Myelodysplastic Neoplasms. Myelodysplastic Neoplasms Con t
|
|
|
- Jemima Cannon
- 5 years ago
- Views:
Transcription
1 Myelodysplastic Neoplasms Found primarily in patients older than 50 years Characterized by indolence, peripheral p cytopenias, hypercellular marrow, less than 20% blasts, and varying amounts and degrees of dysplasia in at least 2 cell lines Oval macrocytes, bizarre giant platelets and dysplastic myeloid cells characterize dysplasia. Thrombocythemia is often found Myelodysplastic Neoplasms Con t MDS is associated with a common mutant defective stem cell. Cytogenetic studies usually demonstrate chromosomal aberrations. The most common is -5, -7, 7q and trisomy 8 A high percentage of the MDS patients (app. 40%) will terminate in AML Treatment is infusion with blood growth factors, such as G-CSF or GM-CSF. The use of these drugs usually results in normal maturation of the malignant dysplastic clone, with relatively normal functionability. 2
2 Myelodysplastic Neoplasms Con t Treatment is infusion with G-CSF or GM-CSF. These drugs usually results in normal maturation of the dysplastic clone, with relatively normal functionability. The function of these drugs in the maturing cells is to increase chemotaxis enhance phagocytosis increase cytotoxic killing improve responsiveness to antigens Myelodysplastic Neoplasms Refractory anemia with unilineage dysplasia(ra) Refractory anemia with ringed sideroblasts (RARS) Refractory cytopenia with multilineage dysplasia Refractory anemia with multilineage dysplasia and ringed sideroblasts (RAMD-RS) Refractory Anemia with Excess of Blasts (RAEB) RAEB 1 (5-9 blasts) RAEB 2 (10-19 blasts MDS unclassified MDS associated with 5q- syndrome Childhood myelodysplastic syndrome Refractory cytopenia of childhood 3
3 Factors Indicating Poor Prognosis > 5% bone marrow blasts and circulating CD34+ cells Abnormal karyotypes and ineffective erythropoiesis with, < 20% ring sideroblasts Less than 1,000 x 103/µL granulocytes, thrombocytopenia (<140 x 103/µL) decreased monocytes hemoglobin less than 9.0g/dL Previous exposure to radiation or chemotherapy Peripheral Blood Bone Marrow Refractory Anemia (RA) Normochromic/macrocytic Normo - hypercellular Median Survival ~ 47 mo. <1% blasts Variable dyserythropoiesis decreased reticulocytes Normal granulocytes and mild anemia megakaryocytes. <5% blasts <15% ringed sideroblasts Refractory Anemia < 1% blasts Ringed sideroblasts account with Ringed Sideroblasts Dimorphic RBCs for >15% of all nucleated (RARS) Hypochromic macrocytes with marrow cells Pappenheimer bodies Dyserythropoiesis Median Survival ~ 52 mo. Mild to severe anemia < 5% blasts Refractory Cytopenias with Variable amounts of dysplasia Dysplasia in 10% of cells Multilineage dysplasia (RCMD) in 2+ lineages <5% blasts <1%blasts <15%ringedsideroblast Refractory Cytopenia with Variable amounts of dysplasia Variableamountsofdysplasia multilineage dysplasia and in 2+ lineages in 2+ lineages ringed Sideroblasts (RCMD-RS). < 1% blasts 15% ringed sideroblast Cytopenias <5% blasts Refractory Anemia Variable cytopenias. Normo hypercellular 5-9% Blasts with Excessive Blasts (RAEB 1) Severe dysplasia Uni or multilineage dysplasia Refractory Anemia with Same as above except Normo hypercellular, with Excessive Blasts (RAEB ll) 5 19% blasts granulocytic hyperplasia Uni or multilineage dysplasia 10-19% blasts Myelodysplastic Syndrome Cytopenias Unilineage dysplasia Unclassified (MDS-U) >1% blasts < 5% blasts MDS Associated with 5q - Anemia Normal to increased Normal to increased plt count dysplastic megakaryocytes <5% blasts <5% blasts Isolated 5q abnormality 4




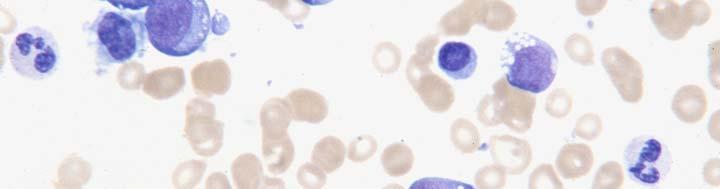
4 Dysplastic RBCs Dysplastic platelets 5






5 Dysplastic granulocytes Hypersegmented Dysplastic PMN 6






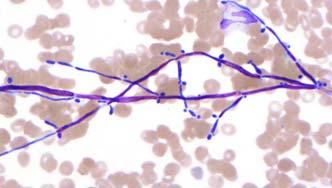
6 Dysplastic RBCs-BONE MARROW Ringed Sideroblasts in MDS 7

7 Dysplastic Grans vs Pelger Huet Hyposegmented usual Occ. Hypersegmented Hyperchromatin Clumping except when hypersegmented Hypogranulated Lymphocytes Normal Hyposegmented Hyperchromatin Clumping Normal Granulation Lymphocyte Hyperclumped PELGER HUET ANOMALY 8


8 DRUG INDUCED DYSPLASIA Dysplastic nucleus, usually round or barely indented Normal to toxic cytoplasmic granulation (depending on therapy) May be confused with a left shifted Pelger Huet Anomaly Patient history important to differentiate 9
")


9 Chronic Myeloproliferative Neoplasms Chronic Myelogenous Leukemia (CML) Polycythemia Vera (PV) Idiopathic Myelofibrosis Essential Thrombocythemia (ET) Chronic MPN, Unclassifiable Chronic Neutrophilic Leukemia Chronic eosinophilic leukemia NOS Mastocytosis 10
10 CML Positive Ph+ chromosomet(9;22) or BCR/C-ABL gene rearrangement characterized by a marked leukocytosis Symptomology when white counts above 50 x 109/L Increase in mature and immature cells of the granulocytic series, including both eosinophils and basophils, thrombocytosis, splenomegaly ( most likely due to extramedullary hematopoiesis) and the presence of the Ph1 chromosome t(9:22) CML con t Normocytic normochromic anemia, if present Platelets counts can rise to 800K/dL, although thrombocytopenia is not uncommon. Occasional giant forms may be seen. The higher the white count, the lower the platelets, due to "squeezing" out of marrow megakaryocytes by extremes in granulocytic hyperplasia. 11

 >20% (blastic phase, PB or BM)")

11 Differential in CML Differential results usually approach the following figures. blasts: 1-5%; (chronic phase, PB and BM) >5 <20% (accelerated phase, PB and BM) >20% (blastic phase, PB or BM) promyelocytes: 1-10% myelocytes: 10-20% metamyelocytes: 10-30% bands: 20-40% neutrophils: 30-50% eosinophils: 2-15% ( with young forms present) basophils 2-10% normoblasts: 2-4%. CML 12
12 Prognosis of CML Blast transformation is usual course of the disease. Transformation may be of myeloid, lymphoid or megakaryocytic type. 1/3 of cases will transform into pre-b ALL. Prognosis for remission, in this case, is better, since patients often have a good response to vincristine and prednisone therapy. However, this remission is short- lived, and relapse is usually of fthe AMLtype, with ithlittle response to therapy. AML transformation is also non-responsive to conventional myeloid therapy. Prognosis of CML con t The drug having the most promising effects is Gleevac. Most efficient in early to mid stage CML. Not much promise with patients in accelerated phase or blast transformation. Hydroxyurea and plasmaphoresis used when WBC exceptionally high. The only real cure is a successful bone marrow transplant. 13
13 Signs of Impending Myeloid Blast Crisis Dysplastic changes of the myeloid line and/or Sudden decrease in the WBC or plt count and/or Increase in the blast count and/or Increasing basophils CML- Early Warning Signs of Impending Acceleration 14



14 CML EARLY ACCELLERATION WHO Criteria for CML in Accelerated Phase PB or BM blasts 10-19% 19% Persistent thrombocytopenia < 100K, not related to treatment Thrombocytosis >1 million, unresponsive to treatment Increasing WBC and spleen size 15



15 CML in Accelerated Phase con t. Evidence of clonal evolution by cytogenetic analysis +Ph, +8, iso(17q), +19 Basophilia >20% in PB Marked dysplasia in granulocytes, or prominent proliferation of dysplastic megakaryocytes associated with marked fibrosis consistent with accelerated phase 16
 > 20% blasts with")


16 CML in AML Transition De Novo (Ph+ AML) > 20% blasts with increased basophils and/or eosinophils > 20% blasts with increase in either normal or abnormal platelets > 20% blasts with Ph+ chromosome. 17






17 CML in AML Transition Lymphoblastic Transition of CML 18





18 Megakaryoblastic Transition Erythroblastic Transition of CML 19
19 WHO Criteria for Dx of Polycythemia Vera Major RBC mass >25% above mean normal predicted value, or Hgb > 18.5 g/dl in men or 16.5 g/dl in women Splenomegaly on palpation Clonal genetic abnormality other than Ph chromosome or BCR/ABL gene in marrow Endogenous erythroid colony formation in vitro Minor Thrombocytoisis i > 400,000/µL000/ WBC > 12,000/µL Panmyelosis with prominent erythroid and megakaryocytic hyperplasia on bone marrow biopsy Low serum erythropoietin levels Clinical Results of P. Vera Iron deficiency results from continual bleeding (due to hypo function of the platelets), repeated therapeutic phlebotomy, increased erythrocyte production and iron turnover, and decreased red cell survival An iron deficiency state is the desired effect, because it limits how extensively the red cell mass can expand. A greatly expanded red cell mass increases the chance of a thromboembolic episode or hemorrhage. Portal vein thrombosis is a classic presenting symptom. Most obvious change in the peripheral blood of long-term P Vera Most obvious change in the peripheral blood of long-term P Vera patients is appearance of tear drop red cells. This heralds the most common transition of P.Vera, that of increasing myelofibrosis with myeloid metaplasia. At this point, the patient is in the "spent phase" or in the "post-polycythemic myelofibrosis" (PPMF) phase of the disease. 20






