Head & Neck Cancer: When to Irradiate
|
|
|
- Beatrice Burke
- 5 years ago
- Views:
Transcription

1


2 Head & Neck Cancer: When to Irradiate ESO-ESMO Latin-America 2018 Talented students colleagues 1




3 > 15 different diseases for RT strategies NC NP OC OP H L 2
4 HPV Prognostic Marker >2010 Trial Cases Marker Survival First author RTOG 323 HPV 82% vs. 57% (3-year) TROG 185 p16 INK4A 91% vs. 74% (2-year) DAHANCA 794 p16 INK4A 66% vs. 28% (5-year) TAX HPV 82% vs. 35% (5-year) Ang, 2010 Rischin, 2010 Lassen, 2011 Posner, 2011
5 No data yet

6 T AFRT vs CFRT no diferences in outcome


7 HPV p16 + vs - Never smokers
8 Selected topics for talented When RT? Locally advanced stages Nasopharynx Postoperative RT Laryngeal preservation Oligo-recurrence New concepts, new trials How? and what? (to expect) 7


9 Highest level of clinical evidence Australian National Health and Medical Research Council 48% all cancer pts indication of RT 73% chemoradiation level I-II 34% curative 14% palliative Radiation type LC 5y OS 5y RT 10 % all pts 2,4% all pts CRT 0,6% all pts 0,3% all pts Head & Neck CRT 32% 16% Cervix CRT 33% 18%
 Technique: IMRT (except for early stage glottic")
10 Principles of RT technique/target delineation Simulation Head extended Supine Arms down IV contrast 5-pt mask Thin cut (2-3 mm) Technique: IMRT (except for early stage glottic cancer)
 Secondary echelon At risk if primary echelon contains bulky or high-volume disease Dose-Volume")
11 Target delineation (elective nodes) Primary echelon Location/drainage of primary Lateralized (ipsilateral) vs. midline» (bilateral) Secondary echelon At risk if primary echelon contains bulky or high-volume disease Dose-Volume Histograms DVH



12 PARSPORT Nutting. Lancet Oncol 2011;12:127-36



13 H&N IMRT Practice Heterogeneity T2 N1 M0 Tonsil Cancer P. Harari: Radiotherapy & Oncology 2012 Courtesy of Dr. Harari

14 Isodoses or Heterodoses: 3D!
15 IMRT: decisions boost & fractionation: sequential vs SIB Gross Disease High-Risk Risk 70 Gy in daily fractions Gy in daily fractions Gy in daily fractions Macro micro nano level of risk

16 3DCRT IMRT IMRT
17 Selected topics for talented When RT? Locally advanced stages Nasopharynx Postoperative RT New concepts, new trials How? and what? (to expect) 16
18 Loco-regional Advanced when, how and what to expect - Unresectable: radical chemoradiation - Consolidation: post-induction CT - Oligo-recurrent: radical rescue
19
20
21 Selected topics for talented Locally advanced stages: randomized trials RT FRACTIONATION altered vs standard 20
22 RTOG Standard fractionation Hyperfractionation Accelerated fractionation, split course Accelerated fractionation, concomitant boost 7000 cgy/35 fx 7 weeks 8160 cgy/68 fx 7 weeks (1.2 Gy Bid) 6720 cgy/42 fx 6 weeks (1.6 Gy Bid) 7200 cgy/42 fx 6 weeks
23 33 trials and 11,423 patients Any Hiperfractionation Overall survival Moderately accelerated Very accelerated Fractionation RT 5y 10 y Hiperfractionation 8,1% 3,9% Very accelerated 1,3% 0,4%
24 Any Hiperfractionation Moderately accelerated Very accelerated Progression-free survival

25 Selected topics for talented FRACTIONATION +/- CRT 24


26 Clin Oncol (R Coll Radiol) ;28: Systematic Review and Meta-analysis of Conventionally Fractionated Concurrent Chemoradiotherapy versus Altered Fractionation Radiotherapy Alone in the Definitive Management of Locoregionally Advanced Head and Neck Squamous Cell Carcinoma. Gupta T 1, Kannan S 2, Ghosh-Laskar S 3, Agarwal JP 3 No form of acceleration can potentially compensate fully for the lack of concurrent chemotherapy
27 Chemoradiotherapy updated meta-analysis, Jan 1, 2009, and July 15, 2015 conventional fractionation RT vs altered fractionation radiotherapy conventional fractionation CRT vs altered fractionation radiotherapy alone 33 trials and 11,423 patients Eligible trials had to start randomisation on or after Jan 1, 1970, and completed accrual before Dec 31, 2010


28 OS LR failures New England Journal of Medicine, 2006;354:567-78


29



30 LRC OS HPV + HPV - OS The addition of an anti-egfr agent to RT or CRT do not improve outcomes compared with CRT in LA-HNSCC. Except for patients with coexisting medical conditions or decreased performance status, concurrent CRT should remain the standard of care for patients with LA-HNSCC.
31 Loco-regional Advanced when, how and what to expect - Unresectable: radical chemoradiation - Consolidation: post-induction CT - Oligo-recurrent: radical rescue
32 Why to Still Consider Induction Chemotherapy Pros: Salvage subclinical M1 disease and OS benefit Assessment of response Reduce dose/volume of RT Cons: Prolongs treatment time/cost Increases toxicity No clinical benefit
33 N2 / N3
34 Responders
35 HPV Oroph Non-Oroph N2 N3
36 Induction chemotherapy followed by concurrent chemoradiotherapy (sequential chemoradiotherapy) versus concurrent chemoradiotherapy alone in locally advanced head and neck cancer (PARADIGM): a randomised phase 3 trial. Lancet Oncol Mar;14(3): Study terminated early due to poor accrual (145 enrolled) Median f/u 49 mos 3-yr OS: (73% ICT vs 78% CRT, NS) Febrile neutropenia (23% ICT vs 1% CRT) Haddad, Lancet Oncol. 2013; 14: 257.


37 LRC DFS Induction CT Surgery +/- RT OS

38 5 randomized trials 1022 patients TPF induction CT Pt / Tx CRT
39
40 LRR Distant faliure

41 ECOG 1308: Phase II trial of IC followed by cetuximab + 54 Gy vs 69 Gy IMRT in HPV-associated resectable oropharyngeal SCCA
42 Loco-regional Advanced when, how and what to expect - Unresectable: radical chemoradiation - Consolidation: post-induction CT - Oligo-recurrent: radical rescue


43 bio-guided IMRT for oligo-recurrences

44 22 articles 1105 patients published 1976 and 2014 The 5-year OS improved over time: 18% pre % mixed pre-2000 and post % in the post-2000 (p <.001).
; mucositis and/or dyspha-gia/pharyngitis (11 52%) late fibrosis (range, 2 44%) pharynx dysfunction (range, 2 70%).")
45 Re-RT after salvage surgery, 16 publications 919 patients 522 patients POreRT to highly selected patients with high-risk features (R+) Re-irradiation with highly conformal techniques and only when a dose > 50 Gy can be delivered LC from 21% to 100% 2-years-OS of 48% (range, 24 81%); mucositis and/or dyspha-gia/pharyngitis (11 52%) late fibrosis (range, 2 44%) pharynx dysfunction (range, 2 70%). death up to 6,8%
46 Selected topics for talented When RT? Locally advanced stages Nasopharynx Postoperative RT New concepts, new trials How? and what? (to expect) 45

47 Nasopharynx: Anatomy Nasal choanae Clivus Soft Palate
48 Treatment Approach Stage I RT alone (10 yr LC and DSS > 90%) Stage II-IVb Concurrent chemoradiation + adjuvant chemotherapy Stage IVc (M1 disease) Chemotherapy RT for symptom palliation
49 RT Treatment planning IMRT LC > 90% Gross disease (primary + nodes): ~70 Gy High-risk CTV (bilateral RP, II-V, subclinical nasopharynx): Gy Low-risk CTV: Gy


50 NPC: Imaging

51 Induction Adjuvant Experimental arm all combinations Concomitant CRT + adjuvant
52 EBV: Prognostic Marker Pre-RT 1 wk post-rt Lin N Engl J Med 2004; 350: 2461
53 Rmyistwr
54 Nasopharynx: Summary RT is the curative modality RT alone: stage I CRT: stage II-IVb IMRT: standard of care High rates of local control (> 90%) Failures predominantly systemic Approaches to address to systemic relapse warranted Role of adjuvant chemotherapy? Risk stratification via EBV
55 Selected topics for talented When RT? Locally advanced stages Nasopharynx Postoperative RT New concepts, new trials How? and what? (to expect) 54


56 Poor / Imposible Volume Definition


57 Ipsilateral Level 3 Failure T2N1 oral tongue cancer, postoperative radiation Damast, et al. Head Neck 2012;34:

58 Submental Failure Damast, et al. Head Neck 2012;34:


59 Postoperative IMRT for Laryngeal Cancer Stoma > 60 Gy
60 Postop RT: Indications Multiple lymph nodes involved Extracapsular extension (ECE) Positive/close surgical margins Perineural invasion Lymphovascular invasion Deep (>5mm) invasion
61 Postop RT: Treatment Decisions May deliver RT as soon as the wound is healed Ideally initiate within 6 weeks after surgery Intermediate Risk: 60 Gy / 30 fractions High Risk (Positive margin / ECE): 66 Gy / 33 fx Concurrent systemic therapy in high risk patients
62 Combined RTOG/EORTC Analysis Bernier, Cooper. Head Neck 2005;27:843
63 Long Term Follow Up of RTOG 9501 Patients with Positive Margin and/or ECE Cooper et al. IJROBP 2012


