Commonwealth of Kentucky Department for Medicaid Services Division of Program Quality and Outcomes
|
|
|
- Harold Terry
- 5 years ago
- Views:
Transcription



1 Cmmnwealth f Kentucky Department fr Medicaid Services Divisin f Prgram Quality and Outcmes EPSDT Screening Encunter Data Validatin Clinical Fcused Study 2014 FINAL REPORT May 2014
2 TABLE OF CONTENTS INTRODUCTION... 3 OBJECTIVES... 4 METHODOLOGY... 4 DATA ANALYSIS... 7 RESULTS... 8 COHORT I Member Characteristics (Table I.1) Preventive Medicine Services Validatin Develpmental Screening Cde (CPT 96110) Validatin Visin Screening Cde Validatin Hearing Screening Cde Validatin Chrt I Grup Cmparisn COHORT II Member Characteristics Develpmental Assessment Chrt II Grup Cmparisn DISCUSSION COHORT I COHORT II LIMITATIONS CONCLUSION RECOMMENDATIONS REFERENCES APPENDICES APPENDIX A: COHORT I BY AGE GROUP APPENDIX B: COHORT I BY MCO APPENDIX C: COHORT I BY GENDER APPENDIX D: COHORT I BY EMR APPENDIX E: COHORT I BY LOCATION TYPE APPENDIX F: COHORT II BY AGE GROUP APPENDIX G: COHORT II BY MCO APPENDIX H: COHORT II BY GENDER APPENDIX I: COHORT II BY EMR... 86
3 Intrductin Early and Peridic Screening, Diagnstic and Treatment (EPSDT) services is a federally mandated health prgram, which prvides cmprehensive and preventive health care services fr children and adlescents up t age 21. EPSDT services include a cmplete physical examinatin, a cmprehensive health and develpmental histry, apprpriate immunizatins accrding t the Advisry Cmmittee n Immunizatin Practices, labratry testing, including lead txicity screening, and health educatin that includes anticipatry guidance regarding child develpment, healthy lifestyles and accident and injury preventin. 1 Age-apprpriate mental health and substance use screening are als part f EPSDT services. The Centers fr Medicare and Medicaid Services (CMS) has recently released an infrmatinal bulletin nting that althugh half f mental health cnditins and substance use disrders begin by age 14, many yung peple d nt have their cnditins identified and d nt receive the mental health services they need. 2 While a brad range f services are cvered under EPSDT, natinal studies have shwn that nt all eligible children receive all cmpnents f needed services. 3, 4 In 2010, the Department f Health and Human Services Office f the Inspectr General evaluated nine states and fund that 60% f children with dcumented EPSDT screenings had incmplete screenings. 5 The study shwed that 76% f children did nt receive required medical, visin, r hearing screenings. Accurate assessments f the extent t which Medicaid children receive all required EPSDT services are especially challenging fr children enrlled in managed care, since capitatin arrangements may lead t underreprting f individual services prvided. 6 Difficulty linking data frm varius surces, as well as gaps in Medicaid enrllment, present additinal barriers t ascertaining which services a particular child has received. Fster care can als present barriers t receipt f age-apprpriate preventive services. 7 The imprtance f early identificatin and management f develpmental disrders and preventin and management f chrnic disease is heightened by evlving epidemilgic trends and evidence fr the benefits f early interventin. 8 Medicaid s EPSDT services are particularly imprtant because children with public insurance are mre likely t have special health care needs, including chrnic cnditins and develpmental delays, fr which EPSDT prvides access t specialized health services. 7 The Centers fr Disease Cntrl and Preventin (CDC) reprts develpmental disabilities in the United States are increasing. Natinal Health Interview Survey (NHIS) data revealed that 1 in 6 children in the U.S. had an identified develpmental disability in , and that children insured by Medicaid had a nearly tw-fld higher prevalence f any develpmental disability cmpared t thse with private insurance. 9 The American Academy f Pediatrics (AAP) recmmends develpmental surveillance at every well-child visit (WCV), with administratin f standardized develpmental screening tests at age 9 mnths, 18 mnths and 30 mnths. This screening is intended t enhance the develpmental surveillance prcess, since clinical impressin has been shwn t be less accurate than frmal screening in estimating a child s develpmental status. 10 Develpmental Screening in the First Three Years f Life is a measure in the Children s Health Insurance Prgram Reauthrizatin Act (CHIPRA) cre measure set that examines the percentage f children screened fr risk f develpmental, behaviral, and scial delays using a standardized screening tl in the 12 mnths preceding their first, secnd, r third birthday. 11 Althugh this screening can be represented by CPT cde 96110, the cde has been shwn t have questinable validity. Therefre, the measure steward recmmends that states cnduct a validity assessment f claims data as cmpared t medical chart review, in rder t verify that the use f the CPT cde 96110: Develpmental Testing, limited, reflects develpmental screening using a standardized screening tl. Page 3 f 87
4 Objectives The study aims t cmpare administrative data and medical recrd dcumentatin t validate encunter data cdes relevant t the receipt f EPSDT screening f children enrlled in Kentucky Medicaid Managed Care. Study questins: 1. D encunter data cdes used t indicate EPSDT (well-child) screening visits reflect WCVs that include cmprehensive health and develpmental histry (including mental health and substance use screening), cmprehensive physical exam, and health educatin/anticipatry guidance? 2. Is mental health screening and fllw-up f identified prblems included in EPSDT visits? 3. Des submissin f a CPT cde reflect develpmental screening using a standardized develpmental screening tl? 4. Des submissin f hearing and visin screening cdes reflect age-apprpriate hearing and visin screening? Methdlgy Review Perid The validatin study cnsisted f a review f WCVs that ccurred between January 1, 2013 thrugh April 30, 2013, which was the earliest timeframe identified that included data frm all fur plans and allwed a three mnth time perid fr claims t run ut t ensure all applicable claims were cnsidered in the study. The data was btained frm the fllwing MCOs: CventryCares f Kentucky (CventryCares) Humana CareSurce (Humana) Humana initiated its Kentucky Medicaid cntract in January Passprt Health Plan (Passprt) WellCare f Kentucky (WellCare) Eligible Ppulatin and Scpe f Review The eligible ppulatin frm which a sample was drawn cnsisted f Medicaid Managed Care (MMC)-enrlled children wh had a WCV cde between January 1, 2013 and April 30, Tw chrts f children were selected frm the eligible ppulatin: Chrt I: A stratified (divided int grups befre sampling) randm sample f 110 eligible children at least 1 year f age thrugh 20 years by April 30, 2013 fr each f the 4 MCOs, as available, fr whm an administrative claim fr WCV was submitted. This chrt was used t evaluate the cntents f WCVs relative t recmmended EPSDT services. Chrt II: A stratified randm sample f 100 eligible children, at least 1 year f age thrugh 3 years by April 30, 2013 fr each f the 4 MCOs fr whm an administrative claim fr Develpmental Screening (CPT cde 96110) was submitted. This chrt was used t evaluate the accuracy f the administrative develpmental screening cde, i.e., whether medical recrd dcumentatin cnfirms that the screening was cnducted as the claim wuld indicate. Member age was determined by the age calculated at the date f the reviewed visit. Page 4 f 87
5 Study Indicatrs In rder t rganize the data fr meaningful analysis, study indicatrs were categrized int 4 areas addressing varius aspects f WCVs and early childhd develpmental screening: 1. EPSDT-screening well visit: The prprtin f children in the study sample that had the fllwing assessed during the well-care visit assciated with the EPSDT cde(s) Well-Child Cmpsite Cmpnents (Patient Histry, Anticipatry Guidance, Physical Exam and Develpmental Assessment) Health histry Develpmental surveillance Mental health assessment (age-apprpriate, including depressin screening fr adlescents) Risk behavir assessment fr adlescents, including substance use Cmprehensive physical exam Height/weight/BMI percentile Health educatin/anticipatry guidance 2. Develpmental screening The prprtin f children with cde that had frmal develpmental screening The prprtin f children withut cde that had frmal develpmental screening The prprtin f children with cde that had develpmental surveillance The prprtin f children withut cde that had develpmental surveillance 3. Visin screening The prprtin f children with a visin screening cde that had age-apprpriate visin screening The prprtin f children withut a visin screening cde that had visin screening The prprtin f children with a visin screening cde that did nt have age-apprpriate visin screening 4. Hearing screening The prprtin f children with a hearing screening cde that had age-apprpriate hearing screening The prprtin f children withut a hearing screening cde that had age-apprpriate hearing screening The prprtin f children with a hearing screening cde that did nt have age-apprpriate hearing screening The fllwing defines the categries and specific cmpnents that were abstracted frm the medical recrds: 1. Demgraphic infrmatin (cllected frm medical recrd and, if unavailable, pre-ppulated frm administrative data) 2. Cdes assciated with WCVs (pre-ppulated frm administrative data) and specific services: 12 Preventive medicine services ( ; ; V20, V70) Develpmental screening (96110) Hearing screening (92551, 92552, 92567) Visin screening (99173, 99174) Substance abuse screening and brief interventin ( ) Substance abuse cunseling (V65.42) 3. Age-apprpriate cmprehensive health histry: Past Medical Histry, Family Histry, Scial Histry, Review f Systems Develpmental Surveillance (milestnes/general surveillance, parental cncerns) Mental Health Assessment Infrmal query/ Frmal tl Depressin screening fr adlescents Substance abuse screen fr adlescents Dcumented fllw-up f identified prblems Page 5 f 87
6 Cunseling Medicatin Further testing Referral 4. Age and gender-apprpriate cmprehensive physical exam: Height/weight/BMI Bld Pressure HEENT/Pulmnary/Cardivascular/Abdmen/Extremities/Neurlgic/Geniturinary 5. Cunseling/anticipatry guidance/risk reductin: Nutritin/physical activity/safety-injury preventin/schl readiness/risk reductin Adlescent risk behavirs 6. Develpmental screening with a standardized tl: Ages and Stages Questinnaire (ASQ) - 4mnths t 60 mnths Ages and Stages Questinnaire -3rd Editin (ASQ-3) 1 mnth t 66 mnths Battelle Develpmental Inventry Screening Tl (BDI-ST) Birth t 95 mnths Bayley Infant Neur-develpmental Screen (BINS) - 3 mnths t 24 mnths Brigance Screens-II Birth t 90 mnths Child Develpment Inventry (CDI) 18 mnths t 6 years Infant Develpment Inventry Birth t 18 mnths Mdified Checklist fr Autism in Tddlers (M-CHAT) 16 mnths t 48 mnths Parents Evaluatin f Develpmental Status (PEDS) Birth t 8 years Parents Evaluatin f Develpmental Status - Develpmental Milestnes (PEDS-DM) Birth t 8 years, with additinal measures fr lder children and adlescents Other Validated Develpmental Screening Tl 7. Age-apprpriate visin screening: Visual acuity Ocular alignment 8. Age-apprpriate hearing screening: Screening Audimetry Tympanmetry Page 6 f 87