20 Polycythemia Vera Post Polycythemic Myelofibrosis 21

21 PPMF s/p Splenectomy Chronic IdiopathicMyelofibrosis Associated with 13q ; t(1;13) Clonal chronic myeloproliferative disorder Found mostly in older people Found on rare occasion in children, both as a primary idiopathic disease, or secondary to acute leukemia Closely related to the other myeloproliferative diseases All of the other chronic myeloproliferative disorders can have varying amounts of fibrosis as a secondary complication. Myeloid metaplasia means there are marrow cells produced in hematopoietic sites outside the marrow. This is also referred to as extra medullary hematopoiesis. 22
22 Idiopathic Myelofibrosis con t The sites that can form hematopoietic elements are the same tissues that form blood cells in utero, such as the liver, spleen and reticuloendothelial system. Many tear drops are present, a significant ifi finding in patients t with normocytic, normochromic anemia, and should alert the technologist to search for conclusive evidence of myeloid metaplasia. Examination of the blood film usually reveals at least one other pathological finding: an occasional nucleated red blood cell, an abnormal giant agranular platelet, a rare megakaryocyte fragment, and occasional immature myeloid cell, including a rare myeloblast. Note, that although a slight reticulocytosis may be found, it is usually out of proportion to the number of nucleated red blood cells found. This is especially true as the disease progresses, indicating ineffective erythropoiesis. Idiopathic Myelofibrosis Con t Blood counts may demonstrate an increase or decrease in the number of WBCs and platelets. A mild anemia may be present, but is usually normocytic ocyt c normochromic. oc o c Occasionally, a microcytic anemia is found, usually in patients with repeated episodes of G.I. bleeding. These patients usually have abnormal coagulation studies. As diseases progresses NRBCs immature As diseases progresses, NRBCs, immature granulocytes (including myeloblasts), megakaryocytic fragments and micromegakaryocytes increase. Patients may become severely thrombocytopenic with increasing splenic sequestration, or the platelet count may become abnormally high, with giant and bizarre forms. 23
23 Idiopathic Myelofibrosis con t Splenectomy is usually palliative, and done when symptomatology dictates. Prognosis is grave, and eventually patients die from complications of total marrow failure. This failure usually results in hemorrhage, infections, or cardiac complications. Approximately 5-8% terminate in acute myeloid leukemia (M1 type) or megakaryocytic leukemia (M7 type). 3 Things Needed to Prove CIMF in Peripheral Blood Tear drop RBCs in a normocytic normochromic anemia Giant and bizarre platelets A leukoerythroblastic blood picture, preferably with at least 1 blast 24

24 Chronic Idiopathic Myelofibrosis Myelophthistic Anemia Is a non hematopoietic tumor in the marrow Associated with a leukoerythroblastic blood picture Only tumors that can cause compensatory extramedulary hematopoiesis will have tear drops. They most commonly are Breast Prostate Bladder 25
25 Essential Thrombocythemia Associated with variable chromosomal aberrations Chronic myeloproliferative disease characterized by a thrombocytosis in excess of 1 x10 12 /L. (1 million). Closely related to polycythemia vera, the major difference is that polycythemia vera is an increase in the total red cell mass; and essential thrombocythemia is an increase in the total platelet mass. Hgb must be <13 gms Most striking element is the persistence of a marked thrombocytosis, with platelet counts reaching greater than one million. On rare occasions, platelet counts reach levels of fourteen million. Essential Thrombocythemia, con t Spontaneous aggregation of platelets that have an abnormal function. Large masses of platelet aggregates seen on the blood film, with abnormal appearing giant and bizarre forms, some normal immature forms, many small forms, and an occasional megakaryocyte fragment. Gastrointestinal hemorrhage is a common risk with these patients, and is often the cause of death. Patients whose hemorrhagic tendencies have been kept under control, run the risk of an acute leukemia transformation (5-10% of cases), the most common of which is transformation to acute myelogenous leukemia. Transformation into acute lymphocytic or megakaryocytic leukemia has the same probability as the patients with CML. Treated with hydroxyurea or the newest drug, Anagrelide, which is specific for megakaryocytes. 26



26 Essential Thrombocythemia CMPD - Unclassifiable Have all characteristics of a CMPD but fail to meet any specific criteria of a specific CMPD Usually have initial stages of PV, Pre fibrotic CIMF, or ET but characteristic features are missing No Philadelphia chromosome or BCR/Fusion gene No basophilia or dysplasia No signs of reactive myelopoiesis or thrombopoiesis are present It is essential to determine which specific CMPD is present, once the distinction becomes obvious, because of prognostic and therapeutic differences. 27



27 CMPD - U Chronic Neutrophilic Leukemia Rarest of the chronic myeloproliferative disease Most obvious finding is the persistence of neutrophils and bands, without t evidence of increased left shifting, and an absence of sepsis and/or fever. Toxic granulation and Döhle bodies are present Rarely, a nucleated red blood cell may be found. White blood counts may go as high as 100 x 10 9 /L, with a normal to slightly decreased platelet count, and a mild anemia. 28



28 CNL con t Hemoglobin is approximately 11 g/dl. LAP scores are extremely high, ranging from Markedly elevated B12 and B12-binding capacity is common Bone marrow shows normal maturing myeloid hyperplasia There is tissue infiltration ti with mature PMNs Hepatosplenomegaly No evidence of another myeloproliferative disorder or myelodysplastic syndrome CNL 29
29 Chronic Eosinophilic Leukemia Persistent eosinophilia 1.5 x 109/L in blood and increased in bone marrow. Hypercellular marrow <20% blasts in bone marrow, fibrosis in some cases Clonality of the eosinophils must be proved Exclude all other causes of eosinophilia: Reactive (allergy, parasites, infectious diseases, pulmonary diseases such as Loeffler s, and collagen diseases) Neoplastic disorders with secondary eosinophilia Neoplastic disorders in which eosinophils are a part of the neoplastic clone (other myeloproliferative disorders Taken from WHO Classification of Tumors - Diagnostic criteria of chronic eosinophilic leukemia Chronic Eosinophilic Leukemia 30






30 Loeffler Syndrome Also called Simple Pulmonary Eosinophilia Often caused by Ascarid infections Does well without treatment. If not can treat with anti allergens or anti parasitic drugs Marked peripheral eosinophilia, often with signs of degranulation Loeffler Endocarditis Prominent eosinophilic infiltration in tissues, such as heart, lungs, skin and CNS causing severe organ damage. 31
31 Transitions in the Chronic Myeloproliferative Disorders Myelofibrosis with Myeloid Metaplasia (Secondary) Chronic Myeloid Leukemia Polycythemia Vera 30% 20% AML (De Novo) ACUTE MYELOCYTIC LEUKEMIA Aplastic Anemia Acute Lymphocytic Leukemia Essential Thrombocythemia Paroxysmal Nocturnal Hemoglobinuria Myelodysplastic Syndromes and SML Agnogenic Myeloid Metaplasia (Primary) Frequent Infrequent Myelodysplastic/Myeloproliferative Atypical CML (acml) Juvenile CMML (jcmml) Chronic Myelomonocytic y Leukemia (CMML) Myeloproliferative/myelodysplastic neoplasm, unclassifiable 32
32 MDS/CMPD Peripheral Blood Bone Marrow Chronic Myelomonocytic Persistent monocytosis of Increase in dysplastic monos Leukemia (CMML) >1x109/L for 3 or more months <20% blasts Variable dysgranulopoiesis. Variable dysgranulopoiesis <5% blasts More aggressive forms may Monos appear mature but have Auer rods in marrow Median Survival dysplastic myeloblasts highly variable CMML - 1 = <5% blasts <10% in bone marrow CMML - 2 = 5-19% blasts 10-19% in bone marrow Atypical CML (acml) Granulocytic Leukocytosis Neg for Ph+ and BCR/ABL Marked dysplasia in granulocytes Dysplastic granulocytic No monocytosis hyperplasia No Basophilia Variable dysplasia in erythroid or megakaryocytic line. < 20% blasts Juvenile CMML (jcmml) Monocytosis of >1x109/L Blasts < 20% (includes Blasts < 20% (includes promonocytes) promonocytes) Neg for Ph+ and BCR/ABL Increase in immature grans Common for monosomy 7 WHO Criteria for CMML Persistent blood monocytosis >1000/µL Negative Philadelphia chromosome and BCR/ABL fusion gene. <20% *blasts in blood or bone marrow Usually have multilineage dysplasia; if not then other requirements are necessary Acquired cytogenetic abnormality in bone marrow cells or Monocytosis persistent for at least 3 months and All other causes of monocytosis has been eliminated. *Blasts include myeloblasts, promonoytes and monoblasts. 33



33 WHO Criteria for jmml Abnormal granulocytes and monocytes (promonocytes are equivalent to blasts Monocytes >1000/µL, with blasts and promonocytes < 20% in blood and marrow Philadelphia chromosome and BCR/ABL fusion gene negative Plus 2 or more of the following Hgb F increased for age Immature granulocytes in blood WBC > 10,000/µL. 000/µL Clonal chromosomal abnormality often monosomy 7 GM-CSF hypersensitivity of myeloidprogenitors in vitro Taken from WHO Classification of Tumors - Diagnostic criteria of juvenile myelomonocytic leukemia. CMML 34



34 Atypical CML (acml) Leukemic disorder that has both myelodysplastic and myeloproliferative features Leukocytosis with mature and immature granulocytes Dysplastic features often seen in all 3 lines Basophilia is absent Philadelphia l chromosome and/or BCR/ABL fusion gene absent Found in older people median age is 7 th to 8 th decade Hepatosplenomegaly is common acml 35
35 Acute Myeloid Leukemia (NOS AML (M0) with minimal differentiation AML (M1) no maturation AML (M2) with maturation AML (M4) myelomonocytic AML (M5) monocytic AML (M6) erythrocytic AML (M7) megakaryocytic Acute Basophilic Leukemia Acute Panmyelosis with Myelofibrosis Myeloid Sarcoma Acute Leukemia of Ambiguous Lineage Undifferentiated acute leukemia Biclonal acute leukemia Biphenotypic acute leukemia 36
36 Acute Myeloid Leukemia with Recurrent Cytogenetic AML with maturation t(8;21) AML with abnormal BM eosinophils (inv)16 Acute promyelocytic leukemia AML with 11q23 (MLL) abnormalities t(15;17) AML with inversion 3 (inv 3) AML with multilineage dysplasia AML and MDS syndromes, therapy related Factors predicting a poor prognosis >than 5% bone marrow blasts Abnormal karyotypes Less than 1,000 x 103/µL granulocytes Thrombocytopenia (<140 x 103/µL) Decreased monocytes 37
37 Factors predicting a poor prognosis (con t) Ineffective erythropoiesis Hemoglobin less than 9.0g/dL Previous exposure to radiation or chemotherapy Less than 20% ring sideroblasts in bone marrow Circulating blasts and circulating CD34+ cells. AML Minimally Differentiated No evidence of myeloid differentiation by morphology or microscopic cytochemistry Diagnosed by immunophenotyping with positivity for CD34, CD38 and DR. Also express pan-myeloid antigens of CD13, CD33 and CD117. Very poor prognosis 38
 Blasts >90% of non erythroid")


38 Minimally Differentiated AML AML (M1) Blasts >90% of non erythroid cells in the marrow with no maturation. Several of the Blasts may be type l or ll blasts Auer rods may be seen Special stains = MPO + NSE - 39



39 AML (M1) AML with Maturation (M2) >20% marrow blasts with maturation seen in blood or bone marrow Auer rods may be present Type ll and lll blasts are common. Promyelocytes, myelocytes, and mature neutrophils make up >10% of marrow cells Dysplasia in the myeloid line may be seen. Special stains = MPO + NSE - 40



40 AML with Maturation (M2) Acute Myelomonocytic Leukemia (M4) Both myeloblasts and monoblasts present, with some maturation in both lines. Special stains = MPO + NSE + in bone marrow and blood Maturation appears dysplastic Bone marrow morphologically, tends to appear more myeloid than monocytic; monocytic element and their precursors + neutrophils and their precursors exceeds 20% of nucleated cells in marrow. Cytogenetics = abnormalities involving chromosome 11. Inv(3) seen with normal to increased plts. 41
.")