64
65
66
67


68 CRT vs RT alone: postoperative Loco-regional Disease free Survival

69 Selected topics for talented When RT? Locally advanced stages Nasopharynx Postoperative RT Laryngeal preservation New concepts, new trials How? and what? (to expect) 68

70 Anatomy Supraglottis Epiglottis Arytenoids AE folds False cords Ventricles Glottis True vocal cords Subglottis 5mm below glottis to bottom of cricoid
71 Treatment Approach Glottic, early stage: single modality RT: limited field Surgery: partial laryngectomy, cordectomy, laser Supraglottic, early stage: single modality RT: include regional nodes (bilateral levels II-IV) Surgery: partial laryngectomy + neck dissection Advanced stage: combined modality Organ preservation (concurrent chemoradiation): VA larynx, RTOG Surgery + adjuvant RT (+/- chemo) Selection: need to consider disease and patient characteristics
72 Dose and fractionation: T1 glottis (Yamazaki et al. IJROBP 2006) Prospective, Randomized Trial, pts with T1N0 Glottic Cancers Randomized to A)2.00 Gy/fraction 1)60 Gy in 30 fractions (<2/3 VC) 2)66 Gy in 33 fractions (>2/3 VC) B)2.25 Gy/fraction 1)56.25 Gy in 25 fractions (<2/3 VC) 2)63 Gy in 28 fractions (>2/3 VC) No significant increase in acute or chronic toxicity Conclusion: Use 225 cgy per fraction to 63 Gy for T1 Glottic Ca
73 RTOG LARYNX TRIAL 84% 72% 67% Median F/U 3.8 years Forastiere et al, NEJM 2003; 349:
74 Long Term Update of RTOG LARYNGEAL PRESERVATION OVERALL SURVIVAL Forastiere et al, JCO 2013
75 EORTC Laryngeal Preservation Trial R A N D O M I Z E Surgery Induction Chemotherapy (3 Cycles) RT Complete Responders* RT PR/NR Surgery XRT Induction Chemotherapy: Cisplatin and 5 FU J.L. Lefebvre et al, JNCI 88: , 1996
76 EORTC Laryngeal Preservation Trial Median F/U: 10.5yrs S + RT CT+ RT+ S No. of patients yr. PFS 8.5% 10.5% 10-yr. Survival 13.8% 13.1% Distant Mets. 36% 25% 10 yr. Alive w/larynx 8.7% J.L. Lefebvre et al, JNCI 88: , 1996; Annals Oncology, 2012


77 T4a Laryngeal Cancer
 NCDB 969 pts RT for T4a larynx cancer from 2003-2006 Patterns of care/survival")
78 Patient selection/patterns of care/t4a (Grover et al. IJROBP 2015) NCDB 969 pts RT for T4a larynx cancer from Patterns of care/survival Results 2/3 treated with OP, 1/3 with initial TL


79


80 Selected topics for talented When RT? Locally advanced stages Nasopharynx Postoperative RT Laryngeal preservation Re-irradiation New concepts, new trials How? and what? (to expect) 79




81 22 retrospective studies >550 pts 14% - 54% 5y 51% post y 5y Time recruitment Surgery RT
 specificity (87% vs 95%; p <0.005).")
82 FDG-PET/CT in detecting nodal disease within 6 months after treatment Systematic review + meta-analysis 20 studies (1293 patients) Sensitivity 83%, specificity 91% HPV positive tumors were associated with lower sensitivity(75%vs89%;p=0.01) specificity (87% vs 95%; p <0.005). FDG-PET/CT within 6 months after (chemo)radiotherapy in HNSCC patients is a reliable method for ruling out residual/recurrent nodal disease (less reliable in HPV positive tumors) optimal surveillance strategy remains to be determined.
83 Ongoing RT practice oriented research 7 ECOG 1308: HPV + Induction CT + Cetuximab +IMRT/Cetuximab RTOG 1016: HPV + IMRT/CDDP vs IMRT/Cetuximab RTOG 1216: > 60 Gy + CDDP vs Docetaxel vs Docetaxel/Cetuximab ECOG 3311: HPV + risk adapted IMRT 50 vs 60 vs 66 Gy/CDDP RTOG 1221: HPV + IMRT 70 Gy vs surgery (PORT) RTOG 1305: IMRT 70 Gy/CDDP plasma EBV +/- Chemo/adjuvant 82



84 MOLECULAR IMAGE GUIDED RT (M-IGRT) GTV s aller Nodes ore Mis- atch GTV 20-40% 83



85 5 cm Macroscópic 5 cm TAC 5 cm 18 F-FDG PET Daisne et al, 2004


86 T3 N2c oropharynx: target adapted to M-IGRT 85

87 DOSE-ESCALATION BASED ON HIPOXIA M-IGRT A: GTV Hipoxia B: STANDARD PLAN C: Dose-escalation based on HIPOXIA gradients D: Dose-escalation based on HIPOXIA presence 86

88 TIME-IMAGE GUIDED RT (T-IGRT) 4D = time = movement = changes = adaptation = ART 87


89 Potential Target Deformations during Tx T-IGRT implications 88


90 Potential Dosimetric Changes Hansen et al Int. J. Radiation Oncology Biol. Phys. 2006;64:
 85")
91 4.2 mm INCREASED MEAN DOSE TO PAROTID 5 Gy Nishi et al, Radiother and Oncol 106 (2013)

