Interpretation guide. Abnormal cytology can t hide anymore
|
|
|
- Esmond Sullivan
- 5 years ago
- Views:
Transcription
















1 Interpretation guide Abnormal cytology can t hide anymore Unique dual-biomarker technology makes you certain about the presence of transforming HPV infection. The science that creates certainty.
2
3 Table of Contents Introduction... 1 Biomarkers p16 and Ki-67 and their role in identifying oncogenic transformation... 2 The role of p16 in identifying oncogenic transformation... 2 The role of Ki-67 in identifying oncogenic transformation... 4 Purpose of Interpretation Guide Clinical Evaluation of the CINtec PLUS Cytology Test... 7 Criteria for a dual-stained cervical epithelial cell... 8 Criteria for a negative CINtec PLUS Cytology staining result... 8 Slide Screening Procedure CINtec PLUS Cytology cell cluster interpretation flowchart Cellular Adequacy Assessment Positive and Negative Controls Positive Controls Negative Controls Non-specific background staining Non-specific, brown background staining Non-specific red background staining Criteria for differentiating specific and non-specific Ki-67 nuclear staining Examples of brown and red non-specific background staining Non-specific background staining assessment Definition of background acceptability Red Chromogen Bleeding Non-specific staining of extracellular elements Differences between non-specific background staining and non-specific staining of extracellular elements Preparation related artifacts Challenging Cases Knowledge Check Knowledge Check Answer Key References i
4
5 Introduction Human papillomavirus (HPV) infections are very common, and most are transient in nature with less than 10% of HPV infections actually progressing to high-grade lesions or cancer. 1, 2, 3 As a result, many women undergo additional procedures (e.g. repeat Pap smears, colposcopy and cervical biopsies) unnecessarily as no significant precursor lesion is found. 4 It has been well demonstrated that HPV testing improves the sensitivity for detection of high-grade precursor lesions when compared to cytology. 5, 6, 7, 8, 9 With a greater understanding of cell cycle alterations induced by HPV oncoproteins in cervical neoplasia, biomarkers can be used as a tool to identify women who are at an increased risk for harboring cervical cancer precursors. Biomarkers offer improved specificity over HR-HPV testing as their altered expression represents evidence of true cellular neoplastic transformation. 4 Detection of overexpression of p16ink4a protein (p16), a biomarker of transforming HPV infections and precancerous cervical lesions, has been shown to be an efficient tool in managing patients with atypical squamous cells of undetermined significance (ASC-US) or low-grade squamous intraepithelial lesion (LSIL) cytology results, and for triaging HPV-positive women. 10, 11, 12, 13 Most recently, several studies have analyzed the diagnostic performance of a novel p16/ki-67 dual-stained cytology approach that combines simultaneous p16 and Ki-67 detection in the same cell as a hallmark of cell cycle deregulation. 14, 15, 16, 17 In normal cells, the expression of p16 and Ki-67 are mutually exclusive. p16/ki-67 dual-stained cytology, a morphology independent test, showed similar sensitivity and significantly higher specificity than HPV testing in ASC-US and LSIL triage, and in women with negative Pap cytology but positive HPV 14, 15 screening results. A variety of novel approaches to screening for cervical disease exist, however, few are widely used in standard clinical practice. Each approach provides information that must be considered to ensure effective implementation. It is important to understand the wide range of technologies that are available as the screening paradigm continues to shift away from Pap testing alone, and as HPV vaccination is introduced. The expanding implementation of HPV vaccination programs will demand the transition to more objective testing methods such as primary HPV testing and p16 / Ki-67 dual-staining. As cervical disease becomes less prevalent in vaccinated populations, the use of objective molecular and biomarker-based tests are critical to more accurately identify patients at risk of developing cervical cancer. Roche has developed the CINtec PLUS Cytology test to identify cells that have undergone HR-HPV-mediated oncogenic transformation and to identify women harboring high-grade cervical disease. When used as a triage for primary HPV cervical screening for the FDA approved cobas HPV test, the CINtec PLUS Cytology test identifies cervical cells where the HR-HPV infection has disrupted cellular control, confirming the presence of a transforming HPV infection. The CINtec PLUS Cytology test helps to accurately predict which women are most likely to have precancerous cervical lesions and, therefore, would benefit from immediate colposcopy. The CINtec PLUS Cytology test simultaneously detects the presence of p16 and Ki-67 in the same cervical cell which Serves as an indicator of cell cycle deregulation Correlates with the presence of HPV-induced oncogenic transformation Provides an objective result to identify women who are likely to harbor high-grade cervical disease
6 The co-localization of p16/ki-67 expression in cervical cells identifies women that may benefit most from immediate colposcopy. 19 Biomarkers p16 and Ki-67 and their role in identifying oncogenic transformation In the development of cervical cancer, the majority of cellular changes take place in the transformation zone of the cervix. During normal maturation of the cervical squamous epithelium, cellular proliferation is limited to basal cell layers. The role of p16 in identifying oncogenic transformation In normal cells, the tumor suppressor protein, retinoblastoma (prb), binds to the transcription factor, E2F, blocking transcription of genes that promote cell cycle progression and proliferation. This leads to cell cycle arrest. When E2F is released from prb, this results in cell cycle progression/proliferation. After mitosis, the p16 gene is activated causing low-level expression of the p16 protein. The p16 protein serves as a cell cycle regulator by facilitating a cascade of biochemical events resulting in re-binding E2F with prb. When E2F and prb reassociate, the cell returns to cell cycle arrest. This feedback control mechanism is critical to maintaining the balance between cell cycle progression/proliferation and cell cycle arrest. 20 In healthy cervical squamous cells, this feedback control mechanism contributes to maintaining the normal balance between cell cycle progression/proliferation, and cell cycle arrest.


7 Figure 1.0 prb, E2F and p16 in normal cell cycle function HPV is known to be the cause of cervical cancer. HPV is transmitted sexually and once it is introduced to the cervix, it may infect the epithelial cells of the cervical transformation zone. The vast majority of HPV infections are transient, being cleared by the immune system within 6 to 12 months. In transforming infections with HR-HPV, the viral oncoprotein E7 competes with E2F and binds to prb. The prb:e7 oncoprotein complex functionally inactivates prb, disrupting the negative feedback control of prb on p16 expression. p16 continues to be overexpressed and cells continue to proliferate. This strong upregulation of p16 protein expression is detectable by immunohistochemistry (IHC) and serves as an indicator of HPV-mediated cellular oncogenic transformation in cervical tissue. 19 Figure 1.1 prb, E2F and p16 in oncogenic transformation

8 When p16 is overexpressed it can be detected by p16 immunohistochemistry, as shown in Figure 1.2. The IHC staining in cervical tissue is characterized by continuous diffuse staining comprising the basal and parabasal cell layers of the epithelium. This is indicative of HPV-mediated cervical disease. Figure 1.2 Positive p16 staining result diffuse (brown) stain of the cervical squamous epithelium The role of Ki-67 in identifying oncogenic transformation The protein, Ki-67, is expressed during various phases of the cell cycle and is a marker for active cellular proliferation. In normal squamous cervical tissue, Ki-67 expression is confined to the actively proliferating parabasal cell layer, as shown in Figure 1.3. A positive Ki-67 immunostain is represented as a red nuclear stain. Note that the intermediate and superficial cell layers within the normal cervical squamous epithelium are not stained. Cells within these layers are terminally differentiated and are no longer actively proliferating. In normal cells, expression of p16 and Ki-67 are mutually exclusive X
 Therefore, the p16/ki-67 dual-biomarker")
9 Figure 1.3 Normal cervical squamous epithelium immunostained with Ki-67 The combination of both p16 and Ki-67 immunostaining is important when evaluating cervical cytology specimens. The morphologic context and architecture of the cervical tissue is not visualized in the liquid-based cytology preparations (compare Figure 1 with Figure 2) Therefore, the p16/ki-67 dual-biomarker strategy that provides additional objective, antigenic information in cytology specimens is critical in identifying cells that are associated with transforming HPV infections. Co-localization p16 and Ki-67 in the same cell is a clear indicator of cell cycle deregulation. Co-expression of p16/ki-67 may, therefore, indicate cellular oncogenic transformation associated with a persistent HPV infection. The CINtec PLUS Cytology test can appropriately stratify women to identify high-grade cervical disease independent of 20, 21 HPV genotype, patient age or morphologic interpretation.
10 Figure 1.4 A dual-stained squamous cell, staining with p16 (brown cytoplasm) and Ki-67 (red nucleus) positive for CINtec PLUS Cytology 20X Purpose of Interpretation Guide The CINtec PLUS Cytology interpretation guide is intended to Provide cytotechnologists and pathologists with a tool to facilitate the clinical evaluation of the CINtec PLUS Cytology test Explain recommended slide evaluation methods to screen and confirm results of the CINtec PLUS Cytology test Provide photomicrographic images that illustrate staining patterns of cells from cervical samples stained with the CINtec PLUS Cytology test Illustrate challenging cases to provide guidance for cytotechnologists and pathologists with all degrees of positive and negative staining including the presence of non-specific background staining Provide guidance in using a known CINtec PLUS Cytology positive cervical sample as a positive control for use as a system control when running the CINtec PLUS Cytology test on the BenchMark ULTRA advanced staining IHC/ISH platform
11 Clinical Evaluation of the CINtec PLUS Cytology Test CINtec PLUS Cytology is an immunocytochemistry test that includes a mouse monoclonal antibody directed against human p16 protein, and a primary recombinant rabbit monoclonal antibody directed against human Ki-67 protein. The detection chemistry in the CINtec PLUS Cytology kit is similar to VENTANA OptiView detection technology. DAB (brown) detection chemistry is used for p16 detection. p16 may stain the cytoplasm and nucleus, or only the cytoplasm of the cell. Ki-67 will only stain the nucleus and/or nucleoli. Fast red detection chemistry is used for Ki-67 detection. Hematoxylin counterstains the non-reactive cells cytoplasm and nucleus with a blue color. The cytoplasm and nuclei of the superficial squamous cells that do not stain with p16 and/or Ki-67 can be used as reference cells to compare stain intensity of other cells with specific p16 and Ki-67 staining. Figure 2.0 (Left) Dual-stained cell, positive for CINtec PLUS Cytology; (Right) Counterstained intermediate squamous cell used as a reference for contrast and comparison to other cells staining with p16 (brown) and Ki-67 (red). Counterstained- stained
12 Criteria for a dual-stained cervical epithelial cell The interpretation of the CINtec PLUS Cytology test is independent of cytomorphologic criteria The cytoplasm stains brown (p16) and the nucleus stains red (Ki-67) The p16 signal (brown) and Ki-67 signal (red) is co-localized within the same cell The red stained nucleus and the brown stained cytoplasm must be within the same microscopic plane of focus The level of staining intensity may be weak to strong Specific Ki-67 signal (red) may be uniformly stained within the nucleus of the cell or partially stained including: A speckled or granular staining pattern Red staining of nucleoli One dual-stained cervical epithelial cell indicates a positive test result Criteria for a negative CINtec PLUS Cytology staining result Cervical epithelial cells stain with only the blue counterstain Cervical epithelial cells stain with only p16, brown cytoplasmic and/or nuclear stain Cervical epithelial cells stain with only Ki-67, red nuclear stain Co-localization of p16 and Ki-67 must be present in the same cervical epithelial cell to be evaluated as a positive staining result. The counterstain shows as a blue stain, visible in cervical epithelial cells that are not staining with p16 or Ki-67, or in cells that are only staining with Ki-67. NOTE: Recommend the use of a microscope equipped with a halogen or LED light source set to the daylight or white light setting and the use of a neutral color balance (NCB) or LBD filter, to help eliminate yellow light. The use of filters, which can also include Neutral Density (ND) filters, provides a white light field of view, and will aid in distinguishing the red Ki-67 nuclear staining from the brown p16 staining in the nucleus and cytoplasm.
 Presence of at least one dual-stained cervical epithelial cell Dual-stained cervical")

 - Only with blue counterstain Figures 2.")
13 Clinical Interpretation Staining Description Positive for CINtec PLUS Cytology (See Figure 2.1) Presence of at least one dual-stained cervical epithelial cell Dual-stained cervical epithelial cell(s) may be present in sheets, overlapping clusters or isolated clusters of cells Negative for CINtec PLUS Cytology (See Figure 2.2) Cervical epithelial cells staining with: - Only p16 (nuclear and/or cytoplasmic) - Only Ki-67(nuclear) - Only with blue counterstain Figures 2.1 Examples of single dual-stain cells, positive for CINtec PLUS Cytology
")

14 Figures 2.1 continued: A single, dual-stained cell (circled) with intense, dark p16 staining, positive for CINtec PLUS Cytology Increasing the microscope light improves the differentiation of the red nuclear signal.
15 Figures 2.1 continued: A single dual-stained cell with cytoplasmic p16 staining and nuclear Ki-67 staining, positive for CINtec PLUS Cytology 20X


16 Figures 2.1, continued: Cluster of cells containing dual-stained cells, positive for CINtec PLUS Cytology 60X

17 Figures 2.2: Examples of CINtec PLUS Cytology negative cells stained with p16 or Ki-67 No dual-stained cells are present in the following images. The squamous metaplastic cell on the left is staining only with p16; the nucleus of the squamous metaplastic cell on the right is staining with Ki-67. Both cells are negative for CINtec PLUS Cytology. The cytoplasm of the metaplastic cell on the right is stained with the blue counterstain. Squamous cell with weak nuclear Ki-67 staining, negative for CINtec PLUS Cytology