41 Acute Myelomonocytic Leukemia (M4) Acute Monocytic Leukemia >80% of marrow cells are monoblasts, promonocytes, and some monocytes. WHO separates the monoblastic leukemias and monocytic leukemias listed under one heading, similar to FAB. In monoblastic leukemias, the majority of the monocytic cells are monoblasts (>80%).This is the FAB M5A. In the acute monocytic leukemias, the majority of monocytic cells are promonocytes. This is the FAB M5B. Monoblasts very large with abundant cytoplasm, sometimes with pseudopod formation. May have few azurophilic granules and vacuoles. They have a round nucleus with delicate lacey chromatin. Large nucleoli. Convolutions are not seen Promonocytes more irregular than the blast, with delicate convolutions. Nucleoli may be seen. Vacuoles and azurophilic granules are more obvious. Smaller nucleoli than in blast. 42






42 Acute Monoblastic Leukemia Acute Monocytic Leukemia 43


.")
43 Acute Erythroid Leukemia Greater than 50% erythroblasts and 20% myeloblasts in the marrow. Anemia is often severe Peripheral blood may have blood picture identical to MDS patients with more extreme RBC changes. Patient is often pancytopenic. This actually is a three stage disease, starting out as an erythroid leukemia, slowly transforming to an intermediate stage with an increase in myeloblasts, and finally terminating into a phase indistinguishable from acute myeloid leukemia (M1). This is probably not an acute leukemia de novo, but a rapid transformation from a myelodysplastic syndrome. Acute Erythroid Leukemia 44

44 Pure Erythroblastic Leukemia Referred to in the past as erythemic myelosis This is a pure erythroblastic leukemia. Leukopenia, marked anemia and thrombocytopenia are the classic signs, with either increased or decreased numbers of proerythroblasts in the peripheral blood. The bone marrow is hypercellular, with a marked increase in promegaloblastoid cells. There is a marked decrease in both myeloid and megakaryocytic elements. This is the rarest of the myeloid leukemias, with a life expectancy of approximately 5-8 weeks. Pure Erythroblastic Leukemia 45
45 Acute Megakaryocytic Leukemia Acute myelosclerosis is similar to M7, however it does not have the trilineage dysplasia. Megakaryoblasts have basophilic cytoplasm, some of which show cytoplasmic blebbing and vacuoles Bizarre platelets may be present with exact morphology as the megakaryoblast cytoplasm. Micromegakaryocytes may be present Bone marrow is often fibrotic Acute Megakaryocytic Leukemia con t If associated with abnormal chromosome 3, patient often appears normal shortly before the acute phase The acute leukemia presents with normal to increased numbers of giant and bizarre platelets Appears to have a poorer prognosis than the other myeloid leukemias CD61 positive. Should be proven with slide immunophenotyping 46

46 Acute Megakaryocytic Leukemia Transient Megakaryocytic Leukemia of Downs Syndrome (TMPD) Children born with Downs Syndrome Severe granulocytopenia and thrombocytopenia Megakaryoblastic leukemia in blood and bone marrow Disappears at approximately 3 months of age. Stands a high probability of returning as AML at 3-5 years of age. 47


47 ACUTE BASOPHILIC LEUKEMIA < 1% of all AML cases Could be de novo or transition from other BCR/ABL + CML All other features of AML are present May show signs of some lytic lesions, cutaneous involvement, organomegaly, g and symptoms usually related to hyperhystaminemia Positive for toluidine blue positive.\ 48



48 Acute Leukemia of Ambiguous Lineage Undifferentiated acute leukemia Biclonal acute leukemia Biphenotypic acute leukemia 49






49 AML NOS Biphenotypic AML/T-Cell ALL 50
50 Acute Myeloid Leukemia with Recurrent Cytogenetic Abnormalities AML with maturation t(8;21) AML with abnormal BM eosinophils (inv)16 Acute promyelocytic leukemia AML with 11q23 (MLL) abnormalities AML with inv (3) AML with multilineage dysplasia t(15;17) AML and MDS syndromes, therapy related AML t(8;21) This is the most common translocations in AML Associated with good response to chemotherapy and with high complete remission and long term disease free survival The presence of CD56 expression and other karyotypic abnormalities affect survival The only acute myeloid leukemia that can have blasts below 20% and still be considered an acute leukemia, as long as t(8;21) is present 51


 is blasts containing very large salmon colored")
51 AML t(8;21) con t Contain large blasts and promyelocytes with abundant granules. Dysplasia in the maturing granulocytes often seen in the blood Promyelocytes have a distinct Golgi Single Auer Rods often found that are long and sharp with tapered ends The single feature that distinguishes a t(8;21) is blasts containing very large salmon colored granules. Often find increased numbers of normal eosinophils AML t(8;21) 52



52 AMML Eo inv(16) AML with features of myeloid and monocytic differentiation Good prognosis, with high rates of complete remission when treated with cytarabine in the consolidation phase Increased numbers of eosinophils in all stages. Immature eosinophils contain not only large eosinophilic granules, but also varying numbers of large purple to black granules. Granules of some eosinophils sometimes so dense, the morphology of nucleus is obscured ASD chloracetate esterase, usually negative in normal eosinophils is characteristically faintly positive in these eosinophils. AML EOS (inv 16) 53
53 Acute Promyelocytic Leukemia t(15;17) AML with a predominence of abnormal microgranular, hypogranular, or rarely hypergranular promyelocytes Distinct nuclear shapes, with bi-nucleate and butterfly forms Variable numbers of azurophilic granules in the microgranule variant to sub microscopic granules in the hypogranular variant Bundles of Auer rods (faggot cells) often present Gene Rearrangement Findings Associated with t(15;17). There is a breakpoint on chromosome 17 in the region of the retinoic acid receptoralpha (RAR-a) Present chemotherapy - this receptor, (RAR-a), has been shown to be involved with growth and differentiation of myeloid cells in vitro, and treatment with All Transretinoic Acid (ATRA) induces complete remission Response to this therapy shows: maturation of leukemic cells during initial induction and remission achieved with low morbidity Complications of DIC are possibly related to release of granules during treatment Patients with the occ. T(11;17) do not respond to ATRA therapy 54


54 A new therapy now in clinical trials is Is called Tamibarotene It s a synthetic retinoid It is approximately ten times more potent than ATRA in inducing cell differentiation and apoptosis in vitro Acute Promyelocytic Leukemia t(15;17) 55


55 M1 with Inversion 3 Characterized with giant and bizarre platelets l t in blood. No other dysplasia present Bone marrow shows increased uninuclear and binuclear megakaryocytes 56



56 AML with Myelodysplastic Changes Non Malignant and Toxic Conditions May Hegglin Anomaly Muccopolysacharide Disorders Chediak-Higashi Disorder Parvo virus B19 Infection Bacterial, Fungal, Parasitic Infections Histoplasmosis 57
 found in PMNs, eos, basos, monos, and rarely lymphs.")


57 May Hegglin Anomaly Transmitted as autosomal dominant. Giant Döhle-like bodies (crescent shaped) found in PMNs, eos, basos, monos, and rarely lymphs. These Döhle - like bodies probably represent alterations in RNA. Moderate thrombocytopenia, with giant bizarre platelets, having abnormal thromboplastic function. It is important to recognize the bizarreness of the platelets. Sometimes they are agranular, but often have abnormal granules centrally located in an adentritic platelet. l t Patients rarely have spontaneous bleeding tendencies, but have excess bleeding even after minor trauma. May Hegglin Anomaly 58






58 Muccopolysacharidosis Chediak Higashi Syndrome 59
59 PARVOVIRUS B19 INFECTION Parvovirus B19 is the only known human pathogenic parvovirus asymptomatic in the non immunocompromised in patients infected during hemolytic crisis episode, a marked, but transient, erythroid aplasia can occur due to failure of erythroid line to mature beyond proerythroblast stage. In patients infected during a hemolytic crisis episode, a marked, but transient, erythroid aplasia can occur due to failure of the erythroid line to mature beyond the proerythroblast stage. This viral cytopathology is only evident in the erythroid line PARVOVIRUS B19 con t Infection creates an inability of the pronormoblast to mature beyond the pronormoblastic stage Studies demonstrate that it s essential for RBCs to have a specific cellular receptor before viral infection can occur. It is proposed that the receptor for infection with parvovirus B19 is the erythrocyte P antigen Marrow pronormoblasts have a giant appearance, with smooth chromatin pattern with intense cytoplasmic RNA staining. There are characteristic large pink to lilac intranuclear inclusions present 60