92
93
94 Selected topics for talented when, how and what HPV a d RT! De-escalatio? Not et but Locall ad a ced stages CRT + dose-escalation + AFX? induction CT? Nasophar CRT tailored volume Larynx preservation: CRT supra-tailored strategy Postoperati e RT risk adapted CRT Oligo-recurrent: 50% OS radical rescue ( 40% 2y OS re-rt) Ne co cepts M-IGRT / T-IGRT Ne trials Induction CT, viral status tailoring 93
Locally advanced head and neck cancer
 Locally advanced head and neck cancer Radiation Oncology Perspective Petek Erpolat, MD Gazi University, Turkey Definition and Management of LAHNC Stage III or IV cancers generally include larger primary
Locally advanced head and neck cancer Radiation Oncology Perspective Petek Erpolat, MD Gazi University, Turkey Definition and Management of LAHNC Stage III or IV cancers generally include larger primary
Laryngeal Preservation Using Radiation Therapy. Chemotherapy and Organ Preservation
 1 Laryngeal Preservation Using Radiation Therapy 1903: Schepegrell was the first to perform radiation therapy for the treatment of laryngeal cancer Conventional external beam radiation produced disappointing
1 Laryngeal Preservation Using Radiation Therapy 1903: Schepegrell was the first to perform radiation therapy for the treatment of laryngeal cancer Conventional external beam radiation produced disappointing
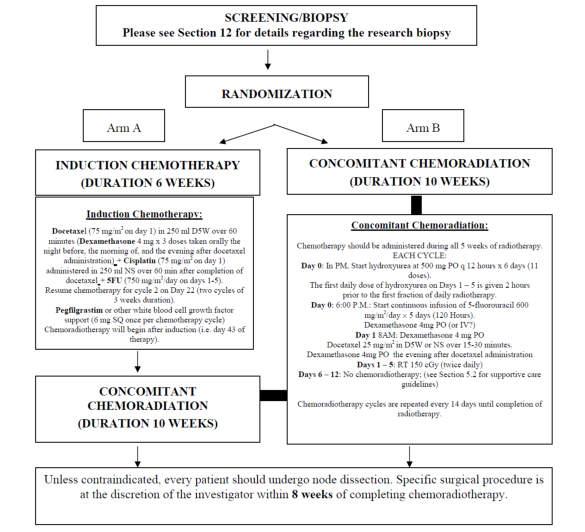
Protocol of Radiotherapy for Head and Neck Cancer
 106 年 12 月修訂 Protocol of Radiotherapy for Head and Neck Cancer Indication of radiotherapy Indication of definitive radiotherapy with or without chemotherapy (1) Resectable, but medically unfit, or high
106 年 12 月修訂 Protocol of Radiotherapy for Head and Neck Cancer Indication of radiotherapy Indication of definitive radiotherapy with or without chemotherapy (1) Resectable, but medically unfit, or high
Pre- Versus Post-operative Radiotherapy
 Postoperative Radiation and Chemoradiation: Indications and Optimization of Practice Dislosures Clinical trial support from Genentech Inc. Sue S. Yom, MD, PhD Associate Professor UCSF Radiation Oncology
Postoperative Radiation and Chemoradiation: Indications and Optimization of Practice Dislosures Clinical trial support from Genentech Inc. Sue S. Yom, MD, PhD Associate Professor UCSF Radiation Oncology
Simultaneous Integrated Boost or Sequential Boost in the Setting of Standard Dose or Dose De-escalation for HPV- Associated Oropharyngeal Cancer
 Simultaneous Integrated Boost or Sequential Boost in the Setting of Standard Dose or Dose De-escalation for HPV- Associated Oropharyngeal Cancer Dawn Gintz, CMD, RTT Dosimetry Coordinator of Research and
Simultaneous Integrated Boost or Sequential Boost in the Setting of Standard Dose or Dose De-escalation for HPV- Associated Oropharyngeal Cancer Dawn Gintz, CMD, RTT Dosimetry Coordinator of Research and
MANAGEMENT OF CA HYPOPHARYNX
 MANAGEMENT OF CA HYPOPHARYNX GENERAL TREATMENT RECOMMENDATIONS BASED ON HYPOPHARYNX TUMOR STAGE For patients presenting with early-stage definitive radiotherapy alone or voice-preserving surgery are viable
MANAGEMENT OF CA HYPOPHARYNX GENERAL TREATMENT RECOMMENDATIONS BASED ON HYPOPHARYNX TUMOR STAGE For patients presenting with early-stage definitive radiotherapy alone or voice-preserving surgery are viable
The International Federation of Head and Neck Oncologic Societies. Current Concepts in Head and Neck Surgery and Oncology
 The International Federation of Head and Neck Oncologic Societies Current Concepts in Head and Neck Surgery and Oncology www.ifhnos.net The International Federation of Head and Neck Oncologic Societies
The International Federation of Head and Neck Oncologic Societies Current Concepts in Head and Neck Surgery and Oncology www.ifhnos.net The International Federation of Head and Neck Oncologic Societies
De-Escalate Trial for the Head and neck NSSG. Dr Eleanor Aynsley Consultant Clinical Oncologist
 De-Escalate Trial for the Head and neck NSSG Dr Eleanor Aynsley Consultant Clinical Oncologist 3 HPV+ H&N A distinct disease entity Leemans et al., Nature Reviews, 2011 4 Good news Improved response to
De-Escalate Trial for the Head and neck NSSG Dr Eleanor Aynsley Consultant Clinical Oncologist 3 HPV+ H&N A distinct disease entity Leemans et al., Nature Reviews, 2011 4 Good news Improved response to
HPV INDUCED OROPHARYNGEAL CARCINOMA radiation-oncologist point of view. Prof. dr. Sandra Nuyts Dep. Radiation-Oncology UH Leuven Belgium
 HPV INDUCED OROPHARYNGEAL CARCINOMA radiation-oncologist point of view Prof. dr. Sandra Nuyts Dep. Radiation-Oncology UH Leuven Belgium DISCLOSURE OF INTEREST Nothing to declare HEAD AND NECK CANCER -HPV
HPV INDUCED OROPHARYNGEAL CARCINOMA radiation-oncologist point of view Prof. dr. Sandra Nuyts Dep. Radiation-Oncology UH Leuven Belgium DISCLOSURE OF INTEREST Nothing to declare HEAD AND NECK CANCER -HPV
Organ-Preservation Strategies in head and neck cancer. Teresa Bonfill Abella Oncologia Mèdica Parc Taulí Sabadell. Hospital Universitari
 Organ-Preservation Strategies in head and neck cancer Teresa Bonfill Abella Oncologia Mèdica Parc Taulí Sabadell. Hospital Universitari Larynx Hypopharynx The goal of treatment is to achieve larynx preservation
Organ-Preservation Strategies in head and neck cancer Teresa Bonfill Abella Oncologia Mèdica Parc Taulí Sabadell. Hospital Universitari Larynx Hypopharynx The goal of treatment is to achieve larynx preservation
Sequencing Chemo with Radiation therapy Locally Advanced Head and Neck Cancer. Dr P Vijay Anand Reddy Director Apollo Cancer Hospital
 Sequencing Chemo with Radiation therapy Locally Advanced Head and Neck Cancer Dr P Vijay Anand Reddy Director Apollo Cancer Hospital H&N Ca - Disease Burden 15-20% of all cancers in India, 8% worldwide
Sequencing Chemo with Radiation therapy Locally Advanced Head and Neck Cancer Dr P Vijay Anand Reddy Director Apollo Cancer Hospital H&N Ca - Disease Burden 15-20% of all cancers in India, 8% worldwide
Clinical Trials in Transoral Endoscopic Head &Neck Surgery ECOG3311 and RTOG1221. Chris Holsinger, MD, FACS Bob Ferris, MD, PhD, FACS
 Clinical Trials in Transoral Endoscopic Head &Neck Surgery ECOG3311 and RTOG1221 Chris Holsinger, MD, FACS Bob Ferris, MD, PhD, FACS 1 Disclosure I have no conflicts of interest to disclose 2 Robotic H&N
Clinical Trials in Transoral Endoscopic Head &Neck Surgery ECOG3311 and RTOG1221 Chris Holsinger, MD, FACS Bob Ferris, MD, PhD, FACS 1 Disclosure I have no conflicts of interest to disclose 2 Robotic H&N
Self-Assessment Module 2016 Annual Refresher Course
 LS16031305 The Management of s With r. Lin Learning Objectives: 1. To understand the changing demographics of oropharynx cancer, and the impact of human papillomavirus on overall survival and the patterns
LS16031305 The Management of s With r. Lin Learning Objectives: 1. To understand the changing demographics of oropharynx cancer, and the impact of human papillomavirus on overall survival and the patterns
Adjuvant Therapy in Locally Advanced Head and Neck Cancer. Ezra EW Cohen University of Chicago. Financial Support
 Adjuvant Therapy in Locally Advanced Head and Neck Cancer Ezra EW Cohen University of Chicago Financial Support This program is made possible by an educational grant from Eli Lilly Oncology, who had no
Adjuvant Therapy in Locally Advanced Head and Neck Cancer Ezra EW Cohen University of Chicago Financial Support This program is made possible by an educational grant from Eli Lilly Oncology, who had no
Head and NeckCancer: multi-modal therapeuticintegration
 Head and NeckCancer: multi-modal therapeuticintegration P. Ponticelli, L. Lastrucci, R. De Majo, A. Rampini U.O.C. Radioterapia Ospedale S. Donato ASL 8 -AREZZO Summary Biological considerations Clinical
Head and NeckCancer: multi-modal therapeuticintegration P. Ponticelli, L. Lastrucci, R. De Majo, A. Rampini U.O.C. Radioterapia Ospedale S. Donato ASL 8 -AREZZO Summary Biological considerations Clinical
Head and Neck cancer
 Head and Neck cancer Medical Oncologist s Role in Multidisciplinary Teams - Focus on Adjuvant & Neo-adjuvant Therapy - Hye Ryun Kim, M.D. Yonsei Cancer Center, Medical Oncology Contents I. Introduction
Head and Neck cancer Medical Oncologist s Role in Multidisciplinary Teams - Focus on Adjuvant & Neo-adjuvant Therapy - Hye Ryun Kim, M.D. Yonsei Cancer Center, Medical Oncology Contents I. Introduction
