuolated (translucent) cytoplasm, Fine nuclear chromatin and often prominent nucleoli Nuclei are often eccentrically situated No clear ADC or SQCC morphology: NSCLC-NOS NSCLC, favor SQCC Morgensztern, D-C et al. Journal of Thoracic Oncology. 10:S1-S63, January 2015 NEXT GENERATION SEQUENCING IMMUNOMODULATORY THERAPY (e.g. PD-L1) ADC marker and/or Mucin +ve; SQCC marker ve (or weak in same cells) Classic morphology: ADC NSCLC, favor ADC Molecular analysis: e.g. EGFR mutation, ALK rearrangement STEP 2 Apply ancillary panel of one SQCC and one ADC marker +/or Mucin IHC ve and Mucin -ve NSCLC NOS STEP 3 If tumor tissue inadequate for molecular testing, discuss need for further sampling - back to Step 1 SQCC marker +ve ADC marker -ve/or Mucin -ve ADC marker or Mucin +ve; as well as SQCC marker +ve in different cells NSCLC, NOS, possible adenosquamous ca
38 = reflex molecular testing = molecular testing on request = all samples SAMPLE Undifferentiated NSCC on H&E ADC, SQCC on H&E SCLC or carcinoid on H&E Diagnostic IHC panel TTF-1 p40 (or p63 or CK5/6) *CD56, chromogranin, synaptophysin only if there is suggestion of neuroendocrine morphology NSCC- favour ADC, NSCC- favour SQCC NSCC- NOS NSCC-? LCNEC NSCC-? ADSQCC Other MDT review Diagnostic IHC, if appropriate TTF-1, CD56 Chromogranin, Synaptophysin MNF116 *other IHC only if there is a question as to primary site not being lung TREATMENT Therapy-related IHC, if appropriate: ALK, PD-L1, (ROS1) MOLECULAR TESTING, if appropriate: Current therapies (e.g. EGFR) Clinical trials
39 AIMS OF PRESENTATION Updated staging Discuss changes to T, N, M staging categories in the 8 th TNM Discuss handling of multiple pulmonary tumour nodules Dealing with in-situ components/subsolid nodules Present correct terminology for small biopsies and cytology specimens (2015 WHO classification) Discuss the lung dataset in relation to molecular testing
40 MOLECULAR ISSUES Come to recognise the increasing importance of immunohistochemistry and genetics in the diagnosis of lung tumours. TREATMENT OPTIONS.. will drive changes in classification and pathology practice Conventional chemotherapy Pemetrexed (non-squamous NSCLC), Bevacizumab (non-squamous NSCLC) Targeted agents EGFR mutations: Gefitinib, Erlotinib, Afatinib (T790M mutation) ALK translocations: Crizotinib, Alectinib ROS translocations: Crizotinib Immunomodulatory drugs Therapeutic vaccines priming the immune response e.g., MAGE-A3 (vaccine targeting MAGE-A3) 3, TG4010 (vaccine encoding MUC-1 and IL-2) 4, IMA901 (peptide vaccine) 5, racotumomab (anti-idiotype vaccine) 6, sipuleucel-t (Provenge, cellular therapeutic vaccine) 7, nelipepimut-s (E75/NeuVax, peptide vaccine) 8 Agents targeting T-cell checkpoint dysregulation 2 e.g., nivolumab (anti-pd-1), pembrolizumab (anti-pd-1), MPDL3280A (anti-pd-l1), MEDI4736 (anti-pd-l1), ipilimumab (anti-ctla-4), tremelimumab (anti-ctla-4)
41 Evolution and importance of biomarker use in NSCLC Targets today EGFR ALK ROS1 Targets in the future KRAS and others BRAF HER2 RET DDR2 MET and others FGR1 P13K Adenocarcinoma Large-cell carcinoma Squamous cell carcinoma Small-cell lung cancer Small-cell lung cancer 2000 Non-small-cell lung cancer Small-cell lung cancer 1990 Lung cancer Adenocarcinoma Adenocarcinoma and treatable oncogenic alterations with approved drugs (EGFR mutation and ALK translocation) Figure adapted from Reck M, et al. Lancet 2013;383: Large-cell carcinoma Small-cell lung cancer Squamous cell carcinoma without oncogenic alteration Squamous cell carcinoma with oncogenic alteration Evolution of biomarkers has driven guideline development Patient selection expedites clinical trials and drug approvals The resultant increase in complexity of therapy is also reflected in guidelines Courtesy of Prof Keith Kerr, Aberdeen

42 2017/8 2015/

43 Molecular targeted therapy has proven benefits



44 Molecular Testing Guideline for Selection of Lung Cancer Patients Revision. Yasushi Yatabe, MD, PhD AMP Co-chair, CAP/IASLC/AMP Lung Cancer Biomarkers Revision Workgroup Eric Bernicker, MD CAP Expert Panelist - CAP/IASLC/AMP Lung Cancer Biomarkers Revision Workgroup Ming Tsao, MD IASLC Expert Panelist, CAP/IASLC/AMP Lung Cancer Biomarkers Revision Workgroup Expertise that advances patient care through education, innovation, and advocacy.
45 PD-1 and PD-Ll - Drugs and assays Methodology Kit assay Automated Platform Checkpoint inhibitors APPROVAL FOR LUNG CANCER TREATEMENT (as of Nov 15) All second line Dako pharmdx 22C3 Dako Autostainer Link 48 Pembrolizumab (PD- 1) Keytruda (MSD) All NSCLCs (FDA and UK/EU) COMPANION DIAGNOSTIC Tumour cells? 1%,? 50% Dako PD-L1 IHC 28-8 pharmdx Dako Autostainer Link 48 Nivolumab (PD-1) (BMS) Opdivo Squamous NSCLC (FDA and UK/EU) All NSCLC (FDA) COMPLEMENTARY DIAGNOSTIC Tumour cells 1%, 5%, 10% Kit based Assay Tumour cells (1%, 5%, 50%) SP142: Kit form TBC Ventana: TBC Atezolizumab L1) (Roche) (PD- Not yet licensed COMPANION DIAGNOSTIC TILs (%age of surface area infiltrated by positive TILs) (1%, 5%, 10%) SP263: Kit form TBC Ventana Ultra, XT and GX platforms Durvalumab (PD-L1) (AZ/Medimmune) Not yet licensed COMPANION DIAGNOSTIC Tumour cells? 25% Avulumab (PD-1) (Merck Serono) 1% (and? 80%) Stand alone PD-L1 antibodies 28-8 (RabMab): BMS clone available from Abcam E1L3N (RabMab): Cell Signaling SP142 (RabMab): Spring Bioscience Updated from Kerr K et al. JTO 2015.
46 Analytical Comparison of Tumor cell/immune Cell Staining Each dot represents the mean score of 3 pathologists


47 Variability in Tumor Cells Staining between Assays Strong staining tumor Weak staining tumor
48 Conclusion of Blueprint 1 Project Three of the four assays were closely aligned on tumor cell staining whereas the fourth showed consistently fewer tumor cells stained. All of the assays demonstrated immune cell staining, but with greater variability than with tumor cell staining. Despite similar analytical performance of PD-L1 expression for three assays, interchanging assays (with cut-offs) would lead to misclassification of PD-L1 status for some patients. However, using drug-specified cut-off, the use of 3 assays (22C3, 28-8 and SP263) may potentially be harmonized.