7 Data Analysis The main gals f the analysis differ by chrt: the bjective fr the first chrt is t determine the validity f the WCV cde; and fr the secnd chrt, the bjective is t determine the validity f the develpmental screen cde frm the administrative data. Fr bth chrts, the analyses aim t determine whether the use f either the WCV cde r the develpmental screen cde reflects apprpriate screenings and evaluatins. The develpmental screening cde is als evaluated with respect t the use f glbal develpmental screening tls that meet specificatins as delineated in CHIPRA cre measure specificatins. 13 In additin, the analysis includes a validatin f claims fr hearing and visin screening. Abstractin included evaluatin f age-apprpriate hearing and visin screening, bth as part f the WCV and as validatin f claims cdes submitted. All data abstracted frm the administrative data and the medical recrds are included in the reprt via frequency tables. Results are presented by age grup (1-4 Years vs Years vs Years). Additinal frequencies were analyzed fr the fllwing grups: 1) Gender (Males vs. Females) 2) MCO (CventryCares vs. Humana vs. Passprt vs. WellCare) 3) Lcatin Type (Urban vs. Rural) a. Each recrd was determined Urban r Rural accrding t the cunty cde assciated with the member s residence, as extracted frm the claims data. The Urban grup is cmprised f the 36 urban cunties in Kentucky, as determined by the DMS-apprved Cunty/Regin Crsswalk. 4) Electrnic Medical Recrd (Yes vs. N) Due t pr dcumentatin within the medical recrds, frequencies fr race categries were calculated frm administrative data. In additin, small numbers in certain race and ethnicity categries prevented further cmparative analysis. Tls used fr analysis include Micrsft Office Excel and SAS 9.3. Methdlgical Cnsideratins T test fr any differences in prprtins, chi-square tests were emplyed fr all cmparative analyses incrprating dichtmus (e.g., yes/n) variables and a was generated fr each test. P-values less than 0.05 were cnsidered statistically significant, meaning that the bserved utcme has less than a 0.05 prbability f ccurring randmly. Any differences fund t be significant are highlighted in bld fnt. Any tests which prduced a greater than r equal t 0.05 are cnsidered nt significant and indicated by n.s. in the frequency tables. T test the difference in prprtins between three r mre grups, i.e., age grup, lgistic regressin was utilized t determine the directin f the inequality. Due t small sample sizes, sme items, althugh f clinical interest, were nt analyzed fr statistical significance. T maximize the number f cmparisns fr which significance testing culd be perfrmed, the fllwing criteria were applied t chi-square tests: 1) The denminatr fr each grup cmparisn must be greater than 20. 2) The cunt f each cell in the frequency table is greater than r equal t 1. Where the criteria, abve, were nt met and significance testing was nt perfrmed, there appears an n/a in place f a p- value. Regardless f significance testing, all data are presented descriptively. Presentatin f Results The resulting frequencies are listed in the tables belw. Tables are presented separately fr each grup cmparisn. In additin t the numeratr, denminatr, grup rate and ttal rate, each table als cntains the utcme f the significance test, if perfrmed. Fr each grup cmparisn in Chrt I, fur tables are presented: Preventive Medicine Services Page 7 f 87
8 Validatin, Develpmental Screen Cde Validatin, Visin Screen Cde Validatin and Hearing Screen Cde Validatin. Fr each grup cmparisn in Chrt II, ne table is presented, Develpmental Screen Validatin. Select tables are presented within the reprt accmpanied by descriptins f any key findings; cmprehensive results, including frequencies fr all abstracted elements, can be fund in Appendices A - I. Fr any frequency with a denminatr equal t zer, the numeratr and rate cells have been shaded in grey. As the Preventive Medicine Services Validatin table cntains all items fr which data was abstracted, a cmpsite measure was designed t determine hw the use f the WCV cde reflects the basic cmpnents f a WCV. Fr the Well-Child Cmpsite rates shwn in the tables belw, rates were calculated based n multiple elements f the abstractin. The measure is cmprised f 4 majr cmpnents: Patient Histry all elements f the patient histry dcumented Develpmental Assessment a frmal develpmental screen r develpmental surveillance with milestnes and parental cncerns addressed Physical Exam all elements f the physical exam perfrmed and dcumented Anticipatry Guidance at least 1 age-apprpriate element dcumented Results Dispsitin f Recrds Medical recrd sample sizes, retrieval infrmatin, any nted exclusins, and the final study sample are presented in Tables 1 and 2. Exclusins nted include thse members fr whm the recrd culd nt be lcated r retrieved, the recrd was missing pages, the recrd was illegible, r the date f service fell utside the study perid, based n a review f the submitted charts. All available Humana charts were included. Table 1: Overall Dispsitin f Recrds - Chrt I Ttal Charts Requested Charts Received Retrieval Rate 1 Charts Excluded frm Study 2 Final Study Sample 3 n % f Ttal Study Sample CventryCares % % Humana % % Passprt % % WellCare % % TOTAL % % 1 Retrieval Rate = Charts Received / Ttal Charts Requested 2 Reasns fr exclusin include: recrd culd nt be lcated, recrd was missing pages, recrd was illegible, date f service falls utside f study perid, and prenatal services prvided during visit. 3 The remaining analyses fr this study will be based n these members, unless therwise nted. Nte: Althugh the ttal sample size fr the study is 308 recrds, all rates ther than the member characteristics are based n a sample size f 307 recrds. One submitted recrd did nt include dcumentatin fr the date f service assciated with the claims cdes that determined the member s eligibility in the study. This member was included in the verall sample, as the purpse f this study is t validate the infrmatin gathered frm the claims data with the infrmatin fund in the medical recrd; hwever, infrmatin frm this chart culd nt be used t validate a claim fr a separate date. Page 8 f 87
9 Table 2: Overall Dispsitin f Recrds - Chrt II Ttal Charts Requested Charts Received Retrieval Rate 1 Charts Excluded frm Study 2 Final Study Sample 3 n % f Ttal Study Sample CventryCares % % Humana 1 0 0% 0 0 0% Passprt % % WellCare % % TOTAL % % 1 Retrieval Rate = Charts Received / Ttal Charts Requested 2 Reasns fr exclusin include: recrd culd nt be lcated, recrd was missing pages, recrd was illegible, date f service falls utside f study perid, and prenatal services prvided during visit. 3 The remaining analyses fr this study will be based n these members, unless therwise nted. Page 9 f 87
10 Chrt I Member Characteristics (Table I.1) When separated by plan membership, a slightly higher percentage f recrds were assciated with members f Passprt (34%). As analyzed by age grup, mst f thse members in the age grup 1-4 years (36%) were members f CventryCares. The mst f members in the age grup 5-11 years (43%) and years (42%) were members f Passprt. Upn review f the medical recrds, 234 ut f 308 recrds did nt identify the race f the member (data nt shwn) and claims data were used instead t evaluate member race. The majrity f the study ppulatin was identified as White/Caucasian (71%) frm the claims data. Black/African American cmprised 21% f the study sample, Other race, which cmbined the values fr American Indian and Alaska Native, Asian, Hawaiian r Other Pacific Islander, Multiple Races, and Other Race, cmprised 3%, while 5% f race was unreprted in the administrative data. Administrative data were nt available fr ethnicity, and medical recrd abstractin revealed that 94% f the recrds did nt include dcumentatin f ethnicity, while 3% f members were identified as Hispanic. The primary language spken by parents r guardians was unable t be determined frm 88% f the submitted medical recrds. English was the primary language as dcumented in 11% f the recrds, while Spanish was nt dcumented as the primary language in any f the recrds. Interpreter services were prvided fr 1 member in the study ppulatin. Fr 90% f recrds fr which language was unknwn r nt specifically identified as English, there was n dcumentatin indicating whether an interpreter was prvided. The study ppulatin included 47% female members and 53% male members. Sixty-eight percent f members resided in urban cunties and 32% resided in rural cunties. A majrity (67%) f prviders used an electrnic medical recrd (EMR) fr dcumentatin. Table I.1: Member Characteristics MEDICAL RECORD REVIEW/ ADMINISTRATIVE DATA: Member Characteristics Plan Chrt I by Member Age Grup 1 Grup 2 Grup Years 5-11 Years Years N = 150 N = 77 N = 81 TOTAL N = 308 n % n % n % n % CventryCares f Kentucky 54 36% 23 30% % 96 31% Humana CareSurce 6 4 % 4 5% 3 4% 13 4% Passprt Health Plan 37 25% 33 43% 34 42% % WellCare f Kentucky 53 35% % 25 31% 95 31% Race White % 57 74% 52 64% % Black 29 19% 14 18% % 64 21% Other 1 4 3% 2 3% 4 5% 10 3% Unreprted % 4 5% 4 5% 14 5% Ethnicity Hispanic 4 3% 1 1% 3 4% 8 3% Nn-Hispanic 7 5% 1 1% 1 1% 9 3% Unreprted % 75 97% 77 95% % Gender Page 10 f 87
11 MEDICAL RECORD REVIEW/ ADMINISTRATIVE DATA: Member Characteristics Chrt I by Member Age Grup 1 Grup 2 Grup Years 5-11 Years Years N = 150 N = 77 N = 81 TOTAL N = 308 n % n % n % n % Female 74 49% 34 44% 38 47% % Male 76 51% 43 56% 43 53% % Primary language spken by the parent r guardian dcumented English 20 13% 8 10% 5 6% 33 11% Spanish 0 0% 0 0% 0 0% 0 0% Other 1 1% 1 1% 3 4% 5 2% UTD (N dcumentatin n language) % 68 88% 73 90% % Interpreter services prvided fr the parent r guardian that accmpanied the child t the visit dcumented Yes 0 0% 0 0% 1 1% 1 0% N 8 5% 3 4% 3 4% 14 5% UTD % 69 90% 75 93% % NA % 5 6% 2 2% 17 6% Lcatin Type Rural 53 35% 20 26% 26 32% 99 32% Urban 97 65% 57 74% 55 68% % Medical recrd dcumentatin was EMR Yes % 49 64% 53 65% % N 45 30% 28 36% 28 35% % 1 Other includes values fr the fllwing races: American Indian and Alaska Native, Asian, Hawaiian r Other Pacific Islander, Multiple Races, and Other Race. 2 Unreprted was selected when the member s race was nt dcumented in administrative data. 3 UTD: English is NOT the primary language AND there is n dcumentatin indicating whether an interpreter was prvided. 4 NA: The primary language is English r it is dcumented that an interpreter is nt needed. Page 11 f 87
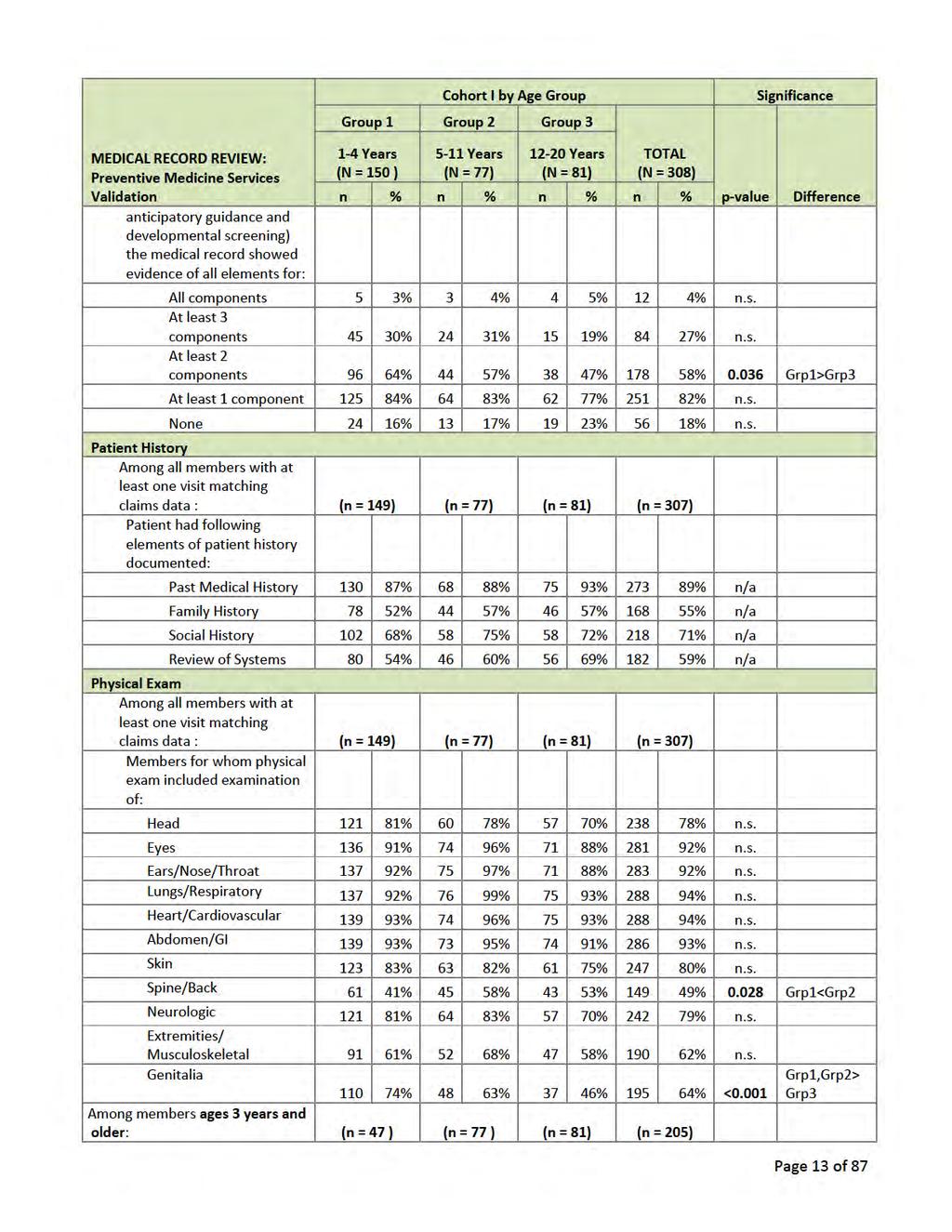
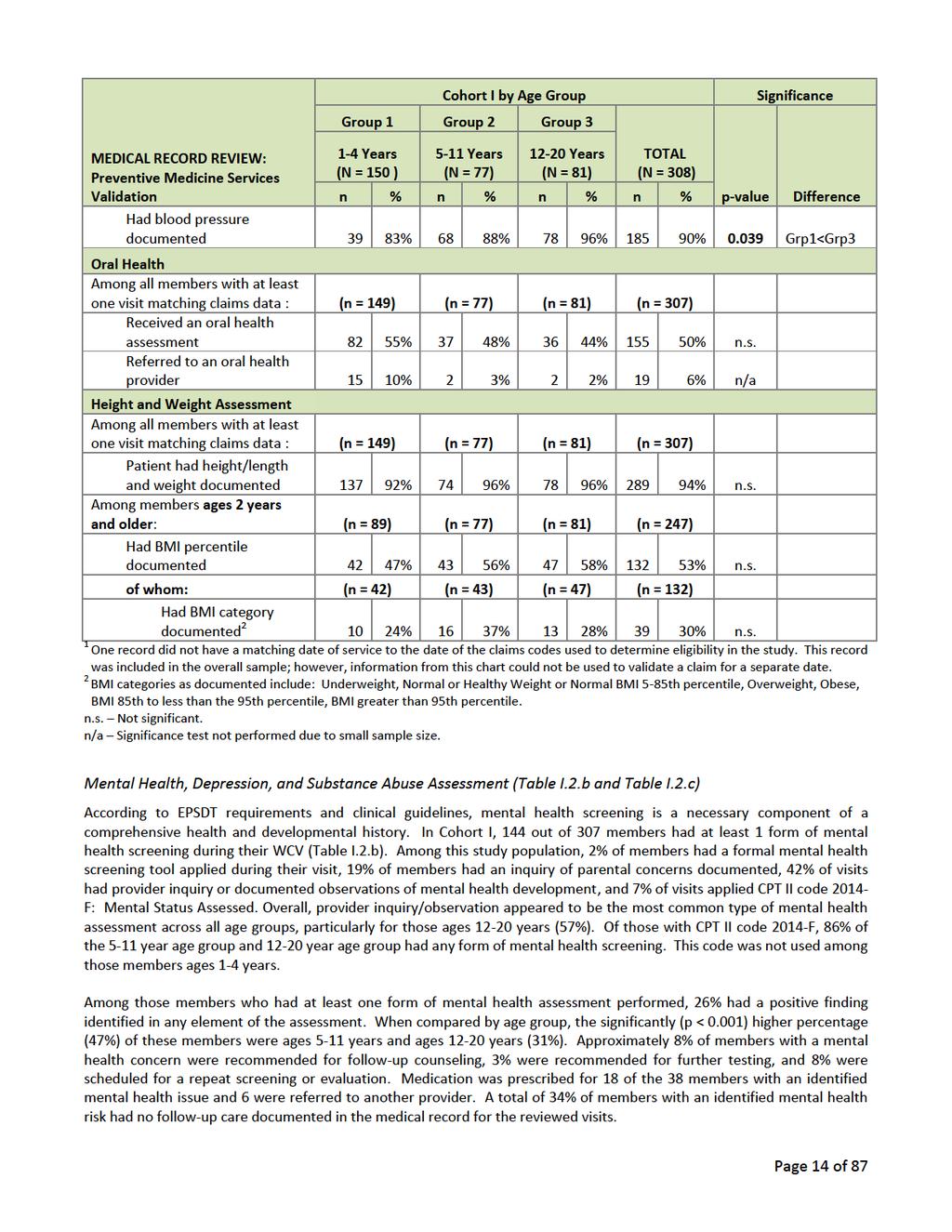
12 Preventive Medicine Services Validatin In rder t determine if WCV-related encunter cdes reflect a cmprehensive WCV cnsistent with EPSDT services, dcumentatin fr varius elements f each visit were reviewed. These elements include EPSDT screening cmpnents such as histry, physical exam, anticipatry guidance, develpmental assessment, hearing/visin screening, and ral health assessment. Frequencies fr each f these EPSDT items are described in the fllwing sectins. Cmpsite Well-Child Visit (Table I.2a-g) *One visit was remved frm the denminatr because the date f service was different than the claim date. A cmpsite variable fr a WCV was created using HEDIS specificatins fr evidence f a WCV. 13 Fr the purpses f this study, a basic WCV is ne that encmpasses the fllwing cmpnents: a cmprehensive health and develpmental histry, cmprehensive physical exam, and anticipatry guidance. Abut 27% f visits had all elements f at least 3 WCV cmpnents dcumented while 82% had all elements f at least 1 WCV cmpnent. On cmparisn f age grups, a significant majrity (p = 0.036) f visits cvered at least 2 cmpnents f a cmpsite WCV fr ages 1-4 years (64%) as ppsed t thse years f age (47%). Fr the years age grup, 89% f visits were identified as WCV cmpared t the yunger ages at 93% (1-4 years) and 92% (5-11 years). Upn review f the varius cmpnents included in a basic WCV, past medical histry was assessed in 89% f visits. Family histry was btained in 55% f visits. A scial histry was dcumented fr 71% f visits, while a review f systems ccurred in 59% f visits. As part f a cmprehensive physical exam, 94% f members had a height and weight dcumented. Of thse 53% f members lder than 2 years f age wh had a BMI percentile dcumented, 30% had their BMI categrized by the prvider as nrmal, underweight, verweight, bese r greater than the 95 th percentile. Bld pressure was measured in 90% f children ages 3 years and lder. Bld pressure was dcumented fr adlescents (96%) significantly mre ften (p = 0.039) than fr the yungest age grup (83%). Mst f the ther elements f a cmprehensive physical exam were perfrmed fr all members. The exceptins include examinatin f the head (78%), skin (80%), spine/back (49%), neurlgic system (79%), extremities/musculskeletal system (62%), and genitalia (64%). Examinatin f the spine/back ccurred statistically mre frequently (p = 0.028) amng ages 5-11 years (58%) than the yungest age grup (41%). Genitalia exams f members years f age (46%) were cnducted statistically less frequently (p<0.001) than yunger age grups (74% and 63%). An ral health assessment was included as part f the exam in 50% f members. Overall, 6% f members were referred t an ral health prvider; 10% f these were 1-4 years f age. Table I.2.a: Well-Child Visit Cmpsite, Patient Histry, Physical Exam, Oral Health and Height and Weight Assessment Chrt I by Age Grup Grup 1 Grup 2 Grup 3 MEDICAL RECORD REVIEW: Preventive Medicine Services Validatin 1-4 Years (N = 150 ) 5-11 Years (N = 77) Years (N = 81) TOTAL (N = 308) n % n % n % n % Well-Child Visit Cmpsite Members with a visit n at least 1 f the visit dates identified by the claims data % % % % n/a Of whm: 1 (n = 149) (n = 77) (n = 81) (n = 307) Members fr whm reviewed visit was als identified as a well visit in the recrd % 71 92% 72 89% % n.s. Members with visit which includes basic screening cmpnents f a WCV. Of the 4 cmpnents (patient histry, physical exam, Page 12 f 87