The International Federation of Head and Neck Oncologic Societies. Current Concepts in Head and Neck Surgery and Oncology
 The International Federation of Head and Neck Oncologic Societies Current Concepts in Head and Neck Surgery and Oncology 2018 www.ifhnos.net The International Federation of Head and Neck Oncologic Societies
The International Federation of Head and Neck Oncologic Societies Current Concepts in Head and Neck Surgery and Oncology 2018 www.ifhnos.net The International Federation of Head and Neck Oncologic Societies
RADIO- AND RADIOCHEMOTHERAPY OF HEAD AND NECK TUMORS. Zoltán Takácsi-Nagy PhD Department of Radiotherapy National Institute of Oncology, Budapest 1.
 RADIO- AND RADIOCHEMOTHERAPY OF HEAD AND NECK TUMORS Zoltán Takácsi-Nagy PhD Department of Radiotherapy National Institute of Oncology, Budapest 1. 550 000 NEW PATIENTS/YEAR WITH HEAD AND NECK CANCER ALL
RADIO- AND RADIOCHEMOTHERAPY OF HEAD AND NECK TUMORS Zoltán Takácsi-Nagy PhD Department of Radiotherapy National Institute of Oncology, Budapest 1. 550 000 NEW PATIENTS/YEAR WITH HEAD AND NECK CANCER ALL
Neoplasie del laringe Diagnosi e trattamento
 Neoplasie del laringe Diagnosi e trattamento Venerdì 22 maggio 2015 Alessandria Trattamenti non chirurgici: Preservazione d organo, malattia localmente avanzata Marco C Merlano A.O. S.Croce e Carle, Ospedale
Neoplasie del laringe Diagnosi e trattamento Venerdì 22 maggio 2015 Alessandria Trattamenti non chirurgici: Preservazione d organo, malattia localmente avanzata Marco C Merlano A.O. S.Croce e Carle, Ospedale
Head and Neck Reirradiation: Perils and Practice
 Head and Neck Reirradiation: Perils and Practice David J. Sher, MD, MPH Department of Radiation Oncology Dana-Farber Cancer Institute/ Brigham and Women s Hospital Conflicts of Interest No conflicts of
Head and Neck Reirradiation: Perils and Practice David J. Sher, MD, MPH Department of Radiation Oncology Dana-Farber Cancer Institute/ Brigham and Women s Hospital Conflicts of Interest No conflicts of
State of the art for radiotherapy of SCCHN
 State of the art for radiotherapy of SCCHN Less side effects Cured More organ & function preservation Head & neck cancer = 42 000 new cases / year in Europe Not cured Local failure Distant failure More
State of the art for radiotherapy of SCCHN Less side effects Cured More organ & function preservation Head & neck cancer = 42 000 new cases / year in Europe Not cured Local failure Distant failure More
Oral Cavity Cancer Combined modality therapy
 Oral Cavity Cancer Combined modality therapy Dr. Christos CHRISTOPOULOS Radiation Oncologist Head and Neck Cancers Centre Hospitalier Universitaire (C.H.U.) de Limoges, France Disclosure slide I have no
Oral Cavity Cancer Combined modality therapy Dr. Christos CHRISTOPOULOS Radiation Oncologist Head and Neck Cancers Centre Hospitalier Universitaire (C.H.U.) de Limoges, France Disclosure slide I have no
Emerging Role of Immunotherapy in Head and Neck Cancer
 Emerging Role of Immunotherapy in Head and Neck Cancer Jared Weiss, MD Associate Professor of Medicine and Section Chief of Thoracic and Head/Neck Oncology UNC Lineberger Comprehensive Cancer Center Copyright
Emerging Role of Immunotherapy in Head and Neck Cancer Jared Weiss, MD Associate Professor of Medicine and Section Chief of Thoracic and Head/Neck Oncology UNC Lineberger Comprehensive Cancer Center Copyright
SAMO MASTERCLASS HEAD & NECK CANCER. Nicolas Mach, PD Geneva University Hospital
 SAMO MASTERCLASS HEAD & NECK CANCER Nicolas Mach, PD Geneva University Hospital Epidemiology Prevention Best treatment for localized disease Best treatment for relapsed or metastatic disease Introduction
SAMO MASTERCLASS HEAD & NECK CANCER Nicolas Mach, PD Geneva University Hospital Epidemiology Prevention Best treatment for localized disease Best treatment for relapsed or metastatic disease Introduction
TREATMENT TIME & TOBACCO: TWIN TERRORS Of H&N Therapy
 TREATMENT TIME & TOBACCO: TWIN TERRORS Of H&N Therapy Anurag K. Singh, MD Professor of Medicine University at Buffalo School of Medicine Professor of Oncology Director of Radiation Research Roswell Park
TREATMENT TIME & TOBACCO: TWIN TERRORS Of H&N Therapy Anurag K. Singh, MD Professor of Medicine University at Buffalo School of Medicine Professor of Oncology Director of Radiation Research Roswell Park
Larynx Hypopharynx. Therapy algorithms. Why larynx preservation at all? State of the art Jean Louis Lefebvre,Lille Jan Klozar,Prague
 Larynx Hypopharynx Moderation Rainald Knecht,Hamburg State of the art Jean Louis Lefebvre,Lille Debate pro CRT Jan Klozar,Prague contra CRT Marshall Posner,Boston Clinical cases all Therapy algorithms
Larynx Hypopharynx Moderation Rainald Knecht,Hamburg State of the art Jean Louis Lefebvre,Lille Debate pro CRT Jan Klozar,Prague contra CRT Marshall Posner,Boston Clinical cases all Therapy algorithms
Update on Limited Small Cell Lung Cancer. Laurie E Gaspar MD, MBA Prof/Chair Radiation Oncology University of Colorado Denver
 Update on Limited Small Cell Lung Cancer Laurie E Gaspar MD, MBA Prof/Chair Radiation Oncology University of Colorado Denver Objectives - Limited Radiation Dose Radiation Timing Radiation Volume PCI Neurotoxicity
Update on Limited Small Cell Lung Cancer Laurie E Gaspar MD, MBA Prof/Chair Radiation Oncology University of Colorado Denver Objectives - Limited Radiation Dose Radiation Timing Radiation Volume PCI Neurotoxicity
Multimodular treatment in Head and Neck Squamous Cell Carcinoma (HNSCC)
") Multimodular treatment in Head and Neck Squamous Cell Carcinoma (HNSCC) Amanda Psyrri, MD,FACP Attikon University Hospital Athens, Greece Learning objectives After reading and reviewing this material,
Multimodular treatment in Head and Neck Squamous Cell Carcinoma (HNSCC) Amanda Psyrri, MD,FACP Attikon University Hospital Athens, Greece Learning objectives After reading and reviewing this material,
肺癌放射治療新進展 Recent Advance in Radiation Oncology in Lung Cancer 許峰銘成佳憲國立台灣大學醫學院附設醫院腫瘤醫學部
 肺癌放射治療新進展 Recent Advance in Radiation Oncology in Lung Cancer 許峰銘成佳憲國立台灣大學醫學院附設醫院腫瘤醫學部 Outline Current status of radiation oncology in lung cancer Focused on stage III non-small cell lung cancer Radiation
肺癌放射治療新進展 Recent Advance in Radiation Oncology in Lung Cancer 許峰銘成佳憲國立台灣大學醫學院附設醫院腫瘤醫學部 Outline Current status of radiation oncology in lung cancer Focused on stage III non-small cell lung cancer Radiation
Clinical Discussion. Dr Pankaj Chaturvedi. Professor and Surgeon Tata Memorial Hospital
 Clinical Discussion Dr Pankaj Chaturvedi Professor and Surgeon Tata Memorial Hospital chaturvedi.pankaj@gmail.com 47/M/smoker Hopkins : Transglottic lesion No cartilage infiltration but sclerosis Left
Clinical Discussion Dr Pankaj Chaturvedi Professor and Surgeon Tata Memorial Hospital chaturvedi.pankaj@gmail.com 47/M/smoker Hopkins : Transglottic lesion No cartilage infiltration but sclerosis Left
Head and Neck Cancer:
 Head and Neck Cancer: Robert Haddad M.D. Clinical Director Head and Neck Oncology Program Dana Farber Cancer Institute Boston, MA Predictive Biomarkers: HPV Abstract 6003: Survival Outcomes By HPV Status
Head and Neck Cancer: Robert Haddad M.D. Clinical Director Head and Neck Oncology Program Dana Farber Cancer Institute Boston, MA Predictive Biomarkers: HPV Abstract 6003: Survival Outcomes By HPV Status
CURRENT STANDARD OF CARE IN NASOPHARYNGEAL CANCER
 CURRENT STANDARD OF CARE IN NASOPHARYNGEAL CANCER Jean-Pascal Machiels Department of medical oncology Institut I Roi Albert II Cliniques universitaires Saint-Luc Université catholique de Louvain, Brussels,
CURRENT STANDARD OF CARE IN NASOPHARYNGEAL CANCER Jean-Pascal Machiels Department of medical oncology Institut I Roi Albert II Cliniques universitaires Saint-Luc Université catholique de Louvain, Brussels,
The PARADIGM Study: A Phase III Study Comparing Sequential Therapy (ST) to Concurrent Chemoradiotherapy (CRT) in Locally Advanced Head and Neck Cancer
 to Concurrent Chemoradiotherapy (CRT) in Locally Advanced Head and Neck Cancer") The PARADIGM Study: A Phase III Study Comparing Sequential Therapy (ST) to Concurrent Chemoradiotherapy (CRT) in Locally Advanced Head and Neck Cancer Robert I. Haddad, Guilherme Rabinowits, Roy B. Tishler,
