ESMO Preceptorship Programme, Colorectal Cancer, Vienna
|
|
|
- Vivian Willis
- 5 years ago
- Views:
Transcription
1 State of the art multimodal treatment of anal cancer ESMO Preceptorship Programme, Colorectal Cancer, Vienna Rob Glynne-Jones Mount Vernon Centre for Cancer Treatment
2 Disclosures: last 5 years Speaker: Roche, Merck Serono, Sanofi Aventis, Pfizer Advisory Boards: Roche, Merck Serono, Sanofi Aventis, Astra Zeneca Funding to attend meetings: Roche, Merck Serono, Sanofi Aventis, Research funding: Roche, Merck Serono, Sanofi Aventis
3 Topics Specialised MDT Imaging Dose of RT brachytherapy Decision regarding drugs with CRT Interval to wait before assessment Surgical Salvage Checkpoint inhibition/pd-1 Drugs for metastatic disease

4 You need a Team!
5
6 Nigro suggested that CTRT Low doses of RT - 30Gy could achieve path CR in tumours 5cm or less Response is sustained Failure to respond is usually associated with rapid systemic relapse

7 Anal canal squamous cell carcinoma should not be treated by the same procedure as adenocarcinoma of the lower rectum, because both these diseases differ markedly.
8
9 Squamous carcinoma of anus Three phase III trials UKCCCR ACT 1 n=585 EORTC n=110 RTOG 87-04/ECOG 1289 n=310 Three phase III trials UKCCCR ACT II n=940 RTOG 9811 n=644 ACCORD-03 n=307
10 Anal cancer Predominantly loco-regional disease
11 Role of surgery limited Radical surgery if RT contraindicated If already administered Defunctioning stoma Transposition of the ovaries Salvage APER Local excision
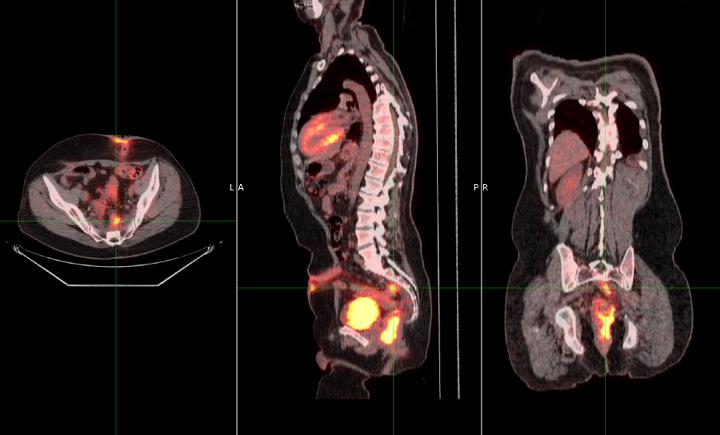
12 Work-up and diagnosis Standard work up includes proctoscopy Examination under anaesthetic (EUA) is necessary on occasions in anal cancer to inspect and obtain biopsy Pelvic MRI mandatory for loco-regional staging TRUS if MRI not available but difficult in advanced anal lesions Whole body CT to determine if metastatic disease Positron emission tomography (PET/CT) scan

13 N1 Stage Perirectal nodes N1 Stage disease: Several perirectal lymph nodes are seen within the mesorectum. The veins surrounding the anal canal drain cranially and therefore mesorectal nodes are often a first side of nodal disease.
14
15 We investigated Chemotherapy Options Induction chemotherapy prior to CRT Different concurrent chemotherapy in CRT Consolidation chemotherapy after CRT
16 Concurrent Chemoradiation 03/01/13
17 Mid eighties first phase III trials Arm A Arm B EORTC RT RT + 5 FU-Mito C UKCCCR ACT I RT RT + 5 FU-Mito C US RTOG 8704 RT+ 5 FU RT + 5 FU-Mito C
18 ACT I - Trial Design Pts with epidermoid anal cancer 585 randomised Randomisation Radiotherapy (45Gy in 20/25#) Radiotherapy + 5FU + MMC 290 pts radiotherapy alone (RT) 295 pts chemoradiation (CMT) Assessed at 6 weeks Poor response salvage surgery 50% response boost radiotherapy 285 eligible 5 ineligible 292 eligible 3 ineligible
19 75 UKCCR ACT I local failure HR 0.46, p<0.001 RT alone CMT Percentage of patients having a local relapse (%) Time since randomisation (years) 03/01/13
20 ACT I Phase III Trial Time to Disease by T Stage N/K T1 T2 T3 T4 CMT betterrt better CMT RT /11 (36%) (63%) 5/8 7/35 (20%) (50%) 18/36 26/84 (31%) (53%) 53/100 41/111 (37%) (65%) 70/108 25/43 (58%) (83%) 24/29 Combined Stratified by T Stage /284 (36%) (60%) 170/281
21 EORTC trial DFS 68 vs 55 % at 3 years p = 0,03 Colostomy FS 72 vs 47 % at 3 years p = H. Bartelink, J Clin Oncol 1997 : Colostomy free survival
22 RTOG trial XRT+ 5 FU XRT + 5 FU-MMC p value Complete response Colostomy- free survival 86% 92.2% 59% 71% Colostomy rate 22% 9% DFS 51% 73% OS 71% 78% 0.1
23 Intergroup RTOG CMT 45 to 59 Gy + 5-FU/MMC T2-4 N0 N+ R 5-FU-CDDP 2 NACT cycles then RT 45 to FU/CDDP
24 RTOG updated JCO 2012
25 ACCORD 03 Titre du diagramme R CT CDDP 5FU 2 cycles CT CDDP 5FU 2 cycles No CT No CT 45 Gy CDDP 5 FU 2 cycles 45 Gy CDDP 5 FU 2 cycles 45 Gy CDDP 5 FU 2 cycles 45 Gy CDDP 5 FU 2 cycles low boost 15 Gy high boost Gy low boost 15 Gy high boost Gy
26 ACT II Trial Design n=940 - Recruitment Arm 1 MMC 5FU 50.4Gy Arm 2 MMC 5FU 50.4Gy CisP 5FU x 2 Arm 3 CisP 5FU 50.4Gy Arm 4 CisP 5FU 50.4Gy CisP 5FU x 2
27 ACT II Chemoradiation Treatment RT week 5FU MMC mg/m 2 d1-4 & hour continuous iv infusion 12mg/m 2 d1 only iv bolus, max single dose 20 mg RT week 5FU CisP mg/m 2 d1-4 & hour continuous iv infusion 60mg/m 2 d1 & 29 iv infusion

28 ACT II Radiotherapy 50.4 Gy 28 daily fractions 5 ½ weeks Two-phase technique Both phases planned simultaneously
 Median age 62 (29-85) 55 (25-83) 57 (25-85) 58 (25 81) RT OTT in days Not stated Median 49 days (Kachnic) Median 45 days (range 1-158) Median 38 days (range a-b) Median Total Between 41.")