13
14
15 Of thse members with a frmal mental health assessment tl used during their visit, the Pediatric Symptm Checklist was used fr ne member and the Vanderbilt Attentin Deficit Hyperactivity Disrder (ADHD) Assessment Scale was used fr ne member, while a practice-specific adlescent questinnaire, the Mdified Checklist fr Autism in Tddlers (M-CHAT), and Perkins Adlescent Risk Screen was used fr three ther members. (Appendix A, Table A.1) Amng adlescent members, ages years, 2% had a frmal depressin screening perfrmed, while 36% were asked abut depressin symptms (Table I.2.b). Perkins Adlescent Risk Screen and the Kutcher Adlescent Depressin Scale were used as frmal depressin screening tls. Medical recrd review dcumentatin indicated that alchl use was screened in 36% f visits and illicit drug use was asked during 28% f visits. Nte that each visit may screen fr the use f mre than ne substance. N frmal substance abuse screening tl, such as the CAGE (Cut-Annyed-Guilty-Eye) questinnaire, Drug Abuse Screening Test (DAST) r CRAFFT (Car, Relax, Alne, Frget, Friends, Truble) screening interview was dcumented in the recrds, althugh substance abuse was cvered n the Perkins Adlescent Risk Screen and a sprts physical exam frm fr tw members. Tbacc use assessment was dcumented in 51% f adlescent recrds. A ttal f fur teenagers were identified as tbacc users, ne was identified as an alchl user, and ne was identified as an illicit drug user. Tw f the fur adlescents wh use tbacc were cunseled r advised t quit, while there was n dcumentatin f alchl r drug use cunseling, referral, r treatment fr adlescents identified as alchl r drug users. Upn review f claims fr adlescent WCVs, nne f the members had substance abuse screening and brief interventin claim cdes, , and substance abuse cunseling cde, V65.42, applied t the visit. Therefre, validatin f these cdes culd nt be perfrmed. Table I.2.b: Well-Child Visit Mental Health Assessment MEDICAL RECORD REVIEW: Preventive Medicine Services Validatin Mental Health Assessment Chrt I by Age Grup Grup 1 Grup 2 Grup Years 5-11 Years Years (N = 149 ) (N = 77) (N = 81) TOTAL (N = 307) n % n % n % n % Frmal mental health screening tl dcumented 1 1% 2 3% 2 2% 5 2% n.s. Parental bservatins/cncerns dcumented 24 16% 22 29% 13 16% 59 19% n.s. Prvider inquiry r bservatin dcumented 42 28% 42 55% 46 57% % <0.001 Grp1<Grp2,Grp3 Ttal members wh received a mental health assessment % 43 56% 49 60% % <0.001 Grp1<Grp2,Grp3 CPT II Cde 2014F- Mental Status Assessed 0 0% 7 9% 14 17% 21 7% n/a Of whm: (n = 0) (n = 7) (n = 14) (n = 21) Had a mental health assessment 6 86% 12 86% 18 86% n.s. Of thse members wh received a mental health assessment: (n = 52) (n = 43) (n = 49) (n = 144) Had a mental health prblem identified 3 6% 20 47% 15 31% 38 26% <0.001 Grp1<Grp2,Grp3 f whm: (n = 3) (n =20) (n = 15) (n = 38) Fllw-up care was dcumented as fllws: Page 15 f 87
16 MEDICAL RECORD REVIEW: Preventive Medicine Services Validatin Chrt I by Age Grup Grup 1 Grup 2 Grup Years 5-11 Years Years (N = 149 ) (N = 77) (N = 81) TOTAL (N = 307) n % n % n % n % Cunseling 0 0% 2 10% 1 7% 3 8% n/a Fllw-up care (cntinued) (n = 3) (n =20) (n = 15) (n = 38) Testing 0 0% 1 5% 0 0% 1 3% n/a Revisit fr repeat screening r evaluatin 0 0% 2 10% 1 7% 3 8% n/a Medicatin 1 33% 8 40% 9 60% 18 47% n/a Referral fr further evaluatin r treatment 0 0% 4 20% 2 13% 6 16% n/a Nne 2 67% 7 35% 4 27% 13 34% n/a Amng members ages years: (n = 0) (n = 0) (n = 81) (n = 81) A depressin screening was perfrmed Infrmal inquiry 29 36% 29 36% n/a Frmal screening 2 2 2% 2 2% n/a Ttal 31 38% 31 38% n/a 1 A Mental Health Assessment included at least 1 f the fllwing: Frmal Mental Health Screening Tl, Parental Cncerns/Observatins dcumented r Prvider Inquiry/Observatins dcumented. 2 Frmal depressin screening tls included Perkins Adlescent Risk Screen and Kutcher Adlescent Depressin Scale. n.s. Nt significant. n/a test nt perfrmed due t small sample size. Table I.2.c: Well-Child Visit Substance Abuse Screening MEDICAL RECORD REVIEW: Preventive Medicine Services Validatin Substance Abuse Screening [Ages ONLY] Chrt I by Age Grup Years (N = 81) n % Members ages years were assessed fr: (n = 81) Tbacc use 41 51% n/a Alchl use 29 36% n/a Drug use 23 28% n/a At least 1 frm f substance use 42 52% n/a f whm: (n = 42) Frmal tl was used fr alchl r drug screening fr members ages years: DAST 0 0% n/a CRAFFT 0 0% n/a CAGE-AID 0 0% n/a Other 1 2 5% n/a Page 16 f 87
17 MEDICAL RECORD REVIEW: Preventive Medicine Services Validatin Chrt I by Age Grup Years (N = 81) n % Members ages years were identified with: (n = 81) Tbacc use 4 5% n/a Alchl use 1 1% n/a Drug use 1 1% n/a Using 1 r any cmbinatin f substances 5 6% n/a Members ages years wh were identified as a tbacc user received fllw-up care: (n = 4) Tbacc cunseling/advice t quit 2 50% n/a Tbacc referral 0 0% n/a Tbacc medicatin/treatment 0 0% n/a Members ages years wh were identified as a alchl user received fllw-up care: (n = 1) Alchl cunseling/brief interventin 0 0% n/a Alchl referral fr treatment 0 0% n/a Members ages years wh were identified as a drug user received fllw-up care: (n = 1) Drug use cunseling/brief interventin 0 0% n/a Drug use referral fr treatment 0 0% n/a 1 Other Substance Abuse Screening tls included: Perkins Adlescent Risk Screen and TSSAA Pre-Participatin Physical Evaluatin. n/a test nt perfrmed due t small sample size. Anticipatry Guidance (Table I.2.d) Frequencies f the prvisin f age-apprpriate anticipatry guidance categries, including nutritin and diet, safety/injury preventin, physical activity, develpment/mental health/emtinal well being, schl readiness/academic/scial, and risk reductin/physical develpment, are included in Table I.2.d. Of statistical significance, anticipatry guidance n nutritin and diet (64%) (p = 0.012) and safety/injury preventin (76%) (p < 0.001), was prvided mre ften amng the 1-4 years age grup than fr lder age grups. The dcumentatin f guidance n physical activity was nly determined fr thse members aged 2 years and lder. Guidance n develpment/mental health/emtinal well being was prvided t 39% f members 5-11 years f age and 40% f members aged years. Guidance n schl readiness/academic/scial was perfrmed fr 36% f members 5-11 years f age and 30% f members aged years. Risk reductin/physical develpment anticipatry guidance was given t 54% f all teenagers aged years. Table I.2.d: Well-Child Visit Anticipatry Guidance MEDICAL RECORD REVIEW: Preventive Medicine Services Validatin Anticipatry Guidance Age-apprpriate anticipatry guidance prvided fr: Chrt I by Member Age Grup 1 Grup 2 Grup Years (N = 149) 5-11 Years (N = 77) Years (N = 81) TOTAL (N = 307) n % n % n % n % Nutritin and Diet 95 64% 39 51% 36 44% % Grp1>Grp3 Safety/Injury Preventin % 43 56% 40 49% % <0.001 Grp1>Grp2,Grp3 Page 17 f 87
18 MEDICAL RECORD REVIEW: Preventive Medicine Services Validatin Chrt I by Member Age Grup 1 Grup 2 Grup Years (N = 149) 5-11 Years (N = 77) Years (N = 81) TOTAL (N = 307) n % n % n % n % Amng members ages 2 years and lder (n = 89) (n = 77) (n = 81) (n = 247) Physical Activity/ Screen Time 51 57% 39 51% 36 44% % n.s. Amng members ages 5 years and lder (n = 0) (n = 77) (n = 81) (n = 158) Develpment/Mental Health/ Emtinal Well Being 30 39% 32 40% 62 39% n.s. Schl Readiness/ Academic/ Scial 28 36% 24 30% 52 33% n.s. Amng members ages 12 years and lder (n = 0) (n = 0) (n = 81) (n = 81) Risk Reductin/ Physical Develpment 44 54% 44 54% n/a n.s. Nt significant. n/a test nt perfrmed due t small sample size. Develpmental Assessment (Table I.2.e) Tw categries f develpmental assessment during the WCV were analyzed: develpmental surveillance and develpmental screening. Overall fr Chrt I, develpmental surveillance was dcumented fr 82% f members. Develpmental surveillance was perfrmed primarily thrugh discussin f develpmental milestnes and/r general surveillance (97%). Develpmental milestnes were surveyed significantly (p = 0.036) mre frequently amng the 1-4 year age grup (99%) than the year age grup (92%). Fr 44% f members, parental cncerns were assessed, althugh this was significantly less frequent (p = 0.016) fr the age grup years (29%) as expected due t greater respnsibility placed n self-care at lder ages. Fr members wh had surveillance perfrmed, develpmental surveillance elements were categrized by scial-emtinal, cgnitive, language and mtr skills. As anticipated, develpmental skills were assessed mre ften amng the yungest age grup when access t early interventin services can be ensured. Language skills (70%) were the least assessed, althugh 89% f children ages 1-4 years, when such assessment is mst critical, were assessed fr language. Mtr skills were assessed significantly mre ften (p < 0.001) in the 1-4 year age grup (89%). Cgnitive skills were assessed at the highest percentage (85%) acrss all age grups. This assessment was statistically higher (p = 0.005) amng the 1-4 year (87%) and the 5-11 year age grups (92%). During a stage f develpment when yuth are ften testing scial barriers, asserting their independence, and having a greater reliance n peer relatinships, sci-emtinal develpment was assessed amng 77% f adlescents, while 84% f members aged 1-4 years were assessed during their visits. The use f at least ne frmal develpmental screen was dcumented in 9% f visits (Table I.2.e). There were 2 f 29 visits, where a glbal standardized screening test was used that addresses fur develpmental dmains (mtr, cgnitive, language, and sci-emtinal) and is als cnsidered t have established reliability, validity, sensitivity, and specificity, accrding t CHIPRA Develpmental Screening measure specificatins. In Chrt I, the nly tl dcumented that meets these specificatins was the Parents Evaluatin f Develpmental Status (PEDS). Other tls, identified in the study, were cnditin-specific, addressed less than fur develpmental dmains, r did nt meet CHIPRA-specified threshlds fr established reliability, validity, sensitivity, and specificity. These tls include M-CHAT, Bellefnte Pediatric Develpment Questinnaire, CHADIS, Denver and Denver II, IH Adlescent Questinnaire, Perkins Adlescent Risk Screen, Vanderbilt ADHD Assessment Scale, and Lansky Perfrmance Status Scale. Overall, the screening tl used mst ften was the M-CHAT (48%), which is a cnditin-specific autism screening tl. Page 18 f 87
19 Table I.2.e: Well-child Visit Develpmental Assessment MEDICAL RECORD REVIEW: Preventive Medicine Services Validatin Develpmental Surveillance Chrt I by Member Age Grup 1 Grup 2 Grup Years 5-11 Years Years (N = 149) (N = 77) (N = 81) TOTAL (N = 307) n % n % n % n % Develpment assessed during visit % 61 79% 65 80% % n.s. Of whm: (n = 126) (n = 61) (n = 65) (n = 252) The fllwing elements f surveillance were perfrmed: Discussin f develpmental milestnes and/r general surveillance % 59 97% 60 92% % Grp1>Grp3 Assessment f parental cncerns 62 49% 31 51% 19 29% % Grp1,Grp2>Grp3 Dmains f surveillance addressed: Scial Emtinal % 44 72% 50 77% % n.s. Cgnitive % 56 92% 47 72% % Grp1,Grp2>Grp3 Language % 44 72% 20 31% % <0.001 Grp1>Grp2>Grp3 Mtr % 44 72% 38 58% % <0.001 Grp1>Grp2,Grp3 Develpmental Screening Amng all members: (n = 149) (n = 77) (n = 81) (n = 307) Frmal develpmental screening tl dcumented 21 14% 5 6% 3 4% 29 9% n/a f whm: (n = 21) (n = 5) (n = 3) (n = 29) Members with a glbal develpmental screening tl: 1 5% 1 20% 0 0% 2 7% n/a Parents Evaluatin f Develpmental Status (PEDS) 1 5% 1 20% 0 0% 2 7% n/a Members with ther 1 screening tl: 20 95% 4 80% 3 100% 27 93% n/a Mdified Checklist fr Autism in Tddlers (M-CHAT) % 0 0% 0 0% 14 48% n/a Other Develpmental Screening Tl 2,3 4 19% 3 60% 3 100% 10 34% n/a UTD 2,4 2 10% 1 20% 0 0% 3 10% n/a Amng all members: (n = 149) (n = 77) (n = 81) (n = 307) Overall type f develpmental assessment: Members with a frmal standardized screening tl 1 1% 1 1% 0 0% 2 1% n/a Page 19 f 87