The PARADIGM Study: A Phase III Study Comparing Sequential Therapy (ST) to Concurrent Chemoradiotherapy (CRT) in Locally Advanced Head and Neck Cancer Robert I. Haddad, Guilherme Rabinowits, Roy B. Tishler,
Radio(chemo)therapy for head and neck cancer HNSCC: indications and modalities Prof. dr. Sandra Nuyts Radiotherapy-Oncology
therapy for head and neck cancer HNSCC: indications and modalities Prof. dr. Sandra Nuyts Radiotherapy-Oncology") Radio(chemo)therapy for head and neck cancer HNSCC: indications and modalities Prof. dr. Sandra Nuyts Radiotherapy-Oncology March 2018 > Half million new cases HNC/year in world 50-60% cured not cured
Radio(chemo)therapy for head and neck cancer HNSCC: indications and modalities Prof. dr. Sandra Nuyts Radiotherapy-Oncology March 2018 > Half million new cases HNC/year in world 50-60% cured not cured
Locally advanced disease & challenges in management
 Gynecologic Cancer InterGroup Cervix Cancer Research Network Cervix Cancer Education Symposium, February 2018 Locally advanced disease & challenges in management Carien Creutzberg Radiation Oncology, Leiden
Gynecologic Cancer InterGroup Cervix Cancer Research Network Cervix Cancer Education Symposium, February 2018 Locally advanced disease & challenges in management Carien Creutzberg Radiation Oncology, Leiden
Thomas Gernon, MD Otolaryngology THE EVOLVING TREATMENT OF SCCA OF THE OROPHARYNX
 Thomas Gernon, MD Otolaryngology THE EVOLVING TREATMENT OF SCCA OF THE OROPHARYNX Disclosures I have nothing to disclose. 3 Changing Role of Surgery N=42,688 Chen Ay et al. Larygoscope. 2007; 117:16-21
Thomas Gernon, MD Otolaryngology THE EVOLVING TREATMENT OF SCCA OF THE OROPHARYNX Disclosures I have nothing to disclose. 3 Changing Role of Surgery N=42,688 Chen Ay et al. Larygoscope. 2007; 117:16-21
Rob Glynne-Jones Mount Vernon Cancer Centre
 ESMO Preceptorship Programme Colorectal Cancer Prague July 2016 State of the art: Standard of care for anal squamous cancer Rob Glynne-Jones Mount Vernon Cancer Centre Aim to discuss Background The trials
ESMO Preceptorship Programme Colorectal Cancer Prague July 2016 State of the art: Standard of care for anal squamous cancer Rob Glynne-Jones Mount Vernon Cancer Centre Aim to discuss Background The trials
MANAGEMENT OF LOCALLY ADVANCED OROPHARYNGEAL CANER: HPV AND NON-HPV MEDIATED CANCERS
 MANAGEMENT OF LOCALLY ADVANCED OROPHARYNGEAL CANER: HPV AND NON-HPV MEDIATED CANCERS Kyle Arneson, MD PhD Avera Medical Group Radiation Oncology Avera Cancer Institute 16 th Annual Oncology Symposium September
MANAGEMENT OF LOCALLY ADVANCED OROPHARYNGEAL CANER: HPV AND NON-HPV MEDIATED CANCERS Kyle Arneson, MD PhD Avera Medical Group Radiation Oncology Avera Cancer Institute 16 th Annual Oncology Symposium September
67 F, 40 PY Smoker, Past heavy alcohol consumer, h/o COPD, Congestive heart failure. Presentation: Lump left upper neck x 1 year, non-tender, no
 67 F, 40 PY Smoker, Past heavy alcohol consumer, h/o COPD, Congestive heart failure. Presentation: Lump left upper neck x 1 year, non-tender, no overlying skin changes, gradually increasing in size. Recent
67 F, 40 PY Smoker, Past heavy alcohol consumer, h/o COPD, Congestive heart failure. Presentation: Lump left upper neck x 1 year, non-tender, no overlying skin changes, gradually increasing in size. Recent
Quality Variation and Clinical Impact in Head and Neck IMRT
 Quality Variation and Clinical Impact in Head and Neck IMRT 6 th IMRT Symposium, New York Sep. 20, 2010 K.S. Clifford Chao, MD Chairman, Combined Radiation Oncology, New York Presbyterian Hospital Chairman,
Quality Variation and Clinical Impact in Head and Neck IMRT 6 th IMRT Symposium, New York Sep. 20, 2010 K.S. Clifford Chao, MD Chairman, Combined Radiation Oncology, New York Presbyterian Hospital Chairman,
Oral cavity cancer Post-operative treatment
 Oral cavity cancer Post-operative treatment Dr. Christos CHRISTOPOULOS Radiation Oncologist Centre Hospitalier Universitaire (C.H.U.) de Limoges, France Important issues RT -techniques Patient selection
Oral cavity cancer Post-operative treatment Dr. Christos CHRISTOPOULOS Radiation Oncologist Centre Hospitalier Universitaire (C.H.U.) de Limoges, France Important issues RT -techniques Patient selection
ES-SCLC Joint Case Conference. Anthony Paravati Adam Yock
 ES-SCLC Joint Case Conference Anthony Paravati Adam Yock Case 57 yo woman with 35 pack year smoking history presented with persistent cough and rash Chest x-ray showed a large left upper lobe/left hilar
ES-SCLC Joint Case Conference Anthony Paravati Adam Yock Case 57 yo woman with 35 pack year smoking history presented with persistent cough and rash Chest x-ray showed a large left upper lobe/left hilar
CANCERS of OROPHARYNX and HYPOPHARYNX. STAGING and TREATMENT
 1 CANCERS of OROPHARYNX and HYPOPHARYNX STAGING and TREATMENT 2 1. Staging 2. General Principles of Treatment 3. Site Specific Treatment Guidelines 4. Selected Abstracts from Relevant Studies 3 1. Staging
1 CANCERS of OROPHARYNX and HYPOPHARYNX STAGING and TREATMENT 2 1. Staging 2. General Principles of Treatment 3. Site Specific Treatment Guidelines 4. Selected Abstracts from Relevant Studies 3 1. Staging
Laryngeal Conservation
 Laryngeal Conservation Sarah Rodriguez, MD Faculty Advisor: Shawn Newlands, MD, PhD The University of Texas Medical Branch Department of Otolaryngolgy Grand Rounds Presentation February 2005 Introduction
Laryngeal Conservation Sarah Rodriguez, MD Faculty Advisor: Shawn Newlands, MD, PhD The University of Texas Medical Branch Department of Otolaryngolgy Grand Rounds Presentation February 2005 Introduction
Dose escalation for NSCLC using conformal RT: 3D and IMRT. Hasan Murshed
 Dose escalation for NSCLC using conformal RT: 3D and IMRT. Hasan Murshed Take home message Preliminary data shows CRT technique in NSCLC allows dose escalation to an unprecedented level maintaining cancer
Dose escalation for NSCLC using conformal RT: 3D and IMRT. Hasan Murshed Take home message Preliminary data shows CRT technique in NSCLC allows dose escalation to an unprecedented level maintaining cancer
ESMO Preceptorship Programme, Colorectal Cancer, Vienna
 State of the art multimodal treatment of anal cancer ESMO Preceptorship Programme, Colorectal Cancer, Vienna Rob Glynne-Jones Mount Vernon Centre for Cancer Treatment Disclosures: last 5 years Speaker:
State of the art multimodal treatment of anal cancer ESMO Preceptorship Programme, Colorectal Cancer, Vienna Rob Glynne-Jones Mount Vernon Centre for Cancer Treatment Disclosures: last 5 years Speaker:
Squamous Cell Carcinoma of the Oral Cavity: Radio therapeutic Considerations
 Squamous Cell Carcinoma of the Oral Cavity: Radio therapeutic Considerations Troy G. Scroggins Jr. MD Chairman, Department of Radiation Oncology Ochsner Health Systems 1 Association of Postoperative Radiotherapy
Squamous Cell Carcinoma of the Oral Cavity: Radio therapeutic Considerations Troy G. Scroggins Jr. MD Chairman, Department of Radiation Oncology Ochsner Health Systems 1 Association of Postoperative Radiotherapy
Tratamiento Multidisciplinar de Estadios Localmente Avanzados en Cáncer de Pulmón
 Tratamiento Multidisciplinar de Estadios Localmente Avanzados en Cáncer de Pulmón Santiago Ponce Aix Servicio Oncología Médica Hospital Universitario 12 de Octubre Madrid Stage III: heterogenous disease
Tratamiento Multidisciplinar de Estadios Localmente Avanzados en Cáncer de Pulmón Santiago Ponce Aix Servicio Oncología Médica Hospital Universitario 12 de Octubre Madrid Stage III: heterogenous disease
Practice teaching course on head and neck cancer management
 28-29 October 2016 - Saint-Priest en Jarez, France Practice teaching course on head and neck cancer management IMPROVING THE PATIENT S LIFE LIFE THROUGH MEDICAL MEDICAL EDUCATION EDUCATION www.excemed.org
28-29 October 2016 - Saint-Priest en Jarez, France Practice teaching course on head and neck cancer management IMPROVING THE PATIENT S LIFE LIFE THROUGH MEDICAL MEDICAL EDUCATION EDUCATION www.excemed.org
HPV POSITIVE OROPHARYNGEAL CARCINOMA the radiation oncologist point of view. Prof. dr. Sandra Nuyts Dep. Radiation-Oncology UH Leuven Belgium
 HPV POSITIVE OROPHARYNGEAL CARCINOMA the radiation oncologist point of view Prof. dr. Sandra Nuyts Dep. Radiation-Oncology UH Leuven Belgium HEAD AND NECK CANCER -HPV Change in incidence: HEAD AND NECK
