Synchronous and Subsequent Lesions of Serrated Adenomas and Tubular Adenomas of the Colorectum
|
|
|
- Jasmin Owen
- 5 years ago
- Views:
Transcription
1 Tsumura T, et al 1 Synchronous and Subsequent Lesions of Serrated Adenomas and Tubular Adenomas of the Colorectum T. Tsumura a T. Hiyama d S. Tanaka b M. Yoshihara d K. Arihiro c K. Chayama a Departments of a Gastroenterology and Metabolism, b Endoscopy and c Anatomical Pathology, Hiroshima University Hospital, and d Health Service Center, Hiroshima University, Higashihiroshima, Japan Running title: Synchronous and Subsequent Lesions of SA Conflict of interest: None Grant support: None Corresponding author: Toru Hiyama, MD, PhD Health Service Center, Hiroshima University Kagamiyama, Higashihiroshima , Japan Phone: Fax: tohiyama@hiroshima-u.ac.jp
2 Tsumura T, et al 2 Abstract The characteristics of synchronous and subsequent lesions of serrated adenomas (SAs) of the colorectum are still unclear. This study aimed to clarify the characteristics of synchronous and subsequent lesions of SAs compared with tubular adenomas (TAs) of the colorectum. Patients were divided into 2 groups: SA (127 patients) and TA (158 patients) groups. The mean follow-up durations in the SA and TA groups were 39.7 months and 42.7 months, respectively. The number and clinical features of synchronous and subsequent lesions of both groups were examined. In the SA group, 19 (15%) patients had synchronous lesions, and 3 (2%) patients had subsequent lesions. In the TA group, 68 (43%) patients had synchronous lesions, and 14 (9%) patients had subsequent lesions. The frequencies of patient with synchronous and subsequent lesions in the SA group were significantly lower than those in the TA group (p < and p = 0.02, respectively). The most frequent synchronous lesion was SA (67%) in the SA group, and TA (95%) in the TA group. The most subsequent lesion was SA (62%) in the SA group, and TA (100%) in the TA group. The histology of the index polyp and synchronous and subsequent lesions tended to be identical. No invasive colorectal carcinomas were observed in either group. Our data suggest that the colonic tumorigenesis potential of patient with SA may differ from that of patient with TA. Key Words: Serrated adenoma, Tubular adenoma, Synchronous lesion, Subsequent lesion
3 Tsumura T, et al 3 Introduction Serrated adenomas (SAs) of the colorectum are recognized as a distinct form of neoplasia, histologically defined by the presence of hyperplastic and adenomatous features as proposed by Longacre and Fenoglio-Preiser in 1990 [1]. Histological diagnosis of SA is made by the observation of a serrated glandular pattern, the presence of goblet cell immaturity and upper zone mitoses, prominence of nucleoli, and the absence of a thickened collagen table. SAs harbor malignant potential, and high-grade dysplasia has been observed in 11% of SAs [1, 2]. Recently, the clinical and molecular differences between SAs and conventional tubular adenomas (TAs) have been detected. Clinically, SAs are located predominantly in the sigmoid colon and rectum, and incidences of high-grade dysplasia differ between SAs and TAs [3]. Genetically, SAs have frequent mutations of p53, K-ras, and B-raf, and methylations of hmlh1, p16, and IGFBP7 [4]. However, researches on synchronous and subsequent lesions of SA are quite few. To our knowledge, there is only one study on the issue at present [5]. Thus, characteristics of those lesions are still unclear. The purpose of this study was to clarify the characteristics of synchronous and subsequent lesions of SAs, compared to those of TAs. Patients and Methods This is a retrospective study, and patients described in this paper were diagnosed from their first colonoscopy by polypectomy or endoscopic mucosal resection (EMR) via endoscope report files and pathology database files collected between January 2003 and December 2008 in Hiroshima University Hospital (Hiroshima, Japan). The cases that fulfilled the following criteria were selected in this study and were classified into the SA and TA groups: (1) underwent complete colonoscopy, (2) polyp(s) was resected by polypectomy or EMR for full evaluation, (3) diagnosed as SA and/or TA at the initial colonoscopic examination, (4) followed-up after at least one year and had at least one follow-up colonoscopy, (5) if only one SA or TA was present, the polyp was regarded as an index polyp, (6) if synchronous SA and/or TA were present, the largest polyp was regarded as the index polyp, and (7) excluded patients with polyposis syndrome such as
4 Tsumura T, et al 4 familial adenomatous polyposis and hyperplastic/serrated polyposis (HSP), those after colectomy, and those with advanced colorectal cancer (CRC) because of the followed surgical treatment. The diagnosis of all SAs and TAs was confirmed by a pathologist (K.A.). The location of the lesion was divided into proximal (from the cecum to the splenic flexure) and distal (from the descending colon to the rectum). We identified 127 patients in the SA group and 158 randomly selected, age and sex-matched patients, were enrolled in the TA group. The mean follow-up duration was 39.7 months (13-58 months) in the SA group, and 42.7 months (14-62 months) in the TA group. We investigated the number and clinicopathologic features of synchronous and subsequent lesions in both groups. Statistical analysis was evaluated by the chi-square test. p < 0.05 was considered to be significant. Results In the SA group, the male/female ratio was 86/41, and the mean age at the first diagnosis was 63.4 (range 36-91). In the TA group, the male/female ratio was 116/42, and the mean age at the first diagnosis was 65.3 (range 38-88) (Table 1, Figure 1). In the SA group, 19 (15%) patients had synchronous lesions, and 3 (2%) patients had subsequent lesions in the follow-up period (Table 1). In the TA group, 68 (43%) patients had synchronous lesions, and 14 (9%) patients had subsequent lesions in the follow-up period. The frequencies of patients with synchronous and subsequent lesions in the SA group were significantly lower than those in the TA group (p < and p = 0.02 by chi-square test, respectively). As for synchronous lesions, a total of 87 and 196 lesions were detected in the SA group and the TA group, respectively (Table 2). Interestingly, the most frequent synchronous lesion was SA (67%) in the SA group, and TA (95%) in the TA group. Thus, the histology of the index polyp and synchronous lesions was identical in the most patients. No invasive colorectal carcinomas were observed in either group. As for subsequent lesions, a total of 8 and 22 lesions were detected in the SA group and the TA group, respectively (Table 3). No invasive CRCs were observed in either group. The most frequent subsequent lesion was SA (62%) in the SA group, and TA
5 Tsumura T, et al 5 (100%) in the TA group. Thus, similar to synchronous lesions, the histology of the index polyp and subsequent lesions was identical in the most patients. The locations of synchronous and subsequent lesions of both groups are indicated in Table 4. The distribution pattern did not differ significantly between SA and TA groups. Discussion In the present study, we showed that the colonic tumorigenesis potential of patient with SA may differ from that of patient with TA. The frequencies of synchronous and subsequent lesions in the SA group were significantly lower than those in the TA group. In addition to this, the most frequent synchronous and subsequent lesions were SAs in the SA group, and TAs in the TA group. The frequency of SAs has been reported to be 1-2.4% of all colorectal polyps, indicating that SAs are rare polyps in the colorectum [1, 6]. However, 22.6% of rectosigmoid polyps originally diagnosed as hyperplastic polyps (HPs) demonstrated features of SAs on reanalysis [8]. In a recent study, the proportion of SAs among all index polyps was 10% [7]. It has been also reported that serrated adenocarcinoma arising from SA has been reported to account for at least 5.8% of CRCs [5]. These data suggest that SAs may not be rare lesions, but that SAs may be lesions of significant importance. The grade of malignant potential of SAs is of great interest. To evaluate the malignant potential, examination of the incidence of malignant lesions including high-grade dysplasia and carcinoma in SAs is one method. Song et al [8] compared clinicopathologic features of 124 SAs from 116 patients and 419 TAs from 200 randomly selected patients. The incidence of malignant lesions including high-grade dysplasia and carcinoma in SA was found to be lower than in TA (3.2% vs 9.3%, P<0.05). Iwabuchi et al [3] reported that the percentage of concomitant carcinoma in cases of SA was significantly lower than in TA. These data suggest that SAs may be premalignant lesions but have a lower malignant potential than TAs. Examining of synchronous and subsequent lesions of SA compared with those of TA is another method to evaluate the malignant potential of SA. However, there are few reports on characteristics of synchronous and subsequent lesions of SAs compared with