49 Blueprint phase 2 - Goals Validation of Blueprint phase 1 results using different types of clinical samples (resection, small biopsy, cytology cell block) Comparability and heterogeneity of PD-L1 assay results in surgical tumor resection, core needle and FNA samples prepared from same tumor. Inter-observers concordance among larger panel of pulmonary pathologists Concordance of PD-L1 scoring using standard light microscopy vs. digital images accessed by web-based system. Available later this year
50 CONCLUSIONS Reporting of lung cancer - classification 1967 Histologic Typing of Lung Tumours 1981 Histologic Typing of Lung Tumours 1999 Histologic Typing of Tumours of the Lung and Pleura 2004 Pathology and Genetics: Tumours of the Lung, Pleura, Thymus and Heart Pathology and Genetics: Tumours of the Lung, Pleura, Thymus and Heart INCREASING COMPLEXITY New treatment options, Increasing molecular data New sampling techniques, New investigative methods
51 CONCLUSION Major Changes in Classification that Impact Diagnosis of Surgically Resected Patients Main advances in lung adenocarcinoma: adopted the 2011 IASLC/ATS/ERS Lung Adenocarcinoma classification. Improved prognostic significance. Proposed changes to TNM staging. Restrict large cell carcinoma to tumors lacking clear differentiation by both IHC and morphology Reclassify squamous ca: keratinizing, need IHC (i.e. p40) for nonkeratinizing and basaloid Group NE tumors together (TC, AC, LCNEC, SCLC)
52 CONCLUSION 2015 Classification: Impact on Management of Advanced Lung Cancer Patients Criteria/terminology for small bx/cytology More accurate histologic subtyping Strategic management of small tissues Streamlining workflow for molecular testing Need for local multidisciplinary team

53 CONCLUSION Reporting of lung cancer Molecular testing Future classification Balance of morphology and molecular data needs to be maintained How to select core items.? based on availability on treatments in the NHS Guidance on ensuring that tissue is handled as efficiently as possible to ensure optimal patient management. Pre-examination phase Examination phase Post-examination phase Research/clinical trials

54 Acknowledgements: Bill Travis, USA Keith Kerr, UK; Lynette Sholl, USA; Yasushi Yatabe, Japan.
Histopathology of NSCLC, IHC markers and ptnm classification
 ESMO Preceptorship on Non-Small Cell Lung Cancer November 15 th & 16 th 2017 Singapore Histopathology of NSCLC, IHC markers and ptnm classification Prof Keith M Kerr Department of Pathology, Aberdeen University
ESMO Preceptorship on Non-Small Cell Lung Cancer November 15 th & 16 th 2017 Singapore Histopathology of NSCLC, IHC markers and ptnm classification Prof Keith M Kerr Department of Pathology, Aberdeen University
LUNG CANCER. pathology & molecular biology. Izidor Kern University Clinic Golnik, Slovenia
 LUNG CANCER pathology & molecular biology Izidor Kern University Clinic Golnik, Slovenia 1 Pathology and epidemiology Small biopsy & cytology SCLC 14% NSCC NOS 4% 70% 60% 50% 63% 62% 61% 62% 59% 54% 51%
LUNG CANCER pathology & molecular biology Izidor Kern University Clinic Golnik, Slovenia 1 Pathology and epidemiology Small biopsy & cytology SCLC 14% NSCC NOS 4% 70% 60% 50% 63% 62% 61% 62% 59% 54% 51%
Disclosure of Relevant Financial Relationships NON-SMALL CELL LUNG CANCER: 70% PRESENT IN ADVANCED STAGE
 MORPHOLOGY AND MOLECULAR TESTING IN NON-SMALL CELL OF LUNG NEW FRONTIEIRS IN CYTOPATHOLOGY PRACTICE American Society for Cytopathology San Antonio, Texas Sunday March 5, 2017 Disclosure of Relevant Financial
MORPHOLOGY AND MOLECULAR TESTING IN NON-SMALL CELL OF LUNG NEW FRONTIEIRS IN CYTOPATHOLOGY PRACTICE American Society for Cytopathology San Antonio, Texas Sunday March 5, 2017 Disclosure of Relevant Financial
3/23/2017. Disclosure of Relevant Financial Relationships. Pathologic Staging Updates in Lung Cancer T STAGE OUTLINE SURVIVAL ACCORDING TO SIZE ONLY
 Pathologic Staging Updates in Lung Cancer Disclosure of Relevant Financial Relationships USCAP requires that all planners (Education Committee) in a position to influence or control the content of CME
Pathologic Staging Updates in Lung Cancer Disclosure of Relevant Financial Relationships USCAP requires that all planners (Education Committee) in a position to influence or control the content of CME
Cytological Sub-classification of Lung Cancer: Morphologic and Molecular Characteristics. Mercè Jordà, University of Miami
 Cytological Sub-classification of Lung Cancer: Morphologic and Molecular Characteristics Mercè Jordà, University of Miami Mortality Lung cancer is the most frequent cause of cancer incidence and mortality
Cytological Sub-classification of Lung Cancer: Morphologic and Molecular Characteristics Mercè Jordà, University of Miami Mortality Lung cancer is the most frequent cause of cancer incidence and mortality
Impact of immunostaining of pulmonary and mediastinal cytology
 Impact of immunostaining of pulmonary and mediastinal cytology Harman Sekhon MD, PhD Director of Cytopathology Head of Ottawa-site Ontario Tumour Bank June 20, 2014 Disclaimer Pfizer: Honorarium-Advisory
Impact of immunostaining of pulmonary and mediastinal cytology Harman Sekhon MD, PhD Director of Cytopathology Head of Ottawa-site Ontario Tumour Bank June 20, 2014 Disclaimer Pfizer: Honorarium-Advisory
Steering Committee. Waiting on photo. Paul A. Bunn, Jr., MD Kavita Garg, MD Kim Geisinger, MD Fred R. Hirsch, Gregory Riely, MD, PhD.
 Steering Committee Paul A. Bunn, Jr., MD Kavita Garg, MD Kim Geisinger, MD Fred R. Hirsch, Gregory Riely, MD, PhD MD, PhD Waiting on photo Paul Van Schil, MD, PhD William D. Travis, MD Ming-Sound Tsao,
Steering Committee Paul A. Bunn, Jr., MD Kavita Garg, MD Kim Geisinger, MD Fred R. Hirsch, Gregory Riely, MD, PhD MD, PhD Waiting on photo Paul Van Schil, MD, PhD William D. Travis, MD Ming-Sound Tsao,
Lung Neoplasia II Resection specimens Pathobasic. Lukas Bubendorf Pathology
 Lung Neoplasia II Resection specimens Pathobasic Lukas Bubendorf Pathology Agenda Preneoplastic lesions Histological subtypes of lung cancer Histological patterns of AC Cells of origin and characteristic
Lung Neoplasia II Resection specimens Pathobasic Lukas Bubendorf Pathology Agenda Preneoplastic lesions Histological subtypes of lung cancer Histological patterns of AC Cells of origin and characteristic
Non-Small Cell Lung Carcinoma - Myers
 Role of Routine Histology and Special Testing in Managing Patients with Non- Small Cell Lung Carcinoma Jeffrey L. Myers, M.D. A. James French Professor Director, Anatomic Pathology & MLabs University of
Role of Routine Histology and Special Testing in Managing Patients with Non- Small Cell Lung Carcinoma Jeffrey L. Myers, M.D. A. James French Professor Director, Anatomic Pathology & MLabs University of
Non Small Cell Lung Cancer Histopathology ד"ר יהודית זנדבנק
 Non Small Cell Lung Cancer Histopathology ד"ר יהודית זנדבנק 26.06.09 Lecture outlines WHO histological classification Macro/Micro assessment Early diagnosis Minimal pathology Main subtypes SCC, AdCa, LCLC
Non Small Cell Lung Cancer Histopathology ד"ר יהודית זנדבנק 26.06.09 Lecture outlines WHO histological classification Macro/Micro assessment Early diagnosis Minimal pathology Main subtypes SCC, AdCa, LCLC
Steering Committee. Waiting on photo. Paul A. Bunn, Jr., MD Kavita Garg, MD Kim Geisinger, MD Fred R. Hirsch, Gregory Riely, MD, PhD.