18 Figures 2.2, continued: Examples of CINtec PLUS Cytology negative cells stained with p16 or Ki-67 No dual-stained cells are present in the following images. Squamous cells with nuclear Ki-67 staining, negative for CINtec PLUS Cytology Squamous cell with nuclear Ki-67 staining, negative for CINtec PLUS Cytology

19 Figures 2.2 continued: Examples of CINtec PLUS Cytology negative cells stained with p16 or Ki-67 No dual-stained cells are present in the following images. Squamous cell with nuclear and cytoplasmic p16 staining, negative for CINtec PLUS Cytology Squamous metaplastic cell with nuclear and cytoplasmic p16 staining, negative for CINtec PLUS Cytology

20 Figures 2.2, continued: Examples of CINtec PLUS Cytology negative cells stained with p16 or Ki-67 No dual-stained cells are present in the following images. Cluster of squamous metaplastic or endocervical cells with no dual-stained cells present, negative for CINtec PLUS Cytology
 staining is dark, increasing the microscope light may be necessary to evaluate the presence of Ki-67 (red) nuclear")
21 Slide Screening Procedure The cytologist or pathologist screen CINtec PLUS Cytology-stained slides systematically overlapping fields of view at 10x or 20x magnification. Isolated or single dual-stained cells are easiest to evaluate If the p16 (brown) staining is dark, increasing the microscope light may be necessary to evaluate the presence of Ki-67 (red) nuclear staining If an isolated dual-stained cell has been identified, the stained nucleus and the cytoplasm must be clearly allocated to the same cell Verify the cytoplasm and nucleus are in the same plane of focus (no overlying or underlying red nucleus) With cases screened negative for CINtec PLUS Cytology by a cytologist, the pathologist s review of the slide should include the use of 10x, 20x and/or 40x magnification when confirming or upgrading the result. If the nuclei and cytoplasm appear dark and it is difficult to evaluate specific, red Ki-67 staining due to intense brown p16 staining, increasing the intensity of the microscope light will aid in evaluating the presence of any red signal in the nucleus.
22 When evaluating cell clusters with specific p16 (brown) and Ki-67 (red) staining, use the following cell cluster interpretation algorithm. 1. Look for dual-stained cell(s) at the edge of the cluster If Yes à Test result is positive If No à Proceed to step 2 2. Assess if the p16 staining of the cluster can be defined as diffuse* or focal ^ If focal p16 staining: No further evaluation of this negative cluster If diffuse p16 staining: Proceed to step 3 3. Assess if the Ki-67 stained red nuclei are over/underlying or embedded? (use the fine focus) If the Ki-67 stained, red nuclei are over/underlying à No further evaluation is necessary; result is negative If the Ki-67 stained, red nuclei are embedded à Test result is positive; dual-stained cells present *Diffuse p16 staining is defined as continuous or complete cytoplasmic staining of all cells in the cluster ^Focal p16 staining is defined as patchy, non-continuous or incomplete cytoplasmic staining of the cells in the cluster
 at the edge of the cluster Negative Is the p16 (brown) staining in the cluster diffuse or focal?")
23 CINtec PLUS Cytology cell cluster interpretation flowchart Dual- stained cell(s) at the edge of the cluster? No dual- stain cell(s) at the edge of the cluster Negative Is the p16 (brown) staining in the cluster diffuse or focal? Diffuse p16 staining in the cluster Is the Ki- 67 staining nuclei embedded over/underlying?

24 Figures 2.3: Examples of p16 and Ki-67 staining in cell clusters Each description follows the CINtec PLUS Cytology cell cluster interpretation algorithm to evaluate the staining results. Cluster of cells with no dual-stained cells at the edge of the cluster, focal p16 staining, nuclear Ki-67 staining with no dual-stained cells, negative for CINtec PLUS Cytology. It is difficult to clearly identify dual-stained cells at the edge of this cell cluster, however there is diffuse p16 staining and embedded nuclei with Ki-67 staining. The cell cluster is positive for CINtec PLUS Cytology.
25 Figures 2.3, continued: Examples of p16 and Ki-67 staining in cell clusters 20X Cluster of cells with dual-stained cells at the edge of the cluster, positive for CINtec PLUS Cytology. The cluster also exhibits diffuse p16 staining, and embedded nuclei with Ki-67 staining, supporting the positive staining result.

26 Figures 2.3, continued: Examples of p16 and Ki-67 staining in cell clusters 20X Cluster of cells with dual-stained cells at the edge of the cluster, positive for CINtec PLUS Cytology This cluster also exhibits diffuse p16 staining.
27 Figures 2.3, continued: Examples of p16 and Ki-67 staining in cell clusters 20X Cluster of cells with no dual-stained cells at the edge of the cluster, focal p16 staining, nuclear Ki-67 staining, negative for CINtec PLUS Cytology
28 Figures 2.3, continued: Examples of p16 and Ki-67 staining in cell clusters 20X Cluster of cells with one dual-stained cell at the edge of the cluster, positive for CINtec PLUS Cytology The cluster also demonstrates focal p16 staining, specific nuclear Ki-67 staining.

29 Figures 2.3, continued: Examples of p16 and Ki-67 staining in cell clusters Cluster of glandular cells demonstrating diffuse p16 staining, and embedded nuclei with Ki-67 staining, positive for CINtec PLUS Cytology It may be difficult to see dual-stained cells at the edge of the cluster. 20X Cluster of glandular cells with dual-stained cells at the edge of the cluster, positive for CINtec PLUS Cytology
30 Figures 2.3, continued: Examples of p16 and Ki-67 staining in cell clusters Cluster of cells with dual-stained cells at the edge of the cluster, positive for CINtec PLUS Cytology The cluster also demonstrates diffuse p16 staining. Cluster of cells with dual-stained cells at the edge of the cluster, positive for CINtec PLUS Cytology In addition, diffuse p16 staining is present throughout the cluster. Specific p16 and Ki-67 staining is at varying levels of intensity in this example.
31 Figures 2.3, continued: Examples of p16 and Ki-67 staining in cell clusters 20X It may be difficult to see individual dual-stained cells at the edge of this cluster of cells. The p16 staining is diffuse and there are embedded nuclei with red, Ki-67 staining. This cluster is positive for CINtec PLUS Cytology.

32 Figures 2.3, continued: Examples of p16 and Ki-67 staining in cell clusters A cluster of specific p16 and Ki-67 stained cells with dual-stained cells at the edge of the cluster The cells in the cluster are also exhibiting specific, diffuse p16 staining. Cells identified with the green arrows have weak specific cytoplasmic p16 staining and speckled red nuclear staining, specific for Ki-67. The weak, but specific, p16 staining of the cytoplasm in the cells identified with the green arrows are more intense and have a different hue than the non-specific, brown background staining in the reference cells. Non-specific, red speckling background staining is not present in the cytoplasm of reference cells or in the areas outside of the cells. This cluster is positive for CINtec PLUS Cytology. Non-specific background staining and reference cells will be covered in the next section.
33 Figures 2.3, continued: Examples of p16 and Ki-67 staining in cell clusters Each description follows the CINtec PLUS Cytology cell cluster interpretation algorithm to evaluate the staining results. 20X Cluster of cells with no dual-stained cells at the edge of the cluster and focal p16 staining, negative for CINtec PLUS Cytology There is one cell with nucleus staining with Ki-67 and no p16 staining in the cytoplasm.
34 Cellular Adequacy Assessment Similar to screening Pap cytology slides, CINtec PLUS Cytology slides should be assessed for sample adequacy according to The Bethesda System for Reporting Cervical Cytology, Solomon, The Bethesda guidelines state that at least 5,000 well-visualized/well-preserved squamous cells must be present per pap stained liquid based cytology (LBC) slide, to access adequate cellularity for interpretation. To accurately estimate at least 5,000 cells on ThinPrep and SurePath LBC slides ThinPrep: Minimum average count of at least 3-4 nucleated squamous cells in 10 random, 40x fields of view SurePath: Minimum average count of at least 7-9 nucleated squamous cells in 10 random, 40x fields of view A CINtec PLUS Cytology result should not be reported for a case that is considered unsatisfactory for evaluation due to inadequate cellularity only if no dual-stained cells are identified. If at least one dual-stained cell is present on a slide where there are less than 5,000 well-visualized/well-preserved squamous cells present, regardless of inadequate cellularity, the case shall be evaluated and reported as positive for CINtec PLUS Cytology. Positive and Negative Controls Positive Controls Known positive controls are recommended for monitoring all steps of specimen processing and staining. The positive cytology cell control slide should only be used to monitor performance; it should not be used to aid the clinical diagnosis of patient samples. Specimens processed in the same manner as the patient sample(s) should be used as positive controls. Positive controls are indicative of correctly-prepared specimens and proper staining techniques. One positive control should be included in each staining run. Known positive controls should only be utilized for monitoring the correct performance of processed specimens and test reagents rather than as an aid in formulating a specific diagnosis of patient samples. If the positive controls fail to demonstrate appropriate positive staining, results with the test specimens should be considered invalid. Negative Controls A variety of different cell types present in representative cervical cytology specimens known to be negative for the expression of the p16ink4a and Ki-67 antigens (such as superficial cells) may serve as an internal negative control to assess background staining. Intermediate and superficial squamous epithelial cells present in cervical cytology specimens have undergone cellular differentiation and terminal cell cycle arrest, and are known to be negative for the expression of the p16 and Ki-67 proteins, will serve as an internal negative control. These cells are known as reference cells and will be discussed in section five.
35 Non-specific background staining and artifacts While most cases stained with the CINtec PLUS Cytology test can be easily read as positive or negative, some cases may present challenges to evaluate and interpret. This section explains how to evaluate CINtec PLUS Cytology slides that exhibit non-specific background staining and other artifacts, including Non-specific, brown background staining Non-specific, red background staining and artifacts Non-specific staining of extracellular elements - Including obscuring extracellular elements Preparation related artifacts Non-specific background staining DAB (Brown) and/or fast red detection chemistry can cause non-specific background staining which may be challenging to evaluate. DAB and fast red chromogens can become trapped within cells or appear overlying or underlying of the cells At various intensities: Low/medium/high At various distribution: Few cells to all cells At various characteristics: Homogeneous and/or heterogeneous
36 Non-specific, brown background staining Proliferating cells with Ki-67 staining nuclei, in combination with non-specific, brown background staining in the cytoplasm, may potentially cause a false positive result unless the reader accounts for non-specific, brown background staining present in the cells being thought to be dual-stained. Normal superficial squamous cells can be used as a reference to differentiate specific cytoplasmic p16 staining from non-specific cytoplasmic brown background staining. Since normal superficial squamous cells are mature and terminally differentiated, they cannot express p16 or express Ki-67. Reference cells can be visualized as individual cells or in sheets of cells. If brown staining is present in a moderate to high number of the reference cells in a slide, it should be considered non-specific brown background staining. When evaluating dual-stained cells, the specific p16 staining should be darker than the non-specific staining in the surrounding reference cells. Do not evaluate background staining in reference cells that are arranged in overlapping clusters. Overlapping of cells will intensify the true level of nonspecific background staining. Reference cells should be arranged in a single layer sheets of cells or as isolated cells. The key point To avoid false positive results when non-specific, brown background staining is present in reference cells, the following guidance is recommended. When evaluating a dual stained cell, or cells, (positive for CINtec PLUS Cytology), the cytoplasmic brown p16 stain in the dual-stained cell(s) must be more intense than the surrounding non-specific, cytoplasmic brown background staining of the reference cells within the same 20x to 40x field of view. See Figures 3.0 to 3.3

37 Figure 3.0: Assessing non-specific brown background staining 20X When evaluating dual stained cells in a case with non-specific, brown background staining of reference cells consider the following, using the image above as an example. Compare the non-specific brown background staining in the sheets of squamous cells (reference cells) with the other cells of interest (cells with brown cytoplasmic and specific red, nuclear Ki-67 staining) The intensity of the brown cytoplasmic stain in the cells of interest must be higher than the non-specific brown background staining in the reference cells to be considered specific p16 staining. If the cells of interest are confirmed to have specific p16 staining, with specific Ki-67 stained nuclei, then the cells are evaluated as dual-stained cells, positive for CINtec PLUS Cytology

38 Figure 3.1: Illustration of non-specific, brown background staining in cells stained with CINtec PLUS Cytology Assessing non-specific, brown background staining 1. Compare the reference cells, normal squamous cells, to the cells of interest, or the cells with brown cytoplasmic and specific red, nuclear Ki-67 staining. 2. Is the intensity of the brown cytoplasm in the cells of interest higher than any brown staining in the reference cells? a. No: If the brown staining in the cytoplasm of the cell(s) of interest contain non-specific brown staining à negative for CINtec PLUS Cytology b. Yes: The brown staining in the cytoplasm of the cell(s) of interest is specific p16 staining à positive for CINtec PLUS Cytology