HPV POSITIVE OROPHARYNGEAL CARCINOMA the radiation oncologist point of view Prof. dr. Sandra Nuyts Dep. Radiation-Oncology UH Leuven Belgium HEAD AND NECK CANCER -HPV Change in incidence: HEAD AND NECK
Evaluation of Whole-Field and Split-Field Intensity Modulation Radiation Therapy (IMRT) Techniques in Head and Neck Cancer
 Techniques in Head and Neck Cancer") 1 Charles Poole April Case Study April 30, 2012 Evaluation of Whole-Field and Split-Field Intensity Modulation Radiation Therapy (IMRT) Techniques in Head and Neck Cancer Abstract: Introduction: This study
1 Charles Poole April Case Study April 30, 2012 Evaluation of Whole-Field and Split-Field Intensity Modulation Radiation Therapy (IMRT) Techniques in Head and Neck Cancer Abstract: Introduction: This study
Some Seminal Studies. Chemotherapy Alone is Inadequate. Bladder Cancer Role of Radiation in Bladder Sparing. Primary Radiation for Bladder Cancer
 Bladder Cancer Role of Radiation in Bladder Sparing David C. Beyer M.D., FACR, FACRO, FASTRO Arizona Oncology Services Phoenix, Arizona Primary Radiation for Bladder Cancer No modern surgery / XRT randomized
Bladder Cancer Role of Radiation in Bladder Sparing David C. Beyer M.D., FACR, FACRO, FASTRO Arizona Oncology Services Phoenix, Arizona Primary Radiation for Bladder Cancer No modern surgery / XRT randomized
San Antonio Breast Cancer Symposium 2010 Highlights Radiotherapy
 San Antonio Breast Cancer Symposium 2010 Highlights Radiotherapy Kathleen C. Horst, M.D. Assistant Professor Department of Radiation Oncology Stanford University The Optimal SEquencing of Adjuvant Chemotherapy
San Antonio Breast Cancer Symposium 2010 Highlights Radiotherapy Kathleen C. Horst, M.D. Assistant Professor Department of Radiation Oncology Stanford University The Optimal SEquencing of Adjuvant Chemotherapy
REIRRADIATION OF HEAD & NECK TARGETS
 REIRRADIATION OF HEAD & NECK TARGETS WORKSHOP-Current challenges of patient re-irradiation 6-7 september 2018, Stockholm, Sweden Claes Mercke Karolinska Institute and Karolinska University Hospital STOCKHOLM
REIRRADIATION OF HEAD & NECK TARGETS WORKSHOP-Current challenges of patient re-irradiation 6-7 september 2018, Stockholm, Sweden Claes Mercke Karolinska Institute and Karolinska University Hospital STOCKHOLM
The Evolution of SBRT and Hypofractionation in Thoracic Radiation Oncology
 The Evolution of SBRT and Hypofractionation in Thoracic Radiation Oncology (specifically, lung cancer) 2/10/18 Jeffrey Kittel, MD Radiation Oncology, Aurora St. Luke s Medical Center Outline The history
The Evolution of SBRT and Hypofractionation in Thoracic Radiation Oncology (specifically, lung cancer) 2/10/18 Jeffrey Kittel, MD Radiation Oncology, Aurora St. Luke s Medical Center Outline The history
Case Scenario 1. Pathology: Specimen type: Incisional biopsy of the glottis Histology: Moderately differentiated squamous cell carcinoma
 Case Scenario 1 History A 52 year old male with a 20 pack year smoking history presented with about a 6 month history of persistent hoarseness. The patient had a squamous cell carcinoma of the lip removed
Case Scenario 1 History A 52 year old male with a 20 pack year smoking history presented with about a 6 month history of persistent hoarseness. The patient had a squamous cell carcinoma of the lip removed
Cetuximab/cisplatin and radiotherapy in HNSCC: is there a favorite choice?
 Cent. Eur. J. Med. 9(2) 2014 279-284 DOI: 10.2478/s11536-013-0154-9 Central European Journal of Medicine Cetuximab/cisplatin and radiotherapy in HNSCC: is there a favorite choice? Jacopo Giuliani* 1, Marina
Cent. Eur. J. Med. 9(2) 2014 279-284 DOI: 10.2478/s11536-013-0154-9 Central European Journal of Medicine Cetuximab/cisplatin and radiotherapy in HNSCC: is there a favorite choice? Jacopo Giuliani* 1, Marina
Laryngeal and hypopharyngeal cancers
 Laryngeal and hypopharyngeal cancers Induction Chemotherapy in combined modality approaches Atenas 16.09.2017 Ana Ferreira Castro, MD Medical Oncology Centro Hospitalar do Porto Instituto de Ciências Biomédicas
Laryngeal and hypopharyngeal cancers Induction Chemotherapy in combined modality approaches Atenas 16.09.2017 Ana Ferreira Castro, MD Medical Oncology Centro Hospitalar do Porto Instituto de Ciências Biomédicas
3/8/2014. Case Presentation. Primary Treatment of Anal Cancer. Anatomy. Overview. March 6, 2014
 Case Presentation Primary Treatment of Anal Cancer 65 year old female presents with perianal pain, lower GI bleeding, and anemia with Hb of 7. On exam 6 cm mass protruding through the anus with bulky R
Case Presentation Primary Treatment of Anal Cancer 65 year old female presents with perianal pain, lower GI bleeding, and anemia with Hb of 7. On exam 6 cm mass protruding through the anus with bulky R
Adjuvant Radiotherapy for completely resected NSCLC
 Adjuvant Radiotherapy for completely resected NSCLC ESMO Preceptorship on lung Cancer Manchester February 2017 Cécile Le Péchoux Radiation Oncology Department IOT Institut d Oncologie Thoracique Local
Adjuvant Radiotherapy for completely resected NSCLC ESMO Preceptorship on lung Cancer Manchester February 2017 Cécile Le Péchoux Radiation Oncology Department IOT Institut d Oncologie Thoracique Local
Upper Gastrointestinal. Friday, March 2, :00 p.m. 2:45 p.m.
 Upper Gastrointestinal Friday, March 2, 2018 2:00 p.m. 2:45 p.m. Social Q&A Use your phone, tablet, or laptop to Submit questions to speakers and moderators Answer interactive questions / audience response
Upper Gastrointestinal Friday, March 2, 2018 2:00 p.m. 2:45 p.m. Social Q&A Use your phone, tablet, or laptop to Submit questions to speakers and moderators Answer interactive questions / audience response
RADIATION THERAPY AND CHEMOTHERAPY IN LOCALLY ADVANCED CANCER OF THE HEAD AND NECK Carlos A. Perez, M.D. Former Chairman/Professor Emeritus
 RADIATION THERAPY AND CHEMOTHERAPY IN LOCALLY ADVANCED CANCER OF THE HEAD AND NECK Carlos A. Perez, M.D. Former Chairman/Professor Emeritus Department of Radiation Oncology Mallinckrodt Institute of Radiology/
RADIATION THERAPY AND CHEMOTHERAPY IN LOCALLY ADVANCED CANCER OF THE HEAD AND NECK Carlos A. Perez, M.D. Former Chairman/Professor Emeritus Department of Radiation Oncology Mallinckrodt Institute of Radiology/
Case Scenario 1. 7/13/12 Anterior floor of mouth biopsy: Infiltrating squamous cell carcinoma, not completely excised.
 Case Scenario 1 7/5/12 History A 51 year old white female presents with a sore area on the floor of her mouth. She claims the area has been sore for several months. She is a current smoker and user of
Case Scenario 1 7/5/12 History A 51 year old white female presents with a sore area on the floor of her mouth. She claims the area has been sore for several months. She is a current smoker and user of
Opportunity for palliative care Research
 Opportunity for palliative care Research Role of Radiotherapy in Multidisciplinary Management of Rectal Cancers Dr Sushmita Pathy Associate Professor Department of Radiation Oncology Dr BRA Institute Rotary
Opportunity for palliative care Research Role of Radiotherapy in Multidisciplinary Management of Rectal Cancers Dr Sushmita Pathy Associate Professor Department of Radiation Oncology Dr BRA Institute Rotary
Recent Advances & Ongoing Challenges in Head & Neck Cancers
 Recent Advances & Ongoing Challenges in Head & Neck Cancers Robert Haddad, MD Disease Center Leader Head and Neck Oncology Program Dana Farber Cancer Institute Harvard Medical School Boston, MA Disclosures
Recent Advances & Ongoing Challenges in Head & Neck Cancers Robert Haddad, MD Disease Center Leader Head and Neck Oncology Program Dana Farber Cancer Institute Harvard Medical School Boston, MA Disclosures
Workshop LA RADIOTERAPIA DEI TUMORI RARI I TIMOMI : INDICAZIONI
 XXI CONGRESSO NAZIONALE AIRO Genova, 19-22 novembre 2011 Workshop LA RADIOTERAPIA DEI TUMORI RARI I TIMOMI : INDICAZIONI PIERA NAVARRIA Unità Operativa di Radioterapia e Radiochirurgia Humanitas Cancer
XXI CONGRESSO NAZIONALE AIRO Genova, 19-22 novembre 2011 Workshop LA RADIOTERAPIA DEI TUMORI RARI I TIMOMI : INDICAZIONI PIERA NAVARRIA Unità Operativa di Radioterapia e Radiochirurgia Humanitas Cancer
Diagnosis and what happens after referral
 Diagnosis and what happens after referral Dr Kate Newbold Consultant in Clinical Oncology The Royal Marsden Women's cancers Breast cancer introduction 1 Treatment Modalities Early stage disease -larynx