60 PARVOVIRUS B19 INFECTION Bacterial, Fungal and Parasitic Infections E. Coli Candida Yeast Hyphae Erlichiosis 61










61 Histoplasmosis Spirochetes Babesia Malaria 62
62 References Bareford D, Jacobs B: Chronic neutrophilic leukemia. Am J ClinPath 73 : 837, 1980 Beutler E; Paroxysmal nocturnal hemoglobinuria. in Williams WJ Beutler E, Erslev AJ, Lichtman MA, Hematology; 4th ed. ch 20 pp , Mcgraw-Hill, N.Y Brown KE, Anderson SM, Young NS. Erythrocyte P antigen: cellular receptor for B19 parvovirus. Science 262: Coiffer B, Adeline P, Gentilhomme O, et al. Myelodysplastic syndromes: a multiparametric study of prognostic factors in 336 patients. Cancer; 60: Feremans W, Marceles L, Ardichvili D: CNL with enlarged lymph nodes and lysozyme deficiency. Am J Clin Pathol 36: , 1983 George TI, Arber DA. Pathology of the Myeloproliferative Diseases Hematol Oncol Clin N Am 17(2003) References Jaffe ES, Harris NL, Stein H, Vardiman JS Eds. WHO Classification of Tumours. Pathology & Genetics. Tumours of Haematopoietic and Lymphoid Tissues. IARC Press Krause JR, Penchansky MD, Knisely AS: Morphological Diagnosis of Parvovirus B19 Infection. Arch Pathol Lab Med 116: Feb Mehrotra DA, Winfield DA, Fergusson LH: Cellular l abnormalities and reduced colony-forming cells in chronic neutrophilic leukemia. Acta Hematol 73:47-505, 1985 Pangburn MK, Schreiber RD, Muller-Eberhard HJ: Dysfunction of two erythrocyte membrane proteins in paroxysmal nocturnal hemoglobinuria. Proc Natl Acad Sci USA 80:5430, 1983 Pereira IT: Chronic Myeloproliferative Disorders 2 nd ed; in Lotspeich-Steininger CA, Stiene-Martin EA, Koepke JA; Clinical Hematology, Principles, Procedures, Correlations: ch 35 pp , JB Lippincott Co. Philadelphia, 1992 Shindo T, Sakai C, Shibata A: Neutrophilic leukaemia and blastic crisis. Ann Intern Med 87 : 66, 1977 Spivak JL: Erythrocytosis and Polycythemia. In Fundamentals of Clinical Hematology: 2nd ed, , Philadelphia, Harper & Row,
63 References Sullivan SA, Marsden KA, Lowentha RM, et al. Circulating CD34+ cells: an adverse prognostic factor in the myelodysplastic syndromes. Am J Hematol. 39: Towatare M, Adachi K, Kato H, Saito H: Absence of the human retinoblastoma gene product in the megakaryoblastic crisis i of chronic myelogenous leukemia; Blood, vol 78, 9: , Nov 1, 1991 Woo Y, Weisbrot IM; Chronic Neutrophilic Leukemia; Am J Clin Path; vol 2, pp , Aug You W, Weisbrot IM: Chronic neutrophilic leukemia. Report of 2 cases and review of the literature. Am J ClinPath 72 : ,1978 Young N. Hematologic and hematopoietic consequences of B19 parvovirus infection. Semin Hematol; 25: , 1988 WHO Classification of Tumours of Haematopoietic and Lymphoid Tissues. Eds: Swerdlow SH, Campo E, Harris NH, Jaffe ES, Pileri SA, Stein H, Thiele J, Vardiman JW. International Agency for Research on Cancer; Lyon
Hematology Unit Lab 2 Review Material
 Objectives Hematology Unit Lab 2 Review Material - 2018 Laboratory Instructors: 1. Assist students during lab session Students: 1. Review the introductory material 2. Study the case histories provided
Objectives Hematology Unit Lab 2 Review Material - 2018 Laboratory Instructors: 1. Assist students during lab session Students: 1. Review the introductory material 2. Study the case histories provided
Chronic Idiopathic Myelofibrosis (CIMF)
") Chronic Idiopathic Myelofibrosis (CIMF) CIMF Synonyms Agnogenic myeloid metaplasia Myelosclerosis with myeloid metaplasia Chronic granulocytic-megakaryocytic myelosis CIMF Megakaryocytic proliferation
Chronic Idiopathic Myelofibrosis (CIMF) CIMF Synonyms Agnogenic myeloid metaplasia Myelosclerosis with myeloid metaplasia Chronic granulocytic-megakaryocytic myelosis CIMF Megakaryocytic proliferation
Polycthemia Vera (Rubra)
") Polycthemia Vera (Rubra) Polycthemia Vera (Rubra) Increased red cells Clonal Myeloid lineages also increased 2-13 cases per million Mean age: 60 years Sites of Involvement Bone marrow Peripheral blood
Polycthemia Vera (Rubra) Polycthemia Vera (Rubra) Increased red cells Clonal Myeloid lineages also increased 2-13 cases per million Mean age: 60 years Sites of Involvement Bone marrow Peripheral blood
Juvenile Myelomonocytic Leukemia (JMML)
") Juvenile Myelomonocytic Leukemia (JMML) JMML: Definition Monoclonal hematopoietic disorder of childhood characterized by proliferation of the granulocytic and monocytic lineages Erythroid and megakaryocytic
Juvenile Myelomonocytic Leukemia (JMML) JMML: Definition Monoclonal hematopoietic disorder of childhood characterized by proliferation of the granulocytic and monocytic lineages Erythroid and megakaryocytic
HENATOLYMPHOID SYSTEM THIRD YEAR MEDICAL STUDENTS- UNIVERSITY OF JORDAN AHMAD T. MANSOUR, MD. Part 4 MYELOID NEOPLASMS
 HENATOLYMPHOID SYSTEM THIRD YEAR MEDICAL STUDENTS- UNIVERSITY OF JORDAN AHMAD T. MANSOUR, MD Part 4 MYELOID NEOPLASMS Introduction: o Myeloid neoplasms are divided into three major categories: o Acute
HENATOLYMPHOID SYSTEM THIRD YEAR MEDICAL STUDENTS- UNIVERSITY OF JORDAN AHMAD T. MANSOUR, MD Part 4 MYELOID NEOPLASMS Introduction: o Myeloid neoplasms are divided into three major categories: o Acute
Heme 9 Myeloid neoplasms
 Heme 9 Myeloid neoplasms The minimum number of blasts to diagnose acute myeloid leukemia is 5% 10% 20% 50% 80% AML with the best prognosis is AML with recurrent cytogenetic abnormality AML with myelodysplasia
Heme 9 Myeloid neoplasms The minimum number of blasts to diagnose acute myeloid leukemia is 5% 10% 20% 50% 80% AML with the best prognosis is AML with recurrent cytogenetic abnormality AML with myelodysplasia
Myeloid neoplasms. Early arrest in the blast cell or immature cell "we call it acute leukemia" Myoid neoplasm divided in to 3 major categories:
 Myeloid neoplasms Note: Early arrest in the blast cell or immature cell "we call it acute leukemia" Myoid neoplasm divided in to 3 major categories: 1. AML : Acute myeloid leukemia(stem cell with myeloid
Myeloid neoplasms Note: Early arrest in the blast cell or immature cell "we call it acute leukemia" Myoid neoplasm divided in to 3 major categories: 1. AML : Acute myeloid leukemia(stem cell with myeloid
Myelodysplastic syndrome (MDS) & Myeloproliferative neoplasms
 & Myeloproliferative neoplasms") Myelodysplastic syndrome (MDS) & Myeloproliferative neoplasms Myelodysplastic syndrome (MDS) A multipotent stem cell that can differentiate into any of the myeloid lineage cells (RBCs, granulocytes, megakaryocytes)
Myelodysplastic syndrome (MDS) & Myeloproliferative neoplasms Myelodysplastic syndrome (MDS) A multipotent stem cell that can differentiate into any of the myeloid lineage cells (RBCs, granulocytes, megakaryocytes)
HEMATOLOGIC MALIGNANCIES BIOLOGY
 HEMATOLOGIC MALIGNANCIES BIOLOGY Failure of terminal differentiation Failure of differentiated cells to undergo apoptosis Failure to control growth Neoplastic stem cell FAILURE OF TERMINAL DIFFERENTIATION
HEMATOLOGIC MALIGNANCIES BIOLOGY Failure of terminal differentiation Failure of differentiated cells to undergo apoptosis Failure to control growth Neoplastic stem cell FAILURE OF TERMINAL DIFFERENTIATION
Acute Myeloid Leukemia with Recurrent Cytogenetic Abnormalities
 Acute Myeloid Leukemia with Recurrent Cytogenetic Abnormalities Acute Myeloid Leukemia with recurrent cytogenetic Abnormalities -t(8;21)(q22;q22)(aml/eto) -inv(16) or t(16;16) -t(15;17) -11q23 Acute Myeloid
Acute Myeloid Leukemia with Recurrent Cytogenetic Abnormalities Acute Myeloid Leukemia with recurrent cytogenetic Abnormalities -t(8;21)(q22;q22)(aml/eto) -inv(16) or t(16;16) -t(15;17) -11q23 Acute Myeloid
Myelodysplastic Syndromes Myeloproliferative Disorders
 Myelodysplastic Syndromes Myeloproliferative Disorders Myelodysplastic Syndromes characterized by maturation defects that are associated with ineffective hematopoiesis and a high risk of transformation
Myelodysplastic Syndromes Myeloproliferative Disorders Myelodysplastic Syndromes characterized by maturation defects that are associated with ineffective hematopoiesis and a high risk of transformation
WHO Classification 7/2/2009
 Least Malignant Myeloproliferative Disorders Myelodysplastic Syndromes Most Malignant Acute Leukemia Classifying Hematopoietic Disorders French-American-British (FAB) World Health Organization (WHO) Thanks
Least Malignant Myeloproliferative Disorders Myelodysplastic Syndromes Most Malignant Acute Leukemia Classifying Hematopoietic Disorders French-American-British (FAB) World Health Organization (WHO) Thanks
Myelodysplastic Syndromes: Everyday Challenges and Pitfalls
 Myelodysplastic Syndromes: Everyday Challenges and Pitfalls Kathryn Foucar, MD kfoucar@salud.unm.edu Henry Moon lecture May 2007 Outline Definition Conceptual overview; pathophysiologic mechanisms Incidence,
Myelodysplastic Syndromes: Everyday Challenges and Pitfalls Kathryn Foucar, MD kfoucar@salud.unm.edu Henry Moon lecture May 2007 Outline Definition Conceptual overview; pathophysiologic mechanisms Incidence,
Pathology. #11 Acute Leukemias. Farah Banyhany. Dr. Sohaib Al- Khatib 23/2/16
 35 Pathology #11 Acute Leukemias Farah Banyhany Dr. Sohaib Al- Khatib 23/2/16 1 Salam First of all, this tafreegh is NOT as long as you may think. If you just focus while studying this, everything will
35 Pathology #11 Acute Leukemias Farah Banyhany Dr. Sohaib Al- Khatib 23/2/16 1 Salam First of all, this tafreegh is NOT as long as you may think. If you just focus while studying this, everything will
ADx Bone Marrow Report. Patient Information Referring Physician Specimen Information
 ADx Bone Marrow Report Patient Information Referring Physician Specimen Information Patient Name: Specimen: Bone Marrow Site: Left iliac Physician: Accession #: ID#: Reported: 08/19/2014 - CHRONIC MYELOGENOUS
ADx Bone Marrow Report Patient Information Referring Physician Specimen Information Patient Name: Specimen: Bone Marrow Site: Left iliac Physician: Accession #: ID#: Reported: 08/19/2014 - CHRONIC MYELOGENOUS
Group of malignant disorders of the hematopoietic tissues characteristically associated with increased numbers of white cells in the bone marrow and