39 Figure 3.2: The specific, brown p16 staining of the dual-stained cell is more intense than the non-specific cytoplasmic brown background staining in the reference cells. Figure 3.3: The specific, brown p16 staining of the dual-stained cell is more intense than the non-specific brown background staining in the reference cells.
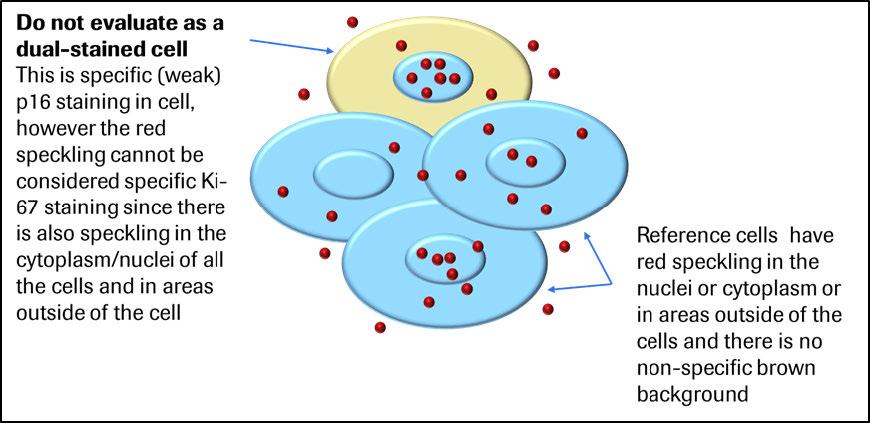
40 Non-specific red background staining Non-specific, red background staining typically exhibits in a speckled pattern that may appear over, under, or in the cytoplasm and nuclei of a cervical cell. This may also be seen in the cytoplasm and nuclei of reference cells or in the cytoplasm of dual-stained cells staining positive for CINtec PLUS Cytology, as well. Non-specific, red speckling background staining can also be present in areas outside of cells on the slide. As stated earlier, the criteria for specific, Ki-67 nuclear staining includes red signal that may be uniformly stained within the nucleus of the cell, or partially stained displaying as a granular or speckled staining pattern. Since red staining in a speckled pattern can be specific Ki-67 nuclear staining, this must be differentiated from non-specific, red speckling background staining. Criteria for differentiating specific and non-specific Ki-67 nuclear staining Non-specific red speckling background staining: If red speckling is present in the nucleus of a cell and the same red speckling pattern is also present in the cytoplasm, in the areas outside of the cell, or in other reference cells, it is non-specific, red speckling background staining and this nucleus should not be evaluated as specific Ki-67 staining. See Figure 3.4 Specific Ki-67 nuclear red staining in a speckled pattern: Red speckling or a granular staining pattern in the nucleus can only be specific if there is no red speckling in the cytoplasm of the cell, the cytoplasm of other reference cells, or in the areas around the cells. If present in a cell stained with specific p16 staining, this cell can be evaluated as a dual-stained positive cell, as long as the red speckled staining is localized to the nucleus of the cell. See illustration in figure 3.5 In cells with uniform, red nuclear staining, indicative of specific Ki-67 staining, any red speckling in reference cells or else ware can be disregarded as non-specific, red background staining. See Figure 3.6 In a case with only one to three dual-stained cells identified, it is advisable to find a cell with uniform Ki-67 staining and specific p16 staining to confirm a positive result. In a similar case with only one to three dual-stained cells demonstrating specific, cytoplasmic p16 staining and specific, speckled or partial Ki-67 staining in the nuclei, but no dual-stained cells demonstrating a uniform Ki-67 staining pattern, a positive result should be based on the dual-stained cells with speckled or partial nuclear Ki-67 staining. See Figures for additional examples of red-speckling NOTE: Use the microscope s fine focus knob to verify red speckling is in the same focal plane as the nucleus to evaluate as specific Ki-67 staining.

41 Figure 3.4 Figure 3.5


42 Figure 3.6 Figure 3.7: Non-specific red speckling background staining in a case positive for CINtec PLUS Cytology The non-specific red speckling background staining typically does not interfere with the interpretation of the dual-stained cell. 60X
43 Figure 3.8: Cluster of cells with non-specific red speckling background staining in extra cellular particles in or on the cytoplasm, negative for CINtec PLUS Cytology NOTE: If red speckling was also located on or in the nuclei of the cells, this cluster would remain negative.
44 Figure 3.9: Non-specific red speckling background staining of mucus or blood This artifact staining is located outside of the cervical cells and typically does not typically interfere with the interpretation of CINtec PLUS Cytology. Dual-stained cells (circled) are present, positive for CINtec PLUS Cytology.
45 Figure 3.10: Dual-stained cell with cytoplasmic p16 staining and weak, nuclear Ki-67 staining, Positive for CINtec PLUS Cytology There is non-specific, red speckling background staining in the cytoplasm of the dual-stained cell, not interfering with the specific p16 and Ki-67 staining. 60X


46 Examples of brown and red non-specific background staining Figure 3.11: Non-specific brown and red staining with specific p16 staining Figure 3.12: Non-Specific brown and red staining with a dual-stained cell

47 Figure 3.13: Non-specific brown and red staining with specific p16 and Ki-67 staining in different cells
48 Non-specific background staining assessment CINtec PLUS Cytology slides must be evaluated for non-specific background staining and be judged as acceptable or unacceptable as defined in table below. Non-specific background staining can occur with individual normal squamous cells, or reference cells as opposed to the specific cytoplasmic (p16) and or nuclear (p16 or Ki-67) staining of normal or abnormal cells contained within the cytology specimens. Definition of background acceptability Acceptable No discernible non-specific (background) staining Slight discernible non-specific staining that does not interfere with specific stain interpretation Some discernible non-specific staining that does not interfere with specific stain interpretation Substantial discernible non-specific staining that does not interfere with specific stain interpretation Unacceptable Substantial discernible non-specific staining that interferes with specific stain interpretation A case with unacceptable background should be reported as unsatisfactory for evaluation or unevaluable.
49 Red Chromogen Bleeding Red chromogen bleeding is a non-specific, red staining artifact, which may occasionally occur when specific strong nuclear Ki-67 staining is expressed and the fast red chromogen bleeds into the cytoplasm of the cervical cell(s). Figure 3.14: Cluster of cell with fast red chromogen bleeding into the cytoplasm of the cell 20X Figure 3.15: An example of an isolated cell with fast red chromogen bleeding into the cytoplasm of the cell Notice the dual-stained cell (lower right) which exhibits a thin rim of specific, cytoplasmic p16 staining, positive for CINtec PLUS Cytology present.
50 Non-specific staining of extracellular elements Extracellular elements can become stained with components of the DAB (brown) and fast red detection chemistries. This can cause non-specific staining reactions of extracellular elements including Bacteria Blood Mucus Inflammation Yeast or Candida Non-specific obscuring staining of extracellular material Non-specific staining of bacteria, blood, mucus and inflammation is considered an obscuring element if it obscures more than 75% of the epithelial cells in the sample preparation area of the slide. These cases should not be evaluated, and reported as Unsatisfactory for evaluation due to obscuring extracellular elements, assuming no dual-stained cells are visible. A slide with more than 75% obscuring, non-specific staining of extra cellular material, containing at least one dual- stained cell, should be reported as positive for CINtec PLUS Cytology. Non-specific staining of bacteria, blood, mucus and inflammation is not the same as non-specific background staining of reference cells, and cannot be used as a comparison to evaluate specific brown staining. If both non-specific artifact staining of bacteria, blood, mucus, or inflammation and non-specific background staining of reference cells are present in the same case, you must first differentiate the non-specific staining of bacteria, blood, mucus, or inflammation from the non-specific background staining of the reference cells when evaluating dual-stained cervical cells. See Figures for examples of non-specific staining of extracellular elements that may be present on slides stained with CINtec PLUS Cytology.
51 Figure 3.16: Non-specific, red and brown staining of mucus and blood with entrapped degenerating Ki-67 staining nuclei. Non-specific staining of mucus or blood should not be evaluated as specific cytoplasmic staining. This case is negative for CINtec PLUS Cytology. 20X Figure 3.17: Non-specific red speckling background staining of mucus or blood, with dual-stained cells (circled) present, positive for CINtec PLUS Cytology This artifact staining is located outside of the cervical cells and typically does not typically interfere with the interpretation of CINtec PLUS Cytology.

52 Figure 3.18: Obscuring non-specific brown staining of mucus Non-specific staining of mucus can occur with with DAB (brown) or fast red chromogens. Figure 3.19: Non-specific red artifact staining of Neutrophils.

53 Figure 3.20: Non-specific, red artifact staining of bacteria Bacteria may also non-specifically stain brown. 10X 20X Figure 3.21: Staining of Candida 10X 20X


54 Figure 3.22: Non-specific brown staining of mucus or blood with a dual-stained cell, positive for CINtec PLUS Cytology 20X Dual-stained cells are present within the brown staining of the mucus or blood. The p16 staining of the dual-stained cell is more intense than any non-specific brown background staining in the reference cells. The non-specific brown artifact staining of the mucus or blood is not considered background staining, and should not be used as a reference to evaluate specific staining of squamous cells. See the Challenging Cases section for more details on non-specific background staining.
55 Differences between non-specific background staining and non-specific staining of extracellular elements Non-specific background staining Non-specific artifact staining Brown staining in cytoplasm and or nucleus of reference cells Brown or red staining of blood and mucus Red staining typically occurring in a speckling pattern, located in nuclei and cytoplasm of reference cells or dual-stained cells, and in areas outside of cells on the slide. Red staining of inflammatory cells Specific red nuclear staining, bleeding into the cytoplasm of the cell(s) Red and brown staining of bacteria Preparation related artifacts Artifacts related to the technical preparation of stained CINtec PLUS Cytology slides include Cracking of the aqueous mounting media due to insufficient drying of the aqueous mounting media during the post processing procedure. See Figure Cornflaking, associated with airdrying artifacts during the post processing procedure. See Figure Inconsistent or uneven counterstaining of the reference squamous cells with brown background staining may be associated with poor tap water quality. If present in the majority of stained slides, recommend using either deionized or distilled water with mild detergent when rinsing liquid coverslip from the stained slides prior to the post processing procedure. See Figures 3.25 and 3.26.


56 Figure 3.23: Insufficient drying of the CC/Mount aqueous mounting medium can cause a cracking artifact. Slides maybe evaluated normally, however be sure the cracking does not obscure staining and cellular detail. Figure 3.24: Air drying, cornflaking artifact as a result of not following the post processing procedure Note: A post-processing procedure using an aqueous mounting media is required to mount and coverslip the stained CINtec PLUS Cytology slides. Fast red chromogen is soluble in alcohol and its signal will fade if exposed to alcohol. CC/Mount aqueous mounting media eliminates the need to dehydrate the stained slides with ascending changes of gradient alcohols, and prevents any fading of the red signal, which may cause false negative results. See the CINtec PLUS Cytology package insert for more details.


57 Figure 3.25: Inconsistent or uneven counterstaining of the reference squamous cells with a brown background This artifact may be associated with poor tap water quality. If present in the majority of stained slides, recommend using either deionized or distilled water with mild detergent when rinsing liquid coverslip from the stained slides prior to mounting. Figure 3.26: Inconsistent or uneven counterstaining of the reference squamous cells with brown background staining This artifact may be associated with poor tap water quality. If present in the majority of stained slides, recommend using either deionized or distilled water with mild detergent when rinsing liquid coverslip from the stained slides prior to mounting. 10X
58
59 Challenging Cases There will be cases that may present challenges to the interpretation and evaluation of the staining results. Challenging cases typically include the following characteristics: Low number of dual-stained cells or cells suspicious for being dual-stained Background staining Cell clusters with variable staining patterns Weak or dark staining intensity of specific p16 and Ki-67 staining When screening and evaluating slides stained with CINtec PLUS Cytology, identifying at least one dual-stained cell is the cut-off for a positive test result. In cases where there are low numbers of cells with weak but specific cytoplasmic p16 and/or nuclear Ki-67 staining, reporting a positive or negative result may be challenging, especially if there is nonspecific brown background staining present in the reference cells. When evaluating slides with one to three cells demonstrating weak cytoplasmic p16 staining and weak or specific speckled nuclear Ki-67 staining,, always compare the specific p16 staining intensity of the suspected dual-stained cell(s) with the reference cells to differentiate the specific brown staining from non-specific, brown background staining. Any red signal that is located in the nucleus of a cervical cell can be considered specific Ki-67 staining when there is no red speckling (non-specific background staining) located in the cytoplasm of a cell and/or on the areas outside of the cells. In a case with only one to three dual-stained cells identified, it is advisable to find a cell with uniform Ki-67 staining and specific p16 staining to confirm a positive result. In a similar case with only one to three dual-stained cells demonstrating specific cytoplasmic p16 staining, and specific, speckled or partial Ki-67 staining in the nuclei, but no dual-stained cells demonstrating uniform Ki-67 staining, a positive result should be based on the dual-stained cells with speckled or partial nuclear Ki-67 staining. Dual-stained cells with intense, specific cytoplasmic and nuclear p16 staining can be challenging to evaluate. The nuclei and cytoplasm may appear dark and difficult to evaluate specific red Ki-67 staining due to intense brown p16 staining, increasing the intensity of the microscope light will aid in evaluating the presence of any red signal in the nucleus. Clusters can be challenging to evaluate, however following the CINtec PLUS Cytology cell cluster interpretation algorithm will assist in the evaluation of cases which contain challenging clusters of cells with specific p16 and Ki-67 staining.