29 Comparison of trials (Not Accord Brachtherapy) Factor RTOG 8704 RT + FU + MMC (n = 146) RTOG 9811 RT + FU + MMC (n = 324) Combined RTOG RT + FU + MMC (n = 472) ACT II RT + FU + MMC (n = 472) Median age 62 (29-85) 55 (25-83) 57 (25-85) 58 (25 81) RT OTT in days Not stated Median 49 days (Kachnic) Median 45 days (range 1-158) Median 38 days (range a-b) Median Total Between Gy 50.4Gy 50.4 Gy primary central axis dose in Gy and 47.25Gy (range 9-69Gy) (range Gy) (range 9 54 Gy) RT intensity Not possible to ( Range 1.29 (Range a-b) calculate )
30 ACT II CR at 26 weeks Difference (95% CI) P value MMC CisP 83% (358/432) 84% (362/431) +1% (-3.8 to 6.1) p =0.66 No Maint Mainten 82% (337/409) 85% (348/410) +3% (-2.6 to 7.5) p = 0.34

31 Acute Grade 3/4 Toxicity CRT Comparison P= % 72% P<0.001 % 26% 16% MMC CisP Haematological Overall
32 ACT II Progression free survival Comparison group 3-year rate, % (95%CI) 5-year rate, % (95% CI) HR (95% CI), p value MMC 73 (69 to 77) 69 (65 to 73) CisP 74 (69 to 77) 69 (64 to 73) 0.95 (0.75 to 1.19), p= 0.63 No-maint 73 (68 to 77) 69 (64 to 73) Maint 74 (69 to 77) 70 (65 to 74) 0.95 (0.75 to 1.21), p=0.70
33 ACT II Progression free survival According to T stage 3-year rate, % (95% CI) 5-year rate, % (95% CI) T1/T2 81 (78 to 85) 77 (73 to 81) T3/T4 64 (59 to 68) 60 (55 to 64) According to N stage Negative 76 (72 to 79) 72 (68 to 76) Positive 68 (62 to 73) 62 (56 to 68)
34 ACT II Overall survival Comparison group 3-year rate, % (95%CI) 5-year rate, % (95% CI) HR (95% CI), p value MMC 84 (80 to 87) 79 (74 to 82) CisP 84 (80 to 87) 77 (73 to 81) 1.05 (0.80to 1.38), p=0.70 No-maint 85 (81 to 88) 79 (75 to 83) Maint 83 (79 to 86) 76 (72 to 80) 1.07 (0.81 to 1.41). p=0.65
35 Conclusions from ACT II MMC/cisplatin no difference Maintenance chemo no benefit Majority of survivors with morbidity 03/01/13
36 Impact of RT Compliance on PFS n=933 Group Total events 3 year PFS Treatment adjusted HR (95% CI) A. 50.4Gy per protocol 221/786 (28%) 76% 1.00 P value B. < 40Gy 11/18 (61%) 44% 3.71 ( ) C. > Gy in 23-27F 11/21 (52%) 56% 2.26 ( ) D. 50.4Gy in > 42 days 39/93 (42%) 62% 1.62 ( ) E. >52Gy compensated 6/15 (40%) 59% 1.60 ( )
37 Impact of RT Compliance on PFS n=933
38 Impact of CT Compliance on PFS n=862
39 Conclusions In ACT II poor treatment compliance adversely impacted on PFS for both Radiotherapy (lower dose and or prolonged OTT Chemotherapy in week 5 Interruptions in radiotherapy should be minimised Unavoidable prolonged treatment times require compensation by additional doses or hyperfractionation There are no significant predictive factors for poor compliance Patients with poor compliance may need closer monitoring
40 Key learning points Currently 5FU/MMC is the standard partner for CRT (NB no data on late toxicity or second malignancy)
41 Capecitabine integrated into CRT in anal cancer Study RT MMC Capecitabine Glynne-Jones Gy in 28 fractions in 2 phases Single dose of MMC 12mg/m2 max 20mg 825 mg/m 2 b.i.d on radiation days Deenen Gy in 33 fractions with SIB- IMRT Single dose of MMC 10mg/m2 max 15mg 825 mg/m 2 b.i.d on radiation days Wan Gy Two doses But compliance poor if Capecitabine 825 mg/m 2 b.i.d on radiation days
42 Trials with Cetuximab in anal cancer Trial N of patients IMRT Regimen Toxicity Efficacy Olivatto et al, Cancer (stopped DLT) No 5-FU/CP +RT + cetuximab High OK ACCORD 16 Deutsch et al Ann Oncol (stopped DLT) No 5-FU/CP +RT + cetuximab High low Levy et al Radiother Oncol 2015 ECOG 3205, J Clin Oncol some 5-FU/CP +RT + cetuximab?ok?ok Norwegian Study Leon et al in press 13 (complete) Yes 5-FU/MMC +RT + cetuximab??
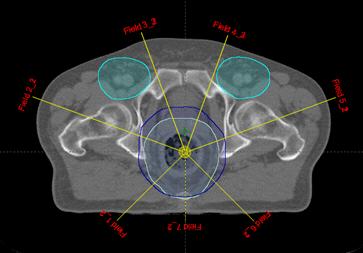
43 IMRT


44 IMRT Michael NG et al, IJROBP 2012
45 Summary of IMRT Dosimetric studies and clinical trials have shown reduced dosing and toxicity to normal structures with the use of IMRT. No decreases in treatment effectiveness or local control rates have been detected. Limited sample sizes and duration of follow-up minimize the ability to detect small variations in local control rates.
46 ACT II how long is it safe to wait? Conclusions Excellent CR rate at 6 months - 84% 83% v 151/209 (72%) patients not in ccr at Assessment 1 (11 weeks) achieved ccr at 18 or 26 weeks. Assessment safe at 26 weeks

47 Surgical Salvage Not the same as APER in rectal cancer Often late effects of radiotherapy En bloc resection of adjacent viscera more common Need for reconstruction R0 important for survival

48 Salisbury Colorectal Prognosis Post salvage 40-60% at 5years No salvage 5% at 3 years Renehan et al. BJS 2005
49 IRCI anal cancer metastatic trial
50 HPV and viral gene products E6 and E7 Responsible for the oncogenic potential of the virus Inhibits normal cell cycle checkpoints and induces cell division
51 ADXS immunotherapy live attenuated Listeria monocytogenes (Lm) bioengineered to secrete a HPV-16-E7 fusion protein targeting HPV transformed cells. Anal cancer cells infected with HPV have the tumour associated antigen HPV E7. So ADXS causes antigen presenting cells to be stimulated to facilitate immune cells to attach to cancer cells expressing HPV E7
52 Pembrolizumab a humanized monoclonal antibody against PD-1 25 heavily pretreated patients with PD-L1-positive advanced SCCA Overall response rate of 5/25 (20%) Stable disease in a further 10/25 patients (40%) (Ott P et al. Preliminary safety and efficacy results from KEYNOTE-028 ESMO 2015).

53 Precision radiotherapy dose in anal cancer (PLATO) T1 N0 Anal margin T1,T2<4cm N0 ACT3 Standard T3/4 NO T2N2, T3/4 N1-3 ACT4 53.2Gy 28F 58.8Gy 28F 61.6Gy 28F 41.4Gy 23F 50.4Gy 28F 41.4Gy 23F Pilot Ph II Courtesy of David Sebag-Montefiore Phase II trial Ph III Stratify for Cape vs. 5-FU Phase II/III trial
54 Conclusions Ideally patients should be treated in specialist units Imaging with CT and MRI? PET Advice re smoking Limited local excisions CRT with 5FU and MMC IMRT better for toxicity and compliance RT dose open Assess CCR up to 6 months Surveillance
55 03/01/13 Thank you for listening
56 Induction chemotherapy delays the start of definitive CRT: Any initial beneficial response to chemo may be lost owing to More proliferation prior to start of CRT. Acute toxicity causing delay to CRT Development of resistance mechanisms. Creating inherent bias in terms of smaller dose/field size
57 Aim to discuss - Chemotherapy Role of capecitabine Role of MMC (1 or 2 doses) Role of cisplatin Role of Cetuximab/panitumumab Neoadjuvant chemotherapy Palliative chemotherapy IRCI Where do we go from here?
58 Dose of synchronous cisplatin used in the ACT II study 60 mg/m2 compared with 100 mg/m2 used commonly in head and neck cancer (Where it is important to ensure 3 rd dose is applied)
Rob Glynne-Jones Mount Vernon Cancer Centre
 ESMO Preceptorship Programme Colorectal Cancer Prague July 2016 State of the art: Standard of care for anal squamous cancer Rob Glynne-Jones Mount Vernon Cancer Centre Aim to discuss Background The trials
ESMO Preceptorship Programme Colorectal Cancer Prague July 2016 State of the art: Standard of care for anal squamous cancer Rob Glynne-Jones Mount Vernon Cancer Centre Aim to discuss Background The trials
Rob Glynne-Jones Mount Vernon Cancer Centre
 ESMO Preceptorship Programme Anal Cancer Valencia May 2018 Standard of care for anal squamous cancer Rob Glynne-Jones Mount Vernon Cancer Centre My Disclosures: last 5 years Speaker: Roche, Merck Serono,
ESMO Preceptorship Programme Anal Cancer Valencia May 2018 Standard of care for anal squamous cancer Rob Glynne-Jones Mount Vernon Cancer Centre My Disclosures: last 5 years Speaker: Roche, Merck Serono,
Carcinoma del Canale Anale. Approcci RadioChemioterapici. Antonino De Paoli.. Oncologia Radioterapica, CRO Aviano.
 Carcinoma del Canale Anale Approcci RadioChemioterapici Antonino De Paoli.. Oncologia Radioterapica, CRO Aviano. Anal Cancer Epidemiology and Risk Factors Uncommon Disease; 2-4% of all GI Tumors Increasing
Carcinoma del Canale Anale Approcci RadioChemioterapici Antonino De Paoli.. Oncologia Radioterapica, CRO Aviano. Anal Cancer Epidemiology and Risk Factors Uncommon Disease; 2-4% of all GI Tumors Increasing
3/8/2014. Case Presentation. Primary Treatment of Anal Cancer. Anatomy. Overview. March 6, 2014
 Case Presentation Primary Treatment of Anal Cancer 65 year old female presents with perianal pain, lower GI bleeding, and anemia with Hb of 7. On exam 6 cm mass protruding through the anus with bulky R
Case Presentation Primary Treatment of Anal Cancer 65 year old female presents with perianal pain, lower GI bleeding, and anemia with Hb of 7. On exam 6 cm mass protruding through the anus with bulky R
Supplementary appendix
 Supplementary appendix This appendix formed part of the original submission and has been peer reviewed. We post it as supplied by the authors. Supplement to: James RD, Glynne-Jones R, Meadows HM, et al.