6 Tsumura T, et al 6 those of TAs. To our knowledge, there is only one study on the issue at present. Lazarus et al [5] reported that synchronous lesions identified at the index colonoscopy were of the same histological type as the index polyp (87% of the SA group, 94% of the TA group), and subsequent lesions were also the same histological type as the index polyp (75% of the SA group, 70% of the TA group), which is similar to our results. These findings suggest that the genetic and environmental factors determining the predominant type of polyp may influence the histology of colorectal polyps. In addition, the same authors reported that the frequencies of synchronous and subsequent lesions in the SA group were significantly lower than those in the TA group, which is also similar to our results. Serrated lesions of the colorectum are subclassified primarily into 3 subtypes: hyperplastic polyp, traditional serrated adenoma (TSA) and sessile serrated adenoma/polyp (SSA/P). SSA/P has architectural features that include dilatation of base of the crypts, often with crypts that seem to grow parallel to the muscularis mucosa and result in T- or L-shaped crypts. TSA also has serration but a uniform population of dysplastic epithelial cells that are columnar cells with eosinophilic cytoplasm, and have a villiform configuration and appear protuberant rather than sessile [4]. In the present study, SA included both TSA and SSA/P. Although differences in clinicopathologic and molecular characteristics between these lesions have been reported, histologic diagnosis of these lesions is still confused among pathologists at present. There are some differences in diagnosis of TSA, SSA/P and hyperplastic polyp among pathologists. In addition to this, the number of lesions examined in the present study was relatively limited. Therefore, we did not subclassified the SA in the present study. Of course, further examinations with subclassification of SA may be needed to clarify the differences between TSA and SSA/P. It has been suggested that left- and right-sided colorectal cancers differ in their associated genetic alterations in neoplastic transformation, based on studies in Western countries. For example, microsatellite instability (MSI)-positive cancers are preferentially found in right-sided colon cancers and in older women. Previous study has indicated a higher incidence of CpG island methylator phenotype (CIMP)-positive tumors in right-sided colon cancers compared with left-sided colon cancers. On the other hand, chromosomal instability (CIN) is said to characterize left-sided colorectal cancers. These findings have provided further evidence for the existence of at least two
7 Tsumura T, et al 7 mechanisms of colorectal cancer pathogenesis. One group (CIMP+/MSI+) occurs predominantly in the right side of the colon, and the other (CIN) occurs predominantly in the left side of the colon. There are several studies on genetic alterations of SAs: for example, presence of B-raf or K-ras mutations [9], extensive DNA methylations [10], and inactivation of hmlh1 or MGMT [10, 11]. We previously reported frequent p53 mutations in SAs [12]. Recently, serrated pathway has been proposed as one of carcinogenetic pathways of the colorectum, and are divided into 2 categories: CIMP+/MSI+ cancer with B-raf mutation, and CIMP+/MSI- and B-raf mutation [4]. SSA/P is most often right-sided lesion characterized by B-raf mutation whereas TSA is most often left-sided with K-ras mutation [13]. The B-raf mutation is commonly seen in CIMP+/MSI- cancers (44%) although at a lower frequency than in CIMP+/MSI+ cancers (94%), and MSI+ cancers occur predominantly in the proximal colon. SSA/P is likely to be the principal precursors of MSI+ colorectal cancers [14]. We excluded patients with polyposis syndrome such as familial adenomatous polyposis and HSP in this study. HSP, however, is a distinctive entity. Definition of HSP is as follows; the presence of either (1) >30 HPs/SAs distributed throughout the colon, (2) more than 5 HPs/SAs proximal to the sigmoid colon, of which at least 2 polyps are >1 cm in size, and (3) any number of HPs/SAs located proximal to the sigmoid colon in a patient with a first degree relative with HSP [15]. In the case of HSP, Hyman et al [16] reported that 7 of these 13 (54%) patients with HSP developed CRC during the follow-up period. Rubio et al [17] summarized 30 publications about HSP in , that 51% (67/131) of the HSP patients had CRC at the time of diagnosis of HSP and/or during the follow-up period. This percentage is very high when compared with a recent study of 1,552 consecutive colorectal adenomas, where only 1.7% (27/1,552) showed invasive carcinoma [18], and which reported that the overall lifetime cumulative incidence of CRC in a population is only 5.5% [18, 19]. Several researchers have postulated that, in HSP patients, carcinomas may evolve through the HP-SA sequence [20, 21]. Although patients with SA seem not to be at high risk for CRC development, patients with HSP seem to be at very high risk for CRC development. The prevalence of HSP is still unclear, and the point should also be investigated. In conclusion, our data suggest that the colonic tumorigenesis potential of patient with SA may differ from that of patient with TA. Large-scale, prospective study on the
8 Tsumura T, et al 8 synchronous and subsequent lesions of SAs and TAs of the colorectum should be performed to confirm the results.
9 Tsumura T, et al 9 References 1. Longacre TA, Fenoglio-Preiser CM: Mixed hyperplastic adenomatous polyps/serrated adenomas. A distinct form of colorectal neoplasia. Am J Surg Pathol 1990; 14: Harvey NT, Ruszkiewicz A: Serrated neoplasia of the colorectum. World J Gastroenterol 2007; 13: Iwabuchi M, Sasano H, Hiwatashi N, et al: Serrated adenoma: a clinicopathological, DNA ploidy, and immunohistochomical study. Anticancer Res 2000; 20: Leggett B, Whitehall V. Role of the serrated pathway in colorectal cancer pathogenesis. Gastroenterology 2010; 138: Lazarus R, Juunttila OE, Karttunen TJ, et al: The risk of metachronous neoplasia in parients with serrated adenoma. Am J Clin Pathol 2005; 123: Bariol C, Hawkins NJ, Turner JJ, et al: Histopathological and clinical evaluation of serrated adenomas of the colon and rectum. Mod Pathol 2003; 16: Goldstein NS, Bhanot P, Odish E, et al: Hyperplastic-like colon polyps that preceded microsatellite-unstable adenocarcinomas. Am J Clin Pathol 2003; 119: Song SY, Kim YH, Yu MK, et al: Comparison of malignant potential between serrated adenomas and traditional adenomas. J Gastroenterol Hepatol 2007; 22: Chan TL, Zhao W, Leung SY, et al: BRAF and KRAS mutations in colorectal hyperplastic polyps and serrated adenomas. Cancer Res 2003; 63: Park SJ, Rashid A, Lee JH, et al: Frequent CpG island methylation in serrated adenomas of the colorectum. Am J Pathol 2003; 162: Jass JR, Young J, Leggett BA: Hyperplastic polyps and DNA microsatellite unstable cancers of the colorectum. Histopathology 2000; 37: Hiyama T, Yokozaki H, Shimamoto F, et al: Frequent p53 gene mutations in serrated adenomas of the colorectum. J Pathol 1998; 186: Emina Emilia Torlakovic, Jose D.Gomez, et al: Sessile Serrated Adenoma (SSA) vs. Traditional Serrated Adenoma (TSA). Am J Pathol 2008; 32: T Kambara, L A Simms, et al: BRAF mutation is associated with DNA methylation in serrated polyps and cancers of the colorectum. Gut.bmj.com 2008; 4:
10 Tsumura T, et al Burt RW, Jass J: Hyperplastic polyposis. In World Health Organisation Classification of Tumours Pathology and Genetics, Hamilton SR, Aaltonen LA eds). Springer-Verlag: Berlin, 2000; Hyman NH, Anderson P, Blasyk H: Hyperplastic polyposis and the risk of colorectal cancer. Dis Colon Rectum 2004; 47: Rubio CA, Stemme S, Jaramillo E, et al: Hyperplastic polyposis coli syndrome and colorectal carcinoma. Endoscopy 2006; 38: Rubio CA, Nesi G, Messerini L, et al: Serrated and microtubular colorectal adenomas in Italian patients. A 5-years survey. Anticancer Res 2005; 25: Atkin W, Saunders B. Surveillance guidelines after removal of colorectal adenomatous polyps. Gut 2002; 51(Suppl 5): v6-v Shimamoto F, Tanaka S, Tahara E: Pathogenesis of serrated adenoma of the colorectum: implication for malignant progression. In Molecular pathology of gastroenterological cancer, Tahara E eds). Springer-Verlag; Tokyo, 1997; Oka S, Tanaka S, Hiyama T, et al: Clinicopathologic and endoscopic features of colorectal serrated adenoma: differences between polypoid and superficial types. Gastrointest Endosc 2004; 59:
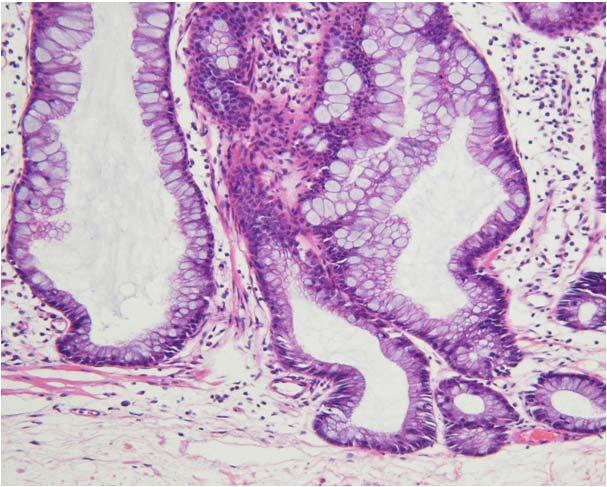
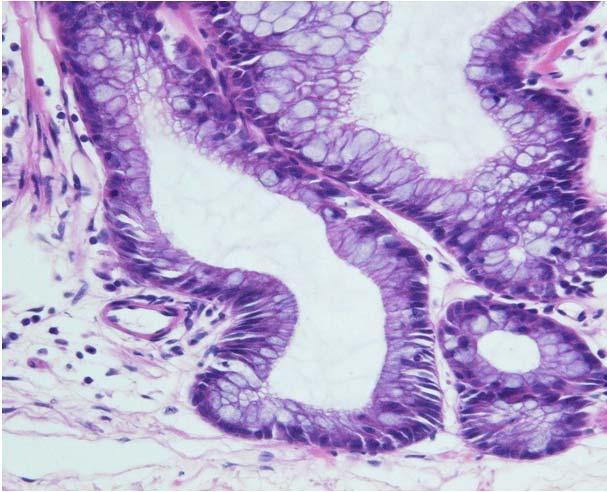
11 Tsumura T, et al 11 Figure Legends Fig. 1. Colonoscopic and microscopic findings of serrated adenoma. a Conventional colonoscopic finding. A sessile polyp is seen in the ascending colon. b Microscopic finding (HE staining, X40). Serrated pattern of the crypt is shown. c Microscopic finding (HE staining, X200). Pseudoinvasion of the tumor into the submucosa is observed. d Microscopic finding (HE staining, X400). The nuclei show atypia.