60 Figures : Examples of challenging cases Figure 4.0: A dual-stained cell with weak, cytoplasmic p16 staining and weak nuclear Ki-67 staining, positive for CINtec PLUS Cytology The cytoplasmic p16 staining of the dual-stained cell is a different hue than the brown-grey background staining and more intense than the overall brown background staining of the reference cells. Although the red nuclear signal is not intense, the staining signal is located in the nucleus of the cell and considered specific staining. This is the only one dual-stained cell on the slide. 20X


61 Figure 4.1: A dual-stained cell with weak, but specific, cytoplasmic p16 staining and specific red nuclear staining in a speckled, granular pattern The granular or red speckling is considered specific Ki-67 staining since there is no red speckling in the cytoplasm of the cell, in other reference cells or in the areas outside of the cells. The cytoplasmic p16 staining of the dual-stained cell is weak, however more intense compared to the surrounding reference cells which do not exhibit any significant level of non-specific, brown background staining. This is the only dual-stained cell identified on the slide. Based on this single dual-stained cell, the case is positive for CINtec PLUS Cytology. 20X
62 Figure 4.2: A single dual-stained cell with both cytoplasmic and nuclear p16 staining, and weak nuclear Ki-67 staining The red, Ki-67 signal is visible in the nuclei that are also staining with the brown p16 signal. The microscope light may need to be increased to evaluate cells that have both nuclear Ki-67 and p16 staining to confirm specific Ki-67 (red) staining. In this case, the reference cells are not exhibiting non-specific, brown background staining, which permits easier evaluation of the specific cytoplasmic p16 staining in the dual-stained cell. Based on the single dual-stained cell, this case is positive result for CINtec PLUS Cytology.


63 Figures 4.3: Additional examples of challenging cells stained with CINtec PLUS Cytology A single dual-stained cell with weak, cytoplasmic p16 staining and weak nuclear Ki-67 staining, positive for CINtec PLUS Cytology The cytoplasmic p16 staining of the dual-stained cell is a different hue than the brown-grey background staining seen in the reference cells, and more intense than the overall brown background staining. 20X
64 Figure 4.4: Two dual-stained cells, circled, with weak cytoplasmic p16 staining The cell on the left exhibits weak Ki-67 staining and the cell on the right has moderate nuclear Ki-67 staining. This case is positive for CINtec PLUS Cytology. The reference cells have no significant brown background staining, which allows for easier evaluation of the weak, specific p16 staining in the dual-stained cells. Non-specific red speckling is absent in the cytoplasm of reference cells and in the areas outside of the cells. 20X


65 Figure 4.5: A single dual-stained cell with,cytoplasmic p16 staining and nuclear Ki-67 staining, positive for CINtec PLUS Cytology The nuclear to cytoplasmic ratio of the dual-stained cell is relatively high, and the cytoplasmic p16 staining is visible. The cytoplasmic p16 staining is darker than the background staining seen in the reference cell. To the right of the dual-stained cell is a single cell exhibiting specific p16 staining. 20X

66 Figure 4.6: Two dual-stained cells with weak, specific cytoplasmic p16 staining and specific nuclear Ki-67 staining, positive for CINtec PLUS Cytology The cytoplasmic p16 staining of the dual-stained cell is a different hue and slightly more intense than the overall brown background staining of the reference cells. Red speckling is present as non-specific red background staining in the cytoplasm of the reference cells, however it does not interfere with the uniform Ki-67 staining in the nuclei of the dualstained cells. 20X Figure 4.7: Two dual-stained cells (circled), positive for CINtec PLUS Cytology The dual-stained cell in the right side of the circle is considered more challenging to evaluate. The cytoplasm of this cell has specific but weak cytoplasmic p16 staining. The nuclei in this cell exhibits weak, partial red staining, and is considered specific Ki-67 staining. The reference cells do not have any noticeable non-specific brown background staining, which allows for easier evaluation of the weak, specific p16 staining. There is no non-specific red speckling present in the cytoplasm of reference cells or in the areas outside of the cells. 20X

67 Figure 4.8: An isolated cell, suspicious for being dual-stained, with specific nuclear Ki-67 staining and questionable p16 staining. The cytoplasm has an area of weak brown staining that does not appear to be higher than the background staining in the reference cells. The cytoplasmic brown staining does not appear to be specific p16 staining, and is showing folded cytoplasm, which can falsely intensify the brown background staining. If evaluating only this cell for the entire slide, it would be considered negative for CINtec PLUS Cytology. The reference cell exhibits background staining, and appears to be similar to the brown staining in the circled cell, therefore be cautious in evaluating the circled cell as a dual-stained cell. 20X


68 Figure 4.9: An example of variable staining in cell cluster with many dual-stained cells at the edge of the cluster exhibiting specific p16 and Ki-67 staining. This cluster is positive for CINtec PLUS Cytology; diffuse p16 staining is also present. The reference cells do not exhibit non-specific, brown background staining, allowing for easier evaluation of the weaker p16 signal in the cells towards the edge of the cluster. The nuclei in the dual-stained cells exhibit varying intensities of staining. There are nuclei with strong Ki-67 signals and others with weak, speckled Ki-67 staining. 20X
69 Knowledge Check Evaluate the following images to discern between positive and negative CINtec PLUS Cytology staining. An answer key is provided in the following section. 60X 1. CINtec PLUS Cytology staining is: Positive Negative

70 2. CINtec PLUS Cytology staining is: Positive Negative 3. CINtec PLUS Cytology staining is: Positive Negative

71 60X 4. CINtec PLUS Cytology staining is: Positive Negative 5. CINtec PLUS Cytology staining is: Positive Negative

72 6. CINtec PLUS Cytology staining is: Positive Negative 7. CINtec PLUS Cytology staining is: Positive Negative

73 60X 8. CINtec PLUS Cytology staining is: Positive Negative 9. CINtec PLUS Cytology staining is: Positive Negative
74 10. CINtec PLUS Cytology staining is: Positive Negative 11. CINtec PLUS Cytology staining is: Positive Negative

75 12. CINtec PLUS Cytology staining is: Positive Negative 60X 13. CINtec PLUS Cytology staining is: Positive Negative

76 14. CINtec PLUS Cytology staining is: Positive Negative
 and Ki-67 (red), positive for CINtec PLUS Cytology 2.")
77 Knowledge Check Answer Key 1. A dual-stained squamous cell staining positive for p16 (brown) and Ki-67 (red), positive for CINtec PLUS Cytology 2. Two squamous metaplastic cells with only specific Ki-67 (red) staining; both cells are negative for CINtec PLUS Cytology

78 3. Cluster of squamous cells showing focal p16 staining and a few cells with Ki-67 stained nuclei, negative for CINtec PLUS Cytology 4. Cluster of cells with no dual-stained cells at the edge of the cluster, focal, specific p16 staining and nuclei staining with Ki-67, negative for CINtec PLUS Cytology

79 5. Sheet of squamous cells exhibiting weak, specific p16 staining and weak, specific Ki-67 stained nuclei, positive for CINtec PLUS Cytology Reference cells do not have noticeable non-specific, brown background staining, allowing for easier evaluation of the weak, specific p16 staining of the sheet of cells. 6. Cluster of Glandular cells with dual-stained cells which may be difficult to see at the edge of the cluster. Strong diffuse, specific p16 staining and strong, specific Ki-67 stained nuclei embedded in the cluster, positive for CINtec PLUS Cytology
80 7. Two dual-stained squamous cells, staining positive for weak, but specific cytoplasmic p16 staining and nuclear Ki-67 (red) staining, positive for CINtec PLUS Cytology 8. Two squamous cells: (Top) Staining only with specific p16 in the cytoplasm and the nucleus, (Bottom) cell nucleus is staining with Ki-67 both cells are negative for CINtec PLUS Cytology

81 20X 9. Dual-stained cell with specific, weak cytoplasmic p16 staining and weak nuclear Ki-67 staining, positive for CINtec PLUS Cytology The cytoplasmic p16 staining of the dual-stained cell is a different hue than the brown-grey background staining and more intense than the overall brown background staining of the reference cells. 20X 10. Dual-stained cell with specific, weak cytoplasmic p16 staining and weak, nuclear Ki-67 staining, positive for CINtec PLUS Cytology The cytoplasmic p16 staining of the dual-stained cell is a different hue than the brown-grey background staining and more intense than the overall brown background staining of the reference cells.

82 11. Cluster of squamous cells with one dual-stained cell at the edge of the cluster, diffuse, specific p16 staining, and a few nuclei with specific Ki-67 staining embedded in the cluster, positive for CINtec PLUS Cytology Red speckling artifact is noted in this cluster, and where present, this artifact cannot be considered as specific nuclear Ki-67 staining. 12. One suspicious squamous cell with weak, specific nuclear Ki-67 staining and cytoplasm with very weak brown staining, and no background staining In a clinical setting, cases where there may be only one similarly stained cell, a consensus review of the case considering patient history is recommended to report as positive or negative for CINtec PLUS Cytology.
 with weak, specific p16 cytoplasmic and nuclear staining and weak, specific Ki-67 nuclear staining, positive for CINtec PLUS Cytology; the cytoplasm and nucleus in")

83 60X 13. One dual-stained cell (upper right) with weak, specific p16 cytoplasmic and nuclear staining and weak, specific Ki-67 nuclear staining, positive for CINtec PLUS Cytology; the cytoplasm and nucleus in the other cell (bottom left) is staining only with p16. The microscope light may need to be increased to differentiate the specific red and brown staining to confirm dual-staining of the cell. The reference cells are not exhibiting non-specific, brown background staining, making it easier to differentiate the weak, specific p16 staining in the dual-stained cell. 14. Cluster of squamous cells with a dual-stained cell at the edge of the cluster, positive for CINtec PLUS Cytology There are three nuclei in this cluster demonstrating specific Ki-67 staining. The Ki-67 stained nuclei lowest in the field, at the edge of the cluster exhibits specific, brown stained cytoplasm. The cluster is also exhibiting weak, diffuse p16 staining.
84 References 1. Castle, P.E.P. et al., Evidence for frequent regression of cervical intraepithelial neoplasia-grade 2. Obstetrics and gynecology, 113(1), pp Available at: [Accessed June 4, 2014]. 2. Arends, M.J., Buckley, C.H. & Wells, M., Aetiology, pathogenesis, and pathology of cervical neoplasia. Journal of clinical pathology, 51(2), pp Available at: 3. Muñoz, N. et al., Chapter 1: HPV in the etiology of human cancer. Vaccine, 24 Suppl 3, pp.s3/1 10. Available at: [Accessed May 23, 2014]. 4. Killeen, J.L. et al., Improved abnormal pap smear triage using cervical cancer biomarkers. Journal of lower genital tract disease, 18(1), pp.1 7. Available at: 5. Van Ballegooijen, M. et al., Present evidence on the value of HPV testing for cervical cancer screening: a model-based exploration of the (cost-)effectiveness. British journal of cancer, 76(5), pp Available at: 6. Zappacosta, R. et al., Implementing specificity of HPV-DNA primary screening in a successful organised cervical cancer prevention programme. Gynecologic oncology, 128(3), pp Available at: [Accessed May 27, 2014]. 7. Franco, E.L. et al., The expected impact of HPV vaccination on the accuracy of cervical cancer screening: the need for a paradigm change. Archives of medical research, 40(6), pp Available at: [Accessed June 3, 2014]. 8. Naucler, P. et al., Efficacy of HPV DNA testing with cytology triage and/or repeat HPV DNA testing in primary cervical cancer screening. Journal of the National Cancer Institute, 101(2), pp Available at: [Accessed June 3, 2014]. 9. Chelmow, D. et al., The evolution of cervical screening and the specialty of obstetrics and gynecology. Obstetrics and gynecology, 119(4), pp Available at: [Accessed June 3, 2014]. 10. Wentzensen, N. & von Knebel Doeberitz, M., Biomarkers in cervical cancer screening. Disease markers, 23(4), pp Available at: Arbyn, M. et al., The APTIMA HPV assay versus the Hybrid Capture 2 test in triage of women with ASC- US or LSIL cervical cytology: a meta-analysis of the diagnostic accuracy. International journal of cancer. Journal
85 international du cancer, 132(1), pp Available at: [Accessed June 2, 2014]. 12. Roelens, J. et al., p16ink4a immunocytochemistry versus human papillomavirus testing for triage of women with minor cytologic abnormalities: a systematic review and meta-analysis. Cancer cytopathology, 120(5), pp Available at: [Accessed May 27, 2014]. 13. Carozzi, F. et al., Risk of high-grade cervical intraepithelial neoplasia during follow-up in HPV-positive women according to baseline p16-ink4a results: a prospective analysis of a nested substudy of the NTCC randomised controlled trial. The lancet oncology, 14(2), pp Available at: [Accessed May 29, 2014]. 14. Schmidt, D. et al., p16/ki-67 dual-stain cytology in the triage of ASCUS and LSIL papanicolaou cytology: results from the European equivocal or mildly abnormal Papanicolaou cytology study. Cancer cytopathology, 119(3), pp Available at: [Accessed May 19, 2014]. 15. Petry, K.U. et al., Triaging Pap cytology negative, HPV positive cervical cancer screening results with p16/ki-67 Dual-stained cytology. Gynecologic oncology, 121(3), pp Available at: [Accessed May 19, 2014]. 16. Ravarino, A. et al., CINtec PLUS immunocytochemistry as a tool for the cytologic diagnosis of glandular lesions of the cervix uteri. American journal of clinical pathology, 138(5), pp Available at: [Accessed June 3, 2014]. 17. Singh, M. et al., Immunocytochemical colocalization of P16(INK4a) and Ki-67 predicts CIN2/3 and AIS/adenocarcinoma. Cancer cytopathology, 120(1), pp Available at: [Accessed May 27, 2014]. 18. Ikenberg H, Bergeron C, Schmidt D, Griesser H, Alameda F, Angeloni C, Bogers J, Dachez R, Denton K, Hariri J, Keller T, von Knebel Doeberitz M, Neumann HH, Puig-Tintore LM, Sideri M, Rehm S, Ridder R; PALMS Study Group. Screening for cervical cancer precursors with p16/ki-67 dual-stained cytology: results of the PALMS study. J Natl Cancer Inst Oct 16;105(20): Scholzen, T. and Gerdes, J. (2000), The Ki-67 protein: From the known and the unknown. J. Cell. Physiol., 182: doi: /(SICI) (200003)182:3<311::AID-JCP1>3.0.CO; Roche, 2014d. Module 3: Cervical Cancer Screening and Diagnosis Methods., p Waldstrøm, M., The Value of Adding CINtec PLUS Dual-Staining for p16 (INK4A)/ Ki-67 on COBAS HPV Positive Women for Detection of High Grade CIN 22. Bethesda system: Terminology for reporting results of cervical cytology, 2014