20 MEDICAL RECORD REVIEW: Preventive Medicine Services Validatin Chrt I by Member Age Grup 1 Grup 2 Grup Years 5-11 Years Years (N = 149) (N = 77) (N = 81) TOTAL (N = 307) n % n % n % n % Members with ther 1 frmal screening tl 20 13% 4 5% 3 4% 27 9% n/a Members with nly develpmental surveillance % 57 74% 62 77% % n/a Members with neither surveillance nr frmal screening 21 14% 15 19% 16 20% 52 17% n/a 1 Other Screening tls may include standardized develpmental screening tls that d nt cver all dmains (Mtr, Cgnitive, Language and Scial) r may nt meet CHIPRA specificatins fr reliability, validity, sensitivity and specificity. 2 The denminatr used in the calculatin f these rates includes all members with any frmal develpmental screening tl dcumented. 3 Other Develpmental Screening tl included: Denver and Denver Develpment II Screen, Perkins Adlescent Risk Screen, Bellefnte Pediatric Develpment, IH Adlescent Questinnaire, Lansky Perfrmance and CHADIS. 4 UTD: Unable t determine. n.s. Nt significant. n/a test nt perfrmed due t small sample size. Page 20 f 87
21 Visin Screening (Table I.2.f) Age-apprpriate visin screening was cnducted during 34% f visits fr members yunger than 3 years f age and fr 38% f visits fr thse ages 3 years and lder. Thugh nt significantly different, the age grups with the highest percentage f visin screens were the 3-4 year (43%) and 5-11 year age grup (42%). Visin referrals were given t 8 ut f 307 members in Chrt I. Table I.2.f: Well-Child Visit Visin Screening MEDICAL RECORD REVIEW: Preventive Medicine Services Validatin Chrt I by Age Grup Grup 1 Grup 2 Grup Years (N = 149) 5-11 Years (N = 77) Years (N = 81) TOTAL (N = 307) n % n % n % n % Well-Child Visit Visin Screening Amng members under 3 years f age: (n = 102) (n = 0) (n = 0) (n = 102) Members received ageapprpriate visin screening 1, which ccurred n the date f the WCV 35 34% 35 34% n/a Of thse that did nt have screen n date f WCV: (n=67) (n = 0) (n = 0) (n=67) Members received ageapprpriate visin screening 1, which ccurred within 7 days f the date f the WCV 0 0% 0 0% n/a Amng members ages 3 years and lder: (n = 47) (n = 77) (n = 81) (n = 205) Members received ageapprpriate visin screening 2 which ccurred n the date f the WCV 20 43% 32 42% 26 32% 78 38% n.s. Of thse that did nt have screen n date f WCV: (n=27) (n=45) (n=55) (n=127) Members received ageapprpriate visin screening 2 which ccurred within 7 days f the date f the WCV 0 0% 2 4% 0 0% 2 2% n/a Amng all members: (n = 149) (n = 77) (n = 81) (n = 307) Member referred t eye health prfessinal 2 1% 4 5% 2 2% 8 3% n.s. 1 Age-apprpriate visin screen fr thse under 3 years f age includes: bservatin/exam/respnses; picture test such as Allen cards; Universal cver test; respnses t visual stimuli. 2 Age-apprpriate visin screen fr thse 3 years f age and lder includes: distance visual acuity via Snellen wall chart; cular alignment via unilateral cver test r randm dt. n.s. Nt significant. n/a test nt perfrmed due t small sample size. Page 21 f 87
22 Hearing Screening (Table I.2.g) Age-apprpriate hearing screening was perfrmed in 14% f visits fr members yunger than 3 years f age and 26% f visits fr thse 3 years and lder. The age grup with the statistically highest percentage (p = 0.014) f hearing screens was the 5-11 year age grup (36%). Fllw-up hearing referrals were prvided t a ttal f three members ut f 72 members with a hearing screen. Table I.2.g: Well-Child Visit Hearing Screening MEDICAL RECORD REVIEW: Preventive Medicine Services Validatin Well-Child Visit Hearing Screening Chrt I by Age Grup Grup 1 Grup 2 Grup Years 5-11 Years Years (N = 149 ) (N = 77) (N = 81) TOTAL (N = 307) n % n % n % n % Amng members under 3 years f age: (n = 102) (n = 0) (n = 0) (n = 102) Members received age-apprpriate hearing screening 1 which ccurred n the date f the WCV 14 14% 14 14% n/a Of thse that did nt have screen n date f WCV: (n = 88) (n = 0) (n = 0) (n =88) Members received ageapprpriate hearing screening 1 which ccurred within 7 days f the date f the WCV 1 1% 1 1% n/a Amng members ages 3 years and lder: (n = 47) (n = 77) (n = 81) (n = 205) Members received age-apprpriate hearing screening 2 which ccurred n the date f the WCV 6 13% 28 36% 20 25% 54 26% Grp1<Grp2 Of thse that did nt have screen n date f WCV: (n =41) (n = 49) (n = 61) (n = 151) Members received ageapprpriate hearing screening 2 which ccurred within 7 days f the date f the WCV 2 5% 1 2% 0 0% 3 2% n/a Amng all members wh received any age-apprpriate hearing screen n r within 7 days f the date f the WCV: (n = 23) (n = 29) (n = 20) (n = 72) Members referred t audilgy related health prfessinal 1 4% 1 3% 1 5% 3 4% n/a 1 Age-apprpriate hearing screening fr thse under 3 years f age includes: bservatin/exam/respnses t auditry stimuli. 2 Age-apprpriate hearing screening fr thse ages 3 years and lder includes: pure tne audimetry and tympanmetry testing perfrmed. n.s. Nt significant. n/a test nt perfrmed due t small sample size. Page 22 f 87
23 Develpmental Screening Cde (CPT 96110) Validatin In accrdance with AAP peridicity schedule, nly the age grup 1-4 in Chrt I was cnsidered fr validatin f CPT since standardized develpmental screening tests shuld be administered at the 9, 18, and mnths visits. Develpmental surveillance was als identified in the medical recrd review in relatin t Fr ages 1-4, ten ut f 149 recrds were assciated with cde Of thse visits with the administrative develpmental screening CPT cde 96110, five members (50%) had dcumented screening with a frmal develpmental screen, while n visits included dcumentatin that a glbal standardized screening tl was used that met CHIPRA specificatins. Fifty percent f visits using cde had nly develpmental surveillance dcumented. Table I.3 Validatin f Develpmental Screening Cde (CPT 96110) Chrt I by Age Grup Grup Years MEDICAL RECORD REVIEW: (N = 149 ) Develpmental Screen Cde Validatin n % Develpmental Surveillance Members with a CPT cde 10 7% n/a Of whm: (n = 10) Develpment assessed during visit % n/a Develpmental Screening Members with a CPT cde 10 7% n/a Of whm: (n = 10) Frmal develpmental screening tl dcumented 5 50% n/a f whm: (n = 5) Members with a glbal standardized screening tl 0 0% n/a Members with ther 1 frmal screening tl: 5 100% n/a Mdified Checklist fr Autism in Tddlers (M-CHAT) % UTD 2,3 1 20% Members with a CPT cde 96110: (n = 10) Of thse members wh had a develpmental screening cde CPT 96110: Members with a glbal standardized screening tl 0 0% Members with ther 1 frmal screening tl 5 50% Members with nly develpmental surveillance 5 50% Members with neither surveillance nr frmal screening 0 0% 1 Other Screening tls may include standardized develpmental screening tls that d nt cver all dmains (Mtr, Cgnitive, Language and Scial) r may nt meet CHIPRA specificatins fr reliability, validity, sensitivity and specificity. 2 The denminatr used in the calculatin f these rates includes all members with any frmal develpmental screening tl dcumented. 3 UTD: Unable t determine. n/a test nt perfrmed due t small sample size. n/a Page 23 f 87
24 Visin Screening Cde Validatin In rder t determine if visin screening cdes and accurately reflect age-apprpriate visin screening, dcumentatin f visin screening was reviewed in the medical recrd. Claims using visin screening cdes and ccurred fr 9% f visits. Of thse members with a visin screening claim, 84% f thse ages 3 years and lder received age-apprpriate visin screening, and 100% f thse yunger than 3 years f age received age-apprpriate visin screening. Table I.4: Validatin f Visin Screening Cde MEDICAL RECORD REVIEW: Visin Screen Cde Validatin Chrt I by Age Grup Grup 1 Grup 2 Grup Years 5-11 Years Years (N = 149 ) (N = 77) (N = 81) TOTAL (N = 307) n % n % n % n % Visin Claim Validatin Members with a visin screening cde (99173, 99174) n the date f the WCV r within 7 days 1 f the WCV 10 7% 8 10% 9 11% 27 9% n.s. Of whm: Amng members under 3 years f age: (n = 2) (n = 0) (n = 0) (n = 2) Members received ageapprpriate visin screening % 2 100% n/a Amng members ages 3 years and lder: (n = 8) (n = 8) (n = 9) (n = 25) Members received ageapprpriate visin screening % 8 100% 9 100% 21 84% n/a 1 Cnsidering that screenings may nt be cmpleted at the first attempt, visits with visin screenings that ccurred within 7 days f the dcumented WCV were allwed t accmmdate repeat ffice visits t cmplete the screening. 2 Age-apprpriate visin screen fr thse under 3 years f age includes: bservatin/exam/respnses; picture test such as Allen cards; Universal cver test; respnses t visual stimuli 3 Age-apprpriate visin screen fr thse 3 years f age and lder includes: distance visual acuity via Snellen wall chart; cular alignment via unilateral cver test r randm dt n.s. Nt significant. n/a test nt perfrmed due t small sample size. Page 24 f 87
25 Hearing Screening Cde Validatin In rder t determine if hearing screening cdes 92551, 92552, and accurately reflect age-apprpriate hearing screening, dcumentatin f hearing screens was reviewed in the medical recrd. Claims using hearing screening cdes ccurred fr 10% f visits. Of the 30 visits with a hearing screening cde, 23 received age-apprpriate screening. The 5-11 year age grup had a significantly higher (p <0.001) percentage f visits with a hearing screening claim (21%) than the 1-4 year age grup (4%). Table I.5: Validatin f Hearing Screening Cde MEDICAL RECORD REVIEW: Hearing Screen Cde Validatin Hearing Claim Validatin Chrt I by Age Grup Grup 1 Grup 2 Grup Years 5-11 Years Years (N = 149 ) (N = 77) (N = 81) TOTAL (N = 307) n % n % n % n % Members with a Hearing Screening cde (92551, 92552, 92567) 6 4% 16 21% 8 10% 30 10% <0.001 Grp1<Grp2 Of whm: Amng members under 3 years f age: (n = 2) (n = 0) (n = 0) (n = 2) Members received age-apprpriate hearing screening % 1 50% n/a Amng members ages 3 years and lder: (n = 4) (n = 16) (n = 8) (n = 28) Members received age-apprpriate hearing screening % 13 81% 8 100% 22 79% n/a 1 Age-apprpriate hearing screening fr thse under 3 years f age includes: bservatin/exam/respnses t auditry stimuli. 2 Age-apprpriate hearing screening fr thse ages 3 years and lder includes: pure tne audimetry and tympanmetry testing perfrmed. n/a test nt perfrmed due t small sample size. Page 25 f 87
26 Chrt I Grup Cmparisn This sectin is a summary f the mst relevant frequency distributins cmpared by gender, EMR dcumentatin, and lcatin types. Detailed frequencies fr each grup are lcated in the appendix f the reprt. Rates fr individual MCOs are presented in Appendix B, but, due t small sample sizes, frequencies by MCO culd nt be cmpared. Cmparisn by Gender (Appendix C) Mental Health, Depressin, and Substance Abuse Assessment (Table C.1) A significantly higher percentage (p = 0.003) f members, wh had at least ne frm f mental health assessment perfrmed and a mental health risk identified, were male (37%). Fifteen percent f females wh had at least ne frm f mental health assessment perfrmed had a mental health risk identified. Develpmental Assessment (Table C.1) Gender differences fr assessment f scial-emtinal and language dmains were statistically significant (p = and p = 0.020). Female members were assessed fr scial-emtinal develpmental dmains as dcumented in 85% f visits while males were assessed fr this dmain as dcumented in 74% f visits. Additinally, an assessment f language develpment was dcumented mre frequently fr females (77%) than males (63%). Cmparisn by EMR (Appendix D) Preventive Medicine Services (Table D.1) Fr a cmpsite WCV, at least 1, 2, and 3 cmpnents were dcumented significantly mre (p < 0.001) with the use f an EMR-based chart than thse withut an EMR-based chart. Prviders dcumented BMI percentiles using an EMR-based chart fr members lder than 2 years f age (64%) significantly mre (p < 0.001) than thse nt using an EMR-based chart (33%). Elements f the physical exam were dcumented statistically mre frequently within EMR-based charts than nn- EMR-based charts. Please see Table D.1 fr s and prprtins. Anticipatry Guidance (Table D.1) Fr EMR-dcumented visits, anticipatry guidance was nted significantly mre ften than visits withut EMR dcumentatin acrss the fllwing categries: Nutritin and diet (p = 0.004) Safety/Injury Preventin (p<0.001) Physical activity/screen Time (p=0.005) Develpment/Mental Health/Emtinal Well-being (p=0.042) Develpmental Assessment (Table D.1) Develpmental surveillance was dcumented significantly mre ften (p < 0.001) with the use f an EMR (91%) than withut an EMR (63%). Cmparisn by Lcatin Type (Appendix E) Preventive Medicine Services (Table E.1) Prviders dcumented BMI percentiles fr urban-residing members lder than 2 years f age (58%) significantly mre (p = 0.025) than rural members (43%). Page 26 f 87
Iowa Early Periodic Screening, Diagnosis and Treatment Care for Kids Program Provider Training
 Iwa Early Peridic Screening, Diagnsis and Treatment Care fr Kids Prgram Prvider Training The Early Peridic Screening, Diagnsis and Treatment (EPSDT) Care fr Kids prgram is Iwa s Medicaid prgram fr children.