12 Table 1. Frequencies of patients with synchronous and subsequent lesions in the SA and TA groups SA group (N=127) TA group (N=158) p value Male/female ratio 86/41 116/42 NS Mean age (range) (y) 63.4 (36-91) 65.3 (38-88) NS No. of patients with synchronous lesions 19 (15%) 68 (43%) < No. of patients with subsequent lesions 3 (2%) 14 (9%) 0.02 SA, serrated adenoma; TA, tubular adenoma; NS, not significant.
13 Table 2. Histology of synchronous lesions in the SA and TA groups SA (%) TA (%) HP (%) Total (%) SA group (N=19) 58 (67) 12 (14) 17 (19) 87 (100) TA group (N=68) 0 (0) 187 (95) 9 (5) 196 (100) SA, serrated adenoma; TA, tubular adenoma; HP, hyperplastic polyp.
14 Table 3. Histology of subsequent lesions in the SA and TA groups SA (%) TA (%) HP (%) Total (%) SA group (N=3) 5 (62) 3 (38) 0 (0) 8 (100) TA group (N=14) 0 (0) 22 (100) 0 (0) 22 (100) SA, serrated adenoma; TA, tubular adenoma; HP, hyperplastic polyp.
15 Table 4. locations of synchronous and subsequent lesions of SA and TA groups Proximal Distal p value SA group SA NS TA 11 4 HP 5 12 TA group SA 0 0 NS TA HP 5 4 SA, serrated adenoma; TA, tubular adenoma; HP, hyperplastic polyp, NS, not significant.


16 Fig. 1 A a b B c d
General Session 7: Controversies in Screening and Surveillance in Colorectal Cancer
 General Session 7: Controversies in Screening and Surveillance in Colorectal Cancer Complexities of Pathological Assessment: Serrated Polyps/Adenomas Carolyn Compton, MD, PhD Professor of Life Sciences,
General Session 7: Controversies in Screening and Surveillance in Colorectal Cancer Complexities of Pathological Assessment: Serrated Polyps/Adenomas Carolyn Compton, MD, PhD Professor of Life Sciences,
Serrated Colorectal Polyps New Challenges to Old Dogma. Kenneth Batts, M.D. Abbott Northwestern Hospital Minneapolis, MN
 Serrated Colorectal Polyps New Challenges to Old Dogma Kenneth Batts, M.D. Abbott Northwestern Hospital Minneapolis, MN A Sneak Preview.... This was in the good old days: Adenomas HPPs Mixed Polyps A Sneak
Serrated Colorectal Polyps New Challenges to Old Dogma Kenneth Batts, M.D. Abbott Northwestern Hospital Minneapolis, MN A Sneak Preview.... This was in the good old days: Adenomas HPPs Mixed Polyps A Sneak
Hyperplastische Polyps Innocent bystanders?
 Hyperplastische Polyps Innocent bystanders?? K. Geboes P th l i h O tl dk d Pathologische Ontleedkunde, KULeuven Content Historical Classification Relation Hyperplastic polyps carcinoma The concept cept
Hyperplastische Polyps Innocent bystanders?? K. Geboes P th l i h O tl dk d Pathologische Ontleedkunde, KULeuven Content Historical Classification Relation Hyperplastic polyps carcinoma The concept cept
Serrated Lesions in the Bowel Cancer Screening Programme
 Serrated Lesions in the Bowel Cancer Screening Programme Mark Arends Cambridge & Edinburgh Serrated Lesions of Large Bowel 1. Hyperplastic polyp 2. Serrated adenoma 3. Mixed polyp 4. Sessile serrated lesion
Serrated Lesions in the Bowel Cancer Screening Programme Mark Arends Cambridge & Edinburgh Serrated Lesions of Large Bowel 1. Hyperplastic polyp 2. Serrated adenoma 3. Mixed polyp 4. Sessile serrated lesion
Serrated Polyps, Part 2: Their Mechanisms and Management Ryan C. Romano, DO
 Polyps, Part 2: Their Mechanisms and Management Ryan C. Romano, DO In the prelude to this article ( Polyps Part I: Their Confusing History) we discussed the evolution of colorectal serrated polyp classification,
Polyps, Part 2: Their Mechanisms and Management Ryan C. Romano, DO In the prelude to this article ( Polyps Part I: Their Confusing History) we discussed the evolution of colorectal serrated polyp classification,
Serrated polyps of the colorectum: is sessile serrated adenoma distinguishable from hyperplastic polyp in a daily practice?
 Virchows Arch (2007) 450:613 618 DOI 10.1007/s00428-007-0413-8 ORIGINAL ARTICLE Serrated polyps of the colorectum: is sessile serrated adenoma distinguishable from hyperplastic polyp in a daily practice?
Virchows Arch (2007) 450:613 618 DOI 10.1007/s00428-007-0413-8 ORIGINAL ARTICLE Serrated polyps of the colorectum: is sessile serrated adenoma distinguishable from hyperplastic polyp in a daily practice?
Sessile Serrated Polyps
 Årsmøtet i Den norske Patologforening 2014 Sessile Serrated Polyps Tor J. Eide Oslo Universitetssykehus The term serrated include a group of lesions with a sawtoothlike appearance of the crypts and the
Årsmøtet i Den norske Patologforening 2014 Sessile Serrated Polyps Tor J. Eide Oslo Universitetssykehus The term serrated include a group of lesions with a sawtoothlike appearance of the crypts and the
Alberta Colorectal Cancer Screening Program (ACRCSP) Post Polypectomy Surveillance Guidelines
 Post Polypectomy Surveillance Guidelines") Alberta Colorectal Cancer Screening Program (ACRCSP) Post Polypectomy Surveillance Guidelines June 2013 ACRCSP Post Polypectomy Surveillance Guidelines - 2 TABLE OF CONTENTS Background... 3 Terms, Definitions
Alberta Colorectal Cancer Screening Program (ACRCSP) Post Polypectomy Surveillance Guidelines June 2013 ACRCSP Post Polypectomy Surveillance Guidelines - 2 TABLE OF CONTENTS Background... 3 Terms, Definitions
A WHO update on Serrated Polyps
 A WHO update on Serrated Polyps Arzu Ensari, MD, PhD Department of Pathology Ankara University Medical School Am J Gastroenterol. 2010 Nov 2. [Epub ahead of The Clinical Significance of Serrated Polyps.
A WHO update on Serrated Polyps Arzu Ensari, MD, PhD Department of Pathology Ankara University Medical School Am J Gastroenterol. 2010 Nov 2. [Epub ahead of The Clinical Significance of Serrated Polyps.
Frequency of coexistent carcinoma in sessile serrated adenoma/polyps and traditional serrated adenomas removed by endoscopic resection
 THIEME E451 Frequency of coexistent carcinoma in sessile serrated adenoma/polyps and traditional serrated adenomas removed by endoscopic resection Authors Hirotsugu Saiki 1, Tsutomu Nishida 1, Masashi
THIEME E451 Frequency of coexistent carcinoma in sessile serrated adenoma/polyps and traditional serrated adenomas removed by endoscopic resection Authors Hirotsugu Saiki 1, Tsutomu Nishida 1, Masashi
Serrated Polyps and a Classification of Colorectal Cancer
 Serrated Polyps and a Classification of Colorectal Cancer Ian Chandler June 2011 Structure Serrated polyps and cancer Molecular biology The Jass classification The familiar but oversimplified Vogelsteingram
Serrated Polyps and a Classification of Colorectal Cancer Ian Chandler June 2011 Structure Serrated polyps and cancer Molecular biology The Jass classification The familiar but oversimplified Vogelsteingram
The Importance of Complete Colonoscopy and Exploration of the Cecal Region
 The Importance of Complete Colonoscopy and Exploration of the Cecal Region Kuangi Fu, Takahiro Fujii, Takahisa Matsuda, and Yutaka Saito 2 2.1 The Importance of a Complete Colonoscopy Ever since case-control
The Importance of Complete Colonoscopy and Exploration of the Cecal Region Kuangi Fu, Takahiro Fujii, Takahisa Matsuda, and Yutaka Saito 2 2.1 The Importance of a Complete Colonoscopy Ever since case-control
Endoscopic discrimination of sessile serrated adenomas from other serrated lesions
 ONCOLOGY LETTERS 2: 785-789, 2011 Endoscopic discrimination of sessile serrated adenomas from other serrated lesions SHIN HSEGW 1, KEIICHI MITSUYM 1, HIROSHI KWNO 1, KEIKO RIT 1, YSUHIKO MEYM 1, YOSHITO
ONCOLOGY LETTERS 2: 785-789, 2011 Endoscopic discrimination of sessile serrated adenomas from other serrated lesions SHIN HSEGW 1, KEIICHI MITSUYM 1, HIROSHI KWNO 1, KEIKO RIT 1, YSUHIKO MEYM 1, YOSHITO
A Significant Number of Sessile Serrated Adenomas Might Not Be Accurately Diagnosed in Daily Practice
 Gut and Liver, Vol. 4, No. 4, December 2010, pp. 498-502 original article A Significant Number of Sessile Serrated Adenomas Might Not Be Accurately Diagnosed in Daily Practice Soo Woong Kim*, Jae Myung
Gut and Liver, Vol. 4, No. 4, December 2010, pp. 498-502 original article A Significant Number of Sessile Serrated Adenomas Might Not Be Accurately Diagnosed in Daily Practice Soo Woong Kim*, Jae Myung
Update on Colonic Serrated (and Conventional) Adenomatous Polyps
 Adenomatous Polyps") Update on Colonic Serrated (and Conventional) Adenomatous Polyps Maui, HI 2018 Robert D. Odze, MD, FRCPC Chief, Division of GI Pathology Professor of Pathology Brigham and Women s Hospital Harvard Medical
Update on Colonic Serrated (and Conventional) Adenomatous Polyps Maui, HI 2018 Robert D. Odze, MD, FRCPC Chief, Division of GI Pathology Professor of Pathology Brigham and Women s Hospital Harvard Medical
Update on the serrated pathway to colorectal carcinoma
 Human Pathology (2010) xx, xxx xxx www.elsevier.com/locate/humpath Progress in pathology Update on the serrated pathway to colorectal carcinoma Dale C. Snover MD Department of Pathology, Fairview Southdale
Human Pathology (2010) xx, xxx xxx www.elsevier.com/locate/humpath Progress in pathology Update on the serrated pathway to colorectal carcinoma Dale C. Snover MD Department of Pathology, Fairview Southdale
Pathology of serrated colorectal lesions
 Correspondence to Dr Adrian C Bateman, Department of Cellular Pathology, University Hospital Southampton NHS Foundation Trust, MP002, Level E, South Block, Southampton General Hospital, Tremona Road, Southampton
Correspondence to Dr Adrian C Bateman, Department of Cellular Pathology, University Hospital Southampton NHS Foundation Trust, MP002, Level E, South Block, Southampton General Hospital, Tremona Road, Southampton
Cancer emerging from the recurrence of sessile serrated adenoma/polyp resected endoscopically 5 years ago
 Japanese Journal of Clinical Oncology, 2016, 46(1) 89 95 doi: 10.1093/jjco/hyv154 Advance Access Publication Date: 3 November 2015 Case Report Case Report Cancer emerging from the recurrence of sessile
Japanese Journal of Clinical Oncology, 2016, 46(1) 89 95 doi: 10.1093/jjco/hyv154 Advance Access Publication Date: 3 November 2015 Case Report Case Report Cancer emerging from the recurrence of sessile
Molecular features of colorectal polyps presenting Kudo s type II mucosal crypt pattern: are they based on the same mechanism of tumorigenesis?