86 Roche VENTANA, BENCHMARK, CINTEC and COBAS are trademarks of Roche. All other trademarks are the property of their respective owners. 6139B 0816 RTDPCASFC0043
CINtec PLUS Cytology. Interpretation training
 CINtec PLUS Cytology Interpretation training Objectives After reviewing this learning module, you will have a basic understanding of how to interpret CINtec PLUS Cytology, including: The mechanism of action
CINtec PLUS Cytology Interpretation training Objectives After reviewing this learning module, you will have a basic understanding of how to interpret CINtec PLUS Cytology, including: The mechanism of action
Table of Contents. 1. Overview. 2. Interpretation Guide. 3. Staining Gallery Cases Negative for CINtec PLUS
 Staining Atlas Table of Contents 1. Overview 1.1 Introduction 1.2 Role of p16 INK4a 1.3 Role of Ki-67 1.4 Molecular Pathogenesis 1.5 p16 INK4a Expression in Cervical Dysplasia 1.6 The Concept of CINtec
Staining Atlas Table of Contents 1. Overview 1.1 Introduction 1.2 Role of p16 INK4a 1.3 Role of Ki-67 1.4 Molecular Pathogenesis 1.5 p16 INK4a Expression in Cervical Dysplasia 1.6 The Concept of CINtec
CINtec p16 INK4a Staining Atlas
 CINtec p16 INK4a Staining Atlas Rating Rating Positive The rating positive will be assigned if the p16 INK4a -stained slide shows a continuous staining of cells of the basal and parabasal cell layers of
CINtec p16 INK4a Staining Atlas Rating Rating Positive The rating positive will be assigned if the p16 INK4a -stained slide shows a continuous staining of cells of the basal and parabasal cell layers of
P16 et Ki67 Biomarkers: new tool for risk management and low grade intraepithelial lesions (LGSIL): be ready for the future.
: be ready for the future.") P16 et Ki67 Biomarkers: new tool for risk management and low grade intraepithelial lesions (LGSIL): be ready for the future. Mark H Stoler, MD University of Virginia Health System, Charlottesville, VA,
P16 et Ki67 Biomarkers: new tool for risk management and low grade intraepithelial lesions (LGSIL): be ready for the future. Mark H Stoler, MD University of Virginia Health System, Charlottesville, VA,
chapter 4. The effect of oncogenic HPV on transformation zone epithelium
 chapter 4. The effect of oncogenic HPV on transformation zone epithelium CHAPTER 1 All squamous cervical cancer (and probably all cervical adenocarcinoma) is associated with oncogenic HPV, and the absence
chapter 4. The effect of oncogenic HPV on transformation zone epithelium CHAPTER 1 All squamous cervical cancer (and probably all cervical adenocarcinoma) is associated with oncogenic HPV, and the absence
SQUAMOUS CELLS: Atypical squamous cells (ASC) - of undetermined significance (ASC-US) - cannot exclude HSIL (ASC-H)
 - of undetermined significance (ASC-US) - cannot exclude HSIL (ASC-H)") SQUAMOUS CELLS: Atypical squamous cells (ASC) - of undetermined significance (ASC-US) - cannot exclude HSIL (ASC-H) ASC refers to cytologic changes suggestive of SIL, which are qualitativley or quantitatively
SQUAMOUS CELLS: Atypical squamous cells (ASC) - of undetermined significance (ASC-US) - cannot exclude HSIL (ASC-H) ASC refers to cytologic changes suggestive of SIL, which are qualitativley or quantitatively
New Diagnoses Need New Approaches: A Glimpse into the Near Future of Gynecologic Pathology
 New Diagnoses Need New Approaches: A Glimpse into the Near Future of Gynecologic Pathology United States and Canadian Academy of Pathology 102 nd Annual Meeting Baltimore, Maryland Christina S. Kong, M.D.
New Diagnoses Need New Approaches: A Glimpse into the Near Future of Gynecologic Pathology United States and Canadian Academy of Pathology 102 nd Annual Meeting Baltimore, Maryland Christina S. Kong, M.D.
Appropriate Use of Cytology and HPV Testing in the New Cervical Cancer Screening Guidelines
 Appropriate Use of Cytology and HPV Testing in the New Cervical Cancer Screening Guidelines Tim Kremer, MD Ralph Anderson, MD 1 Objectives Describe the natural history of HPV particularly as it relates
Appropriate Use of Cytology and HPV Testing in the New Cervical Cancer Screening Guidelines Tim Kremer, MD Ralph Anderson, MD 1 Objectives Describe the natural history of HPV particularly as it relates
Cervical Dysplasia and HPV
 Cervical Dysplasia and HPV J. Anthony Rakowski D.O., F.A.C.O.O.G. MSU SCS Board Review Coarse HPV Double stranded DNA virus The HPV infect epithelial cells of the skin and mucous membranes Highest risk
Cervical Dysplasia and HPV J. Anthony Rakowski D.O., F.A.C.O.O.G. MSU SCS Board Review Coarse HPV Double stranded DNA virus The HPV infect epithelial cells of the skin and mucous membranes Highest risk
Histopathology: Cervical HPV and neoplasia
 Histopathology: Cervical HPV and neoplasia These presentations are to help you identify basic histopathological features. They do not contain the additional factual information that you need to learn about
Histopathology: Cervical HPV and neoplasia These presentations are to help you identify basic histopathological features. They do not contain the additional factual information that you need to learn about
Cervical Cancer Screening for the Primary Care Physician for Average Risk Individuals Clinical Practice Guidelines. June 2013
 Cervical Cancer Screening for the Primary Care Physician for Average Risk Individuals Clinical Practice Guidelines General Principles: Since its introduction in 1943, Papanicolaou (Pap) smear is widely
Cervical Cancer Screening for the Primary Care Physician for Average Risk Individuals Clinical Practice Guidelines General Principles: Since its introduction in 1943, Papanicolaou (Pap) smear is widely
Cervical cancer prevention: Advances in primary screening and triage system
 Cervical cancer prevention: Advances in primary screening and triage system Dr Farid Hadi Regional Medical and Scientific Affairs Roche Diagnostics Asia-Pacific, Singapore Cervical cancer is highly preventable
Cervical cancer prevention: Advances in primary screening and triage system Dr Farid Hadi Regional Medical and Scientific Affairs Roche Diagnostics Asia-Pacific, Singapore Cervical cancer is highly preventable
HPV: cytology and molecular testing
 HPV: cytology and molecular testing Human Papillomavirus and how we test for it at Medlab Central Palmerston North for Cervical Cancer prevention and management. Developed by Reem Mustafa Cytology and
HPV: cytology and molecular testing Human Papillomavirus and how we test for it at Medlab Central Palmerston North for Cervical Cancer prevention and management. Developed by Reem Mustafa Cytology and
Cervical Cancer : Pap smear
 Taking a PAP SMEAR Cervical Cancer : Pap smear George N Papanicolaou introduced cervical cytology in clinical practice in 1940 In 1945, PAP smear was endorsed by American cancer society as an effective
Taking a PAP SMEAR Cervical Cancer : Pap smear George N Papanicolaou introduced cervical cytology in clinical practice in 1940 In 1945, PAP smear was endorsed by American cancer society as an effective
Pushing the Boundaries of the Lab Diagnosis in Asia
 Pushing the Boundaries of the Lab Diagnosis in Asia Diana Lim MBBS, FRCPA, FRCPath (UK) Senior Consultant National University Health System and National University of Singapore Department of Pathology
Pushing the Boundaries of the Lab Diagnosis in Asia Diana Lim MBBS, FRCPA, FRCPath (UK) Senior Consultant National University Health System and National University of Singapore Department of Pathology
Workshop for O& G trainees and paramedics 17 Dec 2011 Cytological Interpretation
 Workshop for O& G trainees and paramedics 17 Dec 2011 Cytological Interpretation May Yu Director of Cytology Laboratory Service Department of Anatomical & Cellular Pathology Prince of Wales Hospital Cervical
Workshop for O& G trainees and paramedics 17 Dec 2011 Cytological Interpretation May Yu Director of Cytology Laboratory Service Department of Anatomical & Cellular Pathology Prince of Wales Hospital Cervical
p16ink4a expression in cervical intraepithelial neoplasia and cervical cancer
 Original Article Brunei Int Med J. 2013; 9 (3): 165-171 p16ink4a expression in cervical intraepithelial neoplasia and cervical cancer Kalpana KUMARI 1 and Akhila Arcot VADIVELAN 2 1 Department of Pathology,
Original Article Brunei Int Med J. 2013; 9 (3): 165-171 p16ink4a expression in cervical intraepithelial neoplasia and cervical cancer Kalpana KUMARI 1 and Akhila Arcot VADIVELAN 2 1 Department of Pathology,
Clinical Practice Guidelines June 2013
 Clinical Practice Guidelines June 2013 General Principles: The Papanicolaou (Pap) smear is widely credited with reducing mortality from cervical cancer, and remains the single best method for the early
Clinical Practice Guidelines June 2013 General Principles: The Papanicolaou (Pap) smear is widely credited with reducing mortality from cervical cancer, and remains the single best method for the early
VENTANA MMR IHC Panel Interpretation Guide for Staining of Colorectal Tissue
 VENTANA MMR IHC Panel Interpretation Guide for Staining of Colorectal Tissue VENTANA anti-mlh1 (M1) Mouse Monoclonal Primary Antibody VENTANA anti-pms2 (A16-4) Mouse Monoclonal Primary Antibody VENTANA
VENTANA MMR IHC Panel Interpretation Guide for Staining of Colorectal Tissue VENTANA anti-mlh1 (M1) Mouse Monoclonal Primary Antibody VENTANA anti-pms2 (A16-4) Mouse Monoclonal Primary Antibody VENTANA
Faculty Pap Smear Guidelines: Family Planning Update 2008 Part Two
 Faculty Pap Smear Guidelines: Family Planning Update 2008 Part Two Seshu P. Sarma, MD, FAAP Emory University Regional Training Center Atlanta, Georgia Produced by the Alabama Department of Public Health
Faculty Pap Smear Guidelines: Family Planning Update 2008 Part Two Seshu P. Sarma, MD, FAAP Emory University Regional Training Center Atlanta, Georgia Produced by the Alabama Department of Public Health
Chapter 10: Pap Test Results
 Chapter 10: Pap Test Results On completion of this section, the learner will be able to: 1. Identify how Pap test results are interpreted and the reasons for normal and abnormal results. 2. Describe the
Chapter 10: Pap Test Results On completion of this section, the learner will be able to: 1. Identify how Pap test results are interpreted and the reasons for normal and abnormal results. 2. Describe the
Lessons From Cases of Screened Women Who Developed Cervical Carcinoma
 Lessons From Cases of Screened Women Who Developed Cervical Carcinoma R. Marshall Austin MD,PhD Magee-Womens Hospital of University of Pittsburgh Medical Center raustin@magee.edu Why Focus Study On Cases
Lessons From Cases of Screened Women Who Developed Cervical Carcinoma R. Marshall Austin MD,PhD Magee-Womens Hospital of University of Pittsburgh Medical Center raustin@magee.edu Why Focus Study On Cases
Cervical Cancer Screening. David Quinlan December 2013
 Cervical Cancer Screening David Quinlan December 2013 Cervix Cervical Cancer Screening Modest variation provincially WHO and UK begin at 25 stop at 60 Finland begin at 30 stop at 60 Rationale for
Cervical Cancer Screening David Quinlan December 2013 Cervix Cervical Cancer Screening Modest variation provincially WHO and UK begin at 25 stop at 60 Finland begin at 30 stop at 60 Rationale for
Hyperchromatic Crowded Groups: What is Your Diagnosis? Session 3000
 Hyperchromatic Crowded Groups: What is Your Diagnosis? Session 3000 Thomas A. Bonfiglio, M.D. Professor Emeritus, Pathology and Laboratory Medicine University of Rochester Disclosures In the past 12 months,
Hyperchromatic Crowded Groups: What is Your Diagnosis? Session 3000 Thomas A. Bonfiglio, M.D. Professor Emeritus, Pathology and Laboratory Medicine University of Rochester Disclosures In the past 12 months,
Objectives. Atypical Glandular Cells. Atypical Endocervical Cells. Reactive Endocervical Cells
 2013 California Society of Pathologists 66 th Annual Meeting San Francisco, CA Atypical Glandular Cells to Early Invasive Adenocarcinoma: Cervical Cytology and Histology Christina S. Kong, MD Associate
2013 California Society of Pathologists 66 th Annual Meeting San Francisco, CA Atypical Glandular Cells to Early Invasive Adenocarcinoma: Cervical Cytology and Histology Christina S. Kong, MD Associate
Prepared By Jocelyn Palao and Layla Faqih