 Steering Committee Paul A. Bunn, Jr., MD Kavita Garg, MD Kim Geisinger, MD Fred R. Hirsch, Gregory Riely, MD, PhD MD, PhD Waiting on photo Paul Van Schil, MD, PhD William D. Travis, MD Ming-Sound Tsao,
Steering Committee Paul A. Bunn, Jr., MD Kavita Garg, MD Kim Geisinger, MD Fred R. Hirsch, Gregory Riely, MD, PhD MD, PhD Waiting on photo Paul Van Schil, MD, PhD William D. Travis, MD Ming-Sound Tsao,
LUNG CANCER PATHOLOGY: UPDATE ON NEUROENDOCRINE LUNG TUMORS
 LUNG CANCER PATHOLOGY: UPDATE ON NEUROENDOCRINE LUNG TUMORS William D. Travis, M.D. Attending Thoracic Pathologist Memorial Sloan Kettering Cancer Center New York, NY PULMONARY NE TUMORS CLASSIFICATION
LUNG CANCER PATHOLOGY: UPDATE ON NEUROENDOCRINE LUNG TUMORS William D. Travis, M.D. Attending Thoracic Pathologist Memorial Sloan Kettering Cancer Center New York, NY PULMONARY NE TUMORS CLASSIFICATION
HOW TO GET THE MOST INFORMATION FROM A TUMOR BIOPSY
 HOW TO GET THE MOST INFORMATION FROM A TUMOR BIOPSY 7 TH Annual New York Lung Cancer Symposium Saturday, November 10, 2012 William D. Travis, M.D. Attending Thoracic Pathologist Memorial Sloan Kettering
HOW TO GET THE MOST INFORMATION FROM A TUMOR BIOPSY 7 TH Annual New York Lung Cancer Symposium Saturday, November 10, 2012 William D. Travis, M.D. Attending Thoracic Pathologist Memorial Sloan Kettering
Difficult Diagnoses and Controversial Entities in Neoplastic Lung
 Difficult Diagnoses and Controversial Entities in Neoplastic Lung Lynette M. Sholl, M.D. Associate Pathologist, Brigham and Women s Hospital Chief, Pulmonary Pathology Service Associate Professor, Harvard
Difficult Diagnoses and Controversial Entities in Neoplastic Lung Lynette M. Sholl, M.D. Associate Pathologist, Brigham and Women s Hospital Chief, Pulmonary Pathology Service Associate Professor, Harvard
Update on 2015 WHO Classification of Lung Adenocarcinoma 1/3/ Mayo Foundation for Medical Education and Research. All rights reserved.
 1 Our speaker for this program is Dr. Anja Roden, an associate professor of Laboratory Medicine and Pathology at Mayo Clinic as well as consultant in the Anatomic Pathology Laboratory and co-director of
1 Our speaker for this program is Dr. Anja Roden, an associate professor of Laboratory Medicine and Pathology at Mayo Clinic as well as consultant in the Anatomic Pathology Laboratory and co-director of
Ground Glass Opacities
 Ground Glass Opacities A pathologist s perspective Marie-Christine Aubry, M.D. Professor of Pathology Mayo Clinic Objectives Discuss the proposed new pathologic classification of adenocarcinoma with historical
Ground Glass Opacities A pathologist s perspective Marie-Christine Aubry, M.D. Professor of Pathology Mayo Clinic Objectives Discuss the proposed new pathologic classification of adenocarcinoma with historical
The 2015 World Health Organization Classification for Lung Adenocarcinomas: A Practical Approach
 The 2015 World Health Organization Classification for Lung Adenocarcinomas: A Practical Approach Dr. Carol Farver Director, Pulmonary Pathology Pathology and Laboratory Medicine Institute Objectives Discuss
The 2015 World Health Organization Classification for Lung Adenocarcinomas: A Practical Approach Dr. Carol Farver Director, Pulmonary Pathology Pathology and Laboratory Medicine Institute Objectives Discuss
Role of the pathologist in the diagnosis and mutational analysis of lung cancer Professor J R Gosney
 Role of the pathologist in the diagnosis and mutational analysis of lung cancer Professor J R Gosney Consultant Thoracic Pathologist Royal Liverpool University Hospital Disclosure JRG is a paid advisor
Role of the pathologist in the diagnosis and mutational analysis of lung cancer Professor J R Gosney Consultant Thoracic Pathologist Royal Liverpool University Hospital Disclosure JRG is a paid advisor
8/22/2016. Major risk factors for the development of lung cancer are: Outline
 Carcinomas of the Lung: Changes in Staging, Adenocarcinoma Classification and Genetics Grace Y. Lin, M.D., Ph.D. Outline Background Staging of Lung Cancer: Review of the 2010 7 th Edition of the AJCC Cancer
Carcinomas of the Lung: Changes in Staging, Adenocarcinoma Classification and Genetics Grace Y. Lin, M.D., Ph.D. Outline Background Staging of Lung Cancer: Review of the 2010 7 th Edition of the AJCC Cancer
The 8th Edition of the TNM Classification for Lung Cancer Background, Innovations and Implications for Clinical Practice
 The 8th Edition of the TNM Classification for Lung Cancer Background, Innovations and Implications for Clinical Practice University of Torino Lecture 28th June 2017 Torino, Italy Ramón Rami-Porta Thoracic
The 8th Edition of the TNM Classification for Lung Cancer Background, Innovations and Implications for Clinical Practice University of Torino Lecture 28th June 2017 Torino, Italy Ramón Rami-Porta Thoracic
Minimally invasive adenocarcinoma. 5mm or less = microinvasion No necrosis No lymphatic or pleural invasion No spread through air-spaces (STAS)
") Minimally invasive adenocarcinoma 5mm or less = microinvasion No necrosis No lymphatic or pleural invasion No spread through air-spaces (STAS) 2b lepidic acinar 2c papillary micropapillary solid 2d cribriform
Minimally invasive adenocarcinoma 5mm or less = microinvasion No necrosis No lymphatic or pleural invasion No spread through air-spaces (STAS) 2b lepidic acinar 2c papillary micropapillary solid 2d cribriform
Lung Cancer Update on Pathology Zhaolin Xu, MD, FRCPC, FCAP
 Lung Cancer Update on Pathology Zhaolin Xu, MD, FRCPC, FCAP Professor, Dept of Pathology, Dalhousie University Pulmonary Pathologist and Cytopathologist, QEII HSC Senior Scientist, Beatrice Hunter Cancer
Lung Cancer Update on Pathology Zhaolin Xu, MD, FRCPC, FCAP Professor, Dept of Pathology, Dalhousie University Pulmonary Pathologist and Cytopathologist, QEII HSC Senior Scientist, Beatrice Hunter Cancer
Advances in Pathology and molecular biology of lung cancer. Lukas Bubendorf Pathologie
 Advances in Pathology and molecular biology of lung cancer Lukas Bubendorf Pathologie Agenda The revolution of predictive markers Liquid biopsies PD-L1 Molecular subtypes (non-squamous NSCLC) Tsao AS et
Advances in Pathology and molecular biology of lung cancer Lukas Bubendorf Pathologie Agenda The revolution of predictive markers Liquid biopsies PD-L1 Molecular subtypes (non-squamous NSCLC) Tsao AS et
5/1/2009. Squamous Dysplasia/CIS AAH DIPNECH. Adenocarcinoma
 Pathological Assessment of Diagnostic Specimens Keith Kerr Department of Pathology Aberdeen University Medical School Aberdeen Royal Infirmary Foresterhill, Aberdeen, Scotland, UK Tumours of the Lung:
Pathological Assessment of Diagnostic Specimens Keith Kerr Department of Pathology Aberdeen University Medical School Aberdeen Royal Infirmary Foresterhill, Aberdeen, Scotland, UK Tumours of the Lung:
The International Association for the Study of Lung Cancer (IASLC) Lung Cancer Staging Project, Data Elements
 Lung Cancer Staging Project, Data Elements") Page 1 Contents 1.1. Registration... 2 1.2. Patient Characteristics... 3 1.3. Laboratory Values at Diagnosis... 5 1.4. Lung Cancers with Multiple Lesions... 6 1.5. Primary Tumour Description... 10 1.6.
Page 1 Contents 1.1. Registration... 2 1.2. Patient Characteristics... 3 1.3. Laboratory Values at Diagnosis... 5 1.4. Lung Cancers with Multiple Lesions... 6 1.5. Primary Tumour Description... 10 1.6.