 E171 Molecular features of colorectal polyps presenting Kudo s type II mucosal crypt pattern: are they based on the same mechanism of tumorigenesis? Authors Kensuke Shinmura 1, Kazuo Konishi 1, Toshiko
E171 Molecular features of colorectal polyps presenting Kudo s type II mucosal crypt pattern: are they based on the same mechanism of tumorigenesis? Authors Kensuke Shinmura 1, Kazuo Konishi 1, Toshiko
Colonic Polyp. Najmeh Aletaha. MD
 Colonic Polyp Najmeh Aletaha. MD 1 Polyps & classification 2 Colorectal cancer risk factors 3 Pathogenesis 4 Surveillance polyp of the colon refers to a protuberance into the lumen above the surrounding
Colonic Polyp Najmeh Aletaha. MD 1 Polyps & classification 2 Colorectal cancer risk factors 3 Pathogenesis 4 Surveillance polyp of the colon refers to a protuberance into the lumen above the surrounding
Douglas K. Rex, MD Indiana University Hospital Indianapolis, IN
 Serrated Adenomas: What do they mean and what to do about them? Douglas K. Rex, MD Indiana University Hospital Indianapolis, IN Colorectal Cancer Molecular Basis Pathway Frequency Genes MSI Precursor Speed
Serrated Adenomas: What do they mean and what to do about them? Douglas K. Rex, MD Indiana University Hospital Indianapolis, IN Colorectal Cancer Molecular Basis Pathway Frequency Genes MSI Precursor Speed
The Detection of Proximal Colon Polyps and Its Importance in Screening Colonoscopy
 ORIGINAL RESEARCH GASTROENTEROLOGY // INTERNAL MEDICINE The Detection of Proximal Colon Polyps and Its Importance in Screening Colonoscopy Răzvan Opaschi 1, Simona Băţagă 1, Ioan Macarie 2, Imola Török
ORIGINAL RESEARCH GASTROENTEROLOGY // INTERNAL MEDICINE The Detection of Proximal Colon Polyps and Its Importance in Screening Colonoscopy Răzvan Opaschi 1, Simona Băţagă 1, Ioan Macarie 2, Imola Török
Inflammatory bowel disease (IBD) patients have a higher risk of
 patients have a higher risk of") Serrated Colorectal Lesions in Patients With Inflammatory Bowel Disease Alyssa M. Parian, MD, and Mark G. Lazarev, MD Dr Parian and Dr Lazarev are assistant professors of medicine at Johns Hopkins University
Serrated Colorectal Lesions in Patients With Inflammatory Bowel Disease Alyssa M. Parian, MD, and Mark G. Lazarev, MD Dr Parian and Dr Lazarev are assistant professors of medicine at Johns Hopkins University
Sessile serrated polyps: Cancer risk and appropriate surveillance
 REVIEW CME CREDIT EDUCATIONAL OBJECTIVE: Readers will understand the role of the recently recognized serrated neoplasia pathway in the development of colorectal cancer ROHIT MAKKAR, MD St. Michael s Hospital,
REVIEW CME CREDIT EDUCATIONAL OBJECTIVE: Readers will understand the role of the recently recognized serrated neoplasia pathway in the development of colorectal cancer ROHIT MAKKAR, MD St. Michael s Hospital,
Sessile serrated adenomas: prevalence of dysplasia and carcinoma in 2139 patients
 Caris Research Institute, Irving, Texas, USA Correspondence to Richard H Lash, MD, Caris Research Institute, 6655 MacArthur Blvd, Irving, TX 75039, USA; rlash@carisdx.com Accepted 11 March 2010 Published
Caris Research Institute, Irving, Texas, USA Correspondence to Richard H Lash, MD, Caris Research Institute, 6655 MacArthur Blvd, Irving, TX 75039, USA; rlash@carisdx.com Accepted 11 March 2010 Published
Disclaimer: I belong to the speakers bureau of the American Serrated Society, often referred to as the ASS
 An Exposé on Serrated Lesions of the Colorectum How do you know it is a hyperplastic polyp and not something else? How do you know it is something else and not a hyperplastic polyp? Disclaimer: I belong
An Exposé on Serrated Lesions of the Colorectum How do you know it is a hyperplastic polyp and not something else? How do you know it is something else and not a hyperplastic polyp? Disclaimer: I belong
Sessile Serrated Polyps: An Important Route to Colorectal Cancer
 Focused Review 1585 Sessile Serrated Polyps: An Important Route to Colorectal Cancer Matthew F. Kalady, MD Abstract The serrated neoplastic pathway accounts for approximately 30% of colorectal cancers.
Focused Review 1585 Sessile Serrated Polyps: An Important Route to Colorectal Cancer Matthew F. Kalady, MD Abstract The serrated neoplastic pathway accounts for approximately 30% of colorectal cancers.