 Prepared By Jocelyn Palao and Layla Faqih The structure of the suspected atypical cell should always be compared to the structure of other similar, benign, cells which are present in the smears. The diagnosis
Prepared By Jocelyn Palao and Layla Faqih The structure of the suspected atypical cell should always be compared to the structure of other similar, benign, cells which are present in the smears. The diagnosis
LGM International, Inc.
 Liqui-PREP TM Cytology Atlas Preface The following pictures are examples with descriptions of cytology slides processed with the Liqui-PREP TM System.. The descriptions are reviewed by Pathologists. It
Liqui-PREP TM Cytology Atlas Preface The following pictures are examples with descriptions of cytology slides processed with the Liqui-PREP TM System.. The descriptions are reviewed by Pathologists. It
PAP SMEAR by Dr.Shantha Krishnamurthy MD Senior Consultant Pathology Fortis Hospitals
 PAP SMEAR by Dr.Shantha Krishnamurthy MD Senior Consultant Pathology Fortis Hospitals Historical Named after George Papanicolaou, a Greek American Studied cervical epithelium in menstrual cycle of guinea
PAP SMEAR by Dr.Shantha Krishnamurthy MD Senior Consultant Pathology Fortis Hospitals Historical Named after George Papanicolaou, a Greek American Studied cervical epithelium in menstrual cycle of guinea
To further assess abnormalities detected on cervical cytological sample. To guide colposcopically directed biopsy
 1 To further assess abnormalities detected on cervical cytological sample To guide colposcopically directed biopsy To exclude invasive disease To aid in outpatient management and treatment of precancerous
1 To further assess abnormalities detected on cervical cytological sample To guide colposcopically directed biopsy To exclude invasive disease To aid in outpatient management and treatment of precancerous
CYTOMORPHOLOGY MODULE 28.1 INTRODUCTION OBJECTIVES 28.2 GENERAL GUIDELINES. Notes
 28 CYTOMORPHOLOGY 28.1 INTRODUCTION Light microscopic examination of stained cells in smears is the method of choice of diagnostic cytology. It allows classification of most normal cells as to type and
28 CYTOMORPHOLOGY 28.1 INTRODUCTION Light microscopic examination of stained cells in smears is the method of choice of diagnostic cytology. It allows classification of most normal cells as to type and
Cytyc Corporation - Case Presentation Archive - July 2002
 ThinPrep Pap Test History: 34 Year Old Female LMP: Day 20 Specimen Type: Cervical/Vaginal Case provided by Mark Tulecke, M.D. and Gabrielle Trawinski CT (ASCP), Mount Auburn Hospital, Cambridge, Massachusetts.
ThinPrep Pap Test History: 34 Year Old Female LMP: Day 20 Specimen Type: Cervical/Vaginal Case provided by Mark Tulecke, M.D. and Gabrielle Trawinski CT (ASCP), Mount Auburn Hospital, Cambridge, Massachusetts.
Making Sense of Cervical Cancer Screening
 Making Sense of Cervical Cancer Screening New Guidelines published November 2012 Tammie Koehler DO, FACOG The incidence of cervical cancer in the US has decreased more than 50% in the past 30 years because
Making Sense of Cervical Cancer Screening New Guidelines published November 2012 Tammie Koehler DO, FACOG The incidence of cervical cancer in the US has decreased more than 50% in the past 30 years because
Biomarkers for cervical cancer screening: the role of p16 INK4a to highlight transforming HPV infections
 Review For reprint orders, please contact reprints@expert-reviews.com Biomarkers for cervical cancer screening: the role of p16 INK4a to highlight transforming HPV infections Expert Rev. Proteomics 9(2),
Review For reprint orders, please contact reprints@expert-reviews.com Biomarkers for cervical cancer screening: the role of p16 INK4a to highlight transforming HPV infections Expert Rev. Proteomics 9(2),
BOSNIAN-TURKISH CYTOPATHOLOGY SCHOOL June 18-19, 2016 Sarajevo. Case Discussions. 60 year old woman Routine gynecologic control LBC
 BOSNIAN-TURKISH CYTOPATHOLOGY SCHOOL June 18-19, 2016 Sarajevo Case Discussions Prof Dr Sıtkı Tuzlalı Tuzlalı Pathology Laboratory 60 year old woman Routine gynecologic control LBC 1 2 Endometrial thickening
BOSNIAN-TURKISH CYTOPATHOLOGY SCHOOL June 18-19, 2016 Sarajevo Case Discussions Prof Dr Sıtkı Tuzlalı Tuzlalı Pathology Laboratory 60 year old woman Routine gynecologic control LBC 1 2 Endometrial thickening
Almost any suspected tumor can be aspirated easily and safely. Some masses are more risky to aspirate including:
 DOES THIS PATIENT HAVE CANCER? USING IN-HOUSE CYTOLOGY TO HELP YOU MAKE THIS DIAGNOSIS. Joyce Obradovich, DVM, Diplomate, ACVIM (Oncology) Animal Cancer & Imaging Center, Canton, Michigan Almost every
DOES THIS PATIENT HAVE CANCER? USING IN-HOUSE CYTOLOGY TO HELP YOU MAKE THIS DIAGNOSIS. Joyce Obradovich, DVM, Diplomate, ACVIM (Oncology) Animal Cancer & Imaging Center, Canton, Michigan Almost every
Cytology Report Format
 Squamous Precursor Lesions and Malignancies In Pap Test Dina R. Mody, MD, FCAP Director of Cytology The Methodist Hospital, Houston, TX Professor of Pathology and Laboratory Medicine Weill Medical College
Squamous Precursor Lesions and Malignancies In Pap Test Dina R. Mody, MD, FCAP Director of Cytology The Methodist Hospital, Houston, TX Professor of Pathology and Laboratory Medicine Weill Medical College
HPV Testing & Cervical Cancer Screening:
 HPV Testing & Cervical Cancer Screening: Are they linked? By William Chapman, MD, FRCPC Screening for precursor lesions of cervical cancer by the Papanicolaou (Pap) smear has been one of the greatest success
HPV Testing & Cervical Cancer Screening: Are they linked? By William Chapman, MD, FRCPC Screening for precursor lesions of cervical cancer by the Papanicolaou (Pap) smear has been one of the greatest success
It depends on the site: In Cervix 99%, in Anus ~ 85-90% and in Vulva, Penis ~ 40-50%. True.
 Are all high grade lesions caused by HPV, or are there other etiologies? The issue is not if you are infected with HPV high risk, but which of the patients infected with HR hpv would go into progressive
Are all high grade lesions caused by HPV, or are there other etiologies? The issue is not if you are infected with HPV high risk, but which of the patients infected with HR hpv would go into progressive
Cervical Cancer Prevention in the 21 st Century Changing Paradigms
 Cervical Cancer Prevention in the 21 st Century Changing Paradigms Teresa M. Darragh, MD UCSF Departments of Pathology and Obstetrics, Gynecology & Reproductive Sciences Faculty Disclosures: Teresa M.
Cervical Cancer Prevention in the 21 st Century Changing Paradigms Teresa M. Darragh, MD UCSF Departments of Pathology and Obstetrics, Gynecology & Reproductive Sciences Faculty Disclosures: Teresa M.
Understanding Your Pap Test Results
 Understanding Your Pap Test Results Most laboratories in the United States use a standard set of terms called the Bethesda System to report pap test results. Normal: Pap samples that have no cell abnormalities
Understanding Your Pap Test Results Most laboratories in the United States use a standard set of terms called the Bethesda System to report pap test results. Normal: Pap samples that have no cell abnormalities
p16 Cervical HISTOLOGY Histology Compendium & Staining Atlas
 p16 Cervical HISTOLOGY Histology Compendium & Staining Atlas Chapter 1: An Introduction to p16...... 3 Normal Cervical Epithelium and the Cell Cycle....4 HPV Infection and Cervical Disease......................................
p16 Cervical HISTOLOGY Histology Compendium & Staining Atlas Chapter 1: An Introduction to p16...... 3 Normal Cervical Epithelium and the Cell Cycle....4 HPV Infection and Cervical Disease......................................
Cervicovaginal Cytology: Normal and Abnormal Cells and Adequacy of Specimens
 Cervicovaginal Cytology: Normal and Abnormal Cells and Adequacy of Specimens 3 Christine Bergeron, MD, PhD Introduction Carcinoma of the cervix is a slow growing cancer, which is preceded by precancerous
Cervicovaginal Cytology: Normal and Abnormal Cells and Adequacy of Specimens 3 Christine Bergeron, MD, PhD Introduction Carcinoma of the cervix is a slow growing cancer, which is preceded by precancerous
Colposcopy. Attila L Major, MD, PhD
 Colposcopy Attila L Major, MD, PhD Histology Colposcopy Cytology It has been estimated that annual Pap smear testing reduces a woman s chance of dying of cervical cancer from 4 in 1000 to about 5 in 10,000
Colposcopy Attila L Major, MD, PhD Histology Colposcopy Cytology It has been estimated that annual Pap smear testing reduces a woman s chance of dying of cervical cancer from 4 in 1000 to about 5 in 10,000
Human Papillomavirus
 Human Papillomavirus Dawn Palaszewski, MD Assistant Professor of Obstetrics and Gynecology University of February 18, 2018 9:40 am Dawn Palaszewski, MD Assistant Professor Department of Obstetrics and
Human Papillomavirus Dawn Palaszewski, MD Assistant Professor of Obstetrics and Gynecology University of February 18, 2018 9:40 am Dawn Palaszewski, MD Assistant Professor Department of Obstetrics and
National Cervical Screening Program MBS Item Descriptors
 National Cervical Screening Program MBS Item Descriptors Item Item descriptor 73070 A test, including partial genotyping, for oncogenic human papillomavirus that may be associated with cervical pre-cancer
National Cervical Screening Program MBS Item Descriptors Item Item descriptor 73070 A test, including partial genotyping, for oncogenic human papillomavirus that may be associated with cervical pre-cancer
Course Title: Thin Prep PAP Smears. Number of Clock Hours: 3 Course Title #
 Course Title: Thin Prep PAP Smears Number of Clock Hours: 3 Course Title #5240303 Course Introduction There is a new laboratory test that is gaining popularity as a cancer screening tool for cervical cancer.
Course Title: Thin Prep PAP Smears Number of Clock Hours: 3 Course Title #5240303 Course Introduction There is a new laboratory test that is gaining popularity as a cancer screening tool for cervical cancer.
EU guidelines for reporting gynaecological cytology
 EU guidelines for reporting gynaecological cytology Amanda Herbert Guy s & St Thomas Foundation NHS Trust 5th EFCS Annual Tutorial, Trondheim, Norway 28 th May 1 st June 2012 EU guidelines aim to harmonize
EU guidelines for reporting gynaecological cytology Amanda Herbert Guy s & St Thomas Foundation NHS Trust 5th EFCS Annual Tutorial, Trondheim, Norway 28 th May 1 st June 2012 EU guidelines aim to harmonize
EDUCATIONAL COMMENTARY DIFFERENTIATING IMMATURE PERIPHERAL BLOOD CELLS
 Educational commentary is provided through our affiliation with the American Society for Clinical Pathology (ASCP). To obtain FREE CME/CMLE credits click on Continuing Education on the left side of the
Educational commentary is provided through our affiliation with the American Society for Clinical Pathology (ASCP). To obtain FREE CME/CMLE credits click on Continuing Education on the left side of the
Objectives. I have no financial interests in any product I will discuss today. Cervical Cancer Screening Guidelines: Updates and Controversies
 Cervical Cancer Screening Guidelines: Updates and Controversies I have no financial interests in any product I will discuss today. Jody Steinauer, MD, MAS University of California, San Francisco Objectives
Cervical Cancer Screening Guidelines: Updates and Controversies I have no financial interests in any product I will discuss today. Jody Steinauer, MD, MAS University of California, San Francisco Objectives
Key Words: SurePath. CINtec; p16; Ki-67, MIB1; sensitivity; specificity;
 Evaluation of CINtec PLUS 1 Testing as an Adjunctive Test in ASC-US Diagnosed Surepath 1 Preparations Neil Edgerton, M.D., Cynthia Cohen, M.D., andmomint. Siddiqui,M.D., F.I.A.C.* The CINtec PLUS 1 system
Evaluation of CINtec PLUS 1 Testing as an Adjunctive Test in ASC-US Diagnosed Surepath 1 Preparations Neil Edgerton, M.D., Cynthia Cohen, M.D., andmomint. Siddiqui,M.D., F.I.A.C.* The CINtec PLUS 1 system
Cervical Screening for Dysplasia and Cancer in Patients with HIV
 Cervical Screening for Dysplasia and Cancer in Patients with HIV Adult Clinical Guideline from the New York State Department of Health AIDS Institute w w w.hivg uidelines.org Purpose of the Guideline Increase
Cervical Screening for Dysplasia and Cancer in Patients with HIV Adult Clinical Guideline from the New York State Department of Health AIDS Institute w w w.hivg uidelines.org Purpose of the Guideline Increase