Histology: Its Influence on Therapeutic Decision Making
 Histology: Its Influence on Therapeutic Decision Making Mark A. Socinski, MD Professor of Medicine and Thoracic Surgery Director, Lung Cancer Section, Division of Hematology/Oncology Co-Director, UPMC
Histology: Its Influence on Therapeutic Decision Making Mark A. Socinski, MD Professor of Medicine and Thoracic Surgery Director, Lung Cancer Section, Division of Hematology/Oncology Co-Director, UPMC
MICROSCOPY PREDICTIVE PROFILING
 Immunomodulatory therapy in NSCLC: a year into clinical practice Professor J R Gosney Consultant Thoracic Pathologist Royal Liverpool University Hospital Disclosure JRG is a paid advisor to and speaker
Immunomodulatory therapy in NSCLC: a year into clinical practice Professor J R Gosney Consultant Thoracic Pathologist Royal Liverpool University Hospital Disclosure JRG is a paid advisor to and speaker
Neuroendocrine Lung Tumors Myers
 Diagnosis and Classification of Neuroendocrine Lung Tumors Jeffrey L. Myers, M.D. A. James French Professor Director, Anatomic Pathology & MLabs University of Michigan, Ann Arbor, MI myerjeff@umich.edu
Diagnosis and Classification of Neuroendocrine Lung Tumors Jeffrey L. Myers, M.D. A. James French Professor Director, Anatomic Pathology & MLabs University of Michigan, Ann Arbor, MI myerjeff@umich.edu
THE IASLC/ERS/ATS ADENOCARCINOMA CLASSIFICATION RATIONALE AND STRENGTHS
 THE IASLC/ERS/ATS ADENOCARCINOMA CLASSIFICATION RATIONALE AND STRENGTHS PULMONARY PATHOLOGY SOCIETY USCAP, BALTIMORE, March 2, 2013 William D. Travis, M.D. Dept of Pathology, Memorial Sloan-Kettering Cancer
THE IASLC/ERS/ATS ADENOCARCINOMA CLASSIFICATION RATIONALE AND STRENGTHS PULMONARY PATHOLOGY SOCIETY USCAP, BALTIMORE, March 2, 2013 William D. Travis, M.D. Dept of Pathology, Memorial Sloan-Kettering Cancer
Diagnostic & Predictive Immunohistochemistry in Lung Carcinomas
 Diagnostic & Predictive Immunohistochemistry in Lung Carcinomas Lynette M. Sholl, M.D. Associate Pathologist, Brigham and Women s Hospital Associate Professor, Harvard Medical School Boston, MA Disclosures
Diagnostic & Predictive Immunohistochemistry in Lung Carcinomas Lynette M. Sholl, M.D. Associate Pathologist, Brigham and Women s Hospital Associate Professor, Harvard Medical School Boston, MA Disclosures
The role of the Pathologist in the diagnosis and biomarker profiling of Lung Cancer
 The role of the Pathologist in the diagnosis and biomarker profiling of Lung Cancer Prof Keith M Kerr Department of Pathology Aberdeen University Medical School & Aberdeen Royal Infirmary, UK The management
The role of the Pathologist in the diagnosis and biomarker profiling of Lung Cancer Prof Keith M Kerr Department of Pathology Aberdeen University Medical School & Aberdeen Royal Infirmary, UK The management
The 8th Edition Lung Cancer Stage Classification
 The 8th Edition Lung Cancer Stage Classification Elwyn Cabebe, M.D. Medical Oncology, Hematology, and Hospice and Palliative Care Valley Medical Oncology Consultants Director of Quality, Medical Oncology
The 8th Edition Lung Cancer Stage Classification Elwyn Cabebe, M.D. Medical Oncology, Hematology, and Hospice and Palliative Care Valley Medical Oncology Consultants Director of Quality, Medical Oncology
Lung/Thoracic Neoplasms. Manish Powari
 Lung/Thoracic Neoplasms Manish Powari Biopsy Techniques in Lung cancer diagnosis Decreased cellularity and architecture; thereby influencing subtyping Thoracotomy, resection VATS biopsy/resection L.node
Lung/Thoracic Neoplasms Manish Powari Biopsy Techniques in Lung cancer diagnosis Decreased cellularity and architecture; thereby influencing subtyping Thoracotomy, resection VATS biopsy/resection L.node
Classification of non-small cell lung carcinomas (NSCLC)
") Classification of non-small cell lung carcinomas (NSCLC) 1. NordiQC Conference on Standardization in Applied Immunohistochemistry 4-7 June 2013 Birgit Guldhammer Skov, MD. DMeSci, Dept. Of Pathology, Rigshospitalet,
Classification of non-small cell lung carcinomas (NSCLC) 1. NordiQC Conference on Standardization in Applied Immunohistochemistry 4-7 June 2013 Birgit Guldhammer Skov, MD. DMeSci, Dept. Of Pathology, Rigshospitalet,
Early-stage locally advanced non-small cell lung cancer (NSCLC) Clinical Case Discussion
 Clinical Case Discussion") Early-stage locally advanced non-small cell lung cancer (NSCLC) Clinical Case Discussion Pieter Postmus The Clatterbridge Cancer Centre Liverpool Heart and Chest Hospital Liverpool, United Kingdom 1 2
Early-stage locally advanced non-small cell lung cancer (NSCLC) Clinical Case Discussion Pieter Postmus The Clatterbridge Cancer Centre Liverpool Heart and Chest Hospital Liverpool, United Kingdom 1 2
What is New in the 2015 WHO Lung Cancer Classification? Zhaolin Xu, MD, FRCPC, FCAP
 What is New in the 2015 WHO Lung Cancer Classification? Zhaolin Xu, MD, FRCPC, FCAP Professor, Dept of Pathology, Dalhousie University, Canada Pulmonary Pathologist and Cytopathologist, QEII HSC Senior
What is New in the 2015 WHO Lung Cancer Classification? Zhaolin Xu, MD, FRCPC, FCAP Professor, Dept of Pathology, Dalhousie University, Canada Pulmonary Pathologist and Cytopathologist, QEII HSC Senior
Lung cancer is now a major cause of death in developed
 Original Article New IASLC/ATS/ERS Classification and Invasive Tumor Size are Predictive of Disease Recurrence in Stage I Lung Adenocarcinoma Naoki Yanagawa, MD, PhD,* Satoshi Shiono, MD, PhD, Masami Abiko,
Original Article New IASLC/ATS/ERS Classification and Invasive Tumor Size are Predictive of Disease Recurrence in Stage I Lung Adenocarcinoma Naoki Yanagawa, MD, PhD,* Satoshi Shiono, MD, PhD, Masami Abiko,
Molecular Testing in Lung Cancer
 Molecular Testing in Lung Cancer Pimpin Incharoen, M.D. Assistant Professor, Thoracic Pathology Department of Pathology, Ramathibodi Hospital Genetic alterations in lung cancer Source: Khono et al, Trans
Molecular Testing in Lung Cancer Pimpin Incharoen, M.D. Assistant Professor, Thoracic Pathology Department of Pathology, Ramathibodi Hospital Genetic alterations in lung cancer Source: Khono et al, Trans
Predictive markers for treatment with Immune checkpoint inhibitors - PD-L1 et al -
 Predictive markers for treatment with Immune checkpoint inhibitors - PD-L1 et al - Lukas Bubendorf Pathology Improved overall survival as a result of combination therapy Predictive biomarkers for the treatment
Predictive markers for treatment with Immune checkpoint inhibitors - PD-L1 et al - Lukas Bubendorf Pathology Improved overall survival as a result of combination therapy Predictive biomarkers for the treatment
Immunotherapy in NSCLC Pathologist role
 Immunotherapy in NSCLC Pathologist role Pimpin Incharoen, M.D. Assistant Professor, Thoracic Pathology Department of Pathology, Ramathibodi Hospital Genetic alterations in NSCLC Khono et al, Trans Lung
Immunotherapy in NSCLC Pathologist role Pimpin Incharoen, M.D. Assistant Professor, Thoracic Pathology Department of Pathology, Ramathibodi Hospital Genetic alterations in NSCLC Khono et al, Trans Lung
Protocol for the Examination of Specimens From Patients With Primary Non-Small Cell Carcinoma, Small Cell Carcinoma, or Carcinoid Tumor of the Lung
 Protocol for the Examination of Specimens From Patients With Primary Non-Small Cell Carcinoma, Small Cell Carcinoma, or Carcinoid Tumor of the Lung Version: Protocol Posting Date: June 2017 Includes ptnm
Protocol for the Examination of Specimens From Patients With Primary Non-Small Cell Carcinoma, Small Cell Carcinoma, or Carcinoid Tumor of the Lung Version: Protocol Posting Date: June 2017 Includes ptnm
Historical Note 5/2/2017. Advances in Lung Cancer Cytohistology. Purpose of FNA in Patients with Lung Cancer
 Advances in Lung Cancer Cytohistology Martha Bishop Pitman, M.D. Director, Cytopathology Massachusetts General Hospital Professor of Pathology Harvard Medical School Boston, MA Purpose of FNA in Patients
Advances in Lung Cancer Cytohistology Martha Bishop Pitman, M.D. Director, Cytopathology Massachusetts General Hospital Professor of Pathology Harvard Medical School Boston, MA Purpose of FNA in Patients
Vernieuwing en diagnostiek bij NSCLC: Immunotherapy: PD-L1 analyse: waar staan we
 9e avondsymposium: "Nieuwe ontwikkelingen in de behandeling van NSCLC" 9 november 2016, UMCG Vernieuwing en diagnostiek bij NSCLC: Immunotherapy: PD-L1 analyse: waar staan we Wim Timens Professor and Chair
9e avondsymposium: "Nieuwe ontwikkelingen in de behandeling van NSCLC" 9 november 2016, UMCG Vernieuwing en diagnostiek bij NSCLC: Immunotherapy: PD-L1 analyse: waar staan we Wim Timens Professor and Chair
Steering Committee. Waiting on photo. Paul A. Bunn, Jr., MD Kavita Garg, MD Kim Geisinger, MD Fred R. Hirsch, Gregory Riely, MD, PhD.