Diagnosis and what happens after referral Dr Kate Newbold Consultant in Clinical Oncology The Royal Marsden Women's cancers Breast cancer introduction 1 Treatment Modalities Early stage disease -larynx
From GTV to CTV: A Critical Step Towards Cure. Kenneth Hu, MD Associate Professor New York University Langone Medical Center June 21, 2017
 From GTV to CTV: A Critical Step Towards Cure Kenneth Hu, MD Associate Professor New York University Langone Medical Center June 21, 2017 Head and Neck Cancer Model for Understanding CTV Expansion Radiation
From GTV to CTV: A Critical Step Towards Cure Kenneth Hu, MD Associate Professor New York University Langone Medical Center June 21, 2017 Head and Neck Cancer Model for Understanding CTV Expansion Radiation
CALGB Thoracic Radiotherapy for Limited Stage Small Cell Lung Cancer
 CALGB 30610 Thoracic Radiotherapy for Limited Stage Small Cell Lung Cancer Jeffrey A. Bogart Department of Radiation Oncology Upstate Medical University Syracuse, NY Small Cell Lung Cancer Estimated 33,000
CALGB 30610 Thoracic Radiotherapy for Limited Stage Small Cell Lung Cancer Jeffrey A. Bogart Department of Radiation Oncology Upstate Medical University Syracuse, NY Small Cell Lung Cancer Estimated 33,000
Mini J.Elnaggar M.D. Radiation Oncology Ochsner Medical Center 9/23/2016. Background
 Mini J.Elnaggar M.D. Radiation Oncology Ochsner Medical Center 9/23/2016 Background Mostly adenocarcinoma (scc possible, but treated like anal cancer) 39, 220 cases annually Primary treatment: surgery
Mini J.Elnaggar M.D. Radiation Oncology Ochsner Medical Center 9/23/2016 Background Mostly adenocarcinoma (scc possible, but treated like anal cancer) 39, 220 cases annually Primary treatment: surgery
Case Scenario. 7/13/12 Anterior floor of mouth biopsy: Infiltrating squamous cell carcinoma, not completely excised.
 Case Scenario 7/5/12 History A 51 year old white female presents with a sore area on the floor of her mouth. She claims the area has been sore for several months. She is a current smoker and user of alcohol.
Case Scenario 7/5/12 History A 51 year old white female presents with a sore area on the floor of her mouth. She claims the area has been sore for several months. She is a current smoker and user of alcohol.
Non-surgical treatment for locally advanced head and neck squamous cell carcinoma: beyond the upper limit
 Editorial Non-surgical treatment for locally advanced head and neck squamous cell carcinoma: beyond the upper limit Hiroto Ishiki, Satoru Iwase Department of Palliative Medicine, The Institute of Medical
Editorial Non-surgical treatment for locally advanced head and neck squamous cell carcinoma: beyond the upper limit Hiroto Ishiki, Satoru Iwase Department of Palliative Medicine, The Institute of Medical
Head and Neck Cancer Update Sandro V Porceddu
 Head and Neck Cancer Update Sandro V Porceddu Director, Radiation Oncology Research Princess Alexandra Hospital, Brisbane Associate Professor, University of Queensland President, Trans Tasman Radiation
Head and Neck Cancer Update Sandro V Porceddu Director, Radiation Oncology Research Princess Alexandra Hospital, Brisbane Associate Professor, University of Queensland President, Trans Tasman Radiation
Protons for Head and Neck Cancer. William M Mendenhall, M.D.
 Protons for Head and Neck Cancer William M Mendenhall, M.D. Protons for Head and Neck Cancer Potential Advantages: Reduce late complications via more conformal dose distributions Likely to be the major
Protons for Head and Neck Cancer William M Mendenhall, M.D. Protons for Head and Neck Cancer Potential Advantages: Reduce late complications via more conformal dose distributions Likely to be the major
Vincent Grégoire, Radiation Oncologist, Brussels, Belgium Cai Grau, Radiation Oncologist, Aarhus, Denmark. Tunis March 2017
 Guidelines for the delineation of the primary tumour Clinical Target Volumes (CTV) in laryngeal, hypopharyngeal, oropharyngeal and oral cavity SCC (version 5.1) Vincent Grégoire, Radiation Oncologist,
Guidelines for the delineation of the primary tumour Clinical Target Volumes (CTV) in laryngeal, hypopharyngeal, oropharyngeal and oral cavity SCC (version 5.1) Vincent Grégoire, Radiation Oncologist,
Utilizzo delle tecniche VMAT nei trattamenti del testa collo Marta Scorsetti M.D.
 Utilizzo delle tecniche VMAT nei trattamenti del testa collo Marta Scorsetti M.D. Radiotherapy and Radiosurgery Dpt. Istituto Clinico Humanitas, Milan, Italy. Higher doses to the tumor Better sparing of
Utilizzo delle tecniche VMAT nei trattamenti del testa collo Marta Scorsetti M.D. Radiotherapy and Radiosurgery Dpt. Istituto Clinico Humanitas, Milan, Italy. Higher doses to the tumor Better sparing of
The management of advanced supraglottic and
 ORIGINAL ARTICLE ORGAN PRESERVATION FOR ADVANCED LARYNGEAL CARCINOMA Robert L. Foote, MD, 1 R. Tyler Foote, 1 Paul D. Brown, MD, 1 Yolanda I. Garces, MD, 1 Scott H. Okuno, MD, 2 Scott E. Strome, MD 3 1
ORIGINAL ARTICLE ORGAN PRESERVATION FOR ADVANCED LARYNGEAL CARCINOMA Robert L. Foote, MD, 1 R. Tyler Foote, 1 Paul D. Brown, MD, 1 Yolanda I. Garces, MD, 1 Scott H. Okuno, MD, 2 Scott E. Strome, MD 3 1
Adenoid Cystic Carcinoma Minor Salivary Gland Origin
 Adenoid Cystic Carcinoma Minor Salivary Gland Origin Educational Session Presenter: Smith JA Supervisors: Palme CE, Gupta R Content Case report Imaging Primary Therapy Surgery Adjuvant Therapy Radiotherapy
Adenoid Cystic Carcinoma Minor Salivary Gland Origin Educational Session Presenter: Smith JA Supervisors: Palme CE, Gupta R Content Case report Imaging Primary Therapy Surgery Adjuvant Therapy Radiotherapy
AJCC Cancer Staging 8 th edition. Lip and Oral Cavity Oropharynx (p16 -) and Hypopharynx Larynx
 and Hypopharynx Larynx") AJCC Cancer Staging 8 th edition Lip and Oral Cavity Oropharynx (p16 -) and Hypopharynx Larynx AJCC 7 th edition Lip and Oral cavity Pharynx Larynx KEY CHANGES Skin of head and neck (Vermilion of the lip)
AJCC Cancer Staging 8 th edition Lip and Oral Cavity Oropharynx (p16 -) and Hypopharynx Larynx AJCC 7 th edition Lip and Oral cavity Pharynx Larynx KEY CHANGES Skin of head and neck (Vermilion of the lip)
Combined Modality Therapy State of the Art. Everett E. Vokes The University of Chicago
 Combined Modality Therapy State of the Art Everett E. Vokes The University of Chicago What we Know Some patients are cured (20%) Induction and concurrent chemoradiotherapy are each superior to radiotherapy
Combined Modality Therapy State of the Art Everett E. Vokes The University of Chicago What we Know Some patients are cured (20%) Induction and concurrent chemoradiotherapy are each superior to radiotherapy
Therapy of Locally Advanced Head and Neck Cancer: State of the Art
 Therapy of Locally Advanced Head and Neck Cancer: State of the Art Barbara Burtness, MD Chief, Head and Neck ncology Medical ncology Co-Leader Senior Member Fox Chase Cancer Center Philadelphia, PA Therapy
Therapy of Locally Advanced Head and Neck Cancer: State of the Art Barbara Burtness, MD Chief, Head and Neck ncology Medical ncology Co-Leader Senior Member Fox Chase Cancer Center Philadelphia, PA Therapy
FINE NEEDLE ASPIRATION OF ENLARGED LYMPH NODE: Metastatic squamous cell carcinoma
 Case Scenario 1 HNP: A 70 year old white male presents with dysphagia. The patient is a current smoker, current user of alcohol and is HPV positive. A CT of the Neck showed mass in the left pyriform sinus.
Case Scenario 1 HNP: A 70 year old white male presents with dysphagia. The patient is a current smoker, current user of alcohol and is HPV positive. A CT of the Neck showed mass in the left pyriform sinus.
PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES
 PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES HEAD AND NECK HYPOPHARYNX Head & Neck Site Group Hypopharynx 1. INTRODUCTION 3 2. PREVENTION 3 3. SCREENING AND EARLY DETECTION 3 4. DIAGNOSIS
PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES HEAD AND NECK HYPOPHARYNX Head & Neck Site Group Hypopharynx 1. INTRODUCTION 3 2. PREVENTION 3 3. SCREENING AND EARLY DETECTION 3 4. DIAGNOSIS
Nasopharynx Cancer. 1 Feb Presenters: Dr Raghav Murali-Ganesh (Radiation Oncology Registrar) Dr Peter Luk (Pathology Registrar)