Molecular Triage: Partial and Extended Genotyping and More!
 Molecular Triage: Partial and Extended Genotyping and More! Thomas C. Wright, Jr. MD Professor Emeritus Columbia University, New York Pathologist, Enzo Clinical Laboratories, Farmingdale, NY Disclosures
Molecular Triage: Partial and Extended Genotyping and More! Thomas C. Wright, Jr. MD Professor Emeritus Columbia University, New York Pathologist, Enzo Clinical Laboratories, Farmingdale, NY Disclosures
The LAST Guidelines in Clinical Practice. Implementing Recommendations for p16 Use
 AJCP / Original Article The LAST Guidelines in Clinical Practice Implementing Recommendations for p16 Use Lani K. Clinton, MD, PhD, 1,2 Kyle Miyazaki, 1 Asia Ayabe, 1 James Davis, PhD, 2 Pamela Tauchi-Nishi,
AJCP / Original Article The LAST Guidelines in Clinical Practice Implementing Recommendations for p16 Use Lani K. Clinton, MD, PhD, 1,2 Kyle Miyazaki, 1 Asia Ayabe, 1 James Davis, PhD, 2 Pamela Tauchi-Nishi,
Detecting High-Grade Cervical Disease on ASC-H Cytology. Role of BD ProEx C and Digene Hybrid Capture II HPV DNA Testing
 Anatomic Pathology / BD ProEx C Use in ASC-H Cy t o l o g y Detecting High-Grade Cervical Disease on ASC-H Cytology Role of BD ProEx C and Digene Hybrid Capture II HPV DNA Testing Momin T. Siddiqui, MD,
Anatomic Pathology / BD ProEx C Use in ASC-H Cy t o l o g y Detecting High-Grade Cervical Disease on ASC-H Cytology Role of BD ProEx C and Digene Hybrid Capture II HPV DNA Testing Momin T. Siddiqui, MD,
GYN (Glandulars) Still Difficult After All These Years! Dina R Mody, MD Director of Cytology Laboratories and fellowship Program Methodist Hospital
 Still Difficult After All These Years! Dina R Mody, MD Director of Cytology Laboratories and fellowship Program Methodist Hospital") GYN (Glandulars) Still Difficult After All These Years! Dina R Mody, MD Director of Cytology Laboratories and fellowship Program Methodist Hospital and Bioreference Labs (Houston) Department of Pathology
GYN (Glandulars) Still Difficult After All These Years! Dina R Mody, MD Director of Cytology Laboratories and fellowship Program Methodist Hospital and Bioreference Labs (Houston) Department of Pathology
CINtec PLUS and the Pap smear: a co-testing alternative
 CINtec PLUS and the Pap smear: a co-testing alternative Rosemary Tambouret MD p16/ki67 (CINtec PLUS) and the Pap smear Rosemary Tambouret MD CINtec PLUS dual stain: p16 and Ki67 p16 is anti-proliferative
CINtec PLUS and the Pap smear: a co-testing alternative Rosemary Tambouret MD p16/ki67 (CINtec PLUS) and the Pap smear Rosemary Tambouret MD CINtec PLUS dual stain: p16 and Ki67 p16 is anti-proliferative
P16 INK4A EXPRESSION AS A POTENTIAL PROGNOSTIC MARKER IN CERVICAL PRECANCEROUS AND CANCEROUS LESIONS IN MOROCCO
 P16 INK4A EXPRESSION AS A POTENTIAL PROGNOSTIC MARKER IN CERVICAL PRECANCEROUS AND CANCEROUS LESIONS IN MOROCCO Yassine Zouheir Laboratory of histo-cytopathology of Institut Pasteur of Morocco, Casablanca,
P16 INK4A EXPRESSION AS A POTENTIAL PROGNOSTIC MARKER IN CERVICAL PRECANCEROUS AND CANCEROUS LESIONS IN MOROCCO Yassine Zouheir Laboratory of histo-cytopathology of Institut Pasteur of Morocco, Casablanca,
Transformation of Gynaecologic cytology: A Liquid Based Approach
 Transformation of Gynaecologic cytology: A Liquid Based Approach Dr KIRTI CHADHA MD(PATH),PDCC(ONCOPATH) CONSULTANT SURGICAL PATHOLOGIST METROPOLIS HEALTHCARE LTD MUMBAI Carcinoma Cervix Used to be the
Transformation of Gynaecologic cytology: A Liquid Based Approach Dr KIRTI CHADHA MD(PATH),PDCC(ONCOPATH) CONSULTANT SURGICAL PATHOLOGIST METROPOLIS HEALTHCARE LTD MUMBAI Carcinoma Cervix Used to be the
Colposcopic Principles. Simon Leeson Consultant Obstetrician/ Gynaecologist Betsi Cadwaladr University Health Board UK
 Colposcopic Principles Simon Leeson Consultant Obstetrician/ Gynaecologist Betsi Cadwaladr University Health Board UK The cervix topics discussed are: original squamous epithelium endocervical epithelium
Colposcopic Principles Simon Leeson Consultant Obstetrician/ Gynaecologist Betsi Cadwaladr University Health Board UK The cervix topics discussed are: original squamous epithelium endocervical epithelium
Done by khozama jehad. Neoplasia of the cervix
 Done by khozama jehad Neoplasia of the cervix An overview of cervical neoplasia very import. Most tumors of the cervix are of epithelial origin and are caused by oncogenic strains of human papillomavirus
Done by khozama jehad Neoplasia of the cervix An overview of cervical neoplasia very import. Most tumors of the cervix are of epithelial origin and are caused by oncogenic strains of human papillomavirus
Update on Thyroid FNA The Bethesda System. Shikha Bose M.D. Associate Professor Cedars Sinai Medical Center
 Update on Thyroid FNA The Bethesda System Shikha Bose M.D. Associate Professor Cedars Sinai Medical Center Thyroid Nodules Frequent occurrence Palpable: 4-7% of adults Ultrasound: 10-31% Majority benign
Update on Thyroid FNA The Bethesda System Shikha Bose M.D. Associate Professor Cedars Sinai Medical Center Thyroid Nodules Frequent occurrence Palpable: 4-7% of adults Ultrasound: 10-31% Majority benign
CERVIX. MLS Basic histological diagnosis MLS HIST 422 Semester 8- batch 7 L12 : Dr. Ali Eltayb.
 CERVIX MLS Basic histological diagnosis MLS HIST 422 Semester 8- batch 7 L12 : Dr. Ali Eltayb. CERVIX Most cervical lesions are: Most are Cervicitis. cancers ( common in women worldwide). CERVICITIS Extremely
CERVIX MLS Basic histological diagnosis MLS HIST 422 Semester 8- batch 7 L12 : Dr. Ali Eltayb. CERVIX Most cervical lesions are: Most are Cervicitis. cancers ( common in women worldwide). CERVICITIS Extremely
Management Algorithms for Abnormal Cervical Cytology and Colposcopy
 Management Algorithms for Abnormal Cervical Cytology and Colposcopy Table of Contents Standard Colposcopic Definitions... 1 Guidelines for the Assessment of Abnormal Cervical Cytology... 2 Ia: Persistent
Management Algorithms for Abnormal Cervical Cytology and Colposcopy Table of Contents Standard Colposcopic Definitions... 1 Guidelines for the Assessment of Abnormal Cervical Cytology... 2 Ia: Persistent
Welcome. THE ROLE OF oncofish cervical ASSESSMENT OF CERVICAL DYSPLASIA. March 26, 2013
 THE ROLE OF oncofish cervical IN THE ASSESSMENT OF CERVICAL DYSPLASIA The phone lines will open, 15 minutes prior to the start of the webinar. Toll Free: 1-800-867-0864. Entry Code: 83956484. You may download
THE ROLE OF oncofish cervical IN THE ASSESSMENT OF CERVICAL DYSPLASIA The phone lines will open, 15 minutes prior to the start of the webinar. Toll Free: 1-800-867-0864. Entry Code: 83956484. You may download
Focus. International #52. HPV infection in High-risk HPV and cervical cancer. HPV: Clinical aspects. Natural history of HPV infection
 HPV infection in 2014 Papillomaviruses (HPV) are non-cultivable viruses with circular DNA. They can establish productive infections in the skin (warts) and in mucous membranes (genitals, larynx, etc.).
HPV infection in 2014 Papillomaviruses (HPV) are non-cultivable viruses with circular DNA. They can establish productive infections in the skin (warts) and in mucous membranes (genitals, larynx, etc.).
ACGME Competency / Milestone Assessment. The Pap Test. Ricardo R. Lastra, MD Zubair W. Baloch, MD, PhD
 1 ACGME Competency / Milestone Assessment The Pap Test Ricardo R. Lastra, MD Zubair W. Baloch, MD, PhD Department of Pathology & Laboratory Medicine University of Pennsylvania, Perelman School of Medicine
1 ACGME Competency / Milestone Assessment The Pap Test Ricardo R. Lastra, MD Zubair W. Baloch, MD, PhD Department of Pathology & Laboratory Medicine University of Pennsylvania, Perelman School of Medicine
Salivary Gland Cytology: A Clinical Approach to Diagnosis and Management of Atypical and Suspicious Lesions
 Salivary Gland Cytology: A Clinical Approach to Diagnosis and Management of Atypical and Suspicious Lesions W.C. Faquin, M.D., Ph.D. Massachusetts General Hospital Harvard Medical School, USA Marc Pusztaszeri,
Salivary Gland Cytology: A Clinical Approach to Diagnosis and Management of Atypical and Suspicious Lesions W.C. Faquin, M.D., Ph.D. Massachusetts General Hospital Harvard Medical School, USA Marc Pusztaszeri,
EDUCATIONAL COMMENTARY DISTINGUISHING MORPHOLOGIC LOOK-ALIKES
 EDUCATIONAL COMMENTARY DISTINGUISHING MORPHOLOGIC LOOK-ALIKES Educational commentary is provided through our affiliation with the American Society for Clinical Pathology (ASCP). To obtain FREE CME/CMLE
EDUCATIONAL COMMENTARY DISTINGUISHING MORPHOLOGIC LOOK-ALIKES Educational commentary is provided through our affiliation with the American Society for Clinical Pathology (ASCP). To obtain FREE CME/CMLE
Beyond Pap Morphological Triage: p16/ki67 Dual Staining
 Moving away from Beyond Pap Morphological Triage: p16/ki67 Dual Staining Nicolas Wentzensen MD, PhD, MS Deputy Chief, Clinical Genetics Branch; Head, Clinical Epidemiology Unit National Cancer Institute
Moving away from Beyond Pap Morphological Triage: p16/ki67 Dual Staining Nicolas Wentzensen MD, PhD, MS Deputy Chief, Clinical Genetics Branch; Head, Clinical Epidemiology Unit National Cancer Institute
Estimated New Cancers Cases 2003
 Harvard-MIT Division of Health Sciences and Technology HST.071: Human Reproductive Biology Course Director: Professor Henry Klapholz Estimated New Cancers Cases 2003 Images removed due to copyright reasons.
Harvard-MIT Division of Health Sciences and Technology HST.071: Human Reproductive Biology Course Director: Professor Henry Klapholz Estimated New Cancers Cases 2003 Images removed due to copyright reasons.
Application of Chromogenic In Situ Hybridization (CISH) for Human Papillomavirus (HPV) Genotyping
 for Human Papillomavirus (HPV) Genotyping") Research Article imedpub Journals http://www.imedpub.com Archives in Cancer Research Vol. 4 No. 2:70 Application of Chromogenic In Situ Hybridization (CISH) for Human Papillomavirus (HPV) Genotyping Ekaterina
Research Article imedpub Journals http://www.imedpub.com Archives in Cancer Research Vol. 4 No. 2:70 Application of Chromogenic In Situ Hybridization (CISH) for Human Papillomavirus (HPV) Genotyping Ekaterina
Gynecologic Cytopathology: Glandular lesions
 Gynecologic Cytopathology: Glandular lesions Lin Wai Fung (MSc, MPH, CMIAC) 17/4/2014 Glandular lesions of the uterus Endocervix Endometrium Normal endocervical cells Sheets, strips well-preserved architecture:
Gynecologic Cytopathology: Glandular lesions Lin Wai Fung (MSc, MPH, CMIAC) 17/4/2014 Glandular lesions of the uterus Endocervix Endometrium Normal endocervical cells Sheets, strips well-preserved architecture:
Efficacy evaluation of a test CINtec p16ink4a in screening for cervical HPV infection
 Vol.1, No.3, 154-163 (2011) doi:10.4236/ojpm.2011.13020 Open Journal of Preventive Medicine Efficacy evaluation of a test CINtec p16ink4a in screening for cervical HPV infection Pafumi Carlo, Leanza Vito,
Vol.1, No.3, 154-163 (2011) doi:10.4236/ojpm.2011.13020 Open Journal of Preventive Medicine Efficacy evaluation of a test CINtec p16ink4a in screening for cervical HPV infection Pafumi Carlo, Leanza Vito,
HPV and Lower Genital Tract Disease. Simon Herrington University of Edinburgh, UK Royal Infirmary of Edinburgh, UK
 HPV and Lower Genital Tract Disease Simon Herrington University of Edinburgh, UK Royal Infirmary of Edinburgh, UK Conflict of interest/funding X None Company: Product royalties Paid consultant Research
HPV and Lower Genital Tract Disease Simon Herrington University of Edinburgh, UK Royal Infirmary of Edinburgh, UK Conflict of interest/funding X None Company: Product royalties Paid consultant Research
Instructions For Use
 MAN-02624-001 Rev. 004 page 1 of 15 Instructions For Use INTENDED USE The ThinPrep 2000 System is intended as a replacement for the conventional method of Pap smear preparation for use in screening for
MAN-02624-001 Rev. 004 page 1 of 15 Instructions For Use INTENDED USE The ThinPrep 2000 System is intended as a replacement for the conventional method of Pap smear preparation for use in screening for
What is a Pap smear?
 Pap smear What is a Pap smear? A Pap smear is a test that checks for changes in the cells of your cervix. The cervix is the lower part of the uterus that opens into the vagina. Developed over forty years