 Group of malignant disorders of the hematopoietic tissues characteristically associated with increased numbers of white cells in the bone marrow and / or peripheral blood Classified based on cell type
Group of malignant disorders of the hematopoietic tissues characteristically associated with increased numbers of white cells in the bone marrow and / or peripheral blood Classified based on cell type
2 nd step do Bone Marrow Study If possible both the aspiration and
 Blood Malignancies-I Prof. Herman Hariman,SpPK a (KH). Ph.D.(U.K) Prof. Dr. Adikoesoema Aman, SpPK (KH) Dept. Clinpath, FK-USU First do the Full Blood Count Hb, WBCS, Platelets Morphology!! Such as blasts,
Blood Malignancies-I Prof. Herman Hariman,SpPK a (KH). Ph.D.(U.K) Prof. Dr. Adikoesoema Aman, SpPK (KH) Dept. Clinpath, FK-USU First do the Full Blood Count Hb, WBCS, Platelets Morphology!! Such as blasts,
Hematology 101. Blanche P Alter, MD, MPH, FAAP Clinical Genetics Branch Division of Cancer Epidemiology and Genetics Bethesda, MD
 Hematology 101 Blanche P Alter, MD, MPH, FAAP Clinical Genetics Branch Division of Cancer Epidemiology and Genetics Bethesda, MD Hematocrits Plasma White cells Red cells Normal, Hemorrhage, IDA, Leukemia,
Hematology 101 Blanche P Alter, MD, MPH, FAAP Clinical Genetics Branch Division of Cancer Epidemiology and Genetics Bethesda, MD Hematocrits Plasma White cells Red cells Normal, Hemorrhage, IDA, Leukemia,
Participants Identification No. % Evaluation. Mitotic figure Educational Erythrocyte precursor, abnormal/
 Cell Identification BMD-09 Participants Identification No. % Evaluation Mitotic figure 233 96.7 Educational Erythrocyte precursor, abnormal/ 4 1.7 Educational dysplastic nuclear features Erythrocyte precursor
Cell Identification BMD-09 Participants Identification No. % Evaluation Mitotic figure 233 96.7 Educational Erythrocyte precursor, abnormal/ 4 1.7 Educational dysplastic nuclear features Erythrocyte precursor
Participants Identification No. % Evaluation. Mitotic figure Educational Erythrocyte precursor, abnormal 1 0.
 Cell Identification Mitotic figure 212 99.5 Educational Erythrocyte precursor, abnormal BMD-02 The arrowed cell is a mitotic figure. It was correctly identified by 99.5% of the participants. A cell containing
Cell Identification Mitotic figure 212 99.5 Educational Erythrocyte precursor, abnormal BMD-02 The arrowed cell is a mitotic figure. It was correctly identified by 99.5% of the participants. A cell containing
Extramedullary precursor T-lymphoblastic transformation of CML at presentation
 Extramedullary precursor T-lymphoblastic transformation of CML at presentation Neerja Vajpayee, Constance Stein, Bernard Poeisz & Robert E. Hutchison Clinical History 30 year old man presented to the emergency
Extramedullary precursor T-lymphoblastic transformation of CML at presentation Neerja Vajpayee, Constance Stein, Bernard Poeisz & Robert E. Hutchison Clinical History 30 year old man presented to the emergency
Beyond the CBC Report: Extended Laboratory Testing in the Evaluation for Hematologic Neoplasia Disclosure
 Beyond the CBC Report: Extended Laboratory Testing in the Evaluation for Hematologic Neoplasia Disclosure I am receiving an honorarium from Sysmex for today s presentation. 1 Determining the Etiology for
Beyond the CBC Report: Extended Laboratory Testing in the Evaluation for Hematologic Neoplasia Disclosure I am receiving an honorarium from Sysmex for today s presentation. 1 Determining the Etiology for
Myeloproliferative Disorders - D Savage - 9 Jan 2002
 Disease Usual phenotype acute leukemia precursor chronic leukemia low grade lymphoma myeloma differentiated Total WBC > 60 leukemoid reaction acute leukemia Blast Pro Myel Meta Band Seg Lymph 0 0 0 2
Disease Usual phenotype acute leukemia precursor chronic leukemia low grade lymphoma myeloma differentiated Total WBC > 60 leukemoid reaction acute leukemia Blast Pro Myel Meta Band Seg Lymph 0 0 0 2
Disclosures. Myeloproliferative Neoplasms: A Case-Based Approach. Objectives. Myeloproliferative Neoplasms. Myeloproliferative Neoplasms
 Myeloproliferative Neoplasms: A Case-Based Approach Disclosures No conflicts of interests regarding the topic being presented Adam M. Miller, MD PGY-4 Resident Physician Department of Pathology and Laboratory
Myeloproliferative Neoplasms: A Case-Based Approach Disclosures No conflicts of interests regarding the topic being presented Adam M. Miller, MD PGY-4 Resident Physician Department of Pathology and Laboratory
2007 Workshop of Society for Hematopathology & European Association for Hematopathology Indianapolis, IN, USA Case # 228
 2007 Workshop of Society for Hematopathology & European Association for Hematopathology Indianapolis, IN, USA Case # 228 Vishnu V. B Reddy, MD University of Alabama at Birmingham Birmingham, AL USA 11/03/07
2007 Workshop of Society for Hematopathology & European Association for Hematopathology Indianapolis, IN, USA Case # 228 Vishnu V. B Reddy, MD University of Alabama at Birmingham Birmingham, AL USA 11/03/07
Case Presentation No. 075
 Case Presentation No. 075 Session 4. Myelodysplastic Syndrome Cristina Montalvo, MD Baylor College of Medicine Houston, Texas 2007 Workshop of Society for Hematopathology and European Association for Haematopathology
Case Presentation No. 075 Session 4. Myelodysplastic Syndrome Cristina Montalvo, MD Baylor College of Medicine Houston, Texas 2007 Workshop of Society for Hematopathology and European Association for Haematopathology
Myeloproliferative Disorders: Diagnostic Enigmas, Therapeutic Dilemmas. James J. Stark, MD, FACP
 Myeloproliferative Disorders: Diagnostic Enigmas, Therapeutic Dilemmas James J. Stark, MD, FACP Medical Director, Cancer Program and Palliative Care Maryview Medical Center Professor of Medicine, EVMS
Myeloproliferative Disorders: Diagnostic Enigmas, Therapeutic Dilemmas James J. Stark, MD, FACP Medical Director, Cancer Program and Palliative Care Maryview Medical Center Professor of Medicine, EVMS
Opportunities for Optimal Testing in the Myeloproliferative Neoplasms. Curtis A. Hanson, MD
 Opportunities for Optimal Testing in the Myeloproliferative Neoplasms Curtis A. Hanson, MD 2013 MFMER slide-1 DISCLOSURES: Relevant Financial Relationship(s) None Off Label Usage None 2013 MFMER slide-2
Opportunities for Optimal Testing in the Myeloproliferative Neoplasms Curtis A. Hanson, MD 2013 MFMER slide-1 DISCLOSURES: Relevant Financial Relationship(s) None Off Label Usage None 2013 MFMER slide-2
MYELOPROLIFERATIVE DISEASE. Dr Mere Kende MBBS (UPNG), MMED (Path),MAACB, MACTM, MACRRM (Aus) Lecturer-SMHS UPNG
, MMED (Path),MAACB, MACTM, MACRRM (Aus) Lecturer-SMHS UPNG") MYELOPROLIFERATIVE DISEASE Dr Mere Kende MBBS (UPNG), MMED (Path),MAACB, MACTM, MACRRM (Aus) Lecturer-SMHS UPNG Myeloproliferative Diseases Essential to diagnosis Acquired clonal abnormalities of the hematopoietic
MYELOPROLIFERATIVE DISEASE Dr Mere Kende MBBS (UPNG), MMED (Path),MAACB, MACTM, MACRRM (Aus) Lecturer-SMHS UPNG Myeloproliferative Diseases Essential to diagnosis Acquired clonal abnormalities of the hematopoietic
74y old Female with chronic elevation of Platelet count. August 18, 2005 Faizi Ali, MD Hematopathology Fellow
 74y old Female with chronic elevation of Platelet count August 18, 2005 Faizi Ali, MD Hematopathology Fellow Clinical History Patient is a 74y old otherwise healthy Caucasian female with no major complaint
74y old Female with chronic elevation of Platelet count August 18, 2005 Faizi Ali, MD Hematopathology Fellow Clinical History Patient is a 74y old otherwise healthy Caucasian female with no major complaint
Evaluation of Bone Marrow Biopsies and Aspirates ANNA PORWIT DEPARTMENT OF PATHOLOGY, LUND UNIVERSITY
 Evaluation of Bone Marrow Biopsies and Aspirates ANNA PORWIT DEPARTMENT OF PATHOLOGY, LUND UNIVERSITY DISCLOSURES NONE Learning objectives To review the rules of BMA evaluation To review the main issues
Evaluation of Bone Marrow Biopsies and Aspirates ANNA PORWIT DEPARTMENT OF PATHOLOGY, LUND UNIVERSITY DISCLOSURES NONE Learning objectives To review the rules of BMA evaluation To review the main issues
WHO Classification of Myeloid Neoplasms with Defined Molecular Abnormalities
 WHO Classification of Myeloid Neoplasms with Defined Molecular Abnormalities Robert W. McKenna, M.D. 1/2009 WHO Classification of Myeloid Neoplasms (4th Edition)--2008 Incorporates new information that
WHO Classification of Myeloid Neoplasms with Defined Molecular Abnormalities Robert W. McKenna, M.D. 1/2009 WHO Classification of Myeloid Neoplasms (4th Edition)--2008 Incorporates new information that
Blood Cell Identification: 2011-B Mailing: Acute Myeloid Leukemia (AML)
") Please Note: To view the Figures and Images contained within this education activity in color, access the electronic version of the reading. CASE HISTORY This peripheral blood smear is from a 51-year-old
Please Note: To view the Figures and Images contained within this education activity in color, access the electronic version of the reading. CASE HISTORY This peripheral blood smear is from a 51-year-old
Chronic Myelomonocytic Leukemia with molecular abnormalities SH
 Chronic Myelomonocytic Leukemia with molecular abnormalities SH2017-0351 Madhu P. Menon MD,PhD, Juan Gomez MD, Kedar V. Inamdar MD,PhD and Kristin Karner MD Madhu P Menon, MD, PhD Henry Ford Hospital Patient
Chronic Myelomonocytic Leukemia with molecular abnormalities SH2017-0351 Madhu P. Menon MD,PhD, Juan Gomez MD, Kedar V. Inamdar MD,PhD and Kristin Karner MD Madhu P Menon, MD, PhD Henry Ford Hospital Patient
Done By : WESSEN ADNAN BUTHAINAH AL-MASAEED
 Done By : WESSEN ADNAN BUTHAINAH AL-MASAEED Acute Myeloid Leukemia Firstly we ll start with this introduction then enter the title of the lecture, so be ready and let s begin by the name of Allah : We
Done By : WESSEN ADNAN BUTHAINAH AL-MASAEED Acute Myeloid Leukemia Firstly we ll start with this introduction then enter the title of the lecture, so be ready and let s begin by the name of Allah : We
Lymphoma Tumor Board Quiz! Laboratory Hematology: Basic Cell Morphology
 Lymphoma Tumor Board Quiz! Laboratory Hematology: Basic Cell Morphology CABOT RINGS Cabot rings in a patient with hemolytic anemia. Cabot ring (red arrow) and Howell-Jolly body (blue arrow). Observed in