Supplementary appendix This appendix formed part of the original submission and has been peer reviewed. We post it as supplied by the authors. Supplement to: James RD, Glynne-Jones R, Meadows HM, et al.
Adjuvant Chemotherapy for Rectal Cancer: Are we making progress?
 Adjuvant Chemotherapy for Rectal Cancer: Are we making progress? Hagen Kennecke, MD, MHA, FRCPC Division Of Medical Oncology British Columbia Cancer Agency October 25, 2008 Objectives Review milestones
Adjuvant Chemotherapy for Rectal Cancer: Are we making progress? Hagen Kennecke, MD, MHA, FRCPC Division Of Medical Oncology British Columbia Cancer Agency October 25, 2008 Objectives Review milestones
Rob Glynne-Jones Mount Vernon Cancer Centre
 ESMO Preceptorship Programme Colorectal Cancer Valencia May 2018 State of the art: Standards of care in preoperative treatment for rectal cancer Rob Glynne-Jones Mount Vernon Cancer Centre My Disclosures:
ESMO Preceptorship Programme Colorectal Cancer Valencia May 2018 State of the art: Standards of care in preoperative treatment for rectal cancer Rob Glynne-Jones Mount Vernon Cancer Centre My Disclosures:
Carcinoma del retto: Highlights
 Carcinoma del retto: Highlights Stefano Cordio Struttura Complessa di Oncologia Medica ARNAS Garibaldi Catania Roma 17 Febbraio 2018 Disclosures Advisory Committee, research funding and speakers bureau
Carcinoma del retto: Highlights Stefano Cordio Struttura Complessa di Oncologia Medica ARNAS Garibaldi Catania Roma 17 Febbraio 2018 Disclosures Advisory Committee, research funding and speakers bureau
Radiotherapy for rectal cancer. Karin Haustermans Department of Radiation Oncology
 Radiotherapy for rectal cancer Karin Haustermans Department of Radiation Oncology O U T L I N E RT with TME surgery? Neoadjuvant or adjuvant RT? 5 x 5 Gy or long-course CRT? RT with new drugs? Selection
Radiotherapy for rectal cancer Karin Haustermans Department of Radiation Oncology O U T L I N E RT with TME surgery? Neoadjuvant or adjuvant RT? 5 x 5 Gy or long-course CRT? RT with new drugs? Selection
The optimum time to assess complete clinical response (CR)
") The optimum time to assess complete clinical response (CR) following chemoradiation (CRT) using mitomycin C (MMC) or Cisplatin (CisP) with or without Maintenance CisP/5FU in squamous cell carcinoma of
The optimum time to assess complete clinical response (CR) following chemoradiation (CRT) using mitomycin C (MMC) or Cisplatin (CisP) with or without Maintenance CisP/5FU in squamous cell carcinoma of
Locally advanced disease & challenges in management
 Gynecologic Cancer InterGroup Cervix Cancer Research Network Cervix Cancer Education Symposium, February 2018 Locally advanced disease & challenges in management Carien Creutzberg Radiation Oncology, Leiden
Gynecologic Cancer InterGroup Cervix Cancer Research Network Cervix Cancer Education Symposium, February 2018 Locally advanced disease & challenges in management Carien Creutzberg Radiation Oncology, Leiden
Dr Mark Saunders Christie Hospital and Paterson Institute of Cancer Research. Anal cancer chemoradiotherapy
 Dr Mark Saunders Christie Hospital and Paterson Institute of Cancer Research Anal cancer chemoradiotherapy No disclosures to declare Anal tumours - pathology SCC Basaloid* Cloacogenic (transitional)* Adenocarcinoma
Dr Mark Saunders Christie Hospital and Paterson Institute of Cancer Research Anal cancer chemoradiotherapy No disclosures to declare Anal tumours - pathology SCC Basaloid* Cloacogenic (transitional)* Adenocarcinoma
Department of Radiotherapy, Pt. BDS PGIMS, Rohtak, Haryana, India
 Bharti et al., IJPSR, 2010; Vol. 1 (11): 169-173 ISSN: 0975-8232 IJPSR (2010), Vol. 1, Issue 11 (Research Article) Received on 29 September, 2010; received in revised form 21 October, 2010; accepted 26
Bharti et al., IJPSR, 2010; Vol. 1 (11): 169-173 ISSN: 0975-8232 IJPSR (2010), Vol. 1, Issue 11 (Research Article) Received on 29 September, 2010; received in revised form 21 October, 2010; accepted 26
De-Escalate Trial for the Head and neck NSSG. Dr Eleanor Aynsley Consultant Clinical Oncologist
 De-Escalate Trial for the Head and neck NSSG Dr Eleanor Aynsley Consultant Clinical Oncologist 3 HPV+ H&N A distinct disease entity Leemans et al., Nature Reviews, 2011 4 Good news Improved response to
De-Escalate Trial for the Head and neck NSSG Dr Eleanor Aynsley Consultant Clinical Oncologist 3 HPV+ H&N A distinct disease entity Leemans et al., Nature Reviews, 2011 4 Good news Improved response to
Rob Glynne-Jones Mount Vernon Cancer Centre
 ESMO Preceptorship Programme Colorectal Cancer Barcelona October 2017 Interventional radiology and stereotactic radiotherapy Rob Glynne-Jones Mount Vernon Cancer Centre My Disclosures: last 5 years Speaker:
ESMO Preceptorship Programme Colorectal Cancer Barcelona October 2017 Interventional radiology and stereotactic radiotherapy Rob Glynne-Jones Mount Vernon Cancer Centre My Disclosures: last 5 years Speaker:
Combined Modality Treatment of Anal Carcinoma
 Combined Modality Treatment of Anal Carcinoma F. ROELOFSEN, a H. BARTELINK b a Bethesda Krankenhaus, Essen, Germany; b The Netherlands Cancer Institute/Antoni van Leeuwenhoek Ziekenhuis, Amsterdam, The
Combined Modality Treatment of Anal Carcinoma F. ROELOFSEN, a H. BARTELINK b a Bethesda Krankenhaus, Essen, Germany; b The Netherlands Cancer Institute/Antoni van Leeuwenhoek Ziekenhuis, Amsterdam, The
Tratamiento Multidisciplinar de Estadios Localmente Avanzados en Cáncer de Pulmón
 Tratamiento Multidisciplinar de Estadios Localmente Avanzados en Cáncer de Pulmón Santiago Ponce Aix Servicio Oncología Médica Hospital Universitario 12 de Octubre Madrid Stage III: heterogenous disease
Tratamiento Multidisciplinar de Estadios Localmente Avanzados en Cáncer de Pulmón Santiago Ponce Aix Servicio Oncología Médica Hospital Universitario 12 de Octubre Madrid Stage III: heterogenous disease
Chemoradiation (CRT) Safety Analysis of ACOSOG Z6041: A Phase II Trial of Neoadjuvant CRT followed by Local Excision in ut2 Rectal Cancer
 Safety Analysis of ACOSOG Z6041: A Phase II Trial of Neoadjuvant CRT followed by Local Excision in ut2 Rectal Cancer") Chemoradiation (CRT) Safety Analysis of ACOSOG Z6041: A Phase II Trial of Neoadjuvant CRT followed by Local Excision in ut2 Rectal Cancer Emily Chan, Qian Shi, Julio Garcia-Aguilar, Peter Cataldo, Jorge
Chemoradiation (CRT) Safety Analysis of ACOSOG Z6041: A Phase II Trial of Neoadjuvant CRT followed by Local Excision in ut2 Rectal Cancer Emily Chan, Qian Shi, Julio Garcia-Aguilar, Peter Cataldo, Jorge
Oral Cavity Cancer Combined modality therapy
 Oral Cavity Cancer Combined modality therapy Dr. Christos CHRISTOPOULOS Radiation Oncologist Head and Neck Cancers Centre Hospitalier Universitaire (C.H.U.) de Limoges, France Disclosure slide I have no
Oral Cavity Cancer Combined modality therapy Dr. Christos CHRISTOPOULOS Radiation Oncologist Head and Neck Cancers Centre Hospitalier Universitaire (C.H.U.) de Limoges, France Disclosure slide I have no
Management of Squamous Cell Cancer of the Esophagus: Surgery Should Follow Chemo + RT
 Management of Squamous Cell Cancer of the Esophagus: Surgery Should Follow Chemo + RT David H. Ilson, MD, PhD Gastrointestinal Oncology Service Memorial Sloan Kettering Cancer Center Disclosure Consulting
Management of Squamous Cell Cancer of the Esophagus: Surgery Should Follow Chemo + RT David H. Ilson, MD, PhD Gastrointestinal Oncology Service Memorial Sloan Kettering Cancer Center Disclosure Consulting
ANAL CANCER Updated May 2016 by Dr. Daniel Yokom (PGY-5 Medical Oncology Resident, University of Toronto)
") ANAL CANCER Updated May 2016 by Dr. Daniel Yokom (PGY-5 Medical Oncology Resident, University of Toronto) Reviewed by Dr. Lee-Ying (Staff Medical Oncologist, University of Calgary), Dr. Kzyzanowska (Staff
ANAL CANCER Updated May 2016 by Dr. Daniel Yokom (PGY-5 Medical Oncology Resident, University of Toronto) Reviewed by Dr. Lee-Ying (Staff Medical Oncologist, University of Calgary), Dr. Kzyzanowska (Staff