Pap smear What is a Pap smear? A Pap smear is a test that checks for changes in the cells of your cervix. The cervix is the lower part of the uterus that opens into the vagina. Developed over forty years
Cervical Precancer: Evaluation and Management
 TAJ June 2002; Volume 15 Number 1 ISSN 1019-8555 The Journal of Teachers Association RMC, Rajshahi Review fam Cervical Precancer: Evaluation and Management SM Khodeza Nahar Begum 1 Abstract Carcinoma of
TAJ June 2002; Volume 15 Number 1 ISSN 1019-8555 The Journal of Teachers Association RMC, Rajshahi Review fam Cervical Precancer: Evaluation and Management SM Khodeza Nahar Begum 1 Abstract Carcinoma of
Dako IT S ABOUT TIME. Interpretation Guide. Agilent Pathology Solutions. ALK, ROS1 and RET IQFISH probes (Dako Omnis) MET IQFISH probe (Dako Omnis)
 MET IQFISH probe (Dako Omnis)") INTERPRETATION Dako Agilent Pathology Solutions IQFISH Interpretation Guide ALK, ROS1 and RET IQFISH probes (Dako Omnis) MET IQFISH probe (Dako Omnis) IT S ABOUT TIME For In Vitro Diagnostic Use ALK, ROS1,
INTERPRETATION Dako Agilent Pathology Solutions IQFISH Interpretation Guide ALK, ROS1 and RET IQFISH probes (Dako Omnis) MET IQFISH probe (Dako Omnis) IT S ABOUT TIME For In Vitro Diagnostic Use ALK, ROS1,
EDUCATIONAL COMMENTARY MORPHOLOGIC ABNORMALITIES IN LEUKOCYTES
 EDUCATIONAL COMMENTARY MORPHOLOGIC ABNORMALITIES IN LEUKOCYTES Educational commentary is provided through our affiliation with the American Society for Clinical Pathology (ASCP). To obtain FREE CME/CMLE
EDUCATIONAL COMMENTARY MORPHOLOGIC ABNORMALITIES IN LEUKOCYTES Educational commentary is provided through our affiliation with the American Society for Clinical Pathology (ASCP). To obtain FREE CME/CMLE
!"#$%&'(#)*$+&,$-&.#,$/#0()1-$ ),1')$2(%&,2#,%$%(0'#$34567$
*$+&,$-&.#,$/#0()1-$ ),1')$2(%&,2#,%$%(0'#$34567$") !"#$%&'(#)*$+&,$-&.#,$/#0()1-$ ),1')$2(%&,2#,%$%(0'#$34567$ Updated Consensus Guidelines for Managing Abnormal Cervical Cancer Screening Tests and Cancer Precursors American Society for and Cervical Pathology
!"#$%&'(#)*$+&,$-&.#,$/#0()1-$ ),1')$2(%&,2#,%$%(0'#$34567$ Updated Consensus Guidelines for Managing Abnormal Cervical Cancer Screening Tests and Cancer Precursors American Society for and Cervical Pathology
Dysplasia: layer of the cervical CIN. Intraepithelial Neoplasia. p16 immunostaining. 1, Cervical. Higher-risk, requires CIN.
 CLINICAL PRACTICE GUIDELINE Guideline Number: DHMP_DHMC_PG1015 Guideline Subject: Routine Cervical Cancer Screening Effective Date: 9/2018 Revision Date: 9/2019 Pages: 2 of 2 Quality Management Committee
CLINICAL PRACTICE GUIDELINE Guideline Number: DHMP_DHMC_PG1015 Guideline Subject: Routine Cervical Cancer Screening Effective Date: 9/2018 Revision Date: 9/2019 Pages: 2 of 2 Quality Management Committee
CK17 and p16 expression patterns distinguish (atypical) immature squamous metaplasia from high-grade cervical intraepithelial neoplasia (CIN III)
 immature squamous metaplasia from high-grade cervical intraepithelial neoplasia (CIN III)") Histopathology 2007, 50, 629 635. DOI: 10.1111/j.1365-2559.2007.02652.x CK17 and p16 expression patterns distinguish (atypical) immature squamous metaplasia from high-grade cervical intraepithelial neoplasia
Histopathology 2007, 50, 629 635. DOI: 10.1111/j.1365-2559.2007.02652.x CK17 and p16 expression patterns distinguish (atypical) immature squamous metaplasia from high-grade cervical intraepithelial neoplasia
A Study on Diagnostic Accuracy of Cervical Pap Smear by Correlating with Histopathology in a Tertiary Care Centre
 Original Article DOI: 10.21276/APALM.1878 A Study on Diagnostic Accuracy of Cervical Pap Smear by Correlating with Histopathology in a Tertiary Care Centre Rachana L Y, S.S. Hiremath*, Prabhu M H, S.S
Original Article DOI: 10.21276/APALM.1878 A Study on Diagnostic Accuracy of Cervical Pap Smear by Correlating with Histopathology in a Tertiary Care Centre Rachana L Y, S.S. Hiremath*, Prabhu M H, S.S
Morphology I Slide: 1
 Morphology I Slide: 1 Morphology I Slide: 2 ThinPrep Morphology Normal Cytology Morphology I Slide: 3 CT & Pathologist Training Training program begins with ThinPrep morphology presentation Microscopic
Morphology I Slide: 1 Morphology I Slide: 2 ThinPrep Morphology Normal Cytology Morphology I Slide: 3 CT & Pathologist Training Training program begins with ThinPrep morphology presentation Microscopic
Cervical Cancer Screening
 Todd R. Jenkins, MD, MSHA Senior Vice Chair Director, Division of Women s Reproductive Healthcare Learning Objectives Describe the etiology, natural history, and usage of the human papillomavirus (HPV)
Todd R. Jenkins, MD, MSHA Senior Vice Chair Director, Division of Women s Reproductive Healthcare Learning Objectives Describe the etiology, natural history, and usage of the human papillomavirus (HPV)
PRESENTATION PLAN. Aim: Bethesda System 2001
 REACTIVE CELLULAR CHANGES AND INFECTIONS OF FEMALE GENITAL TRACT Aysun Uğuz, Prof, MD, FIAC Çukurova Üniv. Tıp Fak. Pathology Department-Cytology Division 18.Nisan.2015 Aim: The aim of the presentation
REACTIVE CELLULAR CHANGES AND INFECTIONS OF FEMALE GENITAL TRACT Aysun Uğuz, Prof, MD, FIAC Çukurova Üniv. Tıp Fak. Pathology Department-Cytology Division 18.Nisan.2015 Aim: The aim of the presentation
LARYNGEAL DYSPLASIA. Tomas Fernandez M; 3 rd year ENT resident, Son Espases University Hospital
 LARYNGEAL DYSPLASIA Tomas Fernandez M; 3 rd year ENT resident, Son Espases University Hospital INTRODUCTION Laryngeal cancer constitutes 1-2% of all malignancies diagnosed worldwide Survival is related
LARYNGEAL DYSPLASIA Tomas Fernandez M; 3 rd year ENT resident, Son Espases University Hospital INTRODUCTION Laryngeal cancer constitutes 1-2% of all malignancies diagnosed worldwide Survival is related
Disclosures Teresa M Darragh, MD
 Below the Belt: Screening for HPV-associated Cancers Teresa M. Darragh, MD UCSF Departments of Pathology and Obstetrics, Gynecology & Reproductive Sciences Disclosures Teresa M Darragh, MD Hologic: Research
Below the Belt: Screening for HPV-associated Cancers Teresa M. Darragh, MD UCSF Departments of Pathology and Obstetrics, Gynecology & Reproductive Sciences Disclosures Teresa M Darragh, MD Hologic: Research
HER2 CISH pharmdx TM Kit Interpretation Guide Breast Cancer
 P A T H O L O G Y HER2 CISH pharmdx TM Kit Interpretation Guide Breast Cancer FROM CERTAINTY COMES TRUST For in vitro diagnostic use HER2 CISH pharmdx Kit HER2 CISH pharmdx Kit is intended for dual-color
P A T H O L O G Y HER2 CISH pharmdx TM Kit Interpretation Guide Breast Cancer FROM CERTAINTY COMES TRUST For in vitro diagnostic use HER2 CISH pharmdx Kit HER2 CISH pharmdx Kit is intended for dual-color
I have no financial interests in any product I will discuss today.
 Cervical Cancer Screening Update and Implications for Annual Exams George F. Sawaya, MD Professor Department of Obstetrics, Gynecology and Reproductive Sciences Department of Epidemiology and Biostatistics
Cervical Cancer Screening Update and Implications for Annual Exams George F. Sawaya, MD Professor Department of Obstetrics, Gynecology and Reproductive Sciences Department of Epidemiology and Biostatistics
Utilization of the Biomarkers to Improve Cervical Cancer Screening
 Utilization of the Biomarkers to Improve Cervical Cancer Screening Elena BERNAD Victor Babes University of Medicine and Pharmacy Timisoara, Romania Cervical cancer is at the second most common cancer in
Utilization of the Biomarkers to Improve Cervical Cancer Screening Elena BERNAD Victor Babes University of Medicine and Pharmacy Timisoara, Romania Cervical cancer is at the second most common cancer in
Human Papillomavirus Genotyping and Cervical Smear in Duhok/Iraq
 Human Papillomavirus Genotyping and Cervical Smear in Duhok/Iraq Intisar Salim Pity (Professor pathology) MBChB, MSc, FIBMS Hanaa Mohammad Abdo (MSc microbiology) Amer A. Goreal (Microbiology) MBChB, FIBMS
Human Papillomavirus Genotyping and Cervical Smear in Duhok/Iraq Intisar Salim Pity (Professor pathology) MBChB, MSc, FIBMS Hanaa Mohammad Abdo (MSc microbiology) Amer A. Goreal (Microbiology) MBChB, FIBMS
Can LBC Completely Replace Conventional Pap Smear in Developing Countries
 The Journal of Obstetrics and Gynecology of India (January February 2019) 69(1):69 76 https://doi.org/10.1007/s13224-018-1-7 ORIGINAL ARTICLE Can LBC Completely Replace Conventional Pap Smear in Developing
The Journal of Obstetrics and Gynecology of India (January February 2019) 69(1):69 76 https://doi.org/10.1007/s13224-018-1-7 ORIGINAL ARTICLE Can LBC Completely Replace Conventional Pap Smear in Developing
Human Papillomavirus. Kathryn Thiessen, ARNP, ACRN The Kansas AIDS Education and Training Center The University of Kansas School of Medicine Wichita
 Human Papillomavirus Kathryn Thiessen, ARNP, ACRN The Kansas AIDS Education and Training Center The University of Kansas School of Medicine Wichita What is Genital HPV Infection Human papillomavirus is
Human Papillomavirus Kathryn Thiessen, ARNP, ACRN The Kansas AIDS Education and Training Center The University of Kansas School of Medicine Wichita What is Genital HPV Infection Human papillomavirus is
number Done by Corrected by Doctor Maha Shomaf
 number 16 Done by Waseem Abo-Obeida Corrected by Zeina Assaf Doctor Maha Shomaf MALIGNANT NEOPLASMS The four fundamental features by which benign and malignant tumors can be distinguished are: 1- differentiation
number 16 Done by Waseem Abo-Obeida Corrected by Zeina Assaf Doctor Maha Shomaf MALIGNANT NEOPLASMS The four fundamental features by which benign and malignant tumors can be distinguished are: 1- differentiation
SAMPLE LITERATURE Please refer to included weblink for correct version. Morphology of Cancer Cells. Edvo-Kit #990. Experiment Objective:
 Edvo-Kit #990 Morphology of Cancer Cells Experiment Objective: 990 In this lab, students will explore the morphology of normal and cancerous cells by staining pre-fi xed cells with methylene blue and eosin.
Edvo-Kit #990 Morphology of Cancer Cells Experiment Objective: 990 In this lab, students will explore the morphology of normal and cancerous cells by staining pre-fi xed cells with methylene blue and eosin.
Screening for the Precursors of Cervical Cancer in the Era of HPV Vaccination. Dr Stella Heley Senior Liaison Physician Victorian Cytology Service
 Screening for the Precursors of Cervical Cancer in the Era of HPV Vaccination Dr Stella Heley Senior Liaison Physician Victorian Cytology Service Victorian Cytology Service Dr Stella Heley Dr Siobhan Bourke
Screening for the Precursors of Cervical Cancer in the Era of HPV Vaccination Dr Stella Heley Senior Liaison Physician Victorian Cytology Service Victorian Cytology Service Dr Stella Heley Dr Siobhan Bourke
The Biology of HPV Infection and Cervical Cancer
 The Biology of HPV Infection and Cervical Cancer Kaitlin Sundling, M.D., Ph.D. Clinical Instructor Faculty Director, Cytotechnology Program Wisconsin State Laboratory of Hygiene and University of Wisconsin
The Biology of HPV Infection and Cervical Cancer Kaitlin Sundling, M.D., Ph.D. Clinical Instructor Faculty Director, Cytotechnology Program Wisconsin State Laboratory of Hygiene and University of Wisconsin
The society for lower genital tract disorders since 1964.
 The society for lower genital tract disorders since 1964. Updated Consensus Guidelines for Managing Abnormal Cervical Cancer Screening Tests and Cancer Precursors American Society for and Cervical Pathology
The society for lower genital tract disorders since 1964. Updated Consensus Guidelines for Managing Abnormal Cervical Cancer Screening Tests and Cancer Precursors American Society for and Cervical Pathology
Evaluation of Low-Grade Squamous Intraepithelial Lesions, Cannot Exclude High-Grade Squamous Intraepithelial Lesions on Cervical Smear
 The Korean Journal of Pathology 2010; 44: 528-35 DOI: 10.4132/KoreanJPathol.2010.44.5.528 Evaluation of Low-Grade Squamous Intraepithelial Lesions, Cannot Exclude High-Grade Squamous Intraepithelial Lesions
The Korean Journal of Pathology 2010; 44: 528-35 DOI: 10.4132/KoreanJPathol.2010.44.5.528 Evaluation of Low-Grade Squamous Intraepithelial Lesions, Cannot Exclude High-Grade Squamous Intraepithelial Lesions