WEO CRC SC Meeting. Barcelona, Spain October 23, 2015
 WEO CRC SC Meeting Barcelona, Spain October 23, 2015 Identification of serrated polyposis syndrome in the context of population-based CRC screening programs Evelien Dekker Academic Medical Center Amsterdam,
WEO CRC SC Meeting Barcelona, Spain October 23, 2015 Identification of serrated polyposis syndrome in the context of population-based CRC screening programs Evelien Dekker Academic Medical Center Amsterdam,
The Clinical Significance of Serrated Polyps
 CLINICAL AND SYSTEMATIC S nature publishing group 229 CME The Clinical Significance of Serrated Polyps Christopher S. Huang, MD 1, Fr anc is A. Far raye, M D, M S c 1, Sh i Yang, M D 2 and Michael J. O
CLINICAL AND SYSTEMATIC S nature publishing group 229 CME The Clinical Significance of Serrated Polyps Christopher S. Huang, MD 1, Fr anc is A. Far raye, M D, M S c 1, Sh i Yang, M D 2 and Michael J. O
General Surgery Grand Grounds
 General Surgery Grand Grounds University of Colorado Health Sciences Center Case Presentation December 24, 2009 Adam Lackey, PGY-5 J.L. - 2111609 27 YO female with chief complaint of abdominal pain. PMHx:
General Surgery Grand Grounds University of Colorado Health Sciences Center Case Presentation December 24, 2009 Adam Lackey, PGY-5 J.L. - 2111609 27 YO female with chief complaint of abdominal pain. PMHx:
Arzu Ensari, MD, PhD Department of Pathology Ankara University Medical School
 Precursors of Colorectal Carcinoma Arzu Ensari, MD, PhD Department of Pathology Ankara University Medical School Hyperplastic polyp Adenomatous polyp Colorectal carcinoma IBD-associated (1-2%) Sporadic
Precursors of Colorectal Carcinoma Arzu Ensari, MD, PhD Department of Pathology Ankara University Medical School Hyperplastic polyp Adenomatous polyp Colorectal carcinoma IBD-associated (1-2%) Sporadic
D uring the past few years, it has become
 682 REVIEW My approach to serrated polyps of the colorectum T Higuchi, J R Jass... Hyperplastic polyps of the colorectum are heterogeneous lesions, a subset of which is now regarded as the precursor of
682 REVIEW My approach to serrated polyps of the colorectum T Higuchi, J R Jass... Hyperplastic polyps of the colorectum are heterogeneous lesions, a subset of which is now regarded as the precursor of
Characteristics and outcomes of endoscopically resected colorectal cancers that arose from sessile serrated adenomas and traditional serrated adenomas
 ORIGINAL ARTICLE pissn 1598-9100 eissn 2288-1956 http://dx.doi.org/10.5217/ir.2016.14.3.270 Intest Res 2016;14(3):270-279 Characteristics and outcomes of endoscopically resected colorectal cancers that
ORIGINAL ARTICLE pissn 1598-9100 eissn 2288-1956 http://dx.doi.org/10.5217/ir.2016.14.3.270 Intest Res 2016;14(3):270-279 Characteristics and outcomes of endoscopically resected colorectal cancers that
The Detection of Proximal Colon Polyps and Its Importance in Screening Colonoscopy
 ORIGINAL RESEARCH GASTROENTEROLOGY // INTERNAL MEDICINE The Detection of Proximal Colon Polyps and Its Importance in Screening Colonoscopy Răzvan Opaschi 1, Simona Bățagă 1, Ioan Macarie 2, Imola Török
ORIGINAL RESEARCH GASTROENTEROLOGY // INTERNAL MEDICINE The Detection of Proximal Colon Polyps and Its Importance in Screening Colonoscopy Răzvan Opaschi 1, Simona Bățagă 1, Ioan Macarie 2, Imola Török
Large Colorectal Adenomas An Approach to Pathologic Evaluation
 Anatomic Pathology / LARGE COLORECTAL ADENOMAS AND PATHOLOGIC EVALUATION Large Colorectal Adenomas An Approach to Pathologic Evaluation Elizabeth D. Euscher, MD, 1 Theodore H. Niemann, MD, 1 Joel G. Lucas,
Anatomic Pathology / LARGE COLORECTAL ADENOMAS AND PATHOLOGIC EVALUATION Large Colorectal Adenomas An Approach to Pathologic Evaluation Elizabeth D. Euscher, MD, 1 Theodore H. Niemann, MD, 1 Joel G. Lucas,
Arthur Purdy Stout Society of Surgical Pathologists Companion Meeting. Microsatellite Instability and Serrated Adenomas in Common Practice
 Arthur Purdy Stout Society of Surgical Pathologists Companion Meeting Microsatellite Instability and Serrated Adenomas in Common Practice United States and Canadian Academy of Pathology Annual Meeting
Arthur Purdy Stout Society of Surgical Pathologists Companion Meeting Microsatellite Instability and Serrated Adenomas in Common Practice United States and Canadian Academy of Pathology Annual Meeting
Review Article Serrated Polyposis: An Enigmatic Model of Colorectal Cancer Predisposition
 SAGE-Hindawi Access to Research Pathology Research International Volume 2011, Article ID 157073, 13 pages doi:10.4061/2011/157073 Review Article Serrated Polyposis: An Enigmatic Model of Colorectal Cancer
SAGE-Hindawi Access to Research Pathology Research International Volume 2011, Article ID 157073, 13 pages doi:10.4061/2011/157073 Review Article Serrated Polyposis: An Enigmatic Model of Colorectal Cancer
Beyond the APC era Alternative pathways to CRC. Jeremy R Jass McGill University
 Beyond the APC era Alternative pathways to CRC Jeremy R Jass McGill University Outline Limitations of APC model KRAS and serrated polyps CRC and CpG island methylation Serrated pathway to CRC Fusion pathways
Beyond the APC era Alternative pathways to CRC Jeremy R Jass McGill University Outline Limitations of APC model KRAS and serrated polyps CRC and CpG island methylation Serrated pathway to CRC Fusion pathways
PERSPECTIVES IN CLINICAL GASTROENTEROLOGY AND HEPATOLOGY
 CLINICAL GASTROENTEROLOGY AND HEPATOLOGY 2013;11:760 767 PERSPECTIVES IN CLINICAL GASTROENTEROLOGY AND HEPATOLOGY Serrated Colon Polyps as Precursors to Colorectal Cancer SETH SWEETSER,* THOMAS C. SMYRK,
CLINICAL GASTROENTEROLOGY AND HEPATOLOGY 2013;11:760 767 PERSPECTIVES IN CLINICAL GASTROENTEROLOGY AND HEPATOLOGY Serrated Colon Polyps as Precursors to Colorectal Cancer SETH SWEETSER,* THOMAS C. SMYRK,
Endoscopic Corner CASE 1. Kimtrakool S Aniwan S Linlawan S Muangpaisarn P Sallapant S Rerknimitr R
 170 Endoscopic Corner Kimtrakool S Aniwan S Linlawan S Muangpaisarn P Sallapant S Rerknimitr R CASE 1 A 54-year-old woman underwent a colorectal cancer screening. Her fecal immunochemical test was positive.
170 Endoscopic Corner Kimtrakool S Aniwan S Linlawan S Muangpaisarn P Sallapant S Rerknimitr R CASE 1 A 54-year-old woman underwent a colorectal cancer screening. Her fecal immunochemical test was positive.
Serrated architecture in colonic mucosa means having
 A Historical Perspective and Exposé on Serrated Polyps of the Colorectum This article offers a historical perspective on the discovery of 3 types of serrated colorectal polyps recognized in the past 60
A Historical Perspective and Exposé on Serrated Polyps of the Colorectum This article offers a historical perspective on the discovery of 3 types of serrated colorectal polyps recognized in the past 60
SERRATED POLYPS OF THE COLORECTUM: HISTOLOGICAL
 POL J PATHOL 2010; 1: 8-22 SERRATED POLYPS OF THE COLORECTUM: HISTOLOGICAL CLASSIFICATION AND CLINICAL SIGNIFICANCE JANINA ORŁOWSKA Histopathology Laboratory of the Department of Gastroenterology and Hepatology,
POL J PATHOL 2010; 1: 8-22 SERRATED POLYPS OF THE COLORECTUM: HISTOLOGICAL CLASSIFICATION AND CLINICAL SIGNIFICANCE JANINA ORŁOWSKA Histopathology Laboratory of the Department of Gastroenterology and Hepatology,
Neal S. Goldstein, MD. Abstract
 Anatomic Pathology / HIGH-RISK SESSILE SERRATED ADENOMAS Small Colonic Microsatellite Unstable Adenocarcinomas and High-Grade Epithelial Dysplasias in Sessile Serrated Adenoma Polypectomy Specimens A Study
Anatomic Pathology / HIGH-RISK SESSILE SERRATED ADENOMAS Small Colonic Microsatellite Unstable Adenocarcinomas and High-Grade Epithelial Dysplasias in Sessile Serrated Adenoma Polypectomy Specimens A Study
Clinical characteristics of patients with serrated polyposis syndrome in Korea: comparison with Western patients
 ORIGINAL ARTICLE pissn 1598-9100 eissn 2288-1956 https://doi.org/10.5217/ir.2017.15.3.402 Intest Res 2017;15(3):402-410 Clinical characteristics of patients with serrated polyposis syndrome in Korea: comparison
ORIGINAL ARTICLE pissn 1598-9100 eissn 2288-1956 https://doi.org/10.5217/ir.2017.15.3.402 Intest Res 2017;15(3):402-410 Clinical characteristics of patients with serrated polyposis syndrome in Korea: comparison
Morphologic Criteria of Invasive Colonic Adenocarcinoma on Biopsy Specimens
 ISPUB.COM The Internet Journal of Pathology Volume 12 Number 1 Morphologic Criteria of Invasive Colonic Adenocarcinoma on Biopsy Specimens C Rose, H Wu Citation C Rose, H Wu.. The Internet Journal of Pathology.
ISPUB.COM The Internet Journal of Pathology Volume 12 Number 1 Morphologic Criteria of Invasive Colonic Adenocarcinoma on Biopsy Specimens C Rose, H Wu Citation C Rose, H Wu.. The Internet Journal of Pathology.