Update on Neoadjuvant Chemotherapy (NACT) in Cervical Cancer
 in Cervical Cancer") Update on Neoadjuvant Chemotherapy (NACT) in Cervical Cancer Nicoletta Colombo, MD University of Milan-Bicocca European Institute of Oncology Milan, Italy NACT in Cervical Cancer NACT Stage -IB2 -IIA>4cm
Update on Neoadjuvant Chemotherapy (NACT) in Cervical Cancer Nicoletta Colombo, MD University of Milan-Bicocca European Institute of Oncology Milan, Italy NACT in Cervical Cancer NACT Stage -IB2 -IIA>4cm
Locally advanced head and neck cancer
 Locally advanced head and neck cancer Radiation Oncology Perspective Petek Erpolat, MD Gazi University, Turkey Definition and Management of LAHNC Stage III or IV cancers generally include larger primary
Locally advanced head and neck cancer Radiation Oncology Perspective Petek Erpolat, MD Gazi University, Turkey Definition and Management of LAHNC Stage III or IV cancers generally include larger primary
Mini J.Elnaggar M.D. Radiation Oncology Ochsner Medical Center 9/23/2016. Background
 Mini J.Elnaggar M.D. Radiation Oncology Ochsner Medical Center 9/23/2016 Background Mostly adenocarcinoma (scc possible, but treated like anal cancer) 39, 220 cases annually Primary treatment: surgery
Mini J.Elnaggar M.D. Radiation Oncology Ochsner Medical Center 9/23/2016 Background Mostly adenocarcinoma (scc possible, but treated like anal cancer) 39, 220 cases annually Primary treatment: surgery
Laryngeal Preservation Using Radiation Therapy. Chemotherapy and Organ Preservation
 1 Laryngeal Preservation Using Radiation Therapy 1903: Schepegrell was the first to perform radiation therapy for the treatment of laryngeal cancer Conventional external beam radiation produced disappointing
1 Laryngeal Preservation Using Radiation Therapy 1903: Schepegrell was the first to perform radiation therapy for the treatment of laryngeal cancer Conventional external beam radiation produced disappointing
Gastroesophag Gastroesopha eal Junction Adenocarcinoma: What is the best adjuvant regimen? Michael G. G. H addock Haddock M.D.
 Gastroesophageal Junction Adenocarcinoma: What is the best adjuvant regimen? Michael G. Haddock M.D. Mayo Clinic Rochester, MN Locally Advanced GE Junction ACA CT S CT or CT S CT/RT Proposition Chemoradiation
Gastroesophageal Junction Adenocarcinoma: What is the best adjuvant regimen? Michael G. Haddock M.D. Mayo Clinic Rochester, MN Locally Advanced GE Junction ACA CT S CT or CT S CT/RT Proposition Chemoradiation
CURRENT STANDARD OF CARE IN NASOPHARYNGEAL CANCER
 CURRENT STANDARD OF CARE IN NASOPHARYNGEAL CANCER Jean-Pascal Machiels Department of medical oncology Institut I Roi Albert II Cliniques universitaires Saint-Luc Université catholique de Louvain, Brussels,
CURRENT STANDARD OF CARE IN NASOPHARYNGEAL CANCER Jean-Pascal Machiels Department of medical oncology Institut I Roi Albert II Cliniques universitaires Saint-Luc Université catholique de Louvain, Brussels,
THE ROLE OF RADIATION THERAPY IN MANAGEMENT OF PANCREATIC ADENOCARCINOMA. TIMUR MITIN, MD, PhD
 THE ROLE OF RADIATION THERAPY IN MANAGEMENT OF PANCREATIC ADENOCARCINOMA TIMUR MITIN, MD, PhD RESECTABLE DISEASE MANAGEMENT: RESECTABLE DISEASE Resection offers the only possibility of long term survival
THE ROLE OF RADIATION THERAPY IN MANAGEMENT OF PANCREATIC ADENOCARCINOMA TIMUR MITIN, MD, PhD RESECTABLE DISEASE MANAGEMENT: RESECTABLE DISEASE Resection offers the only possibility of long term survival
New Paradigms for Treatment of. Erminia Massarelli, MD, PHD, MS Clinical Associate Professor
 New Paradigms for Treatment of Head and Neck cancers Erminia Massarelli, MD, PHD, MS Clinical Associate Professor City of Hope Disclosure Statement Grant/Research Support frommerck Bristol Grant/Research
New Paradigms for Treatment of Head and Neck cancers Erminia Massarelli, MD, PHD, MS Clinical Associate Professor City of Hope Disclosure Statement Grant/Research Support frommerck Bristol Grant/Research
Can we omit prophylactic inguinal nodal irradiation in anal cancer patients?
 Original Article Radiat Oncol J 215;33(2):83-88 http://dx.doi.org/1.3857/roj.215.33.2.83 pissn 2234-19 eissn 2234-3156 Can we omit prophylactic inguinal nodal irradiation in anal cancer patients? Hakyoung
Original Article Radiat Oncol J 215;33(2):83-88 http://dx.doi.org/1.3857/roj.215.33.2.83 pissn 2234-19 eissn 2234-3156 Can we omit prophylactic inguinal nodal irradiation in anal cancer patients? Hakyoung
HPV INDUCED OROPHARYNGEAL CARCINOMA radiation-oncologist point of view. Prof. dr. Sandra Nuyts Dep. Radiation-Oncology UH Leuven Belgium
 HPV INDUCED OROPHARYNGEAL CARCINOMA radiation-oncologist point of view Prof. dr. Sandra Nuyts Dep. Radiation-Oncology UH Leuven Belgium DISCLOSURE OF INTEREST Nothing to declare HEAD AND NECK CANCER -HPV
HPV INDUCED OROPHARYNGEAL CARCINOMA radiation-oncologist point of view Prof. dr. Sandra Nuyts Dep. Radiation-Oncology UH Leuven Belgium DISCLOSURE OF INTEREST Nothing to declare HEAD AND NECK CANCER -HPV
Combined modality treatment for N2 disease
 Combined modality treatment for N2 disease Dr Clara Chan Consultant in Clinical Oncology 3 rd March 2017 Overview Background The evidence base Systemic treatment Radiotherapy Future directions/clinical
Combined modality treatment for N2 disease Dr Clara Chan Consultant in Clinical Oncology 3 rd March 2017 Overview Background The evidence base Systemic treatment Radiotherapy Future directions/clinical
Immunotherapy in head and neck cancer and MSI in solid tumors
 Immunotherapy in head and neck cancer and MSI in solid tumors Brian Hunis, MD, MBA Associate Medical Director, Memorial Cancer Institute. Hollywood, FL »No disclosures Objectives»Discuss the role of immunology
Immunotherapy in head and neck cancer and MSI in solid tumors Brian Hunis, MD, MBA Associate Medical Director, Memorial Cancer Institute. Hollywood, FL »No disclosures Objectives»Discuss the role of immunology
Update on Limited Small Cell Lung Cancer. Laurie E Gaspar MD, MBA Prof/Chair Radiation Oncology University of Colorado Denver
 Update on Limited Small Cell Lung Cancer Laurie E Gaspar MD, MBA Prof/Chair Radiation Oncology University of Colorado Denver Objectives - Limited Radiation Dose Radiation Timing Radiation Volume PCI Neurotoxicity
Update on Limited Small Cell Lung Cancer Laurie E Gaspar MD, MBA Prof/Chair Radiation Oncology University of Colorado Denver Objectives - Limited Radiation Dose Radiation Timing Radiation Volume PCI Neurotoxicity
Prognostic factors in squamous cell anal cancers
 Prognostic factors in squamous cell anal cancers Zainul Abedin Kapacee Year 4-5 Intercalating Medical Student, University of Manchester Dr. Shabbir Susnerwala, Mr. Nigel Scott Dr. Falalu Danwata, Dr. Marcus
Prognostic factors in squamous cell anal cancers Zainul Abedin Kapacee Year 4-5 Intercalating Medical Student, University of Manchester Dr. Shabbir Susnerwala, Mr. Nigel Scott Dr. Falalu Danwata, Dr. Marcus
Radiotherapy & Cervical Cancer Dr Mary McCormack Consultant Clinical Oncologist University College Hospital, London,UK
 Lead Group Log Radiotherapy & Cervical Cancer Dr Mary McCormack Consultant Clinical Oncologist University College Hospital, London,UK Cervical Cancer treatment Treatment planning should be made on a multidisciplinary
Lead Group Log Radiotherapy & Cervical Cancer Dr Mary McCormack Consultant Clinical Oncologist University College Hospital, London,UK Cervical Cancer treatment Treatment planning should be made on a multidisciplinary
Pre- Versus Post-operative Radiotherapy
 Postoperative Radiation and Chemoradiation: Indications and Optimization of Practice Dislosures Clinical trial support from Genentech Inc. Sue S. Yom, MD, PhD Associate Professor UCSF Radiation Oncology
Postoperative Radiation and Chemoradiation: Indications and Optimization of Practice Dislosures Clinical trial support from Genentech Inc. Sue S. Yom, MD, PhD Associate Professor UCSF Radiation Oncology
The following slides are provided as presented by the author during the live educa7onal ac7vity and are intended for reference purposes only.