 Steering Committee Paul A. Bunn, Jr., MD Kavita Garg, MD Kim Geisinger, MD Fred R. Hirsch, Gregory Riely, MD, PhD MD, PhD Waiting on photo Paul Van Schil, MD, PhD William D. Travis, MD Ming-Sound Tsao,
Steering Committee Paul A. Bunn, Jr., MD Kavita Garg, MD Kim Geisinger, MD Fred R. Hirsch, Gregory Riely, MD, PhD MD, PhD Waiting on photo Paul Van Schil, MD, PhD William D. Travis, MD Ming-Sound Tsao,
EBUS-TBNA Diagnosis and Staging of Lung Cancer
 EBUS-TBNA Diagnosis and Staging of Lung Cancer Nirag Jhala MD, MIAC Professor of Pathology and Lab Med. Director of Anatomic Pathology and Cytopathology Lewis Katz School of Medicine@ Temple University
EBUS-TBNA Diagnosis and Staging of Lung Cancer Nirag Jhala MD, MIAC Professor of Pathology and Lab Med. Director of Anatomic Pathology and Cytopathology Lewis Katz School of Medicine@ Temple University
Molly Boyd, MD Glenn Mills, MD Syed Jafri, MD 1/1/2010
 LSU HEALTH SCIENCES CENTER NSCLC Guidelines Feist-Weiller Cancer Center Molly Boyd, MD Glenn Mills, MD Syed Jafri, MD 1/1/2010 Initial Evaluation/Intervention: 1. Pathology Review 2. History and Physical
LSU HEALTH SCIENCES CENTER NSCLC Guidelines Feist-Weiller Cancer Center Molly Boyd, MD Glenn Mills, MD Syed Jafri, MD 1/1/2010 Initial Evaluation/Intervention: 1. Pathology Review 2. History and Physical
Thoracic CT pattern in lung cancer: correlation of CT and pathologic diagnosis
 19 th Congress of APSR PG of Lung Cancer (ESAP): Update of Lung Cancer Thoracic CT pattern in lung cancer: correlation of CT and pathologic diagnosis Kazuma Kishi, M.D. Department of Respiratory Medicine,
19 th Congress of APSR PG of Lung Cancer (ESAP): Update of Lung Cancer Thoracic CT pattern in lung cancer: correlation of CT and pathologic diagnosis Kazuma Kishi, M.D. Department of Respiratory Medicine,
Lecture Goals. Lung (Bronchogenic) Cancer. Causes of Lung Cancer. Elizabeth Weihe, MD Assistant Professor of Radiology Director of UCSD RECIST clinic
 Cancer. Causes of Lung Cancer. Elizabeth Weihe, MD Assistant Professor of Radiology Director of UCSD RECIST clinic") Lecture Goals Origin of Lung Cancer Subtypes New Treatment Paradigms in Lung Cancer Overview of Lung Cancer Elizabeth Weihe, MD Assistant Professor of Radiology Director of UCSD RECIST clinic Lung (Bronchogenic)
Lecture Goals Origin of Lung Cancer Subtypes New Treatment Paradigms in Lung Cancer Overview of Lung Cancer Elizabeth Weihe, MD Assistant Professor of Radiology Director of UCSD RECIST clinic Lung (Bronchogenic)
Insulinoma-associated protein (INSM1) is a sensitive and specific marker for lung neuroendocrine tumors in cytologic and surgical specimens
 is a sensitive and specific marker for lung neuroendocrine tumors in cytologic and surgical specimens") Insulinoma-associated protein (INSM1) is a sensitive and specific marker for lung neuroendocrine tumors in cytologic and surgical specimens Kartik Viswanathan, M.D., Ph.D New York Presbyterian - Weill
Insulinoma-associated protein (INSM1) is a sensitive and specific marker for lung neuroendocrine tumors in cytologic and surgical specimens Kartik Viswanathan, M.D., Ph.D New York Presbyterian - Weill
OBJECTIVES. Solitary Solid Spiculated Nodule. What would you do next? Case Based Discussion: State of the Art Management of Lung Nodules.
 Organ Imaging : September 25 2015 OBJECTIVES Case Based Discussion: State of the Art Management of Lung Nodules Dr. Elsie T. Nguyen Dr. Kazuhiro Yasufuku 1. To review guidelines for follow up and management
Organ Imaging : September 25 2015 OBJECTIVES Case Based Discussion: State of the Art Management of Lung Nodules Dr. Elsie T. Nguyen Dr. Kazuhiro Yasufuku 1. To review guidelines for follow up and management
Plotting the course: optimizing treatment strategies in patients with advanced adenocarcinoma
 Pieter E. Postmus University of Liverpool Liverpool, UK Plotting the course: optimizing treatment strategies in patients with advanced adenocarcinoma Disclosures Advisor Bristol-Myers Squibb AstraZeneca
Pieter E. Postmus University of Liverpool Liverpool, UK Plotting the course: optimizing treatment strategies in patients with advanced adenocarcinoma Disclosures Advisor Bristol-Myers Squibb AstraZeneca
Reflex Testing Guidelines for Immunotherapy in Non-Small Cell Lung Cancer
 Reflex Testing Guidelines for Immunotherapy in Non-Small Cell Lung Cancer Jimmy Ruiz, MD Assistant Professor Thoracic Oncology Program Wake Forest Comprehensive Cancer Center Disclosures I have no actual
Reflex Testing Guidelines for Immunotherapy in Non-Small Cell Lung Cancer Jimmy Ruiz, MD Assistant Professor Thoracic Oncology Program Wake Forest Comprehensive Cancer Center Disclosures I have no actual
Presentation material is for education purposes only. All rights reserved URMC Radiology Page 1 of 98
 Presentation material is for education purposes only. All rights reserved. 2011 URMC Radiology Page 1 of 98 Radiology / Pathology Conference February 2011 Brooke Koltz, Cytopathology Resident Presentation
Presentation material is for education purposes only. All rights reserved. 2011 URMC Radiology Page 1 of 98 Radiology / Pathology Conference February 2011 Brooke Koltz, Cytopathology Resident Presentation
Diagnosis of lung cancer. Diagnosis Subtyping. Morphologic features Approach to small samples
 Lung Cytology Lung Cytology Pınar Fırat,MD,MIAC Diagnosis of lung cancer Detection of infections Evaluation of interstitial diseases Morphologic features Approach to small samples Lung Cancer Second most
Lung Cytology Lung Cytology Pınar Fırat,MD,MIAC Diagnosis of lung cancer Detection of infections Evaluation of interstitial diseases Morphologic features Approach to small samples Lung Cancer Second most
UPDATES IN THE SURGICAL PATHOLOGY OF LUNG CANCER. Four Ps of Pulmonary Cytopathology: Procedural, Predictive, Personalized and Participatory
 UPDATES IN THE SURGICAL PATHOLOGY OF LUNG CANCER travisw@mskcc.org Four Ps of Pulmonary Cytopathology: Procedural, Predictive, Personalized and Participatory American Society of Cytopathology Companion
UPDATES IN THE SURGICAL PATHOLOGY OF LUNG CANCER travisw@mskcc.org Four Ps of Pulmonary Cytopathology: Procedural, Predictive, Personalized and Participatory American Society of Cytopathology Companion
Lung Cancer Genetics: Common Mutations and How to Treat Them David J. Kwiatkowski, MD, PhD. Mount Carrigain 2/4/17
 Lung Cancer Genetics: Common Mutations and How to Treat Them David J. Kwiatkowski, MD, PhD Mount Carrigain 2/4/17 Histology Adenocarcinoma: Mixed subtype, acinar, papillary, solid, micropapillary, lepidic