Hyperplastic-like Colon Polyps That Preceded Microsatellite-Unstable Adenocarcinomas
 Anatomic Pathology / HYPERPLASTIC-LIKE COLON POLYPS PRECEDING MICROSATELLITE-UNSTABLE ADENOCARCINOMAS Hyperplastic-like Colon Polyps That Preceded Microsatellite-Unstable Adenocarcinomas Neal S. Goldstein,
Anatomic Pathology / HYPERPLASTIC-LIKE COLON POLYPS PRECEDING MICROSATELLITE-UNSTABLE ADENOCARCINOMAS Hyperplastic-like Colon Polyps That Preceded Microsatellite-Unstable Adenocarcinomas Neal S. Goldstein,
Neoplastic Colon Polyps. Joyce Au SUNY Downstate Grand Rounds, October 18, 2012
 Neoplastic Colon Polyps Joyce Au SUNY Downstate Grand Rounds, October 18, 2012 CASE 55M with Hepatitis C, COPD (FEV1=45%), s/p vasectomy, knee surgery Meds: albuterol, flunisolide, mometasone, tiotropium
Neoplastic Colon Polyps Joyce Au SUNY Downstate Grand Rounds, October 18, 2012 CASE 55M with Hepatitis C, COPD (FEV1=45%), s/p vasectomy, knee surgery Meds: albuterol, flunisolide, mometasone, tiotropium
Title: Serrated polyposis syndrome associated with long-standing inflammatory bowel disease
 Title: Serrated polyposis syndrome associated with long-standing inflammatory bowel disease Authors: Jesús Castro, Miriam Cuatrecasas, Francesc Balaguer, Elena Ricart, María Pellisé DOI: 10.17235/reed.2017.5068/2017
Title: Serrated polyposis syndrome associated with long-standing inflammatory bowel disease Authors: Jesús Castro, Miriam Cuatrecasas, Francesc Balaguer, Elena Ricart, María Pellisé DOI: 10.17235/reed.2017.5068/2017
The Natural History of Right-Sided Lesions
 The Natural History of Right-Sided Lesions Jasper L.A. Vleugels Dept of Gastroenterology and Hepatology, Academic Medical Center, Amsterdam, the Netherlands. None Disclosures Agenda Is there evidence that
The Natural History of Right-Sided Lesions Jasper L.A. Vleugels Dept of Gastroenterology and Hepatology, Academic Medical Center, Amsterdam, the Netherlands. None Disclosures Agenda Is there evidence that
Gastroenterology, Hepatology & Digestive Disorders
 Research Article Gastroenterology, Hepatology & Digestive Disorders Investigating the Prevalence and Progression of Serrated Polyps Tampa VA Experience Shreya Narayanan MD 1*, Brijesh B. Patel MD 2, David
Research Article Gastroenterology, Hepatology & Digestive Disorders Investigating the Prevalence and Progression of Serrated Polyps Tampa VA Experience Shreya Narayanan MD 1*, Brijesh B. Patel MD 2, David
removal of adenomatous polyps detects important effectively as follow-up colonoscopy after both constitute a low-risk Patients with 1 or 2
 Supplementary Table 1. Study Characteristics Author, yr Design Winawer et al., 6 1993 National Polyp Study Jorgensen et al., 9 1995 Funen Adenoma Follow-up Study USA Multi-center, RCT for timing of surveillance
Supplementary Table 1. Study Characteristics Author, yr Design Winawer et al., 6 1993 National Polyp Study Jorgensen et al., 9 1995 Funen Adenoma Follow-up Study USA Multi-center, RCT for timing of surveillance
Incidence and Multiplicities of Adenomatous Polyps in TNM Stage I Colorectal Cancer in Korea
 Original Article Journal of the Korean Society of J Korean Soc Coloproctol 2012;28(4):213-218 http://dx.doi.org/10.3393/jksc.2012.28.4.213 pissn 2093-7822 eissn 2093-7830 Incidence and Multiplicities of
Original Article Journal of the Korean Society of J Korean Soc Coloproctol 2012;28(4):213-218 http://dx.doi.org/10.3393/jksc.2012.28.4.213 pissn 2093-7822 eissn 2093-7830 Incidence and Multiplicities of
UvA-DARE (Digital Academic Repository) Serrated polyps of the colon and rectum Hazewinkel, Y. Link to publication
 Serrated polyps of the colon and rectum Hazewinkel, Y. Link to publication") UvA-DARE (Digital Academic Repository) Serrated polyps of the colon and rectum Hazewinkel, Y. Link to publication Citation for published version (APA): Hazewinkel, Y. (2014). Serrated polyps of the colon
UvA-DARE (Digital Academic Repository) Serrated polyps of the colon and rectum Hazewinkel, Y. Link to publication Citation for published version (APA): Hazewinkel, Y. (2014). Serrated polyps of the colon
Colorectal adenomatous polyps are precursors of
 GASTROENTEROLOGY 2010;139:1503 1510 The Presence of Large Serrated Polyps Increases Risk for Colorectal Cancer SAKIKO HIRAOKA,* JUN KATO,* SHIGEATSU FUJIKI, EISUKE KAJI,*,, TAMIYA MORIKAWA, TAKATOSHI MURAKAMI,
GASTROENTEROLOGY 2010;139:1503 1510 The Presence of Large Serrated Polyps Increases Risk for Colorectal Cancer SAKIKO HIRAOKA,* JUN KATO,* SHIGEATSU FUJIKI, EISUKE KAJI,*,, TAMIYA MORIKAWA, TAKATOSHI MURAKAMI,
2015 Winter School 대장종양성병변의진단과치료. Dong Kyung Chang. Sungkyunkwan University, School of Medicine Samsung Medical Center
 2017 gastroenterology Winter School 77 2015 Winter School 대장종양성병변의진단과치료 Dong Kyung Chang Sungkyunkwan University, School of Medicine Samsung Medical Center Colon Polyps (Epithelial origin) Neoplastic Premalignant
2017 gastroenterology Winter School 77 2015 Winter School 대장종양성병변의진단과치료 Dong Kyung Chang Sungkyunkwan University, School of Medicine Samsung Medical Center Colon Polyps (Epithelial origin) Neoplastic Premalignant
UvA-DARE (Digital Academic Repository) Serrated polyps of the colon and rectum Hazewinkel, Y. Link to publication
 Serrated polyps of the colon and rectum Hazewinkel, Y. Link to publication") UvA-DARE (Digital Academic Repository) Serrated polyps of the colon and rectum Hazewinkel, Y. Link to publication Citation for published version (APA): Hazewinkel, Y. (2014). Serrated polyps of the colon
UvA-DARE (Digital Academic Repository) Serrated polyps of the colon and rectum Hazewinkel, Y. Link to publication Citation for published version (APA): Hazewinkel, Y. (2014). Serrated polyps of the colon
Colorectal adenocarcinoma leading cancer in developed countries In US, annual deaths due to colorectal adenocarcinoma 57,000.
 Colonic Neoplasia Remotti Colorectal adenocarcinoma leading cancer in developed countries In US, annual incidence of colorectal adenocarcinoma 150,000. In US, annual deaths due to colorectal adenocarcinoma
Colonic Neoplasia Remotti Colorectal adenocarcinoma leading cancer in developed countries In US, annual incidence of colorectal adenocarcinoma 150,000. In US, annual deaths due to colorectal adenocarcinoma
Imaging Evaluation of Polyps. CT Colonography: Sessile Adenoma. Polyps, DALMs & Megacolon Objectives
 Polyps, DALMs & Megacolon: Pathology and Imaging of the Colon and Rectum Angela D. Levy and Leslie H. Sobin Washington, DC Drs. Levy and Sobin have indicated that they have no relationships which, in the
Polyps, DALMs & Megacolon: Pathology and Imaging of the Colon and Rectum Angela D. Levy and Leslie H. Sobin Washington, DC Drs. Levy and Sobin have indicated that they have no relationships which, in the
Romanian Journal of Morphology and Embryology 2006, 47(3):
:") Romanian Journal of Morphology and Embryology 26, 7(3):239 23 ORIGINAL PAPER Predictive parameters for advanced neoplastic adenomas and colorectal cancer in patients with colonic polyps a study in a tertiary
Romanian Journal of Morphology and Embryology 26, 7(3):239 23 ORIGINAL PAPER Predictive parameters for advanced neoplastic adenomas and colorectal cancer in patients with colonic polyps a study in a tertiary
Carol A. Burke, MD, FACG
 Updated Guidelines for CRC C Screening and Surveillance Carol A. Burke MD, FACG, FASGE, FACP Cleveland Clinic, Cleveland, OH Gastroenterology t 2012;143:844 143 Gut 2010;59:666 1 Caveat for all Recommendations
Updated Guidelines for CRC C Screening and Surveillance Carol A. Burke MD, FACG, FASGE, FACP Cleveland Clinic, Cleveland, OH Gastroenterology t 2012;143:844 143 Gut 2010;59:666 1 Caveat for all Recommendations
Page 1. Is the Risk This High? Dysplasia in the IBD Patient. Dysplasia in the Non IBD Patient. Increased Risk of CRC in Ulcerative Colitis
 Screening for Colorectal Neoplasia in Inflammatory Bowel Disease Francis A. Farraye MD, MSc Clinical Director, Section of Gastroenterology Co-Director, Center for Digestive Disorders Boston Medical Center
Screening for Colorectal Neoplasia in Inflammatory Bowel Disease Francis A. Farraye MD, MSc Clinical Director, Section of Gastroenterology Co-Director, Center for Digestive Disorders Boston Medical Center
Magnifying Colonoscopy Findings for Differential Diagnosis of Sessile Serrated Adenoma / Polyps and Hyperplastic Polyps
 ShowaUnivJMedSci282,147154,June2016 Original Magnifying Colonoscopy Findings for Differential Diagnosis of Sessile Serrated Adenoma / Polyps and Hyperplastic Polyps Toshihiro KIHARA 1, Yutaro KUBOTA 1,
ShowaUnivJMedSci282,147154,June2016 Original Magnifying Colonoscopy Findings for Differential Diagnosis of Sessile Serrated Adenoma / Polyps and Hyperplastic Polyps Toshihiro KIHARA 1, Yutaro KUBOTA 1,
Pathology in Slovenian CRC screening programme:
 Pathology in Slovenian CRC screening programme: Findings, organisation and quality assurance Snježana Frković Grazio University Medical Center Ljubljana, Slovenia Slovenia s population: 2 million Incidence
Pathology in Slovenian CRC screening programme: Findings, organisation and quality assurance Snježana Frković Grazio University Medical Center Ljubljana, Slovenia Slovenia s population: 2 million Incidence
Clinicopathological features of colorectal polyps in 2002 and 2012
 ORIGINAL ARTICLE Korean J Intern Med 2019;34:65-71 Clinicopathological features of colorectal polyps in 2002 and 2012 Yoon Jeong Nam, Kyeong Ok Kim, Chan Seo Park, Si Hyung Lee, and Byung Ik Jang Division
ORIGINAL ARTICLE Korean J Intern Med 2019;34:65-71 Clinicopathological features of colorectal polyps in 2002 and 2012 Yoon Jeong Nam, Kyeong Ok Kim, Chan Seo Park, Si Hyung Lee, and Byung Ik Jang Division
Luminal Histological Outline and Colonic Adenoma Phenotypes
 Luminal Histological Outline and Colonic Adenoma Phenotypes CARLOS A. RUBIO Gastrointestinal and Liver Pathology Research Laboratory, Department of Pathology, Karolinska Institute and University Hospital,
Luminal Histological Outline and Colonic Adenoma Phenotypes CARLOS A. RUBIO Gastrointestinal and Liver Pathology Research Laboratory, Department of Pathology, Karolinska Institute and University Hospital,
Clinicopathologic and endoscopic features of early-stage colorectal serrated adenocarcinoma
 Hirano et al. BMC Gastroenterology (2017) 17:158 DOI 10.1186/s12876-017-0702-x RESEARCH ARTICLE Open Access Clinicopathologic and endoscopic features of early-stage colorectal serrated adenocarcinoma Daiki
Hirano et al. BMC Gastroenterology (2017) 17:158 DOI 10.1186/s12876-017-0702-x RESEARCH ARTICLE Open Access Clinicopathologic and endoscopic features of early-stage colorectal serrated adenocarcinoma Daiki
Patologia sistematica V Gastroenterologia Prof. Stefano Fiorucci. Colon polyps. Colorectal cancer
 Patologia sistematica V Gastroenterologia Prof. Stefano Fiorucci Colon polyps Colorectal cancer Harrison s Principles of Internal Medicine 18 Ed. 2012 Colorectal cancer 70% Colorectal cancer CRC and colon
Patologia sistematica V Gastroenterologia Prof. Stefano Fiorucci Colon polyps Colorectal cancer Harrison s Principles of Internal Medicine 18 Ed. 2012 Colorectal cancer 70% Colorectal cancer CRC and colon
INTRODUCTION.