 The following slides are provided as presented by the author during the live educa7onal ac7vity and are intended for reference purposes only. If you have any ques7ons, please contact Imedex via email at:
The following slides are provided as presented by the author during the live educa7onal ac7vity and are intended for reference purposes only. If you have any ques7ons, please contact Imedex via email at:
ADJUVANT CHEMOTHERAPY...
 Colorectal Pathway Board: Non-Surgical Oncology Guidelines October 2015 Organization» Table of Contents ADJUVANT CHEMOTHERAPY... 2 DUKES C/ TNM STAGE 3... 2 DUKES B/ TNM STAGE 2... 3 LOCALLY ADVANCED
Colorectal Pathway Board: Non-Surgical Oncology Guidelines October 2015 Organization» Table of Contents ADJUVANT CHEMOTHERAPY... 2 DUKES C/ TNM STAGE 3... 2 DUKES B/ TNM STAGE 2... 3 LOCALLY ADVANCED
RTOG Lung Cancer Committee 2012 Clinical Trial Update. Wally Curran RTOG Group Chairman
 RTOG Lung Cancer Committee 2012 Clinical Trial Update Wally Curran RTOG Group Chairman 1 RTOG Lung Committee: Active Trials Small Cell Lung Cancer Limited Stage (Intergroup Trial) Extensive Stage (RTOG
RTOG Lung Cancer Committee 2012 Clinical Trial Update Wally Curran RTOG Group Chairman 1 RTOG Lung Committee: Active Trials Small Cell Lung Cancer Limited Stage (Intergroup Trial) Extensive Stage (RTOG
Upper Gastrointestinal. Friday, March 2, :00 p.m. 2:45 p.m.
 Upper Gastrointestinal Friday, March 2, 2018 2:00 p.m. 2:45 p.m. Social Q&A Use your phone, tablet, or laptop to Submit questions to speakers and moderators Answer interactive questions / audience response
Upper Gastrointestinal Friday, March 2, 2018 2:00 p.m. 2:45 p.m. Social Q&A Use your phone, tablet, or laptop to Submit questions to speakers and moderators Answer interactive questions / audience response
Opportunity for palliative care Research
 Opportunity for palliative care Research Role of Radiotherapy in Multidisciplinary Management of Rectal Cancers Dr Sushmita Pathy Associate Professor Department of Radiation Oncology Dr BRA Institute Rotary
Opportunity for palliative care Research Role of Radiotherapy in Multidisciplinary Management of Rectal Cancers Dr Sushmita Pathy Associate Professor Department of Radiation Oncology Dr BRA Institute Rotary
Adjuvant Therapy in Locally Advanced Head and Neck Cancer. Ezra EW Cohen University of Chicago. Financial Support
 Adjuvant Therapy in Locally Advanced Head and Neck Cancer Ezra EW Cohen University of Chicago Financial Support This program is made possible by an educational grant from Eli Lilly Oncology, who had no
Adjuvant Therapy in Locally Advanced Head and Neck Cancer Ezra EW Cohen University of Chicago Financial Support This program is made possible by an educational grant from Eli Lilly Oncology, who had no
Practice changing studies in lung cancer 2017
 1 Practice changing studies in lung cancer 2017 Rolf Stahel University Hospital of Zürich Cape Town, February 16, 2018 DISCLOSURE OF INTEREST Consultant or Advisory Role in the last two years I have received
1 Practice changing studies in lung cancer 2017 Rolf Stahel University Hospital of Zürich Cape Town, February 16, 2018 DISCLOSURE OF INTEREST Consultant or Advisory Role in the last two years I have received
Clinical Management Guideline for Small Cell Lung Cancer
 Diagnosis and Staging: Key Points 1. Ensure a CT scan that is
Diagnosis and Staging: Key Points 1. Ensure a CT scan that is
Some Seminal Studies. Chemotherapy Alone is Inadequate. Bladder Cancer Role of Radiation in Bladder Sparing. Primary Radiation for Bladder Cancer
 Bladder Cancer Role of Radiation in Bladder Sparing David C. Beyer M.D., FACR, FACRO, FASTRO Arizona Oncology Services Phoenix, Arizona Primary Radiation for Bladder Cancer No modern surgery / XRT randomized
Bladder Cancer Role of Radiation in Bladder Sparing David C. Beyer M.D., FACR, FACRO, FASTRO Arizona Oncology Services Phoenix, Arizona Primary Radiation for Bladder Cancer No modern surgery / XRT randomized
Chemotherapy Treatment Algorithms for Urology Cancer
 Chemotherapy Treatment Algorithms for Urology Cancer Chemoradiation for bladder cancer; Chemotherapy algorithm for non TCC bladder cancer Squamous cell carcinoma; Chemotherapy Algorithm for Non Transitional
Chemotherapy Treatment Algorithms for Urology Cancer Chemoradiation for bladder cancer; Chemotherapy algorithm for non TCC bladder cancer Squamous cell carcinoma; Chemotherapy Algorithm for Non Transitional
Emerging Role of Immunotherapy in Head and Neck Cancer
 Emerging Role of Immunotherapy in Head and Neck Cancer Jared Weiss, MD Associate Professor of Medicine and Section Chief of Thoracic and Head/Neck Oncology UNC Lineberger Comprehensive Cancer Center Copyright
Emerging Role of Immunotherapy in Head and Neck Cancer Jared Weiss, MD Associate Professor of Medicine and Section Chief of Thoracic and Head/Neck Oncology UNC Lineberger Comprehensive Cancer Center Copyright
RECTAL CANCER CLINICAL CASE PRESENTATION
 RECTAL CANCER CLINICAL CASE PRESENTATION Francesco Sclafani Medical Oncologist, Clinical Research Fellow The Royal Marsden NHS Foundation Trust, London, UK esmo.org Disclosure I have nothing to declare
RECTAL CANCER CLINICAL CASE PRESENTATION Francesco Sclafani Medical Oncologist, Clinical Research Fellow The Royal Marsden NHS Foundation Trust, London, UK esmo.org Disclosure I have nothing to declare
Bladder Preservation Strategies for Muscle Invasive Bladder Cancer
 Bladder Preservation Strategies for Muscle Invasive Bladder Cancer Jeff M. Michalski, MD, MBA, FACR, FASTRO The Carlos A. Perez Distinguished Professor of Radiation Oncology Department of Radiation Oncology
Bladder Preservation Strategies for Muscle Invasive Bladder Cancer Jeff M. Michalski, MD, MBA, FACR, FASTRO The Carlos A. Perez Distinguished Professor of Radiation Oncology Department of Radiation Oncology
The following slides are provided as presented by the author during the live educa7onal ac7vity and are intended for reference purposes only.