Lymphoma Tumor Board Quiz! Laboratory Hematology: Basic Cell Morphology CABOT RINGS Cabot rings in a patient with hemolytic anemia. Cabot ring (red arrow) and Howell-Jolly body (blue arrow). Observed in
HEMATOLOGIC MORPHOLOGY- AECOM HEMATOLOGY COURSE
 Log Out Help current login :lcytryn@montefiore.org HEMATOLOGIC MORPHOLOGY- AECOM HEMATOLOGY COURSE Lawrence Cytryn, M.D. - Course Director 1998 Edward Burns, M.D. Images used by permission within AECOM
Log Out Help current login :lcytryn@montefiore.org HEMATOLOGIC MORPHOLOGY- AECOM HEMATOLOGY COURSE Lawrence Cytryn, M.D. - Course Director 1998 Edward Burns, M.D. Images used by permission within AECOM
WBCs Disorders 1. Dr. Nabila Hamdi MD, PhD
 WBCs Disorders 1 Dr. Nabila Hamdi MD, PhD ILOs Compare and contrast ALL, AML, CLL, CML in terms of age distribution, cytogenetics, morphology, immunophenotyping, laboratory diagnosis clinical features
WBCs Disorders 1 Dr. Nabila Hamdi MD, PhD ILOs Compare and contrast ALL, AML, CLL, CML in terms of age distribution, cytogenetics, morphology, immunophenotyping, laboratory diagnosis clinical features
Hematopathology Lab. Third year medical students
 Hematopathology Lab Third year medical students Objectives Identify the lesion Know the specific name of the lesion Know associated disease Know relevant pathologic background Spherocytes: appear small,
Hematopathology Lab Third year medical students Objectives Identify the lesion Know the specific name of the lesion Know associated disease Know relevant pathologic background Spherocytes: appear small,
Blood Cell Identification Graded
 BCP-21 Blood Cell Identification Graded Case History The patient is a 37-year-old female with a history of multiple sickle cell crises. She now presents with avascular necrosis of the left hip. Laboratory
BCP-21 Blood Cell Identification Graded Case History The patient is a 37-year-old female with a history of multiple sickle cell crises. She now presents with avascular necrosis of the left hip. Laboratory
MYELODYSPLASTIC SYNDROMES
 MYELODYSPLASTIC SYNDROMES Babak Tamizi Far MD. Assistant professor of internal medicine Al-zahra university hospital, Isfahan university of medical sciences Key Features ESSENTIALS OF DIAGNOSIS Cytopenias
MYELODYSPLASTIC SYNDROMES Babak Tamizi Far MD. Assistant professor of internal medicine Al-zahra university hospital, Isfahan university of medical sciences Key Features ESSENTIALS OF DIAGNOSIS Cytopenias
Hematopathology Case Study
 www.medfusionservices.com Hematopathology Case Study CV3515-14 JUNE Clinical Presentation: Clinical Information: A 42 year old male with history of chronic myelogenous leukemia (CML) presents with an elevated
www.medfusionservices.com Hematopathology Case Study CV3515-14 JUNE Clinical Presentation: Clinical Information: A 42 year old male with history of chronic myelogenous leukemia (CML) presents with an elevated
Year 2003 Paper two: Questions supplied by Tricia
 QUESTION 65 A 36-year-old man presents in a post-ictal state after an observed generalised seizure. Full blood investigation shows: haemoglobin 0 g/l [128-175] mean corpuscular volume (MCV) 106 fl [80-7]
QUESTION 65 A 36-year-old man presents in a post-ictal state after an observed generalised seizure. Full blood investigation shows: haemoglobin 0 g/l [128-175] mean corpuscular volume (MCV) 106 fl [80-7]
MYELOPROLIFERATIVE NEOPLASMS
 9 : 2 MYELOPROLIFERATIVE NEOPLASMS Introduction William Dameshek in 1951 introduced the term Myeloproliferative disorders (MPD). This included polycythemia vera (PV), essential thrombocythemia (ET), primary
9 : 2 MYELOPROLIFERATIVE NEOPLASMS Introduction William Dameshek in 1951 introduced the term Myeloproliferative disorders (MPD). This included polycythemia vera (PV), essential thrombocythemia (ET), primary
Acute myeloid leukemia. M. Kaźmierczak 2016
 Acute myeloid leukemia M. Kaźmierczak 2016 Acute myeloid leukemia Malignant clonal disorder of immature hematopoietic cells characterized by clonal proliferation of abnormal blast cells and impaired production
Acute myeloid leukemia M. Kaźmierczak 2016 Acute myeloid leukemia Malignant clonal disorder of immature hematopoietic cells characterized by clonal proliferation of abnormal blast cells and impaired production
Allogeneic Hematopoietic Stem-Cell Transplantation for Myelodysplastic Syndromes and Myeloproliferative Neoplasms. Policy Specific Section:
 Medical Policy Allogeneic Hematopoietic Stem-Cell Transplantation for Myelodysplastic Syndromes and Myeloproliferative Type: Medical Necessity and Investigational / Experimental Policy Specific Section:
Medical Policy Allogeneic Hematopoietic Stem-Cell Transplantation for Myelodysplastic Syndromes and Myeloproliferative Type: Medical Necessity and Investigational / Experimental Policy Specific Section:
WHO Update to Myeloproliferative Neoplasms
 WHO Update to Myeloproliferative Neoplasms Archana M Agarwal, MD, Associate Professor of Pathology University of Utah Department of Pathology/ARUP Laboratories Myeloproliferative Neoplasms The categories
WHO Update to Myeloproliferative Neoplasms Archana M Agarwal, MD, Associate Professor of Pathology University of Utah Department of Pathology/ARUP Laboratories Myeloproliferative Neoplasms The categories
SWOG ONCOLOGY RESEARCH PROFESSIONAL (ORP) MANUAL LEUKEMIA FORMS CHAPTER 16A REVISED: DECEMBER 2017
 MANUAL LEUKEMIA FORMS CHAPTER 16A REVISED: DECEMBER 2017") LEUKEMIA FORMS The guidelines and figures below are specific to Leukemia studies. The information in this manual does NOT represent a complete set of required forms for any leukemia study. Please refer
LEUKEMIA FORMS The guidelines and figures below are specific to Leukemia studies. The information in this manual does NOT represent a complete set of required forms for any leukemia study. Please refer
Bone Marrow. Procedures Blood Film Aspirate, Cell Block Trephine Biopsy, Touch Imprint
 Bone Marrow Protocol applies to acute leukemias, myelodysplastic syndromes, myeloproliferative disorders, chronic lymphoproliferative disorders, malignant lymphomas, plasma cell dyscrasias, histiocytic
Bone Marrow Protocol applies to acute leukemias, myelodysplastic syndromes, myeloproliferative disorders, chronic lymphoproliferative disorders, malignant lymphomas, plasma cell dyscrasias, histiocytic
Formation of Blood Cells
 Hematopoiesis Lecture Objectives Name organs responsible for hematopoiesis in the fetus. List the developmental stages of hematopoiesis both prenatally and postnatally. Outline the major steps of post
Hematopoiesis Lecture Objectives Name organs responsible for hematopoiesis in the fetus. List the developmental stages of hematopoiesis both prenatally and postnatally. Outline the major steps of post
VETERINARY HEMATOLOGY ATLAS OF COMMON DOMESTIC AND NON-DOMESTIC SPECIES COPYRIGHTED MATERIAL SECOND EDITION
 VETERINARY HEMATOLOGY ATLAS OF COMMON DOMESTIC AND NON-DOMESTIC SPECIES SECOND EDITION COPYRIGHTED MATERIAL CHAPTER ONE HEMATOPOIESIS GENERAL FEATURES All blood cells have a finite life span, but in normal
VETERINARY HEMATOLOGY ATLAS OF COMMON DOMESTIC AND NON-DOMESTIC SPECIES SECOND EDITION COPYRIGHTED MATERIAL CHAPTER ONE HEMATOPOIESIS GENERAL FEATURES All blood cells have a finite life span, but in normal
r). SUPPLEMENTARY/SECOND OPPORTUNITY EXAMINATION PAPER nnmlbih UNIVERSITY Sophia Blaauw INSTRUCTIONS FACULTY OF HEALTH AND APPLIED SCIENCES
. SUPPLEMENTARY/SECOND OPPORTUNITY EXAMINATION PAPER nnmlbih UNIVERSITY Sophia Blaauw INSTRUCTIONS FACULTY OF HEALTH AND APPLIED SCIENCES") r). nnmlbih UNIVERSITY OF SCIEFICE nnd TECHNOLOGY FACULTY OF HEALTH AND APPLIED SCIENCES DEPARTMENT OF HEALTH SCIENCES QUALIFICATION: BACHELOR OF MEDICAL LABORATORY SCIENCES QUALIFICATION CODE: 08BMLS
r). nnmlbih UNIVERSITY OF SCIEFICE nnd TECHNOLOGY FACULTY OF HEALTH AND APPLIED SCIENCES DEPARTMENT OF HEALTH SCIENCES QUALIFICATION: BACHELOR OF MEDICAL LABORATORY SCIENCES QUALIFICATION CODE: 08BMLS
Case Presentation. Attilio Orazi, MD
 Case Presentation Attilio Orazi, MD Weill Cornell Medical College/ NYP Hospital Department of Pathology and Laboratory Medicine New York, NY United States History 60 year old man presented with anemia
Case Presentation Attilio Orazi, MD Weill Cornell Medical College/ NYP Hospital Department of Pathology and Laboratory Medicine New York, NY United States History 60 year old man presented with anemia
Myeloproliferative Neoplasms
 Myeloproliferative Neoplasms (MPN and MDS/MPN) Attilio Orazi, MD, FRCPath Weill Cornell Medical College/ NY Presbyterian Hospital, New York, NY USA EAHP EDUCATIONAL SESSION: Updated WHO classification
Myeloproliferative Neoplasms (MPN and MDS/MPN) Attilio Orazi, MD, FRCPath Weill Cornell Medical College/ NY Presbyterian Hospital, New York, NY USA EAHP EDUCATIONAL SESSION: Updated WHO classification
MS.4/ 1.Nov/2015. Acute Leukemia: AML. Abdallah Abbadi
 MS.4/ 1.Nov/2015. Acute Leukemia: AML Abdallah Abbadi Case 9: Acute Leukemia 29 yr old lady complains of fever and painful gums for 1 week. She developed easy bruising and hemorrhagic spots on her trunk
MS.4/ 1.Nov/2015. Acute Leukemia: AML Abdallah Abbadi Case 9: Acute Leukemia 29 yr old lady complains of fever and painful gums for 1 week. She developed easy bruising and hemorrhagic spots on her trunk
2013 Pathology Student
 About this guide If you re reading this introduction, it means you are probably either a) covering hematopathology in your pathology class right now, or b) studying for boards. Either way, you ve come
About this guide If you re reading this introduction, it means you are probably either a) covering hematopathology in your pathology class right now, or b) studying for boards. Either way, you ve come
Primary myelofibrosis
 - It s a bone marrow fibrosis Primary myelofibrosis - It's type of myeloproliferative disease i.e. neoplastic proliferation of mature cell of myloid linage. - Its similar to chronic myloid leukemia (CML).
- It s a bone marrow fibrosis Primary myelofibrosis - It's type of myeloproliferative disease i.e. neoplastic proliferation of mature cell of myloid linage. - Its similar to chronic myloid leukemia (CML).