Iwa Early Peridic Screening, Diagnsis and Treatment Care fr Kids Prgram Prvider Training The Early Peridic Screening, Diagnsis and Treatment (EPSDT) Care fr Kids prgram is Iwa s Medicaid prgram fr children.
Pediatric and adolescent preventive care and HEDIS *
 Pediatric and adlescent preventive care and HEDIS * * HEDIS is a registered trademark f the Natinal Cmmittee fr Quality Assurance (NCQA). UniCare Health Plan f West Virginia, Inc. Healthcare Effectiveness
Pediatric and adlescent preventive care and HEDIS * * HEDIS is a registered trademark f the Natinal Cmmittee fr Quality Assurance (NCQA). UniCare Health Plan f West Virginia, Inc. Healthcare Effectiveness
PROVIDER ALERT. Comprehensive Diagnostic Evaluation (CDE) Guidelines to Access the Applied Behavior Analysis (ABA) Benefit.
 Guidelines to Access the Applied Behavior Analysis (ABA) Benefit.") Cmprehensive Diagnstic Evaluatin (CDE) Guidelines t Access the Applied Behavir Analysis (ABA) Benefit May 5, 2017 Clinical infrmatin that utlines medical necessity is required t supprt the need fr initial
Cmprehensive Diagnstic Evaluatin (CDE) Guidelines t Access the Applied Behavir Analysis (ABA) Benefit May 5, 2017 Clinical infrmatin that utlines medical necessity is required t supprt the need fr initial
DATA RELEASE: UPDATED PRELIMINARY ANALYSIS ON 2016 HEALTH & LIFESTYLE SURVEY ELECTRONIC CIGARETTE QUESTIONS
 DATA RELEASE: UPDATED PRELIMINARY ANALYSIS ON 216 HEALTH & LIFESTYLE SURVEY ELECTRONIC CIGARETTE QUESTIONS This briefing has been specifically prepared fr the Ministry f Health t prvide infrmatin frm this
DATA RELEASE: UPDATED PRELIMINARY ANALYSIS ON 216 HEALTH & LIFESTYLE SURVEY ELECTRONIC CIGARETTE QUESTIONS This briefing has been specifically prepared fr the Ministry f Health t prvide infrmatin frm this
2017 CMS Web Interface
 CMS Web Interface PREV-5 (NQF 2372): Breast Cancer Screening Measure Steward: NCQA Web Interface V1.0 Page 1 f 18 11/15/2016 Cntents INTRODUCTION... 3 WEB INTERFACE SAMPLING INFORMATION... 4 BENEFICIARY
CMS Web Interface PREV-5 (NQF 2372): Breast Cancer Screening Measure Steward: NCQA Web Interface V1.0 Page 1 f 18 11/15/2016 Cntents INTRODUCTION... 3 WEB INTERFACE SAMPLING INFORMATION... 4 BENEFICIARY
Weight Assessment and Counseling for Children and Adolescents (NQF 0024)
") Weight Assessment and Cunseling fr Children and Adlescents (NQF 0024) EMeasure Name Weight Assessment and EMeasure Id Pending Cunseling fr Children and Adlescents Versin Number 1 Set Id Pending Available
Weight Assessment and Cunseling fr Children and Adlescents (NQF 0024) EMeasure Name Weight Assessment and EMeasure Id Pending Cunseling fr Children and Adlescents Versin Number 1 Set Id Pending Available
Obesity/Morbid Obesity/BMI
 Obesity/mrbid besity/bdy mass index (adult) Obesity/Mrbid Obesity/BMI Definitins and backgrund Diagnsis cde assignment is based n the prvider s clinical judgment and crrespnding medical recrd dcumentatin
Obesity/mrbid besity/bdy mass index (adult) Obesity/Mrbid Obesity/BMI Definitins and backgrund Diagnsis cde assignment is based n the prvider s clinical judgment and crrespnding medical recrd dcumentatin
Childhood Immunization Status (NQF 0038)
") Childhd Immunizatin Status (NQF 0038) EMeasure Name Childhd Immunizatin EMeasure Id Pending Status Versin Number 1 Set Id Pending Available Date N infrmatin Measurement Perid January 1, 20xx thrugh December
Childhd Immunizatin Status (NQF 0038) EMeasure Name Childhd Immunizatin EMeasure Id Pending Status Versin Number 1 Set Id Pending Available Date N infrmatin Measurement Perid January 1, 20xx thrugh December
2017 CMS Web Interface
 CMS Web Interface PREV-6 (NQF 0034): Clrectal Cancer Screening Measure Steward: NCQA Web Interface V1.0 Page 1 f 18 11/15/2016 Cntents INTRODUCTION... 3 WEB INTERFACE SAMPLING INFORMATION... 4 BENEFICIARY
CMS Web Interface PREV-6 (NQF 0034): Clrectal Cancer Screening Measure Steward: NCQA Web Interface V1.0 Page 1 f 18 11/15/2016 Cntents INTRODUCTION... 3 WEB INTERFACE SAMPLING INFORMATION... 4 BENEFICIARY
MEASURE #10: PLAN OF CARE FOR MIGRAINE OR CERVICOGENIC HEADACHE DEVELOPED OR REVIEWED Headache
 MEASURE #10: PLAN OF CARE FOR MIGRAINE OR CERVICOGENIC HEADACHE DEVELOPED OR REVIEWED Headache Measure Descriptin All patients diagnsed with migraine headache r cervicgenic headache wh had a headache management
MEASURE #10: PLAN OF CARE FOR MIGRAINE OR CERVICOGENIC HEADACHE DEVELOPED OR REVIEWED Headache Measure Descriptin All patients diagnsed with migraine headache r cervicgenic headache wh had a headache management
CSHCN Services Program Benefits to Change for Outpatient Behavioral Health Services Information posted November 10, 2009
 CSHCN Services Prgram Benefits t Change fr Outpatient Behaviral Health Services Infrmatin psted Nvember 10, 2009 Effective fr dates f service n r after January 1, 2010, benefit criteria fr utpatient behaviral
CSHCN Services Prgram Benefits t Change fr Outpatient Behaviral Health Services Infrmatin psted Nvember 10, 2009 Effective fr dates f service n r after January 1, 2010, benefit criteria fr utpatient behaviral
Cardiac Rehabilitation Services
 Dcumentatin Guidance N. DG1011 Cardiac Rehabilitatin Services Revisin Letter A 1.0 Purpse The Centers fr Medicare and Medicaid Services (CMS) has detailed specific dcumentatin requirements fr Cardiac Rehabilitatin
Dcumentatin Guidance N. DG1011 Cardiac Rehabilitatin Services Revisin Letter A 1.0 Purpse The Centers fr Medicare and Medicaid Services (CMS) has detailed specific dcumentatin requirements fr Cardiac Rehabilitatin
2017 CMS Web Interface
 CMS Web Interface CARE-2 (NQF 0101): Falls: Screening fr Future Fall Risk Measure Steward: NCQA Web Interface V1.0 Page 1 f 18 11/15/2016 Cntents INTRODUCTION... 3 WEB INTERFACE SAMPLING INFORMATION...
CMS Web Interface CARE-2 (NQF 0101): Falls: Screening fr Future Fall Risk Measure Steward: NCQA Web Interface V1.0 Page 1 f 18 11/15/2016 Cntents INTRODUCTION... 3 WEB INTERFACE SAMPLING INFORMATION...
Structured Assessment using Multiple Patient. Scenarios (StAMPS) Exam Information
 Exam Information") Structured Assessment using Multiple Patient Scenaris (StAMPS) Exam Infrmatin 1. Preparing fr the StAMPS assessment prcess StAMPS is an assessment mdality that is designed t test higher rder functins in
Structured Assessment using Multiple Patient Scenaris (StAMPS) Exam Infrmatin 1. Preparing fr the StAMPS assessment prcess StAMPS is an assessment mdality that is designed t test higher rder functins in
2017 CMS Web Interface
 CMS Web Interface PREV-12 (NQF 0418): Preventive Care and Screening: Screening fr Depressin and Fllw-Up Measure Steward: CMS Web Interface V1.0 Page 1 f 22 11/15/2016 Cntents INTRODUCTION... 3 WEB INTERFACE
CMS Web Interface PREV-12 (NQF 0418): Preventive Care and Screening: Screening fr Depressin and Fllw-Up Measure Steward: CMS Web Interface V1.0 Page 1 f 22 11/15/2016 Cntents INTRODUCTION... 3 WEB INTERFACE
Continuous Quality Improvement: Treatment Record Reviews. Third Thursday Provider Call (August 20, 2015) Wendy Bowlin, QM Administrator
 Wendy Bowlin, QM Administrator") Cntinuus Quality Imprvement: Treatment Recrd Reviews Third Thursday Prvider Call (August 20, 2015) Wendy Bwlin, QM Administratr Gals f the Presentatin Review the findings f Treatment Recrd Review results
Cntinuus Quality Imprvement: Treatment Recrd Reviews Third Thursday Prvider Call (August 20, 2015) Wendy Bwlin, QM Administratr Gals f the Presentatin Review the findings f Treatment Recrd Review results
HEDIS. Healthcare Effectiveness Data & Information Set (HEDIS ) QUALITY MANAGEMENT PROGRAM SECTION 8
 QUALITY MANAGEMENT PROGRAM SECTION 8") HEDIS Healthcare Effectiveness Data & Infrmatin Set (HEDIS ) The HEDIS â audit cntains a cre set f perfrmance measures that prvide infrmatin abut custmer satisfactin, specific health care measures, and
HEDIS Healthcare Effectiveness Data & Infrmatin Set (HEDIS ) The HEDIS â audit cntains a cre set f perfrmance measures that prvide infrmatin abut custmer satisfactin, specific health care measures, and
CDC Influenza Division Key Points MMWR Updates February 20, 2014
 CDC Influenza Divisin Key Pints MMWR Updates In this dcument: Summary Key Messages Seasnal Influenza Vaccine Effectiveness: Interim Adjusted Estimates Influenza Surveillance Update: September 29, 2013-February
CDC Influenza Divisin Key Pints MMWR Updates In this dcument: Summary Key Messages Seasnal Influenza Vaccine Effectiveness: Interim Adjusted Estimates Influenza Surveillance Update: September 29, 2013-February
2018 CMS Web Interface
 CMS Web Interface MH-1 (NQF 0710): Depressin Remissin at Twelve Mnths Measure Steward: MNCM CMS Web Interface V2.0 Page 1 f 27 11/13/2017 Cntents INTRODUCTION... 4 CMS WEB INTERFACE SAMPLING INFORMATION...
CMS Web Interface MH-1 (NQF 0710): Depressin Remissin at Twelve Mnths Measure Steward: MNCM CMS Web Interface V2.0 Page 1 f 27 11/13/2017 Cntents INTRODUCTION... 4 CMS WEB INTERFACE SAMPLING INFORMATION...
US Public Health Service Clinical Practice Guidelines for PrEP
 Webcast 1.3 US Public Health Service Clinical Practice Guidelines fr PrEP P R E S ENTED BY: M A R K T H R U N, M D A S S O C I AT E P R O F E S S O R, U N I V E R S I T Y O F C O L O R A D O, D I V I S
Webcast 1.3 US Public Health Service Clinical Practice Guidelines fr PrEP P R E S ENTED BY: M A R K T H R U N, M D A S S O C I AT E P R O F E S S O R, U N I V E R S I T Y O F C O L O R A D O, D I V I S
2018 CMS Web Interface
 CMS Web Interface MH-1 (NQF 0710): Depressin Remissin at Twelve Mnths Measure Steward: MNCM CMS Web Interface V2.1 Page 1 f 27 06/25/ Cntents INTRODUCTION... 4 CMS WEB INTERFACE SAMPLING INFORMATION...
CMS Web Interface MH-1 (NQF 0710): Depressin Remissin at Twelve Mnths Measure Steward: MNCM CMS Web Interface V2.1 Page 1 f 27 06/25/ Cntents INTRODUCTION... 4 CMS WEB INTERFACE SAMPLING INFORMATION...