Lung Cancer Genetics: Common Mutations and How to Treat Them David J. Kwiatkowski, MD, PhD Mount Carrigain 2/4/17 Histology Adenocarcinoma: Mixed subtype, acinar, papillary, solid, micropapillary, lepidic
In the mid 1970s, visceral pleural invasion (VPI) was included
 was included") ORIGINAL ARTICLE Tumor Invasion of Extralobar Soft Tissue Beyond the Hilar Region Does Not Affect the Prognosis of Surgically Resected Lung Cancer Patients Hajime Otsuka, MD,* Genichiro Ishii, MD, PhD,*
ORIGINAL ARTICLE Tumor Invasion of Extralobar Soft Tissue Beyond the Hilar Region Does Not Affect the Prognosis of Surgically Resected Lung Cancer Patients Hajime Otsuka, MD,* Genichiro Ishii, MD, PhD,*
Biomarcatori per la immunoterapia: cosa e come cercare Paolo Graziano
 Biomarcatori per la immunoterapia: cosa e come cercare Paolo Graziano Unit of Pathology Fondazione IRCCS Casa Sollievo della Sofferenza San Giovanni Rotondo, Foggia,Italy p.graziano@operapadrepio.it Disclosure
Biomarcatori per la immunoterapia: cosa e come cercare Paolo Graziano Unit of Pathology Fondazione IRCCS Casa Sollievo della Sofferenza San Giovanni Rotondo, Foggia,Italy p.graziano@operapadrepio.it Disclosure
Neuroendocrine neoplasms of the lung
 Neuroendocrine neoplasms of the lung M Papotti, L Righi, & M Volante University of Turin at San Luigi Hospital TORINO NETs OF THE LUNG Menu - Spectrum of NE lung tumors - CARCINOID TUMORS - SCLC /LCNEC
Neuroendocrine neoplasms of the lung M Papotti, L Righi, & M Volante University of Turin at San Luigi Hospital TORINO NETs OF THE LUNG Menu - Spectrum of NE lung tumors - CARCINOID TUMORS - SCLC /LCNEC
Validation of the T descriptor in the new 8th TNM classification for non-small cell lung cancer
 Original Article Validation of the T descriptor in the new 8th TNM classification for non-small cell lung cancer Hee Suk Jung 1, Jin Gu Lee 2, Chang Young Lee 2, Dae Joon Kim 2, Kyung Young Chung 2 1 Department
Original Article Validation of the T descriptor in the new 8th TNM classification for non-small cell lung cancer Hee Suk Jung 1, Jin Gu Lee 2, Chang Young Lee 2, Dae Joon Kim 2, Kyung Young Chung 2 1 Department
Patient Selection: The Search for Immunotherapy Biomarkers
 Patient Selection: The Search for Immunotherapy Biomarkers Mark A. Socinski, MD Executive Medical Director Florida Hospital Cancer Institute Orlando, Florida Patient Selection Clinical smoking status Histologic
Patient Selection: The Search for Immunotherapy Biomarkers Mark A. Socinski, MD Executive Medical Director Florida Hospital Cancer Institute Orlando, Florida Patient Selection Clinical smoking status Histologic
Standards and datasets for reporting cancers. Dataset for histopathological reporting of lung cancer. September 2018
 Standards and datasets for reporting cancers Dataset for histopathological reporting of lung cancer September 2018 Authors: Professor Andrew G Nicholson, Royal Brompton and Harefield NHS Foundation Trust,
Standards and datasets for reporting cancers Dataset for histopathological reporting of lung cancer September 2018 Authors: Professor Andrew G Nicholson, Royal Brompton and Harefield NHS Foundation Trust,
North of Scotland Cancer Network Clinical Management Guideline for Non Small Cell Lung Cancer
 THIS DOCUMENT IS North of Scotland Cancer Network Clinical Management Guideline for Non Small Cell Lung Cancer [Based on WOSCAN NSCLC CMG with further extensive consultation within NOSCAN] UNCONTROLLED
THIS DOCUMENT IS North of Scotland Cancer Network Clinical Management Guideline for Non Small Cell Lung Cancer [Based on WOSCAN NSCLC CMG with further extensive consultation within NOSCAN] UNCONTROLLED
YOUR LUNG CANCER PATHOLOGY REPORT
 UNDERSTANDING SERIES YOUR LUNG CANCER PATHOLOGY REPORT 1-800-298-2436 LungCancerAlliance.org A GUIDE FOR THE PATIENT 1 CONTENTS What is a Pathology Report?...2 The Basics...3 Sections of a Pathology Report...6
UNDERSTANDING SERIES YOUR LUNG CANCER PATHOLOGY REPORT 1-800-298-2436 LungCancerAlliance.org A GUIDE FOR THE PATIENT 1 CONTENTS What is a Pathology Report?...2 The Basics...3 Sections of a Pathology Report...6
Lung /4/18. Please submit all questions concerning the webinar content through the Q&A panel.
 Lung NAACCR 2018 2019 WEBINAR SERIES 1 Q&A Please submit all questions concerning the webinar content through the Q&A panel. If you have participants watching this webinar at your site, please collect
Lung NAACCR 2018 2019 WEBINAR SERIES 1 Q&A Please submit all questions concerning the webinar content through the Q&A panel. If you have participants watching this webinar at your site, please collect
Problem 1: Differential of Neuroendocrine Carcinoma 3/23/2017. Disclosure of Relevant Financial Relationships
 Differential of Neuroendocrine Carcinoma Alain C. Borczuk,MD Weill Cornell Medicine Disclosure of Relevant Financial Relationships USCAP requires that all faculty in a position to influence or control
Differential of Neuroendocrine Carcinoma Alain C. Borczuk,MD Weill Cornell Medicine Disclosure of Relevant Financial Relationships USCAP requires that all faculty in a position to influence or control
Respiratory Tract Cytology
 Respiratory Tract Cytology 40 th European Congress of Cytology Liverpool, UK Momin T. Siddiqui M.D. Professor of Pathology and Laboratory Medicine Director of Cytopathology Emory University Hospital, Atlanta,
Respiratory Tract Cytology 40 th European Congress of Cytology Liverpool, UK Momin T. Siddiqui M.D. Professor of Pathology and Laboratory Medicine Director of Cytopathology Emory University Hospital, Atlanta,
I appreciate the courtesy of Kusumoto at NCC for this presentation. What is Early Lung Cancers. Early Lung Cancers. Early Lung Cancers 18/10/55
 I appreciate the courtesy of Kusumoto at NCC for this presentation. Dr. What is Early Lung Cancers DEATH Early period in its lifetime Curative period in its lifetime Early Lung Cancers Early Lung Cancers
I appreciate the courtesy of Kusumoto at NCC for this presentation. Dr. What is Early Lung Cancers DEATH Early period in its lifetime Curative period in its lifetime Early Lung Cancers Early Lung Cancers
Pulmonary adenocarcinoma Issues, Issues and more issues. Why the headache?
 Issues Pulmonary adenocarcinoma Issues, Issues and more issues. Why the headache? Classification Multiple nodules Invasive size Alain Borczuk, MD Weill Cornell Medicine Chronic headache - Classification
Issues Pulmonary adenocarcinoma Issues, Issues and more issues. Why the headache? Classification Multiple nodules Invasive size Alain Borczuk, MD Weill Cornell Medicine Chronic headache - Classification
The 7th Edition of TNM in Lung Cancer.