 Citation: (2012) 3, e6; doi:10.1038/ctg.2011.5 & 2012 the American College of Gastroenterology All rights reserved 2155-384x/12 www.nature.com/ctg Prevalence of Different Subtypes of Serrated Polyps and
Citation: (2012) 3, e6; doi:10.1038/ctg.2011.5 & 2012 the American College of Gastroenterology All rights reserved 2155-384x/12 www.nature.com/ctg Prevalence of Different Subtypes of Serrated Polyps and
Original Article Frequent CpG island methylation: a risk factor in the progression of traditional serrated adenoma of the colorectum
 Int J Clin Exp Pathol 2017;10(9):9666-9674 www.ijcep.com /ISSN:1936-2625/IJCEP0045970 Original Article Frequent CpG island methylation: a risk factor in the progression of traditional serrated adenoma
Int J Clin Exp Pathol 2017;10(9):9666-9674 www.ijcep.com /ISSN:1936-2625/IJCEP0045970 Original Article Frequent CpG island methylation: a risk factor in the progression of traditional serrated adenoma
Clinicopathological Study of Serrated Polyps of the Colorectum, with Special Reference to Maspin Expression
 Showa Univ J Med Sci 24 4, 285 292, December 2012 Original Clinicopathological Study of Serrated Polyps of the Colorectum, with Special Reference to Maspin Expression Yasuo OCHIAI 1 2, Nobuyuki OHIKE 1,
Showa Univ J Med Sci 24 4, 285 292, December 2012 Original Clinicopathological Study of Serrated Polyps of the Colorectum, with Special Reference to Maspin Expression Yasuo OCHIAI 1 2, Nobuyuki OHIKE 1,
Accepted Article. Association between the location of colon polyps at baseline and surveillance colonoscopy - A retrospective study
 Accepted Article Association between the location of colon polyps at baseline and surveillance colonoscopy - A retrospective study Ana Oliveira, Paulo Freire, Paulo Souto, Manuela Ferreira, Sofia Mendes,
Accepted Article Association between the location of colon polyps at baseline and surveillance colonoscopy - A retrospective study Ana Oliveira, Paulo Freire, Paulo Souto, Manuela Ferreira, Sofia Mendes,
Clinicopathologic Characteristics of Left-Sided Colon Cancers with High Microsatellite Instability
 The Korean Journal of Pathology 29; 43: 428-34 DOI: 1.4132/KoreanJPathol.29.43.5.428 Clinicopathologic Characteristics of Left-Sided Colon Cancers with High Microsatellite Instability Sang Kyum Kim Junjeong
The Korean Journal of Pathology 29; 43: 428-34 DOI: 1.4132/KoreanJPathol.29.43.5.428 Clinicopathologic Characteristics of Left-Sided Colon Cancers with High Microsatellite Instability Sang Kyum Kim Junjeong
Quality indicators for colonoscopy and colonoscopist. Mirjana Kalauz Clinical Hospital Center Zagreb
 Quality indicators for colonoscopy and colonoscopist Mirjana Kalauz Clinical Hospital Center Zagreb Why is quality monitoring important in CRC screening programme? Quality adjustment in all endoscopic
Quality indicators for colonoscopy and colonoscopist Mirjana Kalauz Clinical Hospital Center Zagreb Why is quality monitoring important in CRC screening programme? Quality adjustment in all endoscopic
IN THE DEVELOPMENT and progression of colorectal
 Digestive Endoscopy 2014; 26 (Suppl. 2): 73 77 doi: 10.1111/den.12276 Treatment strategy of diminutive colorectal polyp
Digestive Endoscopy 2014; 26 (Suppl. 2): 73 77 doi: 10.1111/den.12276 Treatment strategy of diminutive colorectal polyp
6 semanas de embarazo. Tubulovillous adenoma with dysplasia icd 10. Inicio / Embarazo / 6 semanas de embarazo
 Inicio / Embarazo / 6 semanas de embarazo 6 semanas de embarazo Tubulovillous adenoma with dysplasia icd 10 Free, official coding info for 2018 ICD-10-CM D13.2 - includes detailed rules, notes, synonyms,
Inicio / Embarazo / 6 semanas de embarazo 6 semanas de embarazo Tubulovillous adenoma with dysplasia icd 10 Free, official coding info for 2018 ICD-10-CM D13.2 - includes detailed rules, notes, synonyms,
Colon Cancer Screening & Surveillance. Amit Patel, MD PGY-4 GI Fellow
 Colon Cancer Screening & Surveillance Amit Patel, MD PGY-4 GI Fellow Epidemiology CRC incidence and mortality rates vary markedly around the world. Globally, CRC is the third most commonly diagnosed cancer
Colon Cancer Screening & Surveillance Amit Patel, MD PGY-4 GI Fellow Epidemiology CRC incidence and mortality rates vary markedly around the world. Globally, CRC is the third most commonly diagnosed cancer
Index. Note: Page numbers of article titles are in boldface type.
 Index Note: Page numbers of article titles are in boldface type. A Abdominal surgery prior as factor in laparoscopic colorectal surgery, 554 555 Abscess(es) CRC presenting as, 539 540 Adenocarcinoma of
Index Note: Page numbers of article titles are in boldface type. A Abdominal surgery prior as factor in laparoscopic colorectal surgery, 554 555 Abscess(es) CRC presenting as, 539 540 Adenocarcinoma of
Summary. Cezary ŁozińskiABDF, Witold KyclerABCDEF. Rep Pract Oncol Radiother, 2007; 12(4):
:") Rep Pract Oncol Radiother, 2007; 12(4): 201-206 Original Paper Received: 2006.12.19 Accepted: 2007.04.02 Published: 2007.08.31 Authors Contribution: A Study Design B Data Collection C Statistical Analysis
Rep Pract Oncol Radiother, 2007; 12(4): 201-206 Original Paper Received: 2006.12.19 Accepted: 2007.04.02 Published: 2007.08.31 Authors Contribution: A Study Design B Data Collection C Statistical Analysis
Colorectal Neoplasia. Dr. Smita Devani MBChB, MRCP. Consultant Physician and Gastroenterologist Aga Khan University Hospital, Nairobi
 Colorectal Neoplasia Dr. Smita Devani MBChB, MRCP Consultant Physician and Gastroenterologist Aga Khan University Hospital, Nairobi Case History BT, 69yr male Caucasian History of rectal bleeding No change
Colorectal Neoplasia Dr. Smita Devani MBChB, MRCP Consultant Physician and Gastroenterologist Aga Khan University Hospital, Nairobi Case History BT, 69yr male Caucasian History of rectal bleeding No change
Supplementary Appendix
 Supplementary Appendix This appendix has been provided by the authors to give readers additional information about their work. Supplement to: Kaminski MF, Regula J, Kraszewska E, et al. Quality indicators
Supplementary Appendix This appendix has been provided by the authors to give readers additional information about their work. Supplement to: Kaminski MF, Regula J, Kraszewska E, et al. Quality indicators
Serrated and Microtubular Colorectal Adenomas in Italian Patients. A 5-year Survey
 Serrated and Microtubular Colorectal Adenomas in Italian Patients. A 5-year Survey C.A. RUBIO, G. NESI, L. MESSERINI and G. ZAMPI Dipartimento di Patologia Umana ed Oncologia, Universita degli Studi di
Serrated and Microtubular Colorectal Adenomas in Italian Patients. A 5-year Survey C.A. RUBIO, G. NESI, L. MESSERINI and G. ZAMPI Dipartimento di Patologia Umana ed Oncologia, Universita degli Studi di
In current practice in surgical pathology, colorectal polyps
 Colorectal Polyps With Extensive Absorptive Enterocyte Differentiation Histologically Distinct Variant of Hyperplastic Polyps Hidejiro Yokoo, MD; M. Irtaza Usman, Bsc(Hons); Susan Wheaton, MD; Patricia
Colorectal Polyps With Extensive Absorptive Enterocyte Differentiation Histologically Distinct Variant of Hyperplastic Polyps Hidejiro Yokoo, MD; M. Irtaza Usman, Bsc(Hons); Susan Wheaton, MD; Patricia
Diagnostic Difficulties Encountered Among Colorectal Polyps
 Diagnostic Difficulties Encountered Among Colorectal Polyps Rhonda K. Yantiss, M.D. Professor of Pathology and Laboratory Medicine Department of Pathology and Laboratory Medicine Weill Cornell Medical
Diagnostic Difficulties Encountered Among Colorectal Polyps Rhonda K. Yantiss, M.D. Professor of Pathology and Laboratory Medicine Department of Pathology and Laboratory Medicine Weill Cornell Medical
Polypectomy and Local Resections of the Colorectum Structured Pathology Reporting Proforma
 Polypectomy and Local Resections of the Colorectum Structured Pathology Reporting Proforma Mandatory questions (i.e. protocol standards) are in bold (e.g. S1.03). Family name Given name(s) Date of birth
Polypectomy and Local Resections of the Colorectum Structured Pathology Reporting Proforma Mandatory questions (i.e. protocol standards) are in bold (e.g. S1.03). Family name Given name(s) Date of birth
Guidelines for Colonoscopy Surveillance After Screening and Polypectomy: A Consensus Update by the US Multi-Society Task Force on Colorectal Cancer
 Guidelines for Colonoscopy Surveillance After Screening and Polypectomy: A Consensus Update by the US Multi-Society Task Force on Colorectal Cancer David A. Lieberman, 1 Douglas K. Rex, 2 Sidney J. Winawer,
Guidelines for Colonoscopy Surveillance After Screening and Polypectomy: A Consensus Update by the US Multi-Society Task Force on Colorectal Cancer David A. Lieberman, 1 Douglas K. Rex, 2 Sidney J. Winawer,
Screening & Surveillance Guidelines
 Chapter 2 Screening & Surveillance Guidelines I. Eligibility Coloradans ages 50 and older (average risk) or under 50 at elevated risk for colon cancer (personal or family history) that meet the following
Chapter 2 Screening & Surveillance Guidelines I. Eligibility Coloradans ages 50 and older (average risk) or under 50 at elevated risk for colon cancer (personal or family history) that meet the following
SOME OBSERVATIONS ON COLORECTAL POLYPS; ONLY CONCERNS THOSE WHO HAVE A COLON.