 Dr Peter Luk (Pathology Registrar)") Nasopharynx Cancer 1 Feb 2016 Presenters: Dr Raghav Murali-Ganesh (Radiation Oncology Registrar) Dr Peter Luk (Pathology Registrar) Expert Panels Prof Mo Mo Tin Prof Michael Boyer Dr Raewyn Campbell Prof
Nasopharynx Cancer 1 Feb 2016 Presenters: Dr Raghav Murali-Ganesh (Radiation Oncology Registrar) Dr Peter Luk (Pathology Registrar) Expert Panels Prof Mo Mo Tin Prof Michael Boyer Dr Raewyn Campbell Prof
Anatomy of Head of Neck Cancer
 Anatomy of Head of Neck Cancer J. Robert Newman, MD The ENT Center of Central GA H&N Cancer Overview Most categories of cancer are represented in the H&N Squamous cell carcinoma most common mucosal cancer
Anatomy of Head of Neck Cancer J. Robert Newman, MD The ENT Center of Central GA H&N Cancer Overview Most categories of cancer are represented in the H&N Squamous cell carcinoma most common mucosal cancer
NEOADJUVANT THERAPY IN CARCINOMA STOMACH. Dr Jyotirup Goswami Consultant Radiation Oncologist Narayana Superspeciality Hospital, Howrah
 NEOADJUVANT THERAPY IN CARCINOMA STOMACH Dr Jyotirup Goswami Consultant Radiation Oncologist Narayana Superspeciality Hospital, Howrah NEOADJUVANT THERAPY?! Few believers Limited evidence Many surgeons
NEOADJUVANT THERAPY IN CARCINOMA STOMACH Dr Jyotirup Goswami Consultant Radiation Oncologist Narayana Superspeciality Hospital, Howrah NEOADJUVANT THERAPY?! Few believers Limited evidence Many surgeons
The Integration and Impact of Modern Radiotherapy Techniques in Clinical Practice. Kian Ang
 The Integration and Impact of Modern Radiotherapy Techniques in Clinical Practice Kian Ang Funding: P01-CA06294, R01-CA84415, GF Fletcher Chair, Imclone (phase III trial) From Bench to Bedside Head and
The Integration and Impact of Modern Radiotherapy Techniques in Clinical Practice Kian Ang Funding: P01-CA06294, R01-CA84415, GF Fletcher Chair, Imclone (phase III trial) From Bench to Bedside Head and
Clinical Case Conference Melanoma
 Clinical Case Conference Melanoma Epidemiology ~60,000 cases and 8,000 deaths per year in US Caucasian:African American = 10:1 15% arise from existing nevi 91% are cutaneous 15% are LN+ at presentation
Clinical Case Conference Melanoma Epidemiology ~60,000 cases and 8,000 deaths per year in US Caucasian:African American = 10:1 15% arise from existing nevi 91% are cutaneous 15% are LN+ at presentation
State of the Art: Management of Squamous Cell Carcinoma of the Head and Neck. Raul Giglio
 State of the Art: Management of Squamous Cell Carcinoma of the Head and Neck Raul Giglio Disclosures Nothing to disclose SCCHN Outline 1. General considerations: MTD 2. Epidemiology 3. Locoregional disease
State of the Art: Management of Squamous Cell Carcinoma of the Head and Neck Raul Giglio Disclosures Nothing to disclose SCCHN Outline 1. General considerations: MTD 2. Epidemiology 3. Locoregional disease
IMRT - the physician s eye-view. Cinzia Iotti Department of Radiation Oncology S.Maria Nuova Hospital Reggio Emilia
 IMRT - the physician s eye-view Cinzia Iotti Department of Radiation Oncology S.Maria Nuova Hospital Reggio Emilia The goals of cancer therapy Local control Survival Functional status Quality of life Causes
IMRT - the physician s eye-view Cinzia Iotti Department of Radiation Oncology S.Maria Nuova Hospital Reggio Emilia The goals of cancer therapy Local control Survival Functional status Quality of life Causes
Accepted 28 April 2005 Published online 13 September 2005 in Wiley InterScience ( DOI: /hed.
 DEFINING RISK LEVELS IN LOCALLY ADVANCED HEAD AND NECK CANCERS: A COMPARATIVE ANALYSIS OF CONCURRENT POSTOPERATIVE RADIATION PLUS CHEMOTHERAPY TRIALS OF THE EORTC (#22931) AND RTOG (#9501) Jacques Bernier,
DEFINING RISK LEVELS IN LOCALLY ADVANCED HEAD AND NECK CANCERS: A COMPARATIVE ANALYSIS OF CONCURRENT POSTOPERATIVE RADIATION PLUS CHEMOTHERAPY TRIALS OF THE EORTC (#22931) AND RTOG (#9501) Jacques Bernier,
New Paradigms for Treatment of. Erminia Massarelli, MD, PHD, MS Clinical Associate Professor
 New Paradigms for Treatment of Head and Neck cancers Erminia Massarelli, MD, PHD, MS Clinical Associate Professor City of Hope Disclosure Statement Grant/Research Support frommerck Bristol Grant/Research
New Paradigms for Treatment of Head and Neck cancers Erminia Massarelli, MD, PHD, MS Clinical Associate Professor City of Hope Disclosure Statement Grant/Research Support frommerck Bristol Grant/Research
Comparing Alternative treatment Regimens for intermediate and high risk oropharyngeal cancer CompARE. Prof. Hisham Mehanna.
 Comparing Alternative treatment Regimens for intermediate and high risk oropharyngeal cancer CompARE Prof. Hisham Mehanna Chief investigator: Hisham Mehanna Arm 1: Mehmet Sen Arm2: John Chester/Martin
Comparing Alternative treatment Regimens for intermediate and high risk oropharyngeal cancer CompARE Prof. Hisham Mehanna Chief investigator: Hisham Mehanna Arm 1: Mehmet Sen Arm2: John Chester/Martin
Protocol of Radiotherapy for Small Cell Lung Cancer
 107 年 12 月修訂 Protocol of Radiotherapy for Small Cell Lung Cancer Indication of radiotherapy Limited stage: AJCC (8th edition) stage I-III (T any, N any, M0) that can be safely treated with definitive RT
107 年 12 月修訂 Protocol of Radiotherapy for Small Cell Lung Cancer Indication of radiotherapy Limited stage: AJCC (8th edition) stage I-III (T any, N any, M0) that can be safely treated with definitive RT
ORIGINAL ARTICLE CHEMOTHERAPY ALONE FOR ORGAN PRESERVATION IN ADVANCED LARYNGEAL CANCER
 ORIGINAL ARTICLE CHEMOTHERAPY ALONE FOR ORGAN PRESERVATION IN ADVANCED LARYNGEAL CANCER Vasu Divi, MD, 1 * Francis P. Worden, MD, 1,2 * Mark E. Prince, MD, 1 Avraham Eisbruch, MD, 3 Julia S. Lee, MD, 4
ORIGINAL ARTICLE CHEMOTHERAPY ALONE FOR ORGAN PRESERVATION IN ADVANCED LARYNGEAL CANCER Vasu Divi, MD, 1 * Francis P. Worden, MD, 1,2 * Mark E. Prince, MD, 1 Avraham Eisbruch, MD, 3 Julia S. Lee, MD, 4
Surgical Margins in Transoral Robotic Surgery for Oropharyngeal Squamous Cell Carcinoma
 Surgical Margins in Transoral Robotic Surgery for Oropharyngeal Squamous Cell Carcinoma Consensus update and recommendations, 2018 Head and Neck Steering Committee P. Gorphe *, F. Nguyen, Y. Tao, P. Blanchard,
Surgical Margins in Transoral Robotic Surgery for Oropharyngeal Squamous Cell Carcinoma Consensus update and recommendations, 2018 Head and Neck Steering Committee P. Gorphe *, F. Nguyen, Y. Tao, P. Blanchard,
Tristate Lung Meeting 2014 Pro-Con Debate: Surgery has no role in the management of certain subsets of N2 disease
 Tristate Lung Meeting 2014 Pro-Con Debate: Surgery has no role in the management of certain subsets of N2 disease Jennifer E. Tseng, MD UFHealth Cancer Center-Orlando Health Sep 12, 2014 Background Approximately
Tristate Lung Meeting 2014 Pro-Con Debate: Surgery has no role in the management of certain subsets of N2 disease Jennifer E. Tseng, MD UFHealth Cancer Center-Orlando Health Sep 12, 2014 Background Approximately
Gastroesophag Gastroesopha eal Junction Adenocarcinoma: What is the best adjuvant regimen? Michael G. G. H addock Haddock M.D.
 Gastroesophageal Junction Adenocarcinoma: What is the best adjuvant regimen? Michael G. Haddock M.D. Mayo Clinic Rochester, MN Locally Advanced GE Junction ACA CT S CT or CT S CT/RT Proposition Chemoradiation
Gastroesophageal Junction Adenocarcinoma: What is the best adjuvant regimen? Michael G. Haddock M.D. Mayo Clinic Rochester, MN Locally Advanced GE Junction ACA CT S CT or CT S CT/RT Proposition Chemoradiation
Neck Imaging Reporting and Data System: An Atlas of NI-RADS Categories for Head and Neck Cancer
 Neck Imaging Reporting and Data System: An Atlas of NI-RADS Categories for Head and Neck Cancer Bethany Cavazuti Patricia Hudgins Tanya Rath Char Branstetter Kristen Baugnon Amanda Corey Ashley Aiken Disclosures
Neck Imaging Reporting and Data System: An Atlas of NI-RADS Categories for Head and Neck Cancer Bethany Cavazuti Patricia Hudgins Tanya Rath Char Branstetter Kristen Baugnon Amanda Corey Ashley Aiken Disclosures
Heterogeneity of N2 disease
 Locally Advanced NSCLC Surgery? No. Ramaswamy Govindan M.D Co-Director, Section of Medical Oncology Alvin J Siteman Cancer Center at Washington University School of Medicine St. Louis, Missouri Heterogeneity
Locally Advanced NSCLC Surgery? No. Ramaswamy Govindan M.D Co-Director, Section of Medical Oncology Alvin J Siteman Cancer Center at Washington University School of Medicine St. Louis, Missouri Heterogeneity