 The following slides are provided as presented by the author during the live educa7onal ac7vity and are intended for reference purposes only. If you have any ques7ons, please contact Imedex via email at:
The following slides are provided as presented by the author during the live educa7onal ac7vity and are intended for reference purposes only. If you have any ques7ons, please contact Imedex via email at:
17 th ESO-ESMO Masterclass in clinical Oncology
 17 th ESO-ESMO Masterclass in clinical Oncology Cervical and endometrial Cancer Cristiana Sessa IOSI Bellinzona, Switzerland Berlin, March 28 th, 2018 Presenter Disclosures None Cervical Cancer Estimated
17 th ESO-ESMO Masterclass in clinical Oncology Cervical and endometrial Cancer Cristiana Sessa IOSI Bellinzona, Switzerland Berlin, March 28 th, 2018 Presenter Disclosures None Cervical Cancer Estimated
Simultaneous Integrated Boost or Sequential Boost in the Setting of Standard Dose or Dose De-escalation for HPV- Associated Oropharyngeal Cancer
 Simultaneous Integrated Boost or Sequential Boost in the Setting of Standard Dose or Dose De-escalation for HPV- Associated Oropharyngeal Cancer Dawn Gintz, CMD, RTT Dosimetry Coordinator of Research and
Simultaneous Integrated Boost or Sequential Boost in the Setting of Standard Dose or Dose De-escalation for HPV- Associated Oropharyngeal Cancer Dawn Gintz, CMD, RTT Dosimetry Coordinator of Research and
Chemo-radiotherapy in muscle invasive bladder cancer. Dr Paula Wells St Bartholomew s Hospital London
 Chemo-radiotherapy in muscle invasive bladder cancer Dr Paula Wells St Bartholomew s Hospital London Overview Evidence base for cystectomy vs bladder preservation Chemo-radiotherapy vs radiotherapy alone
Chemo-radiotherapy in muscle invasive bladder cancer Dr Paula Wells St Bartholomew s Hospital London Overview Evidence base for cystectomy vs bladder preservation Chemo-radiotherapy vs radiotherapy alone
HPV VACCINE AND AIN Palefsky NEJM 2011 n=602 MSM 16-26y qhpv = vaccine against HPV 6, 11, 16 and 18 vs placebo They analyzed ITT and per protocol.
 ANAL CANCER Updated Mar 2017 by Doreen Ezeife, PGY-5 resident University of Calgary Reviewed by Dr. Lee-Ying (Staff Medical Oncologist, University of Calgary), Dr. Kzyzanowska (Staff Medical Oncologist,
ANAL CANCER Updated Mar 2017 by Doreen Ezeife, PGY-5 resident University of Calgary Reviewed by Dr. Lee-Ying (Staff Medical Oncologist, University of Calgary), Dr. Kzyzanowska (Staff Medical Oncologist,
Are we making progress? Marked reduction in operative morbidity and mortality
 Are we making progress? Surgical Progress Marked reduction in operative morbidity and mortality Introduction of Minimal-Access approaches for complex esophageal cancer resections Significantly better functional
Are we making progress? Surgical Progress Marked reduction in operative morbidity and mortality Introduction of Minimal-Access approaches for complex esophageal cancer resections Significantly better functional
Non-small Cell Lung Cancer: Multidisciplinary Role: Role of Medical Oncologist
 Non-small Cell Lung Cancer: Multidisciplinary Role: Role of Medical Oncologist Vichien Srimuninnimit, MD. Medical Oncology Division Faculty of Medicine, Siriraj Hospital Outline Resectable NSCLC stage
Non-small Cell Lung Cancer: Multidisciplinary Role: Role of Medical Oncologist Vichien Srimuninnimit, MD. Medical Oncology Division Faculty of Medicine, Siriraj Hospital Outline Resectable NSCLC stage
Rob Glynne-Jones Mount Vernon Cancer Centre
 ESMO Preceptorship Programme Colorectal Cancer Barcelona October 2017 State of the art: Radio- /chemotherapy for rectal cancer Rob Glynne-Jones Mount Vernon Cancer Centre My Disclosures: last 5 years Speaker:
ESMO Preceptorship Programme Colorectal Cancer Barcelona October 2017 State of the art: Radio- /chemotherapy for rectal cancer Rob Glynne-Jones Mount Vernon Cancer Centre My Disclosures: last 5 years Speaker:
Concurrent chemoradiation with volumetric modulated Arc therapy of patients treated for anal cancer acute toxicity and treatment outcome
 Original Article Concurrent chemoradiation with volumetric modulated Arc therapy of patients treated for anal cancer acute toxicity and treatment outcome Kaloyan Yordanov, Simona Cima, Antonella Richetti,
Original Article Concurrent chemoradiation with volumetric modulated Arc therapy of patients treated for anal cancer acute toxicity and treatment outcome Kaloyan Yordanov, Simona Cima, Antonella Richetti,
Where are we with radiotherapy for biliary tract cancers?
 Where are we with radiotherapy for biliary tract cancers? Professor Maria A. Hawkins Associate Professor in Clinical Oncology MRC Group Leader/Honorary Consultant Clinical Oncologist CRUK MRC Oxford Institute
Where are we with radiotherapy for biliary tract cancers? Professor Maria A. Hawkins Associate Professor in Clinical Oncology MRC Group Leader/Honorary Consultant Clinical Oncologist CRUK MRC Oxford Institute
ADJUVANT CHEMOTHERAPY FOR RECTAL CANCER
 ESMO Preceptorship Programme Colorectal Cancer Barcelona November, 25-26, 2016 ADJUVANT CHEMOTHERAPY FOR RECTAL CANCER Andrés Cervantes Professor of Medicine OLD APPROACH TO RECTAL CANCER Surgical resection
ESMO Preceptorship Programme Colorectal Cancer Barcelona November, 25-26, 2016 ADJUVANT CHEMOTHERAPY FOR RECTAL CANCER Andrés Cervantes Professor of Medicine OLD APPROACH TO RECTAL CANCER Surgical resection
Head and Neck Cancer Update Sandro V Porceddu
 Head and Neck Cancer Update Sandro V Porceddu Director, Radiation Oncology Research Princess Alexandra Hospital, Brisbane Associate Professor, University of Queensland President, Trans Tasman Radiation
Head and Neck Cancer Update Sandro V Porceddu Director, Radiation Oncology Research Princess Alexandra Hospital, Brisbane Associate Professor, University of Queensland President, Trans Tasman Radiation
ES-SCLC Joint Case Conference. Anthony Paravati Adam Yock
 ES-SCLC Joint Case Conference Anthony Paravati Adam Yock Case 57 yo woman with 35 pack year smoking history presented with persistent cough and rash Chest x-ray showed a large left upper lobe/left hilar
ES-SCLC Joint Case Conference Anthony Paravati Adam Yock Case 57 yo woman with 35 pack year smoking history presented with persistent cough and rash Chest x-ray showed a large left upper lobe/left hilar
Radiotherapy for Rectal Cancer. Kevin Palumbo Adelaide Radiotherapy Centre
 Radiotherapy for Rectal Cancer Kevin Palumbo Adelaide Radiotherapy Centre Overview CRC are common (3 rd commonest cancer) rectal Ca approx 25-30% of all CRC. Presentation PR bleeding: beware attributing
Radiotherapy for Rectal Cancer Kevin Palumbo Adelaide Radiotherapy Centre Overview CRC are common (3 rd commonest cancer) rectal Ca approx 25-30% of all CRC. Presentation PR bleeding: beware attributing
Rectal Cancer: Classic Hits
 Rectal Cancer: Classic Hits Charles M. Friel, MD Associate Professor of Surgery Section of Colon and Rectal Surgery University of Virginia September 28, 2016 None Disclosures 1 Objectives Review the Classic
Rectal Cancer: Classic Hits Charles M. Friel, MD Associate Professor of Surgery Section of Colon and Rectal Surgery University of Virginia September 28, 2016 None Disclosures 1 Objectives Review the Classic
Head & Neck Cancer: When to Irradiate
 Head & Neck Cancer: When to Irradiate ESO-ESMO Latin-America 2018 Talented students colleagues 1 > 15 different diseases for RT strategies NC NP OC OP H L 2 HPV Prognostic Marker >2010 Trial Cases Marker
Head & Neck Cancer: When to Irradiate ESO-ESMO Latin-America 2018 Talented students colleagues 1 > 15 different diseases for RT strategies NC NP OC OP H L 2 HPV Prognostic Marker >2010 Trial Cases Marker
Combined Modality Therapy State of the Art. Everett E. Vokes The University of Chicago
 Combined Modality Therapy State of the Art Everett E. Vokes The University of Chicago What we Know Some patients are cured (20%) Induction and concurrent chemoradiotherapy are each superior to radiotherapy
Combined Modality Therapy State of the Art Everett E. Vokes The University of Chicago What we Know Some patients are cured (20%) Induction and concurrent chemoradiotherapy are each superior to radiotherapy
Case Conference. Craig Morgenthal Department of Surgery Long Island College Hospital
 Case Conference Craig Morgenthal Department of Surgery Long Island College Hospital Neoadjuvant versus Adjuvant Radiation Therapy in Rectal Carcinoma Epidemiology American Cancer Society statistics for
Case Conference Craig Morgenthal Department of Surgery Long Island College Hospital Neoadjuvant versus Adjuvant Radiation Therapy in Rectal Carcinoma Epidemiology American Cancer Society statistics for
NCCN Guidelines for Hepatobiliary Cancers V Web teleconference on 10/24/17
 Guideline Page and Request HCC-4 the American Society of Radiation Oncology (ASTRO): We recommend further clarification of the eligibility criteria for surgical resection and liver transplantation, respectively.
Guideline Page and Request HCC-4 the American Society of Radiation Oncology (ASTRO): We recommend further clarification of the eligibility criteria for surgical resection and liver transplantation, respectively.