Childhood Immunization Status (NQF 0038)
") Childhd Immunizatin Status (NQF 0038) EMeasure Name Childhd Immunizatin EMeasure Id Pending Status Versin Number 1 Set Id Pending Available Date N infrmatin Measurement Perid January 1, 20xx thrugh December
Childhd Immunizatin Status (NQF 0038) EMeasure Name Childhd Immunizatin EMeasure Id Pending Status Versin Number 1 Set Id Pending Available Date N infrmatin Measurement Perid January 1, 20xx thrugh December
National Imaging Associates, Inc. (NIA) Frequently Asked Questions (FAQ s) For PA Health & Wellness Providers
 Frequently Asked Questions (FAQ s) For PA Health & Wellness Providers") Natinal Imaging Assciates, Inc. (NIA) Frequently Asked Questins (FAQ s) Fr PA Health & Wellness Prviders Questin GENERAL Why is PA Health & Wellness implementing a Medical Specialty Slutins Prgram? Answer
Natinal Imaging Assciates, Inc. (NIA) Frequently Asked Questins (FAQ s) Fr PA Health & Wellness Prviders Questin GENERAL Why is PA Health & Wellness implementing a Medical Specialty Slutins Prgram? Answer
2018 CMS Web Interface
 CMS Web Interface Diabetes Mellitus (DM) Cmpsite (All r Nthing Scring) DM-2 (NQF 0059): Diabetes: Hemglbin A1c (HbA1c) Pr Cntrl (>9%) DM-7 (NQF Measure Steward: NCQA CMS Web Interface V2.1 Page 1 f 26
CMS Web Interface Diabetes Mellitus (DM) Cmpsite (All r Nthing Scring) DM-2 (NQF 0059): Diabetes: Hemglbin A1c (HbA1c) Pr Cntrl (>9%) DM-7 (NQF Measure Steward: NCQA CMS Web Interface V2.1 Page 1 f 26
2017 CMS Web Interface
 CMS Web Interface Diabetes Mellitus (DM) Cmpsite (All r Nthing Scring) DM-2 (NQF 0059): Diabetes: Hemglbin A1c (HbA1c) Pr Cntrl (>9%) DM-7 (NQF 0055): Diabetes: Eye Exam Measure Steward: NCQA Web Interface
CMS Web Interface Diabetes Mellitus (DM) Cmpsite (All r Nthing Scring) DM-2 (NQF 0059): Diabetes: Hemglbin A1c (HbA1c) Pr Cntrl (>9%) DM-7 (NQF 0055): Diabetes: Eye Exam Measure Steward: NCQA Web Interface
Q 5: Is relaxation training better (more effective than/as safe as) than treatment as usual in adults with depressive episode/disorder?
 than treatment as usual in adults with depressive episode/disorder?") updated 2012 Relaxatin training Q 5: Is relaxatin training better (mre effective than/as safe as) than treatment as usual in adults with depressive episde/disrder? Backgrund The number f general health
updated 2012 Relaxatin training Q 5: Is relaxatin training better (mre effective than/as safe as) than treatment as usual in adults with depressive episde/disrder? Backgrund The number f general health
2018 CMS Web Interface
 CMS Web Interface PREV-12 (NQF 0418): Preventive Care and Screening: Screening fr Depressin and Measure Steward: CMS CMS Web Interface V2.1 Page 1 f 23 06/25/ Cntents INTRODUCTION... 3 CMS WEB INTERFACE
CMS Web Interface PREV-12 (NQF 0418): Preventive Care and Screening: Screening fr Depressin and Measure Steward: CMS CMS Web Interface V2.1 Page 1 f 23 06/25/ Cntents INTRODUCTION... 3 CMS WEB INTERFACE
Appendix C. Master of Public Health. Practicum Guidelines
 Appendix C Master f Public Health Practicum Guidelines 0 Gergia State University, Schl f Public Health Master f Public Health Practicum Guidelines Fr mre infrmatin, cntact Jessica Hwell Pratt, MPH Practicum
Appendix C Master f Public Health Practicum Guidelines 0 Gergia State University, Schl f Public Health Master f Public Health Practicum Guidelines Fr mre infrmatin, cntact Jessica Hwell Pratt, MPH Practicum
2018 CMS Web Interface
 CMS Web Interface HTN-2 (NQF 0018): Cntrlling High Bld Pressure Measure Steward: NCQA CMS Web Interface V2.0 Page 1 f 18 11/13/2017 Cntents INTRODUCTION... 3 CMS WEB INTERFACE SAMPLING INFORMATION... 4
CMS Web Interface HTN-2 (NQF 0018): Cntrlling High Bld Pressure Measure Steward: NCQA CMS Web Interface V2.0 Page 1 f 18 11/13/2017 Cntents INTRODUCTION... 3 CMS WEB INTERFACE SAMPLING INFORMATION... 4
2018 CMS Web Interface
 CMS Web Interface PREV-9 (NQF 0421): Preventive Care and Screening: Bdy Mass Index (BMI) Screening Measure Steward: CMS CMS Web Interface V2.0 Page 1 f 23 11/13/2017 Cntents INTRODUCTION... 3 CMS WEB INTERFACE
CMS Web Interface PREV-9 (NQF 0421): Preventive Care and Screening: Bdy Mass Index (BMI) Screening Measure Steward: CMS CMS Web Interface V2.0 Page 1 f 23 11/13/2017 Cntents INTRODUCTION... 3 CMS WEB INTERFACE
Swindon Joint Strategic Needs Assessment Bulletin
 Swindn Jint Strategic Needs Assessment Bulletin Swindn Diabetes 2017 Key Pints: This JSNA gives health facts abut peple with diabetes r peple wh might get diabetes in Swindn. This helps us t plan fr medical
Swindn Jint Strategic Needs Assessment Bulletin Swindn Diabetes 2017 Key Pints: This JSNA gives health facts abut peple with diabetes r peple wh might get diabetes in Swindn. This helps us t plan fr medical
National Imaging Associates, Inc. (NIA) Frequently Asked Questions (FAQs) For Managed Health Services (MHS)
 Frequently Asked Questions (FAQs) For Managed Health Services (MHS)") Questin GENERAL Why did MHS implement a Medical Specialty Slutins Prgram? Natinal Imaging Assciates, Inc. (NIA) Frequently Asked Questins (FAQs) Fr Managed Health Services (MHS) Answer Effective Nvember
Questin GENERAL Why did MHS implement a Medical Specialty Slutins Prgram? Natinal Imaging Assciates, Inc. (NIA) Frequently Asked Questins (FAQs) Fr Managed Health Services (MHS) Answer Effective Nvember
Diabetes: HbA1c Poor Control (NQF 0059)
") Diabetes: HbA1c Pr Cntrl (NQF 0059) EMeasure Name Diabetes: HbA1c Pr Cntrl EMeasure Id Pending Versin Number 1 Set Id Pending Available Date N infrmatin Measurement January 1, 20xx thrugh Perid December
Diabetes: HbA1c Pr Cntrl (NQF 0059) EMeasure Name Diabetes: HbA1c Pr Cntrl EMeasure Id Pending Versin Number 1 Set Id Pending Available Date N infrmatin Measurement January 1, 20xx thrugh Perid December
GUIDANCE DOCUMENT FOR ENROLLING SUBJECTS WHO DO NOT SPEAK ENGLISH
 GUIDANCE DOCUMENT FOR ENROLLING SUBJECTS WHO DO NOT SPEAK ENGLISH Aurra Health Care s Research Subject Prtectin Prgram (RSPP) This guidance dcument will utline the prper prcedures fr btaining and dcumenting
GUIDANCE DOCUMENT FOR ENROLLING SUBJECTS WHO DO NOT SPEAK ENGLISH Aurra Health Care s Research Subject Prtectin Prgram (RSPP) This guidance dcument will utline the prper prcedures fr btaining and dcumenting
CLINICAL MEDICAL POLICY
 Plicy Name: Plicy Number: Respnsible Department(s): CLINICAL MEDICAL POLICY Supervised Exercise Therapy fr Peripheral Artery Disease (PAD) MP-077-MD-DE Medical Management Prvider Ntice Date: 01/15/2019
Plicy Name: Plicy Number: Respnsible Department(s): CLINICAL MEDICAL POLICY Supervised Exercise Therapy fr Peripheral Artery Disease (PAD) MP-077-MD-DE Medical Management Prvider Ntice Date: 01/15/2019
National Imaging Associates, Inc. (NIA) Frequently Asked Questions (FAQs) For Louisiana Healthcare Connections Providers
 Frequently Asked Questions (FAQs) For Louisiana Healthcare Connections Providers") Natinal Imaging Assciates, Inc. (NIA) Frequently Asked Questins (FAQs) Fr Luisiana Healthcare Cnnectins Prviders Questin GENERAL Why did Luisiana Healthcare Cnnectins implement a Medical Prgram? Answer
Natinal Imaging Assciates, Inc. (NIA) Frequently Asked Questins (FAQs) Fr Luisiana Healthcare Cnnectins Prviders Questin GENERAL Why did Luisiana Healthcare Cnnectins implement a Medical Prgram? Answer
Chapter 6: Impact Indicators
 Overview Chapter 6: Impact Indicatrs The best measure f the lng-term impact f all HIV preventin activities is the HIV incidence rate, namely the number f new cases f HIV infectin per year divided by the
Overview Chapter 6: Impact Indicatrs The best measure f the lng-term impact f all HIV preventin activities is the HIV incidence rate, namely the number f new cases f HIV infectin per year divided by the
2017 CMS Web Interface
 CMS Web Interface PREV-9 (NQF 0421): Preventive Care and Screening: Bdy Mass Index (BMI) Screening and Fllw- Measure Steward: CMS Web Interface V1.0 Page 1 f 23 11/15/2016 Cntents INTRODUCTION... 3 WEB
CMS Web Interface PREV-9 (NQF 0421): Preventive Care and Screening: Bdy Mass Index (BMI) Screening and Fllw- Measure Steward: CMS Web Interface V1.0 Page 1 f 23 11/15/2016 Cntents INTRODUCTION... 3 WEB
2018 CMS Web Interface
 CMS Web Interface PREV-9 (NQF 0421): Preventive Care and Screening: Bdy Mass Index (BMI) Screening Measure Steward: CMS CMS Web Interface V2.1 Page 1 f 24 06/25/ Cntents INTRODUCTION... 3 CMS WEB INTERFACE
CMS Web Interface PREV-9 (NQF 0421): Preventive Care and Screening: Bdy Mass Index (BMI) Screening Measure Steward: CMS CMS Web Interface V2.1 Page 1 f 24 06/25/ Cntents INTRODUCTION... 3 CMS WEB INTERFACE
Bariatric Surgery FAQs for Employees in the GRMC Group Health Plan
 Bariatric Surgery FAQs fr Emplyees in the GRMC Grup Health Plan Gergia Regents Medical Center and Gergia Regents Medical Assciates emplyees and eligible dependents wh are in the GRMC Grup Health Plan (Select
Bariatric Surgery FAQs fr Emplyees in the GRMC Grup Health Plan Gergia Regents Medical Center and Gergia Regents Medical Assciates emplyees and eligible dependents wh are in the GRMC Grup Health Plan (Select
The estimator, X, is unbiased and, if one assumes that the variance of X7 is constant from week to week, then the variance of X7 is given by
 ESTIMATION PROCEDURES USED TO PRODUCE WEEKLY FLU STATISTICS FROM THE HEALTH INTERVIEW SURVEY James T. Massey, Gail S. Pe, Walt R. Simmns Natinal Center fr Health Statistics. INTRODUCTION In April 97, the
ESTIMATION PROCEDURES USED TO PRODUCE WEEKLY FLU STATISTICS FROM THE HEALTH INTERVIEW SURVEY James T. Massey, Gail S. Pe, Walt R. Simmns Natinal Center fr Health Statistics. INTRODUCTION In April 97, the
NIA Magellan 1 Spine Care Program Interventional Pain Management Frequently Asked Questions (FAQs) For Medicare Advantage HMO and PPO
 For Medicare Advantage HMO and PPO") NIA Magellan 1 Spine Care Prgram Interventinal Pain Management Frequently Asked Questins (FAQs) Fr Medicare Advantage HMO and PPO Questin GENERAL Why is Flrida Blue implementing a Spine Management prgram
NIA Magellan 1 Spine Care Prgram Interventinal Pain Management Frequently Asked Questins (FAQs) Fr Medicare Advantage HMO and PPO Questin GENERAL Why is Flrida Blue implementing a Spine Management prgram
LEVEL OF CARE GUIDELINES: INTENSIVE BEHAVIORAL THERAPY/APPLIED BEHAVIOR ANALYSIS FOR AUTISM SPECTRUM DISORDER HAWAII MEDICAID QUEST
 OPTUM LEVEL OF CARE GUIDELINES: INTENSIVE BEHAVIORAL THERAPY / APPLIED BEHAVIOR ANALYSIS FOR AUTISM SPECTRUM DISORDER HAWAII MEDICAID QUEST LEVEL OF CARE GUIDELINES: INTENSIVE BEHAVIORAL THERAPY/APPLIED
OPTUM LEVEL OF CARE GUIDELINES: INTENSIVE BEHAVIORAL THERAPY / APPLIED BEHAVIOR ANALYSIS FOR AUTISM SPECTRUM DISORDER HAWAII MEDICAID QUEST LEVEL OF CARE GUIDELINES: INTENSIVE BEHAVIORAL THERAPY/APPLIED
LTCH QUALITY REPORTING PROGRAM
 4 LTCH QUALITY REPORTING PROGRAM GENERAL INFORMATION...3 LTCH FACILITY-LEVEL QUALITY MEASURE REPORT...5 LTCH PATIENT-LEVEL QUALITY MEASURE REPORT...18 LTCH REVIEW AND CORRECT REPORT...23 09/2018 v1.04
4 LTCH QUALITY REPORTING PROGRAM GENERAL INFORMATION...3 LTCH FACILITY-LEVEL QUALITY MEASURE REPORT...5 LTCH PATIENT-LEVEL QUALITY MEASURE REPORT...18 LTCH REVIEW AND CORRECT REPORT...23 09/2018 v1.04
P02-03 CALA Program Description Proficiency Testing Policy for Accreditation Revision 1.9 July 26, 2017
 P02-03 CALA Prgram Descriptin Prficiency Testing Plicy fr Accreditatin Revisin 1.9 July 26, 2017 P02-03 CALA Prgram Descriptin Prficiency Testing Plicy fr Accreditatin TABLE OF CONTENTS TABLE OF CONTENTS...
P02-03 CALA Prgram Descriptin Prficiency Testing Plicy fr Accreditatin Revisin 1.9 July 26, 2017 P02-03 CALA Prgram Descriptin Prficiency Testing Plicy fr Accreditatin TABLE OF CONTENTS TABLE OF CONTENTS...
Health Screening Record: Entry Level Due: August 1st MWF 150 Entry Year
 Health Screening Recrd: Entry Level MIDWIFERY EDUCATION PROGRAM HEALTH SCREENING REQUIREMENTS (Rev. June 2017) 1. Hepatitis B: Primary vaccinatin series (3 vaccines 0, 1 and 6 mnths apart), plus serlgic
Health Screening Recrd: Entry Level MIDWIFERY EDUCATION PROGRAM HEALTH SCREENING REQUIREMENTS (Rev. June 2017) 1. Hepatitis B: Primary vaccinatin series (3 vaccines 0, 1 and 6 mnths apart), plus serlgic
Assessment Field Activity Collaborative Assessment, Planning, and Support: Safety and Risk in Teams
 Assessment Field Activity Cllabrative Assessment, Planning, and Supprt: Safety and Risk in Teams OBSERVATION Identify a case fr which a team meeting t discuss safety and/r safety planning is needed r scheduled.