Bone marrow histopathology in Ph - CMPDs. - the new WHO classification - Juergen Thiele Cologne, Germany
 Bone marrow histopathology in Ph - CMPDs - the new WHO classification - Juergen Thiele Cologne, Germany Current issues in MPNs concerning morphology 1.Prodromal stages of disease 2.Impact of histopathology
Bone marrow histopathology in Ph - CMPDs - the new WHO classification - Juergen Thiele Cologne, Germany Current issues in MPNs concerning morphology 1.Prodromal stages of disease 2.Impact of histopathology
Myelodysplastic Syndromes: WHO 2008
 Myelodysplastic Syndromes: WHO 2008 Attilio Orazi, M.D., FRCPath. (Engl.) Weill Medical College of Cornell University New York, NY Congresso Nazionale SIE - Società Italiana di Ematologia - MIC Milano
Myelodysplastic Syndromes: WHO 2008 Attilio Orazi, M.D., FRCPath. (Engl.) Weill Medical College of Cornell University New York, NY Congresso Nazionale SIE - Società Italiana di Ematologia - MIC Milano
Pathology of Hematopoietic and Lymphoid tissue
 CONTENTS Pathology of Hematopoietic and Lymphoid tissue White blood cells and lymph nodes Quantitative disorder of white blood cells Reactive lymphadenopathies Infectious lymphadenitis Tumor metastasis
CONTENTS Pathology of Hematopoietic and Lymphoid tissue White blood cells and lymph nodes Quantitative disorder of white blood cells Reactive lymphadenopathies Infectious lymphadenitis Tumor metastasis
Leukaemia Section Review
 Atlas of Genetics and Cytogenetics in Oncology and Haematology OPEN ACCESS JOURNAL AT INIST-CNRS Leukaemia Section Review Classification of myelodysplasic syndromes Georges Flandrin Laboratoire d'hématologie,
Atlas of Genetics and Cytogenetics in Oncology and Haematology OPEN ACCESS JOURNAL AT INIST-CNRS Leukaemia Section Review Classification of myelodysplasic syndromes Georges Flandrin Laboratoire d'hématologie,
SH A CASE OF PERSISTANT NEUTROPHILIA: BCR-ABL
 SH2017-0124 A CASE OF PERSISTANT NEUTROPHILIA: BCR-ABL NEGATIVE John R Goodlad 1, Pedro Martin-Cabrera 2, Catherine Cargo 2 1. Department of Pathology, NHS Greater Glasgow & Clyde, QEUH, Glasgow 2. Haematological
SH2017-0124 A CASE OF PERSISTANT NEUTROPHILIA: BCR-ABL NEGATIVE John R Goodlad 1, Pedro Martin-Cabrera 2, Catherine Cargo 2 1. Department of Pathology, NHS Greater Glasgow & Clyde, QEUH, Glasgow 2. Haematological
MYELODYSPLASTIC SYNDROMES: A diagnosis often missed
 MYELODYSPLASTIC SYNDROMES: A diagnosis often missed D R. EMMA W YPKEMA C O N S U LTA N T H A E M AT O L O G I S T L A N C E T L A B O R AT O R I E S THE MYELODYSPLASTIC SYNDROMES DEFINITION The Myelodysplastic
MYELODYSPLASTIC SYNDROMES: A diagnosis often missed D R. EMMA W YPKEMA C O N S U LTA N T H A E M AT O L O G I S T L A N C E T L A B O R AT O R I E S THE MYELODYSPLASTIC SYNDROMES DEFINITION The Myelodysplastic
Integrated Diagnostic Approach to the Classification of Myeloid Neoplasms. Daniel A. Arber, MD Stanford University
 Integrated Diagnostic Approach to the Classification of Myeloid Neoplasms Daniel A. Arber, MD Stanford University What is an integrated approach? What is an integrated approach? Incorporating all diagnostic
Integrated Diagnostic Approach to the Classification of Myeloid Neoplasms Daniel A. Arber, MD Stanford University What is an integrated approach? What is an integrated approach? Incorporating all diagnostic
EHE1-16 Participants Identification No. % Evaluation
 Cell Identification EHE1-16 Participants Identification No. % Evaluation Blast cell 154 90.1 Educational Lymphocyte 4 2.3 Educational Lymphocyte, reactive 1 0.6 Educational Lymphoma cell (malignant) 1
Cell Identification EHE1-16 Participants Identification No. % Evaluation Blast cell 154 90.1 Educational Lymphocyte 4 2.3 Educational Lymphocyte, reactive 1 0.6 Educational Lymphoma cell (malignant) 1
MS.4/ Acute Leukemia: AML. Abdallah Al Abbadi.MD.FRCP.FRCPath Feras Fararjeh MD
 MS.4/ 27.02.2019 Acute Leukemia: AML Abdallah Al Abbadi.MD.FRCP.FRCPath Feras Fararjeh MD Case 9: Acute Leukemia 29 yr old lady complains of fever and painful gums for 1 week. She developed easy bruising
MS.4/ 27.02.2019 Acute Leukemia: AML Abdallah Al Abbadi.MD.FRCP.FRCPath Feras Fararjeh MD Case 9: Acute Leukemia 29 yr old lady complains of fever and painful gums for 1 week. She developed easy bruising
NEW YORK STATE CYTOHEMATOLOGY PROFICIENCY TEST PROGRAM Glass Slide - November 2016
 NEW YORK STATE CYTOHEMATOLOGY PROFICIENCY TEST PROGRAM Glass Slide - November 2016 Results from this proficiency test event are available at: http://www.wadsworth.org/regulatory/clep/pt/summaries SLIDE
NEW YORK STATE CYTOHEMATOLOGY PROFICIENCY TEST PROGRAM Glass Slide - November 2016 Results from this proficiency test event are available at: http://www.wadsworth.org/regulatory/clep/pt/summaries SLIDE
Morfologia normale e patologica
 Morfologia normale e patologica Gina Zini Centro di Ricerca ReCAMH Dpt. Ematologia Università Cattolica S. Cuore - Roma EMATOLOGIA DI LABORATORIO: percorsi diagnostici e obiettivi clinici. Milano 11-12
Morfologia normale e patologica Gina Zini Centro di Ricerca ReCAMH Dpt. Ematologia Università Cattolica S. Cuore - Roma EMATOLOGIA DI LABORATORIO: percorsi diagnostici e obiettivi clinici. Milano 11-12
Myelodysplastic/Myeloproliferative Disorders. MDS/MPD Unclassified Provisional: CMML JMML acml RARS T. K. Foucar November 2007 SH/EAHP Workshop
 Myelodysplastic/Myeloproliferative Disorders CMML JMML acml MDS/MPD Unclassified Provisional: RARS T K. Foucar November 2007 SH/EAHP Workshop MDS/MPD: General Features Blood: Cytosis and cytopenia(s) Dysplasia
Myelodysplastic/Myeloproliferative Disorders CMML JMML acml MDS/MPD Unclassified Provisional: RARS T K. Foucar November 2007 SH/EAHP Workshop MDS/MPD: General Features Blood: Cytosis and cytopenia(s) Dysplasia
MPDs. Myeloproliferative Disorders OBJECTIVES MYELOPROLIFERATIVE NEOPLASMS
 MYELOPROLIFERATIVE NEOPLASMS CLPC Fall Seminar 2016 Angela Foley, MS, MLS(ASCP)SH LSUHSC School of Allied Health Department of Clinical Laboratory Sciences OBJECTIVES Name the 4 most common MPNs Describe
MYELOPROLIFERATIVE NEOPLASMS CLPC Fall Seminar 2016 Angela Foley, MS, MLS(ASCP)SH LSUHSC School of Allied Health Department of Clinical Laboratory Sciences OBJECTIVES Name the 4 most common MPNs Describe
Classification of Hematologic Malignancies. Patricia Aoun MD MPH
 Classification of Hematologic Malignancies Patricia Aoun MD MPH Objectives Know the basic principles of the current classification system for hematopoietic and lymphoid malignancies Understand the differences
Classification of Hematologic Malignancies Patricia Aoun MD MPH Objectives Know the basic principles of the current classification system for hematopoietic and lymphoid malignancies Understand the differences
MYELOPROLIFARATIVE NEOPLASMS. Dr. Hasan Fahmawi, MRCP(UK), FRCP(Edin).
, FRCP(Edin).") MYELOPROLIFARATIVE NEOPLASMS Dr. Hasan Fahmawi, MRCP(UK), FRCP(Edin). These are a group of chronic conditions characterised by clonal proliferation of marrow precursor cells. PRV, essential thrombocyathaemia,
MYELOPROLIFARATIVE NEOPLASMS Dr. Hasan Fahmawi, MRCP(UK), FRCP(Edin). These are a group of chronic conditions characterised by clonal proliferation of marrow precursor cells. PRV, essential thrombocyathaemia,
By Dr. Mohamed Saad Daoud
 By Dr. Mohamed Saad Daoud Part I Introduction Types of White Blood Cells Genesis of the White Blood Cells Life Span of the White Blood Cells Dr. Mohamed Saad Daoud 2 Leucocytes Introduction: Infectious
By Dr. Mohamed Saad Daoud Part I Introduction Types of White Blood Cells Genesis of the White Blood Cells Life Span of the White Blood Cells Dr. Mohamed Saad Daoud 2 Leucocytes Introduction: Infectious
MPDs. Myeloproliferative Disorders OBJECTIVES MYELOPROLIFERATIVE NEOPLASMS
 MYELOPROLIFERATIVE NEOPLASMS CLPC Fall Seminar 2016 Angela Foley, MS, MLS(ASCP)SH LSUHSC School of Allied Health Department of Clinical Laboratory Sciences OBJECTIVES Name the 4 most common MPNs Describe
MYELOPROLIFERATIVE NEOPLASMS CLPC Fall Seminar 2016 Angela Foley, MS, MLS(ASCP)SH LSUHSC School of Allied Health Department of Clinical Laboratory Sciences OBJECTIVES Name the 4 most common MPNs Describe
Hemopoiesis and Blood
 Hemopoiesis and Blood Blood Cells o o o Erythrocytes Leukocytes Thrombocytes Function o Transport nutrients and wastes throughout the bloodstream, fight foreign antigens and blood coagulation. Location
Hemopoiesis and Blood Blood Cells o o o Erythrocytes Leukocytes Thrombocytes Function o Transport nutrients and wastes throughout the bloodstream, fight foreign antigens and blood coagulation. Location
MORPHOLOGY OF BONE MARROW ASPIRATES. Dr.Prasanna N Kumar Head Department of Pathology, Oman Medical College, Oman
 MORPHOLOGY OF BONE MARROW ASPIRATES Dr.Prasanna N Kumar Head Department of Pathology, Oman Medical College, Oman BONE MARROW ASPIRATION Sites Sternum Anterior or posterior iliac spines Aspiration from
MORPHOLOGY OF BONE MARROW ASPIRATES Dr.Prasanna N Kumar Head Department of Pathology, Oman Medical College, Oman BONE MARROW ASPIRATION Sites Sternum Anterior or posterior iliac spines Aspiration from
CHALLENGING CASES PRESENTATION
 CHALLENGING CASES PRESENTATION Michael C. Wiemann, MD, FACP Program Co-Chair and Vice President Indy Hematology Education President, Clinical St. John Providence Physician Network Detroit, Michigan 36
CHALLENGING CASES PRESENTATION Michael C. Wiemann, MD, FACP Program Co-Chair and Vice President Indy Hematology Education President, Clinical St. John Providence Physician Network Detroit, Michigan 36
بسم هللا الرحمن الرحيم
 بسم هللا الرحمن الرحيم WBCs disorders *Slide 2: - we will focus on the disorders that are related to the # of WBCs - in children the # of lymphocyte is more than it in adults,sometimes more than neutrophils
بسم هللا الرحمن الرحيم WBCs disorders *Slide 2: - we will focus on the disorders that are related to the # of WBCs - in children the # of lymphocyte is more than it in adults,sometimes more than neutrophils
Pathology of Hematopoietic and Lymphoid tissue
 Pathology of Hematopoietic and Lymphoid tissue Peerayut Sitthichaiyakul, M.D. Department of Pathology and Forensic Medicine Faculty of Medicine, Naresuan University CONTENTS White blood cells and lymph