RECTAL CANCER APPARENT COMPLETE RESPONSE (acr) AFTER LONG COURSE CHEMORADIOTHERAPY
 AFTER LONG COURSE CHEMORADIOTHERAPY") COLORECTAL CLINICAL SUBGROUP RECTAL CANCER APPARENT COMPLETE RESPONSE (acr) AFTER LONG COURSE CHEMORADIOTHERAPY Finalised by: Dr Simon Gollins Mr Andrew Renehan Dr Mark Saunders Mr Nigel Scott Dr Shabbir
COLORECTAL CLINICAL SUBGROUP RECTAL CANCER APPARENT COMPLETE RESPONSE (acr) AFTER LONG COURSE CHEMORADIOTHERAPY Finalised by: Dr Simon Gollins Mr Andrew Renehan Dr Mark Saunders Mr Nigel Scott Dr Shabbir
Effective treatment of anal cancer in the elderly with low-dose chemoradiotherapy
 British Journal of Cancer (2005) 92, 1221 1225 All rights reserved 0007 0920/05 $30.00 www.bjcancer.com Effective treatment of anal cancer in the elderly with low-dose chemoradiotherapy N Charnley 1, A
British Journal of Cancer (2005) 92, 1221 1225 All rights reserved 0007 0920/05 $30.00 www.bjcancer.com Effective treatment of anal cancer in the elderly with low-dose chemoradiotherapy N Charnley 1, A
Preoperative adjuvant radiotherapy
 Preoperative adjuvant radiotherapy Dr John Hay Radiation Oncology Program BC Cancer Agency Vancouver Cancer Centre The key question for the surgeon Do you think that this tumour can be resected with clear
Preoperative adjuvant radiotherapy Dr John Hay Radiation Oncology Program BC Cancer Agency Vancouver Cancer Centre The key question for the surgeon Do you think that this tumour can be resected with clear
Cochrane metaanalysis 5 year OS Intent to treat
 RADICAL CYSTECTOMY IS THE ONLY EFFECTIVE TREATMENT FOR PATIENTS WITH OPERABLE MUSCLE INVASIVE BLADDER CANCER The Con position Scott Tyldesley Radiation Oncology, Vancouver Centre, BC Cancer Agency Cochrane
RADICAL CYSTECTOMY IS THE ONLY EFFECTIVE TREATMENT FOR PATIENTS WITH OPERABLE MUSCLE INVASIVE BLADDER CANCER The Con position Scott Tyldesley Radiation Oncology, Vancouver Centre, BC Cancer Agency Cochrane
Oral cavity cancer Post-operative treatment
 Oral cavity cancer Post-operative treatment Dr. Christos CHRISTOPOULOS Radiation Oncologist Centre Hospitalier Universitaire (C.H.U.) de Limoges, France Important issues RT -techniques Patient selection
Oral cavity cancer Post-operative treatment Dr. Christos CHRISTOPOULOS Radiation Oncologist Centre Hospitalier Universitaire (C.H.U.) de Limoges, France Important issues RT -techniques Patient selection
Trimodality Therapy for Muscle Invasive Bladder Cancer
 Trimodality Therapy for Muscle Invasive Bladder Cancer Brita Danielson, MD, FRCPC Radiation Oncologist, Cross Cancer Institute Assistant Professor, Department of Oncology University of Alberta Edmonton,
Trimodality Therapy for Muscle Invasive Bladder Cancer Brita Danielson, MD, FRCPC Radiation Oncologist, Cross Cancer Institute Assistant Professor, Department of Oncology University of Alberta Edmonton,
NEOADJUVANT THERAPY IN CARCINOMA STOMACH. Dr Jyotirup Goswami Consultant Radiation Oncologist Narayana Superspeciality Hospital, Howrah
 NEOADJUVANT THERAPY IN CARCINOMA STOMACH Dr Jyotirup Goswami Consultant Radiation Oncologist Narayana Superspeciality Hospital, Howrah NEOADJUVANT THERAPY?! Few believers Limited evidence Many surgeons
NEOADJUVANT THERAPY IN CARCINOMA STOMACH Dr Jyotirup Goswami Consultant Radiation Oncologist Narayana Superspeciality Hospital, Howrah NEOADJUVANT THERAPY?! Few believers Limited evidence Many surgeons
Gynecologic Cancer InterGroup Cervix Cancer Research Network. Management of Cervical Cancer in Resource Limited Settings.
 Management of Cervical Cancer in Resource Limited Settings Linus Chuang MD Conflict of Interests None Cervical cancer is the fourth most common malignancy in women worldwide 530,000 new cases per year
Management of Cervical Cancer in Resource Limited Settings Linus Chuang MD Conflict of Interests None Cervical cancer is the fourth most common malignancy in women worldwide 530,000 new cases per year
Rectal cancer with synchroneous liver mets: A challenging clinical case
 ESMO Preceptorship Programme Rectal cancer Singapur November 2017 Rectal cancer with synchroneous liver mets: A challenging clinical case Andrés Cervantes Disclosures Consulting and advisory services,
ESMO Preceptorship Programme Rectal cancer Singapur November 2017 Rectal cancer with synchroneous liver mets: A challenging clinical case Andrés Cervantes Disclosures Consulting and advisory services,
Resectable locally advanced oesophagogastric cancer
 Resectable locally advanced oesophagogastric cancer Clinical Case Discussion Florian Lordick University Cancer Center Leipzig University Clinic Leipzig Leipzig, Germany esmo.org DISCLOSURES Honoraria for
Resectable locally advanced oesophagogastric cancer Clinical Case Discussion Florian Lordick University Cancer Center Leipzig University Clinic Leipzig Leipzig, Germany esmo.org DISCLOSURES Honoraria for
PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES
 PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES GASTROINTESTINAL RECTAL CANCER GI Site Group Rectal Cancer Authors: Dr. Jennifer Knox, Dr. Mairead McNamara 1. INTRODUCTION 3 2. SCREENING AND
PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES GASTROINTESTINAL RECTAL CANCER GI Site Group Rectal Cancer Authors: Dr. Jennifer Knox, Dr. Mairead McNamara 1. INTRODUCTION 3 2. SCREENING AND
Guideline for the Management of Vulval Cancer
 Version History Guideline for the Management of Vulval Cancer Version Date Brief Summary of Change Issued 2.0 20.02.08 Endorsed by the Governance Committee 2.1 19.11.10 Circulated at NSSG meeting 2.2 13.04.11
Version History Guideline for the Management of Vulval Cancer Version Date Brief Summary of Change Issued 2.0 20.02.08 Endorsed by the Governance Committee 2.1 19.11.10 Circulated at NSSG meeting 2.2 13.04.11
Comparing Alternative treatment Regimens for intermediate and high risk oropharyngeal cancer CompARE. Prof. Hisham Mehanna.
 Comparing Alternative treatment Regimens for intermediate and high risk oropharyngeal cancer CompARE Prof. Hisham Mehanna Chief investigator: Hisham Mehanna Arm 1: Mehmet Sen Arm2: John Chester/Martin
Comparing Alternative treatment Regimens for intermediate and high risk oropharyngeal cancer CompARE Prof. Hisham Mehanna Chief investigator: Hisham Mehanna Arm 1: Mehmet Sen Arm2: John Chester/Martin
Workshop LA RADIOTERAPIA DEI TUMORI RARI I TIMOMI : INDICAZIONI
 XXI CONGRESSO NAZIONALE AIRO Genova, 19-22 novembre 2011 Workshop LA RADIOTERAPIA DEI TUMORI RARI I TIMOMI : INDICAZIONI PIERA NAVARRIA Unità Operativa di Radioterapia e Radiochirurgia Humanitas Cancer
XXI CONGRESSO NAZIONALE AIRO Genova, 19-22 novembre 2011 Workshop LA RADIOTERAPIA DEI TUMORI RARI I TIMOMI : INDICAZIONI PIERA NAVARRIA Unità Operativa di Radioterapia e Radiochirurgia Humanitas Cancer
CALGB Thoracic Radiotherapy for Limited Stage Small Cell Lung Cancer
 CALGB 30610 Thoracic Radiotherapy for Limited Stage Small Cell Lung Cancer Jeffrey A. Bogart Department of Radiation Oncology Upstate Medical University Syracuse, NY Small Cell Lung Cancer Estimated 33,000
CALGB 30610 Thoracic Radiotherapy for Limited Stage Small Cell Lung Cancer Jeffrey A. Bogart Department of Radiation Oncology Upstate Medical University Syracuse, NY Small Cell Lung Cancer Estimated 33,000
Index. Note: Page numbers of article titles are in boldface type.
 Index Note: Page numbers of article titles are in boldface type. A Abdominal drainage, after hepatic resection, 159 160 Ablation, radiofrequency, for hepatocellular carcinoma, 160 161 Adenocarcinoma, pancreatic.