 10th European Conference Perspectives in Lung Cancer. Brussels, March 2009. The 7th Edition of TNM in Lung Cancer. Peter Goldstraw, Consultant Thoracic Surgeon, Royal Brompton Hospital, Professor of Thoracic
10th European Conference Perspectives in Lung Cancer. Brussels, March 2009. The 7th Edition of TNM in Lung Cancer. Peter Goldstraw, Consultant Thoracic Surgeon, Royal Brompton Hospital, Professor of Thoracic
8th Edition of the TNM Classification for Lung Cancer. Proposed by the IASLC
 8th Edition of the TNM Classification for Lung Cancer Proposed by the IASLC Introduction Stage classification - provides consistency in nomenclature - improves understanding of anatomic extent of tumour
8th Edition of the TNM Classification for Lung Cancer Proposed by the IASLC Introduction Stage classification - provides consistency in nomenclature - improves understanding of anatomic extent of tumour
Quality ID #395: Lung Cancer Reporting (Biopsy/Cytology Specimens) National Quality Strategy Domain: Communication and Care Coordination
 National Quality Strategy Domain: Communication and Care Coordination") Quality ID #395: Lung Cancer Reporting (Biopsy/Cytology Specimens) National Quality Strategy Domain: Communication and Care Coordination 2018 OPTIONS FOR INDIVIDUAL MEASURES: REGISTRY ONLY MEASURE TYPE:
Quality ID #395: Lung Cancer Reporting (Biopsy/Cytology Specimens) National Quality Strategy Domain: Communication and Care Coordination 2018 OPTIONS FOR INDIVIDUAL MEASURES: REGISTRY ONLY MEASURE TYPE:
Disclosures Genomic testing in lung cancer
 Disclosures Genomic testing in lung cancer No disclosures Objectives Understand how FISH and NGS provide complementary data for the evaluation of lung cancer Recognize the challenges of performing testing
Disclosures Genomic testing in lung cancer No disclosures Objectives Understand how FISH and NGS provide complementary data for the evaluation of lung cancer Recognize the challenges of performing testing
Agilent companion diagnostics for cancer immunotherapy
 Agilent companion diagnostics for cancer immunotherapy Annika Eklund, PhD Global Product Manager Companion Diagnostics Agilent Technologies Aalborg 1 Agilent Trusted Answers. Together OUR FOCUS life sciences,
Agilent companion diagnostics for cancer immunotherapy Annika Eklund, PhD Global Product Manager Companion Diagnostics Agilent Technologies Aalborg 1 Agilent Trusted Answers. Together OUR FOCUS life sciences,
ACCME/Disclosures. Diagnosing Mesothelioma in Limited Tissue Samples. Papanicolaou Society of Cytopathology Companion Meeting March 12 th, 2016
 Diagnosing Mesothelioma in Limited Tissue Samples Papanicolaou Society of Cytopathology Companion Meeting March 12 th, 2016 Sanja Dacic, MD, PhD University of Pittsburgh ACCME/Disclosures GENERAL RULES
Diagnosing Mesothelioma in Limited Tissue Samples Papanicolaou Society of Cytopathology Companion Meeting March 12 th, 2016 Sanja Dacic, MD, PhD University of Pittsburgh ACCME/Disclosures GENERAL RULES
The new international multidisciplinary lung adenocarcinoma
 Eur Respir J 2011; 38: 239 243 DOI: 10.1183/09031936.00026711 CopyrightßERS 2011 EDITORIAL Paradigm shifts in lung cancer as defined in the new IASLC/ATS/ERS lung adenocarcinoma classification W.D. Travis*,"",
Eur Respir J 2011; 38: 239 243 DOI: 10.1183/09031936.00026711 CopyrightßERS 2011 EDITORIAL Paradigm shifts in lung cancer as defined in the new IASLC/ATS/ERS lung adenocarcinoma classification W.D. Travis*,"",
The lung adenocarcinoma guidelines: what to be considered by surgeons
 Review Article The lung adenocarcinoma guidelines: what to be considered by surgeons Rodrigo A. S. Sardenberg 1, Evandro Sobroza Mello 1, Riad N. Younes 2 1 Hospital Alemão Oswaldo Cruz, São Paulo, Brazil;
Review Article The lung adenocarcinoma guidelines: what to be considered by surgeons Rodrigo A. S. Sardenberg 1, Evandro Sobroza Mello 1, Riad N. Younes 2 1 Hospital Alemão Oswaldo Cruz, São Paulo, Brazil;
Greater Manchester & Cheshire Guidelines for Pathology Reporting for Oesophageal and Gastric Malignancy
 Greater Manchester & Cheshire Guidelines for Pathology Reporting for Oesophageal and Gastric Malignancy Authors: Dr Gordon Armstrong, Dr Sue Pritchard 1. General Comments 1.1 Cancer reporting: Biopsies
Greater Manchester & Cheshire Guidelines for Pathology Reporting for Oesophageal and Gastric Malignancy Authors: Dr Gordon Armstrong, Dr Sue Pritchard 1. General Comments 1.1 Cancer reporting: Biopsies
Imaging of Lung Cancer: A Review of the 8 th TNM Staging System
 Imaging of Lung Cancer: A Review of the 8 th TNM Staging System Travis S Henry, MD Associate Professor of Clinical Radiology Cardiac and Pulmonary Imaging Section University of California, San Francisco
Imaging of Lung Cancer: A Review of the 8 th TNM Staging System Travis S Henry, MD Associate Professor of Clinical Radiology Cardiac and Pulmonary Imaging Section University of California, San Francisco
Updated Molecular Testing Guideline for the Selection of Lung Cancer Patients for Treatment with Targeted Tyrosine Kinase Inhibitors
 Q: How is the strength of recommendation determined in the new molecular testing guideline? A: The strength of recommendation is determined by the strength of the available data (evidence). Strong Recommendation:
Q: How is the strength of recommendation determined in the new molecular testing guideline? A: The strength of recommendation is determined by the strength of the available data (evidence). Strong Recommendation:
Quality ID #395: Lung Cancer Reporting (Biopsy/Cytology Specimens) National Quality Strategy Domain: Communication and Care Coordination
 National Quality Strategy Domain: Communication and Care Coordination") Quality ID #395: Lung Cancer Reporting (Biopsy/Cytology Specimens) National Quality Strategy Domain: Communication and Care Coordination 2018 OPTIONS FOR INDIVIDUAL MEASURES: CLAIMS ONLY MEASURE TYPE:
Quality ID #395: Lung Cancer Reporting (Biopsy/Cytology Specimens) National Quality Strategy Domain: Communication and Care Coordination 2018 OPTIONS FOR INDIVIDUAL MEASURES: CLAIMS ONLY MEASURE TYPE:
Protocol for the Examination of Specimens From Patients With Thymic Tumors
 Protocol for the Examination of Specimens From Patients With Thymic Tumors Version: Protocol Posting Date: June 2017 Includes ptnm requirements from the 8 th Edition, AJCC Staging Manual For accreditation
Protocol for the Examination of Specimens From Patients With Thymic Tumors Version: Protocol Posting Date: June 2017 Includes ptnm requirements from the 8 th Edition, AJCC Staging Manual For accreditation
Follicular Derived Thyroid Tumors
 Follicular Derived Thyroid Tumors Jennifer L. Hunt, MD, MEd Aubrey J. Hough Jr, MD, Endowed Professor of Pathology Chair of Pathology and Laboratory Medicine University of Arkansas for Medical Sciences
Follicular Derived Thyroid Tumors Jennifer L. Hunt, MD, MEd Aubrey J. Hough Jr, MD, Endowed Professor of Pathology Chair of Pathology and Laboratory Medicine University of Arkansas for Medical Sciences
Pulmonary Nodules & Masses
 Pulmonary Nodules & Masses A Diagnostic Approach Heber MacMahon The University of Chicago Department of Radiology Disclosure Information Consultant for Riverain Technology Minor equity in Hologic Royalties
Pulmonary Nodules & Masses A Diagnostic Approach Heber MacMahon The University of Chicago Department of Radiology Disclosure Information Consultant for Riverain Technology Minor equity in Hologic Royalties
Lung Tumor Cases: Common Problems and Helpful Hints
 Lung Tumor Cases: Common Problems and Helpful Hints Brandon T. Larsen, MD, PhD Senior Associate Consultant Department of Laboratory Medicine and Pathology Mayo Clinic Arizona Arizona Society of Pathologists
Lung Tumor Cases: Common Problems and Helpful Hints Brandon T. Larsen, MD, PhD Senior Associate Consultant Department of Laboratory Medicine and Pathology Mayo Clinic Arizona Arizona Society of Pathologists
Personalized Medicine: Lung Biopsy and Tumor
 Personalized Medicine: Lung Biopsy and Tumor Mutation Testing Elizabeth H. Moore, MD Personalized Medicine: Lung Biopsy and Tumor Mutation Testing Genomic testing has resulted in a paradigm shift in the
Personalized Medicine: Lung Biopsy and Tumor Mutation Testing Elizabeth H. Moore, MD Personalized Medicine: Lung Biopsy and Tumor Mutation Testing Genomic testing has resulted in a paradigm shift in the
Cool Stains for Hot Diagnoses in Thoracic Pathology
 Cool Stains for Hot Diagnoses in Thoracic Pathology Anja C. Roden, M.D. Department of Laboratory Medicine and Pathology, Mayo Clinic, Rochester, MN, USA No disclosures Disclosure Learning Objectives Know
Cool Stains for Hot Diagnoses in Thoracic Pathology Anja C. Roden, M.D. Department of Laboratory Medicine and Pathology, Mayo Clinic, Rochester, MN, USA No disclosures Disclosure Learning Objectives Know
04/09/2018. Follicular Thyroid Tumors Updates in Classification & Practical Tips. Dissecting Indeterminants. In pursuit of the low grade malignancy
 Follicular Thyroid Tumors Updates in Classification & Practical Tips Jennifer L. Hunt, MD, MEd Aubrey J. Hough Jr, MD, Endowed Professor of Pathology Chair of Pathology and Laboratory Medicine University
Follicular Thyroid Tumors Updates in Classification & Practical Tips Jennifer L. Hunt, MD, MEd Aubrey J. Hough Jr, MD, Endowed Professor of Pathology Chair of Pathology and Laboratory Medicine University
The 8 th Edition of TNM for Lung Cancer: The IASLC Proposals.