Pathology of Hematopoietic and Lymphoid tissue Peerayut Sitthichaiyakul, M.D. Department of Pathology and Forensic Medicine Faculty of Medicine, Naresuan University CONTENTS White blood cells and lymph
Update on Myelodysplastic Syndromes and Myeloproliferative Neoplasms. Kaaren Reichard Mayo Clinic Rochester
 Update on Myelodysplastic Syndromes and Myeloproliferative Neoplasms Kaaren Reichard Mayo Clinic Rochester Reichard.kaaren@mayo.edu Nothing to disclose Conflict of Interest Learning Objectives Present
Update on Myelodysplastic Syndromes and Myeloproliferative Neoplasms Kaaren Reichard Mayo Clinic Rochester Reichard.kaaren@mayo.edu Nothing to disclose Conflict of Interest Learning Objectives Present
Notes for the 2 nd histology lab
 Notes for the 2 nd histology lab Note : Please refer to the slides and see the morphological characteristics of each cell, as the practical exam will be in the form of figures. SLIDE #2 Erythropoiesis
Notes for the 2 nd histology lab Note : Please refer to the slides and see the morphological characteristics of each cell, as the practical exam will be in the form of figures. SLIDE #2 Erythropoiesis
Ordering Physician CLIENT,CLIENT. Collected REVISED REPORT
 HPWET Hematopathology Consultation, MML Embed Client Hematopathology Consult REVISED INAL DIAGNOSIS Interpretation Peripheral blood, bone marrow aspirate and biopsies, bilateral iliac crests: 1. Normocellular
HPWET Hematopathology Consultation, MML Embed Client Hematopathology Consult REVISED INAL DIAGNOSIS Interpretation Peripheral blood, bone marrow aspirate and biopsies, bilateral iliac crests: 1. Normocellular
Hematology Page 1 of 8
 Hematology Page 1 of 8 Hematology Major Category Code Headings Revised 12/17 1 Basic methodology and test armamentarium 20000 2 Normal hematopoiesis & hemostasis 20100 3 RBC disorders, non-neoplastic 20340
Hematology Page 1 of 8 Hematology Major Category Code Headings Revised 12/17 1 Basic methodology and test armamentarium 20000 2 Normal hematopoiesis & hemostasis 20100 3 RBC disorders, non-neoplastic 20340
What is MDS? Epidemiology, Diagnosis, Classification & Risk Stratification
 What is MDS? Epidemiology, Diagnosis, Classification & Risk Stratification Rami Komrokji, MD Clinical Director Malignant Hematology Moffitt Cancer Center Normal Blood and Bone Marrow What is MDS Myelodysplastic
What is MDS? Epidemiology, Diagnosis, Classification & Risk Stratification Rami Komrokji, MD Clinical Director Malignant Hematology Moffitt Cancer Center Normal Blood and Bone Marrow What is MDS Myelodysplastic
ACCME/Disclosures. History. Hematopathology Specialty Conference Case #4 4/13/2016
 Hematopathology Specialty Conference Case #4 Sherrie L. Perkins MD, PhD University of Utah ACCME/Disclosures The USCAP requires that anyone in a position to influence or control the content of CME disclose
Hematopathology Specialty Conference Case #4 Sherrie L. Perkins MD, PhD University of Utah ACCME/Disclosures The USCAP requires that anyone in a position to influence or control the content of CME disclose
Board Review- Part 2A: Malignant HemePath 4/25/2018
 Board Review- Part 2A: Malignant HemePath 4/25/2018 Chronic Myelogenous Leukemia, bcr/abl1 pos Morphology-Chronic Phase Peripheral blood Leukocytosis (median 100k/µL), due mainly to neutrophils (peak in
Board Review- Part 2A: Malignant HemePath 4/25/2018 Chronic Myelogenous Leukemia, bcr/abl1 pos Morphology-Chronic Phase Peripheral blood Leukocytosis (median 100k/µL), due mainly to neutrophils (peak in
Blood Cell Identification Graded
 Blood Cell Identification Graded Case History An 11-year-old girl presented to the emergency room with wheezing and was diagnosed as having asthma. Her CBC showed WBC = 12.5 x 10 9 /L; Hgb = 12.4g/dL;
Blood Cell Identification Graded Case History An 11-year-old girl presented to the emergency room with wheezing and was diagnosed as having asthma. Her CBC showed WBC = 12.5 x 10 9 /L; Hgb = 12.4g/dL;
MYELODYSPLASTIC AND MYELOPROLIFERATIVE
 MYELODYSPLASTIC AND MYELOPROLIFERATIVE DISORDERS Pediatric Hemato-Oncology Division Medical Faculty University of Sumatera Utara 1 MYELODYSPLASIA SYNDROME A group of disorder defect in hematopoetic cell
MYELODYSPLASTIC AND MYELOPROLIFERATIVE DISORDERS Pediatric Hemato-Oncology Division Medical Faculty University of Sumatera Utara 1 MYELODYSPLASIA SYNDROME A group of disorder defect in hematopoetic cell
Diagnostic challenge: Acute leukemia with biphenotypic blasts and BCR-ABL1 translocation
 Case Study Diagnostic challenge: Acute leukemia with biphenotypic blasts and BCR-ABL1 translocation Ling Wang 1 and Xiangdong Xu 1,2,* 1 Department of Pathology, University of California, San Diego; 2
Case Study Diagnostic challenge: Acute leukemia with biphenotypic blasts and BCR-ABL1 translocation Ling Wang 1 and Xiangdong Xu 1,2,* 1 Department of Pathology, University of California, San Diego; 2
MDS 101. What is bone marrow? Myelodysplastic Syndrome: Let s build a definition. Dysplastic? Syndrome? 5/22/2014. What does bone marrow do?
 101 May 17, 2014 Myelodysplastic Syndrome: Let s build a definition Myelo bone marrow Gail J. Roboz, M.D. Director, Leukemia Program Associate Professor of Medicine What is bone marrow? What does bone
101 May 17, 2014 Myelodysplastic Syndrome: Let s build a definition Myelo bone marrow Gail J. Roboz, M.D. Director, Leukemia Program Associate Professor of Medicine What is bone marrow? What does bone
Welcome to Master Class for Oncologists. Session 3: 9:15 AM - 10:00 AM
 Welcome to Master Class for Oncologists Session 3: 9:15 AM - 10:00 AM Miami, FL December 18, 2009 Myeloproliferative Neoplasms: Bringing Order to Complexity and Achieving Optimal Outcomes Speaker: Andrew
Welcome to Master Class for Oncologists Session 3: 9:15 AM - 10:00 AM Miami, FL December 18, 2009 Myeloproliferative Neoplasms: Bringing Order to Complexity and Achieving Optimal Outcomes Speaker: Andrew
Myelodysplastic Syndrome: Let s build a definition
 1 MDS: Diagnosis and Treatment Update Gail J. Roboz, M.D. Director, Leukemia Program Associate Professor of Medicine Weill Medical College of Cornell University The New York Presbyterian Hospital Myelodysplastic
1 MDS: Diagnosis and Treatment Update Gail J. Roboz, M.D. Director, Leukemia Program Associate Professor of Medicine Weill Medical College of Cornell University The New York Presbyterian Hospital Myelodysplastic
Practical Diagnosis of Hematologic Disorders. Vol 2 Malignant Disorders
 5 th ed Practical Diagnosis of Hematologic Disorders Vol 2 Malignant Disorders Vol2_FrontMatter_v03_0804 final.indd i 8/6/2009 10:00:11 PM Authors Carl R Kjeldsberg, MD Professor of Pathology, University
5 th ed Practical Diagnosis of Hematologic Disorders Vol 2 Malignant Disorders Vol2_FrontMatter_v03_0804 final.indd i 8/6/2009 10:00:11 PM Authors Carl R Kjeldsberg, MD Professor of Pathology, University
Polycythemia Vera and other Myeloproliferative Neoplasms. A.Mousavi
 Polycythemia Vera and other Myeloproliferative Neoplasms A.Mousavi Chronic MPNs Multipotent hematopoietic progenitor cell is origin. Overproduction of one or more formed element of blood cells without
Polycythemia Vera and other Myeloproliferative Neoplasms A.Mousavi Chronic MPNs Multipotent hematopoietic progenitor cell is origin. Overproduction of one or more formed element of blood cells without
Adult Acute leukemia. Matthew Seftel. August
 Adult Acute leukemia Matthew Seftel August 21 2007 mseftel@cancercare.mb.ca Principles 3 cases Diagnosis and classification of acute leukemia (AL) Therapy Emergencies Remission induction BMT Complications
Adult Acute leukemia Matthew Seftel August 21 2007 mseftel@cancercare.mb.ca Principles 3 cases Diagnosis and classification of acute leukemia (AL) Therapy Emergencies Remission induction BMT Complications
If unqualified, Complete remission is considered to be Haematological complete remission
 Scroll right to see the database codes for Disease status and Response Diagnosis it refers to Disease status or response to treatment AML ALL CML CLL MDS or MD/MPN or acute leukaemia secondary to previous
Scroll right to see the database codes for Disease status and Response Diagnosis it refers to Disease status or response to treatment AML ALL CML CLL MDS or MD/MPN or acute leukaemia secondary to previous
Approaching myeloid neoplasms: diagnostic algorithms
 Approaching myeloid neoplasms: diagnostic algorithms Alexandar Tzankov Histopathology Pathology Content Integration of clinical and laboratory data Bone marrow evaluation approaching Myeloproliferative
Approaching myeloid neoplasms: diagnostic algorithms Alexandar Tzankov Histopathology Pathology Content Integration of clinical and laboratory data Bone marrow evaluation approaching Myeloproliferative
Leukocytosis - Some Learning Points
 Leukocytosis - Some Learning Points Koh Liang Piu Department of Hematology-Oncology National University Cancer Institute National University Health System Objectives of this talk: 1. To provide some useful
Leukocytosis - Some Learning Points Koh Liang Piu Department of Hematology-Oncology National University Cancer Institute National University Health System Objectives of this talk: 1. To provide some useful
If unqualified, Complete remission is considered to be Haematological complete remission
 Scroll right to see the database codes for Disease status and Response Diagnosis it refers to Disease status or response to treatment AML ALL CML CLL MDS or MD/MPN or acute leukaemia secondary to previous
Scroll right to see the database codes for Disease status and Response Diagnosis it refers to Disease status or response to treatment AML ALL CML CLL MDS or MD/MPN or acute leukaemia secondary to previous
EDUCATIONAL COMMENTARY DIFFERENTIATING IMMATURE PERIPHERAL BLOOD CELLS
 Educational commentary is provided through our affiliation with the American Society for Clinical Pathology (ASCP). To obtain FREE CME/CMLE credits click on Continuing Education on the left side of the
Educational commentary is provided through our affiliation with the American Society for Clinical Pathology (ASCP). To obtain FREE CME/CMLE credits click on Continuing Education on the left side of the