Index Note: Page numbers of article titles are in boldface type. A Abdominal drainage, after hepatic resection, 159 160 Ablation, radiofrequency, for hepatocellular carcinoma, 160 161 Adenocarcinoma, pancreatic.
Concurrent Chemo- and Radiotherapy for Ororpharynx Cancer
 Concurrent Chemo- and Radiotherapy for Ororpharynx Cancer Faye Johnson MD, PhD Associate Professor Thoracic/Head and Neck Medical Oncology August 2017 Objectives Review data that support concurrent chemo-
Concurrent Chemo- and Radiotherapy for Ororpharynx Cancer Faye Johnson MD, PhD Associate Professor Thoracic/Head and Neck Medical Oncology August 2017 Objectives Review data that support concurrent chemo-
PROCARE FINAL FEEDBACK
 1 PROCARE FINAL FEEDBACK General report 2006-2014 Version 2.1 08/12/2015 PROCARE indicators 2006-2014... 3 Demographic Data... 3 Diagnosis and staging... 4 Time to first treatment... 6 Neoadjuvant treatment...
1 PROCARE FINAL FEEDBACK General report 2006-2014 Version 2.1 08/12/2015 PROCARE indicators 2006-2014... 3 Demographic Data... 3 Diagnosis and staging... 4 Time to first treatment... 6 Neoadjuvant treatment...
Radiotherapy in DLCL is often worthwhile. Dr. Joachim Yahalom Memorial Sloan-Kettering, New York
 Radiotherapy in DLCL is often worthwhile Dr. Joachim Yahalom Memorial Sloan-Kettering, New York The case for radiotherapy Past: Pre-Rituximab randomized trials Present: R-CHOP as backbone, retrospective
Radiotherapy in DLCL is often worthwhile Dr. Joachim Yahalom Memorial Sloan-Kettering, New York The case for radiotherapy Past: Pre-Rituximab randomized trials Present: R-CHOP as backbone, retrospective
GCIG Rare Tumour Brainstorming Day
 GCIG Rare Tumour Brainstorming Day Relatively (Not So) Rare Tumours Adenocarcinoma of Cervix Keiichi Fujiwara, Ros Glasspool Benedicte Votan, Jim Paul Aim of the Day To develop at least one clinical trial
GCIG Rare Tumour Brainstorming Day Relatively (Not So) Rare Tumours Adenocarcinoma of Cervix Keiichi Fujiwara, Ros Glasspool Benedicte Votan, Jim Paul Aim of the Day To develop at least one clinical trial
Enterprise Interest None
 Enterprise Interest None Cervical Cancer -Management of late stages ESP meeting Bilbao Spain 2018 Dr Mary McCormack PhD FRCR Consultant Clinical Oncologist University College Hospital London On behalf
Enterprise Interest None Cervical Cancer -Management of late stages ESP meeting Bilbao Spain 2018 Dr Mary McCormack PhD FRCR Consultant Clinical Oncologist University College Hospital London On behalf
Heterogeneity of N2 disease
 Locally Advanced NSCLC Surgery? No. Ramaswamy Govindan M.D Co-Director, Section of Medical Oncology Alvin J Siteman Cancer Center at Washington University School of Medicine St. Louis, Missouri Heterogeneity
Locally Advanced NSCLC Surgery? No. Ramaswamy Govindan M.D Co-Director, Section of Medical Oncology Alvin J Siteman Cancer Center at Washington University School of Medicine St. Louis, Missouri Heterogeneity
Clinical Trials in Transoral Endoscopic Head &Neck Surgery ECOG3311 and RTOG1221. Chris Holsinger, MD, FACS Bob Ferris, MD, PhD, FACS
 Clinical Trials in Transoral Endoscopic Head &Neck Surgery ECOG3311 and RTOG1221 Chris Holsinger, MD, FACS Bob Ferris, MD, PhD, FACS 1 Disclosure I have no conflicts of interest to disclose 2 Robotic H&N
Clinical Trials in Transoral Endoscopic Head &Neck Surgery ECOG3311 and RTOG1221 Chris Holsinger, MD, FACS Bob Ferris, MD, PhD, FACS 1 Disclosure I have no conflicts of interest to disclose 2 Robotic H&N
Collection of Recorded Radiotherapy Seminars
 IAEA Human Health Campus Collection of Recorded Radiotherapy Seminars http://humanhealth.iaea.org Conservative Treatment of Invasive Bladder Cancer Luis Souhami, MD Professor Department of Radiation Oncology
IAEA Human Health Campus Collection of Recorded Radiotherapy Seminars http://humanhealth.iaea.org Conservative Treatment of Invasive Bladder Cancer Luis Souhami, MD Professor Department of Radiation Oncology
Role of Prophylactic Cranial Irradiation in Small Cell Lung Cancer
 Role of Prophylactic Cranial Irradiation in Small Cell Lung Cancer Kazi S. Manir MD,DNB,ECMO,PDCR Clinical Tutor Department of Radiotherapy R. G. Kar Medical College and Hospital, Kolkata SCLC 15% of lung
Role of Prophylactic Cranial Irradiation in Small Cell Lung Cancer Kazi S. Manir MD,DNB,ECMO,PDCR Clinical Tutor Department of Radiotherapy R. G. Kar Medical College and Hospital, Kolkata SCLC 15% of lung
Chemotherapy of colon cancers
 Chemotherapy of colon cancers Stage distribution Stage I : 15% T 1,2 NO Stage IV: 20 25% M+ Stage II : 20 30% T3,4 NO Stage III N+: 30 40% clinical stages I, II, or III colon cancer are at risk for having
Chemotherapy of colon cancers Stage distribution Stage I : 15% T 1,2 NO Stage IV: 20 25% M+ Stage II : 20 30% T3,4 NO Stage III N+: 30 40% clinical stages I, II, or III colon cancer are at risk for having
3/12/2018. Head & Neck Cancer Review INTRODUCTION
 Head & Neck Cancer Review Joseph Rosales, MD March 12, 2018 INTRODUCTION Epidemiology/Risk Factors Anatomy Presentation/Workup Treatment Surgery vs Radiation Chemotherapy Side effects Special circumstances
Head & Neck Cancer Review Joseph Rosales, MD March 12, 2018 INTRODUCTION Epidemiology/Risk Factors Anatomy Presentation/Workup Treatment Surgery vs Radiation Chemotherapy Side effects Special circumstances
Therapy of Locally Advanced Head and Neck Cancer: State of the Art
 Therapy of Locally Advanced Head and Neck Cancer: State of the Art Barbara Burtness, MD Chief, Head and Neck ncology Medical ncology Co-Leader Senior Member Fox Chase Cancer Center Philadelphia, PA Therapy
Therapy of Locally Advanced Head and Neck Cancer: State of the Art Barbara Burtness, MD Chief, Head and Neck ncology Medical ncology Co-Leader Senior Member Fox Chase Cancer Center Philadelphia, PA Therapy
State of the art: Standard(s) of radio/chemotherapy for rectal cancer
 of radio/chemotherapy for rectal cancer") State of the art: Standard(s) of radio/chemotherapy for rectal cancer Dr Ian Chau Consultant Medical Oncologist The Royal Marsden Hospital London & Surrey Disclosure Advisory Board: Sanofi Oncology, Eli-
State of the art: Standard(s) of radio/chemotherapy for rectal cancer Dr Ian Chau Consultant Medical Oncologist The Royal Marsden Hospital London & Surrey Disclosure Advisory Board: Sanofi Oncology, Eli-
Nasopharynx Cancer. 1 Feb Presenters: Dr Raghav Murali-Ganesh (Radiation Oncology Registrar) Dr Peter Luk (Pathology Registrar)
 Dr Peter Luk (Pathology Registrar)") Nasopharynx Cancer 1 Feb 2016 Presenters: Dr Raghav Murali-Ganesh (Radiation Oncology Registrar) Dr Peter Luk (Pathology Registrar) Expert Panels Prof Mo Mo Tin Prof Michael Boyer Dr Raewyn Campbell Prof
Nasopharynx Cancer 1 Feb 2016 Presenters: Dr Raghav Murali-Ganesh (Radiation Oncology Registrar) Dr Peter Luk (Pathology Registrar) Expert Panels Prof Mo Mo Tin Prof Michael Boyer Dr Raewyn Campbell Prof
Gastric and Colon Cancer. Dr. Andres Wiernik 2017
 Gastric and Colon Cancer Dr. Andres Wiernik 2017 GASTRIC CANCER Gastric Cancer Classification Epidemiology General principles of Management 25% GE Junction Gastric Cancer 75% Gastric Cancer Epidemiology
Gastric and Colon Cancer Dr. Andres Wiernik 2017 GASTRIC CANCER Gastric Cancer Classification Epidemiology General principles of Management 25% GE Junction Gastric Cancer 75% Gastric Cancer Epidemiology