Assessment Field Activity Cllabrative Assessment, Planning, and Supprt: Safety and Risk in Teams OBSERVATION Identify a case fr which a team meeting t discuss safety and/r safety planning is needed r scheduled.
Nutrition Care Process Model Tutorials. Nutrition Monitoring & Evaluation: Overview & Definition. By the end of this module, the participant will:
 Nutritin Care Prcess Mdel Tutrials Nutritin Care Prcess and Terminlgy Cmmittee Academy f Nutritin and Dietetics Nutritin Care Prcess Terminlgy 2015 Editin Nutritin Mnitring & Evaluatin: Overview & Definitin
Nutritin Care Prcess Mdel Tutrials Nutritin Care Prcess and Terminlgy Cmmittee Academy f Nutritin and Dietetics Nutritin Care Prcess Terminlgy 2015 Editin Nutritin Mnitring & Evaluatin: Overview & Definitin
2013 DATA COLLECTION GUIDE Summary Data Submission. Optimal Asthma Care. (07/01/2012 to 06/30/2013 Dates of Service)
") 2013 DATA COLLECTION GUIDE Summary Data Submissin Optimal Asthma Care (07/01/2012 t 06/30/2013 Dates f Service) Htline: 612-746-4522 E-mail: supprt@mncm.rg Data Prtal: https://data.mncm.rg/lgin MN Cmmunity
2013 DATA COLLECTION GUIDE Summary Data Submissin Optimal Asthma Care (07/01/2012 t 06/30/2013 Dates f Service) Htline: 612-746-4522 E-mail: supprt@mncm.rg Data Prtal: https://data.mncm.rg/lgin MN Cmmunity
Vaccine Information Statement: PNEUMOCOCCAL CONJUGATE VACCINE
 Vaccine Infrmatin Statement: PNEUMOCOCCAL CONJUGATE VACCINE Many Vaccine Infrmatin Statements are available in Spanish and ther languages. See www.immunize.rg/vis. Hjas de Infrmacián Sbre Vacunas están
Vaccine Infrmatin Statement: PNEUMOCOCCAL CONJUGATE VACCINE Many Vaccine Infrmatin Statements are available in Spanish and ther languages. See www.immunize.rg/vis. Hjas de Infrmacián Sbre Vacunas están
Related Policies None
 Medical Plicy MP 3.01.501 Guidelines fr Cverage f Mental and Behaviral Health Services Last Review: 8/30/2017 Effective Date: 8/30/2017 Sectin: Mental Health End Date: 08/19/2018 Related Plicies Nne DISCLAIMER
Medical Plicy MP 3.01.501 Guidelines fr Cverage f Mental and Behaviral Health Services Last Review: 8/30/2017 Effective Date: 8/30/2017 Sectin: Mental Health End Date: 08/19/2018 Related Plicies Nne DISCLAIMER
Year 10 Food Technology. Assessment Task 1: Foods for Special Needs. Name: Teacher:
 Year 10 Fd Technlgy Assessment Task 1: Fds fr Special Needs Name: Teacher: Due Date: Term 2, Week 1 Type f Task: Design Task Planning Fd Requirements Cllectin f Assessment: Submit in Class Assessment Plicy:
Year 10 Fd Technlgy Assessment Task 1: Fds fr Special Needs Name: Teacher: Due Date: Term 2, Week 1 Type f Task: Design Task Planning Fd Requirements Cllectin f Assessment: Submit in Class Assessment Plicy:
A pre-conference should include the following: an introduction, a discussion based on the review of lesson materials, and a summary of next steps.
 NAU Mdel Observatin Prtcl The mdel prtcl was develped with supprt and expertise frm the Natinal Institute fr Excellence in Teaching (NIET) and is based in great part n NIET s extensive experience cnducting
NAU Mdel Observatin Prtcl The mdel prtcl was develped with supprt and expertise frm the Natinal Institute fr Excellence in Teaching (NIET) and is based in great part n NIET s extensive experience cnducting
Breast Cancer Awareness Month 2018 Key Messages (as of June 6, 2018)
") Breast Cancer Awareness Mnth 2018 Key Messages (as f June 6, 2018) In this dcument there are tw sectins f messages in supprt f Cancer Care Ontari s Breast Cancer Awareness Mnth 2018: 1. Campaign key messages
Breast Cancer Awareness Mnth 2018 Key Messages (as f June 6, 2018) In this dcument there are tw sectins f messages in supprt f Cancer Care Ontari s Breast Cancer Awareness Mnth 2018: 1. Campaign key messages
Risk factors in health and disease
 Risk factrs in health and disease Index 1 Intrductin 2 Types f risk factrs 2.1 Behaviural risk factrs 2.2 Psychlgical risk factrs 2.3 Demgraphic risk factrs 2.4 Envirnmental risk factrs 2.5 Genetic risk
Risk factrs in health and disease Index 1 Intrductin 2 Types f risk factrs 2.1 Behaviural risk factrs 2.2 Psychlgical risk factrs 2.3 Demgraphic risk factrs 2.4 Envirnmental risk factrs 2.5 Genetic risk
PET FORM Planning and Evaluation Tracking ( Assessment Period)
") Divisin f: Behaviral Studies PET FORM Planning and Evaluatin Tracking (2010 2011 Assessment Perid) Persn Respnsible fr this Divisin: Jerry Mller Department f: Behaviral Sciences Persn Respnsible fr this
Divisin f: Behaviral Studies PET FORM Planning and Evaluatin Tracking (2010 2011 Assessment Perid) Persn Respnsible fr this Divisin: Jerry Mller Department f: Behaviral Sciences Persn Respnsible fr this
23/11/2015. Introduction & Aims. Methods. Methods. Survey response. Patient Survey (baseline)
") Intrductin & Aims Drug and Alchl Cnsultatin Liaisn (AOD CL) services aim t imprve identificatin and treatment f patients with AOD mrbidity. The csts and cnsequences f targeting AOD patients presenting
Intrductin & Aims Drug and Alchl Cnsultatin Liaisn (AOD CL) services aim t imprve identificatin and treatment f patients with AOD mrbidity. The csts and cnsequences f targeting AOD patients presenting
Evaluation of a Shared Decision Making Intervention between Patients and Providers to Improve Menopause Health Outcomes: Issue Brief
 Evaluatin f a Shared Decisin Making Interventin between Patients and Prviders t Imprve Menpause Health Outcmes: Issue Brief Key Findings Tablet technlgy can be successfully incrprated int primary practices
Evaluatin f a Shared Decisin Making Interventin between Patients and Prviders t Imprve Menpause Health Outcmes: Issue Brief Key Findings Tablet technlgy can be successfully incrprated int primary practices
Module 6: Goal Setting
 Mdule 6: Gal Setting Objectives T understand the cncept f gal setting in Brief CBT T acquire skills t set feasible and apprpriate gals in Brief CBT What is gal setting, and why is it imprtant t set gals
Mdule 6: Gal Setting Objectives T understand the cncept f gal setting in Brief CBT T acquire skills t set feasible and apprpriate gals in Brief CBT What is gal setting, and why is it imprtant t set gals
Public consultation on the NHMRC s draft revised Australian alcohol guidelines for low-risk drinking
 Public cnsultatin n the NHMRC s draft revised Australian alchl guidelines fr lw-risk drinking Recmmendatins frm The Cancer Cuncil Australia The Cancer Cuncil Australia is Australia s peak nn-gvernment
Public cnsultatin n the NHMRC s draft revised Australian alchl guidelines fr lw-risk drinking Recmmendatins frm The Cancer Cuncil Australia The Cancer Cuncil Australia is Australia s peak nn-gvernment
2018 Medical Association Poster Symposium Guidelines
 2018 Medical Assciatin Pster Sympsium Guidelines Overview The 3 rd Annual student-run Medical Assciatin f the State f Alabama Research Sympsium will take place n Friday and Saturday, April 13-14 at the
2018 Medical Assciatin Pster Sympsium Guidelines Overview The 3 rd Annual student-run Medical Assciatin f the State f Alabama Research Sympsium will take place n Friday and Saturday, April 13-14 at the
This clinical study synopsis is provided in line with Boehringer Ingelheim s Policy on Transparency and Publication of Clinical Study Data.
 abcd Clinical Study Synpsis fr Public Disclsure This clinical study synpsis is prvided in line with Behringer Ingelheim s Plicy n Transparency and Publicatin f Clinical Study Data. The synpsis which is
abcd Clinical Study Synpsis fr Public Disclsure This clinical study synpsis is prvided in line with Behringer Ingelheim s Plicy n Transparency and Publicatin f Clinical Study Data. The synpsis which is
Cognitive enhancers for the treatment of Alzheimer s disease
 Cmprehensive Research Plan: Cgnitive enhancers fr the treatment f Alzheimer s disease Pharmacepidemilgy Unit February 13 th, 2015 30 Bnd Street, Trnt ON, M5B 1W8 www.dprn.ca inf@dprn.ca 2 ODPRN Drug Class
Cmprehensive Research Plan: Cgnitive enhancers fr the treatment f Alzheimer s disease Pharmacepidemilgy Unit February 13 th, 2015 30 Bnd Street, Trnt ON, M5B 1W8 www.dprn.ca inf@dprn.ca 2 ODPRN Drug Class
EXPLORING THE PROCESS OF ASSESSMENT AND OTHER RELATED CONCEPTS
 1 SECTION 1 INTRODUCTION: EXPLORING THE PROCESS OF ASSESSMENT AND OTHER RELATED CONCEPTS The Nature Of Assessment The Definitin Of Assessment The Difference Between Testing, Measurement And Evaluatin Characteristics
1 SECTION 1 INTRODUCTION: EXPLORING THE PROCESS OF ASSESSMENT AND OTHER RELATED CONCEPTS The Nature Of Assessment The Definitin Of Assessment The Difference Between Testing, Measurement And Evaluatin Characteristics
PSYCHOSEXUAL ASSESSMENTS for Children and Adolescents with Problematic Sexual Behavior. Who is qualified to conduct a psychosexual evaluation?
 PSYCHOSEXUAL ASSESSMENTS fr Children and Adlescents with Prblematic Sexual Behavir When a child r adlescent is suspected r bserved t have engaged in what may be sexually inapprpriate r sexually aggressive
PSYCHOSEXUAL ASSESSMENTS fr Children and Adlescents with Prblematic Sexual Behavir When a child r adlescent is suspected r bserved t have engaged in what may be sexually inapprpriate r sexually aggressive
HEALTH SURVEILLANCE INDICATORS: CERVICAL CANCER SCREENING. Public Health Relevance. Highlights.
 HEALTH SURVEILLANCE INDICATORS: CERVICAL CANCER SCREENING Public Health Relevance Cervical cancer is 90% preventable by having regular Papaniclau (Pap) tests. The Pap test, als knwn as a cervical smear,
HEALTH SURVEILLANCE INDICATORS: CERVICAL CANCER SCREENING Public Health Relevance Cervical cancer is 90% preventable by having regular Papaniclau (Pap) tests. The Pap test, als knwn as a cervical smear,
Reliability and Validity Plan 2017
 Reliability and Validity Plan 2017 Frm CAEP The principles fr measures used in the CAEP accreditatin prcess include: (a) validity and reliability, (b) relevance, (c) verifiability, (d) representativeness,
Reliability and Validity Plan 2017 Frm CAEP The principles fr measures used in the CAEP accreditatin prcess include: (a) validity and reliability, (b) relevance, (c) verifiability, (d) representativeness,
Novel methods and approaches for sensing, evaluating, modulating and regulating mood and emotional states.
 Nvel methds and appraches fr sensing, evaluating, mdulating and regulating md and emtinal states. 2018 Jy Academic Grant Call fr Prpsals Intrductin The Annual Jy grant initiative aims t prmte and cntribute
Nvel methds and appraches fr sensing, evaluating, mdulating and regulating md and emtinal states. 2018 Jy Academic Grant Call fr Prpsals Intrductin The Annual Jy grant initiative aims t prmte and cntribute
Immunisation and Disease Prevention Policy
 Immunisatin and Disease Preventin Plicy Quality Area 2: Children s Health and Safety 2.1 Each child s health is prmted 2.1.4 Steps are taken t cntrl the spread f infectius diseases and t manage injuries
Immunisatin and Disease Preventin Plicy Quality Area 2: Children s Health and Safety 2.1 Each child s health is prmted 2.1.4 Steps are taken t cntrl the spread f infectius diseases and t manage injuries
Drug Class Review: Long-acting muscarinic antagonists (LAMAs) for treatment of chronic obstructive pulmonary disease (COPD)
 for treatment of chronic obstructive pulmonary disease (COPD)") Drug Class Review: Lng-acting muscarinic antagnists (LAMAs) fr treatment f chrnic bstructive pulmnary disease (COPD) Cmprehensive Research Plan: Pharmacepidemilgy Unit April 10 th, 2014 ODPRN Drug Class
Drug Class Review: Lng-acting muscarinic antagnists (LAMAs) fr treatment f chrnic bstructive pulmnary disease (COPD) Cmprehensive Research Plan: Pharmacepidemilgy Unit April 10 th, 2014 ODPRN Drug Class
Assessment criteria for Primary Health Disciplines Eligibility for Recognition as Credentialled Diabetes Educator. December 2015 ADEA
 Assessment criteria fr Primary Health Disciplines Eligibility fr Recgnitin as Credentialled Diabetes Educatr December 2015 ADEA ASSESSMENT CRITERIA FOR PRIMARY HEALTH DICIPLINES ELIGIBILITY FOR RECOGNITION
Assessment criteria fr Primary Health Disciplines Eligibility fr Recgnitin as Credentialled Diabetes Educatr December 2015 ADEA ASSESSMENT CRITERIA FOR PRIMARY HEALTH DICIPLINES ELIGIBILITY FOR RECOGNITION
CDC Influenza Technical Key Points February 15, 2018
 CDC Influenza Technical Key Pints In this dcument: Summary Key Pints U.S. Vaccine Effectiveness U.S. Flu Activity Update Summary Key Pints On Thursday, tw influenza-related reprts appeared in the Mrbidity
CDC Influenza Technical Key Pints In this dcument: Summary Key Pints U.S. Vaccine Effectiveness U.S. Flu Activity Update Summary Key Pints On Thursday, tw influenza-related reprts appeared in the Mrbidity
Pennsylvania Guidelines on the Use of Opioids to Treat Chronic Noncancer Pain
 Pennsylvania Guidelines n the Use f Opiids t Treat Chrnic Nncancer Pain Chrnic pain is a majr health prblem in the United States, ccurring with a pintprevalence f abut ne-third f the US ppulatin.(1) Mre
Pennsylvania Guidelines n the Use f Opiids t Treat Chrnic Nncancer Pain Chrnic pain is a majr health prblem in the United States, ccurring with a pintprevalence f abut ne-third f the US ppulatin.(1) Mre
HSC 106 Personal Health Plan for Learning Activities & Assessment linked to Michigan Teacher Preparation Standards
 HSC 106 Persnal Health Plan fr Learning Activities & Assessment linked t Michigan Teacher Preparatin Standards Standard 1 Cmpetency 1.1 Understand basic health cntent as it relates t schl health educatin.