 SOME OBSERVATIONS ON COLORECTAL POLYPS; ONLY CONCERNS THOSE WHO HAVE A COLON. Dr Castleman Harvard In 1951 Dr. Benjamin Castleman succeeded Dr. Mallory as Chief of Pathology and Editor of the Case Records
SOME OBSERVATIONS ON COLORECTAL POLYPS; ONLY CONCERNS THOSE WHO HAVE A COLON. Dr Castleman Harvard In 1951 Dr. Benjamin Castleman succeeded Dr. Mallory as Chief of Pathology and Editor of the Case Records
Research Article The CIMP Phenotype in BRAF Mutant Serrated Polyps from a Prospective Colonoscopy Patient Cohort
 Gastroenterology Research and Practice, Article ID 374926, 1 pages http://dx.doi.org/1.1155/214/374926 Research Article The CIMP Phenotype in BRAF Mutant Serrated Polyps from a Prospective Colonoscopy
Gastroenterology Research and Practice, Article ID 374926, 1 pages http://dx.doi.org/1.1155/214/374926 Research Article The CIMP Phenotype in BRAF Mutant Serrated Polyps from a Prospective Colonoscopy
Incidence and Management of Hemorrhage after Endoscopic Removal of Colorectal Lesions
 Showa Univ J Med Sci 12(3), 253-258, September 2000 Original Incidence and Management of Hemorrhage after Endoscopic Removal of Colorectal Lesions Masaaki MATSUKAWA, Mototsugu FUJIMORI, Takahiko KOUDA,
Showa Univ J Med Sci 12(3), 253-258, September 2000 Original Incidence and Management of Hemorrhage after Endoscopic Removal of Colorectal Lesions Masaaki MATSUKAWA, Mototsugu FUJIMORI, Takahiko KOUDA,
Background: The value of narrow band imaging (NBI) for detecting serrated lesions is
 for detecting serrated lesions is") Narrow-band imaging versus white light for the detection of proximal colon serrated lesions: a randomized, controlled trial Douglas K. Rex, Ryan Clodfelter, Farrah Rahmani, Hala Fatima, Toyia N. James-Stevenson,
Narrow-band imaging versus white light for the detection of proximal colon serrated lesions: a randomized, controlled trial Douglas K. Rex, Ryan Clodfelter, Farrah Rahmani, Hala Fatima, Toyia N. James-Stevenson,
Colon Cancer and Hereditary Cancer Syndromes
 Colon Cancer and Hereditary Cancer Syndromes Gisela Keller Institute of Pathology Technische Universität München gisela.keller@lrz.tum.de Colon Cancer and Hereditary Cancer Syndromes epidemiology models
Colon Cancer and Hereditary Cancer Syndromes Gisela Keller Institute of Pathology Technische Universität München gisela.keller@lrz.tum.de Colon Cancer and Hereditary Cancer Syndromes epidemiology models
Diminutive and Small Colorectal Polyps: The Pathologist s Perspective
 REVIEW Clin Endosc 2014;47:404-408 Print ISSN 2234-2400 / On-line ISSN 2234-2443 http://dx.doi.org/10.5946/ce.2014.47.5.404 Open Access Diminutive and Small Colorectal Polyps: The Pathologist s Perspective
REVIEW Clin Endosc 2014;47:404-408 Print ISSN 2234-2400 / On-line ISSN 2234-2443 http://dx.doi.org/10.5946/ce.2014.47.5.404 Open Access Diminutive and Small Colorectal Polyps: The Pathologist s Perspective
colorectal cancer Colorectal cancer hereditary sporadic Familial 1/12/2018
 colorectal cancer Adenocarcinoma of the colon and rectum is the third most common site of new cancer cases and deaths in men (following prostate and lung or bronchus cancer) and women (following breast
colorectal cancer Adenocarcinoma of the colon and rectum is the third most common site of new cancer cases and deaths in men (following prostate and lung or bronchus cancer) and women (following breast
Quality ID #343: Screening Colonoscopy Adenoma Detection Rate National Quality Strategy Domain: Effective Clinical Care
 Quality ID #343: Screening Colonoscopy Adenoma Detection Rate National Quality Strategy Domain: Effective Clinical Care 2018 OPTIONS FOR INDIVIDUAL MEASURES: REGISTRY ONLY MEASURE TYPE: Outcome DESCRIPTION:
Quality ID #343: Screening Colonoscopy Adenoma Detection Rate National Quality Strategy Domain: Effective Clinical Care 2018 OPTIONS FOR INDIVIDUAL MEASURES: REGISTRY ONLY MEASURE TYPE: Outcome DESCRIPTION:
Molecular Differences between Sporadic Serrated and Conventional Colorectal Adenomas
 3082 Vol. 10, 3082 3090, May 1, 2004 Clinical Cancer Research Molecular Differences between Sporadic Serrated and Conventional Colorectal Adenomas Kazuo Konishi, 1 Toshiko Yamochi, 2 Reiko Makino, 1,3
3082 Vol. 10, 3082 3090, May 1, 2004 Clinical Cancer Research Molecular Differences between Sporadic Serrated and Conventional Colorectal Adenomas Kazuo Konishi, 1 Toshiko Yamochi, 2 Reiko Makino, 1,3
what is the alternative mechanism of histogenesis? Aspects of the morphology of the adenomacarcinoma Morphology of the
 Refer to: Morson B: Polyps and cancer of the large bowel. West J Med 125:93-99, Aug 1976 THE WESTERN Journal of Miedicine Polyps and Cancer of the Large Bowel BASIL MORSON, MD, London MORTALITY STATISTICS
Refer to: Morson B: Polyps and cancer of the large bowel. West J Med 125:93-99, Aug 1976 THE WESTERN Journal of Miedicine Polyps and Cancer of the Large Bowel BASIL MORSON, MD, London MORTALITY STATISTICS
Chromoendoscopy and Endomicroscopy for detecting colonic dysplasia
 Chromoendoscopy and Endomicroscopy for detecting colonic dysplasia Ralf Kiesslich I. Medical Department Johannes Gutenberg University Mainz, Germany Cumulative cancer risk in ulcerative colitis 0.5-1.0%
Chromoendoscopy and Endomicroscopy for detecting colonic dysplasia Ralf Kiesslich I. Medical Department Johannes Gutenberg University Mainz, Germany Cumulative cancer risk in ulcerative colitis 0.5-1.0%
Clinical outcomes of the resect and discard strategy using magnifying narrow-band imaging for small (<10 mm) colorectal polyps
 colorectal polyps") Original article Clinical outcomes of the resect and discard strategy using magnifying narrow-band imaging for small (
Original article Clinical outcomes of the resect and discard strategy using magnifying narrow-band imaging for small (
What Every Pathologist Wants the GI Nurse to Know (and how you can help us help you)
") What Every Pathologist Wants the GI Nurse to Know (and how you can help us help you) Jonathan N. Glickman MD PhD Director, GI Pathology, Caris Diagnostics, Newton, MA Associate Professor of Pathology,
What Every Pathologist Wants the GI Nurse to Know (and how you can help us help you) Jonathan N. Glickman MD PhD Director, GI Pathology, Caris Diagnostics, Newton, MA Associate Professor of Pathology,
The Usefulness Of Narrow Band Imaging Endoscopy For The Real Time Characterization Of Colonic Lesions
 Acta Medica Marisiensis 2016;62(2):182-186 DOI: 10.1515/amma-2016-0004 RESEARCH ARTICLE The Usefulness Of Narrow Band Imaging Endoscopy For The Real Time Characterization Of Colonic Lesions Boeriu Alina
Acta Medica Marisiensis 2016;62(2):182-186 DOI: 10.1515/amma-2016-0004 RESEARCH ARTICLE The Usefulness Of Narrow Band Imaging Endoscopy For The Real Time Characterization Of Colonic Lesions Boeriu Alina