 13 th Cambridge Chest Meeting 2015. The 8 th Edition of TNM for Lung Cancer: The IASLC Proposals. Peter Goldstraw, Honorary Consultant Thoracic Surgeon, Royal Brompton Hospital, Emeritus Professor of Thoracic
13 th Cambridge Chest Meeting 2015. The 8 th Edition of TNM for Lung Cancer: The IASLC Proposals. Peter Goldstraw, Honorary Consultant Thoracic Surgeon, Royal Brompton Hospital, Emeritus Professor of Thoracic
57th Annual HSCP Spring Symposium 4/16/2016
 An Unusual Malignant Spindle Cell Lesion to Involve the Breast Erinn Downs-Kelly, D.O. Associate Professor of Pathology University of Utah & ARUP Laboratories No disclosures Case 39 y/o female with no
An Unusual Malignant Spindle Cell Lesion to Involve the Breast Erinn Downs-Kelly, D.O. Associate Professor of Pathology University of Utah & ARUP Laboratories No disclosures Case 39 y/o female with no
Multifocal Lung Cancer
 Multifocal Lung Cancer P. De Leyn, MD, PhD Department of Thoracic Surgery University Hospitals Leuven Belgium LEUVEN LUNG CANCER GROUP Department of Thoracic Surgery Department of Pneumology Department
Multifocal Lung Cancer P. De Leyn, MD, PhD Department of Thoracic Surgery University Hospitals Leuven Belgium LEUVEN LUNG CANCER GROUP Department of Thoracic Surgery Department of Pneumology Department
THYMIC CARCINOMAS AN UPDATE
 THYMIC CARCINOMAS AN UPDATE Mark R. Wick, M.D. University of Virginia Medical Center Charlottesville, VA CARCINOMA OF THE THYMUS General Clinical Features No apparent gender predilection Age range of 35-75
THYMIC CARCINOMAS AN UPDATE Mark R. Wick, M.D. University of Virginia Medical Center Charlottesville, VA CARCINOMA OF THE THYMUS General Clinical Features No apparent gender predilection Age range of 35-75
Case year old female presented with asymmetric enlargement of the left lobe of the thyroid
 Case 4 22 year old female presented with asymmetric enlargement of the left lobe of the thyroid gland. No information available relative to a prior fine needle aspiration biopsy. A left lobectomy was performed.
Case 4 22 year old female presented with asymmetric enlargement of the left lobe of the thyroid gland. No information available relative to a prior fine needle aspiration biopsy. A left lobectomy was performed.
Case 4 Diagnosis 2/21/2011 TGB
 Case 4 22 year old female presented with asymmetric enlargement of the left lobe of the thyroid gland. No information available relative to a prior fine needle aspiration biopsy. A left lobectomy was performed.
Case 4 22 year old female presented with asymmetric enlargement of the left lobe of the thyroid gland. No information available relative to a prior fine needle aspiration biopsy. A left lobectomy was performed.
WHITE PAPER - SRS for Non Small Cell Lung Cancer
 WHITE PAPER - SRS for Non Small Cell Lung Cancer I. Introduction This white paper will focus on non-small cell lung carcinoma with sections one though six comprising a general review of lung cancer from
WHITE PAPER - SRS for Non Small Cell Lung Cancer I. Introduction This white paper will focus on non-small cell lung carcinoma with sections one though six comprising a general review of lung cancer from
Small cell lung cancer and large cell neuroendocrine tumours interobserver variability. Michael den Bakker Erasmus MC
 Small cell lung cancer and large cell neuroendocrine tumours interobserver variability Michael den Bakker Erasmus MC PPC London 2007 WEB presentation Pulmonary pathology Club presentation, London, November
Small cell lung cancer and large cell neuroendocrine tumours interobserver variability Michael den Bakker Erasmus MC PPC London 2007 WEB presentation Pulmonary pathology Club presentation, London, November
AGGRESSIVE VARIANTS OF PAPILLARY THYROID CARCINOMA DIAGNOSIS AND PROGNOSIS
 AGGRESSIVE VARIANTS OF PAPILLARY THYROID CARCINOMA DIAGNOSIS AND PROGNOSIS PAPILLARY THYROID CARCINOMA Clinical Any age Microscopic to large Female: Male= 2-4:1 Radiation history Lymph nodes Prognosis
AGGRESSIVE VARIANTS OF PAPILLARY THYROID CARCINOMA DIAGNOSIS AND PROGNOSIS PAPILLARY THYROID CARCINOMA Clinical Any age Microscopic to large Female: Male= 2-4:1 Radiation history Lymph nodes Prognosis
International Society of Gynecological Pathologists Symposium 2007
 International Society of Gynecological Pathologists Symposium 2007 Anais Malpica, M.D. Department of Pathology The University of Texas M.D. Anderson Cancer Center Grading of Ovarian Cancer Histologic grade
International Society of Gynecological Pathologists Symposium 2007 Anais Malpica, M.D. Department of Pathology The University of Texas M.D. Anderson Cancer Center Grading of Ovarian Cancer Histologic grade
MOLECULAR PREDICTIVE MARKERS OF LUNG CARCINOMA: KFSH&RC EXPERIENCE
 25 th IAP-Arab Division Conference 07-09 November 2013, Amman, Jordan MOLECULAR PREDICTIVE MARKERS OF LUNG CARCINOMA: KFSH&RC EXPERIENCE Fouad Al Dayel, MD, FRCPA, FRCPath Professor and Chairman Department
25 th IAP-Arab Division Conference 07-09 November 2013, Amman, Jordan MOLECULAR PREDICTIVE MARKERS OF LUNG CARCINOMA: KFSH&RC EXPERIENCE Fouad Al Dayel, MD, FRCPA, FRCPath Professor and Chairman Department
An Update: Lung Cancer
 An Update: Lung Cancer Andy Barlow Consultant in Respiratory Medicine Lead Clinician for Lung Cancer (West Herts Hospitals NHS Trust) Lead for EBUS-Harefield Hospital (RB&HFT) Summary Lung cancer epidemiology
An Update: Lung Cancer Andy Barlow Consultant in Respiratory Medicine Lead Clinician for Lung Cancer (West Herts Hospitals NHS Trust) Lead for EBUS-Harefield Hospital (RB&HFT) Summary Lung cancer epidemiology