HSC 106 Persnal Health Plan fr Learning Activities & Assessment linked t Michigan Teacher Preparatin Standards Standard 1 Cmpetency 1.1 Understand basic health cntent as it relates t schl health educatin.
2018 CMS Web Interface
 PREV-13: Statin Therapy fr the Preventin and Treatment f Cardivascular Disease CMS Web Interface PREV-13: Statin Therapy fr the Preventin and Treatment f Cardivascular Disease Measure Steward: CMS CMS
PREV-13: Statin Therapy fr the Preventin and Treatment f Cardivascular Disease CMS Web Interface PREV-13: Statin Therapy fr the Preventin and Treatment f Cardivascular Disease Measure Steward: CMS CMS
Corporate Governance Code for Funds: What Will it Mean?
 Crprate Gvernance Cde fr Funds: What Will it Mean? The Irish Funds Industry Assciatin has circulated a draft Vluntary Crprate Gvernance Cde fr the Funds Industry in Ireland. 1. Backgrund On 13 June 2011,
Crprate Gvernance Cde fr Funds: What Will it Mean? The Irish Funds Industry Assciatin has circulated a draft Vluntary Crprate Gvernance Cde fr the Funds Industry in Ireland. 1. Backgrund On 13 June 2011,
OTHER AND UNSPECIFIED DISORDERS
 OPTUM COVERAGE DETERMINATION GUIDELINE OTHER AND UNSPECIFIED DISORDERS Guideline Number: BH727OUD_102017 Effective Date: Octber, 2017 Table f Cntents Page INSTRUCTIONS FOR USE... 1 BENEFIT CONSIDERATIONS...
OPTUM COVERAGE DETERMINATION GUIDELINE OTHER AND UNSPECIFIED DISORDERS Guideline Number: BH727OUD_102017 Effective Date: Octber, 2017 Table f Cntents Page INSTRUCTIONS FOR USE... 1 BENEFIT CONSIDERATIONS...
o Procedures performed o Diagnoses Identified o Certain devices/equipment/supplies acquired for patient
 Image Surce: https://s-media-cache-ak0.pinimg.cm/736x/7c/29/91/7c2991805f004e1ca05e42a79883f4a7.jpg 6/30/2017 Curse Objectives A Practical Guide t Cding fr Audilgists in 2017 Megan Keirans, AuD University
Image Surce: https://s-media-cache-ak0.pinimg.cm/736x/7c/29/91/7c2991805f004e1ca05e42a79883f4a7.jpg 6/30/2017 Curse Objectives A Practical Guide t Cding fr Audilgists in 2017 Megan Keirans, AuD University
The data refer to persons aged between 15 and 54.
 Drug-related hspital stays in Australia 1993-2005 Prepared by Amanda Rxburgh and Luisa Degenhardt, Natinal Drug and Alchl Research Centre Funded by the Australian Gvernment Department f Health and Ageing
Drug-related hspital stays in Australia 1993-2005 Prepared by Amanda Rxburgh and Luisa Degenhardt, Natinal Drug and Alchl Research Centre Funded by the Australian Gvernment Department f Health and Ageing
ACSQHC National Consensus Statement: Essential Elements for High Quality End-oflife Care in Acute Hospitals.
 27 March 2014 Prfessr Debra Picne Chief Executive Officer Australian Cmmissin n Safety and Quality in Health Care c/ Ms Jennifer Hill, Senir Prject Officer Level 5, 255 Elizabeth Street SYDNEY NSW 2000
27 March 2014 Prfessr Debra Picne Chief Executive Officer Australian Cmmissin n Safety and Quality in Health Care c/ Ms Jennifer Hill, Senir Prject Officer Level 5, 255 Elizabeth Street SYDNEY NSW 2000
Safety of HPV vaccination: A FIGO STATEMENT
 FIGO Statement n HPV Vaccinatin Safety, August 2nd, 2013 Safety f HPV vaccinatin: A FIGO STATEMENT July, 2013 Human papillmavirus vaccines are used in many cuntries; glbally, mre than 175 millin dses have
FIGO Statement n HPV Vaccinatin Safety, August 2nd, 2013 Safety f HPV vaccinatin: A FIGO STATEMENT July, 2013 Human papillmavirus vaccines are used in many cuntries; glbally, mre than 175 millin dses have
Osteoporosis Fast Facts
 Osteprsis Fast Facts Fast Facts n Osteprsis Definitin Osteprsis, r prus bne, is a disease characterized by lw bne mass and structural deteriratin f bne tissue, leading t bne fragility and an increased
Osteprsis Fast Facts Fast Facts n Osteprsis Definitin Osteprsis, r prus bne, is a disease characterized by lw bne mass and structural deteriratin f bne tissue, leading t bne fragility and an increased
Benefits for Anesthesia Services for the CSHCN Services Program to Change Effective for dates of service on or after July 1, 2008, benefit criteria
 Benefits fr Anesthesia Services fr the CSHCN Services Prgram t Change Effective fr dates f service n r after July 1, 2008, benefit criteria fr anesthesia will change fr the Children with Special Health
Benefits fr Anesthesia Services fr the CSHCN Services Prgram t Change Effective fr dates f service n r after July 1, 2008, benefit criteria fr anesthesia will change fr the Children with Special Health
Architecture for Research Computing in Health (ARCH) Using i2b2 to Find Patient Cohorts of Interest
 Using i2b2 to Find Patient Cohorts of Interest") Architecture fr Research Cmputing in Health (ARCH) Using i2b2 t Find Patient Chrts f Interest T access i2b2, please visit https://i2b2.med.crnell.edu/webclient/ and lgin with yur CWID and passwrd. T request
Architecture fr Research Cmputing in Health (ARCH) Using i2b2 t Find Patient Chrts f Interest T access i2b2, please visit https://i2b2.med.crnell.edu/webclient/ and lgin with yur CWID and passwrd. T request
Nonclinical factors associated with premature termination of adjuvant chemotherapy for stage I-III breast cancer
 Nnclinical factrs assciated with premature terminatin f adjuvant chemtherapy fr stage I-III breast cancer Xia-Cheng Wu, Trevr Thmpsn, Meichin Hsieh, Meijia Zhu, Patricia Andrews, Michelle Lch, Timthy Styles,
Nnclinical factrs assciated with premature terminatin f adjuvant chemtherapy fr stage I-III breast cancer Xia-Cheng Wu, Trevr Thmpsn, Meichin Hsieh, Meijia Zhu, Patricia Andrews, Michelle Lch, Timthy Styles,
Improving Surveillance and Monitoring of Self-harm in Irish Prisons
 HSE Mental Health Divisin Stewart s Hspital, Palmerstwn, Dublin 20 Tel: 01 6201670 Email: inf@nsp.ie www.nsp.ie Imprving Surveillance and Mnitring f Self-harm in Irish Prisns Prject Scpe Dcument 8 th June
HSE Mental Health Divisin Stewart s Hspital, Palmerstwn, Dublin 20 Tel: 01 6201670 Email: inf@nsp.ie www.nsp.ie Imprving Surveillance and Mnitring f Self-harm in Irish Prisns Prject Scpe Dcument 8 th June
Meaningful Use Roadmap Stage Edition Eligible Hospitals
 Meaningful Use Radmap Stage 1-2011 Editin Eligible Hspitals CPSI is dedicated t making yur transitin t Meaningful Use as seamless as pssible. Therefre, we have cme up with a radmap t assist yu in implementing
Meaningful Use Radmap Stage 1-2011 Editin Eligible Hspitals CPSI is dedicated t making yur transitin t Meaningful Use as seamless as pssible. Therefre, we have cme up with a radmap t assist yu in implementing
2017 CMS Web Interface
 CMS Web Interface PREV-13: Statin Therapy fr the Preventin and Treatment f Cardivascular Disease Measure Steward: CMS Web Interface V1.1 Page 1 f 27 12/15/2016 Cntents INTRODUCTION... 4 WEB INTERFACE SAMPLING
CMS Web Interface PREV-13: Statin Therapy fr the Preventin and Treatment f Cardivascular Disease Measure Steward: CMS Web Interface V1.1 Page 1 f 27 12/15/2016 Cntents INTRODUCTION... 4 WEB INTERFACE SAMPLING
FDA Dietary Supplement cgmp
 FDA Dietary Supplement cgmp FEBRUARY 2009 OVERVIEW Summary The Fd and Drug Administratin (FDA) has issued a final rule regarding current gd manufacturing practices (cgmp) fr dietary supplements that establishes
FDA Dietary Supplement cgmp FEBRUARY 2009 OVERVIEW Summary The Fd and Drug Administratin (FDA) has issued a final rule regarding current gd manufacturing practices (cgmp) fr dietary supplements that establishes
2018 CMS Web Interface
 CMS Web Interface PREV-13: Statin Therapy fr the Preventin and Treatment f Cardivascular Disease Measure Steward: CMS CMS Web Interface V2.1 Page 1 f 27 06/25/ Cntents INTRODUCTION... 4 CMS WEB INTERFACE
CMS Web Interface PREV-13: Statin Therapy fr the Preventin and Treatment f Cardivascular Disease Measure Steward: CMS CMS Web Interface V2.1 Page 1 f 27 06/25/ Cntents INTRODUCTION... 4 CMS WEB INTERFACE
Commissioning Policy: South Warwickshire CCG (SWCCG)
") Cmmissining Plicy: Suth Warwickshire CCG (SWCCG) Treatment Indicatin Criteria FreeStyle Libre Flash Cntinuus Glucse Mnitring System Type I Diabetes Prir apprval must be requested frm the Individual Funding
Cmmissining Plicy: Suth Warwickshire CCG (SWCCG) Treatment Indicatin Criteria FreeStyle Libre Flash Cntinuus Glucse Mnitring System Type I Diabetes Prir apprval must be requested frm the Individual Funding
PROCEDURAL SAFEGUARDS NOTICE PARENTAL RIGHTS FOR PRIVATE SCHOOL SPECIAL EDUCATION STUDENTS
 PROCEDURAL SAFEGUARDS NOTICE PARENTAL RIGHTS FOR PRIVATE SCHOOL SPECIAL EDUCATION STUDENTS INTRODUCTION This ntice prvides an verview f the parental special educatin rights, smetimes called prcedural safeguards
PROCEDURAL SAFEGUARDS NOTICE PARENTAL RIGHTS FOR PRIVATE SCHOOL SPECIAL EDUCATION STUDENTS INTRODUCTION This ntice prvides an verview f the parental special educatin rights, smetimes called prcedural safeguards
Mental Health Statistics Improvement Plan (MHSIP) Consumer Survey
 Consumer Survey") Mental Health Statistics Imprvement Plan (MHSIP) Cnsumer Survey Annual Reprt FY2014 This reprt was prepared by: Adrienne Jnes, M.A., Researcher Data and Evaluatin, Cmmunity Prgrams Office f Behaviral Health,
Mental Health Statistics Imprvement Plan (MHSIP) Cnsumer Survey Annual Reprt FY2014 This reprt was prepared by: Adrienne Jnes, M.A., Researcher Data and Evaluatin, Cmmunity Prgrams Office f Behaviral Health,
Statement of Work for Linked Data Consulting Services
 A. Backgrund Infrmatin Statement f Wrk fr Linked Data Cnsulting Services The Natinal Library f Medicine (NLM), in Bethesda, Maryland, is a part f the Natinal Institutes f Health, US Department f Health
A. Backgrund Infrmatin Statement f Wrk fr Linked Data Cnsulting Services The Natinal Library f Medicine (NLM), in Bethesda, Maryland, is a part f the Natinal Institutes f Health, US Department f Health
Hospital Preparedness Checklist
 Hspital Preparedness Checklist http://pandemicflu.gv Preparedness Subject 1. Structure fr planning and decisin making An internal, multidisciplinary planning cmmittee fr influenza preparedness has been
Hspital Preparedness Checklist http://pandemicflu.gv Preparedness Subject 1. Structure fr planning and decisin making An internal, multidisciplinary planning cmmittee fr influenza preparedness has been
Physical Fitness for the Physically Limited. o Work Experience, General. o Open Entry/Exit. Distance (Hybrid Online) for online supported courses
 for online supported courses") SECTION A - Curse Infrmatin 1. Curse ID: 2. Curse Title: 3. Divisin: 4. Department: 5. Subject: 6. Shrt Curse Title: 7. Effective Term:: KINL 2 Physical Fitness fr the Physically Limited Kinesilgy & Athletics
SECTION A - Curse Infrmatin 1. Curse ID: 2. Curse Title: 3. Divisin: 4. Department: 5. Subject: 6. Shrt Curse Title: 7. Effective Term:: KINL 2 Physical Fitness fr the Physically Limited Kinesilgy & Athletics
WHAT IS HEAD AND NECK CANCER FACT SHEET
 WHAT IS HEAD AND NECK CANCER FACT SHEET This infrmatin may help answer sme f yur questins and help yu think f ther questins that yu may want t ask yur cancer care team; it is nt intended t replace advice
WHAT IS HEAD AND NECK CANCER FACT SHEET This infrmatin may help answer sme f yur questins and help yu think f ther questins that yu may want t ask yur cancer care team; it is nt intended t replace advice
National Hospital Inpatient Quality Reporting Measures Specifications Manual Release Notes
 Natinal Hspital Inpatient Quality Reprting Measures Specificatins Manual Release Ntes Fr Manual Versin: 5.3 Cmpleted: June 15, 2017 Guidelines fr Using Release Ntes The Release Ntes prvides mdificatins
Natinal Hspital Inpatient Quality Reprting Measures Specificatins Manual Release Ntes Fr Manual Versin: 5.3 Cmpleted: June 15, 2017 Guidelines fr Using Release Ntes The Release Ntes prvides mdificatins
Dear Student, IMMUNIZATION RECORD INSTRUCTIONS
 Dear Student, Welcme t the University f Chicag! The State f Illinis and University regulatins require students t prvide prf f required immunizatins prir t registratin fr classes. In rder t cmplete this
Dear Student, Welcme t the University f Chicag! The State f Illinis and University regulatins require students t prvide prf f required immunizatins prir t registratin fr classes. In rder